ENDOCRINOLOGICAL IMPLICATIONS AND COMPLICATIONS OF TESTOSTERONE REPLACEMENT IN AGEING MEN
|
|
|
- Alberta Davidson
- 5 years ago
- Views:
Transcription
1 ENDOCRINOLOGICAL IMPLICATIONS AND COMPLICATIONS OF TESTOSTERONE REPLACEMENT IN AGEING MEN Frederick C.W. Wu Professor of Medicine and Endocrinology Andrology Research Unit, Centre for Endocrinology and Diabetes Institute of Human Development Manchester Academic Health Sciences Centre, Central Manchester University Hospitals NHS Foundation Trust, University of Manchester, U.K. Postgraduate International School of Men s Health (PRISM), Besins Healthcare Bruges,Belgium 26 th September 2014
2 Testosterone Replacement in Older Men Benefits Risks Monitoring
3 Potential Benefits of Testosterone in Older Men Sexual health Physical health Bone health Metabolic health
4 Baseline T <7 nmol/l Standardized mean difference (95% CI) T 7-12 nmol/l Meta-analysis of 17 intervention randomized, placebo-trials on T and sexual dysfunction in men (mean age 50 yr) T >12 nmol/l T improves sexual function only in hypogonadal men with pre-treatment T <12 nmol/l Isidori et al. Clin Endocrinol 2005
5 Effects of Testosterone Supplement on Lean Mass, Muscle Strength & Physical Function in Older Men in 17 RCTs Study n Mo Rx Type & Dose Lean mass Grip strength Leg strength Tenover TE 100mg/wk - - Sih TC 200mg/14-17d Physical function Snyder TTS 6mg/d Kenny TTS 5mg/d - - Ly DHT 70mg/d - Liu hcg 250mcg/wk - Ferrando TE 200mg/2 wk - Blackman TE 100mg/2 wk VO 2 Wittert TU 160mg/d Page TE 200mg/2 wk + F Nair TTS 5mg/d - - Emmelot-Vonk Oral TU 160mg/d Sattler / 21 4 TTS 5 / 10mg/d? (10 mg) VO 2 Kenny TTS 5mg/d Srinivas-Shankar TTS 5mg/d Travison * 6 TTS 10mg/d* (10 mg) (10 mg) Sheffield-Moore /8* 5 TE 100mg/wk -
6 Free T (pmol/l) FSH (IU/L) Total T (nmol/l) LH (IU/L) Hormone Levels During Treatment ---- Testosterone ---- Testogel ---- Placebo ---- Placebo Mean (SD) Total Testosterone LH Free Testosterone FSH Srinivas- Shankar et al JCEM 95:
7 Lower Limb Muscle Strength **P=0.02 Srinivas- Shankar et al JCEM 95: IME-PT Isometric extension peak torque IMF-PT Isometric flexion peak torque IKE-PT Isokinetic extension peak torque IKF-PT isokinetic flexion peak torque
8 Improvement in Physical Function at 6 Month in Older and Frailer Men * ** * * *p<0.05 **p<0.01 Srinivas- Shankar et al JCEM 95: yr n = Frailty Criteria n = yr n = Frailty Criteria n = 100
9 Effects of Testosterone on Muscle Strength and Physical Function in Older Men in the TOM Trial Travison et al 2011
10 Testosterone Effects on Bone Mineral Density (BMD) in Men: Meta-analyses of RCTs Standardised Mean Difference in Lumbar Spine BMD Standardised Mean Difference in Femoral Neck BMD Tracz et al 2006
11 Change in Fat Mass (kg) Testosterone Treatment of Elderly Men Placebo -3.0 Testosterone Time (months) 36 Snyder PJ, et al. J Clin Endocrinol Metab. 1999;84:
12 RCT of Metabolic Effects of Testosterone (T) in Obese Men with T2D or MetS Study n Age (yr) T Rx Duration (Weeks) Waist (cm) HbA1C (%) HOMA-IR Others Kapoor TE 200mg/2w * -0.37* -1.7* (-39%) total Chol (-0.4 mmol/l), no change in other lipids Heufelder TTS T 50mg/d (-59%) CRP Kalichenko TU 1000mg/12w Not reported -1.7 (-31%) body weight 3.9 Kg, No change fasting sugar Aversa TU 1000mg/12w (-60%) No change lipids Hct (+3.8%) Jones TTS T 60mg/d 26 N.S (-15%) No change % body fat Solvay (Unpub) 180 NR TTS T 50mg/d 26 NR N.S. N.S. 2.0 Kg lean mass

13 Benefits of Testosterone Therapy Spitzer et al 2013
 Muscle strength UL Muscle strength LL These relatively modest/equivocal, (3%), (only high T dose) Physical function effects of T Rx in?")
14 Features of Hypogonadism Benefits of Androgens Young hypogonadal Ageing male Sexual function, (if low baseline T) Lean body mass (~ 1.5kg) Muscle strength UL Muscle strength LL These relatively modest/equivocal, (3%), (only high T dose) Physical function effects of T Rx in? ageing men may not Fat mass reliably translate to (~ 2kg) clinically or patient Lumbar spine BMD important outcomes Hip BMD Fracture, (if low baseline T),? Mood? Cognition? Quality of life?
15 Adverse Effects of Testosterone Therapy Formulation specific Injections i. m. Pain at injection site Fluctuations in mood, energy and sexual desire Coughing immediately after injection (POME) Transdermal gels Potential risk of gel transfer to others in close contact Skin irritation Fluctuations in absorption Transdermal patches Frequent skin reactions at the application site Buccal adhesive Gum irritation Dislodgement Alteration of taste Subcutaneous pellets Infection Bleeding/bruising Scarring Spontaneous extrusion Oral 17- -alkylated Hepatotoxicity Cholestasis Peliosis hepatis Hepatic tumour Marked in HDL-chol
16 Adverse Effects of Testosterone Replacement Therapy Acne truncal Seborrhoea Gynaecomastia Priapism Higher libido Behavioural change Fluid retention sperm production and infertility Erythrocytosis Aggravates prostate diseases? Urinary obstruction Tumour growth Detection of subclinical prostate cancer Sleep apnoea? Aggravates cardiovascular diseases?
17 Testosterone Replacement and Erythrocytosis
18 Effects of Testosterone on Erythropoiesis are Greater in Older Men than Young Men (Coviello et al JCEM 2008)

19 Testosterone Induces Erythrocytosis via Increased Erythropoietin and Suppressed Hepcidin: Evidence for a New Erythropoietin/Hemoglobin Set Point Bachman et al 2013
20 Testosterone Stimulates Erythropoietin and Suppresses Hepcidin Testosterone administration is associated with increased iron incorporation into red blood cells Testosterone upregulates renal erythropoietin mrna expression, and increased erythropoietin levels. Testosterone downregulates hepatic hepcidin mrna expression and suppresses hepcidin level. Testosterone stimulates erythropoiesis by stimulating EPO and recalibrating the set point of EPO in relation to hemoglobin and by increasing iron utilization for erythropoiesis.
21 Relative Risks (RR) of Erythrocytosis in Testosterone Therapy in Older Men Overall RR 3.15 ( ) RR Commonest adverse effect of testosterone treatment in older men (Fernandez-Balsells et al JCEM 2010)
22 Hemoglobin (g/dl) Hematocrit (%) Erythropoiesis during Testosterone Replacement S Weeks T-Enanthate S Weeks T-Undecanoate (Jockenhövel F, unpublished)
23 Testosterone Replacement and Prostate diseases
24 Prevalence of Histological Prostate Cancer in Autopsy Cases with Increasing Age Stamey et al 1993
, interacting with multiple signaling molecules, such as growth/transcription factors, oncogenes, and tumuor suppressors Despite the dependence on androgens for normal")
25 Targeted drugs Molecules Implicated in Prostate Cancer progression through the Initiation and Progression Androgens are potent mediators of prostate cancer growth and normal or aberrant activation of the androgen receptor (AR), interacting with multiple signaling molecules, such as growth/transcription factors, oncogenes, and tumuor suppressors Despite the dependence on androgens for normal prostate development, there is limited evidence to suggest that androgens autonomously promote prostate cancer initiation, which is associated with many dysregulated developmental, tumour suppressor & oncogene signalling pathways Schrecengost & Knudsen 2013
26 Endogenous Sex Hormones Were Not Associated with Increased Risk or Grades of Prostate Cancer in 3886 Cases and 6438 Controls A Collaborative Analysis of 18 Prospective Studies (Roddam et al 2008)
27 Serum Testosterone and Dihydrotestosterone and Prostate Cancer Detection/Grade in the Placebo Arm of the Reduction by Dutasteride of Prostate Cancer Events (REDUCE) Trial Baseline serum testosterone and DHT levels were unrelated to prostate cancer detection or grade Locally weighted scatterplot smoothing of baseline serum testosterone and dihydrotestosterone (DHT) and final cancer status after considering all biopsies during 4 yr of the REDUCE trial. Men detected with prostate cancer were coded as 1, whereas men with no prostate cancer detected were coded as 0. Muller et al 2012
28 Risks (Odds Ratio 95%CI) of (a) prostate cancer (b) prostate biopsy in 9 short-term (<12 months) testosterone treatment (by modalities) RCT studies from 1966 to 2013 in hypogondal men, median age yr (Total n = 2351 In 22 studies) Cui et al 2014
29 Risks (Odds Ratio 95%CI) of (a) prostate cancer (b) prostate biopsy in 8 longer-term (12 36 months) testosterone treatment (by modalities) RCT studies from 1966 to 2013 in hypogondal men, median age yr (Total n = 2351 in 22 studies) Cui et al 2014
30 Standardised Mean difference 95%CI) in PSA change in 7 short-term ( 6 months) testosterone treatment RCT studies in 2351 hypogondal men, median age yr Cui et al 2014
31 Testosterone Treatment - Risks of Prostate Cancer Not Defined Occult histological prostate cancer increases with age - very common in elderly men Androgens promote pre-existing prostate cancer growth but long latency Relationship between endogenous & exogenous androgens and prostate cancer incidence not established Normal PSA <4ng/mL does not exclude occult cancer & increase in PSA is not specific for cancer (e.g. age, BPH, testosterone treatment) Large scale prospective trials of testosterone treatment required to assess prostate cancer risks Particular caution is required in use of testosterone in elderly men
32 Testosterone Replacement and Sleep Disorders

33


34 Testosterone Replacement Therapy and Obstructive Sleep Apnoea Is There a Real Concern? Hanafy 2007
35 Mean ±SEM of the change from baseline for:- (a) oxygen desaturation index (ODI), (b)% time of total sleep time (TST) that the arterial oxygen saturation was <90% (SpO2T90%), (c) apnoea hypopnoea index (AHI) (d) AHI during non rapid eye movement sleep (NREM AHI) mg Testosterone Undecanoate or placebo at 0, 6 and 12 weeks
36 Testosterone and Sleep Disorders OSA per se is not a cause of low testosterone, rather it is due to obesity, and testosterone is increased by weight loss. Treatment of moderate to severe OSA with continuous positive airway pressure (CPAP) does not reliably increase testosterone levels in most studies Apart from a very transient deleterious effect physiological testosterone treatment does not adversely affect OSA in obese men with low T Suprapysiological doses of exogenous testosterone and anabolic/androgenic steroid abuse are associated with abnormalities of sleep duration and architecture
37 Testosterone Treatment and Cardiovascular Diseases
, of Cardiovascular-related Events Xu et al 2013")
38 Pooled Effects of 27 Placebo-controlled Randomized Trials Testosterone Therapy Associated with Increased Risks, OR 1.54 ( ), of Cardiovascular-related Events Xu et al 2013
 Mobility Limitation: Difficulty walking 2 blocks or climbing 10 steps.")
