The craniocervical junction
|
|
|
- Allan Atkinson
- 5 years ago
- Views:
Transcription

1 Anver Jameel, MD
2 The craniocervical junction A biomechanical and anatomical unit that extends from the skull base to C2 Includes the clivus, foramen magnum and contiguous occipital bone, the occipital condyles which articulate with the superior articulating surface of C1, C1 (atlas) and its articulations with the dens and the superior facets of the articulating masses of C2, and C2 (axis). The complex joints and ligaments allow a wide range of motion while ensuring stability

3 The Craniocervical joints.. biconvex occipital condyles articulate with the biconcave superior articulating surface of C1

4 Biconvex inferior articulating surface of C1, articulates with biconvex superior facets of the articulating masses of C2 Biconvex joint surfaces at C1 C2
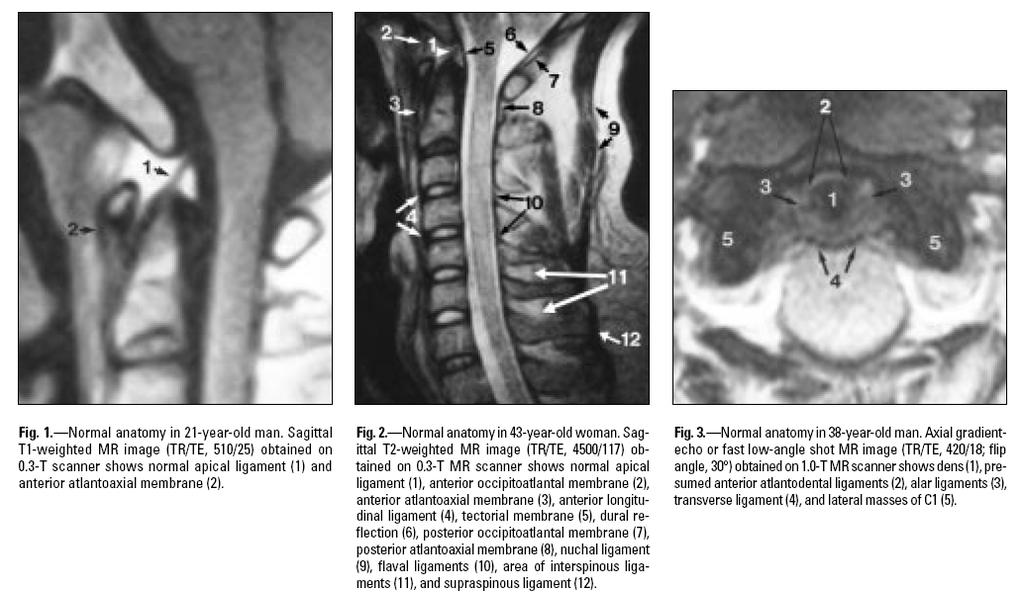
5 The odontoid peg arises from the cranial aspect of C2, projects through the arch of C1 The most anterior ligament is Anterior Longitudinal Ligament (ALL). It inserts in to the antero inferior corner of the C2 body. Deeper to ALL, apical ligament, tip of the odontoid to basion Anterior atlantoaxial membrane is dense fibrous tissue that extends from the C2 body to the anterior arch of C1. Anterior Atlanto Occipital membrane is the the cephalad extension of ALL, extending rostrally from the anterior tubercle of C1 to the clivus.
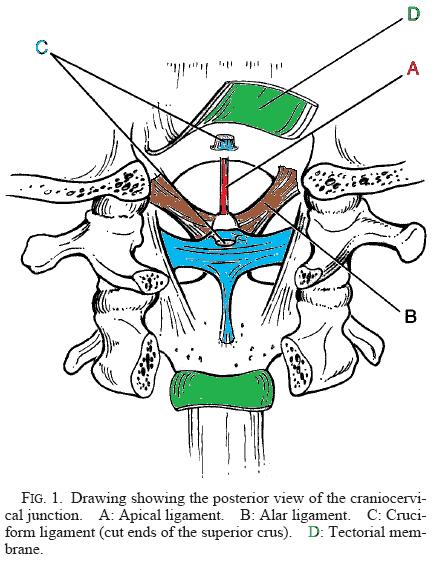
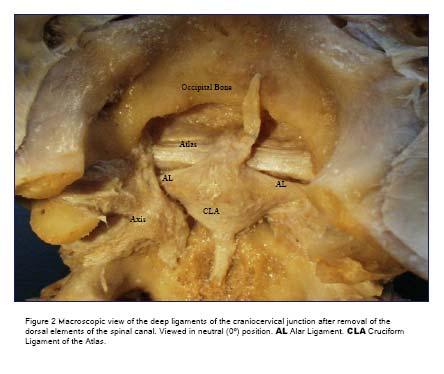
6 Tectorial membrane is the cephalad continuation of PLL, connects the dorsal surface of the dens to the ventral surface of the FM Laterally, it connects C2 to the occipital condyles Transverse ligaments Oriented horizontally dorsal to odontoid, attaches to medial surfaces of the lateral masses of C1 Extends rostrally to FM and caudally to C2 body Alar ligaments connect the dens to Occipital condyles The lateral masses of C1 Each alar arises from the lateral margin of the dens, courses laterally, in a near vertical plane, attaching to the ipsilateral occipital condyle and the subajacent superior margin of the C1 lateral mass. In 30% of people it attaches solely to the condyle.
7
8
9 The tectorial membrane and the alar ligaments are the most important in maintaining stability Alar ligaments are strong and prevent excessive rotation of C1 on C2, and lateral bending of the occiput/c1 on C2 The transverse/cruciate ligaments are next. The apical ligament is considered a vestigial structure that offers no significant added stability to the CCJ (Tubbs et al, 2000). Absent in 20% of cadaveric specimens examined The Posterior atlanto occipital membrane connects the posterior margin of the FM to the posterior arch of C1
10
11
12 The range of motion between Atlas and Axis is the greatest between any two vertebrae. The primary movement at C1 C2 is rotation around the vertical axis of the odontoid peg The two convex surfaces resting upon each other also allows vertical translation with the descent of the the skull The Bi convex shape of the atlanto axial joints and the oblique orientation of the alar ligaments allow a large range of motion but gradually restricts motion at the extremes of axial rotation.
13 Degrees of motion Flexion O C1 is 10 C1 C2 is 5 Extension O C1 is 25 C1C2 is 10 Rotation O C1 is 0 C1 C2 is 45
14 Trauma at the Craniocervical Junction Fractures and dislocations of the cranio cervical junction represent 1/3 of all injuries to the cervical spine. Isolated ligamentous Injuries Isolated Fractures Mixed injuries Disrupted ligaments are incapable of repair and usually require surgery to restore stability Fractures alone can usually heal if reduced and satisfactorily immobolized Mixed injuries require surgery
15 Isolated Ligamentous Injuries Atlanto occipital (AO) dislocation Transverse ligament disruptions Ligaments are avulsed and require surgical fixation Rotatory C1 C2 dislocations Blood or oedema adjacent to an acute ligamentous tear can be seen on mri. Secondary evidence of ligamentous injury is displacement of the dens to the contralateral side. Hypermobility at the atlanto axial joint can reduce blood flow to the contralateral vertebral artery. Hulse et al. 1982, described a cervical nystagmus as a manifestation of vertebral artery insufficiency due to rotator hypermoility at the occipito atlanto axial complex.
16 Atlanto occipital (AO) dislocation.. They are usually caused by high energy trauma. Devastating injury sometimes referred to internal decapitation. AOD is the cause of death in an estimated 8 35% of traffic fatalities and 10% of fatal cervical spine injuries. Disruption of the vascular supply may caused a haematoma esp.sah at the craniovertebral junction.

17 Atlanto occipital (AO) dislocation Pathomechanism flexion and distraction rotation and hyperextension. Rupture of the alar ligaments and the tectorial membrane, as well as the occipito atlantal joint capsules and membranes, lead to severe C0 C1 instability in a vertical, anterior or posterior direction.

18 Established criteria for diagnosis of AO dislocation include basion to dens interval >12 mm, or posterior axis line >12 mm posterior to basion, or posterior axis line >4 mm anterior to basion
 0.")
19 Power s Ratio (Powers etal, 1979) Basion Post. C1 arch divided by Opisthion Ant. C1 arch <0.9 normal (1 s.d. below lowest case of AOD) 0.9 & <1 7% normal 1 All AOD
20 Lateral C spine XR is recommended for the diagnosis of AOD. Radio logically three types longitudinal distraction with axial separation of the occiput, rotational injuries anterior or posterior displacement of the occiput with respect to the atlas. Distraction and rotational injuries are difficult to diagnose on plain radiographs, but the prevertebral soft tissue swelling which is usually present warrants further investigation. CT with reformatted sagittal and coronal images may show widening of the atlanto occipital joint or dislocation of the occipital condyles.
21 Respiratory distress may be secondary to brainstem compression, or lower cranial nerve palsies causing airway obstruction, diaphragmatic paralysis. Hypertension can occur owing to bilateral glossopharyngeal nerve (IX) lesions, whereas complete cord transection can cause hypotension. Medullary compression can lead to bradycardia and apneic spells. Other brainstem signs commonly observed with AOD include rotatory nystagmus, ocular bobbing and decerebrate posturing.
22 Improvements in emergency management of the patient in the field, rapid transport, and better recognition have resulted in more survivors of AOD in the past two decades. AOD is 3 times more common in children attributed to anatomical differences.3 The craniovertebral junction in children is inherently less stable because of the relatively small occipital condyles and the horizontal orientation of the articulation between the cranium and the atlas Cranio cervical fusion with internal fixation is recommended for the treatment of patients with acute traumatic AOD.

