Kobe University Repository : Kernel
|
|
|
- Caroline Francis
- 6 years ago
- Views:
Transcription


1 Title Author(s) Citation Issue date Resource Type Resource Version DOI URL Kobe University Repository : Kernel Marked increase in bone formation markers after cinacalcet treatment by mechanisms distinct from hungry bone syndrome in a haemodialysis patient Goto, Shunsuke / Fujii, Hideki / Matsui, Yutaka / Fukagawa, Masafumi NDT Plus,3(1):71-73 Journal Article / 学術雑誌論文 author /ndtplus/sfp138 Create Date:
2 Marked increase in bone formation markers after cinacalcet treatment by mechanisms distinct from hungry bone syndrome in a hemodialysis patient Shunsuke Goto, MD 1, Hideki Fujii, MD 1, Yutaka Matsui, MD 2, Masafumi Fukagawa, MD 1 1 Division of Nephrology and Kidney Center, Kobe University School of Medicine, Kobe, Japan 2 Matsui-clinic, Akashi, Japan Corresponding author: Masafumi Fukagawa, MD, PhD, FASN Division of Nephrology and Kidney Center, Kobe University School of Medicine, Kusunoki-cho, Chuo-ku, Kobe, Hyogo , Japan Tel: ; Fax: ; fukagawa@med.kobe-u.ac.jp Running title: Cinacalcet may promote bone formation 1
3 Abstract A 59-year-old female who was on dialysis due to diabetic nephropathy was referred to our hospital for severe hyperparathyroidism refractory to intravenous vitamin D receptor activator treatment. With subsequent cinacalcet hydrochloride treatment, parathyroid hormone (PTH) levels were only slightly suppressed. However, progressive increases were observed in serum alkaline phosphatase (ALP) and bone-specific alkaline phosphatase (BAP) levels with mild hypocalcemia. Bone biopsy, obtained immediately before surgical parathyroidectomy after three months of cinacalcet treatment, revealed no disappearance of osteoclasts. These data suggest that cinacalcet hydrochloride treatment may induce marked promotion of bone formation by mechanisms distinct from hungry bone syndrome that usually develops after parathyroidectomy. Keywords: bone formation; cinacalcet hydrochloride; secondary hyperparathyroidism 2
4 Background Cinacalcet hydrochloride is a new class of drugs for the treatment of severe secondary hyperparathyroidism in hemodialysis patients. It has also been reported that successful suppression of parathyroid hormone (PTH) levels results in a decrease in serum markers for bone formation [1, 2]. Here, we report a case of a dialysis patient presenting with severe hyperparathyroidism, who was treated with cinacalcet hydrochloride. Without significant suppression or further increases in PTH levels, marked and progressive increases in serum markers for bone formation were observed. Bone histology did not support the development of hungry bone syndrome, as was presumed in previous cases. Case report A 59-year-old female with diabetic nephropathy was referred to our hospital for bone pain. She was on dialysis therapy three times a week for nine years. She had severe hyperparathyroidism (whole PTH level, 904 pg/ml; normal, 9 39 pg/ml) with a single enlarged parathyroid gland (16 mm 15 mm 19 mm). Although intensive intravenous vitamin D receptor activator (VDRA) treatments were performed several years ago, secondary hyperparathyroidism progressed. The dose of vitamin D was decreased because of concomitant hypercalcemia. Although 22-oxacalcitriol (OCT) was administered at a dose of 2.5 g twice a month since January 2007, OCT was stopped in August Because of the 3
