[No conflicts of interest]
|
|
|
- Gilbert Campbell
- 5 years ago
- Views:
Transcription
1 [No conflicts of interest]

2 Patients and staff at:
3
4 Available evidence pre-calories Three meta-analyses: Gramlich L et al. Does enteral nutrition compared to parenteral nutrition result in better outcomes in critically ill adult patients? A systematic review of the literature. Nutrition 2004;20: Heyland DK et al. Canadian clinical practice guidelines for nutrition support in mechanically ventilated, critically ill adult patients. JPEN 2003;27: Simpson F, Doig GS. Parenteral vs. enteral nutrition in the critically ill patient: a meta-analysis of trials using the intention to treat principle. Intensive Care Med 2005;31: Conflicting evidence (and guidelines) regarding optimal route Within a context of concern about malnutrition in NHS hospitals
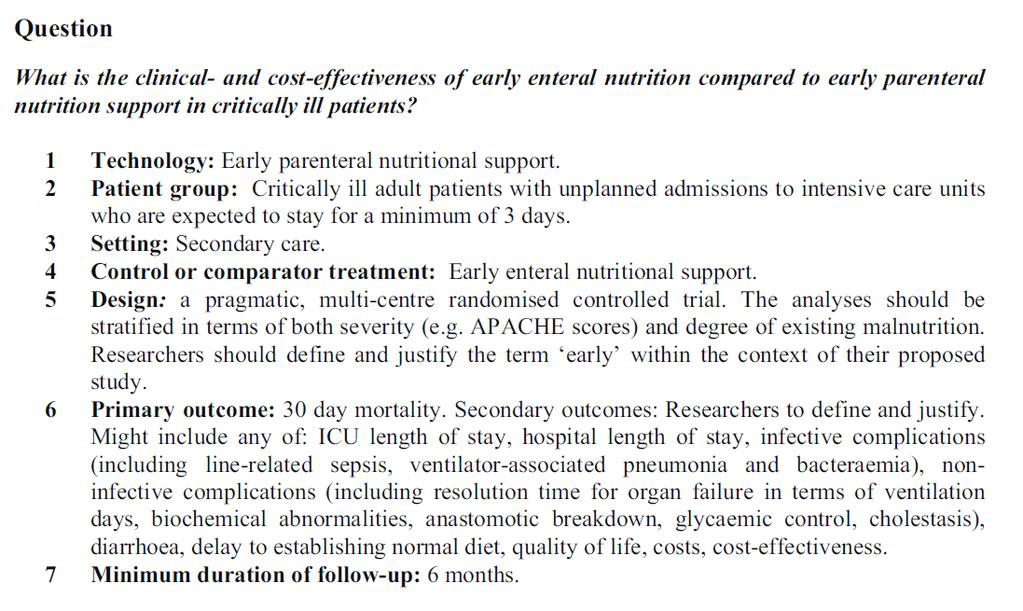

5 Commissioning brief (07/52)
6 Available evidence pre-calories Three meta-analyses: Gramlich L et al. Does enteral nutrition compared to parenteral nutrition result in better outcomes in critically ill adult patients? A systematic review of the literature. Nutrition 2004;20: Heyland DK et al. Canadian clinical practice guidelines for nutrition support in mechanically ventilated, critically ill adult patients. JPEN 2003;27: Simpson F, Doig GS. Parenteral vs. enteral nutrition in the critically ill patient: a meta-analysis of trials using the intention to treat principle. Intensive Care Med 2005;31: Conflicting evidence (and guidelines) regarding optimal route Concern about malnutrition in NHS hospitals Simpson & Doig Significant benefit favouring parenteral nutrition OR (mortality) 0.51 (0.27 to 0.97)
7 Hypothesis that, in critically ill adults, delivery of early nutritional support through the parenteral route is superior to delivery through the enteral route
8 Design A phase III, open, multicentre, pragmatic* randomised controlled trial with an integrated economic evaluation Nested in the national clinical audit database - Case Mix Programme reduce data collection burden enhance generalisability * does this intervention work under usual conditions?

9 Participating sites 33 adult general critical care units, England In a representative sample of NHS hospitals
10 Inclusion criteria sites Active participation in the national clinical audit Pre-existing, established protocols for nutritional support via both routes (and reflecting mainstream practice) Pre-existing implementation of bundles (as promoted by the NHS) to prevent development of: bloodstream infection ventilator-associated pneumonia thromboembolic events Glycaemic control in accordance with international guidelines (<180 mg/dl)
11 Inclusion criteria patients Adult (18+ years) Unplanned admission Expected to receive nutritional support for two or more days Not planned to be discharged within three days
12 Exclusion criteria - patients Pre-existing contraindication to either PN or EN Received PN/EN within the last 7 days PEG, PEJ, needle/surgical jejunostomy in situ Known to be pregnant Admitted for thermal injury (burns) Admitted for palliative care Been in a critical care unit for >36 hours Previously randomised into CALORIES Expected stay in UK less than 6 months
13 Timeline Admission to critical care Eligibility criteria met Informed patient consent, or Consultee agreement Up to 36 hours Randomise Start nutritional support
14 Delivery of nutritional support Randomisation - 24 hour telephone Parenteral route via CVC (dedicated lumen) Enteral route via nasogastric/ nasojejunal tube Followed exclusively for 5 days (120 hours) - target of 25 kcal/kg/day - goal of reaching target within 48 to 72 hours Exclusive oral feeding, unit discharge or death All other care during/after 5 days at discretion of treating clinician(s) If clinically indicated, then oral feeding could be started within the 5 days Enteral trickle feeding not permitted during the 5 days
15 Delivery of early nutritional support Local feeding protocols used All protocols reviewed by trial dietitians - to ensure common boundaries Standard feed within following ranges energy total kcal per bag nitrogen g per bag Additional micronutrients (if clinically indicated/prescribed) Adjust for obese patients, as required Adjust volume for fluid balance requirements
16 Sample size calculation Baseline 30-day mortality 32% Detectable difference RRR 20% (ARR 6.4%) Type I error rate (P value) P<0.05 Type II error rate (power) 90% power 1082 per arm Crossovers/exclusions 2% crossover each way 2% withdrawal (based on PAC-Man) 1200 per arm One planned interim analysis on first 1200 patients
17 Cumulative recruitment Cumulative recruitment N= Jul Jan Jul Jan Jul Jan 2014
18
19
20 Baseline characteristics Case mix Parenteral route Enteral route Age (years), mean (sd) 63.3 (15.1) 62.9 (15.4) Gender, males (%) 689 (57.9%) 725 (60.6%)
21 Baseline characteristics Severe comorbidities Severe comorbidities (APACHE II definitions), n (%) Parenteral route Enteral route Liver 29 (2.5%) 34 (2.8%) Renal 20 (1.7%) 15 (1.3%) Respiratory 34 (2.9%) 23 (1.9%) Cardiovascular 11 (0.9%) 14 (1.2%) Immunocompromised 78 (6.6%) 95 (8.0%)
22 Baseline characteristics Surgical status and mechanical ventilation Surgery within 24 hours prior to randomisation, n (%) Parenteral route Enteral route 162 (13.6%) 167 (14.0%) Mechanical ventilation during 24 hours following critical care admission, n (%) 979 (83.1%) 993 (83.8%)
23 Baseline characteristics Acute severity of illness APACHE II Acute Physiology Score, mean (sd) Parenteral route Enteral route 15.1 (6.2) 15.2 (6.2) APACHE II Score, mean (sd) 19.6 (6.9) 19.6 (7.0) APACHE II predicted risk of death, median (IQR) ICNARC Physiology Score, mean (sd) ICNARC model predicted risk of death, median (IQR) 0.34 ( ) 0.34 ( ) 25.6 (8.0) 25.8 (7.8) 0.42 ( ) 0.43 ( ) SOFA score, mean (sd) 9.5 (3.4) 9.6 (3.3)
24 Baseline characteristics Nutritional status Subjective assessment of severe malnutrition, n (%) Parenteral route Enteral route 151 (12.7%) 152 (12.7%) BMI, mean (sd) 27.7 (7.4) 28.2 (7.5) Degree of malnutrition, n (%) High (BMI<18.5 or weight loss>20%) Moderate (BMI<20 and weight loss>5%) 74 (6.4%) 81 (7.0%) 8 (0.7%) 10 (0.9%) No malnutrition 1070 (92.9%) 1070 (92.2%)
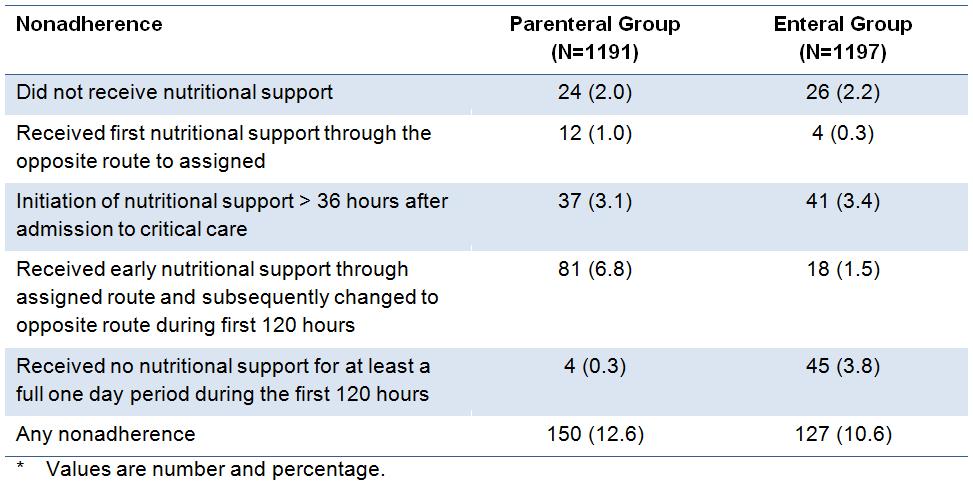
25 Non-adherence
26 Non-adherence Received nutritional support via assigned route and changed during first 120 hours 40 Parenteral route Enteral route Number of patients Time to crossover (hours)
27 Non-adherence Received no nutritional support for at least one full day during first 120 hours 20 Parenteral route Enteral route Number of Patients Days from Initiation of Nutritional Support
28 Clinical management Timing of nutritional support Time from original critical care admission to initiation of nutritional support (hours), median (IQR) Parenteral route Enteral route 24 (17-30) 22 (16-28)
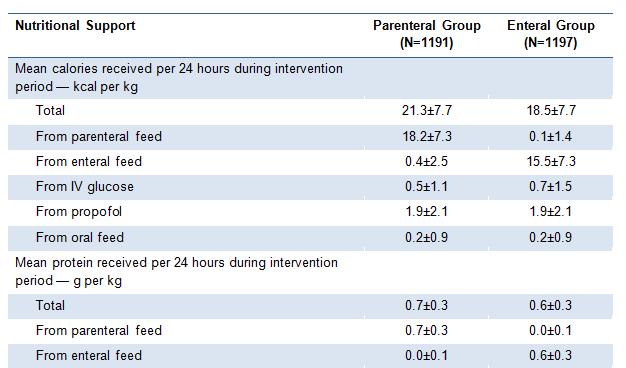
29 Nutritional support
30 Clinical management Daily calories (in relation to the target of 25kcal/kg/day) D Percentage met Target (25kcal/kg/day) Parenteral route Parenteral route (adjusted) Enteral route Enteral route (adjusted) Days from Initation of Early Nutritional Support Adjusted for part days of feeding (e.g. death of a patient)
