Management of an Appendiceal Mass - Approach to acute presentation of appendiceal neoplasms
|
|
|
- Arlene Hawkins
- 5 years ago
- Views:
Transcription


1 Management of an Appendiceal Mass - Approach to acute presentation of appendiceal neoplasms Dr. Claudia LY WONG, Department of Surgery, Kwong Wah Hospital Joint Hospital Surgical Grand Round Presentation, Princess Margaret Hospital, April 20, 2013


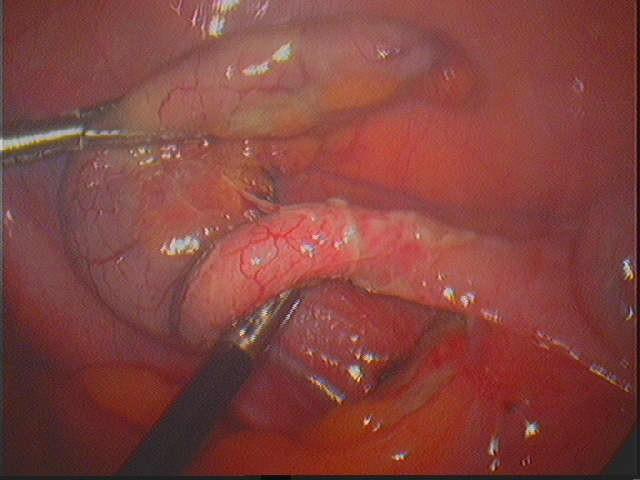
2 Case Scenario M/42; unremarkable past health Periumbilical pain shifted to right lower quadrant for two days Associated with nausea and subjective account of fever Physical examination: Temperature 38.9oC; Stable hemodynamics Localized tenderness and fullness over right lower quadrant

3 Suspected Appendiceal Neoplasm A CT scan was performed Complex cystic appendix with thickened wall Suspicious of underlying neoplasm Tachycardia, persistent tenderness and pyrexia despite antibiotic therapy
4
5 Introduction 1. Overview of commonest appendiceal neoplasms and mucocele 2. Management of acutely presenting appendiceal mass suspicious of underlying neoplasm
 Appendiceal tumors: retrospective clinicopathologic analysis of appendiceal tumors from 7,970 appendectomies.")
6 Differential diagnoses Neoplasms of vermiform appendix Connor et al. (1998) Appendiceal tumors: retrospective clinicopathologic analysis of appendiceal tumors from 7,970 appendectomies. Secondaries from urogenital tract (ovaries), large bowel, lung and breast Others (rare): ganglioneuroma, pheochromocytoma, mesenchymal tumors, Kaposi sarcoma Appendiceal mucocele
7 Appendiceal Neoplasms & Mucoceles

8 Appendiceal Carcinoid Neuroendocrine origin, arise from primitive stem cell Classified according to location of primitive gut Deep in mucosa for intestinal carcinoids Appendix is the commonest site for carcinoid tumor Carcinoid is the commonest primary neoplasm of the appendix


9 Appendiceal Carcinoid % appendicectomies; usually asymptomatic, incidental finding in appendicitis Most affect distal 1/3; invade wall Symptoms occur with metastasis (rare) Liver metastases are rare; Lymphatic spread as 1* route Worse outcome with large size (>1.5-2cm), goblet cell carcinoid (adenocarcinoid)


10 Intestinal and Mucinous Neoplasms Benign: adenomas, cystoadenomas Malignant: adeno/ cystoadenocarcinomas More goblet cells in appendix than in colon -> majority of neoplasms are mucinous in nature
11 Cystoadenocarcinoma (mucinous) Appendiceal carcinomas: 90% mucinous (vs intestinal type) Mucinous subtype: Tip or along lumen Mucocele formation Dissemination to peritoneal space, pseudomyxoma peritonei
12 Adenocarcinomas (intestinal) Appendiceal carcinomas: 10% intestinal type Intestinal subtype: Appendiceal orifice Lymph node spread

; abdominal pain (27%), mass (16%), weight loss (10%), appendicitis (8%) 20% In the presence of pseudomyxoma peritonei or")
13 Appendiceal Mucoceles A rare but not entirely separate entity Morphological description Histological Subtypes of Appendiceal Mucoceles Cystic dilatation of appendix caused by accumulation of mucus secretion 10% % appendicetomy specimens 18% Course and prognosis depends on histological subtype 52% Luca et al. Surgical Management of Appendiceal Mucocele. Arch Surg. 2003; 138: Often asymptomatic (51%); abdominal pain (27%), mass (16%), weight loss (10%), appendicitis (8%) 20% In the presence of pseudomyxoma peritonei or mucinous dissemination, 80-90% are malignant Mucinous cystadenomas Mucosal hyperplasia Simple mucoceles/retention cysts Mucinous cystadenocarcinomas
14 Management of Suspected Appendiceal Neoplasms
15
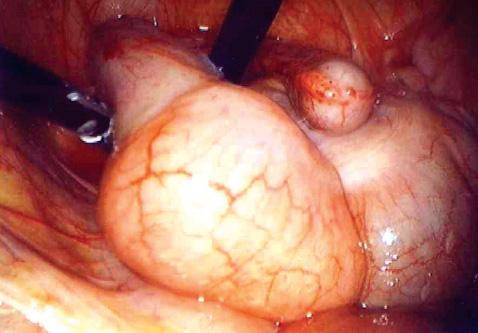
16 1. Emergency Surgery Detailed laparoscopy Macroscopic features of index lesion: Location on appendix, caecal involvement Mesoappendiceal involvement Size of lesion (>2cm) Any mucinous dissemination or spontaneous perforation Any other primary lesion (appendiceal secondary?)
