Nutrition. ICU Fellowship Training Radboudumc
|
|
|
- Brian Byrd
- 6 years ago
- Views:
Transcription
1 Nutrition ICU Fellowship Training Radboudumc
2 Critical Care MCQ s Nasogastric (NG) and nasojejunal (NJ) feeding tubes: A. Enteral nutrition is associated with a reduced risk of bacterial and toxin translocation. B. Gastric residual volumes of 200ml increases the risk of reflux/aspiration and feeding should be stopped. C. NJ feeding is indicated post-gastro-oesophageal surgery. D. NG tubes should not be passed further than 65cm. E. NJ tubes are easily placed.
3 Critical Care MCQ s Regarding critical care nutrition: A. Commencing enteral nutrition within 24 hours of intensive care admission is associated with a significant reduction in mortality. B. Trophic feeding compared to full feeding during the first week of intensive care admission, is associated with worse functional outcomes in patients with acute lung injury. C. During the early phase of critical care, a protein intake (0,5g/kg/day) is recommended. D. Selenium supplementation is of no benefit in septic patients. E. The timing of parenteral nutrition prescription remains uncertain.
4 Critical Care MCQ s Nutritional requirements: A. The Parkland formula is used to predict caloric requirements. B kcal/kg/day is the estimated daily energy requirement. C. The typical daily sodium requirement is 0,7-1mmol/kg/day. D. The typical daily carbohydrate requirement is 3-4g/kg/day, of which 60% should be glucose in parenteral nutrition. E. The typical daily calcium requirement is 0,4mmol/kg/day.
5 Critical Care MCQ s Vitamins and amino acids: A. A non-essential amino acids is one that cannot be synthesized and must be supplied in diet. B. In patients with severe organ failure, it is recommended that the non-essential amino acid, glutamine, is started within the first 24 hours of intensive care unit admission. C mg is the recommended daily allowance for vitamin C. D. Thiamine deficiency may cause wet beri-beri. E. Rebound hypoglycaemia may occur on cessation of parenteral nutrition.
6 Nutrition. 4 essential questions: Why should we take the time to optimize nutrition? Which is the preferred route? Enteral vs Parenteral? What about the timing? Enteral feeding vs SPN? Are supplements beneficial? Special considerations?
7 Introduction Protein/calorie malnutrition is very frequent in critically ill patients Protein/calorie malnutrition is associated with a worse outcome In approximately 10-15% of patients early enteral nutrition is either contraindicated or not tolerated

8 Major trials all show underfeeding Singer P. Intensive Care Med 2015;41:
9 Nutrition support research Enteral vs Parenteral nutrition - Difficult to interpret due to the challenges achieving adequate study size and quality. - However, in a variety of patient populations, the preponderance of data supports the benefits of choosing EN over PN when patients require nutrition support. Seres DS. Therap Adv Gastroenterol Mar; 6(2):
10 Early enteral nutrition Meta-analysis Primary analysis - Total (95% [0.14, Doig GS. Intensive Care Med 2009;35:

11 However... TPN has multiple side-effects
12 Guidelines based on expert opinion ESPEN: consider after two days ASPEN: consider after seven days if no malnutrition present
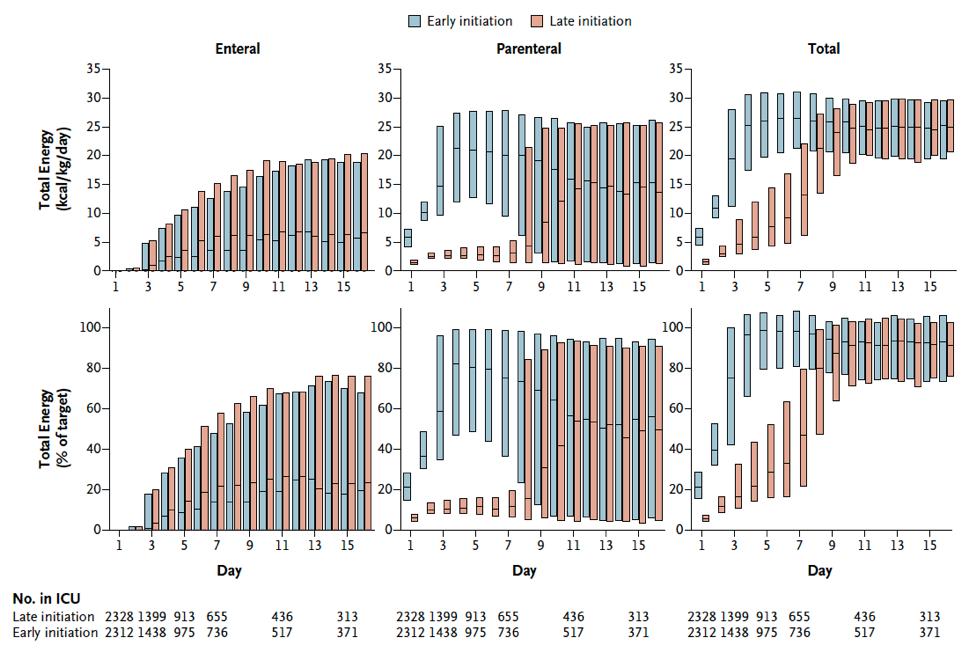
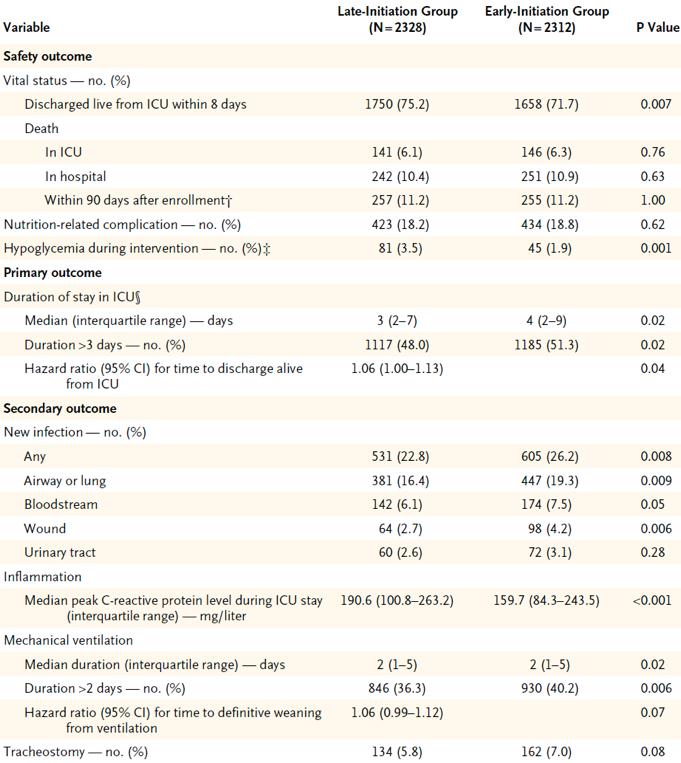
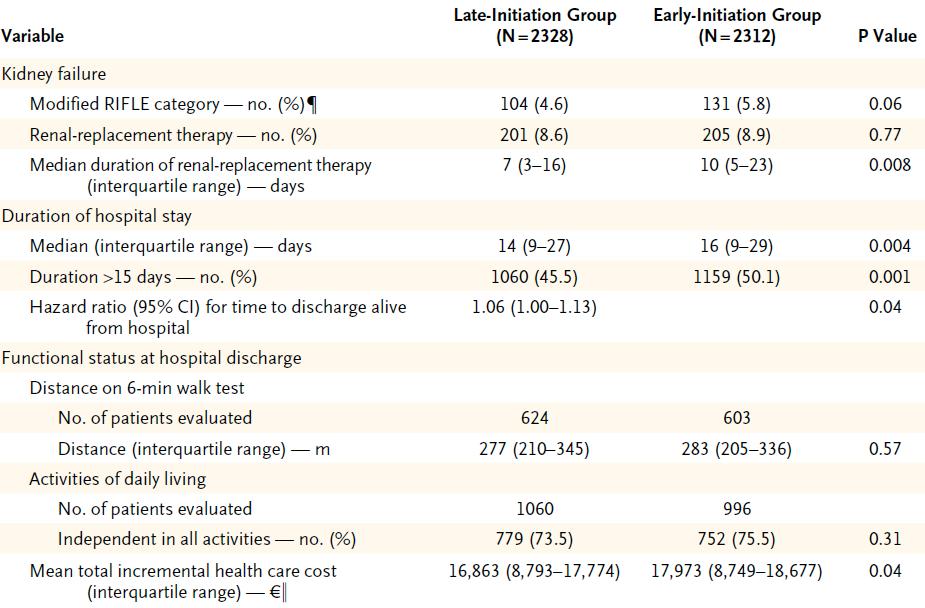
13 EPaNIC trial Multicenter RCT comparing early start SPN (D3) versus late start (D8) Adult ICU patients nutritionally at risk (NRS > 2) but not chronically malnourished (BMI 17) Stratification according to 16 diagnostic categories and randomisation 1:1 Primary endpoint: duration of ICU dependency Casaer MP. NEJM 2011
14 Enrollment
15 Early and late group Early: glucose 20% (D1 400 kcal and D2 800 kcal) - D3 start additional SPN to reach calculated nutritional target - diminished/stop when 80% of target covered by EN - restarted when EN < 50% Late: D1 -D7 glucose 5% and SPN added on D8 if EN was insufficient to reach calculated target Both groups EN started on D2 with standing orders
16
17 Results Study groups perfectly matched - sepsis 22% and mean APACHE II 23. However mostly postoperative cardiac surgery with short ICU stay As expected patients in the early SPN group needed higher mean daily insulin levels to reach target glucose levels
18
19
20 Predefined subgroup analysis Risk of infection much lower in late SPN group when EN contraindicated for the first 7 days
21 Secondary analysis No benefit of early SPN in more severely ill patients Risk of later discharge increases with amount of macronutrients Casaer MP. AJRCCM 2013
22 = more sick medical patients
23
24 EDEN trial Multicenter open label trial in ARDSnet hospitals - stratification by site and presence of shock Trophic versus full EN for the first 6 days of mechanical ventilation ALI < 48 hours and MV < 72 hours. No data on preexistent malnutrition. Severe malnutrition excluded ARDSnet. JAMA 2012
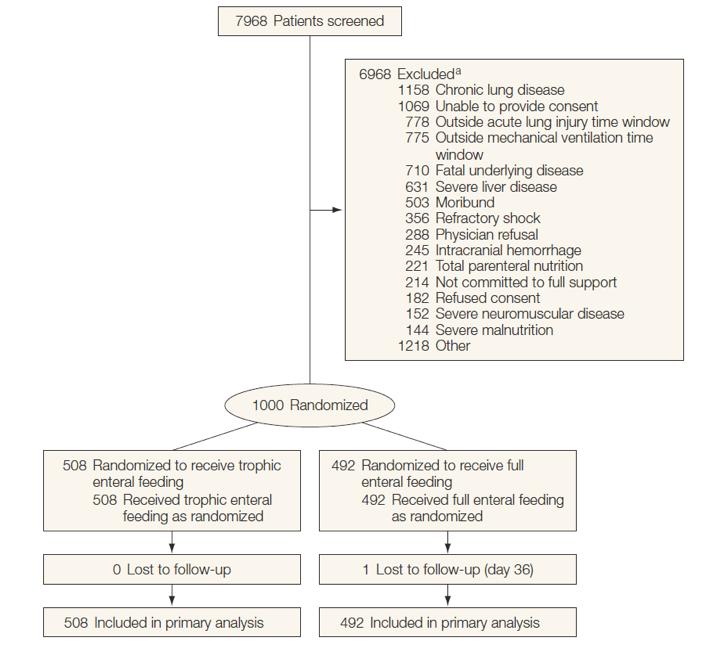
25 Enrollment
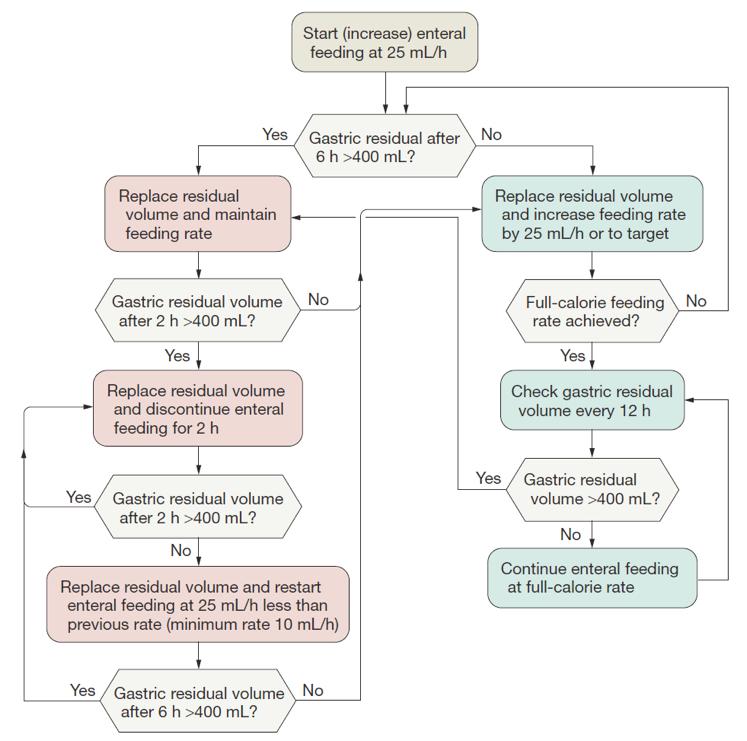
26 Trophic and full EN strategy Started within 6 hours after enrollment and continued until D6, extubation or death - after D6 full EN - glucose 4-8 mmol/l Trophic: kcal/h (first 272 patients), the rest 20 kcal/hour Full: see algorithm - goal non-protein calories/kg/day and gr/kg protein
27
28 Endpoints Primary: VFD's through D28 Multiple secondary endpoints No baseline differences between groups APACHE III score 90
29 Caloric intake
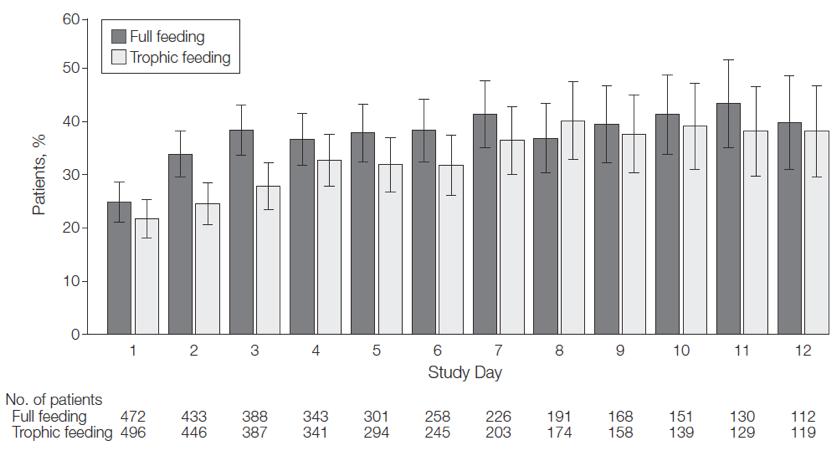
30 Gastro-intestinal intolerance
