Medical management of Intersex disorders. Dr. Abdulmoein Al-Agha, Ass. Professor & Consultant Pediatric Endocrinologist KAAUH, Jeddah
|
|
|
- Darren Stokes
- 5 years ago
- Views:
Transcription
1 Medical management of Intersex disorders Dr. Abdulmoein Al-Agha, Ass. Professor & Consultant Pediatric Endocrinologist KAAUH, Jeddah
2 Is it a boy or a girl?
3 The birth of an intersex infant is often viewed as a major crisis by parents & other family members Pediatric endocrinologists can offer valuable support by helping the parents to understand sex differentiation & medical / surgical options that are available for their child Specifically, should inform parents about: 1) long-term cosmetic & functional outcomes associated with genital reconstruction 2) the need for long-term sex hormone replacement 3) possibilities for reproduction

4 Is it a boy or a girl?

5 Is it a boy or a girl?

6
7 The multidisciplinary team management Medical Surgical Psychological
8 Management of Congenital Adrenal Hyperplasia 1. Classical form (presentation since birth) 2. Non classical form ( presentation in childhood / adolescence due to mild enzyme deficiency) 3. Severe classical form ( with almost complete deficiency of enzymes Null mutation )
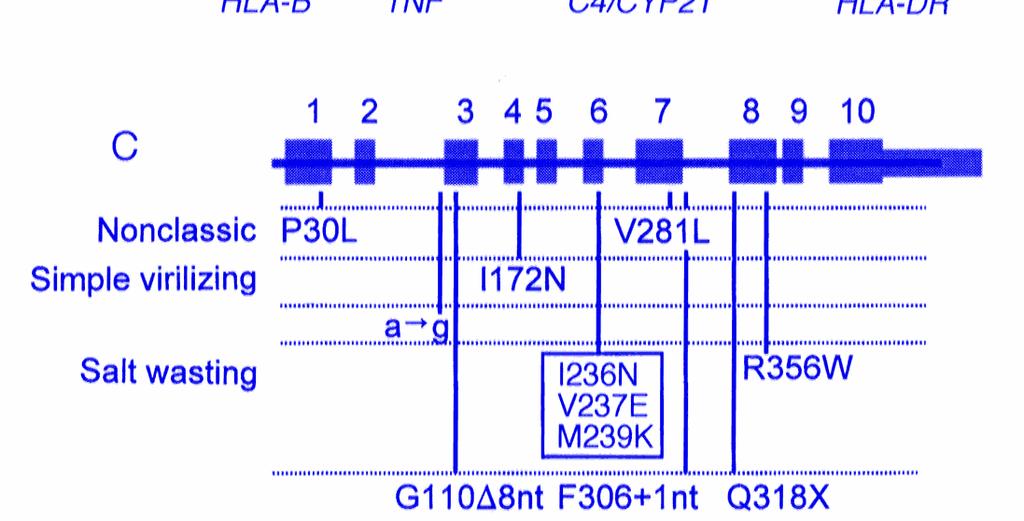
9 Genetics of 21- Hydroxylase Deficiency (Example for CAH) The gene encoding 21 hydroxylase (microsomal cytochrome P450) is called CYP21 Located on the short arm of chromosome 6 So far, 50 mutations in the CYP21 have been identified In general, there is a good correlation of genotype to phenotype (I.e correlation of the disease severity and the type of mutation)
10
11 Management of Congenital Adrenal Hyperplasia Classical form (presentation since birth)
12 Commonest enzyme deficiency is 21- hydroxylase Leads to the accumulation of: 17- hydroxyprogesterone Adrenal androgens (Androstendione, DHEA, DHEAS) Decreased production of glucocorticoid ± mineralocorticoid (salt wasting type) In salt-wasting CAH, additional severe renal salt loss occurs as a consequence of aldosterone deficiency

13 Congenital Adrenal Hyperplasia
14 Overproduction of androgens causes: Virilization Advanced skeletal maturation & early epiphyseal fusion Accelerated growth in childhood with final short as adult Management consists of substitution of cortisol ± aldosterone AND reduction of excessive androgen production Management of children with CAH is challenge to the endocrinologist regard to growth outcome
15 Management Hydrocortisone mg/m 2 /day divided into 2 3 doses In infancy & early childhood, additional sodium replacement is required together with Fludrocortisone mg / day (in salt losing types) Monitoring of growth, signs of androgen excess, pubertal development & blood pressure
16 Glucocorticoid replacement In children, the preferred cortisol replacement is hydrocortisone in doses of mg/m2/day in 2-3 divided doses These doses exceed physiological levels of cortisol secretion, which are 6 7 mg / m 2 /day in children The supra-physiological doses given to children with CAH seem to be required to adequately suppress adrenal androgens & to minimize the possibility of developing adrenal insufficiency
17 The short half-life of hydrocortisone minimizes growth suppression & other adverse side effects in comparison to longer acting, more potent steroids such as prednisone & dexamethasone Challenge is!! There is only a narrow therapeutic window in the treatment of CAH with glucocorticoid Older adolescents & adults may be treated with modest doses of prednisone ( mg daily in 2 divided doses) or dexamethasone ( mg given as 1-2 daily)
18 In over treatment with steroids: (Iatrogenic Cushing s syndrome) Short stature Truncal obesity Osteoporosis Over treatment is a greater risk when potent longer acting glucocorticoid (e.g. prednisone, or dexamethasone when are used in childhood) Under treatment with steroids leads to: Androgen excess with advancement of bone age, and reduced final height due to early epiphyseal closure
19 Patients should be monitored carefully for signs of iatrogenic Cushing s syndrome such as: Rapid weight gain Short stature Hypertension Pigmented striae & osteopenia Treatment efficacy (suppression of adrenal hormones) is assessed by monitoring of: ACTH (preferably at 0800 am physiological peak 17-OHP Androstenedione levels Testosterone is useful parameter in females & prepubertal males
20 Children should have annual bone age x-ray & careful monitoring of linear growth Despite careful monitoring & good patient compliance, most retrospective reviews indicate that final height averages 1 2 SDS below the population mean or the target height based on parental heights Hydrocortisone dose > 20 mg / m 2 / day is potentially detrimental to growth
21 Stress dosing Dose guidelines include tripling the maintenance dose of oral hydrocortisone (administered in three divided doses) in minor febrile illnesses If a patient is unable to tolerate oral medication, intramuscular hydrocortisone may be given For major surgery, administration of hydrocortisone (100 mg / m 2 / day) 4 intravenous doses is warranted for at least 24 h peri- and postoperatively before tapering over several days to a maintenance dose
22 Prenatal treatment Only mothers at risk for 21-hydroxylase Start treatment when pregnancy is confirmed Not after 9 weeks of gestation Dexamethasone 0.5mg TDS (not exceed 20 mcg/kg/d) Stop treatment: Male sex Unaffected female fetus (normal 17OHP & genotype)
23
24 Management of Congenital Adrenal Hyperplasia Severe classical form ( with almost complete deficiency of enzymes Null mutation )
25 New Treatment Approaches Instead of using high-dose hydrocortisone in order to suppress excessive androgens, instead; to use lower doses of hydrocortisone together with anti-androgens & aromatase enzyme inhibitors
26 Poly Pharmacy Therapy
27 Anti - Androgens Intra Adrenal blockage of androgen production Ketoconazole Blocks adrenal steroid production at several enzymatic steps Considered to be reversible medical adrenalectomy Peripheral blockage of androgen action Spirinolactone (aldactone) Cyproterone acetate (Androcur) Finasteride : 5 α- reductase enzyme inhibitor Flutamide: Androgen receptor-blockers
28 Aromatase Enzyme (CYP19) Aromatase enzyme is the enzyme responsible for the last step of estrogen biosynthesis Aromatase enzyme converts Androstedione to estrone Testosterone to estradiol Converts Testosterone into E2
29 Aromatase Inhibitors Testolactone (Teslac) is a competitive steroidal aromatase inhibitors Dose 20 mg/kg/day initially then 40 mg/kg/day divided into 4 doses Anastrozole (Arimidex) 3 rd. generation Aromatase inhibitor more potent and specific inhibitors of aromatase enzyme
30 Bilateral Adrenalectomy Bilateral adrenalectomy has been proposed recently as surgical treatment option for severe classic congenital adrenal hyperplasia To date, 5 operations have been reported; all were done in difficult-to-control cases & 1 was performed laparoscopically
31 Gene therapy Because 21-hydroxylase deficiency is an inherited metabolic defect, the question arises of the feasibility of gene therapy As discussed above, medical therapy, albeit not perfect, is effective and relatively inexpensive. High level expression would need to be targeted to the adrenal cortex, where adequate levels of steroid precursors are available. As the most difficult therapeutic goal to achieve is adequate suppression of adrenal androgens, expression would need to be sufficiently high to permit nearly normal levels of cortisol biosynthesis under both normal and stress conditions, and such levels of expression would need to be maintained indefinitely to be cost effective in comparison with conventional treatment. These criteria seem unlikely to be met for the foreseeable future
