COLLECTIVE REVIEW. Current Surgical Options in Short Bowel Syndrome. PattamapondLimpanopas MD. Assoc.Prof.Dr. SurasakSangkhathat(Supervisor)
|
|
|
- Ronald Palmer
- 5 years ago
- Views:
Transcription

1 COLLECTIVE REVIEW Current Surgical Options in Short Bowel Syndrome PattamapondLimpanopas MD. Assoc.Prof.Dr. SurasakSangkhathat(Supervisor)

2 Current surgical options in Short Bowel Syndrome Definition Intestinal failure (IF) was firstly defined in 1981 by Fleming and Remington as a reduction in the functioning gut mass below the minimal amount necessary for adequate digestion and absorption of food [1]. The European Society for Clinical Nutrition and Metabolism defined intestinal failure (IF) as the reduction of gut function below the minimum necessary for the absorption of macronutrients and/or water and electrolytes, such that intravenous supplementation is required to maintain health and/or growth [2], in which short bowel syndrome is its most frequent cause. Short bowel syndrome (SBS) is a malabsorptive condition that is caused by congenital defect or an acquired shortage of small bowel length - surgical resection of the small intestine - disease-associated loss of absorption and is characterized by the inability to maintain protein-energy, fluid, electrolyte, or micronutrient balances when on a conventionally accepted, normal diet [3], [4]. The classification based on functional outcome was introduced by Shaffer in 2002 [13] Type I IF) an acute, short-term and usually self limiting condition, commonly occurring in the peri-operative setting and/or in association with critical illnesses, and requiring IVS for a few days or a few weeks
3 Type II IF) a prolonged acute condition, often in metabolically unstable patients, such as those with an intraabdominal catastrophe, enterocutaneous fistulae, or acute mesenteric ischemia, requiring complex multi-disciplinary care and intravenous supplementationover periods of weeks or month Type III IF) a chronic condition, in metabolically stable patients, who require intravenous supplementation over months or years. It may be reversible or irreversible. [4], [11-12] The latest revision has been made recently by Pironi et al. (see table 1) In the anatomical classification type I: represents the potentially severest condition being an end-jejunostomy tyoe II: there is jejunocolic continuity but there is no ileocolic valve present type III: there is a jejunoileal anastomosis and the ileocecal valve is preserved
4 The prognostic factor in short bowel syndrome are the age of the patient, diagnosis of an intrinsic bowel disease [Crohn s], systemic disease, the presence of duodenum, IC valve, the colon length, and the length of remnant small bowel. (shown in the table 2) Epidemiology The Retrospectice cohort study in Canada showed the overall incidence of short bowel syndrome is 24.5 per 100,000 live births. The incidence is much greater in premature live births.the Canadian incidence of SBS is approximately 85 cases annually [5]. The incidence and prevalence of short bowel syndrome have increased over the past decades. In Europe, the estimated incidence and prevalence is 2-3 per million and 4 per million, respectively [6],[8]. Etiology Short Bowel Syndrome is the predominant cause of intestinal failure in children and is related to congenital causes such as atresias, gastroschisis or acquired conditions including volvulus, and necrotizing enterocolitis [7]. The main causes of SBS [14] in children remain congenital and perinatal diseases, such as intestinal atresia, abdominal wall defects (gastroschisis), malrotation/ volvulus, and extensive Hirschsprung s disease. In the non-neonatal population; the volvulus, trauma and Crohn s disease are the leading etiologies.
![The etiologies of short bowel syndrome are presented in Table3. [8] injury.](/docs-images/87/97036124/images/5-0.jpg "From the table 3 can be concluded, the etiology of SBS results from bowel resection for ischemia or bowel Embryology (From Larsen WJ.Human Embryology. 2nd ed.")
 elongates and forms the jejunoileal loops.")
5 The etiologies of short bowel syndrome are presented in Table3. [8] injury. From the table 3 can be concluded, the etiology of SBS results from bowel resection for ischemia or bowel Embryology (From Larsen WJ.Human Embryology. 2nd ed. Hong Kong: Churchill Livingstone; 1997:241.) At the end of the 6 th week GA, the intestinal loop herniates through the umbilicus and rotates 90 degrees counterclockwise around the SMA(A,B). The small intestine (prearterial) elongates and forms the jejunoileal loops. During the 10 th week, the jejunoileal loops retract into the abdominal cavity, and rotate an additional 180 degrees counterclockwise(c), makes a total of 270 degrees. The postarterial loop will form the colon, remains relatively straight. As the midgut completes its return, the cecum lies in the RUQ(D). The mesenteries become adherent to the parietal
6 peritoneum. The cecum separates the liver, the increasing distance becomes occupied by the lengthening ascending colon. Finally, the liver position is in RUQ and the cecal position is in RLQ (E). [9] The small bowel is completely formed by 20 weeks of gestation. Most of its growth occurs in the 3rd trimester gestation and increases to approximately 250 cm with a diameter of 1.5 cm after 35 weeks of gestation [10]. The mucosal surface area increases with age; an average infants intestine is about 950 cm 2 compared with an adult intestine of 7500 cm 2. Pathophysiology Intestinal failure can be classified into 5 major pathophysiological conditions, which may originate from various gastrointestinal or systemic diseases(show in table 4 [11] ): 1. Short bowel: A short bowel may be the result of extensive surgical resections or of congenital diseases of the small intestine.the primary pathophysiological mechanism is the reduced intestinal absorptive surface area.
7 The likelihood of developing an SBS-associated IF depends on the residual small bowel length in continuity and on several concomitant mechanisms related to the anatomy, integrity, function and adaptive potential of the small bowel remnant as well as to the underlying clinical condition [15]. The post-resection intestinal adaptation is a spontaneous process that attempts to ensure a more efficient absorption of nutrients per unit length of the remaining bowel. This occurs partly by increasing the absorptive area (structural adaptation) and/or by slowing the gastrointestinal transit (functional adaptation). It is promoted by the presence of nutrients in the gut lumen, by the pancreatic and biliary secretions and by gut hormones mainly produced by the ileum and colon, and usually takes place over 1 or 2 years. Postoperative intestinal adaptation appears to be absent or impaired in the presence of an end-jejunostomy [15]. Other mechanisms contributing to IF may be, excessive fluid and electrolyte intestinal losses in the presence of an end jejunostomy, restriction of oral nutrient intake in an attempt to decrease the intestinal losses, reduced oral intake because of underlying disease-related hypophagia and failure to develop the post-resection adaptive hyperphagia. SBS-associated IF may be reversible because of the intestinal adaptation process and/or intestinal rehabilitation programs based on medical and surgical treatments [16]. 2. Intestinal fistula Abnormal communications between 2 parts of the gastrointestinal tract, between the gut and the other organs, or between the gastrointestinal tract and the skin (enterocutaneousfistulas, EC) [17]. In EC fistulas, the enteric content is prematurely lost from the small bowel lumen. The primary mechanism of IF is the bypass of a large area of intestinal absorption surface, a condition resembling a short bowel [17]. The onset of an EC fistula is often an acute event, associated with intra-abdominal abscess collection, systemic sepsis and the related metabolic derangement, as well as with high intestinal fluid and electrolyte losses with the fistula effluent. Concomitant pathophysiological mechanisms contributing to EC fistula-associated IF may be the impairment of gastro-intestinal motility and the metabolic alterations associated with systemic sepsis or intra-abdominal inflammation, the excessive intestinal losses of fluids and electrolytes, the disruption of the entero hepatic cycle of bile acids, and the restricted or abolished ( bowel rest ) oral/enteral nutrition to decrease the fistula output and/or to favor spontaneous fistula closure [11],[18]. 3. Intestinal dysmotility The presence of disorders of the propulsion of the gut content in the absence of fixed occluding lesions. It may be locoregional, affecting only one bowel segment, as in achalasia, gastroparesis, colonic obstruction and Hirschprungs' disease, or multi-regional, involving more than one part of the GI tract, especially the small bowel. Acute intestinal
8 dysmotility is the primary pathophysiological cause of type I IF due to post-operative or acute critical illness associated ileus, and a frequent concomitant cause of type II IF, due to the impaired gastrointestinal motility associated with systemic or intra-abdominal inflammation. Permanent intestinal dysmotility is termed chronic intestinal pseudoobstruction (CIPO), where the modifier pseudo is used to underline the absence of occluding lesions [11], [19]. In intestinal dysmotility, the primary pathophysiological mechanism is intolerance to oral or enteral nutrition resulting in inadequate nutritional intake. The mucosal surface is generally intact. Secondary mechanisms include nutrient malabsorption due to small bowel bacterial overgrowth, and increased intestinal secretion and/or losses of fluids and electrolytes, occurring in the dilated bowel segments, or after intestinal resection and venting or end-ostomy performed to relieve symptoms. CIPO-associated IF represents approximately 20% of both adults and children on HPN for type III chronic IF. The reversibility of IF in patients with CIPO is lower than that reported in SBS, having been reported in 25 50% in adults and 25 38% in children, with a 78% 5 year survival probability for adults on HPN [20]. 4. Mechanical obstruction Mechanical obstruction results from a physical abnormality affecting the intestine, which may be intraluminal, intrinsic or extrinsic, of benign or malignant origin. It may be an acute event encompassing a feature of type I IF, that resolves in a few days through conservative medical treatment or a surgical procedure. It may also be a prolonged feature, determining a type II or III IF, as in patients with extensive adhesions ( frozen abdomen ), or in those with peritoneal carcinomatosis associated with late-stage intra-abdominal malignancy. The primary pathophysiological mechanism of IF in obstruction is the spontaneous or prescribed ( bowel rest ) abolished oral or enteral nutrition. Secondary mechanisms include the increased intestinal secretion of fluids and electrolytes in the obstructed segment, and increased intestinal losses of fluids and electrolytes with vomiting or NG drainage 5. Extensive small bowel mucosal disease Extensive small bowel mucosal disease is an intact or almost intact, although inefficient, mucosal surface [20-22]. The reduction of nutrient absorption and/or the loss of nutrients through the intestinal mucosa to the point where the body's requirements are no longer met, are the most frequent primary mechanisms of IF. Rarely, increased intestinal secretion of fluids and electrolytes can be present as a concomitant mechanism. Extensive small bowel mucosal disease has been reported to be the cause of CIF in about 25% of children and 5% of adult patients on long term HPN. In adults with type III IF due to extensive mucosal disease, weaning from HPN rarely occurs [20].