31 Clinical management Additives Patients receiving additives during the intervention period*, n (%) Parenteral route Enteral route Glutamine 50 (4.2%) 0 (0.0%) Selenium 268 (22.5%) 3 (0.3%) Fish oils 38 (3.2%) 1 (0.1%) * Only recorded for patients receiving nutritional support via the parenteral route
32 Clinical management Aspirates and put-back Total aspirates during intervention period* (ml), mean (sd) Parenteral route Enteral route 35 (265) 958 (1312) Total aspirates put-back during intervention period* (ml), mean (sd) 24 (170) 618 (863) * Only recorded for patients receiving nutritional support via the enteral route
33 Clinical management Prokinetics, vasoactives, insulin and blood glucose Patients receiving prokinetics during intervention period*, n (%) Parenteral route Enteral route 26 (2.2%) 426 (35.6%) Patients receiving vasoactives during intervention period, n (%) Patients receiving insulin during the intervention period, n (%) Total insulin received during intervention period (IU), mean (sd) 958 (80.9%) 1007 (84.6%) 694 (58.6%) 668 (56.1%) 154 (223) 122 (204) * Prokinetics - only recorded for patients receiving nutritional support via the enteral route
34 Clinical management Blood glucose Mean daily lowest blood glucose during intervention period (mg per dl), mean (sd) Parenteral route 127 (25) [7.0 (1.4)] Enteral route 118 (26) [6.5 (1.4)] Mean daily highest blood glucose during intervention period (mg per dl), mean (sd) 183 (43) [10.2 (2.4)] 181 (45) [10.0 (2.5)] [mmol per L]
35 Clinical management Diarrhoea and constipation Incidence of diarrhoea during intervention period, n (%) Parenteral route Enteral route 192 (16.2%) 250 (21.0%) Incidence of constipation during intervention period, n (%) 726 (61.3%) 643 (54.0%) Diarrhoea loose/unformed or liquid stools on 3 consecutive days Constipation - bowels not opened on 3 consecutive days
36 Primary outcome All-cause mortality at 30 days (from randomisation) Parenteral route, deaths (%) Enteral route, deaths (%) P-value 393 (33.1%) 409 (34.2%) 0.57 Effect estimate (95% CI) [P-value] Absolute risk reduction 1.15 (-2.65 to 4.94) Relative risk 0.97 (0.86 to 1.08) Adjusted* odds ratio 0.95 (0.79 to 1.13) [p=0.55] *Adjusted for age, ICNARC physiology score, surgical status, degree of malnutrition and a unit-level random effect
37 Secondary outcomes All-cause mortality at 90 days (from randomisation) Parenteral route, deaths (%) Enteral route, deaths (%) P-value 442 (37.3%) 464 (39.1%) 0.40 Effect estimate (95% CI) [P-value] Relative risk 0.96 (0.86 to 1.06) Adjusted* odds ratio 0.93 (0.77 to 1.11) [p=0.39] *Adjusted for age, ICNARC physiology score, surgical status, degree of malnutrition and a unit-level random effect
38 Secondary outcomes Duration of survival to 90 days Proportion of Patients Alive Parenteral route Enteral route Unadjusted (log rank test): P = 0.98 Adjusted* (Cox proportional-hazards model): Hazard ratio (95% CI) = 0.94 (0.82 to 1.07) P = Days since Randomization *Adjusted for age, ICNARC physiology score, surgical status, degree of malnutrition and a unit-level random effect
39 Secondary outcomes Duration of organ support in the unit Days alive and free (up to 30 days) of Parenteral route, mean (SD) Enteral route, mean (SD) Difference in means (95% CI) P-value Advanced respiratory 14.3 (12.1) 14.3 (12.2) 0.04 (-0.94 to 1.01) 0.94 Advanced cardiovascular 18.9 (13.5) 18.5 (13.6) 0.41 ( 0.63 to 1.53) 0.44 Renal 19.1 (13.9) 18.8 (14.0) 0.26 ( 0.85 to 1.47) 0.66 Neurological 19.2 (13.8) 18.9 (14.0) 0.34 ( 0.81 to 1.36) 0.57 Gastrointestinal 13.0 (11.7) 13.2 (11.8) 0.12 ( 1.05 to 0.80) 0.81
40 Secondary outcomes Number of new infectious complications per patient Parenteral route, mean (SD) Enteral route, mean (SD) Difference in means (95% CI) P-value Number of infectious complications per patient 0.22 (0.60) 0.21 (0.56) 0.01 (-0.04 to 0.06) 0.72 Either laboratory confirmed or strongly suspected and treated with antibacterials or antifungals (85% laboratory confirmed in both groups) Occurring from second day of nutritional support to discharge from critical care unit
41 Secondary outcomes Infectious complications Infectious complications Chest infection (pneumonia/ lower respiratory tract infection) Parenteral route, n (%) Enteral route, n (%) P-value 135 (11.3%) 143 (11.9%) 0.66 CVC infection 11 (0.9%) 9 (0.8%) 0.66 Other vascular catheter-related infection 4 (0.3%) 3 (0.3%) 0.73 Bloodstream infection 27 (2.3%) 21 (1.8%) 0.39 Infective colitis 8 (0.7%) 4 (0.3%) 0.26 Urinary tract infection 16 (1.3%) 15 (1.3%) 0.86 Surgical site infection 10 (0.8%) 12 (1.0%) 0.83 Other infectious complications 18 (1.5%) 24 (2.0%) 0.44
42 Secondary outcomes Non-infectious complications Non-infectious complications Parenteral route, n (%) Enteral route, n (%) P-value Episodes of hypoglycaemia 44 (3.7%) 74 (6.2%) Elevated liver function tests 212 (17.8%) 179 (15.0%) 0.07 Nausea requiring treatment 44 (3.7%) 53 (4.4%) 0.41 Abdominal distension 78 (6.5%) 99 (8.3%) 0.12 Vomiting 100 (8.4%) 194 (16.2%) <0.001 Pressure ulcers 181 (15.2%) 179 (15.0%) 0.91
43 Secondary outcomes Duration of stay (days) in Critical care -All - critical care survivors - critical care non-survivors Parenteral route, median (IQR) 8.1 ( ) 8.8 ( ) 5.2 ( ) Enteral route, median (IQR) 7.3 ( ) 8.2 ( ) 4.3 ( ) P-value Acute hospital -All - acute hospital survivors - acute hospital non-survivors 17 (8-34) 24 (14-43) 7 (3-16) 16 (8-33) 24 (14-43) 6 (2-14)
44 Serious adverse events Total number of patients with serious adverse events Parenteral route, n (%) Enteral route, n (%) P-value 58 (4.9%) 58 (4.8%) 1.00
45 Subgroup analyses Age Degree of malnutrition None Moderate/Severe APACHE II predicted risk ICNARC model predicted risk Mechanically ventilated No Yes Presence of cancer No Yes Time to start of feeding Less than 24 hours 24 hours or over P Value Adjusted for age, ICNARC physiology score, surgical status, degree of malnutrition and a unit-level random effect Favors parenteral route Favors enteral route Adjusted Odds Ratio
46 Adherence-adjusted analysis Adherence-adjusted analysis Relative risk (95% CI) [P-value] Original result 0.97 (0.86 to 1.08) Adherence-adjusted 0.96 (0.85 to 1.09) [p=0.55] Structural mean model with an instrumental variable of allocated group
47 Summary Primary outcome No significant difference in 30-day mortality by route of delivery of early nutritional support Secondary outcomes (significant) Increased episodes of hypoglycaemia with enteral route Increased episodes of vomiting with enteral route
48 Discussion Reported increase in infectious complications with parenteral route was not seen Improvements in management of vascular access? Improvements in prevention of VAP, etc.? Developments in feeding technology? Caloric targets were not met in either group Expected for enteral route? Lack of availability of nutritional product? Content (use of commercially available rather than individually titrated)? Delivery (delays and/or interruptions)? Clinical preference for lower target?
