USCAP 2013: THE ORIGINS OF OVARIAN CANCER: MUCINOUS TUMORS
|
|
|
- Michael George
- 5 years ago
- Views:
Transcription
1 USCAP 2013: THE ORIGINS OF OVARIAN CANCER: MUCINOUS TUMORS Russell Vang, M.D. Associate Professor Division of Gynecologic Pathology The Johns Hopkins Hospital Table of contents: Powerpoint handout Text handout: Mucinous Tumors Arising in Mature Cystic Teratoma Text handout: Distinction of Primary Ovarian Mucinous Tumors from Mucinous Tumors Secondarily Involving the

2 2/5/2013 Mucinous Tumors in the THE ORIGINS OF OVARIAN CANCER: MUCINOUS TUMORS Primary Gastrointestinal type Primary Seromucinous type Russell Vang, M.D. Associate Professor Div. of GYN Pathology The Johns Hopkins Hospital Secondary origin Mucinous Tumors in the Other Than Primary Gastrointestinal Type Primary Seromucinous type: Precursor: Endometriosis ARID1A mutations Secondary origin: 2 main groups: Metastatic mucinous carcinoma (GI tract, pancreaticobiliary region, endocervix) Secondary involvement in PMP (low-grade adenomatous mucinous neoplasm of appendix) Ability to simulate primary ovarian tumors (carcinoma, borderline tumor, cystadenoma) Potential for misclassification Pathogenesis of Primary Ovarian Gastrointestinal type Mucinous Tumors Surface epithelial type Teratoma-associated Pathogenesis of Surface Epithelial Type Mucinous Tumors Surface Epithelial Type Mucinous Tumors Upper GI differentiation: Morphology: Resembles gastric foveolar epithelium Immunohistochemistry: CK7-diffuse/CK20-variable (CK7 > CK20) W.H.O. Classification: Cystadenoma Borderline tumor (atypical proliferative, low malignant potential) Carcinoma Ovarian mucinous cystadenoma 1



3 2/5/2013 Pathogenesis of Surface Epithelial Type Mucinous Tumors Type I pathway (dualistic model of pathogenesis): Cystadenoma Borderline tumor Invasive carcinoma Morphologic evidence: Cystadenomas with focal epithelial proliferation Borderline tumors: Within background of cystadenoma With intraepithelial carcinoma With microinvasion Invasive carcinomas within background of borderline tumor Tumors with admixed cystadenoma, borderline tumor, and invasive carcinoma Pathogenesis of Surface Epithelial Type Mucinous Tumors Molecular evidence: Cuatrecasas, Cancer 1997: KRAS mutations in intestinal type ovarian mucinous tumors: Cystadenoma Borderline tumor Carcinoma 62% 83% 100% Tumors with different components: Same mutations in cystadenoma + borderline tumor Same mutations in borderline tumor + carcinoma Conclusion: KRAS mutation is early event Mucinous Cystadenoma Mucinous Borderline Tumor Invasive Well-differentiated Mucinous Carcinoma (Confluent Pattern) Pathogenesis of Surface Epithelial Type Mucinous Tumors Progression pathway well accepted Precursors of mucinous cystadenoma?: No normal mucinous component in non-neoplastic ovary Metaplasia?: Ovarian surface epithelium/epithelial inclusion glands mucinous metaplasia neoplastic transformation Mucinous metaplasia would be rare in the ovary Endometriosis? May show mucinous metaplasia Significant association of endometriosis is with clear cell and endometrioid tumors- not mucinous tumors Exception: Seromucinous tumors evolve from endometriosis No definitive evidence of etiology for gastrointestinal type tumors 2
 Brenner tumors may exhibit mucinous differentiation (metaplastic")

 Precursors of Mucinous Cystadenoma? Brenner tumors?")

4 2/5/2013 Precursors of Mucinous Cystadenoma? Brenner tumors?: Known association of mucinous tumors and Brenner tumors (mixed Brenner-mucinous tumor) Brenner tumors may exhibit mucinous differentiation (metaplastic Brenner tumor) Seidman, Arch Pathol Lab Med 2008: Consecutive benign ovarian tumors with mucinous and/or transitional cell components 25% mucinous tumors contained component of Brenner tumor Walthard nests associated with 59% mucinous tumors vs. 28% controls (p<0.001) Type of calcifications in mucinous tumors identical to those in Brenner tumors (spiculated) Precursors of Mucinous Cystadenoma? Brenner tumors?: Seidman, Arch Pathol Lab Med 2008: Proposal: Origin of mucinous tumors from Brenner tumors/walthard nests: Brenner tumor mucinous component undergoes neoplastic transformation mucinous tumor overgrows Brenner component Molecular evidence: Limited data in literature Pejovic, Gynecol Oncol 1999: Case report: Ovarian mucinous carcinoma associated with benign Brenner tumor CGH analysis: Amplification of 12q14-21 in both components Suggest clonal relationship Mucinous cystadenoma arising within Brenner tumor Mucinous cystadenoma arising within Brenner tumor Mucinous cystadenoma arising within Brenner tumor Mucinous cystadenoma arising within Brenner tumor 3



5 2/5/2013 Mucinous cystadenoma arising within Brenner tumor Mucinous cystadenoma arising within Brenner tumor Mucinous cystadenoma arising within Brenner tumor Pathogenesis of GI Type Surface Epithelial Mucinous Tumors Conclusions: Origin from Brenner tumors: A plausible concept An identifiable source of mucinous differentiation Other proposed origins: Limited convincing evidence Pathogenesis of GI Type Surface Epithelial Mucinous Tumors Conclusions: Origin from Brenner tumors: Brenner origin represents at least 1 pathway Question: Are all GI type surface epithelial mucinous tumors of Brenner origin? Not all mucinous tumors have a Brenner component:» Overgrowth of Brenner component?» Non-Brenner pathways exist? Further investigation warranted Teratoma-associated Mucinous Tumors 4

: Histologic patterns: Cystadenomatous Proliferative: Resemble villous adenomas of lower")
6 2/5/2013 Pathogenesis of Primary Ovarian Mucinous Tumors: Germ Cell (Teratomatous) Origin? Known association between ovarian teratomas and mucinous tumors: Teratomas: 2-11% contain mucinous tumors Mucinous tumors: 3-8% contain teratomas Mucinous tissues within teratomas: Colon Appendix Respiratory epithelium Upper GI tract Proposal: Mucinous tumors may arise from teratomas Other somatic type tumors arising from teratomas: Thyroid tissue Papillary thyroid carcinoma Squamous epithelium Squamous cell carcinoma Mucinous Tumors Associated With Teratomas Vang, Am J Surg Pathol 2007 (n=44): Histologic patterns: Cystadenomatous Proliferative: Resemble villous adenomas of lower GI tract (particularly, appendix) Resemble borderline tumors of surface epithelial type Goblet cell carcinoid Carcinomatous: Confluent glandular/villoglandular Infiltrative, including signet ring cell carcinoma Mucinous Tumors Associated With Teratomas Vang, Am J Surg Pathol 2007 (n=44): +/- Abundant hypermucinous epithelium with goblet cells Pseudomyxoma ovarii (48%): Tumors resemble lower GI low-grade adenomatous neoplasms +/- Pseudomyxoma peritonei: Exception to primary appendiceal origin Mucinous Tumors Associated With Teratomas Vang, Am J Surg Pathol 2007 (n=44): Immunohistochemistry: All possible CK7/CK20 coordinate profiles 53% showed lower GI immunophenotype: CK7(-)/CK20(+) CK7-focal/CK20-diffuse Significant association of pseudomyxoma ovarii with CK7(-)/CK20(+) Similar morphologic & IHC findings: McKenney, Am J Surg Pathol 2008 (n=42) Teratoma-associated: Resembles Low-grade Adenomatous Mucinous Neoplasm of Appendix Teratoma-associated: Resembles Low-grade Adenomatous Mucinous Neoplasm of Appendix 5




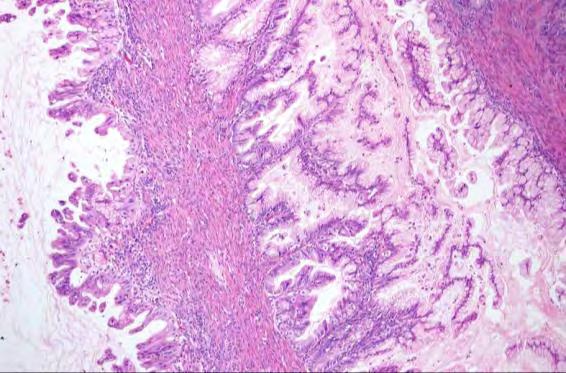
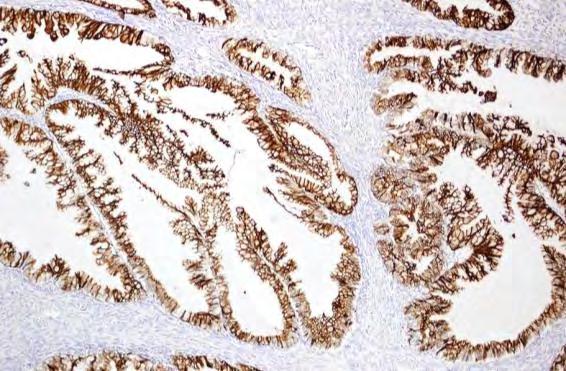
7 2/5/2013 Teratoma-associated: Resembles Low-grade Adenomatous Mucinous Neoplasm of Appendix Teratoma-associated: Resembles Low-grade Adenomatous Mucinous Neoplasm of Appendix CK7 Teratoma-associated: Resembles Low-grade Adenomatous Mucinous Neoplasm of Appendix Teratoma-associated: Resembles Mucinous Borderline Tumor of Surface Epithelial Type CK20 Teratoma-associated: Resembles Mucinous Borderline Tumor of Surface Epithelial Type Teratoma-associated: Resembles Mucinous Borderline Tumor of Surface Epithelial Type CK7 6



: Generally young age Presence of teratoma in all cases Unilateral")
 Clinical work-up, gross sampling of appendix, follow-up: No evidence of")
8 2/5/2013 Teratoma-associated: Resembles Mucinous Borderline Tumor of Surface Epithelial Type Teratoma-associated Goblet Cell Carcinoid CK20 Teratoma-associated Invasive Well-differentiated Mucinous Carcinoma with Pseudomyxoma Ovarii Teratoma-associated Invasive Well-differentiated Mucinous Carcinoma with Pseudomyxoma Ovarii Teratoma-associated Signet Ring Cell Carcinoma Mucinous Tumors Associated With Teratomas H&E + IHC: Many resemble lower GI tumors of the type more commonly encountered as secondary involvement in the ovary Are not just tumor-to-tumor metastases: Clinicopathologic features c/w primary ovarian origin (JHH + Stanford studies): Generally young age Presence of teratoma in all cases Unilateral Large Lack other typical histologic features favoring metastases (surface tumor, nodularity, LVSI/tumor in hilum) Clinical work-up, gross sampling of appendix, follow-up: No evidence of primary non-ovarian tumor 7
9 2/5/2013 Lower GI type Mucinous Tumors Arising From Teratomas Teratomatous elements may be focal Teratomatous elements may not be found initially (for cases w/o evidence of non-ovarian primary): May represent tumor overgrowth Additional gross sampling necessary Regardless of teratomatous elements: Comment section of pathology report: Secondary involvement should be clinically excluded Mucinous Tumors Associated With Teratomas Molecular evidence: Limited data in literature Magi-Galluzi, Mod Pathol 2001 (140A): PCR of microsatellite polymorphisms on different chromosomes: Ovarian mucinous cystadenomas associated with teratomas Ovarian mucinous cystadenomas without teratomas Conclusion: Mucinous cystadenomas associated with teratomas are of germ cell origin Conclusions: Mucinous Tumors Associated With Teratomas Those resembling lower GI tumors: Morphology & IHC distinct from surface epithelial type mucinous tumors Pathogenesis independent of pathway for surface epithelial tumors (i.e., germ cell origin) Importance of Dx: Misclassification as secondary involvement Conclusions: Mucinous Tumors Associated With Teratomas Those resembling surface epithelial tumors: Morphologic + IHC features identical to mucinous tumors w/o teratomas Collision tumors? Germ cell origin?: Upper GI tissues and respiratory epithelium in teratomas Morphology & IHC of surface epithelial type mucinous tumors c/w upper GI differentiation Surface epithelial mucinous tumors w/o Brenner tumor component: Monodermal teratoma? Further study warranted Pathogenesis of Primary Ovarian Gastrointestinal Type Mucinous Tumors Brenner tumor Metaplasia Mucinous tumors resembling Surface Epithelial type Cystadenoma Borderline tumor Invasive carcinoma Endometriosis???? Teratoma Upper GI/ pancreaticobiliary/ sinonasal elements Colorectal/ appendiceal elements Mucinous tumors resembling Lower GI types Low-grade adenomatous tumors Goblet cell carcinoid Invasive carcinoma: Often w/ pseudomyxoma ovarii +/- Signet ring cell CA component THE ORIGINS OF OVARIAN CANCER: MUCINOUS TUMORS Russell Vang, M.D. Associate Professor Div. of GYN Pathology The Johns Hopkins Hospital 8
