SCI EXAM & FUNCTIONAL PROGNOSIS
|
|
|
- Carmella Whitehead
- 6 years ago
- Views:
Transcription
1 SCI EXAM & FUNCTIONAL PROGNOSIS MARCH 20, 2015 JUAN L ASANZA, MD STAFF PHYSICIAN VA PUGET SOUND HEALTH CARE SYSTEM SPINAL CORD INJURY UNIVERSITY OF WASHINGTON PHYSICAL MEDICINE & REHABILITATION OBJECTIVES Anatomy review ASIA Impairment Scale & SCI Examination Functional prognosis and outcomes Clinical Syndromes Clinical cases and examples Disclosures: none FACTS & FIGURES Annual incidence: 40 cases per million population in the US 12,000 new cases per year Prevalence estimated ~275K persons Average age at injury: 42.6 years 80.7% male 76.8% Caucasian 36.5% MVC >> 28.5% Falls >> 14.3% Violence Incomplete tetraplegia 40.6% >> Incomplete paraplegia 18.7% >> Complete paraplegia 18.0% >> Complete tetraplegia 11.6% Estimated lifetime costs: $ million ANATOMY: SPINE Cervical: C1-C7 Thoracic: T1-T12 Lumbar: L1-L5 Sacral: S1-S5 (fused) Coccyx SCI MODEL SYSTEMS FACTS & FIGURES

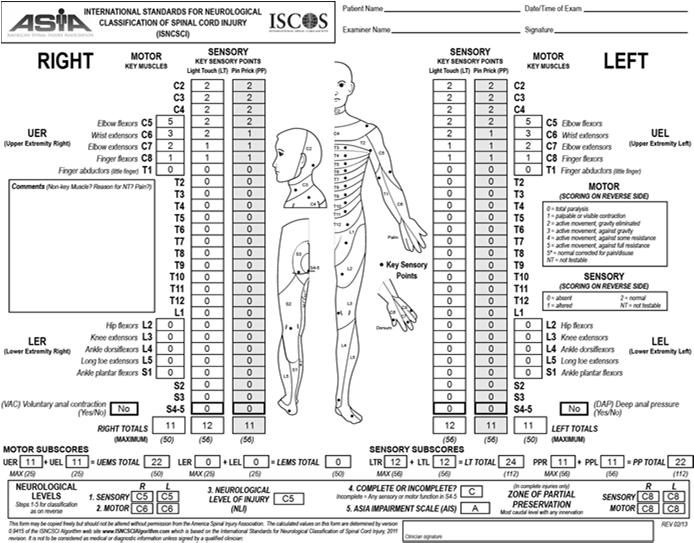
 or Asia Impairment Scale (AIS) - Motor exam (key muscles) - graded 0-5 - 5 key muscles in each extremity")
2 ANATOMY: SPINE Spinal cord: foramen magnum to L1-L2 intervertebral level Conus medullaris and Cauda equina Cord enlargements: C5-T1 and L1-S2 31 pairs of nerve roots: Cervical 8 Thoracic 12 Lumbar 5 Sacral 5 Coccygeal Cord segments do not always correspond to vertebral levels GOALS OF SCI EXAMINATION To provide an assessment tool that would: Standardize patient testing and classification Establish a common language for all clinicians Improve sensitivity to patient changes over time (improvement or deterioration) Prescribe treatment Evaluate outcomes Allow for prognostication Best exam at72 hours SPINAL CORD INJURY EXAMINATION The American Spinal Injury Association (ASIA) or Asia Impairment Scale (AIS) - Motor exam (key muscles) - graded key muscles in each extremity (20 total) - Sensory exam (key sensory points) - graded 0 (absent), 1 (impaired) or 2 (normal) - pinprick and light touch - Sacral testing (S4-5) - voluntary anal contraction - DAP: deep anal pressure/sensation 2

3 KEY MUSCLES/MYOTOMES Upper extremity: C5: elbow flexors C6: wrist extensors C7: elbow extensors C8: finger flexors T1: small finger abductors Total motor score is 100 (5 points for each muscle) Lower extremity: L2: hip flexors L3: knee extensors L4: ankle dorsiflexors L5: long toe extensors S1: ankle plantarflexors MUSCLE INNERVATION All of the key muscles have innervation by two nerve segments. A muscle has a strength of 3/5, it is considered to be innervated by the more rostral segment. Biceps: C5- C6 WE: C6- C7 Triceps: C7- C8 ASIA INTERNATIONAL STANDARDS 2011 Positions for Strength Testing C5 Elbow flexed at 90 deg, arm at patient s side & forearm supinated (EF) C6 Wrist in full extension (WE) C7 Shoulder is neutral rotation, adducted and in 90 deg of flexion with elbow in 45 deg of flexion (EE) C8 Full flexed position of the distal phalanx with the proximal finger joints stabilized in extended position (FDP, digit 3) T1 Full abducted position (ADM) 3
4 ASIA INTERNATIONAL STANDARDS 2011 L2 Hip flexed to 90 deg (HF) L3 Knee flexed to 15 deg (KE) L4 Full dorsiflexed position (AD) L5 First toe fully extended (EHL) S1 Hip in neutral rotation, the knee is fully extended and the ankle in full plantarflexion (AP) MOTOR SCORING 6 point scale: 0 = absent contraction/ total paralysis 1 = palpable or visible muscle contraction without joint movement 2 = full active range of motion in the gravity eliminated plane 3 = full range of motion against gravity 4 = full ROM against moderate resistance 5 = (normal) full ROM against full resistance NT = not testable Only whole numbers: no + or - Use * if other limiting factor MOTOR LEVEL The motor level is the lowest muscle with a strength of at least 3/5, with the key muscles above it having full or normal (5/5) strength. Clarification for the myotomes that are not tested as part of key muscle groups: C1-C4 (above C5) T2 through L1 S2-S4/5 (below S1) The motor level is considered to be the same as the sensory level SACRAL TESTING (S4-5) Testing for: voluntary anal contraction Assess motor sparing (B vs. C) perianal sensation to light touch and pinprick bilaterally DAP: deep anal pressure Determines if injury is complete or incomplete = sacral sparing 4

 2 = intact (same as face) Notes Light touch is tested with cotton wisp Pin point is tested with a disposable safety pin In testing pin")
5 SENSORY (DERMATOMAL) TESTING Testing of a key point in each of the 28 dermatomes on both sides of the body. No C1 dermatome S4-S5 tested together At each dermatome, testing modalities for light touch and sharp/dull discrimination. SENSORY TESTING Demonstrate normal touch on face/cheek Stroke each dermatome region once lightly and briefly across 1cm of skin Three Point Scale for light touch and pinprick 0 = absent 1 = impaired (partial or altered appreciation, including hyperesthesia) 2 = intact (same as face) Notes Light touch is tested with cotton wisp Pin point is tested with a disposable safety pin In testing pin sensation (sharp), the inability to distinguish between the head and the point is graded as 0 (absent). The sensory level is the last (most caudal) level with normal (2/2) sensation for both light touch and pin prick sensation, and will all normal rostral dermatomes. ASIA IMPAIRMENT SCALE CLASSIFICATION Record motor level bilaterally Record sensory level bilaterally Record sacral (S4-5) results Neurological Level of Injury The most caudal (lowest) level with normal motor and sensory function Single neurological level box added to bottom of ASIA sheet (new) Determine final ASIA Impairment Scale classification 5
6 ASIA IMPAIRMENT SCALE CLASSIFICATION Terminology Paraplegia = loss of motor and/or sensory function in thoracic, lumbar, or sacral (but not cervical) segments Tetraplegia = loss of motor and/or sensory function in cervical segments Preferred over quadriplegia (mixes Latin and Greek word roots) Complete Injury = complete absence of sensory and motor function in the lowest sacral segment (S4/5) Incomplete Injury = presence of at least partial sensory or motor function in the lowest sacral segment (S4/5) ASIA IMPAIRMENT SCALE CLASSIFICATION AIS A = complete injury AIS B = incomplete injury Partial or complete sensory preservation (S4/5) No motor function (more than 3 segments) below motor level AIS C = incomplete injury Partial or complete sensory preservation (S4/5), plus Motor function more than 3 segments below motor level Majority (>50% of key muscles) below injury level < 3/5 AIS D = incomplete injury Partial or complete sensory preservation (S4/5), plus Motor function more than 3 segments below motor level Majority (>50% of key muscles) below injury level >/= 3/5 AIS E = sensory and motor function returned to full function following SCI ASIA IMPAIRMENT SCALE CLASSIFICATION Use motor level to distinguish between B and C Use neurologic injury level to distinguish between C and D Use non-key muscle groups to determine sensory vs. motor incomplete status B vs. C or D ZPP = zone of partial preservation Only in complete injuries = AIS A Motor = segments below the motor level that have partial sparing of strength Sensory = segments below the sensory level that have partial sparing of sensation Record for each side, R and L If there is no sparing of motor or sensory function below the motor or sensory levels, the levels themselves are documented in the boxes on the worksheet ASIA A with sensory & motor level of T6 with no other sparing The ZPP recorded is T6 ASIA IMPAIRMENT SCALE CLASSIFICATION Can you be a motor incomplete if there is no VAC? AIS C vs D To be motor incomplete (AIS C & D): need to be sensory incomplete with motor sparing more than 3 levels below the motor level on that side, OR have VAC *Do not need VAC if meet the criteria of motor sparing 3 levels below the motor level For AIS D, need to have motor sparing of > 3/5 in at least 50% of muscles below the NLI. JUNE 2011 REVISIONS 6
 ASIA INTERNATIONAL STANDARDS 2011 Changes have been made to be")
7 AIS EXAM HISTORY SUMMARY JUNE 2011 REVISIONS Frankel Classification ASIA Standards 1982 Revision 1989 ASIA Impairment Scale 1992 Revisions 1996 Revisions 2000 Reprinting in 2002, 2006, 2008 Revisions June th edition of the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) ASIA INTERNATIONAL STANDARDS 2011 Changes have been made to be consistent with the InSTeP training program. A 6-module course enabling clinicians to perform accurate and consistent neurological examinations. Available on the ASIA Learning Center website 2011 Reference Manual is currently available Next revision?may 2015 Pediatric considerations: WeeSteP ASIA INTERNATIONAL STANDARDS 2011 Limitations Exam can change over time In presence of other disorders (plexus, peripheral neuropathy, diabetes, etc.) may be unable to have accurate results Does not test all muscle groups that impact function Does not test all sensory modalities (i.e. proprioception, vibration, temperature) 7
 Determination that if sensation is abnormal at C2, the level that should be designated as C1.")

