Bread and Butter Bone Pathology
|
|
|
- Wilfrid Holmes
- 6 years ago
- Views:
Transcription
1 Bread and Butter Bone Pathology NICOLE D. RIDDLE, MD RUFFOLO, HOOPER, AND ASSOC. / UNIVERSITY OF SOUTH FLORIDA Goals: Fundamentals of neoplastic bone pathology Bone Producing Cartilage Producing Miscellaneous Essential features of bone tumor imaging Importance to recognize one s diagnostic limitations Bone Tumors Are rare Pathologist may not accumulate enough experience Surgeons may not have specialized training Improper excisions Unfamiliarity with terminology Ignorance about the role of molecular studies 1

2 Bone Tumors cont Oncologists may not be familiar with clinical protocols and trials Radiologists may not be familiar with neoplastic bone radiology Initial biopsy is often very small Communication between surgeon and pathologist is key If in doubt.. SEND IT OUT! Clinical presentation: Age Symptoms Radiologic information: Size Bone Pattern Periosteal Reaction Location 2










3 Age Distribution Age group Most Common Benign Most Common Malignant 0-10 Simple bone cyst Ewingʼs sarcoma Leukemia Age Distribution Age group Most Common Benign Most Common Malignant Non-ossifying fibroma Osteosarcoma Simple bone cyst Ewingʼs sarcoma Aneurysmal bone cyst Adamantinoma Osteochondroma Osteoid osteoma Age Distribution Age Group Most Common Benign Most Common Malignant Enchondroma Chondrosarcoma Giant cell tumor Metastatic Tumors 3

 Chordoma CENTRAL Simple")



4 Age Distribution Age Group Most Common Benign Most Common Malignant 40 and above Osteoma Metastatic tumors Enchondroma Myeloma Chondrosarcoma Osteosarcoma (Paget's ) Chordoma CENTRAL Simple Bone Cyst Enchondroma Fibrous Dysplasia ECCENTRIC Giant Cell Tumor Fibrous Cortical Defect Aneurismal Bone Cyst Chondromyxofibroma Osteoma BENIGN Narrow zone Transition Solid Periosteal Reaction Geographic Bone Destruction MALIGNANT Broken Periosteal Reaction Permative Bone Destruction Soft Tissue Mass Wide Zone Transition 4



5 Grade I Grade II Grade III IA IB IIA IIB IIIA IIIB IIIC Geographic With Sclerosis Geographic No Sclerosis Geographic Wide Zone Transition Changing Margin Moth Eaton Permeative Invisible 5
6 BONE FORMING TUMORS OSTEOID OSTEOMA OSTEOBLASTOMA OSTEOSARCOMA OSTEOID OSTEOMA Benign bone-forming tumor of limited growth potential that elicits a prominent reaction on adjacent bone Any age - 75% < 25; average : 19; rare >30 Male : Female = 2.2 : 1 Dull, progressive pain, worse at night, relieved by salicylates (70%) - nerve fibers, prostaglandin E2, prostacyclin PGI2 Pain may precede radiographic manifestations and may be referred to adjacent joints or bones 5%, painless (typically in the fingers) OSTEOID OSTEOMA Long bones, typically cortical Metaphysis and diaphysis - rarely epiphyseal Proximal femur > 50% (neck, inter-trochanteric), tibia Hand: Proximal and distal phalanges Foot: Metatarsal bones and calcaneus Very rare multicentricity Rarely intra-articular 10% in vertebrae: neural arc (scoliosis) 6



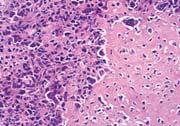
7 OSTEOID OSTEOMA Small, oval, cortical radio-lucency with variable mineralization Sclerosis and cortical reaction Nidus at the center 25% not evident on plain radiography CT ideal for diagnosis and surgical planning OSTEOID OSTEOMA Nidus Hemorrhage around the nidus Reactive sclerosis around the nidus OSTEOID OSTEOMA Round, oval, red, haphazardly arranged, trabeculated osteoid with variable mineralization (greatest at the center) in a background of fibrovascular tissue with occasional giant cells and surrounded by sclerosis that disappears when the nidus is removed NIDUS 7
 Long bones: 38% (75% in diaphysis) Predilection for posterior vertebral column (65% purely dorsal) 43% in spine and sacrum scoliosis More than 2 cm: Osteoblastoma")
 Central nidus rarely seen In 20%, cortical destruction (confused with malignancy) Vertebrae Margin well defined (in 50%,")
8 OSTEOID OSTEOMA Woven bone Variable mineralization OSTEOBLASTOMA Benign bone-forming tumor similar to osteoid osteoma with potential for progressive growth (giant osteoid osteoma) M:F = 2:1 80% in first three decades (average: 20) Long bones: 38% (75% in diaphysis) Predilection for posterior vertebral column (65% purely dorsal) 43% in spine and sacrum scoliosis More than 2 cm: Osteoblastoma Less than 1 cm: Osteoid osteoma Between 1 and 2 cm: Indistinguishable OSTEOBLASTOMA Intense nocturnal pain is uncommon Neurological complaints in vertebral tumors Appendicular skeleton Lucent with variable ossification Well defined, sclerotic margins (50% of cases) Central nidus rarely seen In 20%, cortical destruction (confused with malignancy) Vertebrae Margin well defined (in 50%, sclerosis) In 15% malignancy is considered 8
 Soft tissue")



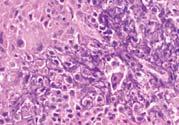
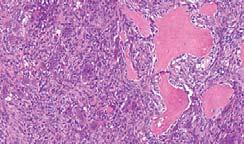
9 OSTEOBLASTOMA Unlimited growth potential (2-12 cm) Soft tissue extension often with a calcified periosteal shell It frequently lacks the halo of osteoid osteoma Confused with giant cell tumor or sarcoma Some stop growing or even regress Aggressive destruction by secondary ABC (10%) OSTEOBLASTOMA OSTEOBLASTOMA 9







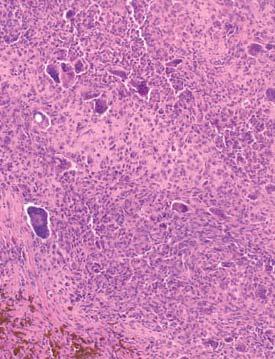
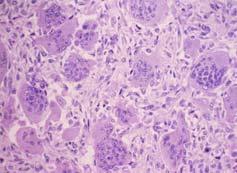
10 OSTEOBLASTOMA OSTEOBLASTOMA Osteoblastic rimming Mineralized trabeculae Lace-like osteoid Cartilaginous differentiation OSTEOSARCOMA Malignant tumor in which bone or osteoid are directly produced by tumor cells 35% of all sarcomas - second to myeloma Males: 58% - Females: 42% 80% in metaphysis of long bones most common, distal femur 46% in second decade - most between 15 and 25 Secondary to Paget s disease (older patients) or radiation therapy Pain may be intermittent, sometimes nocturnal, for weeks to months Swelling and pathologic fracture 10
 10% MFH-like Telangiectatic (ABC-like) Small-cell Epithelioid MEDULLARY LOW-GRADE Fibrous Dysplasia-like NOF-like CMF-like Chondroblastoma-like OSTEOSARCOMA Lytic, blastic or")
11 OSTEOSARCOMA MEDULLARY CORTICAL SURFACE Parosteal Periosteal High Grade OSTEOSARCOMA MEDULLARY HIGH GRADE Osteogenic (osteoblastic, bone-rich) - 50% Chondroblastic (cartilage-rich) - 25% Fibroblastic (spindle cell-rich) 10% MFH-like Telangiectatic (ABC-like) Small-cell Epithelioid MEDULLARY LOW-GRADE Fibrous Dysplasia-like NOF-like CMF-like Chondroblastoma-like OSTEOSARCOMA Lytic, blastic or mixed (10%) Geographic, poorly demarcated Periosteal new bone formation (spiculation, cummulus cloud, Codman s triangle) Cortex erosion and soft tissue extension Variable mineralization on X-rays 11





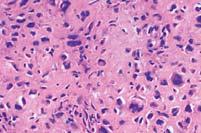
12 OSTEOSARCOMA Codman s angle Spiculated, hair-on-end, mineralization OSTEOSARCOMA Cortex destruction Epiphyseal plate invasion Bone marrow spread (skip areas in 25% of cases) Frozen section of marrow margins: avoid Codman s triangle (non-neoplastic) Variable appearance: Soft, fleshy to firm, fibrous tumor with irregular ossification and various amounts of chondroid material and sclerosis OSTEOSARCOMA Anaplasia + Osteoid = Osteosarcoma 12





13 OSTEOSARCOMA OSTEOSARCOMA Invasion of Skeletal Muscle Necrosis Cortex Invasion Osteoid SURFACE OSTEOSARCOMA MEDULLARY CORTICAL SURFACE Parosteal Periosteal High Grade 13

 80% occur in posterior aspect of distal femur Inability to bend the")
 Large tumors may encircle the bone Dedifferentiation to HGS in 15% Intact cortex")
14 PAROSTEAL OSTEOSARCOMA Well differentiated OS that arises on the bone surface and appears as a heavily mineralized mass Usually low grade Long duration Males 30%; Females 70% 80% between years (a decade older than conventional OS) Pain rare PAROSTEAL OSTEOSARCOMA Usually low grade, Long duration, Pain rare M 30%; F 70% String sign 80% trs (decade older than conv) 80% occur in posterior aspect of distal femur Inability to bend the knee Lobulated, densely mineralized: pasted on Broad attachment to intact, thickened cortex Intramedullary extension in 20% (CT, MRI) Large tumors may encircle the bone Dedifferentiation to HGS in 15% Intact cortex PAROSTEAL OSTEOSARCOMA 14



 PERIOSTEAL OSTEOSARCOMA Moderately")


