Abdominal Trauma. Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital
|
|
|
- Sharyl Matthews
- 5 years ago
- Views:
Transcription

1 Abdominal Trauma Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital
2 overview Quick review abdominal anatomy Review of mechanism of injury Review of investigation management

3 Anatomy of abdomen
4 External Anatomy Flank Anterior abdomen Back

5 Visceral organ

6 visceral organ Retroperitoneal space Pelvic cavity
7 Abdominal injuries No.1 Preventable cause of death Unrecognized Closed spaces Multisystem / multiple organs Need investigations
8 ATLS protocol Primary survey A B C D E Maintain circulation Stop / seek for bleeding Adjunct to primary survey A Monitoring B C D E investigations
 CT")
9 Investigations for abdominal trauma FAST DPA (DPL) CT scan
10 FAST: Focused Abdominal Sonography for Trauma Advantage Good sensitivity Easy to use Repeatable No radiologic exposure Really excellent test? Disadvatage Operator dependent Poor evaluation for hollow viscus and retropertoneal injury Negative FAST?
11 DPL: Diagnostic Peritoneal Lavage Advantage High sensitivity and specificity Hollow viscus injury detection Disadvantage Invasive Poor evaluation for retropertoneal injury
12 DPL: Diagnostic Peritoneal Lavage Indications Equivocal abdominal sign Unexplained shock Unevaluable abdominal status Alcohol / drug Head / spinal injury unconscious Interpretation DPL positive in Receive 10 ml of gross blood Cell count: RBC > WBC > 500 Biochemistry: amylase > 175 iu/ml Microscopic: food particle, bile, bacteria
13 DPL False positive rate in RBC count 11%, esp. in low RBC cell count False positive rate in WBC count: late DPL
14 Computer Tomography Great sensitivity and specificity Detect hollow viscus, retroperitoneal injury Grading organ injury non-operative management plan Blunt VS penetrating
15 Limitation of CT scan Some hollow viscus and mesenteric injury Patient s hemodynamic status
16 Type of injury Blunt injury Penetrating injury Blast injury
17 Algorithm for the management of blunt abdominal trauma Blunt abdominal trauma Clinically evaluable Clinically unevaluable Diffuse abdominal tenderness No diffuse abdominal tenderness Hemodynamic stable OR Hemodynamic stable Hemodynamic labile CT + CT - OR or NOMx observation
18 Hemodynamically labile FAST + FAST - OR Other causes or hemodynamically labile present No other causes or hemodynamically labile present Further evaluation/ resuscitation DPA + DPA - OR Further evaluation/ resuscitation
19 Hemodynamically stable FAST + FAST - CT + CT - CT? observation OR / NOMx observation
20 Algorithm for the management of penetrating abdominal trauma Penetrating abdominal trauma Diffuse abdominal tenderness + Diffuse abdominal tenderness - OR Hemodynamically stable Hemodynamically labile
21 Hemodynamically stable Left thoracoabdominal or right anterior thoracoabdominal injury No left thoracoabdominal injury laparoscopy GSW SW OR? observation
22 Hemodynamically labile Other cause of hemodynamically lability present No other cause of hemodynamic lability DPA + DPA - OR OR Further evaluate/ resuscitate
23 Investigation for penetrating injury with hemodynamic stable Location Thoracoabdomen Anterior abdominal wall Back and flank investigation CT scan thoracoscopy laparoscopy LWE FAST, DPL CT CT
24 Options of evaluation in penetrating injury Investigation % Sensitivity % Specificity Physical Examination Local Wound Exploration DPL FAST CT scan 97 98

25 Blast Injury Primary Secondary Tertiary Quaternary Blast wave Shrapnel Blast wind Other consequences

26 Indication for surgery Hemodynamic unstability Peritonitis Inability to examine patient
27 Non-operative treatment Solid organ injury only Hemodynamically stable No peritonitis Capable for serial examination immediate investigation and celiotomy if needed Multiple / combined injury
28 Missed abdominal trauma Intraabdominal organs Diaphragmatic injury Hollow viscus injury Retroperitoneal injury Mesenteric injury Other combined injury
29 Combined injuries Head and abdominal injuries 5.7% Challenges: Reliability for abdominal evaluation Timing of CT evaluation of the head Severe head trauma in non-operative Mx of abdominal solid organ injury Major intraabdominal injury with severe blood loss leads secondary brain injury
30 Algorhitm for the management of combined head / abdominal trauma Combined head and abdominal injury Hemodynamically stable Hemodynamically labile GCS < 12 GCS > 12 GCS < 9 GCS > 9 Localizing sign No localizing sign Localizing sign No localizing sign CT before laparotomy Laparotomy before CT Laparotomy Then BH / ICP Laparotomy Follow by CY scan Post op CT scan
31 Pelvic fracture

32 Pelvic Fractures Mechanism AP compression Lateral compression Vertical shear
33 Pelvic Fractures Assessment Inspection: Leg-length discrepancy, external rotation Pelvic ring: Pain on palpation of bony pelvic ring Palpate prostate Associated injuries Pelvic bleeding
34 Pelvic Fractures Emergency Management Fluid resuscitation Determine if open or closed fracture Determine associated perineal /GU injuries Determine need for transfer Splint pelvic fracture
35 Splinting fractured pelvis Pelvic wrapping Pelvic C-clamp External fixator ORIF



36

37
38 Special considerations
39 Case I: 32 year-old female GA 37 weeks G2P1001 Patient model for medical student On the way home: MCA Pain on movement both hip joints

40


41 Pelvic wrapping Roll on her left side

42 External fixator

43 Case II: 37 year-old male Short gun wound abdomen Unstable vital signs on arrival

44
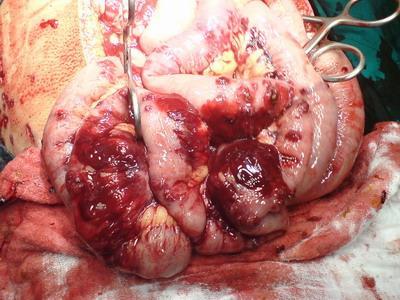
45

46 Case III: 48 year-old male gunshot wound? At posterior right tight Unstable vital signs on arrival No abdominal sign on arrival

