MODULE IV. Pediatric Trauma
|
|
|
- Marsha Rich
- 6 years ago
- Views:
Transcription
1 MODULE IV Pediatric Trauma
2 PRE-HOSPITAL HIGH RISK CRITERIA Blunt injury Significant injury; physiologic compromise Penetrating injuries Thorax, abdomen, head and neck High risk burns: > 10% second degree > 5% third degree Destination: specialized pediatric burn unit after stabilization onsite/initial facility
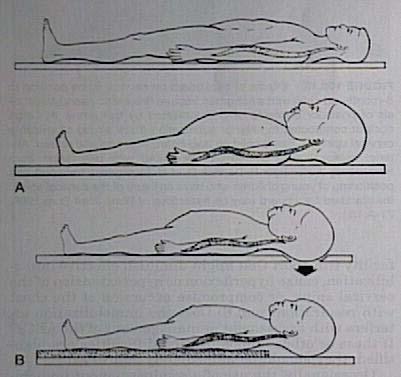
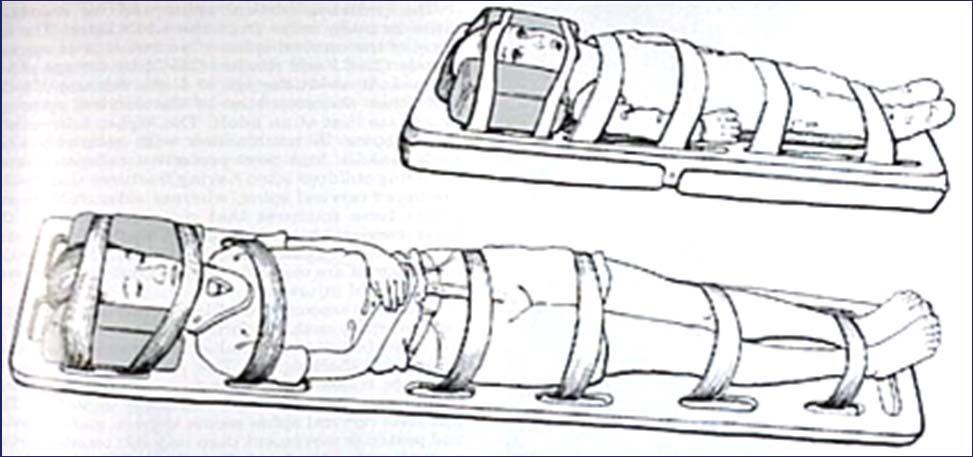
3 SCENE IMMOBILIZATION
4 TRAUMA PRIMARY SURVEY A - Airway patency B - Breathing and ventilation C - Circulation with hemorrhage control D - Disability: Mental status E - Exposure: Completely undress patient
5 A AIRWAY (PRIMARY SURVEY) Midline positioning Do jaw thrust to open airway and protect c-spine Head tilt and chin lift are contraindicated Cervical spine immobilization
6 CHILDREN AIRWAY: PRACTICAL CONSIDERATIONS Prominent occiput More secretions Relatively larger tongue Larger adenoids Softer cartilage Epiglottis omega-shaped in anterior position Subglottic region cone-shaped
7 Airway assessment in children Stable airway If it is possible to keep the airway open - Airway opening maneuvers - Devices: oral or nasal airway If it is NOT possible to keep the airway open - Bag-Valve-Mask (BVM) - Endotracheal tube (rapid sequence intubation) - Cricothyrotomy
8 B - BREATHING Assess minute ventilation Assess chest expansion Breath sounds Heart sounds Chest percussion

9 BAG-VALVE-MASK VENTILATION Midline position Open airway Proper sized mask Proper sized bag

10 C - CIRCULATION Assess pulse, end organ perfusion (capillary refill, temperature/appearance of extremities, CNS) and blood pressure Control external hemorrhage using direct pressure to wounds REMEMBER: Hypotension in children will not be evident until 25% to 30% of blood volume is lost. Begin aggressive fluid resuscitation immediately
11 D - DISABILITY Determine mental status with rapid assessment Is the child responsive? Pupil and motor exam AVPN evaluation: (Alert, responsive to Voice, responsive to Pain, Nonresponsive)



12 E - EXPOSURE Completely undress the patient Perform a complete examination Don t let the patient get cold Glucose, lab tests

13 Polytrauma: Secondary survey Vital signs assessment Head- to- toe examination Laboratory and radiologic studies Splinting fractures and applying wound dressings
14 No ACUTE RESPIRATORY FAILURE (ARF) Yes Tension pneumothorax Open pneumothorax Closed injury Drainage No Massive hemothorax Thoracic instability Persistent airway leakage or initial blood drainage > 20 ml/kg or > 2 ml/kg/h Persistent ARF Intubation and mechanical ventilation No Emergent surgery PERICARDIOCENTESIS Shock No Yes Cardiac tamponade No Secondary assessment Search cause of hemorrhage Laboratory tests and image studies: Chest Rx, ECG, others
15 SHOCK RELATED TO TRAUMA Classify Cause Hypovolemic Cardiogenic Obstructive Distributive Hemorrhage Burns Myocardial contusion Massive hemothorax Tension pneumothorax Tamponade Spinal cord injury
16 SHOCK TREATMENT Control external bleeding Líquids: Cristaloids 20 ml/kg NaCl 3% 10 ml/kg Coloids 5-10 ml/kg Red Cells desplasmatizados 10 ml/kg Blood 20 ml/kg If still unstable surgery

17 PEDIATRIC TRAUMA SCORE Pediatric trauma score


18 ASSESSMENT OF THE CERVICAL SPINE Severe or high-risk mechanism of injury Altered level of consciousness, less than 5 years old Immobilize Radiographic evaluation Neurologic abnormality at any time after injury Complaints of neck pain Cervical spine tenderness Limited or painful neck motion Consider clinical evaluation without radiographs
19 MANAGEMENT OF CERVICAL SPINE INJURIES The main goal is to avoid secondary injuries Total immobilization!!! And hospital referral
20 TRAUMATIC BRAIN / HEAD INJURY Primary injury - Blunt or penetrating - Concussion, cerebral contusion, diffuse axonal injury, intracranial hemorrhage ASSESSMENT: AVPN Secondary injury - Result of metabolic events - Cerebral ischemia, brain edema
 Vital")