23
24 Atlanto occipital subluxation is radiographically subtle and patients usually survive. When flexion occurs without a lateral or rotatory component at the upper cervical level, it can cause an anterior dislocation at the atlantoaxial joint if the transverse ligament is disrupted. Since the transverse ligament is the main stabilizing force of the atlantoaxial joint, this injury is unstable. Neurologic injury may occur from cord compression between the odontoid and posterior arch of C1.

25 C1 C2 Subluxation
26 AO subluxation Radiographically, this injury is suspected if the predental space, ADI, is more than 3.5 mm (5 mm in children); These injuries may require fusion of C1 and C2 for definitive management. Diagnosis of AO subluxation is based on abnormal; basion axial interval and/or basion dental interval. If both are > 12mm, if there is an abnormal cerviocranial prevertebral soft tissue contour. High cervicocranial haematoma associated with AO subluxation makes the contour anteriorly convex.

27 An abnormal anteriorly convex cerviocranial prevertebral softtissue contour due to a high cervicocranial haematoma associated with AO subluxation.
28 Rojas et al. Reassment of the Craniocervical Junction. American Journal of Neuororadiology 28:
29 Rotatory C1 C2 dislocation Primarily in young children & adolescents Present in a cocked robin position 20 tilt to one side, with a 20 rotation to the other Rarely locks in rotation Treated with gradually increasing traction and then immobilization
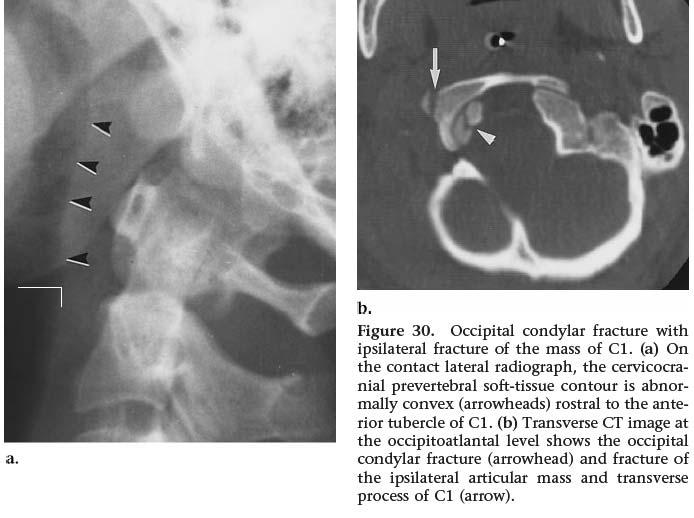
30 Occipital Condyle Fractures Occipital condylar fractures are of three types. They may be associated with other cervicocranial fractures, particularly the lateral masses of C1. Occipital condyle fractures, alone or in conjunction with C1 lateral mass fractures produce an abnormally concave prevertebral soft tissue contour superior to the the C1 anterior tubercle.
31

32 Types of condyle fractures Type I: one or both condyles are split or comminuted by an axial loading force Stable Type II : a fracture of the occipital bone that extends in to the condyle Stable Type II: an avulsion fracture of the medial surface of the condyle at the site of the alar ligament Potentially unstable due to ligamentous disruption Anderson et al., SPINE, 1988 Tuli et al., Neurosurgery, 1997
33 Fractures of the Atlas Four types of atlas fractures (I, II, III, IV) result from impaction of the occipital condyles on the atlas, causing single or multiple fractures around the ring. The first 2 types of atlas fracture are stable isolated fractures of the anterior arch of C1 Anterior arch fractures usually are avulsion fractures from the anterior portion of the ring and have a low morbidity rate and little clinical significance. isolated fractures of the posterior arch of C1 an isolated fracture caused by hyperextension.
34 Fractures of the Atlas.. The third type of atlas fracture is a fracture through the lateral mass of C1. Radiographically, asymmetric displacement of the mass from the rest of the vertebra is seen in the odontoid view. low morbidity rate and little clinical significance. The fourth type of atlas fracture is the burst fracture of the ring of C1 and also is known as a Jefferson fracture (caused by a Vertical (axial) compression injury).
35 Jefferson fracture of C1 Typically caused by an axial loading force on the occiput of the head Fracture variants may include two or three part fractures Usually no associated neurologic deficit as the ring of C1 widens when it fractures limiting cord compression 1/3 are associated with a C2 fracture. Patients usually complain of upper neck pain. Neuro exam usually normal.

36 Jefferson Burst Fracture (Type IV)
 * several weeks followed by halo vest Immediate")

37 Atlas Fractures Treatment Displaced <6.9 mm Halo vest for 3 mos Displaced >6.9 mm Halo traction (reduction) * several weeks followed by halo vest Immediate halo vest Posterior C1 2 fusion (unable to tolerate halo) After brace treatment complete confirm C1 2 stability Flexion/extension films C1 2 fusion for ADI > 5mm

38 Odontoid process fractures The 3 types of odontoid process fractures, classified based on the anatomic level of fracture. Type I avulsion of the tip of the dens at the insertion site of the alar ligament. mechanically stable, treated with hard Collar,SOMI,Halo Often seen in association with AO dislocation and AOD must be ruled out.

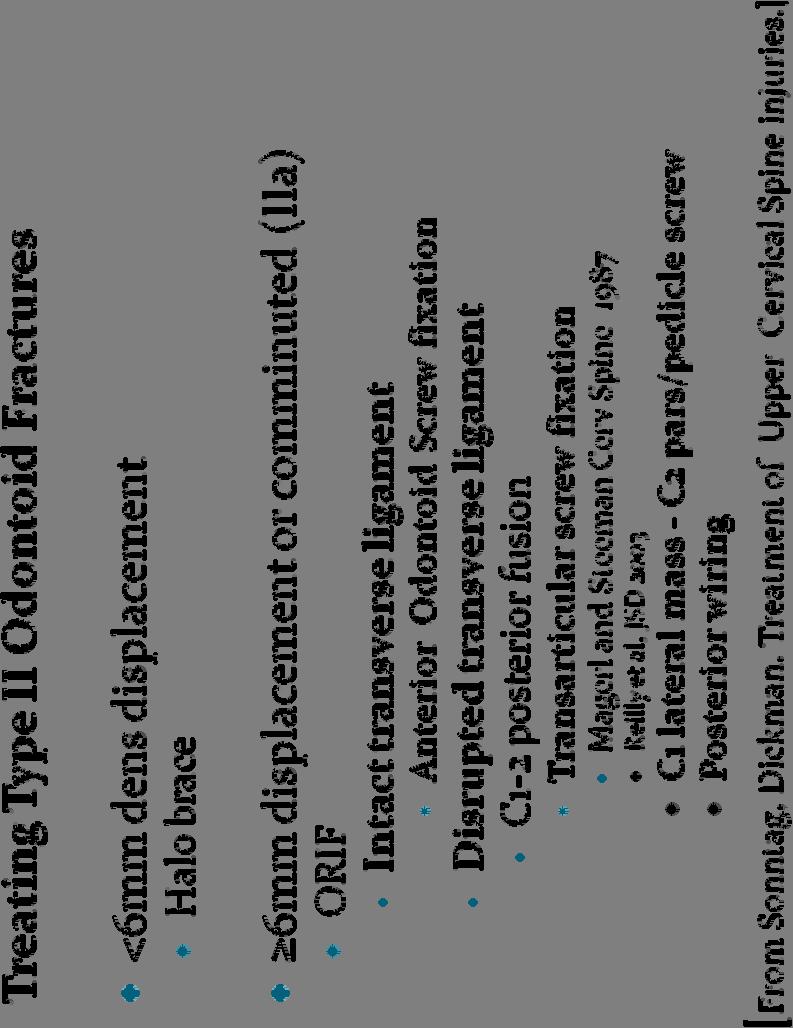
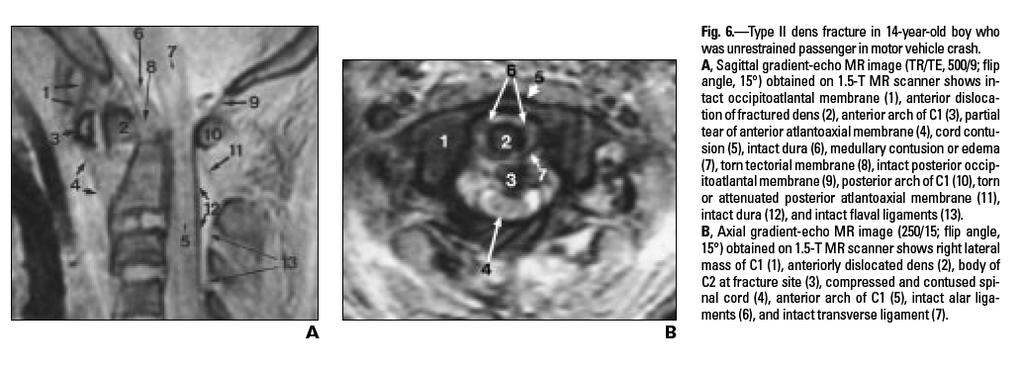
39 Type II fractures occur at the base of the dens the most common odontoid fractures high prevalence of nonunion due to limited vascular supply and small area of cancellous bone.