5 progression of secondary hyperparathyroidism, OCT was started again at a dose of 10 g once a week since October However, OCT was stopped in February Although calcium carbonate was administered at a dose of 1.5 g/day, no phosphate binder was administered since January While planning a surgical parathyroidectromy which was scheduled to be conducted in near future, cinacalcet hydrochloride was started at a dose of 25 mg per day and was finally increased to 75 mg per day. Cinacalcet hydrochloride therapy induced a mild decrease in the patient s serum calcium and phosphate levels. PTH levels also decreased slightly, whereas serum alkaline phosphatase (ALP) levels (normal: IU/L) increased significantly and progressively after the start of cinacalcet treatment, as shown in Figure 1. Serum bone-specific alkaline phosphatase (BAP) levels also significantly increased from 295 U/L to 995 U/L (normal: U/L) during the therapy. The patient had no evidence of bone fracture by X-ray imaging. There was no difference in bone scintigraphies obtained before and after three months of initiating cinacalcet therapy. On the other hand, serum bone resorption marker type I collagen cross-linked N-telopeptide (NTx) levels were significantly high ( nmolbce/l; normal, nmolbce/l) after three months of initiating cinacalcet therapy. We performed surgical parathyroidectomy three months after the start of cinacalcet treatment. During the operation, an iliac bone biopsy was performed before removing the parathyroid tissue to identify the cause of elevation of serum ALP and BAP levels. The bone 4
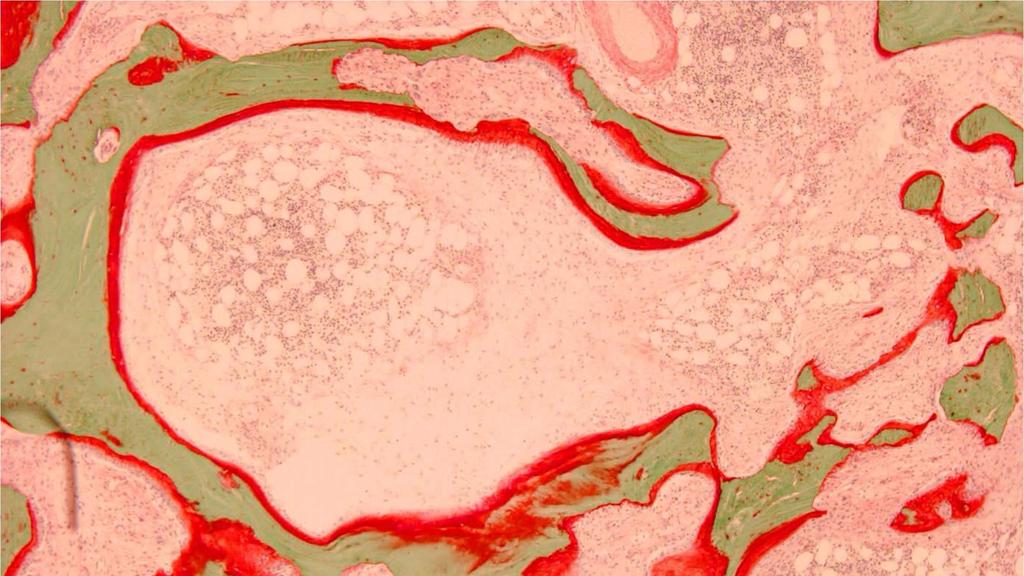
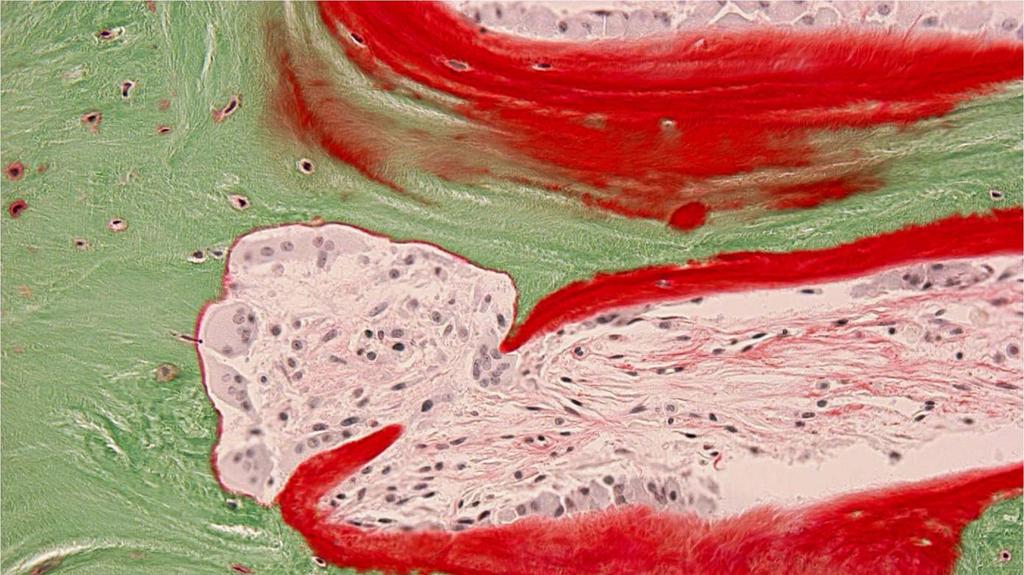
6 biopsy specimen demonstrated osteitis fibrosa (fibrosis volume/tissue volume 21.4%) and defective mineralization (osteoid volume/bone volume 29.1%) (Figure 2A). With regard to bone formation parameters, osteoblast surface/bone surface (BS) increased (25.3%). Bone formation rate (BFR)/BS also increased to m 3 /m 2 /year (normal: 0.015± m 3 /m 2 /year). However, we could not measure BFR precisely due to blurred tetracycline labels. Multinucleated osteoclasts resorbing mineralized bone were observed, in contrast to the mechanisms observed in hungry bone syndrome after parathyroidectomy (Figure 2B). Staining for aluminum was negative and she has never been treated with aluminum gels. After parathyroidectomy, serum PTH levels decreased immediately to levels below the detection limit. In addition, the patient reported the disappearance of bone pain. Serum ALP levels decreased slowly and returned to a normal range at 6 months after parathyroidectomy. Discussion Cinacalcet hydrochloride reduces serum PTH levels by direct action on calcium-sensing receptor in parathyroid, thereby decreasing bone formation markers in hemodialysis patients [1, 2]. Nevertheless, in a recent report of a clinical trial, it has been shown that serum BAP levels increase at early time after the start of cinacalcet treatment [2, 3]. This temporary increase of BAP was assumed to be a result of hungry bone syndrome without bone biopsy. Although development of hungry bone syndrome by cinacalcet was reported previously in two reports [4, 5], the authors failed to describe the changes in bone formation markers after 5
7 the administration of cinacalcet. Typical hungry bone syndrome develops after surgical parathyroidectomy and is characterized by hypocalcemia and a temporary increase in bone formation. According to another recent report, osteoclasts disappear immediately after parathyroidectomy [6]. Bone histology of this particular case did not support the development of hungry bone syndrome seen after parathyroidectomy. In the present case, neither progression of hyperparathyroidism nor the sudden decrease of PTH level, as in spontaneous infarction, were observed during cinacalcet treatment. We could not find any evidence