CALCIUM BALANCE. James T. McCarthy & Rajiv Kumar
|
|
|
- Joseph McCormick
- 5 years ago
- Views:
Transcription

1 CALCIUM BALANCE James T. McCarthy & Rajiv Kumar
2 CALCIUM BALANCE TOTAL BODY CALCIUM (~ 1000g in a normal 60 kg adult) - > 99% in bones - ~ 0.6% in the intracellular space - ~ 0.1% in the extracellular space mg/dl meq/l mmol/l TOTAL , Ionized Ca Complexed to anions Bound to plasma protein (albumin)
3 CHANGES WITHIN PLASMA CALCIUM FRACTIONS 1. Decrease of albumin conc. by 1g/dL => decrease of total Calcium by meq/l (0.7 1 mg/dl) 2. Alkaline ph=> ionized Ca ++ is bound to HCO 3 and Albumin => reduced ionized Ca Hyponatremia increases Ca ++ binding to albumin; hypernatremia has opposite effect

4 CALCIUM BALANCE
5 CALCIUM ABSORPTION FROM GI TRACT % of normal Calcium intake is absorbed 2. Most of absorption occurs in the duodenum, jejunum, ileum 3. Mechanisms: - passive and facilitated diffusion (50-70%) - active transport ( about 30%) 4. Daily intestinal Calcium secretion: about 200 meq/day 5. Calcium absorption is completed within about 4hours after intake 6. Dietary Calcium intake < 400 mg/day => Calcium deficit 7. Calcium absorption decreases with age

6 CALCIUM ABSORPTION FROM GI TRACT
7 7-dehydrocholesterol SKIN Vitamin D3 25-hydroxy-Vitamin D3 LIVER 1,25-hydroxy-Vitamin D3 24,25-hydroxy-Vitamin D3 KIDNEY -PTH -Hypocalcemia -Hypophosphatemia -Hypercalcemia -Hyperphosphatemia
8 RENAL CALCIUM EXCRETION meq/day Filtrable calcium ( ionized + complexed) 97-98% of the filtered calcium is absorbed about 65% in proximal tubules about 15-25% in the thick ascending loop of Henle about 5 15% in the distal convoluted tubule
9 RENAL CALCIUM REABSORPTION PROXIMAL TUBULES Passive transport (depends on ECF volume) - following sodium & water absorption - following chloride reabsorption Active transport (small amount) - calcium enters the cell via calcium channel - transport depends on concentration gradient - calcium leaves the cell - 3Na + /Ca ++ antiport - Ca ++ ATPase
10 RENAL CALCIUM REABSORPTION THICK ASCENDING LOOP OF HENLE - paracellular reabsorption - depends on lumen-positive potential difference - reabsorption proportional to sodium transport - stimulated by PTH - blocked by loop diuretics DISTAL CONVOLUTED TUBULE - transcellular transport - calcium enters the cells due to concentration gradient - calcium leaves the cells via 3Na + /Ca ++ antiport - reabsorption inversely proportional to sodium transport - stimulated by thiazide diuretics - stimulated by PTH - stimulated by vitamin D3
11 CALCIUM SENSING RECEPTORS Parathyroid gland: high Ca ++ => low PTH release Thyroid gland: high Ca ++ => high calcitonin release Proximal tubules: high Ca ++ => inhibition of 1α-hydroxylase Proximal tubules: high Ca ++ => blocks PTH effect on phosphate reabsorption Proximal tubules: high Ca ++ => inhibition of Na-K-ATPase Thick ascending loop of Henle: high Ca ++ => inhibits Na-K-2Cl transport
12 CALCIUM SENSING RECEPTORS PATHOLOGY 1. Loss of function mutation-> Familial Hypocalciuric Hypercalcemia - autosomal dominant syndrome - hyperparathyroidism - hypercalcemia - low urinary calcium excretion 2. Gain of function mutation - autosomal dominant - hypocalcemia - hypoparathyroidism - high urinary calcium excretion - nephrocalcinosis - nephrolithiasis - progressive renal failure Calcimimetics agents increaseing sensitivity of calcium-sensing receptors Calcilytics agents inactivating calcium-sensing receptors
13 HYPOCALCEMIA TOTAL CALCIUM < 4.25 meq/l 1. Impaired calcium absorption 2. Increased calcium sequestration 3. Decreased PTH secretion 4. Decreased PTH action
14 IMPAIRED CALCIUM ABSORPTION Aging (ie. decreased number of receptors for vitamin D 3 ) Malabsorption - intestinal pathology (celiac disease,resection of intestines) - unabsorbed fatty acids => Fatty acids Calcium salts - lack of vitamin D 3 - hyperthyroidism => increased calcium release from bones => hypercalcemia=> low PTH => low vit D 3 - Anticonvulsant drugs (lack of vit.d hydroxylation in liver) - Glucocorticoids - Mg deficiency (impaired PTH secretion, intestinal resistance to vit.d 3 )
15 INCREASED CALCIUM SEQUESTRATION Hyperphosphatemia - when Ca x Phosphate conc. (mg/dl) product > 60 => deposition of calcium salts Calcium chelation (citrates) Soft tissue deposition - fat tissue necrosis =>precipitation of Calcium salts (acute pancreatitis) Bone deposition - hungry bone syndrome rebuilding of bones after normalization of hyperparathyroidism - osteoblastic metastases of prostate, lung cancer
16 DECREASED PTH SECRETION/OR ACTION 1. Resistance to PTH action - vitamin D deficiency: impaired absorption, hydroxylation in the liver (anticonvulsant dugs),hydroxylation in kidneys (renal failure, Fanconi syndrome) 2. Magnesium deficiency => impaired PTH release and action on bones 3. Pseudohypoparathyroidism ( abnormal function of PTH receptors) 4. Removal of parathyroid gland
17 HYPOCALCEMIA - SYMPTOMS 1. Neuromuscular - enhances neuromuscular excitability - paresthesias - hyperreflexia 2. Cardiovascular - arrhytmias - atrial fibrillation - prolonged QT interval - hypotension 3. Bones - fractures - deformations - pain 4. Connective tissue - dry skin, coarse - hair loss - brittle nails - cataract - dental abnormalities
18

19 James T. McCarthy & Rajiv Kumar
20 HYPOCALCEMIA Calcium Phos Vit D 3 PTH phates Hypoparathyroidism LOW HIGH LOW LOW Pseudohypoparathyroidism LOW HIGH LOW HIGH Vitamin D 3 deficiency LOW LOW LOW HIGH Resistance to LOW LOW HIGH HIGH vitamin D 3 Renal Failure LOW HIGH LOW HIGH
21 HYPOCALCEMIA? Serum phosphate <3.5mg/dL >3.5 mg/dl? Renal function Decreased Normal CRF Low? PTH Normal/High Low? Magnesium Normal Pseudohypoparathyroidism Hypoparathyroidism due to hypomagnesemia Primary Hypoparathyroidism Secondary hypoparathyroidism
22 HYPOCALCEMIA? Serum phosphate <3.5mg/dL >3.5 mg/dl? FECa High Normal Renal loss? 1,25(OH) 2 D 3 Low High Vitamin D-Dependent Rickets Type I VitaminD-Dependent Rickets Type II
23 HYPERCALCEMIA TOTAL Calcium > 5.25 meq/l 1. Primary increase in calcium absorption - vitamin D intoxication - granulomatous diseases (ie. Sarcoidosis, tuberculosis) 2. Increased Ca mobilization from bones A. Primary Hyperparathyroidism - parathyroid gland adenoma (80%) - hyperplasia of four glands - parathyroid carcinoma (1%) B. Non-PTH mediated hypercalcemia - hyperthyroidism => stimulation of osteoclasts - release of PTH-related peptide from tumor cells (squamous and oat cell bronchogenic carcinoma, breast cancer, multiple myeloma)
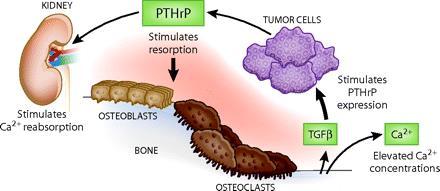
24 PTH-Related Peptide

25 James T. McCarthy & Rajiv Kumar
26 HYPERCALCEMIA Calcium Phos Vit D 3 PTH phates HYPERPARATHYROIDISM HIGH LOW HIGH HIGH PTH-related peptide HIGH LOW NORMAL /LOW LOW Vitamin D 3 excess HIGH HIGH HIGH LOW
27 HYPERCALCEMIA PTH-Mediated Non-PTH-Mediated Phosphate Low Low/Normal/High Chloride High Normal Metabolic Acidosis Mild Not present Chloride/ >33 <33 Phosphate PTH High Low
