Optimizing Osteoporosis Management Dr. Philip A. Baer Seacourses Asia CME December 2017
|
|
|
- Charles Warner
- 6 years ago
- Views:
Transcription

1
2 Optimizing Osteoporosis Management Dr. Philip A. Baer Seacourses Asia CME December 2017
3 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or mechanical, including photocopying, recording, or information storage and retrieval systems without prior written permission of Sea Courses Inc. except where permitted by law. Sea Courses is not responsible for any speaker or participant s statements, materials, acts or omissions.

4
5 Learning Objectives Upon completion of this program participants will be able to: 1. Discuss the clinical impact of fractures and the current care gap in osteoporosis. 2. Evaluate a patient s individualized risk of osteoporotic fracture utilizing a practical risk assessment tool. 3. Treat osteoporosis based on the 2010 Osteoporosis Canada guideline. 4. Analyze controversies surrounding osteoporosis therapy.


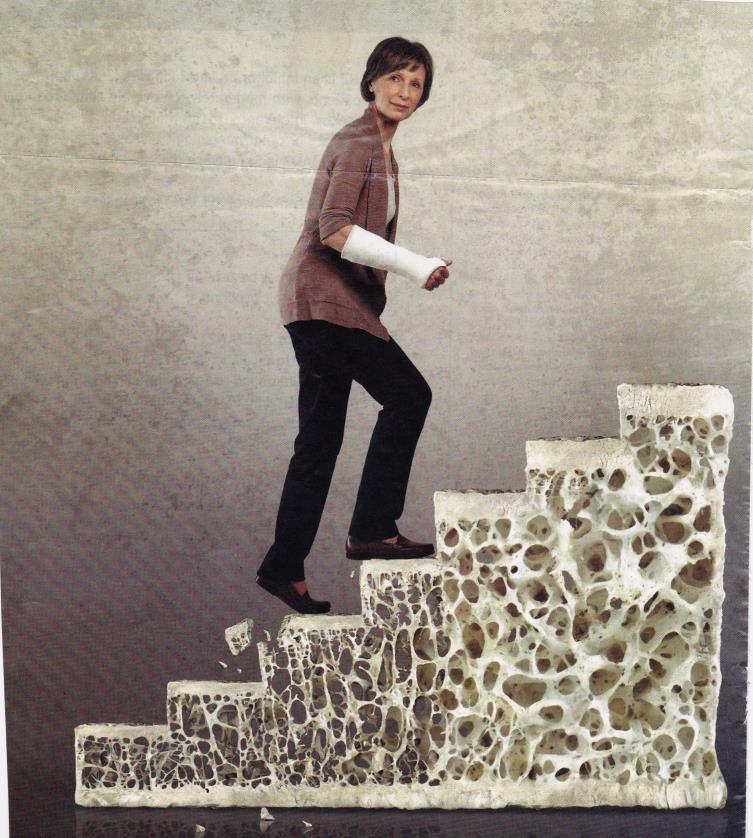
6 Definition of Osteoporosis Normal Bone Osteoporotic Bone WHO Definition 1 Osteoporosis is a systemic skeletal disease characterized by low bone density and microarchitectural deterioration of bone tissue with a consequent increase in bone fragility. NIH Definition 2 Osteoporosis is defined as a skeletal disorder characterized by compromised bone strength predisposing a person to an increased risk of fracture. Bone strength reflects the integration of 2 main features: bone density and bone quality. 1. Genant HK et al. Osteoporos Int 1999;10: NIH Consensus Development Panel on Osteoporosis Prevention, Diagnosis, and Therapy. JAMA 2001;285:

7 Osteoporotic Fracture = Fragility Fracture He tried a little hip-hop. One hop and he broke a hip.
8 Fragility Fracture: Definition A fracture occurring spontaneously or following minor trauma such as a fall from standing height or less 1,2 Excluding craniofacial, hand, ankle and foot fractures 1. Kanis JA, et al. Osteoporos Int 2001; 12(5): Bessette L, et al. Osteoporos Int 2008; 19:79-86.



9 Osteoporosis: Fractures Primarily of Cortical Bone Humerus Tibia Femoral Neck Images courtesy of Dr Robert Josse


10 Osteoporosis: Fractures Primarily of Trabecular Bone Vertebral Vertebral Femur Inter-trochanteric Images courtesy of Dr Robert Josse
11 Burden of Osteoporosis
12 Annual incidence of common diseases Prevalence of Fractures in Canada Fractures from osteoporosis in Canadian women are more common than heart attack, stroke and breast cancer combined 1 200, , ,400 41,500 Other 80,000 40, ,900 Vertebral 32,700 Wrist 30,000 Hip * 10,300 Pelvis Osteoporotic fractures 1,2 49,220 29,874 22,700 Heart Stroke 3 Breast Attack 3 Cancer 4 * Canadian hip fractures from (1); Non-hip fracture data extrapolated from (2). Other represents non-osteoporotic fractures sites (humerus, clavicle, hands/fingers, patella, tibia, fibula) Leslie WD, et al. Osteoporos Int. 2010; 21: ; 2. Burge J, et al. J Bone Miner Res. 2007;22: ; 3. Canadian Institute for Health Information (2009) Health Indicators. ; 4. Canadian Cancer Society


13 Timeline: Consequences post fracture Lifetime risk of hip fracture in women >50 is 12.1% 5 Fracture Begets Future Fracture Deteriorated Quality of Life Long-term Care Admission Mortality 40% 40% 18% 23% In women with hip fracture: 40% had prior fracture 1 In women with hip fracture: 40% need assistance walking 2 In women with hip fracture: 18% enter LTC 3 In women with hip fracture: 23% die within 1 year 4 1. Hajcsar EE, et al. CMAJ 2000, 163: ; 2. Cooper C. Am J Med. 1997:103:12S-19S; 3. Jean et al. JBMR 2013; 28: Ioannidis G, et al. CMAJ 2009;181: Hopkins et al.osteo Intl 2012; 23:

14 Why is this Important to Family Physicians? Osteoporosis is managed primarily by Family Practitioners in Canada Based on Canadian prescriptions of osteoporosis therapies Source: IMSB, Compuscript (Aug 11)


15 Percentage of patients (%) Only 15% of Patients are Treated After an Osteoporotic Fracture A fracture is to osteoporosis what a heart attack is to cardiovascular disease 100% 80% 60% 40% How do we shift this paradigm? 80% 20% 15% 0% Osteoporosis Treatment Post Fracture 1 Beta Blockers Post Heart Attack 2 A history of fracture is the strongest predictor of new fractures, yet post-fracture treatment rates remain low 1. Bessette L, et al. Osteoporos Int. 2008;19: Austin PC, et al. CMAJ. 2008;179:
16 The osteoporosis care gap


17 Sending a letter to the primary care physician after a patient s fracture doubled rates of BMD testing and pharmacologic therapy versus usual care
18 Identifying Patients at High Risk for Fracture
19 Audience Question Is a BMD T-score of -2.5 alone sufficient to diagnose osteoporosis? A. Yes B. No Is a BMD T-score of -2.5 alone sufficient to treat osteoporosis? A. Yes B. No



 Adapted from Siris")
20 BMD is not the Sole Predictor of Fracture Risk 60% of women with fractures have non-osteoporotic bone mineral density (T-score >-2.5) Adapted from Siris ES, et al. JAMA.
21 Fracture rate per 1000 person-years No of Fractures BMD vs. Osteoporotic Fracture Rates/Number 60 BMD distribution 450 Fracture Rate No of Fractures % of women with fragility fractures have non-osteoporotic bone mineral density (T-score >-2.5) > to to to to 3.0 < to to to 1.5 BMD T-scores 2.0 to to 3.5 Adapted from Siris ES, et al: JAMA 2001; 286:
22 OP: Contributors To Bone Strength Bone Quantity Bone Quality Bone Density Bone Turnover Bone Architecture Bone Mineral 22
 Borah et al, The Anatomical Record, 265:101-110, 2001.")
23 Healthy Versus Osteoporotic Bone: MicroCT 52 year old Female 84 year old Female (with vertebral fracture) Borah et al, The Anatomical Record, 265: , 2001.
 by decreasing the effective length of a")
24 Bone Architecture: Key Factor in Bone Strength Euler Buckling Theory: A column will buckle at critical load as a function of: column material crosssectional geometry the length of the column 4 X stronger 16 X stronger Adding horizontal struts to a structure exponentially increases strength (increases buckling load) by decreasing the effective length of a column 24


25 2010 Canadian Osteoporosis Guidelines


26 Who Should Be Screened for Osteoporosis Women (and men) over the age of 50 Any individual with a history of fragility fracture A detailed history and physical exam can help identify individuals at high risk of fractures Papaioannou A, et al CMAJ *Fracture image courtesy of Dr Robert Josse
27 Major Risk Factors for Osteoporosis Age 65 years Vertebral compression fracture Fragility fracture after age 40 Family history of osteoporotic fracture (especially maternal hip fracture) Brown JP, Josse RG. CMAJ 2002;167(10 suppl):s1-s34.
?\" 2. LOOK - Is there kyphosis? - Ability to perform the Get up and Go Test 3.")

28 Three Steps for Quick Screening in Office 1. ASK Since the last visit... "Have you broken any bones? "Have you fallen? "Have you had prolonged and unusual back pain? "Have you received oral or intravenous steroids (cortisone)?" 2. LOOK - Is there kyphosis? - Ability to perform the Get up and Go Test 3. MEASURE The patient s height Rib to pelvis distance Occiput-to-wall distance EMR reminder tools may help to prompt screening 4 1. Siminoski K et al. Osteoporos Int. 2006;17: Papaioannou A, et al CMAJ Timed Up-and-go test. Available at: 4. Loo TS et al. Arch Intern Med 171:
29 Screening for Osteoporosis: When to do a BMD 1 Aged 65 years Aged years Aged <50 years Everyone One or more risk factors for fracture: o Fragility fracture after age 40 o Parental hip fracture o Vertebral fracture or osteopenia identified on radiography o Medication with high risk of bone loss (i.e. steroids) o Smoking, alcohol ( 3/d) o Disorders associated with osteoporosis (i.e. RA) o Low weight or major weight loss 2 causes of osteoporosis (i.e. malabsorption) Prior fragility fracture Medication with high risk of bone loss Clinical Note: If you are ordering unrelated imaging (e.g. chest x-ray) for your patient, consider adding rule out vertebral fracture on the order Papaioannou A, et al CMAJ 2010;182: Steering Group Communications Feb 9 th 2012.