31 VFD's through Day ,9 15 Days Trophic Full
32 60-day mortality ,2 22,2 15 % Trophic Full Other secondary endpoints no differences also when analysed by BMI
33 Other results Higher glucose levels and insulin dose in Full group More positive fluid balance in Full group
34 Heidegger trial RCT in two mixed medical/surgical ICU's (tertiary care university hospitals) Inclusion if after D3 < 60% of nutritional needs were covered by EN AND expected to stay more than 5 days AND functional GI tract 1:1 randomization stratified for sex and admission category (medical/surgical) Heidegger CP. Lancet 2013

35 Nutrition scheme
36 SPN and EN group All patients started on D1 with EN (goal males 30 kcal/kg IBW, females 25 kcal/kg IBW - protein 1.2 gr/kg) SPN: started on D4 - continued for 5 days - energy requirement determined by indirect calorimetry. No glutamine etc. In both groups glucose < 8.5 mmol/l
37 Enrollment Primary outcome: nosocomial infection from D9 - D28
38 Results No differences in baseline characteristics Apache II 23 Indirect calorimetry in only 65% Protein delivery D4 - D8 1.2 gr/kg in SPN and 0.8 gr/kg in EN group
39
40 Nosocomial infections EN TPN supplement P = More antibiotic free days in TPN group
41 Kaplan- Meier

42 Individual infections No differences in LOS or mortality
43 Conclusions (1) Initiation enteral feeding Before start evaluate recent weight loss, disease severity, function GI tract (Gr E) EN is the preferred route of feeding (Gr B) EN should be started within hours (Gr C)
44 Conclusions (2) Initiation enteral feeding EN should be withheld during initial resuscitation for hemodynamic instability (Gr E) For the initiation of EN presence of bowel sounds or passage of stools is unnecessary (Gr B) Gastric and small bowel feeding are both acceptable. With gastric retention small bowel feeding is indicated (Gr C)
45 Conclusions (3) Dosing enteral feeding At the start define target goal preferentially with indirect calorimetry (Gr C) At least 65% of nutritional goals are required < 1 week to achieve clinical benefit of EN (Gr C) Protein g/kg actual BW (Gr E) With morbid obesity hypocaloric feeding (60-70% of target / kcal/kg IBW) with high protein content g/kg IBW (Gr D)
46 Conclusions (4) Early EN and SPN In previously non- malnourished patients it is save AND probably better to withhold SPN for the first 7 days if EN is insufficient to meet caloric needs in most patient groups Uncertainty for the most severely ill (e.g persistent high SOFA). If full EN appears impossible for 7 days, SPN on D4 is reasonable If enteral nutrition is absolutely contraindicated for more than 7 days, starting TPN on D4 is reasonable In case of preexistent severe malnutrition (BMI < 17) AND inability to reach nutritional targets with EN on D4, starting SPN is reasonable
47 Vincent JL. Lancet 2013
48 CALORIES trial RCT (MC - adults) early EN vs PEN in unplanned admissions (start < 36 hrs) Patients > 18 years expected to require nutritional support for at least 2 days Exclusively for 5 D, until ICU discharge or death Energy target 25 kcal/kg Harvey SE. N Engl J Med 2014;371:
49 Clinical outcome P = 0.57 P = 0.40 P = 1.00 P = P < % D mortality 90-D mortality SAE Hypoglycemia Vomiting Harvey SE. N Engl J Med 2014;371:
50 Supplements Glutamine Anti-oxidants: selenium, zinc, beta carotene, Vitamins E and C Essential fatty acids: Omega-3, GLA (y-linolecacid)
51 Glutamine at ICU admission Glutamine > 420 μmol/l Glutamine < 420 μmol/l 50 P = All-cause 6-month mortality N = 174 Rodas PC. Clinical Science 2012
52 Glutamine SIGNET study Multi-centre trial (N=10) Adults with expected LOS 48 hrs with 50% of nutritional requirements by PN 2 2 factorial design. Allocation to one of four isocaloric,iso-nitrogenous groups: glutamine, selenium, both or no additional glutamine or selenium: 7 days ICU, continuation on subsequent wards if practicable Andrews PJD. BMJ 2011;342:d1542
53 Glutamine N = 502 SIGNET study New infections Mortality ICU Mortality 6 M % 30 % Glutamine Selenium Both Neither 0 Any glutamine Any selenium For patients treated > 5 days selenium reduced the number of new infections No differences in secondary outcomes Andrews PJD. BMJ 2011;342:d1542
54 Scandinavian glutamine trial Multi-centre placebo-controlled RCT (N=11) Adult ICU patients with EN/TPN within 72 hours after ICU admission g glutamine/kg/day versus placebo for complete ICU period Analysis per protocol (> 3 days) and ITT Wernerman J. Acta Anaesthesiol Scand 2011;55:
55 Scandinavian glutamine trial N = 413 Placebo Glutamine P = P = P = P = Mortality (%) 20 Mortality (%) ,2 9,3 16,6 10,8 Per protocol ITT 0 34,6 31,2 32,6 34,2 Per protocol ITT ICU mortality 6 M mortality Primary outcome: change in SOFA D1 - D7 in PP group - no differences Wernerman J. Acta Anaesthesiol Scand 2011;55:
56 A Randomized Trial of Glutamine and Antioxidants in Critically Ill Patients MC RCT (40) with 2 2 design (glutamine and antioxidant supplementation for 28 D) Inclusion criterium: mechanical ventilation + organ failures Primary outcome: 28-day mortality Glutamine 0.35 mg/kg IBW Antioxidants: selenium, zinc, beta carotene, Vitamins E and C Heyland D. N Engl J Med 2013
57 Glutamine supplement Glutamine No glutamine Antioxidants No antioxidants 40 P = 0.05 P = % ,4 27,2 % ,8 28,8 In-hospital mortality Secondary outcomes Glutamine No glutamine P-value 37.2% 31% M mortality 43,7% 37,2% Mortality 28 D 0 Mortality 28 D Urea 13,4% 4% < No interaction between glutamine and antioxidants N = 1218 Heyland D. N Engl J Med 2013
58 Subgroup analysis Heyland D. N Engl J Med 2013
 N = 106 Pontes-Arruda A.")