28 HYPERCALCEMIA - SYMPTOMS 1. Neuromuscular - diminished deep tendon reflexes - muscle weakness - depression, lethargy 2. Cardiovascular - positive inotropic effect - hypertension - arrhytmias - shortenning of the QT interval 3. Gastrointestinal - peptic ulcer - pancreatitis 4. Renal - decreased sensitivity to ADH => nephrogenic diabetes insipidus - hypercalciuria => nephrolithiasis - tubulointerstitial nephropathy => distal RTA 5. Bones - hyperparathysoidism => osteitis fibrosa cystica - anemia
29
30 PHOSPHATE HOMEOSTASIS Phosphorous in the body (10g/1 kg bw) 85% in bones 14% in the intracellular space 1% in the extracellular space - organic 70% - inorganic 30% Plasma inorganic phosphorous ( mg/dl) 85% free (HPO 4-2 /H 2 PO 4- = 4:1) 15% bound to albumin or complexed with calcium or magnesium Phosphorous distribution : ICF/ECF 1. pco2 Low pco2 => respiratory alkalosis=> activation of anaerobic glycolysis => phosphorous enters the cells 2. Glucose Glucose uptake into the cells=> activation of glycolysis => phosphorylated intermediates => phosphorous enters the cells
31 Moshe Levi & Mordecai Popovtzer
32 PHOSPHATE RENAL EXCRETION 1. About 80% of the filtered phosphorous is reabsorbed - 75% in proximal tubules - 5% in the thick ascending loop of Henle and distal convoluted tubules REGULATION OF PHOSPHATE REABSORPTION STIMULATION Phosphate depletion INHIBITION Phosphate loading Vitamin D 3 Volume contraction Growth hormone Insulin Thyroid hormones PTH and PTH-related peptide Volume expansion Hypercalcemia Hypercapnia Phosphatonins (Fibroblast Growth Factor 23,Fibroblast Growth Factor 7
33 PHOSPHATONINS - peptides causing phosphaturia - Fibroblast Growth Factor-23 (FGF-23) - secreted Frizzeld Related Protein-4 (sfrp-4) - Matrix Extracelular Phosphoglycoprotein - Fibfrobalst Growth factor-7 (FGF-7) - inhibit Na-Phosphate cotransport in renal epithelial cells - inhibit 1-α-hydroxylase - produced by mesenchymal tumor cells (Tumor Induced Osteomalacia) - produced in genetically determined rickets - X-linked hypophosphatemic rickets - Autosomal dominant hypophosphatemic rickets
34 High Serum Phosphate Low serum Ca ++ High serum PTH Increased Renal Phosphate excretion Low Renal Vit D3 synthesis Low Instestinal & Renal Phosphate absorption Normal Serum Phosphate
35 Low Serum Phosphate High serum Ca ++ Low serum PTH Decreased Renal Phosphate excretion High Renal Vit D3 synthesis High Instestinal & Renal Phosphate absorption Normal Serum Phosphate
36 HYPOPHOSPHATEMIA 1. Internal redistribution - increased insulin - refeeding - respiratory alkalosis - hungry bone syndrome 2. Decreased intestinal absorption - inadequate intake (vitamin D 3 deficiency) - antiacids containing aluminium or magnesium - diarrhea 3. Increased urinary excretion - hyperparathyroidism - vitamin D3 deficiency - Fanconi syndrome - volume expansion - proximal diuretics/osmotic diuresis
37 HYPOPHOSPHATEMIA SYSTEMIC DISORDERS 1. Central Nervous System - irritability, paresthesias,confusion, coma 2. Cardiovascular System - impaired cardiac contractility 3. Skeletal & Smooth Muscles - myopathy, decreased contractility, rhabdomyolysis 4. Blood - hemolysis, impaired leukocytes phagocytosis and chemotaxis, thrombocytopenia, defective clot retraction 5. Bone - increased bone resorption, rickets, osteomalacia 6. Kidney - decreased GFR, decreased bicarbonates reabsorption, hypercalciuria
38 HYPERPHOSPHATEMIA 1. Increased phsophorous absorption - phosphorous rich diet - vitamin D 3 intoxication 2. Increased endogenous load - cells necrosis - acidosis 3. Reduced urinary excretion - renal failure - hypoparathyroidism Hyperphosphatemia => low ionized Ca => high PTH and vitamin D 3 - neuromuscular irritability - tetany - hypotension - precipitation of Calcium-Phosphate => vascular calcification, conduction abnormalieties, pruritus
Major intra and extracellular ions Lec: 1
 Major intra and extracellular ions Lec: 1 The body fluids are solutions of inorganic and organic solutes. The concentration balance of the various components is maintained in order for the cell and tissue
Major intra and extracellular ions Lec: 1 The body fluids are solutions of inorganic and organic solutes. The concentration balance of the various components is maintained in order for the cell and tissue
Chapter 19 The Urinary System Fluid and Electrolyte Balance
 Chapter 19 The Urinary System Fluid and Electrolyte Balance Chapter Outline The Concept of Balance Water Balance Sodium Balance Potassium Balance Calcium Balance Interactions between Fluid and Electrolyte
Chapter 19 The Urinary System Fluid and Electrolyte Balance Chapter Outline The Concept of Balance Water Balance Sodium Balance Potassium Balance Calcium Balance Interactions between Fluid and Electrolyte
Hypocalcemia 6/8/12. Normal value. Physiologic functions. Nephron a functional unit of kidney. Influencing factors in Calcium and Phosphate Balance
 Normal value Hypocalcemia Serum calcium Total mg/dl Ionized mg/dl Cord blood 9.0 ~ 11.5 5.0 ~ 6.o New born (1 st 24 hrs) 9.0 ~ 10.6 4.3 ~ 5.1 24~ 48 hrs 7.0 ~12.0 4.0 ~4.7 Child 8.8 ~10.8 4.8 ~4.92 There
Normal value Hypocalcemia Serum calcium Total mg/dl Ionized mg/dl Cord blood 9.0 ~ 11.5 5.0 ~ 6.o New born (1 st 24 hrs) 9.0 ~ 10.6 4.3 ~ 5.1 24~ 48 hrs 7.0 ~12.0 4.0 ~4.7 Child 8.8 ~10.8 4.8 ~4.92 There
5/18/2017. Specific Electrolytes. Sodium. Sodium. Sodium. Sodium. Sodium
 Specific Electrolytes Hyponatremia Hypervolemic Replacing water (not electrolytes) after perspiration Freshwater near-drowning Syndrome of Inappropriate ADH Secretion (SIADH) Hypovolemic GI disease (decreased
Specific Electrolytes Hyponatremia Hypervolemic Replacing water (not electrolytes) after perspiration Freshwater near-drowning Syndrome of Inappropriate ADH Secretion (SIADH) Hypovolemic GI disease (decreased
WATER, SODIUM AND POTASSIUM
 WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance
 Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Instrumental determination of electrolytes in urine. Amal Alamri
 Instrumental determination of electrolytes in urine Amal Alamri What is the Electrolytes? Electrolytes are positively and negatively chargedions, Found in Within body's cells extracellular fluids, including
Instrumental determination of electrolytes in urine Amal Alamri What is the Electrolytes? Electrolytes are positively and negatively chargedions, Found in Within body's cells extracellular fluids, including
H 2 O, Electrolytes and Acid-Base Balance
 H 2 O, Electrolytes and Acid-Base Balance Body Fluids Intracellular Fluid Compartment All fluid inside the cells 40% of body weight Extracellular Fluid Compartment All fluid outside of cells 20% of body
H 2 O, Electrolytes and Acid-Base Balance Body Fluids Intracellular Fluid Compartment All fluid inside the cells 40% of body weight Extracellular Fluid Compartment All fluid outside of cells 20% of body
Investigations for Disorders of Calcium, Phosphate and Magnesium Homeostasis
 Investigations for Disorders of Calcium, Phosphate and Magnesium Homeostasis Tutorial for Specialist Portfolio Biomedical Scientists 03/02/2014 Dr Petros Kampanis Clinical Scientist 1. Calcium Most abundant
Investigations for Disorders of Calcium, Phosphate and Magnesium Homeostasis Tutorial for Specialist Portfolio Biomedical Scientists 03/02/2014 Dr Petros Kampanis Clinical Scientist 1. Calcium Most abundant
