The Calcium Conundrum: When, What and How to Give Calcium in Pediatric CKD/ESRD
|
|
|
- Dwain Gardner
- 5 years ago
- Views:
Transcription


1 The Calcium Conundrum: When, What and How to Give Calcium in Pediatric CKD/ESRD Jess Tower MS RD LD 3/18/19 Children s Mercy Hospital jdtower@cmh.edu Disclosures Nothing to disclose 1

2 How do bones work? How much calcium is optimal in children without CKD? Why? The Calcium Conundrum: How does CKD affect calcium homeostasis? Are the calcium needs of children with short stature lower? Why do children with CKD develop hypocalcemia? What does hypocalcemia look like and why is it bad? Should we supplement over the RDA in children with hypocalcemia? If so, how much more? How much calcium is optimal in children with CKD? Why do children with CKD develop hypercalcemia? The Calcium Conundrum: What does hypercalcemia look like and why is it bad? Should we supplement to RDA in children with hypercalcemia? When should we intervene? What is the best way to correct calcium? What affects calcium balance and lab interpretation? How do we increase calcium intake when dairy products are limited? Bone Anatomy of bone Functions of skeleton Modeling vs. remodeling Bone mineralization Bone strength 2


3 Bone Anatomy of bone Functions of skeleton Modeling vs. remodeling Bone mineralization Bone strength Longitudinal growth Radial growth Bone Anatomy of bone Functions of skeleton Modeling vs. remodeling Bone mineralization Bone strength Bone Anatomy of bone Functions of skeleton Modeling vs. remodeling Bone mineralization Bone strength 3


4 Bone Anatomy of bone Functions of skeleton Modeling vs. remodeling Bone mineralization Bone strength Bone Anatomy of bone Functions of skeleton Modeling vs. remodeling Bone mineralization Bone strength Calcium Biochemical functions Absorption & factors regulating calcium level Calcium balance & excretion Calcium regulation Effect of CKD on calcium homeostasis 4
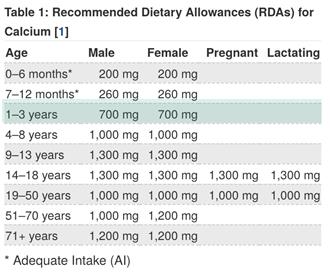
5 Infants 0 6 months: AI Based on mean intake data from infants fed human milk as the principal fluid and on studies that have determined mean calcium content of breast milk Infants 7 12 months: AI Based on mean calcium intake from solid foods and human milk Infants 0 6 months: AI Based on mean intake data from infants fed human milk and on studies that have determined mean calcium content of breast milk Infants 7 12 months: Based on mean calcium intake from solid foods and human milk Infants 0 6 months: Based on mean intake data from infants fed human milk as the principal fluid and on the studies that have determined mean calcium content of breast milk Infants 7 12 months: AI Based on mean calcium intake from solid foods and human milk 5
6 6

7 HealthProfessional/ 7
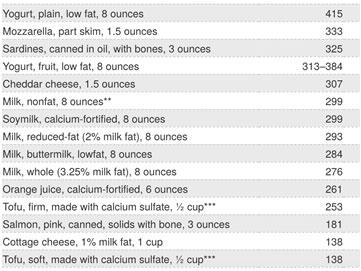
8 Without dairy HealthProfessional/ Without high potassium foods (>300 mg per serving) HealthProfessional/ Without high sodium foods (>140 mg per serving) HealthProfessional/ 8
 SMCL NA Year Sampled 2017 https://www.fda.")


9 Calcium additives in food Calcium carbonate Calcium chloride Calcium disodium EDTA Calcium sulfate Monocalcium phosphate There are 86 Tap water Parameter Calcium KCMO Average 37.4 KCMO Range Units ppm (mg/l) SMCL NA Year Sampled content/uploads/2013/04/2018 Water Quality Report rev.pdf Biochemical functions Hi, we don t even contain 1% of the body s total calcium but it does all of this: muscle contraction, blood clotting, transmission of neural impulses, enzyme activation, intracellular messaging, and more! Hi, I contain 99% of the body s total calcium! Absorption & factors regulating calcium level Active transport + vitamin D Increases with low calcium intake Passive transport Most active at Ca intake >2 gm/d 9


10 Absorption & factors regulating calcium level Inhibits Ca absorption Gut contents that bind Ca Oxalate Phytate Phosphate Free fatty acids Less acidic gastric environment Steroids Magnesium deficiency Promotes Ca absorption Low calcium intake Hormones Vitamin D PTH Calcium balance & excretion Neutral & sweat & feces Total calcium intake = total body calcium losses Negative balance Positive balance Increased risk for osteoporosis and fracture Older adults, especially post menopausal women Increased risk for extraskeletal calcification and cardiovascular events Growing children Calcium balance & excretion Neutral & sweat & feces Total calcium intake < total body calcium losses Negative balance Positive balance Increased risk for osteoporosis and fracture Older adults, especially post menopausal women Increased risk for extraskeletal calcification and cardiovascular events Growing children 10

11 Calcium balance & excretion Neutral & sweat & feces Total calcium intake > total body calcium losses Negative balance Positive balance Increased risk for osteoporosis and fracture Older adults, especially post menopausal women Increased risk for extraskeletal calcification and cardiovascular events Growing children Calcium metabolism & regulation 7 calcium homeostasis interactions of the skeletal system and other organ systems/ Urinary elimination pathway is severely impaired or absent Effect of CKD on calcium homeostasis Calcium intake is limited as a result of phosphate restriction and decreased appetite Calcitriol production is reduced, leading to reduced calcium absorption Medical management of CKD MBD affects serum calcium levels 11




12 Recommended calcium intake in CKD KDOQI: 2008 KDIGO: 2017 What affects interpretation of serum calcium? Albumin Vitamin A Vitamin D Alkaline phosphatase Parathyroid hormone 12


13 Parathyroid hormone Why do kids w/ CKD develop hypocalcemia? Causes Signs/symptoms Long term consequences Intervention Phosphate restriction Hyperphosphatemia Hypovitaminosis D Hypomagnesemia Kayexalate administration Parathyroidectomy Cinacalcet overdose Poor absorption (PPI) Up To Date Low calcium, low ionized calcium Acute: neuromuscular irritability (tetany), cardiovascular symptoms, papilledema, psychiatric Chronic: ectopic calcification, extrapyramidal signs, Parkinsonism, dementia, cataracts, abnormal dentition, dry skin Kidney damage Growth failure Musculoskeletal deformity Soft tissue and vascular calcification Osteitis fibrosa cystica Increase calcium intake Decrease phosphorus intake or add binder Start or increase calcium supplement Start or increase vitamin D supplement or active vitamin D Treat magnesium deficiency Increase dialysate calcium What does hypocalcemia look like? Causes Signs/symptoms Long term consequences Intervention Phosphate restriction Hyperphosphatemia Hypovitaminosis D Hypomagnesemia Kayexalate administration Parathyroidectomy Cinacalcet overdose Poor absorption (PPI) Up To Date Low calcium, low ionized calcium Acute: neuromuscular irritability, cardiovascular symptoms, papilledema, psychiatric manifestations Chronic: ectopic calcification, extrapyramidal signs, dementia, cataracts, abnormal dentition, dry skin Kidney damage Growth failure Musculoskeletal deformity Soft tissue and vascular calcification Osteitis fibrosa cystica Trousseau s sign Increase calcium intake Decrease phosphorus intake or add binder Start or increase calcium supplement Start or increase vitamin D supplement or active vitamin Chvostek s D sign Treat magnesium deficiency Increase dialysate calcium 13