47
48

49
50 Conclusion ATLS initial assessment Primary survey Adjunct to primary survey Select appropriate investigation(s) for the injury
2. Blunt abdominal Trauma
 Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
LIVER INJURIES PROFF. S.FLORET
 LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
Selective Nonoperative Management of Penetrating Abdominal Trauma. Kings County Hospital Center Verena Liu, MD 10/13/2011
 Selective Nonoperative Management of Penetrating Abdominal Trauma Kings County Hospital Center Verena Liu, MD 10/13/2011 Case Presentation 28M admitted on 8/27/2011 s/p GSW to right upper quadrant and
Selective Nonoperative Management of Penetrating Abdominal Trauma Kings County Hospital Center Verena Liu, MD 10/13/2011 Case Presentation 28M admitted on 8/27/2011 s/p GSW to right upper quadrant and
SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad
,Ph.D Dr.Evo Elidar Sp.Rad") SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad Trauma Emergency Room layout Ideally the trauma emergency room is centrally located to provide
SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad Trauma Emergency Room layout Ideally the trauma emergency room is centrally located to provide
Imaging in the Trauma Patient
 Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
Penetrating abdominal trauma clinical view. Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland
 Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
Gunshot Wounds to the Abdomen: From Bullet to Incision. Patrick M Reilly MD FACS
 Gunshot Wounds to the Abdomen: From Bullet to Incision Patrick M Reilly MD FACS Master? I Do Get The Chance to Practice What Are We Not Discussing? Stab Wounds Prehospital Care Management of Specific Injuries
Gunshot Wounds to the Abdomen: From Bullet to Incision Patrick M Reilly MD FACS Master? I Do Get The Chance to Practice What Are We Not Discussing? Stab Wounds Prehospital Care Management of Specific Injuries
2 Blunt Abdominal Trauma
 2 Blunt Abdominal Trauma Ricardo Ferrada, Diego Rivera, and Paula Ferrada Pearls and Pitfalls Patients suffering a high-energy trauma have solid viscera rupture in the abdomen and/or aortic rupture in
2 Blunt Abdominal Trauma Ricardo Ferrada, Diego Rivera, and Paula Ferrada Pearls and Pitfalls Patients suffering a high-energy trauma have solid viscera rupture in the abdomen and/or aortic rupture in
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Blunt Abdominal Trauma Evaluation and Management Guideline PEDIATRIC Practice Management Guideline Contact: Trauma Center
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Blunt Abdominal Trauma Evaluation and Management Guideline PEDIATRIC Practice Management Guideline Contact: Trauma Center
Damage Control in Abdominal and Pelvic Injuries
 Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Pan Scan Instead of Clinical Exam? David A. Spain, MD
 Pan Scan Instead of Clinical Exam? David A. Spain, MD Granted, some patients don t t need CT scan Platinum Package Stanford Special CT Scan Head Neck Chest Abdomen Pelvis Takes about 20 minutes to do
Pan Scan Instead of Clinical Exam? David A. Spain, MD Granted, some patients don t t need CT scan Platinum Package Stanford Special CT Scan Head Neck Chest Abdomen Pelvis Takes about 20 minutes to do
PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University
 PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University Patient survive Low morbidity GOOD JUDGMENT COMES FROM EXPERIENCE EXPERIENCE COMES FROM BAD
PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University Patient survive Low morbidity GOOD JUDGMENT COMES FROM EXPERIENCE EXPERIENCE COMES FROM BAD
A Review on the Role of Laparoscopy in Abdominal Trauma
 10.5005/jp-journals-10007-1109 ORIGINAL ARTICLE WJOLS A Review on the Role of Laparoscopy in Abdominal Trauma Aryan Ahmed Specialist General Surgeon, ATLS Instructor, Department of General Surgery, Hamad
10.5005/jp-journals-10007-1109 ORIGINAL ARTICLE WJOLS A Review on the Role of Laparoscopy in Abdominal Trauma Aryan Ahmed Specialist General Surgeon, ATLS Instructor, Department of General Surgery, Hamad
The Role of the FAST exam in the EDRU
 The Role of the FAST exam in the EDRU A. Robb McLean, MD, MHCM Vice Chair of Clinical Operations, Department of Emergency Medicine Joint Trauma Conference June 20, 2017 Disclosures Goals Describe the performance,
The Role of the FAST exam in the EDRU A. Robb McLean, MD, MHCM Vice Chair of Clinical Operations, Department of Emergency Medicine Joint Trauma Conference June 20, 2017 Disclosures Goals Describe the performance,
Initial Pelvic Fracture Management. Patrick M Reilly MD FACS February 27, 2010
 Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
Which Blunt Trauma Patients Should Be Studied by Abdominal CT?
 MDCT of Bowel and Mesenteric Injury: How Findings Influence Management 4 th Nordic Trauma Radiology Course 2006 4 th Nordic Trauma Radiology Course 2006 Stuart E. Mirvis, M.D., FACR Department of Radiology
MDCT of Bowel and Mesenteric Injury: How Findings Influence Management 4 th Nordic Trauma Radiology Course 2006 4 th Nordic Trauma Radiology Course 2006 Stuart E. Mirvis, M.D., FACR Department of Radiology
MANAGEMENT OF SOLID ORGAN INJURIES
 MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
Still is there a Role of Diagnostic Peritoneal Lavage in the Management of Blunt Abdominal Trauma?
 Still is there a Role of Diagnostic Peritoneal Lavage in the Management of Blunt Abdominal Trauma? KHAWAR AWAIS BUTT 1, NABEEL AHMED 2, MEHMOOD ALAM 3, SOMER MASOOD 4 1 Department of Surgery, Avicenna
Still is there a Role of Diagnostic Peritoneal Lavage in the Management of Blunt Abdominal Trauma? KHAWAR AWAIS BUTT 1, NABEEL AHMED 2, MEHMOOD ALAM 3, SOMER MASOOD 4 1 Department of Surgery, Avicenna
Pelvic fractures. Dr Raymond Yean, MBBS Surgical SRMO
 Pelvic fractures Dr Raymond Yean, MBBS Surgical SRMO PELVIC FRACTURES Pelvic fracture account for 2-8% all skeletal injuries Associated with High energy trauma Soft tissue injuries and blood loss. Shock,
