C. Christopher Smith, M.D. Associate Professor of Medicine Harvard Medical School Beth Israel Deaconess Medical Center
|
|
|
- Marshall Harrell
- 6 years ago
- Views:
Transcription

1



2 Evaluation and Treatment of the Painful Shoulder in the Primary Care Setting C. Christopher Smith, M.D. Associate Professor of Medicine Harvard Medical School Beth Israel Deaconess Medical Center
3 A 65-year-old woman with a history of type II DM presents for evaluation of new left shoulder pain. The pain is in her anterior and lateral shoulder and has gradually worsened over the last three weeks. It is dull and constant and keeps her up at night. She also notices marked discomfort when she combs her hair and cannot get sweaters from the top of her closet due to pain and weakness. She denies any trauma or prior injuries. She works as an investment banker.
4 The Painful Shoulder Recognize, diagnose and treat the most common cause of shoulder pain in the primary care setting Know how to differentiate it from other common causes of shoulder pain
5 The Painful Shoulder Anatomy History Differential based on patient s age and location of pain Physical exam maneuvers Initial treatment
6 Anatomy of the Shoulder UpToDate, 2006
7
8 The Rotator Cuff Muscles UpToDate, 2006
9 Causes of Shoulder Pain Acromioclavicular Osteoarthritis Adhesive Capsulitis Biceps Tendonitis Brachial Plexus Neuritis Cervical Radiculopathy Glenohumeral Arthritis Instability Impingement Syndrome Systemic Inflammatory Disorders Referred Pain - Diaphragmatic, Subdiaphragmatic and Intrathoracic Causes
10 In the primary care setting, what is the most common cause of nontraumatic shoulder pain? A. Bicipital Tendonitis B. Impingement Syndrome C. Adhesive Capsulitis (Frozen Shoulder) D. Osteoarthritis of the Glenohumeral Joint E. Acromioclavicular Joint Osteoarthritis
11 In the primary care setting, what is the most common cause of nontraumatic shoulder pain? A. Bicipital Tendonitis B. Impingement Syndrome C. Adhesive Capsulitis (Frozen Shoulder) D. Osteoarthritis of the Glenohumeral Joint E. Acromioclavicular Joint Osteoarthritis
12 Causes of Shoulder Pain in the Primary Care Setting: Impingement Syndrome > 70% Adhesive Capsulitis 12% Bicipital Tendonitis 4% A/C Joint OA 7% Other 7% Smith, J Gen Intern Med, 1992
13 So what is impingement syndrome?

14 Impingement Syndrome UpToDate, 2006
15 Typical History of Impingement Syndrome Any age, but risk increases with age Anterior or lateral shoulder pain Pain exacerbated by abduction and forward flexion Night pain common
16 Age and Shoulder Pain Young (< 30 y.o.) Dislocations/Instability of Glenohumeral Joint Separation of AC joint Overuse injury Less Young (30-60 y.o.) Impingement Syndrome Adhesive Capsulitis (especially in diabetics) Separation/Overuse as above Older (> 60 y.o.) Impingement Syndrome (non-traumatic tears) Adhesive Capsulitis Systemic Conditions (if bilateral, PMR, RA)
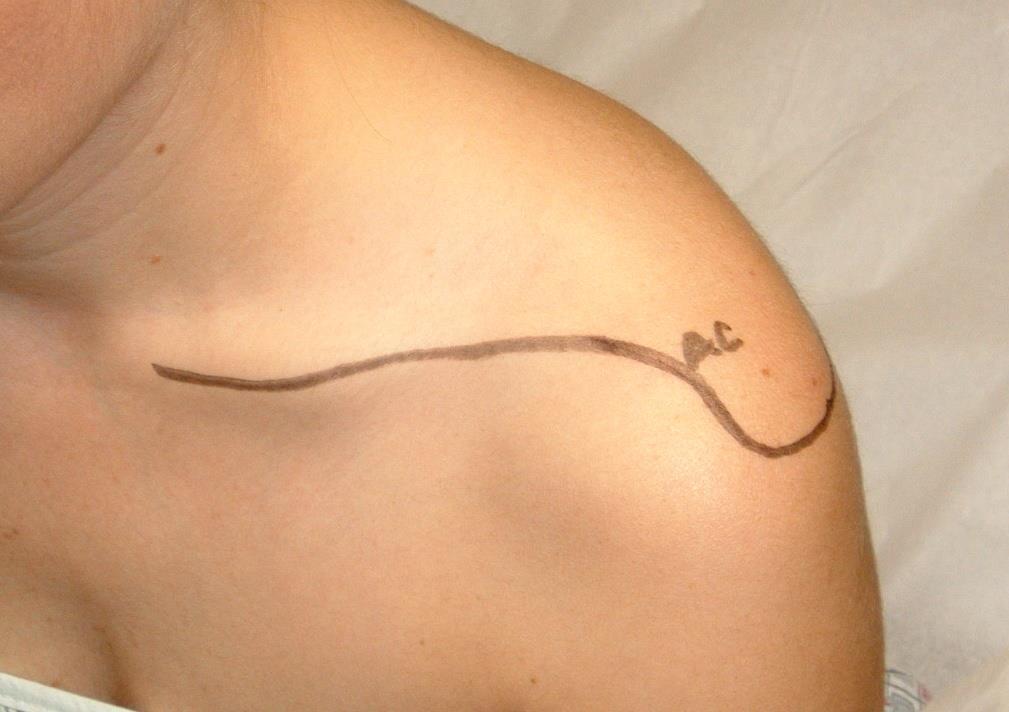
17 Physical Examination Inspection Palpation
18


19

20
21 Physical Examination Inspection Palpation Range of Motion Passive and Active Strength and Sensation Specific Maneuvers to Confirm Diagnosis

22 Maneuvers to Verify Impingement Syndrome Painful arc

23 Maneuvers to Verify Impingement Syndrome Empty Can Test

24 Maneuvers to Verify Impingement Syndrome Neer s Test Neer, Clin Orthop 1983

25 Maneuvers to Verify Impingement Syndrome Hawkins Test Hawkins, Am J Sports Med 1980
26
27 A 65-year-old woman with a history of type II DM presents for evaluation of new left shoulder pain. The pain is in her anterior and lateral shoulder and has gradually worsened over the last three weeks. It is dull and constant and keeps her up at night. She also notices marked discomfort when she combs her hair and cannot get her sweaters from the top of her closet due to pain and weakness. She denies any trauma or prior injuries. She works as an investment banker.
28 On inspection, her left humerus was riding slightly higher than her right. There was pain with palpation of the lateral subacromial space. ROM revealed pain with abduction and forward flexion; it was worse with active than passive movement. Positive empty can, Neer and Hawkins test.
29 What is the most appropriate initial treatment for this patient? A. NSAIDs alone B. NSAIDs with Physical Therapy C. Subacromial Steroid Injection with PT D. NSAIDs plus Steroid Injection E. Orthopedic consultation
30 What is the most appropriate initial treatment for this patient? A. NSAIDs alone B. NSAIDs with Physical Therapy C. Subacromial Steroid Injection with PT D. NSAIDs plus Steroid Injection E. Orthopedic consultation
31 Treatment Reduce offending activities Physical Therapy Aimed at improving mechanical dysfunction and shoulder motion NSAIDs or Subacromial injection Each is better than placebo Little long term difference No benefit in combination treatment White, J Rheumatol 1986 Petri, Arthritis Rheum 1987
32
33 You passively abduct the arm to 160 degrees and ask the patient to slowly lower her arm. At approximately 90 degrees, she is unable to continue to lower her arm due to weakness and she drops it to her side.