49 Conclusion Early nutritional support through the parenteral route as typically administered in ICUs in England - is neither more harmful nor more beneficial than through the enteral route One-year follow-up for the integrated economic evaluation ongoing

50 This project was funded by the National Institute for Health Research Health Technology Assessment Programme (project number 07/52/03) The views and opinions expressed are those of the authors and do not necessarily reflect those of the HTA Programme, NIHR, NHS or the Department of Health
8.0 Parenteral Nutrition vs. Standard care May 2015
 8.0 Parenteral Nutrition vs. Standard care May 015 015 Recommendation: Based on 6 level studies, in critically ill patients with an intact gastrointestinal tract, we recommend that parenteral nutrition
8.0 Parenteral Nutrition vs. Standard care May 015 015 Recommendation: Based on 6 level studies, in critically ill patients with an intact gastrointestinal tract, we recommend that parenteral nutrition
5.1 Strategies to Optimize Delivery and Minimize Risks of EN: Feeding Protocols March 2013
 5.1 Strategies to Optimize Delivery and Minimize Risks of EN: Feeding Protocols March 2013 There were no new randomized controlled trials since the 2009 update and hence there are no changes to the following
5.1 Strategies to Optimize Delivery and Minimize Risks of EN: Feeding Protocols March 2013 There were no new randomized controlled trials since the 2009 update and hence there are no changes to the following
3.2 Nutritional Prescription of Enteral Nutrition: Achieving Target Dose of Enteral Nutrition March 2013
 . Nutritional Prescription of Enteral Nutrition: Achieving Target Dose of Enteral Nutrition March 01 There were no new randomized controlled trials since the 009 update and hence there are no changes to
. Nutritional Prescription of Enteral Nutrition: Achieving Target Dose of Enteral Nutrition March 01 There were no new randomized controlled trials since the 009 update and hence there are no changes to
SECTION 4: RECRUIT PARTICIPANTS
 SECTION 4: RECRUIT PARTICIPANTS Contents Participant Eligibility & Enrollment... 2 Screening... 2 Study ID Numbers... 2 Inclusion Criteria... 2 Exclusion Criteria... 4 Co-Enrollment... 5 Informed Consent
SECTION 4: RECRUIT PARTICIPANTS Contents Participant Eligibility & Enrollment... 2 Screening... 2 Study ID Numbers... 2 Inclusion Criteria... 2 Exclusion Criteria... 4 Co-Enrollment... 5 Informed Consent
5.3 Strategies to Optimize Delivery and Minimize Risks of EN: Small Bowel Feeding vs. Gastric May 2015
 5.3 Strategies to Optimize Delivery and Minimize Risks of EN: Small Bowel Feeding vs. Gastric May 2015 2015 Recommendation: Based on 16 level 2 studies, small bowel feeding compared to gastric feeding
5.3 Strategies to Optimize Delivery and Minimize Risks of EN: Small Bowel Feeding vs. Gastric May 2015 2015 Recommendation: Based on 16 level 2 studies, small bowel feeding compared to gastric feeding
Nutrition. ICU Fellowship Training Radboudumc
 Nutrition ICU Fellowship Training Radboudumc Critical Care MCQ s Nasogastric (NG) and nasojejunal (NJ) feeding tubes: A. Enteral nutrition is associated with a reduced risk of bacterial and toxin translocation.
Nutrition ICU Fellowship Training Radboudumc Critical Care MCQ s Nasogastric (NG) and nasojejunal (NJ) feeding tubes: A. Enteral nutrition is associated with a reduced risk of bacterial and toxin translocation.
3.2 Nutritional Prescription of Enteral Nutrition: Enhanced Dose of Enteral Nutrition May 2015
 . Nutritional Prescription of Enteral Nutrition: Enhanced Dose of Enteral Nutrition May 015 015 Recommendation: Based on 1 level 1 study, level studies and cluster randomized controlled trials, when starting
. Nutritional Prescription of Enteral Nutrition: Enhanced Dose of Enteral Nutrition May 015 015 Recommendation: Based on 1 level 1 study, level studies and cluster randomized controlled trials, when starting
5.3 Strategies to Optimize Delivery and Minimize Risks of EN: Small Bowel Feeding vs. Gastric February 2014
 5.3 Strategies to Optimize Delivery and Minimize Risks of EN: Small Bowel Feeding vs. Gastric February 2014 2013 Recommendation: Based on 15 level 2 studies, small bowel feeding compared to gastric feeding
5.3 Strategies to Optimize Delivery and Minimize Risks of EN: Small Bowel Feeding vs. Gastric February 2014 2013 Recommendation: Based on 15 level 2 studies, small bowel feeding compared to gastric feeding
Parenterale voeding tijdens kritieke ziekte: bijkomende analyses van de EPaNIC studie
 Parenterale voeding tijdens kritieke ziekte: bijkomende analyses van de EPaNIC studie Namens alle auteurs Michaël P. Casaer M.D. Department of Intensive Care Medicine University Hospital Gasthuisberg Catholic
Parenterale voeding tijdens kritieke ziekte: bijkomende analyses van de EPaNIC studie Namens alle auteurs Michaël P. Casaer M.D. Department of Intensive Care Medicine University Hospital Gasthuisberg Catholic
NO DISCLOSURES 5/9/2015
 Annette Stralovich-Romani, RD, CNSC Adult Critical Care Nutritionist UCSF Medical Center NO DISCLOSURES Incidence & consequences of malnutrition Underfeeding in the ICU Causes/ consequences Nutrition intervention
Annette Stralovich-Romani, RD, CNSC Adult Critical Care Nutritionist UCSF Medical Center NO DISCLOSURES Incidence & consequences of malnutrition Underfeeding in the ICU Causes/ consequences Nutrition intervention
Intensive Care Nutrition. Dr Alan Race BSc(Hons) PhD FRCA
 PhD FRCA") Intensive Care Nutrition Dr Alan Race BSc(Hons) PhD FRCA Objectives 1. What examiners say 2. Definition 3. Assessment 4. Requirements 5. Types of delivery 6. CALORIES Trial 7. Timing 8. Immunomodulation
Intensive Care Nutrition Dr Alan Race BSc(Hons) PhD FRCA Objectives 1. What examiners say 2. Definition 3. Assessment 4. Requirements 5. Types of delivery 6. CALORIES Trial 7. Timing 8. Immunomodulation
Statistical Analysis Plan: Post-hoc analysis of the CALORIES trial
 Statistical Analysis Plan: Post-hoc analysis of the CALORIES trial Author: Version 1.0, Role, Name and Position Signature Date Chief investigator: Prof Kathryn Rowan (Director of Scientific & Strategic
Statistical Analysis Plan: Post-hoc analysis of the CALORIES trial Author: Version 1.0, Role, Name and Position Signature Date Chief investigator: Prof Kathryn Rowan (Director of Scientific & Strategic
2.0 Early vs. Delayed Nutrient Intake May 2015
 2.0 Early vs. Delayed Nutrient Intake May 2015 There were no new randomized controlled trials since the 2013 update and hence there are no changes to the following summary of evidence. 2013 Recommendation:
2.0 Early vs. Delayed Nutrient Intake May 2015 There were no new randomized controlled trials since the 2013 update and hence there are no changes to the following summary of evidence. 2013 Recommendation:
Abstract. n engl j med 371;18 nejm.org october 30,
 The new england journal of medicine established in 1812 october 30, 2014 vol. 371 no. 18 Trial of the Route of Early Nutritional Support in Critically Ill Adults Sheila E. Harvey, Ph.D., Francesca Parrott,
The new england journal of medicine established in 1812 october 30, 2014 vol. 371 no. 18 Trial of the Route of Early Nutritional Support in Critically Ill Adults Sheila E. Harvey, Ph.D., Francesca Parrott,
Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Pediatric Critically Ill Patient: ASPEN-SCCM 2017
 Number of Patients Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Pediatric Critically Ill Patient: ASPEN-SCCM 2017 Jorge A. Coss-Bu, MD Associate Professor of Pediatrics
Number of Patients Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Pediatric Critically Ill Patient: ASPEN-SCCM 2017 Jorge A. Coss-Bu, MD Associate Professor of Pediatrics
11.1 Supplemental Antioxidant Nutrients: Combined Vitamins and Trace Elements April 2013
 . Supplemental Antioxidant Nutrients: Combined Vitamins and Trace Elements April 23 23 Recommendation: Based on 7 level and 7 level 2 studies, the use of supplemental combined vitamins and trace elements
. Supplemental Antioxidant Nutrients: Combined Vitamins and Trace Elements April 23 23 Recommendation: Based on 7 level and 7 level 2 studies, the use of supplemental combined vitamins and trace elements
Benchmarking your ICU s feeding performance: How early is early?