of bone fracture by X-ray or in changes of bone scintigraphies. Although we could not completely rule out the possibility of microfractures, we hypothesized that bone formation is possibly enhanced as a result of cinacalcet treatment by unknown mechanisms. We failed to demonstrate the pathomechanism of bone biopsy clearly because of the bone biopsy specimen only at the end of cinacalcet treatment and not prior to treatment. Cinacalcet reduces serum PTH levels maximally around 2 to 4 h after administration. Therefore, cinacalcet induces daily fluctuation of serum PTH levels, which differs from VDRA treatments. As reported previously, PTH (1 34) has different effects on bone mass when administrated by intermittent injections or by continuous infusion [7]. Furthermore, it has been suggested that intermittent decreases in serum PTH levels by oral administration of calcimimetics have an anabolic-like effect on the bones, whereas continuous suppression of PTH by calcimimetics infusion does not have a similar effect [8]. Therefore, we conclude that daily fluctuations of PTH, as induced by cinacalcet treatment, may have promoted bone 6
8 formation. Osteoblasts express calcium-sensing receptors. It has been shown that high extracellular ionized calcium concentration stimulation induces mitogenic action of osteoblasts via calcium-sensing receptors [9]. However, the calcium-sensing receptor in osteoblasts may be different from parathyroid [10]. Therefore, further studies will be necessary to clarify whether cinacalcet has direct effects on osteoblast. The bone histology in our case also showed defective mineralization. Hypovitaminosis D probably induced defective mineralization because serum vitamin D levels at bone biopsy were low (1,25(OH) 2 D 3 level, 5.6 pg/ml; normal, pg/ml: 25(OH)D 3 level, 21 ng/ml; normal, 7 41 ng/ml). However, since hypovitaminosis D may be recognized before the start of cinacalcet treatment, the significance of hypovitaminosis D for bone formation markers in this case is unclear. In summary, we have reported a case with marked increase of serum markers for bone formation due to cinacalcet treatment. The mechanism responsible for bone formation was distinct from hungry bone syndrome. We concluded that the fluctuation of PTH levels may have promoted bone formation. 7
9 References 1. Malluche HH, Monier-Faugere MC, Wang G, et al. An assessment of cinacalcet HCl effects on bone histology in dialysis patients with secondary hyperparathyroidism. Clin Nephrol 2008; 69: Fukagawa M, Yumita S, Akizawa T et al. Cinacalcet (KRN1493) effectively decreases the serum intact PTH level with favorable control of the serum phosphorus and calcium levels in Japanese dialysis patients. Nephrol Dial Transplant 2008; 23: Shigematsu T, Akizawa T, Uchida E et al. Long-term cinacalcet HCl treatment improved bone metabolism in Japanese hemodialysis patients with secondary hyperparathyroidism. Am J Nephrol 2009; 29: Nowack R, Wachtler P. Hypophosphatemia and hungry bone syndrome in a dialysis patient with secondary hyperparathyroidism treated with cinacalcet proposal for an improved monitoring. Clin Lab 2006; 52: Lazar ES, Stankus N. Cinacalcet-induced hungry bone syndrome. Semin Dial 2007; 20: Yajima A, Ogawa Y, Takahashi HE, Tominaga Y, Inou T, Otsubo O. Changes of bone remodeling immediately after parathyroidectomy for secondary hyperparathyroidism. Am J Kidney Dis 2003; 42: Chen P, Satterwhite JH, Licata AA et al. Early changes in biochemical markers of bone formation predict BMD response to teriparatide in postmenopausal women with 8
