John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division
|
|
|
- Marsha Foster
- 6 years ago
- Views:
Transcription

1 John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division
2 John Campbell, MD For the 12 months preceding this CME activity, I disclose the following types of financial relationships: Honoraria received from: Abbott Vascular Consulted for: Cook Medical and W. L. Gore & Associates, Inc. Held common stock in: None Research, clinical trial, or drug study funds received from: None I will be discussing products that are investigational or not labeled for use under discussion.

3 Includes Ischemic rest pain Ulceration Gangrene Symptoms must be present for at least 2 weeks



4 Grade Category Clinical 0 0 Asymptomatic I 1 Mild claudication I 2 Moderate claudication I 3 Severe claudication II 4 Ischemic rest pain III 5 Minor tissue loss III 6 Major tissue loss
. J Vasc Surg.")
5 Primary Treatment 1 Year Later Medical treatment only 25% Primary amputation 25% Revascularization 50% Alive and amputated 30% Continuing CLI 20% CLI resolved 25% Dead 25% Adapted from Norgren L, et al (TASC II). J Vasc Surg. 2007;45S:1-67
6 Remember that we are not just plumbers! Requires addressing multifactorial issues Optimize risk factor modification Antiplatelet therapy HgA1C 7% Statin therapy If tissue loss, assess for infection (? osteomyelitis or wet gangrene) Does the ulcer need off-loaded or protected from shear stress Treatment often requires a multidisciplinary approach
7 Prostanoids: administered parenterally TASC Recommendation Meta-analysis of the data demonstrated that patients on active treatment had a greater chance to survive and keep both legs during follow-up Previous studies with prostanoids in CLI suggested improved healing of ischemic ulcers and reduction in amputations (A) month follow-up However, recent trials do not support the benefit of prostanoids in promoting amputation-free survival (A) There are no other pharmacotherapies that can be recommended for the treatment of CLI (B) However, subsequent trial of lipo-ecraprost vs placebo failed to reduce death and amputation during 6- Direct-acting vasodilators: of no value and primarily increase blood flow to non-ischemic areas Anticoagulants: LMWH evaluated in 2 trials in patients with CLI and ulcers and demonstrated no benefit Vasoactive drugs: Both naftidrofuryl and pentoxifylline evaluated for treatment of CLI and have demonstrated no clear benefit Norgren L, et al (TASC II). J Vasc Surg. 2007;45S:1-67
8 Does the patient have venous conduit? Anatomical factors Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II) Patient s preoperative risk Life expectancy of the patient
: Management of Chronic Lower Limb Ischemia.")
9 4-Year Primary Patency for Below-Knee Femoropopliteal Bypass Reverse saphenous vein 77% In-situ vein bypass 68% PTFE 40% 4-Year Primary Patency for Infrapopliteal Bypass Reverse saphenous vein 62% In-situ vein bypass 68% PTFE 21% Dalman RL. In Mills JL (ed): Management of Chronic Lower Limb Ischemia. London, Arnold, 2000, pp
10 TASC A lesions Single stenosis 10 cm in length Single occlusion 5 cm in length Adapted from Norgren L, et al (TASC II). J Vasc Surg. 2007;45S:1-67
11 Multiple lesions (stenoses or occlusions), each 5 cm Single stenosis or occlusion 15 cm not involving the infrageniculate popliteal artery Single or multiple lesions in the absence of continuous tibial vessels to improve inflow for a distal bypass Heavily calcified occlusion 5 cm in length Single popliteal stenosis Adapted from Norgren L et al (TASC II). J Vasc Surg 2007;45S:1-67
12 Multiple stenoses or occlusions totaling >15 cm with or without heavy calcification Recurrent stenoses or occlusions that need treatment after 2 endovascular interventions Adapted from Norgren L, et al (TASC II). J Vasc Surg. 2007;45S:1-67
13 Chronic total occlusions of the CFA or SFA (>20 cm, involving the popliteal artery) Chronic total occlusion of popliteal artery and proximal trifurcation vessels Adapted from Norgren L, et al (TASC II). J Vasc Surg. 2007;45S:1-67
14 TASC A Single stenoses <1 cm in the tibial or peroneal vessels TASC B Multiple focal stenoses of the tibial or peroneal vessels, each <1 cm in length 1 or 2 focal stenoses, each <1-cm long at the tibial trifurcation Short tibial or peroneal stenosis in conjunction with femoropopliteal angioplasty TASC C Stenoses 1-4 cm in length Occlusions 1-2 cm in length of the tibial or peroneal vessels Extensive stenoses of the tibial trifurcation TASC D Tibial or peroneal occlusions >2 cm Diffusely diseased tibial or peroneal vessels Doormandy JA, et al. J Vasc Surgery. 2000;31:S1-S296
15 Black and white decision A: Endovascular surgery is the treatment of choice D: Surgery is the treatment of choice Gray decision B: Endovascular surgery preferred treatment C: Surgery is the preferred treatment for good-risk patients The patient s comorbidities, fully informed patient preference, and the local operator s long-term success must be considered Adapted from Norgren L, et al (TASC II). J Vasc Surg. 2007;45S:1-67
16 Bypass vs Angioplasty in Severe Ischaemia of the Leg Trial (BASIL) 452 patients enrolled over a 5 year period All patients with severe limb ischemia (rest pain or tissue loss) Randomly assigned to an initial treatment of either open surgery or balloon angioplasty Primary outcomes were amputation-free survival (AFS) and overall survival (OS) Bradbury AW, et al. J Vasc Surg. 2010;51:5S-17S
17 Follow-up: all patients for 3 years and 54% of patients for >5 years Entire cohort 56% dead at end of follow-up 38% alive without amputation 7% alive with amputation AFS and OS did not differ during follow-up For patients who survived 2 years from randomization Bypass surgery first was associated with a reduced HR of 0.85 (p =0.108) for subsequent AFS and for subsequent OS of 0.61 (p = 0.009) Mean OS was increased 7.3 months (p = 0.02) and mean AFS was increased 5.9 months (p = 0.02) during a mean follow-up of 3.1 yrs Bradbury AW, et al. J Vasc Surg. 2010;51:5S-17S
18 Only 10% of patients screened were enrolled in the trial Improvement in endovascular technology since enrollment ( ) Stents not used 20% immediate technical failure The use of prosthetic grafts for bypass surgery 75% of bypasses used GSV as conduit Few patients on optimal medical therapy at the time of randomization Only 1/3 of patients on statin! Bradbury AW, et al. J Vasc Surg. 2010;51:5S-17S
19 Class IIa Recommendations For patients with limb-threatening lower-extremity ischemia and an estimated life expectancy of 2 years or less or in patients in whom an autogenous vein conduit is not available, balloon angioplasty is reasonable to perform when possible as the initial procedure to improve distal blood flow (LOE B) For patients with limb-threatening ischemia and an estimated life expectancy of more than 2 years, bypass surgery when possible and when an autogenous vein conduit is available is reasonable to perform as the initial treatment to improve distal blood flow (LOE B) Rooke TW, et al. Vascular Medicine. 2011;16:



20 CLI Life expectancy >2yrs Life expectancy <2 years Suitable venous conduit No suitable venous conduit Endovascular surgery Consider Open surgery Consider endovascular surgery
21 Normal toe pressures vary from 60% to 80% of the ankle pressure TBI normal is 0.70 Wound healing If toe pressure is <30 mm Hg, then it is likely that the wound will not heal without revascularization If toe pressure is >50 mm Hg, then it is very likely with good wound care that the wound will heal Brooks B, et al. Diabet Med 2001;18:
22 Adequate inflow must be established prior to improvement in the outflow This sometimes requires staged procedures or can be often be performed simultaneously The goal is to restore pulsatile in-line flow to the level of the foot However, outcome is directly related to the number of patent infrapopliteal arteries after PTA 1-year limb salvage rates 0 arteries 56.4% 1 artery 73.1% 2 arteries 80.4% 3 arteries 83% Emerging data that direct revascularization of the artery supplying the angiosome with the wound may improve wound healing Peregrin JH, et al. Cardiovasc Intervent Radiol. 33: ; Neville RF, et al. Ann Vasc Surg. 23: ; Iida O, et al. J Vasc Surg. 55:33-370


23 Angioplasty Stenting Self-expanding Can be covered with PTFE Balloon-expandable in the infrapopliteal segment Cutting balloon Atherectomy Cryoplasty Future technologies Drug-eluting balloon Bioabsorbable stents



24 Specific challenges High biomechanical stress associated with repetitive knee flexion 88% of healthy subjects have occlusion of the popliteal artery during maximal plantar flexion secondary to external compression Fracture Hoffman U, et al. J Vasc Surg. 1997;26:


25 Angioplasty of the Popliteal Artery Primary Patency at 2 years Secondary Patency at 2 years Claudication 86% 94% CLI 54% 83% Dalainas I, et al. Int J Angiol. 2007;16(2):47-49
 1 patency 1/3 years 2 patency 1/3 years")

26 Results From Meta-Analysis of Angioplasty of the Infrapopliteal Arteries N (patients) 1 patency 1/3 years 2 patency 1/3 years Limb salvage rate 1/3 years Romiti et al. 2, %/48.6% 68.2%/62.9% 86%/82.4% Romiti M, et al. J Vasc Surg. 2008;47:
 Required angiographic follow-up at 6 months Results 6-month binary restenosis of 68.")