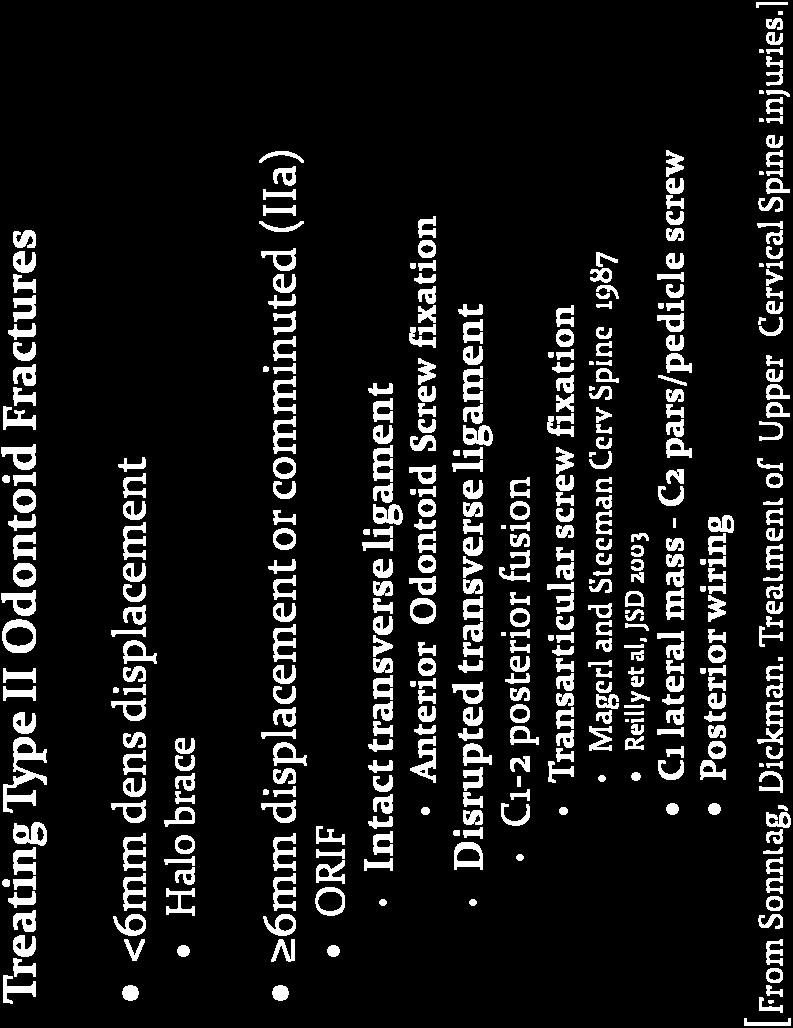
40
41

42 Type III odontoid fracture occurs when the fracture line extends into the body of the axis. Nonunion is not usually a problem because of a good blood supply and the greater amount of cancellous bone.
43 With Odontoid Type II and III fractures, the fractured segment may be displaced anteriorly, laterally, or posteriorly. Since posterior displacement of segment is more common in type III, the prevalence of spinal cord injury is as high as 10% with these fractures.
44 Hangman fracture (traumatic spondylolisthesis of C2) Bilateral fractures through the pedicles of C2 due to hyperextension 2 nd most common C2 fracture (25%) The typical fracture that occurs after judicial hangings Hyperextension & distraction Commonly is caused by MVA /blows to the head Hyperextension & axial compression Radiographically, a fracture line should be evident extending through the pedicles of C2 along with obvious disruption of the spinolaminar contour line A common sign is a constricted pupil on the ipsilateral side due to loss of sympathetic innervation to the eye due to damage to the sympathetic trunk in the neck
45 Type III Treatment Options Posterior Open reduction and C1 C3 fusion Direct pars repair and C2 C3 fusion Anterior C2/C3 ACDF with instrumentation
46 Although considered an unstable fracture, it seldom is associated with spinal injury, since the anteroposterior diameter of the spinal canal is greatest at this level the fractured pedicles allow decompression. When associated with unilateral or bilateral facet dislocation at the level of C2, this particular type of hangman fracture is unstable and has a high rate of neurologic complications that require immediate cervical traction to reduce the facet dislocation.
47 Other C2 Fractures do not involve the odontoid process or the pars interarticularis of C2 Fractures of C2 body, laminae, facets and spinous process Most heal satisfactorily with C collar or SOMI orthosis Displaced or extensive fractures treated with a Halo
48 Traumatic spondylolisthesis of C2 (Hangman s) Usuallay affects a younger age group (Avg 38 yrs) Neurologic injury seen in only 5 10 % (acutely decompresses canal) Traditional treatment has been Halo vest Collar adequate if < 6 mm displaced [Coric et al. JNS. 1996]
49 C1 C2 combination fractures are common 44% of all C1 and 16% of all C2 fractures (Dickman et al, 1989) Higher rate of neurological injury Higher rate of non operative treatment failure
50 Summary Of the entire spine, the CCJ is most difficult to evaluate radiographically and treat because of its complex anatomy, physiologic motions and normal variants Treatment is based on injuries to bone and ligaments responsible for maintaining spinal stability. Isolated ligament injuries tend to be highly unstable and don t heal with non operative management Minimally displaced or non displaced bony injuries tend to heal satisfactorily with an orthosis Combination, comminuted and displaced injuries tend to require internal fixation to restore stability
Imaging of Cervical Spine Trauma Tudor H Hughes, M.D.
 Imaging of Cervical Spine Trauma Tudor H Hughes, M.D. General Considerations Most spinal fractures are due to a single episode of major trauma. Fatigue fractures of the spine are unusual except in the
Imaging of Cervical Spine Trauma Tudor H Hughes, M.D. General Considerations Most spinal fractures are due to a single episode of major trauma. Fatigue fractures of the spine are unusual except in the
Spinal Cord Injuries: The Basics. Kadre Sneddon POS Rounds October 1, 2003
 Spinal Cord Injuries: The Basics Kadre Sneddon POS Rounds October 1, 2003 Anatomy Dorsal columntouch, vibration Corticospinal tract- UMN Anterior horn-lmn Spinothalamic tractpain, temperature (contralateral)
Spinal Cord Injuries: The Basics Kadre Sneddon POS Rounds October 1, 2003 Anatomy Dorsal columntouch, vibration Corticospinal tract- UMN Anterior horn-lmn Spinothalamic tractpain, temperature (contralateral)
Common fracture & dislocation of the cervical spine. Theerachai Apivatthakakul Department of Orthopaedic Chiangmai University
 Common fracture & dislocation of the cervical spine Theerachai Apivatthakakul Department of Orthopaedic Chiangmai University Objective Anatomy Mechanism and type of injury PE.and radiographic evaluation
Common fracture & dislocation of the cervical spine Theerachai Apivatthakakul Department of Orthopaedic Chiangmai University Objective Anatomy Mechanism and type of injury PE.and radiographic evaluation
SUBAXIAL CERVICAL SPINE TRAUMA- DIAGNOSIS AND MANAGEMENT
 SUBAXIAL CERVICAL SPINE TRAUMA- DIAGNOSIS AND MANAGEMENT 1 Anatomy 3 columns- Anterior, middle and Posterior Anterior- ALL, Anterior 2/3 rd body & disc. Middle- Posterior 1/3 rd of body & disc, PLL Posterior-
SUBAXIAL CERVICAL SPINE TRAUMA- DIAGNOSIS AND MANAGEMENT 1 Anatomy 3 columns- Anterior, middle and Posterior Anterior- ALL, Anterior 2/3 rd body & disc. Middle- Posterior 1/3 rd of body & disc, PLL Posterior-
Cervical Spine Anatomy and Biomechanics. Typical Cervical Vertebra C3 6. Typical Cervical Vertebra Anterior 10/5/2017
 Cervical Spine Anatomy and Biomechanics Typical Cervical Vertebra C3 6 Small, relatively broad body Bifid SpinousProcess Long and narrow laminae Spinal Canal: large, triangular; remarkably consistent dimensions
Cervical Spine Anatomy and Biomechanics Typical Cervical Vertebra C3 6 Small, relatively broad body Bifid SpinousProcess Long and narrow laminae Spinal Canal: large, triangular; remarkably consistent dimensions
Outline. Epidemiology Indications for C-spine imaging Modalities Interpretation Types of fractures
 C-Spine Plain Films Outline Epidemiology Indications for C-spine imaging Modalities Interpretation Types of fractures Epidemiology 7000-10000 c-spine injuries treated each year Additional 5000 die at the
C-Spine Plain Films Outline Epidemiology Indications for C-spine imaging Modalities Interpretation Types of fractures Epidemiology 7000-10000 c-spine injuries treated each year Additional 5000 die at the
MDCT and MRI evaluation of cervical spine trauma
 Insights Imaging (2014) 5:67 75 DOI 10.1007/s13244-013-0304-2 PICTORIAL REVIEW MDCT and MRI evaluation of cervical spine trauma Michael Utz & Shadab Khan & Daniel O Connor & Stephen Meyers Received: 10
Insights Imaging (2014) 5:67 75 DOI 10.1007/s13244-013-0304-2 PICTORIAL REVIEW MDCT and MRI evaluation of cervical spine trauma Michael Utz & Shadab Khan & Daniel O Connor & Stephen Meyers Received: 10
Dr Ajit Singh Moderator Dr P S Chandra Dr Rajender Kumar
 BIOMECHANICS OF SPINE Dr Ajit Singh Moderator Dr P S Chandra Dr Rajender Kumar What is biomechanics? Biomechanics is the study of the consequences of application of external force on the spine Primary
BIOMECHANICS OF SPINE Dr Ajit Singh Moderator Dr P S Chandra Dr Rajender Kumar What is biomechanics? Biomechanics is the study of the consequences of application of external force on the spine Primary
A Pictorial Review of the Biomechanics and Imaging Findings in Cervical Spine Injuries
 A Pictorial Review of the Biomechanics and Imaging Findings in Cervical Spine Injuries Award: Certificate of Merit Poster No.: C-1741 Congress: ECR 2011 Type: Educational Exhibit Authors: A. Adams, A.
