Importance of drug antagonism (i) Correcting adverse effects of drugs (ii) Treating drug poisoning. e.g. Morphine with naloxone, organophosphate
|
|
|
- Everett Gray
- 5 years ago
- Views:
Transcription
1 Importance of drug antagonism (i) Correcting adverse effects of drugs (ii) Treating drug poisoning. e.g. Morphine with naloxone, organophosphate compounds with atropine. (iii) Predicting drug combinations which would reduce drug efficacy.
2
3
4
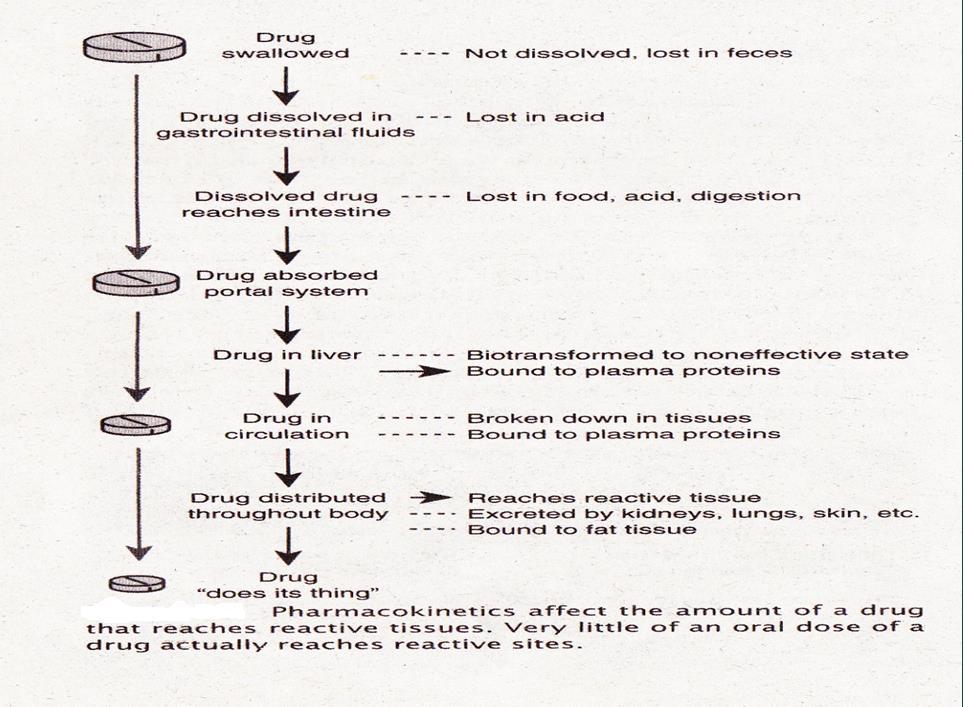
5 Pharmacokinetics : the actions of the body on the drug and includes absorption, distribution, metabolism and excretion drugs in the body. Biotransport of drug: It is translocation of a solute from one side of the biological barrier to the other. Structure of biological membrane: The outer surface of the cell covered by a very thin structure known as plasma membrane. It is composed of lipid and protein molecules.
6 The membrane proteins have many functions like: (a) Contributing structure to the membrane (b)acting as enzyme (c) Acting as carrier for transport of substances (d) Acting as receptors. The plasma membrane is a semipermeable membrane allowing certain chemical substances to pass freely e.g. it allows water, glucose, etc. but it won t allow sucrose until it is converted into glucose and fructose.
7 2. Passage of drug across membrane. (a) Passive transfer i) Simple diffusion ii) Filtration (b) Specialized transport (carrier mediated transport) i) Facilitated diffusion ii) Active transport iii) Endocytosis.
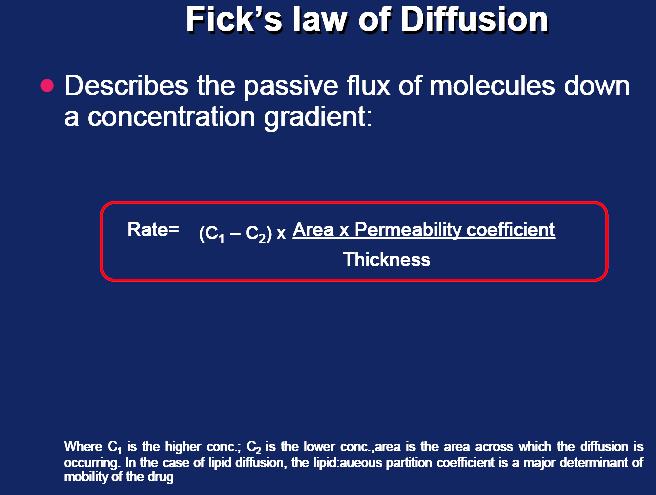
8 i) Simple diffusion: Movement of a solute through a biological barrier from the phase of higher concentration to phase of lower concentration. No need of energy e.g. highly lipid soluble drugs. ii) Filtration: Is the process by which water soluble drug of relatively low molecular weight crosses the plasma membrane through pores as a result of hydrodynamic pressure gradient across the membrane e.g. urea and ethylene glycol.
9
10 i) Facilitated diffusion: It means the passage of drug across the biological membrane along the concentration gradient by the protein carrier mediated system also called as carrier mediated diffusion. It depends on number of carrier e.g. tetracycline, pyrimidine. ii) Active transport: The process by which drugs pass across the biological membrane most often against their concentration gradient with the help of carriers along with the expenditure of energy. e.g. alpha methyl dopa, levodopa, 5-fluoro-uracil, 5 bromouracil. iii) Endocytosis: It is the process by which the large molecules are engulfed by the cell membrane and releases them intracellularly e.g. protein, toxins (botulinum, diphtheria)
11
12 Factors that influence tissue drug concentrations over time include: (ADME) 1.Absorption 2.Distribution 3.Metabolism (biotransformation) 4.Excretion
13 Absorption is the process by which the drug enters in to the systemic circulation from the site of administration through biological barrier. In case of intravenous or intra-arterial administration the drug bypasses absorption processes and it enters into the circulation directly. For a drug to produce effect at the site of action, it should be able to cross/ translocate/ penetrate through the various barriers/ membrans between the site of administration to the site of action. The plasma membrane represents the common barrier to drug distribution
14 The fraction of unchanged drug reaching the systemic circulation following administration by any route It is determined comparing area under concentration curve AUC) a after particular with plasma levels achieved IV injection. The fraction of unchanged drug reaching the systemic circulation following administration by any route

15 When the drug is given IV, the bioavailability is 100%. It is important to know the manner in which a drug is absorbed. The route of administration largely determines the latent period between administration and onset of action. Drugs given by mouth may be inactive for the following reasons: Enzymatic degradation of polypeptides within the lumen of the gastrointestinal tract e.g. insulin, ACTH. Poor absorption through gastrointestinal tract e.g. aminoglycoside antibiotic. Inactivation by liver e.g. testosterone during first passage through the liver before it reaches systemic circulation. It is determined by comparing the area under the concentration curve (AUC) of a drug after a particular route of administration with plasma drug levels achieved by IV injection
16
17 Single dose bioavailability test involves an analysis of plasma or serum concentration of the drug at various time intervals after its oral administration and plotting a serum concentration time curve. MTC: Minimum toxic concentration MEC: Minimum effective concentration Formulation A = would produce quick onset and short duration of action, produce toxic effects. Formation B = Effect would last much longer and The plasma drug level curves following administration of three formulations (A, B and C) of the same basic drug. nontoxic Formulation C = gives inadequate plasma level so therapeutically ineffective.
18 1.Gastric emptying time 2.Intestinal motility 3.Food 4.Drugs 5.Perfusion of the Gastrointestinal Tract 6.Particle size and formulation 7.Solubility of the drug 8.Reverese transporter (p-glycoprotein) 9.Chemical instability 10.First pass metabolism
19 Factors affecting drug absorption and bioavailability: a) Physico-chemical properties of drug. b) Nature of the dosage form. c) Physiological factors. d) Pharmacogenetic factors. e) Disease states.
 Lipid or water solubility: Drugs in aqueous solution mix more readily than those in oily solution.")
20 i) Physical state: Liquids are absorbed better than solids and crystalloids absorbed better than colloids. ii) Lipid or water solubility: Drugs in aqueous solution mix more readily than those in oily solution. However at the cell surface, the lipid soluble drugs penetrate into the cell more rapidly than the water soluble drugs. iii) Ionization: Most of the drugs are organic compounds. Unlike inorganic compounds, the organic drugs are not completely ionized in the fluid. Unionized component is predominantly lipid soluble and is absorbed rapidly and an ionized is often water soluble component which is absorbed poorly.