10 Mucinous Tumors Arising in Mature Cystic Teratoma SUPPLEMENTAL INFORMATION: Mucinous Tumors Arising in Mature Cystic Teratoma Microscopic Features Primary ovarian mucinous tumors associated with a mature cystic teratoma show a spectrum of histologic appearances. 1,2 At the lower end of the spectrum, tumors display a cystadenomatous pattern. Proliferative tumors with architectural complexity and epithelial stratification resemble atypical proliferative (borderline) mucinous tumor of ovarian surface epithelial origin or low-grade adenomatous mucinous neoplasm of the appendix. Pseudomyxoma ovarii can be seen with some cystadenomatous and proliferative neoplasms. Compared to tumors without pseudomyxoma ovarii, neoplasms with pseudomyxoma ovarii more closely resemble lower gastrointestinal tract adenomatous tumors and tend to have hypermucinous columnar epithelium and abundant goblet cells. Other tumors may show goblet cell carcinoid-like morphology. At the upper end of the spectrum, the carcinomatous neoplasms may be of glandular or signet ring cell type. Pseudomyxoma ovarii can also be associated with goblet cell carcinoid-like tumors or carcinoma. Immunohistochemical Features and Differential Diagnosis Immunohistochemical stains for CK7 and CK20 show variable coordinate expression profiles. 2 Tumors without pseudomyxoma ovarii and having cystadenomatous or proliferative patterns show a variety of CK7/CK20 profiles, including a CK7 diffuse/ck20 variable pattern (a pattern frequently seen in ovarian surface epithelial tumors). Those with pseudomyxoma ovarii and having cystadenomatous, proliferative, or goblet cell carcinoid-like patterns characteristically display a CK7(-)/CK20 diffuse or CK7 focal/ck20 diffuse profile (patterns typical of lower gastrointestinal tract tumors). A minority of these tumors histologically and immunohistochemically resembling lower gastrointestinal tract adenomatous tumors can have the clinical syndrome of pseudomyxoma peritonei without a tumor in the appendix. Parenthetically, it should be emphasized that although nearly all cases of pseudomyxoma peritonei are of appendiceal origin, rare cases are of primary ovarian origin due to an appendiceal-type mucinous tumor arising within a mature cystic teratoma. The carcinomas can have variable CK7/CK20 profiles, but some will show a CK7(-)/CK20 diffuse or CK7 focal/ck20 diffuse pattern. Ovarian mucinous tumors of germ cell origin with histologic and immunohistochemical features typical of primary lower gastrointestinal tract tumors can be misclassified as metastatic or secondary tumors involving the ovary. Thus, it is important to search for focal teratomatous components in such ovarian mucinous tumors in order to suggest a possible primary ovarian origin. Nonetheless, when problematic mucinous neoplasms in ovarian mature cystic teratomas histologically and immunohistochemically resemble lower gastrointestinal tract tumors, extensive sampling of the gross specimen and further clinical evaluation to exclude the rare possibility of a similar primary mucinous tumor in the appendix or colorectal region as part of a tumor-to-tumor metastasis (e.g., a primary lower gastrointestinal tract tumor with a metastasis to a co-existing ovarian teratoma) are recommended. Primary ovarian mucinous tumors arising in a teratoma which histologically and immunohistochemically resemble lower gastrointestinal tumors are considered to be of germ cell origin. Tumors that are histologically and immunohistochemically analogous to ovarian surface 1
11 Mucinous Tumors Arising in Mature Cystic Teratoma epithelial mucinous cystadenoma or atypical proliferative (borderline) mucinous tumor may have developed in the same ovary containing a teratoma as an independent tumor; however, it should also be considered that some of those mucinous tumors could be of germ cell origin as it is possible that they arose from upper gastrointestinal/pancreaticobiliary or sinonasal tissue in a teratoma, which would have histologic and immunohistochemical features similar to mucinous tumors of ovarian surface epithelial origin. Nomenclature For primary ovarian mucinous tumors histologically and immunohistochemically resembling lower gastrointestinal tract tumors, descriptive terminology that parallels the nomenclature for tumors in lower gastrointestinal sites (e.g., low-grade adenomatous mucinous neoplasm for ovarian tumors histologically and immunohistochemically analogous to those of the appendix) is preferred, considering that (a) terms such as borderline tumor or atypical proliferative tumor are used for surface epithelial tumors of the ovary, (b) these mucinous tumors are of germ cell rather than surface epithelial origin, and (c) they resemble their counterparts in the lower gastrointestinal tract. Clinical Behavior and Treatment Data on the behavior of mucinous ovarian tumors of germ cell origin are limited, but in the series of McKenney et al and Vang et al, patients with cystadenomatous and proliferative/low malignant potential tumors on follow-up remained well and disease-free. 1,2 For ruptured primary ovarian mucinous tumors (with pseudomyxoma ovarii) which are the histologic and immunohistochemical counterpart of appendiceal low-grade adenomatous mucinous neoplasms, patients are at risk for the development of the clinical syndrome of pseudomyxoma peritonei, and further clinical evaluation and follow-up are prudent. In the two series mentioned above, mucinous carcinomas showed variable outcome but exhibited the potential for aggressive behavior. REFERENCES 1. McKenney JK, Soslow RA, Longacre TA. Ovarian mature teratomas with mucinous epithelial neoplasms: morphologic heterogeneity and association with pseudomyxoma peritonei. Am J Surg Pathol 2008;32: Vang R, Gown AM, Zhao C, et al. Ovarian mucinous tumors associated with mature cystic teratoma. Morphologic and immunohistochemical analysis identifies a subset of potential teratomatous origin that shares features of lower gastrointestinal tract mucinous tumors more commonly encountered as secondary tumors of the ovary. Am J Surg Pathol 2007;31:
12 SUPPLEMENTAL INFORMATION: Distinction of Primary Ovarian Mucinous Tumors from Mucinous Tumors Secondarily Involving the General Features Of Metastases Involving The Ovaries Metastatic neoplasms involving the ovaries account for approximately 8% of malignant ovarian neoplasms in women undergoing surgery for an ovarian mass in the United States. Metastases derived from non-gynecologic sites are 11 times more common than those derived from female genital tract organs, with adenocarcinomas of gastrointestinal tract origin representing the most common type; however, a substantial number of metastases in the ovaries are of unknown origin. 1-4 Metastases in the ovaries can present synchronously or metachronously with the primary neoplasm. Those presenting metachronously can do so subsequent to or prior to the diagnosis of the primary tumor. In the former situation, the diagnosis of an ovarian metastasis often is not difficult, particularly when the history of a prior non-ovarian malignant neoplasm is known to the pathologist and additional sites are involved by metastatic disease. In contrast, the latter scenario often poses a diagnostic challenge, particularly when metastatic disease appears to be confined to the ovaries and other characteristic features of metastatic disease in the ovaries are lacking. In exceptional cases, the primary site may not be identified until months or even years later. Thus, the typical, readily recognized ovarian metastasis presents as multifocal tumor in the setting of a known nonovarian primary malignant neoplasm, but in some cases an ovarian mass can represent the first manifestation of metastatic disease from a clinically occult non-ovarian primary malignant neoplasm. On occasion, metastatic neoplasms can cause virilization, simulating a primary ovarian sex cord-stromal neoplasm. While relatively rare, this phenomenon is most frequently encountered with metastatic mucinous carcinomas, and the women can be relatively young and sometimes present during pregnancy. Metastases in the ovaries are readily recognized as such, even when another primary site has not been identified or is identified concurrently with the ovarian tumor, when they exhibit characteristic gross and microscopic features. Characteristic gross features of metastases in the ovaries include smaller size (often less than 10 cm), bilateral involvement, a nodular growth pattern, and presence of tumor on the surface and/or in the superficial cortex of the ovary. Nodular tumors typically are solid and compress the surrounding ovarian stroma. Characteristic microscopic features of metastases include an infiltrative growth pattern with stromal desmoplasia, a nodular growth pattern with involvement of the ovarian surface and superficial cortex, and hilar and lymph-vascular space involvement. The presence of signet ring cells almost invariably indicates metastatic carcinoma of gastrointestinal tract or breast origin although rare primary ovarian epithelial tumors with a component of signet ring cells without teratomatous elements have been reported. 5,6 It should be noted, however, that primary ovarian carcinomas with a pure component of signet ring cell carcinoma probably represent tumors of germ cell origin in which the teratomatous components were overgrown by carcinoma. Certain other histologic features are characteristic of particular types of metastatic carcinomas, such as a garland pattern of epithelium draped along the periphery 1
13 of zones of so-called dirty necrosis in metastatic colorectal carcinoma. It should be emphasized that none of these individual features are pathognomonic and metastases are most easily recognized when a combination of features is present. 7,8 In addition, certain microscopic features that might suggest origin of a neoplasm in the ovary are actually non-specific and can be seen in metastatic carcinomas. These include the finding of histologically benign-appearing and low-grade proliferative (cystadenomatous and atypical proliferative [borderline] type) mucinous epithelium in metastatic pancreatic, colorectal, and endocervical mucinous carcinomas, and stromal luteinization. It is important to note that some metastases lack characteristic features of metastatic disease and share clinical, gross, and microscopic features with primary ovarian neoplasms. Thus, an ovarian mass involved by metastatic carcinoma can represent the initial clinical manifestation of disease, leading to surgical exploration by a gynecologist or gynecologic oncologist for a presumptive diagnosis of ovarian cancer. Occasionally, the ovarian tumor can be large, unilateral, and multicystic with a smooth surface, suggesting a clinical stage I primary ovarian neoplasm. These deceptive metastatic carcinomas can grow in confluent glandular/expansile or villoglandular patterns, without infiltrative growth, simulating primary ovarian atypical proliferative (borderline) tumors with intraepithelial carcinoma and well-differentiated carcinomas not only at the time of intraoperative consultation but also when examining multiple permanent sections. Thus, recognition of these neoplasms as metastases can be exceedingly difficult, particularly when the primary site has not been identified, and ancillary techniques are often required to establish the correct diagnosis. The distinction of primary and metastatic ovarian neoplasms is further complicated by the known occurrence of synchronous independent ovarian and non-ovarian neoplasms having similar histologic features. This situation usually involves synchronous endometrial and ovarian endometrioid tumors associated with endometriosis, in which the neoplasms are likely independent. However, in other situations, such as synchronous and metachronous ovarian and endocervical endometrioid and mucinous tumors, ancillary tests have provided evidence that the ovarian neoplasms are metastatic despite the presence of clinical, gross, and microscopic features suggesting the ovarian tumors are independent. Features Characteristic of Metastases to the : Bilateral involvement Size < 10 cm Surface and/or superficial cortical involvement Infiltrative growth pattern with stromal desmoplasia Nodular growth pattern Signet ring cell component Hilar involvement or lymph-vascular space invasion Known history of non-ovarian primary tumor 2