34 What is your diagnosis now? A. Bicipital Tendonitis B. Impingement Syndrome C. Adhesive Capsulitis (Frozen Shoulder) D. Tear of Supraspinatus Tendon E. Glenohumeral Joint Osteoarthritis
35 What is your diagnosis now? A. Bicipital Tendonitis B. Impingement Syndrome C. Adhesive Capsulitis (Frozen Shoulder) D. Tear of Supraspinatus Tendon E. Glenohumeral Joint Osteoarthritis
36 Supraspinatus Tendon Tear Positive Drop-Arm Test Supraspinatus weakness External Rotation weakness Impingement Signs Greater than 60 years old Murrell, Lancet 2001
37 Diagnosing Rotator Cuff Tear # Positive signs* Age Probability of rotator cuff tear All 3 Any 98% Any 2 > 60 98% Any 2 < 60 64% Any 1 > 70 76% Any 1 < 40 12% None Any 5% * supraspinatus weakness, weakness in external rotation, positive impingement signs Murrell, Lancet 2001
38 Diagnosis of Rotator Cuff Tear Internal Rotation Lag Sign
39 External Rotation Lag Sign
40 Clinical Tests for Rotator Cuff Disease and Tears Test + LR - LR Painful Arch (RCD) Drop Arm (RCD) External Resistance (RCD) External Lag (Full Tear) Internal Lag (Full Tear) RCD=Rotator Cuff Disease Hermans. JAMA, 2013

41 Diagnosis of Rotator Cuff Tear Internal Rotation Lag Sign
42 External Rotation Lag Sign
43 A 55-year-old male with IDDM, HTN and GERD presents with three months of worsening left lateral shoulder pain, which is worse at night. He reports pain with most any movement. Range of motion testing reveals pain and restricted movement in most directions. Symptoms are present with both passive and active movement.
44 Adhesive Capsulitis or Frozen Shoulder Thickening and contraction of the capsule surrounding the glenohumeral joint Insidious onset of pain Night pain Pain in deltoid, but no tenderness to palpation Pain and limited active and passive ROM Need AP X-ray of glenohumeral joint to rule out glenohumeral arthritis Treatment: Physical Therapy
45 What is the most significant risk factor for adhesive capsulitis? A. Diabetes B. Hypothyroidism C. Immobility D. AVN of glenohumeral head E. Reflex sympathetic dystrophy
46 What is the most significant risk factor for adhesive capsulitis? A. Diabetes B. Hypothyroidism C. Immobility D. AVN of glenohumeral head E. Reflex sympathetic dystrophy
47 46 year old male who moves furniture on the weekends and works as a handyman during the week, presents with right anterior shoulder pain. The pain began after a particularly heavy move, where he moved over a hundred boxes. No fever, chills, night sweats; no weakness or numbness. No prior injuries. He points to his anterior shoulder with one finger. He has a normal ROM and good strength and positive Yergason and Speed s tests.
48 What is your diagnosis? A. Bicipital Tendonitis B. Impingement Syndrome C. Adhesive Capsulitis (Frozen Shoulder) D. Tear of Supraspinatus Tendon E. Glenohumeral Joint Osteoarthritis
49 What is your diagnosis? A. Bicipital Tendonitis B. Impingement Syndrome C. Adhesive Capsulitis (Frozen Shoulder) D. Tear of Supraspinatus Tendon E. Glenohumeral Joint Osteoarthritis
50 Anterior View of Shoulder UpToDate, 2006
51 Biceps Tendonitis Inflammation of long head of the biceps tendon 95% associated with impingement syndrome Repetitive lifting, overhead reaching or forearm supination Anterior humeral pain Tenderness in bicipital groove Exacerbated with resisted elbow flexion or forearm supination Yergason and Speed s Tests Impingement signs Treatment Rest, restriction of lifting, reaching and supination Anti-inflammatory therapy & Ice Physical Therapy Holtby, Arthroscopy 2004

52 Yergason Test Evaluate biceps tendon by palpating bicipital groove while patient flexes elbow to 90 degrees and supinates against resistance Woodward, Am Fam Phys 2000

53 Speed s Test With elbow extended and hand supinated, palpate bicipital groove while patient attempts to forward flex shoulder 30 degrees against resistance Siegel, Am Fam Phys 1999
54 A 62 year old man was pulling a dead branch from a tree when he felt a sudden pain in his upper arm and heard an audible snap. Now, two weeks later, he has no pain and only minimal loss of strength. His exam is significant for the finding below. Which is the most likely diagnosis? A. Rotator cuff strain B. Proximal biceps tendon rupture C. Distal biceps tendon rupture D. Biceps tendonitis

55 A 62 year old man was pulling a dead branch from a tree when he felt a sudden pain in his upper arm and heard an audible snap. Now, two weeks later, he has no pain and only minimal loss of strength. His exam is significant for the finding below. Which is the most likely diagnosis? A. Rotator cuff strain B. Proximal biceps tendon rupture C. Distal biceps tendon rupture D. Biceps tendonitis
56 Biceps Tendon Tear Proximal aspect of long head of biceps tendon After especially vigorous lifting Often in setting of chronically inflamed tendon Weakness of elbow flexion/supination Popeye Sign - bulge just proximal to antecubital fossa Risk Factors: Recurrent tendonitis Prior tear of rotator cuff or biceps Age > 50 RA
57 A proximal bicipital tendon tear can usually be treated conservatively, avoiding surgery. A. True B. False
58 A proximal bicipital tendon tear can usually be treated conservatively, avoiding surgery. A. True B. False
59 Summary Impingement syndrome most common cause of shoulder pain in the primary care setting Systematic approach to physical exam Range of Motion: pain with abduction, forward flexion; active > passive; painful arc Empty can, Neer, Hawkins tests to confirm Drop arm, internal and external lag signs indicate a complete tear - especially in patients > 60 years old
60 Summary Adhesive Capsulitis DM or Immobile shoulder Limited ROM in most planes Pain with both active passive ROM Biceps Tendonitis Associated with impingement syndrome Reproduced with Yergason and Speed s tests Popeye sign for biceps tendon tear
61 Summary A careful history and physical examination can correctly diagnose most common causes of shoulder pain. aspx?mediaid=
62 Questions from the Audience?
63
The Shoulder. Jennifer R Marks, MD
 The Shoulder Jennifer R Marks, MD Shoulder Anatomy Skeletal & ligamentous components: The joint is comprised of a confluence of Scapula Clavicle Humerus https://www.shoulderdoc.co.uk/article/ http/ www.shoulderdoc.co.uk/article/117777
The Shoulder Jennifer R Marks, MD Shoulder Anatomy Skeletal & ligamentous components: The joint is comprised of a confluence of Scapula Clavicle Humerus https://www.shoulderdoc.co.uk/article/ http/ www.shoulderdoc.co.uk/article/117777
Physical Examination of the Shoulder
 General setup Patient will be examined in both the seated and supine position so exam table needed 360 degree access to patient Expose neck and both shoulders (for comparison); female in gown or sports
General setup Patient will be examined in both the seated and supine position so exam table needed 360 degree access to patient Expose neck and both shoulders (for comparison); female in gown or sports
Chronic Shoulder Disorders
 Chronic Shoulder Disorders Dr. Mustafa Elsingergy Consultant orthopedic surgeon Dallah Hospita Prof. Mamoun Kremli Almaarefa Medical College Contents INTRINSIC Shoulder Pain Due to causes in the shoulder
Chronic Shoulder Disorders Dr. Mustafa Elsingergy Consultant orthopedic surgeon Dallah Hospita Prof. Mamoun Kremli Almaarefa Medical College Contents INTRINSIC Shoulder Pain Due to causes in the shoulder
