THINGS ARE NOT ALWAYS AS THEY APPEAR. Assume Nothing!
|
|
|
- Toby O’Connor’
- 5 years ago
- Views:
Transcription
1 THINGS ARE NOT ALWAYS AS THEY APPEAR Assume Nothing!
2

3 UP SIDE DOWN WORLD OF PROSTATE CANCER Paul D. Thompson, M.D. Fort Worth Texas
4 WHAT WE THOUGHT WE KNEW AND WHAT WE KNOW TODAY
5 FINANCIAL DISCLOSURES Carrie Thompson Jo Max Sydney Mate Joey Bindi
6 WHAT IS PROSTATE CANCER? Prostate cancer is the second-leading cause of cancer deaths for men in the U.S. This year, nearly 165,000 men will be diagnosed with prostate cancer About 1 in 9 men will be diagnosed with prostate cancer in their lifetime.

7 DOCTOR PROSTATE
8 CHARLES HUGGINS UPON RECEIVING HIS NOBEL PRIZE OH, LORD, Thy sea is so vast and my bark is so small
9 HIS WORK Established a system to measure the effect Hormone changes have on prostate function Discovered that castration or estrogen administration led to atrophy That the atrophy could be reversed with androgens With Clarence Hodges used acid phosphatase to measure therapeutic efficacy The first to use systemic approach to treat prostate cancer
10 ACID PHOSPHATASE H&H noted acid phosphatase elevated in 21 out of 47 prostate cases and 19 0f 25 with bone mets present 8 were treated with castration and all had acid phosphatase levels fall drastically Administering testosterone restored acid phosphatase to at least pretreatment levels This demonstrated an androgen dependence and the anti cancer effect removal of the androgen had
11 HUGGINS ET AL: 3 men treated with Testosterone Only 2 were reported on Of the 2, 1 was castrated prior
12 HUGGINS ET AL CONT. 1 man received testosterone injections without prior hormonal manipulation The basis for Fuel on a fire was 1 patient and a now known equivocal test The basis of this myth was based on next to nothing
13 VA COOPERATIVE STUDY DEC. 73. The first VA study did not show that orchiectomy was superior to estrogen in treating cancer of the prostate or that the combination orchiectomy plus estrogen had much to offer beyond the benefits of estrogen alone. The results of the clinical trials over 12 years revealed an unsuspected toxicity of DES used in treating patients with cancer of the prostate when given in a dose of 5.0 mg daily. The preponderance of evidence from the second study showed that 1.0 mg of DES appeared to be about as effective as the 5.0 mg dose in treating cancer of the prostate without the excess hazard of cardiovascular deaths
14 Many of us learned from our professors to describe the relationship of T to pca as fuel for a fire and food for a hungry tumor. stratoor estrogen treatment caused metastatic pct To this day, androgen ablation remains a mainstay of treatment for advanced pca, the concern regarding T and the risk of pca has reached to the highest levels of medicine. Abraham Morgentaler MD
15 PROSTATE CANCER & TESTOSTERONE In 2001 the director of the National Cancer Institute in the United States explained his reluctance to fund a large testosterone replacement therapy (TRT) trial, he stated that he was concerned that testosterone could spur the growth of prostate cancer among some men in the study TRT has long been considered taboo among men with a prior history of pca regardless of disease status, and product information mandated by the FDA states that known or suspected carcinoma of the prostate is a contraindication for T products While there is no dispute that castration causes pca to regress, proof for the second part of Huggins assertion, that T causes pca to grow, has been elusive. If testosterone is so bad for prostate cancer, why is it so hard to prove?
16 PROSTATE CANCER AND TESTOSTERONE The original assertion that T caused pca growth in untreated individuals was thus based on equivocal acid phosphatase results in a single individual. exogenous T in men with metastatic pca The largest series of exogenous T in men with metastatic pca was reported by Fowler and Whitmore. Sixty-seven men, all with a history of bone metastases, received T injections under various protocols, Of 52 men with evaluable responses, 45 had unfavorable responses. Four of these men had not previously undergone orchiectomy or estrogen treatment. Within this untreated group oneonehad a subjective beneficial response, and the remaining two eventually developed unfavorable responses at 56 and 310 d of daily T administration, respectively. Given the advanced stage of pca in these men and the lack of a control group, we must consider that the unfavorable responses seen in this population may have been due to the natural history of their disease.
17 TRT & PCA Cancer. 1967;20: Prout and Brewer, daily T injections in 26 men with stage C and D disease. 20 had not undergone castration or hormonal treatment. Majority experienced a sense of well being and some had decrease in pain. Acid phosphatase was variable. Cancer Res. 1957;17; pearson. 1 untreated patient with advanced pca, severe bone pain secondary to mets. With addition of testosterone there was relief of pain, patient remained asymptomatic for 9 months while receiving daily T injections.
18 TESTOSTERONE AND PCA Testosterone flare With the introduction in the 1980s of luteinising hormone-releasing hormone agonists that reduced T to castrate levels, it was noted that a transient rise in T occurred over the first 8 10 d. Reports of adverse events occurring during this period of time, such as increased bone pain, urinary retention, and vertebral collapse with paraplegia, have been attributed to pca growth with the testosterone flare. A few studies have measured PSA in men with advanced pca during the flare, PSA values never rose above baseline PSA. The flat PSA curve noted during the T flare suggests that increased T did not cause pca to progress The adverse events noted during the flare interval may have been due to the natural history of metastatic pca
19 TESTOSTERONE & PCA Clinical trials of TRT No large, long-term studies of TRT have been performed. However, the pca rate in published TRT trials is approximately 1%. This rate is similar to the cancer detection rate in prostate cancer-screening trials.. The relationship of T and other hormones to the development of pca has been studied in at least 16 population-based longitudinal studies. Not one has shown a direct correlation between total T levels and pca. The largest study of this type noted an increased pca risk with low T levels.
20 TRT IN PCA PATIENTS Journal of Urology 2011 April, TRT in untreated pca patients that were low in Testosterone had no growth effect on the cancer British Journal of Urology July 2014, 20 patients s/p brachytherapy some with Gleason scores of 3+4 and one with 4+4 followed for 31 months, no cases of rising PSA
21 TESTOSTERONE & PCA TRT in a high-risk population pca has been reported to develop over 3 years in 25% of men with high-grade prostatic intraepithelial neoplasia (PIN). In one study, TRT was provided to 20 hypogonadal men with PIN and 55 hypogonadal men with benign biopsies. At the end of 12 mo, pca was identified in one man in the PIN group and none in the benign group, which represents a 5% cancer rate in the PIN group and a 1.3% risk overall. These results do not suggest an increase of pca growth or development in this high-risk group.