 Benchmarking your ICU s feeding performance: How early is early? Dr Gordon S. Doig, Associate Professor in Intensive Care, Northern Clinical School Intensive Care Research Unit, University of Sydney, Sydney,
Benchmarking your ICU s feeding performance: How early is early? Dr Gordon S. Doig, Associate Professor in Intensive Care, Northern Clinical School Intensive Care Research Unit, University of Sydney, Sydney,
Providing Optimal Nutritional Support on the ICU common problems and practical solutions. Pete Turner Specialist Nutritional Support Dietitian
 Providing Optimal Nutritional Support on the ICU common problems and practical solutions Pete Turner Specialist Nutritional Support Dietitian ICU Nutritional Support ACCEPT study showed improved ICU survival
Providing Optimal Nutritional Support on the ICU common problems and practical solutions Pete Turner Specialist Nutritional Support Dietitian ICU Nutritional Support ACCEPT study showed improved ICU survival
Kombinierte enterale und parenterale Ernährung für welche PatientInnen?
 2014 Kombinierte enterale und parenterale Ernährung für welche PatientInnen? Dr. CP. Heidegger Intensive Care/Geneva claudia-paula.heidegger@hcuge.ch Bern Freitag, 4. April 2014 Nutrition News Worldwide
2014 Kombinierte enterale und parenterale Ernährung für welche PatientInnen? Dr. CP. Heidegger Intensive Care/Geneva claudia-paula.heidegger@hcuge.ch Bern Freitag, 4. April 2014 Nutrition News Worldwide
Int. Med J Vol. 6 No 1 June 2007 Enteral Nutrition In Intensive Care: Tiger Tube For Small Bowel Feeding In Acute Pancreatitis.
 Page 1 of 6 Int. Med J Vol. 6 No 1 June 2007 Enteral Nutrition In Intensive Care: Tiger Tube For Small Bowel Feeding In Acute Pancreatitis. Case Report Mohd Basri bin Mat Nor. Department of Anaesthesiology
Page 1 of 6 Int. Med J Vol. 6 No 1 June 2007 Enteral Nutrition In Intensive Care: Tiger Tube For Small Bowel Feeding In Acute Pancreatitis. Case Report Mohd Basri bin Mat Nor. Department of Anaesthesiology
5.2 Strategies to Optimize Delivery and Minimize Risks of EN: Motility Agents May 2015
 5.2 Strategies to Optimize Delivery and Minimize Risks of EN: Motility Agents May 2015 There were no new randomized controlled trials since the 2009 and 2013 updates and hence there are no changes to the
5.2 Strategies to Optimize Delivery and Minimize Risks of EN: Motility Agents May 2015 There were no new randomized controlled trials since the 2009 and 2013 updates and hence there are no changes to the
Protein dosing in the ICU: How much, when and why?
 Protein dosing in the ICU: How much, when and why? Dr. Gordon S. Doig, Associate Professor in Intensive Care Northern Clinical School Intensive Care Research Unit, University of Sydney, Sydney, Australia
Protein dosing in the ICU: How much, when and why? Dr. Gordon S. Doig, Associate Professor in Intensive Care Northern Clinical School Intensive Care Research Unit, University of Sydney, Sydney, Australia
Ernährungstherapie des Kritisch Kranken Enteral Parenteral Ganz egal?
 Ernährungstherapie des Kritisch Kranken Enteral Parenteral Ganz egal? PD Dr. med. Claudia Heidegger Service des Soins Intensifs Genf/Schweiz Dresden 11. Juni 2016 Nutrition News Nutrition controversy in
Ernährungstherapie des Kritisch Kranken Enteral Parenteral Ganz egal? PD Dr. med. Claudia Heidegger Service des Soins Intensifs Genf/Schweiz Dresden 11. Juni 2016 Nutrition News Nutrition controversy in
The Meat and Potatoes of Critical Care Nutrition ROSEMARY KOZAR MD PHD SHOCK TRAUMA UNIVERSITY OF MARYLAND
 The Meat and Potatoes of Critical Care Nutrition ROSEMARY KOZAR MD PHD SHOCK TRAUMA UNIVERSITY OF MARYLAND 2013 Canadian Clinical Practice Guidelines www.criticalcarenutrition.com NEJM March 27, 2014 Use
The Meat and Potatoes of Critical Care Nutrition ROSEMARY KOZAR MD PHD SHOCK TRAUMA UNIVERSITY OF MARYLAND 2013 Canadian Clinical Practice Guidelines www.criticalcarenutrition.com NEJM March 27, 2014 Use
Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Enteral Nutrition Algorithm Clinical Practice Guideline
 Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Enteral Nutrition Algorithm Clinical Practice Guideline Original Date: 08/2011 Purpose: To promote the early use of
Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Enteral Nutrition Algorithm Clinical Practice Guideline Original Date: 08/2011 Purpose: To promote the early use of
NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE SCOPE. Nutrition support in adults: oral supplements, enteral and parenteral feeding.
 NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE 1 Guideline title SCOPE Nutrition support in adults: oral supplements, enteral and parenteral feeding. 1.1 Short title Nutrition support 2 Background a) The National
NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE 1 Guideline title SCOPE Nutrition support in adults: oral supplements, enteral and parenteral feeding. 1.1 Short title Nutrition support 2 Background a) The National
Extremely well tolerated. Feeding shock
 Extremely well tolerated Feeding shock FEEDING DURING CIRCULATORY FAILURE Dr S Omar Chris Hani Baragwanath Hospital Hospital/University of Witwatersrand Introduction Circulatory shock lack of adequate
Extremely well tolerated Feeding shock FEEDING DURING CIRCULATORY FAILURE Dr S Omar Chris Hani Baragwanath Hospital Hospital/University of Witwatersrand Introduction Circulatory shock lack of adequate
patients : review of advances in last five years Dr. Aditya Jindal
 Enteral nutrition in medical ICU patients : review of advances in last five years Dr. Aditya Jindal Our food should be our medicine and our medicine should be our food. Hippocrates Introduction ti Nutritional
Enteral nutrition in medical ICU patients : review of advances in last five years Dr. Aditya Jindal Our food should be our medicine and our medicine should be our food. Hippocrates Introduction ti Nutritional
10/3/2012. Pediatric Parenteral Nutrition A Comprehensive Review
 Critical Care Nutrition Foundation for Moving Forward Justine Turner MD PhD Department of Pediatric Gastroenterology and Nutrition University of Alberta I have the following financial relationships to
Critical Care Nutrition Foundation for Moving Forward Justine Turner MD PhD Department of Pediatric Gastroenterology and Nutrition University of Alberta I have the following financial relationships to
Methodological co-investigators
 Protocolised Management In Sepsis: A multicentre randomised controlled trial of the clinical and cost-effectiveness of early, goal-directed, protocolised resuscitation for emerging septic shock Methodological
Protocolised Management In Sepsis: A multicentre randomised controlled trial of the clinical and cost-effectiveness of early, goal-directed, protocolised resuscitation for emerging septic shock Methodological
5.5 Strategies to Optimize the Delivery of EN: Use of and Threshold for Gastric Residual Volumes May 2015
 5.5 Strategies to Optimize the Delivery of EN: Use of and Threshold for Gastric Residual Volumes May 2015 2015 Recommendation: Based on 3 level 2 studies, a gastric residual volume of either 250 or 500
5.5 Strategies to Optimize the Delivery of EN: Use of and Threshold for Gastric Residual Volumes May 2015 2015 Recommendation: Based on 3 level 2 studies, a gastric residual volume of either 250 or 500
ENTERAL NUTRITION IN THE CRITICALLY ILL
 ENTERAL NUTRITION IN THE CRITICALLY ILL 1 Ebb phase Flow phase acute response (catabolic) adoptive response (anabolic) 2 3 Metabolic Response to Stress (catabolic phase) Glucose and Protein Metabolism
ENTERAL NUTRITION IN THE CRITICALLY ILL 1 Ebb phase Flow phase acute response (catabolic) adoptive response (anabolic) 2 3 Metabolic Response to Stress (catabolic phase) Glucose and Protein Metabolism
Early-goal-directed therapy and protocolised treatment in septic shock
 CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
Nutrition Procedures Nutrition Prescription Protein Target Lower Protein Dose Higher Protein Dose 1.2 g/kg/day Calorie Target
 Nutrition Procedures Nutrition Prescription Protein and energy targets will be achieved through any combination of EN, protein supplements, and PN or amino acids. The only difference between the nutrition
Nutrition Procedures Nutrition Prescription Protein and energy targets will be achieved through any combination of EN, protein supplements, and PN or amino acids. The only difference between the nutrition
Nutrition and Sepsis
 Nutrition and Sepsis Todd W. Rice, MD, MSc Associate Professor of Medicine Vanderbilt University 2017 DNS Symposium June 2, 2017 Case 55 y.o. male COPD, DM, HTN, presents with pneumonia and septic shock.
