BRACHIAL PLEXUS INJURY INVESTIGATION, LOCALIZATION AND TREATMENT. Presented By : Dr.Pankaj Jain
|
|
|
- Jeffrey Daniels
- 6 years ago
- Views:
Transcription
1 BRACHIAL PLEXUS INJURY INVESTIGATION, LOCALIZATION AND TREATMENT Presented By : Dr.Pankaj Jain
2 EMBRYOLOGY l Brachial plexus (BP) is developed at 5 weeks of gestation l Afferent fibers develop from neuroblast located alongside neural tube l Efferent fibers originate from neuroblast in the basal plate of tube from where they grow outside l Afferent and efferent fibers join to form the nerve
3 l Nerves divide into anterior and posterior divisions l There are connections between these nerves in the brachial plexus
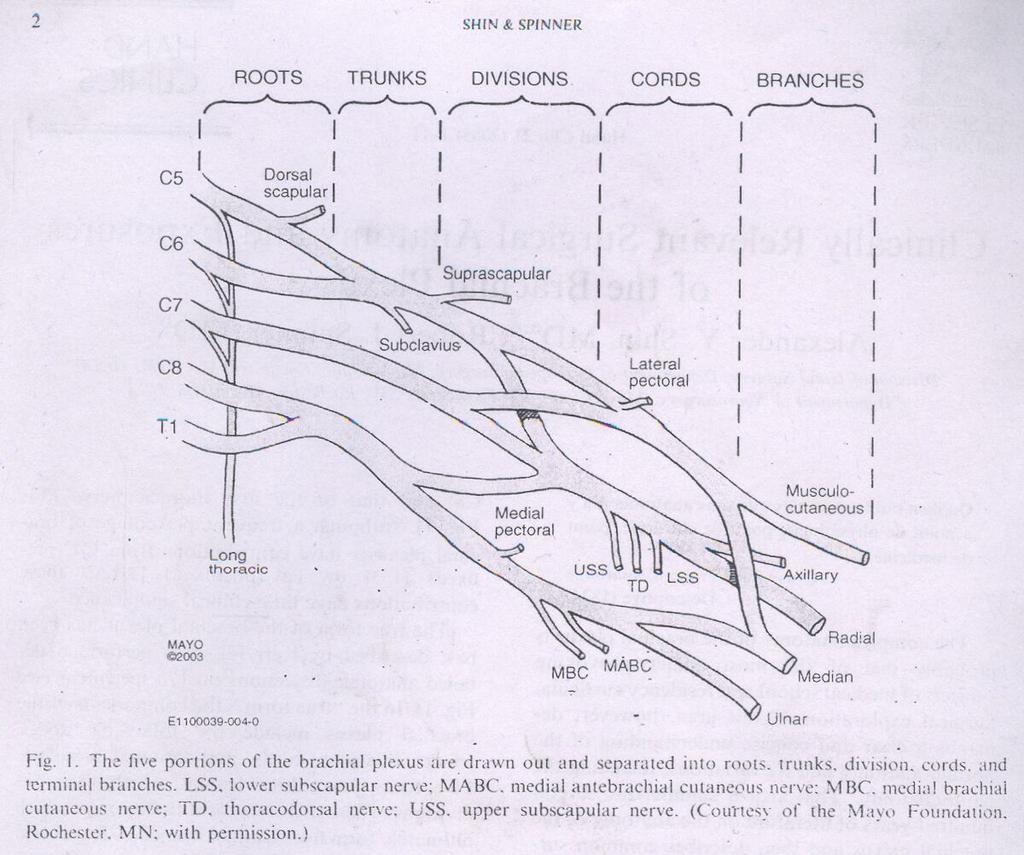
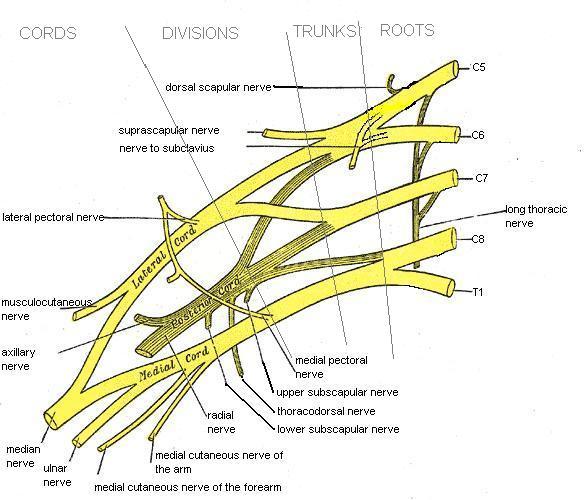
4 Anatomy
5
6 Anatomy l Formed by ventral primary rami of lower four cervical and first thoracic nerve root. l Frequently have contributions from C4(prefixed) or T2(post-fixed).

7 PREFIXED BRACHIAL PLEXUS
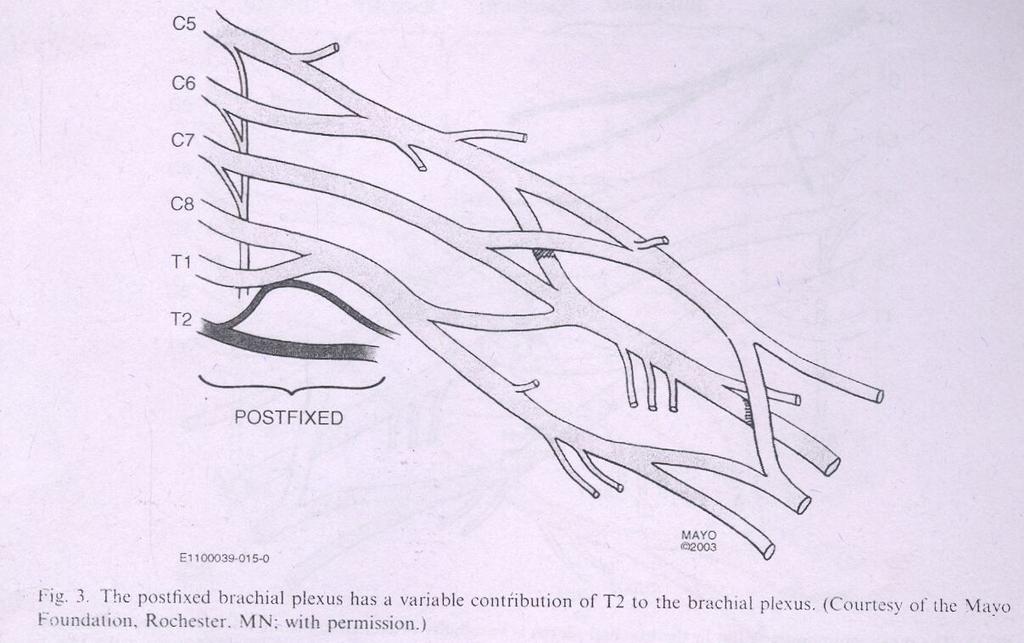
8 Post-fixed plexus

9 RELATIONS OF BRACHIAL PLEXUS
10 Levels l Roots l Trunks l Divisions l Cords l Branches l Real l Athletic Trainers l Drink l Cold l Beer
11 l C5 and C6 roots form upper trunk l C8 and T1 roots the lower trunk l C7 forms the middle trunk l Joining point of C5-C6 roots is ERB S POINT l Each trunk divides into an anterior and a posterior division and passes beneath the clavicle
12 l All 3 posterior divisions merge to form the posterior cord l Anterior division of the upper and middle trunk merge to form the lateral cord l Anterior division of lower trunk forms the medial cord
13 l Lateral cord splits into 2 terminal branches: a) Musculocutaneous nerve b) Lateral cord contribution to median nerve (sensory) l Posterior cord splits into a)axillary nerve and b)radial nerve l Medial cord gives off a) medial cord contribution to the median nerve(motor) and b)ulnar nerve
14 l There are few terminal branches of the roots trunks and cords. l ROOTS: a)dorsal scapular nerve b) branch to phrenic nerve c)long thoracic nerve l TRUNKS: a)nerve to subclavius b) suprascapular nerve l CORDS: a) Lateral cord gives lateral pectoral nerve b)posterior cord gives upper subscapular,lower subscapular and thoracodorsal nerve.
15 l Medial cord gives medial pectoral, medial cut. nerve of arm and forearm.
16 Variations l Found in around 50% l Most commonly pre-fixed(28-62%) and post-fixed(16-73%)
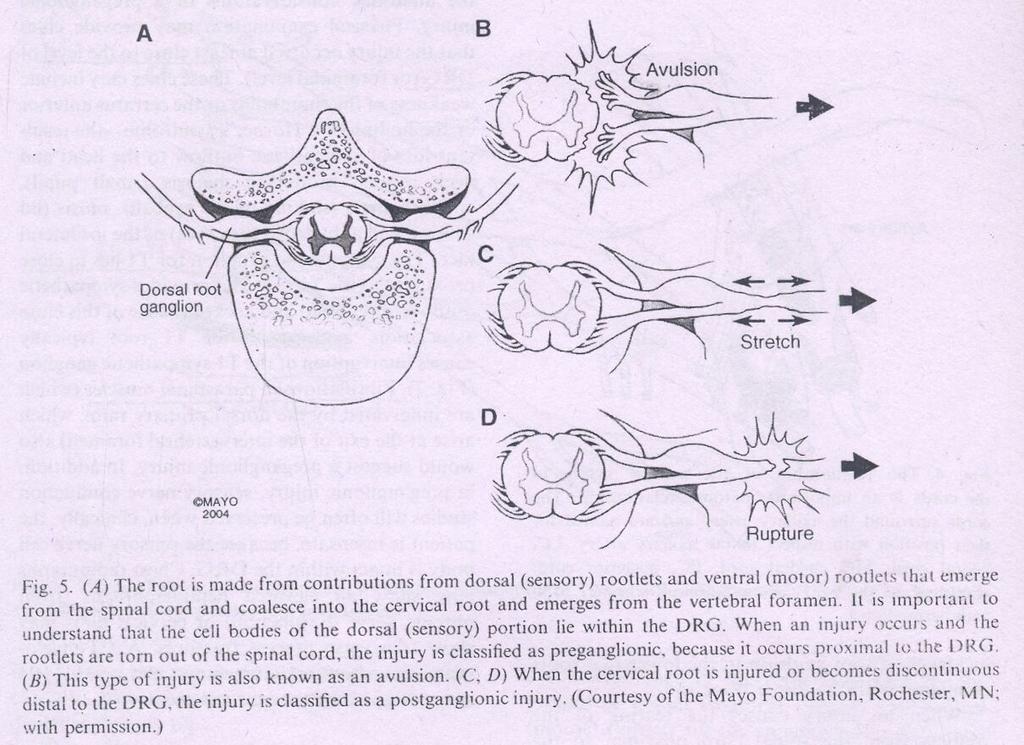
17 Patho-anatomy l Anatomy of rootlets, roots and vertebral foramen contribute to the type of injury l Rootlets forming the cervical roots are intraspinal and lack connective tissue or meningeal envelope. l This feature makes them vulnerable to traction and susceptibility to avulsion at the level of cord. l The spinal nerve is able to move freely in the foramina due to non attachment to it.
