Ehab Abdel-Khalek, M.D.
|
|
|
- Ann Adele Andrews
- 6 years ago
- Views:
Transcription

1
2 Gastrointestinal prophylaxis in critically ill patients Ehab Abdel-Khalek, M.D. Professor of Hepatology and Gastroenterology, Faculty of Medicine, Mansoura University
3 Conflict of Interest I did not receive any financial support from the pharmaceutical companies whose medications were mentioned in this presentation.
4 Critical illness - Definition
5 A critical illness or injury acutely impairs one of more vital organ systems with a high probability of imminent life threatening deterioration in the patient s condition. Messmann H. Crit Care Med 2013; 15(2):
6 Early, specific signs of GI complications are rarely present. Because of late or missed diagnosis, morbidity and mortality related to these complications can be high. Martin B. Adv Crit Care 2007; 18(2):
7 Preventive measures Cost. Stay. Morbidity. Mortality.
8 Strategies related to GIT Stress Ulcer. Gastric Overdistension. Nutritional Support.
9 Stress ulcer Stress-related mucosal disease (SRMD)
10 Outline Definition History Epidemiology Pathophysiology Guidelines Agent Selection & Administration Complications
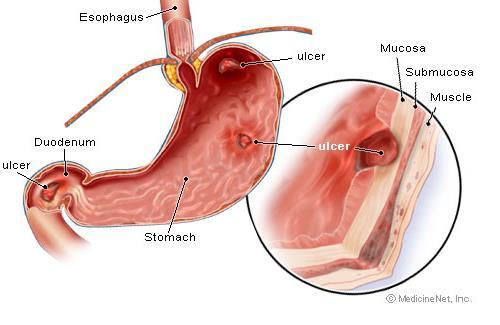
11 Definition Gastrointestinal mucosal injury related to critical illness. Stomach Duodenum Ileum Jejunum Macroscopic bleeding ASHP Therapeutic Guidelines on Stress Ulcer Prophylaxis. 2009; 15(2):
12
13 History 1842: Curling described series in burn patients 1932: Cushing reported ulcers with surgery and trauma 1970s: Development of H2 receptor antagonists Maton PN. Aliment Pharmacol Ther Dec;22 Suppl 3:45-52.
14 History 1990 s: Dr. Cook and the Canadian Critical Care Trials Group perform landmark trials on ICU usage of H2 receptor antagonists. 1990s to 2000: Proton Pump inhibitors make more efficient gastric alkalinization possible. Maton PN. Aliment Pharmacol Ther Dec;22 Suppl 3:45-52.
15 Epidemiology Up through the 1970, stress ulcers were much more common (>30% of ICU patients) Today, less than 5% of ICU patients have stress ulcers with macroscopic bleeding Del Valle J. Peptic Ulcer Disease and Related Disorders, 2010.
16 Pathophysiology Etiology is complex Decreased Gastric ph Ischemia Decreased mucus production Usually occur within hours of trauma/stress Del Valle J. Peptic Ulcer Disease and Related Disorders, 2010.
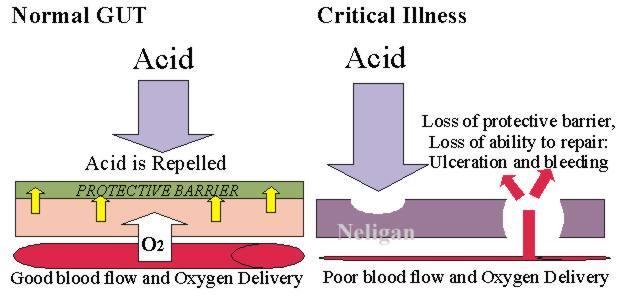
17 Pathophysiology

18 Pathophysiology Absent mucosal barrier + gastric acid =
 Therapeutic Guidelines on Stress Ulcer")
19 Guidelines American Society of Health-system pharmacists (ASHP) Therapeutic Guidelines on Stress Ulcer Prophylaxis
20 Key Guideline Points The Big 3 1. Coagulopathy Platelet count of <50,000mm3 INR>1.5 PTT of >2 times the control 2. Mechanical Ventilation Longer than 24 hours 3. Recent GI ulcers/bleeding Within 12 months of admission ASHP Therapeutic Guidelines on Stress Ulcer Prophylaxis, AJHP 1999;56(4): Pathophysiology and prophylaxis of stress ulcer in ICU patients. J Crit Care Mar;20(1):35-45.
21 Key Guideline Points The Little 2 or more of the following: 1. Sepsis 2. ICU>1 week 3. Occult Bleeding within 6 days 4. High dose corticosteroids 250mg Hydrocortisone 50mg Methylprednisone ASHP Therapeutic Guidelines on Stress Ulcer Prophylaxis, AJHP 1999; 56(4): Pathophysiology and prophylaxis of stress ulcer in ICU patients. J Crit Care Mar;20(1):35-45.
22 Prophylaxis Antacids Sucralfate Histamine 2 receptor antagonists Prostaglandin analogues Proton pump inhibitors Enteral feeding
23 Prophylactic Options Antacids: - Neutralize acid. - Must be given frequently and in larger volumes to be effective.
24 Prophylactic Options Sucralfate: - Adheres to epithelial cells and restores a cytoprotective barrier. - Binds bile salts - Stimulates prostaglandin synthesis - Stimulates local epidermal growth factor Goodman & Gilman s Pharmacological Basis of Therapeutics
25 Prophylactic Options H2 Blockers: - Inhibit acid secretion in a dose-dependent competitive manner. - Reduce volume of gastric acid and [H+] - Well absorbed with half life of 2 to 3 hours. - Most trials show lower risk of significant GI hemorrhage. Shuman, RB. Ann Int Med 2006; 106:
26 Prophylactic Options Prostaglandin analogues: - PGE 2 and PGI 2 inhibit acid secretion and increase mucus and bicarbonate. - May have a more useful role in patients who are dependent on NSAIDS. Goodman & Gilman s Pharmacological Basis of Therapeutics
27 Prophylactic Options Proton pump inhibitors: - The final mediator of acid secretion is the H+, K+ -- ATPase pump unique to the parietal cell. - PPIs are prodrugs that are activated by protonation and covalently bind to a cysteine residue and inactivate the ATPase enzyme. Goodman & Gilman s Pharmacological Basis of Therapeutics
28 Prophylactic Options NUTRITION In multiple burn studies, enteral nutrition alone had a significantly lower GI hemorrhage when compared to H2 Blockers. Raff, T. Burns 1997; 23:313
29 Agents and Dosing IV Agents Pantoprazole 40 mg (Q12-24h) Ranitidine 50mg (Q8h) Oral Agents PPI 40mg (Q24h) Ranitidine 150mg (Q12h) Sucralfate 1-2 grams 4 times per day Management Strategic Healthcare Group and the Medical Advisory Panel 2010; 39:
30 Proton pump inhibitors are at least as effective as histamine 2 receptor antagonists, as a large number of clinical trials have demonstrated. Maton PN. Aliment Pharmacol Ther. 2010; 3:45-52.
31 New data suggest that PPI inhibitors suppress acid production more completely in critically ill patients. Stollman N, Metz DC. J Crit Care. 2012; 20(1):35-45.
32 Negative Health Outcome Risks Associated With Acid Suppression Hospital Acquired Pneumonia(HAP). C. Difficile. Osteoporosis & Hip Fractures. 1. Herzig HJ et al, JAMA 2009;301(20): Dial, S, Delaney, AC, Barkun AN, et al. JAMA 2005;294(3): Yang et al. JAMA 2006:296(24): Targownik, LE et al. CMAJ 2008:179(4):

33 This patient with no Helicobacter infection got this ulcer during a period of severe somatic stress due to a heart disease.
