This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
|
|
|
- Jordan Kennedy
- 6 years ago
- Views:
Transcription

1 Introduction Compartment Syndromes of the Leg Related to Athletic Activity Mark M. Casillas, M.D. Consequences of a misdiagnosis persistence of a performance limitation loss of function/compartment loss of limb Goal: anatomically and physiologically based understanding of the condition 1 Disclosure None relevant to this topic Anatomy Four distinct, inelastic compartments divided by Tibia Fibula Crural fascia Intermuscular septums Introduction Misunderstood Misdiagnosed Increased pressure within one or more of the leg compartments produces symptoms that are bewildering and confusing Anatomy Four distinct, inelastic compartments divided by Tibia Fibula Crural fascia Intermuscular septums
2 Anatomy Anterior Compartment Four distinct, inelastic compartments divided by Tibia Fibula Crural fascia Intermuscular septums Boundaries lateral border of the tibia crural fascia anterior crural septum fibula interosseous membrane Contents anterior tibial m. extensor hallucis longus m. extensor digitorum longus m. Ant. tibial neurovascular bundle Four distinct, inelastic compartments divided by Tibia Fibula Crural fascia Intermuscular septums Anatomy Lateral Compartment Boundaries anterior crural septum crural fascia posterior crural septum lateral border of the fibula Contents P. brevis and longus muscles superficial peroneal nerve Four distinct, inelastic compartments divided by Tibia Fibula Crural fascia Intermuscular septums Anatomy Deep Posterior Compartment Boundaries posterior tibia interosseous membrane fibula posterior crural septum intermuscular septum Contents posterior tibial, flexor hallucis longus, and flexor digitorum muscles posterior tibial and peroneal vessels tibial nerve
 prolonged compression (bandage or cast) Pathology necrosis of muscle and nerve irreversible loss of function below or above")
3 Superficial Posterior Compartment Acute Compartment Syndrome Boundaries intermuscular septum crural fascia Contents soleus and the gastrocnemius muscles no named vessels or nerves Persistent pressure elevation Trigger athletic activity trauma (tibia fracture, muscle tear) prolonged compression (bandage or cast) Pathology necrosis of muscle and nerve irreversible loss of function below or above the knee amputation Classification Chronic Exertional Compartment Syndrome Acute compartment syndrome (ACS) Chronic exertional compartment syndrome (CECS) Short term, reversible and recurrent pressure elevation Trigger athletic activity short walk Symptoms muscle pain swelling loss of sensory and motor function Acute Compartment Syndrome Chronic Exertional Compartment Syndrome Elevated pressure within the inelastic compartment Reduces blood perfusion to the nerves and muscles Vicious cycle of increasing swelling and pressure Symptoms muscle pain swelling loss of sensory and motor function Symptoms force a cessation of activity Compartment pressures fall Symptoms remit as the Can lead to an ACS with all of its associated morbidity



4 History Physical Exam Pain localized to the specific compartment rest activity passive lengthening of the muscle distal referred pain related to the course of a nerve within the compartment. Nerve dysfunction numbness tingling weakness paralysis Swelling firmness muscle herniation Sarrafian SH. Anatomy of the Foot and Ankle,1983. Inspection swollen with or without muscle herniations Palpation firmness and tenderness at the affected compartment muscle herniations History ACS Acute and progressive symptoms Resolution of pain without the recovery of nerve or muscle function may signal the loss of muscle viability Percussion superficial peroneal nerve at its hiatus paresthesias in the distribution of the nerve Loss of sensation first web space anterior compartment and deep peroneal nerve involvement dorsal foot, exclusive of the first web space lateral compartment and the superficial peroneal nerve plantar foot deep posterior compartment and the tibial nerve Physical Exam Sarrafian SH. Anatomy of the Foot and Ankle1983. History CECS Pain or loss of function after activity Recovery following rest Predictable and recurrent CECS can convert to a fulminate ACS without warning Treatment must be directed by the acute condition Weakness or paralysis ankle and toe extensors anterior compartment involvement foot evertors lateral compartment involvement toe flexors deep posterior compartment involvement ankle flexors superficial posterior compartment involvement Pain with passive muscle stretch very sensitive indicator of compartment syndrome Physical Exam

 Correlate with the clinical presentation Focal bone tenderness")



5 Physical Exam Diagnostic Testing Post exertion exam mandatory to rule out CECS type duration intensity time to onset ability to continue activity time to recovery Invasive compartment pressure measurement Anesthetized Arterial line >30mm Hg ACS emergent CECS elective (post exertion) Correlate with the clinical presentation Focal bone tenderness stress fracture Linear tenderness posterior medial tibial stress syndrome Physical Exam Non Surgical Treatment CECS Not ever indicated for ACS Limitation of physical activity Cross training Stretching Warm up Conditioning Infrequently successful CECS may convert to ACS Routine radiographs CT Bone scan MR Post exertion MR may demonstrate muscle edema fracture stress fracture tumor infection Diagnostic Testing Surgical Treatment Compartment release all effected compartments extensile approaches Indications ACS CECS with failed non surgical treatment





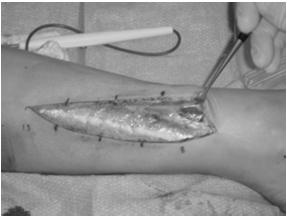
6 Anterior and Lateral Fasciotomy Surgical Treatment 13 cm incision in line with the fibula Hiatus for the superficial peroneal nerve is isolated SPN protected during lateral compartment release Anterior compartment released under direct vision Necrotic muscle must be removed Fascia is never closed Superficial and Deep Posterior Fasciotomy Surgical Treatment 10 cm medial incision in line with the posterior tibia Saphenous vein and nerve protected Fascial attachments of the soleus and flexor digitorum longus are released directly off of the posterior medial border of the tibia to decompress the deep posterior compartment Soleus fascia is released for superficial posterior compartment decompression Skin is closed only if tension free closure is possible VAC repeat debridement delayed closure split thickness skin graft Red color Muscle Viability/The 4 C s Ability to contract No loss of consistency Intact capacity to bleed Orthosis wedged shoe heel AFO Motor Deficit




7 Reconstruction calcaneal osteotomy tendon transfer subtalar arthrodesis ankle arthrodesis Motor Deficit Case 1 17 year old HS football player Initial evaluation by sports specialist Early season exertional leg pain Lateral and anterior Subsequent evaluation Foot drop Dorsal foot numbness Office compartment measurements at rest Ant and lat 30 mm Sup and Deep post 12 mm 2 Weeks Non weightbearing Suture removal 3 weeks Return to activity cross training with pain free activities appropriate stretching, warm up, and conditioning Training log type duration intensity frequency of activity performance and symptom observations Compression stockings Rehabilitation Day 9 Case 1 Orthopaedic Consult DF and eversion weak Numb at DPN Compartment measurement Ant and lat 32 mm Sup and deep post 14 mm Complications Lateral Leg Ant Comp Persistence Recurrence (CECS) Revision fasciectomy as opposed to fasciotomy Nerve injury saphenous superficial peroneal Vascular injury saphenous vein Infection Hematoma Delayed wound healing SPN P. brevis