14 What happens if hypocalcemia is not treated? Causes Signs/symptoms Long term consequences Intervention Phosphate restriction Hyperphosphatemia Hypovitaminosis D Hypomagnesemia Kayexalate administration Parathyroidectomy Cinacalcet overdose Poor absorption (PPI) Up To Date Low calcium, low ionized calcium Acute: neuromuscular irritability, cardiovascular symptoms, papilledema, psychiatric manifestations Chronic: ectopic calcification, extrapyramidal signs, dementia, cataracts, abnormal dentition, dry skin Kidney damage Growth failure Musculoskeletal deformity Soft tissue and vascular calcification Osteitis fibrosa (high turnover bone disease) Increase calcium intake Decrease phosphorus intake or add binder Start or increase calcium supplement Start or increase vitamin D supplement or active vitamin D Treat magnesium deficiency Increase dialysate calcium How do you fix hypocalcemia? Causes Signs/symptoms Long term consequences Interventions Phosphate restriction Hyperphosphatemia Hypovitaminosis D Hypomagnesemia Kayexalate administration Parathyroidectomy Cinacalcet overdose Poor absorption (PPI) Up To Date Low calcium, low ionized calcium Acute: neuromuscular irritability, cardiovascular symptoms, papilledema, psychiatric manifestations Chronic: ectopic calcification, extrapyramidal signs, dementia, cataracts, abnormal dentition, dry skin Kidney damage Growth failure Musculoskeletal deformity Soft tissue and vascular calcification Osteitis fibrosa (high turnover bone disease) Increase calcium intake Decrease phosphorus intake or add binder Start or increase calcium supplement Start or increase vitamin D supplement or active vitamin D Treat magnesium deficiency Increase dialysate calcium Calcium supplements Consider: Type Cost Timing Availability Administration method Pill burden Vitamin D status 14
15 Vitamin D supplementation Serum 25(OH) D Supplementation with cholecalciferol OR ergocalciferol >30 ng/ml Maintenance dose between IU daily 16 to 30 ng/ml 2000 IU daily x 3 months 50,000 IU monthly x 3 months 5 to 15 ng/ml 4000 IU daily x 3 months 50,000 IU every other week x 3 months <5 ng/ml 8000 IU daily x 1 month, then 4000 IU daily x 2 months 50,000 IU weekly x 1 month, then 50,000 IU every other week for 2 months ESPN CKD MBD guidelines recommend a treatment schedule guided by age and vitamin D level which includes an intensive replacement phase followed by a maintenance phase for vitamin D supplementation in children with CKD stage 2 to 5D Monitor serum 25(OH) D 3 months after completion of therapy Up To Date/KDOQI Vitamin D analogues Calcitriol Paricalcitol Why do kids w/ CKD develop hypercalcemia? Causes Signs/symptoms Long term consequences Interventions Excessive calcium intake Loss of renal function Hypervitaminosis D Hypervitaminosis A Severe SHPT Metabolic acidosis High serum calcium, elevated urinary calcium/creatinine ratio Severity, chronicity Common: polyuria, polydipsia, dehydration, constipation, anorexia, nausea, muscle weakness, lethargy, confusion, coma Kidney stones Kidney damage Growth failure Musculoskeletal deformity Soft tissue and vascular calcification Adynamic bone disease Reduce calcium load Reduce Ca based binder or change to/add non Cabased binder Decrease or discontinue vitamin D supplement and/or vitamin D analogue Decrease dialysate calcium Supplement phosphorus? 15
16 What does hypercalcemia look like? Causes Signs/symptoms Long term consequences Interventions Excessive calcium intake Loss of renal function Hypervitaminosis D Hypervitaminosis A Severe SHPT Metabolic acidosis High serum calcium, elevated urinary calcium/creatinine ratio Severity, chronicity Common: polyuria, polydipsia, dehydration, constipation, anorexia, nausea, muscle weakness, lethargy, confusion, coma Kidney stones Kidney damage Growth failure Musculoskeletal deformity Soft tissue and vascular calcification Adynamic bone disease Reduce calcium load Reduce Ca based binder or change to/add non Cabased binder Decrease or discontinue vitamin D supplement and/or vitamin D analogue Decrease dialysate calcium Supplement phosphorus? What happens if hypercalcemia is not treated? Causes Signs/symptoms Long term consequences Interventions Excessive calcium intake Loss of renal function Hypervitaminosis D Hypervitaminosis A Severe SHPT Metabolic acidosis High serum calcium, elevated urinary calcium/creatinine ratio Severity, chronicity Common: polyuria, polydipsia, dehydration, constipation, anorexia, nausea, muscle weakness, lethargy, confusion, coma Kidney stones Kidney damage Growth failure Musculoskeletal deformity Soft tissue and vascular calcification Adynamic bone (lowturnover bone disease) Reduce calcium load Reduce Ca based binder or change to/add non Cabased binder Decrease or discontinue vitamin D supplement and/or vitamin D analogue Decrease dialysate calcium Supplement phosphorus? How do you fix hypercalcemia? Causes Signs/symptoms Long term consequences Interventions Excessive calcium intake Loss of renal function Hypervitaminosis D Hypervitaminosis A Severe SHPT Metabolic acidosis High serum calcium, elevated urinary calcium/creatinine ratio Severity, chronicity Common: polyuria, polydipsia, dehydration, constipation, anorexia, nausea, muscle weakness, lethargy, confusion, coma Kidney stones Kidney damage Growth failure Musculoskeletal deformity Soft tissue and vascular calcification Adynamic bone (lowturnover bone disease) Reduce calcium load Change to a non calciumbased binder Decrease or discontinue vitamin D supplement and/or vitamin D analogue Decrease dialysate calcium Supplement phosphorus? Up To Date 16

17 Age 6+ since 2016 Investigate cause of hypercalcemia Consider changing dialysate Ca concentration Corrected serum Ca (mg/dl) Review changes in dialysate Ca concentration Ca carbonate Ca free P binder Ac ve vitamin D Ca free P binder Ca carbonate Ac ve vitamin D Ca free P binder Ca carbonate between meals Ac ve vitamin D Cinacalcet ** Ca carbonate Switch to Ca free P binder Ac ve vitamin D Cinacalcet * Target Ca and P levels Ca carbonate Ca carbonate between meals Ac ve vitamin D Cinacalcet ** Ca carbonate Ca free P binder Ac ve vitamin D Cinacalcet * Ca free P binder Ca carbonate Ac ve vitamin D Cinacalcet * Ca carbonate Ca free P binder Cinacalcet ** Evaluation of food consumption and nutrition Serum P level (mg/dl) Ensure adequate dialysis dose Dietary guidance (restricted P) When do you start doing something? Stage 2 Stage 3b Stage 5 Kuro o M and Moe OW. FGF23 aklotho as a paradigm for a kidney bone network. Bone. 2017; 100:



 Disturbed mineralization and/or bone")

18 Why do we care? Abnormal labs CKD MBD Vascular & soft tissue calcification Abnormal bone Why do we care? Evaluation of CKD MBD used to be limited to evaluation of rates of bone turnover Bone biopsy required to assess all 3 aspects in the TMV classification system Turnover: alteration in rate of bone resorption and formation Mineralization: alteration in volume of unmineralized bone and mineralization rate Volume: alteration in amount of bone mass (AKA osteoporosis, usually seen in adults) Disturbed mineralization and/or bone volume can occur in the setting of normal bone turnover Ca PTH Ca PTH Sources: Bakkaloglu 2010 Why do we care? Growth failure, bone deformity CKD Biochemical changes Bone changes Soft tissue calcification Heart disease 18
19 Amount and safety of calcium supplementation s/p parathyroidectomy The Calcium Conundrum Continues: The relationship between magnesium and calcium Calculating vitamin A intake for accurate assessment How much calcium does a 6 to 12 month old actually eat? Take Home Points Follow trends Interpret labs in context Consider all factors that contribute to calcium load Would follow KDIGO: keep in normal range Remember: A bone biopsy needed to diagnose osteodystrophy CKD MBD is linked to heart disease Positive calcium balance is not good if you are not growing nope 19
 Committee to Review Dietary Reference Intakes for Vitamin D and Calcium; Ross AC, Taylor CL, Yaktine AL, et al., editors.")