59 INTERSEPT study Omega-3, GLA, anti-oxidants (Oxepa ) N = 106 Pontes-Arruda A. Crit Care 2011;15:R144

60 INTERSEPT study Primary Outcome Pontes-Arruda A. Crit Care 2011;15:R144
61 INTERSEPT study Organ Failure and Mortality % D Mortality Benefits of Oxepa is only proven in critically ill patients with early sepsis without organ failure Pontes-Arruda A. Crit Care 2011;15:R144
62 Omega-3, γ-linolenic acid and antioxidants A randomized, double blinded, placebo-controlled, MC trial (N=44) Patients with ALI (<48h) requiring mechanical ventilation and planned for EN Twice-daily enteral supplementation with N-3 FA, GLA and anti-oxidants or placebo either 21 days or until extubation 2 2 factorial design - low - vs full-calorie EN Rice TW. JAMA 2011;306:
63 Omega-3, γ-linolenic acid and antioxidants N = 272 Stopped for futility 28 Omega 3 Placebo P = 0.02 P = 0.04 P = Ventilator Free Days ICU Free Days Mortality (%) Rice TW. JAMA 2011;306:
64 Special considerations Nutrition and ARF / CRRT
65 Special considerations Nutrition and ARF / CRRT Also Thiamine 100 mg/d Citrate and lactate deliver up to 500 kcal/day Wiesen P. JPEN 2011;35:
When to start SPN in critically ill patients? Refereeravond IC
 When to start SPN in critically ill patients? Refereeravond IC Introduction (1) Protein/calorie malnutrition is very frequent in critically ill patients Protein/calorie malnutrition is associated with
When to start SPN in critically ill patients? Refereeravond IC Introduction (1) Protein/calorie malnutrition is very frequent in critically ill patients Protein/calorie malnutrition is associated with
Feeding the septic patient How and when? Masterclass ICU nurses
 Feeding the septic patient How and when? Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16 - FiO2 60%)
Feeding the septic patient How and when? Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16 - FiO2 60%)
Nutrition and Sepsis
 Nutrition and Sepsis Todd W. Rice, MD, MSc Associate Professor of Medicine Vanderbilt University 2017 DNS Symposium June 2, 2017 Case 55 y.o. male COPD, DM, HTN, presents with pneumonia and septic shock.
Nutrition and Sepsis Todd W. Rice, MD, MSc Associate Professor of Medicine Vanderbilt University 2017 DNS Symposium June 2, 2017 Case 55 y.o. male COPD, DM, HTN, presents with pneumonia and septic shock.
Ernährungstherapie des Kritisch Kranken Enteral Parenteral Ganz egal?
 Ernährungstherapie des Kritisch Kranken Enteral Parenteral Ganz egal? PD Dr. med. Claudia Heidegger Service des Soins Intensifs Genf/Schweiz Dresden 11. Juni 2016 Nutrition News Nutrition controversy in
Ernährungstherapie des Kritisch Kranken Enteral Parenteral Ganz egal? PD Dr. med. Claudia Heidegger Service des Soins Intensifs Genf/Schweiz Dresden 11. Juni 2016 Nutrition News Nutrition controversy in
Nutrition Support in Critically Ill Cardiothoracic Patients
 Nutrition Support in Critically Ill Cardiothoracic Patients อ.นพ.พรพจน เปรมโยธ น สาชาโภชนาการคล น ก ภาคว ชาอาย รศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล Outline Malnutrition in cardiothoracic patients Nutritional
Nutrition Support in Critically Ill Cardiothoracic Patients อ.นพ.พรพจน เปรมโยธ น สาชาโภชนาการคล น ก ภาคว ชาอาย รศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล Outline Malnutrition in cardiothoracic patients Nutritional
Parenterale voeding tijdens kritieke ziekte: bijkomende analyses van de EPaNIC studie
 Parenterale voeding tijdens kritieke ziekte: bijkomende analyses van de EPaNIC studie Namens alle auteurs Michaël P. Casaer M.D. Department of Intensive Care Medicine University Hospital Gasthuisberg Catholic
Parenterale voeding tijdens kritieke ziekte: bijkomende analyses van de EPaNIC studie Namens alle auteurs Michaël P. Casaer M.D. Department of Intensive Care Medicine University Hospital Gasthuisberg Catholic
Kombinierte enterale und parenterale Ernährung für welche PatientInnen?
 2014 Kombinierte enterale und parenterale Ernährung für welche PatientInnen? Dr. CP. Heidegger Intensive Care/Geneva claudia-paula.heidegger@hcuge.ch Bern Freitag, 4. April 2014 Nutrition News Worldwide
2014 Kombinierte enterale und parenterale Ernährung für welche PatientInnen? Dr. CP. Heidegger Intensive Care/Geneva claudia-paula.heidegger@hcuge.ch Bern Freitag, 4. April 2014 Nutrition News Worldwide
Metabolic Control in Critical Care: Nutrition Therapy
 LOGO Metabolic Control in Critical Care: Nutrition Therapy ผศ.นพ.พรพจน เปรมโยธ น สาขาโภชนาการคล น ก ภาคว ชาอาย รศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล 2016 SCCM/ASPEN Guidelines Nutrition Therapy in the ICU
LOGO Metabolic Control in Critical Care: Nutrition Therapy ผศ.นพ.พรพจน เปรมโยธ น สาขาโภชนาการคล น ก ภาคว ชาอาย รศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล 2016 SCCM/ASPEN Guidelines Nutrition Therapy in the ICU
Providing Optimal Nutritional Support on the ICU common problems and practical solutions. Pete Turner Specialist Nutritional Support Dietitian
 Providing Optimal Nutritional Support on the ICU common problems and practical solutions Pete Turner Specialist Nutritional Support Dietitian ICU Nutritional Support ACCEPT study showed improved ICU survival
Providing Optimal Nutritional Support on the ICU common problems and practical solutions Pete Turner Specialist Nutritional Support Dietitian ICU Nutritional Support ACCEPT study showed improved ICU survival
Pharmaconutrition in PICU. Gan Chin Seng Paediatric Intensivist UMMC
 Pharmaconutrition in PICU Gan Chin Seng Paediatric Intensivist UMMC Pharmaconutrition in Critical Care Unit Gan Chin Seng Paediatric Intensivist UMMC Definition New concept Treatment with specific nutrients
Pharmaconutrition in PICU Gan Chin Seng Paediatric Intensivist UMMC Pharmaconutrition in Critical Care Unit Gan Chin Seng Paediatric Intensivist UMMC Definition New concept Treatment with specific nutrients
Timing of Parenteral Nutrition
 Timing of Parenteral Nutrition Arun Bansal; MD, FCCM, MRCPCH Professor Pediatric Critical Care PGIMER, Chandigarh, INDIA drarunbansal@gmail.com Malnutrition in Critically Ill Incidence: from 19 32% Associated
Timing of Parenteral Nutrition Arun Bansal; MD, FCCM, MRCPCH Professor Pediatric Critical Care PGIMER, Chandigarh, INDIA drarunbansal@gmail.com Malnutrition in Critically Ill Incidence: from 19 32% Associated
What s New in Parenteral Nutrition?
