Patellofemoral Pain Syndrome
|
|
|
- Jeremy Jennings
- 6 years ago
- Views:
Transcription
 Patellofemoral Pain Syndrome Presented by Aaron Rutter PT, BScPT, FCAMPT www.")
1 Certificate of Excellence (COE) Program Program delivered by the RMTAO Certificate of Excellence In Assessment Certificate of Excellence in Assessment CMTO and RMTAO member Complete 10 RMTAO run assessment courses over a 5 year period Pass each course s examination with a minimum 70% (multiple choice quiz) Patellofemoral Pain Syndrome Presented by Aaron Rutter PT, BScPT, FCAMPT Introduction Course Objectives Physiotherapist Manual and Manipulative Physiotherapist Acupuncture Queen s University RMTAO courses How do you recognize the signs and symptoms of patellofemoral pain? Does the patella actually track laterally or does the femur move medially to cause patellofemoral pain? How do you know someone has weak gluteus medius, gluteus maximus and quadriceps? Do you need to specifically strengthen vastus medialis oblique? What other dysfunctions can contribute to patellofemoral pain syndrome? 1
 Ligamentous sprains: MCL, LCL, PCL, ACL Bursitis: supra/infra/pre-patellar, pes ancerinus Plica syndrome Fat pad syndrome Loose")
2 Anterior Knee Pain Patellofemoral Pain Syndrome Patellofemoral pain syndrome Fractures: femur, tibia, fibula, patella Muscle strains: quadriceps Tendinopathies: patellar, quadriceps, pes ancerinus ITB friction syndrome Meniscal: anterior horn (medial or lateral) Ligamentous sprains: MCL, LCL, PCL, ACL Bursitis: supra/infra/pre-patellar, pes ancerinus Plica syndrome Fat pad syndrome Loose bodies Synovitis OA, RA and other rheumatic diseases Referred Pain Hip OA, Lumbar disc or nerve root, SIJ, femoral nerve A syndrome, in medicine and psychology, is the collection of signs and symptoms that are observed in, and characteristic of, a single condition Anatomy Anatomy 2




3 Anatomy Anatomy Patellofemoral Joint Patellar Joint Surface Classification Synovial, compound, modified sellar Capsular Patterning Flexion > extension Closed Pack Position Full squat? Resting Position 25 degrees flex End Feel Capsular Largest sesamoid bone in body Modified sellar Convex: medial to lateral Trochlear groove: concave medial to lateral Concave: superior to inferior with a ridge in middle Trochlear groove: convex superior to inferior 3


4 Patellar Facets Contact Points of Patella The entire surface of the patella is never in contact with the femur at any given point in time Medial Odd Superior Middle Inferior Lateral 0 degrees Supra-patellar fat pad/bursa degrees Inferior facet of patella on trochlea degrees Middle facet of patella on trochlea degrees Superior facet of patella on trochlea 135 degrees Odd facet against medial femoral condyle 135 Medial Right Knee Lateral Right Knee Patellofemoral Pain Syndrome Non specific pain around or under the patella caused by poor tracking of the patella/femur Most common cause of anterior knee pain Patellar Pathologies 4

 Irritation of the tibialtubercle")
 in the tendon, decrease and disorientation of collagen, it has a decreased ability to take force (resisted,")
5 Chrondromalacia Patella Chondromalcia Patella Softening and degeneration of the cartilage under the patella Quite often used interchangeably with patellofemoral pain syndrome Usually occurs in adolescents, females greater than males 4 grades Grade I: softening and swelling, intact cartilage Grade II: fragmentation and fissuring of the articular surface within softened area Grade III: fibrillation or breakdown of the articular cartilage with a crap meat appearance Grade IV: erosive changes with exposure of the subchondral bone Normal patella Chondralmalcia patella Tendinopathies Osgood-Schlatter s Disease Quadriceps Patellar (Jumper s Knee) Irritation of the tibialtubercle growth plate in pre-teen or teens, caused by strong quadriceps contractions, causing excessive bone formation Tendinitis vs tendinosis Overuse vslack of use Tendinitis: inflammation Tendinosis: structural change (degeneration) in the tendon, decrease and disorientation of collagen, it has a decreased ability to take force (resisted, stretch, compression etc) 5


6 Sinding-Larson-Johannson Disease Osteoarthritis Boney fragmentation of the inferior pole of the patella in adolescence caused by a tendinitis of the proximal patellar tendon, leading to calcification and ossification Wear and tear of the cartilage Articular cartilage is about 5 mm thick Thickest in body Patellar Function Patellofemoral Pain Improve transmission of force from quadriceps to tibia especially in early ranges of flexion Increases mechanical advantage by up to 50% Lack of compression of the patellofemoraljoint is a source of pain Heino-BrechterJH, Powers CM. Patellofemoralstress during walking in persons with and without patellofemoralpain. Med SciSports Exerc. 2002;34:






7 Patellofemoral Braces Patellofemoral Braces Braces can increase the compression of the patellofemoraljoint by 30-40% and decrease patellofemoral stress by 27% and pain by 56% Braces do not improve the tracking of the patella PowersCM et al. Theeffectofbracingonpatellaalignment and patellofemoraljointcontactarea. MedSciSportsExerc. 2004;36: , PowersCM et al. Theeffectofbracingonpatellarkinematics in patientswithpatellofemoralpain. MedSciSportExerc. 1999:31: Powers CM et al. Theeffectofbracingonpatellofemoraljointstress during free and fast walking. Am J Sports Med. 2004;32: Brace/Taping McConnell Taping Using Hypafix and Leuko (brown) tape 1. Add compression Correct rotation Correct tilt Correct glide 2. Retest comparable sign (squat, stairs) 7

8 Patellofemoral Joint Stress Quadriceps Strengthening Posterior, superior, lateral Patellofemoral Pain Diminished contact area Elevated joint reaction forces Walking 0.5 body weight Up stairs 2.5 times body weight Down stairs 3.5 times body weight Squat to 90 degrees 7.5 times body weight Does vastus medialis oblique exist? Still controversy over if vastusmedialisis a single anatomical structure Smith TO et al. Do the vastusmedialisoblique and vastusmedialis longus really exist? A systematic review. Clin Anat 2009; 22(2): Quadriceps Strengthening Quadriceps Strengthening Can vastus medialis be preferentially activated? Altering lower limb orientation or the addition of co-contractions does not preferentially activate vastus medialis oblique. Smith TO et al. Can vastusmedialisoblique be preferentially activated? A systemic review of electromyographicstudies. Physiother Theory Pract. 2009; 25(2): Is isolated vastus medialis strengthening better than global quadricep strengthening? No. Both had similar improvements after an 8 week program as compared to a control group Symeet al. Disability in patients with chronic patellofemoralpain syndrome: a randomised controlled trial of VMO selective training versus general quadriceps strengthening. Man Ther 2009; 14(3):

9 Quadriceps Strengthening New Concept in the Research One issue with quadriceps strengthening is that the vector of force for the quads will always pull the patella laterally (Q angle) Even though you have improved compression through the patellofemoraljoint which will improve tracking, you may have to address other biomechanical problems that will effect the tracking Souza RB et al. Femur rotation and patellofemoral joint kinematics: A weight-bearing MRI analysis. J Orthop Sports Phys Ther. 2010;40: Historically, the patella was assumed to move on a fixed femur so most research was done in non weight bearing with the femur fixed Current research has been done in weight bearing and the conclusions being drawn are that the femur moves underneath a fixed patella If the femur internally rotates and adducts, this will cause relative laterally tracking of the patella What muscles control the position of the femur? SERF Bracing SERF: stabilization into external rotation of the femur ($85) Helps prevent lateral translation of the patella by preventing the femur from adducting and internally rotating Use for patellar dislocation and persistent patellofemoralpain and/or athletes that want to continue to play through their symptoms Observations 9