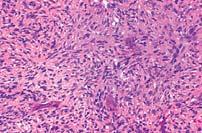
15 PAROSTEAL OSTEOSARCOMA Periosteal expansion WD Osteosarcoma Osteoid formation Chondroblastic component Cortex invasion Fibrosarcoma like component PAROSTEAL OSTEOSARCOMA Hypocellular fibroblastic stroma with no bone marrow Trabeculae parallel to each other Minimal atypia - Rare mitoses Cartilage at the surface may resemble osteochondroma (chondrocytes are mildly atypical and they are not arranged in columns) PERIOSTEAL OSTEOSARCOMA Moderately differentiated, predominantly chondroblastic surface OS with no medullary involvement M 55%; F 45% 85% around the knee Pain and swelling Symptoms for up to 24 months High grade osteosarcoma Diaphyseal saucer Codman s triangle common No intramedullary involvement Adjacent cortex is thickened 15


 Mild atypia in")





16 PERIOSTEAL OSTEOSARCOMA PERIOSTEAL OSTEOSARCOMA Abundant chondroid matrix with spicules of osteoid Spindle cells at the periphery (fine lacelike osteoid) Mild atypia in chondrocytes and spindle cells No intramedullary involvement HIGH GRADE SURFACE OSTEOSARCOMA M 78%; F 22% Warm, painful, erythema Most common in the femur Cortical destruction Periosteal new bone formation None or minimal intramedullary involvement Often chondroid matrix 16

 40% about the")

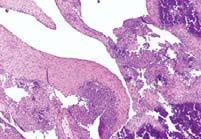
17 HIGH GRADE SURFACE OSTEOSARCOMA CARTILAGE-FORMING TUMORS OSTEOCHONDROMA CHONDROBLASTOMA CHONDROMYXOID FIBROMA ENCHONDROMA PERIOSTEAL CHONDROMA MULTIPLE CHONDROMATA CHONDROSARCOMA OSTEOCHONDROMA Common (second to NOF) Pedunculated or sessile Metaphysis of long bones (limbs) 40% about the knee (lower femur, upper tibia, upper humerus) 1-2 % malignant transformation Corticomedullary continuity Metaphyseal based Growth points away from joint 17




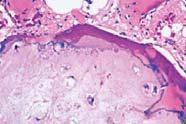
18 OSTEOCHONDROMA OSTEOCHONDROMA Cartilaginous cap Bone marrow inside the tumor Cortex of the bone in continutiy with the cortex of the osteochondroma Broadening of bone OSTEOCHONDROMA The cap resembles endochondral ossification Cancellous bone underlies the cap Chondrocytes in cap are relatively normal 18



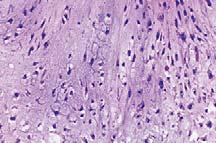
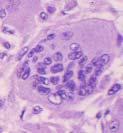
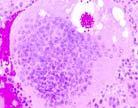
19 CHONDROBLASTOMA Almost always benign - Rarely, non-progressive lung mets M 59% - F 41% 60-70% in 2nd decade 95% < 25 years Epiphyseal, all bones 30% around the knee Lobulated and sharply demarcated 95% chondroid differentiation Ossification rare Secondary ABC in 1/3 CHONDROBLASTOMA Chondroblasts Giant cell CHONDROBLASTOMA Lace-like calcification between degenerated cells in 1/3 of tumors Chicken wire 19
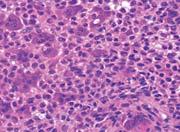
20 CHONDROBLASTOMA Giant cells Moderate Atypia Hemosiderin ABC-like CHONDROBLASTOMA CHONDROMYXOID FIBROMA M 62%; F 38% Metaphysis of long bones It rarely involves the epiphysis 2/3 in long tubular bones - 1/3 in the tibia 20










21 CHONDROMYXOID FIBROMA CHONDROMYXOID FIBROMA Nodules of spindle/stellate cells in myxoid or chondroid stroma containing giant cells Well demarcated by either bone or connective tissue Small amount of fibrous tissue as narrow septa CHONDROMYXOID FIBROMA Hyaline cartilage is rare Mitoses are rare In 1/3 of cases, bizarre nuclei 10% necrosis 21





22 CHONDROMYXOID FIBROMA ENCHONDROMA Intramedullary neoplasm of mature hyaline cartilage Males 48%; Females 52% 55% in 2 nd to 4 th decades Bone cortex uninvolved Bone entrapment should not occur - No permeation Chondrocytes in lacunae with small, round regular nucleus in a bluish matrix Binucleation possible but rarely several cells in lacunae Even mineralization Histology depends on location: In the sternum, likely CHS In small bones, atypia is allowed ENCHONDROMA 22





23 ENCHONDROMA ENCHONDROMA LOBULARITY MILD ATYPIA ENCHONDROMA BENIGN OSSIFICATION Enchondral ossification: pop-corn; arcs and rings 23



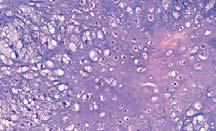
24 ENCHONDROMA Pop-corn calcification ENCHONDROMA Confluent semitranslucent lobular masses of hyaline cartilage, rimmed by fibrous tissue or bone ENCHONDROMA Slightly more atypia allowed in small bones 24
")


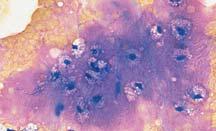
25 CHONDROSARCOMA CHONDROSARCOMA M 60%; F 40% 65% 4 th to 6 th decades 2/3 in the trunk and upper extremities Pelvis (30%) Proximal femur (20%) Benign Expansile lesions displacing bone Hypocellular Solid chondroid matrix Malignant Permeation entrapping bony trabeculae Soft tissue extension Myxoid change Atypia, binucleation CHONDROSARCOMA Grade 2 Scallop Cortical Breakage 25







26 CHONDROSARCOMA CHONDROSARCOMA Metaphyseal, diaphyseal Scalloped cortex Bone expansion Cortical breakthrough Soft tissue extension Punctate, flocculant popcorn mineralization CHONDROSARCOMA SCALLOPING ATYPIA BONE INVASION CELL DEATH 26
 Rare mitoses Rare sheets of spindle cells Tendency to higher grade with")
, rare mitoses, large vesicular or hyperchromatic nuclei, often more than one cell per")

27 CHONDROSARCOMA BONE INVASION CHONDROSARCOMA Necrotic foci often calcify and form osseous masses Small bones of hand and feet affected in syndromes (Ollier s, Mafucci s) Rare mitoses Rare sheets of spindle cells Tendency to higher grade with recurrence CHONDROSARCOMA Grade 1: small nuclei (>8 micron), binucleation, chondroid matrix, rare myxoid areas Grade 2: less matrix (more cellular), rare mitoses, large vesicular or hyperchromatic nuclei, often more than one cell per lacuna, necrosis, myxoid stroma Grade 3: greater cellularity and nuclear pleomorphism, absent chondroid matrix and prominent myxoid matrix, chondrocyte cords with grotesque shape, extensive necrosis, vesicular nuclei 5-10 times larger than normal 27



28 CHONDROSARCOMA GRADE 1 GRADE 2 GRADE 3 DEDIFFERENTIATED CHONDROSARCOMA 12% of chondrosarcomas Large and aggressive Calcification in 50% Extraosseous mass in 55% DEDIFFERENTIATED CHONDROSARCOMA 28

 Fallen")
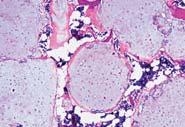
29 MISCELLANEOUS TUMORS OF BONE First two decades of life M:F = 3:1 Children: proximal humerus (62%), proximal femur (27%) Adults: calcaneus, ilium Solitary, intramedullary 30% proximal humerus 17% femur 11% proximal tibia Typically unilocular SIMPLE BONE CYST SIMPLE BONE CYST Bone protuberance with thin periosteal covering Thin cyst wall with few giant cells 10% cementum-like calcospherites (Liesegang s phenomenon) Prior fracture/hemorrhage with fibro-osseous repair (exuberant fibroblasts, osteoid, woven bone, hemosiderin, lymphocytes, cholesterol clefts) Fallen leaf sign 29

 ANEURYSMAL BONE CYST")
 ANEURYSMAL BONE CYST")
 Bony trabeculae with prominent")
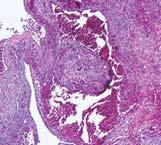
30 ANEURYSMAL BONE CYST Benign lesion with cyst-like walls Up to 50% are secondary to other lesions Fibrous dysplasia GCT Chondroblastoma Osteosarcoma Short duration, pain, swelling Slight female predominance Any bone ; Knee most common Metaphysis of long bones / Vertebrae (posterior, multiple in 50% of cases) ANEURYSMAL BONE CYST 85% < 20 years Long bones (53%), spine (15%) 85% with swelling +/- pain 20% with pathologic fracture Scoliosis or kyphosis (10% of spine cases) ANEURYSMAL BONE CYST Blood-filled spaces separated by septa with giant cells and osteoid Solid areas with spindle cells (prominent in the solid variant) Bony trabeculae with prominent osteoblasticrimming 30

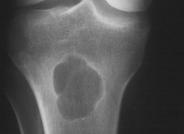
31 SOLID ABC It lacks blood-filled spaces and cyst walls Blowout" evident on x-ray Exuberant spindle cell component Osteoid +/- woven bone; lacy chondroid Maturational areas Osteoclast-like giant cells METAPHYSEAL FIBROUS DEFECT Spindle cell proliferation that involves the cortex, or both the cortex and the medullary cavity, in the metaphysis of long bones of children. It tends to resolve spontaneously Explanation of terms: If only cortex is involved: Fibrous Cortical Defect If both cortex and medulla are involved: Non-Ossifying FIbroma Abundant xanthomatous cells: Fibroxanthoma Similar histology (adults) may be seen in Benign Fibrous Histiocytoma and GCT METAPHYSEAL FIBROUS DEFECT Clinical features First two decades Asymptomatic 30-40% of all children Imaging Metaphyseal, eccentric Soap bubble appearance 31
 M:F = 1:1.")