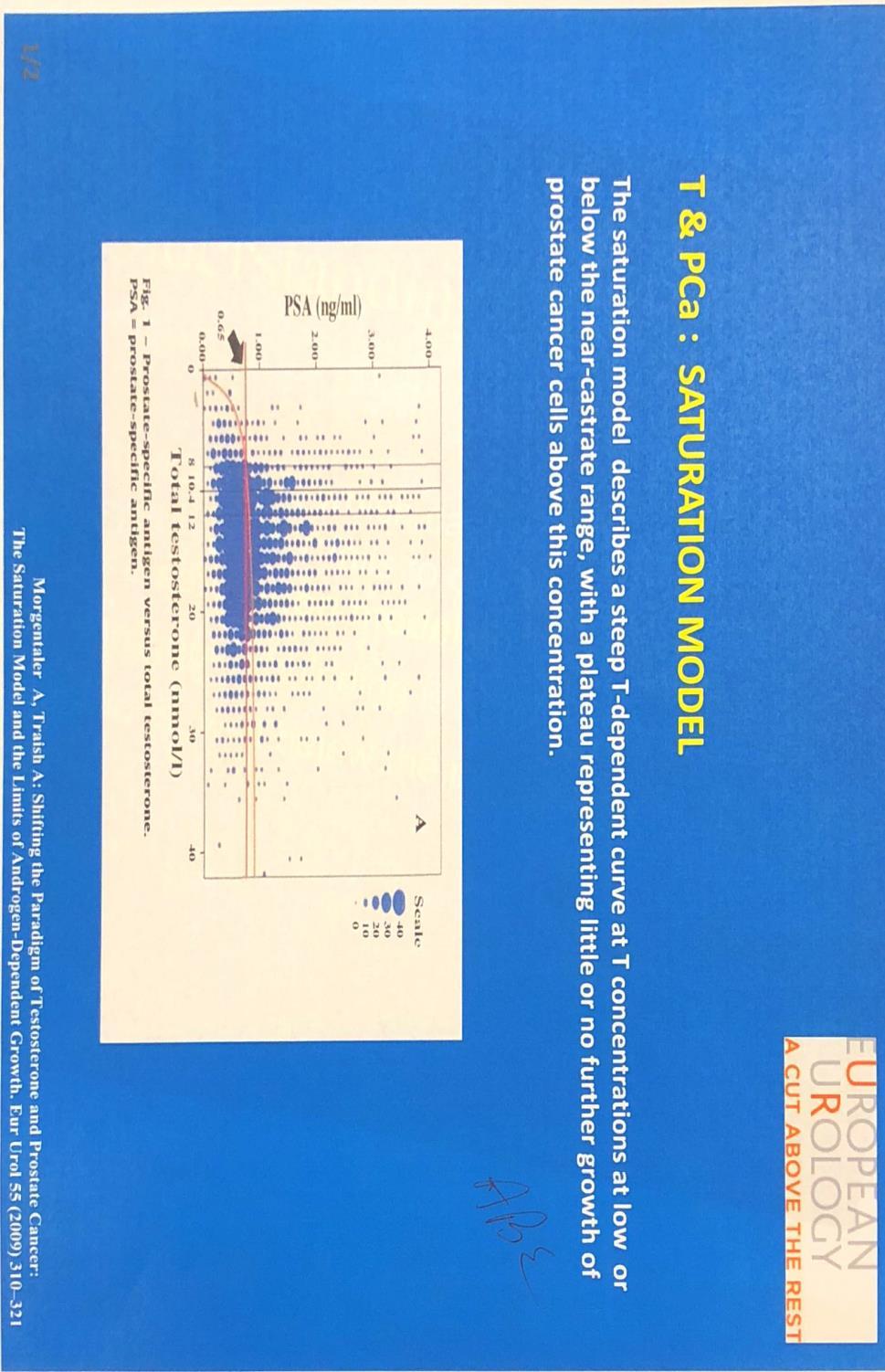
22 TESTOSTERONE & PCA Since lowering T causes pca to regress, why is it that raising T fails to cause pca to grow? The solution lies in the concept of saturation, in which maximal stimulation of pca growth is achieved at some relatively low concentration of T. This model for T and pca was suggested by Fowler and Whitmore, who concluded a quarter century ago that normal endogenous testosterone levels may be sufficient to cause near maximal stimulation of prostatic tumors.
23 SATURATION
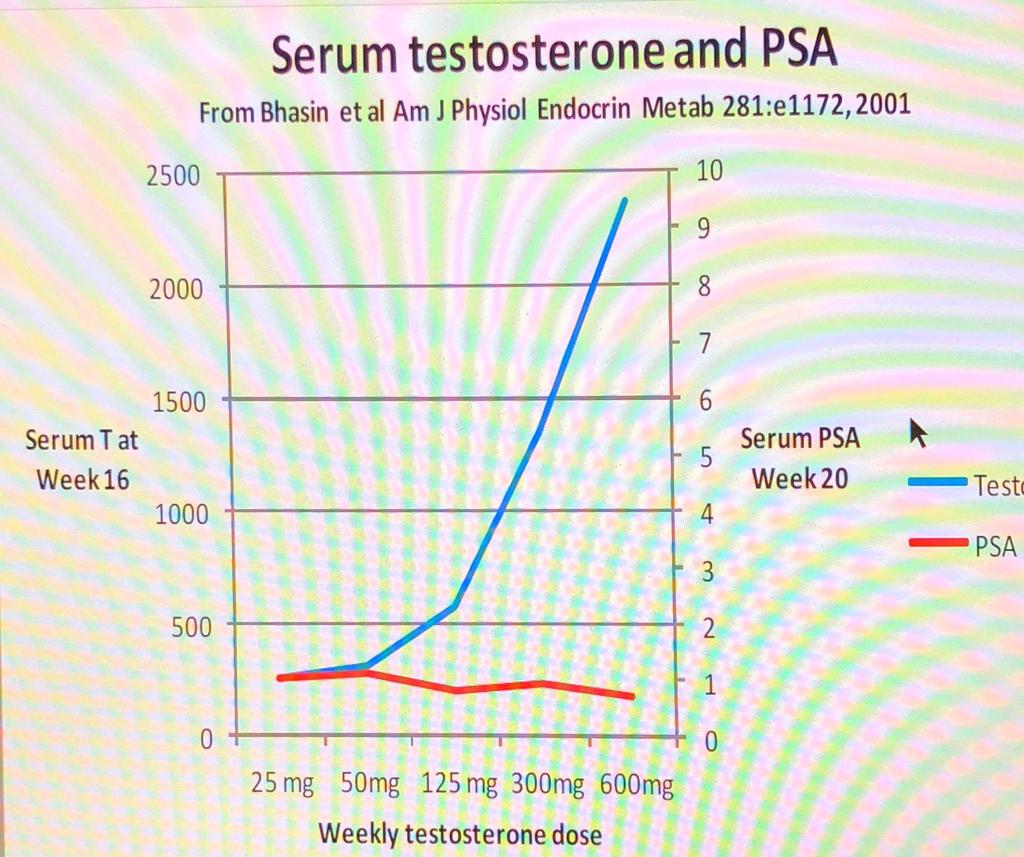
24 TESTOSTERONE & PCA At T levels below the saturation point, pca growth would be expected to vary with T concentration, which is consistent with the observation of pca regrowth with T normalization after androgen ablation. This model is also supported in that exogenous T administered to normal men fails to cause any increase in PSA or prostate volume. In hypogonadal men, TRT results in only modest increases in prostate size, approximately 15% for PSA and prostate volume, with volume increasing to match optimized men, but rising no higher. there is not today nor has there ever been a scientific basis for the contention that a higher T concentration causes pca growth.
25 TESTOSTERONE & PCA accumulating evidence linking low T with pca, including associations with high-grade disease, higher stage at presentation, and worse prognosis? Might it even be possible that androgen administration could prevent pca? After 65 yr it is time to discard the myth and to entertain new ideas regarding the relationship of T and pca. A Morgantaler MD
26 DR MORGANTALER

27 KNOWLEDGE ALLOWS US TO STAND UP TO THE STATUS QUO
28 PROSTATE CANCER FOUNDATION So the short answer is both simple and complicated, and it s the same advice your doctors will give you for almost any question, eat healthy foods, stay in shape, and get enough rest. You should also maintain a thoughtfully designed screening regimen for prostate cancer as you age. The rest. is up to luck.
29 ENDOCRINE DISRUPTORS AND PCA Increasing evidence that endorine disruptors may influence the development and progression of pca Included are pesticides, PCBs and BPA ( found in urine of 93% of US population according to the CDC Calafat et al Appears to be increased risk of in developmental periods utero, neonatal and puberty Infants and children are hgh risk for developing pca with aging.

30 QUALITY OF LIFE There is more to life than quantity

 the Huggins 1941 article and notice details that all had")
31 THE NEW DR PROSTATE Actively promoting the use of TRT and reshaping the therapeutic levels and indications Stood up to former professors who thought he was taking to big of risk using TRT in the 90s The first to re (read) the Huggins 1941 article and notice details that all had missed
32 DR PROSTATE Continues to educate others on prostate Cancer Optimal levels of testosterone Testosterone benefits Educating the lay person on all aspects of Testosterone
33 SO WHAT ROLE DOES ESTROGEN HAVE IN PROSTATECANCER?
34 HAVE YOU READ THE WHI? Risks and Benefits of Estrogen Plus Progestin in Healthy Postmenopausal WomenPrincipal Results From the Women's Health Initiative Randomized Controlled Trial Writing Group for the Women's Health Initiative Investigators JAMA. 2002;288(3): doi: /jama Results from WHI indicate that the combined postmenopausal hormones CEE, mg/d, plus MPA, 2.5 mg/d, should not be initiated or continued for the primary prevention of CHD. In addition, the substantial risks for cardiovascular disease and breast cancer must be weighed against the benefit for fracture in selecting from the available agents to prevent osteoporosis.