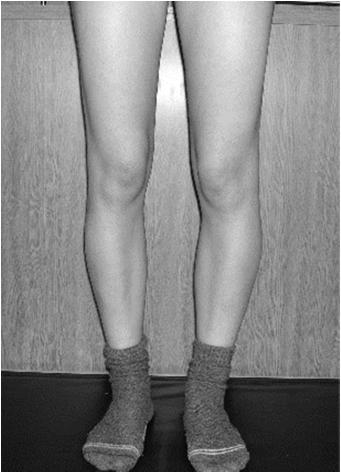

10 Genu Varus Genu Valgus Femeral Anteversion Tibial Torsion/Genu Valgus 10

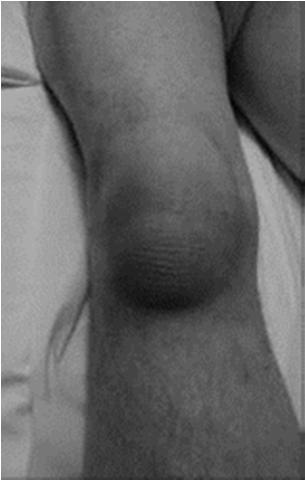


11 Pre-patellar Bursitis Infra-patellar Bursitis Supra-patellar Bursitis & Quadricep Atrophy Dislocated Patella 11




12 Camel Sign (Fat Pad Irritation) Patellar Tendon Rupture Patellar Alignment Patella Alta Patella Alta High riding patella Patella Baja Low riding patella Frog-eyed Patella Patella high riding and lateral Squinting Patella Patella positioned medially Tilted Patella Translated Patella Rotated Patella 12




13 Patella Baja Frog Eyed Patellae Squinting Patellae Lateral Tilt and Translation Merchant s View X-ray taken from above when knee in 45 degrees of flexion 13
 or around the knee cap (peripatellar) It does not refer to any other part of the leg")
14 Subjective Complaints Pain Location Diffuse/specific ache around and/or underneath the patella Gradual onset Weight bearing activities aggravate Stairs, squatting, kneeling, running, jumping Movie goers knee Prolonged sitting in knee flexion Crepitus No/mild swelling Pain is always underneath (retropatellar) or around the knee cap (peripatellar) It does not refer to any other part of the leg Observations Static Posture Muscle bulk: quads, hams, gluts, add, gastroc Swelling Capsular, bursitis, tibial tubercle Femoral anteversion Femoral or tibial torsion Genu varus, valgus Patellar position Alta, baja, squinting, frog eyed Tilted, translated, rotated Observations Dynamic Walking Single Leg Stance Squat (sit to stand off chair) Step down off 8-9 inch step Athletes Lateral shuffle Deceleration Triple jump on 1 leg Side cut 14
 Trunk stays upright instead of forward trunk lean Trunk lean to weight bearing side (compensated")
 side When")
 adducts")
15 What to look for Ankle/Knee Strategy Squat Trunk Upright Initiate movement through ankle and knee instead of the hip (eccentric gastroc) Trunk stays upright instead of forward trunk lean Trunk lean to weight bearing side (compensated Trendelenburg) Pelvic drop (uncompensated Trendelenburg) Internal rotation and adduction of the femur (valgus of the knee) Compensated Trendelenburg Uncompensated Trendelenburg Lateral trunk lean towards the stance (weight bearing) side When bring center of gravity closer to the hip the hip abductors don t have to work as hard to maintain balance Loss of hip abductor strength Pelvis on opposite side drops due to hip abductor insufficiency in single leg stance Hip (femur) adducts and internally rotates 15


16 Valgus of the knee Common Causes of Patellofemoral Pain 1. Femoral anteversion 2. Increased Q angle 3. Tight lateral retinaculum 4. Tensor fascia latae tightness 5. Vastus lateralis tightness 6. Biceps femoris tightness 7. Weak iliacus 8. Tight Gastrocnemius/Soleus 9. Weak Gluteus Medius, Gluteus Maximus and Quadriceps 1. Femoral Anteversion Femoral Anteversion Angle between the neck of femur and the posterior femoral condyles Craig s Test Trochantericprominence angle test Normal Birth: 30 degrees Adult: 8-12 degrees >12 degrees = femoral anteversion IR and ER rotate hip until the greater trochanteris most prominent If hip in more than 12 degrees of IR, then the patient has femoral anteversion 16


 Medial glide of patella restricted May bias when in Ober stest, as")
17 2. Increased Q angle Q Angle 2 lines ASIS to mid patella Mid patella to tibial tubercle Difference between these 2 lines is the Q angle Normal degrees Quads are always pulling the patella laterally Increased Q angle 3. Tight Lateral Retinaculum Femoral anteversion External tibial torsion Lateral displacement of tibial tubercle Broad pelvis (females) Supinated feet (tibial external rotation) Medial glide of patella restricted May bias when in Ober stest, as lateral retinaculumand ITB are interconnected 17

18 ITB Tension Tension vs Tightness 1. Gluteus maximus Direct attachment 2. Tensor fascia latae Direct attachment 3. Biceps femoris(short & long) Fascial attachment 4. Vastus lateralis Fascial attachment 1 2 ITB 3 4 Tension/Hypertonicity Increased elastic/viscoelastic stiffness in the absence of contractile activity DO NOT ASSUME THE MUSCLE IS TIGHT Must check muscle length/flexibility Quite often it is normal or overlengthened Tension will be relieved by strengthening, shortening or unloading the tissue (eg massage, taping, acupuncture) TRY TO FIND THE SOURCE OF THE TENSION Tightness Muscle length/flexibility is decreased Tightness will be relieved by stretching Netter Patient complaints will be the same for both Pain, stiffness, tightness, spasm, trigger points ITB Tension ITB Tension Common Causes The ITB is put on tension by the muscles attaching into it. These are what should be addressed first. Rarely will you have to treat the ITB directly The ITB is such a thick fascia, the muscles attaching into the band is what will stretch more effectively when you treat it Muscle Tightness TFL Gluteus maximus Biceps femoris Vastus lateralis Muscle Weakness Gluteus medius (overuse TFL as a hip abductor) 18







19 4. Tensor Fascia Latae Tightness Tensor Fascia Latae Tightness Stretching Modified Thomas in hip ER Ober s Home Stretch Lunge position ER back leg Posterior pelvic tilt Tensor Fascia Latae Tightness 5. Vastus Lateralis Tightness Home Stretching Knee flexion Does hip and pelvic position matter? 19




20 6. Biceps Femoris Tightness Home Stretching Tibial internal rotation Anterior pelvic tilt, lean forward through groin 7. Weak iliacus Test double straight leg raise with femur in some external rotation Arab AM et al. Sensitivity, specificity and predictive value of the clinical trunk muscle endurance tests in low back pain. Clinical Rehabilitation 2007; 21: Can they hold 28 seconds 8. Gastroc/Soleus Tightness Decreased dorsiflexion can cause the foot to turn out during gait causing tibial ER Increased Q angle Normal DF ROM? Foot pointing straight to wall Heel must stay on ground 9. Weak Gluteus Medius, Maximus and Quadriceps Prins MR et al. Females with patellofemoral pain syndrome have weak hip muscles:a systematic review. Aust J Physiother. 2009;55:9-15. Souza RB, PowersCM. Differencesinhipkinematics, musclestrength, and muscle activation between subjects with and without patellofemoral pain. J Orthop Sports Phys Ther. 2009;39: NoehrenB, DavisI. Theeffectofreal-timegaitretrainingonhip kinematics, pain and function in subjects with patellofemoral pain syndrome. Br J Sports Med. 2011;45:


21 Hip Kinematics Stage 1 Chris Powers Physiotherapist and researcher from California 8 stages for strengthening progression Non weight bearing activation Therabandmust always be above the knee Must hold the femur towards abduction and external rotation Clinically most patients are symptom free by stage 5 Clam Hip Abduction Hold 60 sec Theraband above the knee Hold 60 sec Theraband above the knee 21




22 Fire Hydrant Side Plank Hold 60 sec McGill SM et al. Endurance times for low back stabilization exercises: clinical targets for testing and training from a normal database. Arch Phys Med Rehabil 1999; 80: Males 95 sec Females 75 sec Side Plank Modified Side Planks 22




23 Stage 2 Weight bearing activation Double limb static Squat (Quads:Glut = 1:1) Hold 60 sec When do quads start to work more than gluts? Belt or band around the knees Surfer s Squat Stage 3 Hold 60 sec When do quads start to work more than gluts? Weight bear activation Single leg static 23





24 Wall Push Standing Fire Hydrant Hold 60 sec Prevents compensated Trendelenburg Hold 60 sec Kneeling Bosu Stage 4 Hold 60 sec Weight bearing Double limb dynamic 24





25 Resisted Squats Kettle Bell Squats Crab/Monster Walking Forward Lunge 25




26 Stage 5 Single Leg Squat with Bench Assist Weight bearing Single limb dynamic Single Leg Squat Romanian Deadlift 26



27 Step Ups Step Downs Hip Hikes Stage 6 Weight bearing Double limb ballistic 27


28 Box Jumping Lateral Jumping Bad Good Stage 7 1 Leg Jumping and Cutting Weight bearing Single limb ballistic Focus on variability Agility ladders Jumping forwards Jumping sideways (45 degrees) Jumping laterally Cutting at different angles Box jumping and landing External focus of attention during function movements 28
,")