18 l There is fibrous attachment of spinal nerves to the transverse process seen in the 4 th through 7 th cervical roots l This explains the high incidence of root avulsions in C8-T1 roots
19 l Preganglionic Tearing of rootlets proximal to dorsal root ganglia a) central b) peripheral l Postganglionic Injury distal to DRG
20 Pathogenesis l Most patients are men and boys between years l 70% of traumatic BPI secondary to motor vehicle accidents l Of these 70% involve motorcycles and bicycles l Other major injuries usually associated in 70%
21 l They are usually closed injuries l 95% traction injuries, 5% compression injuries l Supraclavicular more common than infraclavicular involvement l Roots and trunks most commonly involved l Root avulsions: 2 mechanisms peripheral- common central- rare
22 l Traction injuries head and neck move away from shoulder, usually involve C5,C6 andc7 l C8- T1 involved in hyperabduction injuries l Other mechanisms- penetrating injuries iatrogenic injuries

23 MECHANISM OF INJURY

24 MECHANISM OF INJURY
25
26 Clinical features l High degree of suspicion in injury to shoulder girdle, first rib and axillary artery l Median, ulnar and radial nerves can be evaluated by examining finger and wrist motion l Elbow flexion and extension can be used to examine musculocutaneous nerve and high radial nerve function l Injury to posterior cord may affect deltoid function and muscles innervated by radial nerves
27 l Latissimus dorsi innervated by thoracodorsal nerve is palpated posterior axillary fold l Medial and lateral pectoral nerves are branches of medial and lateral cord respectively and supply sternal and clavicular head of pectoralis major respectively l Supra scapular nerve function shoulder extension, rotation and elevation l Look for Horner syndrome, injury to long thoracic nerve and dorsal scapular nerve to differentiate between pre and post ganglionic lesion
28 l Assess spinal accessory nerve l Active passive range of motion l Rule out cord injury l Tinel s sign l Vascular examination l Fractures
29 PREOPERATIVE PLANNING
30 IMAGING l Radiography- cervical spine views - shoulder view- AP and axillary -X- Ray chest l CT myelography- gold standard for root injury, done at 3 to 4 weeks to see for pseudo meningocoele formation l MRI shows whole of brachial plexus, cord injury and neuroma formation
31 ELECTRODIAGNOSTIC STUDIES l Can help confirm a diagnosis l Localize lesions l Define severity of axon loss and completeness of lesion l Serve as an important adjunct to thorough history,physical exam and imaging study
32 l For closed injuries EMG and NCV can best be performed 3 to 4 weeks after the injury because wallerian degeneration will occur by this time
33 EMG l Denervation changes(fibrillation potentials) can be seen in proximal muscles 10 to 14 days and 3to6 weeks post injury in most distal muscles l Reduced MUP(motor unit potential) recruitment can be shown immediately after weakness from LMN injury l Presence of active motor units with voluntary effort and few fibrillations at rest has good prognosis l Can help in distinguishing preganglionic from postganglionic lesions
34 NCS l In post traumatic BPI the amplitude of compound muscle action potentials (CMAP) are generally low l SNAP important in localizing a lesion as pre or postganglionic
35 INTRA OP TESTING l NAP (nerve action potential l SEP (somatosensory evoked potential) l CMAP (compound muscle action potential)
36 Management
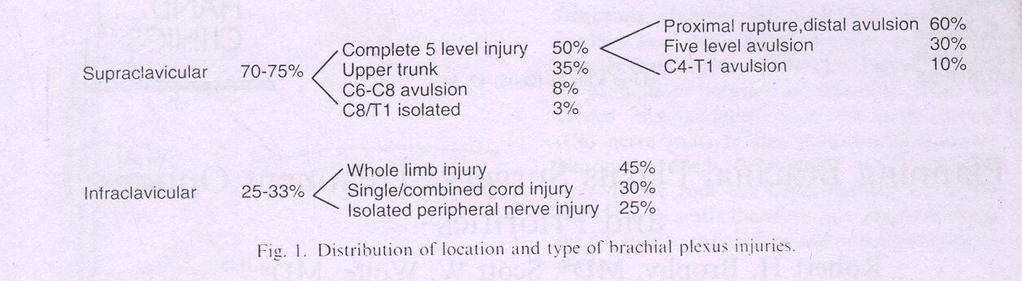
37 Management l 15% of supraclavicular injuries have concomitant segmental injuries at or below the clavicle where the peripheral nerve branch from the plexus l Musculocutaneous, axillary and suprascapular nerves are particularly vulnerable to traction injury because of soft tissue tethering near their origin
38 l Infraclavicular injuries constitute 25-33% of BPI usually occur at cords or peripheral nerves and usually are incomplete l Usually caused by shoulder fracture or dislocation l 5-25% of infraclavicular injuries are associated with axillary artery injury l Penetrating injuries are usually infraclavicular
39 Timing of intervention l A - acute exploration concomittant vascular injury open injury by sharp laceration crush or contaminated wound l B - early exploration (1-2 weeks) unequivocal complete C5- T1 avulsion injuries l C - delayed exploration > 3 months recommended for complete injuries with no recovery by clinical examination or EMG at 12 weeks post injury candidates showing distal recovery without regaining clinical or electrical evidence of proximal muscle function
40 Prioritization l Clearly understand the anatomy of injured plexus l What is available for nerve transfer l Function priority- elbow flexion is the most important to restore followed by abduction, external rotation and scapular stabilization l Long thoracic nerve should be performed whenever possible l Radial nerve motor function can often be restored with triceps function more likely to return
41 Surgical options l Neurolysis l Nerve repair l Nerve graft l Nerve transfer or neurotization l Functional free muscle transfer
42 Neurolysis l Effective only if scar tissue seen around nerve or inside epineurium, preventing recovery or causing pain l Pre and post neurolysis direct nerve stimulation is mandatory to evaluate improvement in nerve conduction
43 Nerve repair l Used in sharp transection with excellent fascicular pattern and minimal scar
44 Nerve graft l Indicated for well defined nerve ends without segmental injuries l Intraoperatively a good fascicular patter should be seen after the neuroma is excised l Possible sources: sural, brachial cutaneous nerve, radial sensory and possibly ulnar nerve l Before implantation graft orientation should be reversed to minimize axonal branch loss l Surgical technique is considered the most important factor in nerve graft
45 Neurotization l A- intraplexal l B- extraplexal l Plexoplexal options are undamaged roots l Other options include medial pectoral nerves and medial cord ulnar nerve l Extraplexal options- spinal accessory, intercostal, phrenic and motor branch of deep cervical plexus
46
47
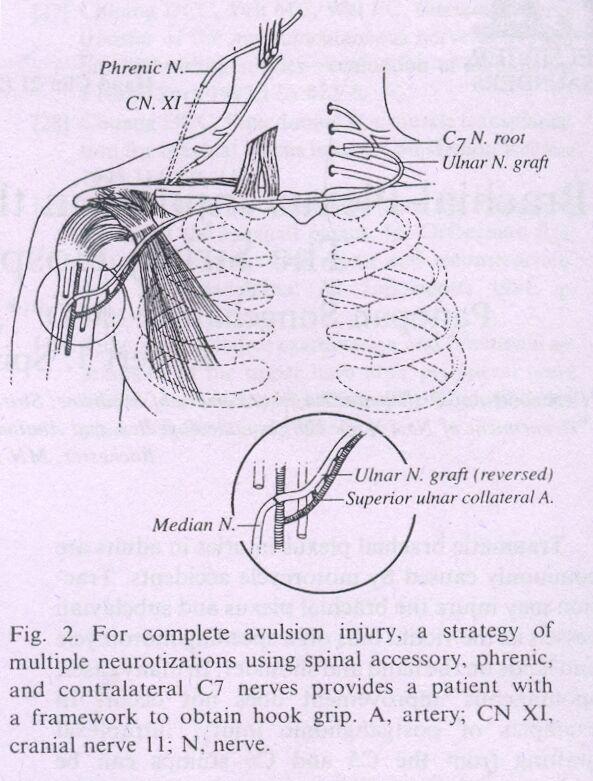
