Associate Professor Rohan Ameratunga
|
|
|
- Barnard Chapman
- 5 years ago
- Views:
Transcription

1 Associate Professor Rohan Ameratunga Adult and Paediatric Clinical Immunologist and Allergist Auckland 8:30-9:25 WS #87: Infections in Children - An Immunologist's View 9:35-10:30 WS #99: Infections in Children - An Immunologist's View (Repeated)
2 The child with recurrent infections
3 Recurrent infections in children Too many Too severe Too long Not responding to treatment

4 Recurrent Infections in children Globally

5 Malnutrition in the world

6 Childhood deaths in the world
7 Main categories Normal child 50% Child with atopy 30% Child with chronic disease and/or anatomical problems 10% Immunodeficiency: primary or secondary 10%- detailed features when to suspect
8 Clinical investigation History detailed history incl pregnancy Examination Investigations- identifying PID Lab and imaging studies
9 Pregnancy history Infections Drug use legal or illegal HIV risk factors Tobacco
10 Birth history Length of gestation Neonatal complications Admission to PICU Any complications in hospital
11 Prematurity Increased risk of RSV in the first year Difficult to identify which subgroups are at most risk Palivizumab Immunoglobulins transferred in the last trimester Increased risk of other infections not as well documented
12 Prematurity Bronchopulmonary dysplasia Still an issue with surfactant, reduced oxygen, changes in ventilation strategy etc

13 Cost-effectiveness of palivizumab in New Zealand. Vogel A, McKinlay M, Ashton T, Lennon D, Harding J, Pinnock R, Graham D, Grimwood K, Pattemore P, Schousboe M. J Paediatr Child Health 2002 Aug;38(4):
14 Growth and development Chronic disease- poor growth, some PIDS Heart and lung disease eg CF GI disease eg diarrhoea
15 Reactions to immunisation Adverse reactions to live vaccines eg rotavirus, BCG Polio no longer live
16 Medications Steroids immunosuppressives
17 Family history Recurrent infections Early deaths Unexplained deaths in childhood Consanguinity Ethnicity
18 Normal child 50% 4-8 infections/yr Increased risk: sibling attending daycare Overcrowding no more than 1 pneumonia or 2 OM in the first three years of life. Generally viral infections Complete recovery between infections
19 Socioeconomic factors and recurrent infections in children The worried well Socio-economic status- Overcrowding Attendance at daycare Number of siblings Birth order Access to medical care
20 Socioeconomic factors and recurrent infections in children
21 Normal infections
22 Clinical features of concern More than two severe infections/ yr 3 respiratory infection incl sinusitis Abx > 2 months/yr Failure to respond to antibiotics Need for IV antibiotics Unusual complications eg empyema, mastoiditis, abscesses
23 Parental smoking and other risk factors for wheezing bronchitis in children. Rylander E, Pershagen G, Eriksson M, Nordvall L. Eur J Epidemiol 1993 Sep;9(5): children with wheezing. 309 controls Parental smoking rr 1.8 Strongest association with maternal smoking and children,18/12
24 Parental smoking, bronchial reactivity and peak flow variability in children Cook, Derek G; Strachan, David P Thorax 1998;53(4):
25 Recurrent wheezy bronchitis and viral respiratory infections. Mertsola J, Ziegler T, Ruuskanen O, Vanto T, Koivikko A, Halonen P. Arch Dis Child 1991 Jan;66(1): pts 1-6 yrs recurrent wheezy bronchitis 115 episodes Mycoplasma 52 Rhinovirus 34 Associated with parental smoking
26 Atopic child AR mistaken for sinusitis Bronchitis vs pneumonia PID or anatomical problems can co-exist with atopy Higher risk of atopy with some PIDS May have allergen specific IgE tests in PID
27 Allergy as a cause of recurrent infections in children 5yr old boy with recurrent muco-purulent nasal discharge. Requiring up to 12 Rx antibiotics per year Symptoms worse in winter Frequent sneezing and rhinorrhoea Other family members also atopic Strongly +ve spt tests to HDM, cats
28 Allergy as a cause of recurrent infections in children Allergy treatment HDM prevention measures Combination of Butacort and Loratadine Reduction in frequency of infections and rhinitis symptoms Allergen-specific immunotherapy
29 The prevalence of atopic disorders in children with chronic otitis media with effusion. Alles R, Parikh A, Hawk L, Darby Y, Romero JN, Scadding G Pediatr Allergy Immunol 2001 Apr;12(2): chronic OME cases from an ENT clinic 89% had allergic rhinitis (hx, spts) cf 20% prevalence of allergic rhinitis
30 Child with chronic disease 10% Barrier failure Inadequate respiratory clearance Obstruction CV problems Foreign body Resistant organism Continuous reinfection eg contaminated water
31 Host factors important in defense Skin Mucous membranes Lysozyme Digestive enzymes Respiratory mucous clearance mechanisms
32 Generalised anatomical factors predisposing to recurrent infections in children Skin defects eg burns, eczema Multiple mechanisms: barrier loss, nutritional compromise, secondary immune defects, use of antibiotics, nosocomial infections, immobility Infections in multiple anatomical areas
33
34 Cystic fibrosis Most patients identified by neonatal screening Can present later Children can look relatively well Nasal polyps in children Chronic cough, chronic sputum production, clubbing Sweat testing +/- genetic testing Genetic testing
35 Localised anatomical factors predisposing to recurrent infections in children Localised defects eg Bronchial obstruction Most infections in the same system and same location Infections may be slow to respond to Rx There may be localised complications eg bronchiectasis. Investigations and management focused on correcting the anatomical defect.

36 Lobar pneumonia
37 Localised anatomical factors predisposing to recurrent infections in children Localised defects eg enlarged adenoids Frequent URTIS and OME ENT referral if suspected. Surgery +/- tympanostomy tubes
38 Localised anatomical factors predisposing to recurrent infections in children Localised defects eg chronic tonsillitis ENT referral Removal if indicated Frequent cause of ill health, URTIS, abdominal symptoms etc Foreign bodies- unilateral nasal symptoms

39 The immune response to cancer
40 Infections in cancer Destruction of the immune system esp Leukemia Drugs- chemotherapy Radiotherapy- multiple mechanisms Localised obstruction eg Ca bronchus Malnutrition Probably worse with hematological malignancy
41 Suspected immunodeficiency 10% Family history of immunodeficiency or unexplained early death (eg, before age 30 years) Failure to gain weight or grow normally (failure to thrive) Need for intravenous antibiotics and/or hospitalization to clear infections Six or more ear or respiratory tract infections/ year Two or more serious sinus infections or pneumonias within one year Four or more new ear infections within one year Two or more episodes of sepsis or meningitis in a lifetime Two or more months of antibiotics with little effect