17 1. Emergency Surgery Pathology and histological characteristics of appendiceal tumor determine extent of definitive surgical resection and need of prophylactic lymph node removal Achieve macroscopic resection margin, including mesoappenix Appendicectomy, ileocaectomy, right hemicolectomy? Avoid trauma or rupture during removal Use of endobag; retrieval from midline (facilitate port site removal if necessary) Thorough peritoneal washout if mucinous dissemination Wait for histology result and consider second operation
18 2. Further Investigations? Non-carcinoid neoplasms: Carcinoid neoplasms: Tumor markers: CA-125, CA-19-9, CEA (in mucinous peritoneal carcinomatosis) Serotonin metabolite 5-HIAA 24- hour urine sample; chromogranin A (lower specificity) Computed tomography: look for distant metastasis, serve as baseline for disease monitoring Surveillance colonoscopy: ALL appendiceal neoplasms are associated with synchronous or metachronous colonic neoplasms Nuclear imaging: OctreoScan (somatostatin analogue) (80% carcinoid with somatostatin receptor); metaiodobenzylguanidine (MIBG) scan PET scan: based on metabolism of trytophan
19 3. When to Consider Completion Right Hemicolectomy? Prophylactic resection for occult lymph node metastasis Based on histolopathological findings of initial resection Carcinoid: right hemicolectomy is recommended for lesions >2cm Increased probability of nodal involvement 30% (<0.1% for lesions <1cm) (Sutton et al); controversy for lesions between 1-2cm Involvement of mesoappendix, atypical microscopic foci, mitotic count of 2 or more per HPF, goblet cell type
20 3. When to Consider Completion Right Hemicolectomy? Adenocarcinoma: tradition approach is to offer right hemicolectomy Much higher incidence of lymph node metastasis in adenocarcinoma (66.7%) than mucinous carinoma (4.2%) (Gonazlex Moreno et al) >2cm, poor differentiation, lymphovascular permeation, submucosal invasion Mucinous adenocarcinoma: more selective approach to right hemicolectomy Median survival similar for those with or without lymph node involvement (28 vs 26 months) (Kiran at al)
21 3. When to Consider Completion Right Hemicolectomy? Presence of mucinous dissemination: Low grade mucinous neoplasms: no recurrence in 6-year follow-up vs those with extra-appendiceal spread: 45% 5-year survival Radical resection does not alter prognosis of mucinous neoplasm with peritoneal dissemination Not advisable unless intraperitoneal chemotherapy and cytoreductive surgery
22 4. Adjunctive Therapy? Carcinoid neoplasms: Metastatic carcinoid: 5-fluorouracil (5-FU) and leucovorin Hepatic metastases: resection/ablation, interferon, hepatic artery embolization (>50% involvement), long-acting somatostatin analogue (carcinoid syndrome) Non-carcinoid neoplasms: NO controlled study Same regime as colonic adenocarcinoma Poor tumor response in case of peritoneal dissemination; intraperitoneal heated chemotherapy
23 Management Algorithm for Suspected Appendiceal Neoplasm Acute appendiceal mass (suspicious CT findings) Failed antibotic therapy Emergency resection (macroscopic margin + mesoappendix) Histology proven neoplasm Further investigations (tumor markers, imaging, colonoscopy) Determine need for completion right hemicolectomy Specialist centre referral/oncologist referral/surveillance
24 Conclusion Appendiceal neoplasms are rare but often present as acute appendicitis Most common lesions are carcinoid neoplasms & adenoma/ adenocarcinoma of intestinal and mucinous types Initial treatment without prior histological diagnosis proves a challenge Achieve macroscopic margin with careful specimen handling Option of a planned second operation is available Follow up management including surveillance colonoscopy is necessary
25 References Walters et al. Treatment of appendiceal adenocarcinoma in the United States: penetration and outcomes of current guidelines. Am Surg. 74(11):1066-8, 2008 Nov Murphy et al. Management of an Unexpected Appendiceal Neoplasm. British Journal of Surgery 2006; 93: Groth et al. Appendiceal carcinoid tumors: Predictors of lymph node metastasis and the impact of right hemicolectomy on survival. J Surg Oncol Jan 1;103(1): Goede, A. C., Caplin, M. E. and Winslet, M. C. (2003), Carcinoid tumour of the appendix. Br J Surg, 90: Connor SJ, Hanna GB, Frizelle FA. Appendiceal tumors: retrospective clinicopathologic analysis of appendiceal tumors from 7,970 appendectomies. Dis Colon Rectum Jan;41(1): Whitefield et al. Surgical management of primary appendiceal malignancy. Colorectal Dis 2012; 14, Luca et al. Surgical Management of Appendiceal Mucocele. Arch Surg. 2003; 138:
Surgical Management of Neuroendocrine Tumors of the Gut. Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School
 Surgical Management of Neuroendocrine Tumors of the Gut Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School Sites of GI Carcinoid Tumors Small intestine 44% Rectum
Surgical Management of Neuroendocrine Tumors of the Gut Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School Sites of GI Carcinoid Tumors Small intestine 44% Rectum
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital
 Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Low-grade appendiceal mucinous neoplasm (LAMN) High-grade appendiceal mucinous neoplasm (HAMN) Adenocarcinoma
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Low-grade appendiceal mucinous neoplasm (LAMN) High-grade appendiceal mucinous neoplasm (HAMN) Adenocarcinoma
Appendiceal Adenocarcinoma with Suppurative Appendicitis: Case Report and Literature Review
 Appendiceal adenocarcinoma presenting with acute appendicitis 155 Appendiceal Adenocarcinoma with Suppurative Appendicitis: Case Report and Literature Review Va-Kei Kok 1, Teh-Kuang Wang 2, Hsi-Che Shen
