of Trauma Assembly 27 th Page 1
|
|
|
- Moses Price
- 5 years ago
- Views:
Transcription


1 Eastern Association for the Surgery of Trauma 27 th Annual Scientific Assembly Sunrise Session 08 To Scan or Not To Scan Thatt is the Question January 16, 2014 Waldorf Astoria Naples Naples, Floridaa Page 1



2 To Scan or Not to Scan: That is the Question Robert W. Letton, Jr., MD Pediatric Trauma Medical Director The Level 1 Pediatric Trauma Center Oklahoma University Medical Center Oklahoma City, Oklahoma A trip to the CT might not be Page 2


3 Radiation Reduction Modifying CT scan parameters Not looking for sub-centimeter metastatic disease in pediatric trauma patients Limit multiple sequences Do it right the first time Insure images can be uploaded Judicious use of CT The BIG three Chest X-ray 0.02mSv Lateral C-spine 0.02mSv Pelvic film 0.03mSv PAN SCAN Head CT Cervical Spine Ct Chest CT Abd/pelvic CT 2mSv 2mSv 8mSv 10mSv Next morning Repeat CT - head 2mSv T&L spine films 0.1mSv Chest Xray 0.02mSv Total (first 18 hours) 24.2mSv Infant with altered Mental Status: Scenario 1 1 year with witnessed fall out of shopping cart at grocery store Brief loss of consciousness but crying when EMS arrives Placed in cervical collar on backboard and taken to hospital where GCS is 15 PERRL, EOMI, TM s clear, small contusion/hematoma over right eye Acting appropriate when mother is present Page 3


4 Infant with altered Mental Status: Scenario 1 Further work-up? Scan or not to scan? What about the cervical spine? Admit or Discharge? Page 4


5 What about the Cervical Spine? Canadian Pediatric C-Spine It is possible to clinically clear the pediatric cervical spine Using a combination of NEXUS and the CCR Pediatric patients should be managed with the lowest possible radiation exposure Page 5

6 Canadian Pediatric C-Spine The ondontoid view may be beneficial in cooperative patients Flexion-Extension may be indicated for the neurologically intact patient with persistent tenderness Plain radiographs should still be the assessment tool of choice CT reserved for cases where more diagnostic certainty is required Upper c-spine C1-C3 Canadian Pediatric C-Spine MRI is recommended for all patients with an abnormal neurologic exam And patients requiring investigation of soft tissues and spinal cord Pediatric patients with an unreliable clinical exam should be managed conservatively and cautiously CT scan should be considered at any time MRI if not alert and cooperative after 24 to 72 hours Page 6

7 Infant with altered Mental Status: Scenario 2 1 year old found unresponsive in crib by mother s boyfriend while she was at work EMS responds to find crying inconsolably, opens eyes to loud noise, localizes pain: GCS=11 Transported to hospital in collar and on board with a PIV Infant with altered Mental Status: Scenario 2 How does this work-up vary from Scenario 1 What other parts of PE are pertinent? Scan or Not? What about cervical spine? Multiple SDH on Head CT Page 7

8 Non-Accidental Trauma Contact DHS/CPS Complete Physical Exam Ophthalmology Consult to look for retinal hemorrhage Skeletal Survey MRI of brain/cervical spine Bone scan or Chest CT to look for occult rib fractures Toddler with Vomiting, Abdominal Distension and Bruising 3 year old reportedly pushed by younger brother down a flight of stairs 6 hours later family called EMS because of vomiting and pain EMS finds child lying perfectly still, holding abdomen, saying tummy hurts Toddler with Vomiting, Abdominal Distension and Bruising Page 8


9 Toddler with Vomiting, Abdominal Distension and Bruising Patent airway, bilateral breath sounds, 100% SaO2 on RA, hemodynamically stable, GCS 15 Distended, tender, with rebound and guarding Foley placed with concentrated urine, and NG has bilious output Scan or not? Plain Films Ultrasound?? Page 9

10 Retinal Scan Child in Motor Vehicle Collision Age appropriate restraint 7 year old, rear seat passenger, age appropriate restraint, in MVC No LOC, no amnesia, GCS 15, hemodynamically stable No chest or abdominal bruising No obvious fractures Minimal complaints that belly hurts No tenderness to palpation, rebound or guarding Child in Motor Vehicle Collision Age appropriate restraint Further workup? Ultrasound? Scan or not? Admit or discharge? Page 10

11 7 Findings in Descending Order No evidence of abdominal wall trauma GCS greater than 13 No abdominal tenderness No evidence of chest wall trauma No complaints of abdominal pain No decreased breath sounds No vomiting Page 11

12 118 patients < 17 with FAST, PE and CT scan FAST vs CT Sensitivity 70%, specificity 100%, PPV 100%, NPV 92% (FAST + PE) vs CT Sensitivity 100%, Specificity 74%, PPV 53%, NPV 100% Surgeon directed FAST + PE can rule out injury The American Surgeon 2004, 70: /193 patients < 15, with a positive FAST 1/22 with USS < 3 required ex lap 8/15 with USS > 3 required ex lap USS > 3: sensitivity of 89% and specificity of 75% for predicting the need for therapeutic laparotomy in patients < 15 J Trauma. 2003;54: Page 12

13 Ultrasound Score (USS) 5 spaces are scanned with US: Morrison s, perisplenic, right and left subphrenic and the pelvis Depth of the deepest pocket of fluid in cm, plus the number or additional spaces where fluid is noted If fluid was present in three areas and the deepest pocket measured 4 cm, the USS would be = 6 If we don t scan the child what are we missing??? Child in Motor Vehicle Collision Seat Belt Stripe 7 year old rear seat passenger, restrained with lap belt, in MVC Positive LOC and GCS 14 Pulse 100, BP stable, and complains of abdominal pain No obvious extremity fractures Tender to palpation, even away from stripe, but no rebound or guarding Page 13

14 Child in Motor Vehicle Collision Seat Belt Stripe Further workup? Role of Ultrasound Role of CT? What about the Chest? Emergent operative intervention? What if FAST positive?? Page 14