42 Suspected immunodeficiency Recurrent or resistant oral or cutaneous candidiasis Recurrent deep skin or organ abscesses Infection caused by an unusual microbe and/or in an unusual location Complications from a live vaccine (eg, rotavirus, varicella, and BCG vaccines) Chronic diarrhea Nonhealing wounds Extensive skin lesions Persistent lymphopenia (age dependent) Unexplained autoimmunity or fevers Granulomas Hemophagocytic lymphohistiocytosis (HLH) Lymphoma in infancy Features typical of syndromic PIDs
43 Primary immune deficiency Stem cell Hematopoeisis X X Thymus BM X X X X antigen X X Th2 Th1 CD8 CD4 IgA IgG IgM
44 WHO classification of primary immune deficiency B cell defects- Bruton s, CVID, XLA T cell defects- di George Combined defects- SCID, XHIM Other well-defined disorders- WAS Complement defects Phagocytic defects- CGD Disorders of innate immunity- TLRs Autoinflammatory disorders- FMF, TRAPS Disorders of Apoptosis- ALPS Phenocopy
45 Patients with PID by Reported Diagnosis Other Ataxia Wiskott-Aldrich DiGeorge Hyper IgM CGD 1% 1% 2% 2% 4% 12% Severe Combined X-Linked Agamma 4% 8% IgA Subclass IgG Subclass Common Variable 17% 24% 34% 0% 10% 20% 30% 40% Source: IDF Patient Survey N=2815
46 When to suspect primary immune deficiency Increased # of infections Unusual organisms Unusual site of infections Failure to respond as predicted Failure to thrive/ growth retardation Other clinical features Family history
47
48 Times Hospitalized before Diagnosis % 21+ 5% % None 30% % One 17% Source: IDF Patient Survey N=2,708
49 Possible presentations of PID ID: GI: Chest: Bronchiectasis, bronchitis Rheum: SLE (comp), Oligoarthritis ENT: Sinusitis, otitis media Endo: Haem: AIHA, tcp, lymphoma Onc: Lymphoma, SCC Rec bacterial, fungal, viral infections Chronic diarrhea with Giardia, Crypto Mucocutaneous Candidiasis
50
51 Recognition of PIDs Institution of correct therapy Prevention of complications Addressing issues related to chronic disease (marriage, work, school, support IDFNZ) Genetic implications for family members
52 Health Status: Before and 80% After Treatment 70% 60% 50% 40% 30% 29% 28% Good Very Good Excellent 20% 10% 0% 11% 4% 4% Year Before Diagnosis 16% Last Year on IVIG
53 Why Patient was Initially Tested for PID Other Overwhelming Infection Unusual Infection 8% 6% 11% Repeated Infections 66% Routine Checkup Family History 1% 7% 0% 20% 40% 60% 80%
54 PID: Typical history 2yr old boy Recurrent chest infections since 6 mo Frequent OM Family history: 2 uncles died at 1 yr of age OE/ Absent tonsils Inx IgG 1.2 g/l No response to specific vaccines
55 Some examples of primary immune deficiencies T cell B cell Combined (HIV), digeorge Bruton s, CVID SCID, XHIM, Complement C1inh Neutrophil CGD, LAD
56 T cell immune defects T cell immune defects eg digeorge syndrome Infections: viral, fungal, parasitic, protozoal Impaired growth in children
57 B cell immune defects B cell immune defects eg XLA (Brutons) Infections: bacterial, protozoal, (viral) Normal growth in children

58 Chronic sinusitis

59 Chronic sinusitis
60 Bronchiectasis

61

62
63 Giardia
64 IVIG
65 Screening tests for immune deficiency FBC ESR Blood film Immunoglobulins Specific antibodies: proteins eg tetanus toxoid Specific antibodies: carbohydrates blood group HIV test
66 Interpretation of immunoglobulin levels Age of the child Prematurity Concurrent infections Medication Lab-lab variations
67 Interpretation of immunoglobulin levels
68 Advanced tests for PID Vaccine responses Flow cytometry Electron microscopy Molecular diagnosis
69
70 Summary: An approach to the child with recurrent infections Accurately document the numbers of infections Are the infections localised to 1 organ system? Are they localised to one anatomical location? Are there obvious predisposing factors? Incl smk Failure to thrive/ growth retardation? Unusual features of the infections Relevant Family history
71 Main categories Normal child 50% Child with atopy 30% Child with anatomical problems 10% Immunodeficiency: primary or secondary 10%

72
73
Approach to a child with recurrent infections. Dave le Roux 9 March 2012
 Approach to a child with recurrent infections Dave le Roux 9 March 2012 Jeffrey Modell Foundation http://www.info4pi.org Primary immune deficiencies: myths PID s are very very rare Selective IgA 1:333
Approach to a child with recurrent infections Dave le Roux 9 March 2012 Jeffrey Modell Foundation http://www.info4pi.org Primary immune deficiencies: myths PID s are very very rare Selective IgA 1:333
When should a Primary Immunodeficiency be Suspected?
 When should a Primary Immunodeficiency be Suspected? Ricardo U Sorensen. MD Head, Jeffrey Modell Diagnostic Center for Primary Immunodeficiencies. LSUHSC, New Orleans Learning Objectives Define Primary
When should a Primary Immunodeficiency be Suspected? Ricardo U Sorensen. MD Head, Jeffrey Modell Diagnostic Center for Primary Immunodeficiencies. LSUHSC, New Orleans Learning Objectives Define Primary
Immunology and the middle ear Andrew Riordan
 Immunology and the middle ear Andrew Riordan The Immune system is NOT there; To baffle medical students To keep Immunologists in a job To encourage experiments on mice The Immune system IS there as a defence
Immunology and the middle ear Andrew Riordan The Immune system is NOT there; To baffle medical students To keep Immunologists in a job To encourage experiments on mice The Immune system IS there as a defence
Primary Immunodeficiency
 Primary Immunodeficiency DiGeorge Syndrome Severe Combined Immunodeficiency SCID X-Linked Agammaglobulinemia Common variable immunodeficiency (CVID) IgA deficiency Hyper- IgM Syndrome Wiskott-Aldrich syndrome
Primary Immunodeficiency DiGeorge Syndrome Severe Combined Immunodeficiency SCID X-Linked Agammaglobulinemia Common variable immunodeficiency (CVID) IgA deficiency Hyper- IgM Syndrome Wiskott-Aldrich syndrome
2014/03/04. An Approach to the Child with Recurrent Respiratory Tract Infections. RRTI s: Frustrating parents
 An Approach to the Child with Recurrent Respiratory Tract Infections andré van niekerk paediatrician & paediatric pulmonologist clinton & alberlito hospitals RRTI s: Frustrating parents A common problem.
An Approach to the Child with Recurrent Respiratory Tract Infections andré van niekerk paediatrician & paediatric pulmonologist clinton & alberlito hospitals RRTI s: Frustrating parents A common problem.