20 Thank you. Questions? Jess Tower References Dietary Reference Intakes for Calcium and Vitamin D. Institute of Medicine (US) Committee to Review Dietary Reference Intakes for Vitamin D and Calcium; Ross AC, Taylor CL, Yaktine AL, et al., editors. Washington (DC): National Academies Press (US); Clarke B. Normal bone anatomy and physiology. Clin J Am Soc Nephrol (suppl 3): S131 S /10/18. Case Study from ListServ Pt history: 7 month old male CGA 6 months on PD (adding another cycle) with formula providing 126 kcal/kg through GT, no PO Questions asked: GA: 34 6/7 weeks Underlying disease state? MCDK K+ trends? Hemolyzed samples, low to normal overall ( mmol/l) Growth trend? Poor, 5 gm/day (goal 12 gm/day) Vitamin D level? Lipid levels? 20
21 Case Study from ListServ Pt history: 7 month old male CGA 6 months on PD (adding another cycle) with formula providing 126 kcal/kg through GT, no PO Current diet: 24 kcal/oz Similac PM 60/ kcal/oz Liquigen to 32 kcal/oz 110 ml 5 times daily 120 ml 5 times daily Current labs: Calcium Ionized calcium 5.1 Phosphorus PTH Alkaline phosphatase (OH) vitamin D 48 a few months ago Current medications: Calcitriol increasing from 0.4 mcg to 0.6 mcg/day 550 ml Energy Protein Phosphorus K+ Ca Vitamin A Vitamin D Case Study from ListServ The team would like to switch to 100% Calcilo XD with Liquigen for the high calcium. 100% Similac 60/40 100% Calcilo XD RDA 6 months Phosphorus mg/day 180 mg/day 100 mg/day Calcium mg/day 17 mg/day 200 mg/day K mg/day mg/day 400 mg/day Would you do a combination of Similac PM 60/40 or Renastart to provide less phosphorus, a bit more calcium and some vitamin D? Case Study from ListServ Created a recipe with Calcilo XD + Renastart + Liquigen to 32 kcal/oz to reduce the amount of calcium and phosphorus in formula. Energy Protein Phosphorus K+ Ca Vitamin A Vitamin D Renastart Calcilo XD Liquigen 216 Totals: 647 kcal 8 gm 92 mg 204 mg 61 mg 228 mcg 106 IU Needs: 106% 89% 92% 51% 31% 57% 27% % reduction
22 Case Study from ListServ: Responses Increase phosphorus intake Pre treat formula with Kayexalate to address increased K+ provision Trial low calcium PD fluid Consider different formula compositions if family capable kcal Similac PM 60/40 + Calcilo XD with Liquigen PRN kcal Similac PM 60/40 + Renastart with Liquigen PRN kcal Caliclo XD + Liquigen short term, then switch Is calcitriol contributing to calcium absorption? Consider paricalcitol. Check vitamin A level Martin KJ Gonzalez EA Metabolic bone disease in CKD JASN (3) /10/18 Effect of CKD 1 5D on calcium homeostasis Stage 2 Stage 3b Stage 5 Reduced calcitriol production Poor calcium & phosphate filtration Reduced calcium & phosphate excretion Limited diet Kuro o M and Moe OW. FGF23 aklotho as a paradigm for a kidney bone network. Bone. 2017; 100:
 Calcinosis Nephrolithiasis Calcium or milk alkali syndrome (>3000 mg) Earlier: Result of early treatment for gastric or duodenal ulcers w/")

23 Tolerable Upper Limits Toxicity Hypercalcemia Hypercalciuria (>0.3 mg calcium/mg creatinine) Calcinosis Nephrolithiasis Calcium or milk alkali syndrome (>3000 mg) Earlier: Result of early treatment for gastric or duodenal ulcers w/ hypercalcemia, severe alkalosis, and hyperphosphatemia Modern: Result of calcium carbonate supplementation w/ hypophosphatemia How do you achieve target serum calcium? Goal: increase serum calcium Increase oral intake of calcium Calcium supplementation Calcium containing binders Start vitamin D Reduce dialysate calcium Goal: decrease serum calcium Decrease oral intake of calcium Discontinue supplementation Select alternative binders Adjust vitamin D Increase dialysate calcium 23
 Dialysis FFQ (Kalantar Zadeh K) Most successful education strategies Available teaching materials Nutrients are")
24 How do you actually achieve target serum calcium? Accurate assessment of baseline calcium intake NIH short calcium FFQ (Sebring NG) Dialysis FFQ (Kalantar Zadeh K) Most successful education strategies Available teaching materials Nutrients are listed in their elemental form Roll out: 1/1/20 for >$10 million in sales 1/1/21 for <$10 million in sales Calcium balance & excretion in CKD Neutral Total calcium intake total body calcium losses = calcium balance Negative balance Loss of bone mineral Risk for mineralization defect Risk for bone fragility fractures Morbidity and mortality Positive balance Soft tissue calcification Cardiovascular events Morbidity and mortality 24
Secondary Hyperparathyroidism: Where are we now?
 Secondary Hyperparathyroidism: Where are we now? Dylan M. Barth, Pharm.D. PGY-1 Pharmacy Resident Mayo Clinic 2017 MFMER slide-1 Objectives Identify risk factors for the development of complications caused
Secondary Hyperparathyroidism: Where are we now? Dylan M. Barth, Pharm.D. PGY-1 Pharmacy Resident Mayo Clinic 2017 MFMER slide-1 Objectives Identify risk factors for the development of complications caused
Incorporating K/DOQI Using a Novel Algorithm Approach: Regina Qu Appelle s Experience
 Incorporating K/DOQI Using a Novel Algorithm Approach: Regina Qu Appelle s Experience Michael Chan, Renal Dietitian Regina Qu Appelle Health Region BC Nephrology Days There is a strong association among
Incorporating K/DOQI Using a Novel Algorithm Approach: Regina Qu Appelle s Experience Michael Chan, Renal Dietitian Regina Qu Appelle Health Region BC Nephrology Days There is a strong association among
Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital
 Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 13, 2017 Disclosures statement: Consultant: Allena, Becker
Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 13, 2017 Disclosures statement: Consultant: Allena, Becker
Approach to a patient with hypercalcemia
 Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
CKD: Bone Mineral Metabolism. Peter Birks, Nephrology Fellow
 CKD: Bone Mineral Metabolism Peter Birks, Nephrology Fellow CKD - KDIGO Definition and Classification of CKD CKD: abnormalities of kidney structure/function for > 3 months with health implications 1 marker
CKD: Bone Mineral Metabolism Peter Birks, Nephrology Fellow CKD - KDIGO Definition and Classification of CKD CKD: abnormalities of kidney structure/function for > 3 months with health implications 1 marker
Persistent post transplant hyperparathyroidism. Shiva Seyrafian IUMS-97/10/18-8/1/2019
 Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
Ramzi Vareldzis, MD Avanelle Jack, MD Dept of Internal Medicine Section of Nephrology and Hypertension LSU Health New Orleans September 13, 2016
 Ramzi Vareldzis, MD Avanelle Jack, MD Dept of Internal Medicine Section of Nephrology and Hypertension LSU Health New Orleans September 13, 2016 1 MBD + CKD in Elderly patients Our focus for today: CKD
Ramzi Vareldzis, MD Avanelle Jack, MD Dept of Internal Medicine Section of Nephrology and Hypertension LSU Health New Orleans September 13, 2016 1 MBD + CKD in Elderly patients Our focus for today: CKD
chapter 1 & 2009 KDIGO
 http://www.kidney-international.org chapter 1 & 2009 DIGO Chapter 1: Introduction and definition of CD MBD and the development of the guideline statements idney International (2009) 76 (Suppl 113), S3
http://www.kidney-international.org chapter 1 & 2009 DIGO Chapter 1: Introduction and definition of CD MBD and the development of the guideline statements idney International (2009) 76 (Suppl 113), S3
Investigations for Disorders of Calcium, Phosphate and Magnesium Homeostasis
 Investigations for Disorders of Calcium, Phosphate and Magnesium Homeostasis Tutorial for Specialist Portfolio Biomedical Scientists 03/02/2014 Dr Petros Kampanis Clinical Scientist 1. Calcium Most abundant
Investigations for Disorders of Calcium, Phosphate and Magnesium Homeostasis Tutorial for Specialist Portfolio Biomedical Scientists 03/02/2014 Dr Petros Kampanis Clinical Scientist 1. Calcium Most abundant
HYPERCALCEMIA. Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences
 HYPERCALCEMIA Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ESSENTIALS OF DIAGNOSIS Serum calcium level > 10.5 mg/dl Serum ionized
HYPERCALCEMIA Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ESSENTIALS OF DIAGNOSIS Serum calcium level > 10.5 mg/dl Serum ionized
Metabolic Bone Disease Related to Chronic Kidney Disease
 Metabolic Bone Disease Related to Chronic Kidney Disease Deborah Sellmeyer, MD Director, Johns Hopkins Metabolic Bone Center Dept of Medicine, Division of Endocrinology Disclosure DSMB member for denosumab
Metabolic Bone Disease Related to Chronic Kidney Disease Deborah Sellmeyer, MD Director, Johns Hopkins Metabolic Bone Center Dept of Medicine, Division of Endocrinology Disclosure DSMB member for denosumab
Hypocalcemia 6/8/12. Normal value. Physiologic functions. Nephron a functional unit of kidney. Influencing factors in Calcium and Phosphate Balance
 Normal value Hypocalcemia Serum calcium Total mg/dl Ionized mg/dl Cord blood 9.0 ~ 11.5 5.0 ~ 6.o New born (1 st 24 hrs) 9.0 ~ 10.6 4.3 ~ 5.1 24~ 48 hrs 7.0 ~12.0 4.0 ~4.7 Child 8.8 ~10.8 4.8 ~4.92 There
Normal value Hypocalcemia Serum calcium Total mg/dl Ionized mg/dl Cord blood 9.0 ~ 11.5 5.0 ~ 6.o New born (1 st 24 hrs) 9.0 ~ 10.6 4.3 ~ 5.1 24~ 48 hrs 7.0 ~12.0 4.0 ~4.7 Child 8.8 ~10.8 4.8 ~4.92 There
Cinacalcet treatment in advanced CKD - is it justified?