29 Agility Ladder 1 Leg Jump Stage 8 Review Return to sport Avoid contact Sport specific drills After many practices (up to 1 month), then add contact FIND THE SOURCE OF FEMORAL INTERNAL ROTATION AND ADDUCTION Strengthen Gluts, gluts, gluts, gluts, and more gluts Strengthen Quads 29


30 Thank you For future courses visit or me at 30
5/14/2013. Acute vs Chronic Mechanism of Injury:
 Third Annual Young Athlete Conference: The Lower Extremity February 22, 2013 Audrey Lewis, DPT Acute vs Chronic Mechanism of Injury: I. Direct: blow to the patella II. Indirect: planted foot with a valgus
Third Annual Young Athlete Conference: The Lower Extremity February 22, 2013 Audrey Lewis, DPT Acute vs Chronic Mechanism of Injury: I. Direct: blow to the patella II. Indirect: planted foot with a valgus
RN(EC) ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT *** - Useful in determining mechanism of injury / overuse
 ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT *** - Useful in determining mechanism of injury / overuse") HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient Sport / Occupation - Certain conditions are more prevalent in particular age groups (Osgood Schlaters in youth / Degenerative Joint Disease
HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient Sport / Occupation - Certain conditions are more prevalent in particular age groups (Osgood Schlaters in youth / Degenerative Joint Disease
Standard of Care: Patellofemoral Pain Syndrome (PFS)
") Department of Rehabilitation Services Physical Therapy Case Type / Diagnosis: Patellofemoral Pain Syndrome (719.46) Patellofemoral Pain syndrome A general category of anterior knee pain from patella malalignment.
Department of Rehabilitation Services Physical Therapy Case Type / Diagnosis: Patellofemoral Pain Syndrome (719.46) Patellofemoral Pain syndrome A general category of anterior knee pain from patella malalignment.
Clinical Evaluation and Imaging of the Patellofemoral Joint Common clinical syndromes
 Clinical Evaluation and Imaging of the Patellofemoral Joint Common clinical syndromes A. Panagopoulos Lecturer in Orthopaedics Medical School, Patras University Objectives Anatomy of patellofemoral joint
Clinical Evaluation and Imaging of the Patellofemoral Joint Common clinical syndromes A. Panagopoulos Lecturer in Orthopaedics Medical School, Patras University Objectives Anatomy of patellofemoral joint
Chapter 20 The knee and related structures
 Chapter 20 The knee and related structures Athletic Training Spring 2014 Jihong Park Bones & joints Femur, tibia, fibula, & patella Femur & tibia Weight bearing & muscle attachment Patella functions Anterior
Chapter 20 The knee and related structures Athletic Training Spring 2014 Jihong Park Bones & joints Femur, tibia, fibula, & patella Femur & tibia Weight bearing & muscle attachment Patella functions Anterior
Anterior knee pain.
 Anterior knee pain What are the symptoms? Anterior knee pain is very common amongst active adolescents and athletes participating in contact sports. It is one of the most common problems/injuries seen
Anterior knee pain What are the symptoms? Anterior knee pain is very common amongst active adolescents and athletes participating in contact sports. It is one of the most common problems/injuries seen
Human anatomy reference:
 Human anatomy reference: Weak Glut Activation Weak gluteal activation comes from poor biomechanics, poor awareness when training or prolonged exposure in deactivated positions such as sitting. Weak Glut
Human anatomy reference: Weak Glut Activation Weak gluteal activation comes from poor biomechanics, poor awareness when training or prolonged exposure in deactivated positions such as sitting. Weak Glut
Anterior Knee Pain in Children. Joseph Chorley, MD Associate Professor, Pediatrics Baylor College of Medicine
 Anterior Knee Pain in Children Joseph Chorley, MD Associate Professor, Pediatrics Baylor College of Medicine Goals and Objectives To learn how to care for patients with chronic knee pain To be able to
Anterior Knee Pain in Children Joseph Chorley, MD Associate Professor, Pediatrics Baylor College of Medicine Goals and Objectives To learn how to care for patients with chronic knee pain To be able to
Balanced Body Movement Principles
 Balanced Body Movement Principles How the Body Works and How to Train it. Module 3: Lower Body Strength and Power Developing Strength, Endurance and Power The lower body is our primary source of strength,
Balanced Body Movement Principles How the Body Works and How to Train it. Module 3: Lower Body Strength and Power Developing Strength, Endurance and Power The lower body is our primary source of strength,
Sports Medicine 15. Unit I: Anatomy. The knee, Thigh, Hip and Groin. Part 4 Anatomies of the Lower Limbs
 Sports Medicine 15 Unit I: Anatomy Part 4 Anatomies of the Lower Limbs The knee, Thigh, Hip and Groin Anatomy of the lower limbs In Part 3 of this section we focused upon 11 of the 12 extrinsic muscles
Sports Medicine 15 Unit I: Anatomy Part 4 Anatomies of the Lower Limbs The knee, Thigh, Hip and Groin Anatomy of the lower limbs In Part 3 of this section we focused upon 11 of the 12 extrinsic muscles
CHAPTER 8: THE BIOMECHANICS OF THE HUMAN LOWER EXTREMITY
 CHAPTER 8: THE BIOMECHANICS OF THE HUMAN LOWER EXTREMITY _ 1. The hip joint is the articulation between the and the. A. femur, acetabulum B. femur, spine C. femur, tibia _ 2. Which of the following is
CHAPTER 8: THE BIOMECHANICS OF THE HUMAN LOWER EXTREMITY _ 1. The hip joint is the articulation between the and the. A. femur, acetabulum B. femur, spine C. femur, tibia _ 2. Which of the following is
DISTANCE RUNNER MECHANICS AMY BEGLEY
 DISTANCE RUNNER MECHANICS AMY BEGLEY FORM Forward motion is thought to be automatic and hard to change. Changing one thing can cause a chain reaction. Can improve: Balance Strength Flexibility Alignment
DISTANCE RUNNER MECHANICS AMY BEGLEY FORM Forward motion is thought to be automatic and hard to change. Changing one thing can cause a chain reaction. Can improve: Balance Strength Flexibility Alignment
7/20/14. Patella Instability. Alignment. PF contact areas. Tissue Restraints. Pain. Acute Blunt force trauma Disorders of the Patellafemoral Joint
 Patella Instability Acute Blunt force trauma Disorders of the Patellafemoral Joint Evan G. Meeks, M.D. Orthopaedic Surgery Sports Medicine The University of Texas - Houston Pivoting action Large effusion
Patella Instability Acute Blunt force trauma Disorders of the Patellafemoral Joint Evan G. Meeks, M.D. Orthopaedic Surgery Sports Medicine The University of Texas - Houston Pivoting action Large effusion
Physical Examination of the Knee
 History: Pain Traumatic vs. atraumatic Acute vs Chronic Mechanism of injury Swelling, catching, instability Previous evaluation and treatment General Setup Examine standing, sitting and supine Evaluate
History: Pain Traumatic vs. atraumatic Acute vs Chronic Mechanism of injury Swelling, catching, instability Previous evaluation and treatment General Setup Examine standing, sitting and supine Evaluate
The Knee. Prof. Oluwadiya Kehinde
 The Knee Prof. Oluwadiya Kehinde www.oluwadiya.sitesled.com The Knee: Introduction 3 bones: femur, tibia and patella 2 separate joints: tibiofemoral and patellofemoral. Function: i. Primarily a hinge joint,
The Knee Prof. Oluwadiya Kehinde www.oluwadiya.sitesled.com The Knee: Introduction 3 bones: femur, tibia and patella 2 separate joints: tibiofemoral and patellofemoral. Function: i. Primarily a hinge joint,
Physical Examination of the Knee
 History: Pain Traumatic vs. atraumatic? Acute vs Chronic Previous procedures done on the knee? Swelling, catching, instability General Setup Examine standing, sitting and supine Evaluate gait Examine hip
History: Pain Traumatic vs. atraumatic? Acute vs Chronic Previous procedures done on the knee? Swelling, catching, instability General Setup Examine standing, sitting and supine Evaluate gait Examine hip