8 Necrotic P. Brevis Muscle Day 5 Persistent, severe, unrelenting pain after brief but intense competitive performance Anterior leg swelling, herniation, dorsal foot numbness at first web space, weak DF Post op Weak DF Weak Eversion AFO 6 months Full recovery Full athletic activity Case 1 Day 5 Assessed by trainer Compartment syndrome suspected Patient sent to ER ER physician discharged patient 17 year old cheerleader New onset exertional anterior leg pain Day 6 Orthopaedic Consult <24 hours after conversion from CECS to ACS Numb DPN Weak (1/5) DF







9 Compartment Pressure Anterior 41 Lateral 44 Sup. Post 23 Deep Post 23 3 weeks post op Full DF power Normal DPN sensation





10 Case 3 48 year old male No hx exertional leg pain Drinking and wrestling until 11pm Awoke at 2 am w severe anterior and lateral leg pain and swelling Presented to ER at 3 am and discharged Day 5 Compartment Pressure Anterior >100 Lateral 35 Sup. Post 9 Deep Post 9 Case 3 Case 3 Day 2 Returned to work with persistent pain Day 3 Resolution of pain Foot drop Day 4 Redness over leg Admitted w cellulitis Case 3 Case 3 Case 3 Day 5 Orthopaedic consult Tight, firm anterior compartment Soft lateral compartment Normal sensation and pulses Pain with active PF No DF power at ankle, toes










11 Case 3 Case 4 Post exertion measurements Compartment Pressure (R/L) Anterior 18/19 Lateral 21/18 Sup. Post 12/10 Deep Post 13/9 Case 3 Repeat debridement and Closure Case 4 Deep NV bundle and lateral compartment intact Case 4 Case 4 19 year old college student 18 month history of exertional anterior and lateral leg pain Initially occurring after running Now occurring after walking






12 Case 4 Mark M. Casillas, M.D. Orthopaedic Surgery, Foot & Ankle Jeremy L. Dickerson, M.D. Family Practice, Sports Medicine Stacé S. Rust, M.D. Orthopaedic Surgery, Hand, Wrist, Elbow & Shoulder Ryane M. Galindo MPAS, PA-C 70 Case 4 Case 4
The Lower Limb VI: The Leg. Anatomy RHS 241 Lecture 6 Dr. Einas Al-Eisa
 The Lower Limb VI: The Leg Anatomy RHS 241 Lecture 6 Dr. Einas Al-Eisa Muscles of the leg Posterior compartment (superficial & deep): primary plantar flexors of the foot flexors of the toes Anterior compartment:
The Lower Limb VI: The Leg Anatomy RHS 241 Lecture 6 Dr. Einas Al-Eisa Muscles of the leg Posterior compartment (superficial & deep): primary plantar flexors of the foot flexors of the toes Anterior compartment:
Leg. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 Leg Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Skin of the Leg Cutaneous Nerves Medially: The saphenous nerve, a branch of the femoral nerve supplies the skin on the medial surface
Leg Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Skin of the Leg Cutaneous Nerves Medially: The saphenous nerve, a branch of the femoral nerve supplies the skin on the medial surface
The Leg. Prof. Oluwadiya KS
 The Leg Prof. Oluwadiya KS www.oluwadiya.sitesled.com Compartments of the leg 4 Four Compartments: 1. Anterior compartment Deep fibular nerve Dorsiflexes the foot and toes 2. Lateral Compartment Superficial
The Leg Prof. Oluwadiya KS www.oluwadiya.sitesled.com Compartments of the leg 4 Four Compartments: 1. Anterior compartment Deep fibular nerve Dorsiflexes the foot and toes 2. Lateral Compartment Superficial
Compartment Syndrome
 Compartment Syndrome Chapter 34 Compartment Syndrome Introduction Compartment syndrome may occur with an injury to any fascial compartment. The fascial defect caused by the injury may not be adequate to
Compartment Syndrome Chapter 34 Compartment Syndrome Introduction Compartment syndrome may occur with an injury to any fascial compartment. The fascial defect caused by the injury may not be adequate to
Review relevant anatomy of the foot and ankle. Learn the approach to examining the foot and ankle
 Objectives Review relevant anatomy of the foot and ankle Learn the approach to examining the foot and ankle Learn the basics of diagnosis and treatment of ankle sprains Overview of other common causes
Objectives Review relevant anatomy of the foot and ankle Learn the approach to examining the foot and ankle Learn the basics of diagnosis and treatment of ankle sprains Overview of other common causes
Topic 4: Fractures and External Fixation
 Topic 4: Fractures and External Fixation Acute Compartment Syndrome Prof. Dr. Andreas Platz Stadtspital Triemli, Zürich Demographics Incidence: Men 7.3/100,000 Women 0.7/100,000 69% due to trauma 36% fx
Topic 4: Fractures and External Fixation Acute Compartment Syndrome Prof. Dr. Andreas Platz Stadtspital Triemli, Zürich Demographics Incidence: Men 7.3/100,000 Women 0.7/100,000 69% due to trauma 36% fx
Anatomy MCQs Week 13
 Anatomy MCQs Week 13 1. Posterior to the medial malleolus of the ankle: The neurovascular bundle lies between Tibialis Posterior and Flexor Digitorum Longus The tendon of Tibialis Posterior inserts into
Anatomy MCQs Week 13 1. Posterior to the medial malleolus of the ankle: The neurovascular bundle lies between Tibialis Posterior and Flexor Digitorum Longus The tendon of Tibialis Posterior inserts into
Injuries to the Hands and Feet
 Injuries to the Hands and Feet Chapter 26 Injuries to the Hands and Feet Introduction Combat injuries to the hands and feet differ from those of the arms and legs in terms of mortality and morbidity. Death
Injuries to the Hands and Feet Chapter 26 Injuries to the Hands and Feet Introduction Combat injuries to the hands and feet differ from those of the arms and legs in terms of mortality and morbidity. Death
موسى صالح عبد الرحمن الحنبلي أحمد سلمان
 8 موسى صالح عبد الرحمن الحنبلي أحمد سلمان 1 P a g e Today we will talk about a new region, which is the leg. And as always, we will start with studying the sensory innervation of the leg. What is the importance
8 موسى صالح عبد الرحمن الحنبلي أحمد سلمان 1 P a g e Today we will talk about a new region, which is the leg. And as always, we will start with studying the sensory innervation of the leg. What is the importance
Case report. Your Diagnosis?
 Case report 18 year Male Panel beater referred with a tibial shin syndrome with pain of 6 months. Pain over the anterolateral aspect of leg, bilateral and is precipitated walking 10 minutes. Your Diagnosis?
Case report 18 year Male Panel beater referred with a tibial shin syndrome with pain of 6 months. Pain over the anterolateral aspect of leg, bilateral and is precipitated walking 10 minutes. Your Diagnosis?
1. A worker falls from a height and lands on his feet. Radiographs reveal a fracture of the sustentaculum tali. The muscle passing immediately
 1. A worker falls from a height and lands on his feet. Radiographs reveal a fracture of the sustentaculum tali. The muscle passing immediately beneath it that would be adversely affected is the: fibularis
1. A worker falls from a height and lands on his feet. Radiographs reveal a fracture of the sustentaculum tali. The muscle passing immediately beneath it that would be adversely affected is the: fibularis
musculoskeletal system anatomy nerves of the lower limb 2 done by: Dina sawadha & mohammad abukabeer
 musculoskeletal system anatomy nerves of the lower limb 2 done by: Dina sawadha & mohammad abukabeer #Sacral plexus : emerges from the ventral rami of the spinal segments L4 - S4 and provides motor and
musculoskeletal system anatomy nerves of the lower limb 2 done by: Dina sawadha & mohammad abukabeer #Sacral plexus : emerges from the ventral rami of the spinal segments L4 - S4 and provides motor and
Prevention and Treatment of Injuries. Anatomy. Anatomy. Tibia: the second longest bone in the body
 Prevention and Treatment of Injuries The Ankle and Lower Leg Westfield High School Houston, Texas Anatomy Tibia: the second longest bone in the body Serves as the principle weight-bearing bone of the leg.