21 CLINICAL ASSESSMENT OF SEVERITY TRAUMATIC BRAIN INJURY (TBI) Vital signs Level of consciousness (AVPN) Muscular strength/ tone Cranial nerve exam
22 TBI: MANAGEMENT Airway control Keep O 2 saturation > 95% Intubate if GCS 8 or if impossible to keep a stable airway Breathing Keep PCO mm Hg, unless there are clinical signs of cerebral hernia or neurological deterioration warranting a transitorily lower PCO 2 Circulation Start IV access Avoid hypotension: Use vasopressors to keep blood pressure once intravascular volume is recovered.
23 MANAGEMENT HEAD INJURY Maintain head in neutral position, use rigid cervical collar Administer short-term sedation and analgesia Midazolam (0.1 mg/kg) and Fentanyl (1-2 mcg/kg) If there are clinical signs of ICP Sedation, Mannitol (0.5-1 gm/kg), and hyperventilation (to PCO 2 of 25-30) until clinical signs improve Consider elevating the head of the bed 30 degrees Consider a foley and nasogastric tube
24 THORACIC INJURIES Pulmonary contusion/laceration (53%) Pneumothorax/hemothorax (38%) Rib/sternal fractures (36%) Other injuries Cardiac (5%) Diaphragm (2%) Major blood vessels (1%)
, hypercarbia (")
25 PULMONARY CONTUSION Most frequent injury Usually undetected! Pulmonary hematoma: Blood and fluid in the alveoli Hypoxemia ( PaO 2 ), hypercarbia ( Pa CO 2) Give oxygen 100%

26 PNEUMOTHORAX Simple vs Tension Tracheal shift Air into pleural space Loss of negative pressure Collapse of lung Open pneumothorax Occlusive dressing


27 HEMOTHORAX Blood accumulates in the pleural space Lung compression Type of injury Large pulmonary injury Large vessels injury Hypovolemia
28 PERICARDIAL TAMPONADE Beck s triad: narrow pulse pressure, neck vein distention, muffled heart tones Fluid in the pericardial sac Compresses heart and cardiac output Impairs venous return Arrhythmias Pericardiocentesis
29 ABDOMINAL INJURIES Third leading cause of death in children, after head and thoracic injuries Silent hypovolemia Solid organ vs hollow viscous Spleen most common Unique features of children s abdomen

30 BONE AND EXTREMITY INJURIES INITIAL MANAGEMENT Splint, splint, splint Clean and cover wound Different types of splints Splint distally and proximally to joint Pain management
31 FRACTURES THAT NEED ORTHOPEDIC REFERRAL Fractures that affect joints or growth plates Fractures around the elbow or knee Significant soft tissue swelling (compartment concern) Fractures associated with an open wound Fractures with signs of vascular or nerve disruption


32 OPEN FRACTURES Implies significant force - Look for other injuries Increased complications - Infections, nerve impingement Management - Clean, cover, do not suture - IV antibiotics, keep NPO, and immobilize Will need OR surgical debridement
33 PELVIC FRACTURES Associated with high energy accidents Blood loss can be significant Pelvic ring fracture: single fracture usually stable Multiple fractures: unstable Genitourinary injuries Abdominal injuries Vascular abnormalities (pelvic vein section)
34 BURN CLASSIFICATION Minor < 10% body surface area (BSA) second-degree, < 1% third-degree Moderate 10-30% BSA second-degree, 1-10% third-degree No hands, feet or genitalia Critical Inhalational injury > 30% BSA second-degree, > 10-20% third-degree Complicating fracture Extensive electric or chemical burns
35 BURNS MANAGEMENT Dilute and wash away offending chemicals Remove clothing Cover burns with clean dressing or sheet Prevents contamination, decreases pain Keep warm Give pain medications Replace fluids Rule of Nines >10% BSA in children IV vs. oral (may attempt up to 25%BSA)

36 RULE OF NINES
37 Surface of the palm
38 INHALATION INJURY The patient faints Fire or smoke present in a closed area Evidence of respiratory distress or upper airway obstruction Soot around the mouth or nose Singed eyebrows, eyelashes Burns around the face or neck Upper airway edema is commonly seen during the first 6 to 24 hours after injury Management: Remove the patient from the gas and allow him to breathe air or oxygen Keep airway open: Early obstruction of the upper airway is managed with intubation Oxygen 100%

39 CIRCUMFERENTIAL BURNS ESCHARECTOMY? Pain and color: unreliable Heat in extremity: good perfusion Remove tight clothing Elevate burned extremity Doppler pulse Indication of escharectomy: full thickness, circumferential burns in limbs and thorax
40 EXPLOSIONS AND BLAST INJURIES Bombs and explosives cause unique injuries Among survivors: Injuries include penetrating and blunt trauma Blast lung is the most common lethal injury Half of all initial casualties will seek medical care over a one-hour period Upside down triage triangle Initial patients: Less injured Later patients: More injured
41 BLAST INJURIES Primary mechanism: (Over-pressurization blast wave) Secondary mechanism: (Flying debris) Tertiary mechanism: (Blast wind throwing the individual) Affects air filled cavities (lungs, ears) Air embolism (stroke, acute abdomen, spinal cord injury) Penetrating or blunt injuries i.e. (eye injuries 10%) Fractures, brain injuries, traumatic amputations Miscellaneous: Burns, crush injuries, respiratory (dust/ toxins)

42 BLAST LUNG Over-pressurization wave Most common fatal injury Can be found 48 hours later Triad: apnea, bradycardia, hypotension Suspect if: dyspnea, cough, hemoptysis, CP, hypoxia. CXR: butterfly pattern
43 BLAST BRAIN INJURIES Severe head injury is a leading cause of death Subarachnoid, subdural hemorrhage most common (fatalities) Mild TBI s are common, but may be occult Signs and symptoms may be subtle Memory problems, headaches, dizziness, uneven gait, blurred vision, irritability, confusion
 Sensorineural disorder in the internal")
44 EXPLOSIONS EAR INJURIES They can be easily omitted Most common: perforation of tympanic membrane Rupture of the ossicular chain (33%) Sensorineural disorder in the internal ear
45 BLAST ABDOMINAL INJURY GI gas-containing structures Petechiae, hemorrhages, large intramural hematomas Severe overpressure leads to intestinal laceration, bowel perforation Colon: most common site of injury Ruptures may occur acutely several days after stretching, ischemia, and subsequent weakening of the bowel wall Tension pneumoperitoneum Ann Emerg Med 2001
46 CRUSH SYNDROME CAUSES OF DEATH Highly severe hypovolemic shock Metabolic and electrolitic disorders: Hyperkalemia, Hypocalcemia, Metabolic acidosis Acute myoglobinuric renal failure Compartment syndrome Treatment: massive volume replacement and alkaline solute (mannitol) diuresis Detection of metabolic abnormalities
47 COMPARTMENT SYNDROME Intracompartment pressure ischemia muscle necrosis and nerve palsies Anterior compartment of lower leg is the most frecuent Trauma does not have to be severe Severe trauma interrupts the compartment Pain, especially with passive extension Absent Pulse, Paresthesia, Pallor, Paralysis/Paresis Direct measurement of compartment pressure