Pelvic fractures Dr Raymond Yean, MBBS Surgical SRMO PELVIC FRACTURES Pelvic fracture account for 2-8% all skeletal injuries Associated with High energy trauma Soft tissue injuries and blood loss. Shock,
Guidelines and Protocols
 TITLE: PELVIC TRAUMA PURPOSE: Develop a protocol of care that will insure rapid identification and treatment of these patients PROCESS: I. CARE OF PATIENTS WITH PELVIC TRAUMA A. Patients in hemorrhagic
TITLE: PELVIC TRAUMA PURPOSE: Develop a protocol of care that will insure rapid identification and treatment of these patients PROCESS: I. CARE OF PATIENTS WITH PELVIC TRAUMA A. Patients in hemorrhagic
Management of Pelvic Fracture
 Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
FAST Focused Assessment with Sonography in Trauma
 FAST Focused Assessment with Sonography in Trauma Wilma Rodriguez Mojica,MD,FACR Professor of Radiology UPR School of Medicine Ultrasound Section - Radiological Sciences Department OBJECTIVES Understand
FAST Focused Assessment with Sonography in Trauma Wilma Rodriguez Mojica,MD,FACR Professor of Radiology UPR School of Medicine Ultrasound Section - Radiological Sciences Department OBJECTIVES Understand
We have reviewed this material in accordance with U.S. Copyright Law and have tried to maximize your ability to
 Author(s): Patrick Carter, Daniel Wachter, Rockefeller Oteng, Carl Seger, 2009-2010. License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution
Author(s): Patrick Carter, Daniel Wachter, Rockefeller Oteng, Carl Seger, 2009-2010. License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Splenic Injury Evaluation and Management Guideline ADULT Practice Management Guideline Contact: Trauma Center Medical
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Splenic Injury Evaluation and Management Guideline ADULT Practice Management Guideline Contact: Trauma Center Medical
Algorithms for managing the common trauma patient
 ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
Pelvic Injuries. Chapter 21
 Chapter 21 Introduction Injuries of the pelvis are an uncommon, but potentially lethal, battlefield injury. Blunt injuries may be associated with major hemorrhage and early mortality. Death within the
Chapter 21 Introduction Injuries of the pelvis are an uncommon, but potentially lethal, battlefield injury. Blunt injuries may be associated with major hemorrhage and early mortality. Death within the
ATLS: Initial Assessment and Management. SAUSHEC Medical Student Lecture Series
 ATLS: Initial Assessment and Management SAUSHEC Medical Student Lecture Series Objectives Identify sequence of priorities in assessing the multiply injured patient Apply principles outlined in primary
ATLS: Initial Assessment and Management SAUSHEC Medical Student Lecture Series Objectives Identify sequence of priorities in assessing the multiply injured patient Apply principles outlined in primary
ABDOMINAL TRAUMA. Aurora Health Care EMS Continuing Education 2 nd Quarter 2011 Packet
 Aurora Health Care EMS Continuing Education 2 nd Quarter 2011 Packet ABDOMINAL TRAUMA Blunt and penetrating abdominal trauma are major causes of morbidity and mortality in the United States, particularly
Aurora Health Care EMS Continuing Education 2 nd Quarter 2011 Packet ABDOMINAL TRAUMA Blunt and penetrating abdominal trauma are major causes of morbidity and mortality in the United States, particularly
Trauma. Neck trauma zones. Neck Injuries 1/3/2018. Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure
 Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Pelvic Fractures. AOCP National Course Belfast City Hospital. 11 th June D Swain BSc; FRCSI; FRCS (Orth.)
") Pelvic Fractures AOCP National Course Belfast City Hospital 11 th June 2010 Who s this bloke? Consultant orthopaedic surgeon RVH Trained in Belfast, England and Toronto Interests - pelvic and acetabular
Pelvic Fractures AOCP National Course Belfast City Hospital 11 th June 2010 Who s this bloke? Consultant orthopaedic surgeon RVH Trained in Belfast, England and Toronto Interests - pelvic and acetabular
Review. 1. Peritonitis would MOST likely result following injury to the: A. liver. B. spleen. C. kidney. D. stomach.
 Chapter 28 Review Review 1. Peritonitis would MOST likely result following injury to the: A. liver. B. spleen. C. kidney. D. stomach. Review Answer: D Rationale: In general, solid organs bleed when injured
Chapter 28 Review Review 1. Peritonitis would MOST likely result following injury to the: A. liver. B. spleen. C. kidney. D. stomach. Review Answer: D Rationale: In general, solid organs bleed when injured
Introduction to Advanced Trauma Life Support ATLS
 Introduction to Advanced Trauma Life Support ATLS Objectives Concepts of primary & secondary survey Priorities & Life threatening conditions Clinical & Surgical skills Basic knowledge Rapid assessment
Introduction to Advanced Trauma Life Support ATLS Objectives Concepts of primary & secondary survey Priorities & Life threatening conditions Clinical & Surgical skills Basic knowledge Rapid assessment
PARA107 Summary. Page 1-3: Page 4-6: Page 7-10: Page 11-13: Page 14-17: Page 18-21: Page 22-25: Page 26-28: Page 29-33: Page 34-36: Page 37-38:
 PARA107 Summary Page 1-3: Page 4-6: Page 7-10: Page 11-13: Page 14-17: Page 18-21: Page 22-25: Page 26-28: Page 29-33: Page 34-36: Page 37-38: Injury, Mechanisms of Injury, Time Critical Guidelines Musculoskeletal
PARA107 Summary Page 1-3: Page 4-6: Page 7-10: Page 11-13: Page 14-17: Page 18-21: Page 22-25: Page 26-28: Page 29-33: Page 34-36: Page 37-38: Injury, Mechanisms of Injury, Time Critical Guidelines Musculoskeletal
Abdomen and Genitalia Injuries. Chapter 28
 Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
Diagnosis & Management of Kidney Trauma. LAU - Urology Residency Program LOP Urology Residents Meeting
 Diagnosis & Management of Kidney Trauma LAU - Urology Residency Program LOP Urology Residents Meeting Outline Introduction Investigation Staging Treatment Introduction The kidneys are the most common genitourinary