14 Pathologic And Immunohistochemical Features Of Primary Ovarian Mucinous Tumors: Atypical proliferative (borderline) mucinous tumors of gastrointestinal type and mucinous carcinomas 9-23 Both types of primary ovarian mucinous tumors are usually stage I unilateral tumors and typically larger than 10 cm, with most reported mean sizes for atypical proliferative tumors ranging from 19 to 22 cm and for carcinomas, 18 to 21 cm. The external surfaces are usually smooth, and the cut surface is multicystic. The cysts are often filled with mucinous material or fluid, and internal surfaces are generally smooth, typically without grossly evident papillations. Solid areas are occasionally encountered, more often in carcinomas than in atypical proliferative tumors. Microscopically, the atypical proliferative tumors form complex organized cysts having basal/peripheral crypts and luminal differentiated villous structures lined by gastrointestinal-type mucinous epithelium with variable numbers of goblet cells. The epithelium typically most closely resembles gastric foveolar-type mucosa. Nuclear atypia generally ranges from mild to moderate, with enlarged, reactive-appearing nuclei and proliferative activity generally restricted to the crypts. The presence of marked nuclear atypia qualifies a tumor for a diagnosis of intraepithelial carcinoma. The carcinomas most often exhibit an exaggerated atypical proliferative growth pattern in which the glandular epithelium of the cysts is sufficiently crowded to form a confluent glandular/cribriform pattern. The complex, confluent labyrinthine growth pattern of the epithelium imparts an expansile rather than infiltrative appearance to the tumor. Some mucinous carcinomas exhibit destructive, infiltrative growth, but this pattern should raise concern for the possibility of a metastasis, especially when bilateral involvement and extra-ovarian disease are present. Primary ovarian mucinous tumors typically exhibit diffuse expression of cytokeratin 7 (CK7). Expression of cytokeratin 20 (CK20) is variable, ranging from negative to multifocal positivity with patchy areas of negative epithelium. The only exception to this pattern is the mucinous tumors arising in ovarian mature cystic teratomas, which exhibit a lower gastrointestinal tract type immunoprofile (CK7- negative, CK20 diffusely positive) [also, see other handout on mucinous tumors arising in mature cystic teratoma]. Primary ovarian mucinous tumors retain expression of Dpc4 and lack expression of hormone receptors (estrogen [ER] and progesterone receptors [PR]). Features Characteristic of Primary Ovarian Tumors: Unilateral involvement Size > 10 cm Lack of surface and/or superficial cortical involvement Lack of nodularity 3
15 Features Shared by Primary Ovarian Tumors and Metastases to the : Cyst formation Areas of microscopic low-grade tumor suggesting a primary ovarian precursor lesion Necrosis Stromal luteinization Guidelines For Distinguishing Primary Ovarian Mucinous Tumors From Mucinous Tumors Secondarily Involving The And For Predicting Primary Site For Metastatic Carcinomas Of Unknown Origin 7,8,10,13,14,16,17,19-39 Intraoperative consultation The first step in evaluating mucinous tumors involving the ovaries is to assess gross and microscopic features, along with any available clinical information, to determine whether the tumor is likely primary or could be metastatic. This is often done at the time of intraoperative consultation under less than ideal circumstances. Frozen section diagnosis of mucinous tumors is challenging for several reasons. These include sampling limitations (it is generally not practical to examine more than one or two sections, yet tumors are frequently heterogeneous) and the aforementioned ability of metastases to simulate primary ovarian tumors. In addition, there is often pressure to render a definitive diagnosis to guide surgical staging decisions. Ideally, in the absence of prior relevant specimens in the pathology laboratory database, the pathologist should ask the surgeon whether the patient has had any other documented tumors. Regardless of the patient s history, the pathologist should also ask whether the ovarian involvement is unilateral or bilateral and if there is any evidence of extra-ovarian disease. In some cases, the features will be sufficiently characteristic to allow for confident diagnosis of a tumor as primary or metastatic. Combined assessment of just size and laterality of mucinous carcinomas is quite useful for predicting whether a tumor is primary or metastatic, but evaluation of morphologic features as part of the diagnostic algorithm is equally important. Not infrequently, however, definitive diagnosis at the time of intraoperative consultation is not possible. The phrasing used to report frozen section diagnoses for difficult mucinous tumors will depend on a variety of factors, including the pathologist s diagnostic impression, degree of certainty regarding that impression, and the needs of the surgeon. Certain intraoperative findings and gross or microscopic features should prompt additional communication between the pathologist and surgeon. The presence of extraovarian disease, bilateral tumor, gross or microscopic nodularity, garland pattern necrosis, or signet ring cells should prompt the pathologist to recommend evaluation of the gastrointestinal tract, the most common source of metastatic mucinous carcinomas in the ovary. The finding of mucinous ascites (pseudomyxoma peritonei) should prompt the surgeon to evaluate and remove the appendix. It is important for both pathologists and surgeons to realize that some mucinous tumors require not only multiple permanent sections but also ancillary diagnostic tests (immunohistochemistry, further clinical evaluation with imaging studies) for definitive diagnosis. 4
16 Synthesis of microscopic findings and immunohistochemical profiles The following summary discussion is intended to provide guidelines for synthesizing particular combinations of microscopic patterns and immunohistochemical profiles to suggest likely primary sites for mucinous tumors suspected to be metastatic from undiagnosed primary neoplasms. A variety of glandular patterns and degrees of mucinous differentiation can be seen in metastatic mucinous carcinomas from different primary sites. Tumors with columnar epithelium exhibiting combined or hybrid mucinous and endometrioid-like differentiation suggest metastatic colorectal or endocervical adenocarcinoma whereas well-differentiated overtly mucinous glands with a more cuboidal appearance suggest metastatic pancreaticobiliary adenocarcinoma. Tumors producing abundant extracellular mucin can be derived from several sites, but those of appendiceal and colorectal origin are most common. Of these, those containing only low-grade adenomatous mucinous epithelium are virtually always of appendiceal origin and are associated with the syndrome of pseudomyxoma peritonei (mucinous ascites). Those containing carcinomatous mucinous epithelium are also commonly of appendiceal origin but also can be of colorectal, pancreatic, endocervical, or gastric origin. Those having a significant signet ring cell component are most often of appendiceal or gastric origin. Primary ovarian mucinous tumors with abundant extracellular mucin production are distinctly unusual and include the rare mucinous tumors arising in ovarian mature cystic teratomas. The morphologic patterns can be used in isolation to suggest a potential primary site of origin for a given metastatic carcinoma, but evaluation in conjunction with selected immunohistochemical markers can provide additional discriminating information: 5
17 Diagnostic algorithm for ovarian mucinous tumors with glandular patterns 6
18 Diagnostic algorithm for ovarian mucinous tumors with signet ring cell patterns Diagnostic algorithm for ovarian mucinous tumors with extracellular mucin production (PMP = pseudomyxoma peritonei) 7
19 A limited panel of antibodies is useful for distinguishing primary ovarian mucinous tumors from metastatic mucinous carcinomas and for distinguishing among the metastatic tumors. For the distinction of primary ovarian mucinous tumors from the metastases listed above, useful markers include CK7, CK20, Dpc4, and p16, whereas ER, PR, CA-125, and CEA, and are not useful. PAX8 has limited diagnostic value in the setting of mucinous tumors. The utility of CK7 and CK20 for distinction of metastases from primary ovarian epithelial tumors is restricted to specific situations. In particular, coordinate expression of these cytokeratins is very useful for distinction of metastatic lower gastrointestinal tract (colorectal, appendiceal) adenocarcinomas from primary ovarian mucinous tumors. However, these markers do not distinguish metastatic upper gastrointestinal tract, pancreaticobiliary, and endocervical adenocarcinomas from primary ovarian mucinous tumors due to shared coordinate expression profiles. For those tumors that can share coexpression of CK7 and CK20, the staining patterns of these markers can be helpful for suggesting that one primary site is more likely than the other. In primary ovarian mucinous tumors (atypical proliferative and carcinoma), the CK7 staining pattern is almost always diffuse (staining of at least 75% of tumor cells and often more than 90%) whereas the CK20 staining pattern is variable, ranging from negative to positive but generally not so diffuse when positive; the rare exception is some mucinous tumors arising in ovarian mature cystic teratomas, which are diffusely positive for CK20 and negative for CK7. Lower gastrointestinal tract (colorectal and appendiceal) tumors are usually negative for CK7 and diffusely positive for CK20. Some appendiceal tumors and a small percentage of colorectal carcinomas can express CK7, but the staining pattern is usually patchy rather than diffuse, with the exception of some appendiceal carcinomas that exhibit diffuse expression of CK7. Therefore, positivity for CK7 should not be considered either proof of ovarian origin or evidence against lower gastrointestinal tract origin without considering the staining distribution in the tumor. In addition, it is critical to avoid letting immunohistochemical results determine that the ovary is the site of origin when the morphology clearly favors a metastasis (for example, diffuse CK7 expression in an appendiceal signet ring cell carcinoma or colorectal carcinoma with patchy strong expression of CK7). Dpc4 expression is retained in all primary ovarian mucinous tumors, but expression is lost in ~50% of metastatic pancreatic carcinomas. Thus, lack of Dpc4 expression distinguishes metastatic pancreatic carcinomas from primary ovarian mucinous tumors; this is useful because both ovarian and pancreatic mucinous tumors share the same pattern of CK7 and CK20 expression (diffuse positivity for CK7 and variable positivity for CK20). However, retained expression does not refute a diagnosis of pancreatic carcinoma. In addition, loss of Dpc4 expression appears to be rather specific for pancreatic carcinomas since colorectal, appendiceal, gastric, and endocervical carcinomas almost always retain expression. Endocervical adenocarcinomas share microscopic features with primary ovarian mucinous and endometrioid tumors, and there is overlap in the CK7/CK20 immunoprofiles of these tumors. Thus, other markers are required to distinguish these tumors. Detection of HPV DNA is useful for distinguishing metastatic endocervical adenocarcinomas of usual type (those related to high-risk HPV infection) from primary ovarian carcinomas because studies on the association between HPV infection and 8