Calcium metabolism and the Parathyroid Glands. Calcium, osteoclasts and osteoblasts-essential to understand the function of parathyroid glands
 Calcium metabolism and the Parathyroid Glands Calcium, osteoclasts and osteoblasts-essential to understand the function of parathyroid glands Calcium is an essential element for contraction of voluntary/smooth
Calcium metabolism and the Parathyroid Glands Calcium, osteoclasts and osteoblasts-essential to understand the function of parathyroid glands Calcium is an essential element for contraction of voluntary/smooth
HYPERCALCEMIA. Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences
 HYPERCALCEMIA Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ESSENTIALS OF DIAGNOSIS Serum calcium level > 10.5 mg/dl Serum ionized
HYPERCALCEMIA Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ESSENTIALS OF DIAGNOSIS Serum calcium level > 10.5 mg/dl Serum ionized
Potassium regulation. -Kidney is a major regulator for potassium Homeostasis.
 Potassium regulation. -Kidney is a major regulator for potassium Homeostasis. Normal potassium intake, distribution, and output from the body. Effects of severe hyperkalemia Partial depolarization of cell
Potassium regulation. -Kidney is a major regulator for potassium Homeostasis. Normal potassium intake, distribution, and output from the body. Effects of severe hyperkalemia Partial depolarization of cell
NORMAL POTASSIUM DISTRIBUTION AND BALANCE
 NORMAL POTASSIUM DISTRIBUTION AND BALANCE 98% of body potassium is contained within cells, principally muscle cells, and is readily exchangeable. Only 2% is in ECF. Daily intake exceeds the amount in ECF.
NORMAL POTASSIUM DISTRIBUTION AND BALANCE 98% of body potassium is contained within cells, principally muscle cells, and is readily exchangeable. Only 2% is in ECF. Daily intake exceeds the amount in ECF.
The Parathyroid Glands
 The Parathyroid Glands Bởi: OpenStaxCollege The parathyroid glands are tiny, round structures usually found embedded in the posterior surface of the thyroid gland ([link]). A thick connective tissue capsule
The Parathyroid Glands Bởi: OpenStaxCollege The parathyroid glands are tiny, round structures usually found embedded in the posterior surface of the thyroid gland ([link]). A thick connective tissue capsule
Acid-Base Balance 11/18/2011. Regulation of Potassium Balance. Regulation of Potassium Balance. Regulatory Site: Cortical Collecting Ducts.
 Influence of Other Hormones on Sodium Balance Acid-Base Balance Estrogens: Enhance NaCl reabsorption by renal tubules May cause water retention during menstrual cycles Are responsible for edema during
Influence of Other Hormones on Sodium Balance Acid-Base Balance Estrogens: Enhance NaCl reabsorption by renal tubules May cause water retention during menstrual cycles Are responsible for edema during
Calcium and Parathyroid Disorders
 Calcium and Parathyroid Disorders Hussain Mahmud, MD Clinical Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism University of Pittsburgh Butler Memorial Hospital November
Calcium and Parathyroid Disorders Hussain Mahmud, MD Clinical Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism University of Pittsburgh Butler Memorial Hospital November
David Bruyette, DVM, DACVIM
 VCAwestlaspecialty.com David Bruyette, DVM, DACVIM Disorders of calcium metabolism are common endocrine disorders in both dogs and cats. In this article we present a logical diagnostic approach to patients
VCAwestlaspecialty.com David Bruyette, DVM, DACVIM Disorders of calcium metabolism are common endocrine disorders in both dogs and cats. In this article we present a logical diagnostic approach to patients
ACID-BASE BALANCE URINE BLOOD AIR
 ACIDBASE BALANCE URINE BLOOD AIR H 2 PO 4 NH 4 HCO 3 KIDNEY H H HCO 3 CELLS Hb H LUNG H 2 CO 3 HHb CO 2 H 2 O ph = 7.4 [HCO 3 ] = 24 meq/l PCO 2 = 40 mm Hg CO 2 PRIMARY RENAL MECHANISMS INVOLVED IN ACIDBASE
ACIDBASE BALANCE URINE BLOOD AIR H 2 PO 4 NH 4 HCO 3 KIDNEY H H HCO 3 CELLS Hb H LUNG H 2 CO 3 HHb CO 2 H 2 O ph = 7.4 [HCO 3 ] = 24 meq/l PCO 2 = 40 mm Hg CO 2 PRIMARY RENAL MECHANISMS INVOLVED IN ACIDBASE
BUFFERING OF HYDROGEN LOAD
 BUFFERING OF HYDROGEN LOAD 1. Extracellular space minutes 2. Intracellular space minutes to hours 3. Respiratory compensation 6 to 12 hours 4. Renal compensation hours, up to 2-3 days RENAL HYDROGEN SECRETION
BUFFERING OF HYDROGEN LOAD 1. Extracellular space minutes 2. Intracellular space minutes to hours 3. Respiratory compensation 6 to 12 hours 4. Renal compensation hours, up to 2-3 days RENAL HYDROGEN SECRETION
1/3/2008. Karen Burke Priscilla LeMone Elaine Mohn-Brown. Medical-Surgical Nursing Care, 2e Karen Burke, Priscilla LeMone, and Elaine Mohn-Brown
 Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 7 Caring for Clients with Altered Fluid, Electrolyte, or Acid-Base Balance Water Primary component of
Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 7 Caring for Clients with Altered Fluid, Electrolyte, or Acid-Base Balance Water Primary component of
CCRN Review - Renal. CCRN Review - Renal 10/16/2014. CCRN Review Renal. Sodium Critical Value < 120 meq/l > 160 meq/l
 CCRN Review Renal Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Sodium 136-145 Critical Value < 120 meq/l > 160 meq/l Sodium Etiology
CCRN Review Renal Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Sodium 136-145 Critical Value < 120 meq/l > 160 meq/l Sodium Etiology
OMICS Journals are welcoming Submissions
 OMICS Journals are welcoming Submissions OMICS International welcomes submissions that are original and technically so as to serve both the developing world and developed countries in the best possible
OMICS Journals are welcoming Submissions OMICS International welcomes submissions that are original and technically so as to serve both the developing world and developed countries in the best possible
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES
 Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Chapter 27: WATER, ELECTROLYTES, AND ACID-BASE BALANCE
 Chapter 27: WATER, ELECTROLYTES, AND ACID-BASE BALANCE I. RELATED TOPICS Integumentary system Cerebrospinal fluid Aqueous humor Digestive juices Feces Capillary dynamics Lymph circulation Edema Osmosis
Chapter 27: WATER, ELECTROLYTES, AND ACID-BASE BALANCE I. RELATED TOPICS Integumentary system Cerebrospinal fluid Aqueous humor Digestive juices Feces Capillary dynamics Lymph circulation Edema Osmosis
Agents that Affect Bone & Mineral Homeostasis
 Agents that Affect Bone & Mineral Homeostasis 1 Agents that Affect Bone & Mineral Homeostasis Calcium and phosphate are the major mineral constituents of bone. They are also two of the most important minerals
Agents that Affect Bone & Mineral Homeostasis 1 Agents that Affect Bone & Mineral Homeostasis Calcium and phosphate are the major mineral constituents of bone. They are also two of the most important minerals
Renal Control of Calcium, Phosphate, and Magnesium Homeostasis