Diagnosis & Management of Kidney Trauma LAU - Urology Residency Program LOP Urology Residents Meeting Outline Introduction Investigation Staging Treatment Introduction The kidneys are the most common genitourinary
Case conference. Past History. Chief Complaint. Physical examination. Patient Profile
 Patient Profile Case conference 指導醫師 : 林俊龍醫師報告者 :PGY 王奕雯日期 :2012/12/17 Age/Sex: 53 y/o Male Date:Day1 03:32 TPR: 37.2/88/16, BP: 124/88mmHg E4M6V5, SpO2: 95% Triage II 喝酒和人打架 Chief Complaint Stabbed over
Patient Profile Case conference 指導醫師 : 林俊龍醫師報告者 :PGY 王奕雯日期 :2012/12/17 Age/Sex: 53 y/o Male Date:Day1 03:32 TPR: 37.2/88/16, BP: 124/88mmHg E4M6V5, SpO2: 95% Triage II 喝酒和人打架 Chief Complaint Stabbed over
Initial Management of Pelvic Injuries
 Initial Management of Pelvic Injuries Olav Røise, MD, PhD Chairman Division of Neuroscience and Skeletal Medicine Ullevål University Hospital Trauma treatment Represent a chain of health services in which
Initial Management of Pelvic Injuries Olav Røise, MD, PhD Chairman Division of Neuroscience and Skeletal Medicine Ullevål University Hospital Trauma treatment Represent a chain of health services in which
Management of Bleeding Pelvic Fractures
 Management of Bleeding Pelvic Fractures Clay Cothren Burlew, MD FACS Professor of Surgery Program Director, SCC and TACS Fellowships Director, Surgical Intensive Care Unit Denver Health Medical Center/University
Management of Bleeding Pelvic Fractures Clay Cothren Burlew, MD FACS Professor of Surgery Program Director, SCC and TACS Fellowships Director, Surgical Intensive Care Unit Denver Health Medical Center/University
West Yorkshire Major Trauma Network Clinical Guidelines 2015
 WYMTN: Pelvic fracture with urogenital trauma KEY RECOMMENDATIONS 1. During the initial exploratory survey / secondary survey, a. The external urethral meatus and the transurethral bladder catheter (if
WYMTN: Pelvic fracture with urogenital trauma KEY RECOMMENDATIONS 1. During the initial exploratory survey / secondary survey, a. The external urethral meatus and the transurethral bladder catheter (if
Clinical Questions. Clinical Questions. Clinical Questions. Health-Process-Evidencebased Clinical Practice Guidelines Acute Abdomen
 Health-Process-Evidencebased Clinical Practice Guidelines Acute Abdomen 1. What is an operational concept of acute abdomen? any abdominal condition of acute onset from various causes involving the intraabdominal
Health-Process-Evidencebased Clinical Practice Guidelines Acute Abdomen 1. What is an operational concept of acute abdomen? any abdominal condition of acute onset from various causes involving the intraabdominal
Genitourinary Trauma Introduction GU Trauma overlooked
 Genitourinary Trauma Introduction GU Trauma overlooked 10-20% of all injured patients Long term morbidity Impotence Incontinence Life-threatening injuries first Urethral Injury Plan Bladder Injury Kidney
Genitourinary Trauma Introduction GU Trauma overlooked 10-20% of all injured patients Long term morbidity Impotence Incontinence Life-threatening injuries first Urethral Injury Plan Bladder Injury Kidney
MEDICAL MANAGEMENT OF ABDOMINAL TRAUMA. LUIS H. TELLO MV, MS, DVM, COS Portland Hospital Classic International Medical Advisor Banfield Pet Hospital
 MEDICAL MANAGEMENT OF ABDOMINAL TRAUMA LUIS H. TELLO MV, MS, DVM, COS Portland Hospital Classic International Medical Advisor Banfield Pet Hospital ABDOMINAL TRAUMA 70-80% of multiple trauma patients 55%
MEDICAL MANAGEMENT OF ABDOMINAL TRAUMA LUIS H. TELLO MV, MS, DVM, COS Portland Hospital Classic International Medical Advisor Banfield Pet Hospital ABDOMINAL TRAUMA 70-80% of multiple trauma patients 55%
Sasha Dubrovsky, MSc MD FRCPC Pediatric Emergency Medicine Montreal Children s Hospital - MUHC October 2010
 Sasha Dubrovsky, MSc MD FRCPC Pediatric Emergency Medicine Montreal Children s Hospital - MUHC October 2010 Learning objectives 1. Discuss diagnostic goals in pediatric trauma Diagnose All vs. Severe Injuries
Sasha Dubrovsky, MSc MD FRCPC Pediatric Emergency Medicine Montreal Children s Hospital - MUHC October 2010 Learning objectives 1. Discuss diagnostic goals in pediatric trauma Diagnose All vs. Severe Injuries
PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE
 PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE Samuel Hawkins MD CASE PRESENTATION 22M BIBEMS s/p multiple GSW ABCs intact Normotensive, non-tachycardic Secondary Survey: 4 truncal bullet holes L superior
PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE Samuel Hawkins MD CASE PRESENTATION 22M BIBEMS s/p multiple GSW ABCs intact Normotensive, non-tachycardic Secondary Survey: 4 truncal bullet holes L superior
Abdominal Ultrasonography
 Abdominal Ultrasonography David A. Masneri, DO, FACEP, FAAEM Assistant Professor of Emergency Medicine Assistant Director, Emergency Medicine Residency Medical Director, Operational Medicine Division Center
Abdominal Ultrasonography David A. Masneri, DO, FACEP, FAAEM Assistant Professor of Emergency Medicine Assistant Director, Emergency Medicine Residency Medical Director, Operational Medicine Division Center
Practice Management Guidelines for. Nonoperative Management of Penetrating. Abdominal Trauma
 Practice Management Guidelines for Nonoperative Management of Penetrating Abdominal Trauma Eastern Association for the Surgery of Trauma: Practice Management Guideline Committee John J. Como, MD Faran
Practice Management Guidelines for Nonoperative Management of Penetrating Abdominal Trauma Eastern Association for the Surgery of Trauma: Practice Management Guideline Committee John J. Como, MD Faran
Radiological Investigations of Abdominal Trauma
 76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
Evaluating an Ultrasound Algorithm for Patients with Blunt Abdominal Trauma
 ABSTRACT Evaluating an Ultrasound Algorithm for Patients with Blunt Abdominal Trauma Ara J. Feinstein, MD, Mark G. McKenney, MD, Stephen M. Cohn, MD Ryder Trauma Center, Department of Surgery University