10 osteoporosis. J Bone Miner Res 2005; 20: Ishii H, Wada M, Furuya Y, Nagano N, Nemeth EF, Fox J. Daily intermittent decreases in serum levels of parathyroid hormone have an anabolic-like action on the bones of uremic rats with low-turnover bone and osteomalacia. Bone 2000; 26: Chattopadhyay N, Yano S, Tfelt-Hansen J et al. Mitogenic action of calcium-sensing receptor on rat calvarial osteoblasts. Endocrinology 2004; 145: Pi M, Quarles LD. Osteoblast calcium-sensing receptor has characteristics of ANF/7TM receptors. J Cell Biochem 2005; 95:
11 Figure legends Figure 1 Change of serum ALP, PTH, calcium, and phosphate levels before and after the administration of cinacalcet hydrochloride. Figure 2 (A) Increased collagen fibres and fraction of trabecular surface covered by osteoid. (Villanueva Goldner stain, 40 ) (B) Multinucleated osteoclasts (arrows) resorbing mineralized bone. (Villanueva Goldner stain, 200 ) 10
12 cinacalcet HCl 22-oxacalcitriol w-pth (pg/ml) ALP (IU/L) Ca (mg/dl) P (mg/dl) ALP w-pth Ca P

13 A

14 B
Ca, Mg metabolism, bone diseases. Tamás Kőszegi Pécs University, Department of Laboratory Medicine Pécs, Hungary
 Ca, Mg metabolism, bone diseases Tamás Kőszegi Pécs University, Department of Laboratory Medicine Pécs, Hungary Calcium homeostasis Ca 1000g in adults 99% in bones (extracellular with Mg, P) Plasma/intracellular
Ca, Mg metabolism, bone diseases Tamás Kőszegi Pécs University, Department of Laboratory Medicine Pécs, Hungary Calcium homeostasis Ca 1000g in adults 99% in bones (extracellular with Mg, P) Plasma/intracellular
Secondary Hyperparathyroidism: Where are we now?
 Secondary Hyperparathyroidism: Where are we now? Dylan M. Barth, Pharm.D. PGY-1 Pharmacy Resident Mayo Clinic 2017 MFMER slide-1 Objectives Identify risk factors for the development of complications caused
Secondary Hyperparathyroidism: Where are we now? Dylan M. Barth, Pharm.D. PGY-1 Pharmacy Resident Mayo Clinic 2017 MFMER slide-1 Objectives Identify risk factors for the development of complications caused
Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital
 Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 13, 2017 Disclosures statement: Consultant: Allena, Becker
Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 13, 2017 Disclosures statement: Consultant: Allena, Becker
Bone Disorders in CKD
 Osteoporosis in Dialysis Patients Challenges in Management David M. Klachko MD FACP Professor Emeritus of Medicine University of Missouri-Columbia Bone Disorders in CKD PTH-mediated high-turnover (osteitis
Osteoporosis in Dialysis Patients Challenges in Management David M. Klachko MD FACP Professor Emeritus of Medicine University of Missouri-Columbia Bone Disorders in CKD PTH-mediated high-turnover (osteitis
Metabolic Bone Disease Related to Chronic Kidney Disease
 Metabolic Bone Disease Related to Chronic Kidney Disease Deborah Sellmeyer, MD Director, Johns Hopkins Metabolic Bone Center Dept of Medicine, Division of Endocrinology Disclosure DSMB member for denosumab
Metabolic Bone Disease Related to Chronic Kidney Disease Deborah Sellmeyer, MD Director, Johns Hopkins Metabolic Bone Center Dept of Medicine, Division of Endocrinology Disclosure DSMB member for denosumab
CKD-Mineral Bone Disorder (MBD) Pathogenesis of Metabolic Bone Disease. Grants: NIH, Abbott, Amgen, OPKO, Shire
 Pathogenesis of Metabolic Bone Disease. Grants: NIH, Abbott, Amgen, OPKO, Shire") Pathogenesis of Metabolic Bone Disease Stuart M. Sprague, D.O. Chief, Division of Nephrology and Hypertension Professor of Medicine NorthShore University HealthSystem University of Chicago Pritzker School
Pathogenesis of Metabolic Bone Disease Stuart M. Sprague, D.O. Chief, Division of Nephrology and Hypertension Professor of Medicine NorthShore University HealthSystem University of Chicago Pritzker School
