Training Course in Sexual and Reproductive Health Research Geneva, February Osteoporosis. Prof René Rizzoli M.D.
|
|
|
- Kelly Moore
- 5 years ago
- Views:
Transcription
1 Training Course in Sexual and Reproductive Health Research Geneva, February Osteoporosis Prof René Rizzoli M.D. Division of bone diseases WHO collaborating center for osteoporosis prevention Department of rehabilitation and geriatrics Geneva university hospitals and Faculty of medicine Geneva, Switzerland
2
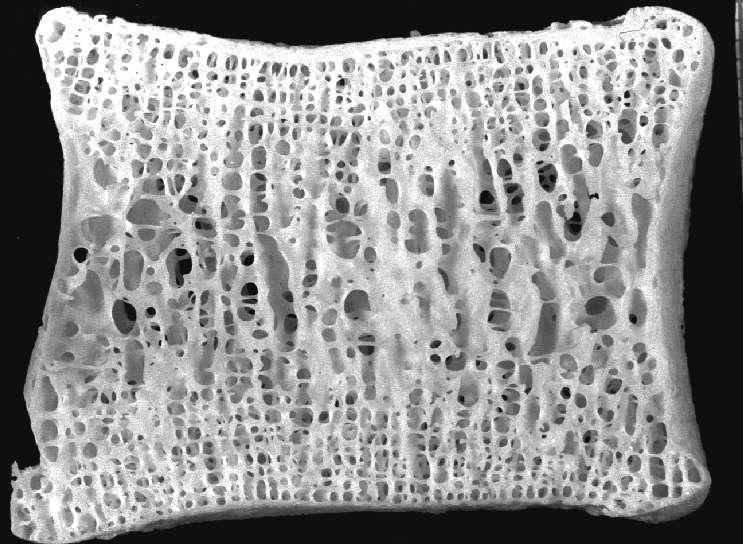
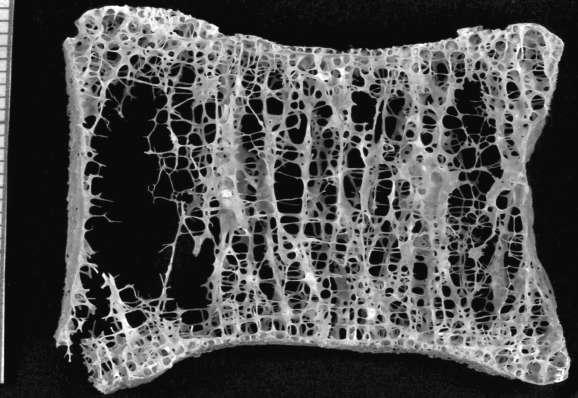
3 Osteoporosis Definition A systemic skeletal disease characterized by low bone mass and microarchitectural deterioration, with a consequent increase in bone fragility with susceptibility to fracture. Consensus Development Conference: Am J Med 1991;90:

4 Osteoporosis: a 2-Stage Disease With Without Fracture
5 Osteoporosis: Lecture Content Disease Definition Epidemiology Burden Diagnosis Pathophysiology Management

6
7 Fractures by Age and Gender Dubbo Osteoporosis Epidemiology Study, Minor Fractures Other Major Fractures Vertebral Fractures Proximal Femur Fractures Center J et al. Lancet. 1999;353: Women Men Women Men Women Men > 80 Age Group (Years)
8 Lifetime risk of fragility fracture in the Swedish population at the age of 50 years (%) Women Men Proximal femur Distal forearm 21 5 Vertebral (clinical) 15 8 Proximal Humerus 13 5 Any 46 % 22 % (Switzerland 51 % 20 %) From Kanis et al 2000
9 Annual incidence x 1000 Osteoporotic Fractures in Women: Comparison With Other Diseases * hip forearm other sites vertebral * annual incidence all ages annual estimate women 29+ annual estimate women new cases,all ages Osteoporotic Fractures Heart Attack Stroke Breast Cancer Riggs BL, Melton LJ. Bone Heart and Stroke Facts American Heart Association. Cancer Facts & Figures American Cancer Society.
10 Projected burden of osteoporotic 3250 hip fractures worldwide Estimated n of hip Fractures (1000s) North America Europe Latin America Asia Number of hip fractures: 1990: 1.66 million; 2050: 6.26 million Adapted from Cooper C., Melton U, Osteoporosis Int 2: , 1992
11 If the prevalence of hip fracture continues to rise at current rates, it may well be that in the next few decades, orthopaedists will do little else but treat this problem. W. C. Hayes, In: Bone Formation and Repair (American Academy of Orthopaedic Surgeons) 1994

12 Burden
13 Degree of dependence Hip fracture Vertebral fracture Forearm fracture normal aging Age (years)
14 Morbidity After Vertebral Fractures Back pain Loss of height Deformity (kyphosis, protuberant abdomen) Reduced pulmonary function Diminished quality of life: loss of self-esteem, distorted body image, dependence on narcotic analgesics, sleep disorder, depression, loss of independence
15 A Fragility Fracture -> Fracture
16 A dangerous vicious circle Low bone mass Social isolation New fracture Depression Loss of autonomy Pain First fracture Inactivity
17 Mortality after Major Types of Osteoporotic Fracture in Men and Women: an Observational Study Center et al, Lancet Year Prospective Cohort Study Age-Standardized Mortality Ratio Fracture Women Men Proximal Femur Vertebral Other Major Other Minor
18 Survival probability 1.00 Survival after Hip Fracture Trombetti et al, Osteoporos Int 2002 Expected survival in the the general population 0.75 Hip fractured Women Women Hip fractured Men Men Time after hip fracture (years)
19 Disability-Adjusted Life-Years Lost because of Non-communicable Diseases in Europe Osteoporosis Ischemic Heart Diseases Chronic Obstructive Pulmonary Diseases Osteoarthritis Alzheimer s Cirrhosis Asthma Migraine Hypertensive Heart Disease Rheumatoid Arthritis Peptic Ulcer Parkinson s Multiple Sclerosis Benign Prostatic Hyperplasia Johnell & Kanis, Osteoporos Int Disability-Adjusted Life-Years (DALYs) Lost
20 Osteoporosis Results in More Cost than Many Other Diseases Number of bed days (men and women) 701,000 for osteoporosis 891,000 for COPD 533,000 for stroke 328,000 for myocardial infarction 201,000 for breast cancer Osteoporosis # 1 when looking at women only Lippuner et al. Osteoporosis Int 1997; 7:
21 Diagnosis





22 pdxa X-ray techniques pqct DXA
23 DXA: Principle Two attenuation profiles: Low energy X-ray attenuation High energy X-ray attenuation I o Multiply high energy profile by k factor (ratio of soft tissue attenuation at low- & high-energy) I BMD along scan = Low-energy profile - k-corrected high energy profile
24 Relative risk 12 Gradients of risk BMD & Hip fracture BP & stroke Cholesterol & MI 2 0 I II III IV Quartile
25 Noninvasive Measurement of Bone Mineral Mass Technique Site Precision Cost Response to Therapy SXA Forearm ++ ± ± Heel DXA Spine Hip Tot. Body ++ + ± QCT Spine ± ++ + Forearm ++ +(+) ± US Heel ± Fingers
26 JAMA 288: ,2002 Medicare Coverage for BMD Tests Procedure Site Fee Schedule Medicare * DXA Axial $ 128 pdxa Appendicular $ 40 RX Absorptiometry Appendicular $ 38 QUS Appendicular $ 53 SXA Appendicular $ 40 QCT Axial $ 185 pqct Appendicular $ 40 * Medicare Allowable Charge = 80% of the Costs
27 Example for T-score = - 2.0, 60 year old and Z-Score = Spine: L1-L4 T-Score +1 BMD g/cm T Z Age
28 Diagnosis of Osteoporosis Using Central DXA WHO-Definition Normal -1 T-score Osteopenia < -1 and > -2.5 Osteoporosis -2.5 Severe Osteoporosis -2.5 with Fracture Mainly for Spine and Hip in Women
29 Pathophysiology
30 Osteoporosis Pathogenesis and Management Fracture Fracture Treatment Rehabilitation -> To Restore Independence -> To Reduce Disabilities Prevention Subsequent Fracture
31 Osteoporosis Pathogenesis and Management Osteoporosis Low Peak Bone Mass Sex Hormone Deficiency Age Nutritional Insufficiency Mechanical Incompetence Fracture Fracture Treatment Rehabilitation -> To Restore Independence -> To Reduce Disabilities Prevention Subsequent Fracture
32 Osteoporosis Pathogenesis and Management Falls Sway Walking Muscle Strength Neuro-muscular Impairment Mechanical Overload Osteoporosis Low Peak Bone Mass Sex Hormone Deficiency Age Nutritional Insufficiency Mechanical Incompetence Fracture Fracture Treatment Rehabilitation -> To Restore Independence -> To Reduce Disabilities Prevention Subsequent Fracture
33 Determinants of Fracture Risk 1.Age 2. Prevalent Fracture 3. Family history of Fracture 4. Glucocorticoid 5. Low BMI 6. Alkohol, Smoking 7. Baseline BMD 8. Baseline Turnover
34 Type I collagen epitopes and Cathepsin K cleavage sites NTX ICTP CTX CK CK CK CK a2 (I) JYDGKGVG GPP-SAGFDFSFLPQPPQ EKAHDGGR a 1 N C CK Deoxypyridinoline Pyridinolines CK Garnero et al., JBC, 1998 Sassi et al., Bone, 2000
35 Bone Mineral Mass Tracking of Bone Mineral Mass Fracture Risk A B Age (years) 50 90
36 Age: Rizzoli et al.,j Mol Endocrinol 2001

37 Heredity Gender Mechanical Forces Peak Bone Mass Hormones Risk Factors Nutrition
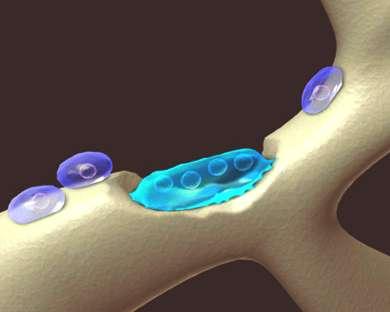
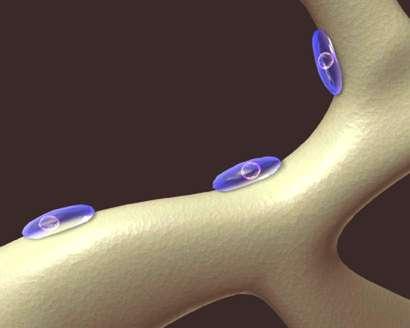
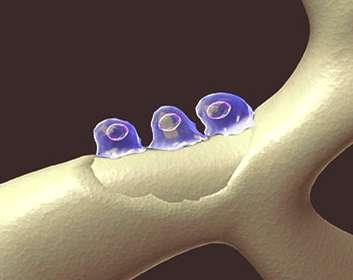
38 Resorption Reversal Resting Formation



39 Coupled and balanced Coupled but imbalanced Uncoupled but balanced Uncoupled and imbalanced