SHOULDER PAIN. A Real Pain in the Neck. Michael Wolk, MD Northeastern Rehabilitation Associates October 31, 2017
 SHOULDER PAIN A Real Pain in the Neck Michael Wolk, MD Northeastern Rehabilitation Associates October 31, 2017 THE SHOULDER JOINT (S) 1. glenohumeral 2. suprahumeral 3. acromioclavicular 4. scapulocostal
SHOULDER PAIN A Real Pain in the Neck Michael Wolk, MD Northeastern Rehabilitation Associates October 31, 2017 THE SHOULDER JOINT (S) 1. glenohumeral 2. suprahumeral 3. acromioclavicular 4. scapulocostal
Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of
 Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of chronic shoulder pain Review with some case questions Bones:
Review shoulder anatomy Review the physical exam of the shoulder Discuss some common causes of acute shoulder pain Discuss some common causes of chronic shoulder pain Review with some case questions Bones:
Evaluation of the Knee and Shoulder
 Evaluation of the Knee and Shoulder Karen J. Boselli, MD Northeast Regional Nurse Practitioner Conference May 2018 Knee Overview History Examination Top 5 diagnoses When to image When to refer Pain most
Evaluation of the Knee and Shoulder Karen J. Boselli, MD Northeast Regional Nurse Practitioner Conference May 2018 Knee Overview History Examination Top 5 diagnoses When to image When to refer Pain most
Evaluating shoulder injuries in primary care Bethany Reed, MSn, AGPCNP-BC One Medical Group
 Evaluating shoulder injuries in primary care Bethany Reed, MSn, AGPCNP-BC One Medical Group Disclosures There has been no commercial support or sponsorship for this program. The planners and presenters
Evaluating shoulder injuries in primary care Bethany Reed, MSn, AGPCNP-BC One Medical Group Disclosures There has been no commercial support or sponsorship for this program. The planners and presenters
The examination of the painful knee. Maja K Artandi, MD, FACP Clinical Associate Professor of Medicine Stanford University
 The examination of the painful knee Maja K Artandi, MD, FACP Clinical Associate Professor of Medicine Stanford University Objectives of the talk By the end of this talk you will know The important anatomy
The examination of the painful knee Maja K Artandi, MD, FACP Clinical Associate Professor of Medicine Stanford University Objectives of the talk By the end of this talk you will know The important anatomy
Shoulder examination. P Sripathi Rao Arthroscopy & Sports Injuries Unit Dean, Kasturba Medical College
 Shoulder examination P Sripathi Rao Arthroscopy & Sports Injuries Unit Dean, Kasturba Medical College Manipal University, Manipal Common symptoms Tingling Numbness Pain Loss of movements Weakness Approach
Shoulder examination P Sripathi Rao Arthroscopy & Sports Injuries Unit Dean, Kasturba Medical College Manipal University, Manipal Common symptoms Tingling Numbness Pain Loss of movements Weakness Approach
1. Occupation; Right or left handed, Age
 SHOULDER HISTORY 1. Occupation; Right or left handed, Age 2. Pain: Site. Any referred pain to the deltoid insertion Any localizing pain at Acromio-clavicular joint How long? Continuous or not Night pain
SHOULDER HISTORY 1. Occupation; Right or left handed, Age 2. Pain: Site. Any referred pain to the deltoid insertion Any localizing pain at Acromio-clavicular joint How long? Continuous or not Night pain
Stefan C Muzin, MD PM&R Attending Physician, Beth Israel Deaconess Medical Center, Harvard Medical School Onsite Physiatrist, GE Aviation, Lynn, MA
 Stefan C Muzin, MD PM&R Attending Physician, Beth Israel Deaconess Medical Center, Harvard Medical School Onsite Physiatrist, GE Aviation, Lynn, MA Consultant, OEHN (Occupational and Environmental Network)
Stefan C Muzin, MD PM&R Attending Physician, Beth Israel Deaconess Medical Center, Harvard Medical School Onsite Physiatrist, GE Aviation, Lynn, MA Consultant, OEHN (Occupational and Environmental Network)
Shoulder Joint Examination. Shoulder Joint Examination. Inspection. Inspection Palpation Movement. Look Feel Move
 Shoulder Joint Examination History Cuff Examination Instability Examination AC Joint Examination Biceps Tendon Examination Superior Labrum Examination Shoulder Joint Examination Inspection Palpation Movement
Shoulder Joint Examination History Cuff Examination Instability Examination AC Joint Examination Biceps Tendon Examination Superior Labrum Examination Shoulder Joint Examination Inspection Palpation Movement
EVALUATION OF ACUTE SHOULDER INJURIES. Douglas J. Moran, MD Orthopaedic Sports Medicine
 EVALUATION OF ACUTE SHOULDER INJURIES Douglas J. Moran, MD Orthopaedic Sports Medicine DISCLOSURES None of the planners or presenters of this session have disclosed any conflict or commercial interest
EVALUATION OF ACUTE SHOULDER INJURIES Douglas J. Moran, MD Orthopaedic Sports Medicine DISCLOSURES None of the planners or presenters of this session have disclosed any conflict or commercial interest
Mastering the Musculoskeletal Exam UCSF Essentials of Women s Health July 7, 2016 Carlin Senter, M.D. Henry Crevensten, M.D.
 Mastering the Musculoskeletal Exam UCSF Essentials of Women s Health July 7, 2016 Carlin Senter, M.D. Henry Crevensten, M.D. I have nothing to disclose Outline Knee exam Shoulder exam Knee Anatomy The
Mastering the Musculoskeletal Exam UCSF Essentials of Women s Health July 7, 2016 Carlin Senter, M.D. Henry Crevensten, M.D. I have nothing to disclose Outline Knee exam Shoulder exam Knee Anatomy The
RN(EC) ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***
 ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***") HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age - Certain conditions are more prevalent in particular age groups (i.e. Full rotator cuff tears are more common over the age of 45, traumatic injuries
HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age - Certain conditions are more prevalent in particular age groups (i.e. Full rotator cuff tears are more common over the age of 45, traumatic injuries
Sick Call Screener Course
 Sick Call Screener Course Musculoskeletal System Upper Extremities (2.7) 2.7-2-1 Enabling Objectives 1.46 Utilize the knowledge of musculoskeletal system anatomy while assessing a patient with a musculoskeletal
Sick Call Screener Course Musculoskeletal System Upper Extremities (2.7) 2.7-2-1 Enabling Objectives 1.46 Utilize the knowledge of musculoskeletal system anatomy while assessing a patient with a musculoskeletal
Subacromial Impingement (diagnostic methods )
") Subacromial Impingement (diagnostic methods ) M.N. Naderi Fellowship in shoulder and arthroscopic surgery Neer : Definition Impingement on the tendinous portion of the rotator cuff by the coracoacromial
Subacromial Impingement (diagnostic methods ) M.N. Naderi Fellowship in shoulder and arthroscopic surgery Neer : Definition Impingement on the tendinous portion of the rotator cuff by the coracoacromial
2015 OPSC Annual Convention. syllabus. February 4-8, 2015 Hyatt Regency Mission Bay San Diego, California
 2015 OPSC Annual Convention syllabus February 4-8, 2015 Hyatt Regency Mission Bay San Diego, California THURSDAY, FEBRUARY 5, 2015: 3:30pm - 4:30pm The Shoulder: 2 View or Not 2 View * Presented by Alexandra
2015 OPSC Annual Convention syllabus February 4-8, 2015 Hyatt Regency Mission Bay San Diego, California THURSDAY, FEBRUARY 5, 2015: 3:30pm - 4:30pm The Shoulder: 2 View or Not 2 View * Presented by Alexandra