20 primary ovarian neoplasms have yielded almost universally negative results. The usual type endocervical adenocarcinomas demonstrate diffuse expression of p16 (always >50% and typically >75% of tumor cells staining moderately to strongly) in association with high-risk HPV infection. Diffuse p16 expression can distinguish these endocervical adenocarcinomas from most primary ovarian mucinous and endometrioid tumors and other metastatic adenocarcinomas having mucinous and/or endometrioid or endometrioid-like differentiation in the ovary because the latter two groups of tumors tend to be negative or exhibit patchy expression of p16. Those uncommon endocervical adenocarcinomas not related to HPV cannot be distinguished from primary ovarian mucinous tumors by HPV DNA detection or p16 expression. Hormone receptor expression is not useful for distinction of primary ovarian mucinous tumors from most metastatic mucinous adenocarcinomas (those of colorectum, appendix, pancreaticobiliary tract, stomach, and endocervix) because all these tumor types, with the exception of a minority of endocervical adenocarcinomas, lack expression of ER and PR. Hormone receptor expression only distinguishes metastatic endocervical adenocarcinomas, which are most often negative, from primary ovarian endometrioid tumors and metastatic endometrial endometrioid carcinomas, both of which usually express hormone receptors. The adenocarcinomas arising in the primary sites listed above account for the more commonly encountered metastatic mucinous carcinomas involving the ovary. Mucinous carcinomas occasionally, albeit uncommonly, arise in other organs, including breast, endometrium, small bowel, lung, and urinary bladder, and these sites should be considered when a non-ovarian primary cannot be found in the more commonly encountered primary sites. Occasional cases of metastatic lobular breast carcinoma involving the ovary may exhibit signet ring cell differentiation. Useful markers for diagnosing these tumors include CK7, CK20, ER, PR, GCDFP-15, and GATA-3. Expression of CK7 in the absence of CK20 is useful for distinguishing this type of breast carcinoma from lower gastrointestinal tract (colorectum, appendix) signet ring cell carcinomas; however, because the CK7+/CK20- immunoprofile does not distinguish these breast carcinomas from gastric signet ring cell carcinomas, the other markers are required as part of a diagnostic panel. REFERENCES 1. Mazur MT, Hsueh S, Gersell DJ. Metastases to the female genital tract. Analysis of 325 cases. Cancer 1984;53: Moore RG, Chung M, Granai CO, et al. Incidence of metastasis to the ovaries from nongenital tract primary tumors. Gynecol Oncol 2004;93: Ulbright TM, Roth LM, Stehman FB. Secondary ovarian neoplasia. A clinicopathologic study of 35 cases. Cancer 1984;53: Yazigi R, Sandstad J. Ovarian involvement in extragenital cancer. Gynecol Oncol 1989;34: McCluggage WG, Young RH. Primary ovarian mucinous tumors with signet ring cells: report of 3 cases with discussion of so-called primary Krukenberg tumor. Am J Surg Pathol 2008;32:
21 6. Reichert RA. Primary ovarian adenofibromatous neoplasms with mucincontaining signet-ring cells: a report of 2 cases. Int J Gynecol Pathol 2007;26: Lee KR, Young RH. The distinction between primary and metastatic mucinous carcinomas of the ovary: gross and histologic findings in 50 cases. Am J Surg Pathol 2003;27: Seidman JD, Kurman RJ, Ronnett BM. Primary and metastatic mucinous adenocarcinomas in the ovaries: incidence in routine practice with a new approach to improve intraoperative diagnosis. Am J Surg Pathol 2003;27: Hoerl HD, Hart WR. Primary ovarian mucinous cystadenocarcinomas: a clinicopathologic study of 49 cases with long-term follow-up. Am J Surg Pathol 1998;22: Ji H, Isacson C, Seidman JD, et al. Cytokeratins 7 and 20, Dpc4, and MUC5AC in the distinction of metastatic mucinous carcinomas in the ovary from primary ovarian mucinous tumors: Dpc4 assists in identifying metastatic pancreatic carcinomas. Int J Gynecol Pathol 2002;21: Khunamornpong S, Settakorn J, Sukpan K, et al. Mucinous tumor of low malignant potential ("borderline" or "atypical proliferative" tumor) of the ovary: a study of 171 cases with the assessment of intraepithelial carcinoma and microinvasion. Int J Gynecol Pathol 2011;30: Lee KR, Scully RE. Mucinous tumors of the ovary: a clinicopathologic study of 196 borderline tumors (of intestinal type) and carcinomas, including an evaluation of 11 cases with 'pseudomyxoma peritonei'. Am J Surg Pathol 2000;24: McKenney JK, Soslow RA, Longacre TA. Ovarian mature teratomas with mucinous epithelial neoplasms: morphologic heterogeneity and association with pseudomyxoma peritonei. Am J Surg Pathol 2008;32: Riopel MA, Ronnett BM, Kurman RJ. Evaluation of diagnostic criteria and behavior of ovarian intestinal-type mucinous tumors: atypical proliferative (borderline) tumors and intraepithelial, microinvasive, invasive, and metastatic carcinomas. Am J Surg Pathol 1999;23: Rodriguez IM, Prat J. Mucinous tumors of the ovary: a clinicopathologic analysis of 75 borderline tumors (of intestinal type) and carcinomas. Am J Surg Pathol 2002;26: Ronnett BM, Kajdacsy-Balla A, Gilks CB, et al. Mucinous borderline ovarian tumors: points of general agreement and persistent controversies regarding nomenclature, diagnostic criteria, and behavior. Hum Pathol 2004;35: Ronnett BM, Seidman JD. Mucinous tumors arising in ovarian mature cystic teratomas: relationship to the clinical syndrome of pseudomyxoma peritonei. Am J Surg Pathol 2003;27: Seidman JD, Soslow RA, Vang R, et al. Borderline ovarian tumors: diverse contemporary viewpoints on terminology and diagnostic criteria with illustrative images. Hum Pathol 2004;35: Vang R, Gown AM, Barry TS, et al. Cytokeratins 7 and 20 in primary and secondary mucinous tumors of the ovary: analysis of coordinate immunohistochemical expression profiles and staining distribution in 179 cases. Am J Surg Pathol 2006;30:
22 20. Vang R, Gown AM, Wu LS, et al. Immunohistochemical expression of CDX2 in primary ovarian mucinous tumors and metastatic mucinous carcinomas involving the ovary: comparison with CK20 and correlation with coordinate expression of CK7. Mod Pathol 2006;19: Vang R, Gown AM, Barry TS, et al. Immunohistochemistry for estrogen and progesterone receptors in the distinction of primary and metastatic mucinous tumors in the ovary: an analysis of 124 cases. Mod Pathol 2006;19: Vang R, Gown AM, Zhao C, et al. Ovarian mucinous tumors associated with mature cystic teratoma. Morphologic and immunohistochemical analysis identifies a subset of potential teratomatous origin that shares features of lower gastrointestinal tract mucinous tumors more commonly encountered as secondary tumors of the ovary. Am J Surg Pathol 2007;31: Yemelyanova AV, Vang R, Judson K, et al. Distinction of primary and metastatic mucinous tumors involving the ovary: analysis of size and laterality data by primary site with re-evaluation of an algorithm for tumor classification. Am J Surg Pathol 2008;32: Chu PG, Chung L, Weiss LM, et al. Determining the site of origin of mucinous adenocarcinoma: an immunohistochemical study of 175 cases. Am J Surg Pathol 2011;35: Elishaev E, Gilks CB, Miller D, et al. Synchronous and metachronous endocervical and ovarian neoplasms: evidence supporting interpretation of the ovarian neoplasms as metastatic endocervical adenocarcinomas simulating primary ovarian surface epithelial neoplasms. Am J Surg Pathol 2005;29: Hristov AC, Young RH, Vang R, et al. Ovarian metastases of appendiceal tumors with goblet cell carcinoid-like and signet ring cell patterns: a report of 30 cases. Am J Surg Pathol 2007;31: Judson K, McCormick C, Vang R, et al. Women with undiagnosed colorectal adenocarcinomas presenting with ovarian metastases: clinicopathologic features and comparison with women having known colorectal adenocarcinomas and ovarian involvement. Int J Gynecol Pathol 2008;27: Meriden Z, Yemelyanova AV, Vang R, et al. Ovarian metastases of pancreaticobiliary tract adenocarcinomas: analysis of 35 cases, with emphasis on the ability of metastases to simulate primary ovarian mucinous tumors. Am J Surg Pathol 2011;35: Ronnett BM, Kurman RJ, Shmookler BM, et al. The morphologic spectrum of ovarian metastases of appendiceal adenocarcinomas: a clinicopathologic and immunohistochemical analysis of tumors often misinterpreted as primary ovarian tumors or metastatic tumors from other gastrointestinal sites. Am J Surg Pathol 1997;21: Ronnett BM, Kurman RJ, Zahn CM, et al. Pseudomyxoma peritonei in women: a clinicopathologic analysis of 30 cases with emphasis on site of origin, prognosis, and relationship to ovarian mucinous tumors of low malignant potential. Hum Pathol 1995;26: Ronnett BM, Shmookler BM, Diener-West M, et al. Immunohistochemical evidence supporting the appendiceal origin of pseudomyxoma peritonei in women. Int J Gynecol Pathol 1997;16:
23 32. Ronnett BM, Yan H, Kurman RJ, et al. Patients with pseudomyxoma peritonei associated with disseminated peritoneal adenomucinosis have a significantly more favorable prognosis than patients with peritoneal mucinous carcinomatosis. Cancer 2001;92: Ronnett BM, Zahn CM, Kurman RJ, et al. Disseminated peritoneal adenomucinosis and peritoneal mucinous carcinomatosis. A clinicopathologic analysis of 109 cases with emphasis on distinguishing pathologic features, site of origin, prognosis, and relationship to "pseudomyxoma peritonei". Am J Surg Pathol 1995;19: Ronnett B, Gown AM, Barry TS, et al. Utility of immunohistochemistry in determining the site of origin of metastatic mucinous carcinomas involving the ovary. Mod Pathol 2005;18:201A (abstract #934). 35. Ronnett BM, Yemelyanova AV, Vang R, et al. Endocervical adenocarcinomas with ovarian metastases: analysis of 29 cases with emphasis on minimally invasive cervical tumors and the ability of the metastases to simulate primary ovarian neoplasms. Am J Surg Pathol 2008;32: Vang R, Ronnett BM. A practical approach to mucinous tumors involving the ovary: distinction of primary from metastatic tumors and prediction of site of origin for metastases of uncertain origin. Pathol Case Rev 2006;11: Vang R, Gown AM, Farinola M, et al. P16 expression in primary ovarian mucinous and endometrioid tumors and metastatic adenocarcinomas in the ovary: utility for identification of metastatic HPV-related endocervical adenocarcinomas. Am J Surg Pathol 2007;31: Vang R, Ronnett BM. Metastatic and miscellaneous primary tumors of the ovary. In: Nucci MR, Oliva E, eds. Gynecologic Pathology. Philadelphia, PA: Elsevier, 2009: Young RH, Scully RE. Metastatic tumors in the ovary: a problem-oriented approach and review of the recent literature. Semin Diagn Pathol 1991;8:
Mucinous Adenocarcinoma Involving the Ovary: Comparative Evaluation of the Classification Algorithms using Tumor Size and Laterality
 J Korean Med Sci 2010; 25: 220-5 ISSN 1011-8934 DOI: 10.3346/jkms.2010.25.2.220 Mucinous Adenocarcinoma Involving the Ovary: Comparative Evaluation of the Classification Algorithms using Tumor Size and
J Korean Med Sci 2010; 25: 220-5 ISSN 1011-8934 DOI: 10.3346/jkms.2010.25.2.220 Mucinous Adenocarcinoma Involving the Ovary: Comparative Evaluation of the Classification Algorithms using Tumor Size and
International Society of Gynecological Pathologists Symposium 2007