30

31 Fracture Risk Assessment
32 68 year old woman Osteoporosis Case 1 BMD done because of age Femoral neck T-score 1.4 Prior vertebral compression fracture She asks what her fracture risk is over the next 10 years




33 There are Two Tools Available for Fracture Risk Assessment These tools incorporate other clinical risk factors for fracture in addition to BMD 1. OC Guidelines tool available at: 2. FRAX tool available at: 3. National Osteoporosis Foundation guidelines:
34 Femoral Neck T-score Calculating 10-Year Absolute Fracture Risk for Postmenopausal Women: CAROC Increases to the next risk category Prior fragility fracture after age 40 Prolonged corticosteroid therapy* 10-year absolute fracture risk in treatment naïve women combining femoral neck T-score and age Low Risk < 10% Moderate Risk 10% 20% Age (years) High Risk >20% Prior hip or vertebral fracture, or >1 nonvertebral fragility fracture Lumbar spine or total hip T-score -2.5: consider the individual to be at least at moderate risk Calibrated using Canadian fracture data and have been directly validated in Canadians 2 *At least three months cumulative use during the preceding year at a prednisone-equivalent dose 7.5 mg daily 1. Papaioannou A, et al. CMAJ. 2010;182: Leslie WD, et al. J Bone Miner Res. 2009;24:
35 68 year old woman Osteoporosis Case 1 BMD done because of age Femoral neck T-score 1.4 Prior vertebral compression fracture She asks what her fracture risk is over the next 10 years Answer: High
36 Pharmacological therapy should be offered to patients at high fracture risk 10-year fracture risk > 20% HIGH RISK OR Prior fragility fracture of hip or spine OR > 1 fragility fracture Papaioannou A, et al. CMAJ 2010;182:

37
 Lifestyle")

38 Treatment Guidelines: The Challenge of the Moderate Risk Patient Low risk (<10%) Lifestyle Modification High risk (>20%) Treat Moderate risk Lifestyle?Treat Papaioannou A, et al. CMAJ. 2010;182:
39 Top 5 Reasons to Consider Treatment in the Moderate Risk Patient: ❶ ❷ Fracture: vertebral (on lateral spine X-ray) or wrist fracture (in patient >65 or BMD -2.5) Lumbar spine T-score << femoral neck T-score ❸ ❹ ❺ Concurrent high risk disorder or medications, including: Hypogonadism or premature menopause (age <45 yr) Primary hyperparathyroidism Hyperthyroidism Rheumatoid arthritis Glucocorticoids (long-term or repeated use) Aromatase inhibitor therapy Falls ( 2 in the past year) Patient preference to be treated Steering Group Communications. Feb 9 th, Based on Osteoporosis Canada Guidelines: Papaioannou A, et al. CMAJ. 2010;182:
40 Medications known to cause/accelerate bone loss Proton Pump Inhibitors (PPI) Selective serotonin reuptake inhibitors (SSRIs) Aromatase inhibitors Hormonal/endocrine therapies - (GnRH agonists, LHRH analogs) Medications that increase fall risk and potential to fracture Benzodiazepines Neuroleptics Anticholinergics Anticonvulsants Antidepressants Antihypertensives Beta-blockers, nitrates, vasodilators * Note: not an exhaustive list
41 What biochemical tests should be ordered in the assessment of osteoporosis?

42 Secondary Causes of Osteoporosis
43 Assessment for Osteoporosis: Recommended Biochemical Tests Calcium, corrected for albumin CBC Creatinine Alkaline phosphatase Thyroid-stimulating hormone Serum protein electrophoresis (for patients with vertebral fractures) 25(OH)D* In clinical practice, these tests help rule out secondary causes of osteoporosis. *Should be measured after 3-4 months of adequate supplementation and should not be repeated if an optimal level (at least 75 nmol/l) is achieved. CBC = complete blood count; 25(OH)D = 25-hydroxyvitamin D Papaioannou A et al. CMAJ 2010; 182:
44 Osteoporosis treatment options NON-PHARMACOLOGIC PHARMACOLOGIC Non-Pharmacological Pharmacological Aerobic/walking-type exercise 3x/week Calcium: 1200 mg from diet and supplement Vitamin D: 800 IU/day or more Restrict alcohol consumption Avoid excess caffeine (> 4 cups of coffee/day) Bisphosphonates Hormone therapy (HRT) Estrogen agonist/antagonists (EAA/SERMs) Parathyroid hormone derivatives RANK Ligand Inhibitor Fall prevention 1. Brown JP et al. JOGC 2006;172:S95-S Brown JP et al. CMAJ 2002;167(10 suppl):s1-s34.
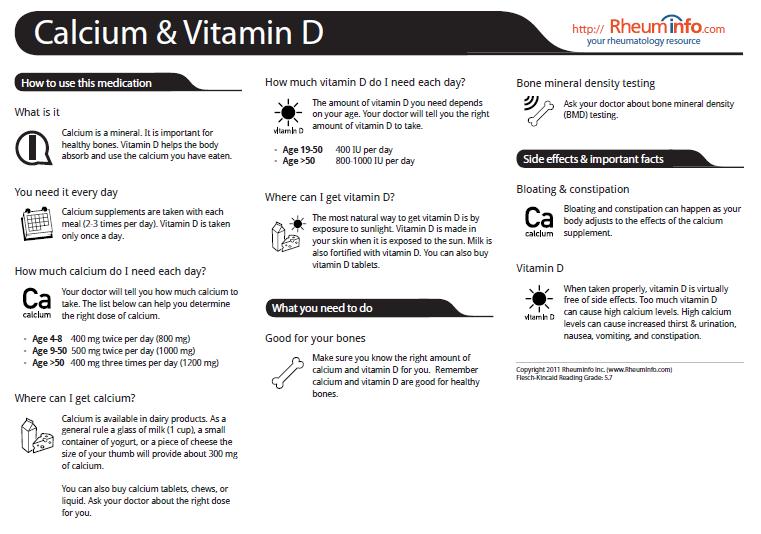
45 Osteoporosis Case 2 64 year old woman with femoral neck T score < -2.5 and prior wrist fracture She is on bisphosphonate therapy She asks what the optimal intake of calcium and vitamin D would be to maintain bone health and ensure efficacy of the bisphosphonate
46 OP: Controversies about Calcium BMJ 2010;341:c3691 and BMJ 2011;342:d2040
47 Proportion with verified MI (%) Vascular Events in Healthy Older Women Receiving Calcium Supplementation: Randomized Controlled Trial Participants received either 1 g of elemental calcium daily (as the citrate) or identical placebo 2 tablets (each with 200 mg elemental calcium) before breakfast and 3 tablets in the evening 6 5 women) Osteoporosis Canada recommendation: Placebo group (739 women) Calcium group ( mg calcium per day from all sources Time to first MI (months) MI = myocardial infarction Bollan MJ et al. BMJ 2008; 336:262-6.
48 IOF Calcium Calculator January 2015 IOF website App for Android and Apple mobile devices
49 Vitamin D Deficiency: 25(OH)D Continuum Deficiency Severe Moderate Mild Sufficiency* Serum 25(OH)D, ng/ml Serum 25(OH)D, nmol/l Severe vitamin D deficiency <12.5 nmol/ml; moderate vitamin D deficiency < nmol/ml; mild vitamin D deficiency nmol/l *Optimal serum 25-OHD level is unknown though threshold values of nmol/l have been proposed Adapted from Working Group of the Australian and New Zealand Bone and Mineral Society, Endocrine Society of Australia and Osteoporosis Australia Med J Aust 2005; 182:281-5.
:S433.")
50 Consequences of Vitamin D Insufficiency parathyroid hormone (PTH) calcium release (i.e. bone resorption) bone mineral density (BMD) Vitamin D insufficiency: 25(OH)D <75 nmol/l fractures muscle strength balance falls Dhesi JK et al. Age Aging 2002; 31:267-71; Simonelli C et al. j Bone Miner Res 2004; 19(Suppl 1):S433.