34 Gastric overdistension
35 Mechanical ventilation in critically ill patients is theoretically associated with a number of gastrointestinal complications, including stress ulcers, hypomotility and diarrhoea. Other aspects of critical illness or the therapies used to treat it may further affect gastrointestinal function. Crit Care Resusc 2010; 12:
36 Although gastrointestinal dysfunction is not a priority in the critically ill, intestinal hypomotility may lead to: Malabsorption. Vomiting. Aspiration pneumonia. Bacterial overgrowth. Endotoxaemia. Crit Care Resusc 2010; 12:
37 Acute gastrointestinal (GI) dysfunction and failure have been increasingly recognized in critically ill patients. A. R. Blaser et al., Intensive Care Med 2012; 38:
38 The international Working Group on Abdominal Problems (WGAP) of the European Society of Intensive Care Medicine (ESICM) developed the definitions for GI dysfunction in intensive care patients. A. R. Blaser et al., Intensive Care Med 2012; 38:
39 Acute gastrointestinal injury (AGI) is a malfunctioning of the GI tract in intensive care patients due to their acute illness. A. R. Blaser et al., Intensive Care Med 2012; 38:
40 AGI grade I = Risk of developing GI dysfunction or failure (a self-limiting condition). AGI grade II = GI dysfunction (a condition that requires interventions). AGI grade III = GI failure (GI function cannot be restored with interventions). AGI grade IV = Dramatic GI failure with severe impact on distant organ function (a condition that is immediately life-threatening).
41 AGI grade I AGI grade I (risk of developing GI dysfunction or failure). Transient and partial impairement GI function.
42 Examples : AGI grade I - Nausea and vomiting after abdominal surgery. - Postoperative absence of bowel sounds. - Diminished bowel motility in the early phase of shock.
43 Management : AGI grade I - Fluid replacement by IV infusions. - Early enteral feeding, h after the injury. - Limitation of drugs impairing GI motility (e.g. catecholamines, opioids).
44 AGI grade II AGI grade II (gastrointestinal dysfunction) The GI tract is not able to perform digestion and absorption adequately. There are no changes in general condition of the patient related to GI problems.
45 AGI grade II Examples: - Gastroparesis with high gastric residuals or reflux. - Paralysis of the lower GI tract. - Intra-abdominal hypertension grade I. (IAP = mmhg). - Visible blood in gastric content or stool.
46 AGI grade II Management: - Prokinetic therapy. - Enteral feeding should be started or continued. - Initiation of postpyloric feeding in patients with gastroparesis.
47 AGI grade III AGI grade III: Loss of GI function, where restoration of GI function is not achieved despite interventions and the general condition is not improving.
48 AGI grade III Examples: - Feeding intolerance is persisting despite treatment. - High gastric residuals, persisting GI paralysis. - Progression of IAH to grade II (IAP mmhg). - Low abdominal perfusion pressure (APP) (below 60 mmhg).
49 Management: AGI grade III -Undiagnosed abdominal problems (cholecystitis, peritonitis, bowel ischaemia) should be excluded. - The medications promoting GI paralysis have to be discontinued as far as possible. - Challenges with small amounts of EN should be regularly considered.
50 AGI grade IV AGI grade IV: GI failure with severe impact on distant organ function. AGI has progressed to become directly and immediately life threatening, with worsening of MODS and shock.
51 Examples: AGI grade IV - Bowel ischaemia with necrosis. - GI bleeding leading to haemorrhagic shock. - Ogilvie s syndrome. -Abdominal compartment syndrome (ACS) requiring decompression.
52 Ogilvie syndrome acute pseudoobstruction and dilatation of the colon in the absence of any mechanical obstruction in severely ill patients.
53 Abdominal compartment syndrome - The abdomen becomes subject to increased pressure. - Cause: sepsis and severe abdominal trauma. - Increasing pressure reduces blood flow to abdominal organs and impairs pulmonary, cardiovascular, renal, and GI function, causing MODS and death.
54 Management: AGI grade IV Condition requires laparotomy or other emergency interventions. There is no proven conservative approach to resolve this situation.
55 Nutritional support
56 Critical illness increases nutrient requirements as well as alters metabolism. Patients in the ICU are unable to nourish themselves orally. Jeejeebhoy KN. Nutr Rev Nov;70(11):
57 ICU patients rapidly become malnourished unless they are provided with involuntary feeding either: - Enteral nutrition (EN): through a tube inserted into the GI tract, or - Parenteral nutrition (PN): directly into the bloodstream. Jeejeebhoy KN. Nutr Rev Nov;70(11):
58 Between the 1960s and the 1980s, PN was the modality of choice which led to overfeeding regimens called hyperalimentation. Later, the dangers of overfeeding, hyperglycemia, fatty liver, and increased sepsis associated with PN became recognized. Acosta E scribano J Med Intensiva, 2011 Nov;35 Suppl 1:77-80.
59 In contrast, EN was not associated with these risks and it gradually became the modality of choice in the ICU. Hence, the balanced perspective has been reached of using EN when possible but avoiding underfeeding by supplementing with PN when required. Acosta E scribano J Med Intensiva, 2011 Nov;35 Suppl 1:77-80.
60 Early EN is superior to delayed EN in the critically ill The expert committee, however favours that critically ill patients, who are haemodynamically stable and have a functioning gastrointestinal tract, should be fed early (< 24 h), if possible.
61 EN in critically ill patients During the acute and initial phase of critical illness, an exogenous energy supply of kcal/kg BW/day is needed. During recovery (anabolic flow phase), the aim is to provide total kcal/kg BW/day.
62 Protein requirement 1.5 g/kg/day. 2 g/kg/day in patients with trauma, severe burns, and head injury. 2.5 g/kg/day in adult patients treated with continuous renal replacement therapy (CRRT). nutritional support can only limit the loss of the body s protein and calorie stores. The goal is to administer sufficient nitrogen to provide a positive or neutral nitrogen balance.
63 Lipid requirements g/kg/d [ 20-40% of energy ] Lipid clearance is reduced in stressed patients due to decreased activity of lipoprotein lipase. infusion rate should not exceed 0.12 g/kg/hr to avoid the development of elevated TG levels. Source of essential FA, fat soluble vitamins. Avoid Omega 6 [ linoleic is a precursor of arachinodic acid].
64 Parenteral nutrition Indications: - In patients who cannot be fed sufficient enterally. - Intolerant to EN
65 Complications of PN PN associated with a more pronounced proinflammatory response than EN. Complications of excess dextrose infusion hyperglycemia hypertriglyceridemia hepatic steatosis, respiratory decompensation depression of immune function
66 SUMMARY
67 Acute gastrointestinal injury (AGI) is a malfunctioning of the GI tract in intensive care patients due to their acute illness. A. R. Blaser et al., Intensive Care Med 2012; 38:
68 AGI grade I = Risk of developing GI dysfunction or failure (a self-limiting condition). AGI grade II = GI dysfunction (a condition that requires interventions). AGI grade III = GI failure (GI function cannot be restored with interventions). AGI grade IV = Dramatic GI failure with severe impact on distant organ function (a condition that is immediately life-threatening).