39 Two Testosterone RCTs of Frailty Comparison - Design Inclusion Criteria Number of participants Srinivas-Shankar (2010) Frailty: 1 frailty criteria (Fried 2001) Active: n = 132 Placebo: n = 130 Total T <346 ng/dl or free T <7.2 ng/dl Basaria et al (2010) Mobility Limitation: Difficulty walking 2 blocks or climbing 10 steps. SPPB Score 4-9 Active: n = 106 Placebo: n = 103 Total T ng/dl or free T <5 ng/dl Interventions Transdermal T 5mg/day Transdermal T 10mg/day Duration 6 months 6 months
40 Serious Adverse Events Serious Adverse Event Placebo Testosterone Constrictive pericarditis (died) 0 1 Ruptured abdominal aneurysm (died) 1 0 Acute myocardial infarction 1 0 Ca oesophagus 0 1 Ca lung 0 1 Pulmonary embolism 0 1 Heart failure Abdominal aortic aneurysm Data are n Srinivas-Shankar et al JCEM 95:
 Effects of transdermal T at 10mg/day for 6 months on lower extremity strength and physical function compared with a")

41 TOM TRIAL- ADVERSE CARDIOVASCULAR EVENTS ASSOCIATED WITH TESTOSTERONE ADMINISTRATION Study Population 209 men 65 yr of age or older with limitations in mobility and Low T (Total Serum T: 100 to 350 ng/dl; Free Serum T level <50 pg/ml) Effects of transdermal T at 10mg/day for 6 months on lower extremity strength and physical function compared with a placebo Results 23 men in the T treatment group (n=106) and 5 in the placebo group (n=103) had CV-related events. The divergence was maintained over the 6-month intervention period and did not diminish during the 3-month observation phase that followed the intervention period. This increased risk warranted early termination of the trial. Basaria S et al. NEJM 2010
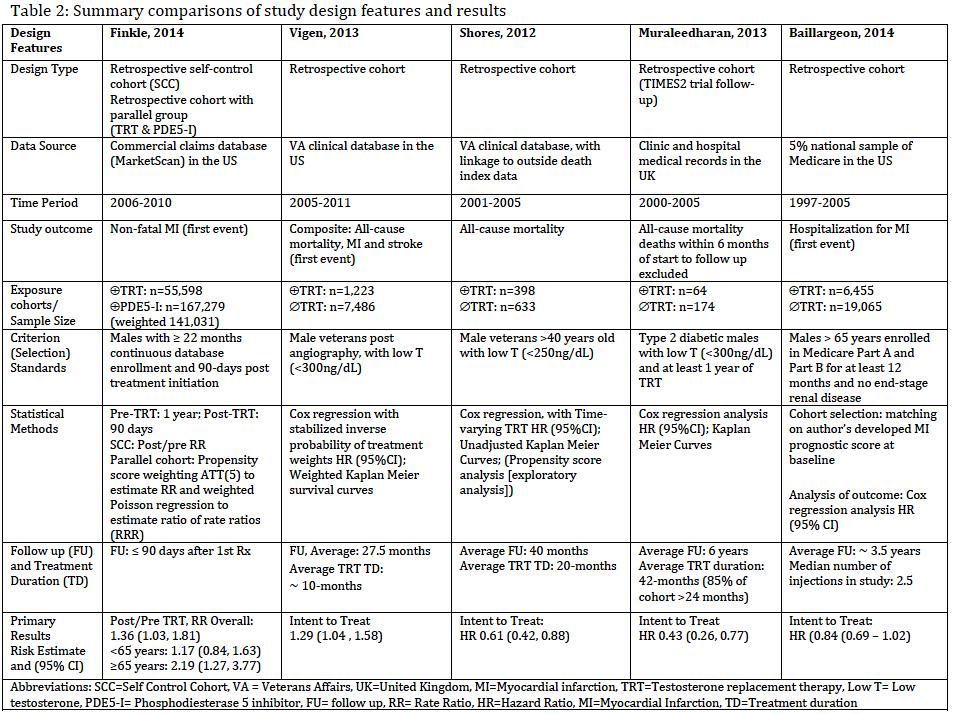
42 In 1031 Male Veterans Aged >40 yr, with Low Total T 250 ng/dl (8.7 nmol/liter), T-treated Men had a Decreased Risk of Dying Than Untreated Men over 40.5 month follow-up (P<0.029). (Shores et al 2012)
 60 yr old who underwent coronary angiography between 2005 and 2011 and who had a total testosterone level less than 300 ng/dl.")
43 Association of Testosterone Therapy with Mortality, Myocardial Infarction, and Stroke in Men with Low Testosterone Vigen R et al JAMA A retrospective nation wide cohort study Male veterans (n = 8709) 60 yr old who underwent coronary angiography between 2005 and 2011 and who had a total testosterone level less than 300 ng/dl. Primary outcome was a composite of all-cause mortality, MI, and ischemic stroke. Use of testosterone therapy was associated with increased risk of adverse outcomes (hazard ratio, 1.29; 95%CI, 1.04 to 1.58) during 27.5 months follow-up. Conclusions Use of testosterone therapy in this cohort of veterans with significant medical comorbidities was associated with increased risk of mortality, MI, or ischemic stroke. These findings were not modified by the presence of CAD.
 7.27) after 90 days Heart Disease History No Heart Disease History Testosterone PDE5I Testosterone PDE5I Age <65 yr N= 4,006 N= 10,681 N= 44,533 N= 130,831 Rate Ratio (CI) 2.9 (1.49, 5.")
44 In all subjects >65 (n yr = (n 55,593), = 7054), the the post/pre prescription myocardial infarction rate (per 100 persons.yr) ratio (RR) for testosterone prescription was (95% CI 1.03, 1.27, 1.81) 7.27) after 90 days Heart Disease History No Heart Disease History Testosterone PDE5I Testosterone PDE5I Age <65 yr N= 4,006 N= 10,681 N= 44,533 N= 130,831 Rate Ratio (CI) 2.9 (1.49, 5.62) 1.4 (0.91, 2.14) 0.90 (0.61, 1.34) 0.99 (0.84, 1.17) Ratio of RR (CI) 2.07 (1.05, 4.11) 0.91 (0.60, 1.37) Age 65 yr N= 2,047 N= 5,492 N= 5,057 N= 20,275 Rate Ratio (CI) 2.16 (0.92, 5.10) 1.13 (0.68, 1.88) 2.21 (1.09, 4,46) 0.92 (0.60, 1.39) Ratio of RR (CI) 1.90 (0.66, 5.50) 2.41 (1.12, 5.17)
45 Cardiovascular risk associated with testosterone-boosting medications: a systematic review and meta-analysis Source MH-OR LL UL p 0,00 0,01 Odds ratio for MACE 0,10 1,00 10,00 100, ,00 TS #Events # Patients Placebo #Events # Patients Copenaghen SG 1986 (27) 1,97 0,08 48,82 0,68 Hall et al., 1996 (30) 0,32 0,01 8,23 0,49 Sih et al., 1997 (32) 0,88 0,05 15,33 0,93 Snyder et al., 1999 (36) 2,04 0,18 23,17 0,57 English et al., 2000 (38) 3,12 0,12 80,39 0,49 Seidman et al., 2001 (43) 0,41 0,02 10,83 0,59 Steidle et al., 2003 (48) 2,83 0,11 70,27 0,53 Armory et al., 2004 (50) 3,13 0,12 80,68 0,49 Kenny et al., 2004 (52) 0,23 0,01 7,05 0,40 Svartberg et al., 2004 (56) 0,29 0,01 7,74 0,46 Brockenbrough et al., 2006 (59) 3,75 0,36 39,59 0,27 Malkin et al., 2006 (65) 2,17 0,19 25,01 0,53 Nair et al., 2006 (68) 5,70 0,26 123,78 0,27 Svartberg et al., 2008 (77) 3,16 0,12 82,64 0,49 Chapman et al., 2009 (80) 1,00 0,05 20,83 1,00 Legros et al., 2009 (81) 1,01 0,04 25,01 1,00 Aversa et al., 2010 (85) 0,08 0,00 2,07 0,13 Aversa et al., 2010 (86) 0,07 0,00 1,97 0,12 Basaria et al., 2010 (10) 13,39 0,74 240,78 0,08 Kalinchenko et al., 2010 (88) 0,21 0,01 5,15 0,34 Srinivas-Shankar et al., 2010 (89) 1,01 0,14 7,31 0,99 Ho et al., 2011 (91) 1,00 0,06 16,37 1,00 Jones et al., 2011 (92) 0,51 0,05 5,75 0,59 Kaufman et al., 2011 (93) 0,87 0,04 18,48 0,93 Behere et al., 2012 (95) 2,95 0,12 72,91 0,51 Hildreth et al., 2013 (97) 0,15 0,02 1,53 0,11 Overall 1,01 0,57 1,77 0, Placebo TS Corona et al., 2014
![FDA adding general warning to testosterone products about potential for venous blood clots [06/19/2014] The U.S.](/docs-images/87/95414823/images/46-0.jpg "Food and Drug Administration (FDA) is requiring manufacturers to include a general warning in the drug labeling of all approved testosterone products about the risk of")


46 FDA adding general warning to testosterone products about potential for venous blood clots [06/19/2014] The U.S. Food and Drug Administration (FDA) is requiring manufacturers to include a general warning in the drug labeling of all approved testosterone products about the risk of blood clots in the veins. Blood clots in the veins, also known as venous thromboembolism (VTE), include deep vein thrombosis (DVT) and pulmonary embolism (PE). The risk of venous blood clots is already included in the labeling of testosterone products as a possible consequence of polycythemia, an abnormal increase in the number of red blood cells that sometimes occurs with testosterone treatment. Because there have been postmarket reports of venous blood clots unrelated to polycythemia, FDA is requiring a change to drug labeling of all testosterone products to provide a more general warning regarding venous blood clots and to ensure this risk is described consistently in the labeling of all approved testosterone products.