32 Management of Congenital Adrenal Hyperplasia Non classical form ( presentation in childhood / adolescence due to mild enzyme deficiency)
33 Individuals diagnosed with non-classic CAH should be offered treatment when they manifest signs or symptoms of androgen excess Low-dose glucocorticoid therapy may be initiated in children with: precocious pubarche, inappropriately early onset of body hair & odor, accompanied by advanced bone age Other common indications for treatment in Adolescents are: hirsutism, oligomenorrhea & acne
34 In adults: Infertile female patients diagnosed with nonclassic CAH should also be treated, as they may more readily become pregnant if the hormonal imbalance is the principal obstacle to conception Men with non-classic CAH may achieve improved sperm counts and fertility with glucocorticoid treatment Although rare, testicular enlargement in nonclassic males is also an indication for glucocorticoid therapy
35 132.8 cm


36 BA= 12 years Height = cm Weight = 33 kg

37

38

39

40

41
42 Management of other sexual differentiation disorders
43 Testosterone Replacement Therapy
44 Testosterone biosynthesis defects Five enzymes needed for conversion of cholesterol to testosterone: 1) P-450 scc (Lipoid adrenal hyperplasia) 2) 3 β- HSD 3) P-450 c17 4) P-450 c17 (17,20 lyase) 5) 17 β-hydroxysteroid dehydrogenase 1, 2 & 3 are needed for glucocorticoid synthesis
45 Testicular Aplasia / Hypoplasia Testicular dysgenesis (incomplete gonadal dysgenesis) PAIS Testicular vanishing syndrome Isolated micropenis
46 Intramuscular depot injections of testosterone esters are commonly used in males; another option is oral testosterone & transdermal preparations Patients with PAIS may require supraphysiologic doses of testosterone for optimal effect Low doses of IM testosterone at 50 mg once a month will bring about some degree of virilization & induce puberty without jeopardizing adult height potential Adolescents should be treated with long-acting injectable testosterone at low dose that increases over 18 to 24 months period from 50 mg monthly up to 200 mg q 2 to 4 wk
47 Potential adverse effects include fluid retention, acne, occasionally, transient gynecomastia Therapy prevents or reduces the risk of osteopenia, vasomotor instability, increases libido & prevents impotence Because they carry the risk of hepatocellular dysfunction or tumour formation, oral androgens should not be used
48 5 α - Reductase deficiency
49 DIHYDRO TESTOSTERONE (ANDRACTIN) Deficiency of 5 α - reductase has been shown to lead to micro penis & hypospadias It is unclear in what percentage of hypospadias cases this occurs, but it could be as much as 20% Applying dihydrotestosterone cream directly to the phallus bypasses the need for 5 alpha reductase Theoretically will promote penile growth without systemic side effects of testosterone injection therapy In PAIS applying high concentrations of the cream may overcome this deficiency
50 It is desirable to measure testosterone & dihydrotestosterone 3 days following HCG stimulation to determine the ratio of T: DHT 5 alpha reductase deficiency if plasma testosterone: dihydrotestosterone ratio >20 following HCG stimulation Dosage The cream to be applied twice / day for 2 months One turn of the tube delivers approximately 5 gm that should then be applied locally to the phallic shaft region The patient is then to be reassessed with measurement of stretched penile length
51 Risks The risks associated with dihydrotestosterone cream should be small The treatment is similar to giving testosterone injections with less systemic side effects of the medications, since it is applied locally as a cream Theoretical risk is that the cream may cause a long term down regulation of DHT receptors which may result in initial penile growth spurt with later decrease in the final penile length achieved at puberty
52 Estrogen Replacement Therapy
53 All 46,XY intersex patients who were reared female will require life-long hormone replacement therapy Except cases of 5 -reductase deficiency, 17- ketosteroid reductase deficiency, and PAIS, patients who were reared male CAIS after bilateral castration Early castration requires subsequent post-pubertal hormone replacement therapy Mixed gonadal dysgenesis with female rearing
54 Estrogen deficiency has potent, deleterious effects on the skeleton that can increase risk for stress fracture Estrogen deficiency also appears to promote fat accumulation There is evidence that hormone replacement attenuates the negative effects of hypogonadism on body composition & bone density which are mediated primarily by estrogens rather than progestins
55 Females with Hypogonadism require estrogen supplementation to induce pubertal changes and menses Doses: Start low dose of conjugated estrogen (Premarin mg) every other day initially at age of 14 to enhance bone growth then increase dose gradually over 2 years time A progestin is usually added after breakthrough bleeding develops or within 6-12 months of continuous estrogen Cycling with Provera (5-10 mg ) to induce regular menstruation There is no evidence that the addition of cyclic progesterone is beneficial in women without uterus

56
SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY
 1 SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY PBL SEMINAR: SEX HORMONES PART 1 An Overview What are steroid hormones? Steroid
1 SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY PBL SEMINAR: SEX HORMONES PART 1 An Overview What are steroid hormones? Steroid
DEFINITION: Masculinization of external genitalia in patients with normal 46XX karyotype.
 INTERSEX DISORDERS DEFINITION: Masculinization of external genitalia in patients with normal 46XX karyotype. - Degree of masculinization variable: - mild clitoromegaly - complete fusion of labia folds
INTERSEX DISORDERS DEFINITION: Masculinization of external genitalia in patients with normal 46XX karyotype. - Degree of masculinization variable: - mild clitoromegaly - complete fusion of labia folds
AMBIGUOUS GENITALIA & CONGENITAL ADRENALHYPERPLASIA
 AMBIGUOUS GENITALIA & CONGENITAL ADRENALHYPERPLASIA BY Dr Numair Ali sheikh FCPS PGT I Department Of Pediatrics BBH RWP AMBIGUOUS GENITALIA Children born with ambiguous genitalia may be subdivided in to
AMBIGUOUS GENITALIA & CONGENITAL ADRENALHYPERPLASIA BY Dr Numair Ali sheikh FCPS PGT I Department Of Pediatrics BBH RWP AMBIGUOUS GENITALIA Children born with ambiguous genitalia may be subdivided in to
IN SUMMARY HST 071 NORMAL & ABNORMAL SEXUAL DIFFERENTIATION Fetal Sex Differentiation Postnatal Diagnosis and Management of Intersex Abnormalities
 Harvard-MIT Division of Health Sciences and Technology HST.071: Human Reproductive Biology Course Director: Professor Henry Klapholz IN SUMMARY HST 071 Title: Fetal Sex Differentiation Postnatal Diagnosis
Harvard-MIT Division of Health Sciences and Technology HST.071: Human Reproductive Biology Course Director: Professor Henry Klapholz IN SUMMARY HST 071 Title: Fetal Sex Differentiation Postnatal Diagnosis
Dr. Nermine Salah El-Din Prof of Pediatrics
 Dr. Nermine Salah El-Din Prof of Pediatrics Diabetes Endocrine Metabolism Pediatric Unit (DEMPU) Children Hospital, Faculty of Medicine Cairo University Congenital adrenal hyperplasia is a common inherited
Dr. Nermine Salah El-Din Prof of Pediatrics Diabetes Endocrine Metabolism Pediatric Unit (DEMPU) Children Hospital, Faculty of Medicine Cairo University Congenital adrenal hyperplasia is a common inherited
Ambiguous genitalia (Disorders of sex development); is any case in which the external genitalia do not appear completely male or completely female.