ABSTRACT Evaluating an Ultrasound Algorithm for Patients with Blunt Abdominal Trauma Ara J. Feinstein, MD, Mark G. McKenney, MD, Stephen M. Cohn, MD Ryder Trauma Center, Department of Surgery University
Management guidelines for penetrating abdominal trauma Walter L. Biffl and Ernest E. Moore
 Management guidelines for penetrating abdominal trauma Walter L. Biffl and Ernest E. Moore Department of Surgery, Denver Health Medical Center/University of Colorado, Denver, Colorado, USA Correspondence
Management guidelines for penetrating abdominal trauma Walter L. Biffl and Ernest E. Moore Department of Surgery, Denver Health Medical Center/University of Colorado, Denver, Colorado, USA Correspondence
Muscle spasm Diminished bowel sounds Nausea/vomiting
 3 4 5 6 7 8 9 0 Chapter 8: Abdomen and Genitalia Injuries Abdominal Injuries Abdomen is major body cavity extending from to pelvis. Contains organs that make up digestive, urinary, and genitourinary systems.
3 4 5 6 7 8 9 0 Chapter 8: Abdomen and Genitalia Injuries Abdominal Injuries Abdomen is major body cavity extending from to pelvis. Contains organs that make up digestive, urinary, and genitourinary systems.
If your patient is stable, perform a complete assessment using inspection, auscultation, percussion, and pal- By Cynthia Blank-Reid, RN, CEN, MSN
 Abdominal trauma: Dealing with the damage Hidden in the abdomen, life-threatening injuries can elude detection. Find out how to evaluate your patient s condition and prevent further harm. By Cynthia Blank-Reid,
Abdominal trauma: Dealing with the damage Hidden in the abdomen, life-threatening injuries can elude detection. Find out how to evaluate your patient s condition and prevent further harm. By Cynthia Blank-Reid,
Penetrating Abdominal Trauma: Evaluation & Treatment
 Penetrating Abdominal Trauma: Evaluation & Treatment Charles Krin & Karim Brohi, London, UK, August 09, 2004; edited & updated by Christian Jones, Baltimore, MD, US, August 21, 2017 About this edition
Penetrating Abdominal Trauma: Evaluation & Treatment Charles Krin & Karim Brohi, London, UK, August 09, 2004; edited & updated by Christian Jones, Baltimore, MD, US, August 21, 2017 About this edition
Study of management of blunt injuries to solid abdominal organs
 Original article: Study of management of blunt injuries to solid abdominal organs 1Dr. Jayant Jain, 2 Dr. S.P. Singh, 3 Dr. Arun Bhargava 1III year resident, Dept of General Surgery NIMS hospital and medical
Original article: Study of management of blunt injuries to solid abdominal organs 1Dr. Jayant Jain, 2 Dr. S.P. Singh, 3 Dr. Arun Bhargava 1III year resident, Dept of General Surgery NIMS hospital and medical
Trauma CT Scanning Protocol
 Northern Trauma Network Trauma CT Scanning Protocol Background Whole body CT (WBCT) has assumed a pivotal position in trauma management. UK trauma is typically described as blunt and blind i.e. blunt trauma
Northern Trauma Network Trauma CT Scanning Protocol Background Whole body CT (WBCT) has assumed a pivotal position in trauma management. UK trauma is typically described as blunt and blind i.e. blunt trauma
The utility of focused abdominal ultrasound in blunt abdominal trauma: a reappraisal
 The American Journal of Surgery 194 (2007) 728 733 Presentation The utility of focused abdominal ultrasound in blunt abdominal trauma: a reappraisal Thomas S. Helling, M.D., F.A.C.S.*, Jennifer Wilson,
The American Journal of Surgery 194 (2007) 728 733 Presentation The utility of focused abdominal ultrasound in blunt abdominal trauma: a reappraisal Thomas S. Helling, M.D., F.A.C.S.*, Jennifer Wilson,
Haemodynamic deterioration in lateral compression pelvic fracture after prehospital pelvic circumferential compression device application
 Haemodynamic deterioration in lateral compression pelvic fracture after prehospital pelvic circumferential compression device application Authors Alan A Garner Retrieval consultant CareFlight Northmead,
Haemodynamic deterioration in lateral compression pelvic fracture after prehospital pelvic circumferential compression device application Authors Alan A Garner Retrieval consultant CareFlight Northmead,
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/1887/39153 holds various files of this Leiden University dissertation. Author: Hommes, M. Title: The injured liver : management and hepatic injuries in the traumapatient
Cover Page The handle http://hdl.handle.net/1887/39153 holds various files of this Leiden University dissertation. Author: Hommes, M. Title: The injured liver : management and hepatic injuries in the traumapatient
Major Trauma Scenarios. Ballarat Health Services Emergency Medicine Training Hub
 Major Trauma Scenarios Ballarat Health Services Emergency Medicine Training Hub Trauma Scenario 1 You receive a phone call from the ambulance service. They have a 27 yr old male involved in a MCA, he is
Major Trauma Scenarios Ballarat Health Services Emergency Medicine Training Hub Trauma Scenario 1 You receive a phone call from the ambulance service. They have a 27 yr old male involved in a MCA, he is
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons
 General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: TRAUMA 7-Nov-2016 DEVELOPED BY: Zsolt Balogh, Peter
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: TRAUMA 7-Nov-2016 DEVELOPED BY: Zsolt Balogh, Peter
ABDOMINAL TRAUMA MODULE
 INTRODUCTION ABDOMINAL TRAUMA MODULE Blunt abdominal trauma most commonly occurs in the setting of motor vehicle accidents, pedestrian related trauma, direct blows and falls. 1 In these situations, blunt
INTRODUCTION ABDOMINAL TRAUMA MODULE Blunt abdominal trauma most commonly occurs in the setting of motor vehicle accidents, pedestrian related trauma, direct blows and falls. 1 In these situations, blunt
The FAST Exam! Dr. David Easton MD FRCPC Critical Care and Emergency Medicine University of Manitoba Canada