69 Guideline Summary Big 3 1. Coagulopathy 2. Mechanical Ventilation 3. GI Bleeding within 12 months Little 4 (2 or more) 1. Sepsis 2. ICU>1 week 3. Occult Bleeding within 6 days 4. High dose corticosteroids


70
STRATEGIES TO IMPROVE ENTERAL FEEDING TOLERANCE. IS IT WORTH IT? ENGELA FRANCIS RD(SA)
") STRATEGIES TO IMPROVE ENTERAL FEEDING TOLERANCE. IS IT WORTH IT? ENGELA FRANCIS RD(SA) DEFINITION OF ENTERAL FEEDING INTOLERANCE Gastrointestinal feeding intolerance are usually defined as: High gastric
STRATEGIES TO IMPROVE ENTERAL FEEDING TOLERANCE. IS IT WORTH IT? ENGELA FRANCIS RD(SA) DEFINITION OF ENTERAL FEEDING INTOLERANCE Gastrointestinal feeding intolerance are usually defined as: High gastric
Stressed Out: Evaluating the Need for Stress Ulcer Prophylaxis in the ICU
 Stressed Out: Evaluating the Need for Stress Ulcer Prophylaxis in the ICU Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds November 8, 2016 2016 MFMER slide-1 Objectives Identify the significance
Stressed Out: Evaluating the Need for Stress Ulcer Prophylaxis in the ICU Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds November 8, 2016 2016 MFMER slide-1 Objectives Identify the significance
ENTERAL NUTRITION IN THE CRITICALLY ILL
 ENTERAL NUTRITION IN THE CRITICALLY ILL 1 Ebb phase Flow phase acute response (catabolic) adoptive response (anabolic) 2 3 Metabolic Response to Stress (catabolic phase) Glucose and Protein Metabolism
ENTERAL NUTRITION IN THE CRITICALLY ILL 1 Ebb phase Flow phase acute response (catabolic) adoptive response (anabolic) 2 3 Metabolic Response to Stress (catabolic phase) Glucose and Protein Metabolism
Audit: Use of stress ulcer prophylaxis in critically ill patients
 Audit: Use of stress ulcer prophylaxis in critically ill patients Dr. Sinan Bahlool Consultant, Anaesthetics & ITU Dr. Krushna Patel FY1 Dr. Andrew Baigey FY1 BACKGROUND Stress ulcer prophylaxis is prescribed
Audit: Use of stress ulcer prophylaxis in critically ill patients Dr. Sinan Bahlool Consultant, Anaesthetics & ITU Dr. Krushna Patel FY1 Dr. Andrew Baigey FY1 BACKGROUND Stress ulcer prophylaxis is prescribed
Optimal Drugs for ICU Stress Ulcer Prophylaxis: Other. Grand Rounds Monday August 9, 2010 Teresa Jones R2
 Optimal Drugs for ICU Stress Ulcer Prophylaxis: Other Grand Rounds Monday August 9, 2010 Teresa Jones R2 Outline Options besides PPIs Comparison to PPIs Negative Effects of PPIs Conclusion Do we really
Optimal Drugs for ICU Stress Ulcer Prophylaxis: Other Grand Rounds Monday August 9, 2010 Teresa Jones R2 Outline Options besides PPIs Comparison to PPIs Negative Effects of PPIs Conclusion Do we really
GASTROINTESTINAL AND ANTIEMETIC DRUGS. Submitted by: Shaema M. Ali
 GASTROINTESTINAL AND ANTIEMETIC DRUGS Submitted by: Shaema M. Ali GASTROINTESTINAL AND ANTIEMETIC DRUGS by: Shaema M. Ali There are four common medical conditions involving the GI system 1) peptic ulcers
GASTROINTESTINAL AND ANTIEMETIC DRUGS Submitted by: Shaema M. Ali GASTROINTESTINAL AND ANTIEMETIC DRUGS by: Shaema M. Ali There are four common medical conditions involving the GI system 1) peptic ulcers
Appropriate Use of Proton Pump Inhibitors (PPIs) Anderson Mabour, Pharm.D., BCPS Clinical Pharmacy Specialist
 Anderson Mabour, Pharm.D., BCPS Clinical Pharmacy Specialist") Appropriate Use of Proton Pump Inhibitors (PPIs) Anderson Mabour, Pharm.D., BCPS Clinical Pharmacy Specialist Disclosures I have no actual or potential conflicts of interest to report in relation to this
Appropriate Use of Proton Pump Inhibitors (PPIs) Anderson Mabour, Pharm.D., BCPS Clinical Pharmacy Specialist Disclosures I have no actual or potential conflicts of interest to report in relation to this
ICU NUTRITION UPDATE : ESPEN GUIDELINES Mirey Karavetian Assistant Professor Zayed University
 ICU NUTRITION UPDATE : ESPEN GUIDELINES 2018 Mirey Karavetian Assistant Professor Zayed University http://www.espen.org/files/espen- Guidelines/ESPEN_Guideline_on_clinical_nutrition_in_-ICU.pdf Medical
ICU NUTRITION UPDATE : ESPEN GUIDELINES 2018 Mirey Karavetian Assistant Professor Zayed University http://www.espen.org/files/espen- Guidelines/ESPEN_Guideline_on_clinical_nutrition_in_-ICU.pdf Medical
Case 4: Peptic Ulcer Disease. Requejo, April Salandanan, Geralyn Talingting, Vennessa Tanay, Arvie
 Case 4: Peptic Ulcer Disease Requejo, April Salandanan, Geralyn Talingting, Vennessa Tanay, Arvie Case 4: PUD Problem List: 1. Peptic Ulcer Disease SOAP Note: S Patient is complaining of abdominal pain
Case 4: Peptic Ulcer Disease Requejo, April Salandanan, Geralyn Talingting, Vennessa Tanay, Arvie Case 4: PUD Problem List: 1. Peptic Ulcer Disease SOAP Note: S Patient is complaining of abdominal pain
A. Incorrect! Histamine is a secretagogue for stomach acid, but this is not the only correct answer.
 Pharmacology - Problem Drill 21: Drugs Used To Treat GI Disorders No. 1 of 10 1. Endogenous secretagogues for stomach acid include: #01 (A) Histamine (B) Gastrin (C) PGE1 (D) A and B (E) A, B and C Histamine
Pharmacology - Problem Drill 21: Drugs Used To Treat GI Disorders No. 1 of 10 1. Endogenous secretagogues for stomach acid include: #01 (A) Histamine (B) Gastrin (C) PGE1 (D) A and B (E) A, B and C Histamine
ESPEN Congress The Hague 2017
 ESPEN Congress The Hague 2017 Meeting nutritional needs of acute care patients Feeding acute pancreatitis patients J. Luttikhold (NL) FEEDING ACUTE PANCREATITIS PATIENTS Joanna Luttikhold, MD PhD Registrar
ESPEN Congress The Hague 2017 Meeting nutritional needs of acute care patients Feeding acute pancreatitis patients J. Luttikhold (NL) FEEDING ACUTE PANCREATITIS PATIENTS Joanna Luttikhold, MD PhD Registrar
STRESS ULCER PROPHYLAXIS SUMMARY
 DISCLAIMER: These guidelines were prepared jointly by the Surgical Critical Care and Medical Critical Care Services at Orlando Regional Medical Center. They are intended to serve as a general statement
DISCLAIMER: These guidelines were prepared jointly by the Surgical Critical Care and Medical Critical Care Services at Orlando Regional Medical Center. They are intended to serve as a general statement
VUMC Multidisciplinary Surgical Critical Care
 VUMC Multidisciplinary Surgical Critical Care Gastrointestinal Stress Ulcer Prophylaxis Guideline: Background: Work by Cooke and colleagues ascribed the risk of overt bleeding to be 4.4% and clinically
VUMC Multidisciplinary Surgical Critical Care Gastrointestinal Stress Ulcer Prophylaxis Guideline: Background: Work by Cooke and colleagues ascribed the risk of overt bleeding to be 4.4% and clinically
CHAPTER 18. PEPTIC ULCER DISEASE, SELF-ASSESSMENT QUESTIONS. 1. Which of the following is not a common cause of peptic ulcer disease (PUD)?