A Pictorial Review of the Biomechanics and Imaging Findings in Cervical Spine Injuries Award: Certificate of Merit Poster No.: C-1741 Congress: ECR 2011 Type: Educational Exhibit Authors: A. Adams, A.
Fractures of the C-2 vertebral body
 J Neurosurg 81:206-212, 1994 Fractures of the C-2 vertebral body EDWARD C. BENZEL, M.D., BLAINE L. HART, M.D., PERRY A. BALL, M.D., NEVAN G. BALDWIN, M.D., WILLIAM W. ORRISON, M.D., AND MARY ESPINOSA,
J Neurosurg 81:206-212, 1994 Fractures of the C-2 vertebral body EDWARD C. BENZEL, M.D., BLAINE L. HART, M.D., PERRY A. BALL, M.D., NEVAN G. BALDWIN, M.D., WILLIAM W. ORRISON, M.D., AND MARY ESPINOSA,
Subaxial Cervical Spine Trauma
 Subaxial Cervical Spine Trauma Pooria Salari, MD Assistant Professor Of Orthopaedics Department of Orthopaedic Surgery St. Louis University School of Medicine St. Louis, Missouri, USA Initial Evaluation
Subaxial Cervical Spine Trauma Pooria Salari, MD Assistant Professor Of Orthopaedics Department of Orthopaedic Surgery St. Louis University School of Medicine St. Louis, Missouri, USA Initial Evaluation
Imaging of Cervical Spine Trauma
 Imaging of Cervical Spine Trauma C Craig Blackmore, MD, MPH Professor of Radiology and Adjunct Professor of Health Services University of Washington, Harborview Medical Center Salary support: AHRQ grant
Imaging of Cervical Spine Trauma C Craig Blackmore, MD, MPH Professor of Radiology and Adjunct Professor of Health Services University of Washington, Harborview Medical Center Salary support: AHRQ grant
ISPUB.COM. Fracture Through the Body of the Axis. B Johnson, N Jayasekera CASE REPORT
 ISPUB.COM The Internet Journal of Orthopedic Surgery Volume 8 Number 1 B Johnson, N Jayasekera Citation B Johnson, N Jayasekera.. The Internet Journal of Orthopedic Surgery. 2007 Volume 8 Number 1. Abstract
ISPUB.COM The Internet Journal of Orthopedic Surgery Volume 8 Number 1 B Johnson, N Jayasekera Citation B Johnson, N Jayasekera.. The Internet Journal of Orthopedic Surgery. 2007 Volume 8 Number 1. Abstract
2. The vertebral arch is composed of pedicles (projecting from the body) and laminae (uniting arch posteriorly).
 and laminae (uniting arch posteriorly).") VERTEBRAL COLUMN 2018zillmusom I. VERTEBRAL COLUMN - functions to support weight of body and protect spinal cord while permitting movements of trunk and providing for muscle attachments. A. Typical vertebra
VERTEBRAL COLUMN 2018zillmusom I. VERTEBRAL COLUMN - functions to support weight of body and protect spinal cord while permitting movements of trunk and providing for muscle attachments. A. Typical vertebra
Ligaments of the vertebral column:
 In the last lecture we started talking about the joints in the vertebral column, and we said that there are two types of joints between adjacent vertebrae: 1. Between the bodies of the vertebrae; which
In the last lecture we started talking about the joints in the vertebral column, and we said that there are two types of joints between adjacent vertebrae: 1. Between the bodies of the vertebrae; which
Upper Cervical Spine - Occult Injury and Trigger for CT Exam
 Upper Cervical Spine - Occult Injury and Trigger for CT Exam Main Menu Introduction Clinical clearance of C-SpineC Radiographic evaluation Norms for C-spineC Triggers for CT exam: Odontoid Lateral view
Upper Cervical Spine - Occult Injury and Trigger for CT Exam Main Menu Introduction Clinical clearance of C-SpineC Radiographic evaluation Norms for C-spineC Triggers for CT exam: Odontoid Lateral view
Why does sideflexion increase ipsilateral vertebral artery occlusion with contralateral atlanto-axial rotation? Thomas Langer
 Why does sideflexion increase ipsilateral vertebral artery occlusion with contralateral atlanto-axial rotation? Thomas Langer 1 Introduction When the head and neck are placed in the premanipulative position
Why does sideflexion increase ipsilateral vertebral artery occlusion with contralateral atlanto-axial rotation? Thomas Langer 1 Introduction When the head and neck are placed in the premanipulative position
Subaxial Cervical Spine Trauma. Introduction. Anatomic Considerations 7/23/2018
 Subaxial Cervical Spine Trauma Sheyan J. Armaghani, MD Florida Orthopedic Institute Assistant Professor USF Dept of Orthopedics Introduction Trauma to the cervical spine accounts for 5 of all spine injuries
Subaxial Cervical Spine Trauma Sheyan J. Armaghani, MD Florida Orthopedic Institute Assistant Professor USF Dept of Orthopedics Introduction Trauma to the cervical spine accounts for 5 of all spine injuries
Subaxial Cervical Spine Trauma Dr Hesarikia BUMS
 Subaxial Cervical Spine Trauma Dr. Hesarikia BUMS Subaxial Cervical Spine From C3-C7 ROM Majority of cervical flexion Lateral bending Approximately 50% rotation Ligamentous Anatomy Anterior ALL, PLL, intervertebral
Subaxial Cervical Spine Trauma Dr. Hesarikia BUMS Subaxial Cervical Spine From C3-C7 ROM Majority of cervical flexion Lateral bending Approximately 50% rotation Ligamentous Anatomy Anterior ALL, PLL, intervertebral
Inferior view of the skull showing foramina (Atlas of Human Anatomy, 5th edition, Plate 12)
") Section 1 Head and Neck Skull, Basal View Incisive foramen Choanae Foramen ovale Foramen lacerum Foramen spinosum Carotid canal Jugular fossa Mastoid process Inferior view of the skull showing foramina
Section 1 Head and Neck Skull, Basal View Incisive foramen Choanae Foramen ovale Foramen lacerum Foramen spinosum Carotid canal Jugular fossa Mastoid process Inferior view of the skull showing foramina
Clarification of Terms
 Clarification of Terms The Spine, Spinal Column, and Vertebral Column are synonymous terms referring to the bony components housing the spinal cord Spinal Cord = made of nervous tissue Facet = a small,
Clarification of Terms The Spine, Spinal Column, and Vertebral Column are synonymous terms referring to the bony components housing the spinal cord Spinal Cord = made of nervous tissue Facet = a small,
Clarification of Terms
 Clarification of Terms The Spine, Spinal Column, and Vertebral Column are synonymous terms referring to the bony components housing the spinal cord Spinal Cord = made of nervous tissue Facet = a small,
Clarification of Terms The Spine, Spinal Column, and Vertebral Column are synonymous terms referring to the bony components housing the spinal cord Spinal Cord = made of nervous tissue Facet = a small,
VERTEBRAL COLUMN VERTEBRAL COLUMN
 VERTEBRAL COLUMN FUNCTIONS: 1) Support weight - transmits weight to pelvis and lower limbs 2) Houses and protects spinal cord - spinal nerves leave cord between vertebrae 3) Permits movements - *clinical
VERTEBRAL COLUMN FUNCTIONS: 1) Support weight - transmits weight to pelvis and lower limbs 2) Houses and protects spinal cord - spinal nerves leave cord between vertebrae 3) Permits movements - *clinical
Atlanto-occipital Dislocation Joseph Junewick, MD FACR
 Atlanto-occipital Dislocation Joseph Junewick, MD FACR 09/23/2009 History 12 year old male restrained back seat passenger in a car hit by a snowplow. Diagnosis Atlanto-occipital Dislocation Discussion
Atlanto-occipital Dislocation Joseph Junewick, MD FACR 09/23/2009 History 12 year old male restrained back seat passenger in a car hit by a snowplow. Diagnosis Atlanto-occipital Dislocation Discussion
Surgical management of combined fracture of atlas associated with fracture of axis vertebrae (CAAF): Case Series
: Case Series") Romanian Neurosurgery (2015) XXIX 3: 335-341 335 Surgical management of combined fracture of atlas associated with fracture of axis vertebrae (CAAF): Case Series Guru Dutta Satyarthee, Gaurang Vaghani,
Romanian Neurosurgery (2015) XXIX 3: 335-341 335 Surgical management of combined fracture of atlas associated with fracture of axis vertebrae (CAAF): Case Series Guru Dutta Satyarthee, Gaurang Vaghani,
Prognosis of neurological deficits associated with upper cervical spine injuries
 Paraplegia (1995) 33, 195-202 1995 International Medical Society of Paraplegia All rights reserved 0031-1758/95 $9.00 Prognosis of neurological deficits associated with upper cervical spine injuries Y
Paraplegia (1995) 33, 195-202 1995 International Medical Society of Paraplegia All rights reserved 0031-1758/95 $9.00 Prognosis of neurological deficits associated with upper cervical spine injuries Y