Shoulder Pain: Diagnosis and Management
 Shoulder Pain: Diagnosis and Management Thomas J. Gill, M.D. Director, Boston Sports Medicine and Research Institute Associate Professor of Orthopedic Surgery Tufts Medical School www.bostonsportsmedicine.com
Shoulder Pain: Diagnosis and Management Thomas J. Gill, M.D. Director, Boston Sports Medicine and Research Institute Associate Professor of Orthopedic Surgery Tufts Medical School www.bostonsportsmedicine.com
Anatomical Considerations/ Pathophysiology The shoulder is the most mobile joint in the body. : Three bones:
 Introduction Musculoskeletal training is generally underrepresented in medical training and residency curriculums. There is a general deficit in musculoskeletal knowledge amongst current medical students,
Introduction Musculoskeletal training is generally underrepresented in medical training and residency curriculums. There is a general deficit in musculoskeletal knowledge amongst current medical students,
ATRAUMATIC SHOULDER CONDITIONS. Matthew J. Landfried, MD Orthopaedic Surgeon Genesee Orthopaedics and Sports Medicine
 ATRAUMATIC SHOULDER CONDITIONS Matthew J. Landfried, MD Orthopaedic Surgeon Genesee Orthopaedics and Sports Medicine MATTHEW LANDFRIED MD Board Certified in Orthopedic Surgery and Sports Medicine Received
ATRAUMATIC SHOULDER CONDITIONS Matthew J. Landfried, MD Orthopaedic Surgeon Genesee Orthopaedics and Sports Medicine MATTHEW LANDFRIED MD Board Certified in Orthopedic Surgery and Sports Medicine Received
4/12/2016. Goals. Anatomy. Basic Anatomy. Biomechanics. Function. Traumatic Rupture of Proximal Biceps: In-season Rehabilitation and Management
 Goals Traumatic Rupture of Proximal Biceps: In-season Rehabilitation and Management Thomas F. LaPorta, MD To understand the anatomy of the biceps at the shoulder To present the mechanism, signs and symptoms,
Goals Traumatic Rupture of Proximal Biceps: In-season Rehabilitation and Management Thomas F. LaPorta, MD To understand the anatomy of the biceps at the shoulder To present the mechanism, signs and symptoms,
 www.fisiokinesiterapia.biz Shoulder Problems Fractures Instability Impingement Miscellaneous Anatomy Bones Joints / Ligaments Muscles Neurovascular Anatomy Anatomy Supraspinatus Anterior Posterior Anatomy
www.fisiokinesiterapia.biz Shoulder Problems Fractures Instability Impingement Miscellaneous Anatomy Bones Joints / Ligaments Muscles Neurovascular Anatomy Anatomy Supraspinatus Anterior Posterior Anatomy
Diagnostic and Management Approach to the Painful Shoulder
 Diagnostic and Management Approach to the Painful Shoulder Introduction What conditions causing shoulder pain commonly present in General Practice? Subacromial impingement Rotator cuff tears AC joint pathology
Diagnostic and Management Approach to the Painful Shoulder Introduction What conditions causing shoulder pain commonly present in General Practice? Subacromial impingement Rotator cuff tears AC joint pathology
Soft Tissue Rheumatism. Elinor Mody, MD Chief, Division of Rheumatology Reliant Medical Group
 Soft Tissue Rheumatism Elinor Mody, MD Chief, Division of Rheumatology Reliant Medical Group Some problems are difficult, but diagnosing and treating most causes of joint pain are not! Common areas of
Soft Tissue Rheumatism Elinor Mody, MD Chief, Division of Rheumatology Reliant Medical Group Some problems are difficult, but diagnosing and treating most causes of joint pain are not! Common areas of
Acute Orthopaedic Injuries Developing a Diagnostic Approach to the Shoulder
 Acute Orthopaedic Injuries Developing a Diagnostic Approach to the Shoulder WWW.FISIOKINESITERAPIA.BIZ Overview To be able to quickly categorize shoulder injuries To take appropriate history and conduct
Acute Orthopaedic Injuries Developing a Diagnostic Approach to the Shoulder WWW.FISIOKINESITERAPIA.BIZ Overview To be able to quickly categorize shoulder injuries To take appropriate history and conduct
Shoulder Pain
 www.fisiokinesiterapia.biz Shoulder Pain Outline Shoulder Anatomy and Biomechanics Patient History and Pain Patterns Etiology and Differential Diagnoses Physical Examination Stepwise Clinical Approach
www.fisiokinesiterapia.biz Shoulder Pain Outline Shoulder Anatomy and Biomechanics Patient History and Pain Patterns Etiology and Differential Diagnoses Physical Examination Stepwise Clinical Approach
Shoulder joint Assessment and General View
 Shoulder joint Assessment and General View Done by; Mshari S. Alghadier BSc Physical Therapy RHPT 366 m.alghadier@sau.edu.sa http://faculty.sau.edu.sa/m.alghadier/ Functional anatomy The shoulder contains
Shoulder joint Assessment and General View Done by; Mshari S. Alghadier BSc Physical Therapy RHPT 366 m.alghadier@sau.edu.sa http://faculty.sau.edu.sa/m.alghadier/ Functional anatomy The shoulder contains
Incorporating OMM to Enhance Your Clinical Practice Osteopathic diagnosis and approach to the upper extremity
 Incorporating OMM to Enhance Your Clinical Practice Osteopathic diagnosis and approach to the upper extremity Sheldon C. Yao, D.O. Acting Department Chair March 1, 2013 Clinical significance Upper extremity
Incorporating OMM to Enhance Your Clinical Practice Osteopathic diagnosis and approach to the upper extremity Sheldon C. Yao, D.O. Acting Department Chair March 1, 2013 Clinical significance Upper extremity
Disclaimer. Evaluation & Treatment of Shoulder and Elbow Pain in the Adult Patient. Objectives. Anatomy
 Evaluation & Treatment of Shoulder and Elbow Pain in the Adult Patient William T. Crowe, RN-C, FNP, MSN, MBA Disclaimer! I, William T Crowe, have relevant financial relationships to be discussed, directly
Evaluation & Treatment of Shoulder and Elbow Pain in the Adult Patient William T. Crowe, RN-C, FNP, MSN, MBA Disclaimer! I, William T Crowe, have relevant financial relationships to be discussed, directly
DISTINGUISHING BETWEEN ACUTE AND CHRONIC ROTATOR CUFF INJURIES IN WORKERS COMPENSATION PATIENTS
 DISTINGUISHING BETWEEN ACUTE AND CHRONIC ROTATOR CUFF INJURIES IN WORKERS COMPENSATION PATIENTS Lyndon B. Gross M.D. Ph.D. The Orthopedic Center of St. Louis SHOULDER PAIN Third most common musculoskeletal
DISTINGUISHING BETWEEN ACUTE AND CHRONIC ROTATOR CUFF INJURIES IN WORKERS COMPENSATION PATIENTS Lyndon B. Gross M.D. Ph.D. The Orthopedic Center of St. Louis SHOULDER PAIN Third most common musculoskeletal
Working with The Shoulder
 Working with The Shoulder Plus BONUS Stretching! Dr Bryan Hawley DC Housekeeping Recording will be sent out tomorrow Certificates Questions All presented today is based off OUR OWN CLINIC system Email
Working with The Shoulder Plus BONUS Stretching! Dr Bryan Hawley DC Housekeeping Recording will be sent out tomorrow Certificates Questions All presented today is based off OUR OWN CLINIC system Email
ROTATOR CUFF DISORDERS/IMPINGEMENT
 ROTATOR CUFF DISORDERS/IMPINGEMENT Dr.KN Subramanian M.Ch Orth., FRCS (Tr & Orth), CCT Orth(UK) Consultant Orthopaedic Surgeon, Special interest: Orthopaedic Sports Injury, Shoulder and Knee Surgery, SPARSH
ROTATOR CUFF DISORDERS/IMPINGEMENT Dr.KN Subramanian M.Ch Orth., FRCS (Tr & Orth), CCT Orth(UK) Consultant Orthopaedic Surgeon, Special interest: Orthopaedic Sports Injury, Shoulder and Knee Surgery, SPARSH
Dr. Stefan C. Muzin, MD PM&R Beth Israel Deaconess Medical Center Harvard Medical School Consultant, GE Aviation, OEHN.