35 AMMG THE PEOPLE IN THIS ROOM. YOU ARE MY GANG

36 LIFE What s really important
EVIDENCE SUPPORTING TESTOSTERONE THERAPY IN MEN WITH PROSTATE CANCER
 EVIDENCE SUPPORTING TESTOSTERONE THERAPY IN MEN WITH PROSTATE CANCER Abraham Morgentaler, MD Director and Founder Men s Health Boston Associate Clinical Professor Harvard Medical School And the Urology
EVIDENCE SUPPORTING TESTOSTERONE THERAPY IN MEN WITH PROSTATE CANCER Abraham Morgentaler, MD Director and Founder Men s Health Boston Associate Clinical Professor Harvard Medical School And the Urology
Testosterone Therapy and the Prostate. Frans M.J. Debruyne Professor of Urology The Netherlands
 Testosterone Therapy and the Prostate Frans M.J. Debruyne Professor of Urology The Netherlands TRT- Risks Prostate ( Cancer, BPH )? Cardiac? Lipids? Polycythemia Sleep apnea Gynecomastia Edema Testosterone
Testosterone Therapy and the Prostate Frans M.J. Debruyne Professor of Urology The Netherlands TRT- Risks Prostate ( Cancer, BPH )? Cardiac? Lipids? Polycythemia Sleep apnea Gynecomastia Edema Testosterone
Testosterone and the Prostate
 Testosterone and the Prostate E. David Crawford, MD Professor of Surgery (Urology) and Radiation Oncology Head, Urologic Oncology E. David and Vicki M. Crawford Endowed Chair in Urologic Oncology University
Testosterone and the Prostate E. David Crawford, MD Professor of Surgery (Urology) and Radiation Oncology Head, Urologic Oncology E. David and Vicki M. Crawford Endowed Chair in Urologic Oncology University
Point-Counterpoint: Late Onset Hypogonadism (LOH)
") Point-Counterpoint: Late Onset Hypogonadism (LOH) We are Under-diagnosing and Treating Men with LOH LOH is a Non-existent Disease ~ Robert E. Donohue, MD Late Onset Hypogonadism LOH: underdx. & undertx
Point-Counterpoint: Late Onset Hypogonadism (LOH) We are Under-diagnosing and Treating Men with LOH LOH is a Non-existent Disease ~ Robert E. Donohue, MD Late Onset Hypogonadism LOH: underdx. & undertx
Does TRT Induce Prostate Cancer?
 Does TRT Induce Prostate Cancer? Prism VI, Bruges, Belgium 21-22November 2014 Herman Leliefeld, Urologist, Utrecht The Netherlands Does TRT Induce Prostate Cancer? Why is it a controversial topic? Is there
Does TRT Induce Prostate Cancer? Prism VI, Bruges, Belgium 21-22November 2014 Herman Leliefeld, Urologist, Utrecht The Netherlands Does TRT Induce Prostate Cancer? Why is it a controversial topic? Is there
TESTOSTERONE REPLACEMENT THERAPY. WHAT IS THE REAL RISK? WHAT TO DO IN PROSTATE CANCER?
 TESTOSTERONE REPLACEMENT THERAPY. WHAT IS THE REAL RISK? WHAT TO DO IN PROSTATE CANCER? TESTOSTERONE REPLACEMENT THERAPY (TRT) Nuno Tomada, MD, PhD Department of Urology of Hospital S. João Faculty of
TESTOSTERONE REPLACEMENT THERAPY. WHAT IS THE REAL RISK? WHAT TO DO IN PROSTATE CANCER? TESTOSTERONE REPLACEMENT THERAPY (TRT) Nuno Tomada, MD, PhD Department of Urology of Hospital S. João Faculty of
HIGH-DOSE TESTOSTERONE REPLACEMENT THERAPY AND PROSTATE CANCER
 Bob Leibowitz, M.D. DIPLOMATE AMERICAN BOARDS OF INTERNAL MEDICINE AND SUBSPECIALTIES OF MEDICAL ONCOLOGY AND HEMATOLOGY HIGH-DOSE TESTOSTERONE REPLACEMENT THERAPY AND PROSTATE CANCER The package insert
Bob Leibowitz, M.D. DIPLOMATE AMERICAN BOARDS OF INTERNAL MEDICINE AND SUBSPECIALTIES OF MEDICAL ONCOLOGY AND HEMATOLOGY HIGH-DOSE TESTOSTERONE REPLACEMENT THERAPY AND PROSTATE CANCER The package insert
PCa Commentary. Prostate Cancer? Where's the Meat? - A Collection of Studies Supporting the Safety of Its Use. Seattle Prostate Institute CONTENTS
 Volume 70 July - August 2011 PCa Commentary SEATTLE PROSTATE INSTITUTE CONTENTS TESTOSTERONE REPLACEMENT in Hypogonadal Men with Treated and Untreated Prostate Cancer? 1 TESTOSTERONE REPLACEMENT in Hypogonadal
Volume 70 July - August 2011 PCa Commentary SEATTLE PROSTATE INSTITUTE CONTENTS TESTOSTERONE REPLACEMENT in Hypogonadal Men with Treated and Untreated Prostate Cancer? 1 TESTOSTERONE REPLACEMENT in Hypogonadal
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 /
 METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
Definition Prostate cancer
 Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
TRT and localized protate cancer
 TRT and localized protate cancer Frans M. J. Debruyne Professor of Urology PRISM BRUGES Increased risk of prostate cancer with TRT? Prostate cancer Testosterone and Prostate Cancer There appears to be
TRT and localized protate cancer Frans M. J. Debruyne Professor of Urology PRISM BRUGES Increased risk of prostate cancer with TRT? Prostate cancer Testosterone and Prostate Cancer There appears to be
Hormone therapy works best when combined with radiation for locally advanced prostate cancer
 Hormone therapy works best when combined with radiation for locally advanced prostate cancer Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Introduction Introduction 1/3 of patients
Hormone therapy works best when combined with radiation for locally advanced prostate cancer Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Introduction Introduction 1/3 of patients
Naviga2ng the Adverse Effects of ADT: Improving Pa2ent Outcomes
 Naviga2ng the Adverse Effects of ADT: Improving Pa2ent Outcomes E. David Crawford, M.D. Professor of Surgery/ Urology/ Radiation Oncology University of Colorado Greetings from Colorado Disclosures Consultant:
Naviga2ng the Adverse Effects of ADT: Improving Pa2ent Outcomes E. David Crawford, M.D. Professor of Surgery/ Urology/ Radiation Oncology University of Colorado Greetings from Colorado Disclosures Consultant:
Hormone Replacement Therapy
 Hormone Replacement Therapy What Role Should It Play With Our Patients? Noel R. Williams MD, FACOG TESTOSTERONE FOR MEN: SALVATION OR SNAKE OIL? Definition Male hypogonadism means the testicles don't produce
Hormone Replacement Therapy What Role Should It Play With Our Patients? Noel R. Williams MD, FACOG TESTOSTERONE FOR MEN: SALVATION OR SNAKE OIL? Definition Male hypogonadism means the testicles don't produce
Disclosures. Learning Objectives. Effects of Hormone Therapy on the Metabolic Syndrome and Cardiovascular Disease. None
 Effects of Hormone Therapy on the Metabolic Syndrome and Cardiovascular Disease Micol S. Rothman, MD Associate Professor of Medicine Endocrinology, Diabetes and Metabolism Clinical Director Metabolic Bone
Effects of Hormone Therapy on the Metabolic Syndrome and Cardiovascular Disease Micol S. Rothman, MD Associate Professor of Medicine Endocrinology, Diabetes and Metabolism Clinical Director Metabolic Bone
Screening and Risk Stratification of Men for Prostate Cancer Metastasis and Mortality
 Screening and Risk Stratification of Men for Prostate Cancer Metastasis and Mortality Sanoj Punnen, MD, MAS Assistant Professor of Urologic Oncology University of Miami, Miller School of Medicine and Sylvester
Screening and Risk Stratification of Men for Prostate Cancer Metastasis and Mortality Sanoj Punnen, MD, MAS Assistant Professor of Urologic Oncology University of Miami, Miller School of Medicine and Sylvester
The Return of My Cancer -Emerging Effective Therapies Jianqing Lin, MD
 Februray, 2013 The Return of My Cancer -Emerging Effective Therapies Jianqing Lin, MD Why/How my cancer is back after surgery and/or radiation? Undetected micro-metastatic disease (spreading) before local
Februray, 2013 The Return of My Cancer -Emerging Effective Therapies Jianqing Lin, MD Why/How my cancer is back after surgery and/or radiation? Undetected micro-metastatic disease (spreading) before local
MODULE 8: PROSTATE CANCER: SCREENING & MANAGEMENT
 MODULE 8: PROSTATE CANCER: SCREENING & MANAGEMENT KEYWORDS: Prostate cancer, PSA, Screening, Radical Prostatectomy LEARNING OBJECTIVES At the end of this clerkship, the medical student will be able to:
MODULE 8: PROSTATE CANCER: SCREENING & MANAGEMENT KEYWORDS: Prostate cancer, PSA, Screening, Radical Prostatectomy LEARNING OBJECTIVES At the end of this clerkship, the medical student will be able to:
Testosterone Replacement Therapy (TRT) - Been diagnosed with and treated for prostate cancer?