 Cinacalcet treatment in advanced CKD - is it justified? Goce Spasovski ERBP Advisory Board member University of Skopje, R. Macedonia TSN Congress October 21, 2017, Antalya Session Objectives From ROD to
Cinacalcet treatment in advanced CKD - is it justified? Goce Spasovski ERBP Advisory Board member University of Skopje, R. Macedonia TSN Congress October 21, 2017, Antalya Session Objectives From ROD to
Contemporary Nutrition 6 th. th ed. Chapter 9 Minerals
 Contemporary Nutrition 6 th th ed. Chapter 9 Minerals Minerals Various functions in the body Major Minerals Require >100 mg /day Calcium, phosphorus Trace Minerals Require < 100 mg/day Iron, zinc Bioavailability
Contemporary Nutrition 6 th th ed. Chapter 9 Minerals Minerals Various functions in the body Major Minerals Require >100 mg /day Calcium, phosphorus Trace Minerals Require < 100 mg/day Iron, zinc Bioavailability
Therapeutic golas in the treatment of CKD-MBD
 Therapeutic golas in the treatment of CKD-MBD Hemodialysis clinic Clinical University Center Sarajevo Bantao, 04-08.10.2017, Sarajevo Abbvie Satellite symposium 06.10.2017 Chronic Kidney Disease Mineral
Therapeutic golas in the treatment of CKD-MBD Hemodialysis clinic Clinical University Center Sarajevo Bantao, 04-08.10.2017, Sarajevo Abbvie Satellite symposium 06.10.2017 Chronic Kidney Disease Mineral
New biological targets for CKD- MBD: From the KDOQI to the
 New biological targets for CKD- MBD: From the KDOQI to the KDIGO Guillaume JEAN, MD. Centre de Rein Artificiel, 42 avenue du 8 mai 1945, Tassin la Demi-Lune, France. E-mail : guillaume-jean-crat@wanadoo.fr
New biological targets for CKD- MBD: From the KDOQI to the KDIGO Guillaume JEAN, MD. Centre de Rein Artificiel, 42 avenue du 8 mai 1945, Tassin la Demi-Lune, France. E-mail : guillaume-jean-crat@wanadoo.fr
5/18/2017. Specific Electrolytes. Sodium. Sodium. Sodium. Sodium. Sodium
 Specific Electrolytes Hyponatremia Hypervolemic Replacing water (not electrolytes) after perspiration Freshwater near-drowning Syndrome of Inappropriate ADH Secretion (SIADH) Hypovolemic GI disease (decreased
Specific Electrolytes Hyponatremia Hypervolemic Replacing water (not electrolytes) after perspiration Freshwater near-drowning Syndrome of Inappropriate ADH Secretion (SIADH) Hypovolemic GI disease (decreased
Bone Disorders in CKD
 Osteoporosis in Dialysis Patients Challenges in Management David M. Klachko MD FACP Professor Emeritus of Medicine University of Missouri-Columbia Bone Disorders in CKD PTH-mediated high-turnover (osteitis
Osteoporosis in Dialysis Patients Challenges in Management David M. Klachko MD FACP Professor Emeritus of Medicine University of Missouri-Columbia Bone Disorders in CKD PTH-mediated high-turnover (osteitis
CKD-MBD CKD mineral bone disorder
 CKD Renal bone disease Dr Mike Stone University Hospital Llandough Affects 5 10 % of population Increasingly common Ageing, diabetes, undetected hypertension Associated with: Cardiovascular disease Premature
CKD Renal bone disease Dr Mike Stone University Hospital Llandough Affects 5 10 % of population Increasingly common Ageing, diabetes, undetected hypertension Associated with: Cardiovascular disease Premature
GLOSSARY OF TERMS. produced in response to an antigen to bond with and neutralize that antigen / the body's way of destroying foreign invaders
 TERM 24-hour urine acidosis acquired aemia (prefix) albumin alkalosis anemia antibodies antigen autocrine autoimmune basal ganglion bone turnover calcilytic calcimimetic calcitonin Calcitriol Calcium carbonate
TERM 24-hour urine acidosis acquired aemia (prefix) albumin alkalosis anemia antibodies antigen autocrine autoimmune basal ganglion bone turnover calcilytic calcimimetic calcitonin Calcitriol Calcium carbonate
The Skeletal Response to Aging: There s No Bones About It!
 The Skeletal Response to Aging: There s No Bones About It! April 7, 2001 Joseph E. Zerwekh, Ph.D. Interrelationship of Intestinal, Skeletal, and Renal Systems to the Overall Maintenance of Normal Calcium
The Skeletal Response to Aging: There s No Bones About It! April 7, 2001 Joseph E. Zerwekh, Ph.D. Interrelationship of Intestinal, Skeletal, and Renal Systems to the Overall Maintenance of Normal Calcium
Calcium Nephrolithiasis and Bone Health. Noah S. Schenkman, MD
 Calcium Nephrolithiasis and Bone Health Noah S. Schenkman, MD Associate Professor of Urology and Residency Program Director, University of Virginia Health System; Charlottesville, Virginia Objectives:
Calcium Nephrolithiasis and Bone Health Noah S. Schenkman, MD Associate Professor of Urology and Residency Program Director, University of Virginia Health System; Charlottesville, Virginia Objectives:
Ca, Phos and Vitamin D Metabolism in Pre-Dialysis Patients
 Ca, Phos and Vitamin D Metabolism in Pre-Dialysis Patients A. WADGYMAR, MD Credit Valley Hospital, Mississauga, Ontario, Canada. June 1, 2007 1 Case: 22 y/o referred to Renal Clinic Case: A.M. 29 y/o Man
Ca, Phos and Vitamin D Metabolism in Pre-Dialysis Patients A. WADGYMAR, MD Credit Valley Hospital, Mississauga, Ontario, Canada. June 1, 2007 1 Case: 22 y/o referred to Renal Clinic Case: A.M. 29 y/o Man
Metabolic Bone Disease (Past, Present and Future Challenges in the Management)
") Metabolic Bone Disease 871 151 Metabolic Bone Disease (Past, Present and Future Challenges in the Management) SNA RIZVI INTRODUCTION The past 40 years have seen some important historical events leading
Metabolic Bone Disease 871 151 Metabolic Bone Disease (Past, Present and Future Challenges in the Management) SNA RIZVI INTRODUCTION The past 40 years have seen some important historical events leading
CKD-Mineral Bone Disorder (MBD) Pathogenesis of Metabolic Bone Disease. Grants: NIH, Abbott, Amgen, OPKO, Shire
 Pathogenesis of Metabolic Bone Disease. Grants: NIH, Abbott, Amgen, OPKO, Shire") Pathogenesis of Metabolic Bone Disease Stuart M. Sprague, D.O. Chief, Division of Nephrology and Hypertension Professor of Medicine NorthShore University HealthSystem University of Chicago Pritzker School
Pathogenesis of Metabolic Bone Disease Stuart M. Sprague, D.O. Chief, Division of Nephrology and Hypertension Professor of Medicine NorthShore University HealthSystem University of Chicago Pritzker School
Magnesium Homeostasis
 ECTS PhD Training Course, Rome 3 rd September 2008 Disorders of Calcium, Phosphate h and Magnesium Homeostasis Richard Eastell Professor of Bone Metabolism Academic Unit of Bone Metabolism University of
ECTS PhD Training Course, Rome 3 rd September 2008 Disorders of Calcium, Phosphate h and Magnesium Homeostasis Richard Eastell Professor of Bone Metabolism Academic Unit of Bone Metabolism University of
Ca, Mg metabolism, bone diseases. Tamás Kőszegi Pécs University, Department of Laboratory Medicine Pécs, Hungary
 Ca, Mg metabolism, bone diseases Tamás Kőszegi Pécs University, Department of Laboratory Medicine Pécs, Hungary Calcium homeostasis Ca 1000g in adults 99% in bones (extracellular with Mg, P) Plasma/intracellular
Ca, Mg metabolism, bone diseases Tamás Kőszegi Pécs University, Department of Laboratory Medicine Pécs, Hungary Calcium homeostasis Ca 1000g in adults 99% in bones (extracellular with Mg, P) Plasma/intracellular
2.0 Synopsis. Paricalcitol Capsules M Clinical Study Report R&D/15/0380. (For National Authority Use Only)
") 2.0 Synopsis AbbVie Inc. Name of Study Drug: ABT-358/Zemplar (paricalcitol) Capsules Name of Active Ingredient: paricalcitol Individual Study Table Referring to Part of Dossier: Volume: Page: (For National
2.0 Synopsis AbbVie Inc. Name of Study Drug: ABT-358/Zemplar (paricalcitol) Capsules Name of Active Ingredient: paricalcitol Individual Study Table Referring to Part of Dossier: Volume: Page: (For National
2017 KDIGO Guidelines Update
 2017 KDIGO Guidelines Update Clinic for Hemodialysis Clinical Center University of Sarajevo 13 th Congress of the Balkan cities Association of Nephrology, Dialysis, and Artificial Organs Transplantation
2017 KDIGO Guidelines Update Clinic for Hemodialysis Clinical Center University of Sarajevo 13 th Congress of the Balkan cities Association of Nephrology, Dialysis, and Artificial Organs Transplantation
Malnutrition and Role of Nutrition in BMD:CKD
 Malnutrition and Role of Nutrition in BMD:CKD PNDS Continuing Nutrition Education Seminar Saturday, 30 th November 2013 Fayza Khan MSC (Foods and Nutrition) R.D President,PNDS Outline Objective Malnutrition
Malnutrition and Role of Nutrition in BMD:CKD PNDS Continuing Nutrition Education Seminar Saturday, 30 th November 2013 Fayza Khan MSC (Foods and Nutrition) R.D President,PNDS Outline Objective Malnutrition
Hypercalcemia. Hypercalcemia: When to Worry, When to Treat! Mineral Metabolism : A Short Course
 Hypercalcemia: When to Worry, When to Treat! Michael A. Levine has no financial relationships to disclose or Conflicts of Interest to resolve. Michael A. Levine, M.D. This presentation will not involve
Hypercalcemia: When to Worry, When to Treat! Michael A. Levine has no financial relationships to disclose or Conflicts of Interest to resolve. Michael A. Levine, M.D. This presentation will not involve