Prevention and Treatment of Injuries The Ankle and Lower Leg Westfield High School Houston, Texas Anatomy Tibia: the second longest bone in the body Serves as the principle weight-bearing bone of the leg.
Ankle Tendons in Athletes. Laura W. Bancroft, M.D.
 Ankle Tendons in Athletes Laura W. Bancroft, M.D. Outline Protocols Normal Anatomy Tendinopathy, partial and complete tears Posterior tibial, Flexor Hallucis Longus, Achilles, Peroneal and Anterior Tibial
Ankle Tendons in Athletes Laura W. Bancroft, M.D. Outline Protocols Normal Anatomy Tendinopathy, partial and complete tears Posterior tibial, Flexor Hallucis Longus, Achilles, Peroneal and Anterior Tibial
~, /' ~::'~ EXTENSOR HALLUCIS LONGUS. Leg-anterolateral :.:~ / ~\,
 TIBIALIS ANTERIOR Lateral condyle of tibia, upper half of lateral surface of tibia, interosseous membrane Medial side and plantar surface of medial cuneiform bone, and base of first metatarsal bone Dorsiflexes
TIBIALIS ANTERIOR Lateral condyle of tibia, upper half of lateral surface of tibia, interosseous membrane Medial side and plantar surface of medial cuneiform bone, and base of first metatarsal bone Dorsiflexes
Lower Limb Nerves. Clinical Anatomy
 Lower Limb Nerves Clinical Anatomy Lumbar Plexus Ventral rami L1 L4 Supplies: Abdominal wall External genitalia Anteromedial thigh Major nerves.. Lumbar Plexus Nerves relation to psoas m. : Obturator n.
Lower Limb Nerves Clinical Anatomy Lumbar Plexus Ventral rami L1 L4 Supplies: Abdominal wall External genitalia Anteromedial thigh Major nerves.. Lumbar Plexus Nerves relation to psoas m. : Obturator n.
Where should you palpate the pulse of different arteries in the lower limb?
 Where should you palpate the pulse of different arteries in the lower limb? The femoral artery In the femoral triangle, its pulse is easily felt just inferior to the inguinal ligament midway between the
Where should you palpate the pulse of different arteries in the lower limb? The femoral artery In the femoral triangle, its pulse is easily felt just inferior to the inguinal ligament midway between the
17 FibulA FlAP Tor Chiu fibula flap 153
 17 Fibula Flap Tor Chiu Fibula Flap 153 Fibula Flap FLAP TERRITORY This flap includes a segment of the fibular bone with or without the overlying skin island on the peroneal/ lateral aspect of the calf.
17 Fibula Flap Tor Chiu Fibula Flap 153 Fibula Flap FLAP TERRITORY This flap includes a segment of the fibular bone with or without the overlying skin island on the peroneal/ lateral aspect of the calf.
Copyright 2004, Yoshiyuki Shiratori. All right reserved.
 Ankle and Leg Evaluation 1. History Chief Complaint: A. What happened? B. Is it a sharp or dull pain? C. How long have you had the pain? D. Can you pinpoint the pain? E. Do you have any numbness or tingling?
Ankle and Leg Evaluation 1. History Chief Complaint: A. What happened? B. Is it a sharp or dull pain? C. How long have you had the pain? D. Can you pinpoint the pain? E. Do you have any numbness or tingling?
HUMAN BODY COURSE LOWER LIMB NERVES AND VESSELS
 HUMAN BODY COURSE LOWER LIMB NERVES AND VESSELS October 22, 2010 D. LOWER LIMB MUSCLES 2. Lower limb compartments ANTERIOR THIGH COMPARTMENT General lfunction: Hip flexion, knee extension, other motions
HUMAN BODY COURSE LOWER LIMB NERVES AND VESSELS October 22, 2010 D. LOWER LIMB MUSCLES 2. Lower limb compartments ANTERIOR THIGH COMPARTMENT General lfunction: Hip flexion, knee extension, other motions
Integrated Manual Therapy & Orthopedic Massage For Complicated Lower Extremity Conditions
 Integrated Manual Therapy & Orthopedic Massage For Complicated Lower Extremity Conditions Assessment Protocols Treatment Protocols Treatment Protocols Corrective Exercises Artwork and slides taken from
Integrated Manual Therapy & Orthopedic Massage For Complicated Lower Extremity Conditions Assessment Protocols Treatment Protocols Treatment Protocols Corrective Exercises Artwork and slides taken from
Year 2004 Paper one: Questions supplied by Megan
 QUESTION 47 A 58yo man is noted to have a right foot drop three days following a right total hip replacement. On examination there is weakness of right ankle dorsiflexion and toe extension (grade 4/5).
QUESTION 47 A 58yo man is noted to have a right foot drop three days following a right total hip replacement. On examination there is weakness of right ankle dorsiflexion and toe extension (grade 4/5).
VENOUS DRAINAGE OF THE LOWER LIMB
 Anatomy of the lower limb Superficial veins & nerve injuries Dr. Hayder VENOUS DRAINAGE OF THE LOWER LIMB The venous drainage of the lower limb is of huge clinical & surgical importance. Since the venous
Anatomy of the lower limb Superficial veins & nerve injuries Dr. Hayder VENOUS DRAINAGE OF THE LOWER LIMB The venous drainage of the lower limb is of huge clinical & surgical importance. Since the venous
Anatomy and evaluation of the ankle.
 Anatomy and evaluation of the ankle www.fisiokinesiterapia.biz Ankle Anatomical Structures Tibia Fibular Talus Tibia This is the strongest largest bone of the lower leg. It bears weight and the bone creates
Anatomy and evaluation of the ankle www.fisiokinesiterapia.biz Ankle Anatomical Structures Tibia Fibular Talus Tibia This is the strongest largest bone of the lower leg. It bears weight and the bone creates
fig fig For the following diagrams
 fig. 1271 For the following diagrams Please draw small circles at the following points (pts in bold are main syllabus pts): Liver-1 Liver-2 Liver-3 Liver-4 Spleen-4 Spleen-5 Stomach-41 Stomach-42 Stomach-43
fig. 1271 For the following diagrams Please draw small circles at the following points (pts in bold are main syllabus pts): Liver-1 Liver-2 Liver-3 Liver-4 Spleen-4 Spleen-5 Stomach-41 Stomach-42 Stomach-43
Disclosures. Syndesmosis Injury. Syndesmosis Ligaments. Objectives. Mark M. Casillas, M.D.
 Disclosures Syndesmosis Injury No relevant disclosures Mark M. Casillas, M.D. 1 Objectives Syndesmosis Ligaments Understand the syndesmosis anatomy and function Classify syndesmosis injuries Describe treatment
Disclosures Syndesmosis Injury No relevant disclosures Mark M. Casillas, M.D. 1 Objectives Syndesmosis Ligaments Understand the syndesmosis anatomy and function Classify syndesmosis injuries Describe treatment
Quillen College of Medicine
 Ea s t T e n n e s s e e St a t e Un i v e r s i t y Quillen College of Medicine Failing to prepare is preparing to fail. John Wooden, UCL A Dr. Tom Kwasigroch Associate Dean Director, Medical Human Gross
Ea s t T e n n e s s e e St a t e Un i v e r s i t y Quillen College of Medicine Failing to prepare is preparing to fail. John Wooden, UCL A Dr. Tom Kwasigroch Associate Dean Director, Medical Human Gross
PUT YOUR BEST FOOT FORWARD
 PUT YOUR BEST FOOT FORWARD Bala Ramanan, MBBS 1 st year vascular surgery fellow Introduction The epidemic of diabetes and ageing of our population ensures critical limb ischemia will continue to grow.