Appendiceal adenocarcinoma presenting with acute appendicitis 155 Appendiceal Adenocarcinoma with Suppurative Appendicitis: Case Report and Literature Review Va-Kei Kok 1, Teh-Kuang Wang 2, Hsi-Che Shen
GOBLET CELL CARCINOID. Hanlin L. Wang, MD, PhD University of California Los Angeles
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
Community Case. Saeed Awan R5
 Community Case Saeed Awan R5 18 year old presents to ER with history of pain right lower quadrant for three days. Nauseated, denies vomiting and bowel movements normal and no urinary complaint. Admitted
Community Case Saeed Awan R5 18 year old presents to ER with history of pain right lower quadrant for three days. Nauseated, denies vomiting and bowel movements normal and no urinary complaint. Admitted
World Journal of Colorectal Surgery
 World Journal of Colorectal Surgery Volume 6, Issue 4 2016 Article 3 Laparoscopic Right Colectomy For Appendiceal Mucinous Cystadenoma: A Case Report Dion A. Putra Adianto Nugroho Ibrahim Basir University
World Journal of Colorectal Surgery Volume 6, Issue 4 2016 Article 3 Laparoscopic Right Colectomy For Appendiceal Mucinous Cystadenoma: A Case Report Dion A. Putra Adianto Nugroho Ibrahim Basir University
BC CRC Update Unusual Colorectal Tumors
 BC CRC Update Unusual Colorectal Tumors Anthony MacLean, MD, FRCSC, FACS, FASCRS Colorectal Surgeon Foothills Medical Centre Clinical Associate Professor of Surgery and Oncology University of Calgary I
BC CRC Update Unusual Colorectal Tumors Anthony MacLean, MD, FRCSC, FACS, FASCRS Colorectal Surgeon Foothills Medical Centre Clinical Associate Professor of Surgery and Oncology University of Calgary I
COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING
 COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING COLON AND RECTUM SOLID TUMOR RULES Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent Terms Terms that are NOT Equivalent
COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING COLON AND RECTUM SOLID TUMOR RULES Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent Terms Terms that are NOT Equivalent
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Specialised Services Policy: CP02 Hyperthermic Intraperitoneal Chemotherapy (HIPEC) and Cytoreductive Surgery for treatment of Pseudomyxoma Peritonei
 and Cytoreductive Surgery for treatment of Pseudomyxoma Peritonei") Specialised Services Policy: CP02 Hyperthermic Intraperitoneal Chemotherapy (HIPEC) of Pseudomyxoma Peritonei Document Author: Assistant Medical Director Executive Lead: Medical Director Approved by: Management
Specialised Services Policy: CP02 Hyperthermic Intraperitoneal Chemotherapy (HIPEC) of Pseudomyxoma Peritonei Document Author: Assistant Medical Director Executive Lead: Medical Director Approved by: Management
Colon and Rectum: 2018 Solid Tumor Rules
 2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING Colon and Rectum: 2018 Solid Tumor Rules 1 Colon and Rectum Solid Tumor Rules Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent
2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING Colon and Rectum: 2018 Solid Tumor Rules 1 Colon and Rectum Solid Tumor Rules Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent
Review Article Cancers of the Appendix: Review of the Literatures
 International Scholarly Research Network ISRN Oncology Volume 2011, Article ID 728579, 6 pages doi:10.5402/2011/728579 Review Article Cancers of the Appendix: Review of the Literatures Carl Ruoff, 1 Louay
International Scholarly Research Network ISRN Oncology Volume 2011, Article ID 728579, 6 pages doi:10.5402/2011/728579 Review Article Cancers of the Appendix: Review of the Literatures Carl Ruoff, 1 Louay
Goblet Cell Carcinoids of the Appendix
 40 Ulster Med J 2006; 75 (1) 40-45 The Ulster Medical Journal Review Goblet Cell Carcinoids of the Appendix R Arnold, K McCallion, C McGailie Accepted 14 October 2005 INTRODUCTION Carcinoid tumours are
40 Ulster Med J 2006; 75 (1) 40-45 The Ulster Medical Journal Review Goblet Cell Carcinoids of the Appendix R Arnold, K McCallion, C McGailie Accepted 14 October 2005 INTRODUCTION Carcinoid tumours are
CT PET SCANNING for GIT Malignancies A clinician s perspective
 CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
Pre-operative assessment of patients for cytoreduction and HIPEC
 Pre-operative assessment of patients for cytoreduction and HIPEC Washington Hospital Center Washington, DC, USA Ovarian Cancer Surgery New Strategies Bergamo, Italy May 5, 2011 Background Cytoreductive
Pre-operative assessment of patients for cytoreduction and HIPEC Washington Hospital Center Washington, DC, USA Ovarian Cancer Surgery New Strategies Bergamo, Italy May 5, 2011 Background Cytoreductive
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Management of Rare Liver Tumours
 Gian Luca Grazi Hepato-Biliary-Pancreatic Surgery National Cancer Institute Regina Elena Rome Fibrolamellar Carcinoma Mixed Hepato Cholangiocellular Carcinoma Hepatoblastoma Carcinosarcoma Primary Hepatic
Gian Luca Grazi Hepato-Biliary-Pancreatic Surgery National Cancer Institute Regina Elena Rome Fibrolamellar Carcinoma Mixed Hepato Cholangiocellular Carcinoma Hepatoblastoma Carcinosarcoma Primary Hepatic
Cancers of the appendix: a case report and review of the literatures
 International Journal of Research in Medical Sciences Devi YS et al. Int J Res Med Sci. 2016 Nov;4(11):5055-5060 www.msjonline.org pissn 2320-6071 eissn 2320-6012 Case Report DOI: http://dx.doi.org/10.18203/2320-6012.ijrms20163817
International Journal of Research in Medical Sciences Devi YS et al. Int J Res Med Sci. 2016 Nov;4(11):5055-5060 www.msjonline.org pissn 2320-6071 eissn 2320-6012 Case Report DOI: http://dx.doi.org/10.18203/2320-6012.ijrms20163817