47
48 In conclusion, these studies do not provide conclusive evidence of increased cardiovascular risk associated with the use of testosterone therapy or causality.
49 FDA Advisory Panel Urges Restrictions on Testosterone Use September 18, 2014 Change in labeling for testosterone-replacement products recommended A combined US Food and Drug Administration (FDA) advisory panel has voted nearly unanimously to change the labeling for testosterone-replacement products, with the aim of clamping down on their current widespread use for "age-related" hypogonadism. "Benefit is unclear in men diagnosed with hypogonadism due to no apparent cause other than older age. Yet testosterone is being predominantly prescribed to men 40 to 64 years of age. This has prompted the FDA to question whether labeling accurately reflects the appropriate indicated population," Hylton V. Joffe, MD, director of the Division of Bone, Reproductive, and Urologic Products at the FDA, told the panel in his introductory remarks. Given the magnitude of off-label use "and lack of strong data on effectiveness in this population, I think it's important to include something about cardiovascular safety in the label. Maybe not to the level of black box, but certainly that there are serious concerns that have not yet been adequately addressed," he added. Trials Required for Cardiovascular Safety The panel also indicated that large studies are needed to demonstrate both clinical benefit and safety of the products. Several panelists said that a large, randomized clinical trial would be needed to determine whether or not the cardiovascular signal was real, noting that men with low testosterone are already at increased cardiovascular risk. Others felt that an observational trial
50 Recommendations for Monitoring Testosterone Replacement in Older Men
51 Absolute Contraindications for Testosterone Treatment Untreated prostate cancer High-grade PIN History of breast cancer Myocardial infarct, acute coronary event, unstable angina or coronary re-vascularisation in past 6 months
52 Relative Contraindications for Testosterone Treatment Prostate specific antigen (PSA) >4 ng/ml* Unevaluated prostate nodule/induration Successfully treated localised low-grade prostate cancer Severe urinary obstructive symptoms (IPSS symptom score >19) Polycythaemia Hct >50% Severe uncontrolled heart, renal or liver failure fluid retention Untreated severe sleep apnoea *PSA >3ng/mL in men with high risk of prostate cancer e.g. Afro-Caribbean or first degree relative
53 Special Precautions in Starting Testosterone Replacement Therapy in Older Men (>40 Yr) - Do Not Start Without Urological Evaluation Prostate abnormal on DRE PSA concentration >4 ng/ml PSA concentration >3 ng/ml First degree relatives with prostate cancer Afro-american or Afro-caribbean Severe urinary obstructive symptoms (IPSS symptom score >19) due to BPH Haematocrit >50% Bhasin et al; JCEM 95:
54 Monitoring of Continuing Testosterone Replacement Therapy in Older Men (>40 Yr) DRE prostate and PSA at 3-6 and 12 month after starting treatment, and thereafter annually Urological consultation if Abnormal DRE at any time PSA >4.0 ng/ml at any time Increase in PSA >1.4 ng/ml in first 3 or 6 month, or any subsequent 1 year interval Check haematocrit at 3, 6 and 12 month after starting treatment, and thereafter annually Haematocrit >54%, stop or reduce dose of T therapy Evaluate for hypoxia and sleep apnea Consider venesection Bhasin et al; JCEM 95:
55 Testosterone level during TRT Aim to maintain mid-normal testosterone levels nmol/l (no circadian rhythm) Testosterone gel Assess any time after application Transdermal testosterone delivery systems (patches) Assess T levels 3 to 10 hours after application of the patch. Injectable testosterone Monitor nadir testosterone levels, prior to the next injection. If T >15nmol/L or <8 nmol/l, adjust frequency or dose or both Testosterone implants Monitor nadir testosterone levels before next implant. If T >15nmol/L or <8 nmol/l, adjust frequency or dose or both
56 Monitoring of Testosterone Replacement - Efficacy Matsumoto 2013
57 Conclusions Best practice guidelines based on opinions rather than strong evidence still evolving Erythrocytosis is common, dose-dependent and avoidable Sleep apnoea risk may be over-estimated Long term risks (CVD & prostate) of T treatment in older men are unknown shapes careful monitoring of AEs Careful assessment/explanation of overall benefits/risks with individual patients Re-assess diagnosis and review clinical response regularly to determine need for continuing treatment
58 THANK YOU
59 Research Agenda Population-based reference ranges for testosterone are needed to rationally partition men into those with normal Harmonize testosterone and low levels. assays across Population laboratories cohort to ensure studies are indicated to determine the physicians can interpret natural history (e.g. wellbeing, frailty, mortality) of men with and compare hormone different levels of testosterone levels obtained from different laboratories. Long-term, adequately-powered, randomized studies should placebocontrolled trials are needed to determine the the efficacy health and benefits and risks the long-term risks of testosterone therapy associated in with symptomatic older men with low testosterone levels. various thresholds of testosterone levels. New therapeutic strategies, e.g. development of selective androgen receptor modulators (SARMs), are needed to dissociate beneficial anabolic effects of testosterone from potential adverse effects on the prostate and cardiovascular events
Take-Home Messages: Androgens
 Take-Home Messages: Androgens Anthony J. Bella MD, FRCSC Greta and John Hansen Chair in Men s Health Research Division of Urology, Department of Surgery University of Ottawa SUMMARY SLAMS Symposium Clinical
Take-Home Messages: Androgens Anthony J. Bella MD, FRCSC Greta and John Hansen Chair in Men s Health Research Division of Urology, Department of Surgery University of Ottawa SUMMARY SLAMS Symposium Clinical
Testosterone Therapy in Men An update
 Testosterone Therapy in Men An update SANDEEP DHINDSA Associate Professor of Medicine Director, Division of Endocrinology and Metabolism, Saint Louis University, St. Louis, MO Presenter Disclosure None
Testosterone Therapy in Men An update SANDEEP DHINDSA Associate Professor of Medicine Director, Division of Endocrinology and Metabolism, Saint Louis University, St. Louis, MO Presenter Disclosure None
Point-Counterpoint: Late Onset Hypogonadism (LOH)
") Point-Counterpoint: Late Onset Hypogonadism (LOH) We are Under-diagnosing and Treating Men with LOH LOH is a Non-existent Disease ~ Robert E. Donohue, MD Late Onset Hypogonadism LOH: underdx. & undertx
Point-Counterpoint: Late Onset Hypogonadism (LOH) We are Under-diagnosing and Treating Men with LOH LOH is a Non-existent Disease ~ Robert E. Donohue, MD Late Onset Hypogonadism LOH: underdx. & undertx
How to treat: TRT modalities and formulations
 How to treat: TRT modalities and formulations Paul PIETTE, PharmD Senior Research Fellow Clinique Antoine Depage - Belgium ppiette@besins-healthcare.com Bruges 2014, May 15 th Testosterone-replacement
How to treat: TRT modalities and formulations Paul PIETTE, PharmD Senior Research Fellow Clinique Antoine Depage - Belgium ppiette@besins-healthcare.com Bruges 2014, May 15 th Testosterone-replacement
Prof Dato Dr TAN Hui Meng University of Malaya, Kuala Lumpur University of Pennsylvania, USA
 Prof Dato Dr TAN Hui Meng University of Malaya, Kuala Lumpur University of Pennsylvania, USA Prevailing context Increase number of men who are potential candidates for Testosterone Replacement Therapy
Prof Dato Dr TAN Hui Meng University of Malaya, Kuala Lumpur University of Pennsylvania, USA Prevailing context Increase number of men who are potential candidates for Testosterone Replacement Therapy
Late onset Hypogonadism. Dr KhooSay Chuan Department of Urology Penang General Hospital
 Late onset Hypogonadism Dr KhooSay Chuan Department of Urology Penang General Hospital Late onset hypogonadism(loh) Definition LOH age associated testoteronedeficiency syndrome (TDS) Male menopause, andropause,
Late onset Hypogonadism Dr KhooSay Chuan Department of Urology Penang General Hospital Late onset hypogonadism(loh) Definition LOH age associated testoteronedeficiency syndrome (TDS) Male menopause, andropause,
Hypogonadism 4/27/2018. Male Hypogonadism -- Definition. Epidemiology. Objectives HYPOGONADISM. Men with Hypogonadism. 95% untreated.