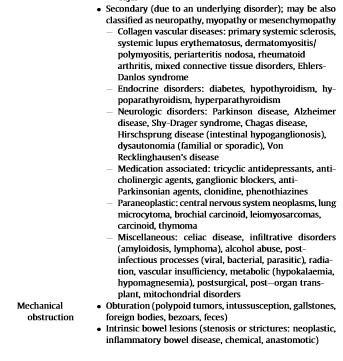
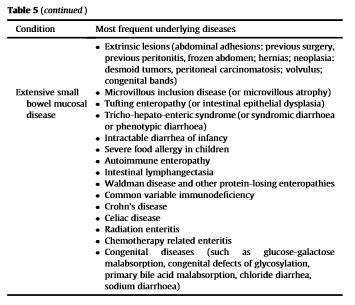
9 Table 5 [11]
10 Imaging Studies 1. Film abdomen 2. UGI study 3. CT whole abdomen 4. Endoscopy or Colonoscopy General Management Scheme Intestinal adaptation Intestinal adaptation is the process following intestinal resection whereby the remaining bowel undergoes macroscopic and microscopic changes that serve to increase its absorptive ability. Adaptation is highly variable and usually occurs during the first two years following intestinal resection in adults and for longer and perhaps more vigorously in children. Adaptive changes are usually most prominent in the ileum and to a lesser extent, in the jejunum and colon. These changes are mediated by a variety of internal and external stimuli including nutrients, gastrointestinal secretions, hormones, and growth factors and other genetic and biochemical factors. In particular, adaptation depends upon the nutrient components of the diet and on influences from the remaining segments of the intestine. Both structural and functional changes can occur: Structural adaptive changes include dilation and elongation of the remnant bowel, an increase in intestinal wet weight, protein and DNA content, villus lengthening, expansion in microvilli, and an increase in crypt cell depth and enterocyte number. These morphologic changes in the mucosa are driven by a proliferative stimulus that affects cellular progression along the crypt-villus axis, resulting in an increase in mucosal weight and enlargement in mucosal folds. Adaptation of the gut muscle layers also takes place, leading to an increase in muscle thickness, circumference, and length. Functional adaptive changes occurring include modifications of the brush border membrane enzyme activity, fluidity and permeability, up- or downregulation of carrier-mediated transport (eg, upregulation of Na+/glucose cotransporters, Na+/H+ exchangers, and other enzymes involved in digestion and absorption) and a slowing in
11 the rate of transit, allowing more time for absorption to occur [49-50]. Adaptive changes in gut microbiota, motor activity, and barrier and immune functions after massive intestinal resection are poorly understood. Animal models of SBS provide insight into the adaptive process. After bowel resection, epithelial hyperplasia is seen within 24 to 48 hours [51-56]. The length of villi and intestinal absorptive area increases and digestive and absorptive function gradually improve. These morphologic changes are associated with changes in expression of a variety of genes [57-59], some of which are known mediators of intestinal growth. These adaptive changes are more apparent in the animal models compared with humans with SBS. Furthermore, most studies investigating the process of adaptation have utilized animal models with a jejuno-ileocolonic anastomosis, a relatively uncommon bowel anatomy in humans with SBS. Thus, the physiologic and structural changes that occur in the animal models are of unclear clinical relevance. Ileal versus jejunal adaptation The ileum is capable of undergoing marked adaptation after small bowel resection, with significant growth in villus surface area, as well as increases in intestinal length, diameter, and motor function [60-61]. These structural changes are primarily responsible for enhancement of nutrient uptake in a given segment of bowel [62]. However, there is also some evidence for functional improvement of absorption through upregulation of transporters and of brush border enzymes. These adaptive changes lead to a gradual improvement in macronutrient absorption during the first one to three years after jejunalresection [63]. The jejunum exhibits more modest adaptive changes in response to intestinal resection, and most of these changes are functional (changes in transport and enzyme activity) rather than structural (changes in absorptive area) [15]. Jejunal adaptation appears to depend on influences from other remaining segments of the bowel; patients with a jejunocolic anastomosis demonstrate functional small bowel adaptation, whereas those with an end-jejunostomy show little to no adaptation. Despite limited evidence, similar effects would be expected in those with colon-in-continuity versus those whose colon remains but is not in continuity, given the lack of nutrient exposure to the excluded colon. This reinforces the importance of the colon in the prognosis of the patient with SBS.
12 Medical management Early management During the first few months after intestinal resection, the predominant goals are maintenance of good nutritional status through administration of parenteral nutrition (PN) and prevention of fluid and electrolyte abnormalities. Parenteral nutrition In this early phase, the major portion of energy is delivered through PN, but enteral nutrition should be initiated promptly to support intestinal adaptation. The principles of prescribing PN to infants and children are discussed in detail in a separate topic review. In patients who will likely require PN for more than three weeks, we commonly restrict soy-based intravenous lipids solutions to a dose of 1 gm/kg/day in order to reduce the risk of intestinal failure-associated liver disease (IFALD). Infants with SBS are at particular risk of developing IFALD and therefore should be monitored carefully for this condition. Fluid management Large-volume fluid losses from gastric or proximal small bowel secretions are common in the early phase. As a result, patients require rigorous replacement of fluids with sodium, potassium, chloride, and magnesium. Fluid and electrolyte losses through an enterostomy or in the feces (if these are >2 ml/kg/hr) should be measured and replaced. Most of the chronic fluid replacement usually can be supplied through PN using a solution that is tailored to the patient's fluid and electrolyte needs. Acute increases in enteral losses may warrant immediate replacement. This should be done with a solution separate from the parenteral nutrition, to allow timely and accurate replacement of the losses. High output ostomy or stool losses can also be replaced with appropriately formulated oral rehydration solutions. These solutions generally contain a suitably designed mix of water, electrolytes, and carbohydrate to replace diarrheal losses. Acid suppression Patients with SBS often exhibit hypersecretion of gastric acid and fluids, which reduces ph below the optimal level needed for fat absorption (by inactivating pancreatic lipase and deconjugating bile salts), alters enteral drug absorption, and increases intestinal fluid losses. Histamine 2 receptor antagonists (eg. ranitidine) and proton pump inhibitors (PPIs; eg, omeprazole) inhibit excessive gastric secretion. Routinely administration the acid suppression to patients during the early phase of SBS after intestinal resection, when gastric hypersecretion is most common. Acid blockade decreases the acid load delivered to the duodenum and may be particularly helpful in managing gastrointestinal outputs in patients with extensive ileal resection.
13 Growth Goals The resting energy expenditure in infants with SBS is similar to that in healthy controls [64]. However, because of malabsorption, patients with SBS typically require 30 to 70 percent more calories if they are fed enterally compared with their energy needs from PN [65]. Growth is monitored by assessing whether increases in weight are proportional to linear growth, using standard growth curves for infants, with adjustment for premature birth until two years of age. Enteral Feeding Enteral feeding is a central goal in management of a patient with SBS. Enteral feeds should be introduced early, and advanced carefully but persistently, as rapidly as tolerated by the patient. Enteral feeding is important for several reasons: The presence of nutrients in the intestinal lumen is essential to promote intestinal adaptation, and appears to be more effective if enteral feeds are initiated early [66-68]. This effect occurs even when only small amounts of feeds are given (sometimes termed "trophic feeds"). Absence of enteral feeding may induce atrophy of the mucosa [69]. As enteral feeds are increased, parenteral nutrition (PN) can be decreased, reducing the risk for complications of long-term PN such as intestinal failure-associated liver disease (IFALD) and metabolic bone disease. Some oral feeding is important in infants in order to avoid feeding aversion. Surgical approaches The initial goal of management in patients with intestinal failure is to wean parenteral nutrition and minimize parenteralnutrition associated comorbidities. Timing is an essential consideration when considering a surgical intervention for intestinal rehabilitation. Early surgery may be an unnecessary, as bowel adaptation and lengthening may prevent the need for long term TPN. Late surgery exposes the patient to additional TPN-related costs and complications
![Phase of treatment Surgical options in patients with long-term intestinal failure fall into 4 main categories as show in table 6 [23] (1) Operations to Correct Slow Transit Slow transit in SBS is](/docs-images/87/97036124/images/14-0.jpg "relatively rare and should trigger a search for strictures, partial obstructions or blind loops, and enteroenteric fistulas [24].")
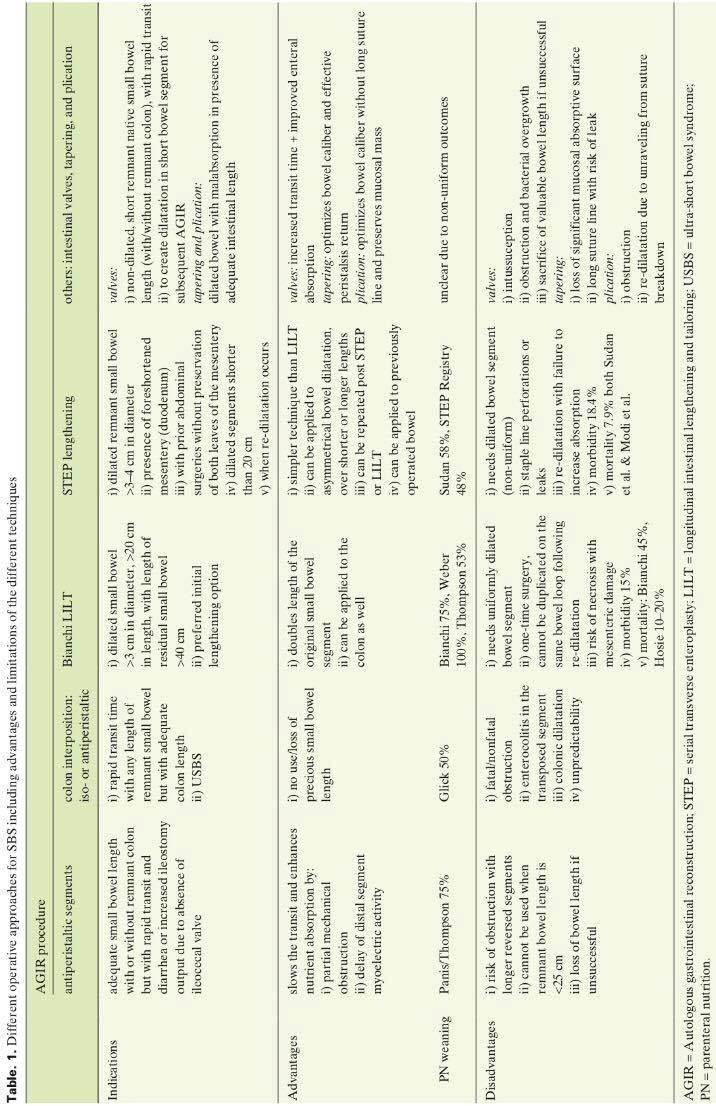
14 Phase of treatment Surgical options in patients with long-term intestinal failure fall into 4 main categories as show in table 6 [23] (1) Operations to Correct Slow Transit Slow transit in SBS is relatively rare and should trigger a search for strictures, partial obstructions or blind loops, and enteroenteric fistulas [24]. These are often sequelae of the underlying disease leading to SBS, such as Crohn s disease, and often require meticulous investigation to diagnose and treat appropriately. A high index of suspicion regarding patients whose clinical behavior is at odds with their underlying anatomical characteristics should permit the discovery and satisfactory resolution of such cases. (2) Operations to Improve Intestinal Motility in Cases of Dilated Bowel Rapid intestinal transit is a nearly universal clinical challenge in SBS and should elicit prompt investigation into underlying structural causes. Segmental bowel dilatation with poor peristalsis is a frequent finding in patients with SBS and rapid transit, and it often results in clinical features of small bowel bacterial overgrowth. (3) Operations to slow intestinal transit in the absence of bowel dilatation Segmental reversal of the small bowel (SRSB) is a procedure that designed to slow transit in the absence of bowel dilatation [36]. SRSB creates an antiperistaltic segment of bowel approximately cm in length, located ~10 cm proximal to an end-stoma or the small bowel-colon anastomosis [37]. Of 38 patients undergoing SRSB over a 25-year period at a single center, 17 (45%) achieved complete independence from PN. Among patients who were not weaned, PN requirements were decreased by a median 3 days per week. A shorter interval between enterectomy and SRSB, an SRSB >10 cm, and an extended stay with the nutrition unit were significantly associated with enteral autonomy [38].
15 (4) Operations to increase mucosal surface area Although the creation of neomucosa remains an elusive goal, use of sequential lengthening procedures and controlled tissue expansion (CTE) before bowel lengthening may have immediate, albeit limited, clinical application. The theoretical basis for the strategy of CTE of non dilated bowel in preparation for definitive intestinal lengthening was laid out in experimental work on pigs by the demonstration of mucosal hypertrophy and gain in length and diameter of partially obstructed intestine [39]. More recent experience from the Ann Arbor group suggests that redilation after prior lengthening may be an overall poor prognostic sign and merits caution [40]. Surgical options 1. Non-intestinal transplantation a. Increase transit time b. Enhance adaptation 2. Intestinal transplantation 1. Non-intestinal transplantation a.increase transit time A simple tapering enteroplasty is most easily managed the excessive intestinal in which a strip of intestine along the antimesenteric border of dilated bowel is removed using a mechanical stapling device [26]. This procedure is most applicable when bowel length is considered adequate and when loss of surface area is an acceptable tradeoff for better prograde peristalsis. Reversing intestinal segments: interposition of a reversed, antiperistaltic segment of bowel creates a physiologic valve Intestinal Valve: Partially obstructing intestinal valves have traditionally employed for patients with short intestinal length and normal caliber, but who are also hampered by rapid transit. The simplest techniques include the placement of sutures or an external Teflon collar around the circumference of the bowel Colon interposition: used consists of interposing of a segment of colon between two limbs of small bowel in patients with rapid intestinal transit b.enhance adaptation
 operation first described by Adrian Bianchi")
![[25] accomplishes intestinal tapering without loss of](/docs-images/87/97036124/images/16-1.jpg "surface area used in cases where bowel length is")
16 The longitudinal intestinal lengthening and tailoring (LILT) operation first described by Adrian Bianchi [25] accomplishes intestinal tapering without loss of surface area used in cases where bowel length is critical.