8 ASIA WORKSHEET CHANGES KEY POINTS Use motor level to distinguish between B and C Use NLI to distinguish between C and D Use non-key muscle groups to determine sensory vs. motor incomplete status (B vs. C) Determination that if sensation is abnormal at C2, the level that should be designated as C1. While further study is required, it was felt that this would allow for consistency amongst clinicians. In patients who have light touch or pin prick sensation at S4-5, examination for DAP is not required as the patient already has a designation for a sensory incomplete injury, although this is still recommended to complete the worksheet. The rectal examination is still required however, to test for motor sparing (i.e. voluntary anal sphincter contraction). 8
9 FACTORS IMPACTING PROGNOSIS FUNCTIONAL OUTCOMES BY AIS CATEGORY Initial mechanism of injury Cord transection & Hemorrhage >> worse GSW & bilateral facet dislocation >> worse Edema & contusion>> better Spinal stenosis & unilateral facet dislocation >> better Neurological classification Incomplete injury >> better Pin sensory sparing >> better Presence of motor function below NLI.>> better Medical co-morbidities Patient motivation Support system Availability of resources and services SCI sequela Admit AIS (72hr) A B (light touch) B (pin prick) C AIS D (at 1 year) 0-5% 20-25% 40-50% 60-75% WHITENECK ET AL FUNCTIONAL OUTCOMES BY AIS CATEGORY Most patients ~80% with complete injury recover 1 motor level For muscle grade of 0/5: 25-50% will be at 3/5 in one year % will be at 1 or 2/5 in one year For muscle grade of 1 or 2/5: 90% will be at 3/5 in one year Greatest rate of change in first 6-9 months. Incomplete injury: recovery up to 2 years FUNCTIONAL OUTCOMES BY AIS LEVEL C1 C3: PWC, ECU, Ventilator, phrenic nerve stimulator C4: may need CPAP or BiPAP for nocturnal hypoventilation C1-C4: dependent for self-care and transfers C5: some ADLs with setup, i.e. feeding, dependent for transfers C6: tenodesis/grasp, more ADLs, i.e. upper body, feeding, assist with transfers and bed mobility, MWC for short distances *C7: I with most ADLs and mobility, MWC, transfers, dressing, driving Can live independently C8 T1: bowel/bladder independence, improved grasp and dexterity, PWC or MWC, I with bed mobility and transfers, I for ADLs WHITENECK ET AL
10 FUNCTIONAL OUTCOMES BY AIS LEVEL T2 L1: MWC, abdominal strength beginning at T6, improved sitting balance, standing with bracing, some ambulation with KAFO and walker (energy consumption) L2 L3+: ambulation >> least restrictive device +/- orthotics Community ambulators AMBULATION Age Spasticity Balance Proprioception (at least hip and ankle) LE muscle strength Need bilateral hip flexor strength (at least one >/= 3/5) + Unilateral knee extensor >/= 3/5 Bracing 1 long leg brace (KAFO) + 1 short leg brace (AFO) AMBULATION Prognosis for community ambulation at 1 yr based on exam 30 days post injury (LEMS at 1 month) Complete tetraplegia Incomplete tetraplegia Complete paraplegia Incomplete paraplegia % NA NA NA 21% 63% 100% 45% 100% 33% 70% 100% 100% AMBULATION Ambulating at discharge from acute rehab AIS A < 1% AIS B 1-15% AIS C 28-40% AIS D 67-75% T12 level and above, do not expect community or household ambulation L2 and below, best prognosis for community ambulation Pinprick sensory preservation better prognosis for ambulation WATERS ET AL. 1992, 1994, 1998 KAY ET AL. 2007, BURNS ET AL
 Axonal regeneration (12-18 months) CENTRAL CORD SYNDROME PICTURE Most common of spinal cord syndromes Cervical")

11 MECHANISMS FOR NEURO RECOVERY Remyelination neuropraxia (0-3 months) Hypertrophy of innervated muscles (3-6 months) Peripheral sprouting from intact nerves to denervated muscles (3-6 months) Axonal regeneration (12-18 months) CENTRAL CORD SYNDROME PICTURE Most common of spinal cord syndromes Cervical injury to central part of cord Hyperextension Older patient, spondylosis, cervical stenosis Osteophytic spine, Spondylosis Arm weakness > leg weakness Walking Quad Person in a Barrel Sacral sparing Bladder and bowel dysfunction >> good prognosis Ambulation >> good prognosis 30-86% return to I ambulation 11




12 BROWN-SEQUARD SYNDROME Cord hemisection injury Ipsilateral loss of motor and proprioception Contralateral loss of pain and temperature sensitivity crossing of pain and temperature fibers at spinal cord level Usually penetrating injury, i.e. stabbing, GSW Favorable prognosis for ambulation, ADL independence, and bowel/bladder ANTERIOR CORD SYNDROME Anterior distribution cord injury Vascular etiology Anterior spinal artery: anterior 2/3 of spinal cord AAA repair Variable loss of motor and sensory function Proprioception & vibration preserved Poor prognosis for motor recovery POSTERIOR CORD SYNDROME Posterior spinal artery to posterior columns Loss of proprioception, deep touch, and vibration Temperature/pain less affected Sparing of motor CONUS MEDULLARIS Spinal level, skeletal injuries T10 L2 Lesions affecting lower sacral segments of spinal cord S1 S5 Rare Usually complete injury Bowel, bladder, and sexual dysfunction Lower motor neuron injury Saddle anesthesia Poor prognosis 12

13 CAUDA EQUINA SYNDROME Lumbo-sacral nerve root injury: L2 and caudal Pain BLE polyradicular distribution No spinal cord involvement Usually incomplete injury Asymmetric Motor weakness Areflexic bowel and bladder Better prognosis QUESTION 1 26yo M status post diving accident with cervical spine trauma. AIS exam performed and sensory level is C4. The elbow flexors are graded as R 4 and L 3. The motor level would be: C4 C5 C6 Cannot Determine QUESTION 1 C5: Motor strength at C5 on both sides is > 3 with the corresponding muscle function above it considered normal; presumably if there were a C4 key muscle to test, it would be graded as normal since the sensation at C4 is intact. 13
14 QUESTION 2 45yo M status post MVA with sensory level of C2. The C5 key muscles are 4/5. What is the motor level? C2 C3 C4 C5 QUESTION 2 C2: The presumed motor levels at C3 and C4 are not considered normal (since the C3 and C4 sensory dermatomes are not normal), and the rule of all levels rostral needing to be intact is not met. QUESTION 3 37yo F status post skiing accident with sensory level of T12. Her arm strength is 5/5 bilaterally. Deep anal pressure sensation is present. Her leg strength is: Right Left L2 1 2 L3 3 2 L4 0 0 L5 0 0 S1 0 0 What is the motor level? QUESTION 3 T12: Muscle strength in UE key muscles is 5/5 Sensory level is T12, AIS B Note: how to grade the motor level when in the intervening levels, there is no key muscle group. Rule: defer to the sensory level Note: how to label AIS B vs C Rule: need to have motor sparing more than 3 levels below the motor level 14
15 QUESTION 4 Which AIS classification level includes a Zone of Partial Preservation (ZPP)? AIS A AIS B AIS C AIS D Both AIS C and D All of the above QUESTION 4 ZPP = zone of partial preservation only in complete injuries = AIS A Motor = segments below the motor level that have partial sparing of strength Sensory = segments below the sensory level that have partial sparing of sensation Record for each side, R and L If there is no sparing of motor or sensory function below the motor or sensory levels, the levels themselves are documented in the boxes on the worksheet ASIA A with sensory & motor level of T6 with no other sparing The ZPP recorded is T6 QUESTION 5 A person with C5 AIS A spinal cord injury should eventually become independent in which of the following: - Intermittent catheterization - Transfer to level surfaces - Feeding -Bathing QUESTION 5 A person with C5 AIS A spinal cord injury should eventually become independent in feeding, and in UE dressing with assistive devices, in driving a power wheelchair, and in propelling a manual wheelchair short distances on level surfaces. 15

16 EXAMPLE 1 EXAMPLE 2 16

17 EXAMPLE 3 EXAMPLE 4 17
18 EXAMPLE 5 EXAMPLE 6 18
.")