48 l Oberlin technique For upper trunk injury with intact lower trunk- 1 to 2 fascicles of ulnar nerve are anastomosed to biceps l Contra lateral C7 is used in pan brachial plexopathy with multiple avulsions and limited donor possibility l Contra lateral C7 root can be extended by means of vascularised ulnar nerve graft in patient with C8 T1 avulsion and median nerve is the most frequent recipient l Another option is transferring nerve to long head of triceps to anterior branch of axillary nerve
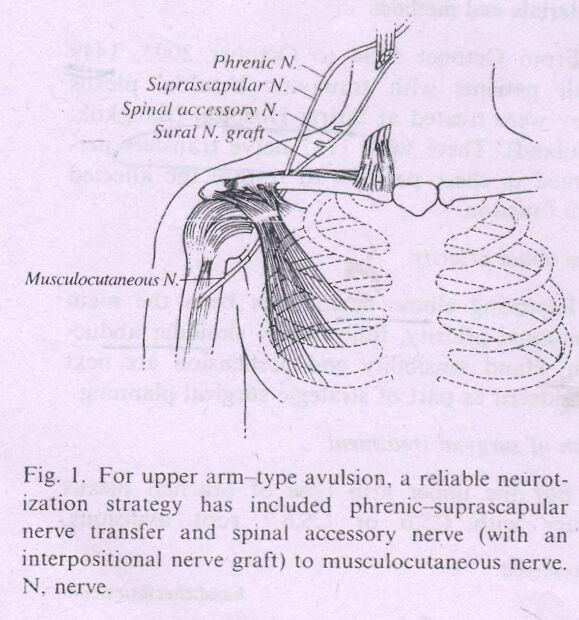
49 Realistic targets to reinnervation l Spinal accessory to surprascapular or musculocutaneous l Phrenic to axillary nerve l Intercostal to musculocutaneous long thoracic, radial and median nerve l Long head of triceps nerve to anterior branch of axillary nerve
50 Functioning free muscle transfer l Usually gracillis is used- single or double gracillis transfer
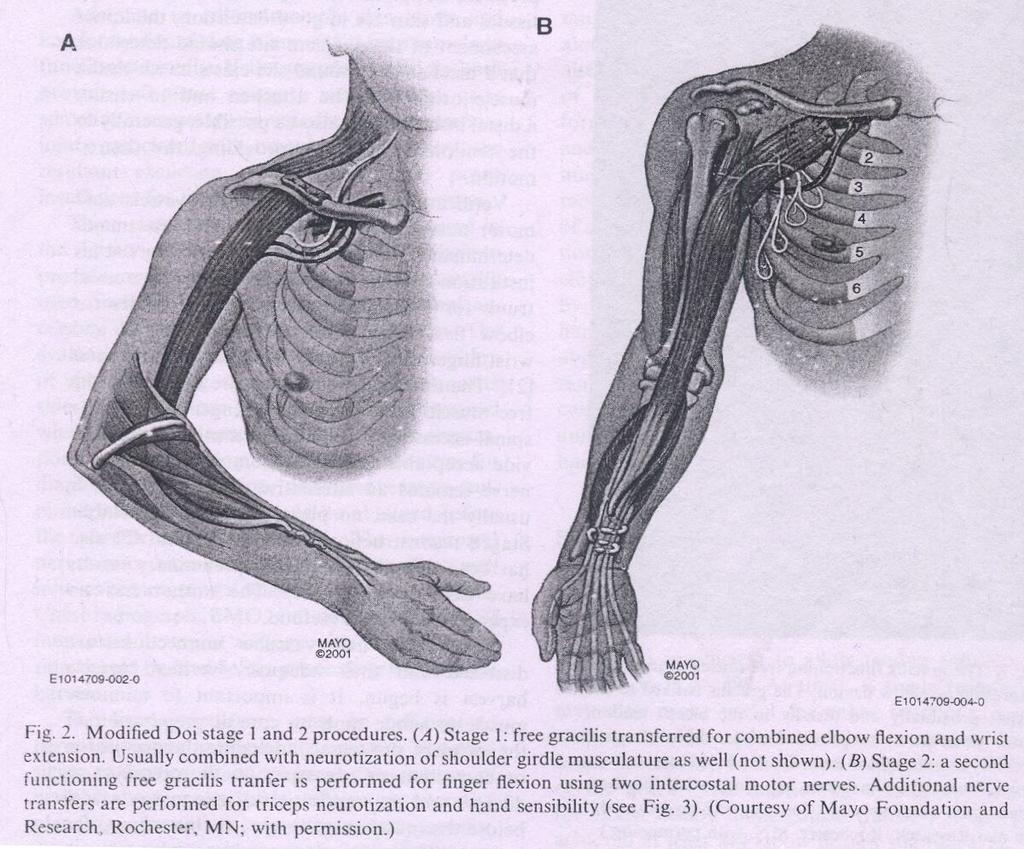
51
52 PROGNOSIS l Highly dependent on pattern of injury l Complete C4 to T1 injuries are considered most severe and virtually irreparable l Avulsion injuries from C5 tot1 amenable to restoration of shoulder and elbow function only l Ideal candidate for surgery are patients with proximal rupture or avulsion and sparing of lower trunk
53 AIIMS STUDY l Since 1995 to2002, 505 patients were studied for functional and occupational outcome after surgery for BPI l In India BPI is most common due to RTA with Rt side involved in 2/3 l 40% cases have pan BPI l 85% of cable graft yielded improvement in motor power compared 68% in neurotized nerve and 66% in patients undergoing neurolysis
54 l Most effective donor nerve for musculocutaneous neurotization was medial pectoral nerve (63.6%) patient improved l Accessory nerve was most effective for neurotization of suprascapular nerve (100%) l Thoracodorsal axillary neurotization gave (66.7% improvement) l 50% patients either remained unemployed or had to change there jobs
55 Thank you
Adult Brachial Plexus Injuries: Introduction and the Role of Surgery
 Adult Brachial Plexus Injuries: Introduction and the Role of Surgery Tim Hems Scottish National Brachial Plexus Injury Service Department of Orthopaedic Surgery, Queen Elizabeth University Hospital, GLASGOW.
Adult Brachial Plexus Injuries: Introduction and the Role of Surgery Tim Hems Scottish National Brachial Plexus Injury Service Department of Orthopaedic Surgery, Queen Elizabeth University Hospital, GLASGOW.
Brachial Plexopathy in a Division I Football Player
 www.fisiokinesiterapia.biz Brachial Plexopathy in a Division I Football Player Brachial Plexus Injuries in Sport Typically a transient neurapraxia - 70% of injured players said they did not always report
www.fisiokinesiterapia.biz Brachial Plexopathy in a Division I Football Player Brachial Plexus Injuries in Sport Typically a transient neurapraxia - 70% of injured players said they did not always report
The Upper Limb III. The Brachial Plexus. Anatomy RHS 241 Lecture 12 Dr. Einas Al-Eisa
 The Upper Limb III The Brachial Plexus Anatomy RHS 241 Lecture 12 Dr. Einas Al-Eisa Brachial plexus Network of nerves supplying the upper limb Compression of the plexus results in motor & sensory changes
The Upper Limb III The Brachial Plexus Anatomy RHS 241 Lecture 12 Dr. Einas Al-Eisa Brachial plexus Network of nerves supplying the upper limb Compression of the plexus results in motor & sensory changes
If head is rapidly forced away from shoulder the injury is generally at C5,C6. If arm is rapidly abducted the lesion is generally at C8-T1.
 BRACHIAL PLEXUS Etiology Generally caused by MVA in adults. Generally males aged 15 to 25 years old. Naracas: Rule of seven seventies. 70% occur secondary to MVA; 70% involve motorcycles or bicycles. 70%
BRACHIAL PLEXUS Etiology Generally caused by MVA in adults. Generally males aged 15 to 25 years old. Naracas: Rule of seven seventies. 70% occur secondary to MVA; 70% involve motorcycles or bicycles. 70%
Management of Brachial Plexus & Peripheral Nerves Blast Injuries. First Global Conflict Medicine Congress
 Management of Brachial Plexus & Peripheral Nerves Blast Injuries Joseph BAKHACH First Global Conflict Medicine Congress Hand & Microsurgery Department American University of Beirut Medical Centre Brachial
Management of Brachial Plexus & Peripheral Nerves Blast Injuries Joseph BAKHACH First Global Conflict Medicine Congress Hand & Microsurgery Department American University of Beirut Medical Centre Brachial
Neurophysiological Diagnosis of Birth Brachial Plexus Palsy. Dr Grace Ng Department of Paed PMH
 Neurophysiological Diagnosis of Birth Brachial Plexus Palsy Dr Grace Ng Department of Paed PMH Brachial Plexus Anatomy Brachial Plexus Cords Medial cord: motor and sensory conduction for median and ulnar
Neurophysiological Diagnosis of Birth Brachial Plexus Palsy Dr Grace Ng Department of Paed PMH Brachial Plexus Anatomy Brachial Plexus Cords Medial cord: motor and sensory conduction for median and ulnar
Gateway to the upper limb. An area of transition between the neck and the arm.
 Gateway to the upper limb An area of transition between the neck and the arm. Pyramidal space inferior to shoulder @ junction of arm & thorax Distribution center for the neurovascular structures that serve
Gateway to the upper limb An area of transition between the neck and the arm. Pyramidal space inferior to shoulder @ junction of arm & thorax Distribution center for the neurovascular structures that serve
*Our main subject is the brachial plexus but it's important to understand the spinal cord first in order to understand the brachial plexus.
 *Our main subject is the brachial plexus but it's important to understand the spinal cord first in order to understand the brachial plexus. *Vertebral column is formed by the union of 33 sequential vertebrae
*Our main subject is the brachial plexus but it's important to understand the spinal cord first in order to understand the brachial plexus. *Vertebral column is formed by the union of 33 sequential vertebrae
Repair of Severe Traction Lesions of the Brachial Plexus
 Repair of Severe Traction Lesions of the Brachial Plexus LAURENT SEDEL, M.D. Since 1972, the author has performed 259 brachial plexus repairs and various associated secondary procedures. The best results
Repair of Severe Traction Lesions of the Brachial Plexus LAURENT SEDEL, M.D. Since 1972, the author has performed 259 brachial plexus repairs and various associated secondary procedures. The best results
Synapse Homework. Back page last question not counted. 4 pts total, each question worth 0.18pts. 26/34 students answered correctly!