51 Proportion with 25-OH D levels above 75 nmol/l? 33-37%



52 What is the source of Vitamin D for supplements? Lanolin from sheep wool containing 7- dehydrocholesterol + UV light = Vitamin D3
53 Annualized adjusted* change in BMD, % Optimal Vitamin D Repletion Helped Maximize Response to Antiresorptive Therapy 2.5 ** Spine 1.70 Total hip 1.5 Neck IU daily for adults 0.22 < 50 yrs IU daily for adults > 50 yrs Postmenopausal Women with Osteoporosis or with a Prior Hip or Vertebral Fracture Treated for Months with Alendronate, Risedronate or Raloxifene Canadian Vitamin D Guidelines recommend: Vitamin D replete (n=1001) Vitamin D deficient (n=514) Note: replete is defined as 25(OH)D 20 ng/ml and deficient is defined as 25(OH)D <20 ng/ml *Adjusted for factors unrelated to vitamin D status (age, type of treatment, calcium intake and baseline BMD); **p=0.002 vs. vitamin D deficient; p<0.05 vs. vitamin D deficient Adami S et al. Osteoporos Int 2009; 20:

54 Criteria for ordering 25-OH Vitamin D test
55 Impact of Criteria on Vitamin D Tests Ordered: Alberta











56 Mechanism of Action of Available Osteoporosis Therapies Osteoclast Precursors Estrogen therapy Selective estrogen receptor modulators Hormones Multinucleated Osteoclast RANKL RANK Bisphosphonates Bind to bone; inhibit osteoclasts Teriparatide PTH analog Denosumab RANK Ligand inhibitor Osteoblast Osteoclast Adapted from: Boyle WJ et al. Nature 2003; 423:
57 Percentage of Patients With Fractures (%) Alendronate reduces Vertebral, Non-vertebral, and Hip Fractures Cochrane meta-analysis: Patient incidence of fracture and weighted relative risk for fractures after treatment with 10 mg alendronate RRR 45% n = 7156 RR 0.55 (95% CI, ) p<0.001 RRR 16% n = 9481 RR 0.84 (95% CI, ) p=0.003 RRR 39% n = 9807 Vertebral Fracture Non-vertebral Fracture Hip Fracture RR 0.61 (95% CI, ) p=0.02 Wells GA, et al. Cochrane Database Syst Rev. 2008, Issue 1, CD001155
58 Percentage of Patients With Fractures (%) Risedronate Reduces Vertebral, Non-vertebral, and Hip Fractures Cochrane meta-analysis: Patients incidence of fracture and weighted relative risk for fractures after treatment with 5 mg risedronate n = 3066 RRR 37% n = n = Vertebral Fracture Non-vertebral Fracture Hip Fracture RR 0.63 (95% CI, ) p< RRR 20% RR 0.80 (95% CI, ) p= RRR 26% RR 0.74 (95% CI, ) p=0.01 Wells GA, et al. Cochrane Database Syst Rev Jan 23;(1):CD004523
59 Cumulative Incidence (%) of New Clinical Fractures Over 3 Years Zoledronic Acid Reduces Vertebral, Non-vertebral, and Hip Fractures RCT: HORIZON 3 year Pivotal Fracture Trial in PMO RRR 70% RRR 25% 10.9% 10.7% n = (310/2853) n = (388/3875) Placebo 8.0% n = (292/3861) Zoledronic Acid 5 mg 5 3.3% n = (92/2822) RRR 41% 2.5% n = (88/3875) 1.4% n = (52/3861) 0 Vertebral Fracture* Non-vertebral Fracture** Hip Fracture** RR 0.30 (95% CI, ) p<0.001 RR 0.75 (95% CI, ) p<0.001 RR 0.59 (95% CI, ) p=0.002 Black DM, et al. N Engl J Med. 2007;356:1809 * Incidence rate ** 3-year cumulative event rates based on Kaplan-Meier estimates.
60 % of Patient with Fracture Hormone Therapy Reduces Vertebral, Non-vertebral, and Hip Fractures in Postmenopausal Women RCT: WHI study with postmenopausal women treated with hormone therapy for 5.2 years 10% 9% 8% 7% 6% 5% 4% 3% 2% 1% 0% Placebo HT RRR 35% 0.74% 0.48% n = (60/8102) n = (41/8506) Clinical Vertebral Fracture RRR 21% 8.70% n = (701/8102) 6.80% n = (579/8506) Non-vertebral Fracture 0.77% n = (62/8102) RRR 32% 0.52% n = (44/8506) Hip Fracture HR 0.66 (95% CI, ) HR 0.77 (95% CI, ) HR 0.66 (95% CI, ) CI = confidence interval, HR = hazard ratio, RRR = relative risk reduction HT = daily combined estrogen and progestin Rossouw JE, et al. JAMA. 2002;288:321
61 Percentage of Patients With Incident Vertebral Fracture (%) 1. Ettinger B, et al. JAMA. 1999;282: Seeman E, et al. Osteoporos Int. 2006;17:313 Raloxifene Reduces Vertebral Fractures RCT: MORE Study in postmenopausal women for 3 years Placebo Raloxifene 60 mg/day 21.2% n = (163/770) RRR 30% 14.7% n = (113/769) % n = (68/1522) RRR 50% 2.3% n = (35/1490) 0 No Pre-existing Vertebral Fractures Low-risk Population (95% CI, ) Pre-existing Vertebral Fractures High-risk Population (95% CI, ) Relative risk of non-vertebral, including hip, fractures was not significant (RR 0.9, 95% CI, ) 1 Meta-analysis of 7 Raloxifene clinical trials reported fracture reductions results consistent with results from the MORE study; overall odds ratio of
62 Percentage of Patients With 1 Fracture in 2 Years (%) Teriparatide Reduces Risk of Vertebral and Non-vertebral Fractures in Women With PMO RCT: Effect of daily PTH for 18 months on vertebral and non-vertebral fractures Placebo PTH 20 mcg 16% 14% 12% 14% n = (64/448) RRR 65% 10% 8% 6% 4% 5% n = (22/444) 5.5% n = (30/544) RRR 53% 2.6% n = (14/541) 2% 0% *Includes hip fracture Vertebral Fracture RR 0.35 (95% CI, ) p<0.001 vs placebo Non-vertebral Fracture* RR 0.47 (95% CI, ) p=0.02 vs placebo Neer RM, et al. N Engl J Med. 2001;344:1434
 RRR 68% 8.0% n = (84/3875) 6.5% n = (19/3861) RRR 40% 5% 2.3% n = (82/3702) 1.2% n = (388/3875) 0.7% n = (292/3861) 0% Vertebral Fracture* Non-vertebral Fracture Hip Fracture RR 0.")
63 Fracture Incidence at Month 36 (%) Denosumab Reduces Vertebral, Non-vertebral, and Hip Fractures in Women With PMO 15% Placebo RCT: FREEDOM 3 year Pivotal Fracture Trial in PMO Denosumab RRR 20% 10% 7.2% n = (264/3691) RRR 68% 8.0% n = (84/3875) 6.5% n = (19/3861) RRR 40% 5% 2.3% n = (82/3702) 1.2% n = (388/3875) 0.7% n = (292/3861) 0% Vertebral Fracture* Non-vertebral Fracture Hip Fracture RR 0.32 (95% CI, ) p<0.001 vs placebo *Crude incidence Kaplan-Meier estimate of incidence RR 0.80 (95% CI, ) p=0.01 vs placebo RR 0.60 (95% CI, ) p=0.04 vs placebo Cummings SR, et al. N Eng J Med. 2009;361:756
64
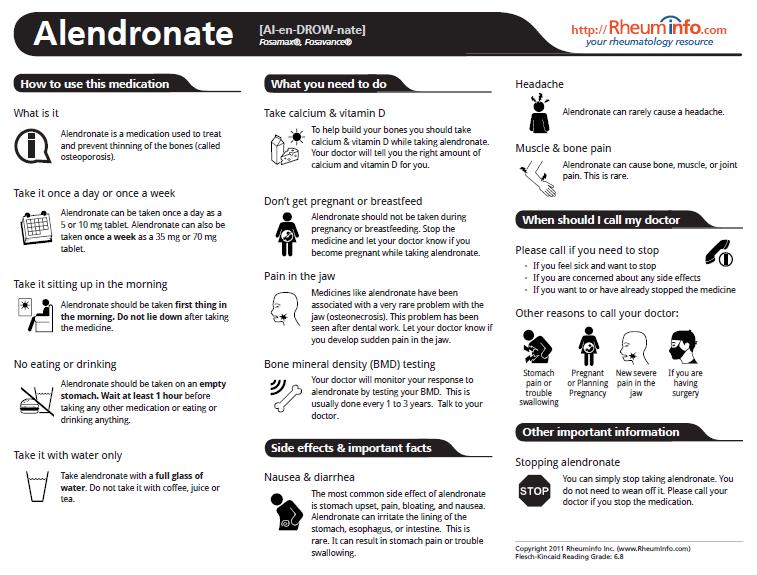
65 Osteoporosis Case 3 62 year old woman No history of fracture Lowest current BMD -3.1 Recommended to start bisphosphonate therapy She is worried about side effects from bisphosphonates
66 Trends in Bisphosphonate Google Searches
67 Trends in Bisphosphonate Use: USA


68 Drug Therapy and the Media: A Crisis in the Treatment of Osteoporosis An article appeared in the New York Times entitled Fearing Rare Side Effects, Millions Take Their Chances with Osteoporosis Sundeep Khosla, M.D and Elizabeth Shane MD. A Crisis in the Treatment of Osteoporosis Date Submitted June 15, 2016; Date Revision Submitted June 16, 2016; Date Final Disposition Set June 17, 2016 Journal of Bone and Mineral Research This article is protected by copyright. All rights reserved. DOI /jbmr.2888

69 Osteonecrosis of the Jaw (ONJ) ONJ is an oral cavity lesion characterized by 1 or more spots of bare alveolar or hard palate bone, in the absence of local malignancy or radiation therapy to the head or neck