SCOPE TODAYS SESSION. Case 1: Case 2. Basic Theory Stuff: Heavy Stuff. Basic Questions. Basic Questions
 MONDAY TEACHING SCOPE TODAYS SESSION Case 1: Basic Questions Case 2 Basic Questions Basic Theory Stuff: AJCC TNM + Stage Group for Carcinoid of the Appendix Management of Carcinoid of the Appendix (NCCN)
MONDAY TEACHING SCOPE TODAYS SESSION Case 1: Basic Questions Case 2 Basic Questions Basic Theory Stuff: AJCC TNM + Stage Group for Carcinoid of the Appendix Management of Carcinoid of the Appendix (NCCN)
GOBLET CELL CARCINOID. Hanlin L. Wang, MD, PhD University of California Los Angeles
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles hanlinwang@mednet.ucla.edu Goblet cell carcinoid (GCC) is a unique type of mixed endocrine-exocrine neoplasm, almost exclusively
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles hanlinwang@mednet.ucla.edu Goblet cell carcinoid (GCC) is a unique type of mixed endocrine-exocrine neoplasm, almost exclusively
Appendiceal diverticular disease
 Formosan Journal of Surgery (2013) 46, 4e9 Available online at www.sciencedirect.com journal homepage: www.e-fjs.com ORIGINAL ARTICLE Appendiceal diverticular disease Yun-Wu Deng a, Hsiao-Bai Yang b,e,
Formosan Journal of Surgery (2013) 46, 4e9 Available online at www.sciencedirect.com journal homepage: www.e-fjs.com ORIGINAL ARTICLE Appendiceal diverticular disease Yun-Wu Deng a, Hsiao-Bai Yang b,e,
Patient Presentation. 32 y.o. female complains of lower abdominal mass CEA = 433, CA125 = 201
 Patient Presentation 32 y.o. female complains of lower abdominal mass CEA = 433, CA125 = 201 CT shows: Thickening of the right hemidiaphragm CT shows: Fluid in the right paracolic sulcus CT shows: Large
Patient Presentation 32 y.o. female complains of lower abdominal mass CEA = 433, CA125 = 201 CT shows: Thickening of the right hemidiaphragm CT shows: Fluid in the right paracolic sulcus CT shows: Large
Appendix cancer mimicking ovarian cancer
 Int J Gynecol Cancer 2002, 12, 768 772 CORRESPONDENCE AND BRIEF REPORTS Appendix cancer mimicking ovarian cancer P. A. GEHRIG *, J. F. BOGGESS*, D. W. OLLILA, P. A. GROBEN & L. VAN LE* *Division of Gynecologic
Int J Gynecol Cancer 2002, 12, 768 772 CORRESPONDENCE AND BRIEF REPORTS Appendix cancer mimicking ovarian cancer P. A. GEHRIG *, J. F. BOGGESS*, D. W. OLLILA, P. A. GROBEN & L. VAN LE* *Division of Gynecologic
Adenocarcinoma of the Appendix
 Adenocarcinoma of the Appendix K atrina Craig, cst Once in a while, what is thought to be a routine appendectomy becomes a more critical issue when cancer is discovered in the appendix. This is a rare
Adenocarcinoma of the Appendix K atrina Craig, cst Once in a while, what is thought to be a routine appendectomy becomes a more critical issue when cancer is discovered in the appendix. This is a rare
Color Codes Pathology and Genetics Medicine and Clinical Pathology Surgery Imaging
 Saturday, November 5, 2005 8:30-10:30 a. m. Poorly Differentiated Endocrine Carcinomas Chairman: E. Van Cutsem, Leuven, Belgium 9:00-9:30 a. m. Working Group Sessions Pathology and Genetics Group leaders:
Saturday, November 5, 2005 8:30-10:30 a. m. Poorly Differentiated Endocrine Carcinomas Chairman: E. Van Cutsem, Leuven, Belgium 9:00-9:30 a. m. Working Group Sessions Pathology and Genetics Group leaders:
TREATMENT OF PERITONEAL COLORECTAL CARCINOMATOSIS
 TREATMENT OF PERITONEAL COLORECTAL CARCINOMATOSIS Anna Lepistö, MD, PhD Department of Colorectal Surgery, Abdominal Center, Helsinki University Hospital Incidence, prevalence and risk factors for peritoneal
TREATMENT OF PERITONEAL COLORECTAL CARCINOMATOSIS Anna Lepistö, MD, PhD Department of Colorectal Surgery, Abdominal Center, Helsinki University Hospital Incidence, prevalence and risk factors for peritoneal
NET und NEC. Endoscopic and oncologic therapy
 NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
Disseminated Peritoneal Adenomucinosis Associated with a Panperitonitis-Like Onset: Report of a Case
 Surg Today (2001) 31:646 650 Disseminated Peritoneal Adenomucinosis Associated with a Panperitonitis-Like Onset: Report of a Case Yoshito Kuroki 1, Shunyou Otagiri 1, and Kazuhiro Tsukada 2 1 Department
Surg Today (2001) 31:646 650 Disseminated Peritoneal Adenomucinosis Associated with a Panperitonitis-Like Onset: Report of a Case Yoshito Kuroki 1, Shunyou Otagiri 1, and Kazuhiro Tsukada 2 1 Department
Appendiceal diverticulosis: a harbinger of underlying primary appendiceal adenocarcinoma?
 Case Report Appendiceal diverticulosis: a harbinger of underlying primary appendiceal adenocarcinoma? Jia Lin Ng 1, Shing Lih Wong 2, Ronnie Mathew 1 1 Department of Colorectal Surgery, 2 Department of
Case Report Appendiceal diverticulosis: a harbinger of underlying primary appendiceal adenocarcinoma? Jia Lin Ng 1, Shing Lih Wong 2, Ronnie Mathew 1 1 Department of Colorectal Surgery, 2 Department of
Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ).
.") SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
Specialespecifikt kursus i Patologisk Anatomi 2009: Fordøjelseskanalens patologi APPENDIX
 Specialespecifikt kursus i Patologisk Anatomi 2009: Fordøjelseskanalens patologi APPENDIX Appendix Occurrence of lesions (%) Acute appendicitis 72 Normal 16 Fibrosis 3 (Cyst-)Adenoma 3 Diverticulitis
Specialespecifikt kursus i Patologisk Anatomi 2009: Fordøjelseskanalens patologi APPENDIX Appendix Occurrence of lesions (%) Acute appendicitis 72 Normal 16 Fibrosis 3 (Cyst-)Adenoma 3 Diverticulitis
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14
 Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
PNET 3/7/2015. GI and Pancreatic NETs. The Postgraduate Course in Breast and Endocrine Surgery. Decision Tree. GI and Pancreatic NETs.