40 MALNUTRITION IN ELDERLY Calcium Deficiency Vitamin D Deficiency - > PTH - > Bone Resorption OSTEOPOROSIS - > IGF-1 Protein Deficiency - > Bone Formation - > Sensitivity to IGF-1
41 Management Indication to treatment Treatment possibilities
42 Subjects Number Osteoporosis Preventive Strategies Present Situation Higher Risk Population Modfication Whole Population Modification Target very High Risk BMD (SD units)
43 Probability of osteoporotic fracture* at age 65 Men Women 10-year probability (%) None Prior fracture +Glucocorticoids +Family history T-score US Caucasian, no CRF, BMI=24 *Hip, spine, humerus, forearm


44 06ca106 FRAX Patient
45 10-Year Risk: 10% 2 20% 30% 40% 1 50% Age
46 General Management Treatment of any Disease Causing Bone Loss Ensure Dietary Calcium Intake 1000 mg /d Ensure Adequate Dietary Protein Intake Correct or Prevent Vitamin D Insufficiency (800 IU/d) Promote Weight-Bearing Physical Exercise Reduce Falling Risk Reduce Fall Consequences (Hip Protectors)
47 Risk Factors Associated with Falls 1. Impaired Mobility, Disability 2. Impaired Gait and Balance 3. Neuromuscular or Musculoskeletal Disorders 4. Age 5. Impaired Vision 6. Neurological, Heart Disorders 7. History of Falls 8. Medication 9. Cognitive Impairment After Myers et al., Bone 1996

48 The Hip Protector Hip Fracture Prevention RCT in Community: No RCT in Nursing Homes: Cluster Random.: Yes Individual Random.: No Left vs Right: No Problems Compliance Persistence



 Parathyroid Hormone")
49 Therapeutic Agents Used in Osteoporosis Anticatabolic Agents Estrogens ± Progestagens SERMs Bisphosphonates Calcitonin Calcium Denosumab Complex Action Vitamin D and Derivatives Anabolic Steroids (Ipriflavone) Tibolone Anabolic Agents (Fluoride) Parathyroid Hormone Mixed Action Strontium Ranelate
50 Vitamin D and Risk of Falling H. Bischoff-Ferrrari et al JAMA 2004

51 Hormone Replacement Therapy and Fracture Risk Hip Placebo HRT Vertebral WHI Study, Cauley et al, 2003 All Fractures
52 Difference % vs. placebo Cardiovascular diseases Stroke Tromb. venous Breast cancer Intestinal cancer Vertebral fracture Hip fracture Women s Health Initiative - First randomized, controlled trial in women (50-79 years) treated with HRT 6700 women with 5.2 years of follow-up Disadvantages +112% +29% +41% +26% -37% -34% -34% Advantages Manson JE at al, N Engl J Med, 2003;349:
53 RLX 60 (MORE)* RLX 60 (MORE)** ALN 5/10 (FIT1)* ALN 5/10 (FIT2)** Anti -fracture efficacy (RR ± 95% CI) Vertebral Fx RIS 5 (VERT-NA)* RIS 5 (VERT-MN)* IBAN 2.5 *** IBAN inter ZOL CT 200 (PROOF)* Teriparatide 20µg* Strontium ranelate (SOTI)* Strontium ranelate (SOTI +TROPOS)** * with prev vert fracture(s) ** without prev vert fractures *** with or without prev vert fractures Update from Delmas 2002
54 Anti -fracture efficacy (RR ± 95% CI) Vertebral Fx Non-Vertebral Fx RLX 60 (MORE)* RLX 60 (MORE)** RLX 60, 120 (MORE)*** ALN 5/10 (FIT1)* ALN 5/10 (FIT1)* ALN 5/10 (FIT2)** ALN 5/10 (FIT2)** RIS 5 (VERT-NA)* RIS 5 (VERT-MN)* IBAN 2.5 *** IBAN inter ZOL RIS 5 (VERT-NA)* RIS 5 (VERT-MN)* RIS 2.5/5 (Hip Study)*** IBAN ZOL CT 200 (PROOF)* Teriparatide 20µg* Strontium ranelate (SOTI)* Strontium ranelate (SOTI +TROPOS)** CT 200 (PROOF)* Teriparatide 20µg* Strontium ranelate (SOTI)* Strontium ranelate (TROPOS)*** * with prev vert fracture(s) ** without prev vert fractures *** with or without prev vert fractures Update from Delmas 2002
55 Anti -fracture efficacy (RR ± 95% CI) RLX 60, 120 (MORE)*** Hip Fx Significant hip fracture risk Reduction: 3 studies Only studies with preplanned analysis: RIS 2.5/5 (Hip Study) ZOL 5 mg (Horizon Study) ALN 5/10 (FIT1)* ALN 5/10 (FIT2)** RIS 5 (VERT-NA)* RIS 5 (VERT-MN)* RIS 2.5/5 (Hip Study)*** IBAN ZOL CT 200 (PROOF)* Teriparatide 20µg* Strontium ranelate (SOTI)* Strontium ranelate (TROPOS)*** * with prev vert *** with or without prev vert fractures
56 Bisphosphonate New Schedules of Administration 1. Weekly (Alendronate, Risedronate) -> Monthly Oral Administration - Ibandronate - Risedronate 2. Trimonthly Intravenous Administration - Ibandronate 3. Annual Intravenous Administration - Zoledronate * 4. Sequential Regimen (PTH -> ALN, RIS or ALN -> PTH) *: Fracture Data
57 Mechanism of Action of Denosumab Growth Factors Hormones Cytokines Denosumab OPG RANKL RANK CFU-M Pre-Fusion Osteoclast Multinucleated Osteoclast BONE Activated Osteoclast
58 Incidence (%) Phase III Trial on the Effects of Denosumab on Vertebral Fracture Risk in Women with Postmenopausal Osteoporosis Reduction in vertebral fracture risk 78 % p < 0, % p < 0,0001 3, % p < 0,0001 3,1 % 3,1 % Placebo 2,5 2 2,2 % Denosumab 1,5 1 0,9 % 0,7 % 1,1 % 0,5 0 Year Year Year ASBMR D après Cummings S.R. et al., San Francisco, États-Unis, abstract 1286,
59 Cumulative Incidence (%) Cumulative Incidence (%) Phase III Trial on the Effects of Denosumab on Non-Vertebral Fracture Risk in Women with Postmenopausal Osteoporosis Hip Fractures Non-Vertebral Fractures 2,0 1,5 1,0 0,5 Placebo Denosumab Hip Fracture : 69 1,2 % 0,7 % 40 % p = 0,036 IC 95 : Placebo Denosumab 8,0 % No-Vertebral Fractures : % p = 0,011 IC 95 : ,5 % Months Months ASBMR D après Cummings S.R. et al., San Francisco, États-Unis, abstract 1286,
60 Osteoporosis Treatment in 2009 Summary HRT: spine fx; hip fx SERMS: spine fx; no effect on peripheral fx Calcitonin: possible spine fx; no hip data Alendronate: spine fx; hip fx Risedronate: spine fx; hip fx Ibandronate: spine fx; no effect on hip Zoledronate: spine fx; hip fx PTH: spine fx Strontium Ranelate: spine fx; hip fx Denosumab: spine fx; hip fx
61 Adapted from E. Seeman (2004) Factors Influencing Treatment Decision Advancing age Lower BMD Presence of Fracture Risk factors or disease causing continued bone loss Leanness Family history BMD T score SD SD HRT Lower BMD Treatment No Yes, if fx Yes Increasing need to treat RALOXIFENE Older Normal Osteopenia Osteoporosis 80 BISPHOSPHONATES STRONTIUM RANELATE PTH CALCIUM Vit D (if deficient)
62 1. Aim of Therapy Treatment of Osteoporosis = Treatment of Patients with Osteoporosis 2. Never Too Late
63
64 Fractures are not Unavoidable Expenses to Pay as a Consequence of Increased Life-Expectancy Because of Better Identification of Risk Factors for Osteoporosis Early Diagnosis, before the First Fracture A Larger Use of Preventive and Therapeutical Strategies, whose Efficacy has been Demonstrated in Randomized Controled Trials, with Fracture Incidence as Primary End- Point
65 Kaplan-Meier (K-M) fracture rate (%) Effect of Bazedoxifene on Vertebral Fracture in Postmenopausal Women with Osteoporosis Incidence of new vertebral fracture (intent-to-treat population 0-36 months) Bazedoxifene 20 mg Bazedoxifene 40 mg Raloxifene 60 mg Placebo * p < 0.05 for any active group versus placebo Months Results * the reduction in the incidence of new vertebral fractures was (as compared to placebo) - 42% in group I - 37% in group II - 42% in group III there was no treatment effect on NVF there was no difference between the different groups with regard to adverse effects Bazedoxifene significantly reduces the risk of new vertebral fracture in postmenopausal women with osteoporosis ASBMR 2007 From Silverman SL et al., Beverly Hills, USA, abstract 1206, updated