 The FAST Exam! Dr. David Easton MD FRCPC Critical Care and Emergency Medicine University of Manitoba Canada Dr. David Easton MD FRCPC Assistant Professor Section of Critical Care and Emergency Medicine
The FAST Exam! Dr. David Easton MD FRCPC Critical Care and Emergency Medicine University of Manitoba Canada Dr. David Easton MD FRCPC Assistant Professor Section of Critical Care and Emergency Medicine
UBC Department of Urologic Sciences Lecture Series. Urological Trauma
 UBC Department of Urologic Sciences Lecture Series Urological Trauma Disclaimer: This is a lot of information to cover and we are unlikely to cover it all today These slides are to be utilized for your
UBC Department of Urologic Sciences Lecture Series Urological Trauma Disclaimer: This is a lot of information to cover and we are unlikely to cover it all today These slides are to be utilized for your
Imaging in Trauma. Dr Amir Ashrafi
 + Imaging in Trauma Dr Amir Ashrafi + Portable x-rays n Plain radiographs play an important role in the primary evaluation of the unstable trauma patient. n Prompt imaging of the lateral cervical spine,
+ Imaging in Trauma Dr Amir Ashrafi + Portable x-rays n Plain radiographs play an important role in the primary evaluation of the unstable trauma patient. n Prompt imaging of the lateral cervical spine,
The Secondary Survey
 The Secondary Survey Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Attending Surgeon, Denver Health Medical Center Associate Professor of Surgery, University of Colorado Outlining
The Secondary Survey Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Attending Surgeon, Denver Health Medical Center Associate Professor of Surgery, University of Colorado Outlining
Selective Management of Penetrating Truncal Injuries: Is Emergency Department Discharge a Reasonable Goal?
 Selective Management of Penetrating Truncal Injuries: Is Emergency Department Discharge a Reasonable Goal? MARK F. CONRAD, M.D., JOE H. FATTON, JR., M.D., MANESH PARIKSHAK, M.D., KURT A. KRALOVICH, M.D.
Selective Management of Penetrating Truncal Injuries: Is Emergency Department Discharge a Reasonable Goal? MARK F. CONRAD, M.D., JOE H. FATTON, JR., M.D., MANESH PARIKSHAK, M.D., KURT A. KRALOVICH, M.D.
CORE STANDARDS STANDARDS USED IN TARN REPORTS
 CORE STANDARDS Time to CT Scan BEST PRACTICE TARIFF SECTION 4.10 MAJOR TRAUMA 7 If the patient is admitted directly to the MTC or transferred as an emergency, the patient must be received by a trauma team
CORE STANDARDS Time to CT Scan BEST PRACTICE TARIFF SECTION 4.10 MAJOR TRAUMA 7 If the patient is admitted directly to the MTC or transferred as an emergency, the patient must be received by a trauma team
Negative Laparotomy in Trauma: Are We Getting Better?
 Negative Laparotomy in Trauma: Are We Getting Better? BEAT SCHNÜRIGER, M.D., LYDIA LAM, M.D., KENJI INABA, M.D., LESLIE KOBAYASHI, M.D., RAFFAELLA BARBARINO, M.D., DEMETRIOS DEMETRIADES, M.D., PH.D. From
Negative Laparotomy in Trauma: Are We Getting Better? BEAT SCHNÜRIGER, M.D., LYDIA LAM, M.D., KENJI INABA, M.D., LESLIE KOBAYASHI, M.D., RAFFAELLA BARBARINO, M.D., DEMETRIOS DEMETRIADES, M.D., PH.D. From
SAS Journal of Surgery ISSN SAS J. Surg., Volume-2; Issue-1 (Jan-Feb, 2016); p Available online at
; p Available online at") SAS Journal of Surgery ISSN 2454-5104 SAS J. Surg., Volume-2; Issue-1 (Jan-Feb, 2016); p-53-59 Available online at http://sassociety.com/sasjs/ Original Research Article Clinical Study, Evaluation and
SAS Journal of Surgery ISSN 2454-5104 SAS J. Surg., Volume-2; Issue-1 (Jan-Feb, 2016); p-53-59 Available online at http://sassociety.com/sasjs/ Original Research Article Clinical Study, Evaluation and
ISPUB.COM. S Gopalswamy, R Mohanraj, P Viswanathan, V Baskaran INTRODUCTION HYPOTHESIS MATERIAL AND METHODS RESULTS
 ISPUB.COM The Internet Journal of Surgery Volume 15 Number 2 Non-Operative Management of Solid Organ Injuries due to Blunt Abdominal Trauma (NOMAT): Seven-year experience in a Teaching District General
ISPUB.COM The Internet Journal of Surgery Volume 15 Number 2 Non-Operative Management of Solid Organ Injuries due to Blunt Abdominal Trauma (NOMAT): Seven-year experience in a Teaching District General
Conservative Versus Delayed Laparoscopic Exploration for Blunt Abdominal Trauma
 Med. J. Cairo Univ., Vol. 80, No. 1, September: 575-584, 2012 www.medicaljournalofcairouniversity.com Conservative Versus Delayed Laparoscopic Exploration for Blunt Abdominal Trauma TAMER M. NABIL, M.D.*;
Med. J. Cairo Univ., Vol. 80, No. 1, September: 575-584, 2012 www.medicaljournalofcairouniversity.com Conservative Versus Delayed Laparoscopic Exploration for Blunt Abdominal Trauma TAMER M. NABIL, M.D.*;
Review. 1. Kinetic energy is a calculation of:
 Chapter 22 Review Review 1. Kinetic energy is a calculation of: A. weight and size. B. weight and speed. Caring for victims of traumatic injuries requires the EMT to have a solid understanding of the trauma
Chapter 22 Review Review 1. Kinetic energy is a calculation of: A. weight and size. B. weight and speed. Caring for victims of traumatic injuries requires the EMT to have a solid understanding of the trauma
Lecture 56 Kidney and Urinary System
 Lecture 56 Kidney and Urinary System The adrenal glands are located on the superomedial aspect of the kidney The right diagram shows a picture of the kidney with the abdominal walls and organs removed
Lecture 56 Kidney and Urinary System The adrenal glands are located on the superomedial aspect of the kidney The right diagram shows a picture of the kidney with the abdominal walls and organs removed
ABDOMINAL TRAUMA Lecture Prof. Zbigniew Wlodarczyk
 ABDOMINAL TRAUMA Lecture Prof. Zbigniew Wlodarczyk Epidemiology 2% of all traumas (4% amongst hospitalized patients) 75% M 25% F Average age 35 years 80% close 20% penetrating 40% liver and spleen, 10%
ABDOMINAL TRAUMA Lecture Prof. Zbigniew Wlodarczyk Epidemiology 2% of all traumas (4% amongst hospitalized patients) 75% M 25% F Average age 35 years 80% close 20% penetrating 40% liver and spleen, 10%