27 XCELL Trial Inclusion criteria included CLI with Rutherford Classification patients (140 limbs) Required angiographic follow-up at 6 months Results 6-month binary restenosis of 68.5% 12-month amputation-free survival of 78.3% 12-month freedom from major amputation 89.6% 12-month complete wound healing rate 54.4% Rocha-Singh KJ, et al. Catheter Cardiovasc Interv. 2012; Epub ahead of print
28 Rastan et al compared drug-eluting balloon-expandable stents (DES) to balloon-expandable bare stents (BS) Double-blind, multicenter, randomized clinical trial 161 patients Patency at 1 year Primary DES (80.6%) BS (55.6%) p=0.004 Secondary DES (91.9%) BS (71.4%) p= No difference in limb salvage rate or mortality Rastan A, et al. Eur Heart J. 2011;32(18):
29 Non-Invasive studies: Unable to obtain ABI (Non-compressible) Left TBI 0.24 (33 mm Hg) Bypass graft velocities: Proximal anastomosis: 168 cm/sec Mid Graft: 68 cm/sec Distal Graft: 78.6 cm/sec The posterior artery appeared to be occluded


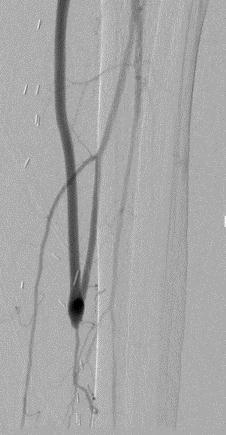

30

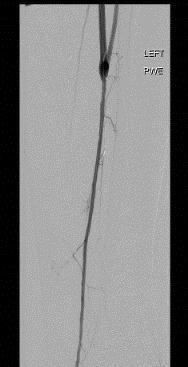
31
32 Should I have used DES instead of using angioplasty??? The primary patency at 1 year would probably be higher But it is off-label use It s expensive (multiple stents required) And does it really effect amputation free survival?
Disclosures. Talking Points. An initial strategy of open bypass is better for some CLI patients, and we can define who they are
 An initial strategy of open bypass is better for some CLI patients, and we can define who they are Fadi Saab, MD, FASE, FACC, FSCAI Metro Heart & Vascular Metro Health Hospital, Wyoming, MI Assistant Clinical
An initial strategy of open bypass is better for some CLI patients, and we can define who they are Fadi Saab, MD, FASE, FACC, FSCAI Metro Heart & Vascular Metro Health Hospital, Wyoming, MI Assistant Clinical
John E. Campbell, MD. Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division
 John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division John Campbell, MD For the 12 months preceding this CME activity,
John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division John Campbell, MD For the 12 months preceding this CME activity,
PAD and CRITICAL LIMB ISCHEMIA: EVALUATION AND TREATMENT 2014
 PAD and CRITICAL LIMB ISCHEMIA: EVALUATION AND TREATMENT 2014 Van Crisco, MD, FACC, FSCAI First Coast Heart and Vascular Center, PLLC Jacksonville, FL 678-313-6695 Conflict of Interest Bayer Healthcare
PAD and CRITICAL LIMB ISCHEMIA: EVALUATION AND TREATMENT 2014 Van Crisco, MD, FACC, FSCAI First Coast Heart and Vascular Center, PLLC Jacksonville, FL 678-313-6695 Conflict of Interest Bayer Healthcare
Stratifying Management Options for Patients with Critical Limb Ischemia: When Should Open Surgery Be the Initial Option for CLI?
 Stratifying Management Options for Patients with Critical Limb Ischemia: When Should Open Surgery Be the Initial Option for CLI? Peter F. Lawrence, M.D. Gonda Vascular Center Division of Vascular Surgery
Stratifying Management Options for Patients with Critical Limb Ischemia: When Should Open Surgery Be the Initial Option for CLI? Peter F. Lawrence, M.D. Gonda Vascular Center Division of Vascular Surgery
LIMB SALVAGE IN THE DIABETIC PATIENT
 LIMB SALVAGE IN THE DIABETIC PATIENT WHO? HOW? BEST? DISCLOSURES Educational grant from Cook Inc OBJECTIVES Review risk stratification and staging schemes for the threatened limb Discuss current concepts
LIMB SALVAGE IN THE DIABETIC PATIENT WHO? HOW? BEST? DISCLOSURES Educational grant from Cook Inc OBJECTIVES Review risk stratification and staging schemes for the threatened limb Discuss current concepts
Olive registry: 3-years outcome of BTK intervention in Japan. Osamu Iida, MD Kansai Rosai Hospital Amagasaki, Hyogo, Japan
 Olive registry: 3-years outcome of BTK intervention in Japan Osamu Iida, MD Kansai Rosai Hospital Amagasaki, Hyogo, Japan What is the optimal treatment for the patient with critical limb ischemia (CLI)?
Olive registry: 3-years outcome of BTK intervention in Japan Osamu Iida, MD Kansai Rosai Hospital Amagasaki, Hyogo, Japan What is the optimal treatment for the patient with critical limb ischemia (CLI)?