 - Been diagnosed with and treated for prostate cancer?") Testosterone Replacement Therapy (TRT) - Been diagnosed with and treated for prostate cancer? Compiled by Charles (Chuck) Maack Prostate Cancer Activist/Mentor DISCLAIMER: Please recognize that I am not
Testosterone Replacement Therapy (TRT) - Been diagnosed with and treated for prostate cancer? Compiled by Charles (Chuck) Maack Prostate Cancer Activist/Mentor DISCLAIMER: Please recognize that I am not
Risk of renal side effects with ADT. E. David Crawford University of Colorado, Aurora, CO, USA
 Risk of renal side effects with ADT E. David Crawford University of Colorado, Aurora, CO, USA ADT: A key treatment for advanced prostate cancer John Hunter 1780-castration 1904: First RP 1938: Acid Phos.
Risk of renal side effects with ADT E. David Crawford University of Colorado, Aurora, CO, USA ADT: A key treatment for advanced prostate cancer John Hunter 1780-castration 1904: First RP 1938: Acid Phos.
ADENOCARCINOMA OF THE PROSTATE
 Ref : ADENOCARCINOMA OF THE PROSTATE Div. of Urology, Dept. Surgery Medical Faculty, University of Sumatera Utara Clinical Manual of Urology, (Philip M. Hanno et al eds), McGraw-Hill Int ed, 3 rd ed, 2001
Ref : ADENOCARCINOMA OF THE PROSTATE Div. of Urology, Dept. Surgery Medical Faculty, University of Sumatera Utara Clinical Manual of Urology, (Philip M. Hanno et al eds), McGraw-Hill Int ed, 3 rd ed, 2001
SERMS, Hormone Therapy and Calcitonin
 SERMS, Hormone Therapy and Calcitonin Tiffany Kim, MD Clinical Fellow VA Advanced Women s Health UCSF Endocrinology and Metabolism I have nothing to disclose Thanks to Clifford Rosen and Steven Cummings
SERMS, Hormone Therapy and Calcitonin Tiffany Kim, MD Clinical Fellow VA Advanced Women s Health UCSF Endocrinology and Metabolism I have nothing to disclose Thanks to Clifford Rosen and Steven Cummings
AllinaHealthSystems 1
 2018 Dimensions in Oncology Genitourinary Cancer Disclosures I have no financial or commercial relationships relevant to this presentation. Matthew O Shaughnessy, MD, PhD Director of Urologic Oncology
2018 Dimensions in Oncology Genitourinary Cancer Disclosures I have no financial or commercial relationships relevant to this presentation. Matthew O Shaughnessy, MD, PhD Director of Urologic Oncology
HORMONE THERAPY IN AGING MALE ATHLETES
 DISCLOSURES HORMONE THERAPY IN AGING MALE ATHLETES No relevant affiliations or financial interests When, Why and is it Safe? OBJECTIVES Summarize the benefits of optimizing hormone balance Examine the
DISCLOSURES HORMONE THERAPY IN AGING MALE ATHLETES No relevant affiliations or financial interests When, Why and is it Safe? OBJECTIVES Summarize the benefits of optimizing hormone balance Examine the
Quality of Life with an Aging Prostate: The Sperling Prostate Center Protocol. Dan Sperling, MD, DABR The Sperling Prostate Center Delray Beach, FL
 Quality of Life with an Aging Prostate: The Sperling Prostate Center Protocol Dan Sperling, MD, DABR The Sperling Prostate Center Delray Beach, FL As men age, physiological changes affect QOL Testosterone
Quality of Life with an Aging Prostate: The Sperling Prostate Center Protocol Dan Sperling, MD, DABR The Sperling Prostate Center Delray Beach, FL As men age, physiological changes affect QOL Testosterone
Outcomes of Prostate Biopsy in Men with Hypogonadism Prior or During Testosterone Replacement Therapy
 ORIGINAL ARTICLE Vol. 41 (6): 1167-1171, November. December, 2015 doi: 10.1590/S1677-5538.IBJU.2014.0528 Outcomes of Prostate Biopsy in Men with Hypogonadism Prior or During Testosterone Replacement Therapy
ORIGINAL ARTICLE Vol. 41 (6): 1167-1171, November. December, 2015 doi: 10.1590/S1677-5538.IBJU.2014.0528 Outcomes of Prostate Biopsy in Men with Hypogonadism Prior or During Testosterone Replacement Therapy
response of PCa to testosterone deprivation in the early 1940s, testosterone has been considered as fuel to the fire of PCa.
 BJUI BJU INTERNATIONAL Low testosterone levels are related to poor prognosis factors in men with prostate cancer prior to treatment Eduardo Garc í a-cruz, Marta Piqueras, Jorge Huguet, Lluis Peri, Laura
BJUI BJU INTERNATIONAL Low testosterone levels are related to poor prognosis factors in men with prostate cancer prior to treatment Eduardo Garc í a-cruz, Marta Piqueras, Jorge Huguet, Lluis Peri, Laura
Prostate Cancer Case Study 2. Medical Student Case-Based Learning
 Prostate Cancer Case Study 2 Medical Student Case-Based Learning The Case of Mr. Powers Prostate Cancer Recurrence Mr. Powers is a young appearing, healthy 73-year old male who underwent a radical prostatectomy
Prostate Cancer Case Study 2 Medical Student Case-Based Learning The Case of Mr. Powers Prostate Cancer Recurrence Mr. Powers is a young appearing, healthy 73-year old male who underwent a radical prostatectomy
Saving. Kidneys. Prostate Cancer
 Saving Kidneys 10 Prostate Cancer This booklet will tell you more about the prostate cancer. It will also help you understand this disease in a better way. You will also come to know the causes and treatment
Saving Kidneys 10 Prostate Cancer This booklet will tell you more about the prostate cancer. It will also help you understand this disease in a better way. You will also come to know the causes and treatment
Diagnosis and management of testosterone deficiency syndrome in adult men: clinical practice guideline (CMAJ)
") Diagnosis and management of testosterone deficiency syndrome in adult men: clinical practice guideline (CMAJ) Alvaro Morales CM MD, Richard A. Bebb MD, Priya Manjoo MD MSc, Peter Assimakopoulos MD, John
Diagnosis and management of testosterone deficiency syndrome in adult men: clinical practice guideline (CMAJ) Alvaro Morales CM MD, Richard A. Bebb MD, Priya Manjoo MD MSc, Peter Assimakopoulos MD, John
Clinical Policy: Goserelin Acetate (Zoladex) Reference Number: ERX.SPA.145 Effective Date:
 Reference Number: ERX.SPA.145 Effective Date:") Clinical Policy: (Zoladex) Reference Number: ERX.SPA.145 Effective Date: 10.01.16 Last Review Date: 11.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Zoladex) Reference Number: ERX.SPA.145 Effective Date: 10.01.16 Last Review Date: 11.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Changes in prostate-specific antigen and hormone levels following withdrawal of prolonged androgen ablation for prostate cancer
 Changes in prostate-specific antigen and hormone levels following withdrawal of prolonged androgen ablation for prostate cancer S Egawa 1 *, H Okusa 1, K Matsumoto 1, K Suyama 1 & S Baba 1 1 Department
Changes in prostate-specific antigen and hormone levels following withdrawal of prolonged androgen ablation for prostate cancer S Egawa 1 *, H Okusa 1, K Matsumoto 1, K Suyama 1 & S Baba 1 1 Department
PCA MORTALITY VS TREATMENTS
 PCA MORTALITY VS TREATMENTS Terrence P McGarty White Paper No 145 July, 2017 In a recent NEJM paper the authors argue that there is no material difference between a prostatectomy and just "observation"
PCA MORTALITY VS TREATMENTS Terrence P McGarty White Paper No 145 July, 2017 In a recent NEJM paper the authors argue that there is no material difference between a prostatectomy and just "observation"
BSO, HRT, and ERT. No relevant financial disclosures
 BSO, HRT, and ERT Jubilee Brown, MD Professor & Associate Director, Gynecologic Oncology Levine Cancer Institute at the Carolinas HealthCare System Charlotte, North Carolina No relevant financial disclosures
BSO, HRT, and ERT Jubilee Brown, MD Professor & Associate Director, Gynecologic Oncology Levine Cancer Institute at the Carolinas HealthCare System Charlotte, North Carolina No relevant financial disclosures
Metastatic prostate carcinoma. Lee Say Bob July 2017
 Metastatic prostate carcinoma Lee Say Bob July 2017 Scenario A 58 year old gentleman presents with PSA 200 ng/ml with hard prostate and bone mets. LUTS but upper tracts are normal with normal RP. history
Metastatic prostate carcinoma Lee Say Bob July 2017 Scenario A 58 year old gentleman presents with PSA 200 ng/ml with hard prostate and bone mets. LUTS but upper tracts are normal with normal RP. history