 Synapse Homework Back page last question not counted 26/34 students answered correctly! 4 pts total, each question worth 0.18pts Business TASS hours extended! MWF 1-2pm, Willamette 204 T and Th 9:30-10:30am,
Synapse Homework Back page last question not counted 26/34 students answered correctly! 4 pts total, each question worth 0.18pts Business TASS hours extended! MWF 1-2pm, Willamette 204 T and Th 9:30-10:30am,
Brachial plexuses and axillary lymph nodes
 Brachial plexuses and axillary lymph nodes Introduction about nervous system nervous system central nervous system periphral nervous system brain spinal cord 31 pairs of spinal nerves 12 paris of cranial
Brachial plexuses and axillary lymph nodes Introduction about nervous system nervous system central nervous system periphral nervous system brain spinal cord 31 pairs of spinal nerves 12 paris of cranial
Assessment of the Brachial Plexus EMG Course CNSF Halifax Fraser Moore, Canadian Society of Clinical Neurophysiology McGill University
 Assessment of the Brachial Plexus EMG Course CNSF Halifax 2018 Fraser Moore, Canadian Society of Clinical Neurophysiology McGill University Angela Scott, Association of Electromyography Technologists of
Assessment of the Brachial Plexus EMG Course CNSF Halifax 2018 Fraser Moore, Canadian Society of Clinical Neurophysiology McGill University Angela Scott, Association of Electromyography Technologists of
The use of thoracodorsal nerve transfer in restoration of irreparable C5 and C6 spinal nerve lesions
 British Journal of Plastic Surgery (2005) 58, 541 546 The use of thoracodorsal nerve transfer in restoration of irreparable C5 and C6 spinal nerve lesions M.M. Samardzic*, D.M. Grujicic, L.G. Rasulic,
British Journal of Plastic Surgery (2005) 58, 541 546 The use of thoracodorsal nerve transfer in restoration of irreparable C5 and C6 spinal nerve lesions M.M. Samardzic*, D.M. Grujicic, L.G. Rasulic,
Upper Limb Muscles Muscles of Axilla & Arm
 Done By : Saleh Salahat Upper Limb Muscles Muscles of Axilla & Arm 1) Muscles around the axilla A- Muscles connecting the upper to thoracic wall (4) 1- pectoralis major Origin:- from the medial half of
Done By : Saleh Salahat Upper Limb Muscles Muscles of Axilla & Arm 1) Muscles around the axilla A- Muscles connecting the upper to thoracic wall (4) 1- pectoralis major Origin:- from the medial half of
Axilla and Brachial Region
 L 4 A B O R A T O R Y Axilla and Brachial Region BRACHIAL PLEXUS 5 Roots/Rami (ventral rami C5 T1) 3 Trunks Superior (C5, C6) Middle (C7) Inferior (C8, T1) 3 Cords Lateral Cord (Anterior Superior and Anterior
L 4 A B O R A T O R Y Axilla and Brachial Region BRACHIAL PLEXUS 5 Roots/Rami (ventral rami C5 T1) 3 Trunks Superior (C5, C6) Middle (C7) Inferior (C8, T1) 3 Cords Lateral Cord (Anterior Superior and Anterior
Planning Brachial Plexus Surgery: Treatment Options and Priorities
 Hand Clin 21 (2005) 47 54 Planning Brachial Plexus Surgery: Treatment Options and Priorities Robert H. Brophy, MD a, Scott W. Wolfe, MD a,b, * a Hospital for Special Surgery, 535 East 70th Street, New
Hand Clin 21 (2005) 47 54 Planning Brachial Plexus Surgery: Treatment Options and Priorities Robert H. Brophy, MD a, Scott W. Wolfe, MD a,b, * a Hospital for Special Surgery, 535 East 70th Street, New
Nerve Conduction Studies and EMG
 Nerve Conduction Studies and EMG Limitations of other methods of investigations of the neuromuscular system - Dr Rob Henderson, Neurologist Assessment of Weakness Thanks Peter Silburn PERIPHERAL NEUROPATHY
Nerve Conduction Studies and EMG Limitations of other methods of investigations of the neuromuscular system - Dr Rob Henderson, Neurologist Assessment of Weakness Thanks Peter Silburn PERIPHERAL NEUROPATHY
BRACHIAL PLEXUS. DORSAL SCAPULAR NERVE (C5) supraclavicular branch innervates rhomboids (major and minor) and levator scapulae
 supraclavicular branch innervates rhomboids (major and minor) and levator scapulae") THE BRACHIAL PLEXUS DORSAL SCAPULAR NERVE (C5) supraclavicular branch innervates rhomboids (major and minor) and levator scapulae SCHEMA OF THE BRACHIAL PLEXUS THE BRACHIAL PLEXUS PHRENIC NERVE supraclavicular
THE BRACHIAL PLEXUS DORSAL SCAPULAR NERVE (C5) supraclavicular branch innervates rhomboids (major and minor) and levator scapulae SCHEMA OF THE BRACHIAL PLEXUS THE BRACHIAL PLEXUS PHRENIC NERVE supraclavicular
G24: Shoulder and Axilla
 G24: Shoulder and Axilla Syllabus - Pg. 2 ANAT 6010- Medical Gross Anatomy David A. Morton, Ph.D. Objectives Upper limb Systemically: Bones (joints) Muscles Nerves Vessels (arteries/veins) Fascial compartments
G24: Shoulder and Axilla Syllabus - Pg. 2 ANAT 6010- Medical Gross Anatomy David A. Morton, Ph.D. Objectives Upper limb Systemically: Bones (joints) Muscles Nerves Vessels (arteries/veins) Fascial compartments
Chapter 14. The Nervous System. The Spinal Cord and Spinal Nerves. Lecture Presentation by Steven Bassett Southeast Community College
 Chapter 14 The Nervous System The Spinal Cord and Spinal Nerves Lecture Presentation by Steven Bassett Southeast Community College Introduction The Central Nervous System (CNS) consists of: The spinal
Chapter 14 The Nervous System The Spinal Cord and Spinal Nerves Lecture Presentation by Steven Bassett Southeast Community College Introduction The Central Nervous System (CNS) consists of: The spinal
Al Hess MD NERVE REPAIR
 Al Hess MD NERVE REPAIR Historical Aspects 300 BC Hippocrates, description of nervous system 200 AD Galen of Pergamon, nerve injury, questioned possibility of regeneration 600 AD Paul of Arginia, first
Al Hess MD NERVE REPAIR Historical Aspects 300 BC Hippocrates, description of nervous system 200 AD Galen of Pergamon, nerve injury, questioned possibility of regeneration 600 AD Paul of Arginia, first
Brachial plexus lesions
 Brachial plexus lesions SGH Course 11.01.18 Esther Vögelin and Team Handchirurgie und Chirurgie der peripheren Nerven, Universitätsspital Bern Surgical anatomy of the brachial plexus 5-3-6-3-5 5 Roots:
Brachial plexus lesions SGH Course 11.01.18 Esther Vögelin and Team Handchirurgie und Chirurgie der peripheren Nerven, Universitätsspital Bern Surgical anatomy of the brachial plexus 5-3-6-3-5 5 Roots:
Region of upper limb attachment to the trunk Proximal segment of limb overlaps parts of the trunk (thorax and back) and lower lateral neck.