15 Abdominal CT Rush to the OR???? Page 15


16 Common conclusions Free fluid on CT scan without peritonitis does not always require operative intervention The decision to operate better based on serial physical exam Children tolerate the delay to intervention better than adults What about the Chest? Page 16
17 Page 17


18 Bad CXR Chest CT Page 18
19 Page 19
Imaging in the Trauma Patient
 Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
SPINE EVALUATION AND CLEARANCE Basic Principles
 SPINE EVALUATION AND CLEARANCE Basic Principles General 1. Entire spine is immobilized during primary survey. 2. Radiographic clearance of the spine is not required before emergent surgical procedures.
SPINE EVALUATION AND CLEARANCE Basic Principles General 1. Entire spine is immobilized during primary survey. 2. Radiographic clearance of the spine is not required before emergent surgical procedures.
Pan Scan Instead of Clinical Exam? David A. Spain, MD
 Pan Scan Instead of Clinical Exam? David A. Spain, MD Granted, some patients don t t need CT scan Platinum Package Stanford Special CT Scan Head Neck Chest Abdomen Pelvis Takes about 20 minutes to do
Pan Scan Instead of Clinical Exam? David A. Spain, MD Granted, some patients don t t need CT scan Platinum Package Stanford Special CT Scan Head Neck Chest Abdomen Pelvis Takes about 20 minutes to do
A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion
 A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion Christopher Butts PhD, DO Surgical Critical Care Fellow Cooper University Hospital H&P 10 year old female presents as a trauma
A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion Christopher Butts PhD, DO Surgical Critical Care Fellow Cooper University Hospital H&P 10 year old female presents as a trauma
SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services OBJECTIVES DEFINITION 11/8/2017. Identify SCIWORA.
 SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services Identify SCIWORA. OBJECTIVES Identify the population at risk. To identify anatomic and physiologic reasons for SCIWORA. To
SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services Identify SCIWORA. OBJECTIVES Identify the population at risk. To identify anatomic and physiologic reasons for SCIWORA. To
Focused History and Physical Examination of the
 Henry: EMT Prehospital Care, Revised 3 rd Edition Lecture Notes Chapter 10: Focused History and Physical Examination of Trauma Patients Chapter 10 Focused History and Physical Examination of the Trauma
Henry: EMT Prehospital Care, Revised 3 rd Edition Lecture Notes Chapter 10: Focused History and Physical Examination of Trauma Patients Chapter 10 Focused History and Physical Examination of the Trauma
Evaluation and Stabilization of the Athlete with Possible Spine Injury
 Evaluation and Stabilization of the Athlete with Possible Spine Injury Jeffrey H. Bohmer, MD, FACEP Emergency Physician Northwestern Medicine Central DuPage Hospital June 12, 2015 Introduction Goals: 1.
Evaluation and Stabilization of the Athlete with Possible Spine Injury Jeffrey H. Bohmer, MD, FACEP Emergency Physician Northwestern Medicine Central DuPage Hospital June 12, 2015 Introduction Goals: 1.
PEDIATRIC TRAUMA I: ABDOMINAL TRAUMA BURNS. December 19, 2012
 PEDIATRIC TRAUMA I: ABDOMINAL TRAUMA BURNS Niel F. Miele,, M.D. December 19, 2012 EPIDEMIOLOGY Major Trauma responsible for
PEDIATRIC TRAUMA I: ABDOMINAL TRAUMA BURNS Niel F. Miele,, M.D. December 19, 2012 EPIDEMIOLOGY Major Trauma responsible for
Sasha Dubrovsky, MSc MD FRCPC Pediatric Emergency Medicine Montreal Children s Hospital - MUHC October 2010
 Sasha Dubrovsky, MSc MD FRCPC Pediatric Emergency Medicine Montreal Children s Hospital - MUHC October 2010 Learning objectives 1. Discuss diagnostic goals in pediatric trauma Diagnose All vs. Severe Injuries
Sasha Dubrovsky, MSc MD FRCPC Pediatric Emergency Medicine Montreal Children s Hospital - MUHC October 2010 Learning objectives 1. Discuss diagnostic goals in pediatric trauma Diagnose All vs. Severe Injuries
Chapter 32. Objectives. Objectives 01/09/2013. Spinal Column and Spinal Cord Trauma
 Chapter 32 Spinal Column and Spinal Cord Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1.
Chapter 32 Spinal Column and Spinal Cord Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1.
Major Trauma Scenarios. Ballarat Health Services Emergency Medicine Training Hub
 Major Trauma Scenarios Ballarat Health Services Emergency Medicine Training Hub Trauma Scenario 1 You receive a phone call from the ambulance service. They have a 27 yr old male involved in a MCA, he is
Major Trauma Scenarios Ballarat Health Services Emergency Medicine Training Hub Trauma Scenario 1 You receive a phone call from the ambulance service. They have a 27 yr old male involved in a MCA, he is
ITLS Pediatric Provider Course Advanced Pre-Test
 ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing
 1 2 3 4 5 6 Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing D-Disability Chief complaint and/or Mechanism
1 2 3 4 5 6 Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing D-Disability Chief complaint and/or Mechanism
History Data Panel. Case 030 Preg Trauma. Presenting Complaint Altered mental status s/p MVC. Person Giving Information EMS
 History Data Panel Presenting Complaint Altered mental status s/p MVC Person Giving Information EMS History of Present Illness 28 year old woman, 35 weeks pregnant per report of her husband the passenger.
History Data Panel Presenting Complaint Altered mental status s/p MVC Person Giving Information EMS History of Present Illness 28 year old woman, 35 weeks pregnant per report of her husband the passenger.
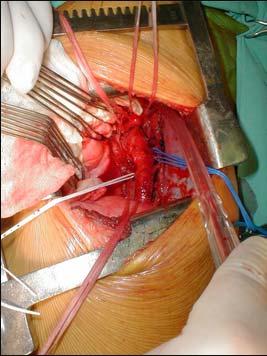
Bilateral rib fractures 2 on right and 1 on left In different stages of healing, with left fracture older than right fractures
 More history: Seen by PCP yesterday because of vomiting and fussinesss. Called by ED today because Mom presents with same complaints. ED found nothing but got an abdominal x ray. ED now wants kid admitted
