Initial Pelvic Fracture Management. Patrick M Reilly MD FACS February 27, 2010
|
|
|
- Rudolf Chase
- 6 years ago
- Views:
Transcription
1 Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010

2 John Pryor MD
3 Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions Bleeding Disorder Anticoagulants ACS-COT 1999
4 Field Triage* * Step One : Physiology Increased / Decreased Heart Rate Decreased Blood Pressure Increased / Decreased Resp Rate Decreased Mental Status ACS-COT 1999
5 Field Triage* * Step Two : Anatomy Penetrating Trauma Head / Neck / Torso / Proximal Extremities Significant Ortho Injuries Paralysis Amputation Proximal to Wrist & Ankle Burn Issues ACS-COT 1999
6 Field Triage* * Step Three : Mechanism Falls > 20 Feet Rollover High Speed Crash Ejection Others ACS-COT 1999
7 Field Triage* * Step Two : Anatomy Penetrating Trauma Head / Neck / Torso / Proximal Extremities Significant Ortho Injuries Paralysis Amputation Proximal to Wrist & Ankle Burn Issues ACS-COT 1999
8 Pelvic Fractures in PA * May 2001 PTSF Report - 5 Year Review * 9% of all PTOS Patients 10% of all HUP PTOS Patients * Mean Hospital LOS 11.3 days * Mean Hospital LOS - HUP 13.7 days
9 Pelvic Fractures in PA * Multiple Injuries Mean ISS - PTOS 12.7 Mean ISS - Pelvis 18.7 Mean ISS - Pelvis/HUP 20.5 * Head Injury 30% * Torso Injury 40% * Upper Ext Fracture 26% * Lower Ext Fracture 31%
10 Pelvic Fractures in PA * Complications PTOS 16% PTOS / Pelvis 30% * Mortality PTOS 7.4% PTOS / Pelvis 9.6% PTOS / Pelvis / HUP 9.3% Pelvis - ISS > 34 50%

11 Anatomy Close Apposition of Vital Structures iliac artery and vein superior gluteal artery bladder/prostate rectum/vagina sacral plexus


12 Anatomy No Inherent Stability Without Ligaments anterior symphysis pubis sacrotuberous and sacrospinous ligaments posterior anterior SI ligament posterior SI ligament iliolumbar ligament


13 Exam of Pelvis Deformity of pelvis Leg length difference Abrasions/swelling over pelvis Scrotal/labial swelling GU--blood at meatus Stability--pelvic rock and push pull Rectal exam-- perineal tears prostate position
14 Pelvic Fracture Recommendations Mechanical Stability (Difficult to Assess) Asymmetry of Legs Pain in Pelvis Pain on Hip Motion Swelling / Tenderness at Symphysis Prehospital & Disaster Med 2007

15 Stabilization for Transport Reducing Pain Circumferential Compression of Pelvis Sheet or Binder Spine Board / Collar Bind Legs Together Prehospital & Disaster Med 2007

16 Prehospital Diagnosis Difficult Altered Mental Status Pelvic Pain Complaint Most Common Pain on Exam Exam Unreliable Importance of Mechanism of Injury Emergency Medicine Journal 2007

17 Emergency Medicine Journal 2007
18 Trauma Pelvic Orthodic Device
19 TPOD - Potential Advantages Stabilizes Pelvis Closes Pelvic Volume Noninvasive Rapid Angiography and Laparotomy Compatible

20
21
22
23 TPOD - HUP Data 23 patients Imaging After TPOD and Definitive Fixation No Difference: Pubic Diastasis Pelvic Cross-Sectional Area Pelvic Volume AAST 2003
24 TPOD - Data 93 TPOD vs 93 EX-Fix patients TPOD Group Less Transfusion Shorter LOS Decreased Mortality (26% vs 37%)* * p=0.11 JACS 2007


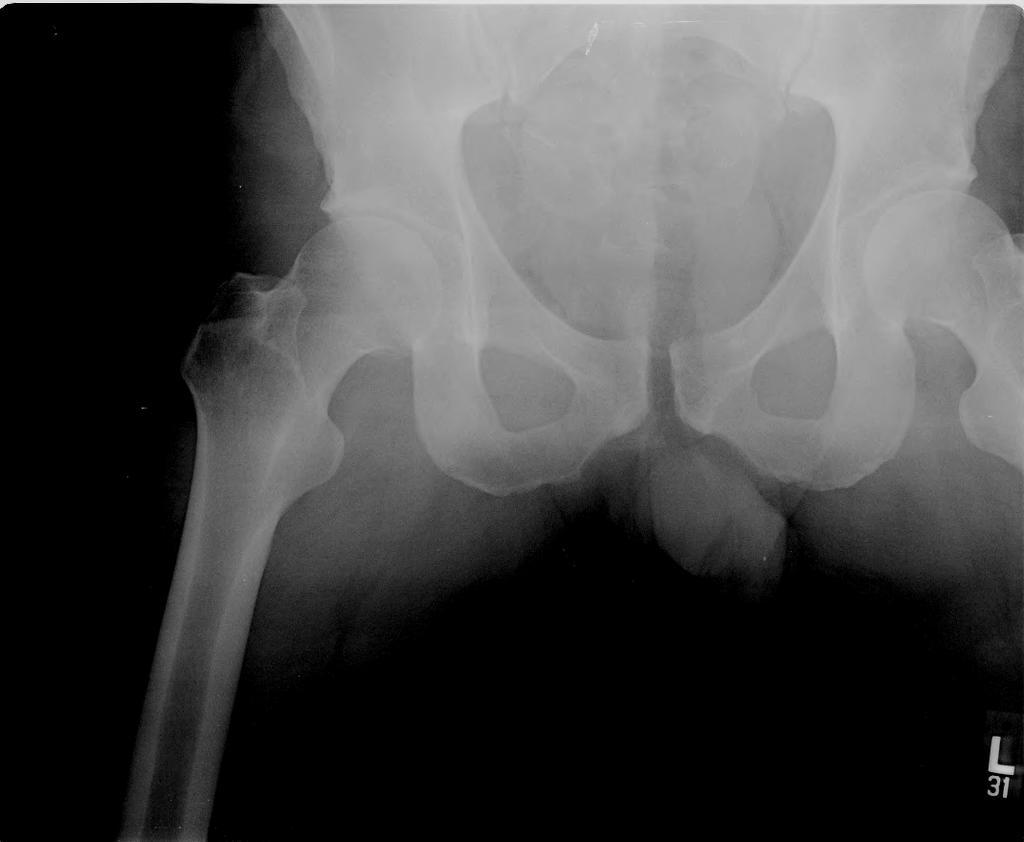
25 Follow ATLS principles (ABC S) Evaluation Primary and secondary survey Find source of bleeding Major lacerations Occult chest--cxr abdomen--dpl / FAST pelvis--ap pelvis

26 Radiographic Evaluation AP pelvis--adequate initial evaluation for 90-95% cases
27 Pelvic X-ray ATLS Recommendation All blunt trauma patients Pelvic architecture Hemodynamically significant fractures Hip dislocation

28 Radiographic Evaluation CT--best view of posterior ring
29 CT Abdomen/Pelvis Commonly used diagnostic modality Rapid interpretation Solid organs Retroperitoneal structures Orthopedic injuries
30 Flow Chart Blunt Trauma Hemodynamically Stable yes Reliable Physical Exam yes Positive Physical Findings no CT planned yes No PXR
31 Flow Chart Blunt Trauma Hemodynamically Stable no PXR no yes Reliable Physical Exam yes PXR Positive Physical Findings yes PXR no CT planned yes No PXR

32 Positive Physical Exam


33 Acute Stabilization Methods Tied sheet Sand bags Lateral decubitus positioning Traction MAST Trousers External Fixation Pelvic clamp

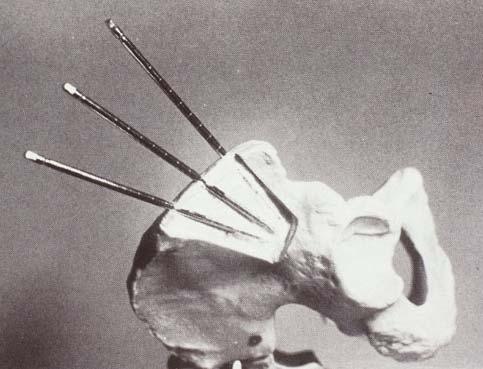
34 External Fixation
 21% vs 41% Overall mortality 6% vs 26% Mortality with closed head")
35 External Fixation vs MAST Hemorrhage control 95% vs 71% success Transfusion 3.7u vs 7.4u prbc Mortality (hypotensives) 21% vs 41% Overall mortality 6% vs 26% Mortality with closed head injury 7% vs 43%


