Magnetic Resonance Atlas of Skeletal Development of the Knee
|
|
|
- Thomas Ross
- 5 years ago
- Views:
Transcription
1 Magnetic Resonance Atlas of Skeletal Development of the Knee A Standard of Reference Andrew T. Pennock, MD James D. Bomar, MPH Rady Children s Hospital, San Diego University of California, San Diego
2 2
3 Disclaimer In view of the possibility of human error or changes in medical science, neither the authors, nor the institutions warrant that the information contained in this atlas is accurate or complete, and they are not responsible for any errors or omission or the results obtained from the use of such information. 3
4 4
5 Contents Introduction Atlas creation Instructions for use Anatomic and radiographic terms Standards Female Age 1 Male Age 1 Validation References
6 6
7 History of Bone Age Assessment Proper assessment of skeletal development is essential for managing many conditions of bone and joints. Interest in this topic began nearly 100 years ago by T. Wingate Todd a Professor of Anatomy at Western Reserve University. In 1926 a series of studies in Cleveland, OH were initiated with a goal of creating radiographic standards of reference for skeletal maturation based on the hand, elbow, shoulder, hip, knee, and foot. Between 1931 and 1937, tentative developmental standards were assembled for each of these joints. Unfortunately, Introduction with the untimely death of Professor Todd, most of these series were never completed. Fortunately, William Walter Greulich and S. Idell Pyle carried on the work of Professor Todd and published the Radiographic Atlas of Skeletal Development of the Hand and Wrist in Since its publication, this reference has become the gold standard for assessing bone age and it is widely used across multiple sub-specialties including endocrinology, pediatrics, and orthopedics. Drawbacks of the Greulich and Pyle Atlas While widely used, there are limitations and drawbacks to the Greulich and Pyle Atlas: 1. It is based on a single left hand radiograph and the maturation of other joints (such as the knee) have been shown to be independent of the hand. 2. The original source films came from carefully selected patients from Cleveland, OH which were largely Caucasian with higher socioeconomic backgrounds. This selection bias has potentially limited the applicability of this data to larger and more diverse patient populations seen across many urban areas in the United States. 3. The source data is nearing 100 years old and it is unclear whether these standards still apply to children that are now entering puberty at an earlier age. 4. Obtaining an additional left hand radiograph exposes patients to additional ionizing radiation, adds additional cost to the health care system, and potentially slows clinic efficiency. 7
8 Alternative Knee Atlas In 1969, S. Idell Pyle and Normand L. Hoerr published a separate reference entitled Radiographic Atlas of Skeletal Development of the Knee. This atlas was created using an identical methodology as the Greulich and Pyle Atlas from knee radiographs that were performed between 1928 and Interestingly, this atlas is rarely referenced and has not been routinely used in the bone age assessment of patients with knee specific conditions. The reason for this in unclear, but possi- bilities include (1) the fact that subtle differences between certain age standards (especially in adolescence) can be subtle and difficult to reproducibly identify, (2) compared to the hand and wrist where there are many bones and growth plates, there are less distinguishing radiographic features about the knee to help differentiate certain ages, (3) unlike the Greulich and Pyle Atlas, the knee atlas combines the male and female standards. Bone Age using Magnetic Resonance Imaging To date, several studies within the forensic literature have evaluated the utility of knee MRIs for assessing chronological age. The rationale for these studies has been to develop better tools for assessing an accurate age of asylum seekers and resolving immigration proceedings (particularly in Europe). As such, these studies have almost ex- clusively focused on the ages of 14 to 30 years, as legal responsibility applies to individuals between the ages of 14 and 22 years in most countries. Therefore, the existing forensic literature is largely inadequate for conditions that require an accurate MRI bone age for patients under the age of 14 years. Purpose of the Current Atlas The aim of this project was to create a new atlas of knee MRIs across a spectrum of pediatric ages that would be comprehensive enough to discriminate patient bone age during the critical pre-ado- lescent and adolescent years of 11 to 18 as well as to adequately cover the earlier period from 2 to 10 years. 8
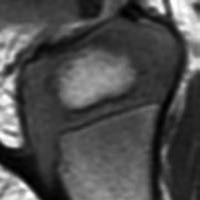
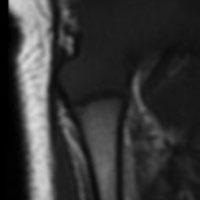
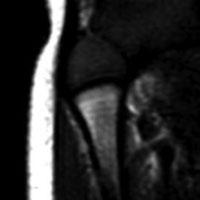
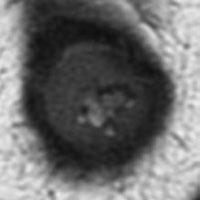
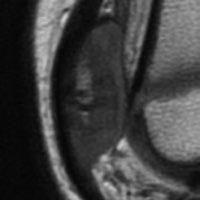
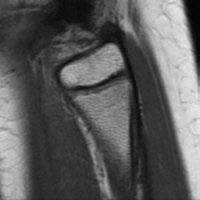
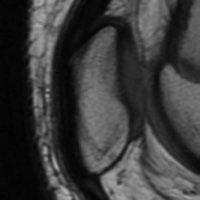
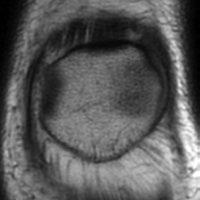
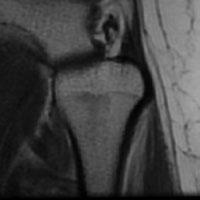
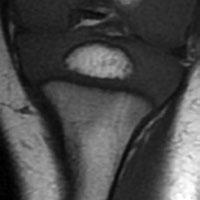
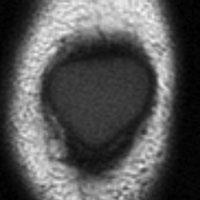
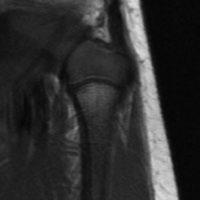
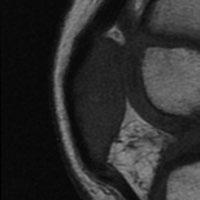
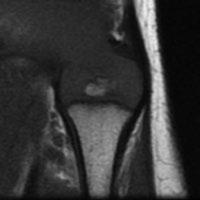
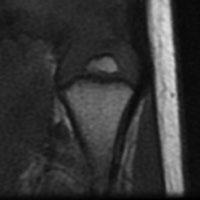
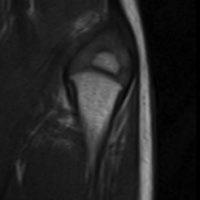
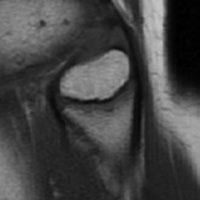
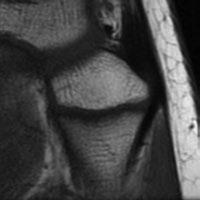
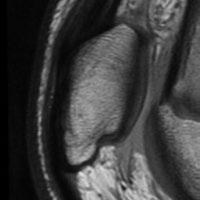
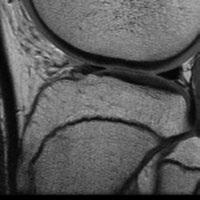
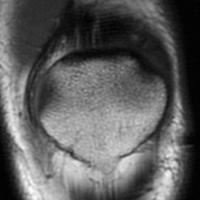
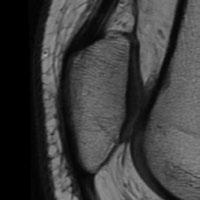
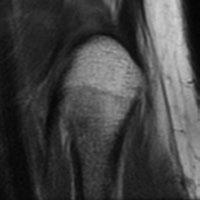
9 Selection of Skeletal Maturity Indicators Atlas Creation The knee MRI atlas was created in a similar fashion as the Greulich and Pyle Hand Atlas and the Pyle and Hoerr Knee Atlas. First, a preliminary series of skeletal maturity indicators were identified by examining knee MRIs across of a spectrum of skeletal maturity. In reviewing hundreds of MRIs, several indicators were identified and independently evaluated for each bone (femur, tibia, patella, and fibula). These features were found to be most identifiable and reproducible on the coronal T1 and sagittal T1 images. For each bone, a single standardized coronal and sagittal slice was identified. A 1.5 Tesla magnet was utilized for all MRIs in this series Slice Standardization The coronal slice through the center of the distal aspect of the femur at the attachment site of the posterior cruciate ligament on the medial femoral condyle was selected. The sagittal slice through the center of the medial femoral condyle was selected 9
, narrowing of the physis, partial closure of the physis, and complete closure of")
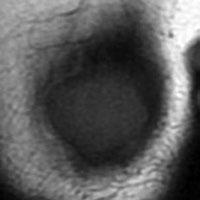
10 Specific Features The following features of the femur were identified: the presence of the epiphyseal secondary (2 ) ossification center, complete ossification of the epiphysis, disappearance of the laminated appearance of the subchondral epiphyseal cartilage (termed the Oreo sign), narrowing of the physis, partial closure of the physis, and complete closure of the physis. 10