 and lower lateral neck.") Region of upper limb attachment to the trunk Proximal segment of limb overlaps parts of the trunk (thorax and back) and lower lateral neck. includes Pectoral Scapular Deltoid regions of the upper limb
Region of upper limb attachment to the trunk Proximal segment of limb overlaps parts of the trunk (thorax and back) and lower lateral neck. includes Pectoral Scapular Deltoid regions of the upper limb
Scapular and Deltoid Regions
 M1 Gross and Developmental Anatomy Scapular and Deltoid Regions Dr. Peters 1 Outline I. Skeleton of the Shoulder and Attachment of the Upper Extremity to Trunk II. Positions and Movements of the Scapula
M1 Gross and Developmental Anatomy Scapular and Deltoid Regions Dr. Peters 1 Outline I. Skeleton of the Shoulder and Attachment of the Upper Extremity to Trunk II. Positions and Movements of the Scapula
MUSCLES. Anconeus Muscle
 LAB 7 UPPER LIMBS MUSCLES Anconeus Muscle anconeus origin: distal end of dorsal surface of humerus insertion: lateral surface of ulna from distal margin of the semilunar notch to proximal end of the olecranon
LAB 7 UPPER LIMBS MUSCLES Anconeus Muscle anconeus origin: distal end of dorsal surface of humerus insertion: lateral surface of ulna from distal margin of the semilunar notch to proximal end of the olecranon
Peripheral nerve injury
 Peripheral nerve injury Classification of peripheral nerve injury: I. Seddon classification: 1. Neurapraxia: conduction block with or without demyelination (the axon, endoneurium, perineurium and epineurium
Peripheral nerve injury Classification of peripheral nerve injury: I. Seddon classification: 1. Neurapraxia: conduction block with or without demyelination (the axon, endoneurium, perineurium and epineurium
Anatomy of the Musculoskeletal System
 Anatomy of the Musculoskeletal System Kyle E. Rarey, Ph.D. Department of Anatomy & Cell Biology and Otolaryngology University of Florida College of Medicine Outline of Presentation Vertebral Column Upper
Anatomy of the Musculoskeletal System Kyle E. Rarey, Ph.D. Department of Anatomy & Cell Biology and Otolaryngology University of Florida College of Medicine Outline of Presentation Vertebral Column Upper
SHOULDER PAIN. A Real Pain in the Neck. Michael Wolk, MD Northeastern Rehabilitation Associates October 31, 2017
 SHOULDER PAIN A Real Pain in the Neck Michael Wolk, MD Northeastern Rehabilitation Associates October 31, 2017 THE SHOULDER JOINT (S) 1. glenohumeral 2. suprahumeral 3. acromioclavicular 4. scapulocostal
SHOULDER PAIN A Real Pain in the Neck Michael Wolk, MD Northeastern Rehabilitation Associates October 31, 2017 THE SHOULDER JOINT (S) 1. glenohumeral 2. suprahumeral 3. acromioclavicular 4. scapulocostal
Upper limb Arm & Cubital region 黃敏銓
 Upper limb Arm & Cubital region 黃敏銓 1 Arm Lateral intermuscular septum Anterior (flexor) compartment: stronger Medial intermuscular septum Posterior (extensor) compartment 2 Coracobrachialis Origin: coracoid
Upper limb Arm & Cubital region 黃敏銓 1 Arm Lateral intermuscular septum Anterior (flexor) compartment: stronger Medial intermuscular septum Posterior (extensor) compartment 2 Coracobrachialis Origin: coracoid
Peripheral Nervous Sytem: Upper Body
 Peripheral Nervous Sytem: Upper Body MSTN121 - Neurophysiology Session 10 Department of Myotherapy Cervical Plexus Accessory nerve (CN11 + C1-5) Motor: trapezius and sternocleidomastoid Greater auricular
Peripheral Nervous Sytem: Upper Body MSTN121 - Neurophysiology Session 10 Department of Myotherapy Cervical Plexus Accessory nerve (CN11 + C1-5) Motor: trapezius and sternocleidomastoid Greater auricular
BRACHIAL PLEXUS 11/12/2014 كيف تتكون الضفيرة FORMATION ENLARGEMENT (INTUMESCENCE) OF THE SPINAL CORD. Grey matter. Cervical intumescence - C 6 - T 2
 OF THE SPINAL CORD. Grey matter. Cervical intumescence - C 6 - T 2") BRACHIAL PLEXUS Prof. Fawzy Elnady ENLARGEMENT (INTUMESCENCE) OF THE SPINAL CORD Grey matter Cervical intumescence - C 6 - T 2 Lumbar intumescence - L 4 S 2 كيف تتكون الضفيرة FORMATION The ventral rami
BRACHIAL PLEXUS Prof. Fawzy Elnady ENLARGEMENT (INTUMESCENCE) OF THE SPINAL CORD Grey matter Cervical intumescence - C 6 - T 2 Lumbar intumescence - L 4 S 2 كيف تتكون الضفيرة FORMATION The ventral rami
213: HUMAN FUNCTIONAL ANATOMY: PRACTICAL CLASS 1: Proximal bones, plexuses and patterns
 213: HUMAN FUNCTIONAL ANATOMY: PRACTICAL CLASS 1: Proximal bones, plexuses and patterns CLAVICLE Examine an isolated clavicle and compare it with a clavicle on an articulated skeleton. Viewed from above,
213: HUMAN FUNCTIONAL ANATOMY: PRACTICAL CLASS 1: Proximal bones, plexuses and patterns CLAVICLE Examine an isolated clavicle and compare it with a clavicle on an articulated skeleton. Viewed from above,
The grouping of nerves connecting the C4 to Th1 junctions of the spinal cord to the left and right arms.
 THE BRACHIAL The grouping of nerves connecting the C4 to Th1 junctions of the spinal cord to the left and right arms. CONTENTS Brachial plexus Brachial plexus anatomy MRI of brachial plexus Dermatome(C8-T1)
THE BRACHIAL The grouping of nerves connecting the C4 to Th1 junctions of the spinal cord to the left and right arms. CONTENTS Brachial plexus Brachial plexus anatomy MRI of brachial plexus Dermatome(C8-T1)
3 Mohammad Al-Mohtasib Areej Mosleh
 3 Mohammad Al-Mohtasib Areej Mosleh ***Muscles Connecting the Upper Limb to the Vertebral Column 1.Trapezius Muscle ***The first muscle on the back is trapezius muscle, it s called so according
3 Mohammad Al-Mohtasib Areej Mosleh ***Muscles Connecting the Upper Limb to the Vertebral Column 1.Trapezius Muscle ***The first muscle on the back is trapezius muscle, it s called so according
imaging sequences obtained in brachial plexopathy with/without TOS MR Imaging Sequences Associated Anatomic Structures or Pathologic Conditions
 Brachial plexus imaging sequences obtained in brachial plexopathy with/without TOS MR Imaging Sequences Associated Anatomic Structures or Pathologic Conditions Sagittal TSE T2WI through cervical spine
Brachial plexus imaging sequences obtained in brachial plexopathy with/without TOS MR Imaging Sequences Associated Anatomic Structures or Pathologic Conditions Sagittal TSE T2WI through cervical spine
Slide 1. Slide 2. Slide 3. The Role Of Plastic Surgery In Reducing A Patient s Disability Score A Reconstructive Approach. Peripheral Nerve Surgery
 Slide 1 The Role Of Plastic Surgery In Reducing A Patient s Disability Score A Reconstructive Approach Andrew I. Elkwood MD FACS Director of the Center for Treatment of Paralysis and Reconstructive Nerve
Slide 1 The Role Of Plastic Surgery In Reducing A Patient s Disability Score A Reconstructive Approach Andrew I. Elkwood MD FACS Director of the Center for Treatment of Paralysis and Reconstructive Nerve
DR SHRENIK M SHAH SHREY HOSPITAL AHMEDABAD
 DR SHRENIK M SHAH SHREY HOSPITAL AHMEDABAD Surgical anatomy Physiology of healing Classification Pre-operative evaluation OVERVIEW Ultrastructure of the nerve Fragile handle with care Damaged by pressure,
DR SHRENIK M SHAH SHREY HOSPITAL AHMEDABAD Surgical anatomy Physiology of healing Classification Pre-operative evaluation OVERVIEW Ultrastructure of the nerve Fragile handle with care Damaged by pressure,
Anatomy of the Shoulder Girdle. Prof Oluwadiya Kehinde FMCS (Orthop)
") Anatomy of the Shoulder Girdle Prof Oluwadiya Kehinde FMCS (Orthop) www.oluwadiya.com Bony Anatomy Shoulder Complex: Sternum(manubrium) Clavicle Scapula Proximal humerus Manubrium Sterni Upper part of
Anatomy of the Shoulder Girdle Prof Oluwadiya Kehinde FMCS (Orthop) www.oluwadiya.com Bony Anatomy Shoulder Complex: Sternum(manubrium) Clavicle Scapula Proximal humerus Manubrium Sterni Upper part of
Human Anatomy Biology 351
 1 Human Anatomy Biology 351 Upper Limb Exam Please place your name on the back of the last page of this exam. You must answer all questions on this exam. Because statistics demonstrate that, on average,
1 Human Anatomy Biology 351 Upper Limb Exam Please place your name on the back of the last page of this exam. You must answer all questions on this exam. Because statistics demonstrate that, on average,
Upper limb Pectoral region & Axilla
 Upper limb Pectoral region & Axilla 黃敏銓 mchuang@ntu.edu.tw 1 Pectoral region Intercostal nerve Anterior branch of lateral cutaneous branch Lateral cutaneous branch Anterior cutaneous branch Anterior cutaneous
Upper limb Pectoral region & Axilla 黃敏銓 mchuang@ntu.edu.tw 1 Pectoral region Intercostal nerve Anterior branch of lateral cutaneous branch Lateral cutaneous branch Anterior cutaneous branch Anterior cutaneous
FUNCTIONAL ANATOMY OF SHOULDER JOINT
 FUNCTIONAL ANATOMY OF SHOULDER JOINT ARTICULATION Articulation is between: The rounded head of the Glenoid cavity humerus and The shallow, pear-shaped glenoid cavity of the scapula. 2 The articular surfaces
FUNCTIONAL ANATOMY OF SHOULDER JOINT ARTICULATION Articulation is between: The rounded head of the Glenoid cavity humerus and The shallow, pear-shaped glenoid cavity of the scapula. 2 The articular surfaces
Nerve Injury. 1) Upper Lesions of the Brachial Plexus called Erb- Duchene Palsy or syndrome.