48 Thank you!
1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D.
 1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D. Sacral-coccygeal 2. A 36-year-old male sustains blunt force thoracic
1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D. Sacral-coccygeal 2. A 36-year-old male sustains blunt force thoracic
3. D Objective: Chapter 4, Objective 4 Page: 79 Rationale: A carbon dioxide level below 35 mmhg indicates hyperventilation.
 1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
European Resuscitation Council
 European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
Emergency Room Resuscitation of the Unstable Trauma Patient
 Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
ITLS Pediatric Provider Course Advanced Pre-Test
 ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
Student Guide Module 4: Pediatric Trauma
 Student Guide Module 4: Pediatric Trauma Problem based learning exercise objectives Understand how to manage traumatic injuries in mass casualty events. Discuss the features and the approach to pediatric
Student Guide Module 4: Pediatric Trauma Problem based learning exercise objectives Understand how to manage traumatic injuries in mass casualty events. Discuss the features and the approach to pediatric
PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT
 PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT Board Approved June 2007 Revised December 2009 Revised July 2011 Revised June 2015 435 Hunter Street Fredericksburg, VA 22401
PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT Board Approved June 2007 Revised December 2009 Revised July 2011 Revised June 2015 435 Hunter Street Fredericksburg, VA 22401
Competency Log Professional Responder Courses
 Competency Log Professional Responder Courses Check off each competency once successfully demonstrated. This log may be used as a support tool when teaching a Professional Responder course. Refer to the
Competency Log Professional Responder Courses Check off each competency once successfully demonstrated. This log may be used as a support tool when teaching a Professional Responder course. Refer to the
ITLS Pediatric Provider Course Basic Pre-Test
 ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
Medical NREMT-PTE. NREMT Paramedic Trauma Exam.
 Medical NREMT-PTE NREMT Paramedic Trauma Exam https://killexams.com/pass4sure/exam-detail/nremt-pte Question: 41 Which of the following most accurately describes the finding of jugular venous distension
Medical NREMT-PTE NREMT Paramedic Trauma Exam https://killexams.com/pass4sure/exam-detail/nremt-pte Question: 41 Which of the following most accurately describes the finding of jugular venous distension
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials
 Preparatory Materials") Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
ITLS Advanced Pre-Test Annotated Key 8 th Edition
 1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
1. Which of the following organs is contained in the retroperitoneal region of the abdomen? A. Stomach B. Liver C. Kidney D.
 1. Which of the following organs is contained in the retroperitoneal region of the abdomen? A. Stomach B. Liver C. Kidney D. Uterus 2. What is Sellick's maneuver? A. A method allowing the rescuer to hold
1. Which of the following organs is contained in the retroperitoneal region of the abdomen? A. Stomach B. Liver C. Kidney D. Uterus 2. What is Sellick's maneuver? A. A method allowing the rescuer to hold
Emergency Care Progress Log
 Emergency Care Progress Log For further details on the National Occupational Competencies for EMRs, please visit www.paramedic.ca. Check off each skill once successfully demonstrated the Instructor. All
Emergency Care Progress Log For further details on the National Occupational Competencies for EMRs, please visit www.paramedic.ca. Check off each skill once successfully demonstrated the Instructor. All
Director, Burn Center MetroHealth Medical Center Professor of Surgery Case Western Reserve University
 Director, Burn Center MetroHealth Medical Center Professor of Surgery Case Western Reserve University BLAST INJURY Which of following statements concerning blast lung injury are FALSE? 1)Blast lung injury
Director, Burn Center MetroHealth Medical Center Professor of Surgery Case Western Reserve University BLAST INJURY Which of following statements concerning blast lung injury are FALSE? 1)Blast lung injury
5/2/2018. Notice. Putting Humpty Dumpty Back Together Again
 Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
ATLS: Initial Assessment and Management. SAUSHEC Medical Student Lecture Series
 ATLS: Initial Assessment and Management SAUSHEC Medical Student Lecture Series Objectives Identify sequence of priorities in assessing the multiply injured patient Apply principles outlined in primary
ATLS: Initial Assessment and Management SAUSHEC Medical Student Lecture Series Objectives Identify sequence of priorities in assessing the multiply injured patient Apply principles outlined in primary
Chapter 29 - Chest_and_Abdominal_Trauma
 Introduction to Emergency Medical Care 1 OBJECTIVES 29.1 Define key terms introduced in this chapter. Slides 11, 15, 18, 27 29.2 Describe mechanisms of injury commonly associated with chest injuries. Slides
Introduction to Emergency Medical Care 1 OBJECTIVES 29.1 Define key terms introduced in this chapter. Slides 11, 15, 18, 27 29.2 Describe mechanisms of injury commonly associated with chest injuries. Slides
Introduction to Emergency Medical Care 1
 Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
Basic Assessment and Treatment of Trauma
 Basic Assessment and Treatment of Trauma Final Exam Version 1 1. In which of the following scenarios would the potential for serious injury or death be the GREATEST? A. 77-kg (170-lb) man who falls 1.2
Basic Assessment and Treatment of Trauma Final Exam Version 1 1. In which of the following scenarios would the potential for serious injury or death be the GREATEST? A. 77-kg (170-lb) man who falls 1.2
Chapter 29 - Chest Injuries
 1 2 3 4 5 6 7 8 9 National EMS Education Standard Competencies (1 of 5) Trauma Applies fundamental knowledge to provide basic emergency care and transportation based on assessment findings for an acutely
1 2 3 4 5 6 7 8 9 National EMS Education Standard Competencies (1 of 5) Trauma Applies fundamental knowledge to provide basic emergency care and transportation based on assessment findings for an acutely