More history: Seen by PCP yesterday because of vomiting and fussinesss. Called by ED today because Mom presents with same complaints. ED found nothing but got an abdominal x ray. ED now wants kid admitted
Pediatric Trauma. July 27 th, Suzana Buac, PGY4. Dr. Neil Merritt
 Pediatric Trauma July 27 th, 2016. Suzana Buac, PGY4 Dr. Neil Merritt Case 5yoM fall from roof Fall from roof of home while father was shingling 5yoM fall from roof Fall from roof of home while father
Pediatric Trauma July 27 th, 2016. Suzana Buac, PGY4 Dr. Neil Merritt Case 5yoM fall from roof Fall from roof of home while father was shingling 5yoM fall from roof Fall from roof of home while father
vel 2 Level 2 3,034 c-spine evaluations with CSR Level 3 detected injury only 53% of the time. Level 3 False (-) rate 47%
 rate 47%") Objectives Blunt and Penetrating Neck Trauma Julie Mayglothling, MD, FACEP Virginia Commonwealth University Richmond, VA Summit to Sound, May 20 th, 2011 Blunt Neck Trauma Evaluation of the low mechanism,
Objectives Blunt and Penetrating Neck Trauma Julie Mayglothling, MD, FACEP Virginia Commonwealth University Richmond, VA Summit to Sound, May 20 th, 2011 Blunt Neck Trauma Evaluation of the low mechanism,
Evaluation of Children with Blunt Abdominal Trauma. James F. Holmes, MD, MPH UC Davis School of Medicine
 Evaluation of Children with Blunt Abdominal Trauma James F. Holmes, MD, MPH UC Davis School of Medicine Objectives Epidemiology of intra-abdominal injury (IAI) Physical examination findings with IAI Laboratory
Evaluation of Children with Blunt Abdominal Trauma James F. Holmes, MD, MPH UC Davis School of Medicine Objectives Epidemiology of intra-abdominal injury (IAI) Physical examination findings with IAI Laboratory
Pediatric Trauma Cases
 Pediatric Trauma Cases QPEM 2018 Barbara Blackie, MD, MEd, FRCPC DISCLOSURE I do not have any relevant financial relationship with commercial interest to disclose. Learning Objectives -Manage interactive
Pediatric Trauma Cases QPEM 2018 Barbara Blackie, MD, MEd, FRCPC DISCLOSURE I do not have any relevant financial relationship with commercial interest to disclose. Learning Objectives -Manage interactive
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of
 Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
TALK TRAUMA Clearing the C-Spine. David Ouellette
 TALK TRAUMA 2011 Clearing the C-Spine David Ouellette Case #1 - Mother / Daughter MVC 34 y/o female Dangerous mechanism CHI Mumbling incoherently Femur # - distracting injury ETOH - 22 9 y/o female Dangerous
TALK TRAUMA 2011 Clearing the C-Spine David Ouellette Case #1 - Mother / Daughter MVC 34 y/o female Dangerous mechanism CHI Mumbling incoherently Femur # - distracting injury ETOH - 22 9 y/o female Dangerous
Patient Assessment. Chapter 8
 Patient Assessment Chapter 8 Patient Assessment Scene size-up Initial assessment Focused history and physical exam Vital signs History Detailed physical exam Ongoing assessment Patient Assessment Process
Patient Assessment Chapter 8 Patient Assessment Scene size-up Initial assessment Focused history and physical exam Vital signs History Detailed physical exam Ongoing assessment Patient Assessment Process
10O SPLINTING OF INJURIES ADULT & PEDIATRIC. 10Oa: Axial/Spine with Selective Spinal Motion Restriction Adult & Pediatric:
 10O SPLINTING OF INJURIES ADULT & PEDIATRIC EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 10Oa: Axial/Spine with Selective Spinal Motion Restriction Adult & Pediatric: Many
10O SPLINTING OF INJURIES ADULT & PEDIATRIC EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 10Oa: Axial/Spine with Selective Spinal Motion Restriction Adult & Pediatric: Many
3/14/2014 USED TO BE SIMPLE.. TO IMMOBILIZE OR NOT TO IMMOBILIZE.THAT IS THE QUESTION THE PROBLEM OLD THINKING
 USED TO BE SIMPLE.. TO IMMOBILIZE OR NOT TO IMMOBILIZE.THAT IS THE QUESTION Immobilization following injury used to be a simple decision--but no one was thinking. Up to 5 million people per year receive
USED TO BE SIMPLE.. TO IMMOBILIZE OR NOT TO IMMOBILIZE.THAT IS THE QUESTION Immobilization following injury used to be a simple decision--but no one was thinking. Up to 5 million people per year receive
Med 536 Communicating About Prognosis Workshop. Case 1
 Med 536 Communicating About Prognosis Workshop Case 1 ID / CC: 39 year-old woman status-post motor-vehicle collision History of the Presenting Illness Previously healthy 39 year-old woman was found in
Med 536 Communicating About Prognosis Workshop Case 1 ID / CC: 39 year-old woman status-post motor-vehicle collision History of the Presenting Illness Previously healthy 39 year-old woman was found in
Shenandoah Co. Fire & Rescue. Injuries to. and Spine. December EMS Training Bill Streett Training Section Chief
 Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#
Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#
Identify the risk management issues involved in caring for patient with orthopedic complaints.
 MACEP Risk Management Course Module 4: Emergency Orthopedics Matthew B. Mostofi, D.O., FACEP Course Objectives Identify the risk management issues involved in caring for patient with orthopedic complaints.
MACEP Risk Management Course Module 4: Emergency Orthopedics Matthew B. Mostofi, D.O., FACEP Course Objectives Identify the risk management issues involved in caring for patient with orthopedic complaints.
A guide to writing clear, concise EMS reports using SIREN
 A guide to writing clear, concise EMS reports using SIREN OBJECTIVE: EMS narratives will document patient assessment findings, interventions, and patient response to interventions such that ED providers
A guide to writing clear, concise EMS reports using SIREN OBJECTIVE: EMS narratives will document patient assessment findings, interventions, and patient response to interventions such that ED providers
Overview. Overview. Chapter 30. Injuries to the Head and Spine 9/11/2012. Review of the Nervous and Skeletal Systems. Devices for Immobilization