 International Society of Gynecological Pathologists Symposium 2007 Anais Malpica, M.D. Department of Pathology The University of Texas M.D. Anderson Cancer Center Grading of Ovarian Cancer Histologic grade
International Society of Gynecological Pathologists Symposium 2007 Anais Malpica, M.D. Department of Pathology The University of Texas M.D. Anderson Cancer Center Grading of Ovarian Cancer Histologic grade
Mucinous Tumors of the Ovary Beirut, Lebanon. Anaís Malpica, M.D. Professor Department of Pathology
 Mucinous Tumors of the Ovary Beirut, Lebanon Anaís Malpica, M.D. Professor Department of Pathology Primary Mucinous Tumors of the Ovary Cystadenoma Borderline (Tumor of Low Malignant Potential/Atypical
Mucinous Tumors of the Ovary Beirut, Lebanon Anaís Malpica, M.D. Professor Department of Pathology Primary Mucinous Tumors of the Ovary Cystadenoma Borderline (Tumor of Low Malignant Potential/Atypical
Bibliography. Serous Tumors of the Ovary. Nomenclature
 Bibliography Serous Tumors of the Ovary Nomenclature 1. Allison KH, Swisher EM, Kerkering KM, et al. Defining an appropriate threshold for the diagnosis of serous borderline tumor of the ovary: when is
Bibliography Serous Tumors of the Ovary Nomenclature 1. Allison KH, Swisher EM, Kerkering KM, et al. Defining an appropriate threshold for the diagnosis of serous borderline tumor of the ovary: when is
Borderline Ovarian Mucinous Tumors: Consensus Points and Persistent Controversies Regarding Nomenclature, Diagnostic Criteria, and Behavior
 Borderline Ovarian Mucinous Tumors: Consensus Points and Persistent Controversies Regarding Nomenclature, Diagnostic Criteria, and Behavior Brigitte M. Ronnett, M.D.; C. Blake Gilks, M.D., Maria J. Merino,
Borderline Ovarian Mucinous Tumors: Consensus Points and Persistent Controversies Regarding Nomenclature, Diagnostic Criteria, and Behavior Brigitte M. Ronnett, M.D.; C. Blake Gilks, M.D., Maria J. Merino,
A Survay on Appendiceal Involvement in Ovarian Mucinous Tumors
 http://www.ijwhr.net Open Access doi 10.15296/ijwhr.2018.33 Original Article International Journal of Women s Health and Reproduction Sciences Vol. 6, No. 2, April 2018, 199 203 ISSN 2330-4456 A Survay
http://www.ijwhr.net Open Access doi 10.15296/ijwhr.2018.33 Original Article International Journal of Women s Health and Reproduction Sciences Vol. 6, No. 2, April 2018, 199 203 ISSN 2330-4456 A Survay
3 cell types in the normal ovary
 Ovarian tumors 3 cell types in the normal ovary Surface (coelomic epithelium) the origin of the great majority of ovarian tumors (neoplasms) 90% of malignant ovarian tumors Totipotent germ cells Sex cord-stromal
Ovarian tumors 3 cell types in the normal ovary Surface (coelomic epithelium) the origin of the great majority of ovarian tumors (neoplasms) 90% of malignant ovarian tumors Totipotent germ cells Sex cord-stromal
Mucinous tumours of appendix and ovary: an overview and evaluation of current practice
 Department of Pathology, Laboratory Medicine Program, University Health Network, University of Toronto, Toronto, Canada Correspondence to Dr Marjan Rouzbahman, Department of Pathology, 11th floor, Eaton
Department of Pathology, Laboratory Medicine Program, University Health Network, University of Toronto, Toronto, Canada Correspondence to Dr Marjan Rouzbahman, Department of Pathology, 11th floor, Eaton
Low-grade serous neoplasia. Robert A. Soslow, MD
 Low-grade serous neoplasia Robert A. Soslow, MD soslowr@mskcc.org Outline Orientation Ovarian tumor overview Non serous borderline tumors Serous borderline tumors Clinical summary Morphologic description
Low-grade serous neoplasia Robert A. Soslow, MD soslowr@mskcc.org Outline Orientation Ovarian tumor overview Non serous borderline tumors Serous borderline tumors Clinical summary Morphologic description
Ovarian carcinoma classification. Robert A. Soslow, MD
 Ovarian carcinoma classification Robert A. Soslow, MD soslowr@mskcc.org WHO classification Serous Mucinous Endometrioid Clear cell Transitional Squamous Mixed epithelial Undifferentiated Introduction Rationale
Ovarian carcinoma classification Robert A. Soslow, MD soslowr@mskcc.org WHO classification Serous Mucinous Endometrioid Clear cell Transitional Squamous Mixed epithelial Undifferentiated Introduction Rationale
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
CASE 4 21/07/2017. Ectopic Prostatic Tissue in Cervix. Female 31. LLETZ for borderline nuclear abnormalities
 Female 31 CASE 4 LLETZ for borderline nuclear abnormalities PSA Ectopic Prostatic Tissue in Cervix AJSP 2006;30;209-215 usually incidental microscopic finding usually in ectocervical stroma? developmental
Female 31 CASE 4 LLETZ for borderline nuclear abnormalities PSA Ectopic Prostatic Tissue in Cervix AJSP 2006;30;209-215 usually incidental microscopic finding usually in ectocervical stroma? developmental
of 20 to 80 and subsequently declines [2].
![of 20 to 80 and subsequently declines [2].](/thumbs/80/81450506.jpg "of 20 to 80 and subsequently declines [2].") - - According to the 2014 World Health Organization (WHO) classification and tumor morphology, primary ovarian tumors are subdivided into three categories: epithelial (60%), germ cell (30%), and sex-cord
- - According to the 2014 World Health Organization (WHO) classification and tumor morphology, primary ovarian tumors are subdivided into three categories: epithelial (60%), germ cell (30%), and sex-cord
3 cell types in the normal ovary
 Ovarian tumors 3 cell types in the normal ovary Surface (coelomic epithelium) the origin of the great majority of ovarian tumors 90% of malignant ovarian tumors Totipotent germ cells Sex cord-stromal cells
Ovarian tumors 3 cell types in the normal ovary Surface (coelomic epithelium) the origin of the great majority of ovarian tumors 90% of malignant ovarian tumors Totipotent germ cells Sex cord-stromal cells
Section 1. Biology of gynaecological cancers: our current understanding
 Section 1 Biology of gynaecological cancers: our current understanding Chapter 1 Morphological sub-types of ovarian carcinoma: new developments and pathogenesis W Glenn McCluggage 1 Introduction In most
Section 1 Biology of gynaecological cancers: our current understanding Chapter 1 Morphological sub-types of ovarian carcinoma: new developments and pathogenesis W Glenn McCluggage 1 Introduction In most
Case Report Ovarian Seromucinous Borderline Tumor and Clear Cell Carcinoma: An Unusual Combination
 Case Reports in Obstetrics and Gynecology Volume 2015, Article ID 690891, 5 pages http://dx.doi.org/10.1155/2015/690891 Case Report Ovarian Seromucinous Borderline Tumor and Clear Cell Carcinoma: An Unusual
Case Reports in Obstetrics and Gynecology Volume 2015, Article ID 690891, 5 pages http://dx.doi.org/10.1155/2015/690891 Case Report Ovarian Seromucinous Borderline Tumor and Clear Cell Carcinoma: An Unusual
GOBLET CELL CARCINOID. Hanlin L. Wang, MD, PhD University of California Los Angeles
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
Urinary Bladder: WHO Classification and AJCC Staging Update 2017
 Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Papillary Lesions of the Breast A Practical Approach to Diagnosis. (Arch Pathol Lab Med. 2016;140: ; doi: /arpa.
 Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Appendix cancer mimicking ovarian cancer
 Int J Gynecol Cancer 2002, 12, 768 772 CORRESPONDENCE AND BRIEF REPORTS Appendix cancer mimicking ovarian cancer P. A. GEHRIG *, J. F. BOGGESS*, D. W. OLLILA, P. A. GROBEN & L. VAN LE* *Division of Gynecologic
Int J Gynecol Cancer 2002, 12, 768 772 CORRESPONDENCE AND BRIEF REPORTS Appendix cancer mimicking ovarian cancer P. A. GEHRIG *, J. F. BOGGESS*, D. W. OLLILA, P. A. GROBEN & L. VAN LE* *Division of Gynecologic
How to Recognize Gynecologic Cancer Cells from Pelvic Washing and Ascetic Specimens
 How to Recognize Gynecologic Cancer Cells from Pelvic Washing and Ascetic Specimens Wenxin Zheng, M.D. Professor of Pathology and Gynecology University of Arizona zhengw@email.arizona.edu http://www.zheng.gynpath.medicine.arizona.edu/index.html
How to Recognize Gynecologic Cancer Cells from Pelvic Washing and Ascetic Specimens Wenxin Zheng, M.D. Professor of Pathology and Gynecology University of Arizona zhengw@email.arizona.edu http://www.zheng.gynpath.medicine.arizona.edu/index.html
Borderline tumors. Borderline tumors. Serous borderline tumor are NOT benign. Low grade serous carcinoma: pathogenesis. Serous carcinoma: pathogenesis
 Serous borderline tumor are NOT benign Robert A. Soslow, MD Memorial Sloan-Kettering Cancer Center soslowr@mskcc.org Borderline tumors Serous BTs and seromucinous BTs are both histopathologically borderline
Serous borderline tumor are NOT benign Robert A. Soslow, MD Memorial Sloan-Kettering Cancer Center soslowr@mskcc.org Borderline tumors Serous BTs and seromucinous BTs are both histopathologically borderline
Case 1. Pathology of gynecological cancer. What do we need to know (Case 1) Luca Mazzucchelli Istituto cantonale di patologia Locarno
 Luca Mazzucchelli Istituto cantonale di patologia Locarno") Case 1 Pathology of gynecological cancer. What do we need to know (Case 1) Luca Mazzucchelli Istituto cantonale di patologia Locarno SAMO Interdisciplinary Workshop on Gynecological Tumors Lucern, October
Case 1 Pathology of gynecological cancer. What do we need to know (Case 1) Luca Mazzucchelli Istituto cantonale di patologia Locarno SAMO Interdisciplinary Workshop on Gynecological Tumors Lucern, October
Chapter 6 Frozen Section Evaluation of the Appendix
 Chapter 6 Frozen Section Evaluation of the Appendix Abstract Appendiceal tumors are rarely diagnosed preoperatively, and their classification is both challenging and controversial owing to their tendency
Chapter 6 Frozen Section Evaluation of the Appendix Abstract Appendiceal tumors are rarely diagnosed preoperatively, and their classification is both challenging and controversial owing to their tendency
SEROUS TUMORS. Dr. Jaime Prat. Hospital de la Santa Creu i Sant Pau. Universitat Autònoma de Barcelona
 SEROUS TUMORS Dr. Jaime Prat Hospital de la Santa Creu i Sant Pau Universitat Autònoma de Barcelona Serous Borderline Tumors (SBTs) Somatic genetics Clonality studies have attempted to dilucidate whether
SEROUS TUMORS Dr. Jaime Prat Hospital de la Santa Creu i Sant Pau Universitat Autònoma de Barcelona Serous Borderline Tumors (SBTs) Somatic genetics Clonality studies have attempted to dilucidate whether
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital
 Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Low-grade appendiceal mucinous neoplasm (LAMN) High-grade appendiceal mucinous neoplasm (HAMN) Adenocarcinoma
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Low-grade appendiceal mucinous neoplasm (LAMN) High-grade appendiceal mucinous neoplasm (HAMN) Adenocarcinoma
Mousa. Najat kayed &Renad Al-Awamleh. Nizar Alkhlaifat
 6 Mousa Najat kayed &Renad Al-Awamleh Nizar Alkhlaifat P a g e 1 This sheet written based on record 13 on website Cover slide( 95-117 ) No need to go back to slide FALLOPIAN TUBE PATHOLOGY In general fallopian
6 Mousa Najat kayed &Renad Al-Awamleh Nizar Alkhlaifat P a g e 1 This sheet written based on record 13 on website Cover slide( 95-117 ) No need to go back to slide FALLOPIAN TUBE PATHOLOGY In general fallopian
Wendy L Frankel. Chair and Distinguished Professor
 1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
Adenocarcinoma of the Cervix
 Question 1. Each of the following statements about cervical adenocarcinoma is true except: Adenocarcinoma of the Cervix SAMS a) A majority of women with cervical adenocarcinoma have stage I tumors at diagnosis.