 Dr. Stefan C. Muzin, MD PM&R Beth Israel Deaconess Medical Center Harvard Medical School Consultant, GE Aviation, OEHN Work Related Workshop WorkInjuries Related Injuries Workshop Think of the Big Picture
Dr. Stefan C. Muzin, MD PM&R Beth Israel Deaconess Medical Center Harvard Medical School Consultant, GE Aviation, OEHN Work Related Workshop WorkInjuries Related Injuries Workshop Think of the Big Picture
The Shoulder. By Patrick Ryan, Bobby Law, Jack Beaty, Alex Newhouse and Chuck Nelson
 The Shoulder By Patrick Ryan, Bobby Law, Jack Beaty, Alex Newhouse and Chuck Nelson Learning Objectives/Agenda Review the anatomy of the shoulder Describe the main diseases of the shoulder Describe the
The Shoulder By Patrick Ryan, Bobby Law, Jack Beaty, Alex Newhouse and Chuck Nelson Learning Objectives/Agenda Review the anatomy of the shoulder Describe the main diseases of the shoulder Describe the
UPPER EXTREMITY INJURIES. Recognizing common injuries to the upper extremity
 UPPER EXTREMITY INJURIES Recognizing common injuries to the upper extremity ANATOMY BONES Clavicle Scapula Spine of the scapula Acromion process Glenoid fossa/cavity Humerus Epicondyles ANATOMY BONES Ulna
UPPER EXTREMITY INJURIES Recognizing common injuries to the upper extremity ANATOMY BONES Clavicle Scapula Spine of the scapula Acromion process Glenoid fossa/cavity Humerus Epicondyles ANATOMY BONES Ulna
The Shoulder Complex. Anatomy. Articulations 12/11/2017. Oak Ridge High School Conroe, Texas. Clavicle Collar Bone Scapula Shoulder Blade Humerus
 The Shoulder Complex Oak Ridge High School Conroe, Texas Anatomy Clavicle Collar Bone Scapula Shoulder Blade Humerus Articulations Sternoclavicular SC joint. Sternum and Clavicle. Acromioclavicular AC
The Shoulder Complex Oak Ridge High School Conroe, Texas Anatomy Clavicle Collar Bone Scapula Shoulder Blade Humerus Articulations Sternoclavicular SC joint. Sternum and Clavicle. Acromioclavicular AC
Pearson Education Limited Edinburgh Gate Harlow Essex CM20 2JE England and Associated Companies throughout the world
 Pearson Education Limited Edinburgh Gate Harlow Essex CM20 2JE England and Associated Companies throughout the world Visit us on the World Wide Web at: www.pearsoned.co.uk Pearson Education Limited 2014
Pearson Education Limited Edinburgh Gate Harlow Essex CM20 2JE England and Associated Companies throughout the world Visit us on the World Wide Web at: www.pearsoned.co.uk Pearson Education Limited 2014
Increase referrals and revenue by incorporating diagnosis and conservative management of subacromial impingement syndrome
 IN THIS ISSUE Issue: July 2002 Rubbing Shoulders by Craig D. Cook, DC, CCSP, QME Normal Version Increase referrals and revenue by incorporating diagnosis and conservative management of subacromial impingement
IN THIS ISSUE Issue: July 2002 Rubbing Shoulders by Craig D. Cook, DC, CCSP, QME Normal Version Increase referrals and revenue by incorporating diagnosis and conservative management of subacromial impingement
Joint G*H. Joint S*C. Joint A*C. Labrum. Humerus. Sternum. Scapula. Clavicle. Thorax. Articulation. Scapulo- Thoracic
 A*C Joint Scapulo- Thoracic Articulation Thorax Sternum Clavicle Scapula Humerus S*C Joint G*H Joint Labrum AC Ligaments SC Ligaments SC JOINT AC Coracoacromial GH GH Ligament Complex Coracoclavicular
A*C Joint Scapulo- Thoracic Articulation Thorax Sternum Clavicle Scapula Humerus S*C Joint G*H Joint Labrum AC Ligaments SC Ligaments SC JOINT AC Coracoacromial GH GH Ligament Complex Coracoclavicular
Evaluation of the Painful Shoulder
 Evaluation of the Painful Shoulder J. Lindsay Quade, MD Clinical Instructor Internal Medicine/Pediatrics Primary Care Sports Medicine Michigan Medicine Objectives Review important shoulder anatomy Review
Evaluation of the Painful Shoulder J. Lindsay Quade, MD Clinical Instructor Internal Medicine/Pediatrics Primary Care Sports Medicine Michigan Medicine Objectives Review important shoulder anatomy Review
Biceps Tendon Rupture
 Disclaimer This movie is an educational resource only and should not be used to manage Orthopaedic Health. All decisions about Biceps Tendon Rupture must be made in conjunction with your Physician or a
Disclaimer This movie is an educational resource only and should not be used to manage Orthopaedic Health. All decisions about Biceps Tendon Rupture must be made in conjunction with your Physician or a
Shoulder Labral Tear and Shoulder Dislocation
 Shoulder Labral Tear and Shoulder Dislocation The shoulder joint is a ball and socket joint with tremendous flexibility and range of motion. The ball is the humeral head while the socket is the glenoid.
Shoulder Labral Tear and Shoulder Dislocation The shoulder joint is a ball and socket joint with tremendous flexibility and range of motion. The ball is the humeral head while the socket is the glenoid.
Upper Extremity Injuries in Youth Baseball: Causes and Prevention
 Upper Extremity Injuries in Youth Baseball: Causes and Prevention Biomechanics Throwing a baseball is an unnatural movement Excessively high forces are generated at the elbow and shoulder Throwing requires
Upper Extremity Injuries in Youth Baseball: Causes and Prevention Biomechanics Throwing a baseball is an unnatural movement Excessively high forces are generated at the elbow and shoulder Throwing requires
Common neuromusculoskeletal disorders in the workplace W. Shane Journeay, PhD, MD, MPH, FRCPC, BC-OEM
 Common neuromusculoskeletal disorders in the workplace W. Shane Journeay, PhD, MD, MPH, FRCPC, BC-OEM OEMAC Calgary September 23, 2018 OBJECTIVES 1. To name key diagnoses of neuromusculoskeletal conditions
Common neuromusculoskeletal disorders in the workplace W. Shane Journeay, PhD, MD, MPH, FRCPC, BC-OEM OEMAC Calgary September 23, 2018 OBJECTIVES 1. To name key diagnoses of neuromusculoskeletal conditions
Inspection. Physical Examination of the Elbow. Anterior Elbow 2/14/2017. Inspection. Carrying angle. Lateral dimple. Physical Exam of the Elbow
 of the Elbow Anthony A. Romeo, MD Professor, Department of Orthopedics Head, Section of Shoulder and Elbow Surgery Rush University President-Elect, American Shoulder Elbow Surgeons Team Physician, Chicago
of the Elbow Anthony A. Romeo, MD Professor, Department of Orthopedics Head, Section of Shoulder and Elbow Surgery Rush University President-Elect, American Shoulder Elbow Surgeons Team Physician, Chicago
The Shoulder. Jill Inouye Primary Care Sports Medicine Family Medicine Resident School February 26, 2014
 The Shoulder Jill Inouye Primary Care Sports Medicine Family Medicine Resident School February 26, 2014 Objectives Review shoulder anatomy Explain and demonstrate shoulder physical exam Diagnosis and management
The Shoulder Jill Inouye Primary Care Sports Medicine Family Medicine Resident School February 26, 2014 Objectives Review shoulder anatomy Explain and demonstrate shoulder physical exam Diagnosis and management
Shoulder vs Neck Pathology. Goal: Simplify Evaluation of the Painful Shoulder. Shoulder: Bony Anatomy Three major bones. Shoulder Disorders: Overview
 Goal: Simplify Evaluation of the Painful Shoulder Can be challenging Overlapping diagnoses Multiple complaints - Neck - Shoulder - Back - Arm Shoulder vs Neck Pathology Very common to have neck pain with
Goal: Simplify Evaluation of the Painful Shoulder Can be challenging Overlapping diagnoses Multiple complaints - Neck - Shoulder - Back - Arm Shoulder vs Neck Pathology Very common to have neck pain with
Rotator Cuff Pathology. Shoulder Instability. Adhesive Capsulitis. AC Joint Dysfunction
 Shoulder Pain Red Flags Unexplained deformity or swelling Significant weakness not due to pain Suspected malignancy Fever/chills/malaise Significant/unexplained sensory/motor deficit Pulmonary or vascular
Shoulder Pain Red Flags Unexplained deformity or swelling Significant weakness not due to pain Suspected malignancy Fever/chills/malaise Significant/unexplained sensory/motor deficit Pulmonary or vascular
POST-SURGICAL POSTERIOR GLENOHUMERAL STABILIZATION REHABILITATION PROTOCOL (Capsulolabral Repair)
") Gregory N. Lervick, MD Andrew Anderson, PA-C 952-456-7111 POST-SURGICAL POSTERIOR GLENOHUMERAL STABILIZATION REHABILITATION PROTOCOL (Capsulolabral Repair) Open Arthroscopic Phase 1: Weeks 0-4 No shoulder
Gregory N. Lervick, MD Andrew Anderson, PA-C 952-456-7111 POST-SURGICAL POSTERIOR GLENOHUMERAL STABILIZATION REHABILITATION PROTOCOL (Capsulolabral Repair) Open Arthroscopic Phase 1: Weeks 0-4 No shoulder