CERVICAL SPINE EVALUATION MARK FIGUEROA PHYSICAL THERAPIST
 CERVICAL SPINE EVALUATION MARK FIGUEROA PHYSICAL THERAPIST OVERVIEW OF CLINICAL REASONING Stage of disorder Pathoanatomical diagnosis Signs and symptoms Consideration of the evidence gathered Common sense
CERVICAL SPINE EVALUATION MARK FIGUEROA PHYSICAL THERAPIST OVERVIEW OF CLINICAL REASONING Stage of disorder Pathoanatomical diagnosis Signs and symptoms Consideration of the evidence gathered Common sense
Unstable Jefferson Variant Atlas Fractures: An Unrecognized Cervical Injury
 1105 Unstable Jefferson Variant Atlas Fractures: An Unrecognized Cervical Injury Charles Lee 1 John H. Woodring We retrospectively reviewed the plain films and CT scans of 11 unstable atlas fractures from
1105 Unstable Jefferson Variant Atlas Fractures: An Unrecognized Cervical Injury Charles Lee 1 John H. Woodring We retrospectively reviewed the plain films and CT scans of 11 unstable atlas fractures from
AXIAL SKELETON FORM THE VERTICAL AXIS OF THE BODY CONSISTS OF 80 BONES INCLUDES BONES OF HEAD, VERTEBRAL COLUMN, RIBS,STERNUM
 AXIAL SKELETON FORM THE VERTICAL AXIS OF THE BODY CONSISTS OF 80 BONES INCLUDES BONES OF HEAD, VERTEBRAL COLUMN, RIBS,STERNUM APPENDICULAR SKELETON BONES OF THE FREE APPENDAGES & THEIR POINTS OF ATTACHMENTS
AXIAL SKELETON FORM THE VERTICAL AXIS OF THE BODY CONSISTS OF 80 BONES INCLUDES BONES OF HEAD, VERTEBRAL COLUMN, RIBS,STERNUM APPENDICULAR SKELETON BONES OF THE FREE APPENDAGES & THEIR POINTS OF ATTACHMENTS
1/15/2012. Cervical Spine Trauma. Who to Image. Who to Image. Who to Image. Who to Image. Trauma Cx Spine Protocols NEXUS. CCR and Nexus CCR CCR
 Trauma Cx Spine Protocols Cervical Spine Trauma Issues The clinically negative Cx-spine Does everyone need a CT Dr. Tudor H. Hughes M.D., FRCR Department of Radiology University of California School of
Trauma Cx Spine Protocols Cervical Spine Trauma Issues The clinically negative Cx-spine Does everyone need a CT Dr. Tudor H. Hughes M.D., FRCR Department of Radiology University of California School of
Clarification of Terms
 Clarification of Terms The Spine, Spinal Column, and Vertebral Column are synonymous terms referring to the bony components housing the spinal cord Spinal Cord = made of nervous tissue Facet = a small,
Clarification of Terms The Spine, Spinal Column, and Vertebral Column are synonymous terms referring to the bony components housing the spinal cord Spinal Cord = made of nervous tissue Facet = a small,
Spine Trauma- Part B
 Spine Trauma- Part B Cervical Spine Injuries Atlanto- Occipital Dislocation Hyperextension and distraction mechanism Down s syndrome, RA more susceptible Asymmetric lateral masses on odontoid view Widened
Spine Trauma- Part B Cervical Spine Injuries Atlanto- Occipital Dislocation Hyperextension and distraction mechanism Down s syndrome, RA more susceptible Asymmetric lateral masses on odontoid view Widened
INDEPENDENT LEARNING: DISC HERNIATION IN THE NATIONAL FOOTBALL LEAGUE: ANATOMICAL FACTORS TO CONSIDER IN REVIEW
 INDEPENDENT LEARNING: DISC HERNIATION IN THE NATIONAL FOOTBALL LEAGUE: ANATOMICAL FACTORS TO CONSIDER IN REVIEW CDC REPORT - CAUSES OF DISABILITY, 2005 REVIEW QUESTIONS ABOUT DISC HERNIATION IN THE NATIONAL
INDEPENDENT LEARNING: DISC HERNIATION IN THE NATIONAL FOOTBALL LEAGUE: ANATOMICAL FACTORS TO CONSIDER IN REVIEW CDC REPORT - CAUSES OF DISABILITY, 2005 REVIEW QUESTIONS ABOUT DISC HERNIATION IN THE NATIONAL
Case Report Occult Cranial Cervical Dislocation: A Case Report and Brief Literature Review
 Hindawi Publishing Corporation Volume 2016, Article ID 4930285, 6 pages http://dx.doi.org/10.1155/2016/4930285 Case Report Occult Cranial Cervical Dislocation: A Case Report and Brief Literature Review
Hindawi Publishing Corporation Volume 2016, Article ID 4930285, 6 pages http://dx.doi.org/10.1155/2016/4930285 Case Report Occult Cranial Cervical Dislocation: A Case Report and Brief Literature Review
Spinal Trauma. Dr T G Kruger
 Spinal Trauma Dr T G Kruger Epidemiology Spine injury in 6% of trauma patients Multiple levels involved in 20% of cases 80% of spinal cord injury patients have concurrent other system injuries 41% have
Spinal Trauma Dr T G Kruger Epidemiology Spine injury in 6% of trauma patients Multiple levels involved in 20% of cases 80% of spinal cord injury patients have concurrent other system injuries 41% have
Pitfalls in the Management of Atlanto-Occipital Dislocation
 Asian Spine Journal Asian Spine Case Journal Report Asian Spine J 2015;9(3):465-470 http://dx.doi.org/10.4184/asj.2015.9.3.465 Atlanto-occipital dislocation 465 Pitfalls in the Management of Atlanto-Occipital
Asian Spine Journal Asian Spine Case Journal Report Asian Spine J 2015;9(3):465-470 http://dx.doi.org/10.4184/asj.2015.9.3.465 Atlanto-occipital dislocation 465 Pitfalls in the Management of Atlanto-Occipital
Upper Cervical Spine Trauma
 Upper Cervical Spine Trauma Amit K. Bhandutia, MD Daniel T. Altman, MD December 2016 Created by Daniel Gelb, MD January 2006 Updated by Robert Morgan, MD November 2010 Upper Cervical Spine Trauma Epidemiology
Upper Cervical Spine Trauma Amit K. Bhandutia, MD Daniel T. Altman, MD December 2016 Created by Daniel Gelb, MD January 2006 Updated by Robert Morgan, MD November 2010 Upper Cervical Spine Trauma Epidemiology
James Buratto May 20 th, 2010
 James Buratto May 20 th, 2010 Discuss relevant anatomy Discuss methods for clinical triage Discuss imaging Discuss fracture types in the cervical spine Discuss classification systems ~150,000 injuries
James Buratto May 20 th, 2010 Discuss relevant anatomy Discuss methods for clinical triage Discuss imaging Discuss fracture types in the cervical spine Discuss classification systems ~150,000 injuries
Craniovertebral Junction Embryology and Anatomy. Presented by: Amandeep Moderators: S.S.Kale G.D.Satyarthi. CVJ-Embryology & Anatomy
 Craniovertebral Junction Embryology and Anatomy Presented by: Amandeep Moderators: S.S.Kale G.D.Satyarthi CVJ-Embryology & Anatomy CVJ-Embryology SOMITE-The building block of vertebrae, skeletal muscle
Craniovertebral Junction Embryology and Anatomy Presented by: Amandeep Moderators: S.S.Kale G.D.Satyarthi CVJ-Embryology & Anatomy CVJ-Embryology SOMITE-The building block of vertebrae, skeletal muscle
Craniocervical Traumatic Injuries: Evaluation and Surgical Decision Making
 37 Craniocervical Traumatic Injuries: Evaluation and Surgical Decision Making Andrei F. Joaquim 1 Alpesh A. Patel 2 1 Department of Neurology, State University of Campinas (UNICAMP), Campinas, SP, Brazil
37 Craniocervical Traumatic Injuries: Evaluation and Surgical Decision Making Andrei F. Joaquim 1 Alpesh A. Patel 2 1 Department of Neurology, State University of Campinas (UNICAMP), Campinas, SP, Brazil
Structure and Function of the Vertebral Column
 Structure and Function of the Vertebral Column Posture Vertebral Alignment Does it really matter? Yes it does! Postural Curves The vertebral column has a series of counterbalancing curves posterior anterior
Structure and Function of the Vertebral Column Posture Vertebral Alignment Does it really matter? Yes it does! Postural Curves The vertebral column has a series of counterbalancing curves posterior anterior
5/13/2009 K S. C ontraindications BACKGROUND METHODS 2 METHODS 1 CRANIOVERTEBRAL INSTABILITY TESTING. DO THE TESTS REALLY REFLECT THE ANATOMY?
 CRANIOVERTEBRAL INSTABILITY TESTING. DO THE TESTS REALLY REFLECT THE ANATOMY? Peter Osmotherly 1 Prof Darren Rivett 1 A/Prof Susan Mercer 2 1. School of Health Sciences, The University of Newcastle, Australia
CRANIOVERTEBRAL INSTABILITY TESTING. DO THE TESTS REALLY REFLECT THE ANATOMY? Peter Osmotherly 1 Prof Darren Rivett 1 A/Prof Susan Mercer 2 1. School of Health Sciences, The University of Newcastle, Australia
Paediatric cervical spine injuries: A pictorial review
 Paediatric cervical spine injuries: A pictorial review Poster No.: C-2863 Congress: ECR 2010 Type: Educational Exhibit Topic: Pediatric Authors: L. L. Wang, W. Thomas, K. Ng, C. C. Hiew ; Randwick/AU,
Paediatric cervical spine injuries: A pictorial review Poster No.: C-2863 Congress: ECR 2010 Type: Educational Exhibit Topic: Pediatric Authors: L. L. Wang, W. Thomas, K. Ng, C. C. Hiew ; Randwick/AU,
THE VERTEBRAL COLUMN. Average adult length: In male: about 70 cms. In female: about 65 cms.