; is any case in which the external genitalia do not appear completely male or completely female.") Ambiguous genitalia (Disorders of sex development); is any case in which the external genitalia do not appear completely male or completely female. Disorders of sex development (DSD); True hermaphrodite;
Ambiguous genitalia (Disorders of sex development); is any case in which the external genitalia do not appear completely male or completely female. Disorders of sex development (DSD); True hermaphrodite;
Laura Stewart, MD, FRCPC Clinical Associate Professor Division of Pediatric Endocrinology University of British Columbia
 Precocious Puberty Laura Stewart, MD, FRCPC Clinical Associate Professor Division of Pediatric Endocrinology University of British Columbia Faculty Disclosure Faculty: Laura Stewart No relationships with
Precocious Puberty Laura Stewart, MD, FRCPC Clinical Associate Professor Division of Pediatric Endocrinology University of British Columbia Faculty Disclosure Faculty: Laura Stewart No relationships with
Learning Objectives 4/17/2013. Toni Eimicke has no conflicts of interest or disclosures Heather Shanholtz has no conflicts of interest or disclosures
 OVERVIEW OF CONGENITAL ADRENAL HYPERPLASIA PATHOPHYSIOLOGY, LAB INTERPRETATION & MANAGEMENT Presented by: Toni Eimicke, MS, CPNP & Heather J Shanholtz, RN Pediatric Endocrinology Barbara Bush Children
OVERVIEW OF CONGENITAL ADRENAL HYPERPLASIA PATHOPHYSIOLOGY, LAB INTERPRETATION & MANAGEMENT Presented by: Toni Eimicke, MS, CPNP & Heather J Shanholtz, RN Pediatric Endocrinology Barbara Bush Children
Disorder name: Congenital Adrenal Hyperplasia Acronym: CAH
 Genetic Fact Sheets for Parents Draft Disorders Screening, Technology, and Research in Genetics is a multi-state project to improve information about the financial, ethical, legal, and social issues surrounding
Genetic Fact Sheets for Parents Draft Disorders Screening, Technology, and Research in Genetics is a multi-state project to improve information about the financial, ethical, legal, and social issues surrounding
Case Based Urology Learning Program
 Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 3 CBULP 2011 019 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 3 CBULP 2011 019 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
ComprehensivePLUS Hormone Profile with hgh
 OLEBound400: 801 SW 16th St Suite 126 Renton WA 98057 425.271.8689 425.271.8674 (Fax) ComprehensivePLUS Hormone Profile with hgh Doctor ID Patient Name 6206 Doe, Jane Age Sex Date of Birth 44 F Date Collected
OLEBound400: 801 SW 16th St Suite 126 Renton WA 98057 425.271.8689 425.271.8674 (Fax) ComprehensivePLUS Hormone Profile with hgh Doctor ID Patient Name 6206 Doe, Jane Age Sex Date of Birth 44 F Date Collected
When testes make no testosterone: Identifying a rare cause of 46, XY female phenotype in adulthood
 When testes make no testosterone: Identifying a rare cause of 46, XY female phenotype in adulthood Gardner DG, Shoback D. Greenspan's Basic & Clinical Endocrinology, 10e; 2017 Sira Korpaisarn, MD Endocrinology
When testes make no testosterone: Identifying a rare cause of 46, XY female phenotype in adulthood Gardner DG, Shoback D. Greenspan's Basic & Clinical Endocrinology, 10e; 2017 Sira Korpaisarn, MD Endocrinology
PRENATAL TREATMENT AND FERTILITY OF FEMALE PATIENTS WITH CONGENITAL ADRENAL HYPERPLASIA
 PRENATAL TREATMENT AND FERTILITY OF FEMALE PATIENTS WITH CONGENITAL ADRENAL HYPERPLASIA Nguyen Ngoc Khanh, Vu Chi Dung et al Vietnam Children s Hospital (VCH) Hanoi, Vietnam Outline Intruduction Prenatal
PRENATAL TREATMENT AND FERTILITY OF FEMALE PATIENTS WITH CONGENITAL ADRENAL HYPERPLASIA Nguyen Ngoc Khanh, Vu Chi Dung et al Vietnam Children s Hospital (VCH) Hanoi, Vietnam Outline Intruduction Prenatal
SEX STERIOD HORMONES I: An Overview. University of PNG School of Medicine & Health Sciences Division of Basic Medical Sciences PBL MBBS III VJ Temple
 SEX STERIOD HORMONES I: An Overview University of PNG School of Medicine & Health Sciences Division of Basic Medical Sciences PBL MBBS III VJ Temple 1 What are the Steroid hormones? Hormones synthesized
SEX STERIOD HORMONES I: An Overview University of PNG School of Medicine & Health Sciences Division of Basic Medical Sciences PBL MBBS III VJ Temple 1 What are the Steroid hormones? Hormones synthesized
Approach to Disorders of Sex Development (DSD)
") Approach to Disorders of Sex Development (DSD) Old name: The Approach to Intersex Disorders Dr. Abdulmoein Al-Agha, FRCP Ass. Professor & Consultant Pediatric Endocrinologist, KAUH, Erfan Hospital & Ibn
Approach to Disorders of Sex Development (DSD) Old name: The Approach to Intersex Disorders Dr. Abdulmoein Al-Agha, FRCP Ass. Professor & Consultant Pediatric Endocrinologist, KAUH, Erfan Hospital & Ibn
Hyperandrogenism. Dr Jack Biko. MB. BCh (Wits), MMED O & G (Pret), FCOG (SA), Dip Advanced Endoscopic Surgery(Kiel, Germany)
, MMED O & G (Pret), FCOG (SA), Dip Advanced Endoscopic Surgery(Kiel, Germany)") Hyperandrogenism Dr Jack Biko MB. BCh (Wits), MMED O & G (Pret), FCOG (SA), Dip Advanced Endoscopic Surgery(Kiel, Germany) 2012 Hyperandrogenism Excessive production of androgens Adrenal glands main source
Hyperandrogenism Dr Jack Biko MB. BCh (Wits), MMED O & G (Pret), FCOG (SA), Dip Advanced Endoscopic Surgery(Kiel, Germany) 2012 Hyperandrogenism Excessive production of androgens Adrenal glands main source
DEVELOPMENT (DSD) 1 4 DISORDERS OF SEX
 1 4 DISORDERS OF SEX") Wit JM, Ranke MB, Kelnar CJH (eds): ESPE classification of paediatric endocrine diagnosis. 4. Disorders of sex development (DSD). Horm Res 2007;68(suppl 2):21 24 ESPE Code Diagnosis OMIM ICD 10 4 DISORDERS
Wit JM, Ranke MB, Kelnar CJH (eds): ESPE classification of paediatric endocrine diagnosis. 4. Disorders of sex development (DSD). Horm Res 2007;68(suppl 2):21 24 ESPE Code Diagnosis OMIM ICD 10 4 DISORDERS
FLASH CARDS. Kalat s Book Chapter 11 Alphabetical
 FLASH CARDS www.biologicalpsych.com Kalat s Book Chapter 11 Alphabetical alpha-fetoprotein alpha-fetoprotein Alpha-Fetal Protein (AFP) or alpha-1- fetoprotein. During a prenatal sensitive period, estradiol
FLASH CARDS www.biologicalpsych.com Kalat s Book Chapter 11 Alphabetical alpha-fetoprotein alpha-fetoprotein Alpha-Fetal Protein (AFP) or alpha-1- fetoprotein. During a prenatal sensitive period, estradiol
BIOSYNTHESIS OF STEROID HORMONES
 BIOSYNTHESIS OF STEROID HORMONES Sri Widia A Jusman Department of Biochemistry & Molecular Biology FMUI sw/steroidrepro/inter/08 1 STEROID HORMONES Progestins (21 C) Glucocorticoids (21 C) Mineralocorticoids
BIOSYNTHESIS OF STEROID HORMONES Sri Widia A Jusman Department of Biochemistry & Molecular Biology FMUI sw/steroidrepro/inter/08 1 STEROID HORMONES Progestins (21 C) Glucocorticoids (21 C) Mineralocorticoids