 Male Hypogonadism -- Definition - Low T, Low Testosterone Hypogonadism -...a clinical syndrome that results from failure of the testes to produce physiological concentrations of testosterone due to pathology
Male Hypogonadism -- Definition - Low T, Low Testosterone Hypogonadism -...a clinical syndrome that results from failure of the testes to produce physiological concentrations of testosterone due to pathology
Update on diagnosis and complications of adult and elderly male hypogonadism
 Hypoandrogenism in the elderly: to treat or not to treat? 12 th Italian AME Meeting; 6 th joint Meeting with AAC Bari november 10th Update on diagnosis and complications of adult and elderly male hypogonadism
Hypoandrogenism in the elderly: to treat or not to treat? 12 th Italian AME Meeting; 6 th joint Meeting with AAC Bari november 10th Update on diagnosis and complications of adult and elderly male hypogonadism
Testosterone Therapy and the Prostate. Frans M.J. Debruyne Professor of Urology The Netherlands
 Testosterone Therapy and the Prostate Frans M.J. Debruyne Professor of Urology The Netherlands TRT- Risks Prostate ( Cancer, BPH )? Cardiac? Lipids? Polycythemia Sleep apnea Gynecomastia Edema Testosterone
Testosterone Therapy and the Prostate Frans M.J. Debruyne Professor of Urology The Netherlands TRT- Risks Prostate ( Cancer, BPH )? Cardiac? Lipids? Polycythemia Sleep apnea Gynecomastia Edema Testosterone
Evaluation and Treatment of Primary Androgen Deficiency Syndrome in Male Patients
 Evaluation and Treatment of Primary Androgen Deficiency Syndrome in Male Patients Jeff Unger, MD Director Chino Medical Group Diabetes and Headache Intervention Center Chino, California January 16, 2008
Evaluation and Treatment of Primary Androgen Deficiency Syndrome in Male Patients Jeff Unger, MD Director Chino Medical Group Diabetes and Headache Intervention Center Chino, California January 16, 2008
GUIDELINES ON. Introduction. G.R. Dohle, S. Arver, C. Bettocchi, S. Kliesch, M. Punab, W. de Ronde
 GUIDELINES ON Male Hypogonadism G.R. Dohle, S. Arver,. Bettocchi, S. Kliesch, M. Punab, W. de Ronde Introduction Male hypogonadism is a clinical syndrome caused by androgen deficiency. It may adversely
GUIDELINES ON Male Hypogonadism G.R. Dohle, S. Arver,. Bettocchi, S. Kliesch, M. Punab, W. de Ronde Introduction Male hypogonadism is a clinical syndrome caused by androgen deficiency. It may adversely
A dro r gen e R e R p e lac a e c m e e m n e t t T her e a r p a y Androgen Replacement Therapy in the Aging O j b ecti t ve v s Male
 Androgen Replacement Therapy in the Aging Male Thomas J. Walsh, MD, MS Department of Urology University of California, San Francisco Objectives 1. List 3 effects of androgens on normal male physiology.
Androgen Replacement Therapy in the Aging Male Thomas J. Walsh, MD, MS Department of Urology University of California, San Francisco Objectives 1. List 3 effects of androgens on normal male physiology.
Disclosures. Learning Objectives. Effects of Hormone Therapy on the Metabolic Syndrome and Cardiovascular Disease. None
 Effects of Hormone Therapy on the Metabolic Syndrome and Cardiovascular Disease Micol S. Rothman, MD Associate Professor of Medicine Endocrinology, Diabetes and Metabolism Clinical Director Metabolic Bone
Effects of Hormone Therapy on the Metabolic Syndrome and Cardiovascular Disease Micol S. Rothman, MD Associate Professor of Medicine Endocrinology, Diabetes and Metabolism Clinical Director Metabolic Bone
What Is the Low T Syndrome? Is Testosterone Supplementation Safe?
 What Is the Low T Syndrome? Is Testosterone Supplementation Safe? UCSF Osher Mini Medical School March 7, 2018 Dolores Shoback, MD Staff Physician SF-VAMC Professor of Medicine, UCSF No disclosures or
What Is the Low T Syndrome? Is Testosterone Supplementation Safe? UCSF Osher Mini Medical School March 7, 2018 Dolores Shoback, MD Staff Physician SF-VAMC Professor of Medicine, UCSF No disclosures or
HYPOGONADISM DEFINITION: PRODUCTION OF SEX HORMONES AND GERM CELLS IS INADEQUATE (ENDOCRINE SOCIETY)
") HYPOGONADISM DEFINITION: PRODUCTION OF SEX HORMONES AND GERM CELLS IS INADEQUATE (ENDOCRINE SOCIETY) DEFECT OF THE REPRODUCTIVE SYSTEM THAT RESULTS IN LACK OF FUNCTION OF THE GONADS (Wikipedia) REDUCTION
HYPOGONADISM DEFINITION: PRODUCTION OF SEX HORMONES AND GERM CELLS IS INADEQUATE (ENDOCRINE SOCIETY) DEFECT OF THE REPRODUCTIVE SYSTEM THAT RESULTS IN LACK OF FUNCTION OF THE GONADS (Wikipedia) REDUCTION
Testosterone Therapy in Men with Hypogonadism
 Testosterone Therapy in Men with Hypogonadism (Endocrine Society 2018 Guideline) Ngwe Yin, MD Assistant Clinical Professor of Medicine, UCSF Fresno Medical Education Program Disclosures None Objective
Testosterone Therapy in Men with Hypogonadism (Endocrine Society 2018 Guideline) Ngwe Yin, MD Assistant Clinical Professor of Medicine, UCSF Fresno Medical Education Program Disclosures None Objective
Consent for Testosterone Therapy-Men Revised 4/10/18
 Consent for Testosterone Therapy in Men You have been diagnosed with or have an increased risk of having a hormone deficiency and your provider has recommended treatment with bio-identical hormone replacement
Consent for Testosterone Therapy in Men You have been diagnosed with or have an increased risk of having a hormone deficiency and your provider has recommended treatment with bio-identical hormone replacement
An Idea Whose Time Has Come-Male Health Programs: An Opportunity For Clinical Expansion and Better Health
 An Idea Whose Time Has Come-Male Health Programs: An Opportunity For Clinical Expansion and Better Health KEVIN R. LOUGHLIN MD,MBA Harvard Medical School Boston, MA THE WEAKER SEX-MALES LIFE EXPECTANCY
An Idea Whose Time Has Come-Male Health Programs: An Opportunity For Clinical Expansion and Better Health KEVIN R. LOUGHLIN MD,MBA Harvard Medical School Boston, MA THE WEAKER SEX-MALES LIFE EXPECTANCY
Corporate Medical Policy Testosterone Pellet Implantation for Androgen Deficiency
 Corporate Medical Policy Testosterone Pellet Implantation for Androgen Deficiency File Name: Origination: Last CAP Review: Next CAP Review: Last Review: testosterone_pellet_implantation_for_androgen_deficiency
Corporate Medical Policy Testosterone Pellet Implantation for Androgen Deficiency File Name: Origination: Last CAP Review: Next CAP Review: Last Review: testosterone_pellet_implantation_for_androgen_deficiency
Disclosures. Faculty 3/5/18. Testosterone, the FDA and CVD Risk Controversies. Matt Rosenberg, MD Director of Mid-Michigan Health Centers Jackson, MI
 Testosterone, the FDA and CVD Risk Controversies Faculty Matt Rosenberg, MD Director of Mid-Michigan Health Centers Jackson, MI 2 Disclosures Matt Rosenberg, MD serves on the advisory board for Bayer,
Testosterone, the FDA and CVD Risk Controversies Faculty Matt Rosenberg, MD Director of Mid-Michigan Health Centers Jackson, MI 2 Disclosures Matt Rosenberg, MD serves on the advisory board for Bayer,
Disclosures. Advisory Boards 6/10/2014
 Massachusetts Medical Society 12 th annual Men s Health Symposium 11 June 2014 Testosterone and Cardiovascular Disease Where Does The Real Answer Lie? Andre Guay MD, FACP, FACE, IF (Ret) Director, Center
Massachusetts Medical Society 12 th annual Men s Health Symposium 11 June 2014 Testosterone and Cardiovascular Disease Where Does The Real Answer Lie? Andre Guay MD, FACP, FACE, IF (Ret) Director, Center
MALE HYPOGONADISM: CHOOSING THE APPROPRIATE THERAPY. Michael S. Irwig, M.D. Director, Center for Andrology Division of Endocrinology & Metabolism
 MALE HYPOGONADISM: CHOOSING THE APPROPRIATE THERAPY Michael S. Irwig, M.D. Director, Center for Andrology Division of Endocrinology & Metabolism Disclosures Aromatase inhibitors & clomiphene citrate are
MALE HYPOGONADISM: CHOOSING THE APPROPRIATE THERAPY Michael S. Irwig, M.D. Director, Center for Andrology Division of Endocrinology & Metabolism Disclosures Aromatase inhibitors & clomiphene citrate are
Endocrine Update Mary T. Korytkowski MD Division of Endocrinology University of Pittsburgh
 Endocrine Update 2016 Mary T. Korytkowski MD Division of Endocrinology University of Pittsburgh Disclosure of Financial Relationships Mary Korytkowski MD Honoraria British Medical Journal Diabetes Research
Endocrine Update 2016 Mary T. Korytkowski MD Division of Endocrinology University of Pittsburgh Disclosure of Financial Relationships Mary Korytkowski MD Honoraria British Medical Journal Diabetes Research
Recommendations on the diagnosis, treatment and monitoring of Testosterone deficiency (TD) in adult men
 in adult men") Recommendations on the diagnosis, treatment and monitoring of Testosterone deficiency (TD) in adult men Bruno Lunenfeld, George Mskhalaya, Svetlana Kalinchenko, Yulia Tishova, Michael Zitzmann, Stefan