PUT YOUR BEST FOOT FORWARD Bala Ramanan, MBBS 1 st year vascular surgery fellow Introduction The epidemic of diabetes and ageing of our population ensures critical limb ischemia will continue to grow.
MEDIAL HEAD GASTROCNEMIUS TEAR (Tennis Leg)
") MEDIAL HEAD GASTROCNEMIUS TEAR (Tennis Leg) Description Expected Outcome Medial head gastrocnemius tear is a strain of the inner part (medial head) of the major calf muscle (gastrocnemius muscle). Muscle
MEDIAL HEAD GASTROCNEMIUS TEAR (Tennis Leg) Description Expected Outcome Medial head gastrocnemius tear is a strain of the inner part (medial head) of the major calf muscle (gastrocnemius muscle). Muscle
Lecture 09. Popliteal Fossa. BY Dr Farooq Khan Aurakzai
 Lecture 09 Popliteal Fossa BY Dr Farooq Khan Aurakzai Dated: 14.02.2018 What is popliteus? Introduction Anything relating to, or near the part of the leg behind the knee. From New Latin popliteus the muscle
Lecture 09 Popliteal Fossa BY Dr Farooq Khan Aurakzai Dated: 14.02.2018 What is popliteus? Introduction Anything relating to, or near the part of the leg behind the knee. From New Latin popliteus the muscle
Femoral Artery. Its entrance to the thigh Position Midway between ASIS and pubic symphysis
 Lower Limb Vessels Lecture Objectives Describe the major arteries of the lower limb. Describe the deep and superficial veins of the lower limb. Describe the topographical relationships of the arteries
Lower Limb Vessels Lecture Objectives Describe the major arteries of the lower limb. Describe the deep and superficial veins of the lower limb. Describe the topographical relationships of the arteries
Introduction to Anatomy. Dr. Maher Hadidi. Laith Al-Hawajreh. Mar/25 th /2013
 Introduction to Anatomy Dr. Maher Hadidi Laith Al-Hawajreh 22 Mar/25 th /2013 Lower limb - The leg The skeleton of the leg is formed by two bones: 1) Medial: Tibia 2) Lateral: Fibula The two bones are
Introduction to Anatomy Dr. Maher Hadidi Laith Al-Hawajreh 22 Mar/25 th /2013 Lower limb - The leg The skeleton of the leg is formed by two bones: 1) Medial: Tibia 2) Lateral: Fibula The two bones are
MUSCLES OF THE LOWER LIMBS
 MUSCLES OF THE LOWER LIMBS Naming, location and general function Dr. Nabil khouri ROLES THAT SHOULD NOT BE FORGOTTEN Most anterior compartment muscles of the hip and thigh Flexor of the femur at the hip
MUSCLES OF THE LOWER LIMBS Naming, location and general function Dr. Nabil khouri ROLES THAT SHOULD NOT BE FORGOTTEN Most anterior compartment muscles of the hip and thigh Flexor of the femur at the hip
Gross Anatomy Coloring Book Series. Lower Extremity Arteries
 Gross Anatomy Coloring Book Series Lower Extremity Arteries 1 Femoral Artery and Associated Branches For the life of the flesh is in the blood. Leviticus 17:11 Femoral Artery and Associated Branches After
Gross Anatomy Coloring Book Series Lower Extremity Arteries 1 Femoral Artery and Associated Branches For the life of the flesh is in the blood. Leviticus 17:11 Femoral Artery and Associated Branches After
Ankle and Foot Orthopaedic Tests Orthopedics and Neurology DX 612
 Ankle and Foot Orthopaedic Tests Orthopedics and Neurology DX 612 James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Ankle & Foot Anatomy Stability of the ankle is dependent
Ankle and Foot Orthopaedic Tests Orthopedics and Neurology DX 612 James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Ankle & Foot Anatomy Stability of the ankle is dependent
Anatomy of Foot and Ankle
 Anatomy of Foot and Ankle Surface anatomy of the ankle & foot Surface anatomy of the ankle & foot Medial orientation point medial malleous sustentaculum tali tuberosity of navicular TA muscle TP muscle
Anatomy of Foot and Ankle Surface anatomy of the ankle & foot Surface anatomy of the ankle & foot Medial orientation point medial malleous sustentaculum tali tuberosity of navicular TA muscle TP muscle
ANKLE JOINT ANATOMY 3. TALRSALS = (FOOT BONES) Fibula. Frances Daly MSc 1 CALCANEUS 2. TALUS 3. NAVICULAR 4. CUBOID 5.
 Fibula. Frances Daly MSc 1 CALCANEUS 2. TALUS 3. NAVICULAR 4. CUBOID 5.") ANKLE JOINT ANATOMY The ankle joint is a synovial joint of the hinge type. The joint is formed by the distal end of the tibia and medial malleolus, the fibula and lateral malleolus and talus bone. It is
ANKLE JOINT ANATOMY The ankle joint is a synovial joint of the hinge type. The joint is formed by the distal end of the tibia and medial malleolus, the fibula and lateral malleolus and talus bone. It is
Case. 5 year old with 2 weeks leg pain and now refusing to walk + Fevers, lower leg swelling, warmth Denies and history of trauma or wounds
 Case 5 year old with 2 weeks leg pain and now refusing to walk + Fevers, lower leg swelling, warmth Denies and history of trauma or wounds Exam I: Swelling over entire tibia extending to foot P: Tenderness
Case 5 year old with 2 weeks leg pain and now refusing to walk + Fevers, lower leg swelling, warmth Denies and history of trauma or wounds Exam I: Swelling over entire tibia extending to foot P: Tenderness
Lumbar Plexus. Ventral rami L1 L4 Supplies: Major nerves.. Abdominal wall External genitalia Anteromedial thigh
 Lower Limb Nerves Lectures Objectives Describe the structure and relationships of the plexuses of the lower limb. Describe the course, relationships and structures supplied for the major nerves of the
Lower Limb Nerves Lectures Objectives Describe the structure and relationships of the plexuses of the lower limb. Describe the course, relationships and structures supplied for the major nerves of the
Cavus Foot: Subtle and Not-So-Subtle AOFAS Resident Review Course September 28, 2013
 Cavus Foot: Subtle and Not-So-Subtle Course September 28, 2013 Matthew M. Roberts, MD Associate Professor of Clinical Orthopaedic Surgery Co-Chief, Foot and Ankle Service Hospital for Special Surgery Disclosure
Cavus Foot: Subtle and Not-So-Subtle Course September 28, 2013 Matthew M. Roberts, MD Associate Professor of Clinical Orthopaedic Surgery Co-Chief, Foot and Ankle Service Hospital for Special Surgery Disclosure
BLUE SKY SCHOOL OF PROFESSIONAL MASSAGE AND THERAPEUTIC BODYWORK Musculoskeletal Anatomy & Kinesiology KNEE & ANKLE MUSCLES
 BLUE SKY SCHOOL OF PROFESSIONAL MASSAGE AND THERAPEUTIC BODYWORK Musculoskeletal Anatomy & Kinesiology KNEE & ANKLE MUSCLES MSAK201-I Session 3 1) REVIEW a) THIGH, LEG, ANKLE & FOOT i) Tibia Medial Malleolus
BLUE SKY SCHOOL OF PROFESSIONAL MASSAGE AND THERAPEUTIC BODYWORK Musculoskeletal Anatomy & Kinesiology KNEE & ANKLE MUSCLES MSAK201-I Session 3 1) REVIEW a) THIGH, LEG, ANKLE & FOOT i) Tibia Medial Malleolus
Versatility of Reverse Sural Artery Flap for Heel Reconstruction
 ORIGINAL ARTICLE Introduction: The heel has two parts, weight bearing and non-weight bearing part. Soft tissue heel reconstruction has been a challenge due to its complex nature of anatomy, weight bearing
ORIGINAL ARTICLE Introduction: The heel has two parts, weight bearing and non-weight bearing part. Soft tissue heel reconstruction has been a challenge due to its complex nature of anatomy, weight bearing
Injuries to the Hands and Feet
 Injuries to the Hands and Feet Chapter 24 Injuries to the Hands and Feet Introduction Combat injuries to the hands and feet differ from those of the arms and legs in terms of mortality and morbidity. The
Injuries to the Hands and Feet Chapter 24 Injuries to the Hands and Feet Introduction Combat injuries to the hands and feet differ from those of the arms and legs in terms of mortality and morbidity. The
Surgery-Ortho. Fractures of the tibia and fibula. Management. Treatment of low energy fractures. Fifth stage. Lec-6 د.