 Upper Lesions of the Brachial Plexus called Erb- Duchene Palsy or syndrome.") Nerve Injury - Every nerve goes to muscle or skin so if the nerve is injured this will cause paralysis in the muscle supplied from that nerve (paralysis means loss of function) then other muscles and other
Nerve Injury - Every nerve goes to muscle or skin so if the nerve is injured this will cause paralysis in the muscle supplied from that nerve (paralysis means loss of function) then other muscles and other
Plastic Surgery - Cyber Lectures. Brachial Plexus Injuries Dr. Ashok K. Gupta
 Plastic Surgery - Cyber Lectures Brachial Plexus Injuries Dr. Ashok K. Gupta Projecting for a useful rehabilitation following Brachial Plexus Injury is one of the most demanding surgical designs. Advent
Plastic Surgery - Cyber Lectures Brachial Plexus Injuries Dr. Ashok K. Gupta Projecting for a useful rehabilitation following Brachial Plexus Injury is one of the most demanding surgical designs. Advent
BPBP. Brachial Plexus Birth Palsy BPBP BPBP 11/2/2015. Traction or compression injury during birth. ~ 1 : 1000 live births R > L (LAO presentation)
") Brachial Plexus Birth Palsy Donald S. Bae, MD Boston Children s Hospital BPBP Traction or compression injury during birth ~ 1 : 1000 live births R > L (LAO presentation) Risk factors: macrosomia, difficult
Brachial Plexus Birth Palsy Donald S. Bae, MD Boston Children s Hospital BPBP Traction or compression injury during birth ~ 1 : 1000 live births R > L (LAO presentation) Risk factors: macrosomia, difficult
Early treatment of birth palsy
 Early treatment of birth palsy The Hong King Society for Surgery of the Hand Dr. W.L.TSE Department of Orthopaedics & Traumatology Prince of Wales Hospital WL Tse Early management how? Early management:
Early treatment of birth palsy The Hong King Society for Surgery of the Hand Dr. W.L.TSE Department of Orthopaedics & Traumatology Prince of Wales Hospital WL Tse Early management how? Early management:
STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 5 October 6, 2006
 STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 5 October 6, 2006 PART l. Answer in the space provided. (8 pts) 1. Identify the structures. (2 pts) B C A. _pisiform B. _ulnar artery A C. _flexor carpi
STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 5 October 6, 2006 PART l. Answer in the space provided. (8 pts) 1. Identify the structures. (2 pts) B C A. _pisiform B. _ulnar artery A C. _flexor carpi
Brachial Plexus Injuries
 Brachial Plexus Injuries 1 / 6 2 / 6 3 / 6 Brachial Plexus Injuries A brachial plexus injury (BPI), also known as brachial plexus lesion, is an injury to the brachial plexus, the network of nerves that
Brachial Plexus Injuries 1 / 6 2 / 6 3 / 6 Brachial Plexus Injuries A brachial plexus injury (BPI), also known as brachial plexus lesion, is an injury to the brachial plexus, the network of nerves that
*the Arm* -the arm extends from the shoulder joint (proximal), to the elbow joint (distal) - it has one bone ; the humerus which is a long bone
, to the elbow joint (distal) - it has one bone ; the humerus which is a long bone") *the Arm* -the arm extends from the shoulder joint (proximal), to the elbow joint (distal) - it has one bone ; the humerus which is a long bone - muscles in the arm : *brachialis muscle *Biceps brachii
*the Arm* -the arm extends from the shoulder joint (proximal), to the elbow joint (distal) - it has one bone ; the humerus which is a long bone - muscles in the arm : *brachialis muscle *Biceps brachii
Index. Note: Page numbers of article titles are in boldface type.
 Neurol Clin N Am 20 (2002) 605 617 Index Note: Page numbers of article titles are in boldface type. A ALS. See Amyotrophic lateral sclerosis (ALS) Amyotrophic lateral sclerosis (ALS) active denervation
Neurol Clin N Am 20 (2002) 605 617 Index Note: Page numbers of article titles are in boldface type. A ALS. See Amyotrophic lateral sclerosis (ALS) Amyotrophic lateral sclerosis (ALS) active denervation
Obstetric Brachial Plexus Injuries. Surgery department grand rounds Bassam MJ Addas, FRCSC Neurological Surgery, KAUH
 Obstetric Brachial Plexus Injuries. Surgery department grand rounds Bassam MJ Addas, FRCSC Neurological Surgery, KAUH Definition Obstetric versus birth palsy Obstetric versus congenital palsy Not all birth
Obstetric Brachial Plexus Injuries. Surgery department grand rounds Bassam MJ Addas, FRCSC Neurological Surgery, KAUH Definition Obstetric versus birth palsy Obstetric versus congenital palsy Not all birth
Anterior deltopectoral approach for axillary nerve neurotisation
 Journal of Orthopaedic Surgery 2012;20(1):66-70 Anterior deltopectoral approach for axillary nerve neurotisation J Terrence Jose Jerome Department of Orthopedics, Hand and Reconstructive Microsurgery,
Journal of Orthopaedic Surgery 2012;20(1):66-70 Anterior deltopectoral approach for axillary nerve neurotisation J Terrence Jose Jerome Department of Orthopedics, Hand and Reconstructive Microsurgery,
Surgical repair of brachial plexus injury: a multinational survey of experienced peripheral nerve surgeons
 Neurosurg Focus 16 (5):Preview Article 1, 2004, Click here to return to Table of Contents Surgical repair of brachial plexus injury: a multinational survey of experienced peripheral nerve surgeons ALLAN
Neurosurg Focus 16 (5):Preview Article 1, 2004, Click here to return to Table of Contents Surgical repair of brachial plexus injury: a multinational survey of experienced peripheral nerve surgeons ALLAN
A Patient s Guide to Burners and Stingers
 A Patient s Guide to Burners and Stingers 264 Pleasant Street Concord, NH 03301 Phone: 6032243368 Fax: 6032287268 marketing.copa@concordortho.com DISCLAIMER: The information in this booklet is compiled
A Patient s Guide to Burners and Stingers 264 Pleasant Street Concord, NH 03301 Phone: 6032243368 Fax: 6032287268 marketing.copa@concordortho.com DISCLAIMER: The information in this booklet is compiled
DOJ ABSTRACT. MATERIALS AND METHODS Following approval by our Institutional Review Board, we performed a search of our institution s perioperative
 10.5005/jp-journals-10017-1038 ORIGINAL Restoration RESEARCH of Shoulder Abduction after Radial to Axillary Nerve Transfer following Trauma or Shoulder Arthroplasty Restoration of Shoulder Abduction after
10.5005/jp-journals-10017-1038 ORIGINAL Restoration RESEARCH of Shoulder Abduction after Radial to Axillary Nerve Transfer following Trauma or Shoulder Arthroplasty Restoration of Shoulder Abduction after
Candidate s instructions Look at this cross-section taken at the level of C5. Answer the following questions.
 Section 1 Anatomy Chapter 1. Trachea 1 Candidate s instructions Look at this cross-section taken at the level of C5. Answer the following questions. Pretracheal fascia 1 2 5 3 4 Questions 1. Label the
Section 1 Anatomy Chapter 1. Trachea 1 Candidate s instructions Look at this cross-section taken at the level of C5. Answer the following questions. Pretracheal fascia 1 2 5 3 4 Questions 1. Label the
Al-Balqa Applied University
 Al-Balqa Applied University Faculty Of Medicine *You can use this checklist as a guide to you for the lab. the items on this checklist represent the main features of the models that you have to know for
Al-Balqa Applied University Faculty Of Medicine *You can use this checklist as a guide to you for the lab. the items on this checklist represent the main features of the models that you have to know for
STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 5. September 30, 2011
 STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 5 September 30, 2011 PART l. Answer in the space provided. (12 pts) 1. Identify the structures. (2 pts) EXAM NUMBER A. Suprascapular nerve B. Axillary nerve
STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 5 September 30, 2011 PART l. Answer in the space provided. (12 pts) 1. Identify the structures. (2 pts) EXAM NUMBER A. Suprascapular nerve B. Axillary nerve
Muscles of the Upper Limb
 Muscles of the Upper Limb anterior surface of ribs 3 5 coracoid process Pectoralis minor pectoral nerves protracts / depresses scapula Serratus anterior Subclavius ribs 1-8 long thoracic nerve rib 1 ----------------
Muscles of the Upper Limb anterior surface of ribs 3 5 coracoid process Pectoralis minor pectoral nerves protracts / depresses scapula Serratus anterior Subclavius ribs 1-8 long thoracic nerve rib 1 ----------------
The arm: *For images refer back to the slides
 The arm: *For images refer back to the slides Muscles of the arm: deltoid, triceps (which is located at the back of the arm), biceps and brachialis (it lies under the biceps), brachioradialis (it lies
The arm: *For images refer back to the slides Muscles of the arm: deltoid, triceps (which is located at the back of the arm), biceps and brachialis (it lies under the biceps), brachioradialis (it lies
Abnormal EMG Patterns in Disease. Amanda C. Peltier, MD MS October 12, 2013
 Abnormal EMG Patterns in Disease Amanda C. Peltier, MD MS October 12, 2013 Disclosures I have no financial relationships to disclose that are relative to the content of my presentation. Basic Tenets of
Abnormal EMG Patterns in Disease Amanda C. Peltier, MD MS October 12, 2013 Disclosures I have no financial relationships to disclose that are relative to the content of my presentation. Basic Tenets of
region of the upper limb between the shoulder and the elbow Superiorly communicates with the axilla.
 1 region of the upper limb between the shoulder and the elbow Superiorly communicates with the axilla. Inferiorly, a number of important structures pass between arm & forearm through cubital fossa. 2 medial
1 region of the upper limb between the shoulder and the elbow Superiorly communicates with the axilla. Inferiorly, a number of important structures pass between arm & forearm through cubital fossa. 2 medial
Obstetric Brachial Plexus Injuries: Evaluation and Management
 Obstetric Brachial Plexus Injuries: Evaluation and Management Peter M. Waters, MD Abstract Most infants with brachial plexus birth palsy who show signs of recovery in the first 2 months of life will subsequently
Obstetric Brachial Plexus Injuries: Evaluation and Management Peter M. Waters, MD Abstract Most infants with brachial plexus birth palsy who show signs of recovery in the first 2 months of life will subsequently
Classification of the nervous system. Prof. Dr. Nikolai Lazarov 2
 1 1. Formation and general organization 2. Spinal ganglia 3. Zonal and segmental innervation 4. Dorsal rami of the spinal nerves 5. Ventral rami of the spinal nerves 6. Cervical plexus Classification of
1 1. Formation and general organization 2. Spinal ganglia 3. Zonal and segmental innervation 4. Dorsal rami of the spinal nerves 5. Ventral rami of the spinal nerves 6. Cervical plexus Classification of
Muscle Action Origin Insertion Nerve Innervation Chapter Page. Deltoid. Trapezius. Latissimus Dorsi
 Muscle Action Origin Insertion Nerve Innervation Chapter Page All Fibers Abduct the shoulder (glenohumeral joint) Deltoid Anterior Fibers Flex the shoulder (G/H joint) Horizontally adduct the shoulder
Muscle Action Origin Insertion Nerve Innervation Chapter Page All Fibers Abduct the shoulder (glenohumeral joint) Deltoid Anterior Fibers Flex the shoulder (G/H joint) Horizontally adduct the shoulder
Multiple Neurovascular... Pit Baran Chakraborty, Santanu Bhattacharya, Sumita Dutta.