Nutrition and Sepsis Todd W. Rice, MD, MSc Associate Professor of Medicine Vanderbilt University 2017 DNS Symposium June 2, 2017 Case 55 y.o. male COPD, DM, HTN, presents with pneumonia and septic shock.
Enteral Nutrition: Whom, Why, When, What and Where to Feed?
 Meier RF, Reddy BR, Soeters PB (eds): The Importance of Nutrition as an Integral Part of Disease Management. Nestlé Nutr Inst Workshop Ser, vol 82, pp 53 59, (DOI: 10.1159/000382002) Nestec Ltd., Vevey/S.
Meier RF, Reddy BR, Soeters PB (eds): The Importance of Nutrition as an Integral Part of Disease Management. Nestlé Nutr Inst Workshop Ser, vol 82, pp 53 59, (DOI: 10.1159/000382002) Nestec Ltd., Vevey/S.
Oklahoma Dietetic Association. Ainsley Malone, MS, RD, LD, CNSD April, 16, 2008 Permissive Underfeeding: What, Where and Why? Mt.
 The What, Why and When of Permissive Ainsley Malone, MS, RD, CNSD Nutrition Support Team Mt. Carmel West Hospital Mt. Carmel West 500 bed academic center Non-physician based NST Dietitian, pharmacist and
The What, Why and When of Permissive Ainsley Malone, MS, RD, CNSD Nutrition Support Team Mt. Carmel West Hospital Mt. Carmel West 500 bed academic center Non-physician based NST Dietitian, pharmacist and
ICU NUTRITION UPDATE : ESPEN GUIDELINES Mirey Karavetian Assistant Professor Zayed University
 ICU NUTRITION UPDATE : ESPEN GUIDELINES 2018 Mirey Karavetian Assistant Professor Zayed University http://www.espen.org/files/espen- Guidelines/ESPEN_Guideline_on_clinical_nutrition_in_-ICU.pdf Medical
ICU NUTRITION UPDATE : ESPEN GUIDELINES 2018 Mirey Karavetian Assistant Professor Zayed University http://www.espen.org/files/espen- Guidelines/ESPEN_Guideline_on_clinical_nutrition_in_-ICU.pdf Medical
Enteral Nutrition in the Critically Ill Child: Challenges and Current Guidelines
 Enteral Nutrition in the Critically Ill Child: Challenges and Current Guidelines 1 Presented on January 24, 2017 Jorge A. Coss-Bu, MD Associate Professor of Pediatrics Section of Critical Care Baylor College
Enteral Nutrition in the Critically Ill Child: Challenges and Current Guidelines 1 Presented on January 24, 2017 Jorge A. Coss-Bu, MD Associate Professor of Pediatrics Section of Critical Care Baylor College
Feeding the septic patient How and when? Masterclass ICU nurses
 Feeding the septic patient How and when? Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16 - FiO2 60%)
Feeding the septic patient How and when? Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16 - FiO2 60%)
ESPEN Congress The Hague 2017
 ESPEN Congress The Hague 2017 Using the gut in acute care patients Permissive underfeeding in practice J.-C. Preiser (BE) PERMISSIVE UNDERFEEDING IN PRACTICE ESPEN congress Jean-Charles Preiser, M.D.,
ESPEN Congress The Hague 2017 Using the gut in acute care patients Permissive underfeeding in practice J.-C. Preiser (BE) PERMISSIVE UNDERFEEDING IN PRACTICE ESPEN congress Jean-Charles Preiser, M.D.,
Metabolic Control in Critical Care: Nutrition Therapy
 LOGO Metabolic Control in Critical Care: Nutrition Therapy ผศ.นพ.พรพจน เปรมโยธ น สาขาโภชนาการคล น ก ภาคว ชาอาย รศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล 2016 SCCM/ASPEN Guidelines Nutrition Therapy in the ICU
LOGO Metabolic Control in Critical Care: Nutrition Therapy ผศ.นพ.พรพจน เปรมโยธ น สาขาโภชนาการคล น ก ภาคว ชาอาย รศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล 2016 SCCM/ASPEN Guidelines Nutrition Therapy in the ICU
Acetaminophen recommendations from the Food and Drug Administration Advisory Committee
 TABLE OF CONTENTS Acetaminophen: recommendations from the FDA Advisory Committee 1 Recombinant human erythropoiesis-stimulating agents and mortality in cancer patients Hospital-acquired pneumonia: risks
TABLE OF CONTENTS Acetaminophen: recommendations from the FDA Advisory Committee 1 Recombinant human erythropoiesis-stimulating agents and mortality in cancer patients Hospital-acquired pneumonia: risks
Current concepts in Critical Care Nutrition
 Current concepts in Critical Care Nutrition Dr.N.Ramakrishnan AB (Int Med), AB (Crit Care), MMM, FACP, FCCP, FCCM Director, Critical Care Services Apollo Hospitals, Chennai Objectives Why? Enteral or Parenteral
Current concepts in Critical Care Nutrition Dr.N.Ramakrishnan AB (Int Med), AB (Crit Care), MMM, FACP, FCCP, FCCM Director, Critical Care Services Apollo Hospitals, Chennai Objectives Why? Enteral or Parenteral
Health economics in ICU nutrition: The time has come
 Health economics in ICU nutrition: The time has come Dr Gordon S. Doig, Associate Professor in Intensive Care, Northern Clinical School Intensive Care Research Unit, University of Sydney, Sydney, Australia
Health economics in ICU nutrition: The time has come Dr Gordon S. Doig, Associate Professor in Intensive Care, Northern Clinical School Intensive Care Research Unit, University of Sydney, Sydney, Australia
5.5 Strategies to Optimize the Delivery of EN: Use of and Threshold for Gastric Residual Volumes March 2013
 5.5 Strategies to Optimize the Delivery of EN: Use of and Threshold for Gastric Residual Volumes March 203 NEW SECTION in 203 Recommendation: There are insufficient data to make a recommendation for not
5.5 Strategies to Optimize the Delivery of EN: Use of and Threshold for Gastric Residual Volumes March 203 NEW SECTION in 203 Recommendation: There are insufficient data to make a recommendation for not
STRATEGIES TO IMPROVE ENTERAL FEEDING TOLERANCE. IS IT WORTH IT? ENGELA FRANCIS RD(SA)
") STRATEGIES TO IMPROVE ENTERAL FEEDING TOLERANCE. IS IT WORTH IT? ENGELA FRANCIS RD(SA) DEFINITION OF ENTERAL FEEDING INTOLERANCE Gastrointestinal feeding intolerance are usually defined as: High gastric
STRATEGIES TO IMPROVE ENTERAL FEEDING TOLERANCE. IS IT WORTH IT? ENGELA FRANCIS RD(SA) DEFINITION OF ENTERAL FEEDING INTOLERANCE Gastrointestinal feeding intolerance are usually defined as: High gastric
When to start SPN in critically ill patients? Refereeravond IC
 When to start SPN in critically ill patients? Refereeravond IC Introduction (1) Protein/calorie malnutrition is very frequent in critically ill patients Protein/calorie malnutrition is associated with
When to start SPN in critically ill patients? Refereeravond IC Introduction (1) Protein/calorie malnutrition is very frequent in critically ill patients Protein/calorie malnutrition is associated with
Feeding Protocols Enteral or Parenteral. AM Poleÿ 2012
 Practical aspects on Feeding Protocols Enteral or Parenteral AM Poleÿ 2012 Enteral Feeding Facts A reduction in mortality Prophylaxis for stress ulcers Full-strength Time to start enteral nutrition If
Practical aspects on Feeding Protocols Enteral or Parenteral AM Poleÿ 2012 Enteral Feeding Facts A reduction in mortality Prophylaxis for stress ulcers Full-strength Time to start enteral nutrition If
E S T A B L I S H I N G N U T R I T I O N I N Y O U R I C U The Need for a Protocol
 E S T A B L I S H I N G N U T R I T I O N I N Y O U R I C U The Need for a Protocol Arthur RH van Zanten, MD PhD Gelderse Vallei Hospital, Ede, The Netherlands Learning objectives Develop an evidence based
E S T A B L I S H I N G N U T R I T I O N I N Y O U R I C U The Need for a Protocol Arthur RH van Zanten, MD PhD Gelderse Vallei Hospital, Ede, The Netherlands Learning objectives Develop an evidence based
Nutritional Support in the Perioperative Period
 Nutritional Support in the Perioperative Period Topic 17 Module 17.3 Nutritional Support in the Perioperative Period Ken Fearon Learning Objectives Understand the principles behind nutritional care for
Nutritional Support in the Perioperative Period Topic 17 Module 17.3 Nutritional Support in the Perioperative Period Ken Fearon Learning Objectives Understand the principles behind nutritional care for