 GI and Pancreatic NETs The Postgraduate Course in Breast and Endocrine Surgery Disclosures Ipsen NET Advisory Board Marines Memorial Club and Hotel San Francisco, CA Eric K Nakakura San Francisco, CA March
GI and Pancreatic NETs The Postgraduate Course in Breast and Endocrine Surgery Disclosures Ipsen NET Advisory Board Marines Memorial Club and Hotel San Francisco, CA Eric K Nakakura San Francisco, CA March
COLON CANCER CARE GUIDELINES NON-METASTATIC DISEASE
 COLON CANCER CARE GUIDELINES NON-METASTATIC DISEASE Guideline Authors: Todd S. Crocenzi, M.D.; Mark Whiteford, M.D.; Matthew Solhjem, M.D.; Carlo Bifulco, M.D.; Melissa Li, M.D.; Christopher Cai, M.D.;
COLON CANCER CARE GUIDELINES NON-METASTATIC DISEASE Guideline Authors: Todd S. Crocenzi, M.D.; Mark Whiteford, M.D.; Matthew Solhjem, M.D.; Carlo Bifulco, M.D.; Melissa Li, M.D.; Christopher Cai, M.D.;
A916: rectum: adenocarcinoma
 General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
malignant polyp Daily Challenges in Digestive Endoscopy for Endoscopists and Endoscopy Nurses BSGIE Annual Meeting 18/09/2014 Mechelen
 Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
GI CARCINOID Dr Mussawar Iqbal Consultant Oncologist Hull and East Yorkshire Hospitals NHS Trust
 GI CARCINOID Dr Mussawar Iqbal Consultant Oncologist Hull and East Yorkshire Hospitals NHS Trust Introduction Carcinoid was old term, introduced in 1906 by German pathologist Cancinoma like More recent
GI CARCINOID Dr Mussawar Iqbal Consultant Oncologist Hull and East Yorkshire Hospitals NHS Trust Introduction Carcinoid was old term, introduced in 1906 by German pathologist Cancinoma like More recent
Hepatobiliary and Pancreatic Malignancies
 Hepatobiliary and Pancreatic Malignancies Gareth Eeson MD MSc FRCSC Surgical Oncologist and General Surgeon Kelowna General Hospital Interior Health Consultant, Surgical Oncology BC Cancer Agency Centre
Hepatobiliary and Pancreatic Malignancies Gareth Eeson MD MSc FRCSC Surgical Oncologist and General Surgeon Kelowna General Hospital Interior Health Consultant, Surgical Oncology BC Cancer Agency Centre
Brief History. Identification : Past History : HTN without regular treatment.
 Brief History Identification : Name : 陳 x - Admission : 94/10/06 Gender : male Age : 75 y/o Chief Complaint : Urinary difficulty for months. Past History : HTN without regular treatment. Brief History
Brief History Identification : Name : 陳 x - Admission : 94/10/06 Gender : male Age : 75 y/o Chief Complaint : Urinary difficulty for months. Past History : HTN without regular treatment. Brief History
HEPATIC METASTASES. We can state 3 types of metastases depending on their treatment options:
 HEPATIC METASTASES 1. Definition Metastasis means the spread of cancer. Cancerous cells can separate from the primary tumor and enter the bloodstream or the lymphatic system (the one that produces, stores,
HEPATIC METASTASES 1. Definition Metastasis means the spread of cancer. Cancerous cells can separate from the primary tumor and enter the bloodstream or the lymphatic system (the one that produces, stores,
Chapter 6 Frozen Section Evaluation of the Appendix
 Chapter 6 Frozen Section Evaluation of the Appendix Abstract Appendiceal tumors are rarely diagnosed preoperatively, and their classification is both challenging and controversial owing to their tendency
Chapter 6 Frozen Section Evaluation of the Appendix Abstract Appendiceal tumors are rarely diagnosed preoperatively, and their classification is both challenging and controversial owing to their tendency
is time consuming and expensive. An intra-operative assessment is not going to be helpful if there is no more tissue that can be taken to improve the
 My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE
 COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
HIPEC Controversies in the Indications and Application of Regional Chemotherapy for Peritoneal Surface Malignancies
 HIPEC Controversies in the Indications and Application of Regional Chemotherapy for Peritoneal Surface Malignancies Crescent City Cancer Update: GI and HPB Saturday September 24, 2016 George M. Fuhrman,
HIPEC Controversies in the Indications and Application of Regional Chemotherapy for Peritoneal Surface Malignancies Crescent City Cancer Update: GI and HPB Saturday September 24, 2016 George M. Fuhrman,
COLORECTAL CANCER CASES
 COLORECTAL CANCER CASES Case #1 Case #2 Colorectal Cancer Case 1 A 52 year-old female attends her family physician for her yearly complete physical examination. Her past medical history is significant
COLORECTAL CANCER CASES Case #1 Case #2 Colorectal Cancer Case 1 A 52 year-old female attends her family physician for her yearly complete physical examination. Her past medical history is significant
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
PET IMAGING (POSITRON EMISSION TOMOGRAPY) FACT SHEET
 FACT SHEET") Positron Emission Tomography (PET) When calling Anthem (1-800-533-1120) or using the Point of Care authorization system for a Health Service Review, the following clinical information may be needed to
Positron Emission Tomography (PET) When calling Anthem (1-800-533-1120) or using the Point of Care authorization system for a Health Service Review, the following clinical information may be needed to
Information for health professionals - pseudomyxoma peritonei
 Colorectal and peritoneal oncology centre Information for health professionals - pseudomyxoma peritonei What is it? Pseudomyxoma Peritonei (PMP) is often a slowly progressive disease that produces extensive
Colorectal and peritoneal oncology centre Information for health professionals - pseudomyxoma peritonei What is it? Pseudomyxoma Peritonei (PMP) is often a slowly progressive disease that produces extensive
Locally Advanced Colon Cancer. Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery
 Locally Advanced Colon Cancer Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery Case 34 yo man presented with severe RLQ abdominal pain X 24 hrs. No nausea/vomiting/fever. + flatus.
Locally Advanced Colon Cancer Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery Case 34 yo man presented with severe RLQ abdominal pain X 24 hrs. No nausea/vomiting/fever. + flatus.