 Chapter 30 Injuries to the Head and Spine Slide 1 Overview Review of the Nervous and Skeletal Systems The Nervous System The Skeletal System Devices for Immobilization Cervical Spine Short Backboards Long
Chapter 30 Injuries to the Head and Spine Slide 1 Overview Review of the Nervous and Skeletal Systems The Nervous System The Skeletal System Devices for Immobilization Cervical Spine Short Backboards Long
Date of Admission: [DATE]. Date of Discharge:
![Date of Admission: [DATE]. Date of Discharge:](/thumbs/74/71277118.jpg "Date of Admission: [DATE]. Date of Discharge:") Date of Admission: [DATE]. Date of Discharge: History of Present Illness: Mr. [NAME] AKA [NAME] is a 31-year-old male who presents to the [PLACE] Trauma Surgery Service as a moderate trauma on [DATE] following
Date of Admission: [DATE]. Date of Discharge: History of Present Illness: Mr. [NAME] AKA [NAME] is a 31-year-old male who presents to the [PLACE] Trauma Surgery Service as a moderate trauma on [DATE] following
Patient Care Report Guidelines
 A rrival on scene / Scene assessment C omplaint H istory A. Position of patient B. Impression of patient C. Does the patient acknowledge your presence D. Any significant characteristics of the scene A.
A rrival on scene / Scene assessment C omplaint H istory A. Position of patient B. Impression of patient C. Does the patient acknowledge your presence D. Any significant characteristics of the scene A.
ITLS Pediatric Provider Course Basic Pre-Test
 ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
Selective Spinal Immobilization
 Selective Spinal Immobilization Objectives Understand the background of spinal immobilization. Understand the rationale for developing a current selective spinal immobilization protocol. Review the data
Selective Spinal Immobilization Objectives Understand the background of spinal immobilization. Understand the rationale for developing a current selective spinal immobilization protocol. Review the data
Spine MRI and Spine CT Test Request Tip Sheet
 Spine MRI and Spine CT With/Without Contrast CT, MRI The study considered best for a specific clinical scenario should be ordered. The second study should be done ONLY if the first study does not provide
Spine MRI and Spine CT With/Without Contrast CT, MRI The study considered best for a specific clinical scenario should be ordered. The second study should be done ONLY if the first study does not provide
Pre-hospital Response to Trauma and Brain Injury. Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center
 Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Assessment of the Trauma Patient
 CHAPTER 10 Assessment of the Trauma Patient Overall Assessment Scheme Scene Size-Up Initial Assessment Trauma Physical Exam Vital Signs & SAMPLE History Medical SAMPLE History Physical Exam & Vital Signs
CHAPTER 10 Assessment of the Trauma Patient Overall Assessment Scheme Scene Size-Up Initial Assessment Trauma Physical Exam Vital Signs & SAMPLE History Medical SAMPLE History Physical Exam & Vital Signs
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours
 Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Spine MRI and Spine CT Test Request Tip Sheet
 Spine MRI and Spine CT With/Without Contrast CT, MRI The study considered best for a specific clinical scenario should be ordered. The second study should be done ONLY if the first study does not provide
Spine MRI and Spine CT With/Without Contrast CT, MRI The study considered best for a specific clinical scenario should be ordered. The second study should be done ONLY if the first study does not provide
Spine MRI and Spine CT Test Request Tip Sheet
 Spine MRI and Spine CT With/Without Contrast CT, MRI Studies should NOT be ordered simultaneously as dual studies (i.e., with and without contrast). Radiation exposure is doubled and both views are rarely
Spine MRI and Spine CT With/Without Contrast CT, MRI Studies should NOT be ordered simultaneously as dual studies (i.e., with and without contrast). Radiation exposure is doubled and both views are rarely
Spine MRI and Spine CT Test Request Tip Sheet
 Spine MRI and Spine CT MRI is almost always preferred over CT scan; if ordering CT, CLEARLY document why MRI is not appropriate. In cases of back pain without red flags, six weeks of multimodality supervised
Spine MRI and Spine CT MRI is almost always preferred over CT scan; if ordering CT, CLEARLY document why MRI is not appropriate. In cases of back pain without red flags, six weeks of multimodality supervised
Head injury in children
 Head injury in children Michael Kim, MD Department of Emergency Medicine University of Wisconsin- Madison #1 cause of death and disability Bimodal distribution 62,000 hospitalization 564,000 ED visits
Head injury in children Michael Kim, MD Department of Emergency Medicine University of Wisconsin- Madison #1 cause of death and disability Bimodal distribution 62,000 hospitalization 564,000 ED visits
Appendicitis USG vs CT
 Appendicitis USG vs CT Dr Sateesh Kumar Kailasam MBBS Dip EM (RCGP, UK) MRCEM (UK) Group Head Maxcure Group of Hospitals National Treasurer Society for Emergency Medicine India (SEMI) My Talk includes
Appendicitis USG vs CT Dr Sateesh Kumar Kailasam MBBS Dip EM (RCGP, UK) MRCEM (UK) Group Head Maxcure Group of Hospitals National Treasurer Society for Emergency Medicine India (SEMI) My Talk includes
NOR-CAL EMS MEDICAL ADVISORY COMMITTEE RUN REVIEW, NOVEMBER 2014
 Eric M. Rudnick, MD, FACEP, FAAEM Medical Director Northern California EMS NOR-CAL EMS MEDICAL ADVISORY COMMITTEE RUN REVIEW, NOVEMBER 2014. meeting by Engineer Bill Bogenreif 1 CASE #1 Call Type : Fall
Eric M. Rudnick, MD, FACEP, FAAEM Medical Director Northern California EMS NOR-CAL EMS MEDICAL ADVISORY COMMITTEE RUN REVIEW, NOVEMBER 2014. meeting by Engineer Bill Bogenreif 1 CASE #1 Call Type : Fall
Abdomen and Genitalia Injuries. Chapter 28
 Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