Question 1. Each of the following statements about cervical adenocarcinoma is true except: Adenocarcinoma of the Cervix SAMS a) A majority of women with cervical adenocarcinoma have stage I tumors at diagnosis.
Select problems in cystic pancreatic lesions
 Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Advanced Stage Mucinous Adenocarcinoma of the Ovary Is Both Rare and Highly Lethal
 Advanced Stage Mucinous Adenocarcinoma of the Ovary Is Both Rare and Highly Lethal A Gynecologic Oncology Group Study Richard J. Zaino, MD 1 ; Mark F. Brady, PhD 2 ; Subodh M. Lele, MD 3 ; Helen Michael,
Advanced Stage Mucinous Adenocarcinoma of the Ovary Is Both Rare and Highly Lethal A Gynecologic Oncology Group Study Richard J. Zaino, MD 1 ; Mark F. Brady, PhD 2 ; Subodh M. Lele, MD 3 ; Helen Michael,
6/5/2010. Outline of Talk. Endometrial Alterations That Mimic Cancer & Vice Versa: Metaplastic / reactive changes. Problems in Biopsies/Curettages
 Outline of Talk Endometrial Alterations That Mimic Cancer & Vice Versa: Problems in Biopsies/Curettages Metaplastic / reactive changes Mucinous change Microglandular hyperplasia-like change Squamous metaplasia
Outline of Talk Endometrial Alterations That Mimic Cancer & Vice Versa: Problems in Biopsies/Curettages Metaplastic / reactive changes Mucinous change Microglandular hyperplasia-like change Squamous metaplasia
Atypical Hyperplasia/EIN
 EIN Atypical Hyperplasia/EIN Based on scientific and diagnostic advances, in 2014 the WHO moved that the precursor lesion for endometrioid carcinoma be atypical hyperplasia/ein, rather than what was previously
EIN Atypical Hyperplasia/EIN Based on scientific and diagnostic advances, in 2014 the WHO moved that the precursor lesion for endometrioid carcinoma be atypical hyperplasia/ein, rather than what was previously
Current Concept in Ovarian Carcinoma: Pathology Perspectives
 Current Concept in Ovarian Carcinoma: Pathology Perspectives Rouba Ali-Fehmi, MD Professor of Pathology The Karmanos Cancer Institute, Wayne State University School of Medicine Current Concept in Ovarian
Current Concept in Ovarian Carcinoma: Pathology Perspectives Rouba Ali-Fehmi, MD Professor of Pathology The Karmanos Cancer Institute, Wayne State University School of Medicine Current Concept in Ovarian
Pathology of Ovarian Tumours. Dr. Jyothi Ranganathan MD ( Path) AFMC Pune PDCC (Cytopathology) PGI Chandigarh
 AFMC Pune PDCC (Cytopathology) PGI Chandigarh") Pathology of Ovarian Tumours Dr. Jyothi Ranganathan MD ( Path) AFMC Pune PDCC (Cytopathology) PGI Chandigarh Outline Incidence Risk factors Classification Pathology of tumours Tumour markers Prevention
Pathology of Ovarian Tumours Dr. Jyothi Ranganathan MD ( Path) AFMC Pune PDCC (Cytopathology) PGI Chandigarh Outline Incidence Risk factors Classification Pathology of tumours Tumour markers Prevention
Cutaneous metastases. Thaddeus Mully. University of California, San Francisco Professor, Departments of Pathology and Dermatology
 Cutaneous metastases Thaddeus Mully University of California, San Francisco Professor, Departments of Pathology and Dermatology DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Thaddeus Mully Course C005 Essential
Cutaneous metastases Thaddeus Mully University of California, San Francisco Professor, Departments of Pathology and Dermatology DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Thaddeus Mully Course C005 Essential
Synonyms. Nephrogenic metaplasia Mesonephric adenoma
 Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
Isabel Alvarado-Cabrero, M.D., Ph.D., Adriana Rodríguez-Gómez, M.D., Jorge Castelan-Pedraza, M.D., and Raquel Valencia-Cedillo, M.D.
 AND QUANTITATIVE CYTOPATHOLOGY AND AQCHANALYTICAL HISTOPATHOLOGY An Official Periodical of The International Academy of Cytology and the Italian Group of Uropathology ARTICLES Metastatic Ovarian Tumors
AND QUANTITATIVE CYTOPATHOLOGY AND AQCHANALYTICAL HISTOPATHOLOGY An Official Periodical of The International Academy of Cytology and the Italian Group of Uropathology ARTICLES Metastatic Ovarian Tumors
Exploring the Histogenesis of Ovarian Mucinous and Transitional Cell (Brenner) Neoplasms and Their Relationship With Walthard Cell Nests
 Neoplasms and Their Relationship With Walthard Cell Nests") Exploring the Histogenesis of Ovarian Mucinous and Transitional Cell (Brenner) Neoplasms and Their Relationship With Walthard Cell Nests A Study of 120 Tumors Jeffrey D. Seidman, MD; Fatemeh Khedmati,
Exploring the Histogenesis of Ovarian Mucinous and Transitional Cell (Brenner) Neoplasms and Their Relationship With Walthard Cell Nests A Study of 120 Tumors Jeffrey D. Seidman, MD; Fatemeh Khedmati,
Case history: Figure 1. H&E, 5x. Figure 2. H&E, 20x.
 1 Case history: A 49 year-old female presented with a 5 year history of chronic anal fissure. The patient s past medical history is otherwise unremarkable. On digital rectal examination there was a very
1 Case history: A 49 year-old female presented with a 5 year history of chronic anal fissure. The patient s past medical history is otherwise unremarkable. On digital rectal examination there was a very
Neoplasias Quisticas del Páncreas
 SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
Gynaecological Malignancies
 Gynaecological Malignancies Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea Division of Pathology School of Medicine & Health Sciences Overview Genital tract tumors
Gynaecological Malignancies Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea Division of Pathology School of Medicine & Health Sciences Overview Genital tract tumors
Syllabus. Appendiceal GCC and LAMN Navigating the Alphabet Soup in the Appendix. Appendiceal tumors. Summary provided Complete presentation
 2016 Current Issues in Surgical Pathology Appendiceal GCC and LAMN Navigating the Alphabet Soup in the Appendix Syllabus Summary provided Complete presentation sanjay.kakar@ucsf.edu Sanjay Kakar, MD University
2016 Current Issues in Surgical Pathology Appendiceal GCC and LAMN Navigating the Alphabet Soup in the Appendix Syllabus Summary provided Complete presentation sanjay.kakar@ucsf.edu Sanjay Kakar, MD University
Pathology of the female genital tract
 Pathology of the female genital tract Common illnesses of the female genital tract Before menarche Developmental anomalies Tumors (ovarial teratoma) Amenorrhea Fertile years PCOS, ovarian cysts Endometriosis
Pathology of the female genital tract Common illnesses of the female genital tract Before menarche Developmental anomalies Tumors (ovarial teratoma) Amenorrhea Fertile years PCOS, ovarian cysts Endometriosis
When Immunostains Can Get You in Trouble: Gynecologic Pathology p16: Panacea or Pandora s Box?