Surgery is and Remains the Gold Standard for Limb-Threatening Ischemia
 Surgery is and Remains the Gold Standard for Limb-Threatening Ischemia Albeir Mousa, MD., FACS.,MPH., MBA Professor of Vascular and Endovascular Surgery West Virginia University Disclosure None What you
Surgery is and Remains the Gold Standard for Limb-Threatening Ischemia Albeir Mousa, MD., FACS.,MPH., MBA Professor of Vascular and Endovascular Surgery West Virginia University Disclosure None What you
Distal By-Pass procedures can reduce limb loss
 Conventional treatment of the diabetic foot Distal By-Pass procedures can reduce limb loss Dr. Nikolaos Melas, PhD Vascular and Endovascular Surgeon Military Doctor Associate in 1st department of Surgery,
Conventional treatment of the diabetic foot Distal By-Pass procedures can reduce limb loss Dr. Nikolaos Melas, PhD Vascular and Endovascular Surgeon Military Doctor Associate in 1st department of Surgery,
Surgical Options for revascularisation P E T E R S U B R A M A N I A M
 Surgical Options for revascularisation P E T E R S U B R A M A N I A M The goal Treat pain Heal ulcer Preserve limb Preserve life The options Conservative Endovascular Surgical bypass Primary amputation
Surgical Options for revascularisation P E T E R S U B R A M A N I A M The goal Treat pain Heal ulcer Preserve limb Preserve life The options Conservative Endovascular Surgical bypass Primary amputation
The present status of selfexpanding. for CLI: Why and when to use. Sean P Lyden MD Cleveland Clinic Cleveland, Ohio
 The present status of selfexpanding and balloonexpandable tibial BMS and DES for CLI: Why and when to use Sean P Lyden MD Cleveland Clinic Cleveland, Ohio Disclosure Speaker name: Sean Lyden, MD I have
The present status of selfexpanding and balloonexpandable tibial BMS and DES for CLI: Why and when to use Sean P Lyden MD Cleveland Clinic Cleveland, Ohio Disclosure Speaker name: Sean Lyden, MD I have
Practical Point in Holistic Diabetic Foot Care 3 March 2016
 Diabetic Foot Ulcer : Vascular Management Practical Point in Holistic Diabetic Foot Care 3 March 2016 Supapong Arworn, MD Division of Vascular and Endovascular Surgery Department of Surgery, Chiang Mai
Diabetic Foot Ulcer : Vascular Management Practical Point in Holistic Diabetic Foot Care 3 March 2016 Supapong Arworn, MD Division of Vascular and Endovascular Surgery Department of Surgery, Chiang Mai
Disclosures. Tips and Tricks for Tibial Intervention. Tibial intervention overview
 Tips and Tricks for Tibial Intervention Donald L. Jacobs, MD C Rollins Hanlon Endowed Professor and Chair Chair of Surgery Saint Louis University SSM-STL Saint Louis University Hospital Disclosures Abbott
Tips and Tricks for Tibial Intervention Donald L. Jacobs, MD C Rollins Hanlon Endowed Professor and Chair Chair of Surgery Saint Louis University SSM-STL Saint Louis University Hospital Disclosures Abbott
Evidence-Based Optimal Treatment for SFA Disease
 Evidence-Based Optimal Treatment for SFA Disease Endo first Don t burn surgical bridge Don t stent if possible Javairiah Fatima, MD Assistant Professor of Surgery Division of Vascular and Endovascular
Evidence-Based Optimal Treatment for SFA Disease Endo first Don t burn surgical bridge Don t stent if possible Javairiah Fatima, MD Assistant Professor of Surgery Division of Vascular and Endovascular
Case Discussion. Disclosures. Critical Limb Ischemia: A Selective Approach to Revascularization Works Best 4/28/2012. None. 58 yo M, DM, CAD, HTN
 Critical Limb Ischemia: A Selective Approach to Revascularization Works Best None Disclosures Michael S. Conte MD, FACS Division of Vascular and Endovascular Surgery Co-Director, Heart and Vascular Center
Critical Limb Ischemia: A Selective Approach to Revascularization Works Best None Disclosures Michael S. Conte MD, FACS Division of Vascular and Endovascular Surgery Co-Director, Heart and Vascular Center
Disclosures. Objectives. Bypass vs. Endo for SFA Disease: Reaching Consensus on a Rational Approach. Christopher D. Owens, MD 4/23/2009
 Disclosures Bypass vs. Endo for SFA Disease: Reaching Consensus on a Rational Approach No disclosures No conflicts of interest Christopher D. Owens, MD Objectives Changing face of our patients presenting
Disclosures Bypass vs. Endo for SFA Disease: Reaching Consensus on a Rational Approach No disclosures No conflicts of interest Christopher D. Owens, MD Objectives Changing face of our patients presenting
Managing Conditions Resulting from Untreated Cardiometabolic Syndrome
 Managing Conditions Resulting from Untreated Cardiometabolic Syndrome Matthew P. Namanny DO, FACOS Vascular/Endovascular Surgery Saguaro Surgical/AZ Vascular Specialist Tucson Medical Center Critical Limb
Managing Conditions Resulting from Untreated Cardiometabolic Syndrome Matthew P. Namanny DO, FACOS Vascular/Endovascular Surgery Saguaro Surgical/AZ Vascular Specialist Tucson Medical Center Critical Limb
Maximally Invasive Vascular Surgery for the Treatment of Critical Limb Ischemia
 Maximally Invasive Vascular Surgery for the Treatment of Critical Limb Ischemia Traci A. Kimball, MD Department of Surgery Grand Rounds Septemember 13, 2010 Overview Defining Critical Limb Ischemia Epidemiology
Maximally Invasive Vascular Surgery for the Treatment of Critical Limb Ischemia Traci A. Kimball, MD Department of Surgery Grand Rounds Septemember 13, 2010 Overview Defining Critical Limb Ischemia Epidemiology
Interventional Treatment First for CLI
 Interventional Treatment First for CLI Patrick Alexander, MD, FACC, FSCAI Interventional Cardiology Medical Director, Critical Limb Clinic Providence Heart Institute, Southfield MI 48075 Disclosures Consultant
Interventional Treatment First for CLI Patrick Alexander, MD, FACC, FSCAI Interventional Cardiology Medical Director, Critical Limb Clinic Providence Heart Institute, Southfield MI 48075 Disclosures Consultant
Pedal Bypass With Deep Venous Arterialization:
 Pedal Bypass With Deep Venous Arterialization: Long Term Result For Critical Limb Ischemia With Unreconstructable Distal Arteries Pramook Mutirangura Professor of Vascular Surgery Faculty of Medicine Siriraj
Pedal Bypass With Deep Venous Arterialization: Long Term Result For Critical Limb Ischemia With Unreconstructable Distal Arteries Pramook Mutirangura Professor of Vascular Surgery Faculty of Medicine Siriraj
The ZILVERPASS study a randomized study comparing ZILVER PTX stenting with Bypass in femoropopliteal lesions
 The ZILVERPASS study a randomized study comparing ZILVER PTX stenting with Bypass in femoropopliteal lesions Dr. Sven Bräunlich Department of Angiology University-Hospital Leipzig, Germany Disclosure Speaker
The ZILVERPASS study a randomized study comparing ZILVER PTX stenting with Bypass in femoropopliteal lesions Dr. Sven Bräunlich Department of Angiology University-Hospital Leipzig, Germany Disclosure Speaker
Limb Salvage in Diabetic Ischemic Foot. Kritaya Kritayakirana, MD, FACS Assistant Professor Chulalongkorn University April 30, 2017
 Limb Salvage in Diabetic Ischemic Foot Kritaya Kritayakirana, MD, FACS Assistant Professor Chulalongkorn University April 30, 2017 Case Male 67 years old Underlying DM, HTN, TVD Present with gangrene
Limb Salvage in Diabetic Ischemic Foot Kritaya Kritayakirana, MD, FACS Assistant Professor Chulalongkorn University April 30, 2017 Case Male 67 years old Underlying DM, HTN, TVD Present with gangrene
Femoropopliteal Above-Knee Bypass: The True Results
 Femoropopliteal Above-Knee Bypass: The True Results Lise Pyndt Jørgensen, Camilla Rasmussen & Torben V Schroeder Rigshospitalet and University of Copenhagen, DENMARK Treatment options in the femoropopliteal
Femoropopliteal Above-Knee Bypass: The True Results Lise Pyndt Jørgensen, Camilla Rasmussen & Torben V Schroeder Rigshospitalet and University of Copenhagen, DENMARK Treatment options in the femoropopliteal
Endovascular Should Be Considered First Line Therapy