 Fifth stage Lec-6 د. مثنى Surgery-Ortho 28/4/2016 Indirect force: (low energy) Fractures of the tibia and fibula Twisting: spiral fractures of both bones Angulatory: oblique fractures with butterfly segment.
Fifth stage Lec-6 د. مثنى Surgery-Ortho 28/4/2016 Indirect force: (low energy) Fractures of the tibia and fibula Twisting: spiral fractures of both bones Angulatory: oblique fractures with butterfly segment.
Ankle Arthroscopy.
 Ankle Arthroscopy Key words: Ankle pain, ankle arthroscopy, ankle sprain, ankle stiffness, day case surgery, articular cartilage, chondral injury, chondral defect, anti-inflammatory medication Our understanding
Ankle Arthroscopy Key words: Ankle pain, ankle arthroscopy, ankle sprain, ankle stiffness, day case surgery, articular cartilage, chondral injury, chondral defect, anti-inflammatory medication Our understanding
Alberta Health Care Insurance Plan. Schedule Of Anaesthetic Rates Applicable To Podiatric Surgery. Procedure List. As Of.
 Alberta Health Care Insurance Plan Procedure List As Of 01 April 2016 Alberta Health Care Insurance Plan Page i Generated 2016/03/22 TABLE OF CONTENTS As of 2016/04/01 07 PHYSICAL MEDICINE, REHABILITATION,
Alberta Health Care Insurance Plan Procedure List As Of 01 April 2016 Alberta Health Care Insurance Plan Page i Generated 2016/03/22 TABLE OF CONTENTS As of 2016/04/01 07 PHYSICAL MEDICINE, REHABILITATION,
Compartment Syndrome
 Compartment Syndrome Dr Keith Holt Compartment syndrome is a relatively common disorder whereby pressure in one or more muscle compartments increases during exercise, causing progressively increasing pain,
Compartment Syndrome Dr Keith Holt Compartment syndrome is a relatively common disorder whereby pressure in one or more muscle compartments increases during exercise, causing progressively increasing pain,
Section Three: The Leg, Ankle, and Foot Lecture: Review of Clinical Anatomy, Patterns of Dysfunction and Injury, and
 Section Three: The Leg, Ankle, and Foot Lecture: Review of Clinical Anatomy, Patterns of Dysfunction and Injury, and Treatment Implications for the Leg, Ankle, and Foot Levels I and II Demonstration and
Section Three: The Leg, Ankle, and Foot Lecture: Review of Clinical Anatomy, Patterns of Dysfunction and Injury, and Treatment Implications for the Leg, Ankle, and Foot Levels I and II Demonstration and
MUSCULOSKELETAL LOWER LIMB
 MUSCULOSKELETAL LOWER LIMB Spinal Cord Lumbar and Sacral Regions Spinal cord Dorsal root ganglion Conus medullaris Cauda equina Dorsal root ganglion of the fifth lumbar nerve End of subarachnoid space
MUSCULOSKELETAL LOWER LIMB Spinal Cord Lumbar and Sacral Regions Spinal cord Dorsal root ganglion Conus medullaris Cauda equina Dorsal root ganglion of the fifth lumbar nerve End of subarachnoid space
Medial Tibial Stress Syndrom
 Medial Tibial Stress Syndrom Ministry of Health:- Hong Kong January 2007 Tibial Fasciitis, Shin Splints Tibial Stress Fracture Definition Overuse, Inflammatory condition Most common cause of lower limb
Medial Tibial Stress Syndrom Ministry of Health:- Hong Kong January 2007 Tibial Fasciitis, Shin Splints Tibial Stress Fracture Definition Overuse, Inflammatory condition Most common cause of lower limb
Located Deep to Flexor Retinaculum on medial aspect of ankle. Posterior to Posterior Tibial Artery. Tom, Dick, and Very Nervous Harry
 ANKLE BLOCK ANESTHESIA GREGORY CLARK D.P.M. HEAD, SECTION OF PODIATRY SCRIPPS CLINIC LA JOLLA, CALIFORNIA A METHOD BY WHICH ONE MAY PROVIDE AN ANESTHETIC BLOCK TO THE FOOT OR ANKLE WITH A MINIMUM OF PATIENT
ANKLE BLOCK ANESTHESIA GREGORY CLARK D.P.M. HEAD, SECTION OF PODIATRY SCRIPPS CLINIC LA JOLLA, CALIFORNIA A METHOD BY WHICH ONE MAY PROVIDE AN ANESTHETIC BLOCK TO THE FOOT OR ANKLE WITH A MINIMUM OF PATIENT
Surgical Technique. Achilles Tendon Repair Using Conexa Reconstructive Tissue Matrix. conexatm. Surgical Technique Described by Tom Chang, DPM
 Surgical Technique Achilles Tendon Repair Using Conexa Reconstructive Tissue Matrix Surgical Technique Described by Tom Chang, DPM conexatm r e c o n s t r u c t i v e t i s s u e m a t r i x Achilles
Surgical Technique Achilles Tendon Repair Using Conexa Reconstructive Tissue Matrix Surgical Technique Described by Tom Chang, DPM conexatm r e c o n s t r u c t i v e t i s s u e m a t r i x Achilles
Compartment Syndrome
 Compartment Syndrome Andrew H. Schmidt, M.D. Professor, Dept. of Orthopedic Surgery, Univ. of Minnesota Chief, Department of Orthopaedic Surgery Hennepin County Medical Center April 2016 Disclosure Information
Compartment Syndrome Andrew H. Schmidt, M.D. Professor, Dept. of Orthopedic Surgery, Univ. of Minnesota Chief, Department of Orthopaedic Surgery Hennepin County Medical Center April 2016 Disclosure Information
So#- Tissue Manipula0on: Supine
 So#- Tissue Manipula0on: Supine Gastrocnemius and soleus stretch Use stretching in the later stages of rehabilita0on Check in with the client as you go to avoid painful tearing Perform joint mobiliza0on
So#- Tissue Manipula0on: Supine Gastrocnemius and soleus stretch Use stretching in the later stages of rehabilita0on Check in with the client as you go to avoid painful tearing Perform joint mobiliza0on
musculoskeletal system anatomy muscles of foot sheet done by: dina sawadha & mohammad abukabeer