36 Pelvic Clamp
37 Trauma Pelvic Orthodic Device
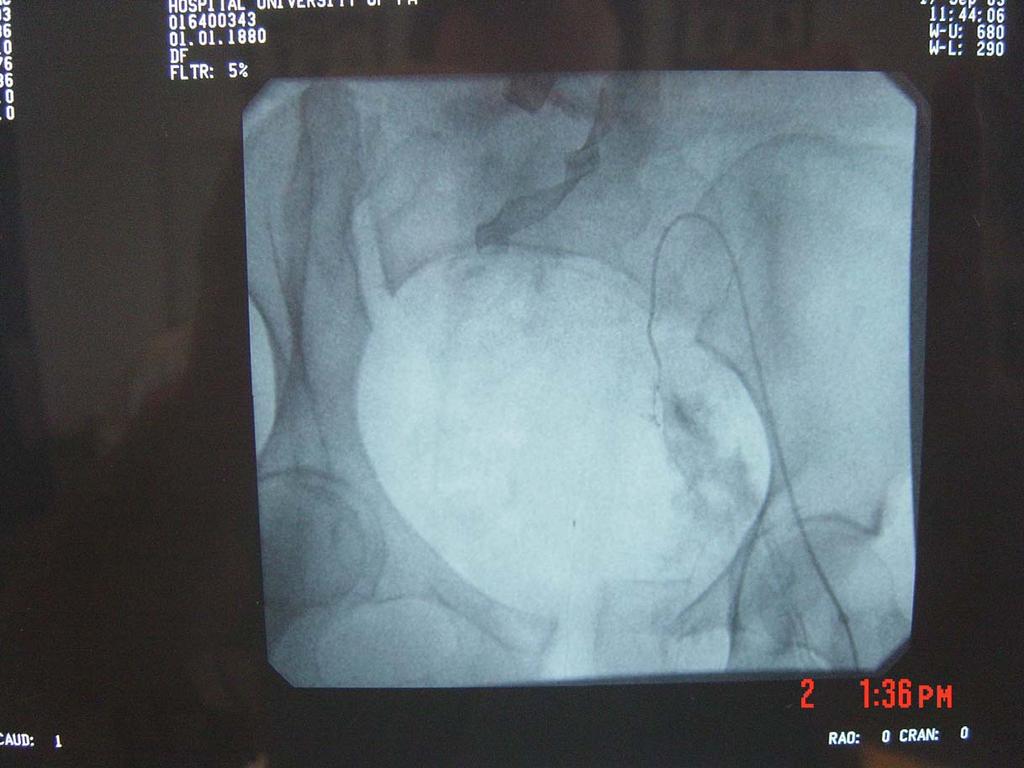
38 Ongoing Hypotension : Now What? Chest Source Abdominal Source FAST Exam Supra-umbilical DPL Gross Blood Negative - Angiography

39 Arteriography Persistent Hemodynamic Instability

40 Arteriography Contrast Extravasation
41 CT Contrast Extravasation 604 Patients 42 Contrast Extravasation 26 Angiograms 19 IR Contrast Extravasation 45% Positive Rate 562 No Contrast Extravasation 6 Angiograms 2 IR Contrast Extravasation 0.4% Positive Rate J Trauma 2007
42 Ongoing Evolution of IR * Traditional - Diagnostic Tool Penetrating Proximity Injuries Neck Trans - Mediastinum / Pelvis Extremity Blunt Aorta
43 Ongoing Evolution of IR * Traditional - Patient Population Hemodynamically Stable Potential for Significant Injury Statistically Low Trauma Surgeon Role Coffee / Donuts Nap
44 Ongoing Evolution of IR * Current - Therapeutic Tool Bleeding Control Pelvis Solid Organs Soft Tissue Vascular Patency Subclavian
45 Ongoing Evolution of IR * Current - Patient Population Hemodynamically Unstable/Meta-Stable Potential for Significant Injury They Have It Trauma Surgeon Role Direct Resuscitation Team Leader
46 Ongoing Evolution of IR : HUP Data Patients Angio/100 PT * % Therapeutic 10% 22%* *p < 0.05 AAST 2003
47 IR Therapy : Data * Vascular Patency Case Reports Case Series * Hemorrhage Control Retrospective Reports
48 IR Therapy : Data - Liver * 40 DC patients * 37 complete medical records * 19/37 (51%) had hepatic injuries * 8/19 patients (42%) underwent angiography 7 post-operatively 1 pre-operatively
49 AAST Grading of Hepatic Injuries 8 * AG- AG+ I II III IV *p= < 0. 01
50 IR Therapy : Data - Liver Operative Phase Parameter AG+ AG- p value LpH LBE LTemp (C) SBP (mmhg)
51 IR Therapy : Data - Liver Operative Phase Fluid AG+ AG- p value Cryst (L/hour) PRBC (units/hour) FFP (units/hour) Plts (units/hour)
52 IR Therapy : Data - Liver Angiographic Phase * Angiography in 8/19 patients (42%) * Overall therapeutic embolization rate 87% * All AG patients were AAST grade IV * No rebleeding
53 IR Therapy : Data - Liver ICU Arrival Parameter AG+ AG- p value ph BE LAC Temp PT
54 IR Therapy : Data * LA County / USC * Intraperitoneal * Retroperitoneal * 7 Year Review Increased Utilization over Time Period World J Surg 2000
55 * 137 Patients IR Therapy : Data 97 Pelvis 26 Liver 12 Kidney * 102 Attempted Embolizations 91% Success Rate * No Major Morbidity Reported World J Surg 2000
56 IR Setup * Trauma Team Present - Continuously * Dedicated Critical Care Nurse * Hypothermia Measures * Trauma Team Leader Maintains Role Think Ortho Relationship The ICU is taken to the patient in IR
57 Repeat Angiography * Ongoing Hemorrhage * 31/678 IR for Pelvic Fractures 16 Embolized 3 Repeat Embolization 15 Negative Studies 5 Repeat Angiography J Trauma Initial Embolization
58 Other Options Direct Preperitoneal Packing J Trauma 2007

59 Retrospective Review 20 Patients per Group Faster to Intervention Less Transfusion Requirements Trend Towards Improved Survival Injury 2009
60 J Trauma 2008 What To Do?
61 Who Do You Call? Blood Bank Interventional Radiology Operating Room? Not Orthopaedic Surgery Emergently
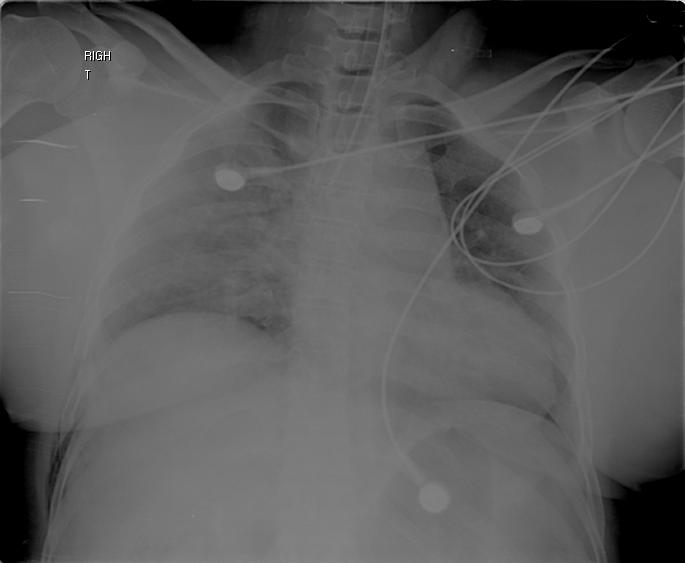
62 Trauma Patient 641/04 Prehospital Unrestrained Driver MVC Multiple Injuries RSI Prehospital PennStar
63 Trauma Patient 641/04 Primary Survey A = Intubated B = Bilateral BS C = Weak L Pedal Pulses; No Pulses on R D = GCS 3 E = Done
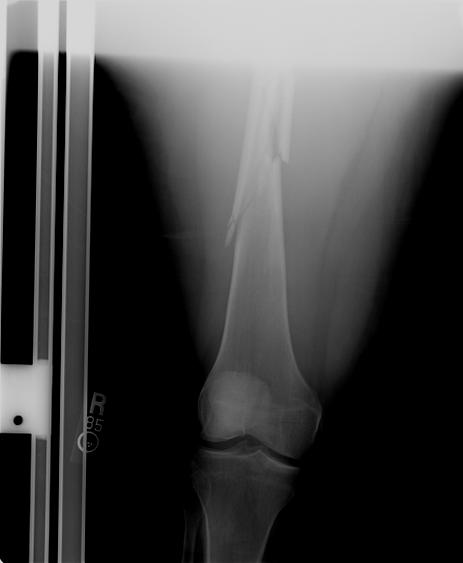
64 Trauma Patient 641/04 Secondary Survey Hypotensive R Chest Crepitance Pelvic Instability R Leg Deformities
65 Trauma Patient 641/04 Dx and Simultaneous Tx CXR Pelvic Xray FAST IV Access Volume
66
67
68