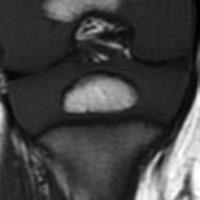
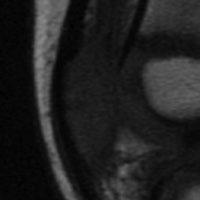
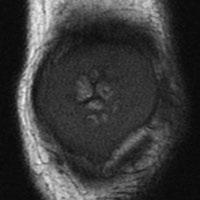
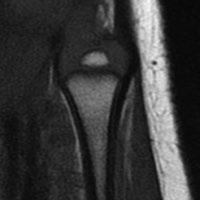
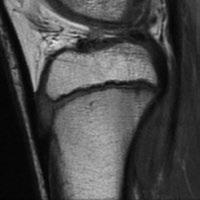
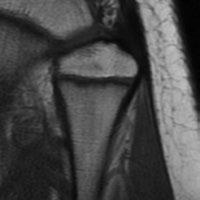
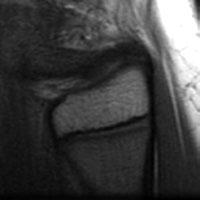
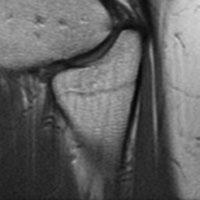
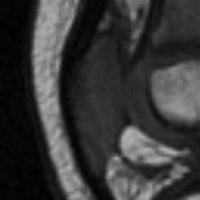
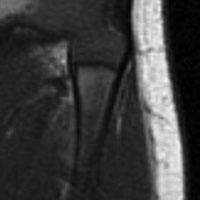
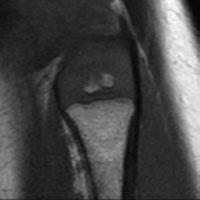
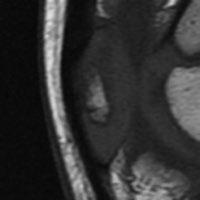
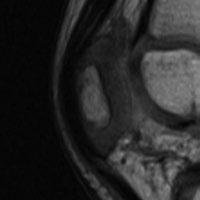
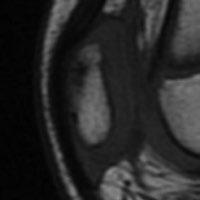
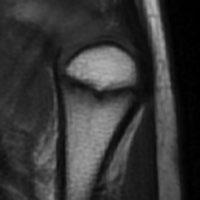
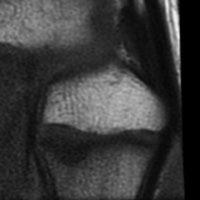
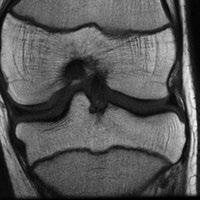
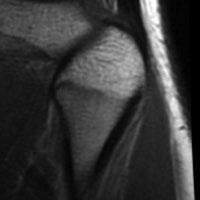
11 Slice Standardization The coronal slice at the attachment site of the ACL on the femur where the tibial spines are most pronounced should be selected. The sagittal slice through the center of the tibial tubercle should be selected 11
, complete ossification of the tibial spine, anterodistal epiphyseal ossification extension toward the tubercle apophysis, appearance of the distal tubercle apophysis")
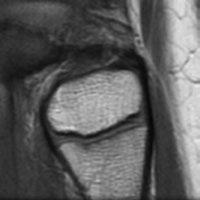
12 Specific Features The following features of the tibia were identified: the presence of the epiphyseal secondary ossification center, partial ossification of the tibial spine (which appears as a bump on the coronal image), complete ossification of the tibial spine, anterodistal epiphyseal ossification extension toward the tubercle apophysis, appearance of the distal tubercle apophysis ossification center, fusion of the tubercle apophysis ossification center with the epiphysis (just prior to fusion of the tubercle apophysis with the epiphysis, a crack can be observed during a narrow window of skeletal maturity), complete ossification of the epiphysis, narrowing of the physis, partial closure of the physis, and complete closure of the physis. 12



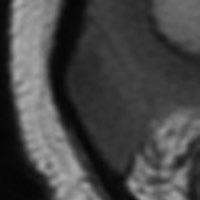
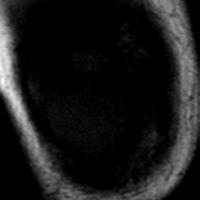
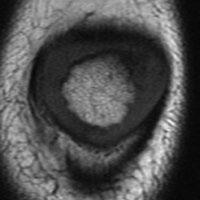
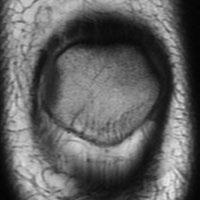
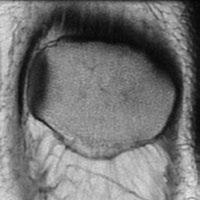
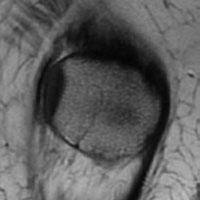
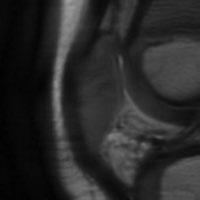
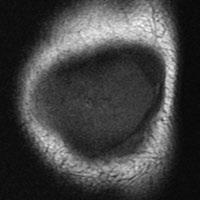
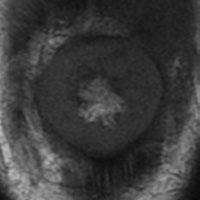
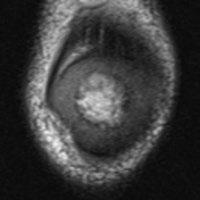
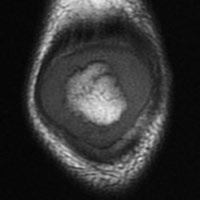
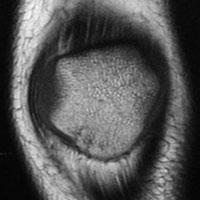
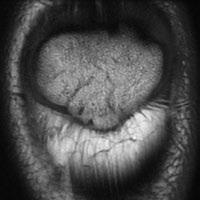
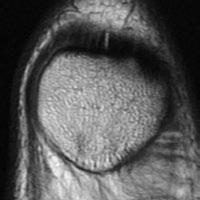
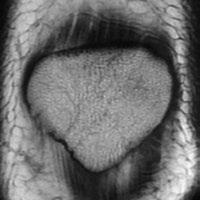
13 Slice Standardization The coronal slice was selected through the center of the patella where the patella was longest in the proximal to distal direction on the sagittal view and where the patella was widest in the medial to lateral direction on the coronal view. The sagittal slice was selected through the center of the patella where the patella was longest in the proximal to distal direction. Specific Features An ossification percentage was calculated on the basis of the amount of ossification within the patella. This calculation was performed using both the coronal and sagittal images. Patients were then grouped according to the percentage of ossification present: 0%, 1% to 24%, 25% to 49%, 50% to 74%, 75% to 99%, or 100% (complete) ossification. Of note, the last portion of the patella to ossify was its superior tip, which was best visualized on the sagittal image. 13

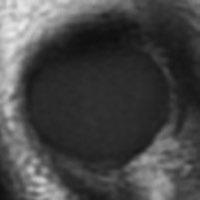
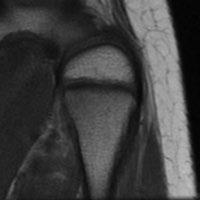
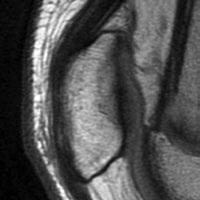
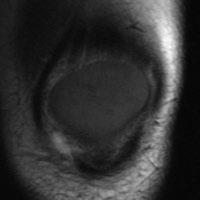
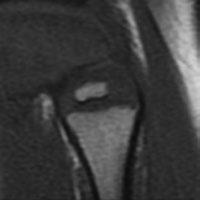
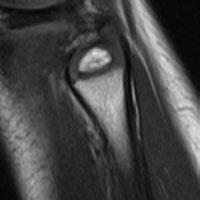
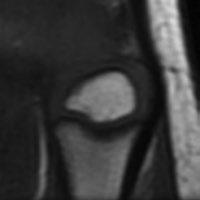
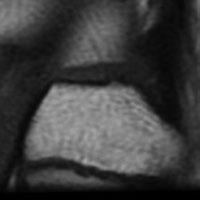
14 Slice Standardization The coronal slice through the center of the fibular styloid was selected. The sagittal slice through the center of the fibular styloid was selected Specific Features The following features of the fibula were identified: the presence of the epiphyseal secondary ossification center, complete epiphyseal ossification (other than the styloid), ossification of the fibular styloid tip, partial closure of the physis, and complete closure of the physis. Standard Reference Creation 14 To create a standard of reference for each age and each gender, we repeatedly ordered approximately 30 patients (when available) for each age and gender from least mature to most mature. The patient determined to be in the middle of the maturity spectrum was identified as the standard. The atlas standard consists of 8 images, including both coronal and sagittal images, of the femur, tibia, patella, and fibula.



15 Instructions for Use If a clinician wishes to determine the skeletal maturity of a knee MRI compared to the standard atlas, we recommend that they proceed to the age and gender standard corresponding to the chronologic age of the patient. By comparing the standardized coronal and sagittal slices from each bone of their patient to this standard as well as to the standard immediately preceding and following the selected age, one can rapidly determine whether the patient s skeletal age corresponds approximately with the age in this standard of reference. If the clinician does not know the patient s age whose MRI they wish to assess, the clinician may look through the atlas until they come to the standard that most closely resembles their patient. Similar to the Greulich and Pyle Hand atlas, the clinician will occasionally find that the MRI features of a patient resemble two successive standards. In these situations, we recommend that that clinician use all available bones (femur, tibia, patella, and fibula) and images (coronal and sagittal) to best match the patient to the standard. Proper Image Selection Slice selection for use of the atlas is performed in the identical fashion as Slice Standardization in creating the atlas, as described in pages Many of the MRI indicators or features identified in this Atlas are subtle making appropriate image selection essential for each individual bone and for each image sequence (coronal and sagittal). The following slides depict which image should be selected for each bone. Slice Selection: The coronal slice through the center of the distal aspect of the femur at the attachment site of the posterior cruciate ligament on the medial femoral condyle was selected. The sagittal slice through the center of the medial femoral condyle was selected 15
16 Slice Selection: The coronal slice at the attachment site of the ACL on the femur where the tibial spines are most pronounced should be selected. The sagittal slice through the center of the tibial tubercle should be selected Slice Selection: The coronal slice was selected through the center of the patella where the patella was widest in the medial to lateral direction. The sagittal slice was selected through the center of the patella where the patella was longest in the proximal to distal direction. 16

17 Slice Selection: The coronal slice through the center of the fibular styloid was selected. The sagittal slice through the center of the fibular styloid was selected Percent Ossification Measurement: Femoral ossification is measured on the coronal view as a percentage of the width of the entire distal femur (both the ossified and unossified portions of the bone) compared to the ossified portion. In this case, 57% of the femur is ossified (29mm/51 mm). 17
 compared to the ossified portion. In this case, 51% of the tibia is ossified (25mm/49mm).")
 compared to the ossified portion.")