 musculoskeletal system anatomy muscles of foot sheet done by: dina sawadha & mohammad abukabeer Extensor retinaculum : A- superior extensor retinaculum (SER) : originates from the distal ends of the tibia
musculoskeletal system anatomy muscles of foot sheet done by: dina sawadha & mohammad abukabeer Extensor retinaculum : A- superior extensor retinaculum (SER) : originates from the distal ends of the tibia
Type II Type III Type IV Triplane
 Fracture in Children [Salter And Harris] Type II Type III Type IV Triplane Surgical Rx III and IV Type II, V Non-operative treatment Type I, II When not reduced ORIF Type III ORIF Informed consent: about
Fracture in Children [Salter And Harris] Type II Type III Type IV Triplane Surgical Rx III and IV Type II, V Non-operative treatment Type I, II When not reduced ORIF Type III ORIF Informed consent: about
Safe corridors in external fixation: the lower leg (tibia, fibula, hindfoot and forefoot)
") Strat Traum Limb Recon (2007) 2:105 110 DOI 10.1007/s11751-007-0023-7 REVIEW Safe corridors in external fixation: the lower leg (tibia, fibula, hindfoot and forefoot) Selvadurai Nayagam Received: 9 August
Strat Traum Limb Recon (2007) 2:105 110 DOI 10.1007/s11751-007-0023-7 REVIEW Safe corridors in external fixation: the lower leg (tibia, fibula, hindfoot and forefoot) Selvadurai Nayagam Received: 9 August
TENDON TRANSFER IN CAVUS FOOT
 TENDON TRANSFER IN CAVUS FOOT Cavovarus deformity is defined by fixed equinus of the forefoot on the hindfoot, resulting in a pathologic elevation of the longitudinal arch, with either a fixed or flexible
TENDON TRANSFER IN CAVUS FOOT Cavovarus deformity is defined by fixed equinus of the forefoot on the hindfoot, resulting in a pathologic elevation of the longitudinal arch, with either a fixed or flexible
بسم هللا الرحمن الرحيم
 بسم هللا الرحمن الرحيم Laboratory RHS 221 Manual Muscle Testing Theory 1 hour practical 2 hours Dr. Ali Aldali, MS, PT Department of Physical Therapy King Saud University Talocrural and Subtalar Joint
بسم هللا الرحمن الرحيم Laboratory RHS 221 Manual Muscle Testing Theory 1 hour practical 2 hours Dr. Ali Aldali, MS, PT Department of Physical Therapy King Saud University Talocrural and Subtalar Joint
FACTS 1. Most need only Gastro aponeurotic release [in positive Silverskiold test]
![FACTS 1. Most need only Gastro aponeurotic release [in positive Silverskiold test]](/thumbs/83/88335212.jpg "FACTS 1. Most need only Gastro aponeurotic release [in positive Silverskiold test]") FOOT IN CEREBRAL PALSY GAIT IN CEREBRAL PALSY I True Equinus II Jump gait III Apparent Equinus IV Crouch gait Group I True Equinus Extended hip and knee Equinus at ankle II Jump Gait [commonest] Equinus
FOOT IN CEREBRAL PALSY GAIT IN CEREBRAL PALSY I True Equinus II Jump gait III Apparent Equinus IV Crouch gait Group I True Equinus Extended hip and knee Equinus at ankle II Jump Gait [commonest] Equinus
ANKLE PLANTAR FLEXION
 ANKLE PLANTAR FLEXION Evaluation and Measurements By Isabelle Devreux 1 Ankle Plantar Flexion: Gastrocnemius and Soleus ROM: 0 to 40-45 A. Soleus: Origin: Posterior of head of fibula and proximal1/3 of
ANKLE PLANTAR FLEXION Evaluation and Measurements By Isabelle Devreux 1 Ankle Plantar Flexion: Gastrocnemius and Soleus ROM: 0 to 40-45 A. Soleus: Origin: Posterior of head of fibula and proximal1/3 of
Results of Calcaneal Osteotomy & Flexor Digitorum Longus transfer in Stage II Acquired Flatfoot Deformity
 Results of Calcaneal Osteotomy & Flexor Digitorum Longus transfer in Stage II Acquired Flatfoot Deformity Mr Amit Chauhan Mr Prasad Karpe Ms Maire-claire Killen Mr Rajiv Limaye University Hospital of North
Results of Calcaneal Osteotomy & Flexor Digitorum Longus transfer in Stage II Acquired Flatfoot Deformity Mr Amit Chauhan Mr Prasad Karpe Ms Maire-claire Killen Mr Rajiv Limaye University Hospital of North
Muscles of the Hip 1. Tensor Fasciae Latae O: iliac crest I: lateral femoral condyle Action: abducts the thigh Nerve: gluteal nerve
 Muscles of the Hip 1. Tensor Fasciae Latae O: iliac crest I: lateral femoral condyle Action: abducts the thigh Nerve: gluteal nerve 2. Gluteus Maximus O: ilium I: femur Action: abduct the thigh Nerve:
Muscles of the Hip 1. Tensor Fasciae Latae O: iliac crest I: lateral femoral condyle Action: abducts the thigh Nerve: gluteal nerve 2. Gluteus Maximus O: ilium I: femur Action: abduct the thigh Nerve:
حسام أبو عوض. - Ahmad. 1 P a g e
 - 9 حسام أبو عوض - - Ahmad 1 P a g e In the last lecture, we finished discussing the superficial part of the posterior compartment and the popliteus muscle of the deep layer[reminder: The entire posterior
- 9 حسام أبو عوض - - Ahmad 1 P a g e In the last lecture, we finished discussing the superficial part of the posterior compartment and the popliteus muscle of the deep layer[reminder: The entire posterior
Alberta Health Care Insurance Plan. Schedule Of Anaesthetic Rates Applicable To Podiatry. Procedure List. As Of. 01 April Government of Alberta
 Alberta Health Care Insurance Plan Procedure List As Of 01 April 2017 Alberta Health Care Insurance Plan Page i Generated 2017/03/14 TABLE OF CONTENTS As of 2017/04/01 II. OPERATIONS ON THE NERVOUS SYSTEM.......................
Alberta Health Care Insurance Plan Procedure List As Of 01 April 2017 Alberta Health Care Insurance Plan Page i Generated 2017/03/14 TABLE OF CONTENTS As of 2017/04/01 II. OPERATIONS ON THE NERVOUS SYSTEM.......................