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Case Report Laparoscopic Diagnosis of Adenocarcinoma of the Appendix Mimicking Serous Papillary Adenocarcinoma of the Peritoneum
 Case Reports in Obstetrics and Gynecology Volume 2013, Article ID 248917, 5 pages http://dx.doi.org/10.1155/2013/248917 Case Report Laparoscopic Diagnosis of Adenocarcinoma of the Appendix Mimicking Serous
Case Reports in Obstetrics and Gynecology Volume 2013, Article ID 248917, 5 pages http://dx.doi.org/10.1155/2013/248917 Case Report Laparoscopic Diagnosis of Adenocarcinoma of the Appendix Mimicking Serous
Basic Data. Birthday: Gender:Female Admission date:
 Basic Data Birthday:1951-07-02 Gender:Female Admission date:2004-06-28 Chief Complaint A protruding mass over RLQ abdomen for many years. Present Illness & Past History Pseudomyxoma peritonei s/p laparotomy
Basic Data Birthday:1951-07-02 Gender:Female Admission date:2004-06-28 Chief Complaint A protruding mass over RLQ abdomen for many years. Present Illness & Past History Pseudomyxoma peritonei s/p laparotomy
Gastrinoma: Medical Management. Haley Gallup
 Gastrinoma: Medical Management Haley Gallup Also known as When to put your knife down Gastrinoma Definition and History Diagnosis Historic Management Sporadic vs MEN-1 Defining surgical candidates Nonsurgical
Gastrinoma: Medical Management Haley Gallup Also known as When to put your knife down Gastrinoma Definition and History Diagnosis Historic Management Sporadic vs MEN-1 Defining surgical candidates Nonsurgical
COLORECTAL CARCINOMA
 QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
Appendix adenocarcinomas are rare and heterogeneous
 ORIGINAL CONTRIBUTION Predicting Survival After Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy for Appendix Adenocarcinoma Omer Aziz, Ph.D., F.R.C.S. 1,2 Ihab Jaradat, F.R.C.S. 1 Bipasha
ORIGINAL CONTRIBUTION Predicting Survival After Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy for Appendix Adenocarcinoma Omer Aziz, Ph.D., F.R.C.S. 1,2 Ihab Jaradat, F.R.C.S. 1 Bipasha
SMALL BOWEL ADENOCARCINOMA. Dr. C. Jeske
 SMALL BOWEL ADENOCARCINOMA Dr. C. Jeske Case presentation 54 year old female. Presents with OJ and weight loss. Abdominal examination only reveals a palpable gallbladder. ERCP reveals a circumferential
SMALL BOWEL ADENOCARCINOMA Dr. C. Jeske Case presentation 54 year old female. Presents with OJ and weight loss. Abdominal examination only reveals a palpable gallbladder. ERCP reveals a circumferential
Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012
 Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012 Version Control This is a controlled document please destroy all previous versions on receipt
Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012 Version Control This is a controlled document please destroy all previous versions on receipt
Staging Colorectal Cancer
 Staging Colorectal Cancer CT is recommended as the initial staging scan for colorectal cancer to assess local extent of the disease and to look for metastases to the liver and/or lung Further imaging for
Staging Colorectal Cancer CT is recommended as the initial staging scan for colorectal cancer to assess local extent of the disease and to look for metastases to the liver and/or lung Further imaging for
Liver Cancer (Hepatocellular Carcinoma or HCC) Overview
 Overview") Liver Cancer (Hepatocellular Carcinoma or HCC) Overview Recent advances in liver cancer care seek to address the rising incidence of liver cancer, which has steadily increased over the past three decades.
Liver Cancer (Hepatocellular Carcinoma or HCC) Overview Recent advances in liver cancer care seek to address the rising incidence of liver cancer, which has steadily increased over the past three decades.
CLINICAL VIGNETTE 2016; 2:1
 CLINICAL VIGNETTE 2016; 2:1 Editor-in-Chief: Olufemi E. Idowu. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria. MANAGEMENT OF APPENDICITIS Ibrahim NA, Njokanma
CLINICAL VIGNETTE 2016; 2:1 Editor-in-Chief: Olufemi E. Idowu. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria. MANAGEMENT OF APPENDICITIS Ibrahim NA, Njokanma
Neoplasia literally means "new growth.
 NEOPLASIA Neoplasia literally means "new growth. A neoplasm, defined as "an abnormal mass of tissue the growth of which exceeds and is uncoordinated with that of the normal tissues and persists in the
NEOPLASIA Neoplasia literally means "new growth. A neoplasm, defined as "an abnormal mass of tissue the growth of which exceeds and is uncoordinated with that of the normal tissues and persists in the
Cytoreductive surgery and perioperative intraperitoneal chemotherapy for Rare Peritoneal Disease. Results of the French multicentric database
 Cytoreductive surgery and perioperative intraperitoneal chemotherapy for Rare Peritoneal Disease Results of the French multicentric database Université Lyon 1 Centre Hospitalo-Universitaire Lyon-Sud EA
Cytoreductive surgery and perioperative intraperitoneal chemotherapy for Rare Peritoneal Disease Results of the French multicentric database Université Lyon 1 Centre Hospitalo-Universitaire Lyon-Sud EA
Structured Follow-Up after Colorectal Cancer Resection: Overrated. R. Taylor Ripley University of Colorado Grand Rounds April 23, 2007
 Structured Follow-Up after Colorectal Cancer Resection: Overrated R. Taylor Ripley University of Colorado Grand Rounds April 23, 2007 Guidelines for Colonoscopy Production: Surveillance US Multi-Society
Structured Follow-Up after Colorectal Cancer Resection: Overrated R. Taylor Ripley University of Colorado Grand Rounds April 23, 2007 Guidelines for Colonoscopy Production: Surveillance US Multi-Society
Despite advances in our understanding of appendiceal. An Update on the Diagnosis, Grading, and Staging of Appendiceal Mucinous Neoplasms
 REVIEW ARTICLE An Update on the Diagnosis, Grading, and Staging of Appendiceal Mucinous Neoplasms Mark A. Valasek, MD, PhD* and Reetesh K. Pai, MD Abstract: Despite advances in our understanding of appendiceal
REVIEW ARTICLE An Update on the Diagnosis, Grading, and Staging of Appendiceal Mucinous Neoplasms Mark A. Valasek, MD, PhD* and Reetesh K. Pai, MD Abstract: Despite advances in our understanding of appendiceal
Disclosure. Acknowledgement. What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Rectal cancer imaging. None
 What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
Subepithelial Lesions of the Gut: When Should I Worry?