19 EXAMPLE 7 NOTE If there is a sensory deficit in C5-T1, with no motor deficit, the rule (confirmed by ASIA committee) is that the motor level as T1 on that side. This reflects that you defer to the sensory for motor level where there is no myotome (i.e. at C2-4, T2-L1, S3-5). The problem in this case is that it would be misleading to say either the R motor level is C7 (because that muscle is fine) or that it s L3 (because the spinal cord has been altered at C8, as demonstrated by the altered sensation). So the solution is a bit of a compromise you say the motor level is the last place where you are absolutely certain about motor function T1. This situation would be different if the deficit in C8 right was pre-existing or for some reason not due to SCI (noted as 1*) then it would be L3. RESOURCES AND REFERENCES earch Education.htm
20 20
3/3/2016. International Standards for the Neurologic Classification of Spinal Cord Injury (ISNCSCI)
") International Standards for the Neurologic Classification of Spinal Cord Injury (ISNCSCI) American Spinal Injury Association International Spinal Cord Society Presented by Adam Stein, MD Chairman and Professor
International Standards for the Neurologic Classification of Spinal Cord Injury (ISNCSCI) American Spinal Injury Association International Spinal Cord Society Presented by Adam Stein, MD Chairman and Professor
SPINAL CORD INJURY-GSW
 SPINAL CORD INJURY-GSW Wayne Cheng, MD Bones and Spine 1 EPIDEMIOLOGY-mechanism Most common cause of traumatic cord inj.: #1 MVA (45%) #2 Fall (22%) #3 Violence (16%) #4 Sports (13%) After 1990, Gsw now
SPINAL CORD INJURY-GSW Wayne Cheng, MD Bones and Spine 1 EPIDEMIOLOGY-mechanism Most common cause of traumatic cord inj.: #1 MVA (45%) #2 Fall (22%) #3 Violence (16%) #4 Sports (13%) After 1990, Gsw now
Sir William Asher ANATOMY
 SPINAL CORD INJURY BASICS RELATED TO LIFE CARE PLANNING Lesson 1 Sir William Asher Picture the pathetic patient lying long abed, the urine leaking from his distended bladder, the lime draining from his
SPINAL CORD INJURY BASICS RELATED TO LIFE CARE PLANNING Lesson 1 Sir William Asher Picture the pathetic patient lying long abed, the urine leaking from his distended bladder, the lime draining from his
Slide 1. Slide 2. Slide 3. Introduction CHAPTER 10:CLIENTS WITH SPINAL CORD INJURY PART I. Introduction - page 252(pathophysiology)
") Slide 1 CHAPTER 10:CLIENTS WITH SPINAL CORD INJURY PART I PT 151 Slide 2 Introduction - page 252(pathophysiology) Traumatic SCI occurs when an external force, such as fracture of the vertebrae or penetration
Slide 1 CHAPTER 10:CLIENTS WITH SPINAL CORD INJURY PART I PT 151 Slide 2 Introduction - page 252(pathophysiology) Traumatic SCI occurs when an external force, such as fracture of the vertebrae or penetration
Definition of Complete Spinal Cord Injury
 29 (1991) 573--581 1991 International Medical Society of Definition of Complete Spinal Cord Injury R. L. Waters, MD,i R. H. Adkins, PhD,2 J. S. Yakura, MS, PT3 1 Clinical Professor of Orthopedic Surgery,
29 (1991) 573--581 1991 International Medical Society of Definition of Complete Spinal Cord Injury R. L. Waters, MD,i R. H. Adkins, PhD,2 J. S. Yakura, MS, PT3 1 Clinical Professor of Orthopedic Surgery,
[ Toolkit For ] Neurology Assessment
![[ Toolkit For ] Neurology Assessment](/thumbs/80/80759512.jpg "[ Toolkit For ] Neurology Assessment") [ Toolkit For ] Neurology Assessment International Standard for Neurological Classification of Spinal Cord Injury (ISNCSCI) Assessment: Rationale and Tips for Completion. February 2016 Version 2.0 TOOLKIT
[ Toolkit For ] Neurology Assessment International Standard for Neurological Classification of Spinal Cord Injury (ISNCSCI) Assessment: Rationale and Tips for Completion. February 2016 Version 2.0 TOOLKIT
Gary Rea MD PhD Medical Director OSU Comprehensive Spine Center
 Gary Rea MD PhD Medical Director OSU Comprehensive Spine Center 1. The less specific the patient is about symptoms and pain, the less likely a specific diagnosis will be made and the less likely the patient
Gary Rea MD PhD Medical Director OSU Comprehensive Spine Center 1. The less specific the patient is about symptoms and pain, the less likely a specific diagnosis will be made and the less likely the patient
ORTHOPEDIC PHYSIOTHERAPY EVALUATION FORM. Age: Gender: M/F IP/OP
 ORTHOPEDIC PHYSIOTHERAPY EVALUATION FORM NAME: DATE: Age: Gender: M/F IP/OP Occupation: Referred by: Address: Phone Number: Registration Number: Civil Status: Diagnosis: Chief Complaints: Past Medical
ORTHOPEDIC PHYSIOTHERAPY EVALUATION FORM NAME: DATE: Age: Gender: M/F IP/OP Occupation: Referred by: Address: Phone Number: Registration Number: Civil Status: Diagnosis: Chief Complaints: Past Medical
Chapter 13: The Spinal Cord and Spinal Nerves
 Chapter 13: The Spinal Cord and Spinal Nerves Spinal Cord Anatomy Protective structures: Vertebral column and the meninges protect the spinal cord and provide physical stability. a. Dura mater, b. Arachnoid,
Chapter 13: The Spinal Cord and Spinal Nerves Spinal Cord Anatomy Protective structures: Vertebral column and the meninges protect the spinal cord and provide physical stability. a. Dura mater, b. Arachnoid,
Chapter 13. The Spinal Cord & Spinal Nerves. Spinal Cord. Spinal Cord Protection. Meninges. Together with brain forms the CNS Functions
 Spinal Cord Chapter 13 The Spinal Cord & Spinal Nerves Together with brain forms the CNS Functions spinal cord reflexes integration (summation of inhibitory and excitatory) nerve impulses highway for upward
Spinal Cord Chapter 13 The Spinal Cord & Spinal Nerves Together with brain forms the CNS Functions spinal cord reflexes integration (summation of inhibitory and excitatory) nerve impulses highway for upward
Spine Trauma- Part B
 Spine Trauma- Part B Cervical Spine Injuries Atlanto- Occipital Dislocation Hyperextension and distraction mechanism Down s syndrome, RA more susceptible Asymmetric lateral masses on odontoid view Widened
Spine Trauma- Part B Cervical Spine Injuries Atlanto- Occipital Dislocation Hyperextension and distraction mechanism Down s syndrome, RA more susceptible Asymmetric lateral masses on odontoid view Widened
Spinal Cord Injuries: The Basics. Kadre Sneddon POS Rounds October 1, 2003
 Spinal Cord Injuries: The Basics Kadre Sneddon POS Rounds October 1, 2003 Anatomy Dorsal columntouch, vibration Corticospinal tract- UMN Anterior horn-lmn Spinothalamic tractpain, temperature (contralateral)
Spinal Cord Injuries: The Basics Kadre Sneddon POS Rounds October 1, 2003 Anatomy Dorsal columntouch, vibration Corticospinal tract- UMN Anterior horn-lmn Spinothalamic tractpain, temperature (contralateral)
Slide 1. Slide 2. Slide 3. Intro to Physical Therapy for Neuromuscular Conditions. PT Evaluation. PT Evaluation
 Slide 1 Intro to Physical Therapy for Neuromuscular Conditions PTA 103 Introduction to Clinical Practice 2 Slide 2 Mental status: consciousness, attention, orientation, cognition Communication: speech
Slide 1 Intro to Physical Therapy for Neuromuscular Conditions PTA 103 Introduction to Clinical Practice 2 Slide 2 Mental status: consciousness, attention, orientation, cognition Communication: speech
RECIPES FOR RATINGS !!! A. FIBROMYALGIA: 0% WPI P. 569 B. THORACIC OUTLET SYNDROME 0% WPI P. 569 C. MYOFASCIAL PAIN SYNDROME 0% WPI P.