 When Immunostains Can Get You in Trouble: Gynecologic Pathology p16: Panacea or Pandora s Box? Teri A. Longacre, MD Stanford Medicine Stanford California pi6 in Gynecologic Pathology: Panacea or Pandora
When Immunostains Can Get You in Trouble: Gynecologic Pathology p16: Panacea or Pandora s Box? Teri A. Longacre, MD Stanford Medicine Stanford California pi6 in Gynecologic Pathology: Panacea or Pandora
4/12/2018. MUSC Pathology Symposium Kiawah Island April 18, Jesse K. McKenney, MD
 MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as
MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as
Cancers of unknown primary : Knowing the unknown. Prof. Ahmed Hossain Professor of Medicine SSMC
 Cancers of unknown primary : Knowing the unknown Prof. Ahmed Hossain Professor of Medicine SSMC Definition Cancers of unknown primary site (CUPs) Represent a heterogeneous group of metastatic tumours,
Cancers of unknown primary : Knowing the unknown Prof. Ahmed Hossain Professor of Medicine SSMC Definition Cancers of unknown primary site (CUPs) Represent a heterogeneous group of metastatic tumours,
Survival Analysis and Prognosis for Patients with Serous and Mucinous Borderline Ovarian Tumors: 14-Year Experience from a Tertiary Center in Iran
 ORIGINAL ARTICLE Survival Analysis and Prognosis for Patients with Serous and Mucinous Borderline Ovarian Tumors: 14-Year Experience from a Tertiary Center in Iran Katayoun Ziari, Ebrahim Soleymani, and
ORIGINAL ARTICLE Survival Analysis and Prognosis for Patients with Serous and Mucinous Borderline Ovarian Tumors: 14-Year Experience from a Tertiary Center in Iran Katayoun Ziari, Ebrahim Soleymani, and
Dr Sanjiv Manek Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Sanjiv Manek Oxford Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust Ovarian Endometrial Vulvo-vaginal Cervical Illustration-Cellular Pathology. Oxford
Dr Sanjiv Manek Oxford Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust Ovarian Endometrial Vulvo-vaginal Cervical Illustration-Cellular Pathology. Oxford
New Developments in Immunohistochemistry for Gynecologic Pathology
 New Developments in Immunohistochemistry for Gynecologic Pathology Michael T. Deavers, M.D. Professor, Departments of Pathology and Gynecologic Oncology Immunohistochemistry in Gynecologic Pathology Majority
New Developments in Immunohistochemistry for Gynecologic Pathology Michael T. Deavers, M.D. Professor, Departments of Pathology and Gynecologic Oncology Immunohistochemistry in Gynecologic Pathology Majority
Invited Re vie W. Molecular genetics of ovarian carcinomas. Histology and Histo pathology
 Histol Histopathol (1 999) 14: 269-277 http://www.ehu.es/histol-histopathol Histology and Histo pathology Invited Re vie W Molecular genetics of ovarian carcinomas J. Diebold Pathological Institute, Ludwig-Maximilians-University
Histol Histopathol (1 999) 14: 269-277 http://www.ehu.es/histol-histopathol Histology and Histo pathology Invited Re vie W Molecular genetics of ovarian carcinomas J. Diebold Pathological Institute, Ludwig-Maximilians-University
Page # 1. Endometrium. Cellular Components. Anatomical Regions. Management of SIL Thomas C. Wright, Jr. Most common diseases:
 Endometrium Pathology of the Endometrium Thomas C. Wright Columbia University, New York, NY Most common diseases: Abnormal uterine bleeding Inflammatory conditions Benign neoplasms Endometrial cancer Anatomical
Endometrium Pathology of the Endometrium Thomas C. Wright Columbia University, New York, NY Most common diseases: Abnormal uterine bleeding Inflammatory conditions Benign neoplasms Endometrial cancer Anatomical
Disseminated Peritoneal Adenomucinosis Associated with a Panperitonitis-Like Onset: Report of a Case
 Surg Today (2001) 31:646 650 Disseminated Peritoneal Adenomucinosis Associated with a Panperitonitis-Like Onset: Report of a Case Yoshito Kuroki 1, Shunyou Otagiri 1, and Kazuhiro Tsukada 2 1 Department
Surg Today (2001) 31:646 650 Disseminated Peritoneal Adenomucinosis Associated with a Panperitonitis-Like Onset: Report of a Case Yoshito Kuroki 1, Shunyou Otagiri 1, and Kazuhiro Tsukada 2 1 Department
The Diagnostic Challenges of Low Grade and High Grade Tubo-Ovarian Serous Carcinomas. W Glenn McCluggage Belfast, Northern Ireland
 The Diagnostic Challenges of Low Grade and High Grade Tubo-Ovarian Serous Carcinomas W Glenn McCluggage Belfast, Northern Ireland Enterprise Interest None OVARIAN SEROUS CARCINOMA (OSC) RECENT DEVELOPMENTS
The Diagnostic Challenges of Low Grade and High Grade Tubo-Ovarian Serous Carcinomas W Glenn McCluggage Belfast, Northern Ireland Enterprise Interest None OVARIAN SEROUS CARCINOMA (OSC) RECENT DEVELOPMENTS
Objectives. Atypical Glandular Cells. Atypical Endocervical Cells. Reactive Endocervical Cells
 2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
 DIAGNOSIS A. RIGHT OVARY: Krukenberg tumor (20 cm in maximum dimension, see comment). B. LEFT OVARY: Krukenberg tumor (8.5 cm in maximum dimension, see comment). C. UTERUS (130 Grams): Cervix: Metastatic
DIAGNOSIS A. RIGHT OVARY: Krukenberg tumor (20 cm in maximum dimension, see comment). B. LEFT OVARY: Krukenberg tumor (8.5 cm in maximum dimension, see comment). C. UTERUS (130 Grams): Cervix: Metastatic
Expression of Cytokeratins 7 and 20 in Ovarian Neoplasia
 Anatomic Pathology / EXPRESSION OF CYTOKERATINS 7 AND 20 IN OVARIAN NEOPLASIA Expression of Cytokeratins 7 and 20 in Ovarian Neoplasia Helen P. Cathro, MBChB, and Mark H. Stoler, MD Key Words: Ovary; Ovarian;
Anatomic Pathology / EXPRESSION OF CYTOKERATINS 7 AND 20 IN OVARIAN NEOPLASIA Expression of Cytokeratins 7 and 20 in Ovarian Neoplasia Helen P. Cathro, MBChB, and Mark H. Stoler, MD Key Words: Ovary; Ovarian;
Biliary tract tumors
 Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,
Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,
The relative frequency and histopathological patterns of ovarian lesions: study of 116 cases
 Original article: The relative frequency and histopathological patterns of ovarian lesions: study of 116 cases Dr Dimple Mehta*,Dr Alpesh Chavda**, Dr Hetal Patel*** *Assistant Professor, **Tutor, ***3
Original article: The relative frequency and histopathological patterns of ovarian lesions: study of 116 cases Dr Dimple Mehta*,Dr Alpesh Chavda**, Dr Hetal Patel*** *Assistant Professor, **Tutor, ***3
Endometrial Metaplasia, Hyperplasia & Other Cancer Mimics: a Consultant s Experience
 Endometrial Metaplasia, Hyperplasia & Other Cancer Mimics: a Consultant s Experience Pacific Northwest Society of Pathologists Vancouver, B.C. September 26, 2015 Teri A. Longacre, M.D. longacre@stanford.edu
Endometrial Metaplasia, Hyperplasia & Other Cancer Mimics: a Consultant s Experience Pacific Northwest Society of Pathologists Vancouver, B.C. September 26, 2015 Teri A. Longacre, M.D. longacre@stanford.edu
Disclosure. Relevant Financial Relationship(s) None. Off Label Usage None MFMER slide-1
 None. Off Label Usage None MFMER slide-1") Disclosure Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-1 Case Presentation A 43 year old male, with partial nephrectomy for a right kidney mass 2013 MFMER slide-2 2013
Disclosure Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-1 Case Presentation A 43 year old male, with partial nephrectomy for a right kidney mass 2013 MFMER slide-2 2013
3/24/2017. Disclosure of Relevant Financial Relationships. Mixed Epithelial Endometrial Carcinoma. ISGyP Endometrial Cancer Project
 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME disclose any relevant financial relationship
Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME disclose any relevant financial relationship
What s (new) and Important in Reporting of Uterine Cancers Katherine Vroobel The Royal Marsden
 and Important in Reporting of Uterine Cancers Katherine Vroobel The Royal Marsden") What s (new) and Important in Reporting of Uterine Cancers Katherine Vroobel The Royal Marsden Maastricht Pathology 2018 Wednesday 20 th June Endometrioid adenocarcinoma High grade carcinomas (common)
What s (new) and Important in Reporting of Uterine Cancers Katherine Vroobel The Royal Marsden Maastricht Pathology 2018 Wednesday 20 th June Endometrioid adenocarcinoma High grade carcinomas (common)
OVARIES. MLS Basic histological diagnosis MLS HIST 422 Semester 8- batch 7 L13 Dr: Ali Eltayb.
 OVARIES MLS Basic histological diagnosis MLS HIST 422 Semester 8- batch 7 L13 Dr: Ali Eltayb. OBJECTIVES Recognize different disease of ovaries Classify ovarian cyst Describe the pathogenesis, morphology
OVARIES MLS Basic histological diagnosis MLS HIST 422 Semester 8- batch 7 L13 Dr: Ali Eltayb. OBJECTIVES Recognize different disease of ovaries Classify ovarian cyst Describe the pathogenesis, morphology
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital
 Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Adenoma Low-grade appendiceal mucinous neoplasm High-grade appendiceal mucinous neoplasm Adenocarcinoma Serrated
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Adenoma Low-grade appendiceal mucinous neoplasm High-grade appendiceal mucinous neoplasm Adenocarcinoma Serrated
Note: The cause of testicular neoplasms remains unknown
 - In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
- In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
Female Genital Tract Lab. Dr. Nisreen Abu Shahin Assistant Professor of Pathology University of Jordan
 Female Genital Tract Lab Dr. Nisreen Abu Shahin Assistant Professor of Pathology University of Jordan Ovarian Pathology A 20-year-old female presented with vague left pelvic pain. Pelvic exam revealed
Female Genital Tract Lab Dr. Nisreen Abu Shahin Assistant Professor of Pathology University of Jordan Ovarian Pathology A 20-year-old female presented with vague left pelvic pain. Pelvic exam revealed
Low-Grade Serous Ovarian Tumors Debra A. Bell, MD Mayo Clinic and Mayo Medical School Rochester, MN
 1 Low-Grade Serous Ovarian Tumors Debra A. Bell, MD Mayo Clinic and Mayo Medical School Rochester, MN It is very appropriate to discuss low-grade ovarian serous neoplasms in a symposium in honor of Dr.
1 Low-Grade Serous Ovarian Tumors Debra A. Bell, MD Mayo Clinic and Mayo Medical School Rochester, MN It is very appropriate to discuss low-grade ovarian serous neoplasms in a symposium in honor of Dr.
Ovarian Clear Cell Carcinoma
 Ovarian Clear Cell Carcinoma Rouba Ali-Fehmi, MD Professor of Pathology The Karmanos Cancer Institute, Wayne State University School of Medicine 50 year old woman with chief complaint of shortness of breath
Ovarian Clear Cell Carcinoma Rouba Ali-Fehmi, MD Professor of Pathology The Karmanos Cancer Institute, Wayne State University School of Medicine 50 year old woman with chief complaint of shortness of breath
Neoplasia 2018 Lecture 2. Dr Heyam Awad MD, FRCPath
 Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
PSA. HMCK, p63, Racemase. HMCK, p63, Racemase
 Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Clinical History USCAP Specialty Conference. Gynecologic Pathology Case 3
 2010 USCA Specialty Conference Gynecologic athology Case Kathleen R. Cho, M.D. Department of athology Clinical History 46 yo woman presented with bilateral ovarian masses and elevated CA-125 TAH/BSO, pelvic
2010 USCA Specialty Conference Gynecologic athology Case Kathleen R. Cho, M.D. Department of athology Clinical History 46 yo woman presented with bilateral ovarian masses and elevated CA-125 TAH/BSO, pelvic
Case 3 - GYN. History: 66 year old, routine Pap test. Dr. Stelow
 Case 3 - GYN History: 66 year old, routine Pap test Dr. Stelow Case 3 66 year year old woman Routine Pap Test Cytologic Features 3 dimensional clusters of cells with small to moderate amount of
Case 3 - GYN History: 66 year old, routine Pap test Dr. Stelow Case 3 66 year year old woman Routine Pap Test Cytologic Features 3 dimensional clusters of cells with small to moderate amount of
Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of
 Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
ENODMETRIAL CARCINOMA: SPECIAL & NOT SO SPECIAL VARIANTS
 ENODMETRIAL CARCINOMA: SPECIAL & NOT SO SPECIAL VARIANTS Pacific Northwest Society of Pathologists Vancouver, B.C. September 26, 2015 Teri A. Longacre, M.D. longacre@stanford.edu Stanford University, Stanford,
ENODMETRIAL CARCINOMA: SPECIAL & NOT SO SPECIAL VARIANTS Pacific Northwest Society of Pathologists Vancouver, B.C. September 26, 2015 Teri A. Longacre, M.D. longacre@stanford.edu Stanford University, Stanford,
Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1)
") Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1) Jae Y. Ro, MD, PhD June 7, 2012 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths By Sex, United States,
Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1) Jae Y. Ro, MD, PhD June 7, 2012 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths By Sex, United States,
Despite advances in our understanding of appendiceal. An Update on the Diagnosis, Grading, and Staging of Appendiceal Mucinous Neoplasms
 REVIEW ARTICLE An Update on the Diagnosis, Grading, and Staging of Appendiceal Mucinous Neoplasms Mark A. Valasek, MD, PhD* and Reetesh K. Pai, MD Abstract: Despite advances in our understanding of appendiceal
REVIEW ARTICLE An Update on the Diagnosis, Grading, and Staging of Appendiceal Mucinous Neoplasms Mark A. Valasek, MD, PhD* and Reetesh K. Pai, MD Abstract: Despite advances in our understanding of appendiceal
Objectives. Salivary Gland FNA: The Milan System. Role of Salivary Gland FNA 04/26/2018
 Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Icd 10 ovarian stroma
 Icd 10 ovarian stroma Struma ovarii; Micrograph of a struma ovarii. Characteristic thyroid follicles are seen on the right, and ovarian stroma on the left. H&E stain. Classification and. Free, official
Icd 10 ovarian stroma Struma ovarii; Micrograph of a struma ovarii. Characteristic thyroid follicles are seen on the right, and ovarian stroma on the left. H&E stain. Classification and. Free, official
64 YO lady THBSO for prolapse At gross : A 3 cm endometrial polyp in the fundus
 Case 6 64 YO lady THBSO for prolapse At gross : A 3 cm endometrial polyp in the fundus Numerous irregular, large glands with leaf-like pattern Large glands with broad-based papillary infolding into the
Case 6 64 YO lady THBSO for prolapse At gross : A 3 cm endometrial polyp in the fundus Numerous irregular, large glands with leaf-like pattern Large glands with broad-based papillary infolding into the
05/07/2018. Types of challenges. Challenging cases in uterine pathology. Case 1 ` 65 year old female Post menopausal bleeding Uterine Polyp
 Types of challenges Challenging cases in uterine pathology Nafisa Wilkinson Gynaecological Pathologist UCLH London Lack of complete history often, NO clinical history at all! Cases from other centres often
Types of challenges Challenging cases in uterine pathology Nafisa Wilkinson Gynaecological Pathologist UCLH London Lack of complete history often, NO clinical history at all! Cases from other centres often
MRI features of primary and metastatic mucinous ovarian tumors
 MRI features of primary and metastatic mucinous ovarian tumors Poster No.: C-0551 Congress: ECR 2014 Type: Authors: Keywords: DOI: Educational Exhibit P.-E. LAURENT, J. Thomassin-Piana, A. JALAGUIER; Marseille/
MRI features of primary and metastatic mucinous ovarian tumors Poster No.: C-0551 Congress: ECR 2014 Type: Authors: Keywords: DOI: Educational Exhibit P.-E. LAURENT, J. Thomassin-Piana, A. JALAGUIER; Marseille/
THE DIFFICULT DIAGNOSIS IN THE URINARY BLADDER: A SELECTIVE CONSIDERATION, MULLERIAN AND MULLERIAN- LIKE CONDITIONS. Robert H. Young, M.D.