Musculoskeletal Examination Benchmarks
 Musculoskeletal Examination Benchmarks _ The approach to examining the musculoskeletal system is the same no matter what joint or limb is being examined. The affected and contralateral region should both
Musculoskeletal Examination Benchmarks _ The approach to examining the musculoskeletal system is the same no matter what joint or limb is being examined. The affected and contralateral region should both
After Arthroscopic Subacromial Decompression Intact Rotator Cuff (Distal Clavicle Resection)
") After Arthroscopic Subacromial Decompression Intact Rotator Cuff (Distal Clavicle Resection) Rehabilitation Protocol Phase 1: Weeks 0-4 Restrictions ROM 140 degrees of forward flexion 40 degrees of external
After Arthroscopic Subacromial Decompression Intact Rotator Cuff (Distal Clavicle Resection) Rehabilitation Protocol Phase 1: Weeks 0-4 Restrictions ROM 140 degrees of forward flexion 40 degrees of external
Office Orthopedics. No conflict of interest No financial disclosures 1/31/2018
 Office Orthopedics Amin Afsari DO Orthopedic Hand and Upper Extremity Surgery Orthopedic Institute of Wisconsin Midwest Orthopedic Specialty Hospital 1 No conflict of interest No financial disclosures
Office Orthopedics Amin Afsari DO Orthopedic Hand and Upper Extremity Surgery Orthopedic Institute of Wisconsin Midwest Orthopedic Specialty Hospital 1 No conflict of interest No financial disclosures
Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD
 Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD Shoulder Articulations Glenohumeral Joint 2/3 total arc of motion Shallow Ball and Socket Joint Allows for excellent ROM Requires
Shoulder and Elbow ORTHOPAEDIC SYPMPOSIUM APRIL 8, 2017 DANIEL DOTY MD Shoulder Articulations Glenohumeral Joint 2/3 total arc of motion Shallow Ball and Socket Joint Allows for excellent ROM Requires
ADHESIVE CAPSULITIS (FROZEN SHOULDER)
") ADHESIVE CAPSULITIS (FROZEN SHOULDER) Frozen shoulder, or adhesive capsulitis is a condition that generally begins with the gradual onset of pain followed by a limitation of shoulder motion. The discomfort
ADHESIVE CAPSULITIS (FROZEN SHOULDER) Frozen shoulder, or adhesive capsulitis is a condition that generally begins with the gradual onset of pain followed by a limitation of shoulder motion. The discomfort
DIAGNOSTIC EVALUATION OF CERVICAL VS. SHOULDER PAIN: A PHYSIATRIST S PERSPECTIVE
 Russ Cantrell, M.D. Physical Medicine and Rehabilitation Orthopedic Sports Medicine and Spine Care Institute DIAGNOSTIC EVALUATION OF CERVICAL VS. SHOULDER PAIN: A PHYSIATRIST S PERSPECTIVE PHYSIATRIST
Russ Cantrell, M.D. Physical Medicine and Rehabilitation Orthopedic Sports Medicine and Spine Care Institute DIAGNOSTIC EVALUATION OF CERVICAL VS. SHOULDER PAIN: A PHYSIATRIST S PERSPECTIVE PHYSIATRIST
OCCUPATIONAL SHOULDER DISORDERS
 OCCUPATIONAL SHOULDER DISORDERS Mark A. Greenfield D.O., F.A.O.A.O. Orthopaedic Surgery May 13, 2016 CREDENTIALS Orthopaedic Surgeon Fellowship Trained Board Certified Licensed to practice in AZ Published
OCCUPATIONAL SHOULDER DISORDERS Mark A. Greenfield D.O., F.A.O.A.O. Orthopaedic Surgery May 13, 2016 CREDENTIALS Orthopaedic Surgeon Fellowship Trained Board Certified Licensed to practice in AZ Published
WEEKEND 2 Shoulder. Shoulder Active Range of Motion Assessment
 Virginia Orthopedic Manual Physical Therapy Institute - 2016 Technique Manual WEEKEND 2 Shoulder Shoulder Active Range of Motion Assessment - Patient Positioning: Standing, appropriately undressed so that
Virginia Orthopedic Manual Physical Therapy Institute - 2016 Technique Manual WEEKEND 2 Shoulder Shoulder Active Range of Motion Assessment - Patient Positioning: Standing, appropriately undressed so that
ACTIVE AGING.
 Shoulder Pain Rehabilitation Protocol Rotator Cuff Syndrome Shoulder impingement The Resistance Chair Solution Shoulder Impingement a. Shoulder impingement is one of the most common causes of shoulder
Shoulder Pain Rehabilitation Protocol Rotator Cuff Syndrome Shoulder impingement The Resistance Chair Solution Shoulder Impingement a. Shoulder impingement is one of the most common causes of shoulder
Diagnosis and Treatment of Common Shoulder Disorders
 Diagnosis and Treatment of Common Shoulder Disorders NAOEM Oct 14 th, 2017 Michael Codsi, M.D. www.drcodsi.com Learning Objectives SLAP tears diagnosis, imaging and treatment How to diagnose rotator cuff
Diagnosis and Treatment of Common Shoulder Disorders NAOEM Oct 14 th, 2017 Michael Codsi, M.D. www.drcodsi.com Learning Objectives SLAP tears diagnosis, imaging and treatment How to diagnose rotator cuff
Orthopedic Physical Assessment with Special Tests Shoulder
 Orthopedic Physical Assessment with Special Tests Shoulder COURSE DESCRIPTION Detailed video demonstrations of tests and procedures common in musculoskeletal assessment are supplemented by high-quality
Orthopedic Physical Assessment with Special Tests Shoulder COURSE DESCRIPTION Detailed video demonstrations of tests and procedures common in musculoskeletal assessment are supplemented by high-quality
Nonoperative Treatment For Rotator Cuff Tendinitis/ Partial Thickness Tear Dr. Trueblood
 Nonoperative Treatment For Rotator Cuff Tendinitis/ Partial Thickness Tear Dr. Trueblood Relieving Pain Patients who present with SIS will have shoulder pain that is exacerbated with overhead activities.
Nonoperative Treatment For Rotator Cuff Tendinitis/ Partial Thickness Tear Dr. Trueblood Relieving Pain Patients who present with SIS will have shoulder pain that is exacerbated with overhead activities.
Shoulder Arthroplasty
 Shoulder Arthroplasty Nathan G. Everding, MD Specializing in Hand, Wrist, Elbow & Shoulder Surgery Syracuse Orthopedic Specialists SJH Family Practice Refresher course 3/8/19 Shoulder Arthroplasty Rate
Shoulder Arthroplasty Nathan G. Everding, MD Specializing in Hand, Wrist, Elbow & Shoulder Surgery Syracuse Orthopedic Specialists SJH Family Practice Refresher course 3/8/19 Shoulder Arthroplasty Rate
Shoulder Injury Evaluation.
 Shoulder Injury Evaluation www.fisiokinesiterapia.biz Basic Anatomy & Kinesiology 3 Bone Structures Clavicle Scapula Humerus Evaluation Principles Always follow a standard progression Determine the target
Shoulder Injury Evaluation www.fisiokinesiterapia.biz Basic Anatomy & Kinesiology 3 Bone Structures Clavicle Scapula Humerus Evaluation Principles Always follow a standard progression Determine the target
6/5/2018. The Management of Shoulder Conditions in Primary Care. Mr Rupen Dattani (FRCS (Tr & Orth) Consultant Shoulder & Elbow Surgeon
 Consultant Shoulder & Elbow Surgeon") The Management of Shoulder Conditions in Primary Care Mr Rupen Dattani (FRCS (Tr & Orth) Consultant Shoulder & Elbow Surgeon Highgate Private Hospital (Chelsea & Westminster Hospital NHS Foundation Trust)
The Management of Shoulder Conditions in Primary Care Mr Rupen Dattani (FRCS (Tr & Orth) Consultant Shoulder & Elbow Surgeon Highgate Private Hospital (Chelsea & Westminster Hospital NHS Foundation Trust)
Rotator Cuff Repair TRENDS OF REPAIRS. Evolution of Arthroscopic Repair. Shoulder Girdle. Rotator Cuff Repair 8/29/2013
 Rotator Cuff Repair Indications, Patient Selection, Outcomes James C. Vailas, M.D. New Hampshire Orthopaedic Center September 14, 2013 New Hampshire Musculoskeletal Institute 20 th Annual Symposium Evolution
Rotator Cuff Repair Indications, Patient Selection, Outcomes James C. Vailas, M.D. New Hampshire Orthopaedic Center September 14, 2013 New Hampshire Musculoskeletal Institute 20 th Annual Symposium Evolution
CLINICAL EXAMINATION OF THE SHOULDER JOINT 대한신경근골격연구회 분당제생병원재활의학과 박준성
 CLINICAL EXAMINATION OF THE SHOULDER JOINT 대한신경근골격연구회 분당제생병원재활의학과 박준성 Clinical Examination of the Shoulder Good history, full clinical examination Detailed knowledge of the anatomy solve the majority of
CLINICAL EXAMINATION OF THE SHOULDER JOINT 대한신경근골격연구회 분당제생병원재활의학과 박준성 Clinical Examination of the Shoulder Good history, full clinical examination Detailed knowledge of the anatomy solve the majority of
MUSCLES OF SHOULDER REGION
 Dr Jamila EL Medany OBJECTIVES At the end of the lecture, students should: List the name of muscles of the shoulder region. Describe the anatomy of muscles of shoulder region regarding: attachments of
Dr Jamila EL Medany OBJECTIVES At the end of the lecture, students should: List the name of muscles of the shoulder region. Describe the anatomy of muscles of shoulder region regarding: attachments of
1-Apley scratch test.