66 Long-Term Vertebral and Non-vertebral FractureRisk Reduction with Strontium Ranelate Favors Strontium ranelate RR Over 5 years - 24% Vertebral fractures P< % - 18% Non vertebral fractures Major non vertebral fractures P=0.032 P= % Vertebral fractures, 80 years - 26% Non-vertebral fractures, 80 years P=0.010 P= Reginster et al 2007 RELATIVE RISKS AND 95% CI
67 Pathogenesis of Osteoporotic Fracture LOW PEAK BONE MASS POSTMENOPAUSAL BONE LOSS AGE-RELATED BONE LOSS LOW BONE MASS Other risk factors Nonskeletal factors (propensity to fall) FRACTURE Poor bone quality (architecture)
68 Hip Fracture Risk Vitamin D & Calcium Versus Placebo/No Treatment Source Favors Treatment Favors Placebo Weight (%) Relative Risk (95% CI) Chapuy et al ( ) 38.9% Dawson-Hughes et al Chapuy et al Porthouse et al RECORD Trial Group 2005 WHI Trial Group, % 6.5% 2.8% 10.9% 40.7% 0.36 ( ) 0.62 ( ) 0.71 ( ) 1.14 ( ) 0.88 ( ) Pooled Estimate 100.0% 0.82 ( ) Relative Risk (95% CI) of Hip Fracture P= Boonen, Lips et al., unpublished observations
69 Bone Mineral Mass Tracking of Bone Mineral Mass Accrual Age (years)
Skeletal Manifestations
 Skeletal Manifestations of Metabolic Bone Disease Mishaela R. Rubin, MD February 21, 2008 The Three Ages of Women Gustav Klimt 1905 1 Lecture Outline Osteoporosis epidemiology diagnosis secondary causes
Skeletal Manifestations of Metabolic Bone Disease Mishaela R. Rubin, MD February 21, 2008 The Three Ages of Women Gustav Klimt 1905 1 Lecture Outline Osteoporosis epidemiology diagnosis secondary causes
Osteoporosis. Current Trend in Osteoporosis Management for Elderly in HK- Medical Perspective. Old Definition of Osteoporosis
 Current Trend in Osteoporosis Management for Elderly in HK- Medical Perspective Dr Dicky T.K. Choy Physician Jockey Club Centre for Osteoporosis Care and Control, CUHK Osteoporosis Global public health
Current Trend in Osteoporosis Management for Elderly in HK- Medical Perspective Dr Dicky T.K. Choy Physician Jockey Club Centre for Osteoporosis Care and Control, CUHK Osteoporosis Global public health
Updates in Osteoporosis. I have no conflicts of interest. What Would You Do? Mrs. C. What s New in Osteoporosis. Page 1
 Updates in Osteoporosis Jeffrey A. Tice, MD Associate Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in
Updates in Osteoporosis Jeffrey A. Tice, MD Associate Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in
Osteoporosis Update. Greg Summers Consultant Rheumatologist
 Osteoporosis Update Greg Summers Consultant Rheumatologist DEFINITION OSTEOPOROSIS is LOW BONE MASS (& micro-architectural deterioration) causing AN INCREASED RISK OF FRACTURE 23 years 82 years 23 y/o
Osteoporosis Update Greg Summers Consultant Rheumatologist DEFINITION OSTEOPOROSIS is LOW BONE MASS (& micro-architectural deterioration) causing AN INCREASED RISK OF FRACTURE 23 years 82 years 23 y/o
Osteoporosis. Overview
 v2 Osteoporosis Overview Osteoporosis is defined as compromised bone strength that increases risk of fracture (NIH Consensus Conference, 2000). Bone strength is characterized by bone mineral density (BMD)
v2 Osteoporosis Overview Osteoporosis is defined as compromised bone strength that increases risk of fracture (NIH Consensus Conference, 2000). Bone strength is characterized by bone mineral density (BMD)
Assessment and Treatment of Osteoporosis Professor T.Masud
 Assessment and Treatment of Osteoporosis Professor T.Masud Nottingham University Hospitals NHS Trust University of Nottingham University of Derby University of Southern Denmark What is Osteoporosis? Osteoporosis
Assessment and Treatment of Osteoporosis Professor T.Masud Nottingham University Hospitals NHS Trust University of Nottingham University of Derby University of Southern Denmark What is Osteoporosis? Osteoporosis
CASE 1 WHY IS IT IMPORTANT TO TREAT? FACTS CONCERNS
 4:30-5:15pm Ask the Expert: Osteoporosis SPEAKERS Silvina Levis, MD OSTEOPOROSIS - FACTS 1:3 older women and 1:5 older men will have a fragility fracture after age 50 After 3 years of treatment, depending
4:30-5:15pm Ask the Expert: Osteoporosis SPEAKERS Silvina Levis, MD OSTEOPOROSIS - FACTS 1:3 older women and 1:5 older men will have a fragility fracture after age 50 After 3 years of treatment, depending
This house believes that HRT should be the first-line prevention for postmenopausal osteoporosis: the case against
 This house believes that HRT should be the first-line prevention for postmenopausal osteoporosis: the case against Juliet Compston Professor of Bone Medicine University of Cambridge School of Clinical
This house believes that HRT should be the first-line prevention for postmenopausal osteoporosis: the case against Juliet Compston Professor of Bone Medicine University of Cambridge School of Clinical
OSTEOPOROSIS: PREVENTION AND MANAGEMENT
 OSTEOPOROSIS: OVERVIEW OSTEOPOROSIS: PREVENTION AND MANAGEMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Key Risk factors Screening and Monitoring
OSTEOPOROSIS: OVERVIEW OSTEOPOROSIS: PREVENTION AND MANAGEMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Key Risk factors Screening and Monitoring
An Update on Osteoporosis Treatments
 An Update on Osteoporosis Treatments Dr Mike Stone University Hospital Llandough Treatments for osteoporosis Calcium and vitamin D HRT Raloxifene Etidronate Alendronate Risedronate Ibandronate (oral and
An Update on Osteoporosis Treatments Dr Mike Stone University Hospital Llandough Treatments for osteoporosis Calcium and vitamin D HRT Raloxifene Etidronate Alendronate Risedronate Ibandronate (oral and
Management of postmenopausal osteoporosis
 Management of postmenopausal osteoporosis Yeap SS, Hew FL, Chan SP, on behalf of the Malaysian Osteoporosis Society Committee Working Group for the Clinical Guidance on the Management of Osteoporosis,
Management of postmenopausal osteoporosis Yeap SS, Hew FL, Chan SP, on behalf of the Malaysian Osteoporosis Society Committee Working Group for the Clinical Guidance on the Management of Osteoporosis,
Overview. Bone Biology Osteoporosis Osteomalacia Paget s Disease Cases. People Centred Positive Compassion Excellence
 Overview Osteoporosis and Metabolic Bone Disease Dr Chandini Rao Consultant Rheumatologist Bone Biology Osteoporosis Osteomalacia Paget s Disease Cases Bone Biology Osteoporosis Increased bone remodelling
Overview Osteoporosis and Metabolic Bone Disease Dr Chandini Rao Consultant Rheumatologist Bone Biology Osteoporosis Osteomalacia Paget s Disease Cases Bone Biology Osteoporosis Increased bone remodelling
Updates in Osteoporosis
 Updates in Osteoporosis Jeffrey A. Tice, MD Associate Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in
Updates in Osteoporosis Jeffrey A. Tice, MD Associate Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in
Prevention of Osteoporotic Hip Fracture
 Prevention of Osteoporotic Hip Fracture Dr Law Sheung Wai 8th July 2007 Associate Consultant Spine team / Orthopedic Rehabilitation Department of Orthopedics and Traumatology NTE Cluster 1 Objectives Problems
Prevention of Osteoporotic Hip Fracture Dr Law Sheung Wai 8th July 2007 Associate Consultant Spine team / Orthopedic Rehabilitation Department of Orthopedics and Traumatology NTE Cluster 1 Objectives Problems