18 Percent Ossification Measurement: l ossification is measured on the coronal view as a percentage of the width of the entire proximal tibia (both the ossified and unossified portions of the bone) compared to the ossified portion. In this case, 51% of the tibia is ossified (25mm/49mm). Percent Ossification Measurement: The patellar ossification is measured on the sagittal view as a percentage of the length of the entire patella (both the ossified and unossified portions of the bone) compared to the ossified portion. In this case, 73% of the patella is ossified (38mm/52 mm). Percent Ossification Measurement: r ossification is measured on the coronal view as a percentage of the width of the entire proximal fibula (both the ossified and unossified portions of the bone) compared to the ossified portion. In this case, 43% of the fibula is ossified (6mm/14mm). 18
19 Quick Reference As a quick reference, we have identified the median ages for each gender as to when specific MRI features become apparent. This table can serve as an expedited means of aging patients. 19


20 Anatomic and Radiographic Terms Several MRI indicators used in this atlas may be unfamiliar to clinicians. Additionally, some of the terms such as tibial tubercle crack and the femoral oreo sign have not been clinically used. In the following figures, we hope to clarify these important findings to make them easier to recognize and anatomically understand. Femoral Oreo Sign During a relatively narrow window of skeletal development the epiphyseal cartilage immediately adjacent to the articular cartilage has an oreo appearance. For boys this disappears at a median age of 15.6 years (range ) For girls this disappears at a median age of 13.9 years (range ) 9 year-old boy 13.5 year-old boy 15.5 year-old boy Presence of Oreo sign Presence of Oreo sign Disappearance of Oreo sign Complete Ossification of the Femoral Epiphysis Unossified cartilage that may be appreciated on coronal imaging, immediately adjacent to the medial and lateral epicondyles, is another maturity marker on the knee. 14 year-old boy For boys this cartilage completely ossifies at a median age of 14.2 years (range ) For girls this cartilage completely ossifies at a median age of 11.9 years (range ) 15 year-old boy 20 Incomplete Ossification Complete Ossification

 For girls, this occurs at a median age of 7.")
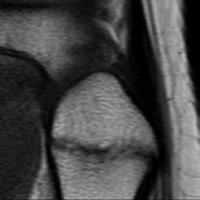
21 l Spine Bump The ossification of the tibial spines progresses through reproducible phases. Initially, no ossification is present. At a median age of 6.9 years for boys and 5.9 for girls, the initial os- sification of the spines represents a bump which then progresses to complete ossification at age 9.1 for boys and 7.1 for girls 6 year-old boy 8 year-old boy 9 year-old boy No bump present Bump present Spines present l Tubercle Epiphyseal Extension As the tubercle begins to ossify, the anterior epiphysis begins extending distal and below the level of the physis. 10 year-old boy For boys, this occurs at a median age of 10.2 years (range ) For girls, this occurs at a median age of 7.3 years (range ) 11.5 year-old boy No tubercle extension Tubercle extension 21


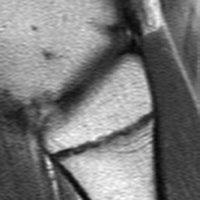
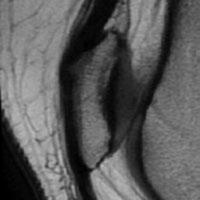
22 l Tubercle Ossification versus Crack As the tubercle apophysis appears (median age 11.8 years for boys and 10.2 years for girls), ossification can first be identified distally. The tubercle epiphyseal extension and the apophyseal ossification then merge giving the appearance of a crack which occurs in boys at a median age of 12.8 years and girls at 10.7 years 12 year-old boy 13 year-old boy 14 year-old boy Tubercle apophysis ossification Crack Complete Ossification of the l Epiphysis The last portions of the tibial epiphysis to ossify can be seen best on coronal imaging medially and sagittal imaging posteriorly. For boys this cartilage completely ossifies at a median age of 14.6 years (range ) For girls this cartilage completely ossifies at a median age of 11.9 years (range ) 14 year-old boy 15 year-old boy 14 year-old boy 15 year-old boy 22
 for boys and a median age of 11.9 years (range 9.8-12.3) for girls.")

23 Superior Tip Ossification The last portion of the patella to ossify is the patella tip which ossifies at a median age of 13.7 years (range ) for boys and a median age of 11.9 years (range ) for girls. 12 year-old boy 14 year-old boy Incomplete ossification Complete ossification r Styloid Ossification The fibular styloid is the last portion of the fibula to ossify and occurs at a median age of 15.6 years for boys and 13.3 years for girls. 14 year-old boy 16 year-old boy r styloid unossified r styloid ossified 23



24 Female Standard Age 1 Year No ossification visible through center of the medial femoral condyle on the sagittal view No ossification No epiphyseal ossification 24





25 Female Standard Age 2 Years (50-75%) (50-75%) No ossification No epiphyseal ossification 25


")




26 Female Standard Age 3 Years (75-90%) (50-75%) (0-25%) No ossification or 26


")
")

27 Female Standard Age 4 Years (75-90%) (50-75%) (25-50%) (25-75%) 27



")



28 Female Standard Age 5 Years (75-90%) (75-90%) l spine bump (50-75%) (25-75%) 28




")



29 Female Standard Age 6 Years (>90%) Oreo sign present l spine bump (>75%) Superior and inferior tips (75-95%) 29







30 Female Standard Age 7 Years (>90%) Oreo sign present (>90%) l spine ossified (Superior and inferior tips) r styloid not ossified 30








31 Female Standard Age 8 Years (Medially and laterally) Oreo sign present No apophyseal ossification l spine ossified Tubercle epiphyseal extension (Especially superior tip) Incomplete epiphyseal ossification r styloid not ossified 31






")

32 Female Standard Age 9 Years (Medially and laterally) Oreo sign present (Medially and laterally) No apophyseal ossification Tubercle epiphyseal extension (Especially superior tip) Incomplete epiphyseal ossification r styloid not ossified 32


")



33 Female Standard Age 10 Years (Especially medially) Oreo sign present (Medially and posteriorly) Apophysis ossification, but not fused (Especially superior tip) r styloid not ossified 33





34 Female Standard Age 11 Years Oreo sign present (Especially medially & posteriorly) Apophysis ossified & fused (Especially superior tip) r styloid not ossified 34





35 Female Standard Age 12 Years Oreo sign present Entire physis visible (especially medially & posteriorly) Entire physis visible r styloid not ossified Entire physis visible 35








36 Female Standard Age 13 Years Disappearance of oreo sign Entire physis visible Minimal physeal thinning Entire physis visible Minimal physeal thinning r styloid not ossified Entire physis visible Minimal physeal thinning 36




 r")

37 Female Standard Age 14 Years Entire physis visible Physis thinning (<2mm in height) Entire physis visible Physis thinning (<2mm in height) r styloid ossified Entire physis visible Physis thinning (<2mm in height) 37








38 Female Standard Age 15 Years Entire physis visible Physis thinning (<2mm in height) Partial closure of physis r styloid ossified Partial closure of physis or Entire physis visible Physis thinning (<2mm in height) 38






39 Female Standard Age 16 Years Partial closure of physis Partial or complete closure of physis Partial or complete closure of physis 39





40 Female Standard Age 17 Years Complete closure of physis Complete closure of physis Complete closure of physis 40

 No")




41 Male Standard Age 1 Year (50-75%) No ossification visible through the center of the medial femoral condyle on the sagittal view (25-50%) No ossification No epiphyseal ossification 41

")



42 Male Standard Age 2 Years (50-75%) Ossification present through the center of the medial femoral condyle on the sagittal view (50-75%) No ossification No epiphyseal ossification 42





43 Male Standard Age 3 Years (50-75%) (50-75%) No ossification No epiphyseal ossification 43


")
 44")
44 Male Standard Age 4 Years (75-90%) (50-75%) (0-25%) (<50%) 44


")
")
45 Male Standard Age 5 Years (75-90%) (50-75%) (25-50%) (25-75%) 45


")
")
46 Male Standard Age 6 Years (75-90%) (50-75%) (33-66%) (25-75%) 46



")

47 Male Standard Age 7 Years (75-90%) (75-90%) l spine bump (50-75%) (50-75%) 47



")



")
48 Male Standard Age 8 Years (>90%) Oreo sign present (75-90%) l spine bump (>75%) (Superior and inferior tips) (75-95%) 48



")



")
49 Male Standard Age 9 Years (>90%) Oreo sign present (75-90%) l spine bump (>75%) (Superior and inferior tips) (75-95%) 49






 r")

50 Male Standard Age 10 Years (>90%) Oreo sign present (>90%) Ossified tibial spines (Superior and inferior tips) r styloid not ossified 50




")

51 Male Standard Age 11 Years (>90%) Oreo sign present (Medially and laterally) No apophyseal ossification Tubercle epiphyseal extension (Superior and inferior tips) r styloid not ossified 51


")


52 Male Standard Age 12 Years (Especially medially) Oreo sign present (Especially medially and posteriorly) Apophysis ossification, but not fused (Superior tip) r styloid not ossified 52








53 Male Standard Age 13 Years (Especially medially) Oreo sign present (Especially medially and posteriorly) Apophysis ossification and fusing crack (Especially superior tip) r styloid not ossified 53





54 Male Standard Age 14 Years Oreo sign present (Especially medially and posteriorly) Apophysis ossification and fused (Especially superior tip) r styloid not ossified 54




55 Male Standard Age 15 Years Disappearance of oreo sign Entire physis visible (Especially medially and posteriorly) Entire physis visible r styloid not ossified Entire physis visible 55








56 Male Standard Age 16 Years Entire physis visible Physis thinning (<2mm in height) Partial closure of physis r styloid ossified Physis thinning (<2mm in height) or Partial closure of physis 56






57 Male Standard Age 17 Years Partial closure of physis Partial or complete closure of physis Partial or complete closure of physis 57