 Renal Physiology Renal Control of Calcium, Phosphate, and Magnesium Homeostasis Judith Blaine, Michel Chonchol, and Moshe Levi Abstract Calcium, phosphate, and magnesium are multivalent cations that are
Renal Physiology Renal Control of Calcium, Phosphate, and Magnesium Homeostasis Judith Blaine, Michel Chonchol, and Moshe Levi Abstract Calcium, phosphate, and magnesium are multivalent cations that are
REGULATION OF CALCIUM AND PHOSPHATE HOMEOSTASIS
 REGULATION OF CALCIUM AND PHOSPHATE HOMEOSTASIS Linda S. Costanzo Virginia Commonwealth University, Medical College of Virginia, Richmond, Virginia 23298 Teaching Ca 2 and phosphate homeostasis in a physiology
REGULATION OF CALCIUM AND PHOSPHATE HOMEOSTASIS Linda S. Costanzo Virginia Commonwealth University, Medical College of Virginia, Richmond, Virginia 23298 Teaching Ca 2 and phosphate homeostasis in a physiology
Serum Inorganic Phosphorus
 198 Serum Inorganic Phosphorus VINOD K. BANSAL Definition Phosphorus is an abundant element that is widespread in its distribution. It is a major intracellular anion in mammals. Total body phosphorus in
198 Serum Inorganic Phosphorus VINOD K. BANSAL Definition Phosphorus is an abundant element that is widespread in its distribution. It is a major intracellular anion in mammals. Total body phosphorus in
CHAPTER 27 LECTURE OUTLINE
 CHAPTER 27 LECTURE OUTLINE I. INTRODUCTION A. Body fluid refers to body water and its dissolved substances. B. Regulatory mechanisms insure homeostasis of body fluids since their malfunction may seriously
CHAPTER 27 LECTURE OUTLINE I. INTRODUCTION A. Body fluid refers to body water and its dissolved substances. B. Regulatory mechanisms insure homeostasis of body fluids since their malfunction may seriously
Parathyoid glands and PTH
 Parathyoid glands and PTH They are four glands located behind the thyroid gland, each one from (20-50) mg in weight, and composed of two types of cells: 1. Cheif cells: that produces PTH. 2-oxyphil cells:
Parathyoid glands and PTH They are four glands located behind the thyroid gland, each one from (20-50) mg in weight, and composed of two types of cells: 1. Cheif cells: that produces PTH. 2-oxyphil cells:
Endocrine Regulation of Calcium and Phosphate Metabolism
 Endocrine Regulation of Calcium and Phosphate Metabolism Huiping Wang ( 王会平 ), PhD Department of Physiology Rm C516, Block C, Research Building, School of Medicine Tel: 88208252 Email: wanghuiping@zju.edu.cn
Endocrine Regulation of Calcium and Phosphate Metabolism Huiping Wang ( 王会平 ), PhD Department of Physiology Rm C516, Block C, Research Building, School of Medicine Tel: 88208252 Email: wanghuiping@zju.edu.cn
Water, Electrolytes, and Acid-Base Balance
 Chapter 27 Water, Electrolytes, and Acid-Base Balance 1 Body Fluids Intracellular fluid compartment All fluids inside cells of body About 40% of total body weight Extracellular fluid compartment All fluids
Chapter 27 Water, Electrolytes, and Acid-Base Balance 1 Body Fluids Intracellular fluid compartment All fluids inside cells of body About 40% of total body weight Extracellular fluid compartment All fluids
Kidneys in regulation of homeostasis
 Kidneys in regulation of homeostasis Assoc. Prof. MUDr. Markéta Bébarová, Ph.D. Department of Physiology Faculty of Medicine, Masaryk University This presentation includes only the most important terms
Kidneys in regulation of homeostasis Assoc. Prof. MUDr. Markéta Bébarová, Ph.D. Department of Physiology Faculty of Medicine, Masaryk University This presentation includes only the most important terms
Magnesium Homeostasis
 ECTS PhD Training Course, Rome 3 rd September 2008 Disorders of Calcium, Phosphate h and Magnesium Homeostasis Richard Eastell Professor of Bone Metabolism Academic Unit of Bone Metabolism University of
ECTS PhD Training Course, Rome 3 rd September 2008 Disorders of Calcium, Phosphate h and Magnesium Homeostasis Richard Eastell Professor of Bone Metabolism Academic Unit of Bone Metabolism University of
Chapter 24 Water, Electrolyte and Acid-Base Balance
 Chapter 24 Water, Electrolyte and Acid-Base Balance Total body water for 150 lb. male = 40L 65% ICF 35% ECF 25% tissue fluid 8% blood plasma, lymph 2% transcellular fluid (CSF, synovial fluid) Water Movement
Chapter 24 Water, Electrolyte and Acid-Base Balance Total body water for 150 lb. male = 40L 65% ICF 35% ECF 25% tissue fluid 8% blood plasma, lymph 2% transcellular fluid (CSF, synovial fluid) Water Movement
Awaisheh. Mousa Al-Abbadi. Abdullah Alaraj. 1 Page
 f #3 Awaisheh Abdullah Alaraj Mousa Al-Abbadi 1 Page *This sheet was written from Section 1 s lecture, in the first 10 mins the Dr. repeated all the previous material relating to osteoporosis from the
f #3 Awaisheh Abdullah Alaraj Mousa Al-Abbadi 1 Page *This sheet was written from Section 1 s lecture, in the first 10 mins the Dr. repeated all the previous material relating to osteoporosis from the
The Parathyroid Glands Secrete Parathyroid Hormone, which Regulates Calcium, Magnesium, and Phosphate Ion Levels
 17.6 The Parathyroid Glands Secrete Parathyroid Hormone, which Regulates Calcium, Magnesium, and Phosphate Ion Levels Partially embedded in the posterior surface of the lateral lobes of the thyroid gland
17.6 The Parathyroid Glands Secrete Parathyroid Hormone, which Regulates Calcium, Magnesium, and Phosphate Ion Levels Partially embedded in the posterior surface of the lateral lobes of the thyroid gland
Acid Base Balance. Chapter 26 Balance. ph Imbalances. Acid Base Balance. CO 2 and ph. Carbonic Acid. Part 2. Acid/Base Balance
 Acid Base Balance Chapter 26 Balance Part 2. Acid/Base Balance Precisely balances production and loss of hydrogen ions (ph) The body generates acids during normal metabolism, tends to reduce ph Kidneys:
Acid Base Balance Chapter 26 Balance Part 2. Acid/Base Balance Precisely balances production and loss of hydrogen ions (ph) The body generates acids during normal metabolism, tends to reduce ph Kidneys:
Urinary System. Dr. ZHANG Xiong. Dept. of Physiology. ZJU School of Medicine. QUESTION 6
 Urinary System Dr. ZHANG Xiong Dept. of Physiology ZJU School of Medicine http://10.71.121.158 Copyright@ Xiong Zhang QUESTION 6 How is the filtrate reabsorbed in tubular system? Copyright@ Xiong Zhang
Urinary System Dr. ZHANG Xiong Dept. of Physiology ZJU School of Medicine http://10.71.121.158 Copyright@ Xiong Zhang QUESTION 6 How is the filtrate reabsorbed in tubular system? Copyright@ Xiong Zhang
11/05/1431. Urine Formation by the Kidneys Tubular Processing of the Glomerular Filtrate
 Urine Formation by the Kidneys Tubular Processing of the Glomerular Filtrate Chapter 27 pages 327 347 1 OBJECTIVES At the end of this lecture you should be able to describe: Absorptive Characteristics
Urine Formation by the Kidneys Tubular Processing of the Glomerular Filtrate Chapter 27 pages 327 347 1 OBJECTIVES At the end of this lecture you should be able to describe: Absorptive Characteristics
Principles of Anatomy and Physiology
 Principles of Anatomy and Physiology 14 th Edition CHAPTER 27 Fluid, Electrolyte, and Acid Base Fluid Compartments and Fluid In adults, body fluids make up between 55% and 65% of total body mass. Body