17 The LILT procedure are 1.An avascular space is created longitudinally along the mesenteric border of a dilated loop of bowel. 2. The bowel is then split lengthwise, taking care to allocate alternating blood vessels to each side. 3. Each side of the split bowel is then tubularized, generating 2 hemi-loops that are anastomosed end to end in isoperistalticfashion (Figure 2 [25],4 [30] ). When completed, LILT creates a loop of bowel that is twice the length of the original and half the original diameter; no new bowel is created. The decrease in bowel diameter accomplished without loss of surface area is likely more important than the gain in length. Anatomical criteria for LILT are 1. Intestinal diameter > 3 cm 2. Residual bowel length > 40 cm 3. A length of dilated bowel loops > 20 cm [70] LILT can lead to less bacterial overgrowth and stasis. Bianchi has described a protocol for the management of SBS with an important role for intermittent clamping of the tube jejunostomy to expand the diameter of the small bowel [71]. Bianchi s early personal experience with the procedure in 20 children resulted in 7 of 9 survivors attaining enteral autonomy from PN at a mean follow-up of 6.4 years [27]. The LILT should be applied with extreme caution in patients with ultrashort bowel and in the presence of liver disease [27,28]. However, notwithstanding the need for cautious patient selection, we have reported on functional liver recovery even in the presence of moderate to advanced liver disease in carefully chosen patients following autologous gut salvage [32]. Based on a recent report, outcomes following autologous gastrointestinal reconstruction are improving with accumulating experience. Of 27 children undergoing various autologous procedures for SBS, including 19 LILT procedures, overall survival was 92%, and >90% of survivors achieved independence from PN [31]. Complications Initially, the reported complication rate was high with anastomotic stenosis (18%), staple line leakage (13%), interloop abscess (7%), and fistula formation (7%) [72-77]. Mortality in these series resulting from intra-abdominal sepsis and liver failure were around 30%. However recent series show that with more surgical experience an acceptable complication rate and no surgical related mortality can be achieved [78]. Survival after LILT is comparable to other AIR procedures between 87 and 95%.
18 The serial transverse enteroplasty (STEP) procedure described by Kim et al in 2003 [29], is a tapering without loss of surface area. It is accomplished effectively and relatively simply. STEP is based on the anatomical principle of the vessels rising from the mesenteric border and enfolding the bowel perpendicularly to the long axis of the bowel. There is no lower limit in bowel length to perform STEP, but a minimal luminal diameter of cm is required The STEP procedure are 1.The luminal channel is placed with the staples in zig-zag pattern 2. The luminal is narrowed by firing a series of staples perpendicular to the long axis of the bowel in a zig-zag pattern without interfering with the blood supply of the bowel (Figure 3 [25] ).

19 In a long-term study of 12 pediatric patients who underwent STEP, 8 (67%) patients remained alive and transplant-free at a median follow-up of 5.7 years. Of those 8 patients, 7 achieved independence from PN. In addition, the dilated segment showed an 87% increase in median length and a 67% decrease in mean internal diameter [33]. A recent retrospective observational study of 111 consecutive patients enrolled in the international STEP registry provides additional impetus for more serious consideration of the appropriateness of the STEP procedure in suitable patients [35]. Of 97 patients for whom complete data were available, 11 patients died and 5 required intestinal transplantation. In a multivariate analysis, risk of progression to transplantation or death was greater among patients with shorter bowel length before surgery and higher conjugated bilirubin levels. The choice of lengthening procedure between the Bianchi LILT and the technically simpler STEP remains somewhat unclear and until recently seemed related to surgeon preference. In a retrospective, uncontrolled, single-center study, Sudan et al [34] reported outcomes of 64 patients who underwent a total of 43 LILT and 34 STEP procedures over a 24-year period. Overall survival was 91% at a median follow-up of 3.8 years. Enteral autonomy was achieved by 69% of PN-dependent patients, and liver disease was reversed in >80% of affected patients. Differences between the 2 procedures were small, although nonsignificant trends were documented for a lower rate of weaning from PN, longer time to PN discontinuation, and a higher incidence of complications requiring reoperation after LILT than after the STEP procedure. Of note in this series, 14% of patients underwent intestinal transplantation at a median of 2.9 years. Transplantation was required more often following LILT than after the STEP procedure (18.6% vs 5%, respectively; P =.03),
![although this difference may be due in part to the longer follow-up time for patients receiving LILT (5.9 vs 1.7 years for STEP) [34].](/docs-images/87/97036124/images/20-0.jpg "Spiral intestinal lengthening and tailoring (SILT)was introduced in 2011 by Cersni et al. in an experimental animal model as a possible alternative and additive to STEP and LILT [47]. 1.")
20 although this difference may be due in part to the longer follow-up time for patients receiving LILT (5.9 vs 1.7 years for STEP) [34]. Spiral intestinal lengthening and tailoring (SILT)was introduced in 2011 by Cersni et al. in an experimental animal model as a possible alternative and additive to STEP and LILT [47]. 1. The incisions in the mesentery are made carefully without damaging any vessels 2. The intestinal wall is cut spirally in angle to the longitudinal axis The total length will increase and its diameter is reduced by stretching the bowel over a tube preserving the adjust luminal diameter (Figure 6) [48]. An advantage of SILT is the mild alteration of the position of the intestinal muscle fibres and therefore should influence peristalsis less. A major disadvantage of SILT is the requirement to open the lumen completely, whereas in a STEP procedure the lumen remains closed, reducing bacterial contamination. Thereto, in an experimental model a modified SILT procedure was developed where the mucosa is remained intact with incisions made only in the muscular and submucosal layer so that the lumen is only opened on the outer ends [81].
21 Table 7 show the comparison of technique and outcome of the Intestinal lengthening procedure. 2.IntestinalTransplantation For patients in whom all attempts at intestinal rehabilitation have failed and who are at risk of life-threatening complications of PN, intestinal transplantation has emerged as the standard of care. The US Centers for Medicare and Medicaid Services (CMS) approved intestinal transplantation for patients with irreversible IF and PN-related complications in 2000 and extended the approval to multivisceral transplantation the following year. The CMS definition of PN failure includes the following: 1. Presence of PN-associated liver disease 2. Loss of central venous access (ie, loss of 3 6 central venous access sites in children or 2 4 central venous access sites in adults) 3. Recurrent catheter-related sepsis or a single episode of fungal sepsis 4. Recurrent bouts of severe dehydration or metabolic abnormalities [41] Absoulte Contraindications to Intestinal transplantation 1. Active infection 2. Malignancy

 or in combination with the liver (i.")
22 Relative Contraindications to Intestinal transplantation 1. Severe neurodevelopmental disability 2. Psychosocial factors In the absence of liver disease, isolated intestine transplantation, often including the right colon, is the procedure of choice. For patients with moderate biochemical and histologic liver disease, we have demonstrated that successful isolated intestinal transplantation results in biochemical improvement of liver function and may also allow histologic liver recovery [42],[43]. Transplantation of the intestine may be performed alone (i.e.,isolated intestine transplantation) or in combination with the liver (i.e., a combined liver/intestine or multivisceral transplantation). 9 8
23 Figure 8 demonstrates details of the surgical technique of isolated intestine transplantation with replacement of the entire jejunum and ileum. A combined liver/intestine transplantation is performed in patients with advanced liver disease and occasionally in patients with mesenteric or pancreatic neoplasms (most commonly enbloc with the duodenum and pancreas to maintain the donor hepatic hilar structures undisturbed). Figure 9 depicts details of the liver/bowel or multivisceral operative technique. Small bowel transplants alone are offered to patients with 1.intestinal failure that cannot be managed on total parenteral nutrition (vide supra) and/or 2.mild to moderate liver dysfunction due to total parenteral nutrition. Combined bowel-liver transplants are offered to patients with 1.intestinal failure and advanced, irreversible liver failure due to total parenteral nutrition and 2.intestinal failure due to a hypercoagulable state associated with enzyme deficiencies that can be corrected by a liver graft (e.g., mesenteric vascular thrombosis secondary to protein C or S deficiency). Complications 1. Immunologic complications - Rejection and graft-versus-host disease Clinical rejection symptoms (including abdominal pain and distention, tenderness on palpation, ileus, increased fecal volume and stomal output, diarrhea) are unspecific and appear often late - after rejection is already apparent on histology. Therefore, biopsy evaluation is - as for all other solid organ grafts - the gold standard for the diagnosis of intestinal rejection. Surveillance intestinal (transstomal) biopsies are obtained twice weekly for the first 2 months, then weekly for the following 4 months, and monthly thereafter. Endoscopic biopsies must be taken from all areas of the graft (because intestinal rejection can be confined to specific bowel segments) and should always include ileal specimens (because rejection is more frequently observed in the ileum than in the jejunum and colon). Clinically relevant graft-versus-host disease is - in contrast to the findings of many experimental studies - relatively rare.
24 - Posttransplantlymphoproliferative disease The PTLD incidence in intestinal recipients (ranging from 15% in adults to up to 25% in children) is higher than in other solid organ recipients(2). Most PTLDs are EBV virus infection-associated and have a deleterious overall effect on graft and patient survival. PTLD therapy includes reduction or cessation of immunosuppression, antiviral therapy with acyclovir and ganciclovir, administration of α-interferon, and chemotherapy. However, these interventions result frequently in rejection episodes and graft losses. More recently, strategies have been focused on surveillance for, and early diagnosis of, EBV infections using molecular biology techniques (polymerase chain reaction)(5). But the impact of therapeutic interventions based on these more refined screening and diagnostic methods is presently unknown and awaits further study. 2. Infectious complications - Bacterial and fungal infections Breakdown of the mucosal barrier of intestinal grafts (e.g., during rejection episodes) can cause bacterial and fungal translocation into the mesenteric lymph nodes and into the portal and systemic circulation, presenting clinically as sepsis. Thus, treatment of translocation-associated infections due to rejection includes both antimicrobial and antirejection therapy. Prophylactic interventions, such as systemic and local (selective gut decontamination) administration of antimicrobial agents have proven ineffective, leading instead to the emergence of multiresistant organisms. - Viral infections The cytomegalovirus is the clinically most significant viral pathogen in intestinal transplant recipients(2). CMV infections still cause considerable morbidity and have been associated with increased mortality, in spite of the availability of effective antiviral therapy (e.g., ganciclovir). At highest risk are CMV-seronegative intestinal recipients of organs from CMV-positive donors. This has led to the recommendation that only seronegative donors be used for seronegative recipients - at least for bowel alone-recipients, since recipient candidates with concomitant liver failure may not survive a prolonged waiting period for a suitable seronegative donor The 1-year graft and patient survival rates for transplants done in the current era were respectively 55% and 69% for intestinal grafts, 63% and 66% for bowel-liver grafts, and 63% and 63% for multivisceral grafts. Of all intestinal recipients alive as of 1997, over 75% were off total parenteral nutrition after successfully resuming an oral diet [82]
25 Despite a trend for earlier consideration of intestinal transplantation, >50% of patients listed for intestinal transplantation are simultaneously listed for liver replacement [44]. The mortality rate on the liver-intestine transplant waiting list can reach 30%, compared with a 9% mortality rate on the isolated intestine transplant list [45]. Thus, early referral of patients who are failing PN may increase the rate of isolated intestinal transplantation and thereby reduce the significant mortality associated with waiting list placement. Patient and graft survival rates at 1 year are 89% and 79%, respectively, following isolated intestinal transplantation and are 72% and 69%, respectively, following combined liverintestine transplantation [44]. The relative tolerogenic capacity of liver-derived lymphocytes compared with intestinederived lymphocytes may explain the immunoprotective effects of combined liver-intestinal transplants compared with isolated intestinal transplants [46]. It is hoped that newer strategies to improve human leukocyte antigen matching and to account for the possible role of B lymphocytes in long-term graft survival may allow us to translate improved early outcomes into prolonged gains.