58 Male Standard Age 18 Years Complete closure of physis Complete closure of physis Complete closure of physis 58
59 Validation This system of assessing bone age was validated using a cohort of 323 knee MRIs. These were separate from the knee MRIs used to create the system. Two orthopedic surgeons were blinded to this cohort of subject s chronological ages while they determined bone age using this new system. Inter-observer reliability between the two surgeons was assessed using the intraclass correlation coefficient (ICC). Inter-observer reliability among our two surgeons was found to be high with an ICC of 0.957, p< The comparison of knee MRI bone ages to chronological bone age was found to be highly correlated, with Spearman s rho being 0.978, p< Left hand x-rays were available on 48 of the patients in the cohort used to validate this system. The Greulich and Pyle atlas was used to determine bone age from the wrist x-rays in this cohort. The graph to the left shows that the Greulich and Pyle bone age method and the knee MRI bone age method were similarly correlated to chronological age, with the knee MRI method having a marginally higher correlation with chronological age. Pennock A.T., Bomar J.D., Manning J.D.: The Creation and Validation of a Knee Bone Age Atlas Utilizing MRI. J Bone Joint Surg Am. 2018;100(4):e20. 59
60 References Pennock AT, Bomar JD, Manning JD. The Creation and Validation of a Knee Bone Age Atlas Utilizing MRI. J Bone Joint Surg Am. 2018;100:e20)1-10 Greulich WW, Pyle SI. Radiographic atlas of skeletal development of the hand and wrist. 2nd ed. Palo Alto: Stanford University Press; Hackman L, Black S. The reliability of the Greulich and Pyle atlas when applied to a modern Scottish population. J Forensic Sci Jan;58(1): Epub 2012 Oct 12. Roche AF, Roberts J, Hamill PV. Skeletal maturity of children 6-11 years: racial, geographic area, and socioeconomic differentials, United States. Vital Health Stat Oct;(149):1-81. Aicardi G, Vignolo M, Milani S, Naselli A, Magliano P, Garzia P. Assessment of skeletal maturity of the hand-wrist and knee: a comparison among methods. Am J Hum Biol Sep;12(5): Dedouit F, Auriol J, Rousseau H, Rougé D, Crubézy E, Telmon N. Age assessment by magnetic resonance imaging of the knee: a preliminary study. Forensic Sci Int Apr 10;217(1-3):232.e1-7. Epub 2011 Dec 5. Pyle SI, Hoerr NL. A radiographic standard of reference for the growing knee. Springfield: Charles C. Thomas; Schaefer M, Hackman L, Gallagher J. Variability in developmental timings of the knee in young American children as assessed through Pyle and Hoerr s radiographic atlas. Int J Legal Med Mar;130(2): Epub 2015 Jan 17. Krämer JA, Schmidt S, Jürgens KU, Lentschig M, Schmeling A, Vieth V. Theuse of magnetic resonance imaging to examine ossification of the proximal tibial epiphysis for forensic age estimation in living individuals. Forensic Sci Med Pathol Sep;10(3): Epub 2014 Apr
PEDIATRIC OVERUSE INJURIES. Nick Monson, DO Assistant Professor University of Utah Orthopedic Center U of U Sports Medicine Symposium
 PEDIATRIC OVERUSE INJURIES Nick Monson, DO Assistant Professor University of Utah Orthopedic Center U of U Sports Medicine Symposium MINI-ME Little adults Different injury patterns Ligaments > bones Changing
PEDIATRIC OVERUSE INJURIES Nick Monson, DO Assistant Professor University of Utah Orthopedic Center U of U Sports Medicine Symposium MINI-ME Little adults Different injury patterns Ligaments > bones Changing
PEM GUIDE CHILDHOOD FRACTURES
 PEM GUIDE CHILDHOOD FRACTURES INTRODUCTION Skeletal injuries account for 10-15% of all injuries in children; 20% of those are fractures, 3 out of 4 fractures affect the physis or growth plate. Always consider
PEM GUIDE CHILDHOOD FRACTURES INTRODUCTION Skeletal injuries account for 10-15% of all injuries in children; 20% of those are fractures, 3 out of 4 fractures affect the physis or growth plate. Always consider
Magnetic resonance imaging of the left wrist: assessment of the bone age in a sample of healthy Iraqi adolescent males
 Original Article Magnetic resonance imaging of the left wrist: assessment of the bone age in a * Mohammed Al-Hilli* Abdullateef Aliasghar** Qasim M. Shaker*** MBChB, CABMS (RAD) MBChB, DMRD, FICMS (RAD)
Original Article Magnetic resonance imaging of the left wrist: assessment of the bone age in a * Mohammed Al-Hilli* Abdullateef Aliasghar** Qasim M. Shaker*** MBChB, CABMS (RAD) MBChB, DMRD, FICMS (RAD)
BASELINE QUESTIONNAIRE (SURGEON)
") SECTION A: STUDY INFORMATION Subject ID: - - Study Visit: Baseline Site Number: Date: / / Surgeon ID: SECTION B: INITIAL SURGEON HISTORY B1. Previous Knee Surgery: Yes No Not recorded B2. Number of Previous
SECTION A: STUDY INFORMATION Subject ID: - - Study Visit: Baseline Site Number: Date: / / Surgeon ID: SECTION B: INITIAL SURGEON HISTORY B1. Previous Knee Surgery: Yes No Not recorded B2. Number of Previous
4/28/2010. Fractures. Normal Bone and Normal Ossification Bone Terms. Epiphysis Epiphyseal Plate (physis) Metaphysis
 Metaphysis") Fractures Normal Bone and Normal Ossification Bone Terms Epiphysis Epiphyseal Plate (physis) Metaphysis Diaphysis 1 Fracture Classifications A. Longitudinal B. Transverse C. Oblique D. Spiral E. Incomplete
Fractures Normal Bone and Normal Ossification Bone Terms Epiphysis Epiphyseal Plate (physis) Metaphysis Diaphysis 1 Fracture Classifications A. Longitudinal B. Transverse C. Oblique D. Spiral E. Incomplete
HOW DO WE DIAGNOSE LAMENESS IN YOUR HORSE?
 HOW DO WE DIAGNOSE LAMENESS IN YOUR HORSE? To help horse owners better understand the tools we routinely use at VetweRx to evaluate their horse s soundness, the following section of this website reviews
HOW DO WE DIAGNOSE LAMENESS IN YOUR HORSE? To help horse owners better understand the tools we routinely use at VetweRx to evaluate their horse s soundness, the following section of this website reviews
Bone Development. V. Gilsanz and O. Ratib, Hand Bone Age, DOI / _2, Springer-Verlag Berlin Heidelberg 2012
 Bone Development 2 Skeletal maturity is a measure of development incorporating the size, shape and degree of mineralization of bone to define its proximity to full maturity. The assessment of skeletal
Bone Development 2 Skeletal maturity is a measure of development incorporating the size, shape and degree of mineralization of bone to define its proximity to full maturity. The assessment of skeletal
Magnetic resonance imaging of femoral head development in roentgenographically normal patients
 Skeletal Radiol (1985) 14:159-163 Skeletal Radiology Magnetic resonance imaging of femoral head development in roentgenographically normal patients Peter J. Littrup, M.D. 1, Alex M. Aisen, M.D. 2, Ethan
Skeletal Radiol (1985) 14:159-163 Skeletal Radiology Magnetic resonance imaging of femoral head development in roentgenographically normal patients Peter J. Littrup, M.D. 1, Alex M. Aisen, M.D. 2, Ethan
Apply this knowledge into proper management strategies and referrals
 1 2 3 Lower Extremity Injuries Jason Kennedy, M.D. Disclosures I have no financial/ industry disclosures. Objectives Identify common lower extremity injury patterns in the child and adolescent Apply this
1 2 3 Lower Extremity Injuries Jason Kennedy, M.D. Disclosures I have no financial/ industry disclosures. Objectives Identify common lower extremity injury patterns in the child and adolescent Apply this
Skeletal Maturity Assessment: Calcaneal Apophyseal Ossification
 Yale University EliScholar A Digital Platform for Scholarly Publishing at Yale Yale Medicine Thesis Digital Library School of Medicine January 2015 Skeletal Maturity Assessment: Calcaneal Apophyseal Ossification
Yale University EliScholar A Digital Platform for Scholarly Publishing at Yale Yale Medicine Thesis Digital Library School of Medicine January 2015 Skeletal Maturity Assessment: Calcaneal Apophyseal Ossification
Knee Contusions and Stress Injuries. Laura W. Bancroft, M.D.
 Knee Contusions and Stress Injuries Laura W. Bancroft, M.D. Objectives Review 5 types of contusion patterns Pivot shift Dashboard Hyperextension Clip Lateral patellar dislocation Demonstrate various stress
Knee Contusions and Stress Injuries Laura W. Bancroft, M.D. Objectives Review 5 types of contusion patterns Pivot shift Dashboard Hyperextension Clip Lateral patellar dislocation Demonstrate various stress
Copyright 2003 Pearson Education, Inc. publishing as Benjamin Cummings. Dr. Nabil Khouri MD, MSc, Ph.D
 Dr. Nabil Khouri MD, MSc, Ph.D Pelvic Girdle (Hip) Organization of the Lower Limb It is divided into: The Gluteal region The thigh The knee The leg The ankle The foot The thigh and the leg have compartments
Dr. Nabil Khouri MD, MSc, Ph.D Pelvic Girdle (Hip) Organization of the Lower Limb It is divided into: The Gluteal region The thigh The knee The leg The ankle The foot The thigh and the leg have compartments
Will She Still Make the WNBA? Sports Injuries & Fractures
 Will She Still Make the WNBA? Sports Injuries & Fractures Aharon Z. Gladstein MD Pediatric Orthopaedic Surgery Pediatric Sports Medicine Sports Injuries Chronic (overuse) Acute Who can be treated in PCP
Will She Still Make the WNBA? Sports Injuries & Fractures Aharon Z. Gladstein MD Pediatric Orthopaedic Surgery Pediatric Sports Medicine Sports Injuries Chronic (overuse) Acute Who can be treated in PCP
Immature ACL Injuries and Reconstruction
 2017 Cook Children s SPORTS Symposium Immature ACL Injuries and Reconstruction Jason Kennedy, M.D. Disclosures I have no financial/ industry disclosures. Objectives Explain the importance of skeletal immaturity
2017 Cook Children s SPORTS Symposium Immature ACL Injuries and Reconstruction Jason Kennedy, M.D. Disclosures I have no financial/ industry disclosures. Objectives Explain the importance of skeletal immaturity
Pediatric Fractures. Objectives. Epiphyseal Complex. Anatomy and Physiology. Ligaments. Bony matrix
 1 Pediatric Fractures Nicholas White, MD Assistant Professor of Pediatrics Eastern Virginia Medical School Attending, Pediatric Emergency Department Children s Hospital of The King s Daughters Objectives