The role of calcimimetics in chronic kidney disease
 http://www.kidney-international.org & 2006 International Society of Nephrology The role of calcimimetics in chronic kidney disease A Gal-Moscovici 1,2 and SM Sprague 1 1 Division of Nephrology and Hypertension,
http://www.kidney-international.org & 2006 International Society of Nephrology The role of calcimimetics in chronic kidney disease A Gal-Moscovici 1,2 and SM Sprague 1 1 Division of Nephrology and Hypertension,
CKD: Bone Mineral Metabolism. Peter Birks, Nephrology Fellow
 CKD: Bone Mineral Metabolism Peter Birks, Nephrology Fellow CKD - KDIGO Definition and Classification of CKD CKD: abnormalities of kidney structure/function for > 3 months with health implications 1 marker
CKD: Bone Mineral Metabolism Peter Birks, Nephrology Fellow CKD - KDIGO Definition and Classification of CKD CKD: abnormalities of kidney structure/function for > 3 months with health implications 1 marker
Sensipar. Sensipar (cinacalcet) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.46 Subject: Sensipar Page: 1 of 5 Last Review Date: June 22, 2018 Sensipar Description Sensipar (cinacalcet)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.46 Subject: Sensipar Page: 1 of 5 Last Review Date: June 22, 2018 Sensipar Description Sensipar (cinacalcet)
Cinacalcet treatment in advanced CKD - is it justified?
 Cinacalcet treatment in advanced CKD - is it justified? Goce Spasovski ERBP Advisory Board member University of Skopje, R. Macedonia TSN Congress October 21, 2017, Antalya Session Objectives From ROD to
Cinacalcet treatment in advanced CKD - is it justified? Goce Spasovski ERBP Advisory Board member University of Skopje, R. Macedonia TSN Congress October 21, 2017, Antalya Session Objectives From ROD to
Guidelines and new evidence on CKD - MBD treatment
 Guidelines and new evidence on CKD - MBD treatment Goce Spasovski ERBP Advisory Board member University of Skopje, R. Macedonia ERA-EDTA CME course IV Congress of Nephrology of B&H, April 25, 2015, Sarajevo,
Guidelines and new evidence on CKD - MBD treatment Goce Spasovski ERBP Advisory Board member University of Skopje, R. Macedonia ERA-EDTA CME course IV Congress of Nephrology of B&H, April 25, 2015, Sarajevo,
Persistent post transplant hyperparathyroidism. Shiva Seyrafian IUMS-97/10/18-8/1/2019
 Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
OSTEOMALACIA UPDATE. Nothing to Disclose. Daniel D Bikle, MD, PhD Professor of Medicine University of California and VA Medical Center San Francisco
 OSTEOMALACIA UPDATE Daniel D Bikle, MD, PhD Professor of Medicine University of California and VA Medical Center San Francisco Nothing to Disclose 1 Case History 59 YO WM referred for evaluation of diffuse
OSTEOMALACIA UPDATE Daniel D Bikle, MD, PhD Professor of Medicine University of California and VA Medical Center San Francisco Nothing to Disclose 1 Case History 59 YO WM referred for evaluation of diffuse
Nuclear Chromatin-concentrated Osteoblasts in Renal Bone Diseases
 tap_919 9..13 Therapeutic Apheresis and Dialysis 15(Supplement 1):9 13 doi: 1.1111/j.1744-9987.211.919.x Therapeutic Apheresis and Dialysis 211 International Society for Apheresis Nuclear Chromatin-concentrated
tap_919 9..13 Therapeutic Apheresis and Dialysis 15(Supplement 1):9 13 doi: 1.1111/j.1744-9987.211.919.x Therapeutic Apheresis and Dialysis 211 International Society for Apheresis Nuclear Chromatin-concentrated
Ramzi Vareldzis, MD Avanelle Jack, MD Dept of Internal Medicine Section of Nephrology and Hypertension LSU Health New Orleans September 13, 2016