Principles of Anatomy and Physiology 14 th Edition CHAPTER 27 Fluid, Electrolyte, and Acid Base Fluid Compartments and Fluid In adults, body fluids make up between 55% and 65% of total body mass. Body
Diuretic Agents Part-2. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Diuretic Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Potassium-sparing diuretics The Ion transport pathways across the luminal and basolateral
Diuretic Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Potassium-sparing diuretics The Ion transport pathways across the luminal and basolateral
Chapter 2. Fluid, Electrolyte, and Acid-Base Imbalances
 Chapter 2 Fluid, Electrolyte, and Acid-Base Imbalances Review of Concepts and Processes The major component of the body is water. Water is located in these compartments: Intracellular fluid (ICF) compartment
Chapter 2 Fluid, Electrolyte, and Acid-Base Imbalances Review of Concepts and Processes The major component of the body is water. Water is located in these compartments: Intracellular fluid (ICF) compartment
Na concentration in the extracellular compartment is 140
 هللامسب Na regulation: Na concentration in the extracellular compartment is 140 meq\l. Na is important because: -It determines the volume of extracellular fluid : the more Na intake will expand extracellular
هللامسب Na regulation: Na concentration in the extracellular compartment is 140 meq\l. Na is important because: -It determines the volume of extracellular fluid : the more Na intake will expand extracellular
Approach to a patient with hypercalcemia
 Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
Calcium (Ca 2+ ) mg/dl
 mg/dl") Quick Guide to Laboratory Values Use this handy cheat-sheet to help you monitor laboratory values related to fluid and electrolyte status. Remember, normal values may vary according to techniques used
Quick Guide to Laboratory Values Use this handy cheat-sheet to help you monitor laboratory values related to fluid and electrolyte status. Remember, normal values may vary according to techniques used
Urinary Calculus Disease. Urinary Stones: Simplified Metabolic Evaluation. Urinary Calculus Disease. Urinary Calculus Disease 2/8/2008
 Urinary Stones: Simplified Metabolic Evaluation Marshall L. Stoller, M.D. Professor and Vice Chairman Department of Urology University of California San Francisco Incidence: 7-21/10,000 3 men: 1 woman
Urinary Stones: Simplified Metabolic Evaluation Marshall L. Stoller, M.D. Professor and Vice Chairman Department of Urology University of California San Francisco Incidence: 7-21/10,000 3 men: 1 woman
Diuretic Agents Part-1. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Diuretic Agents Part-1 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Kidneys eliminates waste products and regulates the volume, electrolyte and ph of
Diuretic Agents Part-1 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Kidneys eliminates waste products and regulates the volume, electrolyte and ph of
Dept. of Physiology. ZJU School of Medicine.
 Urinary System Dr. ZHANG Xiong Dept. of Physiology ZJU School of Medicine Http://10.10.10.151/Able.Acc2.Web/Template/View.aspx?action =view&coursetype=0&courseid=26519 QUESTION 6 How is the filtrate reabsorbed
Urinary System Dr. ZHANG Xiong Dept. of Physiology ZJU School of Medicine Http://10.10.10.151/Able.Acc2.Web/Template/View.aspx?action =view&coursetype=0&courseid=26519 QUESTION 6 How is the filtrate reabsorbed
RENAL PHYSIOLOGY, HOMEOSTASIS OF FLUID COMPARTMENTS
 RENAL PHYSIOLOGY, HOMEOSTASIS OF FLUID COMPARTMENTS (2) Dr. Attila Nagy 2017 TUBULAR FUNCTIONS (Learning objectives 54-57) 1 Tubular Transport About 99% of filtrated water and more than 90% of the filtrated
RENAL PHYSIOLOGY, HOMEOSTASIS OF FLUID COMPARTMENTS (2) Dr. Attila Nagy 2017 TUBULAR FUNCTIONS (Learning objectives 54-57) 1 Tubular Transport About 99% of filtrated water and more than 90% of the filtrated
Body water content. Fluid compartments. Regulation of water output. Water balance and ECF osmolallty. Regulation of water intake
 Body water content Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60% water; females 50% This difference reflects
Body water content Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60% water; females 50% This difference reflects
Hypoparathyroidism By John Halpern, DO, FACEP Coauthored by N. Ewen Wang, MD
 Hypoparathyroidism By John Halpern, DO, FACEP Coauthored by N. Ewen Wang, MD Reprinted with permission from: E-Medicine: Instant Access to the Minds of Medicine http://www.emedicine.com/emerg/topic276.htm
Hypoparathyroidism By John Halpern, DO, FACEP Coauthored by N. Ewen Wang, MD Reprinted with permission from: E-Medicine: Instant Access to the Minds of Medicine http://www.emedicine.com/emerg/topic276.htm
Renal Physiology II Tubular functions
 Renal Physiology II Tubular functions LO. 42, 43 Dr. Kékesi Gabriella Basic points of renal physiology 1. Glomerular filtration (GF) a) Ultrafiltration 2. Tubular functions active and passive a) Reabsorption
Renal Physiology II Tubular functions LO. 42, 43 Dr. Kékesi Gabriella Basic points of renal physiology 1. Glomerular filtration (GF) a) Ultrafiltration 2. Tubular functions active and passive a) Reabsorption
MS1 Physiology Review of Na+, K+, H + /HCO 3. /Acid-base, Ca+² and PO 4 physiology
 MS1 Physiology Review of,, / /Acidbase, Ca+² and PO 4 physiology I. David Weiner, M.D. Professor of Medicine and Physiology University of Florida College of Medicine Basic principles Proximal tubule Majority
MS1 Physiology Review of,, / /Acidbase, Ca+² and PO 4 physiology I. David Weiner, M.D. Professor of Medicine and Physiology University of Florida College of Medicine Basic principles Proximal tubule Majority
Ca, Mg metabolism, bone diseases. Tamás Kőszegi Pécs University, Department of Laboratory Medicine Pécs, Hungary
 Ca, Mg metabolism, bone diseases Tamás Kőszegi Pécs University, Department of Laboratory Medicine Pécs, Hungary Calcium homeostasis Ca 1000g in adults 99% in bones (extracellular with Mg, P) Plasma/intracellular
Ca, Mg metabolism, bone diseases Tamás Kőszegi Pécs University, Department of Laboratory Medicine Pécs, Hungary Calcium homeostasis Ca 1000g in adults 99% in bones (extracellular with Mg, P) Plasma/intracellular
Body Water Content Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are
 Fluid, Electrolyte, and Acid-Base Balance Body Water Content Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60%
Fluid, Electrolyte, and Acid-Base Balance Body Water Content Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60%
DIURETICS. Assoc. Prof. Bilgen Başgut
 DIURETICS Assoc. Prof. Bilgen Başgut Classification of Diuretics The best way to classify diuretics is to look for their Site of action in the nephron A. Diuretics that inhibit transport in the Proximal
DIURETICS Assoc. Prof. Bilgen Başgut Classification of Diuretics The best way to classify diuretics is to look for their Site of action in the nephron A. Diuretics that inhibit transport in the Proximal
Figures and tables in this presentation were adopted from various printed and electronic resorces and serve strictly for educational purposes.