Challenging Cases. With Q&A Panel
 Challenging Cases With Q&A Panel Case Studies Index Patient #1 Jeffrey Wieder, MD Case # 1 72 year old healthy male with mild HTN Early 2011: Preop bone scan and pelvic CT = no mets Radical prostatectomy
Challenging Cases With Q&A Panel Case Studies Index Patient #1 Jeffrey Wieder, MD Case # 1 72 year old healthy male with mild HTN Early 2011: Preop bone scan and pelvic CT = no mets Radical prostatectomy
Prostate Cancer: 2010 Guidelines Update
 Prostate Cancer: 2010 Guidelines Update James L. Mohler, MD Chair, NCCN Prostate Cancer Panel Associate Director for Translational Research, Professor and Chair, Department of Urology, Roswell Park Cancer
Prostate Cancer: 2010 Guidelines Update James L. Mohler, MD Chair, NCCN Prostate Cancer Panel Associate Director for Translational Research, Professor and Chair, Department of Urology, Roswell Park Cancer
Initial hormone therapy (and more) for metastatic prostate cancer
 for metastatic prostate cancer") Initial hormone therapy (and more) for metastatic prostate cancer Silke Gillessen, MD Medical Oncology Kantonsspital St.Gallen Switzerland silke.gillessen@kssg.ch Conflicts of interest Speakers Bureau
Initial hormone therapy (and more) for metastatic prostate cancer Silke Gillessen, MD Medical Oncology Kantonsspital St.Gallen Switzerland silke.gillessen@kssg.ch Conflicts of interest Speakers Bureau
Natural Hormones Replacement An Evidence and Practice Based Approach
 Natural Hormones Replacement An Evidence and Practice Based Approach Andres Ruiz, PharmD, MSc, FACA President/Partner Stonegate Pharmacy PRESENTED BY THE AMERICAN COLLEGE OF APOTHECARIES 2830 SUMMER OAKS
Natural Hormones Replacement An Evidence and Practice Based Approach Andres Ruiz, PharmD, MSc, FACA President/Partner Stonegate Pharmacy PRESENTED BY THE AMERICAN COLLEGE OF APOTHECARIES 2830 SUMMER OAKS
reviews LHRH Agonists in the Treatment of Advanced Carcinoma of the Prostate therapy
 reviews therapy LHRH Agonists in the Treatment of Advanced Carcinoma of the Prostate Martin I. Resnick, MD, Lester Persky Professor and Chief, Department of Urology, Case Western Reserve University School
reviews therapy LHRH Agonists in the Treatment of Advanced Carcinoma of the Prostate Martin I. Resnick, MD, Lester Persky Professor and Chief, Department of Urology, Case Western Reserve University School
Testosterone Therapy in Men with Hypogonadism
 Testosterone Therapy in Men with Hypogonadism (Endocrine Society 2018 Guideline) Ngwe Yin, MD Assistant Clinical Professor of Medicine, UCSF Fresno Medical Education Program Disclosures None Objective
Testosterone Therapy in Men with Hypogonadism (Endocrine Society 2018 Guideline) Ngwe Yin, MD Assistant Clinical Professor of Medicine, UCSF Fresno Medical Education Program Disclosures None Objective
VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE
 Session 3 Advanced prostate cancer VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE 1 PSA is a serine protease and the physiological role is believed to be liquefying the seminal fluid PSA
Session 3 Advanced prostate cancer VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE 1 PSA is a serine protease and the physiological role is believed to be liquefying the seminal fluid PSA
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW
 LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Abiraterone for the treatment of metastatic castration-resistant prostate cancer that has progressed on or after a docetaxel-based chemotherapy regimen Disease
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Abiraterone for the treatment of metastatic castration-resistant prostate cancer that has progressed on or after a docetaxel-based chemotherapy regimen Disease
Testosterone Oral Buccal Nasal. Android, Androxy, Methitest, Natesto, Striant, Testred. Description
 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.32 Subject: Testosterone Oral Buccal Nasal Page: 1 of 10 Last Review Date: March 17, 2017 Testosterone Oral Buccal Nasal Description
1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.32 Subject: Testosterone Oral Buccal Nasal Page: 1 of 10 Last Review Date: March 17, 2017 Testosterone Oral Buccal Nasal Description
HT: Where do we stand after WHI?
 HT: Where do we stand after WHI? Hormone therapy and cardiovascular disease risk Experimental and clinical evidence indicate that hormone therapy (HT) reduces the risk of cardiovascular disease (CVD) Women
HT: Where do we stand after WHI? Hormone therapy and cardiovascular disease risk Experimental and clinical evidence indicate that hormone therapy (HT) reduces the risk of cardiovascular disease (CVD) Women
MENOPAUSE. I have no disclosures 10/11/18 OBJECTIVES WHAT S NEW? WHAT S SAFE?
 MENOPAUSE WHAT S NEW? WHAT S SAFE? I have no disclosures Sara Whetstone, MD, MHS OBJECTIVES To describe risks of HT by age and menopause onset To recommend specific HT regimen for women who undergo early
MENOPAUSE WHAT S NEW? WHAT S SAFE? I have no disclosures Sara Whetstone, MD, MHS OBJECTIVES To describe risks of HT by age and menopause onset To recommend specific HT regimen for women who undergo early
A Competing Risk Analysis of Men Age Years at Diagnosis Managed Conservatively for Clinically Localized Prostate Cancer
 A Competing Risk Analysis of Men Age 55-74 Years at Diagnosis Managed Conservatively for Clinically Localized Prostate Cancer Peter C. Albertsen, MD 1 James A. Hanley, PhD 2 Donald F.Gleason, MD, PhD 3
A Competing Risk Analysis of Men Age 55-74 Years at Diagnosis Managed Conservatively for Clinically Localized Prostate Cancer Peter C. Albertsen, MD 1 James A. Hanley, PhD 2 Donald F.Gleason, MD, PhD 3
Testosterone Oral Buccal Nasal. Android, Androxy, Methitest, Natesto, Striant, Testred. Description
 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.32 Subject: Testosterone Oral Buccal Nasal Page: 1 of 10 Last Review Date: November 30, 2018 Testosterone Oral Buccal Nasal
1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.32 Subject: Testosterone Oral Buccal Nasal Page: 1 of 10 Last Review Date: November 30, 2018 Testosterone Oral Buccal Nasal
Overview. What is Cancer? Prostate Cancer 3/2/2014. Davis A Romney, MD Ironwood Cancer and Research Centers Feb 18, 2014
 Prostate Cancer Davis A Romney, MD Ironwood Cancer and Research Centers Feb 18, 2014 Overview Start with the basics: Definition of cancer Most common cancers in men Prostate, lung, and colon cancers Cancer
Prostate Cancer Davis A Romney, MD Ironwood Cancer and Research Centers Feb 18, 2014 Overview Start with the basics: Definition of cancer Most common cancers in men Prostate, lung, and colon cancers Cancer
Testosterone Oral Buccal Nasal. Android, Androxy, Methitest, Natesto, Striant, Testred. Description
 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.32 Subject: Testosterone Oral Buccal Nasal Page: 1 of 10 Last Review Date: June 24, 2016 Testosterone Oral Buccal Nasal Description
1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.32 Subject: Testosterone Oral Buccal Nasal Page: 1 of 10 Last Review Date: June 24, 2016 Testosterone Oral Buccal Nasal Description
Incorporating New Agents into the Treatment Paradigm for Prostate Cancer
 Incorporating New Agents into the Treatment Paradigm for Prostate Cancer Dr. Celestia S. Higano FACP, Professor, Medicine and Urology, Uni. of Washington Member, Fred Hutchinson Cancer Research Center
Incorporating New Agents into the Treatment Paradigm for Prostate Cancer Dr. Celestia S. Higano FACP, Professor, Medicine and Urology, Uni. of Washington Member, Fred Hutchinson Cancer Research Center
When PSA fails. Urology Grand Rounds Alexandra Perks. Rising PSA after Radical Prostatectomy
 When PSA fails Urology Grand Rounds Alexandra Perks Rising PSA after Radical Prostatectomy Issues Natural History Local vs Metastatic Treatment options 1 10 000 men / year in Canada 4000 RRP 15-year PSA