Calcium metabolism and the Parathyroid Glands. Calcium, osteoclasts and osteoblasts-essential to understand the function of parathyroid glands
 Calcium metabolism and the Parathyroid Glands Calcium, osteoclasts and osteoblasts-essential to understand the function of parathyroid glands Calcium is an essential element for contraction of voluntary/smooth
Calcium metabolism and the Parathyroid Glands Calcium, osteoclasts and osteoblasts-essential to understand the function of parathyroid glands Calcium is an essential element for contraction of voluntary/smooth
Instrumental determination of electrolytes in urine. Amal Alamri
 Instrumental determination of electrolytes in urine Amal Alamri What is the Electrolytes? Electrolytes are positively and negatively chargedions, Found in Within body's cells extracellular fluids, including
Instrumental determination of electrolytes in urine Amal Alamri What is the Electrolytes? Electrolytes are positively and negatively chargedions, Found in Within body's cells extracellular fluids, including
Sensipar. Sensipar (cinacalcet) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.46 Subject: Sensipar Page: 1 of 5 Last Review Date: June 22, 2018 Sensipar Description Sensipar (cinacalcet)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.46 Subject: Sensipar Page: 1 of 5 Last Review Date: June 22, 2018 Sensipar Description Sensipar (cinacalcet)
Guidelines and new evidence on CKD - MBD treatment
 Guidelines and new evidence on CKD - MBD treatment Goce Spasovski ERBP Advisory Board member University of Skopje, R. Macedonia ERA-EDTA CME course IV Congress of Nephrology of B&H, April 25, 2015, Sarajevo,
Guidelines and new evidence on CKD - MBD treatment Goce Spasovski ERBP Advisory Board member University of Skopje, R. Macedonia ERA-EDTA CME course IV Congress of Nephrology of B&H, April 25, 2015, Sarajevo,
CALCITRIOL Oral Solution
 CALCITRIOL Oral Solution Rx only DESCRIPTION Calcitriol Oral Solution is a synthetic vitamin D analog which is active in the regulation of the absorption of calcium from the gastrointestinal tract and
CALCITRIOL Oral Solution Rx only DESCRIPTION Calcitriol Oral Solution is a synthetic vitamin D analog which is active in the regulation of the absorption of calcium from the gastrointestinal tract and
Pediatric Nutrition and Kidney Disease
 Pediatric Nutrition and Kidney Disease Loai Eid, MD, MSHS, FAAP Consultant Pediatric Nephrologist Pediatric Nephrology & Hypertension Division Chief Dubai Hospital - DHA 26 th October, 2017 Objectives
Pediatric Nutrition and Kidney Disease Loai Eid, MD, MSHS, FAAP Consultant Pediatric Nephrologist Pediatric Nephrology & Hypertension Division Chief Dubai Hospital - DHA 26 th October, 2017 Objectives
Parathyoid glands and PTH
 Parathyoid glands and PTH They are four glands located behind the thyroid gland, each one from (20-50) mg in weight, and composed of two types of cells: 1. Cheif cells: that produces PTH. 2-oxyphil cells:
Parathyoid glands and PTH They are four glands located behind the thyroid gland, each one from (20-50) mg in weight, and composed of two types of cells: 1. Cheif cells: that produces PTH. 2-oxyphil cells:
Velphoro (sucroferric oxyhydroxide)
") STRENGTH DOSAGE FORM ROUTE GPID 500mg chewable tablet oral 36003 MANUFACTURER Fresenius Medical Care North America INDICATION(S) For the control of serum phosphorus levels in patients with chronic kidney
STRENGTH DOSAGE FORM ROUTE GPID 500mg chewable tablet oral 36003 MANUFACTURER Fresenius Medical Care North America INDICATION(S) For the control of serum phosphorus levels in patients with chronic kidney
Vitamins. Vitamins (continued) Lipid-Soluble Vitamins (A, D, E, K) Vitamins Serve Important Roles in Function of Body
 Lipid-Soluble Vitamins (A, D, E, K) Vitamins Serve Important Roles in Function of Body") Vitamins Drugs for Nutritional Disorders Organic substances are needed in small amounts Promote growth Maintain health Vitamins Human cells cannot produce vitamins Exception: vitamin D Vitamins or provitamins
Vitamins Drugs for Nutritional Disorders Organic substances are needed in small amounts Promote growth Maintain health Vitamins Human cells cannot produce vitamins Exception: vitamin D Vitamins or provitamins
Index. B BMC. See Bone mineral content BMD. See Bone mineral density Bone anabolic impact, Bone mass acquisition
 A Acid base balance dietary protein detrimental effects of, 19 Acid base balance bicarbonate effects, 176 in bone human studies, 174 mechanisms, 173 174 in muscle aging, 174 175 alkali supplementation
A Acid base balance dietary protein detrimental effects of, 19 Acid base balance bicarbonate effects, 176 in bone human studies, 174 mechanisms, 173 174 in muscle aging, 174 175 alkali supplementation
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES
 Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Clinical Approach to Hypercalcemia For the Primary Care Provider
 Clinical Approach to Hypercalcemia For the Primary Care Provider Christina Maser, MD FACS UCSF Fresno Department of Surgery, Endocrine Surgery 2/2/19 Objectives Recognition of pitfalls of diagnosis of
Clinical Approach to Hypercalcemia For the Primary Care Provider Christina Maser, MD FACS UCSF Fresno Department of Surgery, Endocrine Surgery 2/2/19 Objectives Recognition of pitfalls of diagnosis of
02/27/2018. Objectives. To Replace or Not to Replace: Nutritional Vitamin D in Dialysis.
 To Replace or Not to Replace: Nutritional Vitamin D in Dialysis. Michael Shoemaker-Moyle, M.D. Assistant Professor of Clinical Medicine Objectives Review Vitamin D Physiology Review Current Replacement
To Replace or Not to Replace: Nutritional Vitamin D in Dialysis. Michael Shoemaker-Moyle, M.D. Assistant Professor of Clinical Medicine Objectives Review Vitamin D Physiology Review Current Replacement
BONE AND MINERAL METABOLISM in the PD PATIENT
 BONE AND MINERAL METABOLISM in the PD PATIENT John Burkart, MD Professor of Medicine/Nephrology Wake Forest University Baptist Medical Center Chief Medical Officer Health Systems Management Maria V. DeVita,
BONE AND MINERAL METABOLISM in the PD PATIENT John Burkart, MD Professor of Medicine/Nephrology Wake Forest University Baptist Medical Center Chief Medical Officer Health Systems Management Maria V. DeVita,
HYDROCHLORIDE FOR THE TREATMENT OF SECONDARY HYPERPARATHYROIDISM IN PATIENTS WITH END-STAGE RENAL DISEASE ON MAINTENANCE DIALYSIS THERAPY
 UK RENAL PHARMACY GROUP SUBMISSION TO THE NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE on CINACALCET HYDROCHLORIDE FOR THE TREATMENT OF SECONDARY HYPERPARATHYROIDISM IN PATIENTS WITH END-STAGE RENAL DISEASE
UK RENAL PHARMACY GROUP SUBMISSION TO THE NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE on CINACALCET HYDROCHLORIDE FOR THE TREATMENT OF SECONDARY HYPERPARATHYROIDISM IN PATIENTS WITH END-STAGE RENAL DISEASE
Major intra and extracellular ions Lec: 1
 Major intra and extracellular ions Lec: 1 The body fluids are solutions of inorganic and organic solutes. The concentration balance of the various components is maintained in order for the cell and tissue
Major intra and extracellular ions Lec: 1 The body fluids are solutions of inorganic and organic solutes. The concentration balance of the various components is maintained in order for the cell and tissue
Outline. The Role of Vitamin D in CKD. Essential Role of Vitamin D. Mechanism of Action of Vit D. Mechanism of Action of Vit D 7/16/2010
 Outline The Role of Vitamin D in CKD Priscilla How, Pharm.D., BCPS Assistant Professor National University of Singapore Principal Clinical Pharmacist National University Hospital (Pharmacy and Nephrology,
Outline The Role of Vitamin D in CKD Priscilla How, Pharm.D., BCPS Assistant Professor National University of Singapore Principal Clinical Pharmacist National University Hospital (Pharmacy and Nephrology,
Hyperparathyroidism: Operative Considerations. Financial Disclosures: None. Hyperparathyroidism. Hyperparathyroidism 11/10/2012
 Hyperparathyroidism: Operative Considerations Financial Disclosures: None Steven J Wang, MD FACS Associate Professor Dept of Otolaryngology-Head and Neck Surgery University of California, San Francisco
Hyperparathyroidism: Operative Considerations Financial Disclosures: None Steven J Wang, MD FACS Associate Professor Dept of Otolaryngology-Head and Neck Surgery University of California, San Francisco
Inpatient Pediatric Endocrinology. Tala Dajani MD MPH Pediatric Endocrinology of Phoenix
 Inpatient Pediatric Endocrinology Tala Dajani MD MPH Pediatric Endocrinology of Phoenix Objectives Identify calcium disorders in the hospital Distinguish between temporary versus permanent glucose problems
Inpatient Pediatric Endocrinology Tala Dajani MD MPH Pediatric Endocrinology of Phoenix Objectives Identify calcium disorders in the hospital Distinguish between temporary versus permanent glucose problems
Dosage in renal impairment Kalcipos-D chewable tablets should not be used in patients with severe renal impairment.