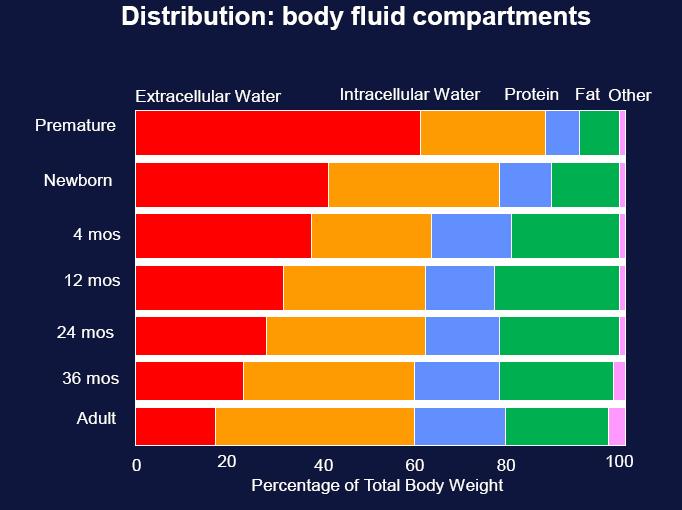
21 It may be assumed for all practical purposes, that the mucosal lining of the G.I.T is impermeable to the ionized form of a weak organic acid or a weak organic base. These drugs exist in two forms. Acidic drugs: rapidly absorbed from the stomach e.g. salicylates and barbiturates. Basic drugs: Not absorbed until they reach to the alkaline environment i.e. small intestine when administered orally e.g. pethidine and ephedrine.
22 Many drugs are weak acids or bases that are present in solution as both the non-ionized and ionized species Nonionized molecules are usually lipid soluble and can diffuse across membrane. The transmembrane distribution of a weak electrolyte is influenced by its pka and the ph gradient across the membrane. The relationship of pka and the ratio of acid-base concentration to ph is expressed by the Henderson- Hasselbalch Equation:
23
24 Equation is clinically important when it is necessary to accelerate the excretion of drugs by the kidney in the case of an overdose by changing the ph of the urine (increase ionized state to trap drug in urine. Excretion of weak acids may be accelerated by alkalinizing the urine giving bicarbonate I.V. Excretion of a weak base may be accelerated by acidifying the urine - giving ammonium chloride I.V.
25 i) Particle size: Small particle size is important for drug absorption. Drugs given in a dispersed or emulsified state are absorbed better e.g. vitamin D and vitamin A. ii) Disintegration time and dissolution rate. Disintegration time: The rate of break up of the tablet or capsule into the drug granules. Dissolution rate: The rate at which the drug goes into solution. iii) Formulation: Usually substances like lactose, sucrose, starch and calcium phosphate are used as inert diluents in formulating powders or tablets. Fillers may not be totally inert but may affect the absorption as well as stability of the medicament. Thus a faulty formulation can render a useful drug totally useless therapeutically.
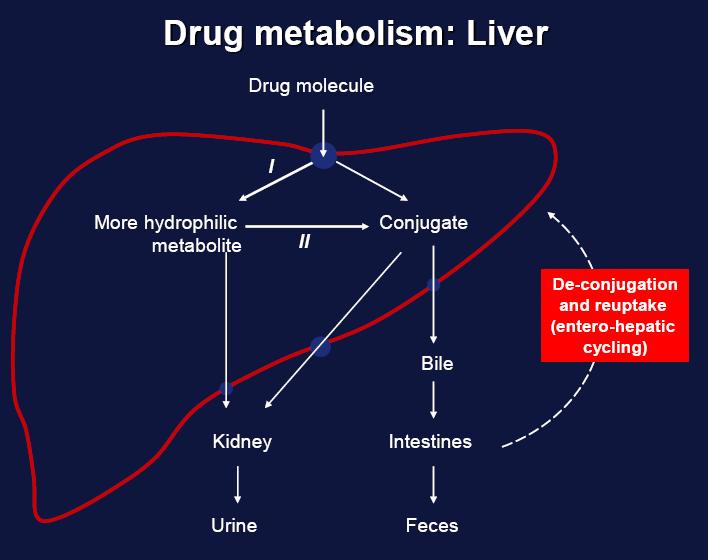
26 i) Gastrointestinal transit time: Rapid absorption occurs when the drug is given on empty stomach. However certain irritant drugs like salicylates and iron preparations are deliberately administred after food to minimize the gastrointestinal irritation. But some times the presence of food in the G.I tract aids the absorption of certain drugs e.g. griseofulvin, propranolol and riboflavin. ii) Presence of other agents: Vitamin C enhances the absorption of iron from the G.I.T. Calcium present in milk and in antacids forms insoluble complexes with the tetracycline antibiotics and reduces their absorption. iii) Area of the absorbing surface and local circulation: Drugs can be absorbed better from the small intestine than from the stomach because of the larger surface area of the former. Increased vascular supply can increase the absorption. iv) Enterohepatic cycling: Some drugs move in between intestines and liver before they reach the site of action. This increases the bioavailability e.g. phenolphthalein. v) Metabolism of drug/first pass effect: Rapid degradation of a drug by the liver during the first pass (propranolol) or by the gut wall (isoprenaline) also affects the bioavailability. Thus a drug though absorbed well when given orally may not be effective because of its extensive first pass metabolism.
27 d) Pharmacogenetic factors: Individual variations occur due to the genetically mediated reason in drug absorption and response. e) Disease states: Absorption and first pass metabolism may be affected in conditions like malabsorption, thyrotoxicosis, and liver cirrhosis.

28 It the process by which a drug reversibly leaves blood and enter interstitium (extracellular fluid) and/ or cells of tissues. Primarily depends on: 1.Regional blood flow. 2.Capillary permeability. 3.Protein binding. 4.Chemical nature of the drug.
29 Drugs distribute through various body fluid compartments such as (a) plasma (b) interstitial fluid compartment (c) trans-cellular compartment. Apparent Volume of distribution (VD): The volume into which the total amount of a drug in the body would have to be uniformly distributed to provide the concentration of the drug actually measured in the plasma. It is an apparent rather than real volume.
30
31 Volume of distribution (Vd) of a drug is the volume of body fluids into which drug is distributed in same concentration as in plasma Total body fluid is about 60% of body weight i.e. about 42 L for a 70 Kg man. 2 / 3 ICF ~ 28 L 1 / 3 ECF ~ 14 L. This is divided into : 3 4 L Plasma 9 10 L Tissue fluid
32 In 70 kg patient : If Vd = 3-4 L, drug is mainly localized in plasma e.g. bound to plasma albumin If Vd = L, then drug is localized in ECF i.e. it is water soluble and poorly enter cells If Vd = 20 L, then drug is lipid soluble, and partially enter into cells across cell membranes of tissues If Vd = 40 L, then drug is enough lipid soluble to be uniformly distributed in total body fluid e.g. alcohol If Vd = > 42 L e.g.100 L, drug is highly lipid soluble & is stored in some tissues e.g. Digoxin Vd = 300 L; hemodialysis is not useful to remove this drug from body in poisoning. Because of this large Vd for stored drugs, Vd is named : apparent i.e. avd
33
34 Drugs confined to the plasma compartment (plasma volume 0.05L/kg BWT) (e.g. heparin and warfarin): very large molecular weight, low lipid solubility, or binds extensively to plasma proteins. Drugs distributed in the extracellular compartment (intracellular volume 0.2L/kg) (e.g. aminoglycoside antibiotics): low molecular weight and hydrophilic
35 Drug distributed throughout the body water (total body water 0.55L/kg): lipidsoluble drugs that readily cross membrane. Other sites: Milk, bone, muscles. Drugs that are extremely lipid soluble (e.g. thiopental) may have unusually high volume of distribution).
 binds basic drugs")

36 1. Protein binding of drug: Many drugs circulate in the bloodstream bound to plasma proteins Albumin is a major carrier for acidic drugs and α1-acid glycoprotein (AAG) binds basic drugs The binding is usually reversible Binding of a drug to plasma proteins limits its concentration in tissues and at its site of action because only unbound drug is in equilibrium across membranes
37 Most drugs are bound to some extent to proteins in the blood to be carried into circulation. The protein-drug complex is relatively large & cannot enter into capillaries & then into tissues to react. The drug must be freed from the protein s binding site at the tissues.
38 Tightly bound released very slowly. these drugs have very long duration of action (not freed to be broken down or excreted), slowly released into the reactive tissue. Loosely bound tend to act quickly and excreted quickly Compete for protein binding sites alters effectiveness or causing toxicity when 2 drugs are given together.
39 The extent of plasma protein binding also may be affected by disease-related factors and drugdrug interactions. Hypoalbuminemia secondary to severe liver disease or nephrotic syndrome results in reduced binding and an increase in the unbound fraction The active concentration of the drug is that part which is not bound, because it is only this fraction which is free to leave the plasma and site of action.
40 (a) Free drug leave plasma to site of action (b) binding of drugs to plasma proteins assists absorption (c) protein binding acts as a temporary store of a drug and tends to prevent large fluctuations in concentration of unbound drug in the body fluids (d) protein binding reduces diffusion of drug into the cell and there by delays its metabolic degradation e.g. high protein bound drug like phenylbutazone is long acting. Low protein bound drug like thiopental sodium is short acting.
41
42 3. Clearance: Volume of plasma cleared off the drug by metabolism and excretion per unit time. Protein binding reduces the amount of drug available for filtration at the glomeruli and hence delays the excretion, thus the protein binding reduces the clearance.