32 METAPHYSEAL FIBROUS DEFECT 80% between 20 and 50 y of age (98% after physeal closure) M:F = 1:1.3 Solitary, meta-epiphyseal 55% around the knee; 10% in distal radius, Vertebral body involvement (anterior) Elevated alkaline phosphatase Normal serum Ca ++ and PO = 4 2% metastasize GIANT CELL TUMOR Malignancy very rare Anaplastic transformation True malignant: < 6 m survival Epiphyseal, metaepiphyseal Intramedullary, eccentric Geographic destruction No host bone sclerosis GIANT CELL TUMOR Lack of ominous periosteal reaction Cortical erosion - A soft tissue mass may be present 32




33 GIANT CELL TUMOR GIANT CELL TUMOR Syncytial fusion of mononuclear cells into a giant cell GIANT CELL TUMOR More Spindly Foamy Histiocytes Bone Formation ABC Changes 33

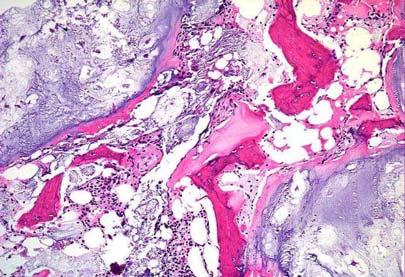
34 GIANT CELL TUMOR FIBROUS DYSPLASIA Benign fibro-osseous proliferation Monostotic 6 times more common than polyostotic Clinical features: 70 % present with pain / limp Pathologic fracture Deformity shepherds crook Fracture McCune-Albright Syndrome Triad: Multifocal FD Café au lait spots coast of maine Precious puberty Endocrine abnormalities 2x malignant transformation risk Metaphyseal or diaphyseal Ground glass X-ray Cortical expansion, Scalloping Sclerotic, well defined margins Very hot on bone scan FIBROUS DYSPLASIA 34
")







35 FIBROUS DYSPLASIA FIBROUS DYSPLASIA No (Minimal) Osteoblastic Rimming Foamy Histiocytes Paucicellular Fibrous Areas Benign Cartilage OSTEOFIBROUS DYSPLASIA Middle third of tibia 2/3 below age 5 Pain uncommon Intracortical, lytic, eccentric Anterior bowing Histology similar to FD, but PROMINENT osteoblastic rimming 35


36 OSTEOFIBROUS DYSPLASIA Hopefully: Fundamentals of neoplastic bone pathology Bone Producing Cartilage Producing Miscellaneous Essential features of bone tumor imaging Importance to recognize one s diagnostic limitations Thank you Credit to Drs. Carlos Muro-Cacho and Douglas Letson for many of these images 36






37 Additional Material CHONDROBLASTIC OSTEOSARCOMA Bone production among chondroblastic areas, atypia, necrosis FIBROBLASTIC OSTEOSARCOMA Prominent fibrous component with focal osteoid 37







38 GIANT CELL OSTEOSARCOMA Prominent giant cell component malignant osteoid production SMALL CELL OSTEOSARCOMA Males 88% - Females 12% Pain in 2/3 of cases Swelling in 15% Symptoms: days to years Neurologic deficit if vertebra involved Metaphysis with epiphyseal involvement in 1/3 of cases Purely diaphyseal 15% Soft tissue mass in 60% of cases (25% mineralized) EPITHELIOID OS Epithelioid appearance Signet-ring, plasma cells 38



 Pain common")


39 CHONDROBLASTOMA-LIKE OS Invasion of fat (bone marrow permeation) Coarse pattern of matrix calcification LOW-GRADE INTRAOSSEOUS OS M/F : 50/50 No specific signs (no swelling) Pain common Medullary extension to the end of the bone Trabeculated or sclerotic Periosteal new bone formation Soft tissue extension LOW-GRADE INTRAOSSEOUS OS 39








40 TELANGIECTATIC OS 3.5% of osteosarcomas Males: 66% - Females 34% Tender mass - often fracture Large, metaphyseal Lytic, poorly marginated Prominent medullary and cortical destruction Periosteal new bone formation common TELANGIECTATIC OS TELANGIECTATIC OS Spaces and septa like ABC Cells lining septa malignant Benign giant cells present Minimal osteoid 40




41 JAWBONES OS 6% of Osteosarcomas Young adults 50% Chondroblastic Peripheral spindle cells Central, poorly formed trabeculae PERIOSTEAL CHONDROMA 75% in second-third decades M:F = 2:1 Local swelling, Pain of long duration Appendicular skeleton 2/3 metaphysis and the remainder diaphysis PERIOSTEAL CHONDROMA Eccentric cortical lucent lesion Reactive periosteal bone Calcification Medulla uninvolved 41




")
42 PERIOSTEAL CHONDROMA Lobules of mature hyaline cartilage embedded under periosteum CLEAR CELL CHONDROSARCOMA M 70%; F 30% Third and fourth decades End of bones, extending to articular cartilage Lobulated growth pattern, capillary proliferation Slow-growing CLEAR CELL CHONDROSARCOMA Well-defined cellular borders Vesicular nucleus Prominent nucleoli Clear cytoplasm (glycogen) Difficult to be recognized as cartilaginous 42







43 CLEAR CELL CHONDROSARCOMA ADAMANTINOMA Low-grade malignancy with epithelial islands of unknown origin 50-75% in second and third decades 90% involved the tibia (diaphysis) Synchronous lesions in tibia and fibula Central to eccentric, elongated Well circumscribed Honeycomb Soft tissue mass possible ADAMANTINOMA 43