 SUMMARY OF THE PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT Kalcipos-D 500 mg/400 IU chewable tablet 2 QUALITATIVE AND QUANTITATIVE COMPOSITION One chewable tablet contains: calcium 500 mg as
SUMMARY OF THE PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT Kalcipos-D 500 mg/400 IU chewable tablet 2 QUALITATIVE AND QUANTITATIVE COMPOSITION One chewable tablet contains: calcium 500 mg as
Draft Labeling Package Insert Not Actual Size. BRAINTREE LABORATORIES, INC. PhosLo Capsules (Calcium Acetate)
") Draft Labeling Package Insert Not Actual Size BRAINTREE LABORATORIES, INC. PhosLo Capsules (Calcium Acetate) DESCRIPTION: Full Size: Each opaque capsule with a white cap and white body is spin printed
Draft Labeling Package Insert Not Actual Size BRAINTREE LABORATORIES, INC. PhosLo Capsules (Calcium Acetate) DESCRIPTION: Full Size: Each opaque capsule with a white cap and white body is spin printed
SERUM PHOSPHORUS TESTING
 MEDICAL POLICY For use with the UnitedHealthcare Laboratory Benefit Management Program, administered by BeaconLBS SERUM PHOSPHORUS TESTING Policy Number: CMP - 035 Effective Date: January 21, 2017 Table
MEDICAL POLICY For use with the UnitedHealthcare Laboratory Benefit Management Program, administered by BeaconLBS SERUM PHOSPHORUS TESTING Policy Number: CMP - 035 Effective Date: January 21, 2017 Table
WATER, SODIUM AND POTASSIUM
 WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
Ipovitaminosi D e metabolismo calcio-fosforo in dialisi peritoneale. Maurizio Gallieni Università degli Studi di Milano
 Ipovitaminosi D e metabolismo calcio-fosforo in dialisi peritoneale Maurizio Gallieni Università degli Studi di Milano G Ital Nefrol 2018 - ISSN 1724-5990 Nutrients 2017, 9, 328 Vitamin D deficiency (
Ipovitaminosi D e metabolismo calcio-fosforo in dialisi peritoneale Maurizio Gallieni Università degli Studi di Milano G Ital Nefrol 2018 - ISSN 1724-5990 Nutrients 2017, 9, 328 Vitamin D deficiency (
Should cinacalcet be used in patients who are not on dialysis?
 Should cinacalcet be used in patients who are not on dialysis? Jorge B Cannata-Andía and José Luis Fernández-Martín Affiliations: Bone and Mineral Research Unit. Hospital Universitario Central de Asturias.
Should cinacalcet be used in patients who are not on dialysis? Jorge B Cannata-Andía and José Luis Fernández-Martín Affiliations: Bone and Mineral Research Unit. Hospital Universitario Central de Asturias.
Pediatric CKD-MBD: pathophysiology and management
 Pediatric CKD-MBD: pathophysiology and management Justine Bacchetta, MD, PhD Reference Center for Rare Renal Diseases Reference Center for Rare Diseases of Calcium and Phosphate Bron, France Overview of
Pediatric CKD-MBD: pathophysiology and management Justine Bacchetta, MD, PhD Reference Center for Rare Renal Diseases Reference Center for Rare Diseases of Calcium and Phosphate Bron, France Overview of
Amani Alghamdi. Slide 1
 Minerals in the body Amani Alghamdi Slide 1 The Minerals Small, naturally occurring, inorganic, chemical elements Serve as structural components Minerals classification The minerals present in the body
Minerals in the body Amani Alghamdi Slide 1 The Minerals Small, naturally occurring, inorganic, chemical elements Serve as structural components Minerals classification The minerals present in the body
1/3/2008. Karen Burke Priscilla LeMone Elaine Mohn-Brown. Medical-Surgical Nursing Care, 2e Karen Burke, Priscilla LeMone, and Elaine Mohn-Brown
 Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 7 Caring for Clients with Altered Fluid, Electrolyte, or Acid-Base Balance Water Primary component of
Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 7 Caring for Clients with Altered Fluid, Electrolyte, or Acid-Base Balance Water Primary component of
Awaisheh. Mousa Al-Abbadi. Abdullah Alaraj. 1 Page
 f #3 Awaisheh Abdullah Alaraj Mousa Al-Abbadi 1 Page *This sheet was written from Section 1 s lecture, in the first 10 mins the Dr. repeated all the previous material relating to osteoporosis from the
f #3 Awaisheh Abdullah Alaraj Mousa Al-Abbadi 1 Page *This sheet was written from Section 1 s lecture, in the first 10 mins the Dr. repeated all the previous material relating to osteoporosis from the
Natpara (parathyroid hormone) Prior Authorization with Quantity Limit Program Summary
 Prior Authorization with Quantity Limit Program Summary") Natpara (parathyroid hormone) Prior Authorization with Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Agent Indication Dosing and Administration Natpara (parathyroid hormone) subcutaneous
Natpara (parathyroid hormone) Prior Authorization with Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Agent Indication Dosing and Administration Natpara (parathyroid hormone) subcutaneous
Natpara (parathyroid hormone) Prior Authorization with Quantity Limit Program Summary
 Prior Authorization with Quantity Limit Program Summary") Natpara (parathyroid hormone) Prior Authorization with Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 2 Available Product Indication Dosing and Administration Natpara (parathyroid hormone)
Natpara (parathyroid hormone) Prior Authorization with Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 2 Available Product Indication Dosing and Administration Natpara (parathyroid hormone)
Figures and tables in this presentation were adopted from various printed and electronic resorces and serve strictly for educational purposes.