 RECIPES FOR RATINGS 1. THE "0% WPI" RATINGS A. FIBROMYALGIA: 0% WPI P. 569 B. THORACIC OUTLET SYNDROME 0% WPI P. 569 C. MYOFASCIAL PAIN SYNDROME 0% WPI P. 569 D. TENDINITIS OF UPPER EXTREMITY 0% WPI P.
RECIPES FOR RATINGS 1. THE "0% WPI" RATINGS A. FIBROMYALGIA: 0% WPI P. 569 B. THORACIC OUTLET SYNDROME 0% WPI P. 569 C. MYOFASCIAL PAIN SYNDROME 0% WPI P. 569 D. TENDINITIS OF UPPER EXTREMITY 0% WPI P.
Case Report: CASE REPORT OF FACET ARTHROPATHY INDUCED NERVE ROOT COMPRESSION RESULTING IN MOTOR WEAKNESS AND PAIN
 Cox Technic Case Report #100 published at www.coxtechnic.com (sent October 2011 on 10/11/11 ) 1 Case Report: CASE REPORT OF FACET ARTHROPATHY INDUCED NERVE ROOT COMPRESSION RESULTING IN MOTOR WEAKNESS
Cox Technic Case Report #100 published at www.coxtechnic.com (sent October 2011 on 10/11/11 ) 1 Case Report: CASE REPORT OF FACET ARTHROPATHY INDUCED NERVE ROOT COMPRESSION RESULTING IN MOTOR WEAKNESS
A comparison of two patients with Guillain-Barre Syndrome J O H N C O R S I N O, S P T
 A comparison of two patients with Guillain-Barre Syndrome J O H N C O R S I N O, S P T Guillain-Barre Acute inflammatory demyelinating polyneuropathy Highly diverse presentation, course, outcome Miller-Fisher:
A comparison of two patients with Guillain-Barre Syndrome J O H N C O R S I N O, S P T Guillain-Barre Acute inflammatory demyelinating polyneuropathy Highly diverse presentation, course, outcome Miller-Fisher:
Note: Please refer to handout Spinal Plexuses and Representative Spinal Nerves for
 Chapter 13 Outline Note: Please refer to handout Spinal Plexuses and Representative Spinal Nerves for what you need to know from Exhibits 13.1 13.4 I. INTRODUCTION A. The spinal cord and spinal nerves
Chapter 13 Outline Note: Please refer to handout Spinal Plexuses and Representative Spinal Nerves for what you need to know from Exhibits 13.1 13.4 I. INTRODUCTION A. The spinal cord and spinal nerves
Neurologic improvement after thoracic, thoracolumbar, and lumbar spinal cord (conus medullaris) injuries
 injuries") Thomas Jefferson University Jefferson Digital Commons Department of Orthopaedic Surgery Faculty Papers Department of Orthopaedic Surgery 1-2011 Neurologic improvement after thoracic, thoracolumbar, and
Thomas Jefferson University Jefferson Digital Commons Department of Orthopaedic Surgery Faculty Papers Department of Orthopaedic Surgery 1-2011 Neurologic improvement after thoracic, thoracolumbar, and
Optimizing Functional Outcomes for Patients with Spinal Cord and Other Neurological Injuries
 Optimizing Functional Outcomes for Patients with Spinal Cord and Other Neurological Injuries Amanda Dailey, PT, DPT, NCS Stephanie Burns, OTR/L Objectives 1. Understand the roles of physical and occupational
Optimizing Functional Outcomes for Patients with Spinal Cord and Other Neurological Injuries Amanda Dailey, PT, DPT, NCS Stephanie Burns, OTR/L Objectives 1. Understand the roles of physical and occupational
Year 2004 Paper one: Questions supplied by Megan
 QUESTION 47 A 58yo man is noted to have a right foot drop three days following a right total hip replacement. On examination there is weakness of right ankle dorsiflexion and toe extension (grade 4/5).
QUESTION 47 A 58yo man is noted to have a right foot drop three days following a right total hip replacement. On examination there is weakness of right ankle dorsiflexion and toe extension (grade 4/5).
1. Spinal cord injury mild flexion-extension whiplash ~ complete transection with permanent quadriplegia
 Wk 5. Management of Clients with Neurologic Trauma 1. Spinal cord injury mild flexion-extension whiplash ~ complete transection with permanent quadriplegia most common in cervical, lower thoracic-upper
Wk 5. Management of Clients with Neurologic Trauma 1. Spinal cord injury mild flexion-extension whiplash ~ complete transection with permanent quadriplegia most common in cervical, lower thoracic-upper
Outline. Introduction / Epidemiology. Anatomy / Pain generators. Diagnosis. Treatment. Most Important lecture!!
 Acute Low Back Pain Outline Introduction / Epidemiology. Most Important lecture!! Anatomy / Pain generators Diagnosis Treatment Course Objectives Know the RED FLAGS in history taking. Know the Pain Generators
Acute Low Back Pain Outline Introduction / Epidemiology. Most Important lecture!! Anatomy / Pain generators Diagnosis Treatment Course Objectives Know the RED FLAGS in history taking. Know the Pain Generators
Algorithm #1 Lumbo-Pelvic Region Examination
 Red Screen for Potentially Serious Conditions (i.e., Red Flags) including Neurologic when indicated Positive Findings Algorithm #1 Lumbo-Pelvic Region Clinical Prediction Rule Screening: Duration of symptoms
Red Screen for Potentially Serious Conditions (i.e., Red Flags) including Neurologic when indicated Positive Findings Algorithm #1 Lumbo-Pelvic Region Clinical Prediction Rule Screening: Duration of symptoms
Anatomy of the Spinal Cord
 Spinal Cord Anatomy of the Spinal Cord Anatomy of the Spinal Cord Posterior spinal arteries Lateral corticospinal tract Dorsal column Spinothalamic tract Anterior spinal artery Anterior white commissure
Spinal Cord Anatomy of the Spinal Cord Anatomy of the Spinal Cord Posterior spinal arteries Lateral corticospinal tract Dorsal column Spinothalamic tract Anterior spinal artery Anterior white commissure
Clinical Information for Wheeled Mobility Page 1 of 6
 Clinical Information for Wheeled Mobility Page 1 of 6 PART A: PATIENT / PROVIDER INFORMATION - Please Print Name: Sponsor Soc. Sec. No: Address: City: St: Zip: Phone: ( ) Age: Sex: Height: Weight: Date
Clinical Information for Wheeled Mobility Page 1 of 6 PART A: PATIENT / PROVIDER INFORMATION - Please Print Name: Sponsor Soc. Sec. No: Address: City: St: Zip: Phone: ( ) Age: Sex: Height: Weight: Date
MULTIPLE CHOICE. Choose the one alternative that best completes the statement or answers the question.
 EPC Ch 24 Quiz w-key Name MULTIPLE CHOICE. Choose the one alternative that best completes the statement or answers the question. 1) Which of the following best explains the presentation and prognosis of
EPC Ch 24 Quiz w-key Name MULTIPLE CHOICE. Choose the one alternative that best completes the statement or answers the question. 1) Which of the following best explains the presentation and prognosis of
Human Anatomy and Physiology I Laboratory Spinal and Peripheral Nerves and Reflexes
 Human Anatomy and Physiology I Laboratory Spinal and Peripheral Nerves and Reflexes 1 This lab involves the second section of the exercise Spinal Cord, Spinal Nerves, and the Autonomic Nervous System,
Human Anatomy and Physiology I Laboratory Spinal and Peripheral Nerves and Reflexes 1 This lab involves the second section of the exercise Spinal Cord, Spinal Nerves, and the Autonomic Nervous System,
Thoracic and Lumbar Spine Fractures and Dislocations: Assessment and Classification
 Thoracic and Lumbar Spine Fractures and Dislocations: Assessment and Classification Mark L Prasarn MD University of Texas Dept of Orthopaedic Surgery Houston, Texas Updated 7/2016 Anatomy of the Spine
Thoracic and Lumbar Spine Fractures and Dislocations: Assessment and Classification Mark L Prasarn MD University of Texas Dept of Orthopaedic Surgery Houston, Texas Updated 7/2016 Anatomy of the Spine
Spinal Cord Protection. Chapter 13 The Spinal Cord & Spinal Nerves. External Anatomy of Spinal Cord. Structures Covering the Spinal Cord
 Spinal Cord Protection Chapter 13 The Spinal Cord & Spinal Nerves We are only going to cover Pages 420-434 and 447 Together with brain forms the CNS Functions spinal cord reflexes integration (summation
Spinal Cord Protection Chapter 13 The Spinal Cord & Spinal Nerves We are only going to cover Pages 420-434 and 447 Together with brain forms the CNS Functions spinal cord reflexes integration (summation
High Yield Neurological Examination
 High Yield Neurological Examination Vanja Douglas, MD Sara & Evan Williams Foundation Endowed Neurohospitalist Chair Director, Neurohospitalist Division Associate Professor of Clinical Neurology UCSF Department
High Yield Neurological Examination Vanja Douglas, MD Sara & Evan Williams Foundation Endowed Neurohospitalist Chair Director, Neurohospitalist Division Associate Professor of Clinical Neurology UCSF Department
The Upper Limb III. The Brachial Plexus. Anatomy RHS 241 Lecture 12 Dr. Einas Al-Eisa
 The Upper Limb III The Brachial Plexus Anatomy RHS 241 Lecture 12 Dr. Einas Al-Eisa Brachial plexus Network of nerves supplying the upper limb Compression of the plexus results in motor & sensory changes
The Upper Limb III The Brachial Plexus Anatomy RHS 241 Lecture 12 Dr. Einas Al-Eisa Brachial plexus Network of nerves supplying the upper limb Compression of the plexus results in motor & sensory changes
Neuro Exam Workshop. AAO Convocation, 2018 Drew Lewis, DO, FAAO, FAOCPMR Associate Professor, OMM Department Des Moines University
 Neuro Exam Workshop AAO Convocation, 2018 Drew Lewis, DO, FAAO, FAOCPMR Associate Professor, OMM Department Des Moines University Table of Contents I. Neuro Exam Screen... 2 A. Inspection... 2 B. Reflexes...