Research Theme. Cal PT Fund Research Symposium 2015 Christopher Powers. Patellofemoral Pain to Pathology Continuum. Applied Movement System Research
 Evaluation and Treatment of Movement Dysfunction: A Biomechanical Approach Research Theme Christopher M. Powers, PhD, PT, FAPTA Understanding injury mechanisms will lead to the development of more effective
Evaluation and Treatment of Movement Dysfunction: A Biomechanical Approach Research Theme Christopher M. Powers, PhD, PT, FAPTA Understanding injury mechanisms will lead to the development of more effective
Anterior Cruciate Ligament (ACL)
") Anterior Cruciate Ligament (ACL) The anterior cruciate ligament (ACL) is one of the 4 major ligament stabilizers of the knee. ACL tears are among the most common major knee injuries in active people of
Anterior Cruciate Ligament (ACL) The anterior cruciate ligament (ACL) is one of the 4 major ligament stabilizers of the knee. ACL tears are among the most common major knee injuries in active people of
Please differentiate an internal derangement from an external knee injury.
 Knee Orthopaedic Tests Sports and Knee Injuries James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Knee Injury Strain, Sprain, Internal Derangement Anatomy of the Knee Please
Knee Orthopaedic Tests Sports and Knee Injuries James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Knee Injury Strain, Sprain, Internal Derangement Anatomy of the Knee Please
World Medical & Health Games
 Management of Patellofemoral Pain Syndrome João Barroso Orthopaedic department ULS Matosinhos Portugal Introduction Anterior Knee Pain affects 1 in 4 athletes very common! (Knowles et al) Patellofemoral
Management of Patellofemoral Pain Syndrome João Barroso Orthopaedic department ULS Matosinhos Portugal Introduction Anterior Knee Pain affects 1 in 4 athletes very common! (Knowles et al) Patellofemoral
Patello-femoral pain
 Patello-femoral pain Dr Keith Holt Patello-femoral pain describes a spectrum of conditions, beginning with the common mild pain coming from under the knee-cap (patella) and extending up to frank arthritis
Patello-femoral pain Dr Keith Holt Patello-femoral pain describes a spectrum of conditions, beginning with the common mild pain coming from under the knee-cap (patella) and extending up to frank arthritis
The Knee. Two Joints: Tibiofemoral. Patellofemoral
 Evaluating the Knee The Knee Two Joints: Tibiofemoral Patellofemoral HISTORY Remember the questions from lecture #2? Girth OBSERVATION TibioFemoral Alignment What are the consequences of faulty alignment?
Evaluating the Knee The Knee Two Joints: Tibiofemoral Patellofemoral HISTORY Remember the questions from lecture #2? Girth OBSERVATION TibioFemoral Alignment What are the consequences of faulty alignment?
Recognizing common injuries to the lower extremity
 Recognizing common injuries to the lower extremity Bones Femur Patella Tibia Tibial Tuberosity Medial Malleolus Fibula Lateral Malleolus Bones Tarsals Talus Calcaneus Metatarsals Phalanges Joints - Knee
Recognizing common injuries to the lower extremity Bones Femur Patella Tibia Tibial Tuberosity Medial Malleolus Fibula Lateral Malleolus Bones Tarsals Talus Calcaneus Metatarsals Phalanges Joints - Knee
Common Conditions and Injuries of the Knee
 Common Conditions and Injuries of the Knee Iliotibial Band (ITB) Syndrome Ø The ITB is fascia, a connective tissue that gives structure to the body. Its function is to protect the knee from sideways movement
Common Conditions and Injuries of the Knee Iliotibial Band (ITB) Syndrome Ø The ITB is fascia, a connective tissue that gives structure to the body. Its function is to protect the knee from sideways movement
W. Dilworth Cannon, M.D. Professor of Clinical Orthopaedic Surgery University of California San Francisco
 Knee Pain And Injuries In Adults W. Dilworth Cannon, M.D. Professor of Clinical Orthopaedic Surgery University of California San Francisco Pain Control Overview Narcotics rarely necessary after 1 st 1-2
Knee Pain And Injuries In Adults W. Dilworth Cannon, M.D. Professor of Clinical Orthopaedic Surgery University of California San Francisco Pain Control Overview Narcotics rarely necessary after 1 st 1-2
RN(EC) ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***
 ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***") HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient - Certain conditions are more prevalent in particular age groups (Hip pain in children may refer to the knee from Legg-Calve-Perthes
HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient - Certain conditions are more prevalent in particular age groups (Hip pain in children may refer to the knee from Legg-Calve-Perthes
Today s session. Common Problems in Rehab. Tim Keeley B.Phty, Cred.MDT, APA Principal Physiotherapist. physiofitness.com.au facebook.
 Tim Keeley B.Phty, Cred.MDT, APA Principal Physiotherapist physiofitness.com.au facebook.com/physiofitness Today s session Essential list for the lower body Rehab starting point Focussing on activation,
Tim Keeley B.Phty, Cred.MDT, APA Principal Physiotherapist physiofitness.com.au facebook.com/physiofitness Today s session Essential list for the lower body Rehab starting point Focussing on activation,
PRIMARY CARE EXAMINATION OF KEY JOINTS. Thomas M. Howard, MD, FACSM FFPC Sports Medicine
 PRIMARY CARE EXAMINATION OF KEY JOINTS Thomas M. Howard, MD, FACSM FFPC Sports Medicine General exam principles: Expose entire joint and opposite limb for comparison Have a Differential Diagnosis Exam
PRIMARY CARE EXAMINATION OF KEY JOINTS Thomas M. Howard, MD, FACSM FFPC Sports Medicine General exam principles: Expose entire joint and opposite limb for comparison Have a Differential Diagnosis Exam
Prevention of common running injuries
 Prevention of common running injuries Lower limb and hip joint pain, along with soft tissue structures of the lower leg, can be extremely painful and frustrating injuries. Some of the most common running
Prevention of common running injuries Lower limb and hip joint pain, along with soft tissue structures of the lower leg, can be extremely painful and frustrating injuries. Some of the most common running
Knee Capsular Disorder. ICD-9-CM: Stiffness in joint of lower leg, not elsewhere classified
 1 Knee Capsular Disorder "Knee Capsulitis" ICD-9-CM: 719.56 Stiffness in joint of lower leg, not elsewhere classified Diagnostic Criteria History: Physical Exam: Stiffness Aching with prolonged weight
1 Knee Capsular Disorder "Knee Capsulitis" ICD-9-CM: 719.56 Stiffness in joint of lower leg, not elsewhere classified Diagnostic Criteria History: Physical Exam: Stiffness Aching with prolonged weight
Overview Ligament Injuries. Anatomy. Epidemiology Very commonly injured joint. ACL Injury 20/06/2016. Meniscus Tears. Patellofemoral Problems
 Overview Ligament Injuries Meniscus Tears Pankaj Sharma MBBS, FRCS (Tr & Orth) Consultant Orthopaedic Surgeon Manchester Royal Infirmary Patellofemoral Problems Knee Examination Anatomy Epidemiology Very
Overview Ligament Injuries Meniscus Tears Pankaj Sharma MBBS, FRCS (Tr & Orth) Consultant Orthopaedic Surgeon Manchester Royal Infirmary Patellofemoral Problems Knee Examination Anatomy Epidemiology Very
Myology of the Knee. PTA 105 Kinesiology
 Myology of the Knee PTA 105 Kinesiology Objectives Describe the planes of motion and axes of rotation of the knee joint Visualize the origins and insertions of the muscles about the knee List the innervations
Myology of the Knee PTA 105 Kinesiology Objectives Describe the planes of motion and axes of rotation of the knee joint Visualize the origins and insertions of the muscles about the knee List the innervations
Evaluating the Athlete Questionnaire
 Evaluating the Athlete Questionnaire Prior to developing the strength and conditioning training plan the coach should first evaluate factors from the athlete s questionnaire that may impact the strength