Luke Droney IMMUNOGLOBULIN LEVELS AND FUNCTION
 IMMUNOGLOBULIN LEVELS AND FUNCTION Interpret changes in immunoglobulin levels within the clinical context including - Immunodeficiency - Disorders characterised by hypergammaglobulinaemia, rheumatoid arthritis,
IMMUNOGLOBULIN LEVELS AND FUNCTION Interpret changes in immunoglobulin levels within the clinical context including - Immunodeficiency - Disorders characterised by hypergammaglobulinaemia, rheumatoid arthritis,
COMMON VARIABLE IMMUNODEFICIENCY
 COMMON VARIABLE IMMUNODEFICIENCY This booklet is intended for use by patients and their families and should not replace advice from a clinical immunologist. 1 COMMON VARIABLE IMMUNODEFICIENCY Also available
COMMON VARIABLE IMMUNODEFICIENCY This booklet is intended for use by patients and their families and should not replace advice from a clinical immunologist. 1 COMMON VARIABLE IMMUNODEFICIENCY Also available
Immune Deficiency Primary and Secondary. Dr Liz McDermott Immunology Department NUH
 Immune Deficiency Primary and Secondary Dr Liz McDermott Immunology Department NUH Summary Different types of Immune Deficiency Why it is important to identify immune deficiency? Diagnostic delay Antibody
Immune Deficiency Primary and Secondary Dr Liz McDermott Immunology Department NUH Summary Different types of Immune Deficiency Why it is important to identify immune deficiency? Diagnostic delay Antibody
X-linked agammaglobulinemia (XLA)
") X-linked agammaglobulinemia (XLA) hello@piduk.org 0800 987 898 www.piduk.org About this booklet This booklet provides information on X-linked agammaglobulinemia (XLA). It has been produced by the PID UK
X-linked agammaglobulinemia (XLA) hello@piduk.org 0800 987 898 www.piduk.org About this booklet This booklet provides information on X-linked agammaglobulinemia (XLA). It has been produced by the PID UK
Problem 7 Unit 6 Clinical: Primary immunodeficiency
 Problem 7 Unit 6 Clinical: Primary immunodeficiency THE IMMUNE SYSTEM - Function: recognizing pathogens (foreign non-self antigens) and organizing a defense response against them by facilitating destruction
Problem 7 Unit 6 Clinical: Primary immunodeficiency THE IMMUNE SYSTEM - Function: recognizing pathogens (foreign non-self antigens) and organizing a defense response against them by facilitating destruction
PRIMARY IMMUNODEFICIENCIES CVID MANAGEMENT CVID MANAGEMENT
 PRIMARY IMMUNODEFICIENCIES CVID MANAGEMENT CVID MANAGEMENT 1 PRIMARY IMMUNODEFICIENCIES KEY ABBREVIATIONS CVID CT IgA IgG IgM IPOPI IVIG SCIG PID Common Variable Immune Deficiency Computerised tomography
PRIMARY IMMUNODEFICIENCIES CVID MANAGEMENT CVID MANAGEMENT 1 PRIMARY IMMUNODEFICIENCIES KEY ABBREVIATIONS CVID CT IgA IgG IgM IPOPI IVIG SCIG PID Common Variable Immune Deficiency Computerised tomography
Clinical Cases: Diagnosis and Management of Primary Immunodeficiency Around the World
 Primary Immune Deficiency: A Global Perspective Friday, February 28, 2014: 2:00 PM-5:00 PM Clinical Cases: Diagnosis and Management of Primary Immunodeficiency Around the World Elham Hossny, MD, PhD, FAAAAI
Primary Immune Deficiency: A Global Perspective Friday, February 28, 2014: 2:00 PM-5:00 PM Clinical Cases: Diagnosis and Management of Primary Immunodeficiency Around the World Elham Hossny, MD, PhD, FAAAAI
1 Immunodeficiencies. Wojciech Feleszko MD
 1 Immunodeficiencies Wojciech Feleszko MD 100 90 80 70 60 50 40 WHY TODAY? WHY WE? 2 30 Respiratory 20 10 0 Gastrointestinal CNS Urinary Tract Bones Skin 3 Immunodeficiencies Congenital/Primary genetic
1 Immunodeficiencies Wojciech Feleszko MD 100 90 80 70 60 50 40 WHY TODAY? WHY WE? 2 30 Respiratory 20 10 0 Gastrointestinal CNS Urinary Tract Bones Skin 3 Immunodeficiencies Congenital/Primary genetic
Autoimmunity and Primary Immune Deficiency
 Autoimmunity and Primary Immune Deficiency Mark Ballow, MD Division of Allergy & Immunology USF Morsani School of Medicine Johns Hopkins All Children s Hospital St Petersburg, FL The Immune System What
Autoimmunity and Primary Immune Deficiency Mark Ballow, MD Division of Allergy & Immunology USF Morsani School of Medicine Johns Hopkins All Children s Hospital St Petersburg, FL The Immune System What
The Link Between Viruses and Asthma
 The Link Between Viruses and Asthma CATHERINE KIER, MD Professor of Clinical Pediatrics Division Chief, Pediatric Pulmonary, and Cystic Fibrosis Center Director, Pediatric Sleep Disorders Center SUNY Stony
The Link Between Viruses and Asthma CATHERINE KIER, MD Professor of Clinical Pediatrics Division Chief, Pediatric Pulmonary, and Cystic Fibrosis Center Director, Pediatric Sleep Disorders Center SUNY Stony
Wheeze. Respiratory Tract Symptoms. Prof RJ Green Department of Paediatrics. Cough. Wheeze/noisy breathing. Acute. Tight chest. Shortness of breath
 Wheeze Prof RJ Green Department of Paediatrics Respiratory Tract Symptoms Cough Tight chest Wheeze/noisy breathing Shortness of breath Acute Chronic Respiratory rate Most important sign of respiratory
Wheeze Prof RJ Green Department of Paediatrics Respiratory Tract Symptoms Cough Tight chest Wheeze/noisy breathing Shortness of breath Acute Chronic Respiratory rate Most important sign of respiratory
Immunodeficiency and Skin (September 21, 2018) By (Arti Nanda, MD, DNBE [Kuwait])
![Immunodeficiency and Skin (September 21, 2018) By (Arti Nanda, MD, DNBE [Kuwait])](/thumbs/90/103062332.jpg "Immunodeficiency and Skin (September 21, 2018) By (Arti Nanda, MD, DNBE [Kuwait])") Immunodeficiency and Skin (September 21, 2018) By (Arti Nanda, MD, DNBE [Kuwait]) Immune deficiency refers to a state in which part of immune system is missing or defective resulting into an inability
Immunodeficiency and Skin (September 21, 2018) By (Arti Nanda, MD, DNBE [Kuwait]) Immune deficiency refers to a state in which part of immune system is missing or defective resulting into an inability
MY CHILD IS ALWAYS SICK! WHAT TO DO?
 2nd SWISS Pediatric Infectious Disease Training Course, Geneva, 23/24 November 2007 MY CHILD IS ALWAYS SICK! WHAT TO DO? Urs B. Schaad University Children s Hospital Basel C O N T E N T S DEFINITION PATHOGENESIS
2nd SWISS Pediatric Infectious Disease Training Course, Geneva, 23/24 November 2007 MY CHILD IS ALWAYS SICK! WHAT TO DO? Urs B. Schaad University Children s Hospital Basel C O N T E N T S DEFINITION PATHOGENESIS
CONNECTIONS. Millions of Smokers May Have Undiagnosed Lung Disease
 National Jewish Health A newsletter for physicians CONNECTIONS Winter 2016 Millions of Smokers May Have Undiagnosed Lung Disease More than half of long-term smokers who pass lung-function tests have respiratory-related
National Jewish Health A newsletter for physicians CONNECTIONS Winter 2016 Millions of Smokers May Have Undiagnosed Lung Disease More than half of long-term smokers who pass lung-function tests have respiratory-related
Reports of efficacy and safety studies of primary immunodeficiency
 2. SYNOPSIS TITLE OF STUDY: Clinical Study to Evaluate the Safety, Efficacy, and Pharmacokinetics of IGIV3I GRIFOLS [Immune Globulin Intravenous (Human)] for Replacement Therapy in Primary Immunodeficiency
2. SYNOPSIS TITLE OF STUDY: Clinical Study to Evaluate the Safety, Efficacy, and Pharmacokinetics of IGIV3I GRIFOLS [Immune Globulin Intravenous (Human)] for Replacement Therapy in Primary Immunodeficiency
Paediatric Wheeze and pneumonia. RCH Asthma RCH bronchiolitis RCH pneumonia Dr S Rajapaksa
 Paediatric Wheeze and pneumonia RCH Asthma RCH bronchiolitis RCH pneumonia Dr S Rajapaksa Case Charlotte is a 2 ½ year old who presents to ED with shortness of breath and wheeze. She had been picked up
Paediatric Wheeze and pneumonia RCH Asthma RCH bronchiolitis RCH pneumonia Dr S Rajapaksa Case Charlotte is a 2 ½ year old who presents to ED with shortness of breath and wheeze. She had been picked up
Primary Immunodeficiencies and Sinusitis. Disclosure. Learning Objectives 3/31/2014. none
 Primary Immunodeficiencies and Sinusitis Hey Jin Chong MD PhD Assistant Professor Of Pediatrics Children s Hospital Of Pittsburgh Division of Pulmonary Medicine, Allergy & Immunology none Disclosure Learning
Primary Immunodeficiencies and Sinusitis Hey Jin Chong MD PhD Assistant Professor Of Pediatrics Children s Hospital Of Pittsburgh Division of Pulmonary Medicine, Allergy & Immunology none Disclosure Learning
2013 National Treatment Survey. Immune Deficiency Foundation
 2013 National Treatment Survey Immune Deficiency Foundation IDF 2013 Treatment Survey Mail-based, pencil & paper survey Over 75 Main questions Survey in the field December 2013-March 2014 IDF mail invitation
2013 National Treatment Survey Immune Deficiency Foundation IDF 2013 Treatment Survey Mail-based, pencil & paper survey Over 75 Main questions Survey in the field December 2013-March 2014 IDF mail invitation
Overview. Barriers help animals defend against many dangerous pathogens they encounter.