70 Risk 1: 100,000 patients Risk 1:100,000 patients over 3 years
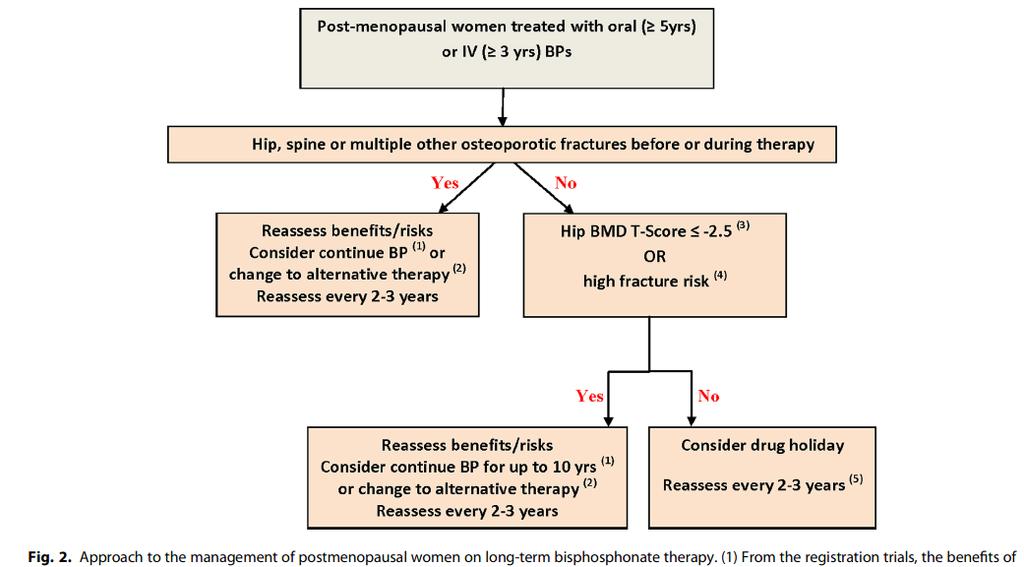
71 70 year old woman Osteoporosis Case 4 No history of fracture Taking weekly bisphosphonate for 5 years Lowest current BMD -2.4 She wants to discuss a drug holiday
; incomplete fractures involve only the lateral cortex *All Major features required to define atypical")
72 Atypical (Subtrochanteric) Femur Fractures ASBMR Task Force Definition 1 : Major Features* Anywhere along the femur No trauma or minimal trauma Transverse or short oblique configuration Non-comminuted Complete fractures through both cortices (may be associated with a medial spike); incomplete fractures involve only the lateral cortex *All Major features required to define atypical femoral fracture. Image from: Lenart BA, et al. N Engl J Med. 2008;358: Shane E, Burr D, et al. Atypical Subtrochanteric and Diaphyseal Femoral Fractures: Report of a Task Force of the American Society for Bone and Mineral Research. JBMR, 2010; On line Sept 7, DOI /jbmr Lenart BA, et al. N Engl J Med. 2008;358:1304

73 Bisphosphonate Risk Benefit Ratio
74
75 Osteoporosis: Future Therapies Sclerostin inhibitors Romosozumab (concern re CV side effects raised in one RCT) Cathepsin K inhibitors Odanacatib (development halted late 2016) PTH analogues Abaloparatide (marketed 2017 in USA as TYMLOS)
76 ROMO: Phase 3 Fracture Trial (FRAME) Cosman et al NEJM 2016
77 Abaloparatide Daily SC Injection
78 Resources
79
80
81
82
83

84 OP Treatment Decision Tools

85 Additional resources for osteoporosis in LTC» Educational resources and tool kits on medications, screening, falls prevention and more are available at:
86 PEARLs: Osteoporosis


87 2010 Clinical Practice Guidelines for the Diagnosis and Management of Osteoporosis in Canada Key points: Management of osteoporosis should be guided by an assessment of the patient s absolute risk of osteoporosis-related fractures Fragility fracture increases the risk of further fractures and should be considered in the assessment Lifestyle modifications and pharmacologic therapy should be individualized to enhance adherence to the treatment plan Papaioannou A et al. CMAJ 2010; 182:
88

89 Fewer Fractures!
90 Barriers to Change: Osteoporosis Lack of coordination between fracture care at hospitals and osteoporosis care in the community Overreliance on BMD versus fracture risk assessment Lack of availability of bone turnover markers to follow therapeutic responses Patient fears of rare side effects of bisphosphonate therapy