 1 What s New in Parenteral Nutrition? พ นโทหญ ง ส รกานต เตชะวณ ช MD, MSc, ABPNS ห วหน าหน วยโภชนศาสตร คล น ก กองอาย รกรรม โรงพยาบาลพระมงก ฎเกล า 7 กรกฎาคม พ.ศ. 2559 What s New in Parenteral Nutrition?
1 What s New in Parenteral Nutrition? พ นโทหญ ง ส รกานต เตชะวณ ช MD, MSc, ABPNS ห วหน าหน วยโภชนศาสตร คล น ก กองอาย รกรรม โรงพยาบาลพระมงก ฎเกล า 7 กรกฎาคม พ.ศ. 2559 What s New in Parenteral Nutrition?
ICU NUTRITION UPDATE : ESPEN GUIDELINES Mirey Karavetian Assistant Professor Zayed University
 ICU NUTRITION UPDATE : ESPEN GUIDELINES 2018 Mirey Karavetian Assistant Professor Zayed University http://www.espen.org/files/espen- Guidelines/ESPEN_Guideline_on_clinical_nutrition_in_-ICU.pdf Medical
ICU NUTRITION UPDATE : ESPEN GUIDELINES 2018 Mirey Karavetian Assistant Professor Zayed University http://www.espen.org/files/espen- Guidelines/ESPEN_Guideline_on_clinical_nutrition_in_-ICU.pdf Medical
[No conflicts of interest]
![[No conflicts of interest]](/thumbs/86/94144068.jpg "[No conflicts of interest]") [No conflicts of interest] Patients and staff at: Available evidence pre-calories Three meta-analyses: Gramlich L et al. Does enteral nutrition compared to parenteral nutrition result in better outcomes
[No conflicts of interest] Patients and staff at: Available evidence pre-calories Three meta-analyses: Gramlich L et al. Does enteral nutrition compared to parenteral nutrition result in better outcomes
This article was published on October 22, 2018, at NEJM.org.
 1 20 8 b E 8 b E C T aa 4 JG R d This article was published on October 22, 2018, at NEJM.org. 2003 2009 (ESPEN) (ASPEN/SCCM) CCPG 20-25kcal/kg/day 25-30kcal/kg/day EN PN( ) Enteral Nutrition EN 24 ICU
1 20 8 b E 8 b E C T aa 4 JG R d This article was published on October 22, 2018, at NEJM.org. 2003 2009 (ESPEN) (ASPEN/SCCM) CCPG 20-25kcal/kg/day 25-30kcal/kg/day EN PN( ) Enteral Nutrition EN 24 ICU
Heather Evans, MD University of Washington Seattle, WA
 Heather Evans, MD University of Washington Seattle, WA 1 American College of Surgeons Division of Education Heather L. Evans, MD, MS, FACS Nothing to disclose 2 Determine nutritional goals Determine when
Heather Evans, MD University of Washington Seattle, WA 1 American College of Surgeons Division of Education Heather L. Evans, MD, MS, FACS Nothing to disclose 2 Determine nutritional goals Determine when
Intensive Care Nutrition. Dr Alan Race BSc(Hons) PhD FRCA
 PhD FRCA") Intensive Care Nutrition Dr Alan Race BSc(Hons) PhD FRCA Objectives 1. What examiners say 2. Definition 3. Assessment 4. Requirements 5. Types of delivery 6. CALORIES Trial 7. Timing 8. Immunomodulation
Intensive Care Nutrition Dr Alan Race BSc(Hons) PhD FRCA Objectives 1. What examiners say 2. Definition 3. Assessment 4. Requirements 5. Types of delivery 6. CALORIES Trial 7. Timing 8. Immunomodulation
The Meat and Potatoes of Critical Care Nutrition ROSEMARY KOZAR MD PHD SHOCK TRAUMA UNIVERSITY OF MARYLAND
 The Meat and Potatoes of Critical Care Nutrition ROSEMARY KOZAR MD PHD SHOCK TRAUMA UNIVERSITY OF MARYLAND 2013 Canadian Clinical Practice Guidelines www.criticalcarenutrition.com NEJM March 27, 2014 Use
The Meat and Potatoes of Critical Care Nutrition ROSEMARY KOZAR MD PHD SHOCK TRAUMA UNIVERSITY OF MARYLAND 2013 Canadian Clinical Practice Guidelines www.criticalcarenutrition.com NEJM March 27, 2014 Use
A R T H U R R. H. V A N Z A N T E N, MD PHD I N T E R N I S T - I N T E N S I V I S T H O S P I T A L MEDICAL DIRECTOR G E L D E R S E V A L L E I
 FEEDING THE OBESE CRITICALLY ILL PATIENT A R T H U R R. H. V A N Z A N T E N, MD PHD I N T E R N I S T - I N T E N S I V I S T H O S P I T A L MEDICAL DIRECTOR G E L D E R S E V A L L E I HOSPITAL, EDE,
FEEDING THE OBESE CRITICALLY ILL PATIENT A R T H U R R. H. V A N Z A N T E N, MD PHD I N T E R N I S T - I N T E N S I V I S T H O S P I T A L MEDICAL DIRECTOR G E L D E R S E V A L L E I HOSPITAL, EDE,
IS THERE A PLACE IN THE ICU FOR PERMISSIVE UNDERFEEDING AND WHERE? ENGELA FRANCIS RD(SA)
") IS THERE A PLACE IN THE ICU FOR PERMISSIVE UNDERFEEDING AND WHERE? ENGELA FRANCIS RD(SA) DEFINITION: PERMISSIVE UNDERFEEDING No clear definition in literature Permissive underfeeding definition prior to
IS THERE A PLACE IN THE ICU FOR PERMISSIVE UNDERFEEDING AND WHERE? ENGELA FRANCIS RD(SA) DEFINITION: PERMISSIVE UNDERFEEDING No clear definition in literature Permissive underfeeding definition prior to
Year in Review Intensive Care Training Program Radboud University Medical Centre Nijmegen
 Year in Review 2013 Intensive Care Training Program Radboud University Medical Centre Nijmegen Contents ARDS Ventilator associated pneumonia Tracheostomy and endotracheal intubation Enteral feeding Fluid
Year in Review 2013 Intensive Care Training Program Radboud University Medical Centre Nijmegen Contents ARDS Ventilator associated pneumonia Tracheostomy and endotracheal intubation Enteral feeding Fluid
ESPEN Congress The Hague 2017
 ESPEN Congress The Hague 2017 Using the gut in acute care patients Permissive underfeeding in practice J.-C. Preiser (BE) PERMISSIVE UNDERFEEDING IN PRACTICE ESPEN congress Jean-Charles Preiser, M.D.,
ESPEN Congress The Hague 2017 Using the gut in acute care patients Permissive underfeeding in practice J.-C. Preiser (BE) PERMISSIVE UNDERFEEDING IN PRACTICE ESPEN congress Jean-Charles Preiser, M.D.,
Nutrition Supplementation in the ICU
 Nutrition Supplementation in the ICU ROSEMARY KOZAR MD PHD SHOCK TRAUMA UNIVERSITY OF MARYLAND Canadian Clinical Practice Guidelines www.criticalcarenutrition.com NEJM March 27, 2014 1 Use of Enteral vs
Nutrition Supplementation in the ICU ROSEMARY KOZAR MD PHD SHOCK TRAUMA UNIVERSITY OF MARYLAND Canadian Clinical Practice Guidelines www.criticalcarenutrition.com NEJM March 27, 2014 1 Use of Enteral vs
Nutrition and GI. How much?
 Nutrition and GI How much? The goal of nutritional supplementation is to meet but not exceed the nutritional requirements of patients with critical illness. Due to the inherent variability between patients
Nutrition and GI How much? The goal of nutritional supplementation is to meet but not exceed the nutritional requirements of patients with critical illness. Due to the inherent variability between patients
E S T A B L I S H I N G N U T R I T I O N I N Y O U R I C U The Need for a Protocol
 E S T A B L I S H I N G N U T R I T I O N I N Y O U R I C U The Need for a Protocol Arthur RH van Zanten, MD PhD Gelderse Vallei Hospital, Ede, The Netherlands Learning objectives Develop an evidence based
E S T A B L I S H I N G N U T R I T I O N I N Y O U R I C U The Need for a Protocol Arthur RH van Zanten, MD PhD Gelderse Vallei Hospital, Ede, The Netherlands Learning objectives Develop an evidence based
NO DISCLOSURES 5/9/2015
 Annette Stralovich-Romani, RD, CNSC Adult Critical Care Nutritionist UCSF Medical Center NO DISCLOSURES Incidence & consequences of malnutrition Underfeeding in the ICU Causes/ consequences Nutrition intervention
Annette Stralovich-Romani, RD, CNSC Adult Critical Care Nutritionist UCSF Medical Center NO DISCLOSURES Incidence & consequences of malnutrition Underfeeding in the ICU Causes/ consequences Nutrition intervention
THE AUTHOR OF THIS WHAT S NEW IN NUTRITION? OBJECTIVES & OUTLINE EVIDENCE-BASED MEDICINE: PARENTERAL NUTRITION (PN)
") WHAT S NEW IN NUTRITION? Alisha Mutch, Pharm.D., BCPS THE AUTHOR OF THIS PRESENTATION HAS NOTHING TO DISCLOSE. OBJECTIVES & OUTLINE MALNUTRITION OBJECTIVES Indicate when parenteral nutrition (PN) is warranted
WHAT S NEW IN NUTRITION? Alisha Mutch, Pharm.D., BCPS THE AUTHOR OF THIS PRESENTATION HAS NOTHING TO DISCLOSE. OBJECTIVES & OUTLINE MALNUTRITION OBJECTIVES Indicate when parenteral nutrition (PN) is warranted
Parenteral nutrition and calorie delivery in the ICU: controversy, clarity, or call to action?