1 Pediatric Fractures Nicholas White, MD Assistant Professor of Pediatrics Eastern Virginia Medical School Attending, Pediatric Emergency Department Children s Hospital of The King s Daughters Objectives
Lower Extremity Alignment: Genu Varum / Valgum
 Lower Extremity Alignment: Genu Varum / Valgum Arthur B Meyers, MD Nemours Children s Hospital & Health System Associate Professor of Radiology, University of Central Florida Clinical Associate Professor
Lower Extremity Alignment: Genu Varum / Valgum Arthur B Meyers, MD Nemours Children s Hospital & Health System Associate Professor of Radiology, University of Central Florida Clinical Associate Professor
Dr.Israa H. Mohsen. Lecture 5. The vertebral column
 Anatomy Lecture 5 Dr.Israa H. Mohsen The vertebral column The vertebral column a flexible structure consisting of 33 vertebrae holds the head and torso upright, serves as an attachment point for the legs,
Anatomy Lecture 5 Dr.Israa H. Mohsen The vertebral column The vertebral column a flexible structure consisting of 33 vertebrae holds the head and torso upright, serves as an attachment point for the legs,
Chapter 7: Skeletal System: Gross Anatomy
 Chapter 7: Skeletal System: Gross Anatomy I. General Considerations A. How many bones in an average adult skeleton? B. Anatomic features of bones are based on II. Axial Skeleton A. Skull 1. Functionally
Chapter 7: Skeletal System: Gross Anatomy I. General Considerations A. How many bones in an average adult skeleton? B. Anatomic features of bones are based on II. Axial Skeleton A. Skull 1. Functionally
General Concepts. Growth Around the Knee. Topics. Evaluation
 General Concepts Knee Injuries in Skeletally Immature Athletes Zachary Stinson, M.D. Increased rate and ability of healing Higher strength of ligaments compared to growth plates Continued growth Children
General Concepts Knee Injuries in Skeletally Immature Athletes Zachary Stinson, M.D. Increased rate and ability of healing Higher strength of ligaments compared to growth plates Continued growth Children
International Journal of Orthopaedics Sciences 2017; 3(2): DOI:
: DOI:") 2017; 3(2): 806-812 ISSN: 2395-1958 IJOS 2017; 3(2): 806-812 2017 IJOS www.orthopaper.com Received: 27-02-2017 Accepted: 28-03-2017 Sakher Alssayed Mohamedahmed Alwahbany Orthopedic Surgeon & Anatomist
2017; 3(2): 806-812 ISSN: 2395-1958 IJOS 2017; 3(2): 806-812 2017 IJOS www.orthopaper.com Received: 27-02-2017 Accepted: 28-03-2017 Sakher Alssayed Mohamedahmed Alwahbany Orthopedic Surgeon & Anatomist
Focal Periphyseal Edema (FOPE) Zone on MRI of the Adolescent Knee: A Potentially Painful Manifestation of Physiologic Physeal Fusion?
 Zone on MRI of the Adolescent Knee: A Potentially Painful Manifestation of Physiologic Physeal Fusion?") Pediatric Imaging Original Research Zbojniewicz and Laor MRI of the Adolescent Knee Pediatric Imaging Original Research Andrew M. Zbojniewicz 1 Tal Laor Zbojniewicz AM, Laor T Keywords: children, knee,
Pediatric Imaging Original Research Zbojniewicz and Laor MRI of the Adolescent Knee Pediatric Imaging Original Research Andrew M. Zbojniewicz 1 Tal Laor Zbojniewicz AM, Laor T Keywords: children, knee,
Growth in the lower lim b following chem otherapy for a malignant prim ary bone tumour: a straight-line graph
 Sarcoma (1997) 1, 75± 77 O RIGINAL ARTIC LE Growth in the lower lim b following chem otherapy for a malignant prim ary bone tumour: a straight-line graph PAUL COOL, M ARK D AVIES, ROB J. GRIM ER, SIM ON
Sarcoma (1997) 1, 75± 77 O RIGINAL ARTIC LE Growth in the lower lim b following chem otherapy for a malignant prim ary bone tumour: a straight-line graph PAUL COOL, M ARK D AVIES, ROB J. GRIM ER, SIM ON
EMERGENCY PITFALLS IN ORTHOPAEDIC TRAUMA. Thierry E. Benaroch, MD, FRCS MCH Trauma Rounds February 9, 2009
 EMERGENCY PITFALLS IN ORTHOPAEDIC TRAUMA Thierry E. Benaroch, MD, FRCS MCH Trauma Rounds February 9, 2009 MORAL OF THE STORY Fracture distal radius and intact ulna W/O radius fracture will most likely
EMERGENCY PITFALLS IN ORTHOPAEDIC TRAUMA Thierry E. Benaroch, MD, FRCS MCH Trauma Rounds February 9, 2009 MORAL OF THE STORY Fracture distal radius and intact ulna W/O radius fracture will most likely
University of Dundee. Published in: International Journal of Legal Medicine. DOI: /s Publication date: 2015
 University of Dundee Variability of developmental timings of the knee in young American children as assessed through Pyle and Hoerr's radiographic atlas Schaefer, Maureen; Hackman, Sarah; Gallagher, John
University of Dundee Variability of developmental timings of the knee in young American children as assessed through Pyle and Hoerr's radiographic atlas Schaefer, Maureen; Hackman, Sarah; Gallagher, John
OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries. Differentiate when an orthopedic injury is a medical emergency
 1 2 How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency
1 2 How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency
Knee Joint Anatomy 101
 Knee Joint Anatomy 101 Bone Basics There are three bones at the knee joint femur, tibia and patella commonly referred to as the thighbone, shinbone and kneecap. The fibula is not typically associated with
Knee Joint Anatomy 101 Bone Basics There are three bones at the knee joint femur, tibia and patella commonly referred to as the thighbone, shinbone and kneecap. The fibula is not typically associated with
Osteochondritis dissecans (OCD) lesions of the knee
 lesions of the knee") Extra-articular, Intraepiphyseal Drilling for Osteochondritis Dissecans of the Knee Andrew T. Pennock, M.D., James D. Bomar, M.P.H., and Henry G. Chambers, M.D. Abstract: Symptomatic osteochondritis dissecans
Extra-articular, Intraepiphyseal Drilling for Osteochondritis Dissecans of the Knee Andrew T. Pennock, M.D., James D. Bomar, M.P.H., and Henry G. Chambers, M.D. Abstract: Symptomatic osteochondritis dissecans
Common Orthopaedic Injuries in Children
 Common Orthopaedic Injuries in Children Rakesh P. Mashru, M.D. Division of Orthopaedic Trauma Cooper University Hospital Cooper Medical School of Rowan University December 1, 2017 1 Learning Objectives
Common Orthopaedic Injuries in Children Rakesh P. Mashru, M.D. Division of Orthopaedic Trauma Cooper University Hospital Cooper Medical School of Rowan University December 1, 2017 1 Learning Objectives
Distribution of Lengths of the Normal Femur and Tibia in Korean Children from Three to Sixteen Years of Age
 J Korean Med Sci 2003; 18: 715-21 ISSN 1011-8934 Copyright The Korean Academy of Medical Sciences of Lengths of the Normal Femur and Tibia in Korean Children from Three to Sixteen Years of Age To develop
J Korean Med Sci 2003; 18: 715-21 ISSN 1011-8934 Copyright The Korean Academy of Medical Sciences of Lengths of the Normal Femur and Tibia in Korean Children from Three to Sixteen Years of Age To develop
Important Parts of Bones
 Important Parts of Bones For 2015 Know: Humerus (posterior) Clavical Femur (Anterior) Foot Hand Mandible Os Coxa Scapula Skull (Anterior, Inferior, Lateral) Sternum Humerus (posterior) A. olecranon fossa
Important Parts of Bones For 2015 Know: Humerus (posterior) Clavical Femur (Anterior) Foot Hand Mandible Os Coxa Scapula Skull (Anterior, Inferior, Lateral) Sternum Humerus (posterior) A. olecranon fossa
Practical 1 Worksheet
 Practical 1 Worksheet ANATOMICAL TERMS 1. Use the word bank to fill in the missing words. reference side stand body arms palms anatomical forward All anatomical terms have a(n) point which is called the
Practical 1 Worksheet ANATOMICAL TERMS 1. Use the word bank to fill in the missing words. reference side stand body arms palms anatomical forward All anatomical terms have a(n) point which is called the
International Society for Magnetic Resonance in Medicine (ISMRM), The 24th Annual Meeting and Exhibition, Singapore, 7-13 May 2016.
, The 24th Annual Meeting and Exhibition, Singapore, 7-13 May 2016.") Development of an Automated Shape and Textural Software Model of the Paediatric Knee for Estimation of Skeletal Age. Caron Parsons 1,2, Charles Hutchinson 1,2, Emma Helm 2, Alexander Clarke 3, Asfand Baig
Development of an Automated Shape and Textural Software Model of the Paediatric Knee for Estimation of Skeletal Age. Caron Parsons 1,2, Charles Hutchinson 1,2, Emma Helm 2, Alexander Clarke 3, Asfand Baig
Lab Exercise #04 The Skeletal System Student Performance Objectives
 Lab Exercise #04 The Skeletal System Student Performance Objectives The material that you are required to learn in this exercise can be found in either the lecture text or the supplemental materials provided
Lab Exercise #04 The Skeletal System Student Performance Objectives The material that you are required to learn in this exercise can be found in either the lecture text or the supplemental materials provided
It is formed by fusion of 3 bones: I. Ilium (superior bone). II. Pubis (antero-inferior bone). III. Ischium (postero-inferior bone).
. II. Pubis (antero-inferior bone). III. Ischium (postero-inferior bone).") It is formed by fusion of 3 bones: I. Ilium (superior bone). II. Pubis (antero-inferior bone). III. Ischium (postero-inferior bone). Pubis Acetabulum Ana (242 ) The three constituent of bones of the hip
It is formed by fusion of 3 bones: I. Ilium (superior bone). II. Pubis (antero-inferior bone). III. Ischium (postero-inferior bone). Pubis Acetabulum Ana (242 ) The three constituent of bones of the hip
On the Field Management of Pediatric Trauma
 On the Field Management of Pediatric Trauma Kyle Nagle, MD MPH University of Colorado Department of Orthopedics Children s Hospital Colorado Orthopedics Institute Disclosures I have no conflicts of interest
On the Field Management of Pediatric Trauma Kyle Nagle, MD MPH University of Colorado Department of Orthopedics Children s Hospital Colorado Orthopedics Institute Disclosures I have no conflicts of interest
CONGENITAL ABSENCE OF FEMUR AND FIBULA Report of Two Cases
 CONGENITAL ABSENCE OF FEMUR AND FIBULA Report of Two Cases Reprinted by permission of the author and publisher from Clinical Orthopaedics, Philadelphia, J.B. Lippincott Co., 1959, 15, 203-207. By ROBERT