 Academic lectures 3rd year of Medical faculty Figures and tables in this presentation were adopted from various printed and electronic resorces and serve strictly for educational purposes. ENDOCRINOLOGY
Academic lectures 3rd year of Medical faculty Figures and tables in this presentation were adopted from various printed and electronic resorces and serve strictly for educational purposes. ENDOCRINOLOGY
The principal functions of the kidneys
 Renal physiology The principal functions of the kidneys Formation and excretion of urine Excretion of waste products, drugs, and toxins Regulation of body water and mineral content of the body Maintenance
Renal physiology The principal functions of the kidneys Formation and excretion of urine Excretion of waste products, drugs, and toxins Regulation of body water and mineral content of the body Maintenance
Chapter 20 8/23/2016. Fluids and Electrolytes. Fluid (Water) Fluid (Water) (Cont.) Functions
 Fluid (Water) (Cont.) Functions") Chapter 20 Fluids and Electrolytes All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights reserved. Fluid (Water) Functions Provides an extracellular transportation
Chapter 20 Fluids and Electrolytes All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights reserved. Fluid (Water) Functions Provides an extracellular transportation
Persistent post transplant hyperparathyroidism. Shiva Seyrafian IUMS-97/10/18-8/1/2019
 Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
CKD: Bone Mineral Metabolism. Peter Birks, Nephrology Fellow
 CKD: Bone Mineral Metabolism Peter Birks, Nephrology Fellow CKD - KDIGO Definition and Classification of CKD CKD: abnormalities of kidney structure/function for > 3 months with health implications 1 marker
CKD: Bone Mineral Metabolism Peter Birks, Nephrology Fellow CKD - KDIGO Definition and Classification of CKD CKD: abnormalities of kidney structure/function for > 3 months with health implications 1 marker
NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS. BY: Shifaa Qa qa
 NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS BY: Shifaa Qa qa Neoplasmas of the thyroid thyroid nodules Neoplastic ---- benign, malignant Non neoplastic Solitary nodules ----- neoplastic Nodules
NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS BY: Shifaa Qa qa Neoplasmas of the thyroid thyroid nodules Neoplastic ---- benign, malignant Non neoplastic Solitary nodules ----- neoplastic Nodules
Rahaf AL-Jafari. Marah Qaddourah. Rahmeh Abdullah. Saleem. 1 P a g e
 15 Rahaf AL-Jafari Marah Qaddourah Rahmeh Abdullah Saleem 1 P a g e If you are following with the record you may notice a little bit difference in information sequences. Hormones that function on growth
15 Rahaf AL-Jafari Marah Qaddourah Rahmeh Abdullah Saleem 1 P a g e If you are following with the record you may notice a little bit difference in information sequences. Hormones that function on growth
Functions of Proximal Convoluted Tubules
 1. Proximal tubule Solute reabsorption in the proximal tubule is isosmotic (water follows solute osmotically and tubular fluid osmolality remains similar to that of plasma) 60-70% of water and solute reabsorption
1. Proximal tubule Solute reabsorption in the proximal tubule is isosmotic (water follows solute osmotically and tubular fluid osmolality remains similar to that of plasma) 60-70% of water and solute reabsorption
Pharmacology I [PHL 313] Diuretics. Dr. Mohammad Nazam Ansari
![Pharmacology I [PHL 313] Diuretics. Dr. Mohammad Nazam Ansari](/thumbs/90/104323364.jpg "Pharmacology I [PHL 313] Diuretics. Dr. Mohammad Nazam Ansari") Pharmacology I [PHL 313] Diuretics Dr. Mohammad Nazam Ansari Renal Pharmacology Kidneys: Each adult kidney weighs 125-170g in males and 115-155g in females, represent 0.5% of total body weight, but receive
Pharmacology I [PHL 313] Diuretics Dr. Mohammad Nazam Ansari Renal Pharmacology Kidneys: Each adult kidney weighs 125-170g in males and 115-155g in females, represent 0.5% of total body weight, but receive
Electrolyte Disorders in ICU. Debashis Dhar
 Electrolyte Disorders in ICU Debashis Dhar INTRODUCTION Monovalent ions most important Na,K main cations and Cl &HCO - 3 main anions Mg,Ca & Phosphate are major divalent ions Normal Physiology Body tries
Electrolyte Disorders in ICU Debashis Dhar INTRODUCTION Monovalent ions most important Na,K main cations and Cl &HCO - 3 main anions Mg,Ca & Phosphate are major divalent ions Normal Physiology Body tries
Answers and Explanations
 Answers and Explanations 1. The answer is D [V B 4 b]. Distal K + secretion is decreased by factors that decrease the driving force for passive diffusion of K + across the luminal membrane. Because spironolactone
Answers and Explanations 1. The answer is D [V B 4 b]. Distal K + secretion is decreased by factors that decrease the driving force for passive diffusion of K + across the luminal membrane. Because spironolactone
PRIMARY HYPERPARATHYROIDISM PRIMARY HYPERPARATHYROIDISM. Hyperparathyroidism Etiology. Common Complex Insidious Chronic Global Only cure is surgery
 ENDOCRINE DISORDER PRIMARY HYPERPARATHYROIDISM Roseann P. Velez, DNP, FNP Francis J. Velez, MD, FACS Common Complex Insidious Chronic Global Only cure is surgery HYPERPARATHYROIDISM PARATHRYOID GLANDS
ENDOCRINE DISORDER PRIMARY HYPERPARATHYROIDISM Roseann P. Velez, DNP, FNP Francis J. Velez, MD, FACS Common Complex Insidious Chronic Global Only cure is surgery HYPERPARATHYROIDISM PARATHRYOID GLANDS
Physio 12 -Summer 02 - Renal Physiology - Page 1
 Physiology 12 Kidney and Fluid regulation Guyton Ch 20, 21,22,23 Roles of the Kidney Regulation of body fluid osmolarity and electrolytes Regulation of acid-base balance (ph) Excretion of natural wastes
Physiology 12 Kidney and Fluid regulation Guyton Ch 20, 21,22,23 Roles of the Kidney Regulation of body fluid osmolarity and electrolytes Regulation of acid-base balance (ph) Excretion of natural wastes
PRINCIPLES OF DIURETIC ACTIONS:
 DIURETIC: A drug that increases excretion of solutes Increased urine volume is secondary All clinically useful diuretics act by blocking Na + reabsorption Has the highest EC to IC ratio = always more sodium
DIURETIC: A drug that increases excretion of solutes Increased urine volume is secondary All clinically useful diuretics act by blocking Na + reabsorption Has the highest EC to IC ratio = always more sodium
Acid Base Balance. Professor Dr. Raid M. H. Al-Salih. Clinical Chemistry Professor Dr. Raid M. H. Al-Salih
 Acid Base Balance 1 HYDROGEN ION CONCENTRATION and CONCEPT OF ph Blood hydrogen ion concentration (abbreviated [H + ]) is maintained within tight limits in health, with the normal concentration being between
Acid Base Balance 1 HYDROGEN ION CONCENTRATION and CONCEPT OF ph Blood hydrogen ion concentration (abbreviated [H + ]) is maintained within tight limits in health, with the normal concentration being between
DBL CALCIUM GLUCONATE INJECTION BP
 Description DBL CALCIUM GLUCONATE INJECTION BP DBL Calcium Gluconate Injection BP is a clear, colourless solution containing in each 10 ml, Calcium Gluconate BP 953 mg and Calcium Saccharate U.S.P. 30
Description DBL CALCIUM GLUCONATE INJECTION BP DBL Calcium Gluconate Injection BP is a clear, colourless solution containing in each 10 ml, Calcium Gluconate BP 953 mg and Calcium Saccharate U.S.P. 30
20. CALCIUM AND PHOSPHOROUS METABOLISM