91 Questions?? Wind up your presentation-he s losing bone mass.
Osteoporosis Management in Older Adults
 Osteoporosis Management in Older Adults Angela M Cheung, MD, PhD, FRCPC, CCD Professor of Medicine, University of Toronto Disclosures Relationship with Commercial Entities: Honoraria from: Amgen, Eli Lilly,
Osteoporosis Management in Older Adults Angela M Cheung, MD, PhD, FRCPC, CCD Professor of Medicine, University of Toronto Disclosures Relationship with Commercial Entities: Honoraria from: Amgen, Eli Lilly,
Module 5 - Speaking of Bones Osteoporosis For Health Professionals: Fracture Risk Assessment. William D. Leslie, MD MSc FRCPC
 Module 5 - Speaking of Bones Osteoporosis For Health Professionals: Fracture Risk Assessment William D. Leslie, MD MSc FRCPC Case #1 Age 53: 3 years post-menopause Has always enjoyed excellent health with
Module 5 - Speaking of Bones Osteoporosis For Health Professionals: Fracture Risk Assessment William D. Leslie, MD MSc FRCPC Case #1 Age 53: 3 years post-menopause Has always enjoyed excellent health with
Treatments for Osteoporosis Expected Benefits, Potential Harms and Drug Holidays. Suzanne Morin MD FRCP FACP McGill University May 2014
 Treatments for Osteoporosis Expected Benefits, Potential Harms and Drug Holidays Suzanne Morin MD FRCP FACP McGill University May 2014 Learning Objectives Overview of osteoporosis management Outline efficacy
Treatments for Osteoporosis Expected Benefits, Potential Harms and Drug Holidays Suzanne Morin MD FRCP FACP McGill University May 2014 Learning Objectives Overview of osteoporosis management Outline efficacy
Fracture=Bone Attack:
 Fracture=Bone Attack: Linking Hip Fractures to Osteoporosis Care Angela M. Cheung, MD, PhD, FRCPC Professor of Medicine, University of Toronto Potential Conflicts of Interests Industry Grants (to UHN)
Fracture=Bone Attack: Linking Hip Fractures to Osteoporosis Care Angela M. Cheung, MD, PhD, FRCPC Professor of Medicine, University of Toronto Potential Conflicts of Interests Industry Grants (to UHN)
Current and Emerging Strategies for Osteoporosis
 Current and Emerging Strategies for Osteoporosis I have nothing to disclose. Anne Schafer, MD Assistant Professor of Medicine Division of Endocrinology & Metabolism December 12, 2014 Outline Osteoporosis
Current and Emerging Strategies for Osteoporosis I have nothing to disclose. Anne Schafer, MD Assistant Professor of Medicine Division of Endocrinology & Metabolism December 12, 2014 Outline Osteoporosis
Updates in Osteoporosis. I have no conflicts of interest. What Would You Do? Mrs. C. What s New in Osteoporosis. Page 1
 Updates in Osteoporosis Jeffrey A. Tice, MD Associate Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in
Updates in Osteoporosis Jeffrey A. Tice, MD Associate Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in
What is Osteoporosis?
 What is Osteoporosis? 2000 NIH Definition A skeletal disorder characterized by compromised bone strength predisposing a person to an increased risk of fracture. Bone strength reflects the integration of
What is Osteoporosis? 2000 NIH Definition A skeletal disorder characterized by compromised bone strength predisposing a person to an increased risk of fracture. Bone strength reflects the integration of
CASE 1 WHY IS IT IMPORTANT TO TREAT? FACTS CONCERNS
 4:30-5:15pm Ask the Expert: Osteoporosis SPEAKERS Silvina Levis, MD OSTEOPOROSIS - FACTS 1:3 older women and 1:5 older men will have a fragility fracture after age 50 After 3 years of treatment, depending
4:30-5:15pm Ask the Expert: Osteoporosis SPEAKERS Silvina Levis, MD OSTEOPOROSIS - FACTS 1:3 older women and 1:5 older men will have a fragility fracture after age 50 After 3 years of treatment, depending
Download slides:
 Download slides: https://www.tinyurl.com/m67zcnn https://tinyurl.com/kazchbn OSTEOPOROSIS REVIEW AND UPDATE Boca Raton Regional Hospital Internal Medicine Conference 2017 Benjamin Wang, M.D., FRCPC Division
Download slides: https://www.tinyurl.com/m67zcnn https://tinyurl.com/kazchbn OSTEOPOROSIS REVIEW AND UPDATE Boca Raton Regional Hospital Internal Medicine Conference 2017 Benjamin Wang, M.D., FRCPC Division
Osteoporosis: An Overview. Carolyn J. Crandall, MD, MS
 Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Professor of Medicine David Geffen School of Medicine at UCLA Objectives Review osteoporosis
Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Professor of Medicine David Geffen School of Medicine at UCLA Objectives Review osteoporosis
Monitoring Osteoporosis Therapy
 Monitoring Osteoporosis Therapy SUZANNE MORIN DEPT OF MEDICINE, DIVISION OF GENERAL INTERNAL MEDICINE, MUHC CENTRE FOR OUTCOMES RESEARCH AND EVALUATION, RI MUHC November 2017 Conflict of Interest Disclosures
Monitoring Osteoporosis Therapy SUZANNE MORIN DEPT OF MEDICINE, DIVISION OF GENERAL INTERNAL MEDICINE, MUHC CENTRE FOR OUTCOMES RESEARCH AND EVALUATION, RI MUHC November 2017 Conflict of Interest Disclosures
Advanced medicine conference. Monday 20 Tuesday 21 June 2016
 Advanced medicine conference Monday 20 Tuesday 21 June 2016 Osteoporosis: recent advances in risk assessment and management Juliet Compston Emeritus Professor of Bone Medicine Cambridge Biomedical Campus
Advanced medicine conference Monday 20 Tuesday 21 June 2016 Osteoporosis: recent advances in risk assessment and management Juliet Compston Emeritus Professor of Bone Medicine Cambridge Biomedical Campus
A Review of Bone Health Issues in Oncology
 A Review of Bone Health Issues in Oncology David L. Kendler MD FRCPC CCD Professor of Medicine (Endocrinology) University of British Columbia Vancouver Canada Disclosures David Kendler has received research
A Review of Bone Health Issues in Oncology David L. Kendler MD FRCPC CCD Professor of Medicine (Endocrinology) University of British Columbia Vancouver Canada Disclosures David Kendler has received research
Learning Objectives. Controversies in Osteoporosis Prevention and Management. Etiology. Presenter Disclosure Information. Epidemiology.
 12:45 1:30pm Controversies in Osteoporosis Prevention and Management SPEAKER Carolyn Crandall, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Carolyn
12:45 1:30pm Controversies in Osteoporosis Prevention and Management SPEAKER Carolyn Crandall, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Carolyn
Osteoporosis/Fracture Prevention
 Osteoporosis/Fracture Prevention NATIONAL GUIDELINE SUMMARY This guideline was developed using an evidence-based methodology by the KP National Osteoporosis/Fracture Prevention Guideline Development Team
Osteoporosis/Fracture Prevention NATIONAL GUIDELINE SUMMARY This guideline was developed using an evidence-based methodology by the KP National Osteoporosis/Fracture Prevention Guideline Development Team
1
 www.osteoporosis.ca 1 2 Overview of the Presentation Osteoporosis: An Overview Bone Basics Diagnosis of Osteoporosis Drug Therapies Risk Reduction Living with Osteoporosis 3 What is Osteoporosis? Osteoporosis:
www.osteoporosis.ca 1 2 Overview of the Presentation Osteoporosis: An Overview Bone Basics Diagnosis of Osteoporosis Drug Therapies Risk Reduction Living with Osteoporosis 3 What is Osteoporosis? Osteoporosis:
Disclosures. Diagnostic Challenges in Osteoporosis: Whom To Treat 9/25/2014
 Disclosures Diagnostic Challenges in Osteoporosis: Whom To Treat Ethel S. Siris, MD Columbia University Medical Center New York, NY Consultant on scientific issues for: AgNovos Amgen Eli Lilly Merck Novartis
Disclosures Diagnostic Challenges in Osteoporosis: Whom To Treat Ethel S. Siris, MD Columbia University Medical Center New York, NY Consultant on scientific issues for: AgNovos Amgen Eli Lilly Merck Novartis
An Update on Osteoporosis Treatments
 An Update on Osteoporosis Treatments Dr Mike Stone University Hospital Llandough Treatments for osteoporosis Calcium and vitamin D HRT Raloxifene Etidronate Alendronate Risedronate Ibandronate (oral and
An Update on Osteoporosis Treatments Dr Mike Stone University Hospital Llandough Treatments for osteoporosis Calcium and vitamin D HRT Raloxifene Etidronate Alendronate Risedronate Ibandronate (oral and
Assessment and Treatment of Osteoporosis Professor T.Masud
 Assessment and Treatment of Osteoporosis Professor T.Masud Nottingham University Hospitals NHS Trust University of Nottingham University of Derby University of Southern Denmark What is Osteoporosis? Osteoporosis
Assessment and Treatment of Osteoporosis Professor T.Masud Nottingham University Hospitals NHS Trust University of Nottingham University of Derby University of Southern Denmark What is Osteoporosis? Osteoporosis
Osteoporosis: current treatment and future prospects. Juliet Compston Professor Emeritus of Bone Medicine Cambridge Biomedical Campus
 Osteoporosis: current treatment and future prospects Juliet Compston Professor Emeritus of Bone Medicine Cambridge Biomedical Campus Disclosures Consultancy and speaking fees for Gilead, related to development
Osteoporosis: current treatment and future prospects Juliet Compston Professor Emeritus of Bone Medicine Cambridge Biomedical Campus Disclosures Consultancy and speaking fees for Gilead, related to development
Osteoporosis. A Silent Killer. David A. Chappell, MD Endocrinology Private Practice Petaluma, California
 Osteoporosis A Silent Killer David A. Chappell, MD Endocrinology Private Practice Petaluma, California Relevant Disclosures Speakers Bureau Astra Zeneca Boehringer Ingelheim AACE/ACE Guidelines American
Osteoporosis A Silent Killer David A. Chappell, MD Endocrinology Private Practice Petaluma, California Relevant Disclosures Speakers Bureau Astra Zeneca Boehringer Ingelheim AACE/ACE Guidelines American
Page 1. Updates in Osteoporosis. I have no conflicts of interest. What is osteoporosis? What s New in Osteoporosis
 Updates in Osteoporosis Jeffrey A. Tice, MD Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in Osteoporosis
Updates in Osteoporosis Jeffrey A. Tice, MD Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in Osteoporosis
Skeletal Manifestations
 Skeletal Manifestations of Metabolic Bone Disease Mishaela R. Rubin, MD February 21, 2008 The Three Ages of Women Gustav Klimt 1905 1 Lecture Outline Osteoporosis epidemiology diagnosis secondary causes
Skeletal Manifestations of Metabolic Bone Disease Mishaela R. Rubin, MD February 21, 2008 The Three Ages of Women Gustav Klimt 1905 1 Lecture Outline Osteoporosis epidemiology diagnosis secondary causes
Page 1. Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018? What s New in Osteoporosis
 Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018? Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco What s
Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018? Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco What s
Page 1. New Developments in Osteoporosis. What s New in Osteoporosis
 New Developments in Osteoporosis Eliseo J. Pérez-Stable MD Professor of Medicine Division of General Internal Medicine Department of Medicine July 4, 2013 Declaration of full disclosure: No conflict of
New Developments in Osteoporosis Eliseo J. Pérez-Stable MD Professor of Medicine Division of General Internal Medicine Department of Medicine July 4, 2013 Declaration of full disclosure: No conflict of