The immediate management of burns patients should be similar to management of trauma.
 CATS Clinical Guideline Burns The National Burn Care Review recommends that children with burns should be treated in a Burn Centre. Chelsea and Westminster may take non-ventilated children, Broomfield
CATS Clinical Guideline Burns The National Burn Care Review recommends that children with burns should be treated in a Burn Centre. Chelsea and Westminster may take non-ventilated children, Broomfield
You Are the Emergency Medical Responder
 Lesson 32: Injuries to the Chest, Abdomen and Genitalia You Are the Emergency Medical Responder Your police unit responds to a call in a part of town plagued by violence. When you arrive, you find the
Lesson 32: Injuries to the Chest, Abdomen and Genitalia You Are the Emergency Medical Responder Your police unit responds to a call in a part of town plagued by violence. When you arrive, you find the
2017 Northern Mine Rescue Contest Written Exam (First Aid Competition)
") 2017 Northern Mine Rescue Contest Written Exam (First Aid Competition) 2017 2010 June 5, 2017 Findley Lake, New York 2017 Northern Mine Rescue Contest Written Exam First Aid Competition Directions: Fill
2017 Northern Mine Rescue Contest Written Exam (First Aid Competition) 2017 2010 June 5, 2017 Findley Lake, New York 2017 Northern Mine Rescue Contest Written Exam First Aid Competition Directions: Fill
Pediatric Advanced Life Support
 Pediatric Advanced Life Support Pediatric Chain of Survival Berg M D et al. Circulation 2010;122:S862-S875 Prevention Early cardiopulmonary resuscitation (CPR) Prompt access to the emergency response system
Pediatric Advanced Life Support Pediatric Chain of Survival Berg M D et al. Circulation 2010;122:S862-S875 Prevention Early cardiopulmonary resuscitation (CPR) Prompt access to the emergency response system
Hypotension / Shock. Adult Medical Section Protocols. Protocol 30
 Hypotension / Shock History Blood loss - vaginal or gastrointestinal bleeding, AAA, ectopic Fluid loss - vomiting, diarrhea, fever nfection Cardiac ischemia (M, CHF) Medications Allergic reaction regnancy
Hypotension / Shock History Blood loss - vaginal or gastrointestinal bleeding, AAA, ectopic Fluid loss - vomiting, diarrhea, fever nfection Cardiac ischemia (M, CHF) Medications Allergic reaction regnancy
Pre-hospital Trauma Life Support. Rattiya Banjungam Emergency Physician, Khon Kaen Hospital
 Pre-hospital Trauma Life Support Rattiya Banjungam Emergency Physician, Khon Kaen Hospital Golden principles of Prehospital Trauma Care Golden Hour There is a golden hour if you are critically injured,
Pre-hospital Trauma Life Support Rattiya Banjungam Emergency Physician, Khon Kaen Hospital Golden principles of Prehospital Trauma Care Golden Hour There is a golden hour if you are critically injured,
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of
 Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
Chapter 26 Head and Spine Trauma The Nervous System The nervous system controls virtually all of our body activities including reflex, voluntary and
 1 2 3 4 5 Chapter 26 Head and Spine Trauma The Nervous System The nervous system controls virtually all of our body activities including reflex, voluntary and involuntary activities Voluntary activities
1 2 3 4 5 Chapter 26 Head and Spine Trauma The Nervous System The nervous system controls virtually all of our body activities including reflex, voluntary and involuntary activities Voluntary activities
Patient Assessment. Chapter 8
 Patient Assessment Chapter 8 Patient Assessment Scene size-up Initial assessment Focused history and physical exam Vital signs History Detailed physical exam Ongoing assessment Patient Assessment Process
Patient Assessment Chapter 8 Patient Assessment Scene size-up Initial assessment Focused history and physical exam Vital signs History Detailed physical exam Ongoing assessment Patient Assessment Process
Abdomen and Genitalia Injuries. Chapter 28
 Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
IMMEDIATE EMERGENCY BURN CARE » THERMAL BURNS » ELECTRICAL BURNS » CHEMICAL BURNS FIRST AID FOR THE THREE MAJOR CATEGORIES
 IMMEDIATE EMERGENCY BURN CARE 1. Treat according to BLS or ACLS Protocol 2. Use airway and C-Spine precautions. 3. Stop the burning process. FIRST AID FOR THE THREE MAJOR CATEGORIES» THERMAL BURNS + Stop
IMMEDIATE EMERGENCY BURN CARE 1. Treat according to BLS or ACLS Protocol 2. Use airway and C-Spine precautions. 3. Stop the burning process. FIRST AID FOR THE THREE MAJOR CATEGORIES» THERMAL BURNS + Stop
The Primary Survey. C. Clay Cothren, MD FACS. Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado
 The Primary Survey C. Clay Cothren, MD FACS Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado Outlining the ABCs Why do we need such an approach? The
The Primary Survey C. Clay Cothren, MD FACS Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado Outlining the ABCs Why do we need such an approach? The
EMS System for Metropolitan Oklahoma City and Tulsa 2019 Medical Control Board Treatment Protocols
 EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
PRE-HOSPITAL EMERGENCY CARE COURSE.
 PRE-HOSPITAL EMERGENCY CARE COURSE www.basics.org.uk Chest Assessment & Management BASICS Education March 2016 Objectives To understand the importance of oxygenation and ventilation To be able to describe
PRE-HOSPITAL EMERGENCY CARE COURSE www.basics.org.uk Chest Assessment & Management BASICS Education March 2016 Objectives To understand the importance of oxygenation and ventilation To be able to describe
Introduction (1 of 3)
") Chapter 10 Shock Introduction (1 of 3) Shock (hypoperfusion) means a state of collapse and failure of the cardiovascular system. In the early stages, the body attempts to maintain homeostasis. As shock
Chapter 10 Shock Introduction (1 of 3) Shock (hypoperfusion) means a state of collapse and failure of the cardiovascular system. In the early stages, the body attempts to maintain homeostasis. As shock
Combined CFRN and CTRN Detailed Content Outline
 Clinical items (primarily category, Assessment (15-20%), 1. General principles of transport nursing practice 19 31 A. Transport physiology 1. Physiologic stressors of transport 2. Effects of altitude on
Clinical items (primarily category, Assessment (15-20%), 1. General principles of transport nursing practice 19 31 A. Transport physiology 1. Physiologic stressors of transport 2. Effects of altitude on