 EDITORIAL C URRENT OPINION Parenteral nutrition and calorie delivery in the ICU: controversy, clarity, or call to action? Paul Wischmeyer Purpose of review This review will highlight recent data evaluating
EDITORIAL C URRENT OPINION Parenteral nutrition and calorie delivery in the ICU: controversy, clarity, or call to action? Paul Wischmeyer Purpose of review This review will highlight recent data evaluating
Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Enteral Nutrition Algorithm Clinical Practice Guideline
 Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Enteral Nutrition Algorithm Clinical Practice Guideline Original Date: 08/2011 Purpose: To promote the early use of
Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Enteral Nutrition Algorithm Clinical Practice Guideline Original Date: 08/2011 Purpose: To promote the early use of
By; Ashraf El Houfi MD MS (pulmonology) MRCP (UK) FRCP (London) EDIC Consultant ICU Dubai Hospital
 MRCP (UK) FRCP (London) EDIC Consultant ICU Dubai Hospital") By; Ashraf El Houfi MD MS (pulmonology) MRCP (UK) FRCP (London) EDIC Consultant ICU Dubai Hospital Introduction The significance of nutrition in hospital setting (especially the ICU) cannot be overstated.
By; Ashraf El Houfi MD MS (pulmonology) MRCP (UK) FRCP (London) EDIC Consultant ICU Dubai Hospital Introduction The significance of nutrition in hospital setting (especially the ICU) cannot be overstated.
L.Mageswary Dietitian Hospital Selayang
 L.Mageswary Dietitian Hospital Selayang 14 15 AUG ASMIC 2015 Learning Objectives 1. To understand the importance of nutrition support in ICU 2. To know the right time to feed 3. To understand the indications
L.Mageswary Dietitian Hospital Selayang 14 15 AUG ASMIC 2015 Learning Objectives 1. To understand the importance of nutrition support in ICU 2. To know the right time to feed 3. To understand the indications
Enteral Nutrition: Whom, Why, When, What and Where to Feed?
 Meier RF, Reddy BR, Soeters PB (eds): The Importance of Nutrition as an Integral Part of Disease Management. Nestlé Nutr Inst Workshop Ser, vol 82, pp 53 59, (DOI: 10.1159/000382002) Nestec Ltd., Vevey/S.
Meier RF, Reddy BR, Soeters PB (eds): The Importance of Nutrition as an Integral Part of Disease Management. Nestlé Nutr Inst Workshop Ser, vol 82, pp 53 59, (DOI: 10.1159/000382002) Nestec Ltd., Vevey/S.
Current concepts in Critical Care Nutrition
 Current concepts in Critical Care Nutrition Dr.N.Ramakrishnan AB (Int Med), AB (Crit Care), MMM, FACP, FCCP, FCCM Director, Critical Care Services Apollo Hospitals, Chennai Objectives Why? Enteral or Parenteral
Current concepts in Critical Care Nutrition Dr.N.Ramakrishnan AB (Int Med), AB (Crit Care), MMM, FACP, FCCP, FCCM Director, Critical Care Services Apollo Hospitals, Chennai Objectives Why? Enteral or Parenteral
Nutrition in Acute Kidney Injury Enrico Fiaccadori
 Nutrition in Acute Kidney Injury Enrico Fiaccadori Nephrology Dept. Parma University Medical School Parma, Italy Diagnosis, epidemiology and prognostic impact of proteinenergy wasting (PEW) in AKI Pathogenetic
Nutrition in Acute Kidney Injury Enrico Fiaccadori Nephrology Dept. Parma University Medical School Parma, Italy Diagnosis, epidemiology and prognostic impact of proteinenergy wasting (PEW) in AKI Pathogenetic
Feeding the Critically Ill Obese Patient
 Feeding the Critically Ill Obese Patient Carla Vartanian 1 Critically Ill Obese Patients WHO: Obesity is abnormal or excessive fat accumulation that may impair health, or as a BMI 30. The American Medical
Feeding the Critically Ill Obese Patient Carla Vartanian 1 Critically Ill Obese Patients WHO: Obesity is abnormal or excessive fat accumulation that may impair health, or as a BMI 30. The American Medical
N U TRITION A N D C R I TICALLY I L L PATIENTS W I TH S E P S I S
 N U TRITION A N D M E TABOLISM: C R I TICALLY I L L PATIENTS W I TH S E P S I S A R T H U R R. H. V A N Z A N T E N, M D P H D I N T E R N IST - IN TENSIV IST H O S P I T AL M E D I C A L D I R E C T OR
N U TRITION A N D M E TABOLISM: C R I TICALLY I L L PATIENTS W I TH S E P S I S A R T H U R R. H. V A N Z A N T E N, M D P H D I N T E R N IST - IN TENSIV IST H O S P I T AL M E D I C A L D I R E C T OR
Appendix. This appendix was part of the submitted manuscript and has been peer reviewed. It is posted as supplied by the authors.
 Appendix This appendix was part of the submitted manuscript and has been peer reviewed It is posted as supplied by the authors Protein delivery and clinical outcomes in the critically ill: A systematic
Appendix This appendix was part of the submitted manuscript and has been peer reviewed It is posted as supplied by the authors Protein delivery and clinical outcomes in the critically ill: A systematic
ENTERAL NUTRITION IN THE CRITICALLY ILL
 ENTERAL NUTRITION IN THE CRITICALLY ILL 1 Ebb phase Flow phase acute response (catabolic) adoptive response (anabolic) 2 3 Metabolic Response to Stress (catabolic phase) Glucose and Protein Metabolism
ENTERAL NUTRITION IN THE CRITICALLY ILL 1 Ebb phase Flow phase acute response (catabolic) adoptive response (anabolic) 2 3 Metabolic Response to Stress (catabolic phase) Glucose and Protein Metabolism
patients : review of advances in last five years Dr. Aditya Jindal
 Enteral nutrition in medical ICU patients : review of advances in last five years Dr. Aditya Jindal Our food should be our medicine and our medicine should be our food. Hippocrates Introduction ti Nutritional
Enteral nutrition in medical ICU patients : review of advances in last five years Dr. Aditya Jindal Our food should be our medicine and our medicine should be our food. Hippocrates Introduction ti Nutritional
Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Pediatric Critically Ill Patient: ASPEN-SCCM 2017
 Number of Patients Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Pediatric Critically Ill Patient: ASPEN-SCCM 2017 Jorge A. Coss-Bu, MD Associate Professor of Pediatrics
Number of Patients Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Pediatric Critically Ill Patient: ASPEN-SCCM 2017 Jorge A. Coss-Bu, MD Associate Professor of Pediatrics
2.0 Early vs. Delayed Nutrient Intake May 2015
 2.0 Early vs. Delayed Nutrient Intake May 2015 There were no new randomized controlled trials since the 2013 update and hence there are no changes to the following summary of evidence. 2013 Recommendation:
2.0 Early vs. Delayed Nutrient Intake May 2015 There were no new randomized controlled trials since the 2013 update and hence there are no changes to the following summary of evidence. 2013 Recommendation:
Nutrition Procedures Nutrition Prescription Protein Target Lower Protein Dose Higher Protein Dose 1.2 g/kg/day Calorie Target
 Nutrition Procedures Nutrition Prescription Protein and energy targets will be achieved through any combination of EN, protein supplements, and PN or amino acids. The only difference between the nutrition
Nutrition Procedures Nutrition Prescription Protein and energy targets will be achieved through any combination of EN, protein supplements, and PN or amino acids. The only difference between the nutrition
Oklahoma Dietetic Association. Ainsley Malone, MS, RD, LD, CNSD April, 16, 2008 Permissive Underfeeding: What, Where and Why? Mt.