44 ADAMANTINOMA Bland nuclei with minimal or no atypia Mitoses from absent to 10/10 HPF Four histologic patterns: Spindle: Fibrosarcoa-like (spindle lesion in tibial cortex = adamantinoma; metastatic lesions to the tibia are uncommon) Basaloid: Basal-like cells palisading around stellate stroma Tubular Squamoid Oosteofibrous dyslasia-like Ewing sarcoma-like IHC - Strong positivity for pancytokeratin ADAMANTINOMA 44
Bone Tumors Clues and Cues
 William Herring, M.D. 2002 Bone Tumors Clues and Cues In Slide Show mode, advance the slides by pressing the spacebar All Photos Retain the Copyright of their Authors Clues by Appearance of Lesion Patterns
William Herring, M.D. 2002 Bone Tumors Clues and Cues In Slide Show mode, advance the slides by pressing the spacebar All Photos Retain the Copyright of their Authors Clues by Appearance of Lesion Patterns
Bone and Joint Part 2. Leslie G Dodd, MD
 Bone and Joint Part 2 Leslie G Dodd, MD Relative rates of cancer Sarcomas are relatively uncommon tumors New cancer cases 2007 All sites 1.4 million prostate 218,890 lung 213,380 breast 180,510 Soft tissue
Bone and Joint Part 2 Leslie G Dodd, MD Relative rates of cancer Sarcomas are relatively uncommon tumors New cancer cases 2007 All sites 1.4 million prostate 218,890 lung 213,380 breast 180,510 Soft tissue
MARK D. MURPHEY MD, FACR. Physician-in-Chief, AIRP. Chief, Musculoskeletal Imaging
 ALPHABET SOUP AND CYSTIC LESIONS OF THE BONE MARK D. MURPHEY MD, FACR Physician-in-Chief, AIRP Chief, Musculoskeletal Imaging ALPHABET SOUP AND CYSTIC LESIONS OF THE BONE Giant cell tumor (GCT) Unicameral
ALPHABET SOUP AND CYSTIC LESIONS OF THE BONE MARK D. MURPHEY MD, FACR Physician-in-Chief, AIRP Chief, Musculoskeletal Imaging ALPHABET SOUP AND CYSTIC LESIONS OF THE BONE Giant cell tumor (GCT) Unicameral
Primary bone tumors > metastases from other sites Primary bone tumors widely range -from benign to malignant. Classified according to the normal cell
 Primary bone tumors > metastases from other sites Primary bone tumors widely range -from benign to malignant. Classified according to the normal cell counterpart and line of differentiation. Among the
Primary bone tumors > metastases from other sites Primary bone tumors widely range -from benign to malignant. Classified according to the normal cell counterpart and line of differentiation. Among the
The Radiology Assistant : Bone tumor - well-defined osteolytic tumors and tumor-like lesions
 Bone tumor - well-defined osteolytic tumors and tumor-like lesions Henk Jan van der Woude and Robin Smithuis Radiology department of the Onze Lieve Vrouwe Gasthuis, Amsterdam and the Rijnland hospital,
Bone tumor - well-defined osteolytic tumors and tumor-like lesions Henk Jan van der Woude and Robin Smithuis Radiology department of the Onze Lieve Vrouwe Gasthuis, Amsterdam and the Rijnland hospital,
APMA 2018 Radiology Track Bone Tumors When to say Gulp!
 APMA 2018 Radiology Track Bone Tumors When to say Gulp! DANIEL P. EVANS, DPM, FACFAOM Professor, Department of Podiatric Medicine and Radiology Dr. Wm. Scholl College of Podiatric Medicine Conflict of
APMA 2018 Radiology Track Bone Tumors When to say Gulp! DANIEL P. EVANS, DPM, FACFAOM Professor, Department of Podiatric Medicine and Radiology Dr. Wm. Scholl College of Podiatric Medicine Conflict of
Bone Tumours - a synopsis. Dr Zena Slim SpR in Histopathology QAH 2009
 Bone Tumours - a synopsis Dr Zena Slim SpR in Histopathology QAH 2009 Aims General approach to diagnosis Common entities.and not so common ones. Mini quiz Challenge of bone tumour diagnosis Bone tumours
Bone Tumours - a synopsis Dr Zena Slim SpR in Histopathology QAH 2009 Aims General approach to diagnosis Common entities.and not so common ones. Mini quiz Challenge of bone tumour diagnosis Bone tumours
Typical skeletal location and differential diagnosis of bone tumors.
 Typical skeletal location and differential diagnosis of bone tumors. Poster No.: C-2418 Congress: ECR 2015 Type: Educational Exhibit Authors: M. Barros, L. A. Ferreira, Y. Costa, P. J. V. Coelho, F. Caseiro
Typical skeletal location and differential diagnosis of bone tumors. Poster No.: C-2418 Congress: ECR 2015 Type: Educational Exhibit Authors: M. Barros, L. A. Ferreira, Y. Costa, P. J. V. Coelho, F. Caseiro
The Radiology Assistant : Bone tumor - ill defined osteolytic tumors and tumor-like lesions
 Bone tumor - ill defined osteolytic tumors and tumor-like lesions Henk Jan van der Woude and Robin Smithuis Radiology department of the Onze Lieve Vrouwe Gasthuis, Amsterdam and the Rijnland hospital,
Bone tumor - ill defined osteolytic tumors and tumor-like lesions Henk Jan van der Woude and Robin Smithuis Radiology department of the Onze Lieve Vrouwe Gasthuis, Amsterdam and the Rijnland hospital,
Introduction to Musculoskeletal Tumors. James C. Wittig, MD Orthopedic Oncologist Sarcoma Surgeon
 Introduction to Musculoskeletal Tumors James C. Wittig, MD Orthopedic Oncologist Sarcoma Surgeon www.tumorsurgery.org Definitions Primary Bone / Soft tissue tumors Mesenchymally derived tumors (Mesodermal)
Introduction to Musculoskeletal Tumors James C. Wittig, MD Orthopedic Oncologist Sarcoma Surgeon www.tumorsurgery.org Definitions Primary Bone / Soft tissue tumors Mesenchymally derived tumors (Mesodermal)
COPYRIGHT 2004 BY THE JOURNAL OF BONE AND JOINT SURGERY, INCORPORATED
 84 COPYRIGHT 2004 BY THE JOURNAL BONE AND JOINT SURGERY, INCORPORATED Radiographic Evaluation of Pathological Bone Lesions: Current Spectrum of Disease and Approach to Diagnosis BY BENJAMIN G. DOMB, MD,
84 COPYRIGHT 2004 BY THE JOURNAL BONE AND JOINT SURGERY, INCORPORATED Radiographic Evaluation of Pathological Bone Lesions: Current Spectrum of Disease and Approach to Diagnosis BY BENJAMIN G. DOMB, MD,
Disclosures. Giant Cell Rich Tumors of Bone. Outline. The osteoclast. Giant cell rich tumors 5/21/11
 Disclosures Giant Cell Rich Tumors of Bone Andrew Horvai, MD, PhD Associate Clinical Professor, Pathology This lecture discusses "off label" uses of a number of pharmaceutical agents. The speaker is describing
Disclosures Giant Cell Rich Tumors of Bone Andrew Horvai, MD, PhD Associate Clinical Professor, Pathology This lecture discusses "off label" uses of a number of pharmaceutical agents. The speaker is describing
Imaging Findings Of Bone Tumors: A Pictorial Review
 Imaging Findings Of Bone Tumors: A Pictorial Review Poster No.: C-2511 Congress: ECR 2015 Type: Educational Exhibit Authors: M. Limeme, N. Benzina, A. BelKhiria, H. Zaghouani, S. Majdoub, N. Mallat, H.
Imaging Findings Of Bone Tumors: A Pictorial Review Poster No.: C-2511 Congress: ECR 2015 Type: Educational Exhibit Authors: M. Limeme, N. Benzina, A. BelKhiria, H. Zaghouani, S. Majdoub, N. Mallat, H.
Bone/Osteoid Producing Lesions
 Chapter 2 Bone/Osteoid Producing Lesions Introduction There are many lesions that are associated with reactive new bone formation; this chapter predominantly covers those in which deposition of osteoid/bone
Chapter 2 Bone/Osteoid Producing Lesions Introduction There are many lesions that are associated with reactive new bone formation; this chapter predominantly covers those in which deposition of osteoid/bone
USCAP 2014 Common problems in bone and soft tissue pathology: Cartilage tumors
 USCAP 2014 Common problems in bone and soft tissue pathology: Cartilage tumors Andrew Horvai MD PhD Clinical Professor, Pathology UCSF, San Francisco, CA Outline Common intramedullary tumors Enchondroma
USCAP 2014 Common problems in bone and soft tissue pathology: Cartilage tumors Andrew Horvai MD PhD Clinical Professor, Pathology UCSF, San Francisco, CA Outline Common intramedullary tumors Enchondroma
Grading of Bone Tumors
 Grading of Bone Tumors Joon Hyuk Choi, M.D. Department of Pathology College of Medicine, Yeungnam University Introduction to grading system of bone tumor used at Mayo Clinic WHO Histologic Classification
Grading of Bone Tumors Joon Hyuk Choi, M.D. Department of Pathology College of Medicine, Yeungnam University Introduction to grading system of bone tumor used at Mayo Clinic WHO Histologic Classification
Bubbly Lesions of Bone
 Residents Section Pattern of the Month w79 08.18.09 Eisenberg Residents Section Pattern of the Month Residents inradiology Ronald L. Eisenberg 1 Eisenberg RL Keywords: bubbly lesions, fegnomashic, skeletal
Residents Section Pattern of the Month w79 08.18.09 Eisenberg Residents Section Pattern of the Month Residents inradiology Ronald L. Eisenberg 1 Eisenberg RL Keywords: bubbly lesions, fegnomashic, skeletal
Bone tumors. RMG: jan
 Bone tumors RMG: jan 217. @Kijohs KIZZA JOHN KIJOHS Diseases arising in bone Lipoma Fibrous cortical defects Non-ossifying fibroma Bone island Benign simple cysts Enchondroma Osteochondroma Osteoid osteoma
Bone tumors RMG: jan 217. @Kijohs KIZZA JOHN KIJOHS Diseases arising in bone Lipoma Fibrous cortical defects Non-ossifying fibroma Bone island Benign simple cysts Enchondroma Osteochondroma Osteoid osteoma
Fluid-fluid levels in bone tumors: A pictorial review
 Fluid-fluid levels in bone tumors: A pictorial review Poster No.: C-578 Congress: ECR 2009 Type: Educational Exhibit Topic: Musculoskeletal Authors: L. Figueroa Nasra, C. Martín Hervás, M. Tapia-Viñé,
Fluid-fluid levels in bone tumors: A pictorial review Poster No.: C-578 Congress: ECR 2009 Type: Educational Exhibit Topic: Musculoskeletal Authors: L. Figueroa Nasra, C. Martín Hervás, M. Tapia-Viñé,
Primary bone tumors according to the WHO classification: a review of 13 years with illustrative examples