AMBIGUOUS GENITALIA. Dr. HAKIMI, SpAK. Dr. MELDA DELIANA, SpAK
 AMBIGUOUS GENITALIA (DISORDERS OF SEXUAL DEVELOPMENT) Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA Pediatric Endocrinology division USU/H. ADAM MALIK HOSPITAL 1 INTRODUCTION Normal
AMBIGUOUS GENITALIA (DISORDERS OF SEXUAL DEVELOPMENT) Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA Pediatric Endocrinology division USU/H. ADAM MALIK HOSPITAL 1 INTRODUCTION Normal
3 year old boy with puberty. Katie Stanley, MD August 1, 2013
 3 year old boy with puberty Katie Stanley, MD August 1, 2013 Initial presentation 3 and 11/12 year old boy with signs of puberty Presented to outside endocrinologist in 2002 with: Pubic hair since 2.5
3 year old boy with puberty Katie Stanley, MD August 1, 2013 Initial presentation 3 and 11/12 year old boy with signs of puberty Presented to outside endocrinologist in 2002 with: Pubic hair since 2.5
Paul Hofman. Professor. Paediatrician Endocrinologist Liggins Institute, The University of Auckland, Starship Children Hospital, Auckland
 Professor Paul Hofman Paediatrician Endocrinologist Liggins Institute, The University of Auckland, Starship Children Hospital, Auckland 14:00-14:55 WS #108: Common pubertal variants how to distinguish
Professor Paul Hofman Paediatrician Endocrinologist Liggins Institute, The University of Auckland, Starship Children Hospital, Auckland 14:00-14:55 WS #108: Common pubertal variants how to distinguish
Clinical Guideline ADRENARCHE MANAGEMENT OF CHILDREN PRESENTING WITH SIGNS OF EARLY ONSET PUBIC HAIR/BODY ODOUR/ACNE
 Clinical Guideline ADRENARCHE MANAGEMENT OF CHILDREN PRESENTING WITH SIGNS OF EARLY ONSET PUBIC HAIR/BODY ODOUR/ACNE Includes guidance for the distinction between adrenarche, precocious puberty and other
Clinical Guideline ADRENARCHE MANAGEMENT OF CHILDREN PRESENTING WITH SIGNS OF EARLY ONSET PUBIC HAIR/BODY ODOUR/ACNE Includes guidance for the distinction between adrenarche, precocious puberty and other
Polycystic Ovarian Syndrome (PCOS) LOGO
 LOGO") Polycystic Ovarian Syndrome (PCOS) Ma qianhong Ob/Gyn Department LOGO Contents Epidemiology and Definition Pathophysiology, Endocrinological Features Diagnostic Criteria Treatment Prognosis Introduction
Polycystic Ovarian Syndrome (PCOS) Ma qianhong Ob/Gyn Department LOGO Contents Epidemiology and Definition Pathophysiology, Endocrinological Features Diagnostic Criteria Treatment Prognosis Introduction
Action of reproductive hormones through the life span 9/22/99
 Action of reproductive hormones through the life span Do reproductive hormones affect the life span? One hypothesis about the rate of aging asserts that there is selective pressure for either high rate
Action of reproductive hormones through the life span Do reproductive hormones affect the life span? One hypothesis about the rate of aging asserts that there is selective pressure for either high rate
Bios 90/95. Jennifer Swann, PhD
 Sexual Differentiation Fall 2007 Bios 90/95 Jennifer Swann, PhD Dept Biol Sci, Lehigh University Why have sexes? What determines sex? Environment Genetics Hormones What causes these differences? The true
Sexual Differentiation Fall 2007 Bios 90/95 Jennifer Swann, PhD Dept Biol Sci, Lehigh University Why have sexes? What determines sex? Environment Genetics Hormones What causes these differences? The true
Adrenal Insufficiency During Pregnancy
 Disclosures Adrenal Insufficiency During Pregnancy Research funding from Diurnal Limited via NIH CRADA mechanism Deborah P. Merke, M.D., M.S. Bethesda, MD Outline Primary Adrenal Insufficiency Physiological
Disclosures Adrenal Insufficiency During Pregnancy Research funding from Diurnal Limited via NIH CRADA mechanism Deborah P. Merke, M.D., M.S. Bethesda, MD Outline Primary Adrenal Insufficiency Physiological
SAMPLE REPORT. Order Number: PATIENT. Age: 40 Sex: F MRN:
 Patient: Age: 40 Sex: F MRN: SAMPLE PATIENT Order Number: Completed: Received: Collected: SAMPLE REPORT Progesterone ng/ml 0.34 0.95 21.00 DHEA-S mcg/dl Testosterone ng/ml 48 35 0.10 0.54 0.80 430 Sex
Patient: Age: 40 Sex: F MRN: SAMPLE PATIENT Order Number: Completed: Received: Collected: SAMPLE REPORT Progesterone ng/ml 0.34 0.95 21.00 DHEA-S mcg/dl Testosterone ng/ml 48 35 0.10 0.54 0.80 430 Sex
International Journal of Health Sciences and Research ISSN:
 International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article Congenital Adrenal Hyperplasia in Saudi Arabia: The Biochemical Characteristics Nasir A. M.
International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article Congenital Adrenal Hyperplasia in Saudi Arabia: The Biochemical Characteristics Nasir A. M.
Hd Hydroxylase. Cholesterol. 17-OH Pregnenolne DHEA Andrstendiol. Pregnenolone. 17-OH Progestrone. Androstendione. Progestrone.
 PATHOPHISIOLOGY OF SEX HORMONES R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES Cholesterol Pregnenolone 17-OH 17βHSD Pregnenolne DHEA
PATHOPHISIOLOGY OF SEX HORMONES R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES Cholesterol Pregnenolone 17-OH 17βHSD Pregnenolne DHEA
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Puberty and Pubertal Disorders Part 2: Precocious Puberty. These podcasts are designed to give medical students an overview
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Puberty and Pubertal Disorders Part 2: Precocious Puberty. These podcasts are designed to give medical students an overview
Let s Talk About Hormones!
 Let s Talk About Hormones! This lesson was created by Serena Reves and Nichelle Penney, with materials from the BCTF and The Pride Education Network. Hormones are responsible for the regulation of many
Let s Talk About Hormones! This lesson was created by Serena Reves and Nichelle Penney, with materials from the BCTF and The Pride Education Network. Hormones are responsible for the regulation of many
Polycystic Ovary Syndrome HEATHER BURKS, MD OU PHYSICIANS REPRODUCTIVE MEDICINE SEPTEMBER 21, 2018
 Polycystic Ovary Syndrome HEATHER BURKS, MD OU PHYSICIANS REPRODUCTIVE MEDICINE SEPTEMBER 21, 2018 Learning Objectives At the conclusion of this lecture, learners should: 1) Know the various diagnostic
Polycystic Ovary Syndrome HEATHER BURKS, MD OU PHYSICIANS REPRODUCTIVE MEDICINE SEPTEMBER 21, 2018 Learning Objectives At the conclusion of this lecture, learners should: 1) Know the various diagnostic
TESTOSTERONE DEFINITION
 DEFINITION A hormone that is a hydroxyl steroid ketone (C19H28O2) produced especially by the testes or made synthetically and that is responsible for inducing and maintaining male secondary sex characteristics.
DEFINITION A hormone that is a hydroxyl steroid ketone (C19H28O2) produced especially by the testes or made synthetically and that is responsible for inducing and maintaining male secondary sex characteristics.