Evaluating the Athlete Questionnaire Prior to developing the strength and conditioning training plan the coach should first evaluate factors from the athlete s questionnaire that may impact the strength
Dynamic Stabilization of the Patellofemoral Joint: Stabilization from above & below
 Dynamic Stabilization of the Patellofemoral Joint: Stabilization from above & below Division Biokinesiology & Physical Therapy Co Director, oratory University of Southern California Movement Performance
Dynamic Stabilization of the Patellofemoral Joint: Stabilization from above & below Division Biokinesiology & Physical Therapy Co Director, oratory University of Southern California Movement Performance
SPORTSSOCIETY Developing attractive and dynamic societies via sports Project Nr: CB67. Preventative and rehabilitation exercises of sports injures
 Preventative and rehabilitation exercises of sports injures Diagnosis: Plantar Facitis What is Plantar Facitis? Plantar fascitis(pf) is a painful inflammatory process of the plantar fascia, the connective
Preventative and rehabilitation exercises of sports injures Diagnosis: Plantar Facitis What is Plantar Facitis? Plantar fascitis(pf) is a painful inflammatory process of the plantar fascia, the connective
Knee Contusions and Stress Injuries. Laura W. Bancroft, M.D.
 Knee Contusions and Stress Injuries Laura W. Bancroft, M.D. Objectives Review 5 types of contusion patterns Pivot shift Dashboard Hyperextension Clip Lateral patellar dislocation Demonstrate various stress
Knee Contusions and Stress Injuries Laura W. Bancroft, M.D. Objectives Review 5 types of contusion patterns Pivot shift Dashboard Hyperextension Clip Lateral patellar dislocation Demonstrate various stress
Disclosures. Objectives. Overview. Patellofemoral Syndrome. Etiology. Management of Patellofemoral Pain
 Management of Patellofemoral Pain Implications of Top Down Mechanics Disclosures I have no actual or potential conflict of interest in relation to this presentation David Nolan, PT, DPT, MS, OCS, SCS,
Management of Patellofemoral Pain Implications of Top Down Mechanics Disclosures I have no actual or potential conflict of interest in relation to this presentation David Nolan, PT, DPT, MS, OCS, SCS,
Female Athlete Injury Prevention
 Female Athlete Injury Prevention Startling Facts Huge rise in knee ligament injuries among young females engaging in sport and exercise Females athletes participating in jumping and pivoting sports are
Female Athlete Injury Prevention Startling Facts Huge rise in knee ligament injuries among young females engaging in sport and exercise Females athletes participating in jumping and pivoting sports are
2. Iliotibial Band syndrome
 2. Iliotibial Band syndrome Iliotibial band (ITB) syndrome (so called runners knee although often seen in other sports e.g. cyclists and hill walkers). It is usually an overuse injury with pain felt on
2. Iliotibial Band syndrome Iliotibial band (ITB) syndrome (so called runners knee although often seen in other sports e.g. cyclists and hill walkers). It is usually an overuse injury with pain felt on
Rehabilitation for Patellar Tendinitis (jumpers knee) and Patellofemoral Syndrome (chondromalacia patella)
 and Patellofemoral Syndrome (chondromalacia patella)") Rehabilitation for Patellar Tendinitis (jumpers knee) and Patellofemoral Syndrome (chondromalacia patella) Patellar Tendinitis The most common tendinitis about the knee is irritation of the patellar tendon.
Rehabilitation for Patellar Tendinitis (jumpers knee) and Patellofemoral Syndrome (chondromalacia patella) Patellar Tendinitis The most common tendinitis about the knee is irritation of the patellar tendon.
Ligamentous and Meniscal Injuries: Diagnosis and Management
 Ligamentous and Meniscal Injuries: Diagnosis and Management Daniel K Williams, MD Franciscan Physician Network Orthopedic Specialists September 29, 2017 No Financial Disclosures INTRODUCTION Overview of
Ligamentous and Meniscal Injuries: Diagnosis and Management Daniel K Williams, MD Franciscan Physician Network Orthopedic Specialists September 29, 2017 No Financial Disclosures INTRODUCTION Overview of
The Knee. Tibio-Femoral
 The Knee Tibio-Femoral Osteology Distal Femur with Proximal Tibia Largest Joint Cavity in the Body A modified hinge joint with significant passive rotation Technically, one degree of freedom (Flexion/Extension)
The Knee Tibio-Femoral Osteology Distal Femur with Proximal Tibia Largest Joint Cavity in the Body A modified hinge joint with significant passive rotation Technically, one degree of freedom (Flexion/Extension)
Gait Analysis: Qualitative vs Quantitative What are the advantages and disadvantages of qualitative and quantitative gait analyses?
 Gait Analysis: Qualitative vs Quantitative What are the advantages and disadvantages of qualitative and quantitative gait analyses? Basics of Gait Analysis Gait cycle: heel strike to subsequent heel strike,
Gait Analysis: Qualitative vs Quantitative What are the advantages and disadvantages of qualitative and quantitative gait analyses? Basics of Gait Analysis Gait cycle: heel strike to subsequent heel strike,
Musculoskeletal Examination Benchmarks
 Musculoskeletal Examination Benchmarks _ The approach to examining the musculoskeletal system is the same no matter what joint or limb is being examined. The affected and contralateral region should both
Musculoskeletal Examination Benchmarks _ The approach to examining the musculoskeletal system is the same no matter what joint or limb is being examined. The affected and contralateral region should both
Jumper s Knee in Children and Adolescents
 A Patient s Guide to Jumper s Knee in Children and Adolescents 2350 Royal Boulevard Suite 200 Elgin, IL 60123 Phone: 847.931.5300 Fax: 847.931.9072 DISCLAIMER: The information in this booklet is compiled
A Patient s Guide to Jumper s Knee in Children and Adolescents 2350 Royal Boulevard Suite 200 Elgin, IL 60123 Phone: 847.931.5300 Fax: 847.931.9072 DISCLAIMER: The information in this booklet is compiled
Subluxation of the Patella
 Subluxation of the Patella Alexandra Zaldivar December 15, 2011 2011 Course, Los Angeles Abstract After reading information from the Internet and anatomy books, it becomes very clear why pilates is an
Subluxation of the Patella Alexandra Zaldivar December 15, 2011 2011 Course, Los Angeles Abstract After reading information from the Internet and anatomy books, it becomes very clear why pilates is an
Solutions for. Patello-femoral knee pain. Today s session. physiofitness.com.au facebook.
 Solutions for Patello-femoral knee pain presented by Tim Keeley B.Phty, Cred.MDT, APAM Principal Physiotherapist Physio Fitness Australia physiofitness.com.au facebook.com/physiofitness Today s session
Solutions for Patello-femoral knee pain presented by Tim Keeley B.Phty, Cred.MDT, APAM Principal Physiotherapist Physio Fitness Australia physiofitness.com.au facebook.com/physiofitness Today s session
Objectives. The BIG Joint. Case 1. Boney Architecture. Presenter Disclosure Information. Common Knee Problems
 3:30 4:15 pm Common Knee Problems SPEAKER Christopher J. Visco, MD Presenter Disclosure Information The following relationships exist related to this presentation: Christopher J. Visco, MD: Speaker s Bureau
3:30 4:15 pm Common Knee Problems SPEAKER Christopher J. Visco, MD Presenter Disclosure Information The following relationships exist related to this presentation: Christopher J. Visco, MD: Speaker s Bureau
Anatomy. ACL PCL MCL LCL Meniscus. Medial Lateral
 Skis for Knees Anatomy ACL PCL MCL LCL Meniscus Medial Lateral Knee Anatomy THE KNEE HISTORY Pain (PQRST) Contact vs noncontact Effusions Mechanical symptoms Locking Instability (falls) Initial treatment
Skis for Knees Anatomy ACL PCL MCL LCL Meniscus Medial Lateral Knee Anatomy THE KNEE HISTORY Pain (PQRST) Contact vs noncontact Effusions Mechanical symptoms Locking Instability (falls) Initial treatment
Peggers Super Summaries: PFJ
 Patellofemoral Joint: ANATOMY: Largest sesamoid ossifying at 3-5 years of age Multiple foci having a sec ossification centre SUPEROLATERAL Helps increase moment arm PATELLOFEMORAL OA Incidence 10% of knee