 Primary bone tumors according to the WHO classification: a review of 13 years with illustrative examples Poster No.: C-1741 Congress: ECR 2015 Type: Educational Exhibit Authors: J. Silva, M. A. Ramírez
Primary bone tumors according to the WHO classification: a review of 13 years with illustrative examples Poster No.: C-1741 Congress: ECR 2015 Type: Educational Exhibit Authors: J. Silva, M. A. Ramírez
Malignant bone tumors. Incidence Myeloma 45% Osteosarcoma 24% Chondrosarcoma 12% Lyphoma 8% Ewing s Sarcoma 7%
 Malignant bone tumors Incidence Myeloma 45% Osteosarcoma 24% Chondrosarcoma 12% Lyphoma 8% Ewing s Sarcoma 7% Commonest primary bone sarcoma is osteosarcoma X ray Questions to ask 1. Solitary or Multiple
Malignant bone tumors Incidence Myeloma 45% Osteosarcoma 24% Chondrosarcoma 12% Lyphoma 8% Ewing s Sarcoma 7% Commonest primary bone sarcoma is osteosarcoma X ray Questions to ask 1. Solitary or Multiple
Recognizing Cartilaginous Tumors: Spectrum of Imaging Characteristics with Radiologic-Pathologic correlation.
 Recognizing Cartilaginous Tumors: Spectrum of Imaging Characteristics with Radiologic-Pathologic correlation. Poster No.: C-1451 Congress: ECR 2012 Type: Educational Exhibit Authors: E. Barcina García,
Recognizing Cartilaginous Tumors: Spectrum of Imaging Characteristics with Radiologic-Pathologic correlation. Poster No.: C-1451 Congress: ECR 2012 Type: Educational Exhibit Authors: E. Barcina García,
Fluid fluid levels in bone tumors and tumoral lesions - Pictorial essay
 Review Fluid fluid levels in bone tumors and tumoral lesions - Pictorial essay Subbarao Kakarla 1,* 1 KIMS Foundation and Research Centre, Minister Road, Secunderabad - 500003, Telangana, India Abstract
Review Fluid fluid levels in bone tumors and tumoral lesions - Pictorial essay Subbarao Kakarla 1,* 1 KIMS Foundation and Research Centre, Minister Road, Secunderabad - 500003, Telangana, India Abstract
Radiography in the Initial Diagnosis of Primary Bone Tumors
 Residents Section Structured Review Costelloe and Madewell Radiography of Primary Bone Tumors Residents Section Structured Review Colleen M. Costelloe 1 John E. Madewell Costelloe CM, Madewell JE Keywords:
Residents Section Structured Review Costelloe and Madewell Radiography of Primary Bone Tumors Residents Section Structured Review Colleen M. Costelloe 1 John E. Madewell Costelloe CM, Madewell JE Keywords:
Multifocal fibrous Dysplasia with enchondroma-like areas: Fibrocartilaginous Dysplasia
 ISPUB.COM The Internet Journal of Pathology Volume 7 Number 2 Multifocal fibrous Dysplasia with enchondroma-like areas: Fibrocartilaginous Dysplasia V Monappa, R Kudva Citation V Monappa, R Kudva. Multifocal
ISPUB.COM The Internet Journal of Pathology Volume 7 Number 2 Multifocal fibrous Dysplasia with enchondroma-like areas: Fibrocartilaginous Dysplasia V Monappa, R Kudva Citation V Monappa, R Kudva. Multifocal
Essential Dermatopathology. Jinah Kim, MD, PhD Department of Pathology and Dermatology Stanford University Medical Center
 Essential Dermatopathology Jinah Kim, MD, PhD Department of Pathology and Dermatology Stanford University Medical Center OBJECTIVES Review clinical, pathologic and molecular aspects of bone and fat tumors
Essential Dermatopathology Jinah Kim, MD, PhD Department of Pathology and Dermatology Stanford University Medical Center OBJECTIVES Review clinical, pathologic and molecular aspects of bone and fat tumors
FEGNOMASHIC: from x-ray to MRI
 FEGNOMASHIC: from x-ray to MRI Poster No.: C-2441 Congress: ECR 2015 Type: Educational Exhibit Authors: S. Fouassier, A. L. C. Duarte, C. Ruivo, J. Velez ; Évora/PT, 1 2 1 2 3 1 3 Coimbra/PT, PT Keywords:
FEGNOMASHIC: from x-ray to MRI Poster No.: C-2441 Congress: ECR 2015 Type: Educational Exhibit Authors: S. Fouassier, A. L. C. Duarte, C. Ruivo, J. Velez ; Évora/PT, 1 2 1 2 3 1 3 Coimbra/PT, PT Keywords:
ORTHOPAEDIC ONCOLOGY OITE REVIEW COURSE
 ORTHOPAEDIC ONCOLOGY OITE REVIEW COURSE Richard D. Lackman, MD FACS Director, Orthopaedic Oncology Center Cancer Institute Introduction In the evaluation of a patient with a bone tumor, there are several
ORTHOPAEDIC ONCOLOGY OITE REVIEW COURSE Richard D. Lackman, MD FACS Director, Orthopaedic Oncology Center Cancer Institute Introduction In the evaluation of a patient with a bone tumor, there are several
History. 33 y/o F with hx of palpable anterior tibial mass x 2 years, only painful with palpation
 History 33 y/o F with hx of palpable anterior tibial mass x 2 years, only painful with palpation Imaging Photo Album Patient also had a smaller lesion 1 cm proximal to this lesion, not seen radiographically.
History 33 y/o F with hx of palpable anterior tibial mass x 2 years, only painful with palpation Imaging Photo Album Patient also had a smaller lesion 1 cm proximal to this lesion, not seen radiographically.
Malignant Bone Tumors - Part I: a brief revision of diagnostic aspects with conventional radiology
 Malignant Bone Tumors - Part I: a brief revision of diagnostic aspects with conventional radiology Poster No.: C-2473 Congress: ECR 2013 Type: Educational Exhibit Authors: I. Candelaria, L. B. Barbosa,
Malignant Bone Tumors - Part I: a brief revision of diagnostic aspects with conventional radiology Poster No.: C-2473 Congress: ECR 2013 Type: Educational Exhibit Authors: I. Candelaria, L. B. Barbosa,
Malignant Bone Tumours. PathoBasic, Daniel Baumhoer
 Malignant Bone Tumours PathoBasic, 20.03.18 Daniel Baumhoer FNCLCC Grading The differentiation score is defined as the extent to which a tumor resembles adult mesenchymal tissue (score 1), the extent to
Malignant Bone Tumours PathoBasic, 20.03.18 Daniel Baumhoer FNCLCC Grading The differentiation score is defined as the extent to which a tumor resembles adult mesenchymal tissue (score 1), the extent to
The Radiology Assistant : Bone tumor A-G
 Bone tumor A-G Bone tumors and tumor-like lesions in alphabethic order Henk Jan van de Woude and Robin Smithuis Radiology department of the Onze Lieve Vrouwe Gasthuis, Amsterdam and the Rijnland hospital,
Bone tumor A-G Bone tumors and tumor-like lesions in alphabethic order Henk Jan van de Woude and Robin Smithuis Radiology department of the Onze Lieve Vrouwe Gasthuis, Amsterdam and the Rijnland hospital,
GIANT CELL-RICH OSTEOSARCOMA: A CASE REPORT
 Nagoya J. Med. Sci. 59. 151-157, 1996 CASE REPORTS GIANT CELL-RICH OSTEOSARCOMA: A CASE REPORT KEIJI SATO!, SHIGEKI YAMAMURA!, HISASHI IWATA!, HIDESHI SUGIURA 2, NOBUO NAKASHIMA 3 and TETSURO NAGASAKA
Nagoya J. Med. Sci. 59. 151-157, 1996 CASE REPORTS GIANT CELL-RICH OSTEOSARCOMA: A CASE REPORT KEIJI SATO!, SHIGEKI YAMAMURA!, HISASHI IWATA!, HIDESHI SUGIURA 2, NOBUO NAKASHIMA 3 and TETSURO NAGASAKA
Radiologic approach to pediatric lytic bone lesions
 Radiologic approach to pediatric lytic bone lesions Poster No.: C-1177 Congress: ECR 2016 Type: Educational Exhibit Authors: J. L. LERMA GALLARDO, I. de la Pedraja, A. Lancharro 1 1 1 2 1 1 Zapata, J.
Radiologic approach to pediatric lytic bone lesions Poster No.: C-1177 Congress: ECR 2016 Type: Educational Exhibit Authors: J. L. LERMA GALLARDO, I. de la Pedraja, A. Lancharro 1 1 1 2 1 1 Zapata, J.
Common Primary Tumors of Bone
 Special Report Common Primary Tumors of Bone Primary bone tumors are a relatively rare occurrence, however, they can have serious deleterious consequences. Many possess the ability to degenerate into malignant
Special Report Common Primary Tumors of Bone Primary bone tumors are a relatively rare occurrence, however, they can have serious deleterious consequences. Many possess the ability to degenerate into malignant
What Do You Need to Know About Bone Pathology? Benjamin L. Hoch M.D. Associate Professor Department of Pathology University of Washington
 What Do You Need to Know About Bone Pathology? Benjamin L. Hoch M.D. Associate Professor Department of Pathology University of Washington What s Do You Need To Know About Bone Pathology? Reactive/pseudosarcomatous
What Do You Need to Know About Bone Pathology? Benjamin L. Hoch M.D. Associate Professor Department of Pathology University of Washington What s Do You Need To Know About Bone Pathology? Reactive/pseudosarcomatous
A review of Tumoral lesions of the shoulder
 A review of Tumoral lesions of the shoulder Poster No.: P-0109 Congress: ESSR 2013 Type: Scientific Exhibit Authors: M. M. Milán Rodríguez, Á. E. Moreno Puertas, J. M. Giménez, 1 1 1 1 2 1 A. Rubio Fernández,
A review of Tumoral lesions of the shoulder Poster No.: P-0109 Congress: ESSR 2013 Type: Scientific Exhibit Authors: M. M. Milán Rodríguez, Á. E. Moreno Puertas, J. M. Giménez, 1 1 1 1 2 1 A. Rubio Fernández,
VALORACIÒN RADIOLÓGICA DE LA LESIÒN ÒSEA SOLITARIA IMAGENOLOGIA MEDICA UNIVERSIDAD HISPANOAMERICANA
 VALORACIÒN RADIOLÓGICA DE LA LESIÒN ÒSEA SOLITARIA IMAGENOLOGIA MEDICA UNIVERSIDAD HISPANOAMERICANA TUMORES ÓSEOS SE PRESENTAN POR RANGOS DE EDAD, PRINCIPALMENTE: MENORES DE 20 AÑOS 20 A 40 AÑOS MAYORES
VALORACIÒN RADIOLÓGICA DE LA LESIÒN ÒSEA SOLITARIA IMAGENOLOGIA MEDICA UNIVERSIDAD HISPANOAMERICANA TUMORES ÓSEOS SE PRESENTAN POR RANGOS DE EDAD, PRINCIPALMENTE: MENORES DE 20 AÑOS 20 A 40 AÑOS MAYORES
Malignant Peripheral Nerve Sheath Tumor
 C H A P T E R 120 Malignant Peripheral Nerve Sheath Tumor Currently, malignant peripheral nerve sheath tumor (MPNST) is the most commonly used generic name for the neoplasms known in the past as neurosarcoma,
C H A P T E R 120 Malignant Peripheral Nerve Sheath Tumor Currently, malignant peripheral nerve sheath tumor (MPNST) is the most commonly used generic name for the neoplasms known in the past as neurosarcoma,
warwick.ac.uk/lib-publications