69
70 Trauma Patient 641/04 Treatment and Decision Making R Chest Tube TPOD Trauma Exsanguination Protocol Rapid Head CT OR - Laparotomy IR Notification
71 Trauma Patient 641/04 Operating Room 35 Minutes Post Arrival Mesenteric Injury Splenic Injury Pelvic Hematoma Damage Control
72 Trauma Patient 641/04 Operating Room OR Labs ph 7.02 Base Excess Hgb 6.0 ica 0.54
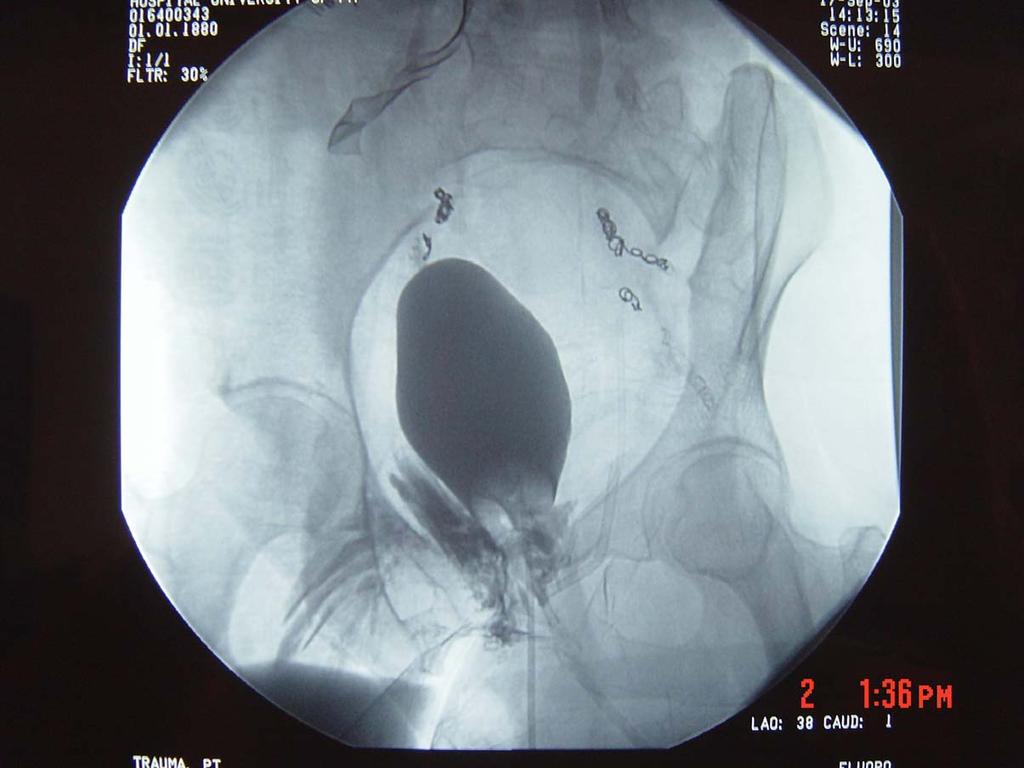
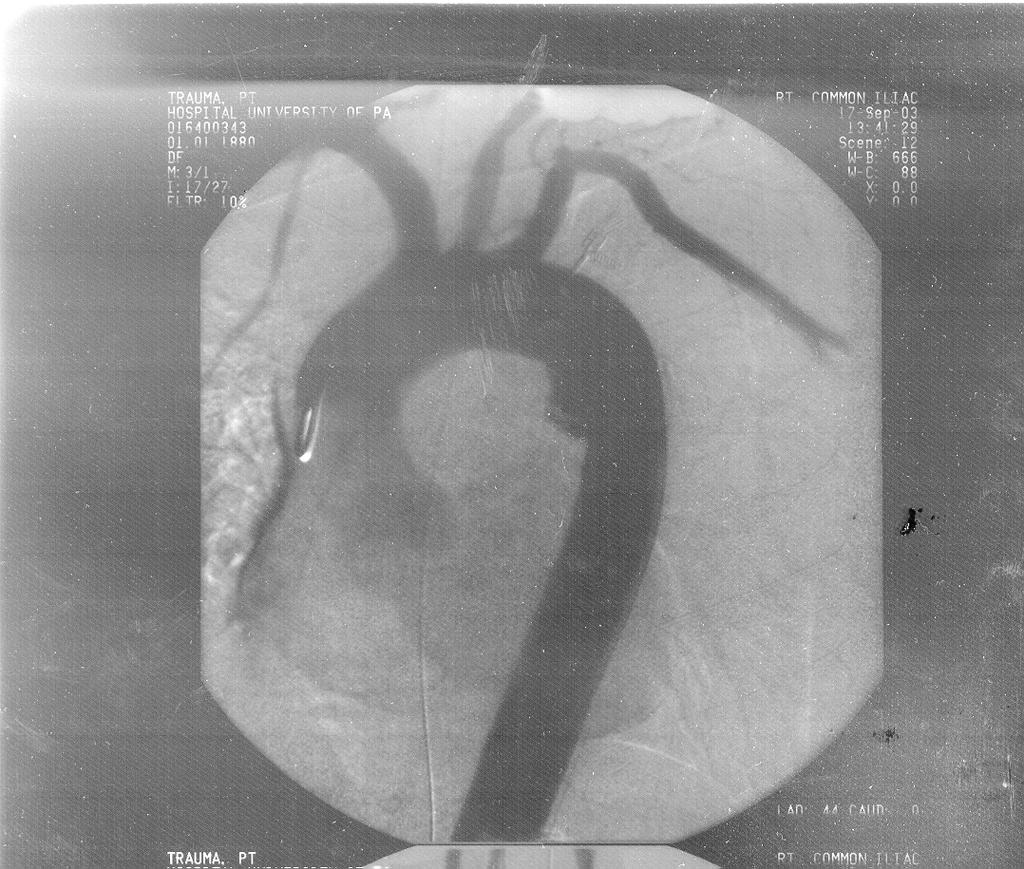
73 Trauma Patient 641/04 Interventional Radiology Bleeding Control Further Diagnostic Studies R Leg Aorta Bladder Ongoing Resuscitation
74

75
76
77
78 Trauma Patient 641/04 Intensive Care Unit Ongoing Resuscitation Cold / Coagulopathic Ongoing Bleeding R Chest Fractures Abdomen Factor VIIa
79 Trauma Patient 641/04 Intensive Care Unit Eventual Physiologic Capture Definitive Fracture Care Definitive Aortic Repair Slow Improvement Neurologically Intact ISS = 50
80 Trauma Patient 641/04 Initial 24 o Blood Requirements* 41 Units prbcs 16 Units Plasma 4 Units Stored Plasma 12 Units FFP 7-4 Packs Platelets * Actually.14 hours
81 Conclusion Pelvic Fractures - Severe Injuries CT vs Pelvic Film in Select Patients CT in Trauma Bay? TPOD Angiography During Resuscitation