Osteoporosis Update. Greg Summers Consultant Rheumatologist
 Osteoporosis Update Greg Summers Consultant Rheumatologist DEFINITION OSTEOPOROSIS is LOW BONE MASS (& micro-architectural deterioration) causing AN INCREASED RISK OF FRACTURE 23 years 82 years 23 y/o
Osteoporosis Update Greg Summers Consultant Rheumatologist DEFINITION OSTEOPOROSIS is LOW BONE MASS (& micro-architectural deterioration) causing AN INCREASED RISK OF FRACTURE 23 years 82 years 23 y/o
Osteoporosis. Overview
 v2 Osteoporosis Overview Osteoporosis is defined as compromised bone strength that increases risk of fracture (NIH Consensus Conference, 2000). Bone strength is characterized by bone mineral density (BMD)
v2 Osteoporosis Overview Osteoporosis is defined as compromised bone strength that increases risk of fracture (NIH Consensus Conference, 2000). Bone strength is characterized by bone mineral density (BMD)
Osteoporosis. Treatment of a Silently Developing Disease
 Osteoporosis Treatment of a Silently Developing Disease Marc K. Drezner, MD Senior Associate Dean Emeritus Professor of Medicine Emeritus University of Wisconsin-Madison Auditorium The Forest at Duke October
Osteoporosis Treatment of a Silently Developing Disease Marc K. Drezner, MD Senior Associate Dean Emeritus Professor of Medicine Emeritus University of Wisconsin-Madison Auditorium The Forest at Duke October
Osteoporosis in Men. CME Away India & Sri Lanka March 23 - April 7, 2018
 Osteoporosis in Men CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright 2017
Osteoporosis in Men CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright 2017
Chau Nguyen, D.O. Rheumatologist Clinical Assistant Professor of Internal Medicine at Western University of Health Sciences
 Chau Nguyen, D.O Rheumatologist Clinical Assistant Professor of Internal Medicine at Western University of Health Sciences I do not have any relationship with the manufacturer of any commercial products
Chau Nguyen, D.O Rheumatologist Clinical Assistant Professor of Internal Medicine at Western University of Health Sciences I do not have any relationship with the manufacturer of any commercial products
Updates in Osteoporosis
 Updates in Osteoporosis Jeffrey A. Tice, MD Associate Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in
Updates in Osteoporosis Jeffrey A. Tice, MD Associate Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in
Diagnosis and Treatment of Osteoporosis: What s New and Controversial in ? What s New in Osteoporosis
 Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018-19? What s New in Osteoporosis The crisis in treatment and compliance Douglas C. Bauer, MD Professor of Medicine and Epidemiology
Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018-19? What s New in Osteoporosis The crisis in treatment and compliance Douglas C. Bauer, MD Professor of Medicine and Epidemiology
Osteoporosis Update: Treatments and Controversies
 Osteoporosis Update: Treatments and Controversies Sabrina Gill MD MPH FRCPC Clinical Professor, UBC St. Paul s Hospital Images provided by D. Dempster, PhD, Helen Hayes Hospital, NY Honoraium for CME and
Osteoporosis Update: Treatments and Controversies Sabrina Gill MD MPH FRCPC Clinical Professor, UBC St. Paul s Hospital Images provided by D. Dempster, PhD, Helen Hayes Hospital, NY Honoraium for CME and
Fragile Bones and how to recognise them. Rod Hughes Consultant physician and rheumatologist St Peter s hospital Chertsey
 Fragile Bones and how to recognise them Rod Hughes Consultant physician and rheumatologist St Peter s hospital Chertsey Osteoporosis Osteoporosis is a skeletal disorder characterised by compromised bone
Fragile Bones and how to recognise them Rod Hughes Consultant physician and rheumatologist St Peter s hospital Chertsey Osteoporosis Osteoporosis is a skeletal disorder characterised by compromised bone
Hot Topics in Osteoporosis and Fracture Prevention
 Hot Topics in Osteoporosis and Fracture Prevention Sid Feldman, MD CCFP (COE) FCFP Sandra Kim, MD, FRCPC November 15, 2018 Family Medicine Forum, Toronto Faculty/Presenter Disclosure Faculty: Sid Feldman
Hot Topics in Osteoporosis and Fracture Prevention Sid Feldman, MD CCFP (COE) FCFP Sandra Kim, MD, FRCPC November 15, 2018 Family Medicine Forum, Toronto Faculty/Presenter Disclosure Faculty: Sid Feldman
Management of postmenopausal osteoporosis
 Management of postmenopausal osteoporosis Yeap SS, Hew FL, Chan SP, on behalf of the Malaysian Osteoporosis Society Committee Working Group for the Clinical Guidance on the Management of Osteoporosis,
Management of postmenopausal osteoporosis Yeap SS, Hew FL, Chan SP, on behalf of the Malaysian Osteoporosis Society Committee Working Group for the Clinical Guidance on the Management of Osteoporosis,
New Developments in Osteoporosis: Screening, Prevention and Treatment
 Osteoporosis: Overview New Developments in Osteoporosis: Screening, Prevention and Treatment Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Risk factors
Osteoporosis: Overview New Developments in Osteoporosis: Screening, Prevention and Treatment Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Risk factors
Osteoporosis. The Silent Killer. Joseph B. Hawkins, Jr., MD, FACE Sierra Endocrine Associates Fresno, California
 Osteoporosis The Silent Killer Joseph B. Hawkins, Jr., MD, FACE Sierra Endocrine Associates Fresno, California Disclosures Speakers Bureau Amgen AACE/ACE Guidilines American Association of Clinical Endocrinologist
Osteoporosis The Silent Killer Joseph B. Hawkins, Jr., MD, FACE Sierra Endocrine Associates Fresno, California Disclosures Speakers Bureau Amgen AACE/ACE Guidilines American Association of Clinical Endocrinologist
8/6/2018. Glucocorticoid induced osteoporosis: overlooked and undertreated? Disclosure. Objectives. Overview
 Disclosure Glucocorticoid induced osteoporosis: overlooked and undertreated? I have no financial disclosure relevant to this presentation Tasma Harindhanavudhi, MD Division of Diabetes and Endocrinology
Disclosure Glucocorticoid induced osteoporosis: overlooked and undertreated? I have no financial disclosure relevant to this presentation Tasma Harindhanavudhi, MD Division of Diabetes and Endocrinology
Page 1. Current and Emerging Strategies What s New in Osteoporosis. Osteoporosis. What is Osteoporosis? Traditional Risk Factors for Fracture
 Current and Emerging Strategies for Osteoporosis What s New in Osteoporosis Risk stratification Douglas C. Bauer, MD University of California, San Francisco Under recognition and poor compliance New potential
Current and Emerging Strategies for Osteoporosis What s New in Osteoporosis Risk stratification Douglas C. Bauer, MD University of California, San Francisco Under recognition and poor compliance New potential
Osteoporosis challenges
 Osteoporosis challenges Osteoporosis challenges Who should have a fracture risk assessment? Who to treat? Drugs, holidays and unusual adverse effects Fracture liaison service? The size of the problem 1
Osteoporosis challenges Osteoporosis challenges Who should have a fracture risk assessment? Who to treat? Drugs, holidays and unusual adverse effects Fracture liaison service? The size of the problem 1
Learning Objectives. Controversies in Osteoporosis Prevention and Management. Definition. Presenter Disclosure Information.
 4 4:45 pm Controversies in Osteoporosis Prevention and Management SPEAKER Carolyn Crandall, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Carolyn
4 4:45 pm Controversies in Osteoporosis Prevention and Management SPEAKER Carolyn Crandall, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Carolyn
BAD TO THE BONE. Peter Jones, Rheumatologist QE Health, Rotorua. GP CME Conference Rotorua, June 2008
 BAD TO THE BONE Peter Jones, Rheumatologist QE Health, Rotorua GP CME Conference Rotorua, June 2008 Agenda Osteoporosis in Men Vitamin D and Calcium Long-term treatment with Bisphosphonates Pathophysiology
BAD TO THE BONE Peter Jones, Rheumatologist QE Health, Rotorua GP CME Conference Rotorua, June 2008 Agenda Osteoporosis in Men Vitamin D and Calcium Long-term treatment with Bisphosphonates Pathophysiology
Drug Intervals (Holidays) with Oral Bisphosphonates
 with Oral Bisphosphonates") Drug Intervals (Holidays) with Oral Bisphosphonates Rizwan Rajak Consultant Rheumatologist & Lead for Osteoporosis GP Postgraduate Meeting April 2018 Contents Case presentation Pathway for Bisphosphonate
Drug Intervals (Holidays) with Oral Bisphosphonates Rizwan Rajak Consultant Rheumatologist & Lead for Osteoporosis GP Postgraduate Meeting April 2018 Contents Case presentation Pathway for Bisphosphonate
SpongeBone Menopants*
 SpongeBone Menopants* Adam Fershko, MD, FACP Kettering Health Network *Postmenopausal Osteoporosis Objectives O Epidemiology O Clinical significance O Pathophysiology O Screening and Diagnosis O Treatment
SpongeBone Menopants* Adam Fershko, MD, FACP Kettering Health Network *Postmenopausal Osteoporosis Objectives O Epidemiology O Clinical significance O Pathophysiology O Screening and Diagnosis O Treatment
Men and Osteoporosis So you think that it can t happen to you
 Men and Osteoporosis So you think that it can t happen to you Jonathan D. Adachi MD, FRCPC Alliance for Better Bone Health Chair in Rheumatology Professor, Department of Medicine Michael G. DeGroote School
Men and Osteoporosis So you think that it can t happen to you Jonathan D. Adachi MD, FRCPC Alliance for Better Bone Health Chair in Rheumatology Professor, Department of Medicine Michael G. DeGroote School
Who cares about fractures! is more important. October 3, 2014 CSIM Workshop Brian Wirzba, MD, FRCPC, FACP Clinical Professor Grey Nuns Hospital
 Isn t Osteoporosis just a T Score less than 2.5?? Who cares about fractures! is more important. Why do I need to know this? October 3, 2014 CSIM Workshop Brian Wirzba, MD, FRCPC, FACP Clinical Professor
Isn t Osteoporosis just a T Score less than 2.5?? Who cares about fractures! is more important. Why do I need to know this? October 3, 2014 CSIM Workshop Brian Wirzba, MD, FRCPC, FACP Clinical Professor
Osteoporosis - New Guidelines. Michelle Glass B.Sc. (Pharm) June 15, 2011
 June 15, 2011") Osteoporosis - New Guidelines Michelle Glass B.Sc. (Pharm) June 15, 2011 Outline What is Osteoporosis? Who is at risk? What treatments are available? Role of the Pharmacy technician Definition of Osteoporosis
Osteoporosis - New Guidelines Michelle Glass B.Sc. (Pharm) June 15, 2011 Outline What is Osteoporosis? Who is at risk? What treatments are available? Role of the Pharmacy technician Definition of Osteoporosis
Osteoporosis: A Tale of 3 Task Forces!
 Osteoporosis: A Tale of 3 Task Forces! Robert A. Adler, MD McGuire Veterans Affairs Medical Center Virginia Commonwealth University Richmond, Virginia, USA Disclosures The opinions are those of the speaker
Osteoporosis: A Tale of 3 Task Forces! Robert A. Adler, MD McGuire Veterans Affairs Medical Center Virginia Commonwealth University Richmond, Virginia, USA Disclosures The opinions are those of the speaker
Osteoporosis: Are your bones at risk of fracturing? Rachel Wallwork, MD Internal medicine resident Massachusetts General Hospital