 Immunity Overview Barriers help animals defend against many dangerous pathogens they encounter. The immune system recognizes foreign bodies and responds with the production of immune cells and proteins.
Immunity Overview Barriers help animals defend against many dangerous pathogens they encounter. The immune system recognizes foreign bodies and responds with the production of immune cells and proteins.
Paediatric Food Allergy. Introduction to the Causes and Management
 Paediatric Food Allergy Introduction to the Causes and Management Allergic Reactions in Children Prevalence of atopic disorders in urbanized societies has increased significantly over the past several
Paediatric Food Allergy Introduction to the Causes and Management Allergic Reactions in Children Prevalence of atopic disorders in urbanized societies has increased significantly over the past several
1/30/2016 RESPIRATORY INFECTIONS AND ASTHMA NO DISCLOSURES NO FINANCIAL INTEREST INFORMATION OBTAINED JACI AJRCCM
 RESPIRATORY INFECTIONS AND ASTHMA NO DISCLOSURES NO FINANCIAL INTEREST INFORMATION OBTAINED JACI AJRCCM 1 2 year old male HISTORY -Daycare since 9 months of age -Recurrent symptoms since 10 months of age:
RESPIRATORY INFECTIONS AND ASTHMA NO DISCLOSURES NO FINANCIAL INTEREST INFORMATION OBTAINED JACI AJRCCM 1 2 year old male HISTORY -Daycare since 9 months of age -Recurrent symptoms since 10 months of age:
Bronchiectasis in Adults - Suspected
 Bronchiectasis in Adults - Suspected Clinical symptoms which may indicate bronchiectasis for patients Take full respiratory history including presenting symptoms, past medical & family history Factors
Bronchiectasis in Adults - Suspected Clinical symptoms which may indicate bronchiectasis for patients Take full respiratory history including presenting symptoms, past medical & family history Factors
Educational paper. Primary immunodeficiencies in children: a diagnostic challenge REVIEW. Esther de Vries & Gertjan Driessen
 Eur J Pediatr (2011) 170:169 177 DOI 10.1007/s00431-010-1358-5 REVIEW Educational paper Primary immunodeficiencies in children: a diagnostic challenge Esther de Vries & Gertjan Driessen Received: 12 September
Eur J Pediatr (2011) 170:169 177 DOI 10.1007/s00431-010-1358-5 REVIEW Educational paper Primary immunodeficiencies in children: a diagnostic challenge Esther de Vries & Gertjan Driessen Received: 12 September
Chapter 24 The Immune System
 Chapter 24 The Immune System The Immune System Layered defense system The skin and chemical barriers The innate and adaptive immune systems Immunity The body s ability to recognize and destroy specific
Chapter 24 The Immune System The Immune System Layered defense system The skin and chemical barriers The innate and adaptive immune systems Immunity The body s ability to recognize and destroy specific
PIDS AND RESPIRATORY DISORDERS
 PRIMARY IMMUNODEFICIENCIES PIDS AND RESPIRATORY DISORDERS PIDS AND RESPIRATORY DISORDERS 1 PRIMARY IMMUNODEFICIENCIES ABBREVIATIONS COPD CT MRI IG PID Chronic obstructive pulmonary disease Computed tomography
PRIMARY IMMUNODEFICIENCIES PIDS AND RESPIRATORY DISORDERS PIDS AND RESPIRATORY DISORDERS 1 PRIMARY IMMUNODEFICIENCIES ABBREVIATIONS COPD CT MRI IG PID Chronic obstructive pulmonary disease Computed tomography
Primary Immunodeficiency Disease: Underdiagnosed at any age. Anne L Sherwood, PhD Director of Scientific Affairs The Binding Site, Inc.
 Primary Immunodeficiency Disease: Underdiagnosed at any age Anne L Sherwood, PhD Director of Scientific Affairs The Binding Site, Inc. Learning Objectives Identify the difference between primary and secondary
Primary Immunodeficiency Disease: Underdiagnosed at any age Anne L Sherwood, PhD Director of Scientific Affairs The Binding Site, Inc. Learning Objectives Identify the difference between primary and secondary
Clinical Immunodeficiency. Dr Claire Bethune Consultant Immunologist
 Clinical Immunodeficiency Dr Claire Bethune Consultant Immunologist Peninsula Specialist Immunodeficiency and Allergy service Eden Unit, Derriford https://www.plymouthhospitals.nhs. uk/eden Or Google Immunology
Clinical Immunodeficiency Dr Claire Bethune Consultant Immunologist Peninsula Specialist Immunodeficiency and Allergy service Eden Unit, Derriford https://www.plymouthhospitals.nhs. uk/eden Or Google Immunology
Primary Immunodeficiency Program at AUBMC (In collaboration with Children's Hospital in Boston and Four Regional Hospitals in the Middle East):
:") Primary Immunodeficiency Program at AUBMC (In collaboration with Children's Hospital in Boston and Four Regional Hospitals in the Middle East): Studies of Immunological Deficiency Syndromes Congenital
Primary Immunodeficiency Program at AUBMC (In collaboration with Children's Hospital in Boston and Four Regional Hospitals in the Middle East): Studies of Immunological Deficiency Syndromes Congenital
NECK MASS. Clinical history and examination: Document detail history of mass. Imaging: US or CT of neck
 ENT ENT Referral Referral Guidelines Guidelines Austin Health ENT Clinic holds fortnightly multidisciplinary meetings with Plastics/ Maxillary Facial and Oncology units to discuss and plan the treatment
ENT ENT Referral Referral Guidelines Guidelines Austin Health ENT Clinic holds fortnightly multidisciplinary meetings with Plastics/ Maxillary Facial and Oncology units to discuss and plan the treatment
IgG subclass deficiencies
 IgG subclass deficiencies hello@piduk.org 0800 987 8986 www.piduk.org About this booklet This booklet provides information on IgG subclass deficiencies. It has been produced by the PID UK Medical Advisory
IgG subclass deficiencies hello@piduk.org 0800 987 8986 www.piduk.org About this booklet This booklet provides information on IgG subclass deficiencies. It has been produced by the PID UK Medical Advisory
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE 1 Guideline title SCOPE Bronchiolitis: diagnosis and management of bronchiolitis in children. 1.1 Short title Bronchiolitis in children 2 The remit The
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE 1 Guideline title SCOPE Bronchiolitis: diagnosis and management of bronchiolitis in children. 1.1 Short title Bronchiolitis in children 2 The remit The
3/29/2011. Algorithms for Diagnosis of Suspected Immunodeficiency. Overview. Case #1. Case #2. Primary Immunodeficiency (PID) Case #3
 Case #3") Overview Algorithms for Diagnosis of Immuno Susan M. Orton, PhD, D(ABMLI), MT(ASCP) Associate Professor Four major categories of primary immuno (PID) Clinical conditions associated with PID and organisms
Overview Algorithms for Diagnosis of Immuno Susan M. Orton, PhD, D(ABMLI), MT(ASCP) Associate Professor Four major categories of primary immuno (PID) Clinical conditions associated with PID and organisms
How the Immune System Works (and Fails) in 45 Minutes or Less. Disclosures. Learning Objectives 10/15/2014. Nothing to Disclose
 in 45 Minutes or Less. Disclosures. Learning Objectives 10/15/2014. Nothing to Disclose") How the Immune System Works (and Fails) in 45 Minutes or Less Christina Ciaccio MD, MSc Assistant Professor of Medicine and Pediatrics Nothing to Disclose Disclosures Learning Objectives List s involved
How the Immune System Works (and Fails) in 45 Minutes or Less Christina Ciaccio MD, MSc Assistant Professor of Medicine and Pediatrics Nothing to Disclose Disclosures Learning Objectives List s involved
Rhinosinusitis. John Ramey, MD Joseph Russell, MD
 Rhinosinusitis John Ramey, MD Joseph Russell, MD Disclosure Statement RSFH as a continuing medical education provider, accredited by the South Carolina Medical Association, it is the policy of RSFH to
Rhinosinusitis John Ramey, MD Joseph Russell, MD Disclosure Statement RSFH as a continuing medical education provider, accredited by the South Carolina Medical Association, it is the policy of RSFH to
Chapter 16 Pneumococcal Infection. Pneumococcal Infection. August 2015
 Chapter 16 16 PPV introduced for at risk 1996 PCV7 introduced for at risk 2002 and as routine 2008 PCV13 replaced PCV7 in 2010 NOTIFIABLE In some circumstances, advice in these guidelines may differ from
Chapter 16 16 PPV introduced for at risk 1996 PCV7 introduced for at risk 2002 and as routine 2008 PCV13 replaced PCV7 in 2010 NOTIFIABLE In some circumstances, advice in these guidelines may differ from
2360 Corporate Circle, Suite 400 Henderson, NV , USA. Innovative Diagnostic Approach in Primary Immunodeficiency
 2360 Corporate Circle, Suite 400 Henderson, NV 89074-7722, USA Innovative Diagnostic Approach in Primary Immunodeficiency Disorders 2360 Corporate Circle, Suite 400 Henderson, NV 89074-7722, USA Innovative
2360 Corporate Circle, Suite 400 Henderson, NV 89074-7722, USA Innovative Diagnostic Approach in Primary Immunodeficiency Disorders 2360 Corporate Circle, Suite 400 Henderson, NV 89074-7722, USA Innovative
A heterogeneous collection of diseases characterised by hypogammaglobulinemia.