82
Management of Pelvic Fracture
 Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
The Acute Management of Pelvic Ring Injuries
 The Acute Management of Pelvic Ring Injuries Brian J Ladner, MD North Oaks Medical Center Original Author: Kyle F. Dickson, MD; Created March 2004 Sean E. Nork, MD; Revised December 2010 New Author: October
The Acute Management of Pelvic Ring Injuries Brian J Ladner, MD North Oaks Medical Center Original Author: Kyle F. Dickson, MD; Created March 2004 Sean E. Nork, MD; Revised December 2010 New Author: October
Pelvic fractures. Dr Raymond Yean, MBBS Surgical SRMO
 Pelvic fractures Dr Raymond Yean, MBBS Surgical SRMO PELVIC FRACTURES Pelvic fracture account for 2-8% all skeletal injuries Associated with High energy trauma Soft tissue injuries and blood loss. Shock,
Pelvic fractures Dr Raymond Yean, MBBS Surgical SRMO PELVIC FRACTURES Pelvic fracture account for 2-8% all skeletal injuries Associated with High energy trauma Soft tissue injuries and blood loss. Shock,
10/2/2018. Acute Management of Pelvic Injuries. Learning Objectives. 17 yo male ped struck by truck
 17 yo male ped struck by truck Acute Management of Pelvic Injuries David Volgas, MD CoxHealth University of Missouri HD unstable Open pelvic wound superior gluteal fold through rectum to scrotum Open rami
17 yo male ped struck by truck Acute Management of Pelvic Injuries David Volgas, MD CoxHealth University of Missouri HD unstable Open pelvic wound superior gluteal fold through rectum to scrotum Open rami
Guidelines and Protocols
 TITLE: PELVIC TRAUMA PURPOSE: Develop a protocol of care that will insure rapid identification and treatment of these patients PROCESS: I. CARE OF PATIENTS WITH PELVIC TRAUMA A. Patients in hemorrhagic
TITLE: PELVIC TRAUMA PURPOSE: Develop a protocol of care that will insure rapid identification and treatment of these patients PROCESS: I. CARE OF PATIENTS WITH PELVIC TRAUMA A. Patients in hemorrhagic
utility of Plain Film Pelvic Radiographs in Blunt Trauma Patients in the Emergency Department
 utility of Plain Film Pelvic Radiographs in Blunt Trauma Patients in the Emergency Department AMAL KAMIL OBAID, M.D., ANDREW BARLEBEN, M.D., DIANA PORRAL, B.S., STEPHANIE LUSH, M.S.N., MARIANNE CINAT,
utility of Plain Film Pelvic Radiographs in Blunt Trauma Patients in the Emergency Department AMAL KAMIL OBAID, M.D., ANDREW BARLEBEN, M.D., DIANA PORRAL, B.S., STEPHANIE LUSH, M.S.N., MARIANNE CINAT,
Management of Bleeding Pelvic Fractures
 Management of Bleeding Pelvic Fractures Clay Cothren Burlew, MD FACS Professor of Surgery Program Director, SCC and TACS Fellowships Director, Surgical Intensive Care Unit Denver Health Medical Center/University
Management of Bleeding Pelvic Fractures Clay Cothren Burlew, MD FACS Professor of Surgery Program Director, SCC and TACS Fellowships Director, Surgical Intensive Care Unit Denver Health Medical Center/University
Initial Management of Pelvic Injuries
 Initial Management of Pelvic Injuries Olav Røise, MD, PhD Chairman Division of Neuroscience and Skeletal Medicine Ullevål University Hospital Trauma treatment Represent a chain of health services in which
Initial Management of Pelvic Injuries Olav Røise, MD, PhD Chairman Division of Neuroscience and Skeletal Medicine Ullevål University Hospital Trauma treatment Represent a chain of health services in which
SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad
,Ph.D Dr.Evo Elidar Sp.Rad") SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad Trauma Emergency Room layout Ideally the trauma emergency room is centrally located to provide
SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad Trauma Emergency Room layout Ideally the trauma emergency room is centrally located to provide
Damage Control in Abdominal and Pelvic Injuries
 Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Haemodynamic deterioration in lateral compression pelvic fracture after prehospital pelvic circumferential compression device application
 Haemodynamic deterioration in lateral compression pelvic fracture after prehospital pelvic circumferential compression device application Authors Alan A Garner Retrieval consultant CareFlight Northmead,
Haemodynamic deterioration in lateral compression pelvic fracture after prehospital pelvic circumferential compression device application Authors Alan A Garner Retrieval consultant CareFlight Northmead,
Major Trauma Scenarios. Ballarat Health Services Emergency Medicine Training Hub
 Major Trauma Scenarios Ballarat Health Services Emergency Medicine Training Hub Trauma Scenario 1 You receive a phone call from the ambulance service. They have a 27 yr old male involved in a MCA, he is
Major Trauma Scenarios Ballarat Health Services Emergency Medicine Training Hub Trauma Scenario 1 You receive a phone call from the ambulance service. They have a 27 yr old male involved in a MCA, he is
MANAGEMENT OF SOLID ORGAN INJURIES
 MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
THE INITIAL MANAGEMENT OF PELVIC AND ACETABULAR TRAUMA LOUIS LEBLOND MD FRCSC DEPT OF ORTHOPAEDICS THE MONCTON HOSPITAL - L HÔPITAL DE MONCTON
 THE INITIAL MANAGEMENT OF PELVIC AND ACETABULAR TRAUMA LOUIS LEBLOND MD FRCSC DEPT OF ORTHOPAEDICS THE MONCTON HOSPITAL - L HÔPITAL DE MONCTON DISCLOSURES + BACKGROUND No. Centre de formation médicale
THE INITIAL MANAGEMENT OF PELVIC AND ACETABULAR TRAUMA LOUIS LEBLOND MD FRCSC DEPT OF ORTHOPAEDICS THE MONCTON HOSPITAL - L HÔPITAL DE MONCTON DISCLOSURES + BACKGROUND No. Centre de formation médicale
Shock and Resuscitation: Part II. Patrick M Reilly MD FACS Professor of Surgery
 Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
Abdominal Trauma. Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital
 Abdominal Trauma Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital overview Quick review abdominal anatomy Review of mechanism of injury Review of investigation
Abdominal Trauma Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital overview Quick review abdominal anatomy Review of mechanism of injury Review of investigation
Pelvic Injuries. Chapter 21
 Chapter 21 Introduction Injuries of the pelvis are an uncommon, but potentially lethal, battlefield injury. Blunt injuries may be associated with major hemorrhage and early mortality. Death within the
Chapter 21 Introduction Injuries of the pelvis are an uncommon, but potentially lethal, battlefield injury. Blunt injuries may be associated with major hemorrhage and early mortality. Death within the
Imaging in the Trauma Patient
 Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
Clinical Module. Pelvic Injury Trauma. Princess Alexandra Hospital Emergency Department. 1 Introduction
 Princess Alexandra Hospital Emergency Department Clinical Module Trauma Review Officers: Katherine Isoardi / Glenn Ryan Version no: 2 Review date: Aug 2015 Key Words: Pelvic Trauma, Pelvic Injury, Pelvic
Princess Alexandra Hospital Emergency Department Clinical Module Trauma Review Officers: Katherine Isoardi / Glenn Ryan Version no: 2 Review date: Aug 2015 Key Words: Pelvic Trauma, Pelvic Injury, Pelvic
EAST MULTICENTER STUDY DATA DICTIONARY. Temporary Intravascular Shunt Study Data Dictionary
 EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
UBC Department of Urologic Sciences Lecture Series. Urological Trauma
 UBC Department of Urologic Sciences Lecture Series Urological Trauma Disclaimer: This is a lot of information to cover and we are unlikely to cover it all today These slides are to be utilized for your
UBC Department of Urologic Sciences Lecture Series Urological Trauma Disclaimer: This is a lot of information to cover and we are unlikely to cover it all today These slides are to be utilized for your
Pelvic Fractures. AOCP National Course Belfast City Hospital. 11 th June D Swain BSc; FRCSI; FRCS (Orth.)
") Pelvic Fractures AOCP National Course Belfast City Hospital 11 th June 2010 Who s this bloke? Consultant orthopaedic surgeon RVH Trained in Belfast, England and Toronto Interests - pelvic and acetabular
Pelvic Fractures AOCP National Course Belfast City Hospital 11 th June 2010 Who s this bloke? Consultant orthopaedic surgeon RVH Trained in Belfast, England and Toronto Interests - pelvic and acetabular