 THE VERTEBRAL COLUMN Average adult length: In male: about 70 cms. In female: about 65 cms. 1 Vertebral Column (Regions and Curvatures) Curvatures of the vertebral column: A. Primary curvature: C-shaped;
THE VERTEBRAL COLUMN Average adult length: In male: about 70 cms. In female: about 65 cms. 1 Vertebral Column (Regions and Curvatures) Curvatures of the vertebral column: A. Primary curvature: C-shaped;
Imaging of Trauma to the Spine. Orthopedic Diplomate Program University of Bridgeport College of Chiropractic
 Imaging of Trauma to the Spine Orthopedic Diplomate Program University of Bridgeport College of Chiropractic Jefferson Fracture Yee, LL: The Jefferson Fracture, Radiology Cases in Pediatric Emergency Medicine.
Imaging of Trauma to the Spine Orthopedic Diplomate Program University of Bridgeport College of Chiropractic Jefferson Fracture Yee, LL: The Jefferson Fracture, Radiology Cases in Pediatric Emergency Medicine.
It consist of two components: the outer, laminar fibrous container (or annulus), and the inner, semifluid mass (the nucleus pulposus).
, and the inner, semifluid mass (the nucleus pulposus).") Lumbar Spine The lumbar vertebrae are the last five vertebrae of the vertebral column. They are particularly large and heavy when compared with the vertebrae of the cervical or thoracicc spine. Their bodies
Lumbar Spine The lumbar vertebrae are the last five vertebrae of the vertebral column. They are particularly large and heavy when compared with the vertebrae of the cervical or thoracicc spine. Their bodies
Fractures of the thoracic and lumbar spine and thoracolumbar transition
 Most spinal column injuries occur in the thoracolumbar transition, the area between the lower thoracic spine and the upper lumbar spine; over half of all vertebral fractures involve the 12 th thoracic
Most spinal column injuries occur in the thoracolumbar transition, the area between the lower thoracic spine and the upper lumbar spine; over half of all vertebral fractures involve the 12 th thoracic
The craniocervical relationships have been studied throughout
 ORIGINAL RESEARCH C.A. Rojas J.C. Bertozzi C.R. Martinez J. Whitlow Reassessment of the Craniocervical Junction: Normal Values on CT BACKGROUND AND PURPOSE: As the standard of care for the evaluation of
ORIGINAL RESEARCH C.A. Rojas J.C. Bertozzi C.R. Martinez J. Whitlow Reassessment of the Craniocervical Junction: Normal Values on CT BACKGROUND AND PURPOSE: As the standard of care for the evaluation of
CHAPTER 139 UPPER CERVICAL SPINE FRACTURES AND INSTABILITY
 Página 1 de 54 Copyright 2001 Lippincott Williams & Wilkins Chapman, Michael W. Chapman's Orthopaedic Surgery, 3rd Edition CHAPTER 139 UPPER CERVICAL SPINE FRACTURES AND INSTABILITY Claude Gelinas Alan
Página 1 de 54 Copyright 2001 Lippincott Williams & Wilkins Chapman, Michael W. Chapman's Orthopaedic Surgery, 3rd Edition CHAPTER 139 UPPER CERVICAL SPINE FRACTURES AND INSTABILITY Claude Gelinas Alan
AO CLASSIFICATIONS THORACO-LUMBAR SPINAL INJURIES
 AO CLASSIFICATIONS THORACO-LUMBAR SPINAL INJURIES T H E A O / A S I F ( A R B E I T S G E M E I N S C H A F T F Ü R O S T E O S Y N T H E S E F R A G E N / A S S O C I A T I O N F O R T H E S T U D Y O
AO CLASSIFICATIONS THORACO-LUMBAR SPINAL INJURIES T H E A O / A S I F ( A R B E I T S G E M E I N S C H A F T F Ü R O S T E O S Y N T H E S E F R A G E N / A S S O C I A T I O N F O R T H E S T U D Y O
Involvement of the spine is common in rheumatoid. Incidence been reported to be 85% radiologically but only 30% have neurological signs and symptoms.
 RHEUMATOID SPINE Involvement of the spine is common in rheumatoid. Incidence been reported to be 85% radiologically but only 30% have neurological signs and symptoms. When neurology is present it may manifest
RHEUMATOID SPINE Involvement of the spine is common in rheumatoid. Incidence been reported to be 85% radiologically but only 30% have neurological signs and symptoms. When neurology is present it may manifest
Copyright 2010 Pearson Education, Inc.
 E. VERTEBRAL COLUMN 1. The vertebral column extends from the skull to the pelvis and forms the vertical axis of the skeleton. 2. The vertebral column is composed of vertebrae that are separated by intervertebral
E. VERTEBRAL COLUMN 1. The vertebral column extends from the skull to the pelvis and forms the vertical axis of the skeleton. 2. The vertebral column is composed of vertebrae that are separated by intervertebral
102 Results RESULTS. Age Mean=S.D Range 42= years -84 years Number % <30 years years >50 years
 102 Results RESULTS A total of 50 cases were studied 39 males and 11females.Their age ranged between 16 years and 84 years (mean 42years). T1 and T2WI were acquired for all cases in sagittal and axial
102 Results RESULTS A total of 50 cases were studied 39 males and 11females.Their age ranged between 16 years and 84 years (mean 42years). T1 and T2WI were acquired for all cases in sagittal and axial
Spinal Dynamics I: The Axio-atlanto-occipital Assemblage
 Spinal Dynamics I: The Axio-atlanto-occipital Assemblage Bones interact through joints. The relative placements of bones across joints determine how they move in space. In this section we will consider
Spinal Dynamics I: The Axio-atlanto-occipital Assemblage Bones interact through joints. The relative placements of bones across joints determine how they move in space. In this section we will consider
Rheumatoid Arthritis and the Cervical Spine. Radiology Rounds November 21, 2006 Derek Haaland
 Rheumatoid Arthritis and the Cervical Spine Radiology Rounds November 21, 2006 Derek Haaland Laiho et al. Semin Arthritis Rheum. 2004:34;267. Laiho et al. Semin Arthritis Rheum. 2004:34;267. *Shen et al.
Rheumatoid Arthritis and the Cervical Spine Radiology Rounds November 21, 2006 Derek Haaland Laiho et al. Semin Arthritis Rheum. 2004:34;267. Laiho et al. Semin Arthritis Rheum. 2004:34;267. *Shen et al.
You have 24 vertebrae in your spinal column. Two are special enough to be individually named.
 You have 24 vertebrae in your spinal column. Two are special enough to be individually named. Your atlas (C01) and axis (C02) are very important vertebrae. Without them, head and neck movement would be
You have 24 vertebrae in your spinal column. Two are special enough to be individually named. Your atlas (C01) and axis (C02) are very important vertebrae. Without them, head and neck movement would be
Cervical Spine Trauma 2016 Nordic Trauma Society
 Cervical Spine Trauma 2016 Nordic Trauma Society Stuart E. Mirvis. M.D., FACR Department of Radiology and Maryland Shock-Trauma Center University of Maryland School of Medicine Topics to Review Definition
Cervical Spine Trauma 2016 Nordic Trauma Society Stuart E. Mirvis. M.D., FACR Department of Radiology and Maryland Shock-Trauma Center University of Maryland School of Medicine Topics to Review Definition
FRACTURES ACCORDING TO MECHANISM. Any combination of forces may occur in any single case!
 VERTEBRAL COLUMN INJURY (SPECIFIC INJURIES) TrS9 (1) Vertebral Column Injury (SPECIFIC INJURIES) Last updated: September 5, 2017 FRACTURES ACCORDING TO MECHANISM... 1 MECHANICAL STABILITY... 2 CERVICAL
VERTEBRAL COLUMN INJURY (SPECIFIC INJURIES) TrS9 (1) Vertebral Column Injury (SPECIFIC INJURIES) Last updated: September 5, 2017 FRACTURES ACCORDING TO MECHANISM... 1 MECHANICAL STABILITY... 2 CERVICAL
Spinal Trauma at the Pediatric Age
 Spinal Trauma at the Pediatric Age Burçak B LG NER Nejat AKALAN ABSTRACT Spinal trauma is relatively rare in pediatric patients. The anatomy and biomechanics of the growing spine produce failure patterns
Spinal Trauma at the Pediatric Age Burçak B LG NER Nejat AKALAN ABSTRACT Spinal trauma is relatively rare in pediatric patients. The anatomy and biomechanics of the growing spine produce failure patterns
Vertebral Column. Backbone consists of 26 vertebrae. Five vertebral regions. Cervical
 Vertebral Column Backbone consists of 26 vertebrae. Five vertebral regions Cervical vertebrae (7) in the neck. Thoracic vertebrae (12) in the thorax. Lumbar vertebrae (5) in the lower back. Sacrum (5,
Vertebral Column Backbone consists of 26 vertebrae. Five vertebral regions Cervical vertebrae (7) in the neck. Thoracic vertebrae (12) in the thorax. Lumbar vertebrae (5) in the lower back. Sacrum (5,
Case Report A Case of Delayed Myelopathy Caused by Atlantoaxial Subluxation without Fracture
 Case Reports in Orthopedics Volume 2013, Article ID 421087, 4 pages http://dx.doi.org/10.1155/2013/421087 Case Report A Case of Delayed Myelopathy Caused by Atlantoaxial Subluxation without Fracture Ryo
Case Reports in Orthopedics Volume 2013, Article ID 421087, 4 pages http://dx.doi.org/10.1155/2013/421087 Case Report A Case of Delayed Myelopathy Caused by Atlantoaxial Subluxation without Fracture Ryo
Ultimate Spinal Analysis PA USA-XRAY ( )
") Page: 1 Spine Atlas Angle 7.24 S Atlas Angle 21.67 S The Atlas Angle is a measurement of the stability of the Atlas. The Atlas Plane Line is compared to true horizontal. Any increase or decrease of this
Page: 1 Spine Atlas Angle 7.24 S Atlas Angle 21.67 S The Atlas Angle is a measurement of the stability of the Atlas. The Atlas Plane Line is compared to true horizontal. Any increase or decrease of this
ANATOMY & PHYSIOLOGY I Laboratory Version B Name Section. REVIEW SHEET Exercise 10 Axial Skeleton
 ANATOMY & PHYSIOLOGY I Laboratory Version B Name Section REVIEW SHEET Exercise 10 Axial Skeleton 1 POINT EACH. THE SKULL MULTIPLE CHOICE 1. The major components of the axial skeleton include the 7. The
ANATOMY & PHYSIOLOGY I Laboratory Version B Name Section REVIEW SHEET Exercise 10 Axial Skeleton 1 POINT EACH. THE SKULL MULTIPLE CHOICE 1. The major components of the axial skeleton include the 7. The
Any of the vertebra in the cervical (neck) region of the spinal column. The cervical vertebra are the smallest vertebra in the spine, reflective of th
 region of the spinal column. The cervical vertebra are the smallest vertebra in the spine, reflective of th") Any of the vertebra in the cervical (neck) region of the spinal column. The cervical vertebra are the smallest vertebra in the spine, reflective of the fact that they support the least load. In humans,
Any of the vertebra in the cervical (neck) region of the spinal column. The cervical vertebra are the smallest vertebra in the spine, reflective of the fact that they support the least load. In humans,
Detailed Finite Element Modeling of the Human Ligamentous Cervical Spine. Faisal Agah
 Detailed Finite Element Modeling of the Human Ligamentous Cervical Spine by Faisal Agah A thesis submitted in partial fulfillment of the requirements for the degree of Master of Science in Structural Engineering
Detailed Finite Element Modeling of the Human Ligamentous Cervical Spine by Faisal Agah A thesis submitted in partial fulfillment of the requirements for the degree of Master of Science in Structural Engineering
No greater tragedy can befall on a young adult in this most
 SUPPLEMENT TO JAPI may 2012 VOL. 60 19 Operative Management of Spinal Injuries Sajan Hegde * Introduction No greater tragedy can befall on a young adult in this most active period of life than a spinal
SUPPLEMENT TO JAPI may 2012 VOL. 60 19 Operative Management of Spinal Injuries Sajan Hegde * Introduction No greater tragedy can befall on a young adult in this most active period of life than a spinal
C2 Body Fracture: Report of Cases Managed Conservatively by Philadelphia Collar
 C2 Body Fracture: Report of Cases Managed Conservatively by Philadelphia Collar The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters.