 1-Apley scratch test. The patient attempts to touch the opposite scapula to test range of motion of the shoulder. 1-Testing abduction and external rotation( +ve sign touch the opposite scapula, -ve sign
1-Apley scratch test. The patient attempts to touch the opposite scapula to test range of motion of the shoulder. 1-Testing abduction and external rotation( +ve sign touch the opposite scapula, -ve sign
Shoulder Instability. Fig 1: Intact labrum and biceps tendon
 Shoulder Instability What is it? The shoulder joint is a ball and socket joint, with the humeral head (upper arm bone) as the ball and the glenoid as the socket. The glenoid (socket) is a shallow bone
Shoulder Instability What is it? The shoulder joint is a ball and socket joint, with the humeral head (upper arm bone) as the ball and the glenoid as the socket. The glenoid (socket) is a shallow bone
Rheumatology & Immunology. Regional pain syndromes to be covered today. Some definitions. Tendinitis. Bursitis. History. History. Exam.
 Rheumatology & Immunology Some problems are difficult, but diagnosing and treating soft tissue syndromes are not! Soft tissue syndromes one of the most common reasons patients present to their doctor.
Rheumatology & Immunology Some problems are difficult, but diagnosing and treating soft tissue syndromes are not! Soft tissue syndromes one of the most common reasons patients present to their doctor.
Frozen shoulder, also called adhesive capsulitis, causes pain and stiffness in the shoulder. Over time, the shoulder becomes very hard to move.
 1 Frozen Shoulder What is frozen shoulder? Frozen shoulder, also called adhesive capsulitis, causes pain and stiffness in the shoulder. Over time, the shoulder becomes very hard to move. Frozen shoulder
1 Frozen Shoulder What is frozen shoulder? Frozen shoulder, also called adhesive capsulitis, causes pain and stiffness in the shoulder. Over time, the shoulder becomes very hard to move. Frozen shoulder
Impingement syndrome. Clinical features. Management. Rotator cuff tear diagnosed. Go to rotator cuff tear
 Impingement syndrome Clinical features Management Poor response Good response Refer to orthopaedic surgery R Review as appropriate Investigations Rotator cuff tear diagnosed Go to rotator cuff tear Consider
Impingement syndrome Clinical features Management Poor response Good response Refer to orthopaedic surgery R Review as appropriate Investigations Rotator cuff tear diagnosed Go to rotator cuff tear Consider
REMINDER. an exercise program. Senior Fitness Obtain medical clearance and physician s release prior to beginning
 Functional Forever: Exercise for Independent Living REMINDER Obtain medical clearance and physician s release prior to beginning an exercise program for clients with medical or orthopedic concerns. What
Functional Forever: Exercise for Independent Living REMINDER Obtain medical clearance and physician s release prior to beginning an exercise program for clients with medical or orthopedic concerns. What
ROTATOR CUFF INJURIES / IMPINGEMENT SYNDROME
 ROTATOR CUFF INJURIES / IMPINGEMENT SYNDROME Shoulder injuries are common in patients across all ages, from young, athletic people to the aging population. Two of the most common problems occur in the
ROTATOR CUFF INJURIES / IMPINGEMENT SYNDROME Shoulder injuries are common in patients across all ages, from young, athletic people to the aging population. Two of the most common problems occur in the
Frozen Shoulder Syndrome Rehabilitation Using the Resistance Chair
 Frozen Shoulder Syndrome Rehabilitation Using the Resistance Chair General Information Frozen shoulder is a condition where the shoulder joint (glenohumeral joint) gradually becomes stiff, resulting in
Frozen Shoulder Syndrome Rehabilitation Using the Resistance Chair General Information Frozen shoulder is a condition where the shoulder joint (glenohumeral joint) gradually becomes stiff, resulting in
APPROPRIATE USE GUIDELINES
 APPROPRIATE USE GUIDELINES Appropriateness of Advanced Imaging Procedures (MRI, CT, Bone Scan/PET) in Patients with Shoulder Pain CDI QUALITY INSTITUTE: PROVIDER LED ENTITY (PLE) Compiled by Rob Liddell,
APPROPRIATE USE GUIDELINES Appropriateness of Advanced Imaging Procedures (MRI, CT, Bone Scan/PET) in Patients with Shoulder Pain CDI QUALITY INSTITUTE: PROVIDER LED ENTITY (PLE) Compiled by Rob Liddell,
Breakout Session #7: Manual therapy for shoulder pain and limited mobility
 Northwestern University Feinberg School of Medicine Breakout Session #7: Manual therapy for shoulder pain and limited mobility @Amee_S Objectives 1. Demonstrate the examination procedures and describe
Northwestern University Feinberg School of Medicine Breakout Session #7: Manual therapy for shoulder pain and limited mobility @Amee_S Objectives 1. Demonstrate the examination procedures and describe
FUNCTIONAL ANATOMY OF SHOULDER JOINT
 FUNCTIONAL ANATOMY OF SHOULDER JOINT ARTICULATION Articulation is between: The rounded head of the Glenoid cavity humerus and The shallow, pear-shaped glenoid cavity of the scapula. 2 The articular surfaces
FUNCTIONAL ANATOMY OF SHOULDER JOINT ARTICULATION Articulation is between: The rounded head of the Glenoid cavity humerus and The shallow, pear-shaped glenoid cavity of the scapula. 2 The articular surfaces
Title Protocol for the Management of Shoulder Injuries in MIUs and WICs
 Document Control Title in MIUs and WICs Author Author s job title Professional Lead, Minor Injuries Unit Directorate, Logistics and Resilience Department Emergency Department Version Date Issued Status
Document Control Title in MIUs and WICs Author Author s job title Professional Lead, Minor Injuries Unit Directorate, Logistics and Resilience Department Emergency Department Version Date Issued Status
REHABILITATION FOR SHOULDER FRACTURES & SURGERIES. Clavicle fractures Proximal head of humerus fractures
 REHABILITATION FOR SHOULDER FRACTURES & SURGERIES Clavicle fractures Proximal head of humerus fractures By Dr. Mohamed Behiry Lecturer Department of physical therapy for Orthopaedic and its surgery. Delta
REHABILITATION FOR SHOULDER FRACTURES & SURGERIES Clavicle fractures Proximal head of humerus fractures By Dr. Mohamed Behiry Lecturer Department of physical therapy for Orthopaedic and its surgery. Delta
A Patient s Guide to Biceps Rupture. William T. Grant, MD
 A Patient s Guide to Biceps Rupture Dr. Grant is a talented orthopedic surgeon with more than 30 years of experience helping people return to their quality of life. He and GM Pugh, PA-C pride themselves
A Patient s Guide to Biceps Rupture Dr. Grant is a talented orthopedic surgeon with more than 30 years of experience helping people return to their quality of life. He and GM Pugh, PA-C pride themselves
Acromioplasty. Surgical Indications and Considerations
 1 Acromioplasty Surgical Indications and Considerations Anatomical Considerations: Any abnormality that disrupts the intricate relationship within the subacromial space may lead to impingement. Both intrinsic
1 Acromioplasty Surgical Indications and Considerations Anatomical Considerations: Any abnormality that disrupts the intricate relationship within the subacromial space may lead to impingement. Both intrinsic
Shoulder Exam Break-out with Case Highlights. Teri Metcalf McCambridge, MD, FAAP, CAQSM Assistant Professor of Pediatrics and Orthopedics University
 Shoulder Exam Break-out with Case Highlights. Teri Metcalf McCambridge, MD, FAAP, CAQSM Assistant Professor of Pediatrics and Orthopedics University of Maryland School of Medicine Faculty Disclosure Information
Shoulder Exam Break-out with Case Highlights. Teri Metcalf McCambridge, MD, FAAP, CAQSM Assistant Professor of Pediatrics and Orthopedics University of Maryland School of Medicine Faculty Disclosure Information
Rehabilitation of Overhead Shoulder Injuries
 Rehabilitation of Overhead Shoulder Injuries 16 th Annual Primary Care Orthopaedic & Sports Medicine Symposium January 29, 2016 Jeremy Sherman, PT, MPT Disclosures No financial disclosures to note. Jeremy
Rehabilitation of Overhead Shoulder Injuries 16 th Annual Primary Care Orthopaedic & Sports Medicine Symposium January 29, 2016 Jeremy Sherman, PT, MPT Disclosures No financial disclosures to note. Jeremy
Labral Tears. Fig 1: Intact labrum and biceps tendon
 Labral Tears What is it? The shoulder joint is a ball and socket joint, with the humeral head (upper arm bone) as the ball and the glenoid as the socket. The glenoid (socket) is a shallow bone that is
Labral Tears What is it? The shoulder joint is a ball and socket joint, with the humeral head (upper arm bone) as the ball and the glenoid as the socket. The glenoid (socket) is a shallow bone that is
11/15/2017. Biceps Lesions. Highgate Private Hospital (Whittington Health NHS Trust) E: LHB Anatomy.