Pan Scan Instead of Clinical Exam? David A. Spain, MD
 Pan Scan Instead of Clinical Exam? David A. Spain, MD Granted, some patients don t t need CT scan Platinum Package Stanford Special CT Scan Head Neck Chest Abdomen Pelvis Takes about 20 minutes to do
Pan Scan Instead of Clinical Exam? David A. Spain, MD Granted, some patients don t t need CT scan Platinum Package Stanford Special CT Scan Head Neck Chest Abdomen Pelvis Takes about 20 minutes to do
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours
 Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
DATA COLLECTION AND MANAGEMENT
 DATA COLLECTION AND MANAGEMENT PURPOSE To specify the components of the data collection and management processes. RELATED POLICIES Patient Care Record, # 8115; Quality Improvement and System Evaluation,
DATA COLLECTION AND MANAGEMENT PURPOSE To specify the components of the data collection and management processes. RELATED POLICIES Patient Care Record, # 8115; Quality Improvement and System Evaluation,
RESUSCITATION IN TRAUMA. Important things I have learnt
 RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
Hemostatic Resuscitation in Trauma. Joanna Davidson, MD 6/6/2012
 Hemostatic Resuscitation in Trauma { Joanna Davidson, MD 6/6/2012 Case of HM 28 yo M arrives CCH trauma bay 5/27/12 at 241 AM Restrained driver in low speed MVC after getting shot in the chest Arrived
Hemostatic Resuscitation in Trauma { Joanna Davidson, MD 6/6/2012 Case of HM 28 yo M arrives CCH trauma bay 5/27/12 at 241 AM Restrained driver in low speed MVC after getting shot in the chest Arrived
Bladder Trauma Data Collection Sheet
 Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Management of the Trauma Patient. Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015
 Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
2. Blunt abdominal Trauma
 Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
Surgical Approaches for Fractures and Injuries of the Pelvic Ring
 Surgical Approaches for Fractures and Injuries of the Pelvic Ring Mara L. Schenker, MD Emory University / Grady Hospital Created by Steven A. Olson, MD in 2004 and Kyle Dickson, MD in 2004 First revised
Surgical Approaches for Fractures and Injuries of the Pelvic Ring Mara L. Schenker, MD Emory University / Grady Hospital Created by Steven A. Olson, MD in 2004 and Kyle Dickson, MD in 2004 First revised
Trauma CT Scanning Protocol
 Northern Trauma Network Trauma CT Scanning Protocol Background Whole body CT (WBCT) has assumed a pivotal position in trauma management. UK trauma is typically described as blunt and blind i.e. blunt trauma
Northern Trauma Network Trauma CT Scanning Protocol Background Whole body CT (WBCT) has assumed a pivotal position in trauma management. UK trauma is typically described as blunt and blind i.e. blunt trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Blunt Abdominal Trauma Evaluation and Management Guideline PEDIATRIC Practice Management Guideline Contact: Trauma Center
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Blunt Abdominal Trauma Evaluation and Management Guideline PEDIATRIC Practice Management Guideline Contact: Trauma Center
Damage Control Resuscitation. VGH Trauma Rounds 2018 Harvey Hawes
 Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
Gunshot Wounds to the Abdomen: From Bullet to Incision. Patrick M Reilly MD FACS
 Gunshot Wounds to the Abdomen: From Bullet to Incision Patrick M Reilly MD FACS Master? I Do Get The Chance to Practice What Are We Not Discussing? Stab Wounds Prehospital Care Management of Specific Injuries
Gunshot Wounds to the Abdomen: From Bullet to Incision Patrick M Reilly MD FACS Master? I Do Get The Chance to Practice What Are We Not Discussing? Stab Wounds Prehospital Care Management of Specific Injuries
Trauma Registry Documentation December 16, 2014
 Trauma Registry Documentation December 16, 2014 The State of Florida now requires ALL Acute Care hospitals to submit data to the statetrauma Registry. Although Baptist Health hospitals are NOT Trauma Centers
Trauma Registry Documentation December 16, 2014 The State of Florida now requires ALL Acute Care hospitals to submit data to the statetrauma Registry. Although Baptist Health hospitals are NOT Trauma Centers
 International Trauma Life Support for Prehospital Care Providers Sixth Edition Patricia M. Hicks, MS, NREMTP Roy Alson, PhD, MD, FACEP Donna Hastings, EMT-P John Emory Campbell, MD, FACEP and Alabama Chapter,
International Trauma Life Support for Prehospital Care Providers Sixth Edition Patricia M. Hicks, MS, NREMTP Roy Alson, PhD, MD, FACEP Donna Hastings, EMT-P John Emory Campbell, MD, FACEP and Alabama Chapter,
Delayed Splenic Rupture After Non-Operative Management of Blunt Splenic Injury A AAST Multi-Institutional Prospective Trial Data Collection Tool
 Delayed Splenic Rupture After Non-Operative Management of Blunt Splenic Injury A AAST Multi-Institutional Prospective Trial Data Collection Tool Enrolling Center: Patient Number (sequential within center):
Delayed Splenic Rupture After Non-Operative Management of Blunt Splenic Injury A AAST Multi-Institutional Prospective Trial Data Collection Tool Enrolling Center: Patient Number (sequential within center):
Penetrating Neck Injuries. Jason Levine MD Lutheran Medical Center July 22, 2010
 Penetrating Neck Injuries Jason Levine MD Lutheran Medical Center July 22, 2010 CASE PRESENTATION 19 YO M 3 Stab Wounds Right zone I neck SW 2 SW anterior abdomen Left epigastrium anterior axillary line
Penetrating Neck Injuries Jason Levine MD Lutheran Medical Center July 22, 2010 CASE PRESENTATION 19 YO M 3 Stab Wounds Right zone I neck SW 2 SW anterior abdomen Left epigastrium anterior axillary line
Financial Disclosure. Objectives 9/24/2018
 Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Evaluation & Management of Penetrating Wounds to the NECK
 Evaluation & Management of Penetrating Wounds to the NECK Goal Effectively identify patients with a high probability of injury requiring surgical intervention Define the role of diagnostic tests in assessing
Evaluation & Management of Penetrating Wounds to the NECK Goal Effectively identify patients with a high probability of injury requiring surgical intervention Define the role of diagnostic tests in assessing
Chapter 39 Trauma in the Elderly
 Chapter 39 Trauma in the Elderly Episode Overview 1) 5 Risk Factors for falls in the elderly? 2) What anatomic and physiologic changes in the elderly patient are important for the management of trauma
Chapter 39 Trauma in the Elderly Episode Overview 1) 5 Risk Factors for falls in the elderly? 2) What anatomic and physiologic changes in the elderly patient are important for the management of trauma
ER-REBOA Patient Selection, the Procedure, and Outcomes Joseph Ibrahim, MD FACS Trauma Medical Director Orlando Regional Medical Center
 ER-REBOA Patient Selection, the Procedure, and Outcomes Joseph Ibrahim, MD FACS Trauma Medical Director Orlando Regional Medical Center Disclosures Speaking Consultant with Prytime Medical Outline Mechanism
ER-REBOA Patient Selection, the Procedure, and Outcomes Joseph Ibrahim, MD FACS Trauma Medical Director Orlando Regional Medical Center Disclosures Speaking Consultant with Prytime Medical Outline Mechanism
ATLS: Initial Assessment and Management. SAUSHEC Medical Student Lecture Series
 ATLS: Initial Assessment and Management SAUSHEC Medical Student Lecture Series Objectives Identify sequence of priorities in assessing the multiply injured patient Apply principles outlined in primary
ATLS: Initial Assessment and Management SAUSHEC Medical Student Lecture Series Objectives Identify sequence of priorities in assessing the multiply injured patient Apply principles outlined in primary
A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion
 A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion Christopher Butts PhD, DO Surgical Critical Care Fellow Cooper University Hospital H&P 10 year old female presents as a trauma