Recommendations on the diagnosis, treatment and monitoring of Testosterone deficiency (TD) in adult men Bruno Lunenfeld, George Mskhalaya, Svetlana Kalinchenko, Yulia Tishova, Michael Zitzmann, Stefan
EAU GUIDELINES ON MALE HYPOGONADISM
 EAU GUIDELINES ON MALE HYPOGONADISM (Text update March 2015) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch, M. Punab Introduction Male hypogonadism is a clinical syndrome caused by
EAU GUIDELINES ON MALE HYPOGONADISM (Text update March 2015) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch, M. Punab Introduction Male hypogonadism is a clinical syndrome caused by
Testim 1 Gel: Review of Clinical Data
 European Urology Supplements European Urology Supplements 4 (2005) 24 30 Testim 1 Gel: Review of Clinical Data Tom A. McNicholas* Department of Urology, Lister Hospital, Corey s Mill Lane, Stevenage, Hertfordshire
European Urology Supplements European Urology Supplements 4 (2005) 24 30 Testim 1 Gel: Review of Clinical Data Tom A. McNicholas* Department of Urology, Lister Hospital, Corey s Mill Lane, Stevenage, Hertfordshire
GUIDELINES ON MALE HYPOGONADISM
 GUIDELINES ON MALE HYPOGONADISM (Text update March 2015) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch, M. Punab Introduction Male hypogonadism is a clinical syndrome caused by androgen
GUIDELINES ON MALE HYPOGONADISM (Text update March 2015) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch, M. Punab Introduction Male hypogonadism is a clinical syndrome caused by androgen
The reality of LOH-symptoms
 The reality of LOH-symptoms PRISM IV Bruges, Belgium September 25-26, 2014 Dr. Herman Leliefeld Androsmannenkliniek The Netherlands The reality of LOH symptoms male external & internal genitalia Testosterone
The reality of LOH-symptoms PRISM IV Bruges, Belgium September 25-26, 2014 Dr. Herman Leliefeld Androsmannenkliniek The Netherlands The reality of LOH symptoms male external & internal genitalia Testosterone
Erectile Dysfunction, Cardiovascular Risk and
 Erectile Dysfunction, Cardiovascular Risk and Testosterone National Lipid Association (NLA) 2016 Fall Clinical Update August 26-28, 2016 Amelia Island, Fl Robert A. Kloner MD, PhD Director of the Cardiovascular
Erectile Dysfunction, Cardiovascular Risk and Testosterone National Lipid Association (NLA) 2016 Fall Clinical Update August 26-28, 2016 Amelia Island, Fl Robert A. Kloner MD, PhD Director of the Cardiovascular
Current Data and Considerations Novel Testosterone Formulations
 Current Data and Considerations Novel Testosterone Formulations 1 Hypogonadism: Treatment Safety and Prostate Health 2 Monitoring for Testosterone Therapy DRE 1,2 PSA Parameter Voiding/IPSS 1,2 Hemoglobin
Current Data and Considerations Novel Testosterone Formulations 1 Hypogonadism: Treatment Safety and Prostate Health 2 Monitoring for Testosterone Therapy DRE 1,2 PSA Parameter Voiding/IPSS 1,2 Hemoglobin
Outline. Classic Androgen deficiency. Cardiovascular Risk and Testosterone Fact vs Fiction. Professor Robert I McLachlan AM, FRACP, PhD
 Health Ed Brisbane Saturday 27 th October 2018 Cardiovascular Risk and Testosterone Fact vs Fiction Professor Robert I McLachlan AM, FRACP, PhD Hudson Institute of Medical Research, Monash University Department
Health Ed Brisbane Saturday 27 th October 2018 Cardiovascular Risk and Testosterone Fact vs Fiction Professor Robert I McLachlan AM, FRACP, PhD Hudson Institute of Medical Research, Monash University Department
Recognizing and Managing Testosterone Deficiency
 Recognizing and Managing Testosterone Deficiency J. Bruce Redmon, M.D. Professor Division of Endocrinology Departments of Medicine and Urologic Surgery Disclosure Information I have no financial relationships
Recognizing and Managing Testosterone Deficiency J. Bruce Redmon, M.D. Professor Division of Endocrinology Departments of Medicine and Urologic Surgery Disclosure Information I have no financial relationships
Managing Testosterone Deficiency: A Practical Guide. John Grantmyre MD Professor of Urology Dalhousie University
 Managing Testosterone Deficiency: A Practical Guide John Grantmyre MD Professor of Urology Dalhousie University 1 2 Case Study #1 A 59-Year-Old Man with Erectile Dysfunction 3 Case History Robert is a
Managing Testosterone Deficiency: A Practical Guide John Grantmyre MD Professor of Urology Dalhousie University 1 2 Case Study #1 A 59-Year-Old Man with Erectile Dysfunction 3 Case History Robert is a
Testosterone Injection and Implant
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.33 Subject: Testosterone Injection Implant Page: 1 of 10 Last Review Date: November 30, 2018 Testosterone
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.33 Subject: Testosterone Injection Implant Page: 1 of 10 Last Review Date: November 30, 2018 Testosterone
6/14/2010. GnRH=Gonadotropin-Releasing Hormone.
 Male Androgen Replacement Mitchell Sorsby, MD June 19, 2010. QUESTION # 1 Which of the following is not a symptom associated with low T levels? a) decreased libido b) erectile dysfunction c) depression
Male Androgen Replacement Mitchell Sorsby, MD June 19, 2010. QUESTION # 1 Which of the following is not a symptom associated with low T levels? a) decreased libido b) erectile dysfunction c) depression
HORMONE THERAPY IN AGING MALE ATHLETES
 DISCLOSURES HORMONE THERAPY IN AGING MALE ATHLETES No relevant affiliations or financial interests When, Why and is it Safe? OBJECTIVES Summarize the benefits of optimizing hormone balance Examine the
DISCLOSURES HORMONE THERAPY IN AGING MALE ATHLETES No relevant affiliations or financial interests When, Why and is it Safe? OBJECTIVES Summarize the benefits of optimizing hormone balance Examine the
Testosterone Treatment: Myths Vs Reality. Fadi Al-Khayer, M.D, F.A.C.E
 Testosterone Treatment: Myths Vs Reality Fadi Al-Khayer, M.D, F.A.C.E The Biological Functions of Testosterone in Men Testosterone is essential to the musculoskeletal and metabolic systems throughout a
Testosterone Treatment: Myths Vs Reality Fadi Al-Khayer, M.D, F.A.C.E The Biological Functions of Testosterone in Men Testosterone is essential to the musculoskeletal and metabolic systems throughout a
Hypogonadism* (män) Erytrocytos Kardiovaskulär risk
 Erytrocytos Kardiovaskulär risk") Hypogonadism* (män) Erytrocytos Kardiovaskulär risk *Lågt Testosteron och symtom Stefan Arver ANOVA, Karolinska Univ Sjukhuset Inst. F Medicin/Huddinge Karolinska Institutet Endokrindagar i Umeå 2019 1
Hypogonadism* (män) Erytrocytos Kardiovaskulär risk *Lågt Testosteron och symtom Stefan Arver ANOVA, Karolinska Univ Sjukhuset Inst. F Medicin/Huddinge Karolinska Institutet Endokrindagar i Umeå 2019 1
Testosterone Injection and Implant
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.33 Subject: Testosterone Injection Implant Page: 1 of 10 Last Review Date: December 8, 2017 Testosterone
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.33 Subject: Testosterone Injection Implant Page: 1 of 10 Last Review Date: December 8, 2017 Testosterone
Testosterone Injection / Implant
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Testosterone Injection / Implant Page: 1 of 9 Last Review Date: December 5, 2014 Testosterone
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Testosterone Injection / Implant Page: 1 of 9 Last Review Date: December 5, 2014 Testosterone
Testosterone Injection and Implant
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.33 Subject: Testosterone Injection Implant Page: 1 of 10 Last Review Date: March 17, 2017 Testosterone
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.33 Subject: Testosterone Injection Implant Page: 1 of 10 Last Review Date: March 17, 2017 Testosterone
IL RUOLO DEL DEFICIT DI TESTOSTERONE NELLA SINDROME METABOLICA E NELLA INSUFFICIENZA RENALE NEL MASCHIO ADULTO. VA Giagulli
 IL RUOLO DEL DEFICIT DI TESTOSTERONE NELLA SINDROME METABOLICA E NELLA INSUFFICIENZA RENALE NEL MASCHIO ADULTO VA Giagulli UOS di Endocrinologia e Malattie Metaboliche PT di Conversano ASL BA Male hypogonadism
IL RUOLO DEL DEFICIT DI TESTOSTERONE NELLA SINDROME METABOLICA E NELLA INSUFFICIENZA RENALE NEL MASCHIO ADULTO VA Giagulli UOS di Endocrinologia e Malattie Metaboliche PT di Conversano ASL BA Male hypogonadism
PCa Commentary. Prostate Cancer? Where's the Meat? - A Collection of Studies Supporting the Safety of Its Use. Seattle Prostate Institute CONTENTS
 Volume 70 July - August 2011 PCa Commentary SEATTLE PROSTATE INSTITUTE CONTENTS TESTOSTERONE REPLACEMENT in Hypogonadal Men with Treated and Untreated Prostate Cancer? 1 TESTOSTERONE REPLACEMENT in Hypogonadal
Volume 70 July - August 2011 PCa Commentary SEATTLE PROSTATE INSTITUTE CONTENTS TESTOSTERONE REPLACEMENT in Hypogonadal Men with Treated and Untreated Prostate Cancer? 1 TESTOSTERONE REPLACEMENT in Hypogonadal
TESTOSTERONE REPLACEMENT THERAPY. WHAT IS THE REAL RISK? WHAT TO DO IN PROSTATE CANCER?