 Subepithelial Lesions of the Gut: When Should I Worry? President, ASGE Chairman, GI & Hepatology Scottsdale, AZ Faigel.douglas@mayo.edu Case 55 yo male with reflux EGD for Barrett s Screening SET, mucosal
Subepithelial Lesions of the Gut: When Should I Worry? President, ASGE Chairman, GI & Hepatology Scottsdale, AZ Faigel.douglas@mayo.edu Case 55 yo male with reflux EGD for Barrett s Screening SET, mucosal
Clinical Study Small Bowel Tumors: Clinical Presentation, Prognosis, and Outcomein33PatientsinaTertiaryCareCenter
 Hindawi Publishing Corporation Journal of Oncology Volume 2008, Article ID 212067, 5 pages doi:10.1155/2008/212067 Clinical Study Small Bowel Tumors: Clinical Presentation, Prognosis, and Outcomein33PatientsinaTertiaryCareCenter
Hindawi Publishing Corporation Journal of Oncology Volume 2008, Article ID 212067, 5 pages doi:10.1155/2008/212067 Clinical Study Small Bowel Tumors: Clinical Presentation, Prognosis, and Outcomein33PatientsinaTertiaryCareCenter
Neuroendocrine Tumors
 Neuroendocrine Tumors Neuroendocrine tumors arise from cells that release a hormone in response to a signal from the nervous system. Neuro refers to the nervous system. Endocrine refers to the hormones.
Neuroendocrine Tumors Neuroendocrine tumors arise from cells that release a hormone in response to a signal from the nervous system. Neuro refers to the nervous system. Endocrine refers to the hormones.
ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID
 ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID Manoop S. Bhutani, MD, FASGE, FACG, FACP, AGAF, Doctor Honoris Causa Professor of Medicine Eminent Scientist of the Year 2008, World
ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID Manoop S. Bhutani, MD, FASGE, FACG, FACP, AGAF, Doctor Honoris Causa Professor of Medicine Eminent Scientist of the Year 2008, World
AJCC 7 th Edition Staging Disease Site Webinar Colorectum
 AJCC 7 th Edition Staging Disease Site Webinar Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310
AJCC 7 th Edition Staging Disease Site Webinar Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310
7 th Edition Staging. AJCC 7 th Edition Staging. Disease Site Webinar. Colorectum. Overview. This webinar is sponsored by
 AJCC 7 th Edition Staging Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310 from The Centers
AJCC 7 th Edition Staging Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310 from The Centers
Bowel obstruction and tumors
 Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
Unexpected Findings at Endoscopy
 The Endoscopic Incidentaloma: What to Tell Your Patient t with Unexpected Endoscopic Findings: Gastric Intestinal Metaplasia, Silent Ileitis, Carcinoid David Greenwald, MD Montefiore Medical Center Albert
The Endoscopic Incidentaloma: What to Tell Your Patient t with Unexpected Endoscopic Findings: Gastric Intestinal Metaplasia, Silent Ileitis, Carcinoid David Greenwald, MD Montefiore Medical Center Albert
Clinical indications for positron emission tomography
 Clinical indications for positron emission tomography Oncology applications Brain and spinal cord Parotid Suspected tumour recurrence when anatomical imaging is difficult or equivocal and management will
Clinical indications for positron emission tomography Oncology applications Brain and spinal cord Parotid Suspected tumour recurrence when anatomical imaging is difficult or equivocal and management will
Quiz. b. 4 High grade c. 9 Unknown
 Quiz 1. 10/11/12 CT scan abdomen/pelvis: Metastatic liver disease with probable primary colon malignancy. 10/17/12 Colonoscopy with polypectomy: Adenocarcinoma of sigmoid colon measuring at least 6 mm
Quiz 1. 10/11/12 CT scan abdomen/pelvis: Metastatic liver disease with probable primary colon malignancy. 10/17/12 Colonoscopy with polypectomy: Adenocarcinoma of sigmoid colon measuring at least 6 mm
Diagnosing and monitoring NET
 Diagnosing and monitoring NET Inaccurate or delayed diagnosis of neuroendocrine tumors (NET) is common, because many NET are small and asymptomatic. 1 When symptoms are present, they are usually nonspecific
Diagnosing and monitoring NET Inaccurate or delayed diagnosis of neuroendocrine tumors (NET) is common, because many NET are small and asymptomatic. 1 When symptoms are present, they are usually nonspecific
Pitfalls in the CT diagnosis of appendicitis
 The British Journal of Radiology, 77 (2004), 792 799 DOI: 10.1259/bjr/95663370 E 2004 The British Institute of Radiology Pictorial review Pitfalls in the CT diagnosis of appendicitis 1 C D LEVINE, 2 O
The British Journal of Radiology, 77 (2004), 792 799 DOI: 10.1259/bjr/95663370 E 2004 The British Institute of Radiology Pictorial review Pitfalls in the CT diagnosis of appendicitis 1 C D LEVINE, 2 O
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Cervical cancer presentation
 Carcinoma of the cervix: Carcinoma of the cervix is the second commonest cancer among women worldwide, with only breast cancer occurring more commonly. Worldwide, cervical cancer accounts for about 500,000
Carcinoma of the cervix: Carcinoma of the cervix is the second commonest cancer among women worldwide, with only breast cancer occurring more commonly. Worldwide, cervical cancer accounts for about 500,000
Radiology Pathology Conference
 Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases
 Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases Date: April 2015 Date for review: April 2018 1. Principles The recognised specialist HPB MDT for Greater
Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases Date: April 2015 Date for review: April 2018 1. Principles The recognised specialist HPB MDT for Greater
Peritoneal Involvement in Stage II Colon Cancer
 Anatomic Pathology / PERITONEAL INVOLVEMENT IN STAGE II COLON CANCER Peritoneal Involvement in Stage II Colon Cancer A.M. Lennon, MB, MRCPI, H.E. Mulcahy, MD, MRCPI, J.M.P. Hyland, MCh, FRCS, FRCSI, C.
Anatomic Pathology / PERITONEAL INVOLVEMENT IN STAGE II COLON CANCER Peritoneal Involvement in Stage II Colon Cancer A.M. Lennon, MB, MRCPI, H.E. Mulcahy, MD, MRCPI, J.M.P. Hyland, MCh, FRCS, FRCSI, C.