 Revascularization of Patients with Critical Limb Ischemia Endovascular Should Be Considered First Line Therapy Michael Conte David Dawson David L. Dawson, MD Revised Presentation Title A Selective Approach
Revascularization of Patients with Critical Limb Ischemia Endovascular Should Be Considered First Line Therapy Michael Conte David Dawson David L. Dawson, MD Revised Presentation Title A Selective Approach
Global Vascular Guideline on the Management of Chronic Limb Threatening Ischemia -a new foundation for evidence-based care
 Global Vascular Guideline on the Management of Chronic Limb Threatening Ischemia -a new foundation for evidence-based care Michael S. Conte MD Professor and Chief, Division of Vascular and Endovascular
Global Vascular Guideline on the Management of Chronic Limb Threatening Ischemia -a new foundation for evidence-based care Michael S. Conte MD Professor and Chief, Division of Vascular and Endovascular
Update on Tack Optimized Balloon Angioplasty (TOBA) Below the Knee. Marianne Brodmann, MD Medical University Graz Graz, Austria
 Below the Knee. Marianne Brodmann, MD Medical University Graz Graz, Austria") Update on Tack Optimized Balloon Angioplasty (TOBA) Below the Knee Marianne Brodmann, MD Medical University Graz Graz, Austria Critical Limb Ischemia Infrapopliteal arterial disease is a leading source
Update on Tack Optimized Balloon Angioplasty (TOBA) Below the Knee Marianne Brodmann, MD Medical University Graz Graz, Austria Critical Limb Ischemia Infrapopliteal arterial disease is a leading source
Specificities for infrapopliteal stents
 Specificities for infrapopliteal stents Nicolas Diehm, M.D. Swiss Cardiovascular Center Clinical and Interventional Angiology University Hospital Bern, Switzerland Disclosures Speaker`s Bureau: MEDRAD,
Specificities for infrapopliteal stents Nicolas Diehm, M.D. Swiss Cardiovascular Center Clinical and Interventional Angiology University Hospital Bern, Switzerland Disclosures Speaker`s Bureau: MEDRAD,
Practical Point in Diabetic Foot Care 3-4 July 2017
 Diabetic Foot Ulcer : Role of Vascular Surgeon Practical Point in Diabetic Foot Care 3-4 July 2017 Supapong Arworn, MD Division of Vascular and Endovascular Surgery Department of Surgery, Chiang Mai University
Diabetic Foot Ulcer : Role of Vascular Surgeon Practical Point in Diabetic Foot Care 3-4 July 2017 Supapong Arworn, MD Division of Vascular and Endovascular Surgery Department of Surgery, Chiang Mai University
Intervention for Lower Extremity PAD: When, why and what?! Robert F Cuff, MD FACS RVT RPVI
 Intervention for Lower Extremity PAD: When, why and what?! Robert F Cuff, MD FACS RVT RPVI 1 Disclosures I have no financial disclosures related to this talk Objectives 1. Discuss indications for intervention
Intervention for Lower Extremity PAD: When, why and what?! Robert F Cuff, MD FACS RVT RPVI 1 Disclosures I have no financial disclosures related to this talk Objectives 1. Discuss indications for intervention
Popliteal Aneurysm: When is surgical therapy indicated? PROF. GRZEGORZ OSZKINIS
 Popliteal Aneurysm: When is surgical therapy indicated? PROF. GRZEGORZ OSZKINIS Asymptomatic mass - 38-40%will develop symptoms at a rate of 14%/yr Intermittent claudic ation (chronic ischemia) - 25%-40%
Popliteal Aneurysm: When is surgical therapy indicated? PROF. GRZEGORZ OSZKINIS Asymptomatic mass - 38-40%will develop symptoms at a rate of 14%/yr Intermittent claudic ation (chronic ischemia) - 25%-40%
PATIENT SPECIFIC STRATEGIES IN CRITICAL LIMB ISCHEMIA. Dr. Manar Trab Consultant Vascular Surgeon European Vascular Clinic DMCC Dubai, UAE
 PATIENT SPECIFIC STRATEGIES IN CRITICAL LIMB ISCHEMIA Dr. Manar Trab Consultant Vascular Surgeon European Vascular Clinic DMCC Dubai, UAE Disclosure Speaker name: DR. Manar Trab I have the following potential
PATIENT SPECIFIC STRATEGIES IN CRITICAL LIMB ISCHEMIA Dr. Manar Trab Consultant Vascular Surgeon European Vascular Clinic DMCC Dubai, UAE Disclosure Speaker name: DR. Manar Trab I have the following potential
DCB in my practice: How the evidence influences my strategy. Yang-Jin Park
 DCB in my practice: How the evidence influences my strategy Yang-Jin Park Associate Professor Division of Vascular Surgery, Department of Surgery Samsung Medical Center Sungkyunkwan University School of
DCB in my practice: How the evidence influences my strategy Yang-Jin Park Associate Professor Division of Vascular Surgery, Department of Surgery Samsung Medical Center Sungkyunkwan University School of
9/7/2018. Disclosures. CV and Limb Events in PAD. Challenges to Revascularization. Challenges. Answering the Challenge
 Disclosures State-of-the-Art Endovascular Lower Extremity Revascularization Promotional Speaker Jansen Pharmaceutical Promotional Speaker Amgen Pharmaceutical C. Michael Brown, MD, FACC al Cardiology Associate
Disclosures State-of-the-Art Endovascular Lower Extremity Revascularization Promotional Speaker Jansen Pharmaceutical Promotional Speaker Amgen Pharmaceutical C. Michael Brown, MD, FACC al Cardiology Associate
Management of In-stent Restenosis after Lower Extremity Endovascular Procedures
 Management of In-stent Restenosis after Lower Extremity Endovascular Procedures Piotr Sobieszczyk, MD Associate Director, Cardiac Catheterization Laboratory Cardiovascular Division and Vascular Medicine
Management of In-stent Restenosis after Lower Extremity Endovascular Procedures Piotr Sobieszczyk, MD Associate Director, Cardiac Catheterization Laboratory Cardiovascular Division and Vascular Medicine
Diagnosis and Endovascular Treatment of Critical Limb Ischemia: What You Need to Know S. Jay Mathews, MD, MS, FACC
 Diagnosis and Endovascular Treatment of Critical Limb Ischemia: What You Need to Know S. Jay Mathews, MD, MS, FACC Interventional Cardiologist/Endovascular Specialist Bradenton Cardiology Center Bradenton,
Diagnosis and Endovascular Treatment of Critical Limb Ischemia: What You Need to Know S. Jay Mathews, MD, MS, FACC Interventional Cardiologist/Endovascular Specialist Bradenton Cardiology Center Bradenton,
Imaging Strategy For Claudication
 Who are the Debators? Imaging Strategy For Claudication Duplex Ultrasound Alone is Adequate to Select Patients for Endovascular Intervention - Pro: Dennis Bandyk MD No Disclosures PRO - Vascular Surgeon
Who are the Debators? Imaging Strategy For Claudication Duplex Ultrasound Alone is Adequate to Select Patients for Endovascular Intervention - Pro: Dennis Bandyk MD No Disclosures PRO - Vascular Surgeon
CLI Treatment Using Long and Scoring Balloons
 CLI Treatment Using Long and Scoring Balloons Robert Beasley, MD Director of Vascular and Interven3onal Radiology Mount Sinai Medical Center Miami Beach, FL Disclosures Consultant/Advisory Board: Abbott
CLI Treatment Using Long and Scoring Balloons Robert Beasley, MD Director of Vascular and Interven3onal Radiology Mount Sinai Medical Center Miami Beach, FL Disclosures Consultant/Advisory Board: Abbott
Current Vascular and Endovascular Management in Diabetic Vasculopathy
 Current Vascular and Endovascular Management in Diabetic Vasculopathy Yang-Jin Park Associate professor Vascular Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine Peripheral artery
Current Vascular and Endovascular Management in Diabetic Vasculopathy Yang-Jin Park Associate professor Vascular Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine Peripheral artery
Use of Laser In BTK Disease (CLI)
") Use of Laser In BTK Disease (CLI) Click to edit academic affiliation, practice or hospital logo(s) of preference. Product and/or sponsor logos not permitted, per CME guidelines. Richard Kovach, MD, FACC,
Use of Laser In BTK Disease (CLI) Click to edit academic affiliation, practice or hospital logo(s) of preference. Product and/or sponsor logos not permitted, per CME guidelines. Richard Kovach, MD, FACC,
Endovascular treatment of infrapopliteal arteries: angioplasty vs stent in the drug-eluting era