CHEST TRAUMA. Dr Naeem Zia FCPS,FACS,FRCS
 CHEST TRAUMA Dr Naeem Zia FCPS,FACS,FRCS Learning objectives Anatomy of chest wall and thoracic viscera Physiology of respiration and nerve pathways for pain Enumerate different thoracic conditions requiring
CHEST TRAUMA Dr Naeem Zia FCPS,FACS,FRCS Learning objectives Anatomy of chest wall and thoracic viscera Physiology of respiration and nerve pathways for pain Enumerate different thoracic conditions requiring
The ABC s of Chest Trauma
 The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
Pediatric Shock. Hypovolemia. Sepsis. Most common cause of pediatric shock Small blood volumes (80cc/kg)
") Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
oriented evaluation of your patient and establishing priorities of care based on existing and
 1 Chapter 12: Patient Assessment in the Field 2 Patient assessment means conducting a - oriented evaluation of your patient and establishing priorities of care based on existing and potential threats to
1 Chapter 12: Patient Assessment in the Field 2 Patient assessment means conducting a - oriented evaluation of your patient and establishing priorities of care based on existing and potential threats to
Anesthesia for multiple trauma: from the scene to the OR
 Anesthesia for multiple trauma: from the scene to the OR Gary Hartstein,, M.D. Service d'anesthésie-réanimationsie-réanimation Service des Urgences CHU Liège B.35 4000 Liège Course outline philosophy of
Anesthesia for multiple trauma: from the scene to the OR Gary Hartstein,, M.D. Service d'anesthésie-réanimationsie-réanimation Service des Urgences CHU Liège B.35 4000 Liège Course outline philosophy of
Chest Trauma.
 Chest Trauma www.fisiokinesiterapia.biz Objectives Anatomy of Thorax Main Causes of Chest Injuries S/S of Chest Injuries Different Types of Chest Injuries Treatments of Chest Injuries Anatomy of the chest
Chest Trauma www.fisiokinesiterapia.biz Objectives Anatomy of Thorax Main Causes of Chest Injuries S/S of Chest Injuries Different Types of Chest Injuries Treatments of Chest Injuries Anatomy of the chest
Pediatric Trauma Practice. Guideline for Management of the Child in Shock. Background
 Pediatric Trauma Practice Guideline for Management of the Child in Shock Background Guideline for Management Trauma is the leading cause of death in children and adolescents in the United States. Although
Pediatric Trauma Practice Guideline for Management of the Child in Shock Background Guideline for Management Trauma is the leading cause of death in children and adolescents in the United States. Although
EMS System for Metropolitan Oklahoma City and Tulsa 2018 Medical Control Board Treatment Protocols
 EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
NOTE If it is necessary to perform abdominal thrusts, expose the abdominal area prior to pressing on the abdomen.
 ENABLING OBJECTIVES: 4.7 List the procedures used in a primary survey. 4.8 Demonstrate primary survey procedures used in a mock trauma (moulage) scenario without injury to personnel or damage to equipment.
ENABLING OBJECTIVES: 4.7 List the procedures used in a primary survey. 4.8 Demonstrate primary survey procedures used in a mock trauma (moulage) scenario without injury to personnel or damage to equipment.
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS
 CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS PRACTICAL STATIONS CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS 1. CARDIAC ARREST MANAGEMENT 2. AIRWAY & RESPIRATORY MANAGEMENT 3. SPINAL IMMOBILIZATION
CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS PRACTICAL STATIONS CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS 1. CARDIAC ARREST MANAGEMENT 2. AIRWAY & RESPIRATORY MANAGEMENT 3. SPINAL IMMOBILIZATION
The Primary Survey. Clay Cothren Burlew, MD FACS
 The Primary Survey Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Attending Surgeon, Denver Health Medical Center Associate Professor of Surgery, University of Colorado Outlining the
The Primary Survey Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Attending Surgeon, Denver Health Medical Center Associate Professor of Surgery, University of Colorado Outlining the
Pediatric Code Blue. Goals of Resuscitation. Focus Conference November Ensure organ perfusion
 Pediatric Code Blue Focus Conference November 2015 Duane C. Williams, MD Pediatric Critical Care Department of Pediatrics Children s Hospital of Richmond at VCU Goals of Resuscitation Ensure organ perfusion
Pediatric Code Blue Focus Conference November 2015 Duane C. Williams, MD Pediatric Critical Care Department of Pediatrics Children s Hospital of Richmond at VCU Goals of Resuscitation Ensure organ perfusion
Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH
 Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH Intended learning outcomes Describe the components of a comprehensive clinician
Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH Intended learning outcomes Describe the components of a comprehensive clinician
Aviation Rescue Swimmer Course
 Aviation Rescue Swimmer Course Primary Survey LT 5.4 December 2003 1 Objectives List the procedures used in a primary survey. Demonstrate primary survey procedures used in a mock trauma (moulage) scenario
Aviation Rescue Swimmer Course Primary Survey LT 5.4 December 2003 1 Objectives List the procedures used in a primary survey. Demonstrate primary survey procedures used in a mock trauma (moulage) scenario
1 Chapter 10 Shock 2 Shock Shock: Inadequate State of collapse and failure of the system Leads to inadequate circulation Without adequate blood flow,
 1 Chapter 10 Shock 2 Shock Shock: Inadequate State of collapse and failure of the system Leads to inadequate circulation Without adequate blood flow, cannot get rid of metabolic wastes Results in hypoperfusion
1 Chapter 10 Shock 2 Shock Shock: Inadequate State of collapse and failure of the system Leads to inadequate circulation Without adequate blood flow, cannot get rid of metabolic wastes Results in hypoperfusion
Advanced Assessment and Treatment of Trauma
 Advanced Assessment and Treatment of Trauma Final Exam Version 1 1. In which of the following scenarios would the potential for serious injury or death be the GREATEST? A. 77-kg (170-lb) man who falls
Advanced Assessment and Treatment of Trauma Final Exam Version 1 1. In which of the following scenarios would the potential for serious injury or death be the GREATEST? A. 77-kg (170-lb) man who falls