?") CHAPTER 18. PEPTIC ULCER DISEASE, SELF-ASSESSMENT QUESTIONS 1. Which of the following is not a common cause of peptic ulcer disease (PUD)? A. Chronic alcohol ingestion B. Nonsteroidal antiinflammatory
CHAPTER 18. PEPTIC ULCER DISEASE, SELF-ASSESSMENT QUESTIONS 1. Which of the following is not a common cause of peptic ulcer disease (PUD)? A. Chronic alcohol ingestion B. Nonsteroidal antiinflammatory
Gastroduodenal Stress Ulceration. Bryan Woolridge POS Rounds 29 October 2003
 Gastroduodenal Stress Ulceration Bryan Woolridge POS Rounds 29 October 2003 Objectives Define entity Etiology Differentiation of UGI ulcers Pathophysiology Identify population at risk/risk factors Clinical
Gastroduodenal Stress Ulceration Bryan Woolridge POS Rounds 29 October 2003 Objectives Define entity Etiology Differentiation of UGI ulcers Pathophysiology Identify population at risk/risk factors Clinical
GI Pharmacology. Dr. Alia Shatanawi 5/4/2018
 GI Pharmacology Dr. Alia Shatanawi 5/4/2018 Drugs Used in Gastrointestinal Diseases Drugs used in Peptic Ulcer Diseases. Drugs Stimulating Gastrointestinal Motility &Laxatives. Antidiarrheal Agents. Drugs
GI Pharmacology Dr. Alia Shatanawi 5/4/2018 Drugs Used in Gastrointestinal Diseases Drugs used in Peptic Ulcer Diseases. Drugs Stimulating Gastrointestinal Motility &Laxatives. Antidiarrheal Agents. Drugs
Providing Optimal Nutritional Support on the ICU common problems and practical solutions. Pete Turner Specialist Nutritional Support Dietitian
 Providing Optimal Nutritional Support on the ICU common problems and practical solutions Pete Turner Specialist Nutritional Support Dietitian ICU Nutritional Support ACCEPT study showed improved ICU survival
Providing Optimal Nutritional Support on the ICU common problems and practical solutions Pete Turner Specialist Nutritional Support Dietitian ICU Nutritional Support ACCEPT study showed improved ICU survival
L.Mageswary Dietitian Hospital Selayang
 L.Mageswary Dietitian Hospital Selayang 14 15 AUG ASMIC 2015 Learning Objectives 1. To understand the importance of nutrition support in ICU 2. To know the right time to feed 3. To understand the indications
L.Mageswary Dietitian Hospital Selayang 14 15 AUG ASMIC 2015 Learning Objectives 1. To understand the importance of nutrition support in ICU 2. To know the right time to feed 3. To understand the indications
Practical Guide to Safety of PPIs What to Tell Your Patient. Proton Pump Inhibitors
 Practical Guide to Safety of PPIs What to Tell Your Patient Joel E Richter, MD, FACP, MACG Professor and Director Division of Digestive Diseases and Nutrition Joy Culverhouse Center for Esophageal Diseases
Practical Guide to Safety of PPIs What to Tell Your Patient Joel E Richter, MD, FACP, MACG Professor and Director Division of Digestive Diseases and Nutrition Joy Culverhouse Center for Esophageal Diseases
Home Total Parenteral Nutrition for Adults
 Home Total Parenteral Nutrition for Adults Policy Number: Original Effective Date: MM.08.007 05/21/1999 Line(s) of Business: Current Effective Date: PPO, HMO, QUEST Integration 05/27/2016 Section: Home
Home Total Parenteral Nutrition for Adults Policy Number: Original Effective Date: MM.08.007 05/21/1999 Line(s) of Business: Current Effective Date: PPO, HMO, QUEST Integration 05/27/2016 Section: Home
Metabolic Control in Critical Care: Nutrition Therapy
 LOGO Metabolic Control in Critical Care: Nutrition Therapy ผศ.นพ.พรพจน เปรมโยธ น สาขาโภชนาการคล น ก ภาคว ชาอาย รศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล 2016 SCCM/ASPEN Guidelines Nutrition Therapy in the ICU
LOGO Metabolic Control in Critical Care: Nutrition Therapy ผศ.นพ.พรพจน เปรมโยธ น สาขาโภชนาการคล น ก ภาคว ชาอาย รศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล 2016 SCCM/ASPEN Guidelines Nutrition Therapy in the ICU
Stress Ulcer Prophylaxis In The ICU. Scott W. Wolf Anesthesiology Critical Care Medicine
 Stress Ulcer Prophylaxis In The ICU Scott W. Wolf Anesthesiology Critical Care Medicine Some history Stress Ulceration described in ICU patients as long as 45 years ago Patients had a constellation of
Stress Ulcer Prophylaxis In The ICU Scott W. Wolf Anesthesiology Critical Care Medicine Some history Stress Ulceration described in ICU patients as long as 45 years ago Patients had a constellation of
Disclosures. None. Enteral Nutrition and Vasoactive Therapy! But actually.. Stocks Advisory boards Grants Speakers Bureau. Paul Marik, MD,FCCM,FCCP
 Enteral Nutrition and Vasoactive Therapy! Paul Marik, MD,FCCM,FCCP Disclosures Stocks Advisory boards Grants Speakers Bureau None But actually.. 1 We suggest a determination of nutrition risk (NUTRIC score)
Enteral Nutrition and Vasoactive Therapy! Paul Marik, MD,FCCM,FCCP Disclosures Stocks Advisory boards Grants Speakers Bureau None But actually.. 1 We suggest a determination of nutrition risk (NUTRIC score)
Nutritional intervention in hospitalised paediatric patients. Dr Y.K.Amdekar
 Nutritional intervention in hospitalised paediatric patients Dr Y.K.Amdekar Back to basics Suboptimal nutrient intake is always dangerous in health and more so in disease to feed or not to feed is it a
Nutritional intervention in hospitalised paediatric patients Dr Y.K.Amdekar Back to basics Suboptimal nutrient intake is always dangerous in health and more so in disease to feed or not to feed is it a
WHEN To Initiate Parenteral Nutrition A Frequent Question With New Answers
 WHEN To Initiate Parenteral Nutrition A Frequent Question With New Answers Ainsley Malone, MS, RD, LD, CNSC, FAND, FASPEN Dubai International Nutrition Conference 2018 Disclosures No commercial relationship
WHEN To Initiate Parenteral Nutrition A Frequent Question With New Answers Ainsley Malone, MS, RD, LD, CNSC, FAND, FASPEN Dubai International Nutrition Conference 2018 Disclosures No commercial relationship
Module 2 Heartburn Glossary
 Absorption Antacids Antibiotic Module 2 Heartburn Glossary Barrett s oesophagus Bloating Body mass index Burping Chief cells Colon Digestion Endoscopy Enteroendocrine cells Epiglottis Epithelium Absorption
Absorption Antacids Antibiotic Module 2 Heartburn Glossary Barrett s oesophagus Bloating Body mass index Burping Chief cells Colon Digestion Endoscopy Enteroendocrine cells Epiglottis Epithelium Absorption
Do PPIs Reduce Bleeding in ICU? Revisiting Stress Ulcer Prophylaxis. Deborah Cook
 Do PPIs Reduce Bleeding in ICU? Revisiting Stress Ulcer Prophylaxis Deborah Cook ICU-Acquired Upper GI Bleeding Case series of 300 ICU patients describing stressrelated erosive syndrome Frequent Fatal
Do PPIs Reduce Bleeding in ICU? Revisiting Stress Ulcer Prophylaxis Deborah Cook ICU-Acquired Upper GI Bleeding Case series of 300 ICU patients describing stressrelated erosive syndrome Frequent Fatal
ESPEN Congress The Hague 2017
 ESPEN Congress The Hague 2017 Using the gut in acute care patients Permissive underfeeding in practice J.-C. Preiser (BE) PERMISSIVE UNDERFEEDING IN PRACTICE ESPEN congress Jean-Charles Preiser, M.D.,
ESPEN Congress The Hague 2017 Using the gut in acute care patients Permissive underfeeding in practice J.-C. Preiser (BE) PERMISSIVE UNDERFEEDING IN PRACTICE ESPEN congress Jean-Charles Preiser, M.D.,
The presence and development of gastric ulcers. Evaluation of Stress Ulcer Prophylaxis in a Family Medicine Residency Inpatient Service
 Evaluation of Stress Ulcer Prophylaxis in a Family Medicine Residency Inpatient Service Heather A. Kehr, PharmD, BCPS, Carrie L. Griffiths, PharmD, R. Wesley Haynes, PharmD, Sonia Everhart, PharmD, BCPS,
Evaluation of Stress Ulcer Prophylaxis in a Family Medicine Residency Inpatient Service Heather A. Kehr, PharmD, BCPS, Carrie L. Griffiths, PharmD, R. Wesley Haynes, PharmD, Sonia Everhart, PharmD, BCPS,
By; Ashraf El Houfi MD MS (pulmonology) MRCP (UK) FRCP (London) EDIC Consultant ICU Dubai Hospital
 MRCP (UK) FRCP (London) EDIC Consultant ICU Dubai Hospital") By; Ashraf El Houfi MD MS (pulmonology) MRCP (UK) FRCP (London) EDIC Consultant ICU Dubai Hospital Introduction The significance of nutrition in hospital setting (especially the ICU) cannot be overstated.
By; Ashraf El Houfi MD MS (pulmonology) MRCP (UK) FRCP (London) EDIC Consultant ICU Dubai Hospital Introduction The significance of nutrition in hospital setting (especially the ICU) cannot be overstated.