Differentiating Pharmacological Therapies for Osteoporosis
 Differentiating Pharmacological Therapies for Osteoporosis Socrates E Papapoulos Department of Endocrinology & Metabolic Diseases Leiden University Medical Center The Netherlands Competing interests: consulting/speaking
Differentiating Pharmacological Therapies for Osteoporosis Socrates E Papapoulos Department of Endocrinology & Metabolic Diseases Leiden University Medical Center The Netherlands Competing interests: consulting/speaking
Advanced medicine conference. Monday 20 Tuesday 21 June 2016
 Advanced medicine conference Monday 20 Tuesday 21 June 2016 Osteoporosis: recent advances in risk assessment and management Juliet Compston Emeritus Professor of Bone Medicine Cambridge Biomedical Campus
Advanced medicine conference Monday 20 Tuesday 21 June 2016 Osteoporosis: recent advances in risk assessment and management Juliet Compston Emeritus Professor of Bone Medicine Cambridge Biomedical Campus
Page 1. New Developments in Osteoporosis. What s New in Osteoporosis
 New Developments in Osteoporosis Eliseo J. Pérez-Stable MD Professor of Medicine Division of General Internal Medicine Department of Medicine July 4, 2013 Declaration of full disclosure: No conflict of
New Developments in Osteoporosis Eliseo J. Pérez-Stable MD Professor of Medicine Division of General Internal Medicine Department of Medicine July 4, 2013 Declaration of full disclosure: No conflict of
Disclosures Fractures:
 Disclosures Fractures: A. Schwartz Epidemiology and Risk Factors Research Funding: GlaxoSmithKline, Merck Ann V. Schwartz, PhD Department of Epidemiology and Biostatistics UCSF Outline Fracture incidence
Disclosures Fractures: A. Schwartz Epidemiology and Risk Factors Research Funding: GlaxoSmithKline, Merck Ann V. Schwartz, PhD Department of Epidemiology and Biostatistics UCSF Outline Fracture incidence
Clinician s Guide to Prevention and Treatment of Osteoporosis
 Clinician s Guide to Prevention and Treatment of Osteoporosis Published: 15 August 2014 committee of the National Osteoporosis Foundation (NOF) Tipawan khiemsontia,md outline Basic pathophysiology screening
Clinician s Guide to Prevention and Treatment of Osteoporosis Published: 15 August 2014 committee of the National Osteoporosis Foundation (NOF) Tipawan khiemsontia,md outline Basic pathophysiology screening
Osteoporosis: Are your bones at risk of fracturing? Rachel Wallwork, MD Internal medicine resident Massachusetts General Hospital
 Osteoporosis: Are your bones at risk of fracturing? Rachel Wallwork, MD Internal medicine resident Massachusetts General Hospital What is Osteoporosis? Osteoporosis causes bones to lose density, become
Osteoporosis: Are your bones at risk of fracturing? Rachel Wallwork, MD Internal medicine resident Massachusetts General Hospital What is Osteoporosis? Osteoporosis causes bones to lose density, become
Horizon Scanning Centre March Denosumab for glucocorticoidinduced SUMMARY NIHR HSC ID: 6329
 Horizon Scanning Centre March 2014 Denosumab for glucocorticoidinduced osteoporosis SUMMARY NIHR HSC ID: 6329 This briefing is based on information available at the time of research and a limited literature
Horizon Scanning Centre March 2014 Denosumab for glucocorticoidinduced osteoporosis SUMMARY NIHR HSC ID: 6329 This briefing is based on information available at the time of research and a limited literature
Download slides:
 Download slides: https://www.tinyurl.com/m67zcnn https://tinyurl.com/kazchbn OSTEOPOROSIS REVIEW AND UPDATE Boca Raton Regional Hospital Internal Medicine Conference 2017 Benjamin Wang, M.D., FRCPC Division
Download slides: https://www.tinyurl.com/m67zcnn https://tinyurl.com/kazchbn OSTEOPOROSIS REVIEW AND UPDATE Boca Raton Regional Hospital Internal Medicine Conference 2017 Benjamin Wang, M.D., FRCPC Division
Osteoporosis: An Overview. Carolyn J. Crandall, MD, MS
 Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Professor of Medicine David Geffen School of Medicine at UCLA Objectives Review osteoporosis
Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Professor of Medicine David Geffen School of Medicine at UCLA Objectives Review osteoporosis
Fractures: Epidemiology and Risk Factors. Osteoporosis in Men (more this afternoon) 1/5 men over age 50 will suffer osteoporotic fracture 7/16/2009
 1/5 men over age 50 will suffer osteoporotic fracture 7/16/2009") Fractures: Epidemiology and Risk Factors Mary L. Bouxsein, PhD Department of Orthopaedic Surgery Beth Israel Deaconess Medical Center Harvard Medical School, Boston, MA Outline Fracture incidence and impact
Fractures: Epidemiology and Risk Factors Mary L. Bouxsein, PhD Department of Orthopaedic Surgery Beth Israel Deaconess Medical Center Harvard Medical School, Boston, MA Outline Fracture incidence and impact
Osteoporosis/Fracture Prevention
 Osteoporosis/Fracture Prevention NATIONAL GUIDELINE SUMMARY This guideline was developed using an evidence-based methodology by the KP National Osteoporosis/Fracture Prevention Guideline Development Team
Osteoporosis/Fracture Prevention NATIONAL GUIDELINE SUMMARY This guideline was developed using an evidence-based methodology by the KP National Osteoporosis/Fracture Prevention Guideline Development Team
1
 www.osteoporosis.ca 1 2 Overview of the Presentation Osteoporosis: An Overview Bone Basics Diagnosis of Osteoporosis Drug Therapies Risk Reduction Living with Osteoporosis 3 What is Osteoporosis? Osteoporosis:
www.osteoporosis.ca 1 2 Overview of the Presentation Osteoporosis: An Overview Bone Basics Diagnosis of Osteoporosis Drug Therapies Risk Reduction Living with Osteoporosis 3 What is Osteoporosis? Osteoporosis:
Page 1. Updates in Osteoporosis. I have no conflicts of interest. What is osteoporosis? What s New in Osteoporosis
 Updates in Osteoporosis Jeffrey A. Tice, MD Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in Osteoporosis
Updates in Osteoporosis Jeffrey A. Tice, MD Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in Osteoporosis
OSTEOPOROSIS IN INDONESIA
 OSTEOPOROSIS IN INDONESIA Hana Ratnawati Faculty of Medicine Maranatha Christian University Bandung - Indonesia 5th SBA Conference 2013 1 5th SBA Conference 2013 2 INTRODUCTION Indonesia is an archipelago
OSTEOPOROSIS IN INDONESIA Hana Ratnawati Faculty of Medicine Maranatha Christian University Bandung - Indonesia 5th SBA Conference 2013 1 5th SBA Conference 2013 2 INTRODUCTION Indonesia is an archipelago
Osteoporosis. Open Access. John A. Kanis. Diseases, University of Sheffield, UK
 Journal of Medical Sciences (2010); 3(3): 00-00 Review Article Osteoporosis Open Access John A. Kanis WHO Collaborating Centre for Metabolic Bone Diseases, University of Sheffield, UK incorporated into
Journal of Medical Sciences (2010); 3(3): 00-00 Review Article Osteoporosis Open Access John A. Kanis WHO Collaborating Centre for Metabolic Bone Diseases, University of Sheffield, UK incorporated into
Interpreting DEXA Scan and. the New Fracture Risk. Assessment. Algorithm
 Interpreting DEXA Scan and the New Fracture Risk Assessment Algorithm Prof. Samir Elbadawy *Osteoporosis affect 30%-40% of women in western countries and almost 15% of men after the age of 50 years. Osteoporosis