 Osteoporosis: Are your bones at risk of fracturing? Rachel Wallwork, MD Internal medicine resident Massachusetts General Hospital What is Osteoporosis? Osteoporosis causes bones to lose density, become
Osteoporosis: Are your bones at risk of fracturing? Rachel Wallwork, MD Internal medicine resident Massachusetts General Hospital What is Osteoporosis? Osteoporosis causes bones to lose density, become
Osteoporosis/Fracture Prevention Clinician Guide SEPTEMBER 2017
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Osteoporosis/Fracture Prevention Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide was developed to assist Primary Care physicians
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Osteoporosis/Fracture Prevention Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide was developed to assist Primary Care physicians
Current Issues in Osteoporosis
 Current Issues in Osteoporosis California AACE 18TH Annual Meeting & Symposium Marina del Rey, CA September 15, 2018 Michael R. McClung, MD, FACP,FACE Director, Oregon Osteoporosis Center Portland, Oregon,
Current Issues in Osteoporosis California AACE 18TH Annual Meeting & Symposium Marina del Rey, CA September 15, 2018 Michael R. McClung, MD, FACP,FACE Director, Oregon Osteoporosis Center Portland, Oregon,
NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT
 NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF OSTEOPOROSIS: OVERVIEW Definitions Risk factors
NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF OSTEOPOROSIS: OVERVIEW Definitions Risk factors
The Bare Bones of Osteoporosis. Wendy Rosenthal, PharmD
 The Bare Bones of Osteoporosis Wendy Rosenthal, PharmD Definition A systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone tissue, with a consequent increase
The Bare Bones of Osteoporosis Wendy Rosenthal, PharmD Definition A systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone tissue, with a consequent increase
Osteoporosis Management
 Osteoporosis Management Lisa Voss PA C, CCD Laura Frontiero NP C, CCD Kaiser Healthy Bones Program San Diego Disclosures: Nothing to disclose www.zazzle.com 1 Overview How to diagnose Osteoporosis FRAX
Osteoporosis Management Lisa Voss PA C, CCD Laura Frontiero NP C, CCD Kaiser Healthy Bones Program San Diego Disclosures: Nothing to disclose www.zazzle.com 1 Overview How to diagnose Osteoporosis FRAX
Osteoporosis Treatment Overview. Colton Larson RFUMS October 26, 2018
 Osteoporosis Treatment Overview Colton Larson RFUMS October 26, 2018 Burden of Disease Most common bone disease 9.9 million Americans + 43.1 million Americans have low bone mineral density (BMD) Stealthy
Osteoporosis Treatment Overview Colton Larson RFUMS October 26, 2018 Burden of Disease Most common bone disease 9.9 million Americans + 43.1 million Americans have low bone mineral density (BMD) Stealthy
AACE/ACE Osteoporosis Treatment Decision Tool
 AACE/ACE Osteoporosis Treatment Decision Tool What is Osteoporosis? OSTEOPOROSIS is defined as reduced bone strength leading to an increased risk of fracture. Osteoporosis, or porous bones, occurs when
AACE/ACE Osteoporosis Treatment Decision Tool What is Osteoporosis? OSTEOPOROSIS is defined as reduced bone strength leading to an increased risk of fracture. Osteoporosis, or porous bones, occurs when
Osteoporosis Case Studies
 2019 Endocrine and Diabetes Symposium for Primary Care Providers Osteoporosis Case Studies Joseph B Hawkins, Jr., MD, FACE Assistant Clinical Professor of Medicine, UCSF Founder, Sierra Endocrine Associates
2019 Endocrine and Diabetes Symposium for Primary Care Providers Osteoporosis Case Studies Joseph B Hawkins, Jr., MD, FACE Assistant Clinical Professor of Medicine, UCSF Founder, Sierra Endocrine Associates
OSTEOPOROSIS: PREVENTION AND MANAGEMENT
 OSTEOPOROSIS: OVERVIEW OSTEOPOROSIS: PREVENTION AND MANAGEMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Key Risk factors Screening and Monitoring
OSTEOPOROSIS: OVERVIEW OSTEOPOROSIS: PREVENTION AND MANAGEMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Key Risk factors Screening and Monitoring
Update on Osteoporosis 2016
 WELCOME! Update on Osteoporosis 2016 Jennifer J. Kelly, D.O., F.A.C.E. Associate Professor of Medicine Division of Endocrinology, Diabetes and Metabolism Upstate Medical University Director of the Clinical
WELCOME! Update on Osteoporosis 2016 Jennifer J. Kelly, D.O., F.A.C.E. Associate Professor of Medicine Division of Endocrinology, Diabetes and Metabolism Upstate Medical University Director of the Clinical
Osteoporosis update. Dr. Claire Vandevelde Consultant Rheumatologist, LTHT
 Osteoporosis update Dr. Claire Vandevelde Consultant Rheumatologist, LTHT Outline Background BMD Tools for assessing fracture risk Case study Denosumab Treatment breaks BMD BMD predicts fracture risk but
Osteoporosis update Dr. Claire Vandevelde Consultant Rheumatologist, LTHT Outline Background BMD Tools for assessing fracture risk Case study Denosumab Treatment breaks BMD BMD predicts fracture risk but
Controversies in Osteoporosis Management
 Controversies in Osteoporosis Management 2018 Northwest Rheumatism Society Meeting Portland, OR April 28, 2018 Michael R. McClung, MD, FACP Director, Oregon Osteoporosis Center Portland, Oregon, USA Institute
Controversies in Osteoporosis Management 2018 Northwest Rheumatism Society Meeting Portland, OR April 28, 2018 Michael R. McClung, MD, FACP Director, Oregon Osteoporosis Center Portland, Oregon, USA Institute
Osteoporosis. Current Trend in Osteoporosis Management for Elderly in HK- Medical Perspective. Old Definition of Osteoporosis
 Current Trend in Osteoporosis Management for Elderly in HK- Medical Perspective Dr Dicky T.K. Choy Physician Jockey Club Centre for Osteoporosis Care and Control, CUHK Osteoporosis Global public health
Current Trend in Osteoporosis Management for Elderly in HK- Medical Perspective Dr Dicky T.K. Choy Physician Jockey Club Centre for Osteoporosis Care and Control, CUHK Osteoporosis Global public health
Pharmacy Management Drug Policy
 SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide), Boniva injection (Ibandronate) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 10/15/2018 If the member s
SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide), Boniva injection (Ibandronate) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 10/15/2018 If the member s
Differentiating Pharmacological Therapies for Osteoporosis
 Differentiating Pharmacological Therapies for Osteoporosis Socrates E Papapoulos Department of Endocrinology & Metabolic Diseases Leiden University Medical Center The Netherlands Competing interests: consulting/speaking
Differentiating Pharmacological Therapies for Osteoporosis Socrates E Papapoulos Department of Endocrinology & Metabolic Diseases Leiden University Medical Center The Netherlands Competing interests: consulting/speaking
Presenter: 翁家嫻 Venue date:
 FOR THE TREATMENT OF OSTEOPOROSIS IN POSTMENOPAUSAL WOMEN AT INCREASED RISK OF FRACTURES 1 Presenter: 翁家嫻 Venue date: 2018.03.13 PMO: postmenopausal osteoporosis. 1. Prolia (denosumab), Summary of Product
FOR THE TREATMENT OF OSTEOPOROSIS IN POSTMENOPAUSAL WOMEN AT INCREASED RISK OF FRACTURES 1 Presenter: 翁家嫻 Venue date: 2018.03.13 PMO: postmenopausal osteoporosis. 1. Prolia (denosumab), Summary of Product
Pharmacy Management Drug Policy
 SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 9/29/2017 If the member s subscriber contract excludes coverage
SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 9/29/2017 If the member s subscriber contract excludes coverage
Parathyroid Hormone Analog for Osteoporosis Prior Authorization with Quantity Limit Criteria Program Summary
 Parathyroid Hormone Analog for Osteoporosis Prior Authorization with Quantity Limit Criteria Program Summary This prior authorization program applies to Commercial, NetResults A series, NetResults F series
Parathyroid Hormone Analog for Osteoporosis Prior Authorization with Quantity Limit Criteria Program Summary This prior authorization program applies to Commercial, NetResults A series, NetResults F series
Screening Guidelines: Women
 The Situation 1 in 2 postmenopausal women and 1 in 5 older men will have an osteoporosis-related fracture in their lifetimes Osteoporosis Definition NIH Consensus Conference A skeletal disorder characterized
The Situation 1 in 2 postmenopausal women and 1 in 5 older men will have an osteoporosis-related fracture in their lifetimes Osteoporosis Definition NIH Consensus Conference A skeletal disorder characterized
Using the FRAX Tool. Osteoporosis Definition
 How long will your bones remain standing? Using the FRAX Tool Gary Salzman M.D. Director Banner Good Samaritan/ Hayden VAMC Internal Medicine Geriatric Fellowship Program Phoenix, Arizona Using the FRAX
How long will your bones remain standing? Using the FRAX Tool Gary Salzman M.D. Director Banner Good Samaritan/ Hayden VAMC Internal Medicine Geriatric Fellowship Program Phoenix, Arizona Using the FRAX
Current and Emerging Approaches for Osteoporosis
 Current and Emerging Approaches for Osteoporosis Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco No Disclosures What s New in Osteoporosis
Current and Emerging Approaches for Osteoporosis Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco No Disclosures What s New in Osteoporosis
Forteo (teriparatide) Prior Authorization Program Summary
 Prior Authorization Program Summary") Forteo (teriparatide) Prior Authorization Program Summary FDA APPROVED INDICATIONS DOSAGE 1 FDA Indication 1 : Forteo (teriparatide) is indicated for: the treatment of postmenopausal women with osteoporosis
Forteo (teriparatide) Prior Authorization Program Summary FDA APPROVED INDICATIONS DOSAGE 1 FDA Indication 1 : Forteo (teriparatide) is indicated for: the treatment of postmenopausal women with osteoporosis
Clinician s Guide to Prevention and Treatment of Osteoporosis
 Clinician s Guide to Prevention and Treatment of Osteoporosis Published: 15 August 2014 committee of the National Osteoporosis Foundation (NOF) Tipawan khiemsontia,md outline Basic pathophysiology screening
Clinician s Guide to Prevention and Treatment of Osteoporosis Published: 15 August 2014 committee of the National Osteoporosis Foundation (NOF) Tipawan khiemsontia,md outline Basic pathophysiology screening
Interpreting DEXA Scan and. the New Fracture Risk. Assessment. Algorithm
 Interpreting DEXA Scan and the New Fracture Risk Assessment Algorithm Prof. Samir Elbadawy *Osteoporosis affect 30%-40% of women in western countries and almost 15% of men after the age of 50 years. Osteoporosis
Interpreting DEXA Scan and the New Fracture Risk Assessment Algorithm Prof. Samir Elbadawy *Osteoporosis affect 30%-40% of women in western countries and almost 15% of men after the age of 50 years. Osteoporosis
Healthy Bones: Osteoporosis Management. Laurel Short, MSN, FNP-C
 Healthy Bones: Osteoporosis Management Laurel Short, MSN, FNP-C Disclosure I have no current affiliation or financial interest with any grantor or commercial interests that may have direct interest in