26
27 References 1. C.R. Fleming, M. Remington. Intestinal failure. G.L. Hill (Ed.), Nutrition and the surgical patient, Churchill Livingstone, Edinburgh (1981), pp Pironi Loris. Definitions of intestinal failure and the short bowel syndrome. Best Practice and Research Clinical Gastroenterology. 2016; 30: O'Keefe SJ, Buchman AL, Fishbein TM, et al. Short bowel syndrome and intestinal failure: consensus definitions and overview. ClinGastroenterolHepatol 2006; 4:6. 4. Matthijs J. Hommel, Robertine van Baren, Jan Willem Haveman. Surgical management and autologous intestinal reconstruction in short bowel syndrome. Best Practice and Research Clinical Gastroenterology. 2016; 30: Wales PW, de Silva N, Kim J, et al. Neonatal short bowel syndrome: population-based estimates of incidence and mortality rates. J PediatrSurg 2004; 39: Eca Rosario, Barbosa Elisabete. Short bowel syndrome: treatment options. Journal of Coloproctology; 2016: 36: 4: Goulet O, Ruemmele F. Causes and management of intestinal failure in children. Gastroenterology 2006; 130 (Suppl): Debora Duro, Daniel Kamin. Overview of short bowel syndrome and intestinal transplantation. Colombia Medica. 2007;38: Dale Huff, Pierre Russo. Congenital and Developmental Disorders of the Gastrointestinal Tract. In: Larsen WJ, editors. Human Embryology. 2 nd ed. Hong Kong: Churchill Livingstone; 1997: 241: p Weaver LT, Austin S, Cole TJ. Small intestinal length: a factor essential for gut adaptation. Gut 1991; 32: Pironi L, Arends J, Baxter J, Bozzetti F, Burgos R, Cuerda C, et al. ESPEN endorsed recommendations. Definition and classification of intestinal failure in adults. ClinNutr 2015; 34: Feldmad M, Friedman LS, Sleisenger MH, In: Sleisenger&Fordtran s gastrointestinal and liver disease: pathofysiologym diagnosis, management. 7 th ed. Elsevier; p Shaffer J. Intestinal failure: definition and service development. Clin Nutrition; 2002: 21(Suppl. 1): Wales PW, Christison-lagay ER. Short bowel syndrome: epidemiology and etiology. SeminPeriatrSurg 2010; 19: A.L. Buchman, J. Scolapio, J. Fryer. AGA technical review on short bowel syndrome and intestinal transplantation. Gastroenterology, 124 (2003), pp
28 16. K.M. Rhoda, N.R. Parekh, E. Lennon, C. Shay-Downer, C. Quintini, E. Steiger, et al. The multidisciplinary approach to the care of patients with intestinal failure at a tertiary care facility.nutrclinpract, 25 (2010), pp Irving M. Spectrum and epidemiology of intestinal failure.clinnutr. 1995; 14: W.P. Schecter, A. Hirshberg, D.S. Chang, H.W. Harris, L.M. Napolitano, S.D. Wexner, et al. Enteric fistulas: principles of management. J Am CollSurg; 2009: C. Di Lorenzo, N.N. Youssef. Diagnosis and management of intestinal motility disorders. SeminPediatrSurg; 2010: 19: L. Pironi, O. Goulet, A. Buchman, B. Messing, S. Gabe, M. Candusso, et al. Outcome on home parenteral nutrition for benign intestinal failure: a review of the literature and benchmarking with the European prospective survey of ESPEN. ClinNutr; 2012: 31: L. D'Antiga, O. Goulet. Intestinal failure in children: the European view. J PediatrGastroenterolNutr; 2013: 56: O. Goulet, F. Ruemmele, F. Lacaille, V. Colomb. Irreversible intestinal failure. J PediatrGastroenterolNutr; 2004: 38: Iyer R. Kishore. Surgical Management of Short Bowel Syndrome. Journal of Parenteral and Enteral Nutrition. 2014: 38: 53S-59S. 24. Thompson JS. Strategies for preserving intestinal length in the shortbowel syndrome. Dis Colon Rectum. 987;30: Bianchi A. Intestinal loop lengthening a technique for increasing small intestinal length. J Pediatr Surg. 1980;15: Weber TR, Vane DW, Grosfeld JL. Tapering enteroplasty in infants with bowel atresia and short gut. Arch Surg. 1982;117: Bianchi A. Longitudinal intestinal lengthening and tailoring: results in 20 children. J R Soc Med. 1997;90: Bianchi A. From the cradle to enteral autonomy: the role of autologous gastrointestinal reconstruction. Gastroenterology. 2006;130:S138-S Kim HB, Fauza D, Garza J, Oh JT, Nurko S, Jaksic T. Serial transverse enteroplasty (STEP): a novel bowel lengthening procedure. J Pediatr Surg. 2003;38: Sommovilla Josh, Warner W. Brad. Surgical Options to Enhance intestinal Function in Patients with Short Bowel Syndrome. CurrOpinPediatr. 2016: 1-12
29 31. Khalil BA, Ba ath ME, Aziz A, et al. Intestinal rehabilitation and bowel reconstructive surgery: improved outcomes in children with short bowel syndrome. J PediatrGastroenterolNutr. 2012;54: Iyer KR, Horslen S, Torres C, Vanderhoof JA, Langnas AN. Functional liver recovery parallels autologous gut salvage in short bowel syndrome. J Pediatr Surg. 2004;39: ; discussion Oliveira C, de Silva N, Wales PW. Five-year outcomes after serial transverse enteroplasty in children with short bowel syndrome. J Pediatr Surg. 2012;47: Sudan D, Thompson J, Botha J, et al. Comparison of intestinal lengthening procedures for patients with short bowel syndrome. Ann Surg. 2007;246: ; discussion Jones BA, Hull MA, Potanos KM, et al. Report of 111 consecutive patients enrolled in the International Serial Transverse Enteroplasty (STEP) Data Registry: a retrospective observational study. J Am Coll Surg. 2013;216: Gibson LD, Carter R, Hinshaw DB. Segmental reversal of small intestine after massive bowel resection: successful case with follow-up examination. JAMA. 1962;182: Panis Y, Messing B, Rivet P, et al. Segmental reversal of the small bowel as an alternative to intestinal transplantation in patients with short bowel syndrome. Ann Surg. 1997;225: Beyer-Berjot L, Joly F, Maggiori L, et al. Segmental reversal of the small bowel can end permanent parenteral nutrition dependency: an experience of 38 adults with short bowel syndrome. Ann Surg. 2012;256: ; discussion Collins J III, Vicente Y, Georgeson K, Kelly D. Partial intestinal obstruction induces substantial mucosal proliferation in the pig. J Pediatr Surg. 1996;31: Miyasaka EA, Brown PI, Teitelbaum DH. Redilation of bowel after intestinal lengthening procedures an indicator for poor outcome. J Pediatr Surg. 2011;46: Centers for Medicare & Medicaid Services. National coverage determination (NCD) for intestinal and multi-visceral transplantation (260.5). AAAABAAAAAA&. Accessed August 22, Fiel MI, Sauter B, Wu HS, et al. Regression of hepatic fibrosis after intestinal transplantation in total parenteral nutrition liver disease. ClinGastroenterolHepatol. 2008;6: Fiel MI, Wu HS, Iyer K, Rodriguez-Laiz G, Schiano TD. Rapid reversal of parenteral-nutrition-associated cirrhosis following isolated intestinal transplantation. J Gastrointest Surg. 2009;13:
30 44. Mazariegos GV, Steffick DE, Horslen S, et al. Intestine transplantation in the United States, Am J Transplant. 2010;10: Chungfat N, Dixler I, Cohran V, Buchman A, Abecassis M, Fryer J. Impact of parenteral nutrition-associated liver disease on intestinal transplant waitlist dynamics. J Am Coll Surg. 2007;205: Murase N, Starzl TE, Tanabe M, et al. Variable chimerism, graft-versus-host disease, and tolerance after different kinds of cell and whole organ transplantation from Lewis to brown Norway rats. Transplantation. 1995;60: Cserni T, Takayasu H et al. New idea of intestinal lengthening and tailoring. PediatrSurgInt 2011; 27(9): Cserni T. Spiral Intestinal Lengthening and Tailoring [Internet]. Available from: www/youtube.com/watch?v=zjl7ajiyxwq. 49. Longshore SW, Wakeman D, McMellen M, Warner BW. Bowel resection induced intestinal adaptation: progress from bench to bedside. Minerva Pediatr 2009; 61: Thiesen A, Drozdowski L, Iordache C, et al. Adaptation following intestinal resection: mechanisms and signals. Best Pract Res ClinGastroenterol 2003; 17: Dowling RH, Booth CC. Functional compensation after small-bowel resection in man. Demonstration by direct measurement. Lancet 1966; 2: Dowling RH, Booth CC. Structural and functional changes following small intestinal resection in the rat. ClinSci 1967; 32: Hanson WR, Osborne JW. Epithelial cell kinetics in the small intestine of the rat 60 days after resection of 70 per cent of the ileum and jejunum. Gastroenterology 1971; 60: Hanson WR, Osborne JW, Sharp JG. Compensation by the residual intestine after intestinal resection in the rat. I. Influence of amount of tissue removed. Gastroenterology 1977; 72: Hanson WR, Osborne JW, Sharp JG. Compensation by the residual intestine after intestinal resection in the rat. II. Influence of postoperative time interval. Gastroenterology 1977; 72: Nygaard K. Resection of the small intestine in rats. 3. Morphological changes in the intestinal tract. ActaChirScand 1967; 133: Juno RJ, Knott AW, Profitt SA, et al. Preventing enterocyte apoptosis after massive small bowel resection does not enhance adaptation of the intestinal mucosa. J PediatrSurg 2004; 39: Stern LE, Erwin CR, Falcone RA, et al. cdna microarray analysis of adapting bowel after intestinal resection. J PediatrSurg 2001; 36: Erwin CR, Jarboe MD, Sartor MA, et al. Developmental characteristics of adapting mouse small intestine crypt cells. Gastroenterology 2006; 130:1324.