C2 Body Fracture: Report of Cases Managed Conservatively by Philadelphia Collar The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters.
Cervical Cooled RF Training Presentation
 Cervical Cooled RF Training Presentation Agenda Patient Selection Considerations Diagnostic Block General Considerations COOLIEF* Cooled RF Technique Posterior Lateral Precautions Summary Appendix 2 Disclaimer
Cervical Cooled RF Training Presentation Agenda Patient Selection Considerations Diagnostic Block General Considerations COOLIEF* Cooled RF Technique Posterior Lateral Precautions Summary Appendix 2 Disclaimer
Original article: Multidetector computed tomographic evaluation of cervical spine trauma
 Original article: Multidetector computed tomographic evaluation of cervical spine trauma 1Sajid Ansari *, 2 R.K. Rauniyar, 3 Kaleem Ahmad, 4 Mukesh Kumar Gupta 1Assistant Professor, Department of Radiodiagnosis,
Original article: Multidetector computed tomographic evaluation of cervical spine trauma 1Sajid Ansari *, 2 R.K. Rauniyar, 3 Kaleem Ahmad, 4 Mukesh Kumar Gupta 1Assistant Professor, Department of Radiodiagnosis,
Anterior Cervical Subluxation: An Unstable Position
 275 Anterior Cervical Subluxation: An Unstable Position, 1 A. T. Scher1 The radioiogic signs of cervical anterior subluxation are subtle. Even when recognized, the injury may not be considered significant.
275 Anterior Cervical Subluxation: An Unstable Position, 1 A. T. Scher1 The radioiogic signs of cervical anterior subluxation are subtle. Even when recognized, the injury may not be considered significant.
Chapter 7 Part B The Skeleton
 Chapter 7 Part B The Skeleton 7.2 The Vertebral Column General Characteristics Extends from skull to pelvis Also called spine or spinal column Functions to transmit weight of trunk to lower limbs, surround
Chapter 7 Part B The Skeleton 7.2 The Vertebral Column General Characteristics Extends from skull to pelvis Also called spine or spinal column Functions to transmit weight of trunk to lower limbs, surround
Cervical Spine Injury Guidelines
 6/15/2018 Cervical Spine Injury Guidelines Benjamin Oshlag, MD, CAQSM Assistant Professor of Emergency Medicine Assistant Professor of Sports Medicine Columbia University Medical Center Nothing to Disclose
6/15/2018 Cervical Spine Injury Guidelines Benjamin Oshlag, MD, CAQSM Assistant Professor of Emergency Medicine Assistant Professor of Sports Medicine Columbia University Medical Center Nothing to Disclose
human anatomy 2015 lecture four Dr meethak ali ahmed neurosurgeon
 The Vertebral Column the vertebral columnis central pillar of the body.it serve to protect the spinal cord and support the weight of the head trunk, which it transmits to the hip bones & the lower limbs.
The Vertebral Column the vertebral columnis central pillar of the body.it serve to protect the spinal cord and support the weight of the head trunk, which it transmits to the hip bones & the lower limbs.
Development of a Novel Biofedelic Skull-Neck- Thorax Model Capable of Quantifying Motions of aged Cervical Spine
 Yale University EliScholar A Digital Platform for Scholarly Publishing at Yale Yale Medicine Thesis Digital Library School of Medicine 11-23-2009 Development of a Novel Biofedelic Skull-Neck- Thorax Model
Yale University EliScholar A Digital Platform for Scholarly Publishing at Yale Yale Medicine Thesis Digital Library School of Medicine 11-23-2009 Development of a Novel Biofedelic Skull-Neck- Thorax Model
SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services OBJECTIVES DEFINITION 11/8/2017. Identify SCIWORA.
 SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services Identify SCIWORA. OBJECTIVES Identify the population at risk. To identify anatomic and physiologic reasons for SCIWORA. To
SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services Identify SCIWORA. OBJECTIVES Identify the population at risk. To identify anatomic and physiologic reasons for SCIWORA. To
Musculoskeletal Development and Sports Injuries in Pediatric Patients
 Dynamic Chiropractic October 21, 2010, Vol. 28, Issue 22 Musculoskeletal Development and Sports Injuries in Pediatric Patients By Deborah Pate, DC, DACBR Physical activity is extremely important for everyone,
Dynamic Chiropractic October 21, 2010, Vol. 28, Issue 22 Musculoskeletal Development and Sports Injuries in Pediatric Patients By Deborah Pate, DC, DACBR Physical activity is extremely important for everyone,
ESSENTIALS OF PLAIN FILM INTERPRETATION: SPINE DR ASIF SAIFUDDIN
 ESSENTIALS OF PLAIN FILM INTERPRETATION: SPINE DR ASIF SAIFUDDIN Consultant Musculoskeletal Radiologist Royal National Orthopaedic Hospital Stanmore,UK. INTRODUCTION 2 INTRODUCTION 3 INTRODUCTION Spinal
ESSENTIALS OF PLAIN FILM INTERPRETATION: SPINE DR ASIF SAIFUDDIN Consultant Musculoskeletal Radiologist Royal National Orthopaedic Hospital Stanmore,UK. INTRODUCTION 2 INTRODUCTION 3 INTRODUCTION Spinal
Posterior cervical fusion in children
 Posterior cervical fusion in children JOE M. MCWHORTER, M.D., EBEN ALEXANDER, JR., M.D., COURTLAND H. DAVIS, JR., M.D., AND DAVID L. KELLY, JR., M.D. Section on Neurosurgery, Department of Surgery, Bowman
Posterior cervical fusion in children JOE M. MCWHORTER, M.D., EBEN ALEXANDER, JR., M.D., COURTLAND H. DAVIS, JR., M.D., AND DAVID L. KELLY, JR., M.D. Section on Neurosurgery, Department of Surgery, Bowman
Physical and Radiographic Examination of the Spine
 Physical and Radiographic Examination of the Spine Christopher M. Bono, MD Assistant Professor, Department of Orthopaedic Surgery Boston University School of Medicine, Boston Medical Center, Boston, MA
Physical and Radiographic Examination of the Spine Christopher M. Bono, MD Assistant Professor, Department of Orthopaedic Surgery Boston University School of Medicine, Boston Medical Center, Boston, MA
4/28/2010. Fractures. Normal Bone and Normal Ossification Bone Terms. Epiphysis Epiphyseal Plate (physis) Metaphysis
 Metaphysis") Fractures Normal Bone and Normal Ossification Bone Terms Epiphysis Epiphyseal Plate (physis) Metaphysis Diaphysis 1 Fracture Classifications A. Longitudinal B. Transverse C. Oblique D. Spiral E. Incomplete
Fractures Normal Bone and Normal Ossification Bone Terms Epiphysis Epiphyseal Plate (physis) Metaphysis Diaphysis 1 Fracture Classifications A. Longitudinal B. Transverse C. Oblique D. Spiral E. Incomplete
Conservative management of craniovertebral junction injuries: Still a good option
 SNI: Spine OPEN ACCESS For entire Editorial Board visit : http://www.surgicalneurologyint.com Editor: Nancy E. Epstein, MD Winthrop University Hospital, Mineola, NY, USA Original Article Conservative management
SNI: Spine OPEN ACCESS For entire Editorial Board visit : http://www.surgicalneurologyint.com Editor: Nancy E. Epstein, MD Winthrop University Hospital, Mineola, NY, USA Original Article Conservative management
DIAGNOSTIC VIDEOFLUOROSCOPY IMPRESSIONS and BIOMECHANICS REPORT
 P.O. Box 6743 New Albany, IN 47151-6743 (812) 945-5515 (812) 945-5632 Fax WWW.KMX.CC DIAGNOSTIC VIDEOFLUOROSCOPY IMPRESSIONS and BIOMECHANICS REPORT Patient Name: Lubna Ibriham Date of Digitization and
P.O. Box 6743 New Albany, IN 47151-6743 (812) 945-5515 (812) 945-5632 Fax WWW.KMX.CC DIAGNOSTIC VIDEOFLUOROSCOPY IMPRESSIONS and BIOMECHANICS REPORT Patient Name: Lubna Ibriham Date of Digitization and
Chest cavity, vertebral column and back muscles. Respiratory muscles. Sándor Katz M.D., Ph.D.