Biology of Reproduction-Biol 326
 Biology of Reproduction-Biol 326 READ ALL INSTRUCTIONS CAREFULLY. ANSWER ALL THE QUESTIONS ON THE ANSWER SHEET. THE ANSWER ON THE ANSWER SHEET IS YOUR OFFICIAL ANSWER REGARDLESS OF WHAT YOU MARK ON THE
Biology of Reproduction-Biol 326 READ ALL INSTRUCTIONS CAREFULLY. ANSWER ALL THE QUESTIONS ON THE ANSWER SHEET. THE ANSWER ON THE ANSWER SHEET IS YOUR OFFICIAL ANSWER REGARDLESS OF WHAT YOU MARK ON THE
John Sutton, DO, FACOI, FACE, CCD. Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989
 John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 Gonadal Physiology and Disease 3 No Disclosures Gonadal Axis Hypothalamic-pituitary-gonadal Feedback mechanisms
John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 Gonadal Physiology and Disease 3 No Disclosures Gonadal Axis Hypothalamic-pituitary-gonadal Feedback mechanisms
Growth hormone therapy in a girl with Turner syndrome showing a large increase over the initially predicted ht of 4 5
 Disorders of Growth and Puberty: How to Recognize the Normal Variants vs Patients Who Need to be Evaluated Paul Kaplowitz, M.D Pediatric Endocrinology. VCU School of Medicine Interpretation of Growth Charts
Disorders of Growth and Puberty: How to Recognize the Normal Variants vs Patients Who Need to be Evaluated Paul Kaplowitz, M.D Pediatric Endocrinology. VCU School of Medicine Interpretation of Growth Charts
PUBERTY. Preetha Krishnamoorthy. Division of Pediatric Endocrinology
 PUBERTY Preetha Krishnamoorthy Division of Pediatric Endocrinology Case 1 8-year-old girl referred for breast development noted by mom What do you want to know? Normal or abnormal? What if this was an
PUBERTY Preetha Krishnamoorthy Division of Pediatric Endocrinology Case 1 8-year-old girl referred for breast development noted by mom What do you want to know? Normal or abnormal? What if this was an
Biology of Reproduction- Zool 346 Exam 2
 Biology of Reproduction- Zool 346 Exam 2 ANSWER ALL THE QUESTIONS ON THE ANSWER SHEET. THE ANSWER ON THE ANSWER SHEET IS YOUR OFFICIAL ANSWER. Some critical words are boldfaced. This exam is 7 pages long.
Biology of Reproduction- Zool 346 Exam 2 ANSWER ALL THE QUESTIONS ON THE ANSWER SHEET. THE ANSWER ON THE ANSWER SHEET IS YOUR OFFICIAL ANSWER. Some critical words are boldfaced. This exam is 7 pages long.
UCL. Gerard Conway. Treatment of AIS patients in multidisciplinary teams in UK. Tratamiento del SIA en equipos multidisciplinares en el Reino Unido
 UCL Treatment of AIS patients in multidisciplinary teams in UK Tratamiento del SIA en equipos multidisciplinares en el Reino Unido Gerard Conway London, UK University College London Hospitals University
UCL Treatment of AIS patients in multidisciplinary teams in UK Tratamiento del SIA en equipos multidisciplinares en el Reino Unido Gerard Conway London, UK University College London Hospitals University
Chapter 18 Development. Sexual Differentiation
 Chapter 18 Development Sexual Differentiation There Are Many Levels of Sex Determination Chromosomal Sex Gonadal Sex Internal Sex Organs External Sex Organs Brain Sex Gender Identity Gender Preference
Chapter 18 Development Sexual Differentiation There Are Many Levels of Sex Determination Chromosomal Sex Gonadal Sex Internal Sex Organs External Sex Organs Brain Sex Gender Identity Gender Preference
Hearing on SJR13 -- Proposes to amend the Nevada Constitution by repealing the limitation on the recognition of marriage.
 Written statement of Lauren A. Scott- Executive Director Equality Nevada. 1350 Freeport Blvd, #107 Sparks, Nevada 89431 Testimony and Statement for the Record of Hearing on SJR13 -- Proposes to amend the
Written statement of Lauren A. Scott- Executive Director Equality Nevada. 1350 Freeport Blvd, #107 Sparks, Nevada 89431 Testimony and Statement for the Record of Hearing on SJR13 -- Proposes to amend the
Synthesis of sex steroids
 Synthesis of sex steroids CH 3 NAD(P)H NAD(P)+ Dehidroepiandroszteron Androszténdion 17- -hidroxiszteroid dehidrogenáz CH 3 dehydroepiandrosterone Dehidroepiandroszteron (DHEA) 3SDH Koleszterin CH 3 aromatase
Synthesis of sex steroids CH 3 NAD(P)H NAD(P)+ Dehidroepiandroszteron Androszténdion 17- -hidroxiszteroid dehidrogenáz CH 3 dehydroepiandrosterone Dehidroepiandroszteron (DHEA) 3SDH Koleszterin CH 3 aromatase
Precocious Puberty. Dr. Abdulmoein Eid Al-Agha Consultant, Pediatric Endocrinologist, King Abdul Aziz University Hospital, Jeddah, Saudi Arabia
 Precocious Puberty Dr. Abdulmoein Eid Al-Agha Consultant, Pediatric Endocrinologist, King Abdul Aziz University Hospital, Jeddah, Saudi Arabia Discussion points When to say this child is having Precocious
Precocious Puberty Dr. Abdulmoein Eid Al-Agha Consultant, Pediatric Endocrinologist, King Abdul Aziz University Hospital, Jeddah, Saudi Arabia Discussion points When to say this child is having Precocious
Safe Harbor Statement
 Safe Harbor Statement These slides contain forward-looking statements based on estimates and assumptions by our management that, although we believe to be reasonable, are inherently uncertain. Forward-looking
Safe Harbor Statement These slides contain forward-looking statements based on estimates and assumptions by our management that, although we believe to be reasonable, are inherently uncertain. Forward-looking
Precocious Puberty. Disclosures. No financial disclosures 2/28/2019
 Precocious Puberty Bracha Goldsweig, MD Pediatric Endocrinologist Children s Hospital and Medical Center, Omaha, NE University of Nebraska Medical Center Disclosures No financial disclosures 1 Objectives
Precocious Puberty Bracha Goldsweig, MD Pediatric Endocrinologist Children s Hospital and Medical Center, Omaha, NE University of Nebraska Medical Center Disclosures No financial disclosures 1 Objectives
Therapeutic Cohort Results
 Patient: PAGE LOVE DOB: January 11, 1983 Sex: F MRN: 1232704193 Order Number: J9020008 Completed: July 08, 2016 Received: July 02, 2016 Collected: July 01, 2016 Aum Healing Center Sarika Arora MD 332 Newbury
Patient: PAGE LOVE DOB: January 11, 1983 Sex: F MRN: 1232704193 Order Number: J9020008 Completed: July 08, 2016 Received: July 02, 2016 Collected: July 01, 2016 Aum Healing Center Sarika Arora MD 332 Newbury
Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone
 Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Prof.Dr. Nabil Lymon Head of Internal Medicine Department
 By Prof.Dr. Nabil Lymon Head of Internal Medicine Department Definitions: Hirsutism: Is the presence of terminal hair in androgendependent sites where hair does not normally grow in women. This hair growth
By Prof.Dr. Nabil Lymon Head of Internal Medicine Department Definitions: Hirsutism: Is the presence of terminal hair in androgendependent sites where hair does not normally grow in women. This hair growth
ADRENAL GLANDS HORMONES
 ADRNAL GLANDS HORMONS Glands Cortex 80% mesoderm Mineralococorticoids Glucocorticoids (phenylethanolamine N- methyl transferase) A Sex Hormones Catecholamines Medulla 20% PNMT, N neuroectoderm N PNMT V
ADRNAL GLANDS HORMONS Glands Cortex 80% mesoderm Mineralococorticoids Glucocorticoids (phenylethanolamine N- methyl transferase) A Sex Hormones Catecholamines Medulla 20% PNMT, N neuroectoderm N PNMT V
Sexual Development. 6 Stages of Development
 6 Sexual Development 6 Stages of Development Development passes through distinct stages, the first of which is fertilization, when one sperm enters one ovum. To enter an ovum, a sperm must undergo the
6 Sexual Development 6 Stages of Development Development passes through distinct stages, the first of which is fertilization, when one sperm enters one ovum. To enter an ovum, a sperm must undergo the
Corticosteroids. Hawler Medical University College of Medicine Department of Pharmacology and Biophysics Dr.Susan Abdulkadir Farhadi MSc Pharmacology
 Corticosteroids Hawler Medical University College of Medicine Department of Pharmacology and Biophysics Dr.Susan Abdulkadir Farhadi MSc Pharmacology Objectives By the end of this lecture you should be
Corticosteroids Hawler Medical University College of Medicine Department of Pharmacology and Biophysics Dr.Susan Abdulkadir Farhadi MSc Pharmacology Objectives By the end of this lecture you should be
Endocrine Steroids 2. Signal transduction 3. Prostaglandins
 Endocrine - 2 1. Steroids 2. Signal transduction 3. Prostaglandins Estrogen Menopause (pause in the menes) ["change of life" at about 50] - lack of estrogen. (Some hysterectomy or ovarian cancer surgeries
Endocrine - 2 1. Steroids 2. Signal transduction 3. Prostaglandins Estrogen Menopause (pause in the menes) ["change of life" at about 50] - lack of estrogen. (Some hysterectomy or ovarian cancer surgeries
74. Hormone synthesis in the adrenal cortex. The glucocorticoids: biosynthesis, regulation, effects. Adrenal cortex is vital for life!