Gastro-oesophageal reflux disease and peptic ulcer disease. By: Dr. Singanamala Suman Assistant Professor Department of Pharm.D
 Gastro-oesophageal reflux disease and peptic ulcer disease By: Dr. Singanamala Suman Assistant Professor Department of Pharm.D Gastro-oesophageal reflux disease and peptic ulcer disease Learning objectives:
Gastro-oesophageal reflux disease and peptic ulcer disease By: Dr. Singanamala Suman Assistant Professor Department of Pharm.D Gastro-oesophageal reflux disease and peptic ulcer disease Learning objectives:
VAP Prevention bundles
 VAP Prevention bundles Dr. Shafiq A.Alimad MD Head of medical department at USTH YICID workshop, 15-12-2014 Care Bundles What are they & why use them? What are Care Bundles? Types of Care Bundles available
VAP Prevention bundles Dr. Shafiq A.Alimad MD Head of medical department at USTH YICID workshop, 15-12-2014 Care Bundles What are they & why use them? What are Care Bundles? Types of Care Bundles available
Fecal incontinence causes 196 epidemiology 8 treatment 196
 Subject Index Achalasia course 93 differential diagnosis 93 esophageal dysphagia 92 95 etiology 92, 93 treatment 93 95 work-up 93 Aminosalicylates, pharmacokinetics and aging effects 36 Antibiotics diarrhea
Subject Index Achalasia course 93 differential diagnosis 93 esophageal dysphagia 92 95 etiology 92, 93 treatment 93 95 work-up 93 Aminosalicylates, pharmacokinetics and aging effects 36 Antibiotics diarrhea
Peptic ulcer disease Disorders of the esophagus
 Peptic ulcer disease Disorders of the esophagus Peptic ulcer disease Burning epigastric pain Exacerbated by fasting Improved with meals Ulcer: disruption of mucosal integrity >5 mm in size, with depth
Peptic ulcer disease Disorders of the esophagus Peptic ulcer disease Burning epigastric pain Exacerbated by fasting Improved with meals Ulcer: disruption of mucosal integrity >5 mm in size, with depth
Proton Pump Inhibitors- Questions & Controversies. Farah Kablaoui, PharmD, BCPS, BCCCP
 Proton Pump Inhibitors- Questions & Controversies Farah Kablaoui, PharmD, BCPS, BCCCP Disclosure Information Proton Pump Inhibitors: Questions & Controversies Farah Kablaoui I have no financial relationship
Proton Pump Inhibitors- Questions & Controversies Farah Kablaoui, PharmD, BCPS, BCCCP Disclosure Information Proton Pump Inhibitors: Questions & Controversies Farah Kablaoui I have no financial relationship
Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Enteral Nutrition Algorithm Clinical Practice Guideline
 Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Enteral Nutrition Algorithm Clinical Practice Guideline Original Date: 08/2011 Purpose: To promote the early use of
Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Enteral Nutrition Algorithm Clinical Practice Guideline Original Date: 08/2011 Purpose: To promote the early use of
Comparison of the clinical characteristics and prognosis of primary versus secondary acute gastrointestinal injury in critically ill patients
 Zhang et al. Journal of Intensive Care (2017) 5:26 DOI 10.1186/s40560-017-0221-4 RESEARCH Open Access Comparison of the clinical characteristics and prognosis of primary versus secondary acute gastrointestinal
Zhang et al. Journal of Intensive Care (2017) 5:26 DOI 10.1186/s40560-017-0221-4 RESEARCH Open Access Comparison of the clinical characteristics and prognosis of primary versus secondary acute gastrointestinal
Nutrition and Sepsis
 Nutrition and Sepsis Todd W. Rice, MD, MSc Associate Professor of Medicine Vanderbilt University 2017 DNS Symposium June 2, 2017 Case 55 y.o. male COPD, DM, HTN, presents with pneumonia and septic shock.
Nutrition and Sepsis Todd W. Rice, MD, MSc Associate Professor of Medicine Vanderbilt University 2017 DNS Symposium June 2, 2017 Case 55 y.o. male COPD, DM, HTN, presents with pneumonia and septic shock.
Second term/
 Second term/ 2015-2016 L. 1 Dr Mohammed AL-Zobaidy Learning objectives GIT pharmacology After completing this chapter the student will be able to: Recognise pathophysiological factors implicated in acid-peptic
Second term/ 2015-2016 L. 1 Dr Mohammed AL-Zobaidy Learning objectives GIT pharmacology After completing this chapter the student will be able to: Recognise pathophysiological factors implicated in acid-peptic
PARENTERAL NUTRITION THERAPY
 UnitedHealthcare Benefits of Texas, Inc. 1. UnitedHealthcare of Oklahoma, Inc. 2. UnitedHealthcare of Oregon, Inc. UnitedHealthcare of Washington, Inc. UnitedHealthcare West BENEFIT INTERPRETATION POLICY
UnitedHealthcare Benefits of Texas, Inc. 1. UnitedHealthcare of Oklahoma, Inc. 2. UnitedHealthcare of Oregon, Inc. UnitedHealthcare of Washington, Inc. UnitedHealthcare West BENEFIT INTERPRETATION POLICY
Chapter 34. Prevention of Clinically Significant Gastrointestinal Bleeding in Intensive Care Unit Patients
 Chapter 34. Prevention of Clinically Significant Gastrointestinal Bleeding in Intensive Care Unit Patients Daniel D. Dressler, MD Mark V. Williams, MD Kimberly Rask, MD, PhD Emory University Schools of
Chapter 34. Prevention of Clinically Significant Gastrointestinal Bleeding in Intensive Care Unit Patients Daniel D. Dressler, MD Mark V. Williams, MD Kimberly Rask, MD, PhD Emory University Schools of
Nutritional Management in Enterocutaneous fistula Dr Deepak Govil
 Nutritional Management in Enterocutaneous fistula Dr Deepak Govil MS, PhD (GI Surgery) Senior Consultant Surgical Gastroenterology Indraprastha Apollo Hospital New Delhi What is enterocutaneous fistula
Nutritional Management in Enterocutaneous fistula Dr Deepak Govil MS, PhD (GI Surgery) Senior Consultant Surgical Gastroenterology Indraprastha Apollo Hospital New Delhi What is enterocutaneous fistula
The Role of Parenteral Nutrition. in PEDIATRIC INTENSIVE CARE UNIT. Dzulfikar DLH. Pediatric Emergency and Intensive Care Unit
 The Role of Parenteral Nutrition in PEDIATRIC INTENSIVE CARE UNIT Dzulfikar DLH Pediatric Emergency and Intensive Care Unit Department of Child Health, Faculty of Medicine Universitas Padjajaran, Hasan
The Role of Parenteral Nutrition in PEDIATRIC INTENSIVE CARE UNIT Dzulfikar DLH Pediatric Emergency and Intensive Care Unit Department of Child Health, Faculty of Medicine Universitas Padjajaran, Hasan
Scott A. Lynch, MD, MPH,FAAFP Assistant Professor
 Scott A. Lynch, MD, MPH,FAAFP Assistant Professor Lynch.Scott@mayo.edu 2015 MFMER 3543652-1 Nutrition in the Hospital Mayo School of Continuous Professional Development 2nd Annual Inpatient Medicine for
Scott A. Lynch, MD, MPH,FAAFP Assistant Professor Lynch.Scott@mayo.edu 2015 MFMER 3543652-1 Nutrition in the Hospital Mayo School of Continuous Professional Development 2nd Annual Inpatient Medicine for
Surgery while taking Protonix? 1,368 conversations on the web about experiences with taking Protonix before or after having a Surgery.
 Surgery while taking Protonix? 1,368 conversations on the web about experiences with taking Protonix before or after having a Surgery. Everything you ever wanted to know about gastric sleeve surgery. What
Surgery while taking Protonix? 1,368 conversations on the web about experiences with taking Protonix before or after having a Surgery. Everything you ever wanted to know about gastric sleeve surgery. What
Int. Med J Vol. 6 No 1 June 2007 Enteral Nutrition In Intensive Care: Tiger Tube For Small Bowel Feeding In Acute Pancreatitis.