Neuro Exam Workshop AAO Convocation, 2018 Drew Lewis, DO, FAAO, FAOCPMR Associate Professor, OMM Department Des Moines University Table of Contents I. Neuro Exam Screen... 2 A. Inspection... 2 B. Reflexes...
The Spinal Cord & Spinal Nerves
 The Spinal Cord & Spinal Nerves Together with brain forms the CNS Functions spinal cord reflexes integration (summation of inhibitory and excitatory) nerve impulses highway for upward and downward travel
The Spinal Cord & Spinal Nerves Together with brain forms the CNS Functions spinal cord reflexes integration (summation of inhibitory and excitatory) nerve impulses highway for upward and downward travel
Common fracture & dislocation of the cervical spine. Theerachai Apivatthakakul Department of Orthopaedic Chiangmai University
 Common fracture & dislocation of the cervical spine Theerachai Apivatthakakul Department of Orthopaedic Chiangmai University Objective Anatomy Mechanism and type of injury PE.and radiographic evaluation
Common fracture & dislocation of the cervical spine Theerachai Apivatthakakul Department of Orthopaedic Chiangmai University Objective Anatomy Mechanism and type of injury PE.and radiographic evaluation
Case Studies, Impairment of the Spine in Washington State
 Case Studies, Impairment of the Spine in Washington State NAOEM at Skamania, 2015 25 Sep, 2015 Tim Gilmore, MD Several Slides from this Presentation Borrowed with permission from the Washington State Department
Case Studies, Impairment of the Spine in Washington State NAOEM at Skamania, 2015 25 Sep, 2015 Tim Gilmore, MD Several Slides from this Presentation Borrowed with permission from the Washington State Department
1-Apley scratch test.
 1-Apley scratch test. The patient attempts to touch the opposite scapula to test range of motion of the shoulder. 1-Testing abduction and external rotation( +ve sign touch the opposite scapula, -ve sign
1-Apley scratch test. The patient attempts to touch the opposite scapula to test range of motion of the shoulder. 1-Testing abduction and external rotation( +ve sign touch the opposite scapula, -ve sign
Spinal Column. Anatomy Of The Spine
 Anatomy Of The Spine The spine is a flexible column, composed of a stack of individual bones. Each bone is called a vertebra. There are seven vertebrae in the neck (cervical vertebrae) twelve in the thoracic
Anatomy Of The Spine The spine is a flexible column, composed of a stack of individual bones. Each bone is called a vertebra. There are seven vertebrae in the neck (cervical vertebrae) twelve in the thoracic
General Procedure and Rules
 General Procedure and Rules PROCEDURE Description: This assessment is a measure of upper extremity (UE) and lower extremity (LE) motor and sensory impairment. Equipment: A chair, bedside table, reflex
General Procedure and Rules PROCEDURE Description: This assessment is a measure of upper extremity (UE) and lower extremity (LE) motor and sensory impairment. Equipment: A chair, bedside table, reflex
Spinal Cord Organization. January 12, 2011
 Spinal Cord Organization January 12, 2011 Spinal Cord 31 segments terminates at L1-L2 special components - conus medullaris - cauda equina no input from the face Spinal Cord, Roots & Nerves Dorsal root
Spinal Cord Organization January 12, 2011 Spinal Cord 31 segments terminates at L1-L2 special components - conus medullaris - cauda equina no input from the face Spinal Cord, Roots & Nerves Dorsal root
HIGH LEVEL - Science
 Learning Outcomes HIGH LEVEL - Science Describe the structure and function of the back and spine (8a) Outline the functional anatomy and physiology of the spinal cord and peripheral nerves (8a) Describe
Learning Outcomes HIGH LEVEL - Science Describe the structure and function of the back and spine (8a) Outline the functional anatomy and physiology of the spinal cord and peripheral nerves (8a) Describe
An Illustrated Guide For Peripheral Nerve Examination. Bedside Teaching for 2 nd year medical Students
 An Illustrated Guide For Peripheral Nerve Examination Bedside Teaching for 2 nd year medical Students Prepared by: Dr. Farid Ghalli Clinical Teacher (Hon) November 2016 Before Examination : Wash hands
An Illustrated Guide For Peripheral Nerve Examination Bedside Teaching for 2 nd year medical Students Prepared by: Dr. Farid Ghalli Clinical Teacher (Hon) November 2016 Before Examination : Wash hands
Spinal Trauma. General Rehabilitation of Patient with Spinal Trauma. Common Spinal Injuries. Important Anatomical Structures at each Vertebral Level
 Asian Association for Dynamic Osteosynthesis Workshop on Management of Spinal Trauma 22 April 2007 (Sunday) Orthopaedic Learning Centre, PWH, Shatin, Hong Kong General Rehabilitation of Patient with Spinal
Asian Association for Dynamic Osteosynthesis Workshop on Management of Spinal Trauma 22 April 2007 (Sunday) Orthopaedic Learning Centre, PWH, Shatin, Hong Kong General Rehabilitation of Patient with Spinal
Nervous System: Spinal Cord and Spinal Nerves (Chapter 13)
") Nervous System: Spinal Cord and Spinal Nerves (Chapter 13) Lecture Materials for Amy Warenda Czura, Ph.D. Suffolk County Community College Eastern Campus Primary Sources for figures and content: Marieb,
Nervous System: Spinal Cord and Spinal Nerves (Chapter 13) Lecture Materials for Amy Warenda Czura, Ph.D. Suffolk County Community College Eastern Campus Primary Sources for figures and content: Marieb,
PNS and ANS Flashcards
 1. Name several SOMATIC SENSES Light touch (being touched by a feather), heat, cold, vibration, pressure, pain are SOMATIC SENSES. 2. What are proprioceptors; and how is proprioception tested? PROPRIOCEPTORS
1. Name several SOMATIC SENSES Light touch (being touched by a feather), heat, cold, vibration, pressure, pain are SOMATIC SENSES. 2. What are proprioceptors; and how is proprioception tested? PROPRIOCEPTORS
A Structural Service Plan: Towards Better and Safer Spine Surgeries. Department of Orthopaedics & Traumatology Tuen Mun Hospital
 A Structural Service Plan: Towards Better and Safer Spine Surgeries Department of Orthopaedics & Traumatology Tuen Mun Hospital Cheung KK Wong CY Chan Andrew Tse Alfred Chow YY Department of Orthopaedics
A Structural Service Plan: Towards Better and Safer Spine Surgeries Department of Orthopaedics & Traumatology Tuen Mun Hospital Cheung KK Wong CY Chan Andrew Tse Alfred Chow YY Department of Orthopaedics
A Hypothesis Driven Approach to the Neurological Exam
 A Hypothesis Driven Approach to the Neurological Exam Vanja Douglas, MD Assistant Clinical Professor UCSF Department of Neurology Disclosures None 1 Purpose of Neuro Exam Screen asymptomatic patients Screen
A Hypothesis Driven Approach to the Neurological Exam Vanja Douglas, MD Assistant Clinical Professor UCSF Department of Neurology Disclosures None 1 Purpose of Neuro Exam Screen asymptomatic patients Screen
How to Think like a Neurologist Review of Exam Process and Assessment Findings
 Lehigh Valley Health Network LVHN Scholarly Works Neurology Update for the Non-Neurologist 2013 Neurology Update for the Non-Neurologist Feb 20th, 5:10 PM - 5:40 PM How to Think like a Neurologist Review
Lehigh Valley Health Network LVHN Scholarly Works Neurology Update for the Non-Neurologist 2013 Neurology Update for the Non-Neurologist Feb 20th, 5:10 PM - 5:40 PM How to Think like a Neurologist Review
Slide 1. Slide 2 Disclosure. Slide 3 Objectives. Functional Mobility and Activities of Daily Living: Assessing and Treating Patients in Rehabilitation
 Slide 1 Functional Mobility and Activities of Daily Living: Assessing and Treating Patients in Rehabilitation Terry Carolan, MSPT, NCS Slide 2 Disclosure Terry Carolan has no industry disclosures to make
Slide 1 Functional Mobility and Activities of Daily Living: Assessing and Treating Patients in Rehabilitation Terry Carolan, MSPT, NCS Slide 2 Disclosure Terry Carolan has no industry disclosures to make
Lab # 2: Spinal Cord & Nerves, Reflexes and General Senses. A & P II Spring, 2014
 Lab # 2: Spinal Cord & Nerves, Reflexes and General Senses A & P II Spring, 2014 Objectives Be able to identify specified spinal cord structures and spinal nerves on models Be familiar with spinal nerve
Lab # 2: Spinal Cord & Nerves, Reflexes and General Senses A & P II Spring, 2014 Objectives Be able to identify specified spinal cord structures and spinal nerves on models Be familiar with spinal nerve
Year 2 MBChB Clinical Skills Session Examination of the Motor System
 Year 2 MBChB Clinical Skills Session Examination of the Motor System Reviewed & ratified by: o o o o Dr D Smith Consultant Neurologist Dr R Davies Consultant Neurologist Dr B Michael Neurology Clinical
Year 2 MBChB Clinical Skills Session Examination of the Motor System Reviewed & ratified by: o o o o Dr D Smith Consultant Neurologist Dr R Davies Consultant Neurologist Dr B Michael Neurology Clinical
Surgery. Conus medullaris and Cauda Equina Syndromes. Anatomy. See online here
 Surgery Conus medullaris and Cauda Equina Syndromes See online here Conus medullaris and cauda equina syndromes are spinal cord injuries that involve injury to the lumbosacral segment of the spinal cord.