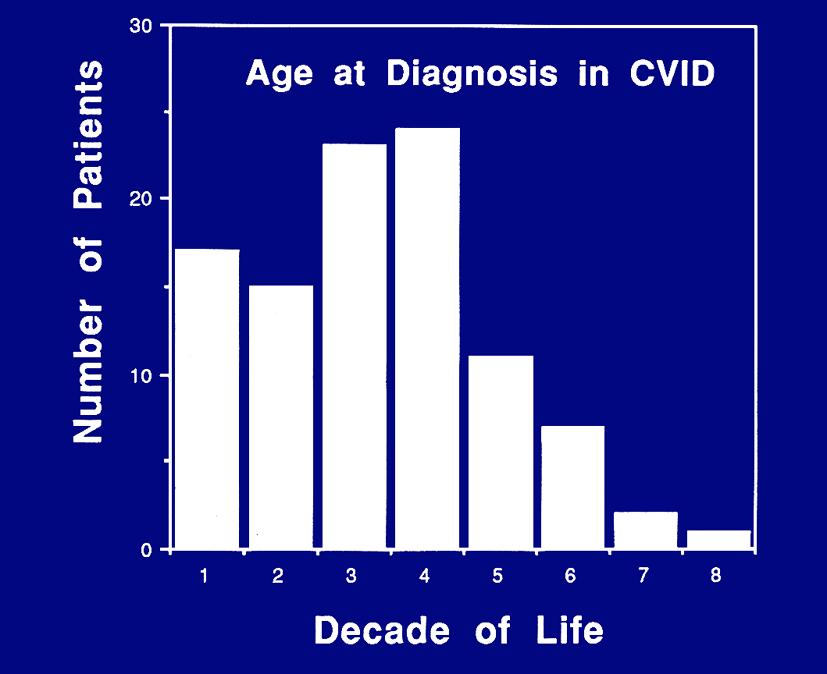
 1 Common variable immunodeficiency () A heterogeneous collection of diseases characterised by hypogammaglobulinemia. Although is the most common primary immune deficiency (PID) symptomatic in adults, it
1 Common variable immunodeficiency () A heterogeneous collection of diseases characterised by hypogammaglobulinemia. Although is the most common primary immune deficiency (PID) symptomatic in adults, it
Non Cystic Fibrosis Bronchiectasis: How to Proceed?
 Non Cystic Fibrosis Bronchiectasis: How to Proceed? Dr Ankit Parakh MD, DNB, MNAMS, RCPCH Fellow (UK), European Diplomate of Pediatric Respiratory Medicine ERS Fellowship Pediatric Medicine & NIV (GOSH,
Non Cystic Fibrosis Bronchiectasis: How to Proceed? Dr Ankit Parakh MD, DNB, MNAMS, RCPCH Fellow (UK), European Diplomate of Pediatric Respiratory Medicine ERS Fellowship Pediatric Medicine & NIV (GOSH,
Disorder name: Severe Combined Immunodeficiency Acronym: SCID
 Genetic Fact Sheets for Parents Other Disorders Screening, Technology, and Research in Genetics is a multi-state project to improve information about the financial, ethical, legal, and social issues surrounding
Genetic Fact Sheets for Parents Other Disorders Screening, Technology, and Research in Genetics is a multi-state project to improve information about the financial, ethical, legal, and social issues surrounding
Primary immunodeficiencies: when to worry about your child's immune system?
 Primary immunodeficiencies: when to worry about your child's immune system? One of the most frequent concerns from the parents of my little patients (and I am sure this is valid for all pediatricians)
Primary immunodeficiencies: when to worry about your child's immune system? One of the most frequent concerns from the parents of my little patients (and I am sure this is valid for all pediatricians)
Support for Immune Globulin Replacement Therapy in IgG Subclass Deficiency. Michelle Huffaker, MD Stanford University
 Support for Immune Globulin Replacement Therapy in IgG Subclass Deficiency Michelle Huffaker, MD Stanford University Disclosures I have nothing to disclose What is an IgG subclass? Subclass IgG1 IgG2 IgG3
Support for Immune Globulin Replacement Therapy in IgG Subclass Deficiency Michelle Huffaker, MD Stanford University Disclosures I have nothing to disclose What is an IgG subclass? Subclass IgG1 IgG2 IgG3
ENT Referral Guidelines
 ENT Referral Guidelines Austin Health ENT Clinic holds fortnightly multidisciplinary meetings with Plastics/ Maxillary Facial and Oncology units to discuss and plan the treatment of patients with cancerous
ENT Referral Guidelines Austin Health ENT Clinic holds fortnightly multidisciplinary meetings with Plastics/ Maxillary Facial and Oncology units to discuss and plan the treatment of patients with cancerous
USAID Health Care Improvement Project. pneumonia) respiratory infections through improved case management (amb/hosp)
 respiratory infections through improved case management (amb/hosp)") Improvement objective: : decrease morbidity and mortality due to acute upper (rhinitis, sinusitis, pharyngitis) and lower (bronchitis, pneumonia) respiratory infections through improved case management
Improvement objective: : decrease morbidity and mortality due to acute upper (rhinitis, sinusitis, pharyngitis) and lower (bronchitis, pneumonia) respiratory infections through improved case management
Wiskott-Aldrich Syndrome
 chapter 7 Wiskott-Aldrich Syndrome Wiskott-Aldrich syndrome is a primary immunodeficiency disease involving both T- and B-lymphocytes. In addition, the blood cells that help control bleeding, called platelets
chapter 7 Wiskott-Aldrich Syndrome Wiskott-Aldrich syndrome is a primary immunodeficiency disease involving both T- and B-lymphocytes. In addition, the blood cells that help control bleeding, called platelets
Transient pulmonary infiltrations in cystic fibrosis due to allergic aspergillosis
 Thorax (1965), 20, 385 Transient pulmonary infiltrations in cystic fibrosis due to allergic aspergillosis MARGARET MEARNS, WINIFRED YOUNG, AND JOHN BATTEN From the Queen Elizabeth Hospital, Hackney, and
Thorax (1965), 20, 385 Transient pulmonary infiltrations in cystic fibrosis due to allergic aspergillosis MARGARET MEARNS, WINIFRED YOUNG, AND JOHN BATTEN From the Queen Elizabeth Hospital, Hackney, and
Name of Primary Immune Deficiency: Patient/Applicant Name: Parent/Carer Name (if child under 16): Address: Phone: GP: Immunologist:
: Address: Phone: GP: Immunologist:") Name of Primary Immune Deficiency: Patient/Applicant Name: Parent/Carer Name (if child under 16): Address: Phone: GP: Immunologist: Date: To whom it may concern: A Primary Immune Deficiency (PI) is a genetic
Name of Primary Immune Deficiency: Patient/Applicant Name: Parent/Carer Name (if child under 16): Address: Phone: GP: Immunologist: Date: To whom it may concern: A Primary Immune Deficiency (PI) is a genetic
WHEEZING IN INFANCY: IS IT ASTHMA?