 A Thesis Submitted for the Degree of PhD at the University of Warwick Permanent WRAP URL: http://wrap.warwick.ac.uk/102063/ Copyright and reuse: This thesis is made available online and is protected by
A Thesis Submitted for the Degree of PhD at the University of Warwick Permanent WRAP URL: http://wrap.warwick.ac.uk/102063/ Copyright and reuse: This thesis is made available online and is protected by
Incidental bone tumors are asymptomatic lesions that are. Incidental Bone Lesions. When to Refer to the Tumor Specialist
 Bulletin of the NYU Hospital for Joint Diseases 2012;70(4):235-40 235 Incidental Bone Lesions When to Refer to the Tumor Specialist LT Suezie Kim, M.D., M.C., U.S.N., Catherine N. Laible, M.D., Leon D.
Bulletin of the NYU Hospital for Joint Diseases 2012;70(4):235-40 235 Incidental Bone Lesions When to Refer to the Tumor Specialist LT Suezie Kim, M.D., M.C., U.S.N., Catherine N. Laible, M.D., Leon D.
GIANT CELL TUMOR OF BONE
 GIANT CELL TUMOR OF BONE Definition. First described by Jaffe et al. 1, giant cell tumor of bone is a locally aggressive primary neoplasm of bone that is composed of proliferation of bland looking oval
GIANT CELL TUMOR OF BONE Definition. First described by Jaffe et al. 1, giant cell tumor of bone is a locally aggressive primary neoplasm of bone that is composed of proliferation of bland looking oval
Bone Tumors: In 1 Simple Chart
 Bone Tumors with PowerPoint Interactivity Download this entire slideshow from When running this on your own computer you can jump from slide to slide using these buttons at bottom of each slide: Last slide
Bone Tumors with PowerPoint Interactivity Download this entire slideshow from When running this on your own computer you can jump from slide to slide using these buttons at bottom of each slide: Last slide
FORMATION OF BONE. Intramembranous Ossification. Bone-Lec-10-Prof.Dr.Adnan Albideri
 FORMATION OF BONE All bones are of mesodermal origin. The process of bone formation is called ossification. We have seen that formation of most bones is preceded by the formation of a cartilaginous model,
FORMATION OF BONE All bones are of mesodermal origin. The process of bone formation is called ossification. We have seen that formation of most bones is preceded by the formation of a cartilaginous model,
ISSN: DISTRIBUTION OF BONE AND CARTILAGINOUS TUMORS IN PEDIATRIC AGE GROUP IN WESTERN UTTAR-PRADESH: AN EVALUATIVE STUDY
 : 289-295 ISSN: 2277 4998 DISTRIBUTION OF BONE AND CARTILAGINOUS TUMORS IN PEDIATRIC AGE GROUP IN WESTERN UTTAR-PRADESH: AN EVALUATIVE STUDY QADRI S, HASAN M, AKHTAR K * AND SHERWANI RK The Departments
: 289-295 ISSN: 2277 4998 DISTRIBUTION OF BONE AND CARTILAGINOUS TUMORS IN PEDIATRIC AGE GROUP IN WESTERN UTTAR-PRADESH: AN EVALUATIVE STUDY QADRI S, HASAN M, AKHTAR K * AND SHERWANI RK The Departments
GIANT CELL TUMOR OF LOWER END OF FEMUR IN A SKELETALLY IMMATURE-A RARE CASE
 GIANT CELL TUMOR OF LOWER END OF FEMUR IN A SKELETALLY IMMATURE-A RARE CASE *Surojit Mondal 1, Aniket Chowdhury 2 and Goutam Bandyopadhyay 3 1 Department of Orthopaedics, B.S.Medical College, Bankura,
GIANT CELL TUMOR OF LOWER END OF FEMUR IN A SKELETALLY IMMATURE-A RARE CASE *Surojit Mondal 1, Aniket Chowdhury 2 and Goutam Bandyopadhyay 3 1 Department of Orthopaedics, B.S.Medical College, Bankura,
Due in Lab. Due next week in lab - Scientific America Article Select one article to read and complete article summary
 Due in Lab 1. Skeletal System 33-34 2. Skeletal System 26 3. PreLab 6 Due next week in lab - Scientific America Article Select one article to read and complete article summary Cell Defenses and the Sunshine
Due in Lab 1. Skeletal System 33-34 2. Skeletal System 26 3. PreLab 6 Due next week in lab - Scientific America Article Select one article to read and complete article summary Cell Defenses and the Sunshine
Review Course «Musculoskeletal Oncology» October 6, 2011 UNIKLINIK BALGRIST. Imaging of Bone and Soft Tissue. Tumors
 Imaging of Bone and Soft Tissue Tumors Approach from a radiologist s point of view Florian Buck Radiology Radio- Radio- Oncologist Oncologist Orthopedist Orthopedist Patient Management Oncologist Oncologist
Imaging of Bone and Soft Tissue Tumors Approach from a radiologist s point of view Florian Buck Radiology Radio- Radio- Oncologist Oncologist Orthopedist Orthopedist Patient Management Oncologist Oncologist
MRI XR, CT, NM. Principal Modality (2): Case Report # 2. Date accepted: 15 March 2013
: Case Report # 2. Date accepted: 15 March 2013") Radiological Category: Musculoskeletal Principal Modality (1): Principal Modality (2): MRI XR, CT, NM Case Report # 2 Submitted by: Hannah Safia Elamir, D.O. Faculty reviewer: Naga R. Chinapuvvula, M.D.
Radiological Category: Musculoskeletal Principal Modality (1): Principal Modality (2): MRI XR, CT, NM Case Report # 2 Submitted by: Hannah Safia Elamir, D.O. Faculty reviewer: Naga R. Chinapuvvula, M.D.
The Skeletal System:Bone Tissue
 The Skeletal System:Bone Tissue Dynamic and ever-changing throughout life Skeleton composed of many different tissues cartilage, bone tissue, epithelium, nerve, blood forming tissue, adipose, and dense
The Skeletal System:Bone Tissue Dynamic and ever-changing throughout life Skeleton composed of many different tissues cartilage, bone tissue, epithelium, nerve, blood forming tissue, adipose, and dense
Functions of the Skeletal System. Chapter 6: Osseous Tissue and Bone Structure. Classification of Bones. Bone Shapes
 Chapter 6: Osseous Tissue and Bone Structure Functions of the Skeletal System 1. Support 2. Storage of minerals (calcium) 3. Storage of lipids (yellow marrow) 4. Blood cell production (red marrow) 5. Protection
Chapter 6: Osseous Tissue and Bone Structure Functions of the Skeletal System 1. Support 2. Storage of minerals (calcium) 3. Storage of lipids (yellow marrow) 4. Blood cell production (red marrow) 5. Protection
Case Report Intramedullary Chondrosarcoma of Proximal Humerus
 Hindawi Publishing Corporation Case Reports in Radiology Volume 2012, Article ID 642062, 7 pages doi:10.1155/2012/642062 Case Report Intramedullary Chondrosarcoma of Proximal Humerus Pratiksha Yadav, Dolly
Hindawi Publishing Corporation Case Reports in Radiology Volume 2012, Article ID 642062, 7 pages doi:10.1155/2012/642062 Case Report Intramedullary Chondrosarcoma of Proximal Humerus Pratiksha Yadav, Dolly
Immunohistochemistry in Bone and Soft Tissue Tumors. Sahar Rassi Zankoul, MD
 Immunohistochemistry in Bone and Soft Tissue Tumors Sahar Rassi Zankoul, MD Introduction Bone tumors represent a wide variety of tumors of various origins and malignant potentials. These different tumor
Immunohistochemistry in Bone and Soft Tissue Tumors Sahar Rassi Zankoul, MD Introduction Bone tumors represent a wide variety of tumors of various origins and malignant potentials. These different tumor
Bizarre parosteal osteochondromatous proliferation
 * * Bizarre Parosteal Osteochondromatous Proliferation A Case Report with Literature Review Chi-Fu Kao Yang-Chih Lin Yu-Hung Wu Be-Fong Chen* We report the case of a 12-year-old female with a slowly erythematous
* * Bizarre Parosteal Osteochondromatous Proliferation A Case Report with Literature Review Chi-Fu Kao Yang-Chih Lin Yu-Hung Wu Be-Fong Chen* We report the case of a 12-year-old female with a slowly erythematous
SMALL ROUND BLUE CELL LESION OF BONE
 DISCLOSURE SMALL ROUND BLUE CELL LESION OF BONE Dr. Alistair Jordan University of South Alabama No financial support or endorsement OBJECTIVES Describe the more common small round cell lesions of bone
DISCLOSURE SMALL ROUND BLUE CELL LESION OF BONE Dr. Alistair Jordan University of South Alabama No financial support or endorsement OBJECTIVES Describe the more common small round cell lesions of bone
Skeletal metastases are the most common variety of bone tumors and should always be considered in the differential diagnosis, particularly in older
 Dr Brajesh Nandan Skeletal metastases are the most common variety of bone tumors and should always be considered in the differential diagnosis, particularly in older patients. Cancers of the breast, prostate,
Dr Brajesh Nandan Skeletal metastases are the most common variety of bone tumors and should always be considered in the differential diagnosis, particularly in older patients. Cancers of the breast, prostate,
The Skeletal System. Chapter 7a. Skeletal System Introduction Functions of the skeleton Framework of bones The skeleton through life
 The Skeletal System Skeletal System Introduction Functions of the skeleton Framework of bones The skeleton through life Chapter 7a Support Protection Movement Storage areas Minerals Lipids Hemopoiesis
The Skeletal System Skeletal System Introduction Functions of the skeleton Framework of bones The skeleton through life Chapter 7a Support Protection Movement Storage areas Minerals Lipids Hemopoiesis
Benign Tumors of Bone
 REVIEW ARTICLE Benign Tumors of Bone Subbarao K Padmshri Prof. Dr. Kakarla Subbara, Hyderabad, India. Benign tumors of bone are common while malignant tumors are rare. Benign tumors constitute about 75%
REVIEW ARTICLE Benign Tumors of Bone Subbarao K Padmshri Prof. Dr. Kakarla Subbara, Hyderabad, India. Benign tumors of bone are common while malignant tumors are rare. Benign tumors constitute about 75%
FRACTURE CALLUS ASSOCIATED WITH BENIGN AND MALIGNANT BONE LESIONS AND MIMICKING OSTEOSARCOMA
 THE AMERICAN JOURNAL OF CLINICAL PATHOLOGY Vol. 52, No. 1 Copyright 1969 by The Williams & Wilkins Co. Printed in U.S.A. FRACTURE CALLUS ASSOCIATED WITH BENIGN AND MALIGNANT BONE LESIONS AND MIMICKING
THE AMERICAN JOURNAL OF CLINICAL PATHOLOGY Vol. 52, No. 1 Copyright 1969 by The Williams & Wilkins Co. Printed in U.S.A. FRACTURE CALLUS ASSOCIATED WITH BENIGN AND MALIGNANT BONE LESIONS AND MIMICKING