Surgery Conus medullaris and Cauda Equina Syndromes See online here Conus medullaris and cauda equina syndromes are spinal cord injuries that involve injury to the lumbosacral segment of the spinal cord.
Motor, Reflex, Coordination and Sensory Screening Examination
 Motor, Reflex, Coordination and Sensory Screening Examination K. Jeffrey Miller, DC, DABCO Miller 2002 2002-2012 K Jeffrey Miller DC DABCO Motor Function Neurological Testing Handedness Right or Left Handed
Motor, Reflex, Coordination and Sensory Screening Examination K. Jeffrey Miller, DC, DABCO Miller 2002 2002-2012 K Jeffrey Miller DC DABCO Motor Function Neurological Testing Handedness Right or Left Handed
Anatomy. Anatomy deals with the structure of the human body, and includes a precise language on body positions and relationships between body parts.
 Anatomy deals with the structure of the human body, and includes a precise language on body positions and relationships between body parts. Proper instruction on safe and efficient exercise technique requires
Anatomy deals with the structure of the human body, and includes a precise language on body positions and relationships between body parts. Proper instruction on safe and efficient exercise technique requires
Spinal Cord Injury Robert Morgan, MD
 Spinal Cord Injury Robert Morgan, MD Original Author: Mitch Harris, MD; March 2004 New Author: Michael J. Vives, MD; Revised January 2006 Updated Author: Robert Morgan, MD; Revised November 2010 Overview
Spinal Cord Injury Robert Morgan, MD Original Author: Mitch Harris, MD; March 2004 New Author: Michael J. Vives, MD; Revised January 2006 Updated Author: Robert Morgan, MD; Revised November 2010 Overview
Normal development & reflex
 Normal development & reflex Definition of Development : acquisition & refinement of skills 1 대근육운동발달 2 소근육운동발달 3 대인관계및사회성발달 4 적응능력혹은비언어성발달 5 의사소통및언어발달 6 학습, 청각, 시각의발달 Department of Rehabilitation Medicine,
Normal development & reflex Definition of Development : acquisition & refinement of skills 1 대근육운동발달 2 소근육운동발달 3 대인관계및사회성발달 4 적응능력혹은비언어성발달 5 의사소통및언어발달 6 학습, 청각, 시각의발달 Department of Rehabilitation Medicine,
Classifications In Brief: American Spinal Injury Association (ASIA) Impairment Scale
 Impairment Scale") Clin Orthop Relat Res (2017) 475:1499 1504 DOI 10.1007/s11999-016-5133-4 Clinical Orthopaedics and Related Research A Publication of The Association of Bone and Joint Surgeons IN BRIEF Classifications
Clin Orthop Relat Res (2017) 475:1499 1504 DOI 10.1007/s11999-016-5133-4 Clinical Orthopaedics and Related Research A Publication of The Association of Bone and Joint Surgeons IN BRIEF Classifications
Chapter 12b. Overview
 Chapter 12b Spinal Cord Overview Spinal cord gross anatomy Spinal meninges Sectional anatomy Sensory pathways Motor pathways Spinal cord pathologies 1 The Adult Spinal Cord About 18 inches (45 cm) long
Chapter 12b Spinal Cord Overview Spinal cord gross anatomy Spinal meninges Sectional anatomy Sensory pathways Motor pathways Spinal cord pathologies 1 The Adult Spinal Cord About 18 inches (45 cm) long
25 Things To Know. Spine
 25 Things To Know Spine Combines Strong bones Flexible connectors Ligaments & tendons Large muscles Sensitive nerves Multi-Layer White Matter Pia Matter = thin, waterproof Arachnoid membrane (web) Dura
25 Things To Know Spine Combines Strong bones Flexible connectors Ligaments & tendons Large muscles Sensitive nerves Multi-Layer White Matter Pia Matter = thin, waterproof Arachnoid membrane (web) Dura
Spinal nerves. Aygul Shafigullina. Department of Morphology and General Pathology
 Spinal nerves Aygul Shafigullina Department of Morphology and General Pathology Spinal nerve a mixed nerve, formed in the vicinity of an intervertebral foramen, where fuse a dorsal root and a ventral root,
Spinal nerves Aygul Shafigullina Department of Morphology and General Pathology Spinal nerve a mixed nerve, formed in the vicinity of an intervertebral foramen, where fuse a dorsal root and a ventral root,
Spinal Cord Anatomy. Key Points. What is the spine? Areas of the spine: Spinal Cord Anatomy
 Spinal Cord Anatomy Authors: SCIRE Community Team Reviewed by: Riley Louie, PT Last updated: Sept 21, 2017 This page provides an overview of the structures of the spinal cord and how the spinal cord works.
Spinal Cord Anatomy Authors: SCIRE Community Team Reviewed by: Riley Louie, PT Last updated: Sept 21, 2017 This page provides an overview of the structures of the spinal cord and how the spinal cord works.
CHAPTER 13 LECTURE OUTLINE
 CHAPTER 13 LECTURE OUTLINE I. INTRODUCTION A. The spinal cord and spinal nerves mediate reactions to environmental changes. B. The spinal cord has several functions. 1. It processes reflexes. 2. It is
CHAPTER 13 LECTURE OUTLINE I. INTRODUCTION A. The spinal cord and spinal nerves mediate reactions to environmental changes. B. The spinal cord has several functions. 1. It processes reflexes. 2. It is
Module Eight. Application of Health Assessment NUR 225. Physical examination of Musculoskeletal System. King Saud University. Collage of Nursing
 King Saud University Collage of Nursing Medical Surgical Nursing depart Application of Health Assessment NUR 225 Module Eight Physical examination of Musculoskeletal System Obtaining a health history Ask
King Saud University Collage of Nursing Medical Surgical Nursing depart Application of Health Assessment NUR 225 Module Eight Physical examination of Musculoskeletal System Obtaining a health history Ask
Spinal Cord Injury Transection Injury, Spinal Shock, and Hermiated Disc. Copyright 2014, 2011, 2006 by Saunders, an imprint of Elsevier, Inc.
 Spinal Cord Injury Transection Injury, Spinal Shock, and Hermiated Disc 1 Spinal Cord Injury Results from fracture and/or dislocation of vertebrae // Compresses, stretches, or tears spinal cord Cervical
Spinal Cord Injury Transection Injury, Spinal Shock, and Hermiated Disc 1 Spinal Cord Injury Results from fracture and/or dislocation of vertebrae // Compresses, stretches, or tears spinal cord Cervical
Spinal Cord- Medulla Spinalis. Cuneyt Mirzanli Istanbul Gelisim University
 Spinal Cord- Medulla Spinalis Cuneyt Mirzanli Istanbul Gelisim University Spinal Column Supports the skull, pectoral girdle, upper limbs and thoracic cage by way of the pelvic girdle. Transmits body weight
Spinal Cord- Medulla Spinalis Cuneyt Mirzanli Istanbul Gelisim University Spinal Column Supports the skull, pectoral girdle, upper limbs and thoracic cage by way of the pelvic girdle. Transmits body weight
Spinal Cord Injury. The nerves that go from the spinal cord to the arms, legs, chest, and abdomen are called peripheral nerves.