CBT 445 Head & Spine Thoracic Scenario 1
 CBT 445 Head & Spine Thoracic Scenario 1 Evaluator s notes: Patient 36 year old male fall patient, Impaled branch, quick transport to ER. Dispatch/Description of the problem: You are dispatched to 36 year
CBT 445 Head & Spine Thoracic Scenario 1 Evaluator s notes: Patient 36 year old male fall patient, Impaled branch, quick transport to ER. Dispatch/Description of the problem: You are dispatched to 36 year
Pediatric Imaging Spine MRI and Spine CT Test Request Tip Sheet
 Pediatric Imaging Spine MRI and Spine CT MRI is almost always preferred over CT scan; if ordering CT, CLEARLY document why MRI is not appropriate. In cases of ongoing back pain, six weeks of conservative
Pediatric Imaging Spine MRI and Spine CT MRI is almost always preferred over CT scan; if ordering CT, CLEARLY document why MRI is not appropriate. In cases of ongoing back pain, six weeks of conservative
Injuries to the Head and Spine
 Injuries to the Head and Spine Anatomy Review Skull Protects the brain Made up of several bones with seam like sutures Regions of the scalp-frontal, occipital, parietal, temporal Bones of face Orbits Mandible
Injuries to the Head and Spine Anatomy Review Skull Protects the brain Made up of several bones with seam like sutures Regions of the scalp-frontal, occipital, parietal, temporal Bones of face Orbits Mandible
Controversies in Spinal Immobilization
 Controversies in Spinal Immobilization Ken Berumen, BSN, MD, FACEP Medical Director El Paso Fire Department Medical Director Emergency Services District #1 Network Director EM Sierra Providence Health
Controversies in Spinal Immobilization Ken Berumen, BSN, MD, FACEP Medical Director El Paso Fire Department Medical Director Emergency Services District #1 Network Director EM Sierra Providence Health
10/27/2014. An experience that causes physical, emotional, or psychological distress or harm.
 Ann Marie Szoke, DNP, CRNP Supervisor Advanced Practitioners St. Luke s University Hospital To review multiple traumatic events through case presentations Discuss the concept of the Hybrid Operating Room
Ann Marie Szoke, DNP, CRNP Supervisor Advanced Practitioners St. Luke s University Hospital To review multiple traumatic events through case presentations Discuss the concept of the Hybrid Operating Room
NON-OPERATIVE MANAGEMENT OF PEDIATRIC SOLID ORGAN INJURY
 NON-OPERATIVE MANAGEMENT OF PEDIATRIC SOLID ORGAN INJURY JESSICA A. NAIDITCH, MD TRAUMA MEDICAL DIRECTOR, DELL CHILDREN S MEDICAL CENTER OF CENTRAL TEXAS ASSISTANT PROFESSOR OF SURGERY AND PERIOPERATIVE
NON-OPERATIVE MANAGEMENT OF PEDIATRIC SOLID ORGAN INJURY JESSICA A. NAIDITCH, MD TRAUMA MEDICAL DIRECTOR, DELL CHILDREN S MEDICAL CENTER OF CENTRAL TEXAS ASSISTANT PROFESSOR OF SURGERY AND PERIOPERATIVE
Patient Assessment From Brady s First Responder (8th Edition) 83 Questions
 83 Questions") Patient Assessment From Brady s First Responder (8th Edition) 83 Questions 1. Which question is important if your patient may be a candidate for surgery? p. 183 *A.) When did you last eat? B.) What is
Patient Assessment From Brady s First Responder (8th Edition) 83 Questions 1. Which question is important if your patient may be a candidate for surgery? p. 183 *A.) When did you last eat? B.) What is
Cervical Spine Precautions A quick review. By Joseph Lewis, M.D. Medical Director, Honolulu EMS Board Certified in Emergency Medicine
 Cervical Spine Precautions A quick review By Joseph Lewis, M.D. Medical Director, Honolulu EMS Board Certified in Emergency Medicine 1 Goals of this Cervical Spine Immobilization In-service Learn Objectives:
Cervical Spine Precautions A quick review By Joseph Lewis, M.D. Medical Director, Honolulu EMS Board Certified in Emergency Medicine 1 Goals of this Cervical Spine Immobilization In-service Learn Objectives:
Pediatric Imaging Spine MRI and Spine CT Test Request Tip Sheet
 Pediatric Imaging Spine MRI and Spine CT MRI is almost always preferred over CT scan; if ordering CT, CLEARLY document why MRI is not appropriate. In cases of back pain without red flags, six weeks of
Pediatric Imaging Spine MRI and Spine CT MRI is almost always preferred over CT scan; if ordering CT, CLEARLY document why MRI is not appropriate. In cases of back pain without red flags, six weeks of
17. Imaging and interventional radiology
 17. Imaging and interventional radiology These guidelines have been adapted from the Leeds Major Trauma Centre Imaging in Paediatric Major Trauma guidelines Written by Dr Annmarie Jeanes (Consultant Paediatric
17. Imaging and interventional radiology These guidelines have been adapted from the Leeds Major Trauma Centre Imaging in Paediatric Major Trauma guidelines Written by Dr Annmarie Jeanes (Consultant Paediatric
Pediatric Trauma. Sept 2nd, Patrick Murphy Neil Merritt
 Pediatric Trauma Sept 2nd, 2015 Patrick Murphy Neil Merritt Objectives Objectives Medical Expert 1. Describe the types of pediatric injuries sustained with a given mode of trauma, and identify the most
Pediatric Trauma Sept 2nd, 2015 Patrick Murphy Neil Merritt Objectives Objectives Medical Expert 1. Describe the types of pediatric injuries sustained with a given mode of trauma, and identify the most
Indications for cervical spine immobilisation: -
 Paediatric Trauma Cervical Spine Guidelines UHW Traumatic injuries of the cervical spine (C-spine) are uncommon in children. However, it is safer assume there is a cervical spine injury until examination
Paediatric Trauma Cervical Spine Guidelines UHW Traumatic injuries of the cervical spine (C-spine) are uncommon in children. However, it is safer assume there is a cervical spine injury until examination
Request Card Task ANSWERS
 Request Card Task ANSWERS Medical Student Workbook Author: Dr Sam Leach, SpR Case 1 What differential diagnoses are most likely? Which investigation is most appropriate? Case 1 The most likely diagnosis