31 60. McDuffie LA, Bucher BT, Erwin CR, et al. Intestinal adaptation after small bowel resection in human infants. J PediatrSurg 2011; 46: Schmidt T, Pfeiffer A, Hackelsberger N, et al. Effect of intestinal resection on human small bowel motility. Gut 1996; 38: Qandeel HG, Alonso F, Hernandez DJ, et al. Peptide absorption after massive proximal small bowel resection: mechanisms of ileal adaptation. J GastrointestSurg 2011; 15: Kurkchubasche AG, Rowe MI, Smith SD. Adaptation in short-bowel syndrome: reassessing old limits. J PediatrSurg 1993; 28: Jaksic T, Shew SB, Keshen TH, et al. Do critically ill surgical neonates have increased energy expenditure? J PediatrSurg 2001; 36: Woolf GM, Miller C, Kurian R, Jeejeebhoy KN. Nutritional absorption in short bowel syndrome. Evaluation of fluid, calorie, and divalent cation requirements. Dig Dis Sci 1987; 32: Andorsky DJ, Lund DP, Lillehei CW, et al. Nutritional and other postoperative management of neonates with short bowel syndrome correlates with clinical outcomes. J Pediatr 2001; 139: Dodge ME, Bertolo RF, Brunton JA. Enteral feeding induces early intestinal adaptation in a parenterally fed neonatal piglet model of short bowel syndrome. JPEN J Parenter Enteral Nutr 2012; 36: Gosselin KB, Duggan C. Enteral nutrition in the management of pediatric intestinal failure. J Pediatr 2014; 165: Buchman AL, Moukarzel AA, Bhuta S, et al. Parenteral nutrition is associated with intestinal morphologic and functional changes in humans. JPEN J Parenter Enteral Nutr 1995; 19: Rege A. The Surgical approach to short bowel syndrome autologous reconstruction versus transplantation. Viszeralmedizin 2014; 30(3): Walker SR, Nucci A, Yaworski JA, Barksdale EM. The Bianchi procedure: a 20-year single institution experience. J PediatrSurg 2006; 41: G. Frongia, M. Kessler, S. Weih, A. Nickkholgh, A. Mehrabi, S. Holland-Cunz. Comparison of LILT and STEP procedures in children with short bowel syndrome a systematic review of the literature 73. T.R. Weber. Isoperistaltic bowel lengthening for short bowel syndrome in children. Am J Surg, 178 (1999), pp R. Figueroa-Colon, P.R. Harris, E. Birdsong, F.A. Franklin, K.E. Georgeson. Impact of intestinal lengthening on the nutritional outcome for children with short bowel syndrome. J PediatrSurg, 31 (7) (1996), pp
Morabito A UK. -Royal Manchester Children s Hospital (PABRRU) -Intestinal Failure Unit Salford Royal Hospital
 -Intestinal Failure Unit Salford Royal Hospital") NON-TRANSPLANT SURGERY IMPROVES OUTCOME IN SHORT BOWEL PATIENTS Morabito A UK -Royal Manchester Children s Hospital (PABRRU) -Intestinal Failure Unit Salford Royal Hospital antonino.morabito@cmft.nhs.uk
NON-TRANSPLANT SURGERY IMPROVES OUTCOME IN SHORT BOWEL PATIENTS Morabito A UK -Royal Manchester Children s Hospital (PABRRU) -Intestinal Failure Unit Salford Royal Hospital antonino.morabito@cmft.nhs.uk
Surgical Management of Short Bowel Syndrome
 529446PENXXX10.1177/0148607114529446Journal of Parenteral and Enteral NutritionIyer research-article2014 Invited Review Surgical Management of Short Bowel Syndrome Kishore R. Iyer, MBBS, FRCS, FACS 1 Journal
529446PENXXX10.1177/0148607114529446Journal of Parenteral and Enteral NutritionIyer research-article2014 Invited Review Surgical Management of Short Bowel Syndrome Kishore R. Iyer, MBBS, FRCS, FACS 1 Journal
Intestinal Rehabilitation and Transplantation
 Intestinal Rehabilitation and Transplantation Joel Lim, MD Associate Professor of Pediatrics Children s Mercy Hospital University of Missouri in Kansas City Objective: Intestinal Failure/Short Bowel Syndrome
Intestinal Rehabilitation and Transplantation Joel Lim, MD Associate Professor of Pediatrics Children s Mercy Hospital University of Missouri in Kansas City Objective: Intestinal Failure/Short Bowel Syndrome
Short Bowel Syndrome: Medical management
 Short Bowel Syndrome: Medical management La Sindrome dell'intestino Corto in età pediatrica Brescia 18 marzo 2011 Jon A.Vanderhoof, M.D. Division of Pediatric GI Harvard Medical School Children s Hospital,
Short Bowel Syndrome: Medical management La Sindrome dell'intestino Corto in età pediatrica Brescia 18 marzo 2011 Jon A.Vanderhoof, M.D. Division of Pediatric GI Harvard Medical School Children s Hospital,
BOWEL LENGTHENING procedures may be beneficial
 Serial Transverse Enteroplasty (STEP): A Novel Bowel Lengthening Procedure By Heung Bae Kim, Dario Fauza, Jennifer Garza, Jung-Tak Oh, Samuel Nurko, and Tom Jaksic Boston, Massachusetts Background/Purpose:
Serial Transverse Enteroplasty (STEP): A Novel Bowel Lengthening Procedure By Heung Bae Kim, Dario Fauza, Jennifer Garza, Jung-Tak Oh, Samuel Nurko, and Tom Jaksic Boston, Massachusetts Background/Purpose:
ESPEN Congress Brussels 2005 INDICATIONS FOR INTESTINAL TRANSPLANTATION. Loris Pironi
 ESPEN Congress Brussels 2005 INDICATIONS FOR INTESTINAL TRANSPLANTATION Loris Pironi 27 th ESPEN - Brussels 2005 INDICATIONS FOR INTESTINAL TRANSPLANTATION Loris Pironi Chronic Intestinal Failure Centre
ESPEN Congress Brussels 2005 INDICATIONS FOR INTESTINAL TRANSPLANTATION Loris Pironi 27 th ESPEN - Brussels 2005 INDICATIONS FOR INTESTINAL TRANSPLANTATION Loris Pironi Chronic Intestinal Failure Centre
Surgical Management and Autologous Intestinal Reconstruction in Short Bowel Syndrome
 Accepted Manuscript Surgical Management and Autologous Intestinal Reconstruction in Short Bowel Syndrome Matthijs J. Hommel, Bsc, Medical Student, Robertine van Baren, MD, Paediatric Surgeon, Jan Willem
Accepted Manuscript Surgical Management and Autologous Intestinal Reconstruction in Short Bowel Syndrome Matthijs J. Hommel, Bsc, Medical Student, Robertine van Baren, MD, Paediatric Surgeon, Jan Willem
Long term home parenteral nutrition or small bowel transplantation? Florence LACAILLE Necker-enfants malades, Paris
 Long term home parenteral nutrition or small bowel transplantation? Florence LACAILLE Necker-enfants malades, Paris Intestinal failure : definitive Ultra-short bowel : ± < 30 cm - valve ± < 20 cm + valve
Long term home parenteral nutrition or small bowel transplantation? Florence LACAILLE Necker-enfants malades, Paris Intestinal failure : definitive Ultra-short bowel : ± < 30 cm - valve ± < 20 cm + valve
Gastroschisis Sequelae and Management
 Gastroschisis Sequelae and Management Mary Finn Gillian Lieberman, MD Primary Care Radiology Beth Israel Deaconess Medical Center Harvard Medical School April 2014 Outline I. Definition and Epidemiology
Gastroschisis Sequelae and Management Mary Finn Gillian Lieberman, MD Primary Care Radiology Beth Israel Deaconess Medical Center Harvard Medical School April 2014 Outline I. Definition and Epidemiology
SHORT GUT SYNDROME (SGS) : A MANAGEMENT CHALLENGE!
 : A MANAGEMENT CHALLENGE!") SHORT GUT SYNDROME (SGS) : A MANAGEMENT CHALLENGE! Muhammad Saaiq DEPARTMENT OF SURGERY,PIMS, ISLAMABAD. Surgical Grand Round, Pakistan Institute of Medical Sciences (PIMS), Islamabad. September 23, 2005.
SHORT GUT SYNDROME (SGS) : A MANAGEMENT CHALLENGE! Muhammad Saaiq DEPARTMENT OF SURGERY,PIMS, ISLAMABAD. Surgical Grand Round, Pakistan Institute of Medical Sciences (PIMS), Islamabad. September 23, 2005.
Surgery for Intestinal Failure
 Surgery for Intestinal Failure Kishore Iyer, MBBS, FRCS (Eng), FACS Director, Adult & Pediatric Intestinal Transplantation Associate Professor of Surgery & Pediatrics Mount Sinai School of Medicine New
Surgery for Intestinal Failure Kishore Iyer, MBBS, FRCS (Eng), FACS Director, Adult & Pediatric Intestinal Transplantation Associate Professor of Surgery & Pediatrics Mount Sinai School of Medicine New
Definition and Types of Intestinal Failure
 Definition and Types of Intestinal Failure Jeremy Nightingale Consultant Gastroenterologist St Mark s Hospital Intestinal Failure - Definitions Reduction in functioning gut mass below the minimum amount
Definition and Types of Intestinal Failure Jeremy Nightingale Consultant Gastroenterologist St Mark s Hospital Intestinal Failure - Definitions Reduction in functioning gut mass below the minimum amount
LA CHIRURGIA RIABILITATIVA
 LA CHIRURGIA RIABILITATIVA SINDROME DA INTESTINO CORTO: GLI ASPETTI ETICI, L APPROCCIO MEDICO E LE ESIGENZE IN CAMPO NORMATIVO VII CONGRESSO NAZIONALE ASSOCIAZIONE A.N.A.D.P. UN FILO PER LA VITA ONLUS
LA CHIRURGIA RIABILITATIVA SINDROME DA INTESTINO CORTO: GLI ASPETTI ETICI, L APPROCCIO MEDICO E LE ESIGENZE IN CAMPO NORMATIVO VII CONGRESSO NAZIONALE ASSOCIAZIONE A.N.A.D.P. UN FILO PER LA VITA ONLUS
Nutritional Requirements in Intestinal Failure
 Nutritional Requirements in Intestinal Failure Christopher Duggan, MD, MPH Center for Nutrition Center for Advanced Intestinal Rehabilitation (CAIR) Division of Gastroenterology, Hepatology and Nutrition
Nutritional Requirements in Intestinal Failure Christopher Duggan, MD, MPH Center for Nutrition Center for Advanced Intestinal Rehabilitation (CAIR) Division of Gastroenterology, Hepatology and Nutrition
Improved survival in a multidisciplinary short bowel syndrome program
 Journal of Pediatric Surgery (2008) 43, 20 24 www.elsevier.com/locate/jpedsurg Improved survival in a multidisciplinary short bowel syndrome program Biren P. Modi a,b, Monica Langer a,b, Y. Avery Ching
Journal of Pediatric Surgery (2008) 43, 20 24 www.elsevier.com/locate/jpedsurg Improved survival in a multidisciplinary short bowel syndrome program Biren P. Modi a,b, Monica Langer a,b, Y. Avery Ching
Management of Short Bowel Syndrome in the Era of Teduglutide. Charlene Compher, PhD, RD University of Pennsylvania
 Management of Short Bowel Syndrome in the Era of Teduglutide Charlene Compher, PhD, RD University of Pennsylvania compherc@nursing.upenn.edu Disclosures Research funding for clinical trials by NPS Pharmaceuticals
Management of Short Bowel Syndrome in the Era of Teduglutide Charlene Compher, PhD, RD University of Pennsylvania compherc@nursing.upenn.edu Disclosures Research funding for clinical trials by NPS Pharmaceuticals
Nutrition Management in GI Diseases
 Nutrition Management in GI Diseases Aryono Hendarto MD Nutrition & Metabolic Diseases Division Department of Child Health Cipto Mangunkusumo Hospital University of Indonesia 1 Patient s Care 1. Drugs 2.
Nutrition Management in GI Diseases Aryono Hendarto MD Nutrition & Metabolic Diseases Division Department of Child Health Cipto Mangunkusumo Hospital University of Indonesia 1 Patient s Care 1. Drugs 2.