When PSA fails Urology Grand Rounds Alexandra Perks Rising PSA after Radical Prostatectomy Issues Natural History Local vs Metastatic Treatment options 1 10 000 men / year in Canada 4000 RRP 15-year PSA
Testosterone therapy in men with prostate cancer: literature review, clinical experience, and recommendations
 (2015) 17, 206 211 2015 AJA, SIMM & SJTU. All rights reserved 1008-682X www.asiaandro.com; www.ajandrology.com Male Endocrinology Open Access INVITED REVIEW Testosterone therapy in men with prostate cancer:
(2015) 17, 206 211 2015 AJA, SIMM & SJTU. All rights reserved 1008-682X www.asiaandro.com; www.ajandrology.com Male Endocrinology Open Access INVITED REVIEW Testosterone therapy in men with prostate cancer:
Breast Cancer and Bone Loss. One in seven women will develop breast cancer during a lifetime
 Breast Cancer and Bone Loss One in seven women will develop breast cancer during a lifetime Causes of Bone Loss in Breast Cancer Patients Aromatase inhibitors Bil Oophorectomy Hypogonadism Steroids Chemotherapy
Breast Cancer and Bone Loss One in seven women will develop breast cancer during a lifetime Causes of Bone Loss in Breast Cancer Patients Aromatase inhibitors Bil Oophorectomy Hypogonadism Steroids Chemotherapy
Evaluation and Treatment of Primary Androgen Deficiency Syndrome in Male Patients
 Evaluation and Treatment of Primary Androgen Deficiency Syndrome in Male Patients Jeff Unger, MD Director Chino Medical Group Diabetes and Headache Intervention Center Chino, California January 16, 2008
Evaluation and Treatment of Primary Androgen Deficiency Syndrome in Male Patients Jeff Unger, MD Director Chino Medical Group Diabetes and Headache Intervention Center Chino, California January 16, 2008
[PDF] ALTERNATIVES TO LUPRON FOR PROSTATE CANCER EBOOK
![[PDF] ALTERNATIVES TO LUPRON FOR PROSTATE CANCER EBOOK](/thumbs/82/85358853.jpg "[PDF] ALTERNATIVES TO LUPRON FOR PROSTATE CANCER EBOOK") 06 March, 2018 [PDF] ALTERNATIVES TO LUPRON FOR PROSTATE CANCER EBOOK Document Filetype: PDF 506.4 KB 0 [PDF] ALTERNATIVES TO LUPRON FOR PROSTATE CANCER EBOOK See information on benefits and safety. We
06 March, 2018 [PDF] ALTERNATIVES TO LUPRON FOR PROSTATE CANCER EBOOK Document Filetype: PDF 506.4 KB 0 [PDF] ALTERNATIVES TO LUPRON FOR PROSTATE CANCER EBOOK See information on benefits and safety. We
Marketing Authorisation Holder Applicant Invented name. Route of administration. Content (concentration) Member State. l form
 Member State. l form") ANNEX I LIST OF THE NAMES, PHARMACEUTICAL FORM, STRENGTH OF THE MEDICINAL PRODUCT, ROUTE OF ADMINISTRATION, APPLICANT AND MARKETING AUTHORISATION HOLDER IN THE MEMBER STATES 1 Member State Marketing Authorisation
ANNEX I LIST OF THE NAMES, PHARMACEUTICAL FORM, STRENGTH OF THE MEDICINAL PRODUCT, ROUTE OF ADMINISTRATION, APPLICANT AND MARKETING AUTHORISATION HOLDER IN THE MEMBER STATES 1 Member State Marketing Authorisation
The Royal Marsden. Prostate case study. Presented by Mr Alan Thompson Consultant Urological Surgeon
 Prostate case study Presented by Mr Alan Thompson Consultant Urological Surgeon 2 Part one Initial presentation A 62 year old male solicitor attends your GP surgery. He has rarely seen you over the last
Prostate case study Presented by Mr Alan Thompson Consultant Urological Surgeon 2 Part one Initial presentation A 62 year old male solicitor attends your GP surgery. He has rarely seen you over the last
Endocrine Steroids 2. Signal transduction 3. Prostaglandins
 Endocrine - 2 1. Steroids 2. Signal transduction 3. Prostaglandins Estrogen Menopause (pause in the menes) ["change of life" at about 50] - lack of estrogen. (Some hysterectomy or ovarian cancer surgeries
Endocrine - 2 1. Steroids 2. Signal transduction 3. Prostaglandins Estrogen Menopause (pause in the menes) ["change of life" at about 50] - lack of estrogen. (Some hysterectomy or ovarian cancer surgeries
Outcomes With "Watchful Waiting" in Prostate Cancer in US Now So Good, Active Treatment May Not Be Better
 1 sur 5 19/09/2009 07:02 www.medscape.com From Medscape Medical News Outcomes With "Watchful Waiting" in Prostate Cancer in US Now So Good, Active Treatment May Not Be Better Zosia Chustecka September
1 sur 5 19/09/2009 07:02 www.medscape.com From Medscape Medical News Outcomes With "Watchful Waiting" in Prostate Cancer in US Now So Good, Active Treatment May Not Be Better Zosia Chustecka September
Clinical Policy: Goserelin Acetate (Zoladex) Reference Number: CP.PHAR.171 Effective Date: Last Review Date: Line of Business: Medicaid
 Reference Number: CP.PHAR.171 Effective Date: Last Review Date: Line of Business: Medicaid") Clinical Policy: (Zoladex) Reference Number: CP.PHAR.171 Effective Date: 10.01.16 Last Review Date: 11.17 Line of Business: Medicaid Coding Implications Revision Log See Important Reminder at the end of
Clinical Policy: (Zoladex) Reference Number: CP.PHAR.171 Effective Date: 10.01.16 Last Review Date: 11.17 Line of Business: Medicaid Coding Implications Revision Log See Important Reminder at the end of
What are ENDROCRINE DISRUPTORS?
 What are ENDROCRINE DISRUPTORS? Endocrine disruptors are naturally occurring compounds or man- made substances that may mimic or interfere with the function of hormones in the body. Endocrine disruptors
What are ENDROCRINE DISRUPTORS? Endocrine disruptors are naturally occurring compounds or man- made substances that may mimic or interfere with the function of hormones in the body. Endocrine disruptors
An Idea Whose Time Has Come-Male Health Programs: An Opportunity For Clinical Expansion and Better Health
 An Idea Whose Time Has Come-Male Health Programs: An Opportunity For Clinical Expansion and Better Health KEVIN R. LOUGHLIN MD,MBA Harvard Medical School Boston, MA THE WEAKER SEX-MALES LIFE EXPECTANCY
An Idea Whose Time Has Come-Male Health Programs: An Opportunity For Clinical Expansion and Better Health KEVIN R. LOUGHLIN MD,MBA Harvard Medical School Boston, MA THE WEAKER SEX-MALES LIFE EXPECTANCY
BY PEGGY EASTMAN BETHESDA, MD A multidisciplinary panel of independent experts has concluded in a draft statement that
 Advertisement Wolters Kluwer Health Logo Login Register Subscribe etoc Help Enter Keywords Search Advanced Search Saved Searches HomePrevious IssuesBlogsCollectionsCEPodcastsInfo & Services Home > Blogs
Advertisement Wolters Kluwer Health Logo Login Register Subscribe etoc Help Enter Keywords Search Advanced Search Saved Searches HomePrevious IssuesBlogsCollectionsCEPodcastsInfo & Services Home > Blogs
Community care of Prostate Cancer. Shaun Costello Southern Cancer Network
 Community care of Prostate Cancer Shaun Costello Southern Cancer Network Introduction Why is GP follow up of prostate cancer important 4Years In Waikato Faster Cancer Treatment Reporting against the 3
Community care of Prostate Cancer Shaun Costello Southern Cancer Network Introduction Why is GP follow up of prostate cancer important 4Years In Waikato Faster Cancer Treatment Reporting against the 3
PCa Commentary. Seattle Prostate Institute CONTENTS. Volume 71 September-October 2011
 Volume 71 September-October 2011 PCa Commentary CONTENTS PERMANENT SEED BRACHYTHERAPY FOR HIGH- RISK PROSTATE CANCER: 1 CABOZANTINIB: Startling Responses Reported at June ASCO Meeting in Metastatic Castrate
Volume 71 September-October 2011 PCa Commentary CONTENTS PERMANENT SEED BRACHYTHERAPY FOR HIGH- RISK PROSTATE CANCER: 1 CABOZANTINIB: Startling Responses Reported at June ASCO Meeting in Metastatic Castrate
Guidelines for the Management of Prostate Cancer West Midlands Expert Advisory Group for Urological Cancer
 Guidelines for the Management of Prostate Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Guidelines for the Management of Prostate Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
MAMTA PARIKH, MD, MS CHALLENGING CASE #2: GU CANCER & STATE OF THE ART: CASTRATION RESISTANT PROSTATE CANCER
 MAMTA PARIKH, MD, MS CHALLENGING CASE #2: GU CANCER & STATE OF THE ART: CASTRATION RESISTANT PROSTATE CANCER NO RELEVANT FINANCIAL RELATIONSHIPS IN THE PAST TWELVE MONTHS BY PRESENTER OR SPOUSE/PARTNER.