 THE DIFFICULT DIAGNOSIS IN THE URINARY BLADDER: A SELECTIVE CONSIDERATION, MULLERIAN AND MULLERIAN- LIKE CONDITIONS Robert H. Young, M.D. Benign and malignant müllerian lesions Mullerian-like appearances
THE DIFFICULT DIAGNOSIS IN THE URINARY BLADDER: A SELECTIVE CONSIDERATION, MULLERIAN AND MULLERIAN- LIKE CONDITIONS Robert H. Young, M.D. Benign and malignant müllerian lesions Mullerian-like appearances
Endometrial hyperplasia vs. Intraepithelial neoplasia. Martin Chang, MD PhD FRCPC Pathology Update Friday November 9, 2012
 Endometrial hyperplasia vs. Intraepithelial neoplasia Martin Chang, MD PhD FRCPC Pathology Update Friday November 9, 2012 Disclosure No relevant financial conflicts to declare. Case 1 Gland crowding Gland
Endometrial hyperplasia vs. Intraepithelial neoplasia Martin Chang, MD PhD FRCPC Pathology Update Friday November 9, 2012 Disclosure No relevant financial conflicts to declare. Case 1 Gland crowding Gland
Update in Salivary Gland Pathology. Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016
 Update in Salivary Gland Pathology Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016 Objectives Review the different appearances of a selection of salivary gland tumor types Establish
Update in Salivary Gland Pathology Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016 Objectives Review the different appearances of a selection of salivary gland tumor types Establish
Metastatic Ovarian Carcinoma of Large Intestinal Origin Simulating Primary Ovarian Carcinoma
 ANATOMIC PATHOLOGY Original Article Metastatic Ovarian Carcinoma of Large Intestinal Origin Simulating Primary Ovarian Carcinoma A Clinicopathologic Study of 25 Cases DEAN DAYA, M.D., F.R.C.P.(C), LATIFA
ANATOMIC PATHOLOGY Original Article Metastatic Ovarian Carcinoma of Large Intestinal Origin Simulating Primary Ovarian Carcinoma A Clinicopathologic Study of 25 Cases DEAN DAYA, M.D., F.R.C.P.(C), LATIFA
TUMOR AND TUMOR-LIKE CONDITIONS OF THE PERITONEUM AND OMENTUM/MESENTERY 40 th. Annual Meeting SCBTMR September 9-13, 2017, Nashville, Tennessee
 TUMOR AND TUMOR-LIKE CONDITIONS OF THE PERITONEUM AND OMENTUM/MESENTERY 40 th. Annual Meeting SCBTMR September 9-13, 2017, Nashville, Tennessee Isaac R Francis University of Michigan Department of Radiology
TUMOR AND TUMOR-LIKE CONDITIONS OF THE PERITONEUM AND OMENTUM/MESENTERY 40 th. Annual Meeting SCBTMR September 9-13, 2017, Nashville, Tennessee Isaac R Francis University of Michigan Department of Radiology
The Origin of Pelvic Low-Grade Serous Proliferative Lesions
 The Origin of Pelvic Low-Grade Serous Proliferative Lesions Ovarian Atypical Proliferative (Borderline) Serous Tumors, Noninvasive Implants and Endosalpingiosis Robert J. Kurman, M.D. Kurman RJ, Vang R,
The Origin of Pelvic Low-Grade Serous Proliferative Lesions Ovarian Atypical Proliferative (Borderline) Serous Tumors, Noninvasive Implants and Endosalpingiosis Robert J. Kurman, M.D. Kurman RJ, Vang R,
Diseases of the breast (1 of 2)
") Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
ONCOLOGY. Csaba Bödör. Department of Pathology and Experimental Cancer Research november 19., ÁOK, III.
 ONCOLOGY Csaba Bödör Department of Pathology and Experimental Cancer Research 2018. november 19., ÁOK, III. bodor.csaba1@med.semmelweis-univ.hu ONCOLOGY Characteristics of Benign and Malignant Neoplasms
ONCOLOGY Csaba Bödör Department of Pathology and Experimental Cancer Research 2018. november 19., ÁOK, III. bodor.csaba1@med.semmelweis-univ.hu ONCOLOGY Characteristics of Benign and Malignant Neoplasms
ACCME/Disclosures. Case History 4/13/2016. USCAP GU Specialty Conference Case 3. Ann Arbor, MI
 USCAP GU Specialty Conference Case 3 March 2016 L. Priya Kunju, M.D. University of Michigan Health System Ann Arbor, MI University of Michigan Health System ACCME/Disclosures The USCAP requires that anyone
USCAP GU Specialty Conference Case 3 March 2016 L. Priya Kunju, M.D. University of Michigan Health System Ann Arbor, MI University of Michigan Health System ACCME/Disclosures The USCAP requires that anyone
Normal endometrium: A, proliferative. B, secretory.
 Normal endometrium: A, proliferative. B, secretory. Nội mạc tử cung Nội mạc tử cung Cyclic changes in endometrium.. Approximate relationship of useful microscopic changes. Arias-Stella reaction in endometrial
Normal endometrium: A, proliferative. B, secretory. Nội mạc tử cung Nội mạc tử cung Cyclic changes in endometrium.. Approximate relationship of useful microscopic changes. Arias-Stella reaction in endometrial
Diagnostically Challenging Cases in Gynecologic Pathology
 Diagnostically Challenging Cases in Gynecologic Pathology Eric C. Huang, M.D., Ph.D. Department of Pathology and Laboratory Medicine University of California, Davis Medical Center Case 1 Presentation 38
Diagnostically Challenging Cases in Gynecologic Pathology Eric C. Huang, M.D., Ph.D. Department of Pathology and Laboratory Medicine University of California, Davis Medical Center Case 1 Presentation 38
Neoplasia literally means "new growth.
 NEOPLASIA Neoplasia literally means "new growth. A neoplasm, defined as "an abnormal mass of tissue the growth of which exceeds and is uncoordinated with that of the normal tissues and persists in the
NEOPLASIA Neoplasia literally means "new growth. A neoplasm, defined as "an abnormal mass of tissue the growth of which exceeds and is uncoordinated with that of the normal tissues and persists in the
Update on Thyroid FNA The Bethesda System. Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center
 Update on Thyroid FNA The Bethesda System Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center Thyroid Nodules Frequent occurrence Palpable: 4-7% of adults Ultrasound: 10-31% Majority benign
Update on Thyroid FNA The Bethesda System Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center Thyroid Nodules Frequent occurrence Palpable: 4-7% of adults Ultrasound: 10-31% Majority benign
Ph.D. THESIS ENDOMETRIAL HYPERPLASIAS IN PERIMENOPAUSE SUMMARY
 UNIVERSITY OF MEDICINE AND PHARMACY OF CRAIOVA FACULTY OF MEDICINE Ph.D. THESIS ENDOMETRIAL HYPERPLASIAS IN PERIMENOPAUSE SUMMARY SCIENTIFIC COORDINATOR: PROF. DR. MIHAI B. BRĂILA, Ph.D. Ph.D. Graduand:
UNIVERSITY OF MEDICINE AND PHARMACY OF CRAIOVA FACULTY OF MEDICINE Ph.D. THESIS ENDOMETRIAL HYPERPLASIAS IN PERIMENOPAUSE SUMMARY SCIENTIFIC COORDINATOR: PROF. DR. MIHAI B. BRĂILA, Ph.D. Ph.D. Graduand:
GOBLET CELL CARCINOID. Hanlin L. Wang, MD, PhD University of California Los Angeles
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles hanlinwang@mednet.ucla.edu Goblet cell carcinoid (GCC) is a unique type of mixed endocrine-exocrine neoplasm, almost exclusively
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles hanlinwang@mednet.ucla.edu Goblet cell carcinoid (GCC) is a unique type of mixed endocrine-exocrine neoplasm, almost exclusively
1.Acute and Chronic Cervicitis - At the onset of menarche, the production of estrogens by the ovary stimulates maturation of the cervical and vaginal
 Diseases of cervix I. Inflammations 1.Acute and Chronic Cervicitis - At the onset of menarche, the production of estrogens by the ovary stimulates maturation of the cervical and vaginal squamous mucosa
Diseases of cervix I. Inflammations 1.Acute and Chronic Cervicitis - At the onset of menarche, the production of estrogens by the ovary stimulates maturation of the cervical and vaginal squamous mucosa
Neoplasia part I. Dr. Mohsen Dashti. Clinical Medicine & Pathology nd Lecture
 Neoplasia part I By Dr. Mohsen Dashti Clinical Medicine & Pathology 316 2 nd Lecture Lecture outline Review of structure & function. Basic definitions. Classification of neoplasms. Morphologic features.
Neoplasia part I By Dr. Mohsen Dashti Clinical Medicine & Pathology 316 2 nd Lecture Lecture outline Review of structure & function. Basic definitions. Classification of neoplasms. Morphologic features.