 Page 1 of 6 Int. Med J Vol. 6 No 1 June 2007 Enteral Nutrition In Intensive Care: Tiger Tube For Small Bowel Feeding In Acute Pancreatitis. Case Report Mohd Basri bin Mat Nor. Department of Anaesthesiology
Page 1 of 6 Int. Med J Vol. 6 No 1 June 2007 Enteral Nutrition In Intensive Care: Tiger Tube For Small Bowel Feeding In Acute Pancreatitis. Case Report Mohd Basri bin Mat Nor. Department of Anaesthesiology
Chapter 20 The Digestive System Exam Study Questions
 Chapter 20 The Digestive System Exam Study Questions 20.1 Overview of GI Processes 1. Describe the functions of digestive system. 2. List and define the four GI Processes: 20.2 Functional Anatomy of the
Chapter 20 The Digestive System Exam Study Questions 20.1 Overview of GI Processes 1. Describe the functions of digestive system. 2. List and define the four GI Processes: 20.2 Functional Anatomy of the
Postoperative Ileus. UCSF Postgraduate Course in General Surgery Maui, HI March 20, 2011
 Postoperative Ileus UCSF Postgraduate Course in General Surgery Maui, HI March 20, 2011 Hobart W. Harris, MD, MPH Introduction Pathophysiology Clinical Research Management Summary Postoperative Ileus:
Postoperative Ileus UCSF Postgraduate Course in General Surgery Maui, HI March 20, 2011 Hobart W. Harris, MD, MPH Introduction Pathophysiology Clinical Research Management Summary Postoperative Ileus:
Current concepts in Critical Care Nutrition
 Current concepts in Critical Care Nutrition Dr.N.Ramakrishnan AB (Int Med), AB (Crit Care), MMM, FACP, FCCP, FCCM Director, Critical Care Services Apollo Hospitals, Chennai Objectives Why? Enteral or Parenteral
Current concepts in Critical Care Nutrition Dr.N.Ramakrishnan AB (Int Med), AB (Crit Care), MMM, FACP, FCCP, FCCM Director, Critical Care Services Apollo Hospitals, Chennai Objectives Why? Enteral or Parenteral
Overview of digestion or, gut reactions - to food
 Key concepts in Digestion. Indigestion module Overview of digestion or, gut reactions - to food Prof. Barry Campbell Gastroenterology Cellular & Molecular Physiology e-mail: bjcampbl@liv.ac.uk http://pcwww.liv.ac.uk/~bjcampbl
Key concepts in Digestion. Indigestion module Overview of digestion or, gut reactions - to food Prof. Barry Campbell Gastroenterology Cellular & Molecular Physiology e-mail: bjcampbl@liv.ac.uk http://pcwww.liv.ac.uk/~bjcampbl
Small Bowel Obstruction after operation in a severely malnourished man. By: Ms Bounmark Phoumesy
 Small Bowel Obstruction after operation in a severely malnourished man By: Ms Bounmark Phoumesy Normal length of GI tract Normal length(achieved by age 9) Small bowel 600cm (Men: 630 cm; Women: 592 cm)
Small Bowel Obstruction after operation in a severely malnourished man By: Ms Bounmark Phoumesy Normal length of GI tract Normal length(achieved by age 9) Small bowel 600cm (Men: 630 cm; Women: 592 cm)
Pancreatitis. Acute Pancreatitis
 Pancreatitis Pancreatitis is an inflammation of the pancreas. The pancreas is a large gland behind the stomach and close to the duodenum. The duodenum is the upper part of the small intestine. The pancreas
Pancreatitis Pancreatitis is an inflammation of the pancreas. The pancreas is a large gland behind the stomach and close to the duodenum. The duodenum is the upper part of the small intestine. The pancreas
Nutrition in ECMO. Elize Craucamp RD(SA)
") Nutrition in ECMO Elize Craucamp RD(SA) ECMO What now!? KEEP CALM AND FEED THE ECMO PATIENT Despite the fact that little is known about nutritional strategies for adult ECMO patients! Neither overcomplicate
Nutrition in ECMO Elize Craucamp RD(SA) ECMO What now!? KEEP CALM AND FEED THE ECMO PATIENT Despite the fact that little is known about nutritional strategies for adult ECMO patients! Neither overcomplicate
Proton Pump Inhibitors:
 Proton Pump Inhibitors: How bad could they be? Andrea Flanagan, Pharm.D. Iowa City VA Medical Center PGY-1 Pharmacy Resident Objectives for Pharmacists At the end of this presentation PHARMACISTS should
Proton Pump Inhibitors: How bad could they be? Andrea Flanagan, Pharm.D. Iowa City VA Medical Center PGY-1 Pharmacy Resident Objectives for Pharmacists At the end of this presentation PHARMACISTS should
PARENTERAL NUTRITION
 PARENTERAL NUTRITION DEFINITION Parenteral nutrition [(PN) or total parenteral nutrition (TPN)] is the intravenous infusion of some or all nutrients for tissue maintenance, metabolic requirements and growth
PARENTERAL NUTRITION DEFINITION Parenteral nutrition [(PN) or total parenteral nutrition (TPN)] is the intravenous infusion of some or all nutrients for tissue maintenance, metabolic requirements and growth
Peptic Ulcer Disease: Zollinger-Ellison Syndrome
 GASTROINTESTINAL PHYSIOLOGY 235 Case 41 Peptic Ulcer Disease: Zollinger-Ellison Syndrome Abe Rosenfeld, who is 47 years old, owns a house painting business with his brothers. The brothers pride themselves
GASTROINTESTINAL PHYSIOLOGY 235 Case 41 Peptic Ulcer Disease: Zollinger-Ellison Syndrome Abe Rosenfeld, who is 47 years old, owns a house painting business with his brothers. The brothers pride themselves
KK College of Nursing Peptic Ulcer Badil D ass Dass, Lecturer 25th July, 2011
 KK College of Nursing Peptic Ulcer Badil Dass, Lecturer 25 th July, 2011 Objectives: By the end of this lecture, the students t will be able to: Define peptic pp ulcer Describe the etiology and pathology
KK College of Nursing Peptic Ulcer Badil Dass, Lecturer 25 th July, 2011 Objectives: By the end of this lecture, the students t will be able to: Define peptic pp ulcer Describe the etiology and pathology
Overview of digestion or, gut reactions - to food
 1 Key concepts in Digestion. Indigestion module Overview of digestion or, gut reactions to food Prof. Barry Campbell Gastroenterology Cellular & Molecular Physiology email: bjcampbl@liv.ac.uk http://pcwww.liv.ac.uk/~bjcampbl
1 Key concepts in Digestion. Indigestion module Overview of digestion or, gut reactions to food Prof. Barry Campbell Gastroenterology Cellular & Molecular Physiology email: bjcampbl@liv.ac.uk http://pcwww.liv.ac.uk/~bjcampbl
Canadian Trauma Trials Collaborative. Occult Pneumothorax in Critical Care (OPTICC): Standardized Data Collection Sheet
: Standardized Data Collection Sheet") Canadian Trauma Trials Collaborative STUDY CENTRE: Institution: City / Province: / Occult Pneumothorax in Critical Care (OPTICC): Standardized Sheet PATIENT DEMOGRAPHICS: First Name: Health record number
Canadian Trauma Trials Collaborative STUDY CENTRE: Institution: City / Province: / Occult Pneumothorax in Critical Care (OPTICC): Standardized Sheet PATIENT DEMOGRAPHICS: First Name: Health record number
PPIs: Good or Bad? 1. Basics of PPIs. Gastric Acid Basics. Outline. Gastric Acid Basics. Proton Pump Inhibitors (PPI)
") Outline Quick basics on Proton Pump Inhibitors (PPIs) PPIs: Good or Bad? What are potential risks of PPI therapy? How to approach your patients American Gastroenterology Association (AGA) recommendations
Outline Quick basics on Proton Pump Inhibitors (PPIs) PPIs: Good or Bad? What are potential risks of PPI therapy? How to approach your patients American Gastroenterology Association (AGA) recommendations
Who Needs Parenteral Nutrition? Is Parenteral Nutrition An Appropriate Intervention?
 Who Needs Parenteral Nutrition? 1 Is Parenteral Nutrition An Appropriate Intervention? Key questions to ask with initial consultation Can the gastrointestinal (GI) tract be utilized? Can the GI tract be
Who Needs Parenteral Nutrition? 1 Is Parenteral Nutrition An Appropriate Intervention? Key questions to ask with initial consultation Can the gastrointestinal (GI) tract be utilized? Can the GI tract be
Enteral and parenteral nutrition in GI failure and short bowel syndrome
 Enteral and parenteral nutrition in GI failure and short bowel syndrome Alastair Forbes University College London Intestinal failure Inadequate functional intestine to allow health to be maintained by
Enteral and parenteral nutrition in GI failure and short bowel syndrome Alastair Forbes University College London Intestinal failure Inadequate functional intestine to allow health to be maintained by
Case Discussion. Nutrition in IBD. Rémy Meier MD. Ulcerative colitis. Crohn s disease
 26.08.2017 Case Discussion Nutrition in IBD Crohn s disease Ulcerative colitis Rémy Meier MD Case Presentation 30 years old female, with diarrhea for 3 months Shool frequency 3-4 loose stools/day with
26.08.2017 Case Discussion Nutrition in IBD Crohn s disease Ulcerative colitis Rémy Meier MD Case Presentation 30 years old female, with diarrhea for 3 months Shool frequency 3-4 loose stools/day with
Oklahoma Dietetic Association. Ainsley Malone, MS, RD, LD, CNSD April, 16, 2008 Permissive Underfeeding: What, Where and Why? Mt.