OUTLINE SHEET 5.4 PRIMARY SURVEY
 ENABLING OBJECTIVES: 4.7 List the procedures used in a primary survey. 4.8 Demonstrate primary survey procedures used in a mock trauma (moulage) scenario without injury to personnel or damage to equipment.
ENABLING OBJECTIVES: 4.7 List the procedures used in a primary survey. 4.8 Demonstrate primary survey procedures used in a mock trauma (moulage) scenario without injury to personnel or damage to equipment.
Introduction to Advanced Trauma Life Support ATLS
 Introduction to Advanced Trauma Life Support ATLS Objectives Concepts of primary & secondary survey Priorities & Life threatening conditions Clinical & Surgical skills Basic knowledge Rapid assessment
Introduction to Advanced Trauma Life Support ATLS Objectives Concepts of primary & secondary survey Priorities & Life threatening conditions Clinical & Surgical skills Basic knowledge Rapid assessment
In ESH we usually see blunt chest trauma but penetrating injuries also treated here (usually as single injuries, like stab wound)
") Chest Trauma Dr Csaba Dioszeghy MD PhD FRCEM FFICM FERC East Surrey Hospital Emergency Department Scope Thoracic injuries are common and can be life threatening In ESH we usually see blunt chest trauma
Chest Trauma Dr Csaba Dioszeghy MD PhD FRCEM FFICM FERC East Surrey Hospital Emergency Department Scope Thoracic injuries are common and can be life threatening In ESH we usually see blunt chest trauma
CHEST INJURIES. Jacek Piątkowski M.D., Ph. D.
 CHEST INJURIES Jacek Piątkowski M.D., Ph. D. CHEST INJURIES 3-4% of all injuries 8% of patients hospitalized due to injuries 65% of patients who died at the accident place CLASSIFICATION OF THE CHEST INJURIES
CHEST INJURIES Jacek Piątkowski M.D., Ph. D. CHEST INJURIES 3-4% of all injuries 8% of patients hospitalized due to injuries 65% of patients who died at the accident place CLASSIFICATION OF THE CHEST INJURIES
PEDIATRIC TRAUMA: Implications for Respiratory Care
 PEDIATRIC TRAUMA: Implications for Respiratory Care 17 th Annual Rainbow Respiratory Conference - September 4, 2015 Mike Dingeldein, MD Pediatric Surgeon Pediatric Trauma Medical Director Disclosures none
PEDIATRIC TRAUMA: Implications for Respiratory Care 17 th Annual Rainbow Respiratory Conference - September 4, 2015 Mike Dingeldein, MD Pediatric Surgeon Pediatric Trauma Medical Director Disclosures none
PEDIATRIC TRAUMA I: ABDOMINAL TRAUMA BURNS. December 19, 2012
 PEDIATRIC TRAUMA I: ABDOMINAL TRAUMA BURNS Niel F. Miele,, M.D. December 19, 2012 EPIDEMIOLOGY Major Trauma responsible for
PEDIATRIC TRAUMA I: ABDOMINAL TRAUMA BURNS Niel F. Miele,, M.D. December 19, 2012 EPIDEMIOLOGY Major Trauma responsible for
Shock. Perfusion. The cardiovascular system s circulation of blood and oxygen to all the cells in different tissues and organs of the body
 Shock Chapter 10 Shock State of collapse and failure of the cardiovascular system Leads to inadequate circulation Without adequate blood flow, cells cannot get rid of metabolic wastes The result- hypoperfusion
Shock Chapter 10 Shock State of collapse and failure of the cardiovascular system Leads to inadequate circulation Without adequate blood flow, cells cannot get rid of metabolic wastes The result- hypoperfusion
9/10/2012. Chapter 44. Learning Objectives. Learning Objectives (Cont d) Bleeding
 Bleeding") Chapter 44 Bleeding 1 Learning Objectives Describe the etiology, history, and physical findings of external bleeding Predict hemorrhage on the basis of the patient s mechanism of injury Distinguish between
Chapter 44 Bleeding 1 Learning Objectives Describe the etiology, history, and physical findings of external bleeding Predict hemorrhage on the basis of the patient s mechanism of injury Distinguish between
The Management of Chest Trauma. Tom Scaletta, MD FAAEM Immediate Past President, AAEM
 The Management of Chest Trauma Tom Scaletta, MD FAAEM Immediate Past President, AAEM Trichotomizing Rib Fractures Upper 1-3 vascular injuries Middle 4-9 Lower 10-12 12 liver/spleen injuries Management
The Management of Chest Trauma Tom Scaletta, MD FAAEM Immediate Past President, AAEM Trichotomizing Rib Fractures Upper 1-3 vascular injuries Middle 4-9 Lower 10-12 12 liver/spleen injuries Management
Penetrating Trauma in Pediatric Patients. Heidi P. Cordi, MD, MPH, MS, EMTP, FACEP, FAADM EMS WEEK 2017
 Penetrating Trauma in Pediatric Patients Heidi P. Cordi, MD, MPH, MS, EMTP, FACEP, FAADM EMS WEEK 2017 Introduction Trauma is the leading cause of death between ages of 1-18 years Penetrating injury accounts
Penetrating Trauma in Pediatric Patients Heidi P. Cordi, MD, MPH, MS, EMTP, FACEP, FAADM EMS WEEK 2017 Introduction Trauma is the leading cause of death between ages of 1-18 years Penetrating injury accounts
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Hatfield & McCoy Mine Safety Competition First-Aid Contest JULY 15, Page 1
 Hatfield & McCoy Mine Safety Competition First-Aid Contest JULY 15, 2014 Page 1 PROBLEM Billy is a maintenance person that has been conducting clean-up and service duties on the number one conveyor belt
Hatfield & McCoy Mine Safety Competition First-Aid Contest JULY 15, 2014 Page 1 PROBLEM Billy is a maintenance person that has been conducting clean-up and service duties on the number one conveyor belt
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #2 Blunt Trauma
 McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #2 Blunt Trauma Blunt trauma is the most common cause of traumatic death and disability. The definition
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #2 Blunt Trauma Blunt trauma is the most common cause of traumatic death and disability. The definition
Aurora Health Care EMS Continuing Education Spring 2011 Packet THORACIC TRAUMA THE PREHOSPITAL APPROACH TO CHEST INJURY MANAGEMENT
 Aurora Health Care EMS Continuing Education Spring 2011 Packet THORACIC TRAUMA Chest injuries are significant contributors to death from major trauma and can be difficult to assess adequately in the pre-hospital
Aurora Health Care EMS Continuing Education Spring 2011 Packet THORACIC TRAUMA Chest injuries are significant contributors to death from major trauma and can be difficult to assess adequately in the pre-hospital
9/10/2012. Chapter 49. Learning Objectives. Learning Objectives (Cont d) Thoracic Trauma