 The What, Why and When of Permissive Ainsley Malone, MS, RD, CNSD Nutrition Support Team Mt. Carmel West Hospital Mt. Carmel West 500 bed academic center Non-physician based NST Dietitian, pharmacist and
The What, Why and When of Permissive Ainsley Malone, MS, RD, CNSD Nutrition Support Team Mt. Carmel West Hospital Mt. Carmel West 500 bed academic center Non-physician based NST Dietitian, pharmacist and
11.1 Supplemental Antioxidant Nutrients: Combined Vitamins and Trace Elements April 2013
 . Supplemental Antioxidant Nutrients: Combined Vitamins and Trace Elements April 23 23 Recommendation: Based on 7 level and 7 level 2 studies, the use of supplemental combined vitamins and trace elements
. Supplemental Antioxidant Nutrients: Combined Vitamins and Trace Elements April 23 23 Recommendation: Based on 7 level and 7 level 2 studies, the use of supplemental combined vitamins and trace elements
Nutrition care plan for surgical patients. Objectives
 Slide 1 Nutrition care plan for surgical patients Surgical Nutrition Training Module Level 1 Philippine Society of General Surgeons Committee on Surgical Training In this session we will discuss the most
Slide 1 Nutrition care plan for surgical patients Surgical Nutrition Training Module Level 1 Philippine Society of General Surgeons Committee on Surgical Training In this session we will discuss the most
ESPEN Congress Geneva 2014 NUTRITION AT EXTREMES: THE UNLIKELY BENEFITS OF STARVATION
 ESPEN Congress Geneva 2014 NUTRITION AT EXTREMES: THE UNLIKELY BENEFITS OF STARVATION Management of the severely malnourished: the case of anorexia nervosa C. De la Cuerda (ES) Management of the severely
ESPEN Congress Geneva 2014 NUTRITION AT EXTREMES: THE UNLIKELY BENEFITS OF STARVATION Management of the severely malnourished: the case of anorexia nervosa C. De la Cuerda (ES) Management of the severely
4.1b(i) Composition of Enteral Nutrition: Fish Oils, Borage Oils and Antioxidants* May 2015
 Composition of Enteral Nutrition: Fish Oils, Borage Oils and Antioxidants* May 2015") 4.1b(i) Composition of Enteral Nutrition: Fish Oils, Borage Oils and Antioxidants* May 2015 2015 Recommendation: Based on 3 level 1 studies and 5 level 2 studies, the use of an enteral formula with fish
4.1b(i) Composition of Enteral Nutrition: Fish Oils, Borage Oils and Antioxidants* May 2015 2015 Recommendation: Based on 3 level 1 studies and 5 level 2 studies, the use of an enteral formula with fish
Nutrition care plan. Components and development
 Nutrition care plan Components and development Objectives To define the nutrition care plan To present the components of the nutrition care plan To discuss the different approaches in determining the contents
Nutrition care plan Components and development Objectives To define the nutrition care plan To present the components of the nutrition care plan To discuss the different approaches in determining the contents
Nutrition Management of the Critically Ill Pediatric Patient: Facilitating the Transition to Enteral Nutrition
 Nutrition Management of the Critically Ill Pediatric Patient: Facilitating the Transition to Enteral Nutrition Ana Abad-Jorge, EdD, MS, RDN, CNSC Program Director, Bachelor of Professional Studies in Health
Nutrition Management of the Critically Ill Pediatric Patient: Facilitating the Transition to Enteral Nutrition Ana Abad-Jorge, EdD, MS, RDN, CNSC Program Director, Bachelor of Professional Studies in Health
ASPEN/SCCM Critical Care Nutrition Guidelines: What s New and Updated?
 ASPEN/SCCM Critical Care Nutrition Guidelines: What s New and Updated? Todd W. Rice, MD, MSc Associate Professor of Medicine Vanderbilt University WiSPEN Annual Fall Symposium 2016 September 16, 2016 Objectives
ASPEN/SCCM Critical Care Nutrition Guidelines: What s New and Updated? Todd W. Rice, MD, MSc Associate Professor of Medicine Vanderbilt University WiSPEN Annual Fall Symposium 2016 September 16, 2016 Objectives
Protein dosing in the ICU: How much, when and why?
 Protein dosing in the ICU: How much, when and why? Dr. Gordon S. Doig, Associate Professor in Intensive Care Northern Clinical School Intensive Care Research Unit, University of Sydney, Sydney, Australia
Protein dosing in the ICU: How much, when and why? Dr. Gordon S. Doig, Associate Professor in Intensive Care Northern Clinical School Intensive Care Research Unit, University of Sydney, Sydney, Australia
Disclosures. None. Enteral Nutrition and Vasoactive Therapy! But actually.. Stocks Advisory boards Grants Speakers Bureau. Paul Marik, MD,FCCM,FCCP
 Enteral Nutrition and Vasoactive Therapy! Paul Marik, MD,FCCM,FCCP Disclosures Stocks Advisory boards Grants Speakers Bureau None But actually.. 1 We suggest a determination of nutrition risk (NUTRIC score)
Enteral Nutrition and Vasoactive Therapy! Paul Marik, MD,FCCM,FCCP Disclosures Stocks Advisory boards Grants Speakers Bureau None But actually.. 1 We suggest a determination of nutrition risk (NUTRIC score)
Case Discussion. Nutrition in IBD. Rémy Meier MD. Ulcerative colitis. Crohn s disease
 26.08.2017 Case Discussion Nutrition in IBD Crohn s disease Ulcerative colitis Rémy Meier MD Case Presentation 30 years old female, with diarrhea for 3 months Shool frequency 3-4 loose stools/day with
26.08.2017 Case Discussion Nutrition in IBD Crohn s disease Ulcerative colitis Rémy Meier MD Case Presentation 30 years old female, with diarrhea for 3 months Shool frequency 3-4 loose stools/day with
SECTION 4: RECRUIT PARTICIPANTS
 SECTION 4: RECRUIT PARTICIPANTS Contents Participant Eligibility & Enrollment... 2 Screening... 2 Study ID Numbers... 2 Inclusion Criteria... 2 Exclusion Criteria... 4 Co-Enrollment... 5 Informed Consent
SECTION 4: RECRUIT PARTICIPANTS Contents Participant Eligibility & Enrollment... 2 Screening... 2 Study ID Numbers... 2 Inclusion Criteria... 2 Exclusion Criteria... 4 Co-Enrollment... 5 Informed Consent
Protein in Critically Ill Patients. Ashraf El Houfi. MD MS(pulmonology) MRCP(UK) FRCP(London) EDIC Consultant ICU Dubai Hospital
 MRCP(UK) FRCP(London) EDIC Consultant ICU Dubai Hospital") Protein in Critically Ill Patients Ashraf El Houfi. MD MS(pulmonology) MRCP(UK) FRCP(London) EDIC Consultant ICU Dubai Hospital Proteins Proteins Protein is needed to Build, Maintain, and Repair body tissue
Protein in Critically Ill Patients Ashraf El Houfi. MD MS(pulmonology) MRCP(UK) FRCP(London) EDIC Consultant ICU Dubai Hospital Proteins Proteins Protein is needed to Build, Maintain, and Repair body tissue
ESPEN Congress Florence 2008
 ESPEN Congress Florence 2008 PN Guidelines presentation PN Guidelines in pancreas diseases L. Gianotti (Italy) ESPEN Guidelines on Parenteral Nutrition: Pancreas L.Gianotti, R.Meier, D.N.Lobo, C.Bassi,
ESPEN Congress Florence 2008 PN Guidelines presentation PN Guidelines in pancreas diseases L. Gianotti (Italy) ESPEN Guidelines on Parenteral Nutrition: Pancreas L.Gianotti, R.Meier, D.N.Lobo, C.Bassi,
Nutrition in ECMO. Elize Craucamp RD(SA)
") Nutrition in ECMO Elize Craucamp RD(SA) ECMO What now!? KEEP CALM AND FEED THE ECMO PATIENT Despite the fact that little is known about nutritional strategies for adult ECMO patients! Neither overcomplicate
Nutrition in ECMO Elize Craucamp RD(SA) ECMO What now!? KEEP CALM AND FEED THE ECMO PATIENT Despite the fact that little is known about nutritional strategies for adult ECMO patients! Neither overcomplicate
ESPEN Congress Madrid 2018
 ESPEN Congress Madrid 2018 New ESPEN Guidelines Nutrition In The ICU P. Singer (IL) ESPEN Guidelines: Nutrition in the ICU Pierre Singer Annika Reintam Blaser Mette M Berger Waleed Alhazzani Philip C Calder
ESPEN Congress Madrid 2018 New ESPEN Guidelines Nutrition In The ICU P. Singer (IL) ESPEN Guidelines: Nutrition in the ICU Pierre Singer Annika Reintam Blaser Mette M Berger Waleed Alhazzani Philip C Calder
10/3/2012. Pediatric Parenteral Nutrition A Comprehensive Review
 Critical Care Nutrition Foundation for Moving Forward Justine Turner MD PhD Department of Pediatric Gastroenterology and Nutrition University of Alberta I have the following financial relationships to
Critical Care Nutrition Foundation for Moving Forward Justine Turner MD PhD Department of Pediatric Gastroenterology and Nutrition University of Alberta I have the following financial relationships to
About OMICS International
 About OMICS International OMICS International through its Open Access Initiative is committed to make genuine and reliable contributions to the scientific community. OMICS International hosts over 700
About OMICS International OMICS International through its Open Access Initiative is committed to make genuine and reliable contributions to the scientific community. OMICS International hosts over 700
Surgical Nutrition for the Cardiothoracic Patient. Stephanie Kunioki RD, CNSC, LD Memorial Hermann TMC
 Surgical Nutrition for the Cardiothoracic Patient Stephanie Kunioki RD, CNSC, LD Memorial Hermann TMC Financial Disclosures NONE Declared PROPER NUTRITION Surgical Effects on Nutrition Intake & Status
Surgical Nutrition for the Cardiothoracic Patient Stephanie Kunioki RD, CNSC, LD Memorial Hermann TMC Financial Disclosures NONE Declared PROPER NUTRITION Surgical Effects on Nutrition Intake & Status
5.3 Strategies to Optimize Delivery and Minimize Risks of EN: Small Bowel Feeding vs. Gastric February 2014
 5.3 Strategies to Optimize Delivery and Minimize Risks of EN: Small Bowel Feeding vs. Gastric February 2014 2013 Recommendation: Based on 15 level 2 studies, small bowel feeding compared to gastric feeding
5.3 Strategies to Optimize Delivery and Minimize Risks of EN: Small Bowel Feeding vs. Gastric February 2014 2013 Recommendation: Based on 15 level 2 studies, small bowel feeding compared to gastric feeding
3.2 Nutritional Prescription of Enteral Nutrition: Achieving Target Dose of Enteral Nutrition March 2013
 . Nutritional Prescription of Enteral Nutrition: Achieving Target Dose of Enteral Nutrition March 01 There were no new randomized controlled trials since the 009 update and hence there are no changes to
. Nutritional Prescription of Enteral Nutrition: Achieving Target Dose of Enteral Nutrition March 01 There were no new randomized controlled trials since the 009 update and hence there are no changes to
Year in Review: Critical Care Medicine
 Year in Review: Critical Care Medicine No disclosures Eric J. Seeley, M.D. Assistant Professor of Medicine Division of Pulmonary and Critical Care Medicine Why I Selected These Studies High quality studies
Year in Review: Critical Care Medicine No disclosures Eric J. Seeley, M.D. Assistant Professor of Medicine Division of Pulmonary and Critical Care Medicine Why I Selected These Studies High quality studies
Nutrition in critical illness:
 Nutrition in critical illness: from theory to daily practice Aim of the presentation Summarize the guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient.