 Academic lectures 3rd year of Medical faculty Figures and tables in this presentation were adopted from various printed and electronic resorces and serve strictly for educational purposes. ENDOCRINOLOGY
Academic lectures 3rd year of Medical faculty Figures and tables in this presentation were adopted from various printed and electronic resorces and serve strictly for educational purposes. ENDOCRINOLOGY
TABLE OF CONTENTS T-1. A-1 Acronyms and Abbreviations. S-1 Stages of Chronic Kidney Disease (CKD)
") A-1 Acronyms and Abbreviations TABLE OF CONTENTS S-1 Stages of Chronic Kidney Disease (CKD) Chapter 1: Nutrition Assessment Charts, Tables and Formulas 1-2 Practical Steps to Nutrition Assessment Adult
A-1 Acronyms and Abbreviations TABLE OF CONTENTS S-1 Stages of Chronic Kidney Disease (CKD) Chapter 1: Nutrition Assessment Charts, Tables and Formulas 1-2 Practical Steps to Nutrition Assessment Adult
Head and Neck Endocrine Surgery
 Objectives Endocrine Physiology Risk factors for hypocalcemia Management strategies Passive vs. active Treatment of hypocalcemia Department of Head and Neck Management of Calcium in Thyroid and Parathyroid
Objectives Endocrine Physiology Risk factors for hypocalcemia Management strategies Passive vs. active Treatment of hypocalcemia Department of Head and Neck Management of Calcium in Thyroid and Parathyroid
Nuove terapie in ambito Nefrologico: Etelcalcetide (AMG-416)
") Nuove terapie in ambito Nefrologico: Etelcalcetide (AMG-416) Antonio Bellasi, MD, PhD U.O.C. Nefrologia & Dialisi ASST-Lariana, Ospedale S. Anna, Como, Italy Improvement of mineral and bone metabolism
Nuove terapie in ambito Nefrologico: Etelcalcetide (AMG-416) Antonio Bellasi, MD, PhD U.O.C. Nefrologia & Dialisi ASST-Lariana, Ospedale S. Anna, Como, Italy Improvement of mineral and bone metabolism
Contents. Authors Name: Christopher Wong: Consultant Nephrologist Anne Waddington: Renal Pharmacist Eimear Fegan : Renal Dietitian
 Cheshire and Merseyside Renal Units Guidelines on the Management of Chronic Kidney Disease - Mineral Bone Disorder (adapted from Greater Manchester) Authors Name: Christopher Wong: Consultant Nephrologist
Cheshire and Merseyside Renal Units Guidelines on the Management of Chronic Kidney Disease - Mineral Bone Disorder (adapted from Greater Manchester) Authors Name: Christopher Wong: Consultant Nephrologist
BEC FEED SOLUTIONS NEW ZEALAND Ltd
 BEC FEED SOLUTIONS NEW ZEALAND Ltd Proudly sponsor Dr Alessandro Mereu Yara Feed Phosphates July 2017 NZARN Meeting www.becfeed.co.nz Phosphorus metabolism in cattle: principles and interactions with Ca
BEC FEED SOLUTIONS NEW ZEALAND Ltd Proudly sponsor Dr Alessandro Mereu Yara Feed Phosphates July 2017 NZARN Meeting www.becfeed.co.nz Phosphorus metabolism in cattle: principles and interactions with Ca
The hart and bone in concert
 The hart and bone in concert Piotr Rozentryt III Department of Cardiology, Silesian Centre for Heart Disease, Silesian Medical University, Zabrze, Poland Disclosure Research grant, speaker`s fee, travel
The hart and bone in concert Piotr Rozentryt III Department of Cardiology, Silesian Centre for Heart Disease, Silesian Medical University, Zabrze, Poland Disclosure Research grant, speaker`s fee, travel
DECALCITROL- cholecalciferol tablet, coated Pharmin USA, LLC DECALCITROL CHOLECALCIFEROL (VITAMIN D3) 1.25 mg TABLETS (50,000 Units)
 1.25 mg TABLETS (50,000 Units)") DECALCITROL- cholecalciferol tablet, coated ---------- DECALCITROL CHOLECALCIFEROL (VITAMIN D3) 1.25 mg TABLETS (50,000 Units) HIGH POTENCY SUPPLEMENT* *Warning: Cholecalciferol 50000 IU can be classified
DECALCITROL- cholecalciferol tablet, coated ---------- DECALCITROL CHOLECALCIFEROL (VITAMIN D3) 1.25 mg TABLETS (50,000 Units) HIGH POTENCY SUPPLEMENT* *Warning: Cholecalciferol 50000 IU can be classified
76 year-old female presents with muscle cramps. Jess Hwang 12/6/12
 76 year-old female presents with muscle cramps Jess Hwang 12/6/12 HPI Worked up for outpatient hypercalcemia Calcium had been 10.3-11.1, PTH ~120 No h/o osteoporosis, CKD, kidney stones Not taking calcium
76 year-old female presents with muscle cramps Jess Hwang 12/6/12 HPI Worked up for outpatient hypercalcemia Calcium had been 10.3-11.1, PTH ~120 No h/o osteoporosis, CKD, kidney stones Not taking calcium
PREVALENCE AND PATTERNS OF HYPERPARATHYROIDISM AND MINERAL BONE DISEASE IN PATIENTS WITH CHRONIC KIDNEY DISEASE AT KENYATTA NATIONAL HOSPITAL
 PREVALENCE AND PATTERNS OF HYPERPARATHYROIDISM AND MINERAL BONE DISEASE IN PATIENTS WITH CHRONIC KIDNEY DISEASE AT KENYATTA NATIONAL HOSPITAL DR. ANNE MUGERA The Problem Chronic Kidney disease is a worldwide
PREVALENCE AND PATTERNS OF HYPERPARATHYROIDISM AND MINERAL BONE DISEASE IN PATIENTS WITH CHRONIC KIDNEY DISEASE AT KENYATTA NATIONAL HOSPITAL DR. ANNE MUGERA The Problem Chronic Kidney disease is a worldwide
International Journal of Health Sciences and Research ISSN:
 International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article Prevalence and Pattern of Mineral Bone Disorder in Chronic Kidney Disease Patients Using Serum
International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article Prevalence and Pattern of Mineral Bone Disorder in Chronic Kidney Disease Patients Using Serum
SUMMARY OF THE PRODUCT CHARACTERISTICS
 SUMMARY OF THE PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT Kalcipos-D mite 500 mg/200 IU film-coated tablet 2 QUALITATIVE AND QUANTITATIVE COMPOSITION Each film-coated tablet contains 500 mg
SUMMARY OF THE PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT Kalcipos-D mite 500 mg/200 IU film-coated tablet 2 QUALITATIVE AND QUANTITATIVE COMPOSITION Each film-coated tablet contains 500 mg
CALCIUM BALANCE. James T. McCarthy & Rajiv Kumar
 CALCIUM BALANCE James T. McCarthy & Rajiv Kumar CALCIUM BALANCE TOTAL BODY CALCIUM (~ 1000g in a normal 60 kg adult) - > 99% in bones - ~ 0.6% in the intracellular space - ~ 0.1% in the extracellular space
CALCIUM BALANCE James T. McCarthy & Rajiv Kumar CALCIUM BALANCE TOTAL BODY CALCIUM (~ 1000g in a normal 60 kg adult) - > 99% in bones - ~ 0.6% in the intracellular space - ~ 0.1% in the extracellular space
Corporate Presentation January 2013
 Corporate Presentation January 2013 0 Forward-Looking Statements Certain statements and information included in this presentation are forwardlooking statements under the Private Securities Litigation Reform
Corporate Presentation January 2013 0 Forward-Looking Statements Certain statements and information included in this presentation are forwardlooking statements under the Private Securities Litigation Reform
Calcium and Parathyroid Disorders
 Calcium and Parathyroid Disorders Hussain Mahmud, MD Clinical Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism University of Pittsburgh Butler Memorial Hospital November
Calcium and Parathyroid Disorders Hussain Mahmud, MD Clinical Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism University of Pittsburgh Butler Memorial Hospital November
Rahaf AL-Jafari. Marah Qaddourah. Rahmeh Abdullah. Saleem. 1 P a g e
 15 Rahaf AL-Jafari Marah Qaddourah Rahmeh Abdullah Saleem 1 P a g e If you are following with the record you may notice a little bit difference in information sequences. Hormones that function on growth
15 Rahaf AL-Jafari Marah Qaddourah Rahmeh Abdullah Saleem 1 P a g e If you are following with the record you may notice a little bit difference in information sequences. Hormones that function on growth
Package Insert. D-Bright
 Package Insert D-Bright Product Summary 1. Name of the medicinal product D-Bright 2. Qualitative and quantitative composition Each ml contains Cholecalciferol (Vitamin D3) IP 400 IU in a flavoured syrupy
Package Insert D-Bright Product Summary 1. Name of the medicinal product D-Bright 2. Qualitative and quantitative composition Each ml contains Cholecalciferol (Vitamin D3) IP 400 IU in a flavoured syrupy
SUMMARY OF PRODUCT CHARACTERISTICS
 SUMMARY OF PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT Colecalciferol Meda 800 IU tablet 2 QUALITATIVE AND QUANTITATIVE COMPOSITION Each tablet contains colecalciferol (vitamin D 3 ) 800 IU
SUMMARY OF PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT Colecalciferol Meda 800 IU tablet 2 QUALITATIVE AND QUANTITATIVE COMPOSITION Each tablet contains colecalciferol (vitamin D 3 ) 800 IU
Renal Association Clinical Practice Guideline in Mineral and Bone Disorders in CKD
 Nephron Clin Pract 2011;118(suppl 1):c145 c152 DOI: 10.1159/000328066 Received: May 24, 2010 Accepted: December 6, 2010 Published online: May 6, 2011 Renal Association Clinical Practice Guideline in Mineral
Nephron Clin Pract 2011;118(suppl 1):c145 c152 DOI: 10.1159/000328066 Received: May 24, 2010 Accepted: December 6, 2010 Published online: May 6, 2011 Renal Association Clinical Practice Guideline in Mineral
Kobe University Repository : Kernel