 Thoracic Trauma") Chapter 49 Thoracic Trauma 1 Learning Objectives Explain relevance of thoracic injuries as part of the overall mortality rate from major trauma List thoracic injuries that may result in early death if
Chapter 49 Thoracic Trauma 1 Learning Objectives Explain relevance of thoracic injuries as part of the overall mortality rate from major trauma List thoracic injuries that may result in early death if
MIAMI-DADE COLLEGE. Common Course Number: HSC Course Title: Basic Emergency Care. Course Catalog Description:
 Common Course Number: HSC 2400 MIAMI-DADE COLLEGE Course Title: Basic Emergency Care Course Catalog Description: Designed to provide opportunities to develop, practice, and display skills concerning emergency
Common Course Number: HSC 2400 MIAMI-DADE COLLEGE Course Title: Basic Emergency Care Course Catalog Description: Designed to provide opportunities to develop, practice, and display skills concerning emergency
INTERNATIONAL TRAUMA LIFE SUPPORT
 INTERNATIONAL TRAUMA LIFE SUPPORT NC ITLS Rev. 2/18 STUDENT GUIDE TO INTERNATIONAL TRAUMA LIFE SUPPORT What to wear ITLS is a practical course that stresses hands-on teaching. You should wear comfortable
INTERNATIONAL TRAUMA LIFE SUPPORT NC ITLS Rev. 2/18 STUDENT GUIDE TO INTERNATIONAL TRAUMA LIFE SUPPORT What to wear ITLS is a practical course that stresses hands-on teaching. You should wear comfortable
Face and Throat Injuries. Chapter 26
 Face and Throat Injuries Chapter 26 Anatomy of the Head Landmarks of the Neck Injuries to the Face Injuries around the face can lead to upper airway obstructions. Bleeding from the face can be profuse.
Face and Throat Injuries Chapter 26 Anatomy of the Head Landmarks of the Neck Injuries to the Face Injuries around the face can lead to upper airway obstructions. Bleeding from the face can be profuse.
Skin Anatomy and Physiology
 Skin Anatomy and Physiology Body s largest organ Three layers: Epidermis Dermis Subcutaneous tissue 1 2 Skin Anatomy and Physiology Complex system, variety of functions Sensation Control of water loss
Skin Anatomy and Physiology Body s largest organ Three layers: Epidermis Dermis Subcutaneous tissue 1 2 Skin Anatomy and Physiology Complex system, variety of functions Sensation Control of water loss
Shenandoah Co. Fire & Rescue. Injuries to. and Spine. December EMS Training Bill Streett Training Section Chief
 Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#
Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#
APPROACH TO TRAUMA. Dr E.Memary Anesthesiologist Assistant Professor of SBMU
 APPROACH TO TRAUMA Dr E.Memary Anesthesiologist Assistant Professor of SBMU Objectives Describe the initial approach to the injured patient, including the primary and secondary surveys. Identify the types
APPROACH TO TRAUMA Dr E.Memary Anesthesiologist Assistant Professor of SBMU Objectives Describe the initial approach to the injured patient, including the primary and secondary surveys. Identify the types
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Pediatric Trauma Care
 2013 Standard Trauma Care Procedures (Pediatric) Traumatic injuries require prompt care and transportation. Always suspect cervical injury. Note the mechanism of injury and any other condition that may
2013 Standard Trauma Care Procedures (Pediatric) Traumatic injuries require prompt care and transportation. Always suspect cervical injury. Note the mechanism of injury and any other condition that may
PEMSS PROTOCOLS INVASIVE PROCEDURES
 PEMSS PROTOCOLS INVASIVE PROCEDURES Panhandle Emergency Medical Services System SURGICAL AND NEEDLE CRICOTHYROTOMY Inability to intubate is the primary indication for creating an artificial airway. Care
PEMSS PROTOCOLS INVASIVE PROCEDURES Panhandle Emergency Medical Services System SURGICAL AND NEEDLE CRICOTHYROTOMY Inability to intubate is the primary indication for creating an artificial airway. Care
FIRST AID WRITTEN EXAM. Team Name: 1. Participation in a critical incident stress debriefing (CISD) is mandatory. a. TRUE b. FALSE
 is mandatory. a. TRUE b. FALSE") 2015 NEW IBERIA MINE RESCUE CONTEST FIRST AID WRITTEN EXAM Name: Date: 1. Participation in a critical incident stress debriefing (CISD) is mandatory. 2. The use of accessory muscles in the chest, abdomen
2015 NEW IBERIA MINE RESCUE CONTEST FIRST AID WRITTEN EXAM Name: Date: 1. Participation in a critical incident stress debriefing (CISD) is mandatory. 2. The use of accessory muscles in the chest, abdomen
Post-Anesthesia Care In the ICU
 Post-Anesthesia Care In the ICU The following is based on current research and regional standards of care. At completion you will be able to identify Basic equipment needed at the bedside. Aldrete scoring
Post-Anesthesia Care In the ICU The following is based on current research and regional standards of care. At completion you will be able to identify Basic equipment needed at the bedside. Aldrete scoring
68W COMBAT MEDIC POCKET GUIDE
 GTA 08-05-058 68W COMBAT MEDIC POCKET GUIDE PART I: TRAUMA TREATMENT This publication contains technical information that is for official Government use only. Distribution is limited to U.S. Government
GTA 08-05-058 68W COMBAT MEDIC POCKET GUIDE PART I: TRAUMA TREATMENT This publication contains technical information that is for official Government use only. Distribution is limited to U.S. Government
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #3 Penetrating Neck Trauma
 McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #3 Penetrating Neck Trauma Penetrating neck injury (PNI) comprises 5 to 10 percent of traumatic injuries
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #3 Penetrating Neck Trauma Penetrating neck injury (PNI) comprises 5 to 10 percent of traumatic injuries
Pediatric Burn Management Justin D. Klein, MD Associate Burn Director Lisa C. Vitale, RN Burn Program Coordinator
 Pediatric Burn Management Justin D. Klein, MD Associate Burn Director Lisa C. Vitale, RN Burn Program Coordinator Lecture Overview Burn statistics and etiologies Pre-hospital evaluation Anatomy of a burn
Pediatric Burn Management Justin D. Klein, MD Associate Burn Director Lisa C. Vitale, RN Burn Program Coordinator Lecture Overview Burn statistics and etiologies Pre-hospital evaluation Anatomy of a burn
Pediatric Patients. BCFPD Paramedic Education Program. EMS Education Paramedic Level
 Pediatric Patients BCFPD Program Basic Considerations Much of the initial patient assessment can be done during visual examination of the scene. Involve the caregiver or parent as much as possible. Allow