Activity Three: Where s the Bleeding?
 Activity Three: Where s the Bleeding? There are five main sites of potentially fatal bleeding in trauma, remembered by the phrase on the floor and four more. On the floor refers to losing blood externally
Activity Three: Where s the Bleeding? There are five main sites of potentially fatal bleeding in trauma, remembered by the phrase on the floor and four more. On the floor refers to losing blood externally
A PROSPECTIVE STUDY OF CONSERVATIVE MANAGEMENT IN CASES OF HEMOPERITONEUM IN SOLID ORGAN INJURIES AT TERTIARY CARE HOSPITAL IN WESTERN INDIA
 RESEARCH ARTICLE A PROSPECTIVE STUDY OF CONSERVATIVE MANAGEMENT IN CASES OF HEMOPERITONEUM IN SOLID ORGAN INJURIES AT TERTIARY CARE HOSPITAL IN WESTERN INDIA Chintan Patel 1, Isha Patel 2, Divyang Dave
RESEARCH ARTICLE A PROSPECTIVE STUDY OF CONSERVATIVE MANAGEMENT IN CASES OF HEMOPERITONEUM IN SOLID ORGAN INJURIES AT TERTIARY CARE HOSPITAL IN WESTERN INDIA Chintan Patel 1, Isha Patel 2, Divyang Dave
The Acute Management of Pelvic Ring Injuries
 The Acute Management of Pelvic Ring Injuries Brian J Ladner, MD North Oaks Medical Center Original Author: Kyle F. Dickson, MD; Created March 2004 Sean E. Nork, MD; Revised December 2010 New Author: October
The Acute Management of Pelvic Ring Injuries Brian J Ladner, MD North Oaks Medical Center Original Author: Kyle F. Dickson, MD; Created March 2004 Sean E. Nork, MD; Revised December 2010 New Author: October
George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon
 George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon Health and Sciences University. Portland, OR Outline
George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon Health and Sciences University. Portland, OR Outline
utility of Plain Film Pelvic Radiographs in Blunt Trauma Patients in the Emergency Department
 utility of Plain Film Pelvic Radiographs in Blunt Trauma Patients in the Emergency Department AMAL KAMIL OBAID, M.D., ANDREW BARLEBEN, M.D., DIANA PORRAL, B.S., STEPHANIE LUSH, M.S.N., MARIANNE CINAT,
utility of Plain Film Pelvic Radiographs in Blunt Trauma Patients in the Emergency Department AMAL KAMIL OBAID, M.D., ANDREW BARLEBEN, M.D., DIANA PORRAL, B.S., STEPHANIE LUSH, M.S.N., MARIANNE CINAT,
Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing
 1 2 3 4 5 6 Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing D-Disability Chief complaint and/or Mechanism
1 2 3 4 5 6 Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing D-Disability Chief complaint and/or Mechanism
Therapeutic and diagnostic role of laparoscopy in penetrating abdominal trauma
 Therapeutic and diagnostic role of laparoscopy in penetrating abdominal trauma Thesis Submitted for fulfillment of the Master degree (M.Sc.) in GENERAL SURGERY By MOHAMED OMAR ABD AL ALIM (M.B, B.Ch.)
Therapeutic and diagnostic role of laparoscopy in penetrating abdominal trauma Thesis Submitted for fulfillment of the Master degree (M.Sc.) in GENERAL SURGERY By MOHAMED OMAR ABD AL ALIM (M.B, B.Ch.)
Imaging in abdominal trauma
 Imaging in abdominal trauma Dilyana Baleva Medical University Varna Landesklinikum Mistelbach-Gänserndorf Learning objectives Definition, demographics and etiology Imaging modalities and protocols Common
Imaging in abdominal trauma Dilyana Baleva Medical University Varna Landesklinikum Mistelbach-Gänserndorf Learning objectives Definition, demographics and etiology Imaging modalities and protocols Common
Gunshot Wounds of the Abdomen: Association of Surface Wounds with Internal Injuries
 Gunshot Wounds of the Abdomen: Association of Surface Wounds with Internal Injuries Abstract Ashfaq A. Razzaq ( Department of Surgery, Jinnah Post-graduate Medical Center, Karachi. ) Objective: To evaluate
Gunshot Wounds of the Abdomen: Association of Surface Wounds with Internal Injuries Abstract Ashfaq A. Razzaq ( Department of Surgery, Jinnah Post-graduate Medical Center, Karachi. ) Objective: To evaluate
RESUSCITATION IN TRAUMA. Important things I have learnt
 RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
10/2/2018. Acute Management of Pelvic Injuries. Learning Objectives. 17 yo male ped struck by truck
 17 yo male ped struck by truck Acute Management of Pelvic Injuries David Volgas, MD CoxHealth University of Missouri HD unstable Open pelvic wound superior gluteal fold through rectum to scrotum Open rami
17 yo male ped struck by truck Acute Management of Pelvic Injuries David Volgas, MD CoxHealth University of Missouri HD unstable Open pelvic wound superior gluteal fold through rectum to scrotum Open rami
Thicker than Water. Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago
 Thicker than Water Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago I have no relevant financial relationships to disclose. Who is bleeding? How much and what kind
Thicker than Water Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago I have no relevant financial relationships to disclose. Who is bleeding? How much and what kind
Canadian Undergraduate Urology Curriculum (CanUUC): Genitourinary Trauma. Last reviewed June 2014
: Genitourinary Trauma. Last reviewed June 2014") Canadian Undergraduate Urology Curriculum (CanUUC): Genitourinary Trauma Last reviewed June 2014 Session Objectives 1. Recognize hematuria as the cardinal symptom of urinary tract trauma. 1. Outline the
Canadian Undergraduate Urology Curriculum (CanUUC): Genitourinary Trauma Last reviewed June 2014 Session Objectives 1. Recognize hematuria as the cardinal symptom of urinary tract trauma. 1. Outline the
A Clinical Study of Blunt Injury Abdomen in a Tertiary Care Hospital
 Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/167 A Clinical Study of Blunt Injury Abdomen in a Tertiary Care Hospital J Amuthan 1, A Vijay 2, C Pradeep 2, Heber
Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/167 A Clinical Study of Blunt Injury Abdomen in a Tertiary Care Hospital J Amuthan 1, A Vijay 2, C Pradeep 2, Heber