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 18 Orthopedic Trauma Key Points 2 18.1 Upper Extremity Injuries Clavicle Fractures Diagnose fractures from the history and by physical examination Treat with a
Surgical Care at the District Hospital 1 18 Orthopedic Trauma Key Points 2 18.1 Upper Extremity Injuries Clavicle Fractures Diagnose fractures from the history and by physical examination Treat with a
OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries. Differentiate when an orthopedic injury is a medical emergency
 1 2 How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency
1 2 How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency
CHAPTER 16 LOWER EXTREMITY. Amanda K Silva, MD and Warren Ellsworth, MD, FACS
 CHAPTER 16 LOWER EXTREMITY Amanda K Silva, MD and Warren Ellsworth, MD, FACS The plastic and reconstructive surgeon is often called upon to treat many wound problems of the lower extremity. These include
CHAPTER 16 LOWER EXTREMITY Amanda K Silva, MD and Warren Ellsworth, MD, FACS The plastic and reconstructive surgeon is often called upon to treat many wound problems of the lower extremity. These include
Tibial Shaft Fractures
 Tibial Shaft Fractures Mr Krishna Vemulapalli Consultant Orthopaedics Surgeon Queens & King George Hospitals Queens Hospital 14/03/2018 Google Maps Map data 2018 Google 10 km Orthopaedics Department Covers
Tibial Shaft Fractures Mr Krishna Vemulapalli Consultant Orthopaedics Surgeon Queens & King George Hospitals Queens Hospital 14/03/2018 Google Maps Map data 2018 Google 10 km Orthopaedics Department Covers
Ankle Sprains and Their Imitators
 Ankle Sprains and Their Imitators Mark Halstead, MD Dr. Mark Halstead is the Associate Professor of the Departments of Orthopedics and Pediatrics at Washington University School of Medicine; Director of
Ankle Sprains and Their Imitators Mark Halstead, MD Dr. Mark Halstead is the Associate Professor of the Departments of Orthopedics and Pediatrics at Washington University School of Medicine; Director of
DISSECTION SCHEDULE. Session I - Hip (Front) & Thigh (Superficial)
 & Thigh (Superficial)") DISSECTION SCHEDULE Session I - Hip (Front) & Thigh (Superficial) Surface anatomy Inguinal region Gluteal region Thigh Leg Foot bones Hip bone Femur Superficial fascia Great saphenous vein Superficial
DISSECTION SCHEDULE Session I - Hip (Front) & Thigh (Superficial) Surface anatomy Inguinal region Gluteal region Thigh Leg Foot bones Hip bone Femur Superficial fascia Great saphenous vein Superficial
EDL EHL. Extensor Hallucis Longus L5 Extensor Digitorum longus L5,1 Peroneus Tertius L5 1 Extensor Digitorum Brevis S1,2 [like intrinsic muscle]
![EDL EHL. Extensor Hallucis Longus L5 Extensor Digitorum longus L5,1 Peroneus Tertius L5 1 Extensor Digitorum Brevis S1,2 [like intrinsic muscle]](/thumbs/78/77875930.jpg "EDL EHL. Extensor Hallucis Longus L5 Extensor Digitorum longus L5,1 Peroneus Tertius L5 1 Extensor Digitorum Brevis S1,2 [like intrinsic muscle]") ANATOMY OF ANKLE AND FOOT Lateral aspect: [Dorsal medial to lateral= dorsal under extensor retinaculum] Tibialis Anterior EHL Artery [Dorsal pedal A] and Anterior tibial N EDL Peroneus Tertius Behind the
ANATOMY OF ANKLE AND FOOT Lateral aspect: [Dorsal medial to lateral= dorsal under extensor retinaculum] Tibialis Anterior EHL Artery [Dorsal pedal A] and Anterior tibial N EDL Peroneus Tertius Behind the
Main Menu. Ankle and Foot Joints click here. The Power is in Your Hands
 1 The Ankle and Foot Joints click here Main Menu Copyright HandsOn Therapy Schools 2009 K.8 http://www.handsonlineeducation.com/classes/k8/k8entry.htm[3/27/18, 1:40:03 PM] Ankle and Foot Joint 26 bones
1 The Ankle and Foot Joints click here Main Menu Copyright HandsOn Therapy Schools 2009 K.8 http://www.handsonlineeducation.com/classes/k8/k8entry.htm[3/27/18, 1:40:03 PM] Ankle and Foot Joint 26 bones
How to Triage Orthopaedic Care. David W. Gray, M.D.
 How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency Determine
How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency Determine
Understanding Leg Anatomy and Function THE UPPER LEG
 Understanding Leg Anatomy and Function THE UPPER LEG The long thigh bone is the femur. It connects to the pelvis to form the hip joint and then extends down to meet the tibia (shin bone) at the knee joint.
Understanding Leg Anatomy and Function THE UPPER LEG The long thigh bone is the femur. It connects to the pelvis to form the hip joint and then extends down to meet the tibia (shin bone) at the knee joint.
Posterior Tibialis Tendon Dysfunction & Repair
 1 Posterior Tibialis Tendon Dysfunction & Repair Surgical Indications and Considerations Anatomical Considerations: The posterior tibialis muscle arises from the interosseous membrane and the adjacent
1 Posterior Tibialis Tendon Dysfunction & Repair Surgical Indications and Considerations Anatomical Considerations: The posterior tibialis muscle arises from the interosseous membrane and the adjacent
Lower Extremity Dislocations: Management and Triage on the Field
 Lower Extremity Dislocations: Management and Triage on the Field Scott J Tarantino, MD Towson Orthopaedic Associates, Towson, MD None Disclsures Purpose To provide you with knowledge which may guide you
Lower Extremity Dislocations: Management and Triage on the Field Scott J Tarantino, MD Towson Orthopaedic Associates, Towson, MD None Disclsures Purpose To provide you with knowledge which may guide you
Sports Injuries of the Ankle and Ankle Arthritis. Mr Amit Amin Consultant Foot and Ankle Surgeon Parkside Hospital
 Sports Injuries of the Ankle and Ankle Arthritis Mr Amit Amin Consultant Foot and Ankle Surgeon Parkside Hospital Impingement Painful mechanical limitation of full ankle movement secondary to osseous
Sports Injuries of the Ankle and Ankle Arthritis Mr Amit Amin Consultant Foot and Ankle Surgeon Parkside Hospital Impingement Painful mechanical limitation of full ankle movement secondary to osseous
Tibial and Common Peroneal Nerve Compression in The Popliteal Fossa: A Case Report and Literature Review
 ISPUB.COM The Internet Journal of Plastic Surgery Volume 2 Number 1 Tibial and Common Peroneal Nerve Compression in The Popliteal Fossa: A Case Report and Literature D Reichner, G Evans Citation D Reichner,
ISPUB.COM The Internet Journal of Plastic Surgery Volume 2 Number 1 Tibial and Common Peroneal Nerve Compression in The Popliteal Fossa: A Case Report and Literature D Reichner, G Evans Citation D Reichner,
Tarsal Tunnel Syndrome
 43 Thames Street, St Albans, Christchurch 8013 Phone: (03) 356 1353. Website: philip-bayliss.com Tarsal Tunnel Syndrome The foot is subjected to forces hundreds of times the bodyweight, thousands of times
43 Thames Street, St Albans, Christchurch 8013 Phone: (03) 356 1353. Website: philip-bayliss.com Tarsal Tunnel Syndrome The foot is subjected to forces hundreds of times the bodyweight, thousands of times
Therapeutic Foot Care Certificate Program Part I: Online Home Study Program
 Therapeutic Foot Care Certificate Program Part I: Online Home Study Program 1 Anatomy And Terminology Of The Lower Extremity Joan E. Edelstein, MA, PT, FISPO Associate Professor of Clinical Physical Therapy
Therapeutic Foot Care Certificate Program Part I: Online Home Study Program 1 Anatomy And Terminology Of The Lower Extremity Joan E. Edelstein, MA, PT, FISPO Associate Professor of Clinical Physical Therapy
Unrecognized acute exertional compartment syndrome of the leg and treatment
 Acta Orthop. Belg., 2011, 77, 265-269 CASE REPORT Unrecognized acute exertional compartment syndrome of the leg and treatment Nebojsa POPOviC, Craig BOTTONi, Charles CASSiDy From Aspetar, Qatar Orthopaedic
Acta Orthop. Belg., 2011, 77, 265-269 CASE REPORT Unrecognized acute exertional compartment syndrome of the leg and treatment Nebojsa POPOviC, Craig BOTTONi, Charles CASSiDy From Aspetar, Qatar Orthopaedic
Dr Nabil khouri MD. MSc. Ph.D
 Dr Nabil khouri MD. MSc. Ph.D Foot Anatomy The foot consists of 26 bones: 14 phalangeal, 5 metatarsal, and 7 tarsal. Toes are used to balance the body. Metatarsal Bones gives elasticity to the foot in
Dr Nabil khouri MD. MSc. Ph.D Foot Anatomy The foot consists of 26 bones: 14 phalangeal, 5 metatarsal, and 7 tarsal. Toes are used to balance the body. Metatarsal Bones gives elasticity to the foot in
Welcome to the: Orthopaedic Opinion Online Website The website for the answer to all your Orthopaedic Questions
 Welcome to the: Orthopaedic Opinion Online Website The website for the answer to all your Orthopaedic Questions Orthopaedic Opinion Online is a website designed to provide information to patients who have
Welcome to the: Orthopaedic Opinion Online Website The website for the answer to all your Orthopaedic Questions Orthopaedic Opinion Online is a website designed to provide information to patients who have
The Lower Limb II. Anatomy RHS 241 Lecture 3 Dr. Einas Al-Eisa
 The Lower Limb II Anatomy RHS 241 Lecture 3 Dr. Einas Al-Eisa Tibia The larger & medial bone of the leg Functions: Attachment of muscles Transfer of weight from femur to skeleton of the foot Articulations
The Lower Limb II Anatomy RHS 241 Lecture 3 Dr. Einas Al-Eisa Tibia The larger & medial bone of the leg Functions: Attachment of muscles Transfer of weight from femur to skeleton of the foot Articulations
Susan Bettcher, MD and Chad Asplund, MD The Ohio State University. exertional compartment syndrome. To minimize confusion, the terms exerciseinduced
 PHYSICIAN PERSPECTIVE Tracy Ray, MD, AMSSM Member, Report Editor Exertional Leg Pain Susan Bettcher, MD and Chad Asplund, MD The Ohio State University EXERCISE-INDUCED leg pain is a common condition in
PHYSICIAN PERSPECTIVE Tracy Ray, MD, AMSSM Member, Report Editor Exertional Leg Pain Susan Bettcher, MD and Chad Asplund, MD The Ohio State University EXERCISE-INDUCED leg pain is a common condition in
Chapter 30 - Musculoskeletal_Trauma
 Introduction to Emergency Medical Care 1 OBJECTIVES 30.1 Define key terms introduced in this chapter. Slides 11 12, 19 20, 22 23, 37 30.2 Describe the anatomy of elements of the musculoskeletal system.