43 4. Physiological barriers to distribution: There are some specialized barriers in the body due to which the drug will not be distributed uniformly in all the tissues. These barriers are: a) Blood brain barrier (BBB) through which thiopental sodium is easily crossed but not dopamine. b) Placental barrier: which allows non-ionized drugs with high lipid/water partition coefficient by a process of simple diffusion to the foetus e.g. alcohol, morphine.
44 5. Affinity of drugs to certain organs: The concentration of a drug in certain tissues after a single dose may persist even when its plasma concentration is reduced to low. Thus the hepatic concentration of mepacrine is more than 200 times that of plasma level. Their concentration may reach a very high level on chronic administration. Iodine is similarly concentrated in the thyroid tissue.


45 Is the irreversible loss of drug from the body It occurs by two processes: Excretion & Metabolism Kidney and liver are the most common organs of drug elimination The kidney is the most important organ for excreting drugs and their metabolites Three fundamental processes account for renal drug excretion: glomerular filtration, active tubular secretion, passive tubular reabsorption

46 Drugs are chemical substances, which interact with living organisms and produce some pharmacological effects and then, they should be eliminated from the body unchanged or by changing to some easily excretable molecules. The process by which the body brings about changes in drug molecule is referred as drug metabolism or biotransformation.
47 Involves enzymic conversion of one chemical entity to another within the body The liver is the major site for drug metabolism Specific drugs may undergo biotransformation in other tissues, such as the kidney and the intestine
48 Enzymes responsible for metabolism of drugs: Microsomal enzymes: Present in the smooth endoplasmic reticulum of the liver, kidney and GIT e.g. glucuronyl transferase, dehydrogenase, hydroxylase and cytochrome P450. Non-microsomal enzymes: Present in the cytoplasm, mitochondria of different organs.e.g. esterases, amidase, hydrolase.
49 The chemical reactions involved in biotransformation are classified as phase-i and phase II (conjugation) reactions. In phase-i reaction the drug is converted to more polar metabolite. If this metabolite is sufficiently polar, then it will be excreted in urine. Some metabolites may not be excreted and further metabolised by phase II reactions.
50 The enzyme systems for drug metabolic biotransformation reactions can be grouped into two categories: Phase-I: Oxidation, reduction and hydrolysis. Phase-II: Glucuronidation, sulfate conjugation, acetylation, glycine conjugation and methylation reactions.
51

52
53 Usually convert the parent drug to a more polar metabolite by introducing a functional group (-OH, - NH2, -SH). Phase I metabolism may increase, decrease, activate (prodrug, e.g. enalapril) or leave unaltered the drug s pharmacologic activity. Phase I reactions are catalyzed by the cytochrome P450 (CYP450) system functional group ( -OH, - NH2, -S H). Phase I metabolism may increase, decrease, activate (prodrug, e.g. enalapril) or leave unaltered the drug s pharmacologic activity. Phase I reactions are catalyzed by the cytochrome P450 (CYP450) system.
54 Species and strain variations exist in amount and activity of cytochrome P- 450 isoforms. Isoforms are classified into families and further into subfamilies. Nomenclature : e.g. CYP3 A4 : CYP : capital letters indicating the human enzyme 3 : numeral indicating the family number A : capital letter indicating the subfamily 4 : numeral that indicates the isoform number in the subfamily Although they are large in number (hundreds), mainly isoforms of 3 families of CYP-450 are important for drug metabolism in man
55 CYP450 is composed of many families of isoenzymes known as isoforms Six isoforms are responsible for the vast majority of CYP450-catalyzed reactions: CYP3A4, CYP2D6, CYP2C9/10, CYP2C19, CYP2E1, and CYP1A2 Variability in the activity of CYP450 enzymes is linked to a range of factors including genetic, environmental, and developmental
56 Lead to the formation of a covalent linkage between a functional group on the parent compound or phase I metabolite and endogenously derived glucuronic acid, sulfate, glutathione, amino acids, or acetate The highly polar conjugates generally are inactive and are excreted rapidly in the urine and feces Nenates are deficient in this conjugation system, making them particularly vulnerable to drugs such as cholamphenicol (gray baby syndrome)
57 Excretion of drugs means the transportation of unaltered or altered form of drug out of the body. The major processes of excretion include renal excretion, hepatobiliary excretion and pulmonary excretion. The minor routes of excretion are saliva, sweat, tears, breast milk, vaginal fluid, nails and hair. The rate of excretion influences the duration of action of drug. The drug that is excreted slowly, the concentration of drug in the body is maintained and the effects of the drug will continue for longer period.




58 Is the elimination of drugs from the body 58


59 The main PK parameter describing elimination. It is the most important concept to consider when designing a rational regimen for long-term drug administration. Drug clearance from the organ of elimination can be described as: Q: blood flow to the organ of elimination ER: Extraction ratio CpA: arterial drug concentration CpV: venous drug concentration
60 Total body (systemic) clearance,cltotal, is the sum of the clearance from various drug metabolizing (mainly the liver) and drug excreting organs (mainly the kidney) [Additive process]: CLtotal = CLhepatic + Clrenal + CLpulmonary + Clother Units of clearance are volume/time (e.g. L/h or ml/min)
It the process by which a drug reversibly leaves blood and enter interstitium (extracellular fluid) and/ or cells of tissues.
 and/ or cells of tissues.") It the process by which a drug reversibly leaves blood and enter interstitium (extracellular fluid) and/ or cells of tissues. Primarily depends on: 1.Regional blood flow. 2.Capillary permeability. 3.Protein
It the process by which a drug reversibly leaves blood and enter interstitium (extracellular fluid) and/ or cells of tissues. Primarily depends on: 1.Regional blood flow. 2.Capillary permeability. 3.Protein
Pharmacokinetics of Drugs. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Pharmacokinetics of Drugs Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Absorption Is the transfer of a drug from its site of administration to the bloodstream.
Pharmacokinetics of Drugs Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Absorption Is the transfer of a drug from its site of administration to the bloodstream.
Industrial Toxicology
 Industrial Toxicology Learning Objectives Know the assumptions of the doseresponse and time-course curves Be able to define and label key points of a curve Know the difference between potency and efficacy
Industrial Toxicology Learning Objectives Know the assumptions of the doseresponse and time-course curves Be able to define and label key points of a curve Know the difference between potency and efficacy
WHY... 8/21/2013 LEARNING OUTCOMES PHARMACOKINETICS I. A Absorption. D Distribution DEFINITION ADME AND THERAPEUIC ACTION
 PHARMACOKINETICS I Absorption & Distribution LEARNING OUTCOMES By the end of the lecture students will be able to.. Dr Ruwan Parakramawansha MBBS, MD, MRCP(UK),MRCPE, DMT(UK) (2013/08/21) Define pharmacokinetics,
PHARMACOKINETICS I Absorption & Distribution LEARNING OUTCOMES By the end of the lecture students will be able to.. Dr Ruwan Parakramawansha MBBS, MD, MRCP(UK),MRCPE, DMT(UK) (2013/08/21) Define pharmacokinetics,
Chapter 4. Drug Biotransformation
 Chapter 4 Drug Biotransformation Drug Biotransformation 1 Why is drug biotransformation necessary 2 The role of biotransformation in drug disposition 3 Where do drug biotransformation occur 4 The enzymes
Chapter 4 Drug Biotransformation Drug Biotransformation 1 Why is drug biotransformation necessary 2 The role of biotransformation in drug disposition 3 Where do drug biotransformation occur 4 The enzymes
Unit 2b: EXCRETION OF DRUGS. Ms.M.Gayathri Mpharm (PhD) Department of Pharmaceutics Krishna Teja Pharmacy college Subject code: 15R00603 (BPPK)
 Department of Pharmaceutics Krishna Teja Pharmacy college Subject code: 15R00603 (BPPK)") Unit 2b: EXCRETION OF DRUGS By Ms.M.Gayathri Mpharm (PhD) Department of Pharmaceutics Krishna Teja Pharmacy college Subject code: 15R00603 (BPPK) Excretion, along with metabolism and tissue redistribution,
Unit 2b: EXCRETION OF DRUGS By Ms.M.Gayathri Mpharm (PhD) Department of Pharmaceutics Krishna Teja Pharmacy college Subject code: 15R00603 (BPPK) Excretion, along with metabolism and tissue redistribution,
Define the terms biopharmaceutics and bioavailability.