 The What, Why and When of Permissive Ainsley Malone, MS, RD, CNSD Nutrition Support Team Mt. Carmel West Hospital Mt. Carmel West 500 bed academic center Non-physician based NST Dietitian, pharmacist and
The What, Why and When of Permissive Ainsley Malone, MS, RD, CNSD Nutrition Support Team Mt. Carmel West Hospital Mt. Carmel West 500 bed academic center Non-physician based NST Dietitian, pharmacist and
Issues in Enteral Feeding: Aspiration
 Issues in Enteral Feeding: Aspiration A webinar for HealthTrust Members February 11, 2019 Co-sponsored by HealthTrust and V NOS Continuing Education Provider Presented by: Kathleen Stoessel, RN, BSN, MS
Issues in Enteral Feeding: Aspiration A webinar for HealthTrust Members February 11, 2019 Co-sponsored by HealthTrust and V NOS Continuing Education Provider Presented by: Kathleen Stoessel, RN, BSN, MS
SEPSIS: IT ALL BEGINS WITH INFECTION. Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft.
 SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
Multimodal Approach for Managing Postoperative Ileus: Role of Health- System Pharmacists (ACPE program H01P)
") 1. In the normal gastrointestinal tract, what percent of nutrient absorption occurs in the jejunum? a. 20%. b. 40%. c. 70%. d. 90%. 2. According to Dr. Erstad, the four components of gastrointestinal control
1. In the normal gastrointestinal tract, what percent of nutrient absorption occurs in the jejunum? a. 20%. b. 40%. c. 70%. d. 90%. 2. According to Dr. Erstad, the four components of gastrointestinal control
Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased
 1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
Name: Class: "Pharmacology NSAIDS (1) Lecture
 Lecture") I Name: Class: "Pharmacology NSAIDS (1) Lecture د. احمد الزهيري Inflammation is triggered by the release of chemical mediators from injured tissues and migrating cells. The specific mediators vary with
I Name: Class: "Pharmacology NSAIDS (1) Lecture د. احمد الزهيري Inflammation is triggered by the release of chemical mediators from injured tissues and migrating cells. The specific mediators vary with
-Mohammad Ashraf. -Anas Raed. -Alia Shatnawi. 1 P a g e
 -1 -Mohammad Ashraf -Anas Raed -Alia Shatnawi 1 P a g e Dr. Alia started the lecture by talking about subjects we are going to cover through this course; you can refer to the record if you are interested.
-1 -Mohammad Ashraf -Anas Raed -Alia Shatnawi 1 P a g e Dr. Alia started the lecture by talking about subjects we are going to cover through this course; you can refer to the record if you are interested.
Prevention of Complications in Hospitalized Patients Part III: Upper Gastrointestinal Stress Ulcers
 CLINICAL REVIEW Prevention of Complications in Hospitalized Patients Part III: Upper Gastrointestinal Stress Ulcers Michael A. Pfeffer, M.D., and Michael S. Galindo, M.D. The Clinical Scenario A 70-year-old
CLINICAL REVIEW Prevention of Complications in Hospitalized Patients Part III: Upper Gastrointestinal Stress Ulcers Michael A. Pfeffer, M.D., and Michael S. Galindo, M.D. The Clinical Scenario A 70-year-old
THE AUTHOR OF THIS WHAT S NEW IN NUTRITION? OBJECTIVES & OUTLINE EVIDENCE-BASED MEDICINE: PARENTERAL NUTRITION (PN)
") WHAT S NEW IN NUTRITION? Alisha Mutch, Pharm.D., BCPS THE AUTHOR OF THIS PRESENTATION HAS NOTHING TO DISCLOSE. OBJECTIVES & OUTLINE MALNUTRITION OBJECTIVES Indicate when parenteral nutrition (PN) is warranted
WHAT S NEW IN NUTRITION? Alisha Mutch, Pharm.D., BCPS THE AUTHOR OF THIS PRESENTATION HAS NOTHING TO DISCLOSE. OBJECTIVES & OUTLINE MALNUTRITION OBJECTIVES Indicate when parenteral nutrition (PN) is warranted
LOUISIANA MEDICAID PROGRAM ISSUED:
 37.12 TOTAL PARENTERAL NUTRITION Overview Introduction In This Section This Section explains the LMPBM program s Total Parenteral Nutrition (TPN) therapy coverage, limitations, prior authorization, reimbursement
37.12 TOTAL PARENTERAL NUTRITION Overview Introduction In This Section This Section explains the LMPBM program s Total Parenteral Nutrition (TPN) therapy coverage, limitations, prior authorization, reimbursement
10/3/2012. Pediatric Parenteral Nutrition A Comprehensive Review
 Critical Care Nutrition Foundation for Moving Forward Justine Turner MD PhD Department of Pediatric Gastroenterology and Nutrition University of Alberta I have the following financial relationships to
Critical Care Nutrition Foundation for Moving Forward Justine Turner MD PhD Department of Pediatric Gastroenterology and Nutrition University of Alberta I have the following financial relationships to
Glencoe Health. Lesson 3 The Digestive System
 Glencoe Health Lesson 3 The Digestive System Health espotlight Video BIG IDEA The digestive system provides nutrients and energy for your body through the digestion of food. New Vocabulary mastication
Glencoe Health Lesson 3 The Digestive System Health espotlight Video BIG IDEA The digestive system provides nutrients and energy for your body through the digestion of food. New Vocabulary mastication
Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Pediatric Critically Ill Patient: ASPEN-SCCM 2017
 Number of Patients Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Pediatric Critically Ill Patient: ASPEN-SCCM 2017 Jorge A. Coss-Bu, MD Associate Professor of Pediatrics
Number of Patients Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Pediatric Critically Ill Patient: ASPEN-SCCM 2017 Jorge A. Coss-Bu, MD Associate Professor of Pediatrics
Nutritional assessments and diagnosis of digestive disorders
 Nutritional assessments and diagnosis of digestive disorders AASER ABDELAZIM Assistant professor of Medical Biochemistry Zagazig University, Egypt University of Bisha, KSA aaserabdelazim@yahoo.com 7 Mal
Nutritional assessments and diagnosis of digestive disorders AASER ABDELAZIM Assistant professor of Medical Biochemistry Zagazig University, Egypt University of Bisha, KSA aaserabdelazim@yahoo.com 7 Mal
MIST. Minimally invasive Infusion & Suction Therapy Device. Effective treatment for deadly abdominal trauma and sepsis
 MIST Minimally invasive Infusion & Suction Therapy Device Effective treatment for deadly abdominal trauma and sepsis Summary Medical device for treating condition that annually kills ~156k intensive care
MIST Minimally invasive Infusion & Suction Therapy Device Effective treatment for deadly abdominal trauma and sepsis Summary Medical device for treating condition that annually kills ~156k intensive care
Chapter 14: Training in Radiology. DDSEP Chapter 1: Question 12
 DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
The following content was supplied by the author as supporting material and has not been copy-edited or verified by JBJS.