 Multiple Neurovascular... Pit Baran Chakraborty, Santanu Bhattacharya, Sumita Dutta. Fig-3: Showing high formation of Median nerve. Fig-1: Showing atypical formation of cords of Brachial plexus. 1 = Upper
Multiple Neurovascular... Pit Baran Chakraborty, Santanu Bhattacharya, Sumita Dutta. Fig-3: Showing high formation of Median nerve. Fig-1: Showing atypical formation of cords of Brachial plexus. 1 = Upper
Faculty of Dental Medicine and Surgery. Sem 4 Peripheral nervous system and nerve plexus Dr. Abbas Garib Alla
 Faculty of Dental Medicine and Surgery Sem 4 Peripheral nervous system and nerve plexus Dr. Abbas Garib Alla PNS Terminology Ganglia neuron cell bodies Peripheral nerves neuronal axons PNS neuroglia Satellite
Faculty of Dental Medicine and Surgery Sem 4 Peripheral nervous system and nerve plexus Dr. Abbas Garib Alla PNS Terminology Ganglia neuron cell bodies Peripheral nerves neuronal axons PNS neuroglia Satellite
Nerve Transfers for Adult Traumatic Brachial Plexus Palsy (Brachial Plexus Nerve Transfer)
") DOI 10.1007/s11420-006-9027-y ORIGINAL ARTICLE Nerve Transfers for Adult Traumatic Brachial Plexus Palsy (Brachial Plexus Nerve Transfer) Rachel S. Rohde, MD & Scott W. Wolfe, MD # Hospital for Special
DOI 10.1007/s11420-006-9027-y ORIGINAL ARTICLE Nerve Transfers for Adult Traumatic Brachial Plexus Palsy (Brachial Plexus Nerve Transfer) Rachel S. Rohde, MD & Scott W. Wolfe, MD # Hospital for Special
G25: Brachium. ANAT Medical Gross Anatomy. David A. Morton, Ph.D.
 G25: Brachium ANAT 6010- Medical Gross Anatomy David A. Morton, Ph.D. Brachial Plexus Randy Travis Drinks Cold Beer What muscle(s) enable her to do the following exercise? What muscle(s) enable her to
G25: Brachium ANAT 6010- Medical Gross Anatomy David A. Morton, Ph.D. Brachial Plexus Randy Travis Drinks Cold Beer What muscle(s) enable her to do the following exercise? What muscle(s) enable her to
Spinal nerves. Aygul Shafigullina. Department of Morphology and General Pathology
 Spinal nerves Aygul Shafigullina Department of Morphology and General Pathology Spinal nerve a mixed nerve, formed in the vicinity of an intervertebral foramen, where fuse a dorsal root and a ventral root,
Spinal nerves Aygul Shafigullina Department of Morphology and General Pathology Spinal nerve a mixed nerve, formed in the vicinity of an intervertebral foramen, where fuse a dorsal root and a ventral root,
Multiple variations involving all the terminal branches of the brachial plexus and the axillary artery a case report
 SHORT REPORT Eur J Anat, 10 (3): 61-66 (2006) Multiple variations involving all the terminal branches of the brachial plexus and the axillary artery a case report K. Ramachandran, I. Kanakasabapathy and
SHORT REPORT Eur J Anat, 10 (3): 61-66 (2006) Multiple variations involving all the terminal branches of the brachial plexus and the axillary artery a case report K. Ramachandran, I. Kanakasabapathy and
Case 3. Your Diagnosis?
 Case 3 45 year-old presenting with a history of injury to the right shoulder whilst working in the freezing work. He was loading a sheep over an incline with his arm around the sheep. He felt pain in the
Case 3 45 year-old presenting with a history of injury to the right shoulder whilst working in the freezing work. He was loading a sheep over an incline with his arm around the sheep. He felt pain in the
Posterior Triangle of the Neck By Prof. Dr. Muhammad Imran Qureshi
 Posterior Triangle of the Neck By Prof. Dr. Muhammad Imran Qureshi For the purpose of anatomical description the neck is sub divided into two major triangles, the Anterior and the Posterior by muscle bellies
Posterior Triangle of the Neck By Prof. Dr. Muhammad Imran Qureshi For the purpose of anatomical description the neck is sub divided into two major triangles, the Anterior and the Posterior by muscle bellies
Nerves of Upper limb. Dr. Brijendra Singh Professor & Head Department of Anatomy AIIMS Rishikesh
 Nerves of Upper limb Dr. Brijendra Singh Professor & Head Department of Anatomy AIIMS Rishikesh 1 Objectives Origin, course & relation of median & ulnar nerves. Motor & sensory distribution Carpal tunnel
Nerves of Upper limb Dr. Brijendra Singh Professor & Head Department of Anatomy AIIMS Rishikesh 1 Objectives Origin, course & relation of median & ulnar nerves. Motor & sensory distribution Carpal tunnel
THE SHOULDER JOINT T H E G L E N O H U M E R A L ( G H ) J O I N T
 J O I N T") THE SHOULDER JOINT T H E G L E N O H U M E R A L ( G H ) J O I N T CLARIFICATION OF TERMS Shoulder girdle = scapula and clavicle Shoulder joint (glenohumeral joint) = scapula and humerus Lippert, p115
THE SHOULDER JOINT T H E G L E N O H U M E R A L ( G H ) J O I N T CLARIFICATION OF TERMS Shoulder girdle = scapula and clavicle Shoulder joint (glenohumeral joint) = scapula and humerus Lippert, p115
Key Relationships in the Upper Limb
 Key Relationships in the Upper Limb This list contains some of the key relationships that will help you identify structures in the lab. They are organized by dissection assignment as defined in the syllabus.
Key Relationships in the Upper Limb This list contains some of the key relationships that will help you identify structures in the lab. They are organized by dissection assignment as defined in the syllabus.
Netter's Anatomy Flash Cards Section 6 List 4 th Edition
 Netter's Anatomy Flash Cards Section 6 List 4 th Edition https://www.memrise.com/course/1577581/ Section 6 Upper Limb (66 cards) Plate 6-1 Humerus and Scapula: Anterior View 1.1 Acromion 1.2 Greater tubercle
Netter's Anatomy Flash Cards Section 6 List 4 th Edition https://www.memrise.com/course/1577581/ Section 6 Upper Limb (66 cards) Plate 6-1 Humerus and Scapula: Anterior View 1.1 Acromion 1.2 Greater tubercle
Fig Cervical spinal nerves. Cervical enlargement C7. Dural sheath. Subarachnoid space. Thoracic. Spinal cord Vertebra (cut) spinal nerves
 spinal nerves") Fig. 13.1 C1 Cervical enlargement C7 Cervical spinal nerves Dural sheath Subarachnoid space Thoracic spinal nerves Spinal cord Vertebra (cut) Lumbar enlargement Medullary cone T12 Spinal nerve Spinal nerve
Fig. 13.1 C1 Cervical enlargement C7 Cervical spinal nerves Dural sheath Subarachnoid space Thoracic spinal nerves Spinal cord Vertebra (cut) Lumbar enlargement Medullary cone T12 Spinal nerve Spinal nerve
Spinal Cord and Spinal Nerves. Spinal Cord. Chapter 12
 Chapter 12 Spinal Cord and Spinal Nerves 1 Spinal Cord Extends from foramen magnum to second lumbar vertebra Segmented: Cervical, Thoracic, Lumbar & Sacral Gives rise to 31 pairs of spinal nerves Not uniform
Chapter 12 Spinal Cord and Spinal Nerves 1 Spinal Cord Extends from foramen magnum to second lumbar vertebra Segmented: Cervical, Thoracic, Lumbar & Sacral Gives rise to 31 pairs of spinal nerves Not uniform
OBJECTIVE: To obtain a fundamental knowledge of the root of the neck with respect to structure and function
 The root of the neck Jeff Dupree, Ph.D. e mail: jldupree@vcu.edu OBJECTIVE: To obtain a fundamental knowledge of the root of the neck with respect to structure and function READING ASSIGNMENT: Moore and
The root of the neck Jeff Dupree, Ph.D. e mail: jldupree@vcu.edu OBJECTIVE: To obtain a fundamental knowledge of the root of the neck with respect to structure and function READING ASSIGNMENT: Moore and
7/31/2012 THE SHOULDER JOINT CLARIFICATION OF TERMS OSTEOLOGY OF THE GH JOINT(BONES)
") THE SHOULDER JOINT T H E G L E N O H U M E R AL ( G H ) J O I N T CLARIFICATION OF TERMS Shoulder girdle = scapula and clavicle Shoulder joint (glenohumerual joint) = scapula and Lippert, p115 OSTEOLOGY
THE SHOULDER JOINT T H E G L E N O H U M E R AL ( G H ) J O I N T CLARIFICATION OF TERMS Shoulder girdle = scapula and clavicle Shoulder joint (glenohumerual joint) = scapula and Lippert, p115 OSTEOLOGY
Traumatic Brachial Plexus Preganglionic Injury: What to look for at MR Neurography?