Introduction to Emergency Medical Care 1 OBJECTIVES 30.1 Define key terms introduced in this chapter. Slides 11 12, 19 20, 22 23, 37 30.2 Describe the anatomy of elements of the musculoskeletal system.
A Patient s Guide to Knee Anatomy. Stephanie E. Siegrist, MD, LLC
 A Patient s Guide to Knee Anatomy Hands, shoulders, knees and toes (and elbows and ankles, too!) Most bone and joint conditions have several treatment options. The best treatment for you is based on your
A Patient s Guide to Knee Anatomy Hands, shoulders, knees and toes (and elbows and ankles, too!) Most bone and joint conditions have several treatment options. The best treatment for you is based on your
Human Anatomy Biology 351
 Human Anatomy Biology 351 Lower Limb Please place your name on the back of the last page of this exam. You must answer all questions on this exam. Because statistics demonstrate that, on average, between
Human Anatomy Biology 351 Lower Limb Please place your name on the back of the last page of this exam. You must answer all questions on this exam. Because statistics demonstrate that, on average, between
Practice Changes I Hope You Make
 Is that Bad? What PCPs (& Parents) Need to Know about Fractures Aharon Z. Gladstein, MD Pediatric Orthopaedics & Sports Medicine Texas Children s Hospital Assistant Professor, Orthopaedics Baylor College
Is that Bad? What PCPs (& Parents) Need to Know about Fractures Aharon Z. Gladstein, MD Pediatric Orthopaedics & Sports Medicine Texas Children s Hospital Assistant Professor, Orthopaedics Baylor College
TRANSTIBIAL AMPUTATION General Principles & Update on Surgical Techniques
 TRANSTIBIAL AMPUTATION General Principles & Update on Surgical Techniques Douglas G. Smith, MD Harborview Medical Center and University of Washington - Emeritus Prosthetic Research Study Amputee Coalition
TRANSTIBIAL AMPUTATION General Principles & Update on Surgical Techniques Douglas G. Smith, MD Harborview Medical Center and University of Washington - Emeritus Prosthetic Research Study Amputee Coalition
5.1 Identify, describe the attachments of and deduce the actions of the muscles of the thigh:
 5.1 Identify, describe the attachments of and deduce the actions of the muscles of the thigh: Anterior group Proximal attachment Distal attachment Sartorius ASIS» Upper part of shaft tibia (middle surface)»
5.1 Identify, describe the attachments of and deduce the actions of the muscles of the thigh: Anterior group Proximal attachment Distal attachment Sartorius ASIS» Upper part of shaft tibia (middle surface)»
Knee Dislocation: Spectrum of Injury, Evolution of Treatment & Modern Outcomes
 Knee Dislocation: Spectrum of Injury, Evolution of Treatment & Modern Outcomes William M Weiss, MD MSc FRCSC Orthopedic Surgery & Rehabilitation Sports Medicine, Arthroscopy & Extremity Reconstruction
Knee Dislocation: Spectrum of Injury, Evolution of Treatment & Modern Outcomes William M Weiss, MD MSc FRCSC Orthopedic Surgery & Rehabilitation Sports Medicine, Arthroscopy & Extremity Reconstruction
Treatment of Acute Traumatic Knee Dislocations
 Treatment of Acute Traumatic Knee Dislocations Angelo J. Colosimo, MD Head Orthopaedic Surgeon University of Cincinnati Athletics Director of Sports Medicine University of Cincinnati Medical Center Associate
Treatment of Acute Traumatic Knee Dislocations Angelo J. Colosimo, MD Head Orthopaedic Surgeon University of Cincinnati Athletics Director of Sports Medicine University of Cincinnati Medical Center Associate
Muscles of the lower extremities. Dr. Nabil khouri MD, MSc, Ph.D
 Muscles of the lower extremities Dr. Nabil khouri MD, MSc, Ph.D Posterior leg Popliteal fossa Boundaries Biceps femoris (superior-lateral) Semitendinosis and semimembranosis (superior-medial) Gastrocnemius
Muscles of the lower extremities Dr. Nabil khouri MD, MSc, Ph.D Posterior leg Popliteal fossa Boundaries Biceps femoris (superior-lateral) Semitendinosis and semimembranosis (superior-medial) Gastrocnemius
THE LOWER LIMB NERVES VESSELS
 THE LOWER LIMB NERVES VESSELS LOWER LIMB: FEMORAL TRIANGLE FEMORAL TRIANGLE LOWER LIMB: FEMORAL TRIANGLE FEMORAL TRIANGLE is a triangular landmark useful in dissection and in understanding relationships
THE LOWER LIMB NERVES VESSELS LOWER LIMB: FEMORAL TRIANGLE FEMORAL TRIANGLE LOWER LIMB: FEMORAL TRIANGLE FEMORAL TRIANGLE is a triangular landmark useful in dissection and in understanding relationships
A Patient s Guide to Ankle Anatomy
 A Patient s Guide to Ankle Anatomy 245 North College Lafayette, LA 70506 Phone: 337.232.5301 Fax: 337.237.6504 DISCLAIMER: The information in this booklet is compiled from a variety of sources. It may
A Patient s Guide to Ankle Anatomy 245 North College Lafayette, LA 70506 Phone: 337.232.5301 Fax: 337.237.6504 DISCLAIMER: The information in this booklet is compiled from a variety of sources. It may
Chronic Exertional Compartment Syndrome
 Michael J. Fraipont, MD, and Gregory J. Adamson, MD Abstract Chronic exertional compartment syndrome is an often overlooked and uncommon cause of pain in the extremities of individuals who engage in repetitive
Michael J. Fraipont, MD, and Gregory J. Adamson, MD Abstract Chronic exertional compartment syndrome is an often overlooked and uncommon cause of pain in the extremities of individuals who engage in repetitive
A Patient s Guide to Ankle Anatomy
 A Patient s Guide to Ankle Anatomy Pond View Professional Park 301 Professional View Drive Freehold, NJ 07728 Phone: 732-720-2555 DISCLAIMER: The information in this booklet is compiled from a variety
A Patient s Guide to Ankle Anatomy Pond View Professional Park 301 Professional View Drive Freehold, NJ 07728 Phone: 732-720-2555 DISCLAIMER: The information in this booklet is compiled from a variety