Interpreting DEXA Scan and the New Fracture Risk Assessment Algorithm Prof. Samir Elbadawy *Osteoporosis affect 30%-40% of women in western countries and almost 15% of men after the age of 50 years. Osteoporosis
Module 5 - Speaking of Bones Osteoporosis For Health Professionals: Fracture Risk Assessment. William D. Leslie, MD MSc FRCPC
 Module 5 - Speaking of Bones Osteoporosis For Health Professionals: Fracture Risk Assessment William D. Leslie, MD MSc FRCPC Case #1 Age 53: 3 years post-menopause Has always enjoyed excellent health with
Module 5 - Speaking of Bones Osteoporosis For Health Professionals: Fracture Risk Assessment William D. Leslie, MD MSc FRCPC Case #1 Age 53: 3 years post-menopause Has always enjoyed excellent health with
Page 1. Current and Emerging Strategies What s New in Osteoporosis. Osteoporosis. What is Osteoporosis? Traditional Risk Factors for Fracture
 Current and Emerging Strategies for Osteoporosis What s New in Osteoporosis Risk stratification Douglas C. Bauer, MD University of California, San Francisco Under recognition and poor compliance New potential
Current and Emerging Strategies for Osteoporosis What s New in Osteoporosis Risk stratification Douglas C. Bauer, MD University of California, San Francisco Under recognition and poor compliance New potential
Presenter: 翁家嫻 Venue date:
 FOR THE TREATMENT OF OSTEOPOROSIS IN POSTMENOPAUSAL WOMEN AT INCREASED RISK OF FRACTURES 1 Presenter: 翁家嫻 Venue date: 2018.03.13 PMO: postmenopausal osteoporosis. 1. Prolia (denosumab), Summary of Product
FOR THE TREATMENT OF OSTEOPOROSIS IN POSTMENOPAUSAL WOMEN AT INCREASED RISK OF FRACTURES 1 Presenter: 翁家嫻 Venue date: 2018.03.13 PMO: postmenopausal osteoporosis. 1. Prolia (denosumab), Summary of Product
Using the FRAX Tool. Osteoporosis Definition
 How long will your bones remain standing? Using the FRAX Tool Gary Salzman M.D. Director Banner Good Samaritan/ Hayden VAMC Internal Medicine Geriatric Fellowship Program Phoenix, Arizona Using the FRAX
How long will your bones remain standing? Using the FRAX Tool Gary Salzman M.D. Director Banner Good Samaritan/ Hayden VAMC Internal Medicine Geriatric Fellowship Program Phoenix, Arizona Using the FRAX
Current and Emerging Strategies for Osteoporosis
 Current and Emerging Strategies for Osteoporosis I have nothing to disclose. Anne Schafer, MD Assistant Professor of Medicine Division of Endocrinology & Metabolism December 12, 2014 Outline Osteoporosis
Current and Emerging Strategies for Osteoporosis I have nothing to disclose. Anne Schafer, MD Assistant Professor of Medicine Division of Endocrinology & Metabolism December 12, 2014 Outline Osteoporosis
Chau Nguyen, D.O. Rheumatologist Clinical Assistant Professor of Internal Medicine at Western University of Health Sciences
 Chau Nguyen, D.O Rheumatologist Clinical Assistant Professor of Internal Medicine at Western University of Health Sciences I do not have any relationship with the manufacturer of any commercial products
Chau Nguyen, D.O Rheumatologist Clinical Assistant Professor of Internal Medicine at Western University of Health Sciences I do not have any relationship with the manufacturer of any commercial products
Learning Objectives. Controversies in Osteoporosis Prevention and Management. Etiology. Presenter Disclosure Information. Epidemiology.
 12:45 1:30pm Controversies in Osteoporosis Prevention and Management SPEAKER Carolyn Crandall, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Carolyn
12:45 1:30pm Controversies in Osteoporosis Prevention and Management SPEAKER Carolyn Crandall, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Carolyn
Osteoporosis: A Tale of 3 Task Forces!
 Osteoporosis: A Tale of 3 Task Forces! Robert A. Adler, MD McGuire Veterans Affairs Medical Center Virginia Commonwealth University Richmond, Virginia, USA Disclosures The opinions are those of the speaker
Osteoporosis: A Tale of 3 Task Forces! Robert A. Adler, MD McGuire Veterans Affairs Medical Center Virginia Commonwealth University Richmond, Virginia, USA Disclosures The opinions are those of the speaker
Page 1. Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018? What s New in Osteoporosis
 Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018? Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco What s
Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018? Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco What s
Osteoporosis - New Guidelines. Michelle Glass B.Sc. (Pharm) June 15, 2011
 June 15, 2011") Osteoporosis - New Guidelines Michelle Glass B.Sc. (Pharm) June 15, 2011 Outline What is Osteoporosis? Who is at risk? What treatments are available? Role of the Pharmacy technician Definition of Osteoporosis
Osteoporosis - New Guidelines Michelle Glass B.Sc. (Pharm) June 15, 2011 Outline What is Osteoporosis? Who is at risk? What treatments are available? Role of the Pharmacy technician Definition of Osteoporosis
nogg Guideline for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK
 nogg NATIONAL OSTEOPOROSIS GUIDELINE GROUP Guideline for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK Produced by J Compston, A Cooper,
nogg NATIONAL OSTEOPOROSIS GUIDELINE GROUP Guideline for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK Produced by J Compston, A Cooper,
NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT
 NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF OSTEOPOROSIS: OVERVIEW Definitions Risk factors
NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF OSTEOPOROSIS: OVERVIEW Definitions Risk factors
Disclosures Fractures: A. Schwartz Epidemiology and Risk Factors Consulting: Merck
 Disclosures Fractures: A. Schwartz Epidemiology and Risk Factors Consulting: Merck Ann V. Schwartz, PhD Department of Epidemiology and Biostatistics UCSF Outline Fracture incidence and impact of fractures
Disclosures Fractures: A. Schwartz Epidemiology and Risk Factors Consulting: Merck Ann V. Schwartz, PhD Department of Epidemiology and Biostatistics UCSF Outline Fracture incidence and impact of fractures
Diagnosis and Treatment of Osteoporosis: What s New and Controversial in ? What s New in Osteoporosis
 Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018-19? What s New in Osteoporosis The crisis in treatment and compliance Douglas C. Bauer, MD Professor of Medicine and Epidemiology
Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018-19? What s New in Osteoporosis The crisis in treatment and compliance Douglas C. Bauer, MD Professor of Medicine and Epidemiology
Osteoporosis: How to Manage Long- Term Use of Bisphosphonates AKA Now What? David E Feinstein, DO, CCD November 15 th, 2017
 Osteoporosis: How to Manage Long- Term Use of Bisphosphonates AKA Now What? David E Feinstein, DO, CCD November 15 th, 2017 Introduction A fracture due to OP occurs every 3 seconds around the world. 1
Osteoporosis: How to Manage Long- Term Use of Bisphosphonates AKA Now What? David E Feinstein, DO, CCD November 15 th, 2017 Introduction A fracture due to OP occurs every 3 seconds around the world. 1
Page 1. Current and Emerging Strategies for Osteoporosis. Osteoporosis Warm-Up: Which of the Following is True?