 74. Hormone synthesis in the adrenal cortex. The glucocorticoids: biosynthesis, regulation, effects. Adrenal cortex is vital for life! 5 g each Zona glomerulosa : Mineralocorticoids ALDOSTERON Zona fasciculata:
74. Hormone synthesis in the adrenal cortex. The glucocorticoids: biosynthesis, regulation, effects. Adrenal cortex is vital for life! 5 g each Zona glomerulosa : Mineralocorticoids ALDOSTERON Zona fasciculata:
One Day Hormone Check
 One Day Hormone Check DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Salivary Hormone Results Estradiol pmol/l >3330.0 Testosterone pmol/l
One Day Hormone Check DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Salivary Hormone Results Estradiol pmol/l >3330.0 Testosterone pmol/l
Reproductive System. Testes. Accessory reproductive organs. gametogenesis hormones. Reproductive tract & Glands
 Reproductive System Testes gametogenesis hormones Accessory reproductive organs Reproductive tract & Glands transport gametes provide nourishment for gametes Hormonal regulation in men Hypothalamus - puberty
Reproductive System Testes gametogenesis hormones Accessory reproductive organs Reproductive tract & Glands transport gametes provide nourishment for gametes Hormonal regulation in men Hypothalamus - puberty
Goals. Disorders of Sex Development (Intersex): An Overview. Joshua May, MD Pediatric Endocrinology
: An Overview. Joshua May, MD Pediatric Endocrinology") Disorders of Sex Development (Intersex): An Overview Joshua May, MD Pediatric Endocrinology Murphy, et al., J Ped Adol Gynecol, 2011 Goals Objectives: Participants will be able to: 1. Apply the medical
Disorders of Sex Development (Intersex): An Overview Joshua May, MD Pediatric Endocrinology Murphy, et al., J Ped Adol Gynecol, 2011 Goals Objectives: Participants will be able to: 1. Apply the medical
Information leaflet for patients and families. Congenital Adrenal Hyperplasia (CAH)
") Information leaflet for patients and families Congenital Adrenal Hyperplasia (CAH) What is CAH? CAH is a disorder causing impaired hormone production from the adrenal glands. Hormones are chemical messengers
Information leaflet for patients and families Congenital Adrenal Hyperplasia (CAH) What is CAH? CAH is a disorder causing impaired hormone production from the adrenal glands. Hormones are chemical messengers
Sexual Differentiation Fall 2008 Bios 90
 Sexual Differentiation Fall 2008 Bios 90 Jennifer Swann, Professor Dept Biol Sci, Lehigh University Asexual reproduction Budding : offspring develop as a growth on the body of the parent jellyfishes, echinoderms,
Sexual Differentiation Fall 2008 Bios 90 Jennifer Swann, Professor Dept Biol Sci, Lehigh University Asexual reproduction Budding : offspring develop as a growth on the body of the parent jellyfishes, echinoderms,
Hearing on SJR13 -- Proposes to amend the Nevada Constitution by repealing the limitation on the recognition of marriage.
 Written statement of Lauren A. Scott- Executive Director Equality Nevada 1350 Freeport Blvd, #107 Sparks, Nevada 89431 Testimony and Statement for the Record of Hearing on SJR13 -- Proposes to amend the
Written statement of Lauren A. Scott- Executive Director Equality Nevada 1350 Freeport Blvd, #107 Sparks, Nevada 89431 Testimony and Statement for the Record of Hearing on SJR13 -- Proposes to amend the
GONADAL FUNCTION: An Overview
 GONADAL FUNCTION: An Overview University of PNG School of Medicine & Health Sciences Division of Basic Medical Sciences Clinical Biochemistry BMLS III & BDS IV VJ Temple 1 What are the Steroid hormones?
GONADAL FUNCTION: An Overview University of PNG School of Medicine & Health Sciences Division of Basic Medical Sciences Clinical Biochemistry BMLS III & BDS IV VJ Temple 1 What are the Steroid hormones?
CUSHING S SYNDROME THE FACTS YOU NEED TO KNOW
 CUSHING S SYNDROME THE FACTS YOU NEED TO KNOW Written by: Paul Margulies, MD, FACE, FACP, Medical Director, NADF. Clinical Associate Professor of Medicine, Zucker School of Medicine at Hofstra/Northwell.
CUSHING S SYNDROME THE FACTS YOU NEED TO KNOW Written by: Paul Margulies, MD, FACE, FACP, Medical Director, NADF. Clinical Associate Professor of Medicine, Zucker School of Medicine at Hofstra/Northwell.
Reproductive physiology
 Reproductive physiology Sex hormones: Androgens Estrogens Gestagens Learning objectives 86 (also 90) Sex Genetic sex Gonadal sex Phenotypic sex XY - XX chromosomes testes - ovaries external features Tha
Reproductive physiology Sex hormones: Androgens Estrogens Gestagens Learning objectives 86 (also 90) Sex Genetic sex Gonadal sex Phenotypic sex XY - XX chromosomes testes - ovaries external features Tha
Transitions For the CAH Patient
 Transitions For the CAH Patient Richard J. Auchus, M.D., Ph.D. Division of Metabolism, Endocrinology & Diabetes Department of Internal Medicine DSD Program University of Michigan Disclosures Contracted
Transitions For the CAH Patient Richard J. Auchus, M.D., Ph.D. Division of Metabolism, Endocrinology & Diabetes Department of Internal Medicine DSD Program University of Michigan Disclosures Contracted
The menstrual Cycle. François Pralong
 The menstrual Cycle François Pralong Services d Endocrinologie, Diabétologie et Métabolisme, Hôpitaux Universitaires de Genève et Lausanne Centre des Maladies CardioVasculaires et Métaboliques, Lausanne
The menstrual Cycle François Pralong Services d Endocrinologie, Diabétologie et Métabolisme, Hôpitaux Universitaires de Genève et Lausanne Centre des Maladies CardioVasculaires et Métaboliques, Lausanne
Congenital Adrenal Hyperplasia
 NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health. Feingold KR, Anawalt B, Boyce A, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.;
NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health. Feingold KR, Anawalt B, Boyce A, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.;
Topic No. & Title: Topic 4 Biosynthesis and secretion of adrenal, ovarian and testicular hormones-factors influencing secretion
 [Academic Script] Biosynthesis and secretion of adrenal, ovarian and testicular hormones-factors influencing secretion Subject: Zoology Course: B.Sc. 2 nd Year Paper No. & Title: Z-203B Vertebrate Endocrinology
[Academic Script] Biosynthesis and secretion of adrenal, ovarian and testicular hormones-factors influencing secretion Subject: Zoology Course: B.Sc. 2 nd Year Paper No. & Title: Z-203B Vertebrate Endocrinology
Therapeutic Cohort Results
 Patient: SAMPLE PATIENT DOB: Sex: MRN: Menopause Plus - Salivary Profile Therapeutic Cohort Results Hormone Average Result QUINTILE DISTRIBUTION 1st 2nd 3rd 4th 5th Therapeutic Range* Estradiol (E2) 8.7
Patient: SAMPLE PATIENT DOB: Sex: MRN: Menopause Plus - Salivary Profile Therapeutic Cohort Results Hormone Average Result QUINTILE DISTRIBUTION 1st 2nd 3rd 4th 5th Therapeutic Range* Estradiol (E2) 8.7
Estrogens and progestogens
 Estrogens and progestogens Estradiol and Progesterone hormones produced by the gonads are necessary for: conception embryonic maturation development of primary and secondary sexual characteristics at puberty.
Estrogens and progestogens Estradiol and Progesterone hormones produced by the gonads are necessary for: conception embryonic maturation development of primary and secondary sexual characteristics at puberty.