Patellofemoral Joint: ANATOMY: Largest sesamoid ossifying at 3-5 years of age Multiple foci having a sec ossification centre SUPEROLATERAL Helps increase moment arm PATELLOFEMORAL OA Incidence 10% of knee
Do Persons with PFP. PFJ Loading? Biomechanical Factors Contributing to Patellomoral Pain: The Dynamic Q Angle. Patellofemoral Pain: A Critical Review
 Biomechanical Factors Contributing to Patellomoral Pain: The Dynamic Q Angle Division Biokinesiology & Physical Therapy Co Director, oratory University of Southern California Movement Performance Institute
Biomechanical Factors Contributing to Patellomoral Pain: The Dynamic Q Angle Division Biokinesiology & Physical Therapy Co Director, oratory University of Southern California Movement Performance Institute
APPLICATION OF THE MOVEMENT SYSTEMS MODEL TO THE MANAGEMENT COMMON HIP PATHOLOGIES
 APPLICATION OF THE MOVEMENT SYSTEMS MODEL TO THE MANAGEMENT COMMON HIP PATHOLOGIES Tracy Porter, PT, DPT Des Moines University Department of Physical Therapy Objectives Review current literature related
APPLICATION OF THE MOVEMENT SYSTEMS MODEL TO THE MANAGEMENT COMMON HIP PATHOLOGIES Tracy Porter, PT, DPT Des Moines University Department of Physical Therapy Objectives Review current literature related
THE LOWER EXTREMITY EXAM FOR THE FAMILY PRACTITIONER
 THE LOWER EXTREMITY EXAM FOR THE FAMILY PRACTITIONER Melinda A. Scott, D.O. Orthopedic Associates of Dayton Board Certified in Primary Care Sports Medicine GOALS Identify landmarks necessary for exam of
THE LOWER EXTREMITY EXAM FOR THE FAMILY PRACTITIONER Melinda A. Scott, D.O. Orthopedic Associates of Dayton Board Certified in Primary Care Sports Medicine GOALS Identify landmarks necessary for exam of
Goals &Objectives. 1. Review the anatomy of the knee 2. Practice your hands-on skills 3. By the end of the workshop:
 Clinical Knee Exam Goals &Objectives 1. Review the anatomy of the knee 2. Practice your hands-on skills 3. By the end of the workshop: Be able to categorize knee injuries Understand the significance of
Clinical Knee Exam Goals &Objectives 1. Review the anatomy of the knee 2. Practice your hands-on skills 3. By the end of the workshop: Be able to categorize knee injuries Understand the significance of
Powers Hip Strengthening Program
 Powers Hip Strengthening Program The Powers Program is an evidenced based exercise progression developed by Chris Powers, PT, PHD from the University of Southern California. Powers and colleagues have
Powers Hip Strengthening Program The Powers Program is an evidenced based exercise progression developed by Chris Powers, PT, PHD from the University of Southern California. Powers and colleagues have
The Problem of Patellofemoral Pain. The Low Back Pain of the Lower Extremity. Objectives. Christopher M. Powers, PhD, PT, FACSM, FAPTA
 Mechanisms Underlying Patellofemoral Joint Pain: What have we learned over the last 20 years? Professor Co Director, Musculoskeletal Biomechanics Research Laboratory Objectives 1. Highlight recent research
Mechanisms Underlying Patellofemoral Joint Pain: What have we learned over the last 20 years? Professor Co Director, Musculoskeletal Biomechanics Research Laboratory Objectives 1. Highlight recent research
APTA Intro to Identity. The Movement System The Kinesiopathologic Model Movement System Impairment Syndromes of the Knee THE HUMAN MOVEMENT SYSTEM
 The Movement System The Kinesiopathologic Model Movement System Impairment Syndromes of the Knee Shirley Sahrmann, PT, PhD, FAPTA Professor Emerita Statement of Privacy To protect the privacy of the subjects
The Movement System The Kinesiopathologic Model Movement System Impairment Syndromes of the Knee Shirley Sahrmann, PT, PhD, FAPTA Professor Emerita Statement of Privacy To protect the privacy of the subjects
Knee Multiligament Rehabilitation
 Knee Multiligament Rehabilitation Orlando Valle, PT, MSPT, SCS, CSCS Director Ironman Sports Medicine Institute TMC Orlando.Valle@memorialhermann.org 4 Major Ligaments ACL PCL MCL LCL (PLC) Anatomy Function
Knee Multiligament Rehabilitation Orlando Valle, PT, MSPT, SCS, CSCS Director Ironman Sports Medicine Institute TMC Orlando.Valle@memorialhermann.org 4 Major Ligaments ACL PCL MCL LCL (PLC) Anatomy Function
The effect of patellofemoral pain syndrome on the hip and knee neuromuscular control on dynamic postural control task
 The University of Toledo The University of Toledo Digital Repository Theses and Dissertations 2009 The effect of patellofemoral pain syndrome on the hip and knee neuromuscular control on dynamic postural
The University of Toledo The University of Toledo Digital Repository Theses and Dissertations 2009 The effect of patellofemoral pain syndrome on the hip and knee neuromuscular control on dynamic postural
The psoas minor is medial to the psoas major. The iliacus is a fan-shaped muscle that when contracted helps bring the swinging leg forward in walking
 1 p.177 2 3 The psoas minor is medial to the psoas major. The iliacus is a fan-shaped muscle that when contracted helps bring the swinging leg forward in walking and running. The iliopsoas and adductor
1 p.177 2 3 The psoas minor is medial to the psoas major. The iliacus is a fan-shaped muscle that when contracted helps bring the swinging leg forward in walking and running. The iliopsoas and adductor
Running Injuries in Children and Adolescents
 Running Injuries in Children and Adolescents Cook Children s SPORTS Symposium July 2, 2014 Running Injuries Overuse injuries Acute injuries Anatomic conditions 1 Overuse Injuries Pain that cannot be tied
Running Injuries in Children and Adolescents Cook Children s SPORTS Symposium July 2, 2014 Running Injuries Overuse injuries Acute injuries Anatomic conditions 1 Overuse Injuries Pain that cannot be tied
Non Surgical Management Of Hip And Knee Osteoarthritis Toolkit. Evaluation and Diagnosis of Osteoarthritis in Primary Care
 Non Surgical Management Of Hip And Knee Osteoarthritis Toolkit Evaluation and Diagnosis of Osteoarthritis in Primary Care OA-HxPE-716.indd 1 TABLE OF CONTENTS HISTORY TAKING... 3 EVALUATION OF SUSPECTED
Non Surgical Management Of Hip And Knee Osteoarthritis Toolkit Evaluation and Diagnosis of Osteoarthritis in Primary Care OA-HxPE-716.indd 1 TABLE OF CONTENTS HISTORY TAKING... 3 EVALUATION OF SUSPECTED
Running Injuries. Rebecca Christenson
 Running Injuries Rebecca Christenson Improve your time? Don t get injured! Think about your training graph Recovery Causes of Overuse Injuries Biomechanics Sudden increase in training Poor recovery strategies
Running Injuries Rebecca Christenson Improve your time? Don t get injured! Think about your training graph Recovery Causes of Overuse Injuries Biomechanics Sudden increase in training Poor recovery strategies
Patellofemoral Pain Syndrome
 43 Thames Street, St Albans, Christchurch 8013 Phone: (03) 356 1353. Website: philip-bayliss.com Patellofemoral Pain Syndrome Patellofemoral pain syndrome can be defined as a Retro-patellar (behind the
43 Thames Street, St Albans, Christchurch 8013 Phone: (03) 356 1353. Website: philip-bayliss.com Patellofemoral Pain Syndrome Patellofemoral pain syndrome can be defined as a Retro-patellar (behind the
The Knee. Clarification of Terms. Osteology of the Knee 7/28/2013. The knee consists of: The tibiofemoral joint Patellofemoral joint
 The Knee Clarification of Terms The knee consists of: The tibiofemoral joint Patellofemoral joint Mansfield, p273 Osteology of the Knee Distal Femur Proximal tibia and fibula Patella 1 Osteology of the
The Knee Clarification of Terms The knee consists of: The tibiofemoral joint Patellofemoral joint Mansfield, p273 Osteology of the Knee Distal Femur Proximal tibia and fibula Patella 1 Osteology of the
Sustained a sprained ankle
 Student Name : Student s Number : 3. Q 1. 2. Sustained a sprained ankle 1. List at least 3 key items you should ask during the history portion of an examination ( ) Possible Answers and Anything Else you