The Skeletal System. Mosby items and derived items 2010, 2006, 2002, 1997, 1992 by Mosby, Inc., an affiliate of Elsevier Inc.
 The Skeletal System Functions of Skeletal System Provides internal framework that supports the body Protects internal organs Helps fight disease by producing white blood cells 2 Functions of Skeletal System
The Skeletal System Functions of Skeletal System Provides internal framework that supports the body Protects internal organs Helps fight disease by producing white blood cells 2 Functions of Skeletal System
UCLA UCLA Previously Published Works
 UCLA UCLA Previously Published Works Title Benign bone tumors Permalink https://escholarship.org/uc/item/7h86k14t Journal Radiologic Clinics of North America, 49(6) ISSN 0033-8389 Authors Motamedi, K Seeger,
UCLA UCLA Previously Published Works Title Benign bone tumors Permalink https://escholarship.org/uc/item/7h86k14t Journal Radiologic Clinics of North America, 49(6) ISSN 0033-8389 Authors Motamedi, K Seeger,
04/27/2017. The Spectrum of Cartilaginous Tumors
 The Spectrum of Cartilaginous Tumors L I S A E R C O L A N O, M D M U S C U L O S K E L E T A L O N C O L O G Y D E P A R T M E N T O F O R T H O P A E D I C S A L L E G H E N Y H E A L T H N E T W O R
The Spectrum of Cartilaginous Tumors L I S A E R C O L A N O, M D M U S C U L O S K E L E T A L O N C O L O G Y D E P A R T M E N T O F O R T H O P A E D I C S A L L E G H E N Y H E A L T H N E T W O R
Fibrocartilaginous Dysplasia of the Bone: A Rare Variant of Fibrous Dysplasia
 Open Access Case Report DOI: 10.7759/cureus.448 Fibrocartilaginous Dysplasia of the Bone: A Rare Variant of Fibrous Dysplasia Raju Vaishya 1, Amit Kumar Agarwal 1, Nishint Gupta 2, Vipul Vijay 1 1. Department
Open Access Case Report DOI: 10.7759/cureus.448 Fibrocartilaginous Dysplasia of the Bone: A Rare Variant of Fibrous Dysplasia Raju Vaishya 1, Amit Kumar Agarwal 1, Nishint Gupta 2, Vipul Vijay 1 1. Department
A Modified Lodwick-Madewell Grading System for the Evaluation of Lytic Bone Lesions
 Musculoskeletal Imaging Original Research Caracciolo et al. Evaluation of Lytic one Lesions Musculoskeletal Imaging Original Research Jamie T. Caracciolo 1 H. Thomas Temple 2 G. Douglas Letson 3 Mark J.
Musculoskeletal Imaging Original Research Caracciolo et al. Evaluation of Lytic one Lesions Musculoskeletal Imaging Original Research Jamie T. Caracciolo 1 H. Thomas Temple 2 G. Douglas Letson 3 Mark J.
Giant cell tumour of the sternum-two cases
 Giant cell tumour of the sternum-two cases Nishaa.P 1, Raghuram.P 2, Navin patil 3, Jaipal B.R 4 Akkamahadevi patel 5 Assistant Professor ESIC medical college and PGIMSR 1 Professor and HOD, 2 Professor
Giant cell tumour of the sternum-two cases Nishaa.P 1, Raghuram.P 2, Navin patil 3, Jaipal B.R 4 Akkamahadevi patel 5 Assistant Professor ESIC medical college and PGIMSR 1 Professor and HOD, 2 Professor
General Approach to Lytic Bone Lesions D. Lee Bennett, MD, MA, Georges Y. El Khoury, MD Appl Radiol. 2004;33(5)
") General Approach to Lytic Bone Lesions D. Lee Bennett, MD, MA, Georges Y. El Khoury, MD Appl Radiol. 2004;33(5) www.medscape.com Abstract and Introduction Abstract When interpreting musculoskeletal radiographs,
General Approach to Lytic Bone Lesions D. Lee Bennett, MD, MA, Georges Y. El Khoury, MD Appl Radiol. 2004;33(5) www.medscape.com Abstract and Introduction Abstract When interpreting musculoskeletal radiographs,
The formation of blood cells is called. hemopoiesis. What does our bone store? Where do our bones store fat? yellow marrow.
 What are the 5/6 functions of the skeletal system? support, protection, movement, blood cell formation, storage, homeostasis The formation of blood cells is called hemopoiesis What does our bone store?
What are the 5/6 functions of the skeletal system? support, protection, movement, blood cell formation, storage, homeostasis The formation of blood cells is called hemopoiesis What does our bone store?
Fig Articular cartilage. Epiphysis. Red bone marrow Epiphyseal line. Marrow cavity. Yellow bone marrow. Periosteum. Nutrient foramen Diaphysis
 Fig. 7.1 Articular cartilage Epiphysis Red bone marrow Epiphyseal line Marrow cavity Yellow bone marrow Nutrient foramen Diaphysis Site of endosteum Compact bone Spongy bone Epiphyseal line Epiphysis Articular
Fig. 7.1 Articular cartilage Epiphysis Red bone marrow Epiphyseal line Marrow cavity Yellow bone marrow Nutrient foramen Diaphysis Site of endosteum Compact bone Spongy bone Epiphyseal line Epiphysis Articular
Key points in the evaluation of focal bone lesions: from plain film to multidetector CT
 Key points in the evaluation of focal bone lesions: from plain film to multidetector CT Poster No.: C-2060 Congress: ECR 2011 Type: Educational Exhibit Authors: I. Rubio Marco, M. Arraiza Sarasa, H. Gómez
Key points in the evaluation of focal bone lesions: from plain film to multidetector CT Poster No.: C-2060 Congress: ECR 2011 Type: Educational Exhibit Authors: I. Rubio Marco, M. Arraiza Sarasa, H. Gómez
Radiologic Pathologic Correlation of Intraosseous Lipomas. Tim Propeck 1, Mary Anne Bullard 1, John Lin 1, Kei Doi 2, William Martel 1
 Downloaded from www.ajronline.org by 148.251.232.83 on 04/10/18 from IP address 148.251.232.83. opyright RRS. For personal use only; all rights reserved Radiologic Pathologic orrelation of Intraosseous
Downloaded from www.ajronline.org by 148.251.232.83 on 04/10/18 from IP address 148.251.232.83. opyright RRS. For personal use only; all rights reserved Radiologic Pathologic orrelation of Intraosseous
The role of CT and MRI in evaluation of Osteoid Oteoma
 The role of CT and MRI in evaluation of Osteoid Oteoma Elene Iordanishvili Tbilisi Sate Medical University Instructor: Prof. Dr. Ketevan Kotetishvili Department of Physics Georgian Technical University
The role of CT and MRI in evaluation of Osteoid Oteoma Elene Iordanishvili Tbilisi Sate Medical University Instructor: Prof. Dr. Ketevan Kotetishvili Department of Physics Georgian Technical University
OSSEOUS TISSUE & BONE STRUCTURE PART I: OVERVIEW & COMPONENTS
 OSSEOUS TISSUE & BONE STRUCTURE PART I: OVERVIEW & COMPONENTS The Skeletal System Skeletal system includes: bones of the skeleton, cartilages, ligaments, and connective tissues What are the functions of
OSSEOUS TISSUE & BONE STRUCTURE PART I: OVERVIEW & COMPONENTS The Skeletal System Skeletal system includes: bones of the skeleton, cartilages, ligaments, and connective tissues What are the functions of
LAC + USC.
 Jeff McDavit,, M.D. LAC + USC mcdavit@usc.edu Clinical History 55 year old male with large, deep, non- tender left thigh mass. Seen at LAC+USC Med Ctr FNA clinic No h/o trauma or radiation Vimentin
Jeff McDavit,, M.D. LAC + USC mcdavit@usc.edu Clinical History 55 year old male with large, deep, non- tender left thigh mass. Seen at LAC+USC Med Ctr FNA clinic No h/o trauma or radiation Vimentin
PATHOLOGY OF THE MUSCULOSKELETAL SYSTEM
 PATHOLOGY OF THE MUSCULOSKELETAL SYSTEM BONES & JOINTS CONGENITAL DISEASES OF BONE Osteogenesis Imperfecta (OI) (Brittle bone diseases) is a group of hereditary disorders caused by gene mutations that
PATHOLOGY OF THE MUSCULOSKELETAL SYSTEM BONES & JOINTS CONGENITAL DISEASES OF BONE Osteogenesis Imperfecta (OI) (Brittle bone diseases) is a group of hereditary disorders caused by gene mutations that
Skeletal Radiology. Solitary (unicameral) bone cyst. The fallen fragment sign revisited
 bone cyst. The fallen fragment sign revisited") Skeletal Radiol (1989) 18:261-265 Skeletal Radiology Solitary (unicameral) bone cyst The fallen fragment sign revisited S. Struhl, M.D., C. Edelson, M.D., H. Pritzker, M.D., L.P. Seimon, M.D., and H.D.
Skeletal Radiol (1989) 18:261-265 Skeletal Radiology Solitary (unicameral) bone cyst The fallen fragment sign revisited S. Struhl, M.D., C. Edelson, M.D., H. Pritzker, M.D., L.P. Seimon, M.D., and H.D.
What are the parts of the skeletal system? Chapter 6- Part I Bones and Skeletal Tissues. Growth of Cartilage. Bones come in many shapes
 Chapter 6- Part I Bones and Skeletal Tissues Components of the skeletal system Classification of Bone (bone shapes) Functions of bone Bone structure Microscopic structure of bone and bone cells What are
Chapter 6- Part I Bones and Skeletal Tissues Components of the skeletal system Classification of Bone (bone shapes) Functions of bone Bone structure Microscopic structure of bone and bone cells What are
Department of Radiology, University of Szeged. Imaging of the skeleton
 Imaging of the skeleton Methods of examination: plain x-ray (radiography, densitometry) x-ray with contrast material (fistulography, angiography) ultrasound (b-mode, Doppler, color, duplex) computed tomography
Imaging of the skeleton Methods of examination: plain x-ray (radiography, densitometry) x-ray with contrast material (fistulography, angiography) ultrasound (b-mode, Doppler, color, duplex) computed tomography
* I have no disclosures or any
 Howard Rosenthal, M.D. Associate Professor of Orthopedic Surgery University of Kansas Sarcoma Center I have no disclosures or any conflicts related to the content of this presentation. Objectives 1. Describe
Howard Rosenthal, M.D. Associate Professor of Orthopedic Surgery University of Kansas Sarcoma Center I have no disclosures or any conflicts related to the content of this presentation. Objectives 1. Describe
BONE TISSUE. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 BONE TISSUE Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology BONE FUNCTION Support Protection (protect internal organs) Movement (provide leverage system for skeletal muscles, tendons, ligaments