Nutrition in critical illness: from theory to daily practice Aim of the presentation Summarize the guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient.
ICU Acquired Weakness: Role of Specific Nutrients
 ICU Acquired Weakness: Role of Specific Nutrients Dr Jonathan TAN Senior Consultant Dept of Anaesthesiology, Intensive Care & Pain Medicine Tan Tock Seng Hospital, Singapore Purpose? Healthcare professionals?
ICU Acquired Weakness: Role of Specific Nutrients Dr Jonathan TAN Senior Consultant Dept of Anaesthesiology, Intensive Care & Pain Medicine Tan Tock Seng Hospital, Singapore Purpose? Healthcare professionals?
5.1 Strategies to Optimize Delivery and Minimize Risks of EN: Feeding Protocols March 2013
 5.1 Strategies to Optimize Delivery and Minimize Risks of EN: Feeding Protocols March 2013 There were no new randomized controlled trials since the 2009 update and hence there are no changes to the following
5.1 Strategies to Optimize Delivery and Minimize Risks of EN: Feeding Protocols March 2013 There were no new randomized controlled trials since the 2009 update and hence there are no changes to the following
SASPEN: Meet the Expert. Pr. Me'e M Berger Service of Intensive Care & Burns CHUV Lausanne Switzerland
 SASPEN: Meet the Expert Pr. Me'e M Berger Service of Intensive Care & Burns CHUV Lausanne Switzerland 40 Ensuring my patients are properly fed. Nutrition therapy must be planned as any other ICU therapy
SASPEN: Meet the Expert Pr. Me'e M Berger Service of Intensive Care & Burns CHUV Lausanne Switzerland 40 Ensuring my patients are properly fed. Nutrition therapy must be planned as any other ICU therapy
Advanced Enteral Nutrition Program For Dietitians. Week 5 Underfeeding in the ICU: Good or Bad? Presented on December 9, 2015
 Advanced Enteral Nutrition Program For Dietitians Week 5 Underfeeding in the ICU: Good or Bad? Presented on December 9, 2015 Sponsor Disclosure: Financial support for this presentation was provided by
Advanced Enteral Nutrition Program For Dietitians Week 5 Underfeeding in the ICU: Good or Bad? Presented on December 9, 2015 Sponsor Disclosure: Financial support for this presentation was provided by
Stellenwert der prä- und postoperativen Sicht des Chirurgen
 Interdisziplinäre Chirurgie Stellenwert der prä- und postoperativen Ernährung Sicht des Chirurgen Kantonsspital Luzern 24.11.2005 Prof. L. Krähenbühl Chirurgische Klinik Hôpital Cantonal Fribourg Problems
Interdisziplinäre Chirurgie Stellenwert der prä- und postoperativen Ernährung Sicht des Chirurgen Kantonsspital Luzern 24.11.2005 Prof. L. Krähenbühl Chirurgische Klinik Hôpital Cantonal Fribourg Problems
5.3 Strategies to Optimize Delivery and Minimize Risks of EN: Small Bowel Feeding vs. Gastric May 2015
 5.3 Strategies to Optimize Delivery and Minimize Risks of EN: Small Bowel Feeding vs. Gastric May 2015 2015 Recommendation: Based on 16 level 2 studies, small bowel feeding compared to gastric feeding
5.3 Strategies to Optimize Delivery and Minimize Risks of EN: Small Bowel Feeding vs. Gastric May 2015 2015 Recommendation: Based on 16 level 2 studies, small bowel feeding compared to gastric feeding
Statistical Analysis Plan: Post-hoc analysis of the CALORIES trial
 Statistical Analysis Plan: Post-hoc analysis of the CALORIES trial Author: Version 1.0, Role, Name and Position Signature Date Chief investigator: Prof Kathryn Rowan (Director of Scientific & Strategic
Statistical Analysis Plan: Post-hoc analysis of the CALORIES trial Author: Version 1.0, Role, Name and Position Signature Date Chief investigator: Prof Kathryn Rowan (Director of Scientific & Strategic
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Influence of Calorie Protein Delivery on Outcomes and Body Composition. Changes in the Intensive Care Unit. Sarah Peterson
 Influence of Calorie Protein Delivery on Outcomes and Body Composition Changes in the Intensive Care Unit BY Sarah Peterson B.A., Nutrition and Dietetics, The College of St. Scholastica, Duluth, MN 1999
Influence of Calorie Protein Delivery on Outcomes and Body Composition Changes in the Intensive Care Unit BY Sarah Peterson B.A., Nutrition and Dietetics, The College of St. Scholastica, Duluth, MN 1999
5.2 Strategies to Optimize Delivery and Minimize Risks of EN: Motility Agents May 2015
 5.2 Strategies to Optimize Delivery and Minimize Risks of EN: Motility Agents May 2015 There were no new randomized controlled trials since the 2009 and 2013 updates and hence there are no changes to the
5.2 Strategies to Optimize Delivery and Minimize Risks of EN: Motility Agents May 2015 There were no new randomized controlled trials since the 2009 and 2013 updates and hence there are no changes to the
TOTAL PARENTERAL NUTRITION
 TOTAL PARENTERAL NUTRITION Indication See algorithm. Timing Start TPN as indicated on algorithm 1. There is no need to build up TPN volume. The volume of TPN (including lipids) should equate to the total
TOTAL PARENTERAL NUTRITION Indication See algorithm. Timing Start TPN as indicated on algorithm 1. There is no need to build up TPN volume. The volume of TPN (including lipids) should equate to the total
3.2 Nutritional Prescription of Enteral Nutrition: Enhanced Dose of Enteral Nutrition May 2015
 . Nutritional Prescription of Enteral Nutrition: Enhanced Dose of Enteral Nutrition May 015 015 Recommendation: Based on 1 level 1 study, level studies and cluster randomized controlled trials, when starting
. Nutritional Prescription of Enteral Nutrition: Enhanced Dose of Enteral Nutrition May 015 015 Recommendation: Based on 1 level 1 study, level studies and cluster randomized controlled trials, when starting
Nutrition Support. John Cha Department of Surgery DHMC/UCHSC
 Nutrition Support John Cha Department of Surgery DHMC/UCHSC Overview Why? When? How much? What route? Fancy stuff: enhanced nutrition Advantages of Nutrition Decreased catabolism Improved wound healing
Nutrition Support John Cha Department of Surgery DHMC/UCHSC Overview Why? When? How much? What route? Fancy stuff: enhanced nutrition Advantages of Nutrition Decreased catabolism Improved wound healing
/03/ $03.00/0 Vol. 27, No. 5 JOURNAL OF PARENTERAL AND ENTERAL NUTRITION
 0148-6071/03/2705-0355$03.00/0 Vol. 27, No. 5 JOURNAL OF PARENTERAL AND ENTERAL NUTRITION Printed in U.S.A. Copyright 2003 by the American Society for Parenteral and Enteral Nutrition Special Interest
0148-6071/03/2705-0355$03.00/0 Vol. 27, No. 5 JOURNAL OF PARENTERAL AND ENTERAL NUTRITION Printed in U.S.A. Copyright 2003 by the American Society for Parenteral and Enteral Nutrition Special Interest
Protein Supplementation in the Pediatric Intensive Care Unit. Jan Hau Lee, MBBS, MRCPCH, MCI Children s Intensive Care Unit 28 th July 2017
 Protein Supplementation in the Pediatric Intensive Care Unit Jan Hau Lee, MBBS, MRCPCH, MCI Children s Intensive Care Unit 28 th July 2017 1 Objectives Basis for protein supplementation Challenges in monitoring
Protein Supplementation in the Pediatric Intensive Care Unit Jan Hau Lee, MBBS, MRCPCH, MCI Children s Intensive Care Unit 28 th July 2017 1 Objectives Basis for protein supplementation Challenges in monitoring
Critically ill patients requiring vital organ support in the intensive
 The new england journal of medicine review article critical care medicine Nutrition in the Acute Phase of Critical Illness Michael P. Casaer, M.D., Ph.D., and Greet Van den Berghe, M.D., Ph.D. Critically
The new england journal of medicine review article critical care medicine Nutrition in the Acute Phase of Critical Illness Michael P. Casaer, M.D., Ph.D., and Greet Van den Berghe, M.D., Ph.D. Critically
Vanderbilt University Medical Center Trauma ICU Nutrition Management Guidelines
 Vanderbilt University Medical Center Trauma ICU Nutrition Management Guidelines Trauma Critical Care Nutrition Guidelines Clinical judgment may supersede guidelines as patient circumstances warrant ASSESSMENT
Vanderbilt University Medical Center Trauma ICU Nutrition Management Guidelines Trauma Critical Care Nutrition Guidelines Clinical judgment may supersede guidelines as patient circumstances warrant ASSESSMENT
A number of observational studies of adult
 Carol Rees Parrish, M.S., R.D., Series Editor Full Force Enteral Nutrition: A New Hope, or the Dark Side? A Critical Look at Enhanced Enteral Feeding Protocols Joe Krenitsky Enteral nutrition (EN) is the