 WHEEZING IN INFANCY: IS IT ASTHMA? Jittlada Deerojanawong Department of Pediatrics, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand Wheezing is common symptoms throughout infancy and childhood
WHEEZING IN INFANCY: IS IT ASTHMA? Jittlada Deerojanawong Department of Pediatrics, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand Wheezing is common symptoms throughout infancy and childhood
HYPER IgM SYNDROME This booklet is intended for use by patients and their families and should not replace advice from a clinical immunologist.
 HYPER IgM SYNDROME This booklet is intended for use by patients and their families and should not replace advice from a clinical immunologist. 1 HYPER IgM SYNDROME Also available : COMMON VARIABLE IMMUNODEFICIENCY
HYPER IgM SYNDROME This booklet is intended for use by patients and their families and should not replace advice from a clinical immunologist. 1 HYPER IgM SYNDROME Also available : COMMON VARIABLE IMMUNODEFICIENCY
Immunodeficiency. (1 of 2)
") Immunodeficiency (1 of 2) Primary immunodeficiency diseases Innate or adaptive Most are detected in infancy (6 months 2 years) Rare but some mild genetic forms exist in many individuals Defects in Innate
Immunodeficiency (1 of 2) Primary immunodeficiency diseases Innate or adaptive Most are detected in infancy (6 months 2 years) Rare but some mild genetic forms exist in many individuals Defects in Innate
New proposals for partial antibody deficiencies
 New proposals for partial antibody deficiencies Helen Chapel, Janne Bjorkander,, Mary-Ellen Conley, Teresa Espanol,, Amos Etzioni, Bodo Grimacher, Lennart Hammarstrom,, Maria Kanariou,, Luigi Notarangelo,,
New proposals for partial antibody deficiencies Helen Chapel, Janne Bjorkander,, Mary-Ellen Conley, Teresa Espanol,, Amos Etzioni, Bodo Grimacher, Lennart Hammarstrom,, Maria Kanariou,, Luigi Notarangelo,,
IMMUNOLOGY. Referral Guidelines NATIONAL REFERRAL GUIDELINES : IMMUNOLOGY. As above Specialist assessment is essential.
 PAGE 1 IMMUNOLOGY National PRIMARY IMMUNODEFICIENCY Primary immunodeficiency should be suspected in any patient with recurrent or persistent infection or unusual infection. Recurrent sinopulmonary infections
PAGE 1 IMMUNOLOGY National PRIMARY IMMUNODEFICIENCY Primary immunodeficiency should be suspected in any patient with recurrent or persistent infection or unusual infection. Recurrent sinopulmonary infections
Pneumococcal Vaccine in Children: current situation
 Pneumococcal Vaccine in Children: current situation LAU Yu Lung Chair Professor of Paediatrics Doris Zimmern Professor in Community Child Health LKS Faculty of Medicine, The University of Hong Kong Chairman
Pneumococcal Vaccine in Children: current situation LAU Yu Lung Chair Professor of Paediatrics Doris Zimmern Professor in Community Child Health LKS Faculty of Medicine, The University of Hong Kong Chairman
The University of Arizona Pediatric Residency Program. Primary Goals for Rotation. Pulmonary
 The University of Arizona Pediatric Residency Program Primary Goals for Rotation Pulmonary 1. GOAL: Diagnose and manage patients with asthma. 2. GOAL: Understand the role of the pediatrician in preventing
The University of Arizona Pediatric Residency Program Primary Goals for Rotation Pulmonary 1. GOAL: Diagnose and manage patients with asthma. 2. GOAL: Understand the role of the pediatrician in preventing
PATHOLOGY & PATHOPHYSIOLOGY
 PATHOLOGY & PATHOPHYSIOLOGY DISORDERS OF THE RESPIRATORY SYSTEM DISORDERS OF THE RESPIRATORY SYSTEM Disorders of the Respiratory System Infections Degenerative Tumours Immune Trauma Congenital Upper respiratory
PATHOLOGY & PATHOPHYSIOLOGY DISORDERS OF THE RESPIRATORY SYSTEM DISORDERS OF THE RESPIRATORY SYSTEM Disorders of the Respiratory System Infections Degenerative Tumours Immune Trauma Congenital Upper respiratory
Atopic Dermatitis and Primary Immunodeficiency: When Should I Worry?
 Atopic Dermatitis and Primary Immunodeficiency: When Should I Worry? Markus Boos, MD PhD Attending Physician, Dermatology Seattle Children s Hospital Assistant Professor of Pediatrics, University of Washington
Atopic Dermatitis and Primary Immunodeficiency: When Should I Worry? Markus Boos, MD PhD Attending Physician, Dermatology Seattle Children s Hospital Assistant Professor of Pediatrics, University of Washington
Respiratory System Virology
 Respiratory System Virology Common Cold: Rhinitis. A benign self limited syndrome caused by several families of viruses. The most frequent acute illness in industrialized world. Mild URT illness involving:
Respiratory System Virology Common Cold: Rhinitis. A benign self limited syndrome caused by several families of viruses. The most frequent acute illness in industrialized world. Mild URT illness involving:
Physiology Unit 3. ADAPTIVE IMMUNITY The Specific Immune Response
 Physiology Unit 3 ADAPTIVE IMMUNITY The Specific Immune Response In Physiology Today The Adaptive Arm of the Immune System Specific Immune Response Internal defense against a specific pathogen Acquired
Physiology Unit 3 ADAPTIVE IMMUNITY The Specific Immune Response In Physiology Today The Adaptive Arm of the Immune System Specific Immune Response Internal defense against a specific pathogen Acquired
Imunodeficiency states
 Imunodeficiency states Primary Caused by defined genetic defects Usually rare, but severe (exception: IgA deficiency) Secondary Consequence of some other disease, treatment, environmental factors Usually
Imunodeficiency states Primary Caused by defined genetic defects Usually rare, but severe (exception: IgA deficiency) Secondary Consequence of some other disease, treatment, environmental factors Usually
WISKOTT-ALDRICH SYNDROME. An X-linked Primary Immunodeficiency
 WISKOTT-ALDRICH SYNDROME An X-linked Primary Immunodeficiency WHAT IS WISKOTT ALDRICH SYNDROME? Wiskott-Aldrich Syndrome (WAS) is a serious medical condition that causes problems both with the immune system
WISKOTT-ALDRICH SYNDROME An X-linked Primary Immunodeficiency WHAT IS WISKOTT ALDRICH SYNDROME? Wiskott-Aldrich Syndrome (WAS) is a serious medical condition that causes problems both with the immune system
IMMUNODEFICIENCIES CLASSIFICATION OF PIDS PRIMARY IMMUNODEFICIENCIES CLASSIFIED?