Spinal Cord Injuries: The Basics. Kadre Sneddon POS Rounds October 1, 2003
 Spinal Cord Injuries: The Basics Kadre Sneddon POS Rounds October 1, 2003 Anatomy Dorsal columntouch, vibration Corticospinal tract- UMN Anterior horn-lmn Spinothalamic tractpain, temperature (contralateral)
Spinal Cord Injuries: The Basics Kadre Sneddon POS Rounds October 1, 2003 Anatomy Dorsal columntouch, vibration Corticospinal tract- UMN Anterior horn-lmn Spinothalamic tractpain, temperature (contralateral)
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #2 Blunt Trauma
 McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #2 Blunt Trauma Blunt trauma is the most common cause of traumatic death and disability. The definition
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #2 Blunt Trauma Blunt trauma is the most common cause of traumatic death and disability. The definition
OUTLINE SHEET 5.4 PRIMARY SURVEY
 ENABLING OBJECTIVES: 4.7 List the procedures used in a primary survey. 4.8 Demonstrate primary survey procedures used in a mock trauma (moulage) scenario without injury to personnel or damage to equipment.
ENABLING OBJECTIVES: 4.7 List the procedures used in a primary survey. 4.8 Demonstrate primary survey procedures used in a mock trauma (moulage) scenario without injury to personnel or damage to equipment.
NOTE If it is necessary to perform abdominal thrusts, expose the abdominal area prior to pressing on the abdomen.
 ENABLING OBJECTIVES: 4.7 List the procedures used in a primary survey. 4.8 Demonstrate primary survey procedures used in a mock trauma (moulage) scenario without injury to personnel or damage to equipment.
ENABLING OBJECTIVES: 4.7 List the procedures used in a primary survey. 4.8 Demonstrate primary survey procedures used in a mock trauma (moulage) scenario without injury to personnel or damage to equipment.
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons
 General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: TRAUMA 5-May-2013 DEVELOPED BY: Zsolt Balogh, Peter
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: TRAUMA 5-May-2013 DEVELOPED BY: Zsolt Balogh, Peter
Penetrating Trauma in Pediatric Patients. Heidi P. Cordi, MD, MPH, MS, EMTP, FACEP, FAADM EMS WEEK 2017
 Penetrating Trauma in Pediatric Patients Heidi P. Cordi, MD, MPH, MS, EMTP, FACEP, FAADM EMS WEEK 2017 Introduction Trauma is the leading cause of death between ages of 1-18 years Penetrating injury accounts
Penetrating Trauma in Pediatric Patients Heidi P. Cordi, MD, MPH, MS, EMTP, FACEP, FAADM EMS WEEK 2017 Introduction Trauma is the leading cause of death between ages of 1-18 years Penetrating injury accounts
2/16/2019 EMRAM IN-SERVICE REVIEW: TRAUMA 3 ABDOMINAL TRAUMA OUTLINE BLUNT ABDOMINAL TRAUMA DIAPHRAGMATIC INJURIES HOLLOW VISCUS INJURIES
 OUTLINE EMRAM IN-SERVICE REVIEW: TRAUMA 3 ANGELA M. PUGLIESE MD DEPARTMENT OF EMERGENCY MEDICINE HENRY FORD HOSPITAL ABDOMINAL TRAUMA PUNCTURE WOUNDS SPECIAL (SENSITIVE LACERATIONS) LID LACERATIONS GLOBE
OUTLINE EMRAM IN-SERVICE REVIEW: TRAUMA 3 ANGELA M. PUGLIESE MD DEPARTMENT OF EMERGENCY MEDICINE HENRY FORD HOSPITAL ABDOMINAL TRAUMA PUNCTURE WOUNDS SPECIAL (SENSITIVE LACERATIONS) LID LACERATIONS GLOBE
Aviation Rescue Swimmer Course
 Aviation Rescue Swimmer Course Primary Survey LT 5.4 December 2003 1 Objectives List the procedures used in a primary survey. Demonstrate primary survey procedures used in a mock trauma (moulage) scenario
Aviation Rescue Swimmer Course Primary Survey LT 5.4 December 2003 1 Objectives List the procedures used in a primary survey. Demonstrate primary survey procedures used in a mock trauma (moulage) scenario
Physical examination of the abdomen has been the
 Clinical Articles The use of ultrasound in blunt trauma Author: Thomas T. Levins, RN, CCRN, CEN, CFRN, Yardley, Pa Physical examination of the abdomen has been the mainstay of assessment for the presence
Clinical Articles The use of ultrasound in blunt trauma Author: Thomas T. Levins, RN, CCRN, CEN, CFRN, Yardley, Pa Physical examination of the abdomen has been the mainstay of assessment for the presence
M Magray, M Shahdhar, M Wani, M Shafi, J Sheikh, H Wani
 ISPUB.COM The Internet Journal of Surgery Volume 30 Number 2 Studying The Role Of Computed Tomography In Selective Management Of Blunt Abdominal Trauma Patients In A Single Tertiary Care Centre In Northern
ISPUB.COM The Internet Journal of Surgery Volume 30 Number 2 Studying The Role Of Computed Tomography In Selective Management Of Blunt Abdominal Trauma Patients In A Single Tertiary Care Centre In Northern
Decision-Making in the Acute Management of Blunt and Penetrating Wounds Mary Somerville, DVM, DACVS
 Decision-Making in the Acute Management of Blunt and Penetrating Wounds Mary Somerville, DVM, DACVS Providing the best quality care and service for the patient, the client, and the referring veterinarian.
Decision-Making in the Acute Management of Blunt and Penetrating Wounds Mary Somerville, DVM, DACVS Providing the best quality care and service for the patient, the client, and the referring veterinarian.
17. Imaging and interventional radiology
 17. Imaging and interventional radiology These guidelines have been adapted from the Leeds Major Trauma Centre Imaging in Paediatric Major Trauma guidelines Written by Dr Annmarie Jeanes (Consultant Paediatric
17. Imaging and interventional radiology These guidelines have been adapted from the Leeds Major Trauma Centre Imaging in Paediatric Major Trauma guidelines Written by Dr Annmarie Jeanes (Consultant Paediatric
TALK TRAUMA Clearing the C-Spine. David Ouellette
 TALK TRAUMA 2011 Clearing the C-Spine David Ouellette Case #1 - Mother / Daughter MVC 34 y/o female Dangerous mechanism CHI Mumbling incoherently Femur # - distracting injury ETOH - 22 9 y/o female Dangerous
TALK TRAUMA 2011 Clearing the C-Spine David Ouellette Case #1 - Mother / Daughter MVC 34 y/o female Dangerous mechanism CHI Mumbling incoherently Femur # - distracting injury ETOH - 22 9 y/o female Dangerous