 Traumatic Brachial Plexus Preganglionic Injury: What to look for at MR Neurography? Poster No.: C-1225 Congress: ECR 2017 Type: Authors: Keywords: DOI: Educational Exhibit D. Binaghi 1, M. Socolovsky 2,
Traumatic Brachial Plexus Preganglionic Injury: What to look for at MR Neurography? Poster No.: C-1225 Congress: ECR 2017 Type: Authors: Keywords: DOI: Educational Exhibit D. Binaghi 1, M. Socolovsky 2,
A Patient s Guide to Burners and Stingers
 A Patient s Guide to Burners and Stingers 763 Larkfield Road 2nd Floor Commack, NY 11725 Phone: (631) 462-2225 Fax: (631) 462-2240 DISCLAIMER: The information in this booklet is compiled from a variety
A Patient s Guide to Burners and Stingers 763 Larkfield Road 2nd Floor Commack, NY 11725 Phone: (631) 462-2225 Fax: (631) 462-2240 DISCLAIMER: The information in this booklet is compiled from a variety
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Spine Neurosurgery Brian L. Hoh, MD 1 and Gregory J. Zipfel, MD 2 1 University of Florida, 2 Washington University Spine Neurosurgery Spine neurosurgeons treat
Introduction to Neurosurgical Subspecialties: Spine Neurosurgery Brian L. Hoh, MD 1 and Gregory J. Zipfel, MD 2 1 University of Florida, 2 Washington University Spine Neurosurgery Spine neurosurgeons treat
Management of Missile Injuries of the Brachial Plexus
 Original Article Indian Journal of Neurotrauma (IJNT) 49 2006, Vol. 3, No. 1, pp. 49-54 Management of Missile Injuries of the Brachial Plexus P S Bhandari M Ch, L P Sadhotra M Ch, P Bhargava M Ch, A S
Original Article Indian Journal of Neurotrauma (IJNT) 49 2006, Vol. 3, No. 1, pp. 49-54 Management of Missile Injuries of the Brachial Plexus P S Bhandari M Ch, L P Sadhotra M Ch, P Bhargava M Ch, A S
Human Anatomy Biology 351
 nnnnn 1 Human Anatomy Biology 351 Exam #2 Please place your name on the back of the last page of this exam. You must answer all questions on this exam. Because statistics demonstrate that, on average,
nnnnn 1 Human Anatomy Biology 351 Exam #2 Please place your name on the back of the last page of this exam. You must answer all questions on this exam. Because statistics demonstrate that, on average,
Pain Assessment Patient Interview (location/nature of symptoms), Body Diagram. Observation and Examination: Tests and Measures
, Body Diagram. Observation and Examination: Tests and Measures") Examination of Upper Quarter Neurogenic Pain Jane Fedorczyk, PT, PhD, CHT Thomas Jefferson University, Philadelphia, PA Center of Excellence for Hand and Upper Limb Rehabilitation I. History Mechanism
Examination of Upper Quarter Neurogenic Pain Jane Fedorczyk, PT, PhD, CHT Thomas Jefferson University, Philadelphia, PA Center of Excellence for Hand and Upper Limb Rehabilitation I. History Mechanism
MUSCLE MECHANICS AND CONTROL
 MUSCLE MECHANICS AND CONTROL STRUCTURE OF A SKELETAL MUSCLE NEUROVASCULAR BUNDLE - CONTAINS THE BLOOD VESSELS AND THE NERVES TO A MUSCLE SKELETAL MUSCLE - LONGITUDINAL SECTION MUSCLE ATTACHMENTS: TENDONS
MUSCLE MECHANICS AND CONTROL STRUCTURE OF A SKELETAL MUSCLE NEUROVASCULAR BUNDLE - CONTAINS THE BLOOD VESSELS AND THE NERVES TO A MUSCLE SKELETAL MUSCLE - LONGITUDINAL SECTION MUSCLE ATTACHMENTS: TENDONS
Review Article Brachial Plexus Injuries in Adults: Evaluation and Diagnostic Approach
 ISRN Orthopedics, Article ID 726103, 9 pages http://dx.doi.org/10.1155/2014/726103 Review Article Brachial Plexus Injuries in Adults: Evaluation and Diagnostic Approach Vasileios I. Sakellariou, 1 Nikolaos
ISRN Orthopedics, Article ID 726103, 9 pages http://dx.doi.org/10.1155/2014/726103 Review Article Brachial Plexus Injuries in Adults: Evaluation and Diagnostic Approach Vasileios I. Sakellariou, 1 Nikolaos
Original Article Selective neurotization of the radial nerve in the axilla using intercostal nerve to treat complete brachial plexus palsy
 Int J Clin Exp Med 2016;9(11):22880-22885 www.ijcem.com /ISSN:1940-5901/IJCEM0032455 Original Article Selective neurotization of the radial nerve in the axilla using intercostal nerve to treat complete
Int J Clin Exp Med 2016;9(11):22880-22885 www.ijcem.com /ISSN:1940-5901/IJCEM0032455 Original Article Selective neurotization of the radial nerve in the axilla using intercostal nerve to treat complete
MUSCLES OF SHOULDER REGION
 Dr Jamila EL Medany OBJECTIVES At the end of the lecture, students should: List the name of muscles of the shoulder region. Describe the anatomy of muscles of shoulder region regarding: attachments of
Dr Jamila EL Medany OBJECTIVES At the end of the lecture, students should: List the name of muscles of the shoulder region. Describe the anatomy of muscles of shoulder region regarding: attachments of
Human Anatomy and Physiology I Laboratory Spinal and Peripheral Nerves and Reflexes
 Human Anatomy and Physiology I Laboratory Spinal and Peripheral Nerves and Reflexes 1 This lab involves the second section of the exercise Spinal Cord, Spinal Nerves, and the Autonomic Nervous System,
Human Anatomy and Physiology I Laboratory Spinal and Peripheral Nerves and Reflexes 1 This lab involves the second section of the exercise Spinal Cord, Spinal Nerves, and the Autonomic Nervous System,
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,000 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,000 116,000 120M Open access books available International authors and editors Downloads Our
Making sense of Nerve conduction & EMG
 Making sense of Nerve conduction & EMG Drs R Arunachalam Consultant Clinical Neurophysiologist Wessex Neurological Centre Southampton University Hospital EMG/NCS EMG machine For the assessment of patients
Making sense of Nerve conduction & EMG Drs R Arunachalam Consultant Clinical Neurophysiologist Wessex Neurological Centre Southampton University Hospital EMG/NCS EMG machine For the assessment of patients
The Spinal Cord, Spinal Nerves, and Spinal Reflexes
 13 The Spinal Cord, Spinal Nerves, and Spinal Reflexes PowerPoint Lecture Presentations prepared by Jason LaPres Lone Star College North Harris An Introduction to the Spinal Cord, Spinal Nerves, and Spinal
13 The Spinal Cord, Spinal Nerves, and Spinal Reflexes PowerPoint Lecture Presentations prepared by Jason LaPres Lone Star College North Harris An Introduction to the Spinal Cord, Spinal Nerves, and Spinal
The Clavicle Right clavicle Deltoid tubercle: Conoid tubercle, conoid ligamen Impression for the
 The Clavicle Muscle Attachment Sites in the Upper Limb Pectoralis major Right clavicle Smooth superior surface of the shaft, under the platysma muscle tubercle: attachment of the deltoid Acromial facet
The Clavicle Muscle Attachment Sites in the Upper Limb Pectoralis major Right clavicle Smooth superior surface of the shaft, under the platysma muscle tubercle: attachment of the deltoid Acromial facet
Demonstrate the bony features of Cl and C2 vertebrae evident on this Xray
 SUBJECT: ANATOMY 7 September 2007 am. TOPIC: X-ray: Lateral C spine NUMBER: JL Demonstrate the bony features of Cl and C2 vertebrae evident on this Xray 1 Odontoid peg (dens) 2 Bodies of Cl andc2 3 anterior
SUBJECT: ANATOMY 7 September 2007 am. TOPIC: X-ray: Lateral C spine NUMBER: JL Demonstrate the bony features of Cl and C2 vertebrae evident on this Xray 1 Odontoid peg (dens) 2 Bodies of Cl andc2 3 anterior
Chapter 13: The Spinal Cord and Spinal Nerves
 Chapter 13: The Spinal Cord and Spinal Nerves Spinal Cord Anatomy Protective structures: Vertebral column and the meninges protect the spinal cord and provide physical stability. a. Dura mater, b. Arachnoid,
Chapter 13: The Spinal Cord and Spinal Nerves Spinal Cord Anatomy Protective structures: Vertebral column and the meninges protect the spinal cord and provide physical stability. a. Dura mater, b. Arachnoid,
Joint G*H. Joint S*C. Joint A*C. Labrum. Humerus. Sternum. Scapula. Clavicle. Thorax. Articulation. Scapulo- Thoracic
 A*C Joint Scapulo- Thoracic Articulation Thorax Sternum Clavicle Scapula Humerus S*C Joint G*H Joint Labrum AC Ligaments SC Ligaments SC JOINT AC Coracoacromial GH GH Ligament Complex Coracoclavicular
A*C Joint Scapulo- Thoracic Articulation Thorax Sternum Clavicle Scapula Humerus S*C Joint G*H Joint Labrum AC Ligaments SC Ligaments SC JOINT AC Coracoacromial GH GH Ligament Complex Coracoclavicular
PNS and ANS Flashcards
 1. Name several SOMATIC SENSES Light touch (being touched by a feather), heat, cold, vibration, pressure, pain are SOMATIC SENSES. 2. What are proprioceptors; and how is proprioception tested? PROPRIOCEPTORS
1. Name several SOMATIC SENSES Light touch (being touched by a feather), heat, cold, vibration, pressure, pain are SOMATIC SENSES. 2. What are proprioceptors; and how is proprioception tested? PROPRIOCEPTORS
THORACIC OUTLET SYNDROME: A FREQUENT CAUSE OF NON-DISCOGENIC BRACHIALGIA
 THORACIC OUTLET SYNDROME: A FREQUENT CAUSE OF NON-DISCOGENIC BRACHIALGIA Debora Garozzo Brachial Plexus and Peripheral Nerve Surgery Unit Neurospinal Hospital Dubai, United Arab Emirates THE THORACIC OUTLET
THORACIC OUTLET SYNDROME: A FREQUENT CAUSE OF NON-DISCOGENIC BRACHIALGIA Debora Garozzo Brachial Plexus and Peripheral Nerve Surgery Unit Neurospinal Hospital Dubai, United Arab Emirates THE THORACIC OUTLET