 Ramzi Vareldzis, MD Avanelle Jack, MD Dept of Internal Medicine Section of Nephrology and Hypertension LSU Health New Orleans September 13, 2016 1 MBD + CKD in Elderly patients Our focus for today: CKD
Ramzi Vareldzis, MD Avanelle Jack, MD Dept of Internal Medicine Section of Nephrology and Hypertension LSU Health New Orleans September 13, 2016 1 MBD + CKD in Elderly patients Our focus for today: CKD
Reversal of adynamic bone disease by lowering of dialysate calcium
 http://www.kidney-international.org & 26 International Society of Nephrology original article Reversal of adynamic bone disease by lowering of dialysate calcium A Haris 1, DJ Sherrard 2 and G Hercz 3 1
http://www.kidney-international.org & 26 International Society of Nephrology original article Reversal of adynamic bone disease by lowering of dialysate calcium A Haris 1, DJ Sherrard 2 and G Hercz 3 1
A calcimimetic agent acutely suppresses parathyroid hormone levels in patients with chronic renal failure Rapid Communication
 Kidney International, Vol. 53 (1998), pp. 223 227 A calcimimetic agent acutely suppresses parathyroid hormone levels in patients with chronic renal failure Rapid Communication JOHN E. ANTONSEN, DONALD
Kidney International, Vol. 53 (1998), pp. 223 227 A calcimimetic agent acutely suppresses parathyroid hormone levels in patients with chronic renal failure Rapid Communication JOHN E. ANTONSEN, DONALD
Renal Osteodystrophy. Chapter 6. I. Introduction. Classification of Bone Disease. Eric W. Young
 Chapter 6 Renal Osteodystrophy Eric W. Young I. Introduction Renal osteodystrophy refers to bone disease that occurs in patients with kidney disease. Bone disease occurs across the full spectrum of kidney
Chapter 6 Renal Osteodystrophy Eric W. Young I. Introduction Renal osteodystrophy refers to bone disease that occurs in patients with kidney disease. Bone disease occurs across the full spectrum of kidney
Effect of percutaneous calcitriol injection therapy on secondary hyperparathyroidism in uraemic patients
 Nephrol Dial Transplant (2003) 18 [Suppl 3]: iii42 iii46 DOI: 10.1093/ndt/gfg1011 Effect of percutaneous calcitriol injection therapy on secondary hyperparathyroidism in uraemic patients Kazuhiro Shiizaki
Nephrol Dial Transplant (2003) 18 [Suppl 3]: iii42 iii46 DOI: 10.1093/ndt/gfg1011 Effect of percutaneous calcitriol injection therapy on secondary hyperparathyroidism in uraemic patients Kazuhiro Shiizaki
Original Article. Introduction. serum calcium and phosphorus levels in Japanese patients, having a longer average dialysis vintage.
 Nephrol Dial Transplant (2008) 23: 328 335 doi:10.1093/ndt/gfm534 Advance Access publication 23 August 2007 Original Article Cinacalcet (KRN1493) effectively decreases the serum intact PTH level with favorable
Nephrol Dial Transplant (2008) 23: 328 335 doi:10.1093/ndt/gfm534 Advance Access publication 23 August 2007 Original Article Cinacalcet (KRN1493) effectively decreases the serum intact PTH level with favorable
Differences in bone turnover and intact PTH levels between African American and Caucasian patients with end-stage renal disease
 Kidney International, Vol. 64 (2003), pp. 737 742 Differences in bone turnover and intact PTH levels between African American and Caucasian patients with end-stage renal disease B. PETER SAWAYA, REZKALLA
Kidney International, Vol. 64 (2003), pp. 737 742 Differences in bone turnover and intact PTH levels between African American and Caucasian patients with end-stage renal disease B. PETER SAWAYA, REZKALLA
Chapter 5: Evaluation and treatment of kidney transplant bone disease Kidney International (2009) 76 (Suppl 113), S100 S110; doi: /ki.2009.