A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion Christopher Butts PhD, DO Surgical Critical Care Fellow Cooper University Hospital H&P 10 year old female presents as a trauma
EMS System for Metropolitan Oklahoma City and Tulsa 2019 Medical Control Board Treatment Protocols
 EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
vel 2 Level 2 3,034 c-spine evaluations with CSR Level 3 detected injury only 53% of the time. Level 3 False (-) rate 47%
 rate 47%") Objectives Blunt and Penetrating Neck Trauma Julie Mayglothling, MD, FACEP Virginia Commonwealth University Richmond, VA Summit to Sound, May 20 th, 2011 Blunt Neck Trauma Evaluation of the low mechanism,
Objectives Blunt and Penetrating Neck Trauma Julie Mayglothling, MD, FACEP Virginia Commonwealth University Richmond, VA Summit to Sound, May 20 th, 2011 Blunt Neck Trauma Evaluation of the low mechanism,
Delayed Presentation of Traumatic Bladder Injury: A case report and review of current treatment trends
 ISPUB.COM The Internet Journal of Urology Volume 5 Number 1 Delayed Presentation of Traumatic Bladder Injury: A case report and review of current treatment trends S Deem, C Lavender, S Agarwal Citation
ISPUB.COM The Internet Journal of Urology Volume 5 Number 1 Delayed Presentation of Traumatic Bladder Injury: A case report and review of current treatment trends S Deem, C Lavender, S Agarwal Citation
REBOA - Real World. Lena M. Napolitano, MD
 REBOA - Real World Lena M. Napolitano, MD Lena M. Napolitano MD, FACS Massey Foundation Professor of Surgery Acute Care Surgery [Trauma, Burn, Critical Care, Emergency Surgery] University of Michigan Ann
REBOA - Real World Lena M. Napolitano, MD Lena M. Napolitano MD, FACS Massey Foundation Professor of Surgery Acute Care Surgery [Trauma, Burn, Critical Care, Emergency Surgery] University of Michigan Ann
Trauma Activation 7/18/17
 Blunt Rupture of the Thoracic Duct after Severe Thoracic Trauma Samuel Brown, MD Trauma Activation 7/18/17 53 year old male, rear end MVC, exited vehicle and was struck by a semi truck. Denies LOC, complaints
Blunt Rupture of the Thoracic Duct after Severe Thoracic Trauma Samuel Brown, MD Trauma Activation 7/18/17 53 year old male, rear end MVC, exited vehicle and was struck by a semi truck. Denies LOC, complaints
TEVAR for trauma is here to stay: Advances in the Treatment of Blunt Thoracic Aortic Injury
 TEVAR for trauma is here to stay: Advances in the Treatment of Blunt Thoracic Aortic Injury Megan Brenner MD MS RPVI FACS Associate Professor of Surgery Division of Trauma/Surgical Critical Care, RA Cowley
TEVAR for trauma is here to stay: Advances in the Treatment of Blunt Thoracic Aortic Injury Megan Brenner MD MS RPVI FACS Associate Professor of Surgery Division of Trauma/Surgical Critical Care, RA Cowley
West Yorkshire Major Trauma Network Clinical Guidelines 2015
 WYMTN: Pelvic fracture with urogenital trauma KEY RECOMMENDATIONS 1. During the initial exploratory survey / secondary survey, a. The external urethral meatus and the transurethral bladder catheter (if
WYMTN: Pelvic fracture with urogenital trauma KEY RECOMMENDATIONS 1. During the initial exploratory survey / secondary survey, a. The external urethral meatus and the transurethral bladder catheter (if
Pediatric Abdomen Trauma
 Pediatric Abdomen Trauma Susan D. John, MD, FACR Pediatric Trauma Trauma is leading cause of death and disability in children and adolescents Causes and effects vary between age groups Blunt trauma predominates
Pediatric Abdomen Trauma Susan D. John, MD, FACR Pediatric Trauma Trauma is leading cause of death and disability in children and adolescents Causes and effects vary between age groups Blunt trauma predominates
Focused History and Physical Examination of the
 Henry: EMT Prehospital Care, Revised 3 rd Edition Lecture Notes Chapter 10: Focused History and Physical Examination of Trauma Patients Chapter 10 Focused History and Physical Examination of the Trauma
Henry: EMT Prehospital Care, Revised 3 rd Edition Lecture Notes Chapter 10: Focused History and Physical Examination of Trauma Patients Chapter 10 Focused History and Physical Examination of the Trauma
2 Blunt Abdominal Trauma
 2 Blunt Abdominal Trauma Ricardo Ferrada, Diego Rivera, and Paula Ferrada Pearls and Pitfalls Patients suffering a high-energy trauma have solid viscera rupture in the abdomen and/or aortic rupture in
2 Blunt Abdominal Trauma Ricardo Ferrada, Diego Rivera, and Paula Ferrada Pearls and Pitfalls Patients suffering a high-energy trauma have solid viscera rupture in the abdomen and/or aortic rupture in
D. Pre-Hospital Trauma Triage and Bypass Algorithm
 D. Pre-Hospital Trauma Triage and Bypass Algorithm Hospital bypass is defined as transporting the patient to the nearest hospital that has the appropriate level of care for the patient s suspected severity
D. Pre-Hospital Trauma Triage and Bypass Algorithm Hospital bypass is defined as transporting the patient to the nearest hospital that has the appropriate level of care for the patient s suspected severity
Interventional Radiology for Solid Organ Trauma. Case Study 8/17/2017. Diagnosis? Case Study (cont d)
") Interventional Radiology for Solid Organ Trauma Jamie Gallivan RN, BSN Interventional Radiology Case Study 6 y/o boy fell out of 2 nd story window onto concrete Hemodynamically stable at scene Arrival
Interventional Radiology for Solid Organ Trauma Jamie Gallivan RN, BSN Interventional Radiology Case Study 6 y/o boy fell out of 2 nd story window onto concrete Hemodynamically stable at scene Arrival
Pediatric Aspects of Advanced Trauma Life Support: Transition from EMS to the Trauma Room PEDIATRIC TRAUMA DIRECTOR, HASBRO CHILDREN S HOSPITAL
 Pediatric Aspects of Advanced Trauma Life Support: Transition from EMS to the Trauma Room HALE WILLS, MD PEDIATRIC TRAUMA DIRECTOR, HASBRO CHILDREN S HOSPITAL Objectives 1. Identify the critical components
Pediatric Aspects of Advanced Trauma Life Support: Transition from EMS to the Trauma Room HALE WILLS, MD PEDIATRIC TRAUMA DIRECTOR, HASBRO CHILDREN S HOSPITAL Objectives 1. Identify the critical components
EMS System for Metropolitan Oklahoma City and Tulsa 2018 Medical Control Board Treatment Protocols
 EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
Updated October 16, 2014
 Updated October 16, 2014 The CDC Trauma Triage Algorithm is designed as a triage tool to help decide patient destination and the clinical care protocolsare designed to provide treatment options Prior to
Updated October 16, 2014 The CDC Trauma Triage Algorithm is designed as a triage tool to help decide patient destination and the clinical care protocolsare designed to provide treatment options Prior to
Clinical aspects in urogenital injuries
 Clinical aspects in urogenital injuries Rolf Wahlqvist Oslo Urological University Clinic Aker University Hospital Nordic Rad.2008 1 Urogenital injuries in trauma patients Renal injury Ureteral injury (infrequent/iatrogenic)
Clinical aspects in urogenital injuries Rolf Wahlqvist Oslo Urological University Clinic Aker University Hospital Nordic Rad.2008 1 Urogenital injuries in trauma patients Renal injury Ureteral injury (infrequent/iatrogenic)
CLINICAL MANUAL. Trauma System Activation Trauma Code Criteria
 CLINICAL MANUAL Policy Number: CM T-28 Approved by: Nursing Congress, Management Forum Issue Date: 09/1999 Applies to: Downtown Value(s): Respect, Integrity, Innovation Page(s): 1 of 4 Trauma System Activation
CLINICAL MANUAL Policy Number: CM T-28 Approved by: Nursing Congress, Management Forum Issue Date: 09/1999 Applies to: Downtown Value(s): Respect, Integrity, Innovation Page(s): 1 of 4 Trauma System Activation
SAN LUIS OBISPO COUNTY EMERGENCY MEDICAL SERVICES AGENCY PREHOSPITAL POLICY
 SAN LUIS OBISPO COUNTY EMERGENCY MEDICAL SERVICES AGENCY PREHOSPITAL POLICY Policy Reference No: 153 [01/08/2013] Formerly Policy No: 201.3 Effective Date: 11/01/2012 Review Date: 03/01/2014 TRAUMA PATIENT
SAN LUIS OBISPO COUNTY EMERGENCY MEDICAL SERVICES AGENCY PREHOSPITAL POLICY Policy Reference No: 153 [01/08/2013] Formerly Policy No: 201.3 Effective Date: 11/01/2012 Review Date: 03/01/2014 TRAUMA PATIENT