 TESTOSTERONE REPLACEMENT THERAPY. WHAT IS THE REAL RISK? WHAT TO DO IN PROSTATE CANCER? TESTOSTERONE REPLACEMENT THERAPY (TRT) Nuno Tomada, MD, PhD Department of Urology of Hospital S. João Faculty of
TESTOSTERONE REPLACEMENT THERAPY. WHAT IS THE REAL RISK? WHAT TO DO IN PROSTATE CANCER? TESTOSTERONE REPLACEMENT THERAPY (TRT) Nuno Tomada, MD, PhD Department of Urology of Hospital S. João Faculty of
Index. urologic.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Acquired hypogonadism, prevalence of, 165 167 primary, 165 secondary, 167 Adipose tissue, as an organ, 240 241 Adrenal hyperplasia, congenital,
Note: Page numbers of article titles are in boldface type. A Acquired hypogonadism, prevalence of, 165 167 primary, 165 secondary, 167 Adipose tissue, as an organ, 240 241 Adrenal hyperplasia, congenital,
Testosterone Replacement Therapy for Hypogonadism: Learning Objectives. What Is the Evidence? Is It Safe? Case Study. Case Study contd.
 4 4:4pm Testosterone Therapy: Examining the Evidence SPEAKER Culley Carson, MD Presenter Disclosure Information The following relationships exist related to this presentation: Culley Carson, MD: Consultant
4 4:4pm Testosterone Therapy: Examining the Evidence SPEAKER Culley Carson, MD Presenter Disclosure Information The following relationships exist related to this presentation: Culley Carson, MD: Consultant
Late Onset Hypogonadism. Toh Charng Chee Hospital Selayang
 Late Onset Hypogonadism Toh Charng Chee Hospital Selayang Introduction Although suppressed serum testosterone (T) is common in ageing men, only a small proportion of them develop the genuine syndrome of
Late Onset Hypogonadism Toh Charng Chee Hospital Selayang Introduction Although suppressed serum testosterone (T) is common in ageing men, only a small proportion of them develop the genuine syndrome of
Hypogonadism in Men. CME Away India & Sri Lanka March 23 - April 7, 2018
 Hypogonadism in Men CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright 2017
Hypogonadism in Men CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright 2017
Over the past decade, androgen replacement
 J. Andrew Hoover, MD; Jeffrey T. Kirchner, DO, FAAFP Department of Family and Community Medicine, Lancaster General Hospital, Pa jhoover4@lghealth.org The authors reported no potential conflict of interest
J. Andrew Hoover, MD; Jeffrey T. Kirchner, DO, FAAFP Department of Family and Community Medicine, Lancaster General Hospital, Pa jhoover4@lghealth.org The authors reported no potential conflict of interest
Pharmacy Coverage Guidelines are subject to change as new information becomes available.
 TESTOSTERONE REPLACEMENT THERAPY: ANDRODERM transdermal patch ANDROGEL pump transdermal gel and transdermal gel ANDROID (methyltestosterone) oral capsule ANDROXY (fluoxymesterone) oral tablet AXIRON transdermal
TESTOSTERONE REPLACEMENT THERAPY: ANDRODERM transdermal patch ANDROGEL pump transdermal gel and transdermal gel ANDROID (methyltestosterone) oral capsule ANDROXY (fluoxymesterone) oral tablet AXIRON transdermal
Diagnosis and management of testosterone deficiency syndrome in adult men: clinical practice guideline (CMAJ)
") Diagnosis and management of testosterone deficiency syndrome in adult men: clinical practice guideline (CMAJ) Alvaro Morales CM MD, Richard A. Bebb MD, Priya Manjoo MD MSc, Peter Assimakopoulos MD, John
Diagnosis and management of testosterone deficiency syndrome in adult men: clinical practice guideline (CMAJ) Alvaro Morales CM MD, Richard A. Bebb MD, Priya Manjoo MD MSc, Peter Assimakopoulos MD, John
Does TRT Induce Prostate Cancer?
 Does TRT Induce Prostate Cancer? Prism VI, Bruges, Belgium 21-22November 2014 Herman Leliefeld, Urologist, Utrecht The Netherlands Does TRT Induce Prostate Cancer? Why is it a controversial topic? Is there
Does TRT Induce Prostate Cancer? Prism VI, Bruges, Belgium 21-22November 2014 Herman Leliefeld, Urologist, Utrecht The Netherlands Does TRT Induce Prostate Cancer? Why is it a controversial topic? Is there
Androderm patch, AndroGel packets and pump, Axiron solution, First- Testosterone, First-Testosterone MC, Fortesta gel, Testim gel, Vogelxo
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.31 Subject: Testosterone Topical Page: 1 of 9 Last Review Date: September 23, 2016 Testosterone topical
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.31 Subject: Testosterone Topical Page: 1 of 9 Last Review Date: September 23, 2016 Testosterone topical
HHS Public Access Author manuscript Int J Impot Res. Author manuscript; available in PMC 2015 September 01.
 Testosterone Therapy and Mortality Risk Michael L. Eisenberg, MD 1, Shufeng Li, MS 2, Danielle Herder, MD 3, Dolores J. Lamb, PhD 4, and Larry I. Lipshultz, MD 4 1 Assistant Professor, Departments of Urology
Testosterone Therapy and Mortality Risk Michael L. Eisenberg, MD 1, Shufeng Li, MS 2, Danielle Herder, MD 3, Dolores J. Lamb, PhD 4, and Larry I. Lipshultz, MD 4 1 Assistant Professor, Departments of Urology
TRT and localized protate cancer
 TRT and localized protate cancer Frans M. J. Debruyne Professor of Urology PRISM BRUGES Increased risk of prostate cancer with TRT? Prostate cancer Testosterone and Prostate Cancer There appears to be
TRT and localized protate cancer Frans M. J. Debruyne Professor of Urology PRISM BRUGES Increased risk of prostate cancer with TRT? Prostate cancer Testosterone and Prostate Cancer There appears to be
Testosterone: Current Opinion and Controversy
 Testosterone: Current Opinion and Controversy Ravi Kacker, MD Metrowest Urology (508) 655 4422 Medical Office Building at Leonard Morse Hospital Disclosures MHB Labs President and CEO of Drug Development
Testosterone: Current Opinion and Controversy Ravi Kacker, MD Metrowest Urology (508) 655 4422 Medical Office Building at Leonard Morse Hospital Disclosures MHB Labs President and CEO of Drug Development
Pharmacy Coverage Guidelines are subject to change as new information becomes available.
 TESTOSTERONE REPLACEMENT THERAPY: ANDRODERM transdermal patch ANDROGEL pump transdermal gel and transdermal gel AXIRON transdermal solution FORTESTA transdermal gel NATESTO nasal gel STRIANT buccal mucoadhesive
TESTOSTERONE REPLACEMENT THERAPY: ANDRODERM transdermal patch ANDROGEL pump transdermal gel and transdermal gel AXIRON transdermal solution FORTESTA transdermal gel NATESTO nasal gel STRIANT buccal mucoadhesive
EAU GUIDELINES ON MALE HYPOGONADISM
 EAU GUIDELINES ON MALE HYPOGONADISM (Limited text update March 2017) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch Introduction Male hypogonadism is a clinical syndrome caused by androgen
EAU GUIDELINES ON MALE HYPOGONADISM (Limited text update March 2017) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch Introduction Male hypogonadism is a clinical syndrome caused by androgen
HORMONE REPLACEMENT THERAPY
 TRIALS OF HR RUTH (Barrett- Connor et al 29 ) JULY 2006 (Country) mean ± sd, range International trial 67.5 an Placebo component in 67.5 ± 6.7 women with Raloxifene or multiple 67.5 ± 6.6 risk factors
TRIALS OF HR RUTH (Barrett- Connor et al 29 ) JULY 2006 (Country) mean ± sd, range International trial 67.5 an Placebo component in 67.5 ± 6.7 women with Raloxifene or multiple 67.5 ± 6.6 risk factors
EFFICACY AND SAFETY OF TESTOSTERONE THERAPY FOR LATE-ONSET HYPOGONADISM: AN UPDATE
 EFFICACY AND SAFETY OF TESTOSTERONE THERAPY FOR LATE-ONSET HYPOGONADISM: AN UPDATE Matthew Ho, PGY-2 Department of Urologic Sciences University of British Columbia OBJECTIVES 1. Review the characteristics
EFFICACY AND SAFETY OF TESTOSTERONE THERAPY FOR LATE-ONSET HYPOGONADISM: AN UPDATE Matthew Ho, PGY-2 Department of Urologic Sciences University of British Columbia OBJECTIVES 1. Review the characteristics
Testosterone Replacement in Adults. John A. Seibel, MD, FACP, MACE
 Testosterone Replacement in Adults John A. Seibel, MD, FACP, MACE Disclosures None! *Privately Authenticated Definition of Male Hypogonadism inadequate gonadal function, as manifested by deficiencies in
Testosterone Replacement in Adults John A. Seibel, MD, FACP, MACE Disclosures None! *Privately Authenticated Definition of Male Hypogonadism inadequate gonadal function, as manifested by deficiencies in
Sleep Apnea: Vascular and Metabolic Complications
 Sleep Apnea: Vascular and Metabolic Complications Vahid Mohsenin, M.D. Professor of Medicine Yale University School of Medicine Director, Yale Center for Sleep Medicine Definitions Apnea: Cessation of
Sleep Apnea: Vascular and Metabolic Complications Vahid Mohsenin, M.D. Professor of Medicine Yale University School of Medicine Director, Yale Center for Sleep Medicine Definitions Apnea: Cessation of
Testosterone and the Prostate
 Testosterone and the Prostate E. David Crawford, MD Professor of Surgery (Urology) and Radiation Oncology Head, Urologic Oncology E. David and Vicki M. Crawford Endowed Chair in Urologic Oncology University
Testosterone and the Prostate E. David Crawford, MD Professor of Surgery (Urology) and Radiation Oncology Head, Urologic Oncology E. David and Vicki M. Crawford Endowed Chair in Urologic Oncology University
ISSM QUICK REFERENCE GUIDE ON TESTOSTERONE DEFICIENCY FOR MEN
 International Society for Sexual Medicine - www.issm.info ISSM QUICK REFERENCE GUIDE ON TESTOSTERONE DEFICIENCY FOR MEN Version: September 2015 What is testosterone deficiency? Testosterone deficiency
International Society for Sexual Medicine - www.issm.info ISSM QUICK REFERENCE GUIDE ON TESTOSTERONE DEFICIENCY FOR MEN Version: September 2015 What is testosterone deficiency? Testosterone deficiency
Transgender Medicine: Essentials for the Primary Care Provider BENJAMIN J. BOH, DO, MS
 Transgender Medicine: Essentials for the Primary Care Provider BENJAMIN J. BOH, DO, MS ASSISTANT PROFESSOR OF MEDICINE SECTION OF ENDOCRINOLOGY GEISEL SCHOOL OF MEDICINE AT DARTMOUTH Disclosure I will
Transgender Medicine: Essentials for the Primary Care Provider BENJAMIN J. BOH, DO, MS ASSISTANT PROFESSOR OF MEDICINE SECTION OF ENDOCRINOLOGY GEISEL SCHOOL OF MEDICINE AT DARTMOUTH Disclosure I will
Male Hypogonadism. Types and causes of hypogonadism. What is male hypogonadism? Symptoms. Testosterone production. Patient Information.