 Title Author(s) Citation Issue date 2009-09 Resource Type Resource Version DOI URL Kobe University Repository : Kernel Marked increase in bone formation markers after cinacalcet treatment by mechanisms
Title Author(s) Citation Issue date 2009-09 Resource Type Resource Version DOI URL Kobe University Repository : Kernel Marked increase in bone formation markers after cinacalcet treatment by mechanisms
Treatment Options for Chronic Kidney
 Treatment Options for Chronic Kidney Disease: Metabolic Introduction Bone Disease to Renagel Goce Spasovski, R. Macedonia The 17th Budapest Nephrology School, August 29, 2010 Session Objectives Definition
Treatment Options for Chronic Kidney Disease: Metabolic Introduction Bone Disease to Renagel Goce Spasovski, R. Macedonia The 17th Budapest Nephrology School, August 29, 2010 Session Objectives Definition
Phosphate Management Guideline for Patients Receiving Extended Duration Hemodialysis
 IAMHD HOME HEMODIALYSIS CLINICAL PRACTICE STANDARDS AND PROCEDURES Phosphate Management Guideline for Patients Receiving Extended Duration Hemodialysis PRINTED copies of Clinical Practice Standards and
IAMHD HOME HEMODIALYSIS CLINICAL PRACTICE STANDARDS AND PROCEDURES Phosphate Management Guideline for Patients Receiving Extended Duration Hemodialysis PRINTED copies of Clinical Practice Standards and
UCLA Nutrition Bytes. Title. Permalink. Journal ISSN. Author. Publication Date. Calcium and Hypertension. https://escholarship.org/uc/item/68b658ss
 UCLA Nutrition Bytes Title Calcium and Hypertension Permalink https://escholarship.org/uc/item/68b658ss Journal Nutrition Bytes, 4(2) ISSN 1548-601X Author Martinez, Christina Publication Date 1998-01-01
UCLA Nutrition Bytes Title Calcium and Hypertension Permalink https://escholarship.org/uc/item/68b658ss Journal Nutrition Bytes, 4(2) ISSN 1548-601X Author Martinez, Christina Publication Date 1998-01-01
Sensipar (cinacalcet)
") Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
hypercalcemia of malignancy hyperparathyroidism PHPT the most common cause of hypercalcemia in the outpatient setting the second most common cause
 hyperparathyroidism A 68-year-old woman with documented osteoporosis has blood tests showing elevated serum calcium and parathyroid hormone (PTH) levels: 11.2 mg/dl (8.8 10.1 mg/dl) and 88 pg/ml (10-60),
hyperparathyroidism A 68-year-old woman with documented osteoporosis has blood tests showing elevated serum calcium and parathyroid hormone (PTH) levels: 11.2 mg/dl (8.8 10.1 mg/dl) and 88 pg/ml (10-60),
The Parsabiv Beginner s Book
 The Parsabiv Beginner s Book A quick guide to help you learn about your treatment with Parsabiv and what to expect Indication Parsabiv (etelcalcetide) is indicated for the treatment of secondary hyperparathyroidism
The Parsabiv Beginner s Book A quick guide to help you learn about your treatment with Parsabiv and what to expect Indication Parsabiv (etelcalcetide) is indicated for the treatment of secondary hyperparathyroidism
Continuing Education for Pharmacy Technicians Dietary Supplements: Calcium and Vitamin D
 1 Continuing Education for Pharmacy Technicians Dietary Supplements: Calcium and Vitamin D Ashley Elliott, PharmD candidate Julie N. Bosler, PharmD McWhorter School of Pharmacy Birmingham, AL Objectives:
1 Continuing Education for Pharmacy Technicians Dietary Supplements: Calcium and Vitamin D Ashley Elliott, PharmD candidate Julie N. Bosler, PharmD McWhorter School of Pharmacy Birmingham, AL Objectives:
Level 1 Strong We recommendyshould A High Moderate Level 2 Weak We suggestymight C Low Very low. K Hyperphosphatemia has been associated with poor
 chapter 4.1 http://www.kidney-international.org & 2009 KDIGO Chapter 4.1: Treatment of CKD MBD targeted at lowering high serum phosphorus and maintaining serum calcium ; doi:10.1038/ki.2009.192 Grade for
chapter 4.1 http://www.kidney-international.org & 2009 KDIGO Chapter 4.1: Treatment of CKD MBD targeted at lowering high serum phosphorus and maintaining serum calcium ; doi:10.1038/ki.2009.192 Grade for
Shon E. Meek, M.D., Ph.D. Assistant Professor of Medicine
 Shon E. Meek, M.D., Ph.D. Assistant Professor of Medicine meek.shon@mayo.edu 2016 MFMER 3561772-1 Update on Vitamin D Shon Meek MD, PhD 20 th Annual Endocrine Update January 30-Feb 3, 2017 Disclosure Relevant
Shon E. Meek, M.D., Ph.D. Assistant Professor of Medicine meek.shon@mayo.edu 2016 MFMER 3561772-1 Update on Vitamin D Shon Meek MD, PhD 20 th Annual Endocrine Update January 30-Feb 3, 2017 Disclosure Relevant
SUMMARY OF PRODUCT CHARACTERISTICS. One chewable tablet contains 1250 mg calcium carbonate (equivalent to 500 mg calcium).
.") SUMMARY OF PRODUCT CHARACTERISTICS 1. NAME OF THE MEDICINAL PRODUCT [XXX] 500 mg chewable tablets 2. QUALITATIVE AND QUANTITATIVE COMPOSITION One chewable tablet contains 1250 mg calcium carbonate (equivalent
SUMMARY OF PRODUCT CHARACTERISTICS 1. NAME OF THE MEDICINAL PRODUCT [XXX] 500 mg chewable tablets 2. QUALITATIVE AND QUANTITATIVE COMPOSITION One chewable tablet contains 1250 mg calcium carbonate (equivalent
CKD FOR INTERNISTS. Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College
 CKD FOR INTERNISTS Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College INTRODUCTION In 2002, the National Kidney Foundation s Kidney Disease Outcomes Quality Initiative(KDOQI)
CKD FOR INTERNISTS Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College INTRODUCTION In 2002, the National Kidney Foundation s Kidney Disease Outcomes Quality Initiative(KDOQI)
CAL360 Tablets (Calcium citrate malate + Vitamin D3 )
") Published on: 18 Jan 2016 CAL360 Tablets ( citrate malate + Vitamin D3 ) Composition Each film-coated tablet contains: Citrate Malate equivalent to Elementary 250 mg Cholecalciferol Concentrate (powder
Published on: 18 Jan 2016 CAL360 Tablets ( citrate malate + Vitamin D3 ) Composition Each film-coated tablet contains: Citrate Malate equivalent to Elementary 250 mg Cholecalciferol Concentrate (powder
For the use only of Registered Medical Practitioners or a Hospital or a Laboratory OSTOCALCIUM FORTE TABLETS
 For the use only of Registered Medical Practitioners or a Hospital or a Laboratory OSTOCALCIUM FORTE TABLETS Calcium and Phosphorus with Vitamin D3 Tablets QUALITATIVE AND QUANTITATIVE COMPOSITION Each
For the use only of Registered Medical Practitioners or a Hospital or a Laboratory OSTOCALCIUM FORTE TABLETS Calcium and Phosphorus with Vitamin D3 Tablets QUALITATIVE AND QUANTITATIVE COMPOSITION Each
SUMMARY OF PRODUCT CHARACTERISTICS. A 2.5ml single-dose bottle containing IU Cholecalciferol (equivalent to 625 micrograms vitamin D 3 )
") SUMMARY OF PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT Fultium 25 000 IU Oral Solution 2 QUALITATIVE AND QUANTITATIVE COMPOSITION A 2.5ml single-dose bottle containing 25 000 IU Cholecalciferol
SUMMARY OF PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT Fultium 25 000 IU Oral Solution 2 QUALITATIVE AND QUANTITATIVE COMPOSITION A 2.5ml single-dose bottle containing 25 000 IU Cholecalciferol
Calcium Management for Patients Receiving Extended Duration Hemodialysis
 Calcium Management for Patients Receiving Extended Duration Hemodialysis Created November 2017; Updated March 2018 Approved by the BCPRA Home Hemodialysis Committee Table of Contents 1.0 Practice Standard...1
Calcium Management for Patients Receiving Extended Duration Hemodialysis Created November 2017; Updated March 2018 Approved by the BCPRA Home Hemodialysis Committee Table of Contents 1.0 Practice Standard...1
Vitamin D. Vitamin functioning as hormone. Todd A Fearer, MD FACP
 Vitamin D Vitamin functioning as hormone Todd A Fearer, MD FACP Vitamin overview Vitamins are organic compounds that are essential in small amounts for normal metabolism They are different from minerals
Vitamin D Vitamin functioning as hormone Todd A Fearer, MD FACP Vitamin overview Vitamins are organic compounds that are essential in small amounts for normal metabolism They are different from minerals
What is the right calcium balance?
 For patients with hypoparathyroidism What is the right calcium balance? Indications and Usage1 NATPARA is a parathyroid hormone indicated as an adjunct to calcium and vitamin D to control hypocalcemia
For patients with hypoparathyroidism What is the right calcium balance? Indications and Usage1 NATPARA is a parathyroid hormone indicated as an adjunct to calcium and vitamin D to control hypocalcemia
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Natpara (parathyroid hormone) Page 1 of 8 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Natpara (parathyroid hormone) Prime Therapeutics will review Prior Authorization
Natpara (parathyroid hormone) Page 1 of 8 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Natpara (parathyroid hormone) Prime Therapeutics will review Prior Authorization