 20. CALCIUM AND PHOSPHOROUS METABOLISM Many physiological processes are regulated directly or indirectly by calcium. Furthermore, the main physical structure of vertebrates and other species depend on
20. CALCIUM AND PHOSPHOROUS METABOLISM Many physiological processes are regulated directly or indirectly by calcium. Furthermore, the main physical structure of vertebrates and other species depend on
SERUM PHOSPHORUS TESTING
 MEDICAL POLICY For use with the UnitedHealthcare Laboratory Benefit Management Program, administered by BeaconLBS SERUM PHOSPHORUS TESTING Policy Number: CMP - 035 Effective Date: January 21, 2017 Table
MEDICAL POLICY For use with the UnitedHealthcare Laboratory Benefit Management Program, administered by BeaconLBS SERUM PHOSPHORUS TESTING Policy Number: CMP - 035 Effective Date: January 21, 2017 Table
Renal Physiology - Lectures
 Renal Physiology - Lectures Physiology of Body Fluids PROBLEM SET, RESEARCH ARTICLE Structure & Function of the Kidneys Renal Clearance & Glomerular Filtration PROBLEM SET Regulation of Renal Blood Flow
Renal Physiology - Lectures Physiology of Body Fluids PROBLEM SET, RESEARCH ARTICLE Structure & Function of the Kidneys Renal Clearance & Glomerular Filtration PROBLEM SET Regulation of Renal Blood Flow
RENAL TUBULAR ACIDOSIS An Overview
 RENAL TUBULAR ACIDOSIS An Overview UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY CLINICAL BIOCHEMISTRY PBL MBBS IV VJ. Temple 1 What is Renal Tubular
RENAL TUBULAR ACIDOSIS An Overview UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY CLINICAL BIOCHEMISTRY PBL MBBS IV VJ. Temple 1 What is Renal Tubular
GLOSSARY OF TERMS. produced in response to an antigen to bond with and neutralize that antigen / the body's way of destroying foreign invaders
 TERM 24-hour urine acidosis acquired aemia (prefix) albumin alkalosis anemia antibodies antigen autocrine autoimmune basal ganglion bone turnover calcilytic calcimimetic calcitonin Calcitriol Calcium carbonate
TERM 24-hour urine acidosis acquired aemia (prefix) albumin alkalosis anemia antibodies antigen autocrine autoimmune basal ganglion bone turnover calcilytic calcimimetic calcitonin Calcitriol Calcium carbonate
RENAL SYSTEM 2 TRANSPORT PROPERTIES OF NEPHRON SEGMENTS Emma Jakoi, Ph.D.
 RENAL SYSTEM 2 TRANSPORT PROPERTIES OF NEPHRON SEGMENTS Emma Jakoi, Ph.D. Learning Objectives 1. Identify the region of the renal tubule in which reabsorption and secretion occur. 2. Describe the cellular
RENAL SYSTEM 2 TRANSPORT PROPERTIES OF NEPHRON SEGMENTS Emma Jakoi, Ph.D. Learning Objectives 1. Identify the region of the renal tubule in which reabsorption and secretion occur. 2. Describe the cellular
What location in the gastrointestinal (GI) tract has tight, or impermeable, junctions between the epithelial cells?
 tract has tight, or impermeable, junctions between the epithelial cells?") CASE 32 A 17-year-old boy presents to his primary care physician with complaints of diarrhea for the last 2 days. The patient states that he just returned to the United States after visiting relatives
CASE 32 A 17-year-old boy presents to his primary care physician with complaints of diarrhea for the last 2 days. The patient states that he just returned to the United States after visiting relatives
TUBULOPATHY Intensive Care Unit Sina Hospital
 TUBULOPATHY Intensive Care Unit Sina Hospital A 13 years old female who is known case of Scoliosis. She was operated 2 months ago for spinal curve repair. PMH:EMG-MCV In 2 years old =>No Motoneuron Disease
TUBULOPATHY Intensive Care Unit Sina Hospital A 13 years old female who is known case of Scoliosis. She was operated 2 months ago for spinal curve repair. PMH:EMG-MCV In 2 years old =>No Motoneuron Disease
17. CALCIUM AND PHOSPHOROUS METABOLISM. Calcium. Role of calcium ROLE OF CALCIUM STORAGE. Calcium movement
 17. CALCIUM AND PHOSPHOROUS METABOLISM Many physiological processes are regulated directly or indirectly by calcium. Furthermore, the main physical structure of vertebrates and other species depend on
17. CALCIUM AND PHOSPHOROUS METABOLISM Many physiological processes are regulated directly or indirectly by calcium. Furthermore, the main physical structure of vertebrates and other species depend on
Hypercalcemia. Hypercalcemia: When to Worry, When to Treat! Mineral Metabolism : A Short Course
 Hypercalcemia: When to Worry, When to Treat! Michael A. Levine has no financial relationships to disclose or Conflicts of Interest to resolve. Michael A. Levine, M.D. This presentation will not involve
Hypercalcemia: When to Worry, When to Treat! Michael A. Levine has no financial relationships to disclose or Conflicts of Interest to resolve. Michael A. Levine, M.D. This presentation will not involve
Factors Affecting Calcium Metabolism in Disorders of the Kidney*
 ANNALS OF CLINICAL AND LABORATORY SCIENCE, Vol. 11, No. 4 Copyright 1981, Institute for Clinical Science, Inc. Factors Affecting Calcium Metabolism in Disorders of the Kidney* MURRAY J. FAVUS, M.D. Departm
ANNALS OF CLINICAL AND LABORATORY SCIENCE, Vol. 11, No. 4 Copyright 1981, Institute for Clinical Science, Inc. Factors Affecting Calcium Metabolism in Disorders of the Kidney* MURRAY J. FAVUS, M.D. Departm
25/10/56. Hypothyroidism Myxedema in adults Cretinism congenital deficiency of thyroid hormone Hashimoto thyroiditis. Simple goiter (nontoxic goiter)
") THERAPEUTIC USES OF THYROID HORMONE Supeecha Wittayalertpunya Wannarasmi Ketchart Nov 2013 Hyperthyroidism (Thyrotoxicosis) Grave s disease (diffuse toxic goiter) Toxic uninodular & Toxic multinodular
THERAPEUTIC USES OF THYROID HORMONE Supeecha Wittayalertpunya Wannarasmi Ketchart Nov 2013 Hyperthyroidism (Thyrotoxicosis) Grave s disease (diffuse toxic goiter) Toxic uninodular & Toxic multinodular
Diuretics having the quality of exciting excessive excretion of urine. OED. Inhibitors of Sodium Reabsorption Saluretics not Aquaretics
 Diuretics having the quality of exciting excessive excretion of urine. OED Inhibitors of Sodium Reabsorption Saluretics not Aquaretics 1 Sodium Absorption Na Entry into the Cell down an electrochemical
Diuretics having the quality of exciting excessive excretion of urine. OED Inhibitors of Sodium Reabsorption Saluretics not Aquaretics 1 Sodium Absorption Na Entry into the Cell down an electrochemical
Part 1 The Cell and the Cellular Environment
 1 Chapter 3 Anatomy and Physiology Part 1 The Cell and the Cellular Environment 2 The Human Cell The is the fundamental unit of the human body. Cells contain all the necessary for life functions. 3 Cell
1 Chapter 3 Anatomy and Physiology Part 1 The Cell and the Cellular Environment 2 The Human Cell The is the fundamental unit of the human body. Cells contain all the necessary for life functions. 3 Cell
3/19/2009. The task of the kidney in acid-base balance Excretion of the daily acid load. Buffering of an acid load. A o B - + H + B - A o +OH - C +
 The task of the kidney in acid-base balance Excretion of the daily acid load Buffering of an acid load Oxidation of amino acids, fats and carbohydrates often lead to acid production. On an average American
The task of the kidney in acid-base balance Excretion of the daily acid load Buffering of an acid load Oxidation of amino acids, fats and carbohydrates often lead to acid production. On an average American
Na + Transport 1 and 2 Linda Costanzo, Ph.D.