8.0 Parenteral Nutrition vs. Standard care January 31 st 2009
 8.0 Parenteral Nutrition vs. Standard care January 31 st 2009 Recommendation: Based on 5 level 2 studies, in critically ill patients with an intact gastrointestinal tract, we recommend that parenteral
8.0 Parenteral Nutrition vs. Standard care January 31 st 2009 Recommendation: Based on 5 level 2 studies, in critically ill patients with an intact gastrointestinal tract, we recommend that parenteral
Timing of Parenteral Nutrition
 Timing of Parenteral Nutrition Arun Bansal; MD, FCCM, MRCPCH Professor Pediatric Critical Care PGIMER, Chandigarh, INDIA drarunbansal@gmail.com Malnutrition in Critically Ill Incidence: from 19 32% Associated
Timing of Parenteral Nutrition Arun Bansal; MD, FCCM, MRCPCH Professor Pediatric Critical Care PGIMER, Chandigarh, INDIA drarunbansal@gmail.com Malnutrition in Critically Ill Incidence: from 19 32% Associated
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Jain S, Kamimoto L, Bramley AM, et al. Hospitalized patients
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Jain S, Kamimoto L, Bramley AM, et al. Hospitalized patients
Nutrition Support. John Cha Department of Surgery DHMC/UCHSC
 Nutrition Support John Cha Department of Surgery DHMC/UCHSC Overview Why? When? How much? What route? Fancy stuff: enhanced nutrition Advantages of Nutrition Decreased catabolism Improved wound healing
Nutrition Support John Cha Department of Surgery DHMC/UCHSC Overview Why? When? How much? What route? Fancy stuff: enhanced nutrition Advantages of Nutrition Decreased catabolism Improved wound healing
Safety profile of Liraglutide: Recent Updates. Mohammadreza Rostamzadeh,M.D.
 Safety profile of Liraglutide: Recent Updates Mohammadreza Rostamzadeh,M.D. Pancreatitis: Victoza post-marketing experience: spontaneous reports of pancreatitis For the majority of the cases, there is
Safety profile of Liraglutide: Recent Updates Mohammadreza Rostamzadeh,M.D. Pancreatitis: Victoza post-marketing experience: spontaneous reports of pancreatitis For the majority of the cases, there is
Vanderbilt University Medical Center Trauma ICU Nutrition Management Guidelines
 Vanderbilt University Medical Center Trauma ICU Nutrition Management Guidelines Trauma Critical Care Nutrition Guidelines Clinical judgment may supersede guidelines as patient circumstances warrant ASSESSMENT
Vanderbilt University Medical Center Trauma ICU Nutrition Management Guidelines Trauma Critical Care Nutrition Guidelines Clinical judgment may supersede guidelines as patient circumstances warrant ASSESSMENT
L.Mageswary Dietitian Hospital Selayang
 L.Mageswary Dietitian Hospital Selayang 14 15 AUG ASMIC 2015 Learning Objectives 1. To understand the importance of nutrition support in ICU 2. To know the right time to feed 3. To understand the indications
L.Mageswary Dietitian Hospital Selayang 14 15 AUG ASMIC 2015 Learning Objectives 1. To understand the importance of nutrition support in ICU 2. To know the right time to feed 3. To understand the indications
7.0 Combination Parenteral Nutrition and Enteral Nutrition January 31 st, 2009
 7.0 Combination Parenteral Nutrition and Enteral Nutrition January 31 st, 009 Recommendation: Based on 5 level studies, for critically ill patients starting on enteral nutrition we recommend that parenteral
7.0 Combination Parenteral Nutrition and Enteral Nutrition January 31 st, 009 Recommendation: Based on 5 level studies, for critically ill patients starting on enteral nutrition we recommend that parenteral
Nutritional intervention in hospitalised paediatric patients. Dr Y.K.Amdekar
 Nutritional intervention in hospitalised paediatric patients Dr Y.K.Amdekar Back to basics Suboptimal nutrient intake is always dangerous in health and more so in disease to feed or not to feed is it a
Nutritional intervention in hospitalised paediatric patients Dr Y.K.Amdekar Back to basics Suboptimal nutrient intake is always dangerous in health and more so in disease to feed or not to feed is it a
2017 ACCP/SCCM Critical Care Preparatory Review and Recertification Course Learning Objectives
 2017 ACCP/SCCM Critical Care Preparatory Review and Recertification Course Learning Objectives Shock Syndromes and Sepsis, Pulmonary Disorders, Hepatic Failure/GI/Endocrine Emergencies, Supportive and
2017 ACCP/SCCM Critical Care Preparatory Review and Recertification Course Learning Objectives Shock Syndromes and Sepsis, Pulmonary Disorders, Hepatic Failure/GI/Endocrine Emergencies, Supportive and
Title The Prescription of Adult Inpatient Parenteral Nutrition (PN) Guideline. Author s job title Consultant Gastroenterologist Directorate Medicine
 Guideline. Author s job title Consultant Gastroenterologist Directorate Medicine") Document Control Title The Prescription of Adult Inpatient Parenteral Nutrition (PN) Guideline Author Author s job title Consultant Gastroenterologist Directorate Medicine Department Medicine Version Date
Document Control Title The Prescription of Adult Inpatient Parenteral Nutrition (PN) Guideline Author Author s job title Consultant Gastroenterologist Directorate Medicine Department Medicine Version Date
Pharmaconutrition in PICU. Gan Chin Seng Paediatric Intensivist UMMC
 Pharmaconutrition in PICU Gan Chin Seng Paediatric Intensivist UMMC Pharmaconutrition in Critical Care Unit Gan Chin Seng Paediatric Intensivist UMMC Definition New concept Treatment with specific nutrients
Pharmaconutrition in PICU Gan Chin Seng Paediatric Intensivist UMMC Pharmaconutrition in Critical Care Unit Gan Chin Seng Paediatric Intensivist UMMC Definition New concept Treatment with specific nutrients
Wali R Johnson et. al. / International Journal of New Technologies in Science and Engineering Vol. 2, Issue 4, October 2015, ISSN
 Enteral Feeding via Percutaneous Endoscopic Gastrojejunostomy(PEGJ) Tubes Decreases Risk of Aspiration and Tube Dislodgement Related Complications Compared to PEGs. Wali R Johnson, MSIV, L Ray Matthews,
Enteral Feeding via Percutaneous Endoscopic Gastrojejunostomy(PEGJ) Tubes Decreases Risk of Aspiration and Tube Dislodgement Related Complications Compared to PEGs. Wali R Johnson, MSIV, L Ray Matthews,
Nutrition Supplementation in the ICU
 Nutrition Supplementation in the ICU ROSEMARY KOZAR MD PHD SHOCK TRAUMA UNIVERSITY OF MARYLAND Canadian Clinical Practice Guidelines www.criticalcarenutrition.com NEJM March 27, 2014 1 Use of Enteral vs
Nutrition Supplementation in the ICU ROSEMARY KOZAR MD PHD SHOCK TRAUMA UNIVERSITY OF MARYLAND Canadian Clinical Practice Guidelines www.criticalcarenutrition.com NEJM March 27, 2014 1 Use of Enteral vs
A Very Early Rehabilitation Trial (AVERT): What we know, what we think and what s to come
: What we know, what we think and what s to come") A Very Early Rehabilitation Trial (AVERT): What we know, what we think and what s to come The AVERT Trial Collaboration group Joshua Kwant, Blinded Assessor 17 th May 2016 NIMAST Nothing to disclose Disclosure
A Very Early Rehabilitation Trial (AVERT): What we know, what we think and what s to come The AVERT Trial Collaboration group Joshua Kwant, Blinded Assessor 17 th May 2016 NIMAST Nothing to disclose Disclosure
Protein Supplementation in the Pediatric Intensive Care Unit. Jan Hau Lee, MBBS, MRCPCH, MCI Children s Intensive Care Unit 28 th July 2017
 Protein Supplementation in the Pediatric Intensive Care Unit Jan Hau Lee, MBBS, MRCPCH, MCI Children s Intensive Care Unit 28 th July 2017 1 Objectives Basis for protein supplementation Challenges in monitoring
Protein Supplementation in the Pediatric Intensive Care Unit Jan Hau Lee, MBBS, MRCPCH, MCI Children s Intensive Care Unit 28 th July 2017 1 Objectives Basis for protein supplementation Challenges in monitoring