MAMTA PARIKH, MD, MS CHALLENGING CASE #2: GU CANCER & STATE OF THE ART: CASTRATION RESISTANT PROSTATE CANCER NO RELEVANT FINANCIAL RELATIONSHIPS IN THE PAST TWELVE MONTHS BY PRESENTER OR SPOUSE/PARTNER.
Your Guide to Prostate Cancer
 Your Guide to Prostate Cancer If you face a diagnosis of prostate cancer, what s next? We can help. A prostate cancer diagnosis can be overwhelming. The good news is that while prostate cancer can be serious,
Your Guide to Prostate Cancer If you face a diagnosis of prostate cancer, what s next? We can help. A prostate cancer diagnosis can be overwhelming. The good news is that while prostate cancer can be serious,
Learning Objectives. Peri menopause. Menopause Overview. Recommendation grading categories
 Learning Objectives Identify common symptoms of the menopause transition Understand the risks and benefits of hormone replacement therapy (HRT) Be able to choose an appropriate hormone replacement regimen
Learning Objectives Identify common symptoms of the menopause transition Understand the risks and benefits of hormone replacement therapy (HRT) Be able to choose an appropriate hormone replacement regimen
Testosterone Injection and Implant
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.33 Subject: Testosterone Injection Implant Page: 1 of 10 Last Review Date: December 8, 2017 Testosterone
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.33 Subject: Testosterone Injection Implant Page: 1 of 10 Last Review Date: December 8, 2017 Testosterone
Breast Cancer Awareness
 Breast Cancer Awareness Presented by BHS Call: 800-327-2251 Visit: www.bhsonline.com 2016 BHS. All rights reserved. 1 Important Notice The information provided in this training is intended to raise awareness
Breast Cancer Awareness Presented by BHS Call: 800-327-2251 Visit: www.bhsonline.com 2016 BHS. All rights reserved. 1 Important Notice The information provided in this training is intended to raise awareness
AETNA BETTER HEALTH Prior Authorization guideline for Injectable Osteoporosis Agents
 AETNA BETTER HEALTH Prior Authorization guideline for Injectable Osteoporosis Agents Injectable Osteoporosis Agents Forteo (teriparatide); zoledronic acid Prolia (denosumab)] Authorization guidelines For
AETNA BETTER HEALTH Prior Authorization guideline for Injectable Osteoporosis Agents Injectable Osteoporosis Agents Forteo (teriparatide); zoledronic acid Prolia (denosumab)] Authorization guidelines For
PCa Commentary. Volume 79 May June 2014
 1221 Madison Street, 1 st Floor Seattle, WA 98104 P 206-215-2480 www.seattleprostate.com PCa Commentary Volume 79 May June 2014 CONTENT: Active Surveillance Page 1 Firmagon and Lupron Page 5 ACTIVE SURVEILLANCE:
1221 Madison Street, 1 st Floor Seattle, WA 98104 P 206-215-2480 www.seattleprostate.com PCa Commentary Volume 79 May June 2014 CONTENT: Active Surveillance Page 1 Firmagon and Lupron Page 5 ACTIVE SURVEILLANCE:
Gary Scott Friedlander, M.D. Urological Consultants, P.A. A Division of Chesapeake Urology Associates, LLC
 Gary Scott Friedlander, M.D. Urological Consultants, P.A. A Division of Chesapeake Urology Associates, LLC 9420 Key West Ave, Suite 420, Rockville, MD 20850 2730 University Blvd, West, Suite 516, Wheaton,
Gary Scott Friedlander, M.D. Urological Consultants, P.A. A Division of Chesapeake Urology Associates, LLC 9420 Key West Ave, Suite 420, Rockville, MD 20850 2730 University Blvd, West, Suite 516, Wheaton,
I AM THE ONLY ONE YOU ARE AFRAID TO BELIEVE
 I AM THE ONLY ONE YOU ARE AFRAID TO BELIEVE On Saturday, January 16, 1999, I had the privilege of speaking to the San Diego Chapter of Informed Prostate Cancer Support Group. Well over 200 people attended
I AM THE ONLY ONE YOU ARE AFRAID TO BELIEVE On Saturday, January 16, 1999, I had the privilege of speaking to the San Diego Chapter of Informed Prostate Cancer Support Group. Well over 200 people attended
Summary of Phase 3 IMPACT Trial Results Presented at AUA Meeting Webcast Conference Call April 28, Nasdaq: DNDN
 Summary of Phase 3 IMPACT Trial Results Presented at AUA Meeting Webcast Conference Call April 28, 2009 Nasdaq: DNDN PROVENGE sipuleucel-t is an autologous active cellular immunotherapy that activates
Summary of Phase 3 IMPACT Trial Results Presented at AUA Meeting Webcast Conference Call April 28, 2009 Nasdaq: DNDN PROVENGE sipuleucel-t is an autologous active cellular immunotherapy that activates
Implantable Hormone Pellets
 Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
PREVALENCE OF PROSTATE CANCER AMONG HYPOGONADAL MEN WITH PROSTATE-SPECIFIC ANTIGEN LEVELS OF 4.0 ng/ml OR LESS
 ADULT UROLOGY PREVALENCE OF PROSTATE CANCER AMONG HYPOGONADAL MEN WITH PROSTATE-SPECIFIC ANTIGEN LEVELS OF 4.0 ng/ml OR LESS ABRAHAM MORGENTALER AND ERNANI LUIS RHODEN ABSTRACT Objectives. To determine
ADULT UROLOGY PREVALENCE OF PROSTATE CANCER AMONG HYPOGONADAL MEN WITH PROSTATE-SPECIFIC ANTIGEN LEVELS OF 4.0 ng/ml OR LESS ABRAHAM MORGENTALER AND ERNANI LUIS RHODEN ABSTRACT Objectives. To determine
Current Topics in Hormone Replacement Therapy
 Current Topics in Hormone Replacement Therapy Corey R. Babb, D.O., FACOOG, IF, NCMP Clinical Assistant Professor of Obstetrics and Gynecology Director of the Oklahoma State University Center for Women
Current Topics in Hormone Replacement Therapy Corey R. Babb, D.O., FACOOG, IF, NCMP Clinical Assistant Professor of Obstetrics and Gynecology Director of the Oklahoma State University Center for Women
James H. Liu, M.D. Arthur H. Bill Professor Chair of Reproductive Biology Dept of Obstetrics and Gynecology
 Disclosure Estrogen Therapy After Postmenopausal Hysterectomy: Issues, Challenges, Risks/Benefits James H. Liu, M.D. Arthur H. Bill Professor Chair of Reproductive Biology Dept of Obstetrics and Gynecology
Disclosure Estrogen Therapy After Postmenopausal Hysterectomy: Issues, Challenges, Risks/Benefits James H. Liu, M.D. Arthur H. Bill Professor Chair of Reproductive Biology Dept of Obstetrics and Gynecology
Lung Cancer in Women: A Different Disease? James J. Stark, MD, FACP
 Lung Cancer in Women: A Different Disease? James J. Stark, MD, FACP Medical Director, Cancer Program and Director of Palliative Care Maryview Medical Center Professor of Medicine Eastern Virginia Medical
Lung Cancer in Women: A Different Disease? James J. Stark, MD, FACP Medical Director, Cancer Program and Director of Palliative Care Maryview Medical Center Professor of Medicine Eastern Virginia Medical
PROSTATE CANCER (PCa)
") PROSTATE CANCER (PCa) Tomasz Drewa Department of Urology, Collegium Medicum, UMK ? PCa = 11/6/16 PCa Urology, 1995 11/6/16 PSA increase Natural history of prostate cancer patient Testosterone Deprywacja
PROSTATE CANCER (PCa) Tomasz Drewa Department of Urology, Collegium Medicum, UMK ? PCa = 11/6/16 PCa Urology, 1995 11/6/16 PSA increase Natural history of prostate cancer patient Testosterone Deprywacja
Navigating the Stream: Prostate Cancer and Early Detection. Ifeanyi Ani, M.D. TPMG Urology Newport News
 Navigating the Stream: Prostate Cancer and Early Detection Ifeanyi Ani, M.D. TPMG Urology Newport News Understand epidemiology of prostate cancer Discuss PSA screening and PSA controversy Review tools
Navigating the Stream: Prostate Cancer and Early Detection Ifeanyi Ani, M.D. TPMG Urology Newport News Understand epidemiology of prostate cancer Discuss PSA screening and PSA controversy Review tools
Tobias S. Kohler, MD, MPH, FACS Southern Illinois University School of Medicine AUA SMSNA Program May 7, 2016
 Tobias S. Kohler, MD, MPH, FACS Southern Illinois University School of Medicine AUA SMSNA Program May 7, 2016 Abbvie Researcher/Consultant/Grant Funding Boston Scientific Researcher/Consultant/Grant Funding
Tobias S. Kohler, MD, MPH, FACS Southern Illinois University School of Medicine AUA SMSNA Program May 7, 2016 Abbvie Researcher/Consultant/Grant Funding Boston Scientific Researcher/Consultant/Grant Funding
Policy. not covered Sipuleucel-T. Considerations Sipuleucel-T. Description Sipuleucel-T. be medically. Sipuleucel-T. covered Q2043.