 Eur Radiol (2014) 24:793 798 DOI 10.1007/s00330-014-3094-0 VASCULAR-INTERVENTIONAL Endovascular treatment of infrapopliteal arteries: angioplasty vs stent in the drug-eluting era Fabrizio Fanelli & Alessandro
Eur Radiol (2014) 24:793 798 DOI 10.1007/s00330-014-3094-0 VASCULAR-INTERVENTIONAL Endovascular treatment of infrapopliteal arteries: angioplasty vs stent in the drug-eluting era Fabrizio Fanelli & Alessandro
GLOBAL VASCULAR GUIDELINES: A NEW PATHWAY FOR LIMB SALVAGE
 GLOBAL VASCULAR GUIDELINES: A NEW PATHWAY FOR LIMB SALVAGE Michael S. Conte MD Professor and Chief, Vascular and Endovascular Surgery Co-Director, Center for Limb Preservation Co-Director, Heart and Vascular
GLOBAL VASCULAR GUIDELINES: A NEW PATHWAY FOR LIMB SALVAGE Michael S. Conte MD Professor and Chief, Vascular and Endovascular Surgery Co-Director, Center for Limb Preservation Co-Director, Heart and Vascular
Critical Limb Ischemia A Collaborative Approach to Patient Care. Christopher LeSar, MD Vascular Institute of Chattanooga July 28, 2017
 Critical Limb Ischemia A Collaborative Approach to Patient Care Christopher LeSar, MD Vascular Institute of Chattanooga July 28, 2017 Surgeons idea Surgeons idea represents the final stage of peripheral
Critical Limb Ischemia A Collaborative Approach to Patient Care Christopher LeSar, MD Vascular Institute of Chattanooga July 28, 2017 Surgeons idea Surgeons idea represents the final stage of peripheral
Endovascular Is The Way To Go: Revascularize As Many Vessels As You Can
 Rafael Malgor, MD Assistant Professor of Surgery The University of Oklahoma, Tulsa Endovascular Is The Way To Go: Revascularize As Many Vessels As You Can Background Lower extremity anatomy (below the
Rafael Malgor, MD Assistant Professor of Surgery The University of Oklahoma, Tulsa Endovascular Is The Way To Go: Revascularize As Many Vessels As You Can Background Lower extremity anatomy (below the
Distal hybrids - an option in long SFA CTO accompanied by severely compromized crural runoff
 Distal hybrids - an option in long SFA CTO accompanied by severely compromized crural runoff P. Kuryanov, A. Lipin, A. Antropov, K. Atmadzas, A. Atmadzas, Y. Eminov, A. Borisov, R. Sobolev, A.Orlov Limb
Distal hybrids - an option in long SFA CTO accompanied by severely compromized crural runoff P. Kuryanov, A. Lipin, A. Antropov, K. Atmadzas, A. Atmadzas, Y. Eminov, A. Borisov, R. Sobolev, A.Orlov Limb
3-year results of the OLIVE registry:
 3-year results of the OLIVE registry: A prospective multicenter study in patients with critical limb ischemia Osamu Iida, MD Kansai Rosai Hospital Cardiovascular Center Amagasaki, Hyogo, Japan Disclosure
3-year results of the OLIVE registry: A prospective multicenter study in patients with critical limb ischemia Osamu Iida, MD Kansai Rosai Hospital Cardiovascular Center Amagasaki, Hyogo, Japan Disclosure
Critical Limb Ischemia: Diagnosis and Current Management
 Research Article Joseph Karam, MD Elliot J. Stephenson, MD From: Minneapolis Heart Institutet at Abbott Northwestern Hospital, Minneapolis, MN Address for correspondence: Joseph Karam, MD Minneapolis Heart
Research Article Joseph Karam, MD Elliot J. Stephenson, MD From: Minneapolis Heart Institutet at Abbott Northwestern Hospital, Minneapolis, MN Address for correspondence: Joseph Karam, MD Minneapolis Heart
Making BTK Interventions more Durable: Are DES and DCB the answer? Thomas Zeller, MD
 Making BTK Interventions more Durable: Are DES and DCB the answer? Thomas Zeller, MD Faculty Disclosure Thomas Zeller, MD For the 12 months preceding this presentation, I disclose the following types of
Making BTK Interventions more Durable: Are DES and DCB the answer? Thomas Zeller, MD Faculty Disclosure Thomas Zeller, MD For the 12 months preceding this presentation, I disclose the following types of
Robert W. Fincher, DO The Ritz-Carlton, Dove Mountain Marana, Arizona February 7th, 2015
 Robert W. Fincher, DO The Ritz-Carlton, Dove Mountain Marana, Arizona February 7th, 2015 Disclosure I have nothing to disclose Randomized Controlled Studies In SFA Technology: What s The Best Tool For
Robert W. Fincher, DO The Ritz-Carlton, Dove Mountain Marana, Arizona February 7th, 2015 Disclosure I have nothing to disclose Randomized Controlled Studies In SFA Technology: What s The Best Tool For
The ZILVERPASS study a randomized study comparing ZILVER PTX stenting with Bypass in femoropopliteal lesions Preliminary report
 The ZILVERPASS study a randomized study comparing ZILVER PTX stenting with Bypass in femoropopliteal lesions Preliminary report G. Biro, M. Bosiers on behalf of ZILVERPASS Study Group Disclosure Speaker
The ZILVERPASS study a randomized study comparing ZILVER PTX stenting with Bypass in femoropopliteal lesions Preliminary report G. Biro, M. Bosiers on behalf of ZILVERPASS Study Group Disclosure Speaker
Do the newest grafts achieve comparable results to saphenous vein bypass? THE HEPARIN-BONDED eptfe GRAFT. C. Pratesi
 Do the newest grafts achieve comparable results to saphenous vein bypass? THE HEPARIN-BONDED eptfe GRAFT C. Pratesi Department of Vascular Surgery University of Florence-Italy www.chirvasc-unifi.it FEMORO-POPLITEAL
Do the newest grafts achieve comparable results to saphenous vein bypass? THE HEPARIN-BONDED eptfe GRAFT C. Pratesi Department of Vascular Surgery University of Florence-Italy www.chirvasc-unifi.it FEMORO-POPLITEAL
Present & future of below the knee stenting
 Session 5 Below the knee arteries & limb salvage Present & future of below the knee stenting M. Bosiers K. Deloose P. Peeters 1 PRESENT Clinical perspective whom to treat CRITICAL LIMB ISCHEMIA (CLI) 0
Session 5 Below the knee arteries & limb salvage Present & future of below the knee stenting M. Bosiers K. Deloose P. Peeters 1 PRESENT Clinical perspective whom to treat CRITICAL LIMB ISCHEMIA (CLI) 0
Treatment Strategies For Patients with Peripheral Artery Disease
 Treatment Strategies For Patients with Peripheral Artery Disease Presented by Schuyler Jones, MD Duke University Medical Center & Duke Clinical Research Institute AHRQ Comparative Effectiveness Review
Treatment Strategies For Patients with Peripheral Artery Disease Presented by Schuyler Jones, MD Duke University Medical Center & Duke Clinical Research Institute AHRQ Comparative Effectiveness Review
Surgical Bypass or. Zilver PTX. 12 months preliminary data. LINC 2016, Leipzig. Marc Bosiers, MD. Marc Bosiers Koen Deloose Joren Callaert
 LINC 2016, Leipzig Surgical Bypass or A.Z. Sint-Blasius, Dendermonde Marc Bosiers Koen Deloose Joren Callaert Imelda Hospital, Bonheiden Patrick Peeters Jürgen Verbist Wouter Van den Eynde OLV Hospital,
LINC 2016, Leipzig Surgical Bypass or A.Z. Sint-Blasius, Dendermonde Marc Bosiers Koen Deloose Joren Callaert Imelda Hospital, Bonheiden Patrick Peeters Jürgen Verbist Wouter Van den Eynde OLV Hospital,
Disclosures. In-Stent Restenosis: The Tail IS Wagging the Dog 4/15/2016. Restenosis: The Continuing Challenge for Peripheral Vascular Intervention
 In-Stent Restenosis: The Tail IS Wagging the Dog Disclosures NONE Michael S. Conte MD Division of Vascular and Endovascular Surgery UCSF Heart and Vascular Center UCSF Vascular Symposium 2016 IF YOU WERE
In-Stent Restenosis: The Tail IS Wagging the Dog Disclosures NONE Michael S. Conte MD Division of Vascular and Endovascular Surgery UCSF Heart and Vascular Center UCSF Vascular Symposium 2016 IF YOU WERE
Current Status and Limitations in the Treatment of Femoropopliteal In-Stent Restenosis
 Current Status and Limitations in the Treatment of Femoropopliteal In-Stent Restenosis Osamu Iida, MD From the Kansai Rosai Hospital Cardiovascular Center, Amagasaki City, Japan. ABSTRACT: Approximately
Current Status and Limitations in the Treatment of Femoropopliteal In-Stent Restenosis Osamu Iida, MD From the Kansai Rosai Hospital Cardiovascular Center, Amagasaki City, Japan. ABSTRACT: Approximately
Are DES and DEB worth the cost in BTK interventions?