 Current and Emerging Strategies for Osteoporosis Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco No Disclosures Osteoporosis Warm-Up:
Current and Emerging Strategies for Osteoporosis Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco No Disclosures Osteoporosis Warm-Up:
The Bare Bones of Osteoporosis. Wendy Rosenthal, PharmD
 The Bare Bones of Osteoporosis Wendy Rosenthal, PharmD Definition A systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone tissue, with a consequent increase
The Bare Bones of Osteoporosis Wendy Rosenthal, PharmD Definition A systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone tissue, with a consequent increase
New Developments in Osteoporosis: Screening, Prevention and Treatment
 Osteoporosis: Overview New Developments in Osteoporosis: Screening, Prevention and Treatment Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Risk factors
Osteoporosis: Overview New Developments in Osteoporosis: Screening, Prevention and Treatment Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Risk factors
Page 1
 Osteoporosis Osteoporosis is a condition characterised by weakened bones that fracture easily. After menopause many women are at risk of developing osteoporosis. Peak bone mass is usually reached during
Osteoporosis Osteoporosis is a condition characterised by weakened bones that fracture easily. After menopause many women are at risk of developing osteoporosis. Peak bone mass is usually reached during
HRT and Risedronate Combined Anabolic and Antiresorptive Therapy
 Optimizing Combined and Sequential Osteoanabolic and Antiresorptive Therapy Benjamin Leder, M.D. Endocrine Unit Massachusetts General Hospital Boston, MA Antiresorptive and Osteoanabolic Therapies Increase
Optimizing Combined and Sequential Osteoanabolic and Antiresorptive Therapy Benjamin Leder, M.D. Endocrine Unit Massachusetts General Hospital Boston, MA Antiresorptive and Osteoanabolic Therapies Increase
An audit of osteoporotic patients in an Australian general practice
 professional Darren Parker An audit of osteoporotic patients in an Australian general practice Background Osteoporosis is a major contributor to morbidity and mortality in Australia, and is predicted to
professional Darren Parker An audit of osteoporotic patients in an Australian general practice Background Osteoporosis is a major contributor to morbidity and mortality in Australia, and is predicted to
Drug Intervals (Holidays) with Oral Bisphosphonates
 with Oral Bisphosphonates") Drug Intervals (Holidays) with Oral Bisphosphonates Rizwan Rajak Consultant Rheumatologist & Lead for Osteoporosis GP Postgraduate Meeting April 2018 Contents Case presentation Pathway for Bisphosphonate
Drug Intervals (Holidays) with Oral Bisphosphonates Rizwan Rajak Consultant Rheumatologist & Lead for Osteoporosis GP Postgraduate Meeting April 2018 Contents Case presentation Pathway for Bisphosphonate
Treatment of Osteoporosis: IHFD 6 th March 2015
 Treatment of Osteoporosis: IHFD 6 th March 2015 Dr. John J. Carey, MB, MS, FACR, FRCPI, CCD. Consultant Physician Galway University Hospitals Associate Professor in Medicine, NUIG, Galway Vice-President
Treatment of Osteoporosis: IHFD 6 th March 2015 Dr. John J. Carey, MB, MS, FACR, FRCPI, CCD. Consultant Physician Galway University Hospitals Associate Professor in Medicine, NUIG, Galway Vice-President
Fragile Bones and how to recognise them. Rod Hughes Consultant physician and rheumatologist St Peter s hospital Chertsey
 Fragile Bones and how to recognise them Rod Hughes Consultant physician and rheumatologist St Peter s hospital Chertsey Osteoporosis Osteoporosis is a skeletal disorder characterised by compromised bone
Fragile Bones and how to recognise them Rod Hughes Consultant physician and rheumatologist St Peter s hospital Chertsey Osteoporosis Osteoporosis is a skeletal disorder characterised by compromised bone
Fractures: Epidemiology and Risk Factors. July 2012 CME (35 minutes) 7/24/ July12 1. Osteoporotic fractures: Comparison with other diseases
 7/24/ July12 1. Osteoporotic fractures: Comparison with other diseases") Financial Disclosures Fractures: Epidemiology and Risk Factors Research grants, speaking or consulting: Amgen, Lilly, Merck, Novartis, Radius Dennis M. Black, PhD Department of Epidemiology and Biostatistics
Financial Disclosures Fractures: Epidemiology and Risk Factors Research grants, speaking or consulting: Amgen, Lilly, Merck, Novartis, Radius Dennis M. Black, PhD Department of Epidemiology and Biostatistics
John J. Wolf, DO Family Medicine
 John J. Wolf, DO Family Medicine Objectives: 1. Review incidence & Risk of Osteoporosis 2.Review indications for testing 3.Review current pharmacologic & Non pharmacologic Tx options 4.Understand & Utilize
John J. Wolf, DO Family Medicine Objectives: 1. Review incidence & Risk of Osteoporosis 2.Review indications for testing 3.Review current pharmacologic & Non pharmacologic Tx options 4.Understand & Utilize
Guideline for the investigation and management of osteoporosis. for hospitals and General Practice
 Guideline for the investigation and management of osteoporosis for hospitals and General Practice Background Low bone density is an important risk factor for fracture. The aim of assessing bone density
Guideline for the investigation and management of osteoporosis for hospitals and General Practice Background Low bone density is an important risk factor for fracture. The aim of assessing bone density
Current and Emerging Approaches for Osteoporosis
 Current and Emerging Approaches for Osteoporosis Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco No Disclosures What s New in Osteoporosis
Current and Emerging Approaches for Osteoporosis Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco No Disclosures What s New in Osteoporosis
Osteoporosis Screening and Treatment in Type 2 Diabetes
 Osteoporosis Screening and Treatment in Type 2 Diabetes Ann Schwartz, PhD! Dept. of Epidemiology and Biostatistics! University of California San Francisco! October 2011! Presenter Disclosure Information
Osteoporosis Screening and Treatment in Type 2 Diabetes Ann Schwartz, PhD! Dept. of Epidemiology and Biostatistics! University of California San Francisco! October 2011! Presenter Disclosure Information
Disclosures. Diagnostic Challenges in Osteoporosis: Whom To Treat 9/25/2014
 Disclosures Diagnostic Challenges in Osteoporosis: Whom To Treat Ethel S. Siris, MD Columbia University Medical Center New York, NY Consultant on scientific issues for: AgNovos Amgen Eli Lilly Merck Novartis
Disclosures Diagnostic Challenges in Osteoporosis: Whom To Treat Ethel S. Siris, MD Columbia University Medical Center New York, NY Consultant on scientific issues for: AgNovos Amgen Eli Lilly Merck Novartis
July 2012 CME (35 minutes) 7/12/2016
 7/12/2016") Financial Disclosures Epidemiology and Consequences of Fractures Advisory Board: Amgen Janssen Pharmaceuticals Inc. Ann V. Schwartz, PhD Department of Epidemiology and Biostatistics UCSF Outline Osteoporotic
Financial Disclosures Epidemiology and Consequences of Fractures Advisory Board: Amgen Janssen Pharmaceuticals Inc. Ann V. Schwartz, PhD Department of Epidemiology and Biostatistics UCSF Outline Osteoporotic
New York State County Comparison of Fall-related Hip Fractures of Older Adults and Number of Dual-X-ray Absorptiometry Machines
 New York State County Comparison of Fall-related Hip Fractures of Older Adults and Number of Dual-X-ray Absorptiometry Machines Michael Bauer New York State Department of Health Bureau of Occupational
New York State County Comparison of Fall-related Hip Fractures of Older Adults and Number of Dual-X-ray Absorptiometry Machines Michael Bauer New York State Department of Health Bureau of Occupational
Healthy Bones: Osteoporosis Management. Laurel Short, MSN, FNP-C
 Healthy Bones: Osteoporosis Management Laurel Short, MSN, FNP-C Disclosure I have no current affiliation or financial interest with any grantor or commercial interests that may have direct interest in
Healthy Bones: Osteoporosis Management Laurel Short, MSN, FNP-C Disclosure I have no current affiliation or financial interest with any grantor or commercial interests that may have direct interest in
SpongeBone Menopants*
 SpongeBone Menopants* Adam Fershko, MD, FACP Kettering Health Network *Postmenopausal Osteoporosis Objectives O Epidemiology O Clinical significance O Pathophysiology O Screening and Diagnosis O Treatment
SpongeBone Menopants* Adam Fershko, MD, FACP Kettering Health Network *Postmenopausal Osteoporosis Objectives O Epidemiology O Clinical significance O Pathophysiology O Screening and Diagnosis O Treatment
Osteoporosis challenges
 Osteoporosis challenges Osteoporosis challenges Who should have a fracture risk assessment? Who to treat? Drugs, holidays and unusual adverse effects Fracture liaison service? The size of the problem 1
Osteoporosis challenges Osteoporosis challenges Who should have a fracture risk assessment? Who to treat? Drugs, holidays and unusual adverse effects Fracture liaison service? The size of the problem 1
Osteoporosis update. Dr. Claire Vandevelde Consultant Rheumatologist, LTHT
 Osteoporosis update Dr. Claire Vandevelde Consultant Rheumatologist, LTHT Outline Background BMD Tools for assessing fracture risk Case study Denosumab Treatment breaks BMD BMD predicts fracture risk but
Osteoporosis update Dr. Claire Vandevelde Consultant Rheumatologist, LTHT Outline Background BMD Tools for assessing fracture risk Case study Denosumab Treatment breaks BMD BMD predicts fracture risk but
Clinical Specialist Statement Template
 Clinical Specialist Statement Template Thank you for agreeing to give us a statement on your organisation s view of the technology and the way it should be used in the NHS. Healthcare professionals can
Clinical Specialist Statement Template Thank you for agreeing to give us a statement on your organisation s view of the technology and the way it should be used in the NHS. Healthcare professionals can
Summary. Background. Diagnosis
 March 2009 Management of post-menopausal osteoporosis This bulletin focuses on the pharmacological management of patients with post-menopausal osteoporosis both those with clinically evident disease (e.g.