Student Name : Student s Number : 3. Q 1. 2. Sustained a sprained ankle 1. List at least 3 key items you should ask during the history portion of an examination ( ) Possible Answers and Anything Else you
Biomechanics of the Knee. Valerie Nuñez SpR Frimley Park Hospital
 Biomechanics of the Knee Valerie Nuñez SpR Frimley Park Hospital Knee Biomechanics Kinematics Range of Motion Joint Motion Kinetics Knee Stabilisers Joint Forces Axes The Mechanical Stresses to which
Biomechanics of the Knee Valerie Nuñez SpR Frimley Park Hospital Knee Biomechanics Kinematics Range of Motion Joint Motion Kinetics Knee Stabilisers Joint Forces Axes The Mechanical Stresses to which
A Patient s Guide to Patellofemoral Problems
 A Patient s Guide to Patellofemoral Problems 2350 Royal Boulevard Suite 200 Elgin, IL 60123 Phone: 847.931.5300 Fax: 847.931.9072 DISCLAIMER: The information in this booklet is compiled from a variety
A Patient s Guide to Patellofemoral Problems 2350 Royal Boulevard Suite 200 Elgin, IL 60123 Phone: 847.931.5300 Fax: 847.931.9072 DISCLAIMER: The information in this booklet is compiled from a variety
ChiroCredit.com Presents Biomechanics: Focus on
 ChiroCredit.com Presents Biomechanics: Focus on the Knee Presented by: Ivo Waerlop, DC Shawn Allen, DC 1 Focus on The Knee 2 Pertinent Anatomy Femur Tibia Fibula Patella Prepatellar bursa Infrapatellar
ChiroCredit.com Presents Biomechanics: Focus on the Knee Presented by: Ivo Waerlop, DC Shawn Allen, DC 1 Focus on The Knee 2 Pertinent Anatomy Femur Tibia Fibula Patella Prepatellar bursa Infrapatellar
ACL Athletic Career. ACL Rupture - Warning Features Intensive pain Immediate swelling Locking Feel a Pop Dead leg Cannot continue to play
 FIMS Ambassador Tour to Eastern Europe, 2004 Belgrade, Serbia Montenegro Acute Knee Injuries - Controversies and Challenges Professor KM Chan OBE, JP President of FIMS Belgrade ACL Athletic Career ACL
FIMS Ambassador Tour to Eastern Europe, 2004 Belgrade, Serbia Montenegro Acute Knee Injuries - Controversies and Challenges Professor KM Chan OBE, JP President of FIMS Belgrade ACL Athletic Career ACL
Exercises to Correct Muscular Imbalances. presented by: Darrell Barnes, LAT, ATC, CSCS
 Exercises to Correct Muscular Imbalances presented by: Darrell Barnes, LAT, ATC, CSCS Objectives Review Functional Anatomy Identify physical imbalances that lead to injury and/or decrease performance
Exercises to Correct Muscular Imbalances presented by: Darrell Barnes, LAT, ATC, CSCS Objectives Review Functional Anatomy Identify physical imbalances that lead to injury and/or decrease performance
Prevention and Treatment of Injuries. Anatomy. Anatomy. Chapter 20 The Knee Westfield High School Houston, Texas
 Prevention and Treatment of Injuries Chapter 20 The Knee Westfield High School Houston, Texas Anatomy MCL, Medial Collateral Ligament LCL, Lateral Collateral Ligament PCL, Posterior Cruciate Ligament ACL,
Prevention and Treatment of Injuries Chapter 20 The Knee Westfield High School Houston, Texas Anatomy MCL, Medial Collateral Ligament LCL, Lateral Collateral Ligament PCL, Posterior Cruciate Ligament ACL,
Doron Sher. 160 Belmore Rd, Randwick Burwood Rd, Concord. MBBS, MBiomedE, FRACS FAOrthA
 Doron Sher MBBS, MBiomedE, FRACS FAOrthA 160 Belmore Rd, Randwick 47 49 Burwood Rd, Concord www.kneedoctor.com.au www.orthosports.com.au Medial PatelloFemoral (MPFL) And AnteroLateral Ligament (ALL) Reconstruction
Doron Sher MBBS, MBiomedE, FRACS FAOrthA 160 Belmore Rd, Randwick 47 49 Burwood Rd, Concord www.kneedoctor.com.au www.orthosports.com.au Medial PatelloFemoral (MPFL) And AnteroLateral Ligament (ALL) Reconstruction
Patellofemoral Pathology
 Patellofemoral Pathology Matthew Murray, MD UT Health Science Center/UT Medicine Sports Medicine and Arthroscopic Surgery I have disclosed that I am a consultant for Biomet Orthopaedics. Anterior Knee
Patellofemoral Pathology Matthew Murray, MD UT Health Science Center/UT Medicine Sports Medicine and Arthroscopic Surgery I have disclosed that I am a consultant for Biomet Orthopaedics. Anterior Knee
During the initial repair and inflammatory phase, focus should be on placing the lower limbs in a position to ensure that:
 The Anatomy Dimensions series of tutorials and workbooks is aimed at improving anatomical and pathological understanding for body movement professionals. It is ideal for teachers in disciplines such as
The Anatomy Dimensions series of tutorials and workbooks is aimed at improving anatomical and pathological understanding for body movement professionals. It is ideal for teachers in disciplines such as
FIT IN LINE EXAMPLE REPORT (15/03/11) THE WHITE HOUSE PHYSIOTHERAPY CLINIC PRESENT
 THE WHITE HOUSE PHYSIOTHERAPY CLINIC PRESENT") THE WHITE HOUSE PHYSIOTHERAPY CLINIC PRESENT FIT IN LINE EXAMPLE REPORT (15/03/11) A 12 part assessment tool to screen your athletic performance in 4 key components: Flexibility, Balance, Strength & Core
THE WHITE HOUSE PHYSIOTHERAPY CLINIC PRESENT FIT IN LINE EXAMPLE REPORT (15/03/11) A 12 part assessment tool to screen your athletic performance in 4 key components: Flexibility, Balance, Strength & Core
ANATYOMY OF The thigh
 ANATYOMY OF The thigh 1- Lateral cutaneous nerve of the thigh Ι) Skin of the thigh Anterior view 2- Femoral branch of the genitofemoral nerve 1, 2 and 3 are From the lumber plexus 5- Intermediate cutaneous
ANATYOMY OF The thigh 1- Lateral cutaneous nerve of the thigh Ι) Skin of the thigh Anterior view 2- Femoral branch of the genitofemoral nerve 1, 2 and 3 are From the lumber plexus 5- Intermediate cutaneous
The Hip Joint. Shenequia Howard David Rivera
 The Hip Joint Shenequia Howard David Rivera Topics Of Discussion Movement Bony Anatomy Ligamentous Anatomy Muscular Anatomy Origin/Insertion/Action/Innervation Common Injuries MOVEMENT Flexion Extension
The Hip Joint Shenequia Howard David Rivera Topics Of Discussion Movement Bony Anatomy Ligamentous Anatomy Muscular Anatomy Origin/Insertion/Action/Innervation Common Injuries MOVEMENT Flexion Extension
In the name of god. Knee. By: Tofigh Bahraminia Graduate Student of the Pathology Sports and corrective actions. Heat: Dr. Babakhani. Nov.
 In the name of god Knee By: Tofigh Bahraminia Graduate Student of the Pathology Sports and corrective actions Heat: Dr. Babakhani Nov. 2014 1 Anatomy-Bones Bones Femur Medial/lateral femoral condyles articulate
In the name of god Knee By: Tofigh Bahraminia Graduate Student of the Pathology Sports and corrective actions Heat: Dr. Babakhani Nov. 2014 1 Anatomy-Bones Bones Femur Medial/lateral femoral condyles articulate
Why does it matter? Patellar Instability 7/23/2018. What is the current operation de jour? Common. Poorly taught. Poorly treated
 Patellar Instability It s Really Not That Difficult! David Shneider MD East Lansing, MI www.patellamdcom Detroit Sports Medicine Foundation July 2018 Why does it matter? Common Poorly taught Poorly treated
Patellar Instability It s Really Not That Difficult! David Shneider MD East Lansing, MI www.patellamdcom Detroit Sports Medicine Foundation July 2018 Why does it matter? Common Poorly taught Poorly treated
Hip Region. PHTY2020: Lecture
 Region PHTY2020: Lecture 2.1 29.02.16 Functional Overview Transfer body weight form trunk to legs Allows leg to adopt numerous positions needed for standing, walking running, stairs, sitting and other
Region PHTY2020: Lecture 2.1 29.02.16 Functional Overview Transfer body weight form trunk to legs Allows leg to adopt numerous positions needed for standing, walking running, stairs, sitting and other
Female Athlete Knee Injury
 Female Athlete Knee Injury Kelly C. McInnis, DO Physical Medicine and Rehabilitation Massachusetts General Hospital Sports Medicine Center Outline Historical Perspective Gender-specific movement patterns
Female Athlete Knee Injury Kelly C. McInnis, DO Physical Medicine and Rehabilitation Massachusetts General Hospital Sports Medicine Center Outline Historical Perspective Gender-specific movement patterns