 76 (Suppl 113), S100 S110; doi: /ki.2009.") http://www.kidney-international.org & 2009 KDIGO Chapter 5: Evaluation and treatment of kidney transplant bone disease ; doi:10.1038/ki.2009.193 Grade for strength of recommendation a Strength Wording
http://www.kidney-international.org & 2009 KDIGO Chapter 5: Evaluation and treatment of kidney transplant bone disease ; doi:10.1038/ki.2009.193 Grade for strength of recommendation a Strength Wording
38 year old Male with Ankylosing Spondylitis. Olesya Krivospitskaya, MD April,
 38 year old Male with Ankylosing Spondylitis Olesya Krivospitskaya, MD April, 11 2013 HPI (Letter from the patient): Diagnosed with Ankylosing Spondylitis and prescribed a Sulfa drug to help with my back
38 year old Male with Ankylosing Spondylitis Olesya Krivospitskaya, MD April, 11 2013 HPI (Letter from the patient): Diagnosed with Ankylosing Spondylitis and prescribed a Sulfa drug to help with my back
Hyperparathyroidism: Operative Considerations. Financial Disclosures: None. Hyperparathyroidism. Hyperparathyroidism 11/10/2012
 Hyperparathyroidism: Operative Considerations Financial Disclosures: None Steven J Wang, MD FACS Associate Professor Dept of Otolaryngology-Head and Neck Surgery University of California, San Francisco
Hyperparathyroidism: Operative Considerations Financial Disclosures: None Steven J Wang, MD FACS Associate Professor Dept of Otolaryngology-Head and Neck Surgery University of California, San Francisco
Bone and Mineral. Comprehensive Menu for the Management of Bone and Mineral Related Diseases
 Bone and Mineral Comprehensive Menu for the Management of Bone and Mineral Related Diseases Innovation to Assist in Clinical Diagnosis and Treatment DiaSorin offers a specialty line of Bone and Mineral
Bone and Mineral Comprehensive Menu for the Management of Bone and Mineral Related Diseases Innovation to Assist in Clinical Diagnosis and Treatment DiaSorin offers a specialty line of Bone and Mineral
( ) , (Donabedian, 1980) We would not choose any treatment with poor outcomes
 , (Donabedian, 1980) We would not choose any treatment with poor outcomes") ..., 2013 Amgen. 1 ? ( ), (Donabedian, 1980) We would not choose any treatment with poor outcomes 1. :, 2. ( ): 3. :.,,, 4. :, [Biomarkers Definitions Working Group, 2001]., (William M. Bennet, Nefrol
..., 2013 Amgen. 1 ? ( ), (Donabedian, 1980) We would not choose any treatment with poor outcomes 1. :, 2. ( ): 3. :.,,, 4. :, [Biomarkers Definitions Working Group, 2001]., (William M. Bennet, Nefrol
Approach to a patient with hypercalcemia
 Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
HYDROCHLORIDE FOR THE TREATMENT OF SECONDARY HYPERPARATHYROIDISM IN PATIENTS WITH END-STAGE RENAL DISEASE ON MAINTENANCE DIALYSIS THERAPY
 UK RENAL PHARMACY GROUP SUBMISSION TO THE NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE on CINACALCET HYDROCHLORIDE FOR THE TREATMENT OF SECONDARY HYPERPARATHYROIDISM IN PATIENTS WITH END-STAGE RENAL DISEASE
UK RENAL PHARMACY GROUP SUBMISSION TO THE NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE on CINACALCET HYDROCHLORIDE FOR THE TREATMENT OF SECONDARY HYPERPARATHYROIDISM IN PATIENTS WITH END-STAGE RENAL DISEASE
Secondary hyperparathyroidism an Update on Pathophysiology and Treatment
 Secondary hyperparathyroidism an Update on Pathophysiology and Treatment Klaus Olgaard Copenhagen Budapest Nephrology School August 2007 HPT IN CRF Renal mass Ca 2+ 1,25(OH) 2 D 3 CaR Hyperparathyroidism
Secondary hyperparathyroidism an Update on Pathophysiology and Treatment Klaus Olgaard Copenhagen Budapest Nephrology School August 2007 HPT IN CRF Renal mass Ca 2+ 1,25(OH) 2 D 3 CaR Hyperparathyroidism
Incorporating K/DOQI Using a Novel Algorithm Approach: Regina Qu Appelle s Experience
 Incorporating K/DOQI Using a Novel Algorithm Approach: Regina Qu Appelle s Experience Michael Chan, Renal Dietitian Regina Qu Appelle Health Region BC Nephrology Days There is a strong association among
Incorporating K/DOQI Using a Novel Algorithm Approach: Regina Qu Appelle s Experience Michael Chan, Renal Dietitian Regina Qu Appelle Health Region BC Nephrology Days There is a strong association among