March 2009 Management of post-menopausal osteoporosis This bulletin focuses on the pharmacological management of patients with post-menopausal osteoporosis both those with clinically evident disease (e.g.
Effective Health Care
 Number 12 Effective Health Care Comparative Effectiveness of Treatments To Prevent Fractures in Men and Women With Low Bone Density or Osteoporosis Executive Summary Background Osteoporosis is a systemic
Number 12 Effective Health Care Comparative Effectiveness of Treatments To Prevent Fractures in Men and Women With Low Bone Density or Osteoporosis Executive Summary Background Osteoporosis is a systemic
BAD TO THE BONE. Peter Jones, Rheumatologist QE Health, Rotorua. GP CME Conference Rotorua, June 2008
 BAD TO THE BONE Peter Jones, Rheumatologist QE Health, Rotorua GP CME Conference Rotorua, June 2008 Agenda Osteoporosis in Men Vitamin D and Calcium Long-term treatment with Bisphosphonates Pathophysiology
BAD TO THE BONE Peter Jones, Rheumatologist QE Health, Rotorua GP CME Conference Rotorua, June 2008 Agenda Osteoporosis in Men Vitamin D and Calcium Long-term treatment with Bisphosphonates Pathophysiology
Clinical Practice. Presented by: Internist, Endocrinologist
 Clinical Practice Management of Osteoporosis Presented by: SaeedBehradmanesh, h MD Internist, Endocrinologist Iran, Isfahan, Feb. 2017 Definition: A disease characterized by low bone mass and microarchitectural
Clinical Practice Management of Osteoporosis Presented by: SaeedBehradmanesh, h MD Internist, Endocrinologist Iran, Isfahan, Feb. 2017 Definition: A disease characterized by low bone mass and microarchitectural
Current Issues in Osteoporosis
 Current Issues in Osteoporosis California AACE 18TH Annual Meeting & Symposium Marina del Rey, CA September 15, 2018 Michael R. McClung, MD, FACP,FACE Director, Oregon Osteoporosis Center Portland, Oregon,
Current Issues in Osteoporosis California AACE 18TH Annual Meeting & Symposium Marina del Rey, CA September 15, 2018 Michael R. McClung, MD, FACP,FACE Director, Oregon Osteoporosis Center Portland, Oregon,
AACE/ACE Osteoporosis Treatment Decision Tool
 AACE/ACE Osteoporosis Treatment Decision Tool What is Osteoporosis? OSTEOPOROSIS is defined as reduced bone strength leading to an increased risk of fracture. Osteoporosis, or porous bones, occurs when
AACE/ACE Osteoporosis Treatment Decision Tool What is Osteoporosis? OSTEOPOROSIS is defined as reduced bone strength leading to an increased risk of fracture. Osteoporosis, or porous bones, occurs when
Page 1. Osteoporosis Warm-Up: Which of the Following is True? Diagnosis and Treatment of Osteoporosis: What is New in What s New in Osteoporosis
 Diagnosis and Treatment of Osteoporosis: What is New in 2017 Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco No Disclosures Osteoporosis
Diagnosis and Treatment of Osteoporosis: What is New in 2017 Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco No Disclosures Osteoporosis
A rational approach to the treatment of osteoporosis
 A rational approach to the treatment of osteoporosis Hough S, MBChB, HonsBSc, MMed, MD (Stell), FCP(SA) Professor of Medicine & Endocrinology Faculty of Health Sciences University of Stellenbosch Correspondence
A rational approach to the treatment of osteoporosis Hough S, MBChB, HonsBSc, MMed, MD (Stell), FCP(SA) Professor of Medicine & Endocrinology Faculty of Health Sciences University of Stellenbosch Correspondence
Pharmacy Management Drug Policy
 SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 9/29/2017 If the member s subscriber contract excludes coverage
SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 9/29/2017 If the member s subscriber contract excludes coverage
Submission to the National Institute for Clinical Excellence on
 Submission to the National Institute for Clinical Excellence on Strontium ranelate for the prevention of osteoporotic fractures in postmenopausal women with osteoporosis by The Society for Endocrinology
Submission to the National Institute for Clinical Excellence on Strontium ranelate for the prevention of osteoporotic fractures in postmenopausal women with osteoporosis by The Society for Endocrinology
Postmenopausal osteoporosis is a systemic
 OSTEOPOROSIS: HARD FACTS ABOUT BONES Steven T. Harris, MD, FACP* ABSTRACT As a consequence of the aging process, osteoporosis affects all men and women. Agerelated loss of bone mass leads to skeletal fragility
OSTEOPOROSIS: HARD FACTS ABOUT BONES Steven T. Harris, MD, FACP* ABSTRACT As a consequence of the aging process, osteoporosis affects all men and women. Agerelated loss of bone mass leads to skeletal fragility
COPD-Related Musculoskeletal Disease. Jessica Bon Field, MD, MS 2017 Update in Internal Medicine October 20, 2017
 COPD-Related Musculoskeletal Disease Jessica Bon Field, MD, MS 2017 Update in Internal Medicine October 20, 2017 A 60-year old man with COPD comes into your office for a routine office visit. He is a former
COPD-Related Musculoskeletal Disease Jessica Bon Field, MD, MS 2017 Update in Internal Medicine October 20, 2017 A 60-year old man with COPD comes into your office for a routine office visit. He is a former
BREAST CANCER AND BONE HEALTH
 BREAST CANCER AND BONE HEALTH Rowena Ridout, MD, FRCPC Toronto Western Hospital Osteoporosis Program University Health Network / Mount Sinai Hospital rowena.ridout@uhn.ca None to declare Conflicts of Interest
BREAST CANCER AND BONE HEALTH Rowena Ridout, MD, FRCPC Toronto Western Hospital Osteoporosis Program University Health Network / Mount Sinai Hospital rowena.ridout@uhn.ca None to declare Conflicts of Interest
HORMONE THERAPY A BALANCED VIEW?? Prof Greta Dreyer
 HORMONE THERAPY A BALANCED VIEW?? Prof Greta Dreyer -- PART 1 -- Definitions HRT hormone replacement therapy HT genome therapy ERT estrogen replacement therapy ET estrogen EPT estrogen progesterone therapy
HORMONE THERAPY A BALANCED VIEW?? Prof Greta Dreyer -- PART 1 -- Definitions HRT hormone replacement therapy HT genome therapy ERT estrogen replacement therapy ET estrogen EPT estrogen progesterone therapy
Meta-analysis: analysis:
 1 Diabetes and TZDs: Risk Factors for Fracture Ann Schwartz, PhD Dept. of Epidemiology and Biostatistics University of California San Francisco July 2010 Osteoporosis CME Presenter Disclosure Information
1 Diabetes and TZDs: Risk Factors for Fracture Ann Schwartz, PhD Dept. of Epidemiology and Biostatistics University of California San Francisco July 2010 Osteoporosis CME Presenter Disclosure Information
Osteoporosis. Treatment of a Silently Developing Disease
 Osteoporosis Treatment of a Silently Developing Disease Marc K. Drezner, MD Senior Associate Dean Emeritus Professor of Medicine Emeritus University of Wisconsin-Madison Auditorium The Forest at Duke October
Osteoporosis Treatment of a Silently Developing Disease Marc K. Drezner, MD Senior Associate Dean Emeritus Professor of Medicine Emeritus University of Wisconsin-Madison Auditorium The Forest at Duke October
Forteo (teriparatide) Prior Authorization Program Summary
 Prior Authorization Program Summary") Forteo (teriparatide) Prior Authorization Program Summary FDA APPROVED INDICATIONS DOSAGE 1 FDA Indication 1 : Forteo (teriparatide) is indicated for: the treatment of postmenopausal women with osteoporosis
Forteo (teriparatide) Prior Authorization Program Summary FDA APPROVED INDICATIONS DOSAGE 1 FDA Indication 1 : Forteo (teriparatide) is indicated for: the treatment of postmenopausal women with osteoporosis
ACP Colorado-Evidence Based Management of Osteoporosis