 Pharmaceutics Reading Notes Define the terms biopharmaceutics and bioavailability. Biopharmaceutics: the area of study concerning the relationship between the physical, chemical, and biological sciences
Pharmaceutics Reading Notes Define the terms biopharmaceutics and bioavailability. Biopharmaceutics: the area of study concerning the relationship between the physical, chemical, and biological sciences
Pharmacokinetics. Karim Rafaat
 Pharmacokinetics Karim Rafaat Pharmacokinetics The therapeutic effect of a drug is determined by the concentration of drug at the receptor site of action. Even though the concentration of drug that reaches
Pharmacokinetics Karim Rafaat Pharmacokinetics The therapeutic effect of a drug is determined by the concentration of drug at the receptor site of action. Even though the concentration of drug that reaches
INTRODUCTION TO PHARMACOKINETICS
 INTRODUCTION TO PHARMACOKINETICS 1 http://www.biology.iupui.edu/biocourses/biol540/4pipeline2css.html 2 PHARMACOKINETICS 1. ABSORPTION 2. DISTRIBUTION 3. METABOLISM 4. EXCRETION ALL THESE PROCESSES ARE
INTRODUCTION TO PHARMACOKINETICS 1 http://www.biology.iupui.edu/biocourses/biol540/4pipeline2css.html 2 PHARMACOKINETICS 1. ABSORPTION 2. DISTRIBUTION 3. METABOLISM 4. EXCRETION ALL THESE PROCESSES ARE
Determination of bioavailability
 Pharmaceutics 2 Bioavailability Bioavailability is the rate and extent to which an administered drug reaches the systemic circulation. For example, if 100 mg of a drug is administered orally and 70 mg
Pharmaceutics 2 Bioavailability Bioavailability is the rate and extent to which an administered drug reaches the systemic circulation. For example, if 100 mg of a drug is administered orally and 70 mg
Introduction to. Pharmacokinetics. University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 Introduction to 1 Pharmacokinetics University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 2 Learning objectives Understand compartment models and how they effects
Introduction to 1 Pharmacokinetics University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 2 Learning objectives Understand compartment models and how they effects
2- Minimum toxic concentration (MTC): The drug concentration needed to just produce a toxic effect.
: The drug concentration needed to just produce a toxic effect.") BIOPHARMACEUTICS Drug Product Performance Parameters: 1- Minimum effective concentration (MEC): The minimum concentration of drug needed at the receptors to produce the desired pharmacologic effect. 2-
BIOPHARMACEUTICS Drug Product Performance Parameters: 1- Minimum effective concentration (MEC): The minimum concentration of drug needed at the receptors to produce the desired pharmacologic effect. 2-
Pharmacokinetics in Drug Development. Edward P. Acosta, PharmD Professor & Director Division of Clinical Pharmacology Director, CCC PK/PD Core
 Pharmacokinetics in Drug Development Edward P. Acosta, PharmD Professor & Director Division of Clinical Pharmacology Director, CCC PK/PD Core Finding new drugs: A crap shoot Clinical Development Phase
Pharmacokinetics in Drug Development Edward P. Acosta, PharmD Professor & Director Division of Clinical Pharmacology Director, CCC PK/PD Core Finding new drugs: A crap shoot Clinical Development Phase
Pharmacokinetics Dr. Iman Lec. 3
 Pharmacokinetics r. Iman Lec. 3 Pharmacokinetics A dequate drug doses must be delivered to the target organ to get therapeutic but not toxic levels. So, pharmacokinetic examines the movement of drug over
Pharmacokinetics r. Iman Lec. 3 Pharmacokinetics A dequate drug doses must be delivered to the target organ to get therapeutic but not toxic levels. So, pharmacokinetic examines the movement of drug over
Many drugs have both lipophilic and hydrophilic chemical substituents. Those drugs that are more lipid soluble tend to traverse cell membranes more
 Lecture-4 Many drugs have both lipophilic and hydrophilic chemical substituents. Those drugs that are more lipid soluble tend to traverse cell membranes more easily than less lipid-soluble or more water-soluble
Lecture-4 Many drugs have both lipophilic and hydrophilic chemical substituents. Those drugs that are more lipid soluble tend to traverse cell membranes more easily than less lipid-soluble or more water-soluble
Pharmacokinetics I. Dr. M.Mothilal Assistant professor
 Pharmacokinetics I Dr. M.Mothilal Assistant professor DRUG TRANSPORT For a drug to produce a therapeutic effect, it must reach to its target and it must accumulate at that site to reach to the minimum
Pharmacokinetics I Dr. M.Mothilal Assistant professor DRUG TRANSPORT For a drug to produce a therapeutic effect, it must reach to its target and it must accumulate at that site to reach to the minimum
Excretion of Drugs. Prof. Hanan Hagar Pharmacology Unit Medical College
 Excretion of Drugs Prof. Hanan Hagar Pharmacology Unit Medical College Excretion of Drugs By the end of this lecture, students should be able to! Identify main and minor routes of excretion including renal
Excretion of Drugs Prof. Hanan Hagar Pharmacology Unit Medical College Excretion of Drugs By the end of this lecture, students should be able to! Identify main and minor routes of excretion including renal
Renal Disease and PK/PD. Anjay Rastogi MD PhD Division of Nephrology
 Renal Disease and PK/PD Anjay Rastogi MD PhD Division of Nephrology Drugs and Kidneys Kidney is one of the major organ of drug elimination from the human body Renal disease and dialysis alters the pharmacokinetics
Renal Disease and PK/PD Anjay Rastogi MD PhD Division of Nephrology Drugs and Kidneys Kidney is one of the major organ of drug elimination from the human body Renal disease and dialysis alters the pharmacokinetics
Drug Distribution. Joseph K. Ritter, Ph.D., Assoc. Prof. Medical Sciences Building, Room
 Drug Distribution Joseph K. Ritter, Ph.D., Assoc. Prof. Medical Sciences Building, Room 531 jkritter@vcu.edu 828-1022 Department of Pharmacology and Toxicology Medical College of Virginia Campus Virginia
Drug Distribution Joseph K. Ritter, Ph.D., Assoc. Prof. Medical Sciences Building, Room 531 jkritter@vcu.edu 828-1022 Department of Pharmacology and Toxicology Medical College of Virginia Campus Virginia
Renal Excretion of Drugs
 Renal Excretion of Drugs 3 1 Objectives : 1 Identify main and minor routes of Excretion including renal elimination and biliary excretion 2 Describe its consequences on duration of drugs. For better understanding:
Renal Excretion of Drugs 3 1 Objectives : 1 Identify main and minor routes of Excretion including renal elimination and biliary excretion 2 Describe its consequences on duration of drugs. For better understanding:
Fundamentals of Pharmacology for Veterinary Technicians Chapter 4
 (A) (B) Figure 4-1 A, B (C) FIGURE 4-1C The active transport process moves particles against the concentration gradient from a region of low concentration to a region of high concentration. Active transport
(A) (B) Figure 4-1 A, B (C) FIGURE 4-1C The active transport process moves particles against the concentration gradient from a region of low concentration to a region of high concentration. Active transport
ENVIRONMENTAL TOXICOLOGY
 ENVIRONMENTAL TOXICOLOGY Chapter 4 Toxicokinetics Mohd Amir Bin Arshad Toxicokinetics study on how a substance gets into the body and what happens to it in the body" The kinetics (movement) of substances
ENVIRONMENTAL TOXICOLOGY Chapter 4 Toxicokinetics Mohd Amir Bin Arshad Toxicokinetics study on how a substance gets into the body and what happens to it in the body" The kinetics (movement) of substances
Assem Al Refaei. Sameer Emeish. Dr.Alia. Hodaifa Ababneh & Abdullah Shurafa
 8 Assem Al Refaei Sameer Emeish Hodaifa Ababneh & Abdullah Shurafa Dr.Alia Sheet Checklist Bioequivalence and Therapeutic equivalence. Factors Influencing Absorption. Revising Bioavailability. Factors
8 Assem Al Refaei Sameer Emeish Hodaifa Ababneh & Abdullah Shurafa Dr.Alia Sheet Checklist Bioequivalence and Therapeutic equivalence. Factors Influencing Absorption. Revising Bioavailability. Factors
Basic Concepts in Pharmacokinetics. Leon Aarons Manchester Pharmacy School University of Manchester
 Basic Concepts in Pharmacokinetics Leon Aarons Manchester Pharmacy School University of Manchester Objectives 1. Define pharmacokinetics 2. Describe absorption 3. Describe distribution 4. Describe elimination
Basic Concepts in Pharmacokinetics Leon Aarons Manchester Pharmacy School University of Manchester Objectives 1. Define pharmacokinetics 2. Describe absorption 3. Describe distribution 4. Describe elimination
Pharmacodynamics & Pharmacokinetics 1
 PCTH 325 Pharmacodynamics & Pharmacokinetics 1 Dr. Shabbits jennifer.shabbits@ubc.ca September 9, 2014 Learning objectives 1. Describe the categories of intended drug action 2. Compare and contrast agonists
PCTH 325 Pharmacodynamics & Pharmacokinetics 1 Dr. Shabbits jennifer.shabbits@ubc.ca September 9, 2014 Learning objectives 1. Describe the categories of intended drug action 2. Compare and contrast agonists
Toxicant Disposition and Metabolism. Jan Chambers Center for Environmental Health Sciences College of Veterinary Medicine
 Toxicant Disposition and Metabolism Jan Chambers Center for Environmental Health Sciences College of Veterinary Medicine chambers@cvm.msstate.edu Definitions Disposition Absorption passage across membrane.
Toxicant Disposition and Metabolism Jan Chambers Center for Environmental Health Sciences College of Veterinary Medicine chambers@cvm.msstate.edu Definitions Disposition Absorption passage across membrane.
ADME Review. Dr. Joe Ritter Associate Professor of Pharmacology
 ADME Review Dr. Joe Ritter Associate Professor of Pharmacology 828-1022 jkritter@vcu.edu What percent of a weak base (pka = 7.5) and weak acid (pka = 3.5) will be respectively ionized in urine of ph 5.5?