Nutritional Management in Enterocutaneous fistula Dr Deepak Govil
 Nutritional Management in Enterocutaneous fistula Dr Deepak Govil MS, PhD (GI Surgery) Senior Consultant Surgical Gastroenterology Indraprastha Apollo Hospital New Delhi What is enterocutaneous fistula
Nutritional Management in Enterocutaneous fistula Dr Deepak Govil MS, PhD (GI Surgery) Senior Consultant Surgical Gastroenterology Indraprastha Apollo Hospital New Delhi What is enterocutaneous fistula
Corporate Medical Policy
 Corporate Medical Policy Small Bowel, Small Bowel with Liver, or Multivisceral Transplant File Name: Origination: Last CAP Review: Next CAP Last Review: small_bowel_liver_and_multivisceral_transplant 2/1996
Corporate Medical Policy Small Bowel, Small Bowel with Liver, or Multivisceral Transplant File Name: Origination: Last CAP Review: Next CAP Last Review: small_bowel_liver_and_multivisceral_transplant 2/1996
Intestinal Obstruction Clinical Presentation & Causes
 Intestinal Obstruction Clinical Presentation & Causes V Chidambaram-Nathan Consultant Transplant and General Surgeon Sheffield Kidney Institute Northern General Hospital Intestinal Obstruction One of the
Intestinal Obstruction Clinical Presentation & Causes V Chidambaram-Nathan Consultant Transplant and General Surgeon Sheffield Kidney Institute Northern General Hospital Intestinal Obstruction One of the
Short bowel syndrome after cytoreductive surgery and HIPEC: nutritional considerations
 JBUON 2014; 19(2): 549-553 ISSN: 1107-0625, online ISSN: 2241-6293 www.jbuon.com E-mail: editorial_office@jbuon.com ORIGINAL ARTICLE Short bowel syndrome after cytoreductive surgery and HIPEC: nutritional
JBUON 2014; 19(2): 549-553 ISSN: 1107-0625, online ISSN: 2241-6293 www.jbuon.com E-mail: editorial_office@jbuon.com ORIGINAL ARTICLE Short bowel syndrome after cytoreductive surgery and HIPEC: nutritional
INTESTINAL FAILURE, REHABILITATION & TRANSPLANTATION: Indications, Techniques and Outcomes
 INTESTINAL FAILURE, REHABILITATION & TRANSPLANTATION: Indications, Techniques and Outcomes Douglas G. Farmer, MD. Professor of Surgery Director, Intestinal Transplant Program Dumont-UCLA Transplant Center
INTESTINAL FAILURE, REHABILITATION & TRANSPLANTATION: Indications, Techniques and Outcomes Douglas G. Farmer, MD. Professor of Surgery Director, Intestinal Transplant Program Dumont-UCLA Transplant Center
WHEN To Initiate Parenteral Nutrition A Frequent Question With New Answers
 WHEN To Initiate Parenteral Nutrition A Frequent Question With New Answers Ainsley Malone, MS, RD, LD, CNSC, FAND, FASPEN Dubai International Nutrition Conference 2018 Disclosures No commercial relationship
WHEN To Initiate Parenteral Nutrition A Frequent Question With New Answers Ainsley Malone, MS, RD, LD, CNSC, FAND, FASPEN Dubai International Nutrition Conference 2018 Disclosures No commercial relationship
Pathology of Intestinal Obstruction. Dr. M. Madhavan, MBBS., MD., MIAC, Professor of Pathology Saveetha Medical College
 Pathology of Intestinal Obstruction Dr. M. Madhavan, MBBS., MD., MIAC, Professor of Pathology Saveetha Medical College Pathology of Intestinal Obstruction Objectives list the causes of intestinal obstruction
Pathology of Intestinal Obstruction Dr. M. Madhavan, MBBS., MD., MIAC, Professor of Pathology Saveetha Medical College Pathology of Intestinal Obstruction Objectives list the causes of intestinal obstruction
SOUTHERN WEST MIDLANDS NEWBORN NETWORK
 SOUTHERN WEST MIDLANDS NEWBORN NETWORK Hereford, Worcester, Birmingham, Sandwell & Solihull Title : Person Responsible for Review : Management of Gastro-Intestinal Stomata In Neonates R. Wragg & G.Jawaheer
SOUTHERN WEST MIDLANDS NEWBORN NETWORK Hereford, Worcester, Birmingham, Sandwell & Solihull Title : Person Responsible for Review : Management of Gastro-Intestinal Stomata In Neonates R. Wragg & G.Jawaheer
ESPEN Congress Florence 2008
 ESPEN Congress Florence 2008 PN Guidelines presentation PN Guidelines in gastroenterology A. van Gossum (Belgium) ESPEN-Parenteral Guidelines in Gastroenterology André Van Gossum, Eduard Cabre, Xavier
ESPEN Congress Florence 2008 PN Guidelines presentation PN Guidelines in gastroenterology A. van Gossum (Belgium) ESPEN-Parenteral Guidelines in Gastroenterology André Van Gossum, Eduard Cabre, Xavier
SUSTAIN BASELINE DATA COLLECTION FORM. Revised 2/4/2014 (both pediatric and adult data elements) 1. Gestational age at birth ( weeks gestation)
 1. Gestational age at birth ( weeks gestation)") SUSTAIN BASELINE DATA COLLECTION FORM Patient Demographics Revised 2/4/2014 (both pediatric and adult data elements) Did the patient begin Home PN over 90 days ago? Yes No Date began Home PN Patient Number
SUSTAIN BASELINE DATA COLLECTION FORM Patient Demographics Revised 2/4/2014 (both pediatric and adult data elements) Did the patient begin Home PN over 90 days ago? Yes No Date began Home PN Patient Number
Isolated Liver Transplantation in Infants with End-Stage Liver Disease Due to Short Bowel Syndrome
 LIVER TRANSPLANTATION 12:1062-1066, 2006 ORIGINAL ARTICLE Isolated Liver Transplantation in Infants with End-Stage Liver Disease Due to Short Bowel Syndrome Jean F. Botha, Wendy J. Grant, Clarivet Torres,
LIVER TRANSPLANTATION 12:1062-1066, 2006 ORIGINAL ARTICLE Isolated Liver Transplantation in Infants with End-Stage Liver Disease Due to Short Bowel Syndrome Jean F. Botha, Wendy J. Grant, Clarivet Torres,
Postgastrectomy Syndromes
 Postgastrectomy Syndromes Postgastrectomy syndromes are iatrogenic conditions that may arise from partial gastrectomies, independent of whether the gastric surgery was initially performed for peptic ulcer
Postgastrectomy Syndromes Postgastrectomy syndromes are iatrogenic conditions that may arise from partial gastrectomies, independent of whether the gastric surgery was initially performed for peptic ulcer
ESPEN Congress Geneva 2014 NUTRITION IN PAEDIATRIC PATIENTS 2. Nutrition treatment in children with intestinal failure S.
 ESPEN Congress Geneva 2014 NUTRITION IN PAEDIATRIC PATIENTS 2 Nutrition treatment in children with intestinal failure S. Kolaček (HR) Nutrition treatment in children with intestinal failure - IF special
ESPEN Congress Geneva 2014 NUTRITION IN PAEDIATRIC PATIENTS 2 Nutrition treatment in children with intestinal failure S. Kolaček (HR) Nutrition treatment in children with intestinal failure - IF special
Nutritional Support outside the Hospital: Home Parenteral Nutrition (HPN) in Adult Patients Topic 19
 in Adult Patients Topic 19") Nutritional Support outside the Hospital: Home Parenteral Nutrition (HPN) in Adult Patients Topic 19 Module 19.1 Indications and outcome André Van Gossum Learning objectives: Learning about indications
Nutritional Support outside the Hospital: Home Parenteral Nutrition (HPN) in Adult Patients Topic 19 Module 19.1 Indications and outcome André Van Gossum Learning objectives: Learning about indications
Total Parenteral Nutrition and Enteral Nutrition in the Home. Original Policy Date 12:2013
 MP 1.02.01 Total Parenteral Nutrition and Enteral Nutrition in the Home Medical Policy Section Durable Medical Equipment Issue Original Policy Date Last Review Status/Date Return to Medical Policy Index
MP 1.02.01 Total Parenteral Nutrition and Enteral Nutrition in the Home Medical Policy Section Durable Medical Equipment Issue Original Policy Date Last Review Status/Date Return to Medical Policy Index
Short Bowel Syndrome and Intestinal Failure: Consensus Definitions and Overview
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2006;4:6 10 REVIEWS Short Bowel Syndrome and Intestinal Failure: Consensus Definitions and Overview STEPHEN J. D. O KEEFE,* ALAN L. BUCHMAN, THOMAS M. FISHBEIN,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2006;4:6 10 REVIEWS Short Bowel Syndrome and Intestinal Failure: Consensus Definitions and Overview STEPHEN J. D. O KEEFE,* ALAN L. BUCHMAN, THOMAS M. FISHBEIN,
Home Total Parenteral Nutrition for Adults
 Home Total Parenteral Nutrition for Adults Policy Number: Original Effective Date: MM.08.007 05/21/1999 Line(s) of Business: Current Effective Date: PPO, HMO, QUEST Integration 05/27/2016 Section: Home
Home Total Parenteral Nutrition for Adults Policy Number: Original Effective Date: MM.08.007 05/21/1999 Line(s) of Business: Current Effective Date: PPO, HMO, QUEST Integration 05/27/2016 Section: Home
Populations Interventions Comparators Outcomes Individuals: With intestinal failure and evidence of impending end-stage liver failure
 Protocol Small Bowel/Liver and Multivisceral Transplant (70305) Medical Benefit Effective Date: 07/01/14 Next Review Date: 05/18 Preauthorization Yes Review Dates: 05/09, 05/10, 05/11, 05/12, 05/13, 07/13,
Protocol Small Bowel/Liver and Multivisceral Transplant (70305) Medical Benefit Effective Date: 07/01/14 Next Review Date: 05/18 Preauthorization Yes Review Dates: 05/09, 05/10, 05/11, 05/12, 05/13, 07/13,
Department of Surgery, Aizu Central Hospital, Fukushima
 Case Reports Resection of Asynchronous Quadruple Advanced Colonic Carcinomas Followed by Reconstruction with Ileal Interposition between the Transverse Colon and Rectum Sho Mineta 1, Kimiyoshi Shimanuki
Case Reports Resection of Asynchronous Quadruple Advanced Colonic Carcinomas Followed by Reconstruction with Ileal Interposition between the Transverse Colon and Rectum Sho Mineta 1, Kimiyoshi Shimanuki
Home FAQ Archives ABP Topics NeoReviews.org My Bookmarks CME Information Help. Print this Page Add to my Bookmarks Page 3 of 10
 Welcome Kristin Ingstrup [ Logout ] SEARCH Home FAQ Archives ABP Topics NeoReviews.org My Bookmarks CME Information Help Overview Editorial Board My Learning Plan January February March May June July August
Welcome Kristin Ingstrup [ Logout ] SEARCH Home FAQ Archives ABP Topics NeoReviews.org My Bookmarks CME Information Help Overview Editorial Board My Learning Plan January February March May June July August
Nutritional Support outside the Hospital: Home Parenteral Nutrition (HPN) in Adult Patients Topic 19
 in Adult Patients Topic 19") Nutritional Support outside the Hospital: Home Parenteral Nutrition (HPN) in Adult Patients Topic 19 Module 19.1 Indications and Outcome Learning Objectives André Van Gossum Head of the Clinic of Intestinal
Nutritional Support outside the Hospital: Home Parenteral Nutrition (HPN) in Adult Patients Topic 19 Module 19.1 Indications and Outcome Learning Objectives André Van Gossum Head of the Clinic of Intestinal
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons
 General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: SMALL BOWEL 7-Nov-2016 DEVELOPED BY: Graham Cullingford,
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: SMALL BOWEL 7-Nov-2016 DEVELOPED BY: Graham Cullingford,
Abdominal Assessment
 Abdominal Assessment Mary Marian, MS,RD,CSO University of AZ, Tucson, AZ Neha Parekh, MS,RD,LD,CNSC Cleveland Clinic, Cleveland, OH Objectives: 1. Outline the steps in performing an abdominal examination.
Abdominal Assessment Mary Marian, MS,RD,CSO University of AZ, Tucson, AZ Neha Parekh, MS,RD,LD,CNSC Cleveland Clinic, Cleveland, OH Objectives: 1. Outline the steps in performing an abdominal examination.
PARENTERAL NUTRITION- ASSOCIATED LIVER DISEASE IN CHILDREN
 PARENTERAL NUTRITION- ASSOCIATED LIVER DISEASE IN CHILDREN Praveen Goday MBBS CNSC Associate Professor Pediatric Gastroenterology Medical College of Wisconsin Milwaukee, WI Parenteral Nutrition-Associated
PARENTERAL NUTRITION- ASSOCIATED LIVER DISEASE IN CHILDREN Praveen Goday MBBS CNSC Associate Professor Pediatric Gastroenterology Medical College of Wisconsin Milwaukee, WI Parenteral Nutrition-Associated
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdominal pain, enteral therapy in acute pancreatitis and, 812 Abscess(es), pancreatic, nutritional support for, 814 815 Acute Physiology and
Note: Page numbers of article titles are in boldface type. A Abdominal pain, enteral therapy in acute pancreatitis and, 812 Abscess(es), pancreatic, nutritional support for, 814 815 Acute Physiology and
Enteral and parenteral nutrition in GI failure and short bowel syndrome
 Enteral and parenteral nutrition in GI failure and short bowel syndrome Alastair Forbes University College London Intestinal failure Inadequate functional intestine to allow health to be maintained by
Enteral and parenteral nutrition in GI failure and short bowel syndrome Alastair Forbes University College London Intestinal failure Inadequate functional intestine to allow health to be maintained by
Development of pancreas and Small Intestine. ANATOMY DEPARTMENT DR.SANAA AL-AlSHAARAWY DR.ESSAM Eldin Salama
 Development of pancreas and Small Intestine ANATOMY DEPARTMENT DR.SANAA AL-AlSHAARAWY DR.ESSAM Eldin Salama OBJECTIVES At the end of the lecture, the students should be able to : Describe the development
Development of pancreas and Small Intestine ANATOMY DEPARTMENT DR.SANAA AL-AlSHAARAWY DR.ESSAM Eldin Salama OBJECTIVES At the end of the lecture, the students should be able to : Describe the development
Advances in intestinal Rehabilitation Susan Hill Gastroenterology Consultant
 Advances in intestinal Rehabilitation Susan Hill Gastroenterology Consultant 2 Indication for intravenous nutrition/pn: Intestinal Failure Inability to maintain weight and growth despite adequate enteral
Advances in intestinal Rehabilitation Susan Hill Gastroenterology Consultant 2 Indication for intravenous nutrition/pn: Intestinal Failure Inability to maintain weight and growth despite adequate enteral
Fistuloclysis (distal limb feeding) Dr Alison Culkin Research Dietitian AuSPEN 2015
 Dr Alison Culkin Research Dietitian AuSPEN 2015") Fistuloclysis (distal limb feeding) Dr Alison Culkin Research Dietitian AuSPEN 2015 Overview Consider the evidence Describe the practicalities Present some cases Fistuloclysis/distal limb feeding Infusion
Fistuloclysis (distal limb feeding) Dr Alison Culkin Research Dietitian AuSPEN 2015 Overview Consider the evidence Describe the practicalities Present some cases Fistuloclysis/distal limb feeding Infusion
Isolated Small Bowel Transplant
 Medical Policy Manual Transplant, Policy No. 09 Isolated Small Bowel Transplant Next Review: January 2019 Last Review: January 2018 Effective: March 1, 2018 IMPORTANT REMINDER Medical Policies are developed
Medical Policy Manual Transplant, Policy No. 09 Isolated Small Bowel Transplant Next Review: January 2019 Last Review: January 2018 Effective: March 1, 2018 IMPORTANT REMINDER Medical Policies are developed
Sustain Follow-up Data Collection Form (Revised 2/4/2014) (both pediatric and adult elements) (Please select) (Please select)
 (both pediatric and adult elements) (Please select) (Please select)") Patient Information Sustain Follow-up Data Collection Form (Revised 2/4/2014) (both pediatric and adult elements) Visit Date Patient Birth Date -- Gender (please select) What is the nature of this follow-up?