Chapter 16: Steroid Hormones (Lecture 17)
") Chapter 16: Steroid Hormones (Lecture 17) A) 21 or fewer carbon atoms B) Precursor: 27 carbon cholesterol C) major classes of steroid hormones 1) progestagens a) progesterone- prepares lining of uterus
Chapter 16: Steroid Hormones (Lecture 17) A) 21 or fewer carbon atoms B) Precursor: 27 carbon cholesterol C) major classes of steroid hormones 1) progestagens a) progesterone- prepares lining of uterus
Reproductive DHEA Analyte Information
 Reproductive DHEA Analyte Information - 1 - DHEA Introduction DHEA (dehydroepiandrosterone), together with other important steroid hormones such as testosterone, DHT (dihydrotestosterone) and androstenedione,
Reproductive DHEA Analyte Information - 1 - DHEA Introduction DHEA (dehydroepiandrosterone), together with other important steroid hormones such as testosterone, DHT (dihydrotestosterone) and androstenedione,
Male Hypogonadism. Types and causes of hypogonadism. What is male hypogonadism? Symptoms. Testosterone production. Patient Information.
 Patient Information English 31 Male Hypogonadism The underlined terms are listed in the glossary. What is male hypogonadism? Male hypogonadism means the testicles do not produce enough of the male sex
Patient Information English 31 Male Hypogonadism The underlined terms are listed in the glossary. What is male hypogonadism? Male hypogonadism means the testicles do not produce enough of the male sex
2. Which male target tissues respond to testosterone, and which require dihydrotestosterone?
 308 PHYSIOLOGY CASES AND PROBLEMS Case 56 Male Pseudohermaphroditism: Sa-Reductase Deficiency Fourteen years ago, Wally and Wanda Garvey, who live in rural North Carolina, had their first child. The baby
308 PHYSIOLOGY CASES AND PROBLEMS Case 56 Male Pseudohermaphroditism: Sa-Reductase Deficiency Fourteen years ago, Wally and Wanda Garvey, who live in rural North Carolina, had their first child. The baby
The menstrual cycle. François Pralong
 The menstrual cycle François Pralong Services d Endocrinologie, Diabétologie et Métabolisme, Hôpitaux Universitaires de Genève et Lausanne Centre des Maladies CardioVasculaires et Métaboliques, Lausanne
The menstrual cycle François Pralong Services d Endocrinologie, Diabétologie et Métabolisme, Hôpitaux Universitaires de Genève et Lausanne Centre des Maladies CardioVasculaires et Métaboliques, Lausanne
Disordered Sex Differentiation Mixed gonadal dysgenesis Congenital adrenal hyperplasia Mixed gonadal dysgenesis
 Disordered Sex Differentiation DSD has superceded intersex in describing genital anomalies in childhood DSD results from hormonal imbalances due to (i) abnormal genetic status, (ii) enzyme defects, or
Disordered Sex Differentiation DSD has superceded intersex in describing genital anomalies in childhood DSD results from hormonal imbalances due to (i) abnormal genetic status, (ii) enzyme defects, or
Reproductive DHEA-S Analyte Information
 Reproductive DHEA-S Analyte Information - 1 - DHEA-S Introduction DHEA-S, DHEA sulfate or dehydroepiandrosterone sulfate, it is a metabolite of dehydroepiandrosterone (DHEA) resulting from the addition
Reproductive DHEA-S Analyte Information - 1 - DHEA-S Introduction DHEA-S, DHEA sulfate or dehydroepiandrosterone sulfate, it is a metabolite of dehydroepiandrosterone (DHEA) resulting from the addition
Dr Stella Milsom. Endocrinologist Fertility Associates Auckland. 12:30-12:40 When Puberty is PCO
 Dr Stella Milsom Endocrinologist Fertility Associates Auckland 12:30-12:40 When Puberty is PCO Puberty or Polycystic Ovary Syndrome? Stella Milsom Endocrinologist Auckland DHB, University of Auckland,
Dr Stella Milsom Endocrinologist Fertility Associates Auckland 12:30-12:40 When Puberty is PCO Puberty or Polycystic Ovary Syndrome? Stella Milsom Endocrinologist Auckland DHB, University of Auckland,
12/27/2013. Kristen Cain, MD FACOG Reproductive Medicine Institute Sanford Health, Fargo ND
 Kristen Cain, MD FACOG Reproductive Medicine Institute Sanford Health, Fargo ND 7% of all women 18-45 Obesity 1/3 of all US women Incidence of PCOS is increasing with increase obesity Obesity Irregular
Kristen Cain, MD FACOG Reproductive Medicine Institute Sanford Health, Fargo ND 7% of all women 18-45 Obesity 1/3 of all US women Incidence of PCOS is increasing with increase obesity Obesity Irregular
Why Sex??? Advantages: It limits harmful mutations Asexual: all offspring get all mutations. Sexual: There is a random distribution of mutations.
 Reproduction Why sex??? Why Sex??? Asexual reproduction is quicker, easier, and produces more offspring per individual. Bacteria do it. Dandelions do it. Unisexual whiptail lizards do it. With sexual reproduction
Reproduction Why sex??? Why Sex??? Asexual reproduction is quicker, easier, and produces more offspring per individual. Bacteria do it. Dandelions do it. Unisexual whiptail lizards do it. With sexual reproduction
Intersex Genital Mutilations in ICD-10 Zwischengeschlecht.org / StopIGM.org 2014 (v2.1)
") Intersex Genital Mutilations in ICD-10 Zwischengeschlecht.org / StopIGM.org 2014 (v2.1) ICD-10 Codes and Descriptions: http://apps.who.int/classifications/icd10/browse/2010/en 1. Reference: 17 Most Common
Intersex Genital Mutilations in ICD-10 Zwischengeschlecht.org / StopIGM.org 2014 (v2.1) ICD-10 Codes and Descriptions: http://apps.who.int/classifications/icd10/browse/2010/en 1. Reference: 17 Most Common
OBJECTIVES. Rebecca McEachern, MD. Puberty: Too early, Too Late or Just Right? Special Acknowledgements. Maryann Johnson M.Ed.