 ACP Colorado-Evidence Based Management of Osteoporosis Micol S. Rothman, MD Associate Professor of Medicine and Radiology Clinical Director Metabolic Bone Program University of Colorado School of Medicine
ACP Colorado-Evidence Based Management of Osteoporosis Micol S. Rothman, MD Associate Professor of Medicine and Radiology Clinical Director Metabolic Bone Program University of Colorado School of Medicine
OSTEOPOROSIS IN MEN. Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO
 OSTEOPOROSIS IN MEN Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO DISCLOSURES Speakers Bureau: Amgen, Radius Consultant: Abbvie, Amgen, Janssen, Radius, Sanofi Watts NB et
OSTEOPOROSIS IN MEN Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO DISCLOSURES Speakers Bureau: Amgen, Radius Consultant: Abbvie, Amgen, Janssen, Radius, Sanofi Watts NB et
New Therapeutic Directions: Osteoanabolic and Antiresorptive Therapy in Combination Therapy and in Sequence
 New Therapeutic Directions: Osteoanabolic and Antiresorptive Therapy in Combination Therapy and in Sequence John P. Bilezikian, MD, PhD(hon), MACE Silberberg Professor of Medicine Vice-Chair for International
New Therapeutic Directions: Osteoanabolic and Antiresorptive Therapy in Combination Therapy and in Sequence John P. Bilezikian, MD, PhD(hon), MACE Silberberg Professor of Medicine Vice-Chair for International
8/6/2018. Glucocorticoid induced osteoporosis: overlooked and undertreated? Disclosure. Objectives. Overview
 Disclosure Glucocorticoid induced osteoporosis: overlooked and undertreated? I have no financial disclosure relevant to this presentation Tasma Harindhanavudhi, MD Division of Diabetes and Endocrinology
Disclosure Glucocorticoid induced osteoporosis: overlooked and undertreated? I have no financial disclosure relevant to this presentation Tasma Harindhanavudhi, MD Division of Diabetes and Endocrinology
Endocrine Unit and Chair of Endocrinology Director Prof. Manuela Simoni. Hot topics in osteoporosis. How long to treat
 Endocrine Unit and Chair of Endocrinology Director Prof. Manuela Simoni Hot topics in osteoporosis How long to treat Dott. Bruno Madeo bruno.madeo@unimore.it www.endocrinologia.unimore.it/on-line/home.html
Endocrine Unit and Chair of Endocrinology Director Prof. Manuela Simoni Hot topics in osteoporosis How long to treat Dott. Bruno Madeo bruno.madeo@unimore.it www.endocrinologia.unimore.it/on-line/home.html
Recent advances in the management of osteoporosis
 CONFERENCE SUMMARIES Clinical Medicine 2009, Vol 9, No 6: 565 9 Recent advances in the management of osteoporosis Juliet Compston Introduction Osteoporotic fractures are a major cause of morbidity and
CONFERENCE SUMMARIES Clinical Medicine 2009, Vol 9, No 6: 565 9 Recent advances in the management of osteoporosis Juliet Compston Introduction Osteoporotic fractures are a major cause of morbidity and
Breast Cancer and Bone Loss. One in seven women will develop breast cancer during a lifetime
 Breast Cancer and Bone Loss One in seven women will develop breast cancer during a lifetime Causes of Bone Loss in Breast Cancer Patients Aromatase inhibitors Bil Oophorectomy Hypogonadism Steroids Chemotherapy
Breast Cancer and Bone Loss One in seven women will develop breast cancer during a lifetime Causes of Bone Loss in Breast Cancer Patients Aromatase inhibitors Bil Oophorectomy Hypogonadism Steroids Chemotherapy
What is Osteoporosis?
 What is Osteoporosis? 2000 NIH Definition A skeletal disorder characterized by compromised bone strength predisposing a person to an increased risk of fracture. Bone strength reflects the integration of
What is Osteoporosis? 2000 NIH Definition A skeletal disorder characterized by compromised bone strength predisposing a person to an increased risk of fracture. Bone strength reflects the integration of
Parathyroid Hormone Analog for Osteoporosis Prior Authorization with Quantity Limit Criteria Program Summary
 Parathyroid Hormone Analog for Osteoporosis Prior Authorization with Quantity Limit Criteria Program Summary This prior authorization program applies to Commercial, NetResults A series, NetResults F series
Parathyroid Hormone Analog for Osteoporosis Prior Authorization with Quantity Limit Criteria Program Summary This prior authorization program applies to Commercial, NetResults A series, NetResults F series
Treatments for Osteoporosis Expected Benefits, Potential Harms and Drug Holidays. Suzanne Morin MD FRCP FACP McGill University May 2014
 Treatments for Osteoporosis Expected Benefits, Potential Harms and Drug Holidays Suzanne Morin MD FRCP FACP McGill University May 2014 Learning Objectives Overview of osteoporosis management Outline efficacy
Treatments for Osteoporosis Expected Benefits, Potential Harms and Drug Holidays Suzanne Morin MD FRCP FACP McGill University May 2014 Learning Objectives Overview of osteoporosis management Outline efficacy
European guidance for the diagnosis and management of osteoporosis in postmenopausal women
 DOI 10.1007/s00198-008-0560-z POSITION PAPER European guidance for the diagnosis and management of osteoporosis in postmenopausal women J. A. Kanis & N. Burlet & C. Cooper & P. D. Delmas & J.-Y. Reginster
DOI 10.1007/s00198-008-0560-z POSITION PAPER European guidance for the diagnosis and management of osteoporosis in postmenopausal women J. A. Kanis & N. Burlet & C. Cooper & P. D. Delmas & J.-Y. Reginster
Osteoporosis in Men Professor Peter R Ebeling
 Osteoporosis in Men MD FRACP Head, Department of Medicine, School for Clinical Sciences Monash Health Translation Precinct Monash University, Clayton, Victoria 1 MonashHealth Potential Conflicts Departmental
Osteoporosis in Men MD FRACP Head, Department of Medicine, School for Clinical Sciences Monash Health Translation Precinct Monash University, Clayton, Victoria 1 MonashHealth Potential Conflicts Departmental
OSTEOPOROSIS, OSTEOARTHRITIS AND MUSKOSKELETAL DISEASE: A CALL FOR ACTION
 V O L U M E 5 6 N U M B E R 2 J U N E 2 0 1 4 OSTEOPOROSIS, OSTEOARTHRITIS AND MUSKOSKELETAL DISEASE: A CALL FOR ACTION PANMINERVA MED 2014;56:97-114 J. Y., A. NEUPREZ, CH. BEAUDART, F. BUCKINX, J. SLOMIAN,
V O L U M E 5 6 N U M B E R 2 J U N E 2 0 1 4 OSTEOPOROSIS, OSTEOARTHRITIS AND MUSKOSKELETAL DISEASE: A CALL FOR ACTION PANMINERVA MED 2014;56:97-114 J. Y., A. NEUPREZ, CH. BEAUDART, F. BUCKINX, J. SLOMIAN,
2017 Santa Fe Bone Symposium McClung
 217 Santa Fe Bone Symposium Insights into the Use of Anti-remodeling and Anabolic Agents for Osteoporosis Developing a Long-term Management Plan Michael R., MD, FACP Oregon Osteoporosis Center Portland,
217 Santa Fe Bone Symposium Insights into the Use of Anti-remodeling and Anabolic Agents for Osteoporosis Developing a Long-term Management Plan Michael R., MD, FACP Oregon Osteoporosis Center Portland,
AMERICAN COLLEGE OF RHEUMATOLOGY POSITION STATEMENT. Committee on Rheumatologic Care
 AMERICAN COLLEGE OF RHEUMATOLOGY POSITION STATEMENT SUBJECT: PRESENTED BY: FOR DISTRIBUTION TO: Bone Mineral Density Measurement and the Role of Rheumatologists in the Management of Osteoporosis Committee
AMERICAN COLLEGE OF RHEUMATOLOGY POSITION STATEMENT SUBJECT: PRESENTED BY: FOR DISTRIBUTION TO: Bone Mineral Density Measurement and the Role of Rheumatologists in the Management of Osteoporosis Committee
Vasu Pai FRACS, Nat Board, MCh, M.S
 Vasu Pai FRACS, Nat Board, MCh, M.S Composition of bone Mineral 70% Protein 22% Water 8% On osteoclast precurssor On Osteoblast Osteoporosis Dx No clinical lsigns No blood tests Gold standard: Bone
Vasu Pai FRACS, Nat Board, MCh, M.S Composition of bone Mineral 70% Protein 22% Water 8% On osteoclast precurssor On Osteoblast Osteoporosis Dx No clinical lsigns No blood tests Gold standard: Bone