 PRIMARY IMMUNODEFICIENCIES CLASSIFICATION OF PIDS HOW ARE PRIMARY IMMUNODEFICIENCIES CLASSIFIED? 1 PRIMARY IMMUNODEFICIENCIES KEY ABBREVIATIONS CGD CVID IBD IgA/D/E/G/M IPOPI PID SCID Chronic granulomatous
PRIMARY IMMUNODEFICIENCIES CLASSIFICATION OF PIDS HOW ARE PRIMARY IMMUNODEFICIENCIES CLASSIFIED? 1 PRIMARY IMMUNODEFICIENCIES KEY ABBREVIATIONS CGD CVID IBD IgA/D/E/G/M IPOPI PID SCID Chronic granulomatous
Immunodeficiency. By Dr. Gouse Mohiddin Shaik
 Immunodeficiency By Dr. Gouse Mohiddin Shaik Immunodeficieny Immunodeficiency is failure of immune system to protect against disease or malignency Immunodeficiency is of two types Primary Secondary immunodeficiency
Immunodeficiency By Dr. Gouse Mohiddin Shaik Immunodeficieny Immunodeficiency is failure of immune system to protect against disease or malignency Immunodeficiency is of two types Primary Secondary immunodeficiency
The child with a troublesome cough. Dr Marco Zampoli Paediatric Pulmonology Red Cross War Memorial Children s Hospital GP Refresher Course 2012
 The child with a troublesome cough Dr Marco Zampoli Paediatric Pulmonology Red Cross War Memorial Children s Hospital GP Refresher Course 2012 Cough is the most common symptom in children Inability to
The child with a troublesome cough Dr Marco Zampoli Paediatric Pulmonology Red Cross War Memorial Children s Hospital GP Refresher Course 2012 Cough is the most common symptom in children Inability to
Potential public health impact of RSV vaccines. R. Karron December 2016
 Potential public health impact of RSV vaccines R. Karron December 2016 1. RSV is The leading cause of hospitalization in infants and in many high-income countries; >2 million medical visits annually in
Potential public health impact of RSV vaccines R. Karron December 2016 1. RSV is The leading cause of hospitalization in infants and in many high-income countries; >2 million medical visits annually in
Recurrent Infection, Pulmonary Disease, and Autoimmunity as Manifestations of Immune Deficiency
 Recurrent Infection, Pulmonary Disease, and Autoimmunity as Manifestations of Immune Deficiency Erwin W. Gelfand, M.D. Professor, Department of Pediatrics National Jewish Health Professor of Immunology
Recurrent Infection, Pulmonary Disease, and Autoimmunity as Manifestations of Immune Deficiency Erwin W. Gelfand, M.D. Professor, Department of Pediatrics National Jewish Health Professor of Immunology
Understanding Diagnostic Tests for Immunodeficiency
 Understanding Diagnostic Tests for Immunodeficiency Manish J. Butte, M.D. Ph.D. Assistant Professor mjbutte@stanford.edu http://tcell.stanford.edu September 21, 2013 PEDIATRICS What are we testing for?
Understanding Diagnostic Tests for Immunodeficiency Manish J. Butte, M.D. Ph.D. Assistant Professor mjbutte@stanford.edu http://tcell.stanford.edu September 21, 2013 PEDIATRICS What are we testing for?
PNEUMONIA IN CHILDREN. IAP UG Teaching slides
 PNEUMONIA IN CHILDREN 1 INTRODUCTION 156 million new episodes / yr. worldwide 151 million episodes developing world 95% in developing countries 19% of all deaths in children
PNEUMONIA IN CHILDREN 1 INTRODUCTION 156 million new episodes / yr. worldwide 151 million episodes developing world 95% in developing countries 19% of all deaths in children
Acute Otitis Media, Acute Bacterial Sinusitis, and Acute Bacterial Rhinosinusitis
 Acute Otitis Media, Acute Bacterial Sinusitis, and Acute Bacterial Rhinosinusitis This guideline, developed by Larry Simmons, MD, in collaboration with the ANGELS team, on October 3, 2013, is a significantly
Acute Otitis Media, Acute Bacterial Sinusitis, and Acute Bacterial Rhinosinusitis This guideline, developed by Larry Simmons, MD, in collaboration with the ANGELS team, on October 3, 2013, is a significantly
Assessing wheeze in pre-school children
 Assessing wheeze in pre-school children 8 Wheeze in children aged less than five years has many potential causes. Often it is regarded as the first sign of asthma, however, a substantial proportion of
Assessing wheeze in pre-school children 8 Wheeze in children aged less than five years has many potential causes. Often it is regarded as the first sign of asthma, however, a substantial proportion of
Immunology: an overview Lecture
 Slide #2: Immunology is sometimes regarded as part of microbiology department because it started there as an investigation of ways used to prevent against infectious agents (e.g. microorganisms ). However
Slide #2: Immunology is sometimes regarded as part of microbiology department because it started there as an investigation of ways used to prevent against infectious agents (e.g. microorganisms ). However
Understanding PIDD. Primary Immunodeficiency Disease (PIDD)
") Understanding PIDD Primary Immunodeficiency Disease (PIDD) Understanding PIDD Primary Immunodeficiency Disease (PIDD) What is Primary Immunodeficiency? Primary Immunodeficiency (PIDD or PID) is a disease
Understanding PIDD Primary Immunodeficiency Disease (PIDD) Understanding PIDD Primary Immunodeficiency Disease (PIDD) What is Primary Immunodeficiency? Primary Immunodeficiency (PIDD or PID) is a disease
Rhinosinusitis: Current Concepts. Frederick S. Rosen, MD Matthew Ryan, MD
 Rhinosinusitis: Current Concepts Frederick S. Rosen, MD Matthew Ryan, MD Introduction 2 Introduction The medical condition most commonly reported by US Census Department Major Factors: Facial pain/pressure,
Rhinosinusitis: Current Concepts Frederick S. Rosen, MD Matthew Ryan, MD Introduction 2 Introduction The medical condition most commonly reported by US Census Department Major Factors: Facial pain/pressure,
Secondary Immunodeficiency
 A guide for patients, their families, friends and healthcare professionals Raising awareness and supporting patients with immunodeficiencies in Australia. Secondary Immunodeficiency Edition 1 Date 15 th
A guide for patients, their families, friends and healthcare professionals Raising awareness and supporting patients with immunodeficiencies in Australia. Secondary Immunodeficiency Edition 1 Date 15 th
Agammaglobulinemia. Vilnius University Children s s Hospital Pediatric Center, R.Duobiene
 Agammaglobulinemia Vilnius University Children s s Hospital Pediatric Center, R.Duobiene Case report R.B., male, born on February 1997. The parents are consanguineous. Eyes pathology in fathers family
Agammaglobulinemia Vilnius University Children s s Hospital Pediatric Center, R.Duobiene Case report R.B., male, born on February 1997. The parents are consanguineous. Eyes pathology in fathers family
Immunology. Anas Abu-Humaidan M.D. Ph.D. Transplant immunology+ Secondary immune deficiency
 Immunology Anas Abu-Humaidan M.D. Ph.D. Transplant immunology+ Secondary immune deficiency Transplant Immunology Transplantation is the process of moving cells, tissues or organs from one site to another
Immunology Anas Abu-Humaidan M.D. Ph.D. Transplant immunology+ Secondary immune deficiency Transplant Immunology Transplantation is the process of moving cells, tissues or organs from one site to another
Reducing unnecessary antibiotic use in respiratory tract infections in children
 Reducing unnecessary antibiotic use in respiratory tract infections in children -a secondary care perspective Dr Conor Doherty (Consultant in paediatric infectious diseases and immunology GGC) Current
Reducing unnecessary antibiotic use in respiratory tract infections in children -a secondary care perspective Dr Conor Doherty (Consultant in paediatric infectious diseases and immunology GGC) Current
Chronic Obstructive Pulmonary Disease
 Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
3002 Seminar. Problem-Based Learning: Evaluating and Managing the Patient with Recurrent Infections DO NOTE TURN THE PAGES UNTIL INSTRUCTED TO DO SO!