Acute appendicitis, inflammatory appendiceal mass and the risk of a hidden malignant tumor: a systematic review of the literature
 Teixeira et al. World Journal of Emergency Surgery (2017) 12:12 DOI 10.1186/s13017-017-0122-9 REVIEW Open Access Acute appendicitis, inflammatory appendiceal mass and the risk of a hidden malignant tumor:
Teixeira et al. World Journal of Emergency Surgery (2017) 12:12 DOI 10.1186/s13017-017-0122-9 REVIEW Open Access Acute appendicitis, inflammatory appendiceal mass and the risk of a hidden malignant tumor:
Disclosure of Relevant Financial Relationships
 Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS
Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS
Appendix 4: WHO Classification of Tumours of the pancreas 17
 S3.01 The WHO histological tumour type must be recorded. CS3.01a The histological type of the tumour should be recorded based on the current WHO classification 17 (refer to Appendices 4-7). Appendix 4:
S3.01 The WHO histological tumour type must be recorded. CS3.01a The histological type of the tumour should be recorded based on the current WHO classification 17 (refer to Appendices 4-7). Appendix 4:
Intraductal papillary neoplasms in the bile ducts
 Intraductal papillary neoplasms in the bile ducts Seok Hwa Youn Myunghee Yoon Dong Hoon Shin Kosin University Gospel Hospital Department of general surgery Hepato-biliary-pancreatic division Introduction
Intraductal papillary neoplasms in the bile ducts Seok Hwa Youn Myunghee Yoon Dong Hoon Shin Kosin University Gospel Hospital Department of general surgery Hepato-biliary-pancreatic division Introduction
IMAGING GUIDELINES - COLORECTAL CANCER
 IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
Management of Pseudomyxoma Peritonei (PMP) and Colon Cancer Carcinomatosis by Cytoreduction and Hyperthermic Intraperitoneal Chemotherapy (HIPEC).
 and Colon Cancer Carcinomatosis by Cytoreduction and Hyperthermic Intraperitoneal Chemotherapy (HIPEC).") Surgical Oncology Department Management of Pseudomyxoma Peritonei (PMP) and Colon Cancer Carcinomatosis by Cytoreduction and Hyperthermic Intraperitoneal Chemotherapy (HIPEC). 21/04/2010 THERMOMETRY 1000-1500
Surgical Oncology Department Management of Pseudomyxoma Peritonei (PMP) and Colon Cancer Carcinomatosis by Cytoreduction and Hyperthermic Intraperitoneal Chemotherapy (HIPEC). 21/04/2010 THERMOMETRY 1000-1500
EDUCATIONAL CASES E1 & E2. Natasha Inglis 20/03/15
 EDUCATIONAL CASES E1 & E2 Natasha Inglis 20/03/15 CASE E1 79 year old female Rectum. Altemeier operation Histology Superficial erosions and mucosal congestion volcano lesion and pseudomembrane formation
EDUCATIONAL CASES E1 & E2 Natasha Inglis 20/03/15 CASE E1 79 year old female Rectum. Altemeier operation Histology Superficial erosions and mucosal congestion volcano lesion and pseudomembrane formation
Gastroenterology Tutorial
 Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
MANAGEMENT OF INCIDENTALLY DETECTED GALLBLADDER CANCER
 MANAGEMENT OF INCIDENTALLY DETECTED GALLBLADDER CANCER Orlando Jorge M. Torres Full Professor and Chairman Department of Gastrointestinal Surgery Hepatopancreatobiliary Unit Federal University of Maranhão
MANAGEMENT OF INCIDENTALLY DETECTED GALLBLADDER CANCER Orlando Jorge M. Torres Full Professor and Chairman Department of Gastrointestinal Surgery Hepatopancreatobiliary Unit Federal University of Maranhão
Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors
 Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors Jaume Capdevila, MD, PhD Vall d'hebron University Hospital Vall d'hebron Institute of Oncology (VHIO)
Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors Jaume Capdevila, MD, PhD Vall d'hebron University Hospital Vall d'hebron Institute of Oncology (VHIO)
Carcinoma mammario: le istologie non frequenti. Valentina Guarneri Università di Padova IOV-IRCCS
 Carcinoma mammario: le istologie non frequenti Valentina Guarneri Università di Padova IOV-IRCCS Histological diversity of breast adenocarcinomas Different histological types are defined according to specific
Carcinoma mammario: le istologie non frequenti Valentina Guarneri Università di Padova IOV-IRCCS Histological diversity of breast adenocarcinomas Different histological types are defined according to specific
ISSN X (Print) Research Article. *Corresponding author Dr. Mohsin-ul-Rasool.
 Research Article. *Corresponding author Dr. Mohsin-ul-Rasool.") Scholars Journal of Applied Medical Sciences (SJAMS) Sch. J. App. Med. Sci., 2014; 2(1B):176-180 Scholars Academic and Scientific Publisher (An International Publisher for Academic and Scientific Resources)
Scholars Journal of Applied Medical Sciences (SJAMS) Sch. J. App. Med. Sci., 2014; 2(1B):176-180 Scholars Academic and Scientific Publisher (An International Publisher for Academic and Scientific Resources)
Planned relaparotomy following curative resection of a locally advanced gastrointestinal cancer
 Planned relaparotomy following curative resection of a locally advanced gastrointestinal cancer PD Dr. med. Michel Adamina, MSc Department of Surgery Agenda Prerequisite for successful CRS HIPEC Planned
Planned relaparotomy following curative resection of a locally advanced gastrointestinal cancer PD Dr. med. Michel Adamina, MSc Department of Surgery Agenda Prerequisite for successful CRS HIPEC Planned
A Survay on Appendiceal Involvement in Ovarian Mucinous Tumors
 http://www.ijwhr.net Open Access doi 10.15296/ijwhr.2018.33 Original Article International Journal of Women s Health and Reproduction Sciences Vol. 6, No. 2, April 2018, 199 203 ISSN 2330-4456 A Survay
http://www.ijwhr.net Open Access doi 10.15296/ijwhr.2018.33 Original Article International Journal of Women s Health and Reproduction Sciences Vol. 6, No. 2, April 2018, 199 203 ISSN 2330-4456 A Survay
Definition of Synoptic Reporting
 Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Alison Douglass Gillian Lieberman, MD. November. Colon Cancer. Alison Douglass, Harvard Medical School Year III Gillian Lieberman, MD
 November Colon Cancer Alison Douglass, Harvard Medical School Year III Our Patient Mr. K. is a 67 year old man with no prior medical problems other than hemorrhoids which have caused occasional rectal
November Colon Cancer Alison Douglass, Harvard Medical School Year III Our Patient Mr. K. is a 67 year old man with no prior medical problems other than hemorrhoids which have caused occasional rectal