 Na + Transport 1 and 2 Linda Costanzo, Ph.D. OBJECTIVES: After studying this lecture, the student should understand: 1. The terminology applied to single nephron function, including the meaning of TF/P
Na + Transport 1 and 2 Linda Costanzo, Ph.D. OBJECTIVES: After studying this lecture, the student should understand: 1. The terminology applied to single nephron function, including the meaning of TF/P
HYPERPARATHYROIDIS M FAISAL GHANI SIDDIQUI MBBS; FCPS; PGDIP-BIOMEDICAL ETHICS; MCPS-HPE
 HYPERPARATHYROIDIS M FAISAL GHANI SIDDIQUI MBBS; FCPS; PGDIP-BIOMEDICAL ETHICS; MCPS-HPE PROFESSOR OF SURGERY J I N N A H S I N D H M E D I C A L U N I V E R S I T Y PREAMBLE Anatomy & physiology of the
HYPERPARATHYROIDIS M FAISAL GHANI SIDDIQUI MBBS; FCPS; PGDIP-BIOMEDICAL ETHICS; MCPS-HPE PROFESSOR OF SURGERY J I N N A H S I N D H M E D I C A L U N I V E R S I T Y PREAMBLE Anatomy & physiology of the
BIO132 Chapter 27 Fluid, Electrolyte and Acid Base Balance Lecture Outline
 BIO132 Chapter 27 Fluid, Electrolyte and Acid Base Balance Lecture Outline Fluid divisions 1. Extracellular fluid (ECF) 2. Intracellular fluid (ICF) Stabilization 1. Fluid balance 2. Electrolyte balance
BIO132 Chapter 27 Fluid, Electrolyte and Acid Base Balance Lecture Outline Fluid divisions 1. Extracellular fluid (ECF) 2. Intracellular fluid (ICF) Stabilization 1. Fluid balance 2. Electrolyte balance
014 Chapter 14 Created: 9:25:14 PM CST
 014 Chapter 14 Created: 9:25:14 PM CST Student: 1. Functions of the kidneys include A. the regulation of body salt and water balance. B. hydrogen ion homeostasis. C. the regulation of blood glucose concentration.
014 Chapter 14 Created: 9:25:14 PM CST Student: 1. Functions of the kidneys include A. the regulation of body salt and water balance. B. hydrogen ion homeostasis. C. the regulation of blood glucose concentration.
Disclosure. Topic Outline. Calcium, Vitamin D, PTH Disorders. PTH/Calcium-Normal Physiology. I have nothing to disclose
 Disclosure Calcium, Vitamin D, PTH Disorders I have nothing to disclose Chienying Liu MD Associate Clinical Professor Division of Endocrinology & Metabolism UCSF Topic Outline Calcium/Vitamin D/PTH physiology
Disclosure Calcium, Vitamin D, PTH Disorders I have nothing to disclose Chienying Liu MD Associate Clinical Professor Division of Endocrinology & Metabolism UCSF Topic Outline Calcium/Vitamin D/PTH physiology
SOCM Fluids Electrolytes and Replacement Products PFN: SOMRXL09. Terminal Learning Objective. References. Hours: 2.0 Last updated: November 2015
 SOCM Fluids Electrolytes and Replacement Products PFN: SOMRXL09 Hours: 2.0 Last updated: November 2015 Slide 1 Terminal Learning Objective Action: Communicate knowledge of Fluid, Electrolyte, and Acid
SOCM Fluids Electrolytes and Replacement Products PFN: SOMRXL09 Hours: 2.0 Last updated: November 2015 Slide 1 Terminal Learning Objective Action: Communicate knowledge of Fluid, Electrolyte, and Acid
Faculty version with model answers
 Faculty version with model answers Urinary Dilution & Concentration Bruce M. Koeppen, M.D., Ph.D. University of Connecticut Health Center 1. Increased urine output (polyuria) can result in a number of
Faculty version with model answers Urinary Dilution & Concentration Bruce M. Koeppen, M.D., Ph.D. University of Connecticut Health Center 1. Increased urine output (polyuria) can result in a number of
Urinary System and Excretion. Bio105 Lecture 20 Chapter 16
 Urinary System and Excretion Bio105 Lecture 20 Chapter 16 1 Outline Urinary System I. Function II. Organs of the urinary system A. Kidneys 1. Function 2. Structure III. Disorders of the urinary system
Urinary System and Excretion Bio105 Lecture 20 Chapter 16 1 Outline Urinary System I. Function II. Organs of the urinary system A. Kidneys 1. Function 2. Structure III. Disorders of the urinary system
Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital
 Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 13, 2017 Disclosures statement: Consultant: Allena, Becker
Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 13, 2017 Disclosures statement: Consultant: Allena, Becker
Renal System. Renal System. levels of organization. structure - function. homeostatic regulation
 Renal System The goal of these lectures is to discuss basic renal physiology. This lecture will present the regulation of H and Ca ions as well as discuss the hormonal and neural regulation of renal function.
Renal System The goal of these lectures is to discuss basic renal physiology. This lecture will present the regulation of H and Ca ions as well as discuss the hormonal and neural regulation of renal function.
Inherited Calcium and Magnesium Disorders
 Inherited Calcium and Magnesium Disorders Martin Konrad University Children s Hospital Münster, Germany IPNA / ESPN Master Class, Leuven, Sep 2nd 2015 Outline Hypercalcemia Hypomagnesemia Outline Hypercalcemia
Inherited Calcium and Magnesium Disorders Martin Konrad University Children s Hospital Münster, Germany IPNA / ESPN Master Class, Leuven, Sep 2nd 2015 Outline Hypercalcemia Hypomagnesemia Outline Hypercalcemia
Chapter 24 Lecture Outline
 Chapter 24 Lecture Outline See separate PowerPoint slides for all figures and tables preinserted into PowerPoint without notes. Copyright McGraw-Hill Education. Permission required for reproduction or
Chapter 24 Lecture Outline See separate PowerPoint slides for all figures and tables preinserted into PowerPoint without notes. Copyright McGraw-Hill Education. Permission required for reproduction or