Carol Rees Parrish, M.S., R.D., Series Editor Full Force Enteral Nutrition: A New Hope, or the Dark Side? A Critical Look at Enhanced Enteral Feeding Protocols Joe Krenitsky Enteral nutrition (EN) is the
ICU ENTERAL FEEDING GUIDELINES
 DISCLAIMER: These guidelines are intended to serve as a general statement regarding appropriate patient care practices based upon the available medical literature and clinical expertise at the time of
DISCLAIMER: These guidelines are intended to serve as a general statement regarding appropriate patient care practices based upon the available medical literature and clinical expertise at the time of
Acetaminophen recommendations from the Food and Drug Administration Advisory Committee
 TABLE OF CONTENTS Acetaminophen: recommendations from the FDA Advisory Committee 1 Recombinant human erythropoiesis-stimulating agents and mortality in cancer patients Hospital-acquired pneumonia: risks
TABLE OF CONTENTS Acetaminophen: recommendations from the FDA Advisory Committee 1 Recombinant human erythropoiesis-stimulating agents and mortality in cancer patients Hospital-acquired pneumonia: risks
ESPEN Congress Copenhagen 2016
 ESPEN Congress Copenhagen 2016 THE DIVERSITY OF OBESITY MALNUTRITION IN THE OBESE R. Barazzoni (IT) Malnutrition in the obese patient Rocco Barazzoni Dept of Medical, Surgical and Health Sciences University
ESPEN Congress Copenhagen 2016 THE DIVERSITY OF OBESITY MALNUTRITION IN THE OBESE R. Barazzoni (IT) Malnutrition in the obese patient Rocco Barazzoni Dept of Medical, Surgical and Health Sciences University
STRATEGIES TO IMPROVE ENTERAL FEEDING TOLERANCE. IS IT WORTH IT? ENGELA FRANCIS RD(SA)
") STRATEGIES TO IMPROVE ENTERAL FEEDING TOLERANCE. IS IT WORTH IT? ENGELA FRANCIS RD(SA) DEFINITION OF ENTERAL FEEDING INTOLERANCE Gastrointestinal feeding intolerance are usually defined as: High gastric
STRATEGIES TO IMPROVE ENTERAL FEEDING TOLERANCE. IS IT WORTH IT? ENGELA FRANCIS RD(SA) DEFINITION OF ENTERAL FEEDING INTOLERANCE Gastrointestinal feeding intolerance are usually defined as: High gastric
ESPEN Congress The Hague 2017
 ESPEN Congress The Hague 2017 Meeting nutritional needs of acute care patients Feeding acute pancreatitis patients J. Luttikhold (NL) FEEDING ACUTE PANCREATITIS PATIENTS Joanna Luttikhold, MD PhD Registrar
ESPEN Congress The Hague 2017 Meeting nutritional needs of acute care patients Feeding acute pancreatitis patients J. Luttikhold (NL) FEEDING ACUTE PANCREATITIS PATIENTS Joanna Luttikhold, MD PhD Registrar
10.2 Strategies to Optimize Parenteral Nutrition and Minimize Risks: Use of lipids May 2015
 10.2 Strategies to Optimize Parenteral Nutrition and Minimize Risks: Use of lipids May 2015 There are no new randomized controlled trials since the 2009 and 2013 updates and hence there are no changes
10.2 Strategies to Optimize Parenteral Nutrition and Minimize Risks: Use of lipids May 2015 There are no new randomized controlled trials since the 2009 and 2013 updates and hence there are no changes
Nutritional intervention in hospitalised paediatric patients. Dr Y.K.Amdekar
 Nutritional intervention in hospitalised paediatric patients Dr Y.K.Amdekar Back to basics Suboptimal nutrient intake is always dangerous in health and more so in disease to feed or not to feed is it a
Nutritional intervention in hospitalised paediatric patients Dr Y.K.Amdekar Back to basics Suboptimal nutrient intake is always dangerous in health and more so in disease to feed or not to feed is it a
Gastro-intestinal failure. ICU Fellowship Training Radboudumc
 Gastro-intestinal failure ICU Fellowship Training Radboudumc Case history (1) Male, 47 No previous medical history Mechanical ventilation for severe CAP Stable HD on NE 0.04 μg/kg/min Early enteral nutrition
Gastro-intestinal failure ICU Fellowship Training Radboudumc Case history (1) Male, 47 No previous medical history Mechanical ventilation for severe CAP Stable HD on NE 0.04 μg/kg/min Early enteral nutrition
Pediatric Nutrition Care as a strategy to prevent hospital malnutrition. Div Pediatric Nutrition and Metabolic Diseases Dept of Child Health
 Pediatric Nutrition Care as a strategy to prevent hospital malnutrition Div Pediatric Nutrition and Metabolic Diseases Dept of Child Health Child is not a miniature adult Specific for child growth and
Pediatric Nutrition Care as a strategy to prevent hospital malnutrition Div Pediatric Nutrition and Metabolic Diseases Dept of Child Health Child is not a miniature adult Specific for child growth and
Refeeding syndrome a practical approach
 Refeeding syndrome a practical approach PENG pre-bapen Conference Teaching Day Birmingham Monday 20 th November 2017 Rhys White Acting Clinical and Operational Lead Dietitian Guys and St Thomas NHS Foundation
Refeeding syndrome a practical approach PENG pre-bapen Conference Teaching Day Birmingham Monday 20 th November 2017 Rhys White Acting Clinical and Operational Lead Dietitian Guys and St Thomas NHS Foundation
ESPEN Congress Madrid 2018
 ESPEN Congress Madrid 2018 Dysglycaemia In Acute Patients With Nutritional Therapy Mechanisms And Consequences Of Dysglycaemia In Patients Receiving Nutritional Therapy M. León- Sanz (ES) Mechanisms and
ESPEN Congress Madrid 2018 Dysglycaemia In Acute Patients With Nutritional Therapy Mechanisms And Consequences Of Dysglycaemia In Patients Receiving Nutritional Therapy M. León- Sanz (ES) Mechanisms and
Feeding Protocols Enteral or Parenteral. AM Poleÿ 2012
 Practical aspects on Feeding Protocols Enteral or Parenteral AM Poleÿ 2012 Enteral Feeding Facts A reduction in mortality Prophylaxis for stress ulcers Full-strength Time to start enteral nutrition If
Practical aspects on Feeding Protocols Enteral or Parenteral AM Poleÿ 2012 Enteral Feeding Facts A reduction in mortality Prophylaxis for stress ulcers Full-strength Time to start enteral nutrition If
SCCM Critical Care Nutrition Guidelines: Would anything t:hange in a 2013 edition?
 SCCM Critical Care Nutrition Guidelines: Would anything t:hange in a 2013 edition? Robert G. Martindale MD, PhD Professor of Surgery Chief r Division of General Surgery Oregon Health and Science University
SCCM Critical Care Nutrition Guidelines: Would anything t:hange in a 2013 edition? Robert G. Martindale MD, PhD Professor of Surgery Chief r Division of General Surgery Oregon Health and Science University
Principles of nutrition in the preterm infant. Importance of nutrition: Undernutrition is very common in VLBW infants
 Principles of nutrition in the preterm infant Dr. S. Navarro-Psihas Pädiatrie IV, Klinik für Neonatologie Medizinische Universität Innsbruck Importance of nutrition: Undernutrition is very common in VLBW
Principles of nutrition in the preterm infant Dr. S. Navarro-Psihas Pädiatrie IV, Klinik für Neonatologie Medizinische Universität Innsbruck Importance of nutrition: Undernutrition is very common in VLBW
Recommendations, Quality of Evidence, and Recommendation Strength
 Recommendations, Quality of Evidence, and Recommendation Strength Category or Condition Recommendation Quality of Evidence Recommendation Strength Question: Does the use of a nutrition risk indicator identify
Recommendations, Quality of Evidence, and Recommendation Strength Category or Condition Recommendation Quality of Evidence Recommendation Strength Question: Does the use of a nutrition risk indicator identify
Extremely well tolerated. Feeding shock
 Extremely well tolerated Feeding shock FEEDING DURING CIRCULATORY FAILURE Dr S Omar Chris Hani Baragwanath Hospital Hospital/University of Witwatersrand Introduction Circulatory shock lack of adequate
Extremely well tolerated Feeding shock FEEDING DURING CIRCULATORY FAILURE Dr S Omar Chris Hani Baragwanath Hospital Hospital/University of Witwatersrand Introduction Circulatory shock lack of adequate
TPN and lipid. RCT of 57 patients. TPN with lipid vs TPN without lipid. TPN associated with increased infectious complications
 TPN and lipid RCT of 57 patients TPN with lipid vs TPN without lipid TPN associated with increased infectious complications * * * * Battistella FD, et al. J Trauma 1997; 43:52. Data Needed 1. New TPN trials
TPN and lipid RCT of 57 patients TPN with lipid vs TPN without lipid TPN associated with increased infectious complications * * * * Battistella FD, et al. J Trauma 1997; 43:52. Data Needed 1. New TPN trials