BONE TISSUE Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology BONE FUNCTION Support Protection (protect internal organs) Movement (provide leverage system for skeletal muscles, tendons, ligaments
Cytology of Neoplasms that Occur on the Limbs Rick Alleman, DVM, PhD, DABVP, DACVP
 Cytology of Neoplasms that Occur on the Limbs Rick Alleman, DVM, PhD, DABVP, DACVP I. Introduction The purpose of this material is to provide information that may be useful in the identification of tumors
Cytology of Neoplasms that Occur on the Limbs Rick Alleman, DVM, PhD, DABVP, DACVP I. Introduction The purpose of this material is to provide information that may be useful in the identification of tumors
Human Skeletal System Glossary
 Acromegaly Apatite Acromegaly - is a condition which involves excessive growth of the jaw, hands, and feet. It results from overproduction of somatotropin in adults (after fusion of the ossification centres
Acromegaly Apatite Acromegaly - is a condition which involves excessive growth of the jaw, hands, and feet. It results from overproduction of somatotropin in adults (after fusion of the ossification centres
The Skeletal System PART A
 5 The Skeletal System PART A PowerPoint Lecture Slide Presentation by Jerry L. Cook, Sam Houston University ESSENTIALS OF HUMAN ANATOMY & PHYSIOLOGY EIGHTH EDITION ELAINE N. MARIEB The Skeletal System
5 The Skeletal System PART A PowerPoint Lecture Slide Presentation by Jerry L. Cook, Sam Houston University ESSENTIALS OF HUMAN ANATOMY & PHYSIOLOGY EIGHTH EDITION ELAINE N. MARIEB The Skeletal System
The Skeletal System Vertebral column Sacrum. Osseous tissue For the body and soft organs. Magnesium, sodium, fluoride Levers for muscle action
 10/1/2016 Cranium Facial s Skull Clavicle Scapula Sternum Rib Humerus Vertebra Radius Ulna Carpals Thoracic cage (ribs and sternum) The Skeletal System Vertebral column Sacrum Phalanges Metacarpals Femur
10/1/2016 Cranium Facial s Skull Clavicle Scapula Sternum Rib Humerus Vertebra Radius Ulna Carpals Thoracic cage (ribs and sternum) The Skeletal System Vertebral column Sacrum Phalanges Metacarpals Femur
Medical Student Rotation Guide Tumor Service
 Medical Student Rotation Guide Tumor Service Overview Welcome to the medical student rotation on the Tumor service in the Department of Orthopaedic Surgery at Rush University Medical Center! We are excited
Medical Student Rotation Guide Tumor Service Overview Welcome to the medical student rotation on the Tumor service in the Department of Orthopaedic Surgery at Rush University Medical Center! We are excited
Case 8 Soft tissue swelling
 Case 8 Soft tissue swelling 26-year-old female presented with a swelling on the back of the left knee joint since the last 6 months and chronic pain in the calf and foot since the last 2 months. Pain in
Case 8 Soft tissue swelling 26-year-old female presented with a swelling on the back of the left knee joint since the last 6 months and chronic pain in the calf and foot since the last 2 months. Pain in
Bone pathology 2. László Kereskai MD.
 Bone pathology 2. László Kereskai MD. BONE-FORMING TUMORS Osteoid osteoma and osteoblastoma: Osteoid osteoma Most frequent btw 10-30 ys. Best known symptom is intensive pain with easy precise localisation.
Bone pathology 2. László Kereskai MD. BONE-FORMING TUMORS Osteoid osteoma and osteoblastoma: Osteoid osteoma Most frequent btw 10-30 ys. Best known symptom is intensive pain with easy precise localisation.
What is bone? Specialized form of connective tissue: mineralized collagen matrix, therefore very rigid and strong while still retaining some degree of
 Bone What is bone? Specialized form of connective tissue: mineralized collagen matrix, therefore very rigid and strong while still retaining some degree of flexibility Other types of connective tissue:
Bone What is bone? Specialized form of connective tissue: mineralized collagen matrix, therefore very rigid and strong while still retaining some degree of flexibility Other types of connective tissue:
Medical Student Rotation Guide Tumor Service
 Medical Student Rotation Guide Tumor Service Overview Welcome to the medical student rotation on the Tumor service in the Department of Orthopaedic Surgery at Rush University Medical Center! We are excited
Medical Student Rotation Guide Tumor Service Overview Welcome to the medical student rotation on the Tumor service in the Department of Orthopaedic Surgery at Rush University Medical Center! We are excited
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Osteosarcoma Anatomic and Histologic Variants
 natomic Pathology / OSTEOSRCOM Osteosarcoma natomic and Histologic Variants Michael J. Klein, MD, and Gene P. Siegal, MD, PhD Key Words: Osteosarcoma; Malignant bone tumors; ones; Imaging DOI: 10.1309/UC6KQHLD9LV2KENN
natomic Pathology / OSTEOSRCOM Osteosarcoma natomic and Histologic Variants Michael J. Klein, MD, and Gene P. Siegal, MD, PhD Key Words: Osteosarcoma; Malignant bone tumors; ones; Imaging DOI: 10.1309/UC6KQHLD9LV2KENN
Skeletal System. Chapter 6.1 Human Anatomy & Physiology
 Skeletal System Chapter 6.1 Human Anatomy & Physiology Overview of Skeletal System Bones Joints Skeletal System Cartilage Tendons (bone to muscle) Ligaments (bone to bone) Function of the Skeletal System
Skeletal System Chapter 6.1 Human Anatomy & Physiology Overview of Skeletal System Bones Joints Skeletal System Cartilage Tendons (bone to muscle) Ligaments (bone to bone) Function of the Skeletal System
ANATOMY & PHYSIOLOGY - CLUTCH CH. 8 - BONE AND CARTILAGE.
 !! www.clutchprep.com CONCEPT: BONE CLASSIFICATIONS There are four classifications of bones based on their 1. Long bones are greater in length than in width - Found in the upper and lower limbs (ex: arm,
!! www.clutchprep.com CONCEPT: BONE CLASSIFICATIONS There are four classifications of bones based on their 1. Long bones are greater in length than in width - Found in the upper and lower limbs (ex: arm,
Musculoskeletal Sarcomas
 Musculoskeletal Sarcomas Robert C. Orth, M.D., Ph.D. Edward B. Singleton Department of Pediatric Radiology Texas Children s Hospital Page 0 xxx00.#####.ppt 9/23/2012 9:01:18 AM No disclosures Page 1 xxx00.#####.ppt
Musculoskeletal Sarcomas Robert C. Orth, M.D., Ph.D. Edward B. Singleton Department of Pediatric Radiology Texas Children s Hospital Page 0 xxx00.#####.ppt 9/23/2012 9:01:18 AM No disclosures Page 1 xxx00.#####.ppt
Osteology. Dr. Carmen E. Rexach Anatomy 35 Mt San Antonio College
 Osteology Dr. Carmen E. Rexach Anatomy 35 Mt San Antonio College Functions of the Skeletal System: Support Movement Protection Hemopoiesis Electrolyte balance (Ca ++ /PO -3 4 ) Acid-base balance Storage
Osteology Dr. Carmen E. Rexach Anatomy 35 Mt San Antonio College Functions of the Skeletal System: Support Movement Protection Hemopoiesis Electrolyte balance (Ca ++ /PO -3 4 ) Acid-base balance Storage
Bone (2) Chapter 8. The bone is surrounded by the periosteum, the periosteum consists of two layers: a fibrous outer layer and an innercellular layer.
 Chapter 8. The bone is surrounded by the periosteum, the periosteum consists of two layers: a fibrous outer layer and an innercellular layer.") Bone (2) Chapter 8 The bone is surrounded by the periosteum, the periosteum consists of two layers: a fibrous outer layer and an innercellular layer. The innercellular layer contains osteoprogenitor cells,
Bone (2) Chapter 8 The bone is surrounded by the periosteum, the periosteum consists of two layers: a fibrous outer layer and an innercellular layer. The innercellular layer contains osteoprogenitor cells,
Skeletal System worksheet
 Skeletal System worksheet Name Section A: Intro to Skeletal System The skeletal system performs vital functions that enable us to move through our daily lives. Support - The skeleton provides support and
Skeletal System worksheet Name Section A: Intro to Skeletal System The skeletal system performs vital functions that enable us to move through our daily lives. Support - The skeleton provides support and
Chapter 6: Skeletal System: Bones and Bone Tissue
 Chapter 6: Skeletal System: Bones and Bone Tissue I. Functions A. List and describe the five major functions of the skeletal system: 1. 2. 3.. 4. 5.. II. Cartilage A. What do chondroblasts do? B. When
Chapter 6: Skeletal System: Bones and Bone Tissue I. Functions A. List and describe the five major functions of the skeletal system: 1. 2. 3.. 4. 5.. II. Cartilage A. What do chondroblasts do? B. When
General osteology. General anatomy of the human skeleton. Development and classification of bones. The bone as a multifunctional organ.
 General osteology. General anatomy of the human skeleton. Development and classification of bones. The bone as a multifunctional organ. Composed by Natalia Leonidovna Svintsitskaya, Associate professor
General osteology. General anatomy of the human skeleton. Development and classification of bones. The bone as a multifunctional organ. Composed by Natalia Leonidovna Svintsitskaya, Associate professor
1/9/2013 EXTRAMEDULLARY TUMORS OF THE PEDIATRIC SPINE. Introduction. Classification for Extramedullary Tumors
 EXTRAMEDULLARY TUMORS OF THE PEDIATRIC SPINE Eugene Wang 1/20/12 Dent Neurologic Institute Introduction 2/3 of all intraspinal tumors of childhood are extramedullary 50% Extradural 10-15% Intradural Back
EXTRAMEDULLARY TUMORS OF THE PEDIATRIC SPINE Eugene Wang 1/20/12 Dent Neurologic Institute Introduction 2/3 of all intraspinal tumors of childhood are extramedullary 50% Extradural 10-15% Intradural Back