CONGENITAL ABSENCE OF FEMUR AND FIBULA Report of Two Cases Reprinted by permission of the author and publisher from Clinical Orthopaedics, Philadelphia, J.B. Lippincott Co., 1959, 15, 203-207. By ROBERT
11/4/2018 SUBTLETIES OF LOWER EXTREMITY TRAUMA IMAGING SPEAKER DISCLOSURES
 SUBTLETIES OF LOWER EXTREMITY TRAUMA IMAGING Charles S. Resnik, M.D. Professor of Radiology University of Maryland School of Medicine Upon completion of this presentation, participants will be better able
SUBTLETIES OF LOWER EXTREMITY TRAUMA IMAGING Charles S. Resnik, M.D. Professor of Radiology University of Maryland School of Medicine Upon completion of this presentation, participants will be better able
Patellofemoral Instability Jacqueline Munch, MD April 23, 2016
 Patellofemoral Instability Jacqueline Munch, MD April 23, 2016 With many thanks to Beth Shubin Stein, MD What is the Problem??? THIS IS THE PROBLEM Patella Stability Factors contributing to stability Articular
Patellofemoral Instability Jacqueline Munch, MD April 23, 2016 With many thanks to Beth Shubin Stein, MD What is the Problem??? THIS IS THE PROBLEM Patella Stability Factors contributing to stability Articular
TRUMATCH PERSONALIZED SOLUTIONS with the SIGMA High Performance Instruments
 TRUMATCH PERSONALIZED SOLUTIONS with the SIGMA High Performance Instruments Resection Guide System SURGICAL TECHNIQUE RESECTION GUIDE SURGICAL TECHNIQUE The following steps are an addendum to the SIGMA
TRUMATCH PERSONALIZED SOLUTIONS with the SIGMA High Performance Instruments Resection Guide System SURGICAL TECHNIQUE RESECTION GUIDE SURGICAL TECHNIQUE The following steps are an addendum to the SIGMA
7/1/2012. Repetitive valgus stresses cause microfractures in the apophyseal cartilage (weak link) Common in year olds
 Common in year olds") 1 2 3 4 5 6 7 When growing pains are not growing pains David W. Gray,M.D. Medical Director Orthopedics Differential Diagnosis Fracture Ligament Injury Disloclation Cartilage Injury Apophysitis Inflammation
1 2 3 4 5 6 7 When growing pains are not growing pains David W. Gray,M.D. Medical Director Orthopedics Differential Diagnosis Fracture Ligament Injury Disloclation Cartilage Injury Apophysitis Inflammation
Case Avulsion fracture of the tibial tubercle in an adolescent
 Case 14039 Avulsion fracture of the tibial tubercle in an adolescent Charlotte Vanhoenacker 1, Kris Van Crombrugge 2, Lieven Tack 2, Filip Vanhoenacker 2, 3, 4 1: Leuven University Hospital, Department
Case 14039 Avulsion fracture of the tibial tubercle in an adolescent Charlotte Vanhoenacker 1, Kris Van Crombrugge 2, Lieven Tack 2, Filip Vanhoenacker 2, 3, 4 1: Leuven University Hospital, Department
Surgical Technique. VISIONAIRE FastPak Instruments for the LEGION Total Knee System
 Surgical Technique VISIONAIRE FastPak Instruments for the LEGION Total Knee System VISIONAIRE FastPak for LEGION Instrument Technique* Nota Bene The technique description herein is made available to the
Surgical Technique VISIONAIRE FastPak Instruments for the LEGION Total Knee System VISIONAIRE FastPak for LEGION Instrument Technique* Nota Bene The technique description herein is made available to the
Torn ACL - Anatomic Footprint ACL Reconstruction
 Torn ACL - Anatomic Footprint ACL Reconstruction The anterior cruciate ligament (ACL) is one of four ligaments that are crucial to the stability of your knee. It is a strong fibrous tissue that connects
Torn ACL - Anatomic Footprint ACL Reconstruction The anterior cruciate ligament (ACL) is one of four ligaments that are crucial to the stability of your knee. It is a strong fibrous tissue that connects
Copyright 2003 Pearson Education, Inc. publishing as Benjamin Cummings. Dr. Nabil khouri
 Dr. Nabil khouri Appendicular Skeleton The appendicular skeleton is made up of the bones of the upper and lower limbs and their girdles Two girdles: Pectoral girdles attach the upper limbs to the body
Dr. Nabil khouri Appendicular Skeleton The appendicular skeleton is made up of the bones of the upper and lower limbs and their girdles Two girdles: Pectoral girdles attach the upper limbs to the body
Current Thinking of the Osteochondroses. Diego Jaramillo, M.D., M.P.H. Department of Radiology Stanford Children s Hospital
 Current Thinking of the Osteochondroses Diego Jaramillo, M.D., M.P.H. Department of Radiology Stanford Children s Hospital What is an osteochondrosis? Abnormal endochondral ossification and epiphyseal
Current Thinking of the Osteochondroses Diego Jaramillo, M.D., M.P.H. Department of Radiology Stanford Children s Hospital What is an osteochondrosis? Abnormal endochondral ossification and epiphyseal
radiologymasterclass.co.uk
 http://radiologymasterclass.co.uk Hip X-ray anatomy - Normal AP (anterior-posterior) Shenton's line is formed by the medial edge of the femoral neck and the inferior edge of the superior pubic ramus Loss
http://radiologymasterclass.co.uk Hip X-ray anatomy - Normal AP (anterior-posterior) Shenton's line is formed by the medial edge of the femoral neck and the inferior edge of the superior pubic ramus Loss
Original Report. The Reverse Segond Fracture: Association with a Tear of the Posterior Cruciate Ligament and Medial Meniscus
 Eva M. Escobedo 1 William J. Mills 2 John. Hunter 1 Received July 10, 2001; accepted after revision October 1, 2001. 1 Department of Radiology, University of Washington Harborview Medical enter, 325 Ninth
Eva M. Escobedo 1 William J. Mills 2 John. Hunter 1 Received July 10, 2001; accepted after revision October 1, 2001. 1 Department of Radiology, University of Washington Harborview Medical enter, 325 Ninth
Mako Partial Knee Medial bicompartmental
 Mako Partial Knee Medial bicompartmental Surgical reference guide Mako Robotic-Arm Assisted Surgery Table of contents Implant compatibility.... 3 Pre-operative planning.... 4 Intra-operative planning....
Mako Partial Knee Medial bicompartmental Surgical reference guide Mako Robotic-Arm Assisted Surgery Table of contents Implant compatibility.... 3 Pre-operative planning.... 4 Intra-operative planning....
Chapter 8 The Skeletal System: The Appendicular Skeleton. Copyright 2009 John Wiley & Sons, Inc.
 Chapter 8 The Skeletal System: The Appendicular Skeleton Appendicular Skeleton It includes bones of the upper and lower limbs Girdles attach the limbs to the axial skeleton The pectoral girdle consists
Chapter 8 The Skeletal System: The Appendicular Skeleton Appendicular Skeleton It includes bones of the upper and lower limbs Girdles attach the limbs to the axial skeleton The pectoral girdle consists
Lower Extremity Fracture Management. Fractures of the Hip. Lower Extremity Fractures. Vascular Anatomy. Lower Extremity Fractures in Children
 Lower Extremity Fracture Management Brian Brighton, MD, MPH Levine Children s s Hospital Carolinas Medical Center Charlotte, NC Oscar Miller Day October 16, 2009 Lower Extremity Fractures in Children Anatomic
Lower Extremity Fracture Management Brian Brighton, MD, MPH Levine Children s s Hospital Carolinas Medical Center Charlotte, NC Oscar Miller Day October 16, 2009 Lower Extremity Fractures in Children Anatomic
THE Salter-Harris classification is a radiologic
 Advanced Emergency Nursing Journal Vol. 29, No. 1, pp. 10 19 Copyright c 2007 Wolters Kluwer Health Lippincott Williams & Wilkins Radiology R O U N D S Column Editor: Jonathan Lee Salter-Harris Fractures
Advanced Emergency Nursing Journal Vol. 29, No. 1, pp. 10 19 Copyright c 2007 Wolters Kluwer Health Lippincott Williams & Wilkins Radiology R O U N D S Column Editor: Jonathan Lee Salter-Harris Fractures
Intramedullary Tibial Preparation
 Surgical Technique Intramedullary Tibial Preparation Primary Total Knee Arthroplasty LEGION Total Knee System Intramedullary tibial preparation Contents Introduction...2 IM tibial highlights...3 Preoperative
Surgical Technique Intramedullary Tibial Preparation Primary Total Knee Arthroplasty LEGION Total Knee System Intramedullary tibial preparation Contents Introduction...2 IM tibial highlights...3 Preoperative
Common Apophyseal Problems in the Athlete
 Disclosure Common Apophyseal Problems in the Athlete Mark Halstead, MD November 19, 2009 Faculty Disclosure Information In the past 12 months, I have no relevant financial relationships with the manufacturer
Disclosure Common Apophyseal Problems in the Athlete Mark Halstead, MD November 19, 2009 Faculty Disclosure Information In the past 12 months, I have no relevant financial relationships with the manufacturer
Extramedullary Tibial Preparation
 Surgical Technique Extramedullary Tibial Preparation Primary Total Knee Arthroplasty LEGION Total Knee System Extramedullary tibial preparation Contents Introduction...2 EM tibial highlights...3 Preoperative
Surgical Technique Extramedullary Tibial Preparation Primary Total Knee Arthroplasty LEGION Total Knee System Extramedullary tibial preparation Contents Introduction...2 EM tibial highlights...3 Preoperative
FieldStrength. Achieva 3.0T enables cutting-edge applications, best-in-class MSK images
 FieldStrength Publication for the Philips MRI Community Issue 33 December 2007 Achieva 3.0T enables cutting-edge applications, best-in-class MSK images Palo Alto Medical Clinic Sports Medicine Center employs
FieldStrength Publication for the Philips MRI Community Issue 33 December 2007 Achieva 3.0T enables cutting-edge applications, best-in-class MSK images Palo Alto Medical Clinic Sports Medicine Center employs
Options in the Young ACL Deficient Knee
 BOSTON SHOULDER AND SPORTS SYMPOSIUM 2013 Thomas M. DeBerardino, MD Disclosure Information Disclosure Information: The following relationships exist: Research Support from: 1. Musculoskeletal Transplant
BOSTON SHOULDER AND SPORTS SYMPOSIUM 2013 Thomas M. DeBerardino, MD Disclosure Information Disclosure Information: The following relationships exist: Research Support from: 1. Musculoskeletal Transplant
The posterolateral corner of the knee: the normal and the pathological
 The posterolateral corner of the knee: the normal and the pathological Poster No.: P-0104 Congress: ESSR 2014 Type: Educational Poster Authors: M. Bartocci 1, C. Dell'atti 2, E. Federici 1, V. Martinelli