 1 Puberty: Too early, Too Late or Just Right? Maryann Johnson M.Ed., BSN, RN Special Acknowledgements Rebecca McEachern, MD OBJECTIVES Illustrate basic endocrine system and hormonal pathways Define the
1 Puberty: Too early, Too Late or Just Right? Maryann Johnson M.Ed., BSN, RN Special Acknowledgements Rebecca McEachern, MD OBJECTIVES Illustrate basic endocrine system and hormonal pathways Define the
Puberty and Pubertal Disorders. Lisa Swartz Topor, MD, MMSc Pediatric Endocrinology July 2018
 Puberty and Pubertal Disorders Lisa Swartz Topor, MD, MMSc Pediatric Endocrinology July 2018 Objectives Review normal pubertal development Recognize common pubertal disorders Identify recent trends in
Puberty and Pubertal Disorders Lisa Swartz Topor, MD, MMSc Pediatric Endocrinology July 2018 Objectives Review normal pubertal development Recognize common pubertal disorders Identify recent trends in
Why is my body not changing? Conflicts of interest. Overview 11/9/2015. None
 Why is my body not changing? Murthy Korada Pediatrician, Pediatric Endocrinologist Ridge Meadows Hospital Surrey Memorial Hospital None Conflicts of interest Overview Overview of normal pubertal timing
Why is my body not changing? Murthy Korada Pediatrician, Pediatric Endocrinologist Ridge Meadows Hospital Surrey Memorial Hospital None Conflicts of interest Overview Overview of normal pubertal timing
Clinical Guideline. SPEG MCN Protocols Sub Group SPEG Steering Group
 Clinical Guideline SECONDARY CARE MANAGEMENT OF SUSPECTED ADRENAL CRISIS IN CHILDREN AND YOUNG PEOPLE Date of First Issue 24/01/2015 Approved 28/09/2017 Current Issue Date 16/06/2017 Review Date 01/09/2019
Clinical Guideline SECONDARY CARE MANAGEMENT OF SUSPECTED ADRENAL CRISIS IN CHILDREN AND YOUNG PEOPLE Date of First Issue 24/01/2015 Approved 28/09/2017 Current Issue Date 16/06/2017 Review Date 01/09/2019
Hormone. Free Androgen Index. 2-Hydroxyestrone. Reference Range. Hormone. Estrone Ratio. Free Androgen Index
 Hormonal Health PATIENT: Sample Report TEST REF: TST-12345 Hormonal Health 0.61 0.30-1.13 ng/ml DHEA-S 91 35-430 mcg/dl tient: SAMPLE TIENT e: x: N: Sex Binding Globulin 80 18-114 nmol/l Testosterone 0.34
Hormonal Health PATIENT: Sample Report TEST REF: TST-12345 Hormonal Health 0.61 0.30-1.13 ng/ml DHEA-S 91 35-430 mcg/dl tient: SAMPLE TIENT e: x: N: Sex Binding Globulin 80 18-114 nmol/l Testosterone 0.34
Therapeutic Cohort Results
 Patient: JANE DOE DOB: December 31, 1968 Sex: F MRN: Order Number: Completed: February 26, 2016 Received: February 26, 2016 Collected: February 26, 2016 One Day Hormone Check - Salivary Profile Therapeutic
Patient: JANE DOE DOB: December 31, 1968 Sex: F MRN: Order Number: Completed: February 26, 2016 Received: February 26, 2016 Collected: February 26, 2016 One Day Hormone Check - Salivary Profile Therapeutic
ASY-857.1: Synacthen Stimulated 17OH-progesterone Test
 ASY-857.1: Synacthen Stimulated 17OH-progesterone ASY-857.2: Associated Documents a Synacthen Standing Order form (ref 0827/2) G:\Division\NDO\common\ETCProtocols\0827 Standing Order Synacthen 2016.pdf
ASY-857.1: Synacthen Stimulated 17OH-progesterone ASY-857.2: Associated Documents a Synacthen Standing Order form (ref 0827/2) G:\Division\NDO\common\ETCProtocols\0827 Standing Order Synacthen 2016.pdf
Assistant Professor of Endocrinology
 Pathophysiology Of Adrenal Disorder Dr.Rezvan Salehidoost Assistant Professor of Endocrinology Pathophysiology Of Adrenal Disorder The adrenal glands lie at the superior pole of each kidney and are composed
Pathophysiology Of Adrenal Disorder Dr.Rezvan Salehidoost Assistant Professor of Endocrinology Pathophysiology Of Adrenal Disorder The adrenal glands lie at the superior pole of each kidney and are composed
Hormones of brain-testicular axis
 (Hormone Function) Hormones of brain-testicular axis anterior pituitary drives changes during puberty controlled by GnRH from hypothalamus begins to secrete FSH, LH LH targets interstitial endocrinocytes
(Hormone Function) Hormones of brain-testicular axis anterior pituitary drives changes during puberty controlled by GnRH from hypothalamus begins to secrete FSH, LH LH targets interstitial endocrinocytes
Estrogens & Antiestrogens
 Estrogens & Antiestrogens Menstrual cycle... Changes and hormonal events Natural estrogens: Estadiol >> Estrone > Estriol Ineffective orally Synthesis: From cholesterol ; role of aromatase enzyme in converting
Estrogens & Antiestrogens Menstrual cycle... Changes and hormonal events Natural estrogens: Estadiol >> Estrone > Estriol Ineffective orally Synthesis: From cholesterol ; role of aromatase enzyme in converting
Chemical Classification of Hormones
 Steroid Hormones Chemical Classification of Hormones Hormones are chemical messengers that transport signals from one cell to another There are 4 major chemical classes of hormones steroid hormones - i.e.
Steroid Hormones Chemical Classification of Hormones Hormones are chemical messengers that transport signals from one cell to another There are 4 major chemical classes of hormones steroid hormones - i.e.
Adrenocortical Insufficiency: Addison's Disease
 280 PHYSIOLOGY CASES AND PROBLEMS Case 49 Adrenocortical Insufficiency: Addison's Disease Susan Oglesby is a 41-year-old divorced mother of two teenagers. She has always been in excellent health. She recently
280 PHYSIOLOGY CASES AND PROBLEMS Case 49 Adrenocortical Insufficiency: Addison's Disease Susan Oglesby is a 41-year-old divorced mother of two teenagers. She has always been in excellent health. She recently
THE VALUE OF 24 HOUR PROFILES IN CONGENITAL ADRENAL HYPERPLASIA
 THE VALUE OF 24 HOUR PROFILES IN CONGENITAL ADRENAL HYPERPLASIA This leaflet is a joint production between Professor Peter Hindmarsh and Kathy Geertsma The series editor is Professor Peter Hindmarsh Professor
THE VALUE OF 24 HOUR PROFILES IN CONGENITAL ADRENAL HYPERPLASIA This leaflet is a joint production between Professor Peter Hindmarsh and Kathy Geertsma The series editor is Professor Peter Hindmarsh Professor
C. Patrick Shahan, MD University of Tennessee Health Science Center Department of Surgery
 C. Patrick Shahan, MD University of Tennessee Health Science Center Department of Surgery Drop use of hermaphrodite and derivatives 1 in 15,000 live births Congenital Adrenal Hyperplasia Mixed Gonadal
C. Patrick Shahan, MD University of Tennessee Health Science Center Department of Surgery Drop use of hermaphrodite and derivatives 1 in 15,000 live births Congenital Adrenal Hyperplasia Mixed Gonadal
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 10 February 2010
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 10 February 2010 ADIXONE 50 µg, tablet Box of 30 (CIP: 390 604.3) Box of 60 (CIP: 390 606.6) Box of 90 (CIP: 390 607.2)
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 10 February 2010 ADIXONE 50 µg, tablet Box of 30 (CIP: 390 604.3) Box of 60 (CIP: 390 606.6) Box of 90 (CIP: 390 607.2)
Klinefelter syndrome ( 47, XXY )
") Sex Chromosome Abnormalities, Sex Chromosome Aneuploidy It has been estimated that, overall, approximately one in 400 infants have some form of sex chromosome aneuploidy. A thorough discussion of sex chromosomes
Sex Chromosome Abnormalities, Sex Chromosome Aneuploidy It has been estimated that, overall, approximately one in 400 infants have some form of sex chromosome aneuploidy. A thorough discussion of sex chromosomes
Reproductive FSH. Analyte Information
 Reproductive FSH Analyte Information 1 Follicle-stimulating hormone Introduction Follicle-stimulating hormone (FSH, also known as follitropin) is a glycoprotein hormone secreted by the anterior pituitary
Reproductive FSH Analyte Information 1 Follicle-stimulating hormone Introduction Follicle-stimulating hormone (FSH, also known as follitropin) is a glycoprotein hormone secreted by the anterior pituitary
POLYCYSTIC OVARIAN SYNDROME WHERE WE ARE AT IN 2018
 POLYCYSTIC OVARIAN SYNDROME WHERE WE ARE AT IN 2018 PCOS: WHERE WE ARE AT IN 2018 Nancy Arquette, MD Premier Women s Health 6135 Trust Drive #114 Holland, OH 43528 February 3, 2018 Kalahari Resorts ME
POLYCYSTIC OVARIAN SYNDROME WHERE WE ARE AT IN 2018 PCOS: WHERE WE ARE AT IN 2018 Nancy Arquette, MD Premier Women s Health 6135 Trust Drive #114 Holland, OH 43528 February 3, 2018 Kalahari Resorts ME
PHYSIOLOGY AND PATHOLOGY OF SEXUAL DIFFERENTIATION
 PHYSIOLOGY AND PATHOLOGY OF SEXUAL DIFFERENTIATION Prof. Dr med. Jolanta Słowikowska-Hilczer Department of Andrology and Reproductive Endocrinology Medical University of Łódź, Poland Sexual determination
PHYSIOLOGY AND PATHOLOGY OF SEXUAL DIFFERENTIATION Prof. Dr med. Jolanta Słowikowska-Hilczer Department of Andrology and Reproductive Endocrinology Medical University of Łódź, Poland Sexual determination
Sexual dysfunction of chronic kidney disease. Razieh salehian.md psychiatrist
 Sexual dysfunction of chronic kidney disease Razieh salehian.md psychiatrist Disturbances in sexual function are a common feature of chronic renal failure. Sexual dysfunction is inversely associated with
Sexual dysfunction of chronic kidney disease Razieh salehian.md psychiatrist Disturbances in sexual function are a common feature of chronic renal failure. Sexual dysfunction is inversely associated with