 Spinal Cord Injury Introduction Spinal cord injuries can be very devastating. More than 10,000 Americans experience spinal cord injuries each year, mainly due to auto or falling accidents. More than 200,000
Spinal Cord Injury Introduction Spinal cord injuries can be very devastating. More than 10,000 Americans experience spinal cord injuries each year, mainly due to auto or falling accidents. More than 200,000
Cervical Spine in Baseball
 Cervical Spine in Baseball Robert G Watkins, IV, MD Co-Director, Marina Spine Center Marina del Rey, CA Vice Chief of Staff Cedars-Marina del Rey Hospital Disclosures n Pioneer / RTI Consulting, Royalties
Cervical Spine in Baseball Robert G Watkins, IV, MD Co-Director, Marina Spine Center Marina del Rey, CA Vice Chief of Staff Cedars-Marina del Rey Hospital Disclosures n Pioneer / RTI Consulting, Royalties
A test of the 1992 International Standards for Neurological and Functional Classi cation of Spinal Cord Injury
 Spinal Cord (1998) 36, 554 ± 560 1998 International Medical Society of Paraplegia All rights reserved 1362 ± 4393/98 $12.00 http://www.stockton-press.co.uk/sc A test of the 1992 International Standards
Spinal Cord (1998) 36, 554 ± 560 1998 International Medical Society of Paraplegia All rights reserved 1362 ± 4393/98 $12.00 http://www.stockton-press.co.uk/sc A test of the 1992 International Standards
Shepherd Center: A Catastrophic Care Hospital. The Jane Woodruff Pavilion
 Shepherd Center: A Catastrophic Care Hospital The Jane Woodruff Pavilion Acute Management of SCI & Prevention of Secondary Complications Joycelyn Craig, BSN, RN, CRRN SCI Nurse Education Manager FACTS
Shepherd Center: A Catastrophic Care Hospital The Jane Woodruff Pavilion Acute Management of SCI & Prevention of Secondary Complications Joycelyn Craig, BSN, RN, CRRN SCI Nurse Education Manager FACTS
Department of Neurology/Division of Anatomical Sciences
 Spinal Cord I Lecture Outline and Objectives CNS/Head and Neck Sequence TOPIC: FACULTY: THE SPINAL CORD AND SPINAL NERVES, Part I Department of Neurology/Division of Anatomical Sciences LECTURE: Monday,
Spinal Cord I Lecture Outline and Objectives CNS/Head and Neck Sequence TOPIC: FACULTY: THE SPINAL CORD AND SPINAL NERVES, Part I Department of Neurology/Division of Anatomical Sciences LECTURE: Monday,
A Syndrome (Pattern) Approach to Low Back Pain. History
 Approach to Low Back Pain. History") A Syndrome (Pattern) Approach to Low Back Pain Hamilton Hall MD FRCSC Professor, Department of Surgery, University of Toronto Medical Director, CBI Health Group Executive Director, Canadian Spine Society
A Syndrome (Pattern) Approach to Low Back Pain Hamilton Hall MD FRCSC Professor, Department of Surgery, University of Toronto Medical Director, CBI Health Group Executive Director, Canadian Spine Society
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Spine Neurosurgery Brian L. Hoh, MD 1 and Gregory J. Zipfel, MD 2 1 University of Florida, 2 Washington University Spine Neurosurgery Spine neurosurgeons treat
Introduction to Neurosurgical Subspecialties: Spine Neurosurgery Brian L. Hoh, MD 1 and Gregory J. Zipfel, MD 2 1 University of Florida, 2 Washington University Spine Neurosurgery Spine neurosurgeons treat
Spinal cord. We have extension of the pia mater below L1-L2 called filum terminale
 Spinal cord Part of the CNS extend from foramen magnum to the level of L1-L2 (it is shorter than the vertebral column) it is covered by spinal meninges. It is cylindrical in shape. It s lower end become
Spinal cord Part of the CNS extend from foramen magnum to the level of L1-L2 (it is shorter than the vertebral column) it is covered by spinal meninges. It is cylindrical in shape. It s lower end become
ICP CSF Spinal Cord Anatomy Cord Transection. Alicia A C Waite March 2nd, 2017
 ICP CSF Spinal Cord Anatomy Cord Transection Alicia A C Waite March 2nd, 2017 Monro-Kellie doctrine Intracranial volume = brain volume (85%) + blood volume (10%) + CSF volume (5%) Brain parenchyma Skull
ICP CSF Spinal Cord Anatomy Cord Transection Alicia A C Waite March 2nd, 2017 Monro-Kellie doctrine Intracranial volume = brain volume (85%) + blood volume (10%) + CSF volume (5%) Brain parenchyma Skull
Degenerative Disease of the Spine
 Degenerative Disease of the Spine Introduction: I. Anatomy Talk Overview II. Overview of Disease Processes: A. Spondylosis B. Intervertebral Disc Disease III. Diagnosis IV. Therapy Introduction: Myelopathy
Degenerative Disease of the Spine Introduction: I. Anatomy Talk Overview II. Overview of Disease Processes: A. Spondylosis B. Intervertebral Disc Disease III. Diagnosis IV. Therapy Introduction: Myelopathy
The Anatomy and Physiology of Spinal Cord Injury
 The Anatomy and Physiology of Spinal Cord Injury A Resource for Health Service Providers WA State Spinal Injury Unit Version 1 November 2013 Review Date November 2016 This document has been developed to
The Anatomy and Physiology of Spinal Cord Injury A Resource for Health Service Providers WA State Spinal Injury Unit Version 1 November 2013 Review Date November 2016 This document has been developed to
Regional Review of Musculoskeletal System: Head, Neck, and Cervical Spine Presented by Michael L. Fink, PT, DSc, SCS, OCS Pre- Chapter Case Study
 Regional Review of Musculoskeletal System: Presented by Michael L. Fink, PT, DSc, SCS, OCS (20 minutes CEU Time) Subjective A 43-year-old male, reported a sudden onset of left-sided neck and upper extremity
Regional Review of Musculoskeletal System: Presented by Michael L. Fink, PT, DSc, SCS, OCS (20 minutes CEU Time) Subjective A 43-year-old male, reported a sudden onset of left-sided neck and upper extremity
Overview. Spinal Anatomy Spaces & Meninges Spinal Cord. Anatomy of the dura. Anatomy of the arachnoid. Anatomy of the spinal meninges
 European Course in Neuroradiology Module 1 - Anatomy and Embryology Dubrovnik, October 2018 Spinal Anatomy Spaces & Meninges Spinal Cord Johan Van Goethem Overview spinal meninges & spaces spinal cord
European Course in Neuroradiology Module 1 - Anatomy and Embryology Dubrovnik, October 2018 Spinal Anatomy Spaces & Meninges Spinal Cord Johan Van Goethem Overview spinal meninges & spaces spinal cord
Traumatic Spinal Cord Injury. 39 th CANP Annual Educational Conference March 18 th, :00pm-6:15pm Carl Wherry, ACNP-bc Amanda Severson, ACNP-bc
 Traumatic Spinal Cord Injury 39 th CANP Annual Educational Conference March 18 th, 2016 5:00pm-6:15pm Carl Wherry, ACNP-bc Amanda Severson, ACNP-bc Disclosures No conflicts of interest to disclose. Introduction
Traumatic Spinal Cord Injury 39 th CANP Annual Educational Conference March 18 th, 2016 5:00pm-6:15pm Carl Wherry, ACNP-bc Amanda Severson, ACNP-bc Disclosures No conflicts of interest to disclose. Introduction
Thoracolumbar Spine Conditions: Treatment and Return to Play
 Thoracolumbar Spine Conditions: Treatment and Return to Play C H R I S T O P H E R B U R K S, MD B I E N V I L L E O R T H O P A E D I C S P E C I A L I S T S O C E A N S P R I N G S, MS Thoracolumbar
Thoracolumbar Spine Conditions: Treatment and Return to Play C H R I S T O P H E R B U R K S, MD B I E N V I L L E O R T H O P A E D I C S P E C I A L I S T S O C E A N S P R I N G S, MS Thoracolumbar
Gillian Wooldridge, DO Houston Methodist Willowbrook Hospital Primary Care Sports Medicine Fellowship May 3, 2018
 Gillian Wooldridge, DO Houston Methodist Willowbrook Hospital Primary Care Sports Medicine Fellowship May 3, 2018 Disclosures Neither I nor any family members have financial disclosures Special thanks
Gillian Wooldridge, DO Houston Methodist Willowbrook Hospital Primary Care Sports Medicine Fellowship May 3, 2018 Disclosures Neither I nor any family members have financial disclosures Special thanks
Human Anatomy. Spinal Cord and Spinal Nerves
 Human Anatomy Spinal Cord and Spinal Nerves 1 The Spinal Cord Link between the brain and the body. Exhibits some functional independence from the brain. The spinal cord and spinal nerves serve two functions:
Human Anatomy Spinal Cord and Spinal Nerves 1 The Spinal Cord Link between the brain and the body. Exhibits some functional independence from the brain. The spinal cord and spinal nerves serve two functions:
Chapter 32. Objectives. Objectives 01/09/2013. Spinal Column and Spinal Cord Trauma
 Chapter 32 Spinal Column and Spinal Cord Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1.
Chapter 32 Spinal Column and Spinal Cord Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1.