ADME Review Dr. Joe Ritter Associate Professor of Pharmacology 828-1022 jkritter@vcu.edu What percent of a weak base (pka = 7.5) and weak acid (pka = 3.5) will be respectively ionized in urine of ph 5.5?
DRUG DISTRIBUTION. Distribution Blood Brain Barrier Protein Binding
 DRUG DISTRIBUTION Distribution Blood Brain Barrier Protein Binding DRUG DISTRIBUTION Drug distribution is a reversible transport of drug through the body by the systemic circulation The drug molecules
DRUG DISTRIBUTION Distribution Blood Brain Barrier Protein Binding DRUG DISTRIBUTION Drug distribution is a reversible transport of drug through the body by the systemic circulation The drug molecules
Principles of Drug Action. Intro to Pharmacology: Principles of Courework Drug Action Intro to Pharmacology
 Principles of Drug Action Intro to Pharmacology: Principles of Courework 102.3 Drug Action Intro to Pharmacology Directions Read the PPT and complete R.E.A.D. Assignment. There are videos embedded within
Principles of Drug Action Intro to Pharmacology: Principles of Courework 102.3 Drug Action Intro to Pharmacology Directions Read the PPT and complete R.E.A.D. Assignment. There are videos embedded within
UNIVERSITY OF THE WEST INDIES, ST AUGUSTINE
 UNIVERSITY OF THE WEST INDIES, ST AUGUSTINE FACULTY OF MEDICAL SCIENCES SCHOOL OF PHARMACY BACHELOR OF SCIENCE IN PHARMACY DEGREE COURSE SYLLABUS COURSE TITLE: COURSE CODE: BIOPHARMACEUTICS, NEW DRUG DELIVERY
UNIVERSITY OF THE WEST INDIES, ST AUGUSTINE FACULTY OF MEDICAL SCIENCES SCHOOL OF PHARMACY BACHELOR OF SCIENCE IN PHARMACY DEGREE COURSE SYLLABUS COURSE TITLE: COURSE CODE: BIOPHARMACEUTICS, NEW DRUG DELIVERY
BASIC PHARMACOKINETICS
 BASIC PHARMACOKINETICS MOHSEN A. HEDAYA CRC Press Taylor & Francis Croup Boca Raton London New York CRC Press is an imprint of the Taylor & Francis Group, an informa business Table of Contents Chapter
BASIC PHARMACOKINETICS MOHSEN A. HEDAYA CRC Press Taylor & Francis Croup Boca Raton London New York CRC Press is an imprint of the Taylor & Francis Group, an informa business Table of Contents Chapter
B. Incorrect! Compounds are made more polar, to increase their excretion.
 Pharmacology - Problem Drill 04: Biotransformation Question No. 1 of 10 Instructions: (1) Read the problem and answer choices carefully, (2) Work the problems on paper as 1. What is biotransformation?
Pharmacology - Problem Drill 04: Biotransformation Question No. 1 of 10 Instructions: (1) Read the problem and answer choices carefully, (2) Work the problems on paper as 1. What is biotransformation?
TOXICOKINETICS; DISPOSITION OF XENOBIOTICS (Absorption, Distribution and Excretion of xenobiotics)
") TOXICOKINETICS; DISPOSITION OF XENOBIOTICS (Absorption, Distribution and Excretion of xenobiotics) Benay Can Eke, Ph.D., ERT Professor of Toxicology Department of Toxicology Faculty of Pharmacy Ankara
TOXICOKINETICS; DISPOSITION OF XENOBIOTICS (Absorption, Distribution and Excretion of xenobiotics) Benay Can Eke, Ph.D., ERT Professor of Toxicology Department of Toxicology Faculty of Pharmacy Ankara
Chapter Questions. Modern Pharmacology With Clinical Applications. Sixth Edition
 Chapter Questions Modern Pharmacology With Clinical Applications Sixth Edition Mechanism of Drug Action Questions 1. Receptors are macromolecules that a. Are designed to attract drugs b. Are resistant
Chapter Questions Modern Pharmacology With Clinical Applications Sixth Edition Mechanism of Drug Action Questions 1. Receptors are macromolecules that a. Are designed to attract drugs b. Are resistant
Section 5.2: Pharmacokinetic properties
 Section 5.2: Pharmacokinetic properties SmPC training presentation Note: for full information refer to the European Commission s Guideline on summary of product characteristics (SmPC) SmPC Advisory Group
Section 5.2: Pharmacokinetic properties SmPC training presentation Note: for full information refer to the European Commission s Guideline on summary of product characteristics (SmPC) SmPC Advisory Group
Pharmacokinetic Phase
 RSPT 2317 Principles of Drug Action Part 2: The Pharmacokinetic Phase Pharmacokinetic Phase This phase describes the time course and disposition of a drug in the body, based on its absorption, distribution,
RSPT 2317 Principles of Drug Action Part 2: The Pharmacokinetic Phase Pharmacokinetic Phase This phase describes the time course and disposition of a drug in the body, based on its absorption, distribution,
Drug Dosing in Renal Insufficiency. Coralie Therese D. Dimacali, MD College of Medicine University of the Philippines Manila
 Drug Dosing in Renal Insufficiency Coralie Therese D. Dimacali, MD College of Medicine University of the Philippines Manila Declaration of Conflict of Interest For today s lecture on Drug Dosing in Renal
Drug Dosing in Renal Insufficiency Coralie Therese D. Dimacali, MD College of Medicine University of the Philippines Manila Declaration of Conflict of Interest For today s lecture on Drug Dosing in Renal
Slide 1. Slide 2. Slide 3. Drug Action and Handling. Lesson 2.1. Lesson 2.1. Drug Action and Handling. Drug Action and Handling.
 Slide 1 Drug Action and Handling Chapter 2 1 Slide 2 Lesson 2.1 Drug Action and Handling 1. Differentiate dose, potency, and efficacy in the context of the actions of drugs. 2. Explain the pharmacologic
Slide 1 Drug Action and Handling Chapter 2 1 Slide 2 Lesson 2.1 Drug Action and Handling 1. Differentiate dose, potency, and efficacy in the context of the actions of drugs. 2. Explain the pharmacologic
Pharmacokinetics Metabolism
 Pharmacokinetics Metabolism Learning object Know the processes involved in ADME of drugs Know how these processes may affect the action of xenobiotics Appreciate how these processes can affect the outcome
Pharmacokinetics Metabolism Learning object Know the processes involved in ADME of drugs Know how these processes may affect the action of xenobiotics Appreciate how these processes can affect the outcome
The ADME properties of most drugs strongly depends on the ability of the drug to pass through membranes via simple diffusion.
 1 MEDCHEM 562 Kent Kunze Lecture 1 Physicochemical Properties and Drug Disposition The ADME properties of most drugs strongly depends on the ability of the drug to pass through membranes via simple diffusion.
1 MEDCHEM 562 Kent Kunze Lecture 1 Physicochemical Properties and Drug Disposition The ADME properties of most drugs strongly depends on the ability of the drug to pass through membranes via simple diffusion.