Request Card Task ANSWERS Medical Student Workbook Author: Dr Sam Leach, SpR Case 1 What differential diagnoses are most likely? Which investigation is most appropriate? Case 1 The most likely diagnosis
Fractures of the Thoracic and Lumbar Spine
 A spinal fracture is a serious injury. Nader M. Hebela, MD Fellow of the American Academy of Orthopaedic Surgeons http://orthodoc.aaos.org/hebela Cleveland Clinic Abu Dhabi Cleveland Clinic Abu Dhabi Neurological
A spinal fracture is a serious injury. Nader M. Hebela, MD Fellow of the American Academy of Orthopaedic Surgeons http://orthodoc.aaos.org/hebela Cleveland Clinic Abu Dhabi Cleveland Clinic Abu Dhabi Neurological
Overview of Abusive Head Trauma: What Everyone Needs to Know. 11 th Annual Keeping Children Safe Conference Boise, ID October 17, 2012
 Overview of Abusive Head Trauma: What Everyone Needs to Know 11 th Annual Keeping Children Safe Conference Boise, ID October 17, 2012 Deborah Lowen, MD Associate Professor Pediatrics Director, Child Abuse
Overview of Abusive Head Trauma: What Everyone Needs to Know 11 th Annual Keeping Children Safe Conference Boise, ID October 17, 2012 Deborah Lowen, MD Associate Professor Pediatrics Director, Child Abuse
2/13/13. Ann S. Botash, MD SUNY Upstate Medical University
 Ann S. Botash, MD SUNY Upstate Medical University 3 month old, previously healthy infant, brought to the primary care physician due to a fall He was being carried by the father, who tripped over the family
Ann S. Botash, MD SUNY Upstate Medical University 3 month old, previously healthy infant, brought to the primary care physician due to a fall He was being carried by the father, who tripped over the family
Little Kids in Big Crashes The Bio-mechanics of Kids in Car Crashes. Lisa Schwing, RN Trauma Program Manager Dayton Children s
 Little Kids in Big Crashes The Bio-mechanics of Kids in Car Crashes Lisa Schwing, RN Trauma Program Manager Dayton Children s Very Little Research There has been very little research on the forces a crash
Little Kids in Big Crashes The Bio-mechanics of Kids in Car Crashes Lisa Schwing, RN Trauma Program Manager Dayton Children s Very Little Research There has been very little research on the forces a crash
Cases from the Streets. Kelly Buchanan MD, ATC/L EMS Fellow December, 2011
 Cases from the Streets Kelly Buchanan MD, ATC/L EMS Fellow December, 2011 The Scene Car vs Light Pole, 35 mph, front right side damage 10 with no PCI + airbag deployment, starring on windshield Given the
Cases from the Streets Kelly Buchanan MD, ATC/L EMS Fellow December, 2011 The Scene Car vs Light Pole, 35 mph, front right side damage 10 with no PCI + airbag deployment, starring on windshield Given the
Objective 1 Review Research on spine injuries and evaluation standards.
 To Backboard or Not To Backboard? Spinal Clearance Protocols Will Smith, MD, NREMT-P Medical Director, Jackson Hole Fire/EMS, Grand Teton National Park Wilderness and Emergency Medicine Consulting (WEMC),
To Backboard or Not To Backboard? Spinal Clearance Protocols Will Smith, MD, NREMT-P Medical Director, Jackson Hole Fire/EMS, Grand Teton National Park Wilderness and Emergency Medicine Consulting (WEMC),
Chapter 13. Objectives. Objectives 01/09/2013. Patient Assessment
 Chapter 13 Patient Assessment Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms
Chapter 13 Patient Assessment Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms
Pediatric Abdomen Trauma
 Pediatric Abdomen Trauma Susan D. John, MD, FACR Pediatric Trauma Trauma is leading cause of death and disability in children and adolescents Causes and effects vary between age groups Blunt trauma predominates
Pediatric Abdomen Trauma Susan D. John, MD, FACR Pediatric Trauma Trauma is leading cause of death and disability in children and adolescents Causes and effects vary between age groups Blunt trauma predominates
PEDIATRIC BLUNT TRAUMA WHAT S DIFFERENT? NORDIC TRAUMA COURSE 2016
 PEDIATRIC BLUNT TRAUMA WHAT S DIFFERENT? NORDIC TRAUMA COURSE 2016 Ken F. Linnau, MD, MS Emergency Radiology Harborview Medical Center University of Washington Seattle, WA Thanks to Nupur Verma, MD University
PEDIATRIC BLUNT TRAUMA WHAT S DIFFERENT? NORDIC TRAUMA COURSE 2016 Ken F. Linnau, MD, MS Emergency Radiology Harborview Medical Center University of Washington Seattle, WA Thanks to Nupur Verma, MD University
Trauma Overview. Chapter 22
 Trauma Overview Chapter 22 Kinematics of Trauma Injuries are the leading cause of death among children and young adults. Kinematics introduces the basic physical concepts that dictate how injuries occur
Trauma Overview Chapter 22 Kinematics of Trauma Injuries are the leading cause of death among children and young adults. Kinematics introduces the basic physical concepts that dictate how injuries occur
Algorithms for managing the common trauma patient
 ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
Pediatric Trauma: Pearls of Management
 Pediatric Trauma: Pearls of Management Judith R. Klein, MD Assistant Professor UCSF-SFGH SFGH Department of Emergency Medicine Pediatric Trauma: The Problem Leading cause of M/M age 1-241 50% of all pediatric
Pediatric Trauma: Pearls of Management Judith R. Klein, MD Assistant Professor UCSF-SFGH SFGH Department of Emergency Medicine Pediatric Trauma: The Problem Leading cause of M/M age 1-241 50% of all pediatric
EMS System for Metropolitan Oklahoma City and Tulsa 2019 Medical Control Board Treatment Protocols
 EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
DUKEMedicine. SMITH, JAMES MRN: D DOB: 2/6/1993, Sex: M Adm: 2/15/2016, D/C: 2/15/2016
 History Chief Complaint Patient presents with Motor Vehicle Crash HPI James Smith is a 23 y.o. male here today for evaluation of injuries sustained today in a MVA. He was a restrained driver of a car struck
History Chief Complaint Patient presents with Motor Vehicle Crash HPI James Smith is a 23 y.o. male here today for evaluation of injuries sustained today in a MVA. He was a restrained driver of a car struck
Restore adequate respiratory and circulatory conditions. Reduce pain