The hip: Built for endurance and mobility
 The hip: Built for endurance and mobility The hip joint Some anatomical landmarks Innominate Ilium, pubis, ischium Sacrum Iliac crests Asis Psis Pubic tubercle Acetabulum Femur Head of femur Neck of femur
The hip: Built for endurance and mobility The hip joint Some anatomical landmarks Innominate Ilium, pubis, ischium Sacrum Iliac crests Asis Psis Pubic tubercle Acetabulum Femur Head of femur Neck of femur
Keys to the Office Based Evaluation of the Youth Runner
 Keys to the Office Based Evaluation of the Youth Runner Michelle Cappello, PT, SCS Clinical Director of Physical Therapy and Athletic Training Sports Medicine Center for Young Athletes UCSF Benioff Children
Keys to the Office Based Evaluation of the Youth Runner Michelle Cappello, PT, SCS Clinical Director of Physical Therapy and Athletic Training Sports Medicine Center for Young Athletes UCSF Benioff Children
ARTHROSCOPIC LABRAL REPAIR WITH CAPSULAR PLICATION PHYSICAL THERAPY PROTOCOL
 ARTHROSCOPIC LABRAL REPAIR WITH CAPSULAR PLICATION PHYSICAL THERAPY PROTOCOL Jovan R. Laskovski, M.D. Hip Arthroscopy Sports Medicine & Orthopaedic Surgery Crystal Clinic Orthopaedic Center Please use
ARTHROSCOPIC LABRAL REPAIR WITH CAPSULAR PLICATION PHYSICAL THERAPY PROTOCOL Jovan R. Laskovski, M.D. Hip Arthroscopy Sports Medicine & Orthopaedic Surgery Crystal Clinic Orthopaedic Center Please use
P-F Biomechanics and Function Conservative Approaches
 P-F Biomechanics and Function Conservative Approaches Russ Paine, PT Memorial Hermann Ironman Sportsmedicine Institute Memorial Hermann Hospital Houston, Texas Function - Patella Increase moment arm Quadriceps
P-F Biomechanics and Function Conservative Approaches Russ Paine, PT Memorial Hermann Ironman Sportsmedicine Institute Memorial Hermann Hospital Houston, Texas Function - Patella Increase moment arm Quadriceps
Jennifer L. Cook, MD
 Jennifer L. Cook, MD Florida Joint Replacement and Sports Medicine Center 5243 Hanff Lane New Port Richey, FL 34652 Phone: (727)848-4249 Fax: (727) 841-8934 ANTERIOR CRUCIATE LIGAMENT RECONSTRUCTION POST-OPERATIVE
Jennifer L. Cook, MD Florida Joint Replacement and Sports Medicine Center 5243 Hanff Lane New Port Richey, FL 34652 Phone: (727)848-4249 Fax: (727) 841-8934 ANTERIOR CRUCIATE LIGAMENT RECONSTRUCTION POST-OPERATIVE
Knee Joint Assessment and General View
 Knee Joint Assessment and General View Done by; Mshari S. Alghadier BSc Physical Therapy RHPT 366 m.alghadier@sau.edu.sa http://faculty.sau.edu.sa/m.alghadier/ Functional anatomy The knee is the largest
Knee Joint Assessment and General View Done by; Mshari S. Alghadier BSc Physical Therapy RHPT 366 m.alghadier@sau.edu.sa http://faculty.sau.edu.sa/m.alghadier/ Functional anatomy The knee is the largest
Evaluation of Knee Problems
 Evaluation of Knee Problems OBJECTIVES Review knee anatomy Explain tests to look for pathology Briefly introduce knee problems Only by a thorough knowledge of anatomy and functional testing can one make
Evaluation of Knee Problems OBJECTIVES Review knee anatomy Explain tests to look for pathology Briefly introduce knee problems Only by a thorough knowledge of anatomy and functional testing can one make
Human Anatomy, First Edition McKinley & O'Loughlin
 Human Anatomy, First Edition McKinley & O'Loughlin Chapter 8 : Appendicular Skeleton 8-1 Appendicular Skeleton Includes the bones of the upper and lower limbs. The girdles of bones that attach the upper
Human Anatomy, First Edition McKinley & O'Loughlin Chapter 8 : Appendicular Skeleton 8-1 Appendicular Skeleton Includes the bones of the upper and lower limbs. The girdles of bones that attach the upper
Evaluation of the Hip and Knee
 Evaluation of the Hip and Knee Causes of hip pain RA Osteoarthritis Psoriatic arthritis Septic arthritis Bursitis Hip fx Labral tear Tendinitis Referred back pain Cancer AVN Legg-Calve-Perthes Paget's
Evaluation of the Hip and Knee Causes of hip pain RA Osteoarthritis Psoriatic arthritis Septic arthritis Bursitis Hip fx Labral tear Tendinitis Referred back pain Cancer AVN Legg-Calve-Perthes Paget's
I have nothing to disclose
 Management of Common Knee Disorders: What You Knee d to Know UCSF Essentials of Women s Health July 8, 2015 Carlin Senter, M.D. I have nothing to disclose Learning objectives: in 1 hour you will be able
Management of Common Knee Disorders: What You Knee d to Know UCSF Essentials of Women s Health July 8, 2015 Carlin Senter, M.D. I have nothing to disclose Learning objectives: in 1 hour you will be able
Apply this knowledge into proper management strategies and referrals
 1 2 3 Lower Extremity Injuries Jason Kennedy, M.D. Disclosures I have no financial/ industry disclosures. Objectives Identify common lower extremity injury patterns in the child and adolescent Apply this
1 2 3 Lower Extremity Injuries Jason Kennedy, M.D. Disclosures I have no financial/ industry disclosures. Objectives Identify common lower extremity injury patterns in the child and adolescent Apply this
Knee Injury Assessment
 Knee Injury Assessment Clinical Anatomy p. 186 Femur Medial condyle Lateral condyle Femoral trochlea Tibia Intercondylar notch Tibial tuberosity Tibial plateau Fibula Fibular head Patella Clinical Anatomy
Knee Injury Assessment Clinical Anatomy p. 186 Femur Medial condyle Lateral condyle Femoral trochlea Tibia Intercondylar notch Tibial tuberosity Tibial plateau Fibula Fibular head Patella Clinical Anatomy
Copyright Vanderbilt Sports Medicine. Table of Contents. The Knee Cap and Knee Joint...2. What is Patellofemoral Pain?...4
 Table of Contents The Knee Cap and Knee Joint...2 What is Patellofemoral Pain?....4 What to Expect From a Medical Evaluation....6 What to Expect After Therapy....7 1 The Kneecap and Knee Joint The knee
Table of Contents The Knee Cap and Knee Joint...2 What is Patellofemoral Pain?....4 What to Expect From a Medical Evaluation....6 What to Expect After Therapy....7 1 The Kneecap and Knee Joint The knee
Muscle Testing of Knee Extensors. Yasser Moh. Aneis, PhD, MSc., PT. Lecturer of Physical Therapy Basic Sciences Department
 Muscle Testing of Knee Extensors Yasser Moh. Aneis, PhD, MSc., PT. Lecturer of Physical Therapy Basic Sciences Department Muscle Testing of Knee Extensors othe Primary muscle Quadriceps Femoris -Rectus
Muscle Testing of Knee Extensors Yasser Moh. Aneis, PhD, MSc., PT. Lecturer of Physical Therapy Basic Sciences Department Muscle Testing of Knee Extensors othe Primary muscle Quadriceps Femoris -Rectus
Knee Movement Coordination Deficits. ICD-9-CM: Sprain of cruciate ligament of knee
 1 Knee Movement Coordination Deficits Anterior Cruciate Ligament ACL Tear ICD-9-CM: 844.2 Sprain of cruciate ligament of knee ACL Insufficiency ICD-9-CM: 717.83 Old disruption of anterior cruciate ligament
1 Knee Movement Coordination Deficits Anterior Cruciate Ligament ACL Tear ICD-9-CM: 844.2 Sprain of cruciate ligament of knee ACL Insufficiency ICD-9-CM: 717.83 Old disruption of anterior cruciate ligament
Other Culprits in Knee Dysfunction
 Unraveling the Mystery of Knee Pain #6: Other Culprits in Knee Dysfunction 1 Webinar Goals Explore the assessment and treatment of other culprits in knee dysfunction. 2 Time: 60 minutes Schedule: Logistics
Unraveling the Mystery of Knee Pain #6: Other Culprits in Knee Dysfunction 1 Webinar Goals Explore the assessment and treatment of other culprits in knee dysfunction. 2 Time: 60 minutes Schedule: Logistics
Checklist for Physical Examination of the Knee Muscuoskeletal Block -- Chris McGrew MD, Andrew Ashbaugh DO
 Checklist for Physical Examination of the Knee Muscuoskeletal Block -- Chris McGrew MD, Andrew Ashbaugh DO This handout is for use as a rough guide and study aid. Your instructor may perform certain maneuvers
Checklist for Physical Examination of the Knee Muscuoskeletal Block -- Chris McGrew MD, Andrew Ashbaugh DO This handout is for use as a rough guide and study aid. Your instructor may perform certain maneuvers