Chapter 3 Drug Absorption and Bioavailability
 Chapter 3 Drug Absorption and Bioavailability Debra Si Mui Sim Abstract Most drugs are prescribed as oral preparations or extravascular injections (other than intravenous injections) for the treatment
Chapter 3 Drug Absorption and Bioavailability Debra Si Mui Sim Abstract Most drugs are prescribed as oral preparations or extravascular injections (other than intravenous injections) for the treatment
Chimica Farmaceutica. Pharmacokinetics and related topics
 Chimica Farmaceutica Pharmacokinetics and related topics INTRODUCTION In order to produce its intended effect, a drug must be present at an appropriate concentration in the fluid surrounding the effect
Chimica Farmaceutica Pharmacokinetics and related topics INTRODUCTION In order to produce its intended effect, a drug must be present at an appropriate concentration in the fluid surrounding the effect
DEPARTMENT OF PHARMACOLOGY AND THERAPEUTIC UNIVERSITAS SUMATERA UTARA
 METABOLISME dr. Yunita Sari Pane DEPARTMENT OF PHARMACOLOGY AND THERAPEUTIC UNIVERSITAS SUMATERA UTARA Pharmacokinetic absorption distribution BIOTRANSFORMATION elimination Intravenous Administration Oral
METABOLISME dr. Yunita Sari Pane DEPARTMENT OF PHARMACOLOGY AND THERAPEUTIC UNIVERSITAS SUMATERA UTARA Pharmacokinetic absorption distribution BIOTRANSFORMATION elimination Intravenous Administration Oral
Principles of Toxicology: The Study of Poisons
 Principles of Toxicology: The Study of Poisons Elizabeth Casarez Department of Pharmacology and Toxicology University it of Arizona The study of the adverse effects of a toxicant on living organisms Adverse
Principles of Toxicology: The Study of Poisons Elizabeth Casarez Department of Pharmacology and Toxicology University it of Arizona The study of the adverse effects of a toxicant on living organisms Adverse
Chapter 1. Introduction
 Chapter 1 Introduction What is Pharmacology From the Greek pharmakon (=drug), logos (=study) Pharmacology is the science that deals with the mechanisms of action, uses, adverse effects and fate of drugs
Chapter 1 Introduction What is Pharmacology From the Greek pharmakon (=drug), logos (=study) Pharmacology is the science that deals with the mechanisms of action, uses, adverse effects and fate of drugs
Metabolic Changes of Drugs and Related Organic Compounds
 Metabolic Changes of Drugs and Related Organic Compounds 3 rd stage/ 1 st course Lecture 3 Shokhan J. Hamid 2 Metabolism plays a central role in the elimination of drugs and other foreign compounds from
Metabolic Changes of Drugs and Related Organic Compounds 3 rd stage/ 1 st course Lecture 3 Shokhan J. Hamid 2 Metabolism plays a central role in the elimination of drugs and other foreign compounds from
METABOLISM. Ali Alhoshani, B.Pharm, Ph.D. Office: 2B 84
 METABOLISM Ali Alhoshani, B.Pharm, Ph.D. ahoshani@ksu.edu.sa Office: 2B 84 Metabolism By the end of this lecture, you should: Recognize the importance of biotransformation Know the different sites for
METABOLISM Ali Alhoshani, B.Pharm, Ph.D. ahoshani@ksu.edu.sa Office: 2B 84 Metabolism By the end of this lecture, you should: Recognize the importance of biotransformation Know the different sites for
Problem Set for Fundamentals 9 Oct 2013
 20.201 Problem Set for Fundamentals 9 ct 2013 Please prepare your answers in electronic format and submit the answers or on ctober 11. While this is not a graded problem set, you will get cr completing
20.201 Problem Set for Fundamentals 9 ct 2013 Please prepare your answers in electronic format and submit the answers or on ctober 11. While this is not a graded problem set, you will get cr completing
Pharmacokinetic Phase
 RSPT 2217 Principles of Drug Action Part 2: The Pharmacokinetic Phase Gardenhire Chapter 2; p. 14-25 From the Text Common Pathways for Drug Box 2-3; page 18 Plasma Half-lives of Common Drugs Table 2-4;
RSPT 2217 Principles of Drug Action Part 2: The Pharmacokinetic Phase Gardenhire Chapter 2; p. 14-25 From the Text Common Pathways for Drug Box 2-3; page 18 Plasma Half-lives of Common Drugs Table 2-4;
Pharmacokinetics in the critically ill. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 Pharmacokinetics in the critically ill Intensive Care Training Program Radboud University Medical Centre Nijmegen In general... Critically ill patients are at higher risk for ADE s and more severe ADE
Pharmacokinetics in the critically ill Intensive Care Training Program Radboud University Medical Centre Nijmegen In general... Critically ill patients are at higher risk for ADE s and more severe ADE
BIOPHARMACEUTICS and CLINICAL PHARMACY
 11 years papers covered BIOPHARMACEUTICS and CLINICAL PHARMACY IV B.Pharm II Semester, Andhra University Topics: Absorption Distribution Protein binding Metabolism Excretion Bioavailability Drug Interactions
11 years papers covered BIOPHARMACEUTICS and CLINICAL PHARMACY IV B.Pharm II Semester, Andhra University Topics: Absorption Distribution Protein binding Metabolism Excretion Bioavailability Drug Interactions
Click to edit Master title style
 A Short Course in Pharmacokinetics Chris Town Research Pharmacokinetics Outline Pharmacokinetics - Definition Ideal Pharmacokinetic Parameters of a New Drug How do we optimize PK for new compounds Why
A Short Course in Pharmacokinetics Chris Town Research Pharmacokinetics Outline Pharmacokinetics - Definition Ideal Pharmacokinetic Parameters of a New Drug How do we optimize PK for new compounds Why
Pharmacokinetics Prepared by: Prof. Abusufyan
 Pharmacokinetics Prepared by: Prof. Abusufyan Learning Object Know the processes involved in ADME of drugs Know how these processes may affect the action of xenobiotics Appreciate how these processes can
Pharmacokinetics Prepared by: Prof. Abusufyan Learning Object Know the processes involved in ADME of drugs Know how these processes may affect the action of xenobiotics Appreciate how these processes can
PHARMACOKINETICS SMALL GROUP I:
 PHARMACOKINETICS SMALL GROUP I: Question 1 Absorption of the anti-fungal agent, itraconazole, is dependent on a low gastric ph. Calculate the relative concentrations of a weak acid (with a pka of 5.4)
PHARMACOKINETICS SMALL GROUP I: Question 1 Absorption of the anti-fungal agent, itraconazole, is dependent on a low gastric ph. Calculate the relative concentrations of a weak acid (with a pka of 5.4)
Introduction to. Pharmacokinetics. University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 Introduction to 1 Pharmacokinetics University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 2 Learning objectives Understand compartment models and how they effects
Introduction to 1 Pharmacokinetics University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 2 Learning objectives Understand compartment models and how they effects
Introduction to Pharmacokinetics (PK) Anson K. Abraham, Ph.D. Associate Principal Scientist, PPDM- QP2 Merck & Co. Inc., West Point, PA 5- June- 2017
 Anson K. Abraham, Ph.D. Associate Principal Scientist, PPDM- QP2 Merck & Co. Inc., West Point, PA 5- June- 2017") Introduction to Pharmacokinetics (PK) Anson K. Abraham, Ph.D. Associate Principal Scientist, PPDM- QP2 Merck & Co. Inc., West Point, PA 5- June- 2017 1 Outline Definition & Relevance of Pharmacokinetics
Introduction to Pharmacokinetics (PK) Anson K. Abraham, Ph.D. Associate Principal Scientist, PPDM- QP2 Merck & Co. Inc., West Point, PA 5- June- 2017 1 Outline Definition & Relevance of Pharmacokinetics
Model Answer B.Pharm. VII sem, Examination 2013 Biopharmaceutics and Pharmacokinetics Paper code: AS-2532
 Section A: Short Answer Model Answer B.Pharm. VII sem, Examination 2013 Biopharmaceutics and Pharmacokinetics Paper code: AS-2532 1. i) Objective of bioavailability studies Primary stages of development
Section A: Short Answer Model Answer B.Pharm. VII sem, Examination 2013 Biopharmaceutics and Pharmacokinetics Paper code: AS-2532 1. i) Objective of bioavailability studies Primary stages of development
Lippincott Questions Pharmacology
 Lippincott Questions Pharmacology Edition Two: Chapter One: 1.Which one of the following statements is CORRECT? A. Weak bases are absorbed efficiently across the epithelial cells of the stomach. B. Coadministration
Lippincott Questions Pharmacology Edition Two: Chapter One: 1.Which one of the following statements is CORRECT? A. Weak bases are absorbed efficiently across the epithelial cells of the stomach. B. Coadministration
Introduction to Pharmacokinetics
 - 1 - Introduction to Pharmacokinetics Outline accompanies required webcast for Marie Biancuzzo s Lactation Exam Review and Marie Biancuzzo s Comprehensive Lactation Course Notes We will not cover this
- 1 - Introduction to Pharmacokinetics Outline accompanies required webcast for Marie Biancuzzo s Lactation Exam Review and Marie Biancuzzo s Comprehensive Lactation Course Notes We will not cover this
Drug elimination and Hepatic clearance Chapter 6
 Drug elimination and Hepatic clearance Chapter 6 DRUG ELIMINATION Drugs are removed from the body by various elimination processes. Drug elimination refers to the irreversible removal of drug from the
Drug elimination and Hepatic clearance Chapter 6 DRUG ELIMINATION Drugs are removed from the body by various elimination processes. Drug elimination refers to the irreversible removal of drug from the
PRESCRIBING IN LIVER AND RENAL DISEASE
 THERAPEUTICS FOR INDEPENDENT PRESCRIBERS PRESCRIBING IN LIVER AND RENAL DISEASE Number 6 in a series of 15 articles on Therapeutics Aims and Objectives To outline the pathophysiological changes that occur
THERAPEUTICS FOR INDEPENDENT PRESCRIBERS PRESCRIBING IN LIVER AND RENAL DISEASE Number 6 in a series of 15 articles on Therapeutics Aims and Objectives To outline the pathophysiological changes that occur
Lecture 1: Physicochemical Properties of Drugs and Drug Disposition
 Lecture 1: Physicochemical Properties of Drugs and Drug Disposition Key objectives: 1. Be able to explain the benefits of oral versus IV drug administration 2. Be able to explain the factors involved in
Lecture 1: Physicochemical Properties of Drugs and Drug Disposition Key objectives: 1. Be able to explain the benefits of oral versus IV drug administration 2. Be able to explain the factors involved in
EVE 491/591 Toxicology. Toxicant Distribution 2/20/2014
 EVE 491/591 Toxicology Lecture #8 1. Distribution, Storage, Elimination, and Biotransformation of Toxicants 2. Case study #2 Part II Toxicant Distribution Distribution: the process in which a chemical
EVE 491/591 Toxicology Lecture #8 1. Distribution, Storage, Elimination, and Biotransformation of Toxicants 2. Case study #2 Part II Toxicant Distribution Distribution: the process in which a chemical
Renal Function. 1. Glomerular filtration 2. Active tubular secretion 3. Passive tubular reabsorption 4. Excretion
 59-291 Section 1, Lecture 5 Drug Excretion -most drugs are excreted in urine either as unchanged or drug metabolites Renal Function 1. Glomerular filtration 2. Active tubular secretion 3. Passive tubular
59-291 Section 1, Lecture 5 Drug Excretion -most drugs are excreted in urine either as unchanged or drug metabolites Renal Function 1. Glomerular filtration 2. Active tubular secretion 3. Passive tubular
Is the science that study relation of physicochemical properties of drug, dosage form, & route of administration on rate and extent of drug
 Chapter 5 Is the science that study relation of physicochemical properties of drug, dosage form, & route of administration on rate and extent of drug absorption. It is the study of the kinetics of absorption,
Chapter 5 Is the science that study relation of physicochemical properties of drug, dosage form, & route of administration on rate and extent of drug absorption. It is the study of the kinetics of absorption,
Pharmacokinetics of strong opioids. Susan Addie Specialist palliative care pharmacist
 Pharmacokinetics of strong opioids Susan Addie Specialist palliative care pharmacist What is the difference between pharmacokinetics and pharmacodynamics? Definitions Pharmacokinetics = what the body does
Pharmacokinetics of strong opioids Susan Addie Specialist palliative care pharmacist What is the difference between pharmacokinetics and pharmacodynamics? Definitions Pharmacokinetics = what the body does
1. Gastric Emptying Time Anatomically, a swallowed drug rapidly reaches the stomach. Eventually, the stomach empties its content in the small
 Lecture-5 1. Gastric Emptying Time Anatomically, a swallowed drug rapidly reaches the stomach. Eventually, the stomach empties its content in the small intestine. Because the duodenum has the greatest
Lecture-5 1. Gastric Emptying Time Anatomically, a swallowed drug rapidly reaches the stomach. Eventually, the stomach empties its content in the small intestine. Because the duodenum has the greatest