Physical Therapist Assistant Principles of Neuromuscular Rehabilitation
 Western Technical College 10524144 Physical Therapist Assistant Principles of Neuromuscular Rehabilitation Course Outcome Summary Course Information Description Career Cluster Instructional Level Total
Western Technical College 10524144 Physical Therapist Assistant Principles of Neuromuscular Rehabilitation Course Outcome Summary Course Information Description Career Cluster Instructional Level Total
Acute to Rehab Spinal Cord Injuries Anna Brown CNC, Certificate SCI Nursing, Grad Dip Rehabilitation Studies, La Trobe
 Acute to Rehab Spinal Cord Injuries Anna Brown CNC, Certificate SCI Nursing, Grad Dip Rehabilitation Studies, La Trobe Victorian Spinal Cord Service Austin Health SCI Acute to Rehab Let the rollercoaster
Acute to Rehab Spinal Cord Injuries Anna Brown CNC, Certificate SCI Nursing, Grad Dip Rehabilitation Studies, La Trobe Victorian Spinal Cord Service Austin Health SCI Acute to Rehab Let the rollercoaster
Nerves of Upper limb. Dr. Brijendra Singh Professor & Head Department of Anatomy AIIMS Rishikesh
 Nerves of Upper limb Dr. Brijendra Singh Professor & Head Department of Anatomy AIIMS Rishikesh 1 Objectives Origin, course & relation of median & ulnar nerves. Motor & sensory distribution Carpal tunnel
Nerves of Upper limb Dr. Brijendra Singh Professor & Head Department of Anatomy AIIMS Rishikesh 1 Objectives Origin, course & relation of median & ulnar nerves. Motor & sensory distribution Carpal tunnel
Spinal Cord: Clinical Applications. Dr. Stuart Inglis
 Spinal Cord: Clinical Applications Dr. Stuart Inglis Tabes dorsalis, also known as syphilitic myelopathy, is a slow degeneration (specifically, demyelination) of the nerves in the dorsal funiculus of the
Spinal Cord: Clinical Applications Dr. Stuart Inglis Tabes dorsalis, also known as syphilitic myelopathy, is a slow degeneration (specifically, demyelination) of the nerves in the dorsal funiculus of the
Restoration of Reaching and Grasping Functions in Hemiplegic Patients with Severe Arm Paralysis
 Restoration of Reaching and Grasping Functions in Hemiplegic Patients with Severe Arm Paralysis Milos R. Popovic* 1,2, Vlasta Hajek 2, Jenifer Takaki 2, AbdulKadir Bulsen 2 and Vera Zivanovic 1,2 1 Institute
Restoration of Reaching and Grasping Functions in Hemiplegic Patients with Severe Arm Paralysis Milos R. Popovic* 1,2, Vlasta Hajek 2, Jenifer Takaki 2, AbdulKadir Bulsen 2 and Vera Zivanovic 1,2 1 Institute
Restraints to Movement... 4 Restraints to flexion... 4 Primary restraint into Extension... 4
 CERVICAL SPINE... 4 Neck Pain Categories... 4 Kinematics... Error! Bookmark not defined. Ranges of Motion C2-7... 4 Coupled Movements... 4 Ranges of Motion C0-2... 4 Coupled Movements... 4 Restraints to
CERVICAL SPINE... 4 Neck Pain Categories... 4 Kinematics... Error! Bookmark not defined. Ranges of Motion C2-7... 4 Coupled Movements... 4 Ranges of Motion C0-2... 4 Coupled Movements... 4 Restraints to
Gross Anatomy of Lower Spinal Cord
 Chapter 13 Spinal Cord, Spinal Nerves and Somatic Reflexes Spinal cord Spinal nerves Somatic reflexes Gross Anatomy of Lower Spinal Cord Meninges of Vertebra & Spinal Cord Spina Bifida Congenital defect
Chapter 13 Spinal Cord, Spinal Nerves and Somatic Reflexes Spinal cord Spinal nerves Somatic reflexes Gross Anatomy of Lower Spinal Cord Meninges of Vertebra & Spinal Cord Spina Bifida Congenital defect
EVALUATION AND MANAGEMENT OF CERVICAL SPINE DISORDERS
 CERVICAL SPINE EVALUATION AND MANAGEMENT OF CERVICAL SPINE DISORDERS Gregory M Yoshida MD Supports the skull Allows movement of the head Houses the spinal cord CERVICAL SPINE Unique anatomy Upper C spine
CERVICAL SPINE EVALUATION AND MANAGEMENT OF CERVICAL SPINE DISORDERS Gregory M Yoshida MD Supports the skull Allows movement of the head Houses the spinal cord CERVICAL SPINE Unique anatomy Upper C spine
Spinal Cord and Spinal Nerves. Spinal Cord. Chapter 12
 Chapter 12 Spinal Cord and Spinal Nerves 1 Spinal Cord Extends from foramen magnum to second lumbar vertebra Segmented: Cervical, Thoracic, Lumbar & Sacral Gives rise to 31 pairs of spinal nerves Not uniform
Chapter 12 Spinal Cord and Spinal Nerves 1 Spinal Cord Extends from foramen magnum to second lumbar vertebra Segmented: Cervical, Thoracic, Lumbar & Sacral Gives rise to 31 pairs of spinal nerves Not uniform
Surgery Under Regional Anesthesia
 Surgery Under Regional Anesthesia Jean Daniel Eloy, MD Assistant Professor Residency Program Director Rutgers-New Jersey Medical School Rutgers The State University of New Jersey Peripheral Nerve Block
Surgery Under Regional Anesthesia Jean Daniel Eloy, MD Assistant Professor Residency Program Director Rutgers-New Jersey Medical School Rutgers The State University of New Jersey Peripheral Nerve Block
Post Operative Total Hip Replacement Protocol Brian J. White, MD
 Post Operative Total Hip Replacement Protocol Brian J. White, MD www.western-ortho.com The intent of this protocol is to provide guidelines for progression of rehabilitation. It is not intended to serve
Post Operative Total Hip Replacement Protocol Brian J. White, MD www.western-ortho.com The intent of this protocol is to provide guidelines for progression of rehabilitation. It is not intended to serve
Upon completion of this course, the healthcare provider should be able to:
 Trauma: Spinal Cord Injuries WWW.RN.ORG Reviewed January, 2017, Expires January, 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017 RN.ORG, S.A.,
Trauma: Spinal Cord Injuries WWW.RN.ORG Reviewed January, 2017, Expires January, 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017 RN.ORG, S.A.,
The International Standards Booklet for Neurological and Functional Classification of Spinal Cord Injury*
 Paraplegia 32 (1994) 70-80 1994 International Medical Society of Paraplegia The International Standards Booklet for Neurological and Functional Classification of Spinal Cord Injury* 1 F Ditunno lr MD,!
Paraplegia 32 (1994) 70-80 1994 International Medical Society of Paraplegia The International Standards Booklet for Neurological and Functional Classification of Spinal Cord Injury* 1 F Ditunno lr MD,!
Posterior/Direct Total Hip Arthroplasty Rehabilitation Guideline
 Posterior/Direct Total Hip Arthroplasty Rehabilitation Guideline This rehabilitation program is designed to return the individual to their activities as quickly and safely as possible. It is designed for
Posterior/Direct Total Hip Arthroplasty Rehabilitation Guideline This rehabilitation program is designed to return the individual to their activities as quickly and safely as possible. It is designed for
Chiropractic Glossary
 Chiropractic Glossary Anatomy Articulation: A joint formed where two or more bones in the body meet. Your foot bone, for example, forms an articulation with your leg bone. You call that articulation an
Chiropractic Glossary Anatomy Articulation: A joint formed where two or more bones in the body meet. Your foot bone, for example, forms an articulation with your leg bone. You call that articulation an
Chapter 32. Injuries to the Spine by Pearson Education, Inc. Upper Saddle River, New Jersey
 Chapter Injuries to the Spine Topics Anatomy and physiology of the spine Spinal injuries Guidelines for immobilization Special considerations Enrichment Introduction Injuries to the spine are among the
Chapter Injuries to the Spine Topics Anatomy and physiology of the spine Spinal injuries Guidelines for immobilization Special considerations Enrichment Introduction Injuries to the spine are among the
Yoga Anatomy & Physiology
 Yoga Anatomy & Physiology Anatomy & Physiology Anatomy- One of the basic essential sciences of medicine that studies the structure of an organism. Physiology- The biological study of the functions of living
Yoga Anatomy & Physiology Anatomy & Physiology Anatomy- One of the basic essential sciences of medicine that studies the structure of an organism. Physiology- The biological study of the functions of living
Pilates for Chronic Low Back Pain
 Pilates for Chronic Low Back Pain Julianne Bettencourt March 23, 2015 Course Year: 2014 Integrated Fitness, Visalia, CA Abstract Low back pain is an injury that affects thousands of people every day and
Pilates for Chronic Low Back Pain Julianne Bettencourt March 23, 2015 Course Year: 2014 Integrated Fitness, Visalia, CA Abstract Low back pain is an injury that affects thousands of people every day and