An introduction to Quality by Design. Dr Martin Landray University of Oxford
 An introduction to Quality by Design Dr Martin Landray University of Oxford Criteria for a good trial Ask an IMPORTANT question Answer it RELIABLY Quality Quality is the absence of errors that matter to
An introduction to Quality by Design Dr Martin Landray University of Oxford Criteria for a good trial Ask an IMPORTANT question Answer it RELIABLY Quality Quality is the absence of errors that matter to
National Horizon Scanning Centre. Methylnaltrexone (MOA-728) for postoperative ileus. April 2008
 for postoperative ileus. April 2008") (MOA-728) for postoperative ileus April 2008 This technology summary is based on information available at the time of research and a limited literature search. It is not intended to be a definitive statement
(MOA-728) for postoperative ileus April 2008 This technology summary is based on information available at the time of research and a limited literature search. It is not intended to be a definitive statement
ACCP/SCCM Critical Care Preparatory Review and Recertification Course Learning Objectives
 ACCP/SCCM Critical Care Preparatory Review and Recertification Course Learning Objectives Module 1 Critical Care Pharmacy Evolution and Validation, Practice Standards, Training, and Professional Development,
ACCP/SCCM Critical Care Preparatory Review and Recertification Course Learning Objectives Module 1 Critical Care Pharmacy Evolution and Validation, Practice Standards, Training, and Professional Development,
10.2 Strategies to Optimize Parenteral Nutrition and Minimize Risks: Use of lipids May 2015
 10.2 Strategies to Optimize Parenteral Nutrition and Minimize Risks: Use of lipids May 2015 There are no new randomized controlled trials since the 2009 and 2013 updates and hence there are no changes
10.2 Strategies to Optimize Parenteral Nutrition and Minimize Risks: Use of lipids May 2015 There are no new randomized controlled trials since the 2009 and 2013 updates and hence there are no changes
Nutrition therapy in the critical care setting: What is best achievable practice? An international multicenter observational study*
 Continuing Medical Education Article Nutrition therapy in the critical care setting: What is best achievable practice? An international multicenter observational study* Naomi E. Cahill, RD, MSc; Rupinder
Continuing Medical Education Article Nutrition therapy in the critical care setting: What is best achievable practice? An international multicenter observational study* Naomi E. Cahill, RD, MSc; Rupinder
6.4 Enteral Nutrition (Other): Gastrostomy vs. Nasogastric feeding January 31 st, 2009
: Gastrostomy vs. Nasogastric feeding January 31 st, 2009") 6.4 Enteral Nutrition (Other): Gastrostomy vs. Nasogastric feeding January 31 st, 2009 Recommendation: There are insufficient data to make a recommendation on gastrostomy feeding vs. nasogastric feeding
6.4 Enteral Nutrition (Other): Gastrostomy vs. Nasogastric feeding January 31 st, 2009 Recommendation: There are insufficient data to make a recommendation on gastrostomy feeding vs. nasogastric feeding
Nutrition in critical illness:
 Nutrition in critical illness: from theory to daily practice Aim of the presentation Summarize the guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient.
Nutrition in critical illness: from theory to daily practice Aim of the presentation Summarize the guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient.
Nutrition care plan for surgical patients. Objectives
 Slide 1 Nutrition care plan for surgical patients Surgical Nutrition Training Module Level 1 Philippine Society of General Surgeons Committee on Surgical Training In this session we will discuss the most
Slide 1 Nutrition care plan for surgical patients Surgical Nutrition Training Module Level 1 Philippine Society of General Surgeons Committee on Surgical Training In this session we will discuss the most
Insulin reduces Neuromuscular Complications and Prolonged Mechanical Ventilation in a Medical ICU. Online data supplement
 Insulin reduces Neuromuscular Complications and Prolonged Mechanical Ventilation in a Medical ICU Greet Hermans 1, Alexander Wilmer 1, Wouter Meersseman 1, Ilse Milants 2, Pieter J. Wouters 2, Herman Bobbaers
Insulin reduces Neuromuscular Complications and Prolonged Mechanical Ventilation in a Medical ICU Greet Hermans 1, Alexander Wilmer 1, Wouter Meersseman 1, Ilse Milants 2, Pieter J. Wouters 2, Herman Bobbaers
Heather Evans, MD University of Washington Seattle, WA
 Heather Evans, MD University of Washington Seattle, WA 1 American College of Surgeons Division of Education Heather L. Evans, MD, MS, FACS Nothing to disclose 2 Determine nutritional goals Determine when
Heather Evans, MD University of Washington Seattle, WA 1 American College of Surgeons Division of Education Heather L. Evans, MD, MS, FACS Nothing to disclose 2 Determine nutritional goals Determine when
Nutrition care plan. Components and development
 Nutrition care plan Components and development Objectives To define the nutrition care plan To present the components of the nutrition care plan To discuss the different approaches in determining the contents
Nutrition care plan Components and development Objectives To define the nutrition care plan To present the components of the nutrition care plan To discuss the different approaches in determining the contents
The NICE-SUGAR (Normoglycaemia in Intensive Care Evaluation and Survival Using Glucose Algorithm Regulation) Study: statistical analysis plan
 Study: statistical analysis plan") The NICE-SUGAR (Normoglycaemia in Intensive Care Evaluation and Survival Using Glucose Algorithm Regulation) Study: statistical analysis plan Crit Care Resusc ISSN: 1441-2772 2 March 2009 11 1 46-55 Crit
The NICE-SUGAR (Normoglycaemia in Intensive Care Evaluation and Survival Using Glucose Algorithm Regulation) Study: statistical analysis plan Crit Care Resusc ISSN: 1441-2772 2 March 2009 11 1 46-55 Crit
Online-Only Supplement: Early parenteral nutrition in critically ill patients with. short term relative contraindications to early enteral nutrition:
 Online-Only Supplement: Early parenteral nutrition in critically ill patients with short term relative contraindications to early enteral nutrition: A randomized controlled trial. Gordon S. Doig PhD, Fiona
Online-Only Supplement: Early parenteral nutrition in critically ill patients with short term relative contraindications to early enteral nutrition: A randomized controlled trial. Gordon S. Doig PhD, Fiona
Protein in Critically Ill Patients. Ashraf El Houfi. MD MS(pulmonology) MRCP(UK) FRCP(London) EDIC Consultant ICU Dubai Hospital
 MRCP(UK) FRCP(London) EDIC Consultant ICU Dubai Hospital") Protein in Critically Ill Patients Ashraf El Houfi. MD MS(pulmonology) MRCP(UK) FRCP(London) EDIC Consultant ICU Dubai Hospital Proteins Proteins Protein is needed to Build, Maintain, and Repair body tissue
Protein in Critically Ill Patients Ashraf El Houfi. MD MS(pulmonology) MRCP(UK) FRCP(London) EDIC Consultant ICU Dubai Hospital Proteins Proteins Protein is needed to Build, Maintain, and Repair body tissue
VAP Prevention bundles
 VAP Prevention bundles Dr. Shafiq A.Alimad MD Head of medical department at USTH YICID workshop, 15-12-2014 Care Bundles What are they & why use them? What are Care Bundles? Types of Care Bundles available
VAP Prevention bundles Dr. Shafiq A.Alimad MD Head of medical department at USTH YICID workshop, 15-12-2014 Care Bundles What are they & why use them? What are Care Bundles? Types of Care Bundles available
Appendix. This appendix was part of the submitted manuscript and has been peer reviewed. It is posted as supplied by the authors.