2. List routes of exposure in the order of most rapid response.
 Practice Test questions: 1. What are the two areas of toxicology that a regulatory toxicologist must integrate in order to determine the "safety" of any chemical? 2. List routes of exposure in the order
Practice Test questions: 1. What are the two areas of toxicology that a regulatory toxicologist must integrate in order to determine the "safety" of any chemical? 2. List routes of exposure in the order
Rational Dose Prediction. Pharmacology. φαρμακον. What does this mean? pharmakon. Medicine Poison Magic Spell
 1 Rational Dose Prediction Nick Holford Dept Pharmacology & Clinical Pharmacology University of Auckland, New Zealand 2 Pharmacology Pharmacology is derived from a Greek word (pharmakon). The Greeks used
1 Rational Dose Prediction Nick Holford Dept Pharmacology & Clinical Pharmacology University of Auckland, New Zealand 2 Pharmacology Pharmacology is derived from a Greek word (pharmakon). The Greeks used
General Pharmacology
 General Pharmacology (Pharmacokinetic III) Principles of Pharmacology (PP VII) Dr. Ahmad Al-Zohyri Dept. of Pharmacology Baghdad College of Medicine References: Basic & clinical pharmacology by Katzung
General Pharmacology (Pharmacokinetic III) Principles of Pharmacology (PP VII) Dr. Ahmad Al-Zohyri Dept. of Pharmacology Baghdad College of Medicine References: Basic & clinical pharmacology by Katzung
Metabolic Changes of Drugs and Related Organic Compounds
 Metabolic Changes of Drugs and Related Organic Compounds 3 rd stage/ 1 st course Lecture 7 Shokhan J. Hamid 1 Phase II or Conjugation Reactions Phase I or functionalization reactions do not always produce
Metabolic Changes of Drugs and Related Organic Compounds 3 rd stage/ 1 st course Lecture 7 Shokhan J. Hamid 1 Phase II or Conjugation Reactions Phase I or functionalization reactions do not always produce
PHARMACOLOGY-1 PHL-313. Ali Alhoshani Office: 2B 84
 PHARMACOLOGY-1 PHL-313 Ali Alhoshani ahoshani@ksu.edu.sa http://fac.ksu.edu.sa/ahoshani Office: 2B 84 General rules Reference: General rules Email [PHL313-1 st Semester 38-39] Student ID- Question Example
PHARMACOLOGY-1 PHL-313 Ali Alhoshani ahoshani@ksu.edu.sa http://fac.ksu.edu.sa/ahoshani Office: 2B 84 General rules Reference: General rules Email [PHL313-1 st Semester 38-39] Student ID- Question Example
Drug dosing in Extremes of Weight
 Drug dosing in Extremes of Weight The Plump & Heavy versus The Skinny & Light Maria Minerva P. Calimag, MD, MSc, PhD, DPBA, FPSECP PROFESSOR Departments of Pharmacology, Anesthesiology and Clinical Epidemiology
Drug dosing in Extremes of Weight The Plump & Heavy versus The Skinny & Light Maria Minerva P. Calimag, MD, MSc, PhD, DPBA, FPSECP PROFESSOR Departments of Pharmacology, Anesthesiology and Clinical Epidemiology
Tamer Barakat. Abdul Aziz ALShamali. Abdul Aziz ALShamali
 10 Tamer Barakat Abdul Aziz ALShamali Abdul Aziz ALShamali Dr. Alia Elimination: Refampin is used to treat TB not malaria (Quinacrine is used for malaria) It s the opposite process of absorption. It's
10 Tamer Barakat Abdul Aziz ALShamali Abdul Aziz ALShamali Dr. Alia Elimination: Refampin is used to treat TB not malaria (Quinacrine is used for malaria) It s the opposite process of absorption. It's
Basic Biopharmaceutics, Pharmacokinetics, and Pharmacodynamics
 Basic Biopharmaceutics, Pharmacokinetics, and Pharmacodynamics Learning Outcomes Define biopharmaceutics Describe 4 processes of pharmacokinetics Describe factors that affect medication absorption Describe
Basic Biopharmaceutics, Pharmacokinetics, and Pharmacodynamics Learning Outcomes Define biopharmaceutics Describe 4 processes of pharmacokinetics Describe factors that affect medication absorption Describe
Biopharmaceutics. Lec: 4
 64 Biopharmaceutics Physicochemical Properties of Drugs Affecting Bioavailability Lec: 4 1 Assist. Lecturer Ali Yaseen Ali BSc Pharmacy MSc Industrial Pharmaceutical Sciences Dept. of Pharmaceutics School
64 Biopharmaceutics Physicochemical Properties of Drugs Affecting Bioavailability Lec: 4 1 Assist. Lecturer Ali Yaseen Ali BSc Pharmacy MSc Industrial Pharmaceutical Sciences Dept. of Pharmaceutics School
Basic Pharmacokinetics and Pharmacodynamics: An Integrated Textbook with Computer Simulations
 Basic Pharmacokinetics and Pharmacodynamics: An Integrated Textbook with Computer Simulations Rosenbaum, Sara E. ISBN-13: 9780470569061 Table of Contents 1 Introduction to Pharmacokinetics and Pharmacodynamics.
Basic Pharmacokinetics and Pharmacodynamics: An Integrated Textbook with Computer Simulations Rosenbaum, Sara E. ISBN-13: 9780470569061 Table of Contents 1 Introduction to Pharmacokinetics and Pharmacodynamics.
PHARMACOKINETICS: DRUG ABSORPTION, DISTRIBUTION, AND ELIMINATION
 CHAPTER 3 PHARMACOKINETICS: DRUG ABSORPTION, DISTRIBUTION, AND ELIMINATION AMANDA J. JENKINS, PH.D. AND EDWARD J. CONE, PH.D. INTRAMURAL RESEARCH PROGRAM, NATIONAL INSTITUTE ON DRUG ABUSE, NATIONAL INSTITUTES
CHAPTER 3 PHARMACOKINETICS: DRUG ABSORPTION, DISTRIBUTION, AND ELIMINATION AMANDA J. JENKINS, PH.D. AND EDWARD J. CONE, PH.D. INTRAMURAL RESEARCH PROGRAM, NATIONAL INSTITUTE ON DRUG ABUSE, NATIONAL INSTITUTES
Tala Saleh. Abdul Aziz ALShamali. Abdul Aziz ALShamali
 9 Tala Saleh Abdul Aziz ALShamali Abdul Aziz ALShamali Alia Shatanawi Volume of Distribution (Vd) Understand the concept Imagine having a container with an unknown volume of water in it. Then 1000mg of
9 Tala Saleh Abdul Aziz ALShamali Abdul Aziz ALShamali Alia Shatanawi Volume of Distribution (Vd) Understand the concept Imagine having a container with an unknown volume of water in it. Then 1000mg of
A primer on pharmacology
 A primer on pharmacology Universidade do Algarve Faro 2017 by Ferdi Engels, Ph.D. 1 2 1 3 Utrecht university campus de Uithof Dept. of Pharmaceutical Sciences Division of Pharmacology 4 2 Bachelor and
A primer on pharmacology Universidade do Algarve Faro 2017 by Ferdi Engels, Ph.D. 1 2 1 3 Utrecht university campus de Uithof Dept. of Pharmaceutical Sciences Division of Pharmacology 4 2 Bachelor and
Biopharmaceutics Dosage form factors influencing bioavailability Lec:5
 Biopharmaceutics Dosage form factors influencing bioavailability Lec:5 Ali Y Ali BSc Pharmacy MSc Industrial Pharmaceutical Sciences Dept. of Pharmaceutics School of Pharmacy University of Sulaimani 09/01/2019
Biopharmaceutics Dosage form factors influencing bioavailability Lec:5 Ali Y Ali BSc Pharmacy MSc Industrial Pharmaceutical Sciences Dept. of Pharmaceutics School of Pharmacy University of Sulaimani 09/01/2019
Definition of bilirubin Bilirubin metabolism
 Definition of bilirubin Bilirubin metabolism obilirubin formation otransport of bilirubin in plasma ohepatic bilirubin transport oexcretion through intestine Other substances conjugated by glucuronyl transferase.