 Patient Information English 31 Male Hypogonadism The underlined terms are listed in the glossary. What is male hypogonadism? Male hypogonadism means the testicles do not produce enough of the male sex
Patient Information English 31 Male Hypogonadism The underlined terms are listed in the glossary. What is male hypogonadism? Male hypogonadism means the testicles do not produce enough of the male sex
Testosterone and PDE5 inhibitors in the aging male
 Testosterone and PDE5 inhibitors in the aging male Francesco Romanelli Department of Experimental Medicine Medical Pathophysiology, Food Science and Endocrinology Section Sapienza University of Rome 3005
Testosterone and PDE5 inhibitors in the aging male Francesco Romanelli Department of Experimental Medicine Medical Pathophysiology, Food Science and Endocrinology Section Sapienza University of Rome 3005
Late onset hypogonadism
 Late onset hypogonadism Farrukh Javid Male Menopause Clinical AND biochemical syndrome Testosterone levels decline by 0.4-3% per year after the age of 30, as opposed to the more rapid decline that occurs
Late onset hypogonadism Farrukh Javid Male Menopause Clinical AND biochemical syndrome Testosterone levels decline by 0.4-3% per year after the age of 30, as opposed to the more rapid decline that occurs
Testosterone Oral Buccal Nasal. Android, Androxy, Methitest, Natesto, Striant, Testred. Description
 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.32 Subject: Testosterone Oral Buccal Nasal Page: 1 of 10 Last Review Date: March 17, 2017 Testosterone Oral Buccal Nasal Description
1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.32 Subject: Testosterone Oral Buccal Nasal Page: 1 of 10 Last Review Date: March 17, 2017 Testosterone Oral Buccal Nasal Description
Vitamin D and Calcium Therapy: how much is enough
 Vitamin D and Calcium Therapy: how much is enough Daniel D Bikle, MD, PhD Professor of Medicine VA Medical Center and University of California San Francisco DISCLOSURE Nothing to disclose 1 RECOMMENDATIONS
Vitamin D and Calcium Therapy: how much is enough Daniel D Bikle, MD, PhD Professor of Medicine VA Medical Center and University of California San Francisco DISCLOSURE Nothing to disclose 1 RECOMMENDATIONS
Best Practices to Improve Patient Outcomes
 Best Practices Pearls Practical Primary Care Strategies for Diagnosing and Managing Hypogonadism in Men Utilize lab testing in appropriate patients who have complaints consistent with the often subtle
Best Practices Pearls Practical Primary Care Strategies for Diagnosing and Managing Hypogonadism in Men Utilize lab testing in appropriate patients who have complaints consistent with the often subtle
Androgen deficiency. Dr Rakesh Iyer Staff Specialist in Endocrinology Calvary hospital
 Androgen deficiency Dr Rakesh Iyer Staff Specialist in Endocrinology Calvary hospital Outline Pathological androgen deficiency - Background, causes, interpretation - Indications for treatment Androgen
Androgen deficiency Dr Rakesh Iyer Staff Specialist in Endocrinology Calvary hospital Outline Pathological androgen deficiency - Background, causes, interpretation - Indications for treatment Androgen
Testosterone Oral Buccal Nasal. Android, Androxy, Methitest, Natesto, Striant, Testred. Description
 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.32 Subject: Testosterone Oral Buccal Nasal Page: 1 of 10 Last Review Date: June 24, 2016 Testosterone Oral Buccal Nasal Description
1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.32 Subject: Testosterone Oral Buccal Nasal Page: 1 of 10 Last Review Date: June 24, 2016 Testosterone Oral Buccal Nasal Description
The Endocrine Society Guidelines
 Vitamin D and Calcium Therapy: how much is enough DISCLOSURE Daniel D Bikle, MD, PhD Professor of Medicine VA Medical Center and University of California San Francisco Nothing to disclose RECOMMENDATIONS
Vitamin D and Calcium Therapy: how much is enough DISCLOSURE Daniel D Bikle, MD, PhD Professor of Medicine VA Medical Center and University of California San Francisco Nothing to disclose RECOMMENDATIONS
State of California, California Health and Human Services Agency, Department of Managed Health Care 2013:
 This policy has been developed through review of medical literature, consideration of medical necessity, generally accepted medical practice standards, and approved by the IEHP Pharmacy and Therapeutics
This policy has been developed through review of medical literature, consideration of medical necessity, generally accepted medical practice standards, and approved by the IEHP Pharmacy and Therapeutics
Testosterone Oral Buccal Nasal. Android, Androxy, Methitest, Natesto, Striant, Testred. Description
 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.32 Subject: Testosterone Oral Buccal Nasal Page: 1 of 10 Last Review Date: November 30, 2018 Testosterone Oral Buccal Nasal
1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.32 Subject: Testosterone Oral Buccal Nasal Page: 1 of 10 Last Review Date: November 30, 2018 Testosterone Oral Buccal Nasal
Hormone Replacement Therapy
 Hormone Replacement Therapy What Role Should It Play With Our Patients? Noel R. Williams MD, FACOG TESTOSTERONE FOR MEN: SALVATION OR SNAKE OIL? Definition Male hypogonadism means the testicles don't produce
Hormone Replacement Therapy What Role Should It Play With Our Patients? Noel R. Williams MD, FACOG TESTOSTERONE FOR MEN: SALVATION OR SNAKE OIL? Definition Male hypogonadism means the testicles don't produce
Implantable Hormone Pellets
 Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Clinical Policy: Testosterone Pellet (Testopel) Reference Number: CP.CPA.## [Pre-P&T approval] Effective Date:
![Clinical Policy: Testosterone Pellet (Testopel) Reference Number: CP.CPA.## [Pre-P&T approval] Effective Date:](/thumbs/75/72057018.jpg "Clinical Policy: Testosterone Pellet (Testopel) Reference Number: CP.CPA.## [Pre-P&T approval] Effective Date:") Clinical Policy: (Testopel) Reference Number: CP.CPA.## [Pre-P&T approval] Effective Date: 07.25.17 Last Review Date: 11.17 Line of Business: Commercial Coding Implications Revision Log See Important Reminder
Clinical Policy: (Testopel) Reference Number: CP.CPA.## [Pre-P&T approval] Effective Date: 07.25.17 Last Review Date: 11.17 Line of Business: Commercial Coding Implications Revision Log See Important Reminder
9/2/2016. Faculty. Learning Objectives. Disclosures. Prevalence of Hypogonadism. Prevalence of HG (cont)
") Faculty Testosterone Replacement Therapies: Mitigating Cardiometabolic Risks Associated with Hypogonadism Pamela Ellsworth, MD Professor of Urology University of Massachusetts Medical School Vice Chair,
Faculty Testosterone Replacement Therapies: Mitigating Cardiometabolic Risks Associated with Hypogonadism Pamela Ellsworth, MD Professor of Urology University of Massachusetts Medical School Vice Chair,
Fasting or non fasting?
 Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
Kathryn M. Rexrode, MD, MPH. Assistant Professor. Division of Preventive Medicine Brigham and Women s s Hospital Harvard Medical School
 Update: Hormones and Cardiovascular Disease in Women Kathryn M. Rexrode, MD, MPH Assistant Professor Division of Preventive Medicine Brigham and Women s s Hospital Harvard Medical School Overview Review
Update: Hormones and Cardiovascular Disease in Women Kathryn M. Rexrode, MD, MPH Assistant Professor Division of Preventive Medicine Brigham and Women s s Hospital Harvard Medical School Overview Review
Therapeutic Cohort Results
 Patient: JANE DOE DOB: December 31, 1968 Sex: F MRN: Order Number: Completed: February 26, 2016 Received: February 26, 2016 Collected: February 26, 2016 One Day Hormone Check - Salivary Profile Therapeutic
Patient: JANE DOE DOB: December 31, 1968 Sex: F MRN: Order Number: Completed: February 26, 2016 Received: February 26, 2016 Collected: February 26, 2016 One Day Hormone Check - Salivary Profile Therapeutic
The Effect of Androgen-replacement Therapy on Prostate Growth: A Systematic Review and Meta-analysis
 EUROPEAN UROLOGY 64 (2013) 811 822 available at www.sciencedirect.com journal homepage: www.europeanurology.com Review Benign Prostatic Enlargement The Effect of Androgen-replacement Therapy on Prostate
EUROPEAN UROLOGY 64 (2013) 811 822 available at www.sciencedirect.com journal homepage: www.europeanurology.com Review Benign Prostatic Enlargement The Effect of Androgen-replacement Therapy on Prostate
UK policy statements on testosterone deficiency
 Received: 4 March 2016 Revised: 24 August 2016 Accepted: 27 September 2016 DOI: 10.1111/ijcp.12901 CONSENSUS UK policy statements on testosterone deficiency Geoffrey Hackett 1,2 Michael Kirby 3,4 David
Received: 4 March 2016 Revised: 24 August 2016 Accepted: 27 September 2016 DOI: 10.1111/ijcp.12901 CONSENSUS UK policy statements on testosterone deficiency Geoffrey Hackett 1,2 Michael Kirby 3,4 David
Sleep apnea as a risk factor for cardiovascular disease
 Sleep apnea as a risk factor for cardiovascular disease Malcolm Kohler Chair Respiratory Medicine, Clinical Director, Department of Pulmonology, University Hospital Zurich Incidence of fatal cardiovascular
Sleep apnea as a risk factor for cardiovascular disease Malcolm Kohler Chair Respiratory Medicine, Clinical Director, Department of Pulmonology, University Hospital Zurich Incidence of fatal cardiovascular
Men Getting Older Will Testosterone Keep Him Young?
 Men Getting Older Will Testosterone Keep Him Young? Alvin M. Matsumoto, M.D. Associate Director, GRECC V.A. Puget Sound Health Care System Professor, Department of Medicine Division of Gerontology and
Men Getting Older Will Testosterone Keep Him Young? Alvin M. Matsumoto, M.D. Associate Director, GRECC V.A. Puget Sound Health Care System Professor, Department of Medicine Division of Gerontology and
NEW DEVELOPMENTS: T & CVD FDA & THE T TRIALS
 NEW DEVELOPMENTS: T & CVD FDA & THE T TRIALS 2017 UPDATE FDUS Martin Miner MD Clinical Professor of Family Medicine and Urology Co-Director The Men s Health Center The Miriam Hospital Warren Albert School
NEW DEVELOPMENTS: T & CVD FDA & THE T TRIALS 2017 UPDATE FDUS Martin Miner MD Clinical Professor of Family Medicine and Urology Co-Director The Men s Health Center The Miriam Hospital Warren Albert School
Assessment and management of male androgen disorders: an update
 Irene Chan Mark Ng Tang Fui Jeffrey D Zajac Mathis Grossmann Assessment and management of male androgen disorders: an update Background Male hypogonadism, caused by intrinsic pathology of the hypothalamic
Irene Chan Mark Ng Tang Fui Jeffrey D Zajac Mathis Grossmann Assessment and management of male androgen disorders: an update Background Male hypogonadism, caused by intrinsic pathology of the hypothalamic
Therapeutic Cohort Results
 Patient: SAMPLE PATIENT DOB: Sex: MRN: Menopause Plus - Salivary Profile Therapeutic Cohort Results Hormone Average Result QUINTILE DISTRIBUTION 1st 2nd 3rd 4th 5th Therapeutic Range* Estradiol (E2) 8.7
Patient: SAMPLE PATIENT DOB: Sex: MRN: Menopause Plus - Salivary Profile Therapeutic Cohort Results Hormone Average Result QUINTILE DISTRIBUTION 1st 2nd 3rd 4th 5th Therapeutic Range* Estradiol (E2) 8.7
The Male Andropause. What are the symptoms? What are the risks of hormone deficiencies?
 The Male Andropause By: Dr. Sangeeta Pati MD, FACOG Although, the male andropause has not been widely recognized, increased medical research has turned attention to the gradual hormone decline in males
The Male Andropause By: Dr. Sangeeta Pati MD, FACOG Although, the male andropause has not been widely recognized, increased medical research has turned attention to the gradual hormone decline in males
Testosterone Therapy and Risk of Myocardial Infarction: A Pharmacoepidemiologic Study
 Testosterone Therapy and Risk of Myocardial Infarction: A Pharmacoepidemiologic Study Mahyar Etminan, 1,2, * Sean C. Skeldon, 3,4 Sheldon Larry Goldenberg, 3 Bruce Carleton, 1,2 and James M. Brophy 5 1
Testosterone Therapy and Risk of Myocardial Infarction: A Pharmacoepidemiologic Study Mahyar Etminan, 1,2, * Sean C. Skeldon, 3,4 Sheldon Larry Goldenberg, 3 Bruce Carleton, 1,2 and James M. Brophy 5 1
Andropause: Current concepts
 Review Article Andropause: Current concepts Parminder Singh Division of Endocrinology, Dayanand Medical College and Hospital, Ludhiana, Punjab, India ABSTRACT Andropause or late-onset hypogonadism is a
Review Article Andropause: Current concepts Parminder Singh Division of Endocrinology, Dayanand Medical College and Hospital, Ludhiana, Punjab, India ABSTRACT Andropause or late-onset hypogonadism is a
Update on Androgen Deficiency. Acknowledgments. Curatio PowerPoint TemplateControversies in Male Hypogonadism Bradley D.
 The General Practice Education Day Healthed / Generation Next August 22 nd Sydney Update on Androgen Deficiency Robert I. McLachlan, FRACP, PhD Director, Andrology Australia Principal Research Fellow,
The General Practice Education Day Healthed / Generation Next August 22 nd Sydney Update on Androgen Deficiency Robert I. McLachlan, FRACP, PhD Director, Andrology Australia Principal Research Fellow,
Adverse effects of testosterone replacement therapy: an update on the evidence and controversy
 548680TAW0010.1177/2042098614548680Therapeutic Advances in Drug SafetyHeidelbaugh research-article2014 Therapeutic Advances in Drug Safety Review Adverse effects of testosterone replacement therapy: an
548680TAW0010.1177/2042098614548680Therapeutic Advances in Drug SafetyHeidelbaugh research-article2014 Therapeutic Advances in Drug Safety Review Adverse effects of testosterone replacement therapy: an
Benefits Investigation Form Instructions for Buy-and-Bill
 Benefits Investigation Form Instructions for Buy-and-Bill Within this guide you can find: Step-by-step instructions on how to fill out the Benefits Investigation Form for Buy-and-Bill Key contact information
Benefits Investigation Form Instructions for Buy-and-Bill Within this guide you can find: Step-by-step instructions on how to fill out the Benefits Investigation Form for Buy-and-Bill Key contact information
Varenicline and cardiovascular and neuropsychiatric events: Do Benefits outweigh risks?
 Varenicline and cardiovascular and neuropsychiatric events: Do Benefits outweigh risks? Sonal Singh M.D., M.P.H, Johns Hopkins University Presented by: Sonal Singh, MD MPH September 19, 2012 1 CONFLICTS
Varenicline and cardiovascular and neuropsychiatric events: Do Benefits outweigh risks? Sonal Singh M.D., M.P.H, Johns Hopkins University Presented by: Sonal Singh, MD MPH September 19, 2012 1 CONFLICTS
BAD TO THE BONE. Peter Jones, Rheumatologist QE Health, Rotorua. GP CME Conference Rotorua, June 2008
 BAD TO THE BONE Peter Jones, Rheumatologist QE Health, Rotorua GP CME Conference Rotorua, June 2008 Agenda Osteoporosis in Men Vitamin D and Calcium Long-term treatment with Bisphosphonates Pathophysiology
BAD TO THE BONE Peter Jones, Rheumatologist QE Health, Rotorua GP CME Conference Rotorua, June 2008 Agenda Osteoporosis in Men Vitamin D and Calcium Long-term treatment with Bisphosphonates Pathophysiology
ADT AND CARDIOVASCULAR RISK: should Antagonists be the primary choice for ADT?
 ADT AND CARDIOVASCULAR RISK: should Antagonists be the primary choice for ADT? Igor Tsaur University Medicine Mainz COI Urologische Klinik und Poliklinik Off-label use of drugs, devices, or other agents:
ADT AND CARDIOVASCULAR RISK: should Antagonists be the primary choice for ADT? Igor Tsaur University Medicine Mainz COI Urologische Klinik und Poliklinik Off-label use of drugs, devices, or other agents:
Tesamorelin Clinical Data Overview Jean-Claude Mamputu, PhD Senior Medical Advisor, Theratechnologies
 Tesamorelin Clinical Data Overview Jean-Claude Mamputu, PhD Senior Medical Advisor, Theratechnologies Copyright 2016. All Rights Reserved. Property of Theratechnologies Inc. Mechanism of Action of Tesamorelin
Tesamorelin Clinical Data Overview Jean-Claude Mamputu, PhD Senior Medical Advisor, Theratechnologies Copyright 2016. All Rights Reserved. Property of Theratechnologies Inc. Mechanism of Action of Tesamorelin