The posterolateral corner of the knee: the normal and the pathological Poster No.: P-0104 Congress: ESSR 2014 Type: Educational Poster Authors: M. Bartocci 1, C. Dell'atti 2, E. Federici 1, V. Martinelli
and K n e e J o i n t Is the most complicated joint in the body!!!!
 K n e e J o i n t K n e e J o i n t Is the most complicated joint in the body!!!! 1-Consists of two condylar joints between: A-The medial and lateral condyles of the femur and The condyles of the tibia
K n e e J o i n t K n e e J o i n t Is the most complicated joint in the body!!!! 1-Consists of two condylar joints between: A-The medial and lateral condyles of the femur and The condyles of the tibia
Fractures of the Ankle Region in the Skeletally Immature Patient. The Salter Classification is Worthless!!
 Fractures of the Ankle Region in the Skeletally Immature Patient. The Salter Classification is Worthless!! Kaye E Wilkins D.V.M,M.D. President's Council/Dielmann Chair in Pediatric Orthopedics Professor
Fractures of the Ankle Region in the Skeletally Immature Patient. The Salter Classification is Worthless!! Kaye E Wilkins D.V.M,M.D. President's Council/Dielmann Chair in Pediatric Orthopedics Professor
Principles of Anatomy and Physiology
 Principles of Anatomy and Physiology 14 th Edition CHAPTER 8 The Skeletal System: The Appendicular Skeleton The Appendicular Skeleton The 126 bones of the appendicular skeleton are primarily concerned
Principles of Anatomy and Physiology 14 th Edition CHAPTER 8 The Skeletal System: The Appendicular Skeleton The Appendicular Skeleton The 126 bones of the appendicular skeleton are primarily concerned
Biology 218 Human Anatomy. Adapted from Martini Human Anatomy 7th ed. Chapter 7 The Skeletal System Appendicular Division
 Adapted from Martini Human Anatomy 7th ed. Chapter 7 The Skeletal System Appendicular Division Introduction The appendicular skeleton includes: Pectoral girdle Shoulder bones Upper limbs Pelvic girdle
Adapted from Martini Human Anatomy 7th ed. Chapter 7 The Skeletal System Appendicular Division Introduction The appendicular skeleton includes: Pectoral girdle Shoulder bones Upper limbs Pelvic girdle
Imaging the musculoskeletal system. An Introduction
 Imaging the musculoskeletal system An Introduction Objectives Discuss: commonly used imaging modalities in the musculoskeletal system normal imaging anatomy in the extremities fracture description Imaging
Imaging the musculoskeletal system An Introduction Objectives Discuss: commonly used imaging modalities in the musculoskeletal system normal imaging anatomy in the extremities fracture description Imaging
RESECTION GUIDE SYSTEM. TRUMATCH Personalized Solutions Surgical Technique with ATTUNE Knee INTUITION Instruments
 RESECTION GUIDE SYSTEM TRUMATCH Personalized Solutions Surgical Technique with ATTUNE Knee INTUITION Instruments RESECTION GUIDE SURGICAL TECHNIQUE The following steps are an addendum to the ATTUNE Knee
RESECTION GUIDE SYSTEM TRUMATCH Personalized Solutions Surgical Technique with ATTUNE Knee INTUITION Instruments RESECTION GUIDE SURGICAL TECHNIQUE The following steps are an addendum to the ATTUNE Knee
11/16/2015. No disclosures or conflicts of interest relevant to the presentation
 Travis C. Burns, MD SAMMC, Ft Sam Houston, Tx Chief, Sports Medicine Advanced Concepts in Sports Medicine Nov 6 8, 2015 Las Vegascourse.com No disclosures or conflicts of interest relevant to the presentation
Travis C. Burns, MD SAMMC, Ft Sam Houston, Tx Chief, Sports Medicine Advanced Concepts in Sports Medicine Nov 6 8, 2015 Las Vegascourse.com No disclosures or conflicts of interest relevant to the presentation
MRI of the Knee: Part 4 - normal variants that may simulate disease. Mark Anderson, M.D. University of Virginia
 MRI of the Knee: Part 4 - normal variants that may simulate disease Mark Anderson, M.D. University of Virginia discuss the most common normal variants in the pediatric knee that may simulate pathology
MRI of the Knee: Part 4 - normal variants that may simulate disease Mark Anderson, M.D. University of Virginia discuss the most common normal variants in the pediatric knee that may simulate pathology
BAD RESULTS OF CONSERVATIVE TREATMENT OF ACL TEARS IN CHILDREN. Guy BELLIER PARIS France
 BAD RESULTS OF CONSERVATIVE TREATMENT OF ACL TEARS IN CHILDREN Guy BELLIER PARIS France TREATMENT OF ACL TEARS IN CHILDREN CONTROVERSIAL DIAGNOSIS clinical exam X-rays (stress) M.R.I. arthroscopy ACL TEARS
BAD RESULTS OF CONSERVATIVE TREATMENT OF ACL TEARS IN CHILDREN Guy BELLIER PARIS France TREATMENT OF ACL TEARS IN CHILDREN CONTROVERSIAL DIAGNOSIS clinical exam X-rays (stress) M.R.I. arthroscopy ACL TEARS
The Lower Limb II. Anatomy RHS 241 Lecture 3 Dr. Einas Al-Eisa
 The Lower Limb II Anatomy RHS 241 Lecture 3 Dr. Einas Al-Eisa Tibia The larger & medial bone of the leg Functions: Attachment of muscles Transfer of weight from femur to skeleton of the foot Articulations
The Lower Limb II Anatomy RHS 241 Lecture 3 Dr. Einas Al-Eisa Tibia The larger & medial bone of the leg Functions: Attachment of muscles Transfer of weight from femur to skeleton of the foot Articulations
Prevalence and location of bone spurs in anterior ankle impingement
 Prevalence and location of bone spurs in anterior ankle impingement C. E. Talbot, S. N. Miskovsky, B. M. Vidalis, L. Shaw University Hospitals Case Medical Center and Case Western Reserve University School
Prevalence and location of bone spurs in anterior ankle impingement C. E. Talbot, S. N. Miskovsky, B. M. Vidalis, L. Shaw University Hospitals Case Medical Center and Case Western Reserve University School
Bone Flashcards for 10a
 Bone Flashcards for 0a CLAVICLE (collar bone). Sternal extremity (end) flat end. Acromial extremity (end) rounded end. SCAPULA (shoulder blade). Right or left scapula?. Superior border (superior margin).
Bone Flashcards for 0a CLAVICLE (collar bone). Sternal extremity (end) flat end. Acromial extremity (end) rounded end. SCAPULA (shoulder blade). Right or left scapula?. Superior border (superior margin).
July 2011 Case of the Month. By Matt Grady, MD
 July 2011 Case of the Month By Matt Grady, MD CC: Knee Pain - Osteochondritis Dissecans or not? A Case Comparison HPI: The first patient is a 12 year old female swimmer with right knee pain. The pain started
July 2011 Case of the Month By Matt Grady, MD CC: Knee Pain - Osteochondritis Dissecans or not? A Case Comparison HPI: The first patient is a 12 year old female swimmer with right knee pain. The pain started
Figure 7: Bones of the lower limb
 BONES OF THE APPENDICULAR SKELETON The appendicular skeleton is composed of the 126 bones of the appendages and the pectoral and pelvic girdles, which attach the limbs to the axial skeleton. Although the
BONES OF THE APPENDICULAR SKELETON The appendicular skeleton is composed of the 126 bones of the appendages and the pectoral and pelvic girdles, which attach the limbs to the axial skeleton. Although the
The Knee. Clarification of Terms. Osteology of the Knee 7/28/2013. The knee consists of: The tibiofemoral joint Patellofemoral joint
 The Knee Clarification of Terms The knee consists of: The tibiofemoral joint Patellofemoral joint Mansfield, p273 Osteology of the Knee Distal Femur Proximal tibia and fibula Patella 1 Osteology of the
The Knee Clarification of Terms The knee consists of: The tibiofemoral joint Patellofemoral joint Mansfield, p273 Osteology of the Knee Distal Femur Proximal tibia and fibula Patella 1 Osteology of the
Amy Warenda Czura, Ph.D. 1 SCCC BIO130 Lab 7 Appendicular Skeleton & Articulations
 The Skeletal System II: Appendicular Skeleton and Articulations Exercises 11, 13 (begins: page 145 in 9 th and 10 th editions) Exercises 10, 11 (begins: page 147 in 11 th edition, page 149 in 12 th edition)
The Skeletal System II: Appendicular Skeleton and Articulations Exercises 11, 13 (begins: page 145 in 9 th and 10 th editions) Exercises 10, 11 (begins: page 147 in 11 th edition, page 149 in 12 th edition)
Physeal fractures in immature cats and dogs: part 1 forelimbs
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk Physeal fractures in immature cats and dogs: part 1 forelimbs Author : Lee Meakin, Sorrel Langley-Hobbs Categories : Canine,
Vet Times The website for the veterinary profession https://www.vettimes.co.uk Physeal fractures in immature cats and dogs: part 1 forelimbs Author : Lee Meakin, Sorrel Langley-Hobbs Categories : Canine,
External Acoustic Meatus. Mastoid Process. Zygomatic Process. Temporal Bone
 Bone lab review 1. Frontal Bone 2. Supra-Orbital Foramen 3. Orbit (Orbital Cavity) 4. Superior Orbital Fissure 5. Inferior Orbital Fissure 6. Zygomatic Bone 7. Infra-Orbital Foramen 8. Maxilla 9. Mandible
Bone lab review 1. Frontal Bone 2. Supra-Orbital Foramen 3. Orbit (Orbital Cavity) 4. Superior Orbital Fissure 5. Inferior Orbital Fissure 6. Zygomatic Bone 7. Infra-Orbital Foramen 8. Maxilla 9. Mandible
How to Triage Orthopaedic Care. David W. Gray, M.D.
 How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency Determine
How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency Determine
The Appendicular Skeleton
 8 The Appendicular Skeleton PowerPoint Lecture Presentations prepared by Jason LaPres Lone Star College North Harris 8-1 The Pectoral Girdle The Pectoral Girdle Also called shoulder girdle Connects the
8 The Appendicular Skeleton PowerPoint Lecture Presentations prepared by Jason LaPres Lone Star College North Harris 8-1 The Pectoral Girdle The Pectoral Girdle Also called shoulder girdle Connects the
Lab Activity 9. Appendicular Skeleton Martini Chapter 8. Portland Community College BI 231
 Lab Activity 9 Appendicular Skeleton Martini Chapter 8 Portland Community College BI 231 Appendicular Skeleton Upper & Lower extremities Shoulder Girdle Pelvic Girdle 2 Humerus 3 Humerus: Proximal End
Lab Activity 9 Appendicular Skeleton Martini Chapter 8 Portland Community College BI 231 Appendicular Skeleton Upper & Lower extremities Shoulder Girdle Pelvic Girdle 2 Humerus 3 Humerus: Proximal End
Bones of Lower Limb. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 Bones of Lower Limb Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Bones of the lower limb Hip Bone Made up of 3 bones: 1) Ilium (flat), superior in position 2) Ischium (L), postero-inferior