 Appendix This appendix was part of the submitted manuscript and has been peer reviewed It is posted as supplied by the authors Protein delivery and clinical outcomes in the critically ill: A systematic
Appendix This appendix was part of the submitted manuscript and has been peer reviewed It is posted as supplied by the authors Protein delivery and clinical outcomes in the critically ill: A systematic
Feeding the critically ill child
 Feeding the critically ill child Khaw Sia (1913 1984) Lee Jan Hau, MBBS, MRCPCH, MCI Children s Intensive Care Unit September 2018 1 2 3 No disclosures Outline Is there a need to optimize enteral nutrition?
Feeding the critically ill child Khaw Sia (1913 1984) Lee Jan Hau, MBBS, MRCPCH, MCI Children s Intensive Care Unit September 2018 1 2 3 No disclosures Outline Is there a need to optimize enteral nutrition?
Antioxidant Dosing and Micronutrient Management in the Intensive Care Unit
 PENSA 2017 November 21, 2017 Antioxidant Dosing and Micronutrient Management in the Intensive Care Unit Lingtak-Neander Chan, PharmD, BCNSP, CNSC, FACN Professor of Pharmacy, Interdisciplinary Faculty
PENSA 2017 November 21, 2017 Antioxidant Dosing and Micronutrient Management in the Intensive Care Unit Lingtak-Neander Chan, PharmD, BCNSP, CNSC, FACN Professor of Pharmacy, Interdisciplinary Faculty
AUTHORS: Luisito O. Llido, MD (1), Mariana S. Sioson, MD (1,2), Jesus Fernando Inciong, MD (1), Grace Manuales, MD (1)
, Mariana S. Sioson, MD (1,2), Jesus Fernando Inciong, MD (1), Grace Manuales, MD (1)") 9 Submitted: September 5, 2011 Posted: January 7, 2012 TITLE: Nutrition team supervision on nutrient intake in critical care patients: report of a ten- year experience in the Philippines (years 2000 to
9 Submitted: September 5, 2011 Posted: January 7, 2012 TITLE: Nutrition team supervision on nutrient intake in critical care patients: report of a ten- year experience in the Philippines (years 2000 to
What s New in Parenteral Nutrition?
 1 What s New in Parenteral Nutrition? พ นโทหญ ง ส รกานต เตชะวณ ช MD, MSc, ABPNS ห วหน าหน วยโภชนศาสตร คล น ก กองอาย รกรรม โรงพยาบาลพระมงก ฎเกล า 7 กรกฎาคม พ.ศ. 2559 What s New in Parenteral Nutrition?
1 What s New in Parenteral Nutrition? พ นโทหญ ง ส รกานต เตชะวณ ช MD, MSc, ABPNS ห วหน าหน วยโภชนศาสตร คล น ก กองอาย รกรรม โรงพยาบาลพระมงก ฎเกล า 7 กรกฎาคม พ.ศ. 2559 What s New in Parenteral Nutrition?
Guide to completing the MODET study CRF
 Guide to completing the MODET study CRF Please record ND for not documented, NA for not applicable and UK for unknown rather than leave blank fields. CRF PAGE 1. Time of injury Complete the time of injury
Guide to completing the MODET study CRF Please record ND for not documented, NA for not applicable and UK for unknown rather than leave blank fields. CRF PAGE 1. Time of injury Complete the time of injury
In 1936, Studley noted that patients who had lost 20%
 GASTROENTEROLOGY 2001;121:970 1001 AGA Technical Review on Parenteral Nutrition This literature review and the recommendations therein were prepared for the American Gastroenterological Association Clinical
GASTROENTEROLOGY 2001;121:970 1001 AGA Technical Review on Parenteral Nutrition This literature review and the recommendations therein were prepared for the American Gastroenterological Association Clinical
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Blum CA, Nigro N, Briel M, et al. Adjunct prednisone
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Blum CA, Nigro N, Briel M, et al. Adjunct prednisone
Control of Blood Glucose in the ICU: Reconciling the Conflicting Data
 Control of Blood Glucose in the ICU: Reconciling the Conflicting Data Steven E. Nissen MD Disclosure Consulting: Many pharmaceutical companies Clinical Trials: AbbVie, Amgen, Astra Zeneca, Esperion, Eli
Control of Blood Glucose in the ICU: Reconciling the Conflicting Data Steven E. Nissen MD Disclosure Consulting: Many pharmaceutical companies Clinical Trials: AbbVie, Amgen, Astra Zeneca, Esperion, Eli
Scott A. Lynch, MD, MPH,FAAFP Assistant Professor
 Scott A. Lynch, MD, MPH,FAAFP Assistant Professor Lynch.Scott@mayo.edu 2015 MFMER 3543652-1 Nutrition in the Hospital Mayo School of Continuous Professional Development 2nd Annual Inpatient Medicine for
Scott A. Lynch, MD, MPH,FAAFP Assistant Professor Lynch.Scott@mayo.edu 2015 MFMER 3543652-1 Nutrition in the Hospital Mayo School of Continuous Professional Development 2nd Annual Inpatient Medicine for
/03/ $03.00/0 Vol. 27, No. 5 JOURNAL OF PARENTERAL AND ENTERAL NUTRITION
 0148-6071/03/2705-0355$03.00/0 Vol. 27, No. 5 JOURNAL OF PARENTERAL AND ENTERAL NUTRITION Printed in U.S.A. Copyright 2003 by the American Society for Parenteral and Enteral Nutrition Special Interest
0148-6071/03/2705-0355$03.00/0 Vol. 27, No. 5 JOURNAL OF PARENTERAL AND ENTERAL NUTRITION Printed in U.S.A. Copyright 2003 by the American Society for Parenteral and Enteral Nutrition Special Interest
Nutrition and GI. How much?
 Nutrition and GI How much? The goal of nutritional supplementation is to meet but not exceed the nutritional requirements of patients with critical illness. Due to the inherent variability between patients
Nutrition and GI How much? The goal of nutritional supplementation is to meet but not exceed the nutritional requirements of patients with critical illness. Due to the inherent variability between patients
Long term monitoring. Dr Alison Culkin Research Dietitian St Mark s Hospital
 Long term monitoring Dr Alison Culkin Research Dietitian St Mark s Hospital Patient 23 year old lady 1/4/14 Colectomy for UC 3-7/4/14 Ischaemic bowel 4 laparotomies Jejunostomy at 35 cm 23/5/14 Weight
Long term monitoring Dr Alison Culkin Research Dietitian St Mark s Hospital Patient 23 year old lady 1/4/14 Colectomy for UC 3-7/4/14 Ischaemic bowel 4 laparotomies Jejunostomy at 35 cm 23/5/14 Weight
Understanding the benefits of early enteral nutrition in the major trauma patient requiring intensive care: From clinical trials to costs.
 Understanding the benefits of early enteral nutrition in the major trauma patient requiring intensive care: From clinical trials to costs. Dr. Gordon S. Doig Associate Professor in Intensive Care Northern
Understanding the benefits of early enteral nutrition in the major trauma patient requiring intensive care: From clinical trials to costs. Dr. Gordon S. Doig Associate Professor in Intensive Care Northern
Issues in Enteral Feeding: Malnutrition
 Issues in Enteral Feeding: Malnutrition A webinar for HealthTrust Members February 22, 2019 Co-sponsored by HealthTrust and V NOS Continuing Education Provider Presented by: Kathleen Stoessel, RN, BSN,
Issues in Enteral Feeding: Malnutrition A webinar for HealthTrust Members February 22, 2019 Co-sponsored by HealthTrust and V NOS Continuing Education Provider Presented by: Kathleen Stoessel, RN, BSN,
Nutrition Protocol for Intensive Care Beatrice CL Lim et al Letter to the Editor
 416 Letter to the Editor Implementation of a Proactive Nutrition Protocol Improves Enteral Nutrition in Mechanically Ventilated Patients Admitted to the Neuro-Intensive Care Unit Dear Editor, The enteral
416 Letter to the Editor Implementation of a Proactive Nutrition Protocol Improves Enteral Nutrition in Mechanically Ventilated Patients Admitted to the Neuro-Intensive Care Unit Dear Editor, The enteral
Gastrointestinal Feedings Post Op: What s the deal on beginning oral feedings?
 Gastrointestinal Feedings Post Op: What s the deal on beginning oral feedings? Kate Willcutts, DCN, RD, CNSC University of Virginia Health System Charlottesville, VA kfw3w@virginia.edu Objectives 1. Discuss
Gastrointestinal Feedings Post Op: What s the deal on beginning oral feedings? Kate Willcutts, DCN, RD, CNSC University of Virginia Health System Charlottesville, VA kfw3w@virginia.edu Objectives 1. Discuss