 Are DES and DEB worth the cost in BTK interventions? Thomas Zeller, MD University Heart-Center Freiburg-Bad Krozingen Bad Krozingen, Germany -1- My Disclosures: Advisory Board: Medtronic-Invatec, Gore,
Are DES and DEB worth the cost in BTK interventions? Thomas Zeller, MD University Heart-Center Freiburg-Bad Krozingen Bad Krozingen, Germany -1- My Disclosures: Advisory Board: Medtronic-Invatec, Gore,
Aggressive BTK Revascularization and Advanced Wound Care - Patient Specific Therapy Concepts
 Aggressive BTK Revascularization and Advanced Wound Care - Patient Specific Therapy Concepts Dr Steven Kum MBBS MMed FRCS FAMS Vascular & Endovascular Surgeon Vascular Centre Department of Surgery Changi
Aggressive BTK Revascularization and Advanced Wound Care - Patient Specific Therapy Concepts Dr Steven Kum MBBS MMed FRCS FAMS Vascular & Endovascular Surgeon Vascular Centre Department of Surgery Changi
Forget about the angiosome theories. Yann Gouëffic, MD, PhD Department of vascular surgery, institut du thorax, Nantes, France
 Forget about the angiosome theories Yann Gouëffic, MD, PhD Department of vascular surgery, institut du thorax, Nantes, France Disclosure of Interest Research grants /Consulting/Honoraria for - Abbott -
Forget about the angiosome theories Yann Gouëffic, MD, PhD Department of vascular surgery, institut du thorax, Nantes, France Disclosure of Interest Research grants /Consulting/Honoraria for - Abbott -
Remote Endarterectomy Update
 Remote Endarterectomy Update An endovascular alternative to bypass? BY JOHN D. MARTIN, MD Treating the superficial femoral artery (SFA) is still one of the most highly debated topics among vascular specialists.
Remote Endarterectomy Update An endovascular alternative to bypass? BY JOHN D. MARTIN, MD Treating the superficial femoral artery (SFA) is still one of the most highly debated topics among vascular specialists.
Angiosome revascularization strategies in real world practice: how much difference does it make?
 Angiosome revascularization strategies in real world practice: how much difference does it make? Peter A. Schneider, MD Kaiser Foundation Hospital Honolulu, Hawaii Disclosure Peter A. Schneider... I have
Angiosome revascularization strategies in real world practice: how much difference does it make? Peter A. Schneider, MD Kaiser Foundation Hospital Honolulu, Hawaii Disclosure Peter A. Schneider... I have
Clinical use and safety of the Lutonix DCB for the treatment of BTK: interim data from a prospective registry
 Clinical use and safety of the Lutonix DCB for the treatment of BTK: interim data from a prospective registry Alexander Zimmermann Department of Vascular and Endovascular Surgery Klinikum rechts der Isar
Clinical use and safety of the Lutonix DCB for the treatment of BTK: interim data from a prospective registry Alexander Zimmermann Department of Vascular and Endovascular Surgery Klinikum rechts der Isar
Intercepting PAD. Playbook for Cardiovascular Care 2018 February 24, Jonathan D Woody, MD, FACS. University Surgical Vascular
 Intercepting PAD Playbook for Cardiovascular Care 2018 February 24, 2018 Jonathan D Woody, MD, FACS University Surgical Vascular Attending Vascular Surgeon - Piedmont Athens Regional Adjunct Clinical Associate
Intercepting PAD Playbook for Cardiovascular Care 2018 February 24, 2018 Jonathan D Woody, MD, FACS University Surgical Vascular Attending Vascular Surgeon - Piedmont Athens Regional Adjunct Clinical Associate
Clinical and morphological features of patients who underwent endovascular interventions for lower extremity arterial occlusive diseases
 Original paper Clinical and morphological features of patients who underwent endovascular interventions for lower extremity arterial occlusive diseases Sakir Arslan, Isa Oner Yuksel, Erkan Koklu, Goksel
Original paper Clinical and morphological features of patients who underwent endovascular interventions for lower extremity arterial occlusive diseases Sakir Arslan, Isa Oner Yuksel, Erkan Koklu, Goksel
Recent Advances in Peripheral Salvage
 Recent Advances in Peripheral Salvage Dr Shaiful Azmi Yahaya, MD, MMed, FNHAM, FAsCC, FAPSIC Consultant Cardiologist and Peripheral Interventionist, Institut Jantung Negara Disclosure I am proctoring for
Recent Advances in Peripheral Salvage Dr Shaiful Azmi Yahaya, MD, MMed, FNHAM, FAsCC, FAPSIC Consultant Cardiologist and Peripheral Interventionist, Institut Jantung Negara Disclosure I am proctoring for
Easy. Not so Easy. Risk Assessment in the CLI Patient: Who is Likely to Benefit from Revascularization and Who is Not? 4/28/2012
 Risk Assessment in the CLI Patient: Who is Likely to Benefit from Revascularization and Who is Not? Easy 89 yo Non-ambulatory Multiple failed interventions Forefoot and heel gangrene Andres Schanzer, MD
Risk Assessment in the CLI Patient: Who is Likely to Benefit from Revascularization and Who is Not? Easy 89 yo Non-ambulatory Multiple failed interventions Forefoot and heel gangrene Andres Schanzer, MD
Fabrizio Fanelli, MD, EBIR Director Vascular and Interventional Radiology Department "Careggi " University Hospital Florence - Italy
 Don t Use Risky and Embolizing Drug Coated Balloons Below The Knee! Fabrizio Fanelli, MD, EBIR Director Vascular and Interventional Radiology Department "Careggi " University Hospital Florence - Italy
Don t Use Risky and Embolizing Drug Coated Balloons Below The Knee! Fabrizio Fanelli, MD, EBIR Director Vascular and Interventional Radiology Department "Careggi " University Hospital Florence - Italy
Angiosome concept myth or truth? Does it make a real difference in real world cases?