Assessment of the Trauma Patient
 CHAPTER 10 Assessment of the Trauma Patient Overall Assessment Scheme Scene Size-Up Initial Assessment Trauma Physical Exam Vital Signs & SAMPLE History Medical SAMPLE History Physical Exam & Vital Signs
CHAPTER 10 Assessment of the Trauma Patient Overall Assessment Scheme Scene Size-Up Initial Assessment Trauma Physical Exam Vital Signs & SAMPLE History Medical SAMPLE History Physical Exam & Vital Signs
PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University
 PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University Patient survive Low morbidity GOOD JUDGMENT COMES FROM EXPERIENCE EXPERIENCE COMES FROM BAD
PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University Patient survive Low morbidity GOOD JUDGMENT COMES FROM EXPERIENCE EXPERIENCE COMES FROM BAD
Restore adequate respiratory and circulatory conditions. Reduce pain
 Pre-hospital management of the trauma patient is best performed by an integrated team focused on minimizing the time from injury to definitive care at an appropriate trauma center. Dispatchers, first responders,
Pre-hospital management of the trauma patient is best performed by an integrated team focused on minimizing the time from injury to definitive care at an appropriate trauma center. Dispatchers, first responders,
Interventional Radiology in Trauma. Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital
 Interventional Radiology in Trauma Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital Disclosures None relevant to this presentation Shareholder Johnson and Johnson Goal
Interventional Radiology in Trauma Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital Disclosures None relevant to this presentation Shareholder Johnson and Johnson Goal
Northern Trauma Network. Management of Haemodynamically Unstable Patients with Pelvic Injury
 Management of Haemodynamically Unstable Patients with Pelvic Injury Northern Trauma Network This guideline focuses on the assessment of haemodynamic instability related to haemorrhage associated with a
Management of Haemodynamically Unstable Patients with Pelvic Injury Northern Trauma Network This guideline focuses on the assessment of haemodynamic instability related to haemorrhage associated with a
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Splenic Injury Evaluation and Management Guideline ADULT Practice Management Guideline Contact: Trauma Center Medical
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Splenic Injury Evaluation and Management Guideline ADULT Practice Management Guideline Contact: Trauma Center Medical
Which Blunt Trauma Patients Should Be Studied by Abdominal CT?
 MDCT of Bowel and Mesenteric Injury: How Findings Influence Management 4 th Nordic Trauma Radiology Course 2006 4 th Nordic Trauma Radiology Course 2006 Stuart E. Mirvis, M.D., FACR Department of Radiology
MDCT of Bowel and Mesenteric Injury: How Findings Influence Management 4 th Nordic Trauma Radiology Course 2006 4 th Nordic Trauma Radiology Course 2006 Stuart E. Mirvis, M.D., FACR Department of Radiology
Assessment and Scoring Tools
 Assessment and Scoring Tools 2013 APGAR Scale 0 points 1 point 2 points Heart Rate Absent 100 Respiratory Rate Absent Slow, irregular Good, drying Irritability Flaccid Some flexion Active motion
Assessment and Scoring Tools 2013 APGAR Scale 0 points 1 point 2 points Heart Rate Absent 100 Respiratory Rate Absent Slow, irregular Good, drying Irritability Flaccid Some flexion Active motion
Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System
 Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System Stomach & Duodenum Frontal (AP) View Nasogastric tube 2 1 3 4 Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum
Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System Stomach & Duodenum Frontal (AP) View Nasogastric tube 2 1 3 4 Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum
11/1/2014. Just The. Pearls. Everything I do is Off-Label! This is the ultimate lecture for the ADHD emergency physician.
 Just The Everything I do is Off-Label! Pearls This is the ultimate lecture for the ADHD emergency physician. 1 >20 Tips in 60 Minutes You re repeatin yourself ½ Trauma ½ Medical Arrest Crit Care in The
Just The Everything I do is Off-Label! Pearls This is the ultimate lecture for the ADHD emergency physician. 1 >20 Tips in 60 Minutes You re repeatin yourself ½ Trauma ½ Medical Arrest Crit Care in The
ESCAMBIA COUNTY TRAUMA TRANSPORT
 TRAUMA ALERT CRITERIA are established state mandated criteria. ADULT TRAUMA ALERT CRITERIA (Physical and anatomical characteristics of a person 16 years of age or older) Any 1 of the following: 1. Airway:
TRAUMA ALERT CRITERIA are established state mandated criteria. ADULT TRAUMA ALERT CRITERIA (Physical and anatomical characteristics of a person 16 years of age or older) Any 1 of the following: 1. Airway:
3/10/2014. Occurs in 70-80% of patients with blunt trauma. Rarely causes immediate threat to life or limb. Orthopedic Trauma. Musculoskeletal Trauma
 Orthopedic Trauma Douglas D. Presta, D.P.M., FACFAS, NREMT-P Spokane County EMS Musculoskeletal Trauma Introduction Primary Assessment Secondary Survey Musculoskeletal assessment Life threatening injuries
Orthopedic Trauma Douglas D. Presta, D.P.M., FACFAS, NREMT-P Spokane County EMS Musculoskeletal Trauma Introduction Primary Assessment Secondary Survey Musculoskeletal assessment Life threatening injuries
The Secondary Survey
 The Secondary Survey Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Attending Surgeon, Denver Health Medical Center Associate Professor of Surgery, University of Colorado Outlining
The Secondary Survey Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Attending Surgeon, Denver Health Medical Center Associate Professor of Surgery, University of Colorado Outlining
Management of the Elderly Anti-coagulated Trauma Patient. Dr Paul Bradford ER Physician, Trauma Team Leader Hotel Dieu Hospital Windsor
 Management of the Elderly Anti-coagulated Trauma Patient Dr Paul Bradford ER Physician, Trauma Team Leader Hotel Dieu Hospital Windsor Geriatric Trauma Issues 5 th leading cause of death Higher mortality,
Management of the Elderly Anti-coagulated Trauma Patient Dr Paul Bradford ER Physician, Trauma Team Leader Hotel Dieu Hospital Windsor Geriatric Trauma Issues 5 th leading cause of death Higher mortality,
Shenandoah Co. Fire & Rescue. Injuries to. and Spine. December EMS Training Bill Streett Training Section Chief
 Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#
Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#
Algorithms for managing the common trauma patient
 ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
T-PODResponder Pelvic Stabilization Device
 T-PODResponder Pelvic Stabilization Device Training Session Pyng Medical Corp. 1-604-303-7964 2014 Pyng Medical Corp. August 2014 PM-176a Why T-PODResponder? Pelvic fractures have a mortality rate of 5%
T-PODResponder Pelvic Stabilization Device Training Session Pyng Medical Corp. 1-604-303-7964 2014 Pyng Medical Corp. August 2014 PM-176a Why T-PODResponder? Pelvic fractures have a mortality rate of 5%
10/27/2014. An experience that causes physical, emotional, or psychological distress or harm.
 Ann Marie Szoke, DNP, CRNP Supervisor Advanced Practitioners St. Luke s University Hospital To review multiple traumatic events through case presentations Discuss the concept of the Hybrid Operating Room
Ann Marie Szoke, DNP, CRNP Supervisor Advanced Practitioners St. Luke s University Hospital To review multiple traumatic events through case presentations Discuss the concept of the Hybrid Operating Room
Genitourinary Trauma Introduction GU Trauma overlooked
 Genitourinary Trauma Introduction GU Trauma overlooked 10-20% of all injured patients Long term morbidity Impotence Incontinence Life-threatening injuries first Urethral Injury Plan Bladder Injury Kidney
Genitourinary Trauma Introduction GU Trauma overlooked 10-20% of all injured patients Long term morbidity Impotence Incontinence Life-threatening injuries first Urethral Injury Plan Bladder Injury Kidney