Healthy Bones: Osteoporosis Management Laurel Short, MSN, FNP-C Disclosure I have no current affiliation or financial interest with any grantor or commercial interests that may have direct interest in
2017 Santa Fe Bone Symposium McClung
 217 Santa Fe Bone Symposium Insights into the Use of Anti-remodeling and Anabolic Agents for Osteoporosis Developing a Long-term Management Plan Michael R., MD, FACP Oregon Osteoporosis Center Portland,
217 Santa Fe Bone Symposium Insights into the Use of Anti-remodeling and Anabolic Agents for Osteoporosis Developing a Long-term Management Plan Michael R., MD, FACP Oregon Osteoporosis Center Portland,
Osteoporosis Agents Drug Class Prior Authorization Protocol
 Osteoporosis Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of
Osteoporosis Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of
11/4/2018. Osteoporosis Update. ACP Oregon Chapter November 9 th, 2018 Sarah Hopkins Providence Medical Group Endocrinology East. No disclosures.
 Osteoporosis Update ACP Oregon Chapter November 9 th, 2018 Sarah Hopkins Providence Medical Group Endocrinology East No disclosures. 1 Goals Review screening recommendations and workup of secondary causes
Osteoporosis Update ACP Oregon Chapter November 9 th, 2018 Sarah Hopkins Providence Medical Group Endocrinology East No disclosures. 1 Goals Review screening recommendations and workup of secondary causes
Overview. Bone Biology Osteoporosis Osteomalacia Paget s Disease Cases. People Centred Positive Compassion Excellence
 Overview Osteoporosis and Metabolic Bone Disease Dr Chandini Rao Consultant Rheumatologist Bone Biology Osteoporosis Osteomalacia Paget s Disease Cases Bone Biology Osteoporosis Increased bone remodelling
Overview Osteoporosis and Metabolic Bone Disease Dr Chandini Rao Consultant Rheumatologist Bone Biology Osteoporosis Osteomalacia Paget s Disease Cases Bone Biology Osteoporosis Increased bone remodelling
OSTEOPOROSIS IN MEN. Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO
 OSTEOPOROSIS IN MEN Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO DISCLOSURES Speakers Bureau: Amgen, Radius Consultant: Abbvie, Amgen, Janssen, Radius, Sanofi Watts NB et
OSTEOPOROSIS IN MEN Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO DISCLOSURES Speakers Bureau: Amgen, Radius Consultant: Abbvie, Amgen, Janssen, Radius, Sanofi Watts NB et
Page 1. Current and Emerging Strategies for Osteoporosis. Osteoporosis Warm-Up: Which of the Following is True?
 Current and Emerging Strategies for Osteoporosis Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco No Disclosures Osteoporosis Warm-Up:
Current and Emerging Strategies for Osteoporosis Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco No Disclosures Osteoporosis Warm-Up:
Disclosures D. Black. Bisphosphonates: Background, Efficacy and Recent Controversies. Page 1. Research Funding: Novartis, Merck
 Bisphosphonates: Background, Efficacy and Recent Controversies Disclosures D. Black Research Funding: Novartis, Merck Dennis M. Black, PhD Consulting: Amgen, Lilly, Zosano, Nycomed Dept. of Epidemiology
Bisphosphonates: Background, Efficacy and Recent Controversies Disclosures D. Black Research Funding: Novartis, Merck Dennis M. Black, PhD Consulting: Amgen, Lilly, Zosano, Nycomed Dept. of Epidemiology
Osteoporosis Clinical Guideline. Rheumatology January 2017
 Osteoporosis Clinical Guideline Rheumatology January 2017 Introduction Osteoporosis is a condition of low bone mass leading to an increased risk of low trauma fractures. The prevalence of osteoporosis
Osteoporosis Clinical Guideline Rheumatology January 2017 Introduction Osteoporosis is a condition of low bone mass leading to an increased risk of low trauma fractures. The prevalence of osteoporosis
Objectives. Discuss bone health and the consequences of osteoporosis on patients medical and disability status.
 Objectives Discuss bone health and the consequences of osteoporosis on patients medical and disability status. Discuss the pathophysiology of osteoporosis and major risk factors. Assess the major diagnostic
Objectives Discuss bone health and the consequences of osteoporosis on patients medical and disability status. Discuss the pathophysiology of osteoporosis and major risk factors. Assess the major diagnostic
HRT and Risedronate Combined Anabolic and Antiresorptive Therapy
 Optimizing Combined and Sequential Osteoanabolic and Antiresorptive Therapy Benjamin Leder, M.D. Endocrine Unit Massachusetts General Hospital Boston, MA Antiresorptive and Osteoanabolic Therapies Increase
Optimizing Combined and Sequential Osteoanabolic and Antiresorptive Therapy Benjamin Leder, M.D. Endocrine Unit Massachusetts General Hospital Boston, MA Antiresorptive and Osteoanabolic Therapies Increase
BREAST CANCER AND BONE HEALTH
 BREAST CANCER AND BONE HEALTH Rowena Ridout, MD, FRCPC Toronto Western Hospital Osteoporosis Program University Health Network / Mount Sinai Hospital rowena.ridout@uhn.ca None to declare Conflicts of Interest
BREAST CANCER AND BONE HEALTH Rowena Ridout, MD, FRCPC Toronto Western Hospital Osteoporosis Program University Health Network / Mount Sinai Hospital rowena.ridout@uhn.ca None to declare Conflicts of Interest
Upcoming Agents for Osteoporosis
 Upcoming Agents for Osteoporosis May 5, 2017 Michael R. McClung, MD, FACP Director, Oregon Osteoporosis Center Portland, Oregon, USA Professorial Fellow, Institute of Health and Ageing Australian Catholic
Upcoming Agents for Osteoporosis May 5, 2017 Michael R. McClung, MD, FACP Director, Oregon Osteoporosis Center Portland, Oregon, USA Professorial Fellow, Institute of Health and Ageing Australian Catholic
Talking to patients with osteoporosis about initiating therapy
 Talking to patients with osteoporosis about initiating therapy Deborah Sellmeyer, MD Director, Johns Hopkins Metabolic Bone Center Dept of Medicine, Division of Endocrinology Disclosure DSMB member for
Talking to patients with osteoporosis about initiating therapy Deborah Sellmeyer, MD Director, Johns Hopkins Metabolic Bone Center Dept of Medicine, Division of Endocrinology Disclosure DSMB member for
Kristen M. Nebel, DO PENN/ LGHP Geriatrics. Temple Family Medicine Review
 Kristen M. Nebel, DO PENN/ LGHP Geriatrics 10/3/17 Temple Family Medicine Review OBJECTIVES Define Revised 2017 American College of Physician Recommendations Screening, Prevention and Treatment Application
Kristen M. Nebel, DO PENN/ LGHP Geriatrics 10/3/17 Temple Family Medicine Review OBJECTIVES Define Revised 2017 American College of Physician Recommendations Screening, Prevention and Treatment Application
NEW HORIZONS IN OSTEOPOROSIS THERAPY. Sundeep Khosla, M.D. Mayo Clinic, Rochester, MN
 NEW HORIZONS IN OSTEOPOROSIS THERAPY Sundeep Khosla, M.D. Mayo Clinic, Rochester, MN DISCLOSURES SUNDEEP KHOSLA, M.D. Investigator-initiated grant Merck No non-fda approved recommendations RISK ASSESSMENT
NEW HORIZONS IN OSTEOPOROSIS THERAPY Sundeep Khosla, M.D. Mayo Clinic, Rochester, MN DISCLOSURES SUNDEEP KHOSLA, M.D. Investigator-initiated grant Merck No non-fda approved recommendations RISK ASSESSMENT
A KL/R / AN A K/O / P O G G
 Outline and New Treatments on the Horizon Steven R. Cummings, MD CPMC and UCSF San Francisco Coordinating Center Support from Lilly and Amgen New treatments, new mechanisms of action Cathepsin K inhibition
Outline and New Treatments on the Horizon Steven R. Cummings, MD CPMC and UCSF San Francisco Coordinating Center Support from Lilly and Amgen New treatments, new mechanisms of action Cathepsin K inhibition
TREATMENT OF OSTEOPOROSIS HOLIDAYS OR NO HOLIDAYS? Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO
 TREATMENT OF OSTEOPOROSIS HOLIDAYS OR NO HOLIDAYS? Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO DISCLOSURES Honoraria: Amgen, Merck, Shire Consulting : AbbVie, Amgen, Merck,
TREATMENT OF OSTEOPOROSIS HOLIDAYS OR NO HOLIDAYS? Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO DISCLOSURES Honoraria: Amgen, Merck, Shire Consulting : AbbVie, Amgen, Merck,
Osteoporosis 2017 Breaking News. Julie L. Carkin, MD The Seattle Arthritis Clinic
 Osteoporosis 2017 Breaking News Julie L. Carkin, MD The Seattle Arthritis Clinic 1 Yes, Hopefully & No Anabolic Teriparatide Abaloparatide Romosozumab blosozumab Anti-catabolic Bisphosphonates Denosumab
Osteoporosis 2017 Breaking News Julie L. Carkin, MD The Seattle Arthritis Clinic 1 Yes, Hopefully & No Anabolic Teriparatide Abaloparatide Romosozumab blosozumab Anti-catabolic Bisphosphonates Denosumab
Summary. Background. Diagnosis
 March 2009 Management of post-menopausal osteoporosis This bulletin focuses on the pharmacological management of patients with post-menopausal osteoporosis both those with clinically evident disease (e.g.
March 2009 Management of post-menopausal osteoporosis This bulletin focuses on the pharmacological management of patients with post-menopausal osteoporosis both those with clinically evident disease (e.g.
Clinical Practice. Presented by: Internist, Endocrinologist
 Clinical Practice Management of Osteoporosis Presented by: SaeedBehradmanesh, h MD Internist, Endocrinologist Iran, Isfahan, Feb. 2017 Definition: A disease characterized by low bone mass and microarchitectural
Clinical Practice Management of Osteoporosis Presented by: SaeedBehradmanesh, h MD Internist, Endocrinologist Iran, Isfahan, Feb. 2017 Definition: A disease characterized by low bone mass and microarchitectural
Page 1
 Osteoporosis Osteoporosis is a condition characterised by weakened bones that fracture easily. After menopause many women are at risk of developing osteoporosis. Peak bone mass is usually reached during
Osteoporosis Osteoporosis is a condition characterised by weakened bones that fracture easily. After menopause many women are at risk of developing osteoporosis. Peak bone mass is usually reached during
Refracture Prevention The Role of Primary Care
 MonashHealth Refracture Prevention The Role of Primary Care Professor Peter R Ebeling AO MBBS MD FRACP Head, Department of Medicine School for Clinical Sciences Monash Health Translation Precinct Monash
MonashHealth Refracture Prevention The Role of Primary Care Professor Peter R Ebeling AO MBBS MD FRACP Head, Department of Medicine School for Clinical Sciences Monash Health Translation Precinct Monash
Keeping old bones from breaking: The diagnosis, prevention, and treatment of osteoporosis
 Keeping old bones from breaking: The diagnosis, prevention, and treatment of osteoporosis Balanced data about medications www.rxfacts.org Copyright 2010 by The Alosa Foundation. All rights reserved. www.rxfacts.org
Keeping old bones from breaking: The diagnosis, prevention, and treatment of osteoporosis Balanced data about medications www.rxfacts.org Copyright 2010 by The Alosa Foundation. All rights reserved. www.rxfacts.org
Osteoporosis Update. Case 2. Case 1: Monday morning, 8:15
 Osteoporosis Update Laura E. Ryan, MD Assistant Director for Special Programs Center for Women s Health Clinical Assistant Professor of Medicine Division of Endocrinology, Diabetes and Metabolism The Ohio
Osteoporosis Update Laura E. Ryan, MD Assistant Director for Special Programs Center for Women s Health Clinical Assistant Professor of Medicine Division of Endocrinology, Diabetes and Metabolism The Ohio