 Angiosome concept myth or truth? Does it make a real difference in real world cases? Osamu Iida, MD, FACC Kansai Rosai Hospital Amagasaki, Hyogo, Japan Disclosure Speaker name:... I have the following
Angiosome concept myth or truth? Does it make a real difference in real world cases? Osamu Iida, MD, FACC Kansai Rosai Hospital Amagasaki, Hyogo, Japan Disclosure Speaker name:... I have the following
SPINACH Making Limb Salvage Salad from Spinach alone
 SPINACH Making Limb Salvage Salad from Spinach alone Surgical reconstruction versus Peripheral Intervention in patients with critical limb ischemia prospective multicenter registry in Japan Nobuyoshi Azuma,
SPINACH Making Limb Salvage Salad from Spinach alone Surgical reconstruction versus Peripheral Intervention in patients with critical limb ischemia prospective multicenter registry in Japan Nobuyoshi Azuma,
Peripheral Artery Disease Interventions Utilizing the Angiosomal Approach to the Complex Wound
 Peripheral Artery Disease Interventions Utilizing the Angiosomal Approach to the Complex Wound Craig M. Walker, MD, FACC, FACP Chairman, New Cardiovascular Horizons Clinical Professor of Medicine Tulane
Peripheral Artery Disease Interventions Utilizing the Angiosomal Approach to the Complex Wound Craig M. Walker, MD, FACC, FACP Chairman, New Cardiovascular Horizons Clinical Professor of Medicine Tulane
TOBA II 12-Month Results Tack Optimized Balloon Angioplasty
 TOBA II 12-Month Results Tack Optimized Balloon Angioplasty William Gray, MD System Chief, Cardiovascular Division Main Line Health, Philadelphia, PA Dissection: The Primary Mechanism of Angioplasty Lesions
TOBA II 12-Month Results Tack Optimized Balloon Angioplasty William Gray, MD System Chief, Cardiovascular Division Main Line Health, Philadelphia, PA Dissection: The Primary Mechanism of Angioplasty Lesions
Retrograde Endovascular Revascularization of Anterior Tibial Artery via the Dorsal and Plantar Arches
 Case Reportc imedpub Journals www.imedpub.com Journal of Vascular and Endovascular Surgery DOI: 10.21767/2573-4482.100020 Retrograde Endovascular Revascularization of Anterior Tibial Artery via the Dorsal
Case Reportc imedpub Journals www.imedpub.com Journal of Vascular and Endovascular Surgery DOI: 10.21767/2573-4482.100020 Retrograde Endovascular Revascularization of Anterior Tibial Artery via the Dorsal
4/23/2009. Vein Bypass Remains the Gold Standard AND We Can Improve Outcomes. Lower Extremity Revascularization Options: Key Factors to Consider
 Vein Bypass Remains the Gold Standard AND We Can Improve Outcomes Lower Extremity Revascularization Options: Key Factors to Consider General health of the patient Michael S. Conte MD Division of Vascular
Vein Bypass Remains the Gold Standard AND We Can Improve Outcomes Lower Extremity Revascularization Options: Key Factors to Consider General health of the patient Michael S. Conte MD Division of Vascular
Clinical Data Update for Drug Coated Balloons (DCB) Seung-Whan Lee, MD, PhD
 Seung-Whan Lee, MD, PhD") Clinical Data Update for Drug Coated Balloons (DCB) Seung-Whan Lee, MD, PhD Asan Medical Center, Heart Institute, University of Ulsan College of Medicine, Werk et al. Circulation Cardiovasc Intervent 2012
Clinical Data Update for Drug Coated Balloons (DCB) Seung-Whan Lee, MD, PhD Asan Medical Center, Heart Institute, University of Ulsan College of Medicine, Werk et al. Circulation Cardiovasc Intervent 2012
Atherectomy is Still Live and Effective. John R. Laird, MD Professor of Medicine Medical Director of the Vascular Center UC Davis Health System
 Atherectomy is Still Live and Effective John R. Laird, MD Professor of Medicine Medical Director of the Vascular Center UC Davis Health System Why is Atherectomy Still Alive? Improved devices Better data
Atherectomy is Still Live and Effective John R. Laird, MD Professor of Medicine Medical Director of the Vascular Center UC Davis Health System Why is Atherectomy Still Alive? Improved devices Better data
Boca Raton Regional Hospital Grand Rounds September 13, 2016
 Boca Raton Regional Hospital Grand Rounds September 13, 2016 W. Anthony Lee, MD, FACS Chief, BocaCare Vascular Surgery Christine E. Lynn Heart and Vascular Institute Boca Raton, Florida Disclosures No
Boca Raton Regional Hospital Grand Rounds September 13, 2016 W. Anthony Lee, MD, FACS Chief, BocaCare Vascular Surgery Christine E. Lynn Heart and Vascular Institute Boca Raton, Florida Disclosures No
Cutting/scoring balloon Cryoplasty Drug-eluting balloon Brachytherapy Debulking Restent (BMS or DES) John R. Laird, MD
 John R. Laird, MD") Current Treatment of Femoropopliteal Instent Restenosis Professor of Medicine Medical Director of the Vascular Center UC Davis Medical Center SFA In-stent Restenosis Common: 18%- 40% at 12 months in recent
Current Treatment of Femoropopliteal Instent Restenosis Professor of Medicine Medical Director of the Vascular Center UC Davis Medical Center SFA In-stent Restenosis Common: 18%- 40% at 12 months in recent
IMPORTANT INFORMATION: These materials are intended to describe common clinical considerations and procedural steps for the on-label use of
 IMPORTANT INFORMATION: These materials are intended to describe common clinical considerations and procedural steps for the on-label use of referenced technologies as well as current standards of care
IMPORTANT INFORMATION: These materials are intended to describe common clinical considerations and procedural steps for the on-label use of referenced technologies as well as current standards of care
The Final Triumph Of Endovascular Therapy In SFA Treatment
 The Final Triumph Of Endovascular Therapy In SFA Treatment MEET 07 Mark W. Mewissen, M.D. Director, St Lukes Vascular Center Milwaukee, WI Endovascular Therapy In SFA Treatment: Works In Progress! Mark
The Final Triumph Of Endovascular Therapy In SFA Treatment MEET 07 Mark W. Mewissen, M.D. Director, St Lukes Vascular Center Milwaukee, WI Endovascular Therapy In SFA Treatment: Works In Progress! Mark
BEST-CLI Trial Study Concept and Current Status
 BEST-CLI Trial Study Concept and Current Status Kenneth Rosenfield, MD, MHCDS National Co-PI BEST-CLI Trial Section Head, Vascular Medicine and Intervention Institute for Heart, Vascular, and Stroke Care
BEST-CLI Trial Study Concept and Current Status Kenneth Rosenfield, MD, MHCDS National Co-PI BEST-CLI Trial Section Head, Vascular Medicine and Intervention Institute for Heart, Vascular, and Stroke Care
Accurate Vessel Sizing Drives Clinical Results. IVUS In the Periphery
 Accurate Vessel Sizing Drives Clinical Results IVUS In the Periphery Discussion Iida O, et. al. Study Efficacy of Intravascular Ultrasound in Femoropopliteal Stenting for Peripheral Artery Disease With
Accurate Vessel Sizing Drives Clinical Results IVUS In the Periphery Discussion Iida O, et. al. Study Efficacy of Intravascular Ultrasound in Femoropopliteal Stenting for Peripheral Artery Disease With
Disclosures. In the DCB Era, How Do I Choose To Use a Stent? When to Stent and What Devices to Use in the SFA
 In the DCB Era, How Do I Choose To Use a Stent? When to Stent and What Devices to Use in the SFA Disclosures No financial disclosures. Cameron M. Akbari, MD, MBA, FACS Site Director, Vascular Surgery Medstar
In the DCB Era, How Do I Choose To Use a Stent? When to Stent and What Devices to Use in the SFA Disclosures No financial disclosures. Cameron M. Akbari, MD, MBA, FACS Site Director, Vascular Surgery Medstar
Introduction History Preceded by Arterial Doppler and ABI Indications
 Elise Brady, RVT, RDMS Introduction History Preceded by Arterial Doppler and ABI Indications 1) Abnormal ABI (within 2weeks of duplex) 2) Abnormal Doppler waveforms 3) Claudication 4) History of PVD 5)
Elise Brady, RVT, RDMS Introduction History Preceded by Arterial Doppler and ABI Indications 1) Abnormal ABI (within 2weeks of duplex) 2) Abnormal Doppler waveforms 3) Claudication 4) History of PVD 5)
Lessons & Perspectives: What is the role of Cryoplasty in SFA Intervention?