Abdominal & retroperitoneal endovascular intervention, Bo Kalin, Karolinska Hospital
 Abdominal & retroperitoneal endovascular intervention, Bo Kalin, Karolinska Hospital What is endovascular therapy. Diagnosing Traumatic Arterial Injury Clinical signs CT / CT-angiography To diminish a
Abdominal & retroperitoneal endovascular intervention, Bo Kalin, Karolinska Hospital What is endovascular therapy. Diagnosing Traumatic Arterial Injury Clinical signs CT / CT-angiography To diminish a
Renal Trauma: Management Options
 Renal Trauma: Management Options Immediate surgical repair Nephrectomy Conservative management Alonso RC et al. Kidney in Danger: CT Findings of Blunt and Penetrating Renal Trauma. RadioGraphics 2009;
Renal Trauma: Management Options Immediate surgical repair Nephrectomy Conservative management Alonso RC et al. Kidney in Danger: CT Findings of Blunt and Penetrating Renal Trauma. RadioGraphics 2009;
PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT
 PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT Board Approved June 2007 Revised December 2009 Revised July 2011 Revised June 2015 435 Hunter Street Fredericksburg, VA 22401
PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT Board Approved June 2007 Revised December 2009 Revised July 2011 Revised June 2015 435 Hunter Street Fredericksburg, VA 22401
Canadian Undergraduate Urology Curriculum (CanUUC): Genitourinary Trauma. Last reviewed June 2014
: Genitourinary Trauma. Last reviewed June 2014") Canadian Undergraduate Urology Curriculum (CanUUC): Genitourinary Trauma Last reviewed June 2014 Session Objectives 1. Recognize hematuria as the cardinal symptom of urinary tract trauma. 1. Outline the
Canadian Undergraduate Urology Curriculum (CanUUC): Genitourinary Trauma Last reviewed June 2014 Session Objectives 1. Recognize hematuria as the cardinal symptom of urinary tract trauma. 1. Outline the
APPROACH TO TRAUMA. Dr E.Memary Anesthesiologist Assistant Professor of SBMU
 APPROACH TO TRAUMA Dr E.Memary Anesthesiologist Assistant Professor of SBMU Objectives Describe the initial approach to the injured patient, including the primary and secondary surveys. Identify the types
APPROACH TO TRAUMA Dr E.Memary Anesthesiologist Assistant Professor of SBMU Objectives Describe the initial approach to the injured patient, including the primary and secondary surveys. Identify the types
Classification, management and outcomes of severe pelvic ring fractures
 Classification, management and outcomes of severe pelvic ring fractures School of Public Health and Preventive Medicine, Monash University The Alfred Hospital, Royal Melbourne Hospital, Epworth Health
Classification, management and outcomes of severe pelvic ring fractures School of Public Health and Preventive Medicine, Monash University The Alfred Hospital, Royal Melbourne Hospital, Epworth Health
Selective Nonoperative Management of Penetrating Abdominal Trauma. Kings County Hospital Center Verena Liu, MD 10/13/2011
 Selective Nonoperative Management of Penetrating Abdominal Trauma Kings County Hospital Center Verena Liu, MD 10/13/2011 Case Presentation 28M admitted on 8/27/2011 s/p GSW to right upper quadrant and
Selective Nonoperative Management of Penetrating Abdominal Trauma Kings County Hospital Center Verena Liu, MD 10/13/2011 Case Presentation 28M admitted on 8/27/2011 s/p GSW to right upper quadrant and
Trauma Alert Step 2 Additions
 Trauma Alert Step 2 Additions MANGLED, DEGLOVED OR PULSELESS EXTREMITY PELVIC INJURY WITH HIGH-RISK MECHANISM OF INJURY Many thanks to Paramedic FTO Justin Bramlette for assembling this training presentation
Trauma Alert Step 2 Additions MANGLED, DEGLOVED OR PULSELESS EXTREMITY PELVIC INJURY WITH HIGH-RISK MECHANISM OF INJURY Many thanks to Paramedic FTO Justin Bramlette for assembling this training presentation
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #2 Blunt Trauma
 McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #2 Blunt Trauma Blunt trauma is the most common cause of traumatic death and disability. The definition
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #2 Blunt Trauma Blunt trauma is the most common cause of traumatic death and disability. The definition
UPDATES, 2018 NTDS PILOT (PROPOSED CHANGES TO 2020 NTDB DATA DICTIONARY) AND TQIP PROCESS MEASURES. Lita Holdeman, BS, CSTR AOTR Education Chair
 AND TQIP PROCESS MEASURES. Lita Holdeman, BS, CSTR AOTR Education Chair") UPDATES, 2018 NTDS PILOT (PROPOSED CHANGES TO 2020 NTDB DATA DICTIONARY) AND TQIP PROCESS MEASURES Lita Holdeman, BS, CSTR AOTR Education Chair Disclaimer Notice: All information provide to you at any
UPDATES, 2018 NTDS PILOT (PROPOSED CHANGES TO 2020 NTDB DATA DICTIONARY) AND TQIP PROCESS MEASURES Lita Holdeman, BS, CSTR AOTR Education Chair Disclaimer Notice: All information provide to you at any
Date of Admission: [DATE]. Date of Discharge:
![Date of Admission: [DATE]. Date of Discharge:](/thumbs/74/71277118.jpg "Date of Admission: [DATE]. Date of Discharge:") Date of Admission: [DATE]. Date of Discharge: History of Present Illness: Mr. [NAME] AKA [NAME] is a 31-year-old male who presents to the [PLACE] Trauma Surgery Service as a moderate trauma on [DATE] following
Date of Admission: [DATE]. Date of Discharge: History of Present Illness: Mr. [NAME] AKA [NAME] is a 31-year-old male who presents to the [PLACE] Trauma Surgery Service as a moderate trauma on [DATE] following
Pediatric Trauma. July 27 th, Suzana Buac, PGY4. Dr. Neil Merritt
 Pediatric Trauma July 27 th, 2016. Suzana Buac, PGY4 Dr. Neil Merritt Case 5yoM fall from roof Fall from roof of home while father was shingling 5yoM fall from roof Fall from roof of home while father
Pediatric Trauma July 27 th, 2016. Suzana Buac, PGY4 Dr. Neil Merritt Case 5yoM fall from roof Fall from roof of home while father was shingling 5yoM fall from roof Fall from roof of home while father
SIERRA-SACRAMENTO VALLEY EMS AGENCY PROGRAM POLICY
 SIERRA-SACRAMENTO VALLEY EMS AGENCY PROGRAM POLICY PURPOSE: To identify those patients who are at greatest risk for severe injury and determine the most appropriate facility to transport persons with different
SIERRA-SACRAMENTO VALLEY EMS AGENCY PROGRAM POLICY PURPOSE: To identify those patients who are at greatest risk for severe injury and determine the most appropriate facility to transport persons with different
Hemorrhage Control. Chapter 6
 Chapter 6 The hemorrhage that take[s] place when a main artery is divided is usually so rapid and so copious that the wounded man dies before help can reach him. Colonel H. M. Gray, 1919 Stop the Bleeding!
Chapter 6 The hemorrhage that take[s] place when a main artery is divided is usually so rapid and so copious that the wounded man dies before help can reach him. Colonel H. M. Gray, 1919 Stop the Bleeding!
journal ORIGINAL RESEARCH
 texas orthopaedic journal ORIGINAL RESEARCH Mortality with Circumferential Pelvic Compression for Pelvic Ring Disruption in Polytraumatized Patients: A Retrospective Analysis of 1,639 Pelvic Ring Injuries
texas orthopaedic journal ORIGINAL RESEARCH Mortality with Circumferential Pelvic Compression for Pelvic Ring Disruption in Polytraumatized Patients: A Retrospective Analysis of 1,639 Pelvic Ring Injuries
Patient Assessment. Chapter 8
 Patient Assessment Chapter 8 Patient Assessment Scene size-up Initial assessment Focused history and physical exam Vital signs History Detailed physical exam Ongoing assessment Patient Assessment Process
Patient Assessment Chapter 8 Patient Assessment Scene size-up Initial assessment Focused history and physical exam Vital signs History Detailed physical exam Ongoing assessment Patient Assessment Process
May Clinical Director, Peninsula Trauma Network (Edited for PTN)
") Network Policy Traumatic vascular injuries Guidelines Purpose Date May 2015 Version Following the national introduction of Regional Trauma Networks, Major Trauma Networks (MTN s) are required to have a
Network Policy Traumatic vascular injuries Guidelines Purpose Date May 2015 Version Following the national introduction of Regional Trauma Networks, Major Trauma Networks (MTN s) are required to have a