Pediatric Patients BCFPD Program Basic Considerations Much of the initial patient assessment can be done during visual examination of the scene. Involve the caregiver or parent as much as possible. Allow
Skin is the largest, most important organ % of total body weight Functions: - -Sensation - Regulation AKA: System
 1 Chapter 20 Soft-Tissue Injury 2 Introduction to Soft-Tissue Injury Skin is the largest, most important organ % of total body weight Functions: - -Sensation - Regulation AKA: System 3 Epidemiology Most
1 Chapter 20 Soft-Tissue Injury 2 Introduction to Soft-Tissue Injury Skin is the largest, most important organ % of total body weight Functions: - -Sensation - Regulation AKA: System 3 Epidemiology Most
EmergencyKT: Management of Thermal Injury in Adult Patients
 EmergencyKT: Management of Thermal Injury in Adult Patients Remove patient from source of injury, including burned clothing and jewelry Does patient appear to have minor burns? (See Box A) No Notify Burn
EmergencyKT: Management of Thermal Injury in Adult Patients Remove patient from source of injury, including burned clothing and jewelry Does patient appear to have minor burns? (See Box A) No Notify Burn
Hanna K. Al-Makhamreh, M.D., FACC Interventional Cardiologist
 Hanna K. Al-Makhamreh, M.D., FACC Interventional Cardiologist Introduction. Basic Life Support (BLS). Advanced Cardiac Life Support (ACLS). Cardiovascular diseases (CVDs) are the number one cause of death
Hanna K. Al-Makhamreh, M.D., FACC Interventional Cardiologist Introduction. Basic Life Support (BLS). Advanced Cardiac Life Support (ACLS). Cardiovascular diseases (CVDs) are the number one cause of death
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University
 Dr Mubarak Abdelrahman Assistant Professor Jazan University") Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Kinetic Energy Energy in Motion KE = Mass (weight) X Velocity (speed)² 2 Double Weight = Energy Double Speed = Energy IS THE GREATEST DETERMINANT
 X Velocity (speed)² 2 Double Weight = Energy Double Speed = Energy IS THE GREATEST DETERMINANT") 1 Chapter 17 Blunt Trauma 2 Introduction to Blunt Trauma Most common cause of trauma death and disability exchange between an object and the human body, without intrusion through the skin 3 Blunt trauma
1 Chapter 17 Blunt Trauma 2 Introduction to Blunt Trauma Most common cause of trauma death and disability exchange between an object and the human body, without intrusion through the skin 3 Blunt trauma
Civilian Hospital Response to Mass Casualty Events The Israeli Experience
 Civilian Hospital Response to Mass Casualty Events The Israeli Experience William Schecter, MD Professor of Clinical Surgery University of California, San Francisco Chief of Surgery San Francisco General
Civilian Hospital Response to Mass Casualty Events The Israeli Experience William Schecter, MD Professor of Clinical Surgery University of California, San Francisco Chief of Surgery San Francisco General
Overview. Overview. Chapter 30. Injuries to the Head and Spine 9/11/2012. Review of the Nervous and Skeletal Systems. Devices for Immobilization
 Chapter 30 Injuries to the Head and Spine Slide 1 Overview Review of the Nervous and Skeletal Systems The Nervous System The Skeletal System Devices for Immobilization Cervical Spine Short Backboards Long
Chapter 30 Injuries to the Head and Spine Slide 1 Overview Review of the Nervous and Skeletal Systems The Nervous System The Skeletal System Devices for Immobilization Cervical Spine Short Backboards Long
Review. A. abrasion B. contusion C. hematoma D. avulsion
 Chapter 24 Review Review 1. A young male was struck in the forearm with a baseball and complains of pain to the area. Slight swelling and ecchymosis are present, but no external bleeding. What type of
Chapter 24 Review Review 1. A young male was struck in the forearm with a baseball and complains of pain to the area. Slight swelling and ecchymosis are present, but no external bleeding. What type of
PALS Pulseless Arrest Algorithm.
 PALS Pulseless Arrest Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Bradycardia Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Tachycardia Algorithm. Kleinman M
PALS Pulseless Arrest Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Bradycardia Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Tachycardia Algorithm. Kleinman M
PEDIATRIC BRAIN CARE
 PEDIATRIC BRAIN CARE The brain matters most! OVERVIEW OF NEURO ASSESSMENT 1. Overall responsiveness/activity 2. The eyes 3.? Increased ICP 4. Movements 5.? Seizures 6. Other OVERALL RESPONSIVENESS/ ACTIVITY
PEDIATRIC BRAIN CARE The brain matters most! OVERVIEW OF NEURO ASSESSMENT 1. Overall responsiveness/activity 2. The eyes 3.? Increased ICP 4. Movements 5.? Seizures 6. Other OVERALL RESPONSIVENESS/ ACTIVITY
yregion I EMERGENCY MEDICAL SERVICES STANDING MEDICAL ORDERS EMT Basic SMO: Airway Management
 yregion I EMERGENCY MEDICAL SERVICES STANDING MEDICAL ORDERS EMT Basic SMO: Airway Management Overview: Managing a patient s airway may be necessitated due to upper or lower airway obstruction, inadequate
yregion I EMERGENCY MEDICAL SERVICES STANDING MEDICAL ORDERS EMT Basic SMO: Airway Management Overview: Managing a patient s airway may be necessitated due to upper or lower airway obstruction, inadequate
Trauma. Neck trauma zones. Neck Injuries 1/3/2018. Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure
 Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
BLS, ILS, ALS OTEP BURNS BURN INTRODUCTION TYPES OF BURNS
 BURNS BLS, ILS, ALS OTEP While we do understand this presentation is an instructional tool for all levels of certification, taking this into consideration everyone taking this class must remember that
BURNS BLS, ILS, ALS OTEP While we do understand this presentation is an instructional tool for all levels of certification, taking this into consideration everyone taking this class must remember that
Chapter 24 Soft Tissue Injuries Presentation Notes
 Names: Chapter 24 Soft Tissue Injuries Presentation Notes Anatomy of the Skin - Function of the Skin control Soft-Tissue Injuries injuries Soft-tissue damage the skin injuries Break in the of the skin
Names: Chapter 24 Soft Tissue Injuries Presentation Notes Anatomy of the Skin - Function of the Skin control Soft-Tissue Injuries injuries Soft-tissue damage the skin injuries Break in the of the skin