Bones of Lower Limb Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Bones of the lower limb Hip Bone Made up of 3 bones: 1) Ilium (flat), superior in position 2) Ischium (L), postero-inferior
Running Injuries in Children and Adolescents
 Running Injuries in Children and Adolescents Cook Children s SPORTS Symposium July 2, 2014 Running Injuries Overuse injuries Acute injuries Anatomic conditions 1 Overuse Injuries Pain that cannot be tied
Running Injuries in Children and Adolescents Cook Children s SPORTS Symposium July 2, 2014 Running Injuries Overuse injuries Acute injuries Anatomic conditions 1 Overuse Injuries Pain that cannot be tied
Exercise 11. The Appendicular Skeleton
 Exercise 11 The Appendicular Skeleton The Appendicular Skeleton The appendicular skeleton contains 126 bones. Consists of the upper and lower limbs, the pectoral girdles, and the pelvic girdles. The pectoral
Exercise 11 The Appendicular Skeleton The Appendicular Skeleton The appendicular skeleton contains 126 bones. Consists of the upper and lower limbs, the pectoral girdles, and the pelvic girdles. The pectoral
Juvenile osteochondritis dissecans (OCD) of the knee is a
 of the knee is a") ORIGINAL ARTICLE Intercondylar Notch Width as a Risk Factor for Medial Femoral Condyle Osteochondritis Dissecans in Skeletally Immature Patients Roxanne M. Chow, MD, Maurice S. Guzman, MD, and Quang Dao,
ORIGINAL ARTICLE Intercondylar Notch Width as a Risk Factor for Medial Femoral Condyle Osteochondritis Dissecans in Skeletally Immature Patients Roxanne M. Chow, MD, Maurice S. Guzman, MD, and Quang Dao,
PRE-LAB EXERCISES. Before we get started, look up the definitions of these common bone marking terms: Canal: Condyle: Facet: Fissure:
 1 PRE-LAB EXERCISES When studying the skeletal system, the bones are often sorted into two broad categories: the axial skeleton and the appendicular skeleton. This lab focuses on the appendicular skeleton,
1 PRE-LAB EXERCISES When studying the skeletal system, the bones are often sorted into two broad categories: the axial skeleton and the appendicular skeleton. This lab focuses on the appendicular skeleton,
Basic Radiographic Principles Part II
 Basic Radiographic Principles Part II Kristopher Avant, D.O. October 19 th, 2016 I have no disclosures relevant to the material presented in this discussion. Good Stuff!!! 1 Really? Really! Musculoskeletal
Basic Radiographic Principles Part II Kristopher Avant, D.O. October 19 th, 2016 I have no disclosures relevant to the material presented in this discussion. Good Stuff!!! 1 Really? Really! Musculoskeletal
Figure 3 Figure 4 Figure 5
 Figure 1 Figure 2 Begin the operation with examination under anesthesia to confirm whether there are any ligamentous instabilities in addition to the posterior cruciate ligament insufficiency. In particular
Figure 1 Figure 2 Begin the operation with examination under anesthesia to confirm whether there are any ligamentous instabilities in addition to the posterior cruciate ligament insufficiency. In particular
Extensor retinaculum avulsion anatomy ankle
 Мобильный портал WAP версия: wap.altmaster.ru Extensor retinaculum avulsion anatomy ankle Dec 26, 2017. The extensor retinaculum describes the set of. Interactive Anatomical Interface and also the extensor
Мобильный портал WAP версия: wap.altmaster.ru Extensor retinaculum avulsion anatomy ankle Dec 26, 2017. The extensor retinaculum describes the set of. Interactive Anatomical Interface and also the extensor
The Accuracy of Current Methods in Deciding the Timing of Epiphysiodesis
 The Accuracy of Current Methods in Deciding the Timing of Epiphysiodesis Soon Chul Lee MD 1, Sung Wook Seo MD 2, Kyung Sup Lim MD 2, Jong Sup Shim MD 2 Department of Orthopaedic Surgery, 1 Bundang CHA
The Accuracy of Current Methods in Deciding the Timing of Epiphysiodesis Soon Chul Lee MD 1, Sung Wook Seo MD 2, Kyung Sup Lim MD 2, Jong Sup Shim MD 2 Department of Orthopaedic Surgery, 1 Bundang CHA
Radiological Estimation of Age from Hand Bone in Sudanese Infants and Toddlers
 Open Journal of Internal Medicine, 2014, 4, 13-21 Published Online March 2014 in SciRes. http://www.scirp.org/journal/ojim http://dx.doi.org/10.4236/ojim.2014.41003 Radiological Estimation of Age from
Open Journal of Internal Medicine, 2014, 4, 13-21 Published Online March 2014 in SciRes. http://www.scirp.org/journal/ojim http://dx.doi.org/10.4236/ojim.2014.41003 Radiological Estimation of Age from
CLASSIFICATION OF JOINTS STRUCTURAL VS FUNCTIONAL
 CHAPTER 8 JOINTS CLASSIFICATION OF JOINTS STRUCTURAL VS FUNCTIONAL The most moveable type of joint is a 1) Synarthrosis 2) Amphiarthrosis 3) Diarthrosis FIBROUS JOINTS Figure 8.1 Fibrous joints. (a) Suture
CHAPTER 8 JOINTS CLASSIFICATION OF JOINTS STRUCTURAL VS FUNCTIONAL The most moveable type of joint is a 1) Synarthrosis 2) Amphiarthrosis 3) Diarthrosis FIBROUS JOINTS Figure 8.1 Fibrous joints. (a) Suture
Practical Reduction Techniques: Diaphyseal Reduction. Philip Wolinsky University of California at Davis Medical Center
 OTA Specialty Day 2016 Practical Reduction Techniques: Diaphyseal Reduction Philip Wolinsky University of California at Davis Medical Center 8:55 am 9:55 am Tips and Tricks: Practical Reduction Techniques
OTA Specialty Day 2016 Practical Reduction Techniques: Diaphyseal Reduction Philip Wolinsky University of California at Davis Medical Center 8:55 am 9:55 am Tips and Tricks: Practical Reduction Techniques
Mako Partial Knee Patellofemoral
 Mako Partial Knee Patellofemoral Mako Robotic-Arm Assisted Surgery Surgical reference guide Table of contents Implant compatibility.... 3 Pre-operative implant planning... 4 Intra-operative planning....
Mako Partial Knee Patellofemoral Mako Robotic-Arm Assisted Surgery Surgical reference guide Table of contents Implant compatibility.... 3 Pre-operative implant planning... 4 Intra-operative planning....
Anatomy & Physiology Skeletal System Worksheet
 1. Name the five functions of the skeleton. c) d) e) Anatomy & Physiology Skeletal System Worksheet 2. The term for the shaft of a bone is:. 3. The bony struts found in spongy bone are called. 4. In ossification,
1. Name the five functions of the skeleton. c) d) e) Anatomy & Physiology Skeletal System Worksheet 2. The term for the shaft of a bone is:. 3. The bony struts found in spongy bone are called. 4. In ossification,
Case Report: Knee MR Imaging of Haemarthrosis in a Case of Haemophilia A
 Clinical > Pediatric Imaging Case Report: Knee MR Imaging of Haemarthrosis in a Case of Haemophilia A M. A. Weber, J. K. Kloth University Hospital Heidelberg, Department of Diagnostic and Interventional
Clinical > Pediatric Imaging Case Report: Knee MR Imaging of Haemarthrosis in a Case of Haemophilia A M. A. Weber, J. K. Kloth University Hospital Heidelberg, Department of Diagnostic and Interventional
Human, European American, Male 13-Year- Old Partial Skeleton
 Human, European American, Male 13-Year- Old Partial Skeleton Product Number: FM-509-SET Known Information: These bones are from a 13-year-old, 5'3" and 120 lbs, European American male. This information
Human, European American, Male 13-Year- Old Partial Skeleton Product Number: FM-509-SET Known Information: These bones are from a 13-year-old, 5'3" and 120 lbs, European American male. This information
Physeal Fractures and Growth Arrest
 Physeal Fractures and Growth Arrest Raymond W. Liu, M.D. Victor M. Goldberg Master Clinician-Scientist in Orthopaedics Rainbow Babies and Children s Hospital Case Western Reserve University Outline General
Physeal Fractures and Growth Arrest Raymond W. Liu, M.D. Victor M. Goldberg Master Clinician-Scientist in Orthopaedics Rainbow Babies and Children s Hospital Case Western Reserve University Outline General
TRAINING LAB SKELETAL REMAINS: IDENTIFYING BONES NAME
 TRAINING LAB SKELETAL REMAINS: IDENTIFYING BONES NAME Background: Skeletal remains are important pieces of evidence. The flesh, muscle, and organs of a victim rapidly decompose; however, the victim s skeleton
TRAINING LAB SKELETAL REMAINS: IDENTIFYING BONES NAME Background: Skeletal remains are important pieces of evidence. The flesh, muscle, and organs of a victim rapidly decompose; however, the victim s skeleton
Riverside Community College Anatomy & Physiology 2B SPRING 2012 EXAM #1-ABC (Nervous System)
") Riverside Community College Anatomy & Physiology 2B SPRING 2012 EXAM #1-ABC (Nervous System) Name: 1) This vertebra is an example of a(n). 1) A) thoracic B) axis C) atlas D) lumbar E) sacral 1 2) W hich
Riverside Community College Anatomy & Physiology 2B SPRING 2012 EXAM #1-ABC (Nervous System) Name: 1) This vertebra is an example of a(n). 1) A) thoracic B) axis C) atlas D) lumbar E) sacral 1 2) W hich
Exercise Science Section 2: The Skeletal System
 Exercise Science Section 2: The Skeletal System An Introduction to Health and Physical Education Ted Temertzoglou Paul Challen ISBN 1-55077-132-9 Role of the Skeleton Protection Framework Attachments for
Exercise Science Section 2: The Skeletal System An Introduction to Health and Physical Education Ted Temertzoglou Paul Challen ISBN 1-55077-132-9 Role of the Skeleton Protection Framework Attachments for
42 nd Annual Symposium on Sports Medicine. Knee Injuries In The Pediatric Athlete. Disclosure
 42 nd Annual Symposium on Sports Medicine Travis Murray, MD Assistant Professor University of Texas Health Science Center San Antonio January 23, 2015 Knee Injuries In The Pediatric Athlete Disclosure
42 nd Annual Symposium on Sports Medicine Travis Murray, MD Assistant Professor University of Texas Health Science Center San Antonio January 23, 2015 Knee Injuries In The Pediatric Athlete Disclosure
Index. orthopedic.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acetabular fractures thromboembolic disease after, 341 Achilles tendon rupture ACL. See Anterior cruciate ligament (ACL) Adolescent idiopathic
Index Note: Page numbers of article titles are in boldface type. A Acetabular fractures thromboembolic disease after, 341 Achilles tendon rupture ACL. See Anterior cruciate ligament (ACL) Adolescent idiopathic