Definition of bilirubin Bilirubin metabolism obilirubin formation otransport of bilirubin in plasma ohepatic bilirubin transport oexcretion through intestine Other substances conjugated by glucuronyl transferase.
D9G : Oro-Mucosal Dosage Forms Development Background Paper
 D9G : Oro-Mucosal Dosage Forms Development Background Paper Introduction This background paper is intended to provide a basic rationale for initial formulation efforts, and define some of the terminology
D9G : Oro-Mucosal Dosage Forms Development Background Paper Introduction This background paper is intended to provide a basic rationale for initial formulation efforts, and define some of the terminology
Name: Class: "Pharmacology NSAIDS (1) Lecture
 Lecture") I Name: Class: "Pharmacology NSAIDS (1) Lecture د. احمد الزهيري Inflammation is triggered by the release of chemical mediators from injured tissues and migrating cells. The specific mediators vary with
I Name: Class: "Pharmacology NSAIDS (1) Lecture د. احمد الزهيري Inflammation is triggered by the release of chemical mediators from injured tissues and migrating cells. The specific mediators vary with
General pharmacology Lecture(3)
") General pharmacology Lecture(3) 2. Specialized transport: It may be: i. Carrier-mediated transport ii. Pinocytosis. i. Carrier-mediated transport: The drug combines with a carrier (a specialized protein
General pharmacology Lecture(3) 2. Specialized transport: It may be: i. Carrier-mediated transport ii. Pinocytosis. i. Carrier-mediated transport: The drug combines with a carrier (a specialized protein
DRUG ELIMINATION II BILIARY EXCRETION MAMMARY, SALIVARY AND PULMONARY EXCRETION
 DRUG ELIMINATION II BILIARY EXCRETION MAMMARY, SALIVARY AND PULMONARY EXCRETION ROUTE OF DRUG ADMINISTRATION AND EXTRAHEPATIC DRUG METABOLISM The decline in plasma concentration after drug administration
DRUG ELIMINATION II BILIARY EXCRETION MAMMARY, SALIVARY AND PULMONARY EXCRETION ROUTE OF DRUG ADMINISTRATION AND EXTRAHEPATIC DRUG METABOLISM The decline in plasma concentration after drug administration
Pharmacokinetics: The Basics
 Pharmacokinetics: The Basics 2017 Otsuka Pharmaceutical Development & Commercialization, Inc., Rockville, MD January 2017 MRC2.CORP.D.00200 1 advice or professional diagnosis. Users seeking medical advice
Pharmacokinetics: The Basics 2017 Otsuka Pharmaceutical Development & Commercialization, Inc., Rockville, MD January 2017 MRC2.CORP.D.00200 1 advice or professional diagnosis. Users seeking medical advice
Helping the liver to detoxify mycotoxins
 Helping the liver to detoxify mycotoxins Mycotoxin strategies have so far focused on binding compounds or detoxifying the compounds by feed additives. Animals however, can also detoxify mycotoxins themselves
Helping the liver to detoxify mycotoxins Mycotoxin strategies have so far focused on binding compounds or detoxifying the compounds by feed additives. Animals however, can also detoxify mycotoxins themselves
RENAL SYSTEM 2 TRANSPORT PROPERTIES OF NEPHRON SEGMENTS Emma Jakoi, Ph.D.
 RENAL SYSTEM 2 TRANSPORT PROPERTIES OF NEPHRON SEGMENTS Emma Jakoi, Ph.D. Learning Objectives 1. Identify the region of the renal tubule in which reabsorption and secretion occur. 2. Describe the cellular
RENAL SYSTEM 2 TRANSPORT PROPERTIES OF NEPHRON SEGMENTS Emma Jakoi, Ph.D. Learning Objectives 1. Identify the region of the renal tubule in which reabsorption and secretion occur. 2. Describe the cellular
Pharmacogenetics and Pharmacokinetics
 Chapter 2 Pharmacogenetics and Pharmacokinetics Mauro Saivezzo/ShutterStock, Inc. L earning O bjectives Upon completion of this chapter, the student will be able to: 1. Recognize the influence of genetic
Chapter 2 Pharmacogenetics and Pharmacokinetics Mauro Saivezzo/ShutterStock, Inc. L earning O bjectives Upon completion of this chapter, the student will be able to: 1. Recognize the influence of genetic
Biopharmaceutics. Tips Worth Tweeting. Contributor: Sandra Earle
 Biopharmaceutics C H A P T E R 2 Contributor: Sandra Earle The physiochemical properties of drugs determine how they will move and interact with the body. By understanding a few principles, predictions
Biopharmaceutics C H A P T E R 2 Contributor: Sandra Earle The physiochemical properties of drugs determine how they will move and interact with the body. By understanding a few principles, predictions
PHA Second Exam. Fall On my honor, I have neither given nor received unauthorized aid in doing this assignment.
 PHA 5127 Second Exam Fall 2012 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Put all answers on the bubble sheet TOTAL /150 pts 1 Question Set I (True or
PHA 5127 Second Exam Fall 2012 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Put all answers on the bubble sheet TOTAL /150 pts 1 Question Set I (True or
The principal functions of the kidneys
 Renal physiology The principal functions of the kidneys Formation and excretion of urine Excretion of waste products, drugs, and toxins Regulation of body water and mineral content of the body Maintenance
Renal physiology The principal functions of the kidneys Formation and excretion of urine Excretion of waste products, drugs, and toxins Regulation of body water and mineral content of the body Maintenance
PHSI2006/2906: Integrated Physiology B
 PHSI2006/2906: Integrated Physiology B TOPIC 1: RESPIRATION 1. The Mechanics of Breathing...2 2. Work of Breathing....5 3. Pulmonary Gas Exchange.. 10 4. Transport of Oxygen...16 5. Control of Respiration...20
PHSI2006/2906: Integrated Physiology B TOPIC 1: RESPIRATION 1. The Mechanics of Breathing...2 2. Work of Breathing....5 3. Pulmonary Gas Exchange.. 10 4. Transport of Oxygen...16 5. Control of Respiration...20
SUMMARY OF PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT
 SUMMARY OF PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT "Carbellon" Tablets. 2. Qualitative and Quantitative Composition Active Constituents: Activated Charcoal Ph.Eur. Magnesium Hydroxide Ph.Eur.
SUMMARY OF PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT "Carbellon" Tablets. 2. Qualitative and Quantitative Composition Active Constituents: Activated Charcoal Ph.Eur. Magnesium Hydroxide Ph.Eur.
Introduction pharmacology and drug administration
 1 Introduction to pharmacology and drug administration INTRODUCTION Pharmacology is the study of drugs or chemicals used to treat and cure disease and their interactions in the body. Within the study of
1 Introduction to pharmacology and drug administration INTRODUCTION Pharmacology is the study of drugs or chemicals used to treat and cure disease and their interactions in the body. Within the study of
Pharmacology Final. 2-Which of the following side effect is not related to atropine?
 Pharmacology Final 1-Which of the following is inhibitory CNS neurotransmitter? a) Acetylcholine b) Dopamine c) Glutamate d) GABA* 2-Which of the following side effect is not related to atropine? a) Dryness
Pharmacology Final 1-Which of the following is inhibitory CNS neurotransmitter? a) Acetylcholine b) Dopamine c) Glutamate d) GABA* 2-Which of the following side effect is not related to atropine? a) Dryness
4-To treat overdose toxicity of acidic drug,you may perform gastric lavage with: a-sodium bicarbonate. b-ascorbic acid c-saline
 Compare between type I and type II adverse drug reaction as regards dose dependency and mechanism.give 2 examples of each type. Define the following terms and mention 3 factors affecting them: Volume of
Compare between type I and type II adverse drug reaction as regards dose dependency and mechanism.give 2 examples of each type. Define the following terms and mention 3 factors affecting them: Volume of
Name: Date: Block: Biology 12
 Name: Date: Block: Biology 12 Provincial Exam Review: Cell Processes and Applications January 2003 Use the following diagram to answer questions 1 and 2. 1. Which labelled organelle produces most of the
Name: Date: Block: Biology 12 Provincial Exam Review: Cell Processes and Applications January 2003 Use the following diagram to answer questions 1 and 2. 1. Which labelled organelle produces most of the