 Chest cavity, vertebral column and back muscles. Respiratory muscles. Sándor Katz M.D., Ph.D. Chest cavity - bony structures Chest cavity- bony structures Sternum Ribs True ribs: first seven pairs connect
Chest cavity, vertebral column and back muscles. Respiratory muscles. Sándor Katz M.D., Ph.D. Chest cavity - bony structures Chest cavity- bony structures Sternum Ribs True ribs: first seven pairs connect
The Positive Findings In Neck Injuries. American Journal of Orthopedics. August-September, 1964, pp
 The Positive Findings In Neck Injuries 1 American Journal of Orthopedics August-September, 1964, pp. 178-187 Ruth Jackson, MD This author analyzed 5,000 patients with disorders and found the following:
The Positive Findings In Neck Injuries 1 American Journal of Orthopedics August-September, 1964, pp. 178-187 Ruth Jackson, MD This author analyzed 5,000 patients with disorders and found the following:
Classification of Thoracolumbar Spine Injuries
 Classification of Thoracolumbar Spine Injuries Guillem Saló Bru 1 IMAS. Hospitals del Mar i de l Esperança. ICATME. Institut Universitari Dexeus USP. UNIVERSITAT AUTÒNOMA DE BARCELONA Objectives of classification
Classification of Thoracolumbar Spine Injuries Guillem Saló Bru 1 IMAS. Hospitals del Mar i de l Esperança. ICATME. Institut Universitari Dexeus USP. UNIVERSITAT AUTÒNOMA DE BARCELONA Objectives of classification
Imaging of Orthopedic Spinal Devices: What Every Radiologist Should Know.
 Imaging of Orthopedic Spinal Devices: What Every Radiologist Should Know. Poster No.: C-1656 Congress: ECR 2016 Type: Educational Exhibit Authors: E. Federici, C. Dell'atti, M. Bartocci, D. Beomonte Zobel,
Imaging of Orthopedic Spinal Devices: What Every Radiologist Should Know. Poster No.: C-1656 Congress: ECR 2016 Type: Educational Exhibit Authors: E. Federici, C. Dell'atti, M. Bartocci, D. Beomonte Zobel,
Human Anatomy and Physiology - Problem Drill 07: The Skeletal System Axial Skeleton
 Human Anatomy and Physiology - Problem Drill 07: The Skeletal System Axial Skeleton Question No. 1 of 10 Which of the following statements about the axial skeleton is correct? Question #01 A. The axial
Human Anatomy and Physiology - Problem Drill 07: The Skeletal System Axial Skeleton Question No. 1 of 10 Which of the following statements about the axial skeleton is correct? Question #01 A. The axial
Copyright 2010 Pearson Education, Inc. Copyright 2010 Pearson Education, Inc. Figure Sectioned spinous process. Interspinous.
 PowerPoint Lecture Slides prepared by Janice Meeking, Mount Royal College C H A P T E R 7 The Skeleton: Part B Vertebral Column Transmits weight of trunk to lower limbs Surrounds and protects spinal cord
PowerPoint Lecture Slides prepared by Janice Meeking, Mount Royal College C H A P T E R 7 The Skeleton: Part B Vertebral Column Transmits weight of trunk to lower limbs Surrounds and protects spinal cord
VERTEBRAL COLUMN ANATOMY IN CNS COURSE
 VERTEBRAL COLUMN ANATOMY IN CNS COURSE Vertebral body Sections of the spine Atlas (C1) Axis (C2) What type of joint is formed between atlas and axis? Pivot joint What name is given to a fracture of both
VERTEBRAL COLUMN ANATOMY IN CNS COURSE Vertebral body Sections of the spine Atlas (C1) Axis (C2) What type of joint is formed between atlas and axis? Pivot joint What name is given to a fracture of both
1 Normal Anatomy and Variants
 1 Normal Anatomy and Variants 1.1 Normal Anatomy MR Technique. e standard MR protocol for a routine evaluation of the spine always comprises imaging in sagittal and axial planes, while coronal images are
1 Normal Anatomy and Variants 1.1 Normal Anatomy MR Technique. e standard MR protocol for a routine evaluation of the spine always comprises imaging in sagittal and axial planes, while coronal images are
SURGICAL AND APPLIED ANATOMY
 Página 1 de 6 Copyright 2001 Lippincott Williams & Wilkins Bucholz, Robert W., Heckman, James D. Rockwood & Green's Fractures in Adults, 5th Edition SURGICAL AND APPLIED ANATOMY Part of "37 - HIP DISLOCATIONS
Página 1 de 6 Copyright 2001 Lippincott Williams & Wilkins Bucholz, Robert W., Heckman, James D. Rockwood & Green's Fractures in Adults, 5th Edition SURGICAL AND APPLIED ANATOMY Part of "37 - HIP DISLOCATIONS
The Trunk and Spinal Column Kinesiology Cuneyt Mirzanli Istanbul Gelisim University
 The Trunk and Spinal Column Kinesiology Cuneyt Mirzanli Istanbul Gelisim University The Trunk and Spinal Column Vertebral column 24 articulating vertebrae 31 pairs of spinal nerves Abdominal muscles some
The Trunk and Spinal Column Kinesiology Cuneyt Mirzanli Istanbul Gelisim University The Trunk and Spinal Column Vertebral column 24 articulating vertebrae 31 pairs of spinal nerves Abdominal muscles some
Papers Arising from the Vertebral Artery Study
 Papers Arising from the Vertebral Artery Study 1. Brief Introduction to quaternions and framed vectors and their application to the description of anatomical movements. The mathematical description of
Papers Arising from the Vertebral Artery Study 1. Brief Introduction to quaternions and framed vectors and their application to the description of anatomical movements. The mathematical description of
The Back. Anatomy RHS 241 Lecture 9 Dr. Einas Al-Eisa
 The Back Anatomy RHS 241 Lecture 9 Dr. Einas Al-Eisa The spine has to meet 2 functions Strength Mobility Stability of the vertebral column is provided by: Deep intrinsic muscles of the back Ligaments
The Back Anatomy RHS 241 Lecture 9 Dr. Einas Al-Eisa The spine has to meet 2 functions Strength Mobility Stability of the vertebral column is provided by: Deep intrinsic muscles of the back Ligaments
Spine and Spinal Cord Injury in Children
 Spine and Spinal Cord Injury in Children S. Danielle Brown, MS, RN, CNRN, SCRN Director, Research Coordination and Education Barrow Neurological Institute at Phoenix Children s Hospital Introduction Trauma
Spine and Spinal Cord Injury in Children S. Danielle Brown, MS, RN, CNRN, SCRN Director, Research Coordination and Education Barrow Neurological Institute at Phoenix Children s Hospital Introduction Trauma
The sacrum is a complex anatomical structure.
 A Review Paper Rongming Xu, MD, Nabil A. Ebraheim, MD, and Nicholas K. Gove, MD Abstract Treatment in spinal disorders, sacroiliac joint disruption, and sacral fractures may involve instrumentation of
A Review Paper Rongming Xu, MD, Nabil A. Ebraheim, MD, and Nicholas K. Gove, MD Abstract Treatment in spinal disorders, sacroiliac joint disruption, and sacral fractures may involve instrumentation of
RETROLISTHESIS. Retrolisthesis. is found mainly in the cervical spine and lumbar region but can also be often seen in the thoracic spine
 RETROLISTHESIS A retrolisthesis is a posterior displacement of one vertebral body with respect to adjacent vertebrae Typically a vertebra is to be in retrolisthesis position when it translates backward
RETROLISTHESIS A retrolisthesis is a posterior displacement of one vertebral body with respect to adjacent vertebrae Typically a vertebra is to be in retrolisthesis position when it translates backward
International Journal of Pharma and Bio Sciences
 Original Research Article Anatomy and Allied sciences International Journal of Pharma and Bio Sciences ISSN 0975-6299 SCREENING FOR ANOMALIES IN OCCIPITO-CERVICAL JUNCTION USING CRANIOMETRY IN COMPUTED
Original Research Article Anatomy and Allied sciences International Journal of Pharma and Bio Sciences ISSN 0975-6299 SCREENING FOR ANOMALIES IN OCCIPITO-CERVICAL JUNCTION USING CRANIOMETRY IN COMPUTED
Axial Skeleton: Vertebrae and Thorax
 Axial Skeleton: Vertebrae and Thorax Function of the vertebral column (spine or backbone): 1) 2) 3) Composition of Vertebral column The vertebral column is formed by 33 individual vertebrae (some of which
Axial Skeleton: Vertebrae and Thorax Function of the vertebral column (spine or backbone): 1) 2) 3) Composition of Vertebral column The vertebral column is formed by 33 individual vertebrae (some of which