 Pre-hospital management of the trauma patient is best performed by an integrated team focused on minimizing the time from injury to definitive care at an appropriate trauma center. Dispatchers, first responders,
Pre-hospital management of the trauma patient is best performed by an integrated team focused on minimizing the time from injury to definitive care at an appropriate trauma center. Dispatchers, first responders,
Deceleration during 'real life' motor vehicle collisions: A sensitive predictor for the risk of sustaining a cervical spine injury?
 Deceleration during 'real life' motor vehicle collisions: A sensitive predictor for the risk of sustaining a cervical spine injury? 1 Patient Safety in Surgery March 8, 2009 Martin Elbel, Michael Kramer,
Deceleration during 'real life' motor vehicle collisions: A sensitive predictor for the risk of sustaining a cervical spine injury? 1 Patient Safety in Surgery March 8, 2009 Martin Elbel, Michael Kramer,
Assessment and Scoring Tools
 Assessment and Scoring Tools 2013 APGAR Scale 0 points 1 point 2 points Heart Rate Absent 100 Respiratory Rate Absent Slow, irregular Good, drying Irritability Flaccid Some flexion Active motion
Assessment and Scoring Tools 2013 APGAR Scale 0 points 1 point 2 points Heart Rate Absent 100 Respiratory Rate Absent Slow, irregular Good, drying Irritability Flaccid Some flexion Active motion
6/23/2017. What do you see? skull fracture
 What do you see? skull fracture 1 Head CT On soft tissue windows, posterior soft tissues swelling and hemorrhage, no definite evidence of fracture Head CT On bone windows, fracture now seen subjacent to
What do you see? skull fracture 1 Head CT On soft tissue windows, posterior soft tissues swelling and hemorrhage, no definite evidence of fracture Head CT On bone windows, fracture now seen subjacent to
Introduction. Objectives C-Spine: Where Are We Now? NAEMSP Medical Director Course 1/9/2013
 NAEMSP Medical Director Course 1/9/2013 Objectives C-Spine: Where Are We Now? Robert M. Domeier, MD EMS Medical Director Washtenaw/Livingston Medical Control Authority Department of Emergency Medicine
NAEMSP Medical Director Course 1/9/2013 Objectives C-Spine: Where Are We Now? Robert M. Domeier, MD EMS Medical Director Washtenaw/Livingston Medical Control Authority Department of Emergency Medicine
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials
 Preparatory Materials") Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
Reviewing the recent literature to answer clinical questions: Should I change my practice?
 Reviewing the recent literature to answer clinical questions: Should I change my practice? JILL MILLER, MD PEM ATTENDING CHKD ASSISTANT PROFESSOR PEDIATRICS, EVMS Objectives Review the literature to answer
Reviewing the recent literature to answer clinical questions: Should I change my practice? JILL MILLER, MD PEM ATTENDING CHKD ASSISTANT PROFESSOR PEDIATRICS, EVMS Objectives Review the literature to answer
Abuse or Accident? Suzanne B. Haney, MD, FAAP Child Abuse Pediatrics
 Abuse or Accident? Suzanne B. Haney, MD, FAAP Child Abuse Pediatrics Disclosure I have nothing to disclose Objectives Describe common accidental injuries which can be confused with child abuse Describe
Abuse or Accident? Suzanne B. Haney, MD, FAAP Child Abuse Pediatrics Disclosure I have nothing to disclose Objectives Describe common accidental injuries which can be confused with child abuse Describe
European Resuscitation Council
 European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
EMS Spinal Assessment and Precautions
 EMS Spinal Assessment and Precautions Adapted from a presentation prepared by Chelsea C. White IV, MD, NREMT-P Medical Director, Bernalillo County Fire Department Robert M. Domeier, MD, EMS Medical Director,
EMS Spinal Assessment and Precautions Adapted from a presentation prepared by Chelsea C. White IV, MD, NREMT-P Medical Director, Bernalillo County Fire Department Robert M. Domeier, MD, EMS Medical Director,
EMT. Chapter 8 Review
 EMT Chapter 8 Review 1. During the scene size-up, you should routinely determine all of the following, EXCEPT: A. the mechanism of injury or nature of illness. B. the ratio of pediatric patients to adult
EMT Chapter 8 Review 1. During the scene size-up, you should routinely determine all of the following, EXCEPT: A. the mechanism of injury or nature of illness. B. the ratio of pediatric patients to adult
The Medical Assessment of Fractures in Suspected Child Maltreatment: Infants and Young Children with Skeletal Injury CPS Podcast
 The Medical Assessment of Fractures in Suspected Child Maltreatment: Infants and Young Children with Skeletal Injury CPS Podcast September 27, 2018 Introduction: Hello everyone, my name is Dominique Piché
The Medical Assessment of Fractures in Suspected Child Maltreatment: Infants and Young Children with Skeletal Injury CPS Podcast September 27, 2018 Introduction: Hello everyone, my name is Dominique Piché
Imaging of Cervical Spine Trauma
 Imaging of Cervical Spine Trauma C Craig Blackmore, MD, MPH Professor of Radiology and Adjunct Professor of Health Services University of Washington, Harborview Medical Center Salary support: AHRQ grant
Imaging of Cervical Spine Trauma C Craig Blackmore, MD, MPH Professor of Radiology and Adjunct Professor of Health Services University of Washington, Harborview Medical Center Salary support: AHRQ grant
Scenario #4A: Geriatric Trauma Resuscitation Version-5
 Scenario #4A: Geriatric Trauma Resuscitation Version-5 Goals & Objectives: 1. Discuss the principles of initial assessment of a geriatric trauma patient. 2. Recognize physiologic and anatomic changes that
Scenario #4A: Geriatric Trauma Resuscitation Version-5 Goals & Objectives: 1. Discuss the principles of initial assessment of a geriatric trauma patient. 2. Recognize physiologic and anatomic changes that
PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT
 PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT Board Approved June 2007 Revised December 2009 Revised July 2011 Revised June 2015 435 Hunter Street Fredericksburg, VA 22401
PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT Board Approved June 2007 Revised December 2009 Revised July 2011 Revised June 2015 435 Hunter Street Fredericksburg, VA 22401
UHSM ED Pathway ELDERLY FALL / COLLAPSE
 UHSM ED Pathway ELDERLY FALL / COLLAPSE Patient name / Pathway for patients who require assessment in ED after a fall or collapse Note: - It can be used if the patient has also sustained a minor head injury
UHSM ED Pathway ELDERLY FALL / COLLAPSE Patient name / Pathway for patients who require assessment in ED after a fall or collapse Note: - It can be used if the patient has also sustained a minor head injury
3/10/17 Spinal a Injury 1
 Spinal Injury 1 'Paralysed' Watmough vows he'll have the backbone for Game Two after treatment for neck injury Watmough will have cortisone injected into his spine this morning to speed up the recovery
Spinal Injury 1 'Paralysed' Watmough vows he'll have the backbone for Game Two after treatment for neck injury Watmough will have cortisone injected into his spine this morning to speed up the recovery
Pediatric Trauma Management For EMS
 Pediatric Trauma Management For EMS Michael D. McGonigal MD Objectives Discuss important concepts in initial pediatric trauma care, including sports and head injuries Review several pediatric trauma cases
Pediatric Trauma Management For EMS Michael D. McGonigal MD Objectives Discuss important concepts in initial pediatric trauma care, including sports and head injuries Review several pediatric trauma cases
Patient Information. Age: 8 y/o Sex: Female. Date of Admission: Date of Discharge:
 Patient Information Age: 8 y/o Sex: Female Date of Admission: 92-10-08 Date of Discharge: 92-10-18 Chief Complaint Severe admominal pain and vomiting with dysuria since last afternoon Present Illness Lower
Patient Information Age: 8 y/o Sex: Female Date of Admission: 92-10-08 Date of Discharge: 92-10-18 Chief Complaint Severe admominal pain and vomiting with dysuria since last afternoon Present Illness Lower
Injuries to the head and spine
 Injuries to the head and spine Aaron J. Katz, AEMT-P, CIC www.es26medic.net 2013 Nervous System Two sub-systems Central Nervous System ( CNS ) Brain and spinal cord Peripheral Nervous System 12 cranial
Injuries to the head and spine Aaron J. Katz, AEMT-P, CIC www.es26medic.net 2013 Nervous System Two sub-systems Central Nervous System ( CNS ) Brain and spinal cord Peripheral Nervous System 12 cranial
Chapter 32. Injuries to the Spine by Pearson Education, Inc. Upper Saddle River, New Jersey
 Chapter Injuries to the Spine Topics Anatomy and physiology of the spine Spinal injuries Guidelines for immobilization Special considerations Enrichment Introduction Injuries to the spine are among the
Chapter Injuries to the Spine Topics Anatomy and physiology of the spine Spinal injuries Guidelines for immobilization Special considerations Enrichment Introduction Injuries to the spine are among the
Trauma Registry Documentation December 16, 2014
 Trauma Registry Documentation December 16, 2014 The State of Florida now requires ALL Acute Care hospitals to submit data to the statetrauma Registry. Although Baptist Health hospitals are NOT Trauma Centers
Trauma Registry Documentation December 16, 2014 The State of Florida now requires ALL Acute Care hospitals to submit data to the statetrauma Registry. Although Baptist Health hospitals are NOT Trauma Centers
To Backboard or Not To Backboard? Selective Spinal Immobilization
 To Backboard or Not To Backboard? Selective Spinal Immobilization Will Smith, MD, EMT-P Medical Director Grand Teton National Park and Jackson Hole Fire/EMS, Jackson, WY www.wildmedconsulting.com Objectives
To Backboard or Not To Backboard? Selective Spinal Immobilization Will Smith, MD, EMT-P Medical Director Grand Teton National Park and Jackson Hole Fire/EMS, Jackson, WY www.wildmedconsulting.com Objectives
Kathryn Nuss, MD Associate Trauma Medical Director Associate Director, Emergency Medicine
 Running on Empty Kathryn Nuss, MD Associate Trauma Medical Director Associate Director, Emergency Medicine Nationwide id Children s Hospital Associate Professor, Department of Pediatrics The Ohio State
Running on Empty Kathryn Nuss, MD Associate Trauma Medical Director Associate Director, Emergency Medicine Nationwide id Children s Hospital Associate Professor, Department of Pediatrics The Ohio State
Heidi Lako-Adamson, MD, NRP, FAEMS FM Ambulance and Sanford EMS Education Medical Director
 Heidi Lako-Adamson, MD, NRP, FAEMS FM Ambulance and Sanford EMS Education Medical Director Spinal cord injury statistics. Definition of spinal motion restriction. Difference between spinal motion restriction
Heidi Lako-Adamson, MD, NRP, FAEMS FM Ambulance and Sanford EMS Education Medical Director Spinal cord injury statistics. Definition of spinal motion restriction. Difference between spinal motion restriction
Dr. Mike Brzozowski Trauma Team Leader and Emergency. Sunnybrook Health Sciences Centre Toronto, Ontario
 Dr. Mike Brzozowski Trauma Team Leader and Emergency Physician i Sunnybrook Health Sciences Centre Toronto, Ontario Learning Objectives To better understand the controversies with respect to the rational
Dr. Mike Brzozowski Trauma Team Leader and Emergency Physician i Sunnybrook Health Sciences Centre Toronto, Ontario Learning Objectives To better understand the controversies with respect to the rational
CERVICAL SPINE CLEARANCE
 DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
 55-year-old male with 2nd and 3rd degree burns to face, chest, and arms on 25% of the body Respirations: 34 Pulse: 120 Mental Status: moans to painful stimulus Mucous membranes charred Stridor 10 cm scalp
55-year-old male with 2nd and 3rd degree burns to face, chest, and arms on 25% of the body Respirations: 34 Pulse: 120 Mental Status: moans to painful stimulus Mucous membranes charred Stridor 10 cm scalp