 3002 Seminar Problem-Based Learning: Evaluating and Managing the Patient with Recurrent Infections DO NOTE TURN THE PAGES UNTIL INSTRUCTED TO DO SO! Discussion leaders: Kenneth Paris, MD Richard L. Wasserman,
3002 Seminar Problem-Based Learning: Evaluating and Managing the Patient with Recurrent Infections DO NOTE TURN THE PAGES UNTIL INSTRUCTED TO DO SO! Discussion leaders: Kenneth Paris, MD Richard L. Wasserman,
Chapter 11. Hyper IgM Syndromes
 Chapter 11 Hyper IgM Syndromes Patients with Hyper-IgM (HIGM) syndrome are susceptible to recurrent and severe infections and in some types of HIGM syndrome opportunistic infections and an increased risk
Chapter 11 Hyper IgM Syndromes Patients with Hyper-IgM (HIGM) syndrome are susceptible to recurrent and severe infections and in some types of HIGM syndrome opportunistic infections and an increased risk
Evelyn A. Kluka, MD FAAP November 30, 2011
 Evelyn A. Kluka, MD FAAP November 30, 2011 > 80% of children will suffer from at least one episode of AOM by 3 years of age 40% will have > 6 recurrences by age 7 years Most common diagnosis for which
Evelyn A. Kluka, MD FAAP November 30, 2011 > 80% of children will suffer from at least one episode of AOM by 3 years of age 40% will have > 6 recurrences by age 7 years Most common diagnosis for which
Autoimmunity and autoinflammation
 Autoimmunity and autoinflammation Primary immunodeficiencies Autoimmunity and autoinflammation 1 Primary immunodeficiencies List of some common abbreviations APECED CAPS CGD CINCA CRMO CVID FCAS FMF HIDS
Autoimmunity and autoinflammation Primary immunodeficiencies Autoimmunity and autoinflammation 1 Primary immunodeficiencies List of some common abbreviations APECED CAPS CGD CINCA CRMO CVID FCAS FMF HIDS
IVIG (intravenous immunoglobulin) Bivigam, Carimune NF, Flebogamma, Gammagard, Gammagard S/D, Gammaked, Gammaplex, Gamunex-C, Octagam, Privigen
 Bivigam, Carimune NF, Flebogamma, Gammagard, Gammagard S/D, Gammaked, Gammaplex, Gamunex-C, Octagam, Privigen") Pre - PA Allowance None Prior-Approval Requirements Diagnoses Patient must have ONE of the following documented indications: 1. Primary Immunodeficiency Disease (PID) with ONE of the a. Hypogammaglobulinemia,
Pre - PA Allowance None Prior-Approval Requirements Diagnoses Patient must have ONE of the following documented indications: 1. Primary Immunodeficiency Disease (PID) with ONE of the a. Hypogammaglobulinemia,
Bronchiolitis Update. Key reviewer: Dr Philip Pattemore, Associate Professor of Paediatrics, University of Otago, Christchurch.
 www.bpac.org.nz keyword: bronchiolitis Bronchiolitis Update Key reviewer: Dr Philip Pattemore, Associate Professor of Paediatrics, University of Otago, Christchurch Key Points: Bronchiolitis is the most
www.bpac.org.nz keyword: bronchiolitis Bronchiolitis Update Key reviewer: Dr Philip Pattemore, Associate Professor of Paediatrics, University of Otago, Christchurch Key Points: Bronchiolitis is the most
Immunocompetence The immune system responds appropriately to a foreign stimulus
 Functions of the immune system Protect the body s internal environment against invading organisms Maintain homeostasis by removing damaged cells from the circulation Serve as a surveillance network for
Functions of the immune system Protect the body s internal environment against invading organisms Maintain homeostasis by removing damaged cells from the circulation Serve as a surveillance network for
Outline. Terms and definitions Evolution Overview of investigations Disorders of immune system
 Clinical immunology Outline Terms and definitions Evolution Overview of investigations Disorders of immune system Immune deficiencies Autoimmunity (Allergy) (Malignancy) (Transplantation medicine) Terms
Clinical immunology Outline Terms and definitions Evolution Overview of investigations Disorders of immune system Immune deficiencies Autoimmunity (Allergy) (Malignancy) (Transplantation medicine) Terms
Unit II Problem 2 Pathology: Pneumonia
 Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
Unit II Problem 2 Pathology: Pneumonia - Definition: pneumonia is the infection of lung parenchyma which occurs especially when normal defenses are impaired such as: Cough reflex. Damage of cilia in respiratory
IMMU 7630 Fall 2011 IMMUNODEFICIENCY
 IMMUNODEFICIENCY CATEGORIES OF IMMUNODEFICIENCY STATES. Immunodeficiency can be primary or secondary. Primary immunodeficiency means a disease with a genetic cause, while secondary implies that some known
IMMUNODEFICIENCY CATEGORIES OF IMMUNODEFICIENCY STATES. Immunodeficiency can be primary or secondary. Primary immunodeficiency means a disease with a genetic cause, while secondary implies that some known
4/28/2016. Host Defenses. Unit 8 Microorganisms & The Immune System. Types of Innate Defenses. Defensive Cells Leukocytes
 Host Defenses Unit 8 Microorganisms & The Immune System CH 16-18 Host defenses that produce resistance can be either innate or adaptive: Innate: those that protect against any type of invading agent Adaptive:
Host Defenses Unit 8 Microorganisms & The Immune System CH 16-18 Host defenses that produce resistance can be either innate or adaptive: Innate: those that protect against any type of invading agent Adaptive:
Seasonal Allergic Rhinitis (Hay Fever)
") Seasonal Allergic Rhinitis (Hay Fever) Link to prescribing guidance: http://www.enhertsccg.nhs.uk/ear-nose-and-oropharynx Clinical Presentation Link to CKS NICE guidance: https://cks.nice.org.uk/allergicrhinitis
Seasonal Allergic Rhinitis (Hay Fever) Link to prescribing guidance: http://www.enhertsccg.nhs.uk/ear-nose-and-oropharynx Clinical Presentation Link to CKS NICE guidance: https://cks.nice.org.uk/allergicrhinitis
Clinical Practice Guideline: Tonsillectomy in Children, Baugh et al Otolaryngology Head and Neck Surgery, 2011 J and: 144 (1 supplement) S1 30.
 S1 30.") Pediatric ENT Guidelines Jane Cooper, FNP, CORLN References: Clinical Practice Guideline: Tympanostomy tubes in children, Rosenfeld et al., American Academy of Otolaryngology Head and Neck Surgery Foundation
Pediatric ENT Guidelines Jane Cooper, FNP, CORLN References: Clinical Practice Guideline: Tympanostomy tubes in children, Rosenfeld et al., American Academy of Otolaryngology Head and Neck Surgery Foundation
Upper Respiratory Tract Infections / 42
 Upper Respiratory Tract Infections 1 Upper Respiratory Tract Infections Acute tonsillitispharyngitis Acute otitis media Acute sinusitis Common cold Acute laryngitis Otitis externa Mastoiditis Acute apiglottis
Upper Respiratory Tract Infections 1 Upper Respiratory Tract Infections Acute tonsillitispharyngitis Acute otitis media Acute sinusitis Common cold Acute laryngitis Otitis externa Mastoiditis Acute apiglottis
Telephone Number Home: Work: Cell:
 Page 1 of 7 Patient Name: DOB: Date: Address: Occupation: Telephone Number Home: Work: Cell: Emergency Contact: Relation: Telephone: Address: Referring Physician: Address: Telephone: ***ALL PATIENTS MUST
Page 1 of 7 Patient Name: DOB: Date: Address: Occupation: Telephone Number Home: Work: Cell: Emergency Contact: Relation: Telephone: Address: Referring Physician: Address: Telephone: ***ALL PATIENTS MUST
What is your diagnosis? a. Lymphocytic colitis. b. Collagenous colitis. c. Common variable immunodeficiency (CVID) associated colitis
 associated colitis") Case History A 24 year old male presented with fatigue, fever, watery diarrhea, and a cough with sputum production for the past three weeks. His past medical history was significant for recurrent bouts
Case History A 24 year old male presented with fatigue, fever, watery diarrhea, and a cough with sputum production for the past three weeks. His past medical history was significant for recurrent bouts
A. Incorrect! The duodenum drains to the superior mesenteric lymph nodes. B. Incorrect! The jejunum drains to the superior mesenteric lymph nodes.
 USMLE Step 1 Problem Drill 11: Immunology Question No. 1 of 10 1. A 67 year old man is discovered to have metastatic disease involving his inferior mesenteric lymph nodes. His primary cancer is most likely
USMLE Step 1 Problem Drill 11: Immunology Question No. 1 of 10 1. A 67 year old man is discovered to have metastatic disease involving his inferior mesenteric lymph nodes. His primary cancer is most likely