Patient Information Sustain Follow-up Data Collection Form (Revised 2/4/2014) (both pediatric and adult elements) Visit Date Patient Birth Date -- Gender (please select) What is the nature of this follow-up?
Who Needs Parenteral Nutrition? Is Parenteral Nutrition An Appropriate Intervention?
 Who Needs Parenteral Nutrition? 1 Is Parenteral Nutrition An Appropriate Intervention? Key questions to ask with initial consultation Can the gastrointestinal (GI) tract be utilized? Can the GI tract be
Who Needs Parenteral Nutrition? 1 Is Parenteral Nutrition An Appropriate Intervention? Key questions to ask with initial consultation Can the gastrointestinal (GI) tract be utilized? Can the GI tract be
Minimal Enteral Nutrition
 Abstract Minimal Enteral Nutrition Although parenteral nutrition has been used widely in the management of sick very low birth weight infants, a smooth transition to the enteral route is most desirable.
Abstract Minimal Enteral Nutrition Although parenteral nutrition has been used widely in the management of sick very low birth weight infants, a smooth transition to the enteral route is most desirable.
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN
 UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
Development of the Digestive System. W.S. O The University of Hong Kong
 Development of the Digestive System W.S. O The University of Hong Kong Plan for the GI system Then GI system in the abdomen first develops as a tube suspended by dorsal and ventral mesenteries. Blood
Development of the Digestive System W.S. O The University of Hong Kong Plan for the GI system Then GI system in the abdomen first develops as a tube suspended by dorsal and ventral mesenteries. Blood
Deep Enteroscopy Methods to Diagnose Small Bowel IBD
 Deep Enteroscopy Methods to Diagnose Small Bowel IBD Name: Institution: Peter Draganov University of Florida, Gainesville, FL Overview Types of enteroscopy Enteroscopy equipment Enetoscopy do and don'ts
Deep Enteroscopy Methods to Diagnose Small Bowel IBD Name: Institution: Peter Draganov University of Florida, Gainesville, FL Overview Types of enteroscopy Enteroscopy equipment Enetoscopy do and don'ts
Original Policy Date
 MP 7.03.02 Small Bowel/Liver and Multivisceral Transplant Medical Policy Section Surgery Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date Reviewed with literature search/12/2013 Return
MP 7.03.02 Small Bowel/Liver and Multivisceral Transplant Medical Policy Section Surgery Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date Reviewed with literature search/12/2013 Return
Surgical Management of IBD. Val Jefford Grand Rounds October 14, 2003
 Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Isolated Small Bowel Transplant
 Isolated Small Bowel Transplant Policy Number: Original Effective Date: MM.07.022 05/23/2001 Line(s) of Business: Current Effective Date: HMO; PPO 08/01/2013 Section: Transplants Place(s) of Service: Inpatient
Isolated Small Bowel Transplant Policy Number: Original Effective Date: MM.07.022 05/23/2001 Line(s) of Business: Current Effective Date: HMO; PPO 08/01/2013 Section: Transplants Place(s) of Service: Inpatient
STRATEGIES TO IMPROVE ENTERAL FEEDING TOLERANCE. IS IT WORTH IT? ENGELA FRANCIS RD(SA)
") STRATEGIES TO IMPROVE ENTERAL FEEDING TOLERANCE. IS IT WORTH IT? ENGELA FRANCIS RD(SA) DEFINITION OF ENTERAL FEEDING INTOLERANCE Gastrointestinal feeding intolerance are usually defined as: High gastric
STRATEGIES TO IMPROVE ENTERAL FEEDING TOLERANCE. IS IT WORTH IT? ENGELA FRANCIS RD(SA) DEFINITION OF ENTERAL FEEDING INTOLERANCE Gastrointestinal feeding intolerance are usually defined as: High gastric
PARENTERAL NUTRITION THERAPY
 UnitedHealthcare Benefits of Texas, Inc. 1. UnitedHealthcare of Oklahoma, Inc. 2. UnitedHealthcare of Oregon, Inc. UnitedHealthcare of Washington, Inc. UnitedHealthcare West BENEFIT INTERPRETATION POLICY
UnitedHealthcare Benefits of Texas, Inc. 1. UnitedHealthcare of Oklahoma, Inc. 2. UnitedHealthcare of Oregon, Inc. UnitedHealthcare of Washington, Inc. UnitedHealthcare West BENEFIT INTERPRETATION POLICY
Different Surgical Techniques in Management of Small Intestinal Atresia in High Risk Neonates
 Annals of Pediatric Surgery Vol 5, No 1, January 2009, PP 31-35 Original Article Different Surgical Techniques in Management of Small Intestinal Atresia in High Risk Neonates Almoutaz A. Eltayeb Pediatric
Annals of Pediatric Surgery Vol 5, No 1, January 2009, PP 31-35 Original Article Different Surgical Techniques in Management of Small Intestinal Atresia in High Risk Neonates Almoutaz A. Eltayeb Pediatric
DIGESTIVE SYSTEM SURGICAL PROCEDURES December 22, 2015 (effective March 1, 2016) INTESTINES (EXCEPT RECTUM) Asst Surg Anae
 INTESTINES (EXCEPT RECTUM) Asst Surg Anae") December 22, 2015 (effective March 1, 201) INTESTINES (EXCEPT RECTUM) Z513 Hydrostatic - Pneumatic dilatation of colon stricture(s) through colonoscope... 10.50 Z50 Fulguration of first polyp through colonoscope...
December 22, 2015 (effective March 1, 201) INTESTINES (EXCEPT RECTUM) Z513 Hydrostatic - Pneumatic dilatation of colon stricture(s) through colonoscope... 10.50 Z50 Fulguration of first polyp through colonoscope...
- Digestion occurs during periods of low activity - Produces more energy than it uses. - Mucosa
 Introduction Digestive System Chapter 29 Provides processes to break down molecules into a state easily used by cells - A disassembly line: Starts at the mouth and ends at the anus Digestive functions
Introduction Digestive System Chapter 29 Provides processes to break down molecules into a state easily used by cells - A disassembly line: Starts at the mouth and ends at the anus Digestive functions
Digestive System 7/15/2015. Outline Digestive System. Digestive System
 Digestive System Biology 105 Lecture 18 Chapter 15 Outline Digestive System I. Functions II. Layers of the GI tract III. Major parts: mouth, pharynx, esophagus, stomach, small intestine, large intestine,
Digestive System Biology 105 Lecture 18 Chapter 15 Outline Digestive System I. Functions II. Layers of the GI tract III. Major parts: mouth, pharynx, esophagus, stomach, small intestine, large intestine,
Midgut. Over its entire length the midgut is supplied by the superior mesenteric artery
 Gi Embryology 3 Midgut the midgut is suspended from the dorsal abdominal wall by a short mesentery and communicates with the yolk sac by way of the vitelline duct or yolk stalk Over its entire length the
Gi Embryology 3 Midgut the midgut is suspended from the dorsal abdominal wall by a short mesentery and communicates with the yolk sac by way of the vitelline duct or yolk stalk Over its entire length the
What location in the gastrointestinal (GI) tract has tight, or impermeable, junctions between the epithelial cells?
 tract has tight, or impermeable, junctions between the epithelial cells?") CASE 32 A 17-year-old boy presents to his primary care physician with complaints of diarrhea for the last 2 days. The patient states that he just returned to the United States after visiting relatives
CASE 32 A 17-year-old boy presents to his primary care physician with complaints of diarrhea for the last 2 days. The patient states that he just returned to the United States after visiting relatives
A Bariatric Patient in my Waiting Room: Choosing the Right Patient for the Right Operation: Bariatric Surgery Indications
 A Bariatric Patient in my Waiting Room: Choosing the Right Patient for the Right Operation: Bariatric Surgery Indications Shahzeer Karmali MD FRCSC FACS Associate Professor Surgery University of Alberta
A Bariatric Patient in my Waiting Room: Choosing the Right Patient for the Right Operation: Bariatric Surgery Indications Shahzeer Karmali MD FRCSC FACS Associate Professor Surgery University of Alberta
Gastroenterology. Certification Examination Blueprint. Purpose of the exam
 Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Dietary management. Dr Alison Culkin Lead Intestinal Failure Dietitian St Mark s Hospital RSM December 2017
 Dietary management Dr Alison Culkin Lead Intestinal Failure Dietitian St Mark s Hospital RSM December 2017 Overview Effect of resection on absorption Evidence for dietary management in short bowel Practicalities
Dietary management Dr Alison Culkin Lead Intestinal Failure Dietitian St Mark s Hospital RSM December 2017 Overview Effect of resection on absorption Evidence for dietary management in short bowel Practicalities
Clinical Policy: Total Parenteral Nutrition and Intradialytic Parenteral Nutrition Reference Number: CP.PHAR.205
 Clinical Policy: Reference Number: CP.PHAR.205 Effective Date: 05.16 Last Review Date: 02.18 See Important Reminder at the end of this policy for important regulatory and legal information. Coding Implications
Clinical Policy: Reference Number: CP.PHAR.205 Effective Date: 05.16 Last Review Date: 02.18 See Important Reminder at the end of this policy for important regulatory and legal information. Coding Implications
Overall Goals and Objectives for Transplant Hepatology EPAs:
 Overall Goals and Objectives for Transplant Hepatology EPAs: 1. DIAGNOSTIC LIST During the one-year Advanced Pediatric Transplant Hepatology Program, fellows are expected to develop comprehensive skills
Overall Goals and Objectives for Transplant Hepatology EPAs: 1. DIAGNOSTIC LIST During the one-year Advanced Pediatric Transplant Hepatology Program, fellows are expected to develop comprehensive skills
GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint
 Examination Blueprint") GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Gastroenterology MOC exam blueprint Based on feedback from physicians that MOC assessments
GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Gastroenterology MOC exam blueprint Based on feedback from physicians that MOC assessments
Case Discussion. Nutrition in IBD. Rémy Meier MD. Ulcerative colitis. Crohn s disease
 26.08.2017 Case Discussion Nutrition in IBD Crohn s disease Ulcerative colitis Rémy Meier MD Case Presentation 30 years old female, with diarrhea for 3 months Shool frequency 3-4 loose stools/day with
26.08.2017 Case Discussion Nutrition in IBD Crohn s disease Ulcerative colitis Rémy Meier MD Case Presentation 30 years old female, with diarrhea for 3 months Shool frequency 3-4 loose stools/day with
Parenteral Nutrition. Outline. Potential Biomarkers for Use in Intestinal Adaptation. Jejunum is primary site of digestion and absorption
 Outline Potential Biomarkers for Use in Intestinal Adaptation Kelly A. Tappenden, Ph.D., R.D. Professor of Nutrition and GI Physiology 1. Intestinal Adaptation potential regulators 2. Intestinal mucosal
Outline Potential Biomarkers for Use in Intestinal Adaptation Kelly A. Tappenden, Ph.D., R.D. Professor of Nutrition and GI Physiology 1. Intestinal Adaptation potential regulators 2. Intestinal mucosal
Strategies for preventing and treating IFALD
 Strategies for preventing and treating IFALD Dr Sue Beath The Liver Unit (including small bowel transplantation) sue.beath@nhs.net Birmingham Children s Hospital Intestinal failure associated liver disease
Strategies for preventing and treating IFALD Dr Sue Beath The Liver Unit (including small bowel transplantation) sue.beath@nhs.net Birmingham Children s Hospital Intestinal failure associated liver disease
A rare case of intestinal obstruction due to internal hernia. Dr. Jayanth 3 rd year PG Dept. Of General Surgery
 A rare case of intestinal obstruction due to internal hernia Dr. Jayanth 3 rd year PG Dept. Of General Surgery One of the common cause of acute abdomen May lead to high morbidity and mortality if not treated
A rare case of intestinal obstruction due to internal hernia Dr. Jayanth 3 rd year PG Dept. Of General Surgery One of the common cause of acute abdomen May lead to high morbidity and mortality if not treated
Medical application of transabdominal ultrasound in gastrointestinal diseases
 Medical application of transabdominal ultrasound in gastrointestinal diseases Hsiu-Po Wang Department of Emergency Medicine National Taiwan University Hospital Real-time ultrasound has become a standard
Medical application of transabdominal ultrasound in gastrointestinal diseases Hsiu-Po Wang Department of Emergency Medicine National Taiwan University Hospital Real-time ultrasound has become a standard
LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL
 SIGNIFICANCE OF EXTRALUMINAL ABDOMINAL GAS: LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL SCBT/MR 2012 October 26,
SIGNIFICANCE OF EXTRALUMINAL ABDOMINAL GAS: LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL SCBT/MR 2012 October 26,
Daniel Hirsch, MD Director of Neonatology Somerset Medical Center Assistant Professor of Pediatrics UMDNJ RWJMS
 Daniel Hirsch, MD Director of Neonatology Somerset Medical Center Assistant Professor of Pediatrics UMDNJ RWJMS Daniel Hirsch, MD Director of Neonatology Somerset Medical Center Assistant Professor of
Daniel Hirsch, MD Director of Neonatology Somerset Medical Center Assistant Professor of Pediatrics UMDNJ RWJMS Daniel Hirsch, MD Director of Neonatology Somerset Medical Center Assistant Professor of
Overview of digestion or, gut reactions - to food
 Key concepts in Digestion. Indigestion module Overview of digestion or, gut reactions - to food Prof. Barry Campbell Gastroenterology Cellular & Molecular Physiology e-mail: bjcampbl@liv.ac.uk http://pcwww.liv.ac.uk/~bjcampbl
Key concepts in Digestion. Indigestion module Overview of digestion or, gut reactions - to food Prof. Barry Campbell Gastroenterology Cellular & Molecular Physiology e-mail: bjcampbl@liv.ac.uk http://pcwww.liv.ac.uk/~bjcampbl
- Digestion occurs during periods of low activity - Produces more energy than it uses. 3 Copyright 2016 by Elsevier Inc. All rights reserved.