 Lessons & Perspectives: What is the role of Cryoplasty in SFA Intervention? Michael Wholey, MD, MBA San Antonio, TX USA 19/06/2009 at 09:35 during 4mn as a Speaker Session: Improving Femoral Artery Recanalization
Lessons & Perspectives: What is the role of Cryoplasty in SFA Intervention? Michael Wholey, MD, MBA San Antonio, TX USA 19/06/2009 at 09:35 during 4mn as a Speaker Session: Improving Femoral Artery Recanalization
Which Stent Is Best for Various Femoropopliteal Anatomy? 2018 Pacific Northwest Endovascular Conference June 15-26, 2018 Seattle, WA
 Which Stent Is Best for Various Femoropopliteal Anatomy? 2018 Pacific Northwest Endovascular Conference June 15-26, 2018 Seattle, WA Brian DeRubertis, MD, FACS Associate Professor of Surgery UCLA Division
Which Stent Is Best for Various Femoropopliteal Anatomy? 2018 Pacific Northwest Endovascular Conference June 15-26, 2018 Seattle, WA Brian DeRubertis, MD, FACS Associate Professor of Surgery UCLA Division
Konstantinos Katsanos, MSc, MD, PhD, EBIR. Consultant Interventional Radiologist Guy's and St.Thomas' Hospitals, NHS Foundation Trust
 Konstantinos Katsanos, MSc, MD, PhD, EBIR Consultant Interventional Radiologist Guy's and St.Thomas' Hospitals, NHS Foundation Trust King's Health Partners, London, United Kingdom Nothing to declare Anatomy
Konstantinos Katsanos, MSc, MD, PhD, EBIR Consultant Interventional Radiologist Guy's and St.Thomas' Hospitals, NHS Foundation Trust King's Health Partners, London, United Kingdom Nothing to declare Anatomy
The incidence of peripheral artery disease (PAD)
") Pharmacologic Options for Treating Restenosis The role of cilostazol in the treatment of patients with infrainguinal lesions. By Osamu Iida, MD, and Yoshimitsu Soga, MD The incidence of peripheral artery
Pharmacologic Options for Treating Restenosis The role of cilostazol in the treatment of patients with infrainguinal lesions. By Osamu Iida, MD, and Yoshimitsu Soga, MD The incidence of peripheral artery
V.A. is a 62-year-old male who presents in referral
 , LLC an HMP Communications Holdings Company Clinical Case Update Latest Trends in Critical Limb Ischemia Imaging Amit Srivastava, MD, FACC, FABVM Interventional Cardiologist Bay Area Heart Center St.
, LLC an HMP Communications Holdings Company Clinical Case Update Latest Trends in Critical Limb Ischemia Imaging Amit Srivastava, MD, FACC, FABVM Interventional Cardiologist Bay Area Heart Center St.
RevIewS. Interventions for lower extremity peripheral artery disease
 RevIewS Interventions for lower extremity peripheral artery disease Jade S. Hiramoto 1, Martin Teraa 2, Gert J. de Borst 2 and Michael S. Conte 1 * Abstract Peripheral artery disease (PAD) of the lower
RevIewS Interventions for lower extremity peripheral artery disease Jade S. Hiramoto 1, Martin Teraa 2, Gert J. de Borst 2 and Michael S. Conte 1 * Abstract Peripheral artery disease (PAD) of the lower
Always Contact a Vascular Interventional Specialist Before Amputating a Patient with Critical Limb Ischemia
 Cardiovasc Intervent Radiol (2010) 33:469 474 DOI 10.1007/s00270-009-9687-3 CLINICAL INVESTIGATION Always Contact a Vascular Interventional Specialist Before Amputating a Patient with Critical Limb Ischemia
Cardiovasc Intervent Radiol (2010) 33:469 474 DOI 10.1007/s00270-009-9687-3 CLINICAL INVESTIGATION Always Contact a Vascular Interventional Specialist Before Amputating a Patient with Critical Limb Ischemia
Peripheral Arterial Disease: the growing role of endovascular management
 Peripheral Arterial Disease: the growing role of endovascular management Poster No.: C-1931 Congress: ECR 2012 Type: Educational Exhibit Authors: E. M. C. Guedes Pinto, E. Rosado, D. Penha, P. Cabral,
Peripheral Arterial Disease: the growing role of endovascular management Poster No.: C-1931 Congress: ECR 2012 Type: Educational Exhibit Authors: E. M. C. Guedes Pinto, E. Rosado, D. Penha, P. Cabral,
Comparison Of Primary Long Stenting Versus Primary Short Stenting For Long Femoropopliteal Artery Disease (PARADE)
") Comparison Of Primary Long Stenting Versus Primary Short Stenting For Long Femoropopliteal Artery Disease (PARADE) Young-Guk Ko, M.D. Severance Cardiovascular Hospital, Yonsei University Health System,
Comparison Of Primary Long Stenting Versus Primary Short Stenting For Long Femoropopliteal Artery Disease (PARADE) Young-Guk Ko, M.D. Severance Cardiovascular Hospital, Yonsei University Health System,
Step by step Hybrid procedures in peripheral obstructive disease. Holger Staab, MD University Hospital Leipzig, Germany Clinic for Vascular Surgery
 Step by step Hybrid procedures in peripheral obstructive disease Holger Staab, MD University Hospital Leipzig, Germany Clinic for Vascular Surgery Disclosure Speaker name: H.H. Staab I have the following
Step by step Hybrid procedures in peripheral obstructive disease Holger Staab, MD University Hospital Leipzig, Germany Clinic for Vascular Surgery Disclosure Speaker name: H.H. Staab I have the following
Making the difference with Live Image Guidance
 Live Image Guidance 2D Perfusion Making the difference with Live Image Guidance In Peripheral Arterial Disease Real-time results, instant assessment Severe foot complications the result of hampered blood
Live Image Guidance 2D Perfusion Making the difference with Live Image Guidance In Peripheral Arterial Disease Real-time results, instant assessment Severe foot complications the result of hampered blood
Current Status of Endovascular Therapies for Critical Limb Ischemia
 Current Status of Endovascular Therapies for Critical Limb Ischemia Bulent Arslan, MD Associate Professor of Radiology Director, Vascular & Interventional Radiology Rush University Medical Center bulent_arslan@rush.edu
Current Status of Endovascular Therapies for Critical Limb Ischemia Bulent Arslan, MD Associate Professor of Radiology Director, Vascular & Interventional Radiology Rush University Medical Center bulent_arslan@rush.edu
Endovascular treatment (EVT) has markedly advanced,
 has markedly advanced,") Ann Vasc Dis Vol. 6, No. 3; 2013; pp 573 577 Online August 12, 2013 2013 Annals of Vascular Diseases doi:10.3400/avd.oa.13-00055 Original Article A Review of Surgically Treated Patients with Obstruction
Ann Vasc Dis Vol. 6, No. 3; 2013; pp 573 577 Online August 12, 2013 2013 Annals of Vascular Diseases doi:10.3400/avd.oa.13-00055 Original Article A Review of Surgically Treated Patients with Obstruction
Vasile Goldiş Western University of Arad Faculty of Medicine, Pharmacy and Dental Medicine, Arad, Romania
 ENDOVASCULAR TREATMENT FOR VASCULAR GRAFT RESTENOSIS Bogdan Totolici 1, Francisca Blanca Călinescu 1*, Ionel Droc 2, Carmen Neamţu 1 1 Vasile Goldiş Western University of Arad Faculty of Medicine, Pharmacy
ENDOVASCULAR TREATMENT FOR VASCULAR GRAFT RESTENOSIS Bogdan Totolici 1, Francisca Blanca Călinescu 1*, Ionel Droc 2, Carmen Neamţu 1 1 Vasile Goldiş Western University of Arad Faculty of Medicine, Pharmacy
Guidelines for Management of Peripheral Arterial Disease
 Guidelines for Management of Peripheral Arterial Disease Subhash Banerjee, MD, FACC, FSCAI Professor of Medicine, Univ. of Texas Southwestern Medical Center Chief, Division of Cardiology, VA North Texas
Guidelines for Management of Peripheral Arterial Disease Subhash Banerjee, MD, FACC, FSCAI Professor of Medicine, Univ. of Texas Southwestern Medical Center Chief, Division of Cardiology, VA North Texas