 Cellular Immunotherapy forr Prostate Cancer Policy Number: 8.01.53 Origination: 11/2010 Last Review: 11/2014 Next Review: 11/2015 Policy BCBSKC will provide coverage for cellular immunotherapy for prostate
Cellular Immunotherapy forr Prostate Cancer Policy Number: 8.01.53 Origination: 11/2010 Last Review: 11/2014 Next Review: 11/2015 Policy BCBSKC will provide coverage for cellular immunotherapy for prostate
THE FACTS, DOC, JUST THE FACTS
 November 1997 April 2004 (Revised) THE FACTS, DOC, JUST THE FACTS I have just reviewed a timely article. Here are some quotes and paraphrases from it: Recently, a number of urologists have begun to question
November 1997 April 2004 (Revised) THE FACTS, DOC, JUST THE FACTS I have just reviewed a timely article. Here are some quotes and paraphrases from it: Recently, a number of urologists have begun to question
WEIGHING UP THE RISKS OF HRT. Department of Endocrinology Chris Hani Baragwanath Academic Hospital
 WEIGHING UP THE RISKS OF HRT V. Nicolaou Department of Endocrinology Chris Hani Baragwanath Academic Hospital Background Issues surrounding post menopausal hormonal therapy (PMHT) are complex given: Increased
WEIGHING UP THE RISKS OF HRT V. Nicolaou Department of Endocrinology Chris Hani Baragwanath Academic Hospital Background Issues surrounding post menopausal hormonal therapy (PMHT) are complex given: Increased
Recent Progress in Management of Advanced Prostate Cancer
 Review Article [1] April 15, 2005 By Philip W. Kantoff, MD [2] Androgen-deprivation therapy, usually with combined androgen blockade, is standard initial treatment for advanced prostate cancer. With failure
Review Article [1] April 15, 2005 By Philip W. Kantoff, MD [2] Androgen-deprivation therapy, usually with combined androgen blockade, is standard initial treatment for advanced prostate cancer. With failure
Dr. Patrick Walsh's Guide To Surviving Prostate Cancer Books
 Dr. Patrick Walsh's Guide To Surviving Prostate Cancer Books Each year, more than 230,000 men are diagnosed with prostate cancer, and 30 to 40 percent of patients who are diagnosed will eventually relapse.
Dr. Patrick Walsh's Guide To Surviving Prostate Cancer Books Each year, more than 230,000 men are diagnosed with prostate cancer, and 30 to 40 percent of patients who are diagnosed will eventually relapse.
16:30-18:30 WS #67: Urology Forum - Prostate Cancer, Stones, Renal Tumours, Voiding Dysfunction (120 minutes, not repeated) -
 -") Dr Anna Lawrence Urologist Auckland Dr Andrew Williams Urologist Auckland Madhu Koya Urologist Auckland Andrew Lienert Urologist Auckland Dr Louise Tomlinson Consultant Gynaecologist Auckland 16:30-18:30
Dr Anna Lawrence Urologist Auckland Dr Andrew Williams Urologist Auckland Madhu Koya Urologist Auckland Andrew Lienert Urologist Auckland Dr Louise Tomlinson Consultant Gynaecologist Auckland 16:30-18:30
Edward P. Gelmann, MD
 Prostate Cancer Edward P. Gelmann, MD Prostate Cancer Etiology and Ep pidemiology Screening Pathology Staging Localized Disease Metastatic Disease normal prostate epithelium GSTP1 CpG island hypermethylation
Prostate Cancer Edward P. Gelmann, MD Prostate Cancer Etiology and Ep pidemiology Screening Pathology Staging Localized Disease Metastatic Disease normal prostate epithelium GSTP1 CpG island hypermethylation
ERLEADA (apalutamide) oral tablet
 oral tablet") ERLEADA (apalutamide) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
ERLEADA (apalutamide) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
PCSANM 2015 Seminar. Basic Knowledge: Test for Prostate Cancer. Jerry Cross. 15 item quiz, no grades given
 Basic Knowledge: Test for Prostate Cancer Jerry Cross 15 item quiz, no grades given Basic Knowledge: Test for Prostate Cancer From http://prostatesnatchers.blogspot.com/ January 27, 2015 BY MARK SCHOLZ,
Basic Knowledge: Test for Prostate Cancer Jerry Cross 15 item quiz, no grades given Basic Knowledge: Test for Prostate Cancer From http://prostatesnatchers.blogspot.com/ January 27, 2015 BY MARK SCHOLZ,
Index. urologic.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Acquired hypogonadism, prevalence of, 165 167 primary, 165 secondary, 167 Adipose tissue, as an organ, 240 241 Adrenal hyperplasia, congenital,
Note: Page numbers of article titles are in boldface type. A Acquired hypogonadism, prevalence of, 165 167 primary, 165 secondary, 167 Adipose tissue, as an organ, 240 241 Adrenal hyperplasia, congenital,
GA KS KY LA MD NJ NV NY TN TX WA Applicable X X N/A N/A X N/A X X X X X X N/A N/A NA *FHK- Florida Healthy Kids. Androgens
 Androgens Override(s) Prior Authorization Quantity Limit Approval Duration Varies upon diagnosis Medication Strengths Quantity Limit Comments Generic Androgel 1% (2.5 g) packet 2 packets per day (testosterone
Androgens Override(s) Prior Authorization Quantity Limit Approval Duration Varies upon diagnosis Medication Strengths Quantity Limit Comments Generic Androgel 1% (2.5 g) packet 2 packets per day (testosterone
Advanced Prostate Cancer. November Jose W. Avitia, M.D
 Advanced Prostate Cancer November 4 2017 Jose W. Avitia, M.D In 2017 161,000 new cases of prostate cancer diagnosed in US, mostly with elevated PSA 5-10% will present with metastatic disease In 2017: 26,000
Advanced Prostate Cancer November 4 2017 Jose W. Avitia, M.D In 2017 161,000 new cases of prostate cancer diagnosed in US, mostly with elevated PSA 5-10% will present with metastatic disease In 2017: 26,000
The Centre for Men s Health
 96 Harley Street (London) and Manchester All Enquiries - +44 (0)20 7486 2277 www.centreformenshealth.co.uk/ This leaflet provides information about: The Centre for Men s Health The conditions we treat:
96 Harley Street (London) and Manchester All Enquiries - +44 (0)20 7486 2277 www.centreformenshealth.co.uk/ This leaflet provides information about: The Centre for Men s Health The conditions we treat:
Cancer Cases Treated and Results
 Cancer Cases Treated and Results Below are some of the cases, from more than 30 cases we have treated so far with good results. When reading the PET/CT scans, the picture on the left is before treatment,
Cancer Cases Treated and Results Below are some of the cases, from more than 30 cases we have treated so far with good results. When reading the PET/CT scans, the picture on the left is before treatment,
Date of preparation- January 2018 Janssen Biotech, Inc /18 em Reporter s guide to. prostate cancer
 Date of preparation- January 2018 Janssen Biotech, Inc. 2018 02/18 em-01856 Reporter s guide to prostate cancer What is the prostate? The prostate is a gland located below the bladder, wrapped around the
Date of preparation- January 2018 Janssen Biotech, Inc. 2018 02/18 em-01856 Reporter s guide to prostate cancer What is the prostate? The prostate is a gland located below the bladder, wrapped around the