 Introduction Digestive System Chapter 29 Provides processes to break down molecules into a state easily used by cells - A disassembly line: Starts at the mouth and ends at the anus Digestive functions
Introduction Digestive System Chapter 29 Provides processes to break down molecules into a state easily used by cells - A disassembly line: Starts at the mouth and ends at the anus Digestive functions
Development of the Digestive System. W.S. O School of Biomedical Sciences, University of Hong Kong.
 Development of the Digestive System W.S. O School of Biomedical Sciences, University of Hong Kong. Organization of the GI tract: Foregut (abdominal part) supplied by coeliac trunk; derivatives include
Development of the Digestive System W.S. O School of Biomedical Sciences, University of Hong Kong. Organization of the GI tract: Foregut (abdominal part) supplied by coeliac trunk; derivatives include
Surgical Management of IBD in the Age of Biologics
 Surgical Management of IBD in the Age of Biologics Lisa S. Poritz, M.D Associate Professor of Surgery Division of Colon and Rectal Surgery Objectives Discuss surgical management of IBD When to operate
Surgical Management of IBD in the Age of Biologics Lisa S. Poritz, M.D Associate Professor of Surgery Division of Colon and Rectal Surgery Objectives Discuss surgical management of IBD When to operate
Outcomes from a 12-Week, Open-Label, Multicenter Clinical Trial of Teduglutide in Pediatric Short Bowel Syndrome.
 Outcomes from a 12-Week, Open-Label, Multicenter Clinical Trial of Teduglutide in Pediatric Short Bowel Syndrome. Carter BA 1, Cohran VC 2, Cole CR 3, Corkins MR 4, Dimmitt RA 5, Duggan C 6, Hill S 7,
Outcomes from a 12-Week, Open-Label, Multicenter Clinical Trial of Teduglutide in Pediatric Short Bowel Syndrome. Carter BA 1, Cohran VC 2, Cole CR 3, Corkins MR 4, Dimmitt RA 5, Duggan C 6, Hill S 7,
Clinical Improvement Following Home Parenteral Nutrition in Pediatric Patients with Intestinal Failure
 ORIGINAL ARTICLE Clinical Improvement Following Home Parenteral Nutrition in Pediatric Patients with Intestinal Failure Yi-Ching Tung, Yen-Hsuan Ni, Hong-Shiee Lai, 1 Der-Yirng Hsieh, 2 Mei-Hwei Chang*
ORIGINAL ARTICLE Clinical Improvement Following Home Parenteral Nutrition in Pediatric Patients with Intestinal Failure Yi-Ching Tung, Yen-Hsuan Ni, Hong-Shiee Lai, 1 Der-Yirng Hsieh, 2 Mei-Hwei Chang*
Mohamed EL-hemaly Gastro- intestinal surgical center, Mansoura University.
 Mohamed EL-hemaly Gastro- intestinal surgical center, Mansoura University. Chronic transmural inflammatory process of the bowel & affects any part of the gastro -intestinal tract from the mouth to the
Mohamed EL-hemaly Gastro- intestinal surgical center, Mansoura University. Chronic transmural inflammatory process of the bowel & affects any part of the gastro -intestinal tract from the mouth to the
LOUISIANA MEDICAID PROGRAM ISSUED:
 37.12 TOTAL PARENTERAL NUTRITION Overview Introduction In This Section This Section explains the LMPBM program s Total Parenteral Nutrition (TPN) therapy coverage, limitations, prior authorization, reimbursement
37.12 TOTAL PARENTERAL NUTRITION Overview Introduction In This Section This Section explains the LMPBM program s Total Parenteral Nutrition (TPN) therapy coverage, limitations, prior authorization, reimbursement
A Multi center Randomized Trial of Laparotomy vs. Drainage
 A Multi center Randomized Trial of Laparotomy vs. Drainage as the Initial Surgical Therapy for ELBW Infants with Necrotizing Enterocolitis (NEC) or Isolated Intestinal Perforation (IP): Outcomes at 18
A Multi center Randomized Trial of Laparotomy vs. Drainage as the Initial Surgical Therapy for ELBW Infants with Necrotizing Enterocolitis (NEC) or Isolated Intestinal Perforation (IP): Outcomes at 18
Malabsorption: etiology, pathogenesis and evaluation
 Malabsorption: etiology, pathogenesis and evaluation Peter HR Green NORMAL ABSORPTION Coordination of gastric, small intestinal, pancreatic and biliary function Multiple mechanisms Fat protein carbohydrate
Malabsorption: etiology, pathogenesis and evaluation Peter HR Green NORMAL ABSORPTION Coordination of gastric, small intestinal, pancreatic and biliary function Multiple mechanisms Fat protein carbohydrate
Small Bowel Obstruction after operation in a severely malnourished man. By: Ms Bounmark Phoumesy
 Small Bowel Obstruction after operation in a severely malnourished man By: Ms Bounmark Phoumesy Normal length of GI tract Normal length(achieved by age 9) Small bowel 600cm (Men: 630 cm; Women: 592 cm)
Small Bowel Obstruction after operation in a severely malnourished man By: Ms Bounmark Phoumesy Normal length of GI tract Normal length(achieved by age 9) Small bowel 600cm (Men: 630 cm; Women: 592 cm)
Eosinophilic Esophagitis (EoE)
") Eosinophilic Esophagitis (EoE) 01.06.2016 EoE: immune-mediated disorder food or environmental antigens => Th2 inflammatory response. Key cytokines: IL-4, IL-5, and IL-13 stimulate the production of eotaxin-3
Eosinophilic Esophagitis (EoE) 01.06.2016 EoE: immune-mediated disorder food or environmental antigens => Th2 inflammatory response. Key cytokines: IL-4, IL-5, and IL-13 stimulate the production of eotaxin-3
Digestive System. In one end and out the other.
 Digestive System In one end and out the other. Overview Every cell in the body needs nourishment, yet most cells cannot leave their position in the body and travel to a food source, so the food must be
Digestive System In one end and out the other. Overview Every cell in the body needs nourishment, yet most cells cannot leave their position in the body and travel to a food source, so the food must be
Visceral aneurysm. Diagnosis and Interventions M.NEDEVSKA
 Visceral aneurysm Diagnosis and Interventions M.NEDEVSKA History 1953 De Bakeyand Cooley Visceral aneurysm VAAs rare, reported incidence of 0.01 to 0.2% on routine autopsies. Clinically important Potentially
Visceral aneurysm Diagnosis and Interventions M.NEDEVSKA History 1953 De Bakeyand Cooley Visceral aneurysm VAAs rare, reported incidence of 0.01 to 0.2% on routine autopsies. Clinically important Potentially
Fecal incontinence causes 196 epidemiology 8 treatment 196
 Subject Index Achalasia course 93 differential diagnosis 93 esophageal dysphagia 92 95 etiology 92, 93 treatment 93 95 work-up 93 Aminosalicylates, pharmacokinetics and aging effects 36 Antibiotics diarrhea
Subject Index Achalasia course 93 differential diagnosis 93 esophageal dysphagia 92 95 etiology 92, 93 treatment 93 95 work-up 93 Aminosalicylates, pharmacokinetics and aging effects 36 Antibiotics diarrhea
Current concepts in Critical Care Nutrition
 Current concepts in Critical Care Nutrition Dr.N.Ramakrishnan AB (Int Med), AB (Crit Care), MMM, FACP, FCCP, FCCM Director, Critical Care Services Apollo Hospitals, Chennai Objectives Why? Enteral or Parenteral
Current concepts in Critical Care Nutrition Dr.N.Ramakrishnan AB (Int Med), AB (Crit Care), MMM, FACP, FCCP, FCCM Director, Critical Care Services Apollo Hospitals, Chennai Objectives Why? Enteral or Parenteral
Bariatric Surgery: How complex is this? Pradeep Pallati, MD, FACS, FASMBS
 Bariatric Surgery: How complex is this? Pradeep Pallati, MD, FACS, FASMBS Nothing to Disclose Types of Bariatric Surgery Restrictive Malabsorptive Combination Restrictive and Malabsorptive Newer Endoluminal
Bariatric Surgery: How complex is this? Pradeep Pallati, MD, FACS, FASMBS Nothing to Disclose Types of Bariatric Surgery Restrictive Malabsorptive Combination Restrictive and Malabsorptive Newer Endoluminal
Overview of digestion or, gut reactions - to food
 1 Key concepts in Digestion. Indigestion module Overview of digestion or, gut reactions to food Prof. Barry Campbell Gastroenterology Cellular & Molecular Physiology email: bjcampbl@liv.ac.uk http://pcwww.liv.ac.uk/~bjcampbl
1 Key concepts in Digestion. Indigestion module Overview of digestion or, gut reactions to food Prof. Barry Campbell Gastroenterology Cellular & Molecular Physiology email: bjcampbl@liv.ac.uk http://pcwww.liv.ac.uk/~bjcampbl
Isolated Small Bowel Transplant. Populations Interventions Comparators Outcomes Individuals: With intestinal failure
 Protocol Isolated Small Bowel Transplant (70304) Medical Benefit Effective Date: 01/01/15 Next Review Date: 03/19 Preauthorization Yes Review Dates: 01/10, 01/11, 01/12, 01/13, 01/14, 11/14, 11/15, 11/16,
Protocol Isolated Small Bowel Transplant (70304) Medical Benefit Effective Date: 01/01/15 Next Review Date: 03/19 Preauthorization Yes Review Dates: 01/10, 01/11, 01/12, 01/13, 01/14, 11/14, 11/15, 11/16,
TPN Discontinuation Post Bowel Resection. Clinical Case Study by: Cody Steiner MSU Dietetic Intern
 TPN Discontinuation Post Bowel Resection Clinical Case Study by: Cody Steiner MSU Dietetic Intern Overview Examine patient post reconstructive surgery Review patients outcome Determine best practice for
TPN Discontinuation Post Bowel Resection Clinical Case Study by: Cody Steiner MSU Dietetic Intern Overview Examine patient post reconstructive surgery Review patients outcome Determine best practice for
Parenteral Nutrition in IBD: Any indication?
 Parenteral Nutrition in IBD: Any indication? Name: Institution: Marianna Arvanitakis Erasme University Hospital, Brussels, Belgium Clinical case 42 year old male Crohn s disease since he was 16 years old
Parenteral Nutrition in IBD: Any indication? Name: Institution: Marianna Arvanitakis Erasme University Hospital, Brussels, Belgium Clinical case 42 year old male Crohn s disease since he was 16 years old