 E: LHB Anatomy.") Biceps Lesions Mr Omar Haddo (Consultant Orthopaedic Surgeon MBBS, BmedSci, FRCS(Orth) ) Highgate Private Hospital (Whittington Health NHS Trust) E: admin@denovomedic.co.uk LHB Anatomy Arise from superior
Biceps Lesions Mr Omar Haddo (Consultant Orthopaedic Surgeon MBBS, BmedSci, FRCS(Orth) ) Highgate Private Hospital (Whittington Health NHS Trust) E: admin@denovomedic.co.uk LHB Anatomy Arise from superior
Management of Shoulder Pain in Persons with SCI
 www.fisiokinesiterapia.biz Management of Shoulder Pain in Persons with SCI Research Program Development from a Clinical Perspective Identification of the problem Identification of potential cause Development
www.fisiokinesiterapia.biz Management of Shoulder Pain in Persons with SCI Research Program Development from a Clinical Perspective Identification of the problem Identification of potential cause Development
Work-related shoulder pain
 Work-related shoulder pain Stadler Kirsten M.B., Ch.B. (1987) (Pret), M. Med. (Orthop) (1998) (Stell.), Orthopaedic Surgeon, Room 333, Louis Leipoldt Medical Centre, Broadway Street, Bellville Cape Town
Work-related shoulder pain Stadler Kirsten M.B., Ch.B. (1987) (Pret), M. Med. (Orthop) (1998) (Stell.), Orthopaedic Surgeon, Room 333, Louis Leipoldt Medical Centre, Broadway Street, Bellville Cape Town
Vol 3, 2008 CEC ARTICLE: Special Medical Conditions Part 2: Shoulder Maintenance and Rehab C. Eggers
 Vol 3, 2008 CEC ARTICLE: Special Medical Conditions Part 2: Shoulder Maintenance and Rehab C. Eggers SHOULDER GIRDLE STABILIZATION Knowledge of the anatomy and biomechanics of the shoulder girdle is essential
Vol 3, 2008 CEC ARTICLE: Special Medical Conditions Part 2: Shoulder Maintenance and Rehab C. Eggers SHOULDER GIRDLE STABILIZATION Knowledge of the anatomy and biomechanics of the shoulder girdle is essential
Upper limb injuries II. Traumatology RHS 231 Dr. Einas Al-Eisa
 Upper limb injuries II Traumatology RHS 231 Dr. Einas Al-Eisa Capsulitis = inflammatory lesion of the glenohumeral joint capsule leading to: thickening and loss of joint volume painful stiffness of the
Upper limb injuries II Traumatology RHS 231 Dr. Einas Al-Eisa Capsulitis = inflammatory lesion of the glenohumeral joint capsule leading to: thickening and loss of joint volume painful stiffness of the
SHOULDER PROBLEMS & ARTHROSCOPIC MANAGEMENT
 SHOULDER PROBLEMS & ARTHROSCOPIC MANAGEMENT DR.SHEKHAR SRIVASTAV Sr. Consultant-KNEE & SHOULDER Arthroscopy Sant Parmanand Hospital,Delhi Peculiarities of Shoulder Elegant piece of machinery It has the
SHOULDER PROBLEMS & ARTHROSCOPIC MANAGEMENT DR.SHEKHAR SRIVASTAV Sr. Consultant-KNEE & SHOULDER Arthroscopy Sant Parmanand Hospital,Delhi Peculiarities of Shoulder Elegant piece of machinery It has the
A Patient s Guide to Cuff (Rotator) Tear Arthropathy
 Tear Arthropathy") A Patient s Guide to Cuff (Rotator) Tear Arthropathy 20295 NE 29th Place, Ste 300 Aventura, FL 33180 Phone: (786) 629-0910 Fax: (786) 629-0920 admin@instituteofsports.com DISCLAIMER: The information in
A Patient s Guide to Cuff (Rotator) Tear Arthropathy 20295 NE 29th Place, Ste 300 Aventura, FL 33180 Phone: (786) 629-0910 Fax: (786) 629-0920 admin@instituteofsports.com DISCLAIMER: The information in
Gross Anatomy Questions That Should be Answerable After October 27, 2017
 Gross Anatomy Questions That Should be Answerable After October 27, 2017 1. The inferior angle of the scapula of a woman who was recently in an automobile accident seems to protrude making a ridge beneath
Gross Anatomy Questions That Should be Answerable After October 27, 2017 1. The inferior angle of the scapula of a woman who was recently in an automobile accident seems to protrude making a ridge beneath
Tendinosis & Subacromial Impingement Syndrome. Gene Desepoli, LMT, D.C.
 Tendinosis & Subacromial Impingement Syndrome Gene Desepoli, LMT, D.C. What is the shoulder joint? Shoulder joint or shoulder region? There is an interrelatedness of all moving parts of the shoulder and
Tendinosis & Subacromial Impingement Syndrome Gene Desepoli, LMT, D.C. What is the shoulder joint? Shoulder joint or shoulder region? There is an interrelatedness of all moving parts of the shoulder and
Mr. Siva Chandrasekaran Orthopaedic Surgeon MBBS MSpMed MPhil (surg) FRACS. Rotator Cuff Tears
 FRACS. Rotator Cuff Tears") Rotator Cuff Tears A rotator cuff tear is a common cause of pain and disability among adults. A torn rotator cuff will weaken your shoulder. This means that many daily activities, like combing your hair
Rotator Cuff Tears A rotator cuff tear is a common cause of pain and disability among adults. A torn rotator cuff will weaken your shoulder. This means that many daily activities, like combing your hair
Anatomy Your shoulder is made up of three bones: your upper arm bone (humerus), your shoulder blade (scapula), and your collarbone (clavicle).
, your shoulder blade (scapula), and your collarbone (clavicle).") Shoulder Impingement/Rotator Cuff Tendinitis One of the most common physical complaints is shoulder pain. Your shoulder is made up of several joints combined with tendons and muscles that allow a great
Shoulder Impingement/Rotator Cuff Tendinitis One of the most common physical complaints is shoulder pain. Your shoulder is made up of several joints combined with tendons and muscles that allow a great
Cervical Radiculopathy: My 32 Year-Old Cyclist is Nervous What do I do on the initial visit?
 Cervical Radiculopathy: My 32 Year-Old Cyclist is Nervous What do I do on the initial visit? Scott D Boden, MD The Emory Spine Center Atlanta, Georgia History of Trauma? 2 History of Trauma? 3 Sometimes
Cervical Radiculopathy: My 32 Year-Old Cyclist is Nervous What do I do on the initial visit? Scott D Boden, MD The Emory Spine Center Atlanta, Georgia History of Trauma? 2 History of Trauma? 3 Sometimes
Anterior Stabilization of the Shoulder: Distal Tibial Allograft
 Anterior Stabilization of the Shoulder: Distal Tibial Allograft Name: Diagnosis: Date: Date of Surgery: Phase I Immediate Post Surgical Phase (approximately Weeks 1-3) Minimize shoulder pain and inflammatory
Anterior Stabilization of the Shoulder: Distal Tibial Allograft Name: Diagnosis: Date: Date of Surgery: Phase I Immediate Post Surgical Phase (approximately Weeks 1-3) Minimize shoulder pain and inflammatory