 Page 1 The following content was supplied by the author as supporting material and has not been copy-edited or verified by JBJS. Appendix TABLE E-1 Care-Module Trigger Events That May Indicate an Adverse
Page 1 The following content was supplied by the author as supporting material and has not been copy-edited or verified by JBJS. Appendix TABLE E-1 Care-Module Trigger Events That May Indicate an Adverse
Use of Prokinetic Agents in Intensive Care Medicine - What is Evidence Based? Dr Martin Sterba PhD EDIC CICM TWH ICU, NSW, Australia
 Use of Prokinetic Agents in Intensive Care Medicine - What is Evidence Based? Dr Martin Sterba PhD EDIC CICM TWH ICU, NSW, Australia Ostrava Ostrava Wollongong Wollongong Wollongong Prokinetics and EBM
Use of Prokinetic Agents in Intensive Care Medicine - What is Evidence Based? Dr Martin Sterba PhD EDIC CICM TWH ICU, NSW, Australia Ostrava Ostrava Wollongong Wollongong Wollongong Prokinetics and EBM
NOTES: The Digestive System (Ch 14, part 2)
") NOTES: The Digestive System (Ch 14, part 2) PANCREAS Structure of the pancreas: The pancreas produces PANCREATIC JUICE that is then secreted into a pancreatic duct. The PANCREATIC DUCT leads to the The
NOTES: The Digestive System (Ch 14, part 2) PANCREAS Structure of the pancreas: The pancreas produces PANCREATIC JUICE that is then secreted into a pancreatic duct. The PANCREATIC DUCT leads to the The
Inflammatory Bowel Disease
 + Inflammatory Bowel Disease Christina Kalafsky, Dietetic Intern University of Maryland College Park Children s National Medical Center Case Study January 31, 2014 + Outline n Inflammatory Bowel Disease
+ Inflammatory Bowel Disease Christina Kalafsky, Dietetic Intern University of Maryland College Park Children s National Medical Center Case Study January 31, 2014 + Outline n Inflammatory Bowel Disease
The usual dose is 40 mg daily with amoxycillin 1.5 g (750 mg b.d.) for 2 weeks. Up to 2 g/day of amoxycillin has been used in clinical trials.
 for 2 weeks. Up to 2 g/day of amoxycillin has been used in clinical trials.") Name Gasec - 2 Gastrocaps Composition Gasec-20 Gastrocaps Each Gastrocaps contains: Omeprazole 20 mg (in the form of enteric-coated pellets) Properties, effects Proton Pump Inhibitor Omeprazole belongs
Name Gasec - 2 Gastrocaps Composition Gasec-20 Gastrocaps Each Gastrocaps contains: Omeprazole 20 mg (in the form of enteric-coated pellets) Properties, effects Proton Pump Inhibitor Omeprazole belongs
patients : review of advances in last five years Dr. Aditya Jindal
 Enteral nutrition in medical ICU patients : review of advances in last five years Dr. Aditya Jindal Our food should be our medicine and our medicine should be our food. Hippocrates Introduction ti Nutritional
Enteral nutrition in medical ICU patients : review of advances in last five years Dr. Aditya Jindal Our food should be our medicine and our medicine should be our food. Hippocrates Introduction ti Nutritional
Chapter 26 The Digestive System
 Chapter 26 The Digestive System Digestive System Gastroenterology is the study of the stomach and intestine. Digestion Catabolism Absorption Anabolism The actions of the digestive system are controlled
Chapter 26 The Digestive System Digestive System Gastroenterology is the study of the stomach and intestine. Digestion Catabolism Absorption Anabolism The actions of the digestive system are controlled
National Digestive Diseases Information Clearinghouse
 Gastritis National Digestive Diseases Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH What is gastritis? Gastritis is a condition in which the stomach
Gastritis National Digestive Diseases Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH What is gastritis? Gastritis is a condition in which the stomach
Nutrition and GI. How much?
 Nutrition and GI How much? The goal of nutritional supplementation is to meet but not exceed the nutritional requirements of patients with critical illness. Due to the inherent variability between patients
Nutrition and GI How much? The goal of nutritional supplementation is to meet but not exceed the nutritional requirements of patients with critical illness. Due to the inherent variability between patients
Digestion. Text. What You Don t Know Can Hurt You!
 Digestion Text What You Don t Know Can Hurt You! Digestive Problems Approximately 36.5 million visits annually to ambulatory care facilities due to the diseases of the digestive system Over 4 million ulcers
Digestion Text What You Don t Know Can Hurt You! Digestive Problems Approximately 36.5 million visits annually to ambulatory care facilities due to the diseases of the digestive system Over 4 million ulcers
Short Bowel Syndrome: Medical management
 Short Bowel Syndrome: Medical management La Sindrome dell'intestino Corto in età pediatrica Brescia 18 marzo 2011 Jon A.Vanderhoof, M.D. Division of Pediatric GI Harvard Medical School Children s Hospital,
Short Bowel Syndrome: Medical management La Sindrome dell'intestino Corto in età pediatrica Brescia 18 marzo 2011 Jon A.Vanderhoof, M.D. Division of Pediatric GI Harvard Medical School Children s Hospital,
CYP2C19-Proton Pump Inhibitors
 CYP2C19-Proton Pump Inhibitors Cameron Thomas, Pharm.D. PGY2 Clinical Pharmacogenetics Resident St. Jude Children s Research Hospital February 1, 2018 Objectives: CYP2C19-PPI Implementation Review the
CYP2C19-Proton Pump Inhibitors Cameron Thomas, Pharm.D. PGY2 Clinical Pharmacogenetics Resident St. Jude Children s Research Hospital February 1, 2018 Objectives: CYP2C19-PPI Implementation Review the
Mechanical ventilation (MV) is a lifesaving therapy
 is a lifesaving therapy") critical care review GI Complications in Patients Receiving Mechanical Ventilation* Gökhan M. Mutlu, MD; Ece A. Mutlu, MD; and Phillip Factor, DO, FCCP Mechanical ventilation (MV) can be lifesaving by
critical care review GI Complications in Patients Receiving Mechanical Ventilation* Gökhan M. Mutlu, MD; Ece A. Mutlu, MD; and Phillip Factor, DO, FCCP Mechanical ventilation (MV) can be lifesaving by
LEARNING RESOURCES. 1. Anatomy: Gross Anatomy of The Liver and Gall Bladder Study from: Essential Moore, 5 th Ed., Pages: DEMO note.
 PROBLEM 1 (Hepatitis) 1. Anatomy: Gross Anatomy of The Liver and Gall Bladder Study from: Essential Moore, 5 th Ed., Pages: 158-166 + DEMO 2. Histology: Histology of The Liver and Gall Bladder Study from:
PROBLEM 1 (Hepatitis) 1. Anatomy: Gross Anatomy of The Liver and Gall Bladder Study from: Essential Moore, 5 th Ed., Pages: 158-166 + DEMO 2. Histology: Histology of The Liver and Gall Bladder Study from:
Amyloidosis & the GI Tract
 Amyloidosis & the GI Tract John O. Clarke, M.D. Director, Esophageal Program Clinical Associate Professor of Medicine Stanford University john.clarke@stanford.edu 2017 Topics to cover 1) Patterns of GI
Amyloidosis & the GI Tract John O. Clarke, M.D. Director, Esophageal Program Clinical Associate Professor of Medicine Stanford University john.clarke@stanford.edu 2017 Topics to cover 1) Patterns of GI
NUTRITION. Elizabeth Viner Smith & Catherine Jones Foundations of Critical Care Nursing September 2017
 NUTRITION Elizabeth Viner Smith & Catherine Jones Foundations of Critical Care Nursing September 2017 Step One Competency 1.19 Factors contributing to nutritional impairment in critical illness. Nutritional
NUTRITION Elizabeth Viner Smith & Catherine Jones Foundations of Critical Care Nursing September 2017 Step One Competency 1.19 Factors contributing to nutritional impairment in critical illness. Nutritional
Jodie R. Orwig, RDN, LDN
 Jodie R. Orwig, RDN, LDN In the first 12-24 hours post injury, the #1goal is stabilizing the patient, not nutrition. Goal #2 is surgery, as indicated, to correct the injury Preservation of organ function
Jodie R. Orwig, RDN, LDN In the first 12-24 hours post injury, the #1goal is stabilizing the patient, not nutrition. Goal #2 is surgery, as indicated, to correct the injury Preservation of organ function
Helicobacter Pylori Testing HELICOBACTER PYLORI TESTING HS-131. Policy Number: HS-131. Original Effective Date: 9/17/2009
 Easy Choice Health Plan, Inc. Harmony Health Plan of Illinois, Inc. Missouri Care, Inc. Ohana Health Plan, a plan offered by WellCare Health Insurance of Arizona, Inc. WellCare Health Insurance of Illinois,
Easy Choice Health Plan, Inc. Harmony Health Plan of Illinois, Inc. Missouri Care, Inc. Ohana Health Plan, a plan offered by WellCare Health Insurance of Arizona, Inc. WellCare Health Insurance of Illinois,