Case Report Use of Percutaneous Ethanol Injection Therapy for Recurrent Secondary Hyperparathyroidism after Subtotal Parathyroidectomy
 SAGE-Hindawi Access to Research International Nephrology Volume 211, Article ID 246734, 6 pages doi:1.461/211/246734 Case Report Use of Percutaneous Ethanol Injection Therapy for Recurrent Secondary Hyperparathyroidism
SAGE-Hindawi Access to Research International Nephrology Volume 211, Article ID 246734, 6 pages doi:1.461/211/246734 Case Report Use of Percutaneous Ethanol Injection Therapy for Recurrent Secondary Hyperparathyroidism
Original Article Fasting Plasma Glucose Levels Are Related to Bone Mineral Density in Postmenopausal Women with Primary Hyperparathyroidism
 www.ijcem.com/ijcem807001 Original Article Fasting Plasma Glucose Levels Are Related to Bone Mineral Density in Postmenopausal Women with Primary Hyperparathyroidism Itoko Hisa 1, Hiroshi Kaji 1, Yoshifumi
www.ijcem.com/ijcem807001 Original Article Fasting Plasma Glucose Levels Are Related to Bone Mineral Density in Postmenopausal Women with Primary Hyperparathyroidism Itoko Hisa 1, Hiroshi Kaji 1, Yoshifumi
Management of mineral and bone disorders in renal transplant recipients
 Nephrology 22, Suppl. 2 (2017) 65 69 Management of mineral and bone disorders in renal transplant recipients MATTHEW J DAMASIEWICZ 1,3 and PETER R EBELING 2,3,4 Departments of 1 Nephrology, and 2 Endocrinology,
Nephrology 22, Suppl. 2 (2017) 65 69 Management of mineral and bone disorders in renal transplant recipients MATTHEW J DAMASIEWICZ 1,3 and PETER R EBELING 2,3,4 Departments of 1 Nephrology, and 2 Endocrinology,
OPEN. Masahiro Yoshikawa 1,2, Osamu Takase 1,2, Taro Tsujimura
 www.nature.com/scientificreports Received: 26 September 2017 Accepted: 19 March 2018 Published: xx xx xxxx OPEN Long-term effects of low calcium dialysates on the serum calcium levels during maintenance
www.nature.com/scientificreports Received: 26 September 2017 Accepted: 19 March 2018 Published: xx xx xxxx OPEN Long-term effects of low calcium dialysates on the serum calcium levels during maintenance
Frequency of Metabolic Bone Disease in Haemodialysis Patients
 Frequency of Metabolic Bone Disease in Haemodialysis Patients Pages with reference to book, From 83 To 86 Rizwan Hussain, Arshad Ahmed, Abdul Salam Soomro, Saeed Hassan Chishty, Syed Ali Jaffar Naqvi (
Frequency of Metabolic Bone Disease in Haemodialysis Patients Pages with reference to book, From 83 To 86 Rizwan Hussain, Arshad Ahmed, Abdul Salam Soomro, Saeed Hassan Chishty, Syed Ali Jaffar Naqvi (
The Parsabiv Beginner s Book
 The Parsabiv Beginner s Book A quick guide to help you learn about your treatment with Parsabiv and what to expect Indication Parsabiv (etelcalcetide) is indicated for the treatment of secondary hyperparathyroidism
The Parsabiv Beginner s Book A quick guide to help you learn about your treatment with Parsabiv and what to expect Indication Parsabiv (etelcalcetide) is indicated for the treatment of secondary hyperparathyroidism
chapter 1 & 2009 KDIGO
 http://www.kidney-international.org chapter 1 & 2009 DIGO Chapter 1: Introduction and definition of CD MBD and the development of the guideline statements idney International (2009) 76 (Suppl 113), S3
http://www.kidney-international.org chapter 1 & 2009 DIGO Chapter 1: Introduction and definition of CD MBD and the development of the guideline statements idney International (2009) 76 (Suppl 113), S3
Sensipar (cinacalcet)
") Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Treatment Options for Chronic Kidney
 Treatment Options for Chronic Kidney Disease: Metabolic Introduction Bone Disease to Renagel Goce Spasovski, R. Macedonia The 17th Budapest Nephrology School, August 29, 2010 Session Objectives Definition
Treatment Options for Chronic Kidney Disease: Metabolic Introduction Bone Disease to Renagel Goce Spasovski, R. Macedonia The 17th Budapest Nephrology School, August 29, 2010 Session Objectives Definition
Posttransplant Bone Disease. Budapest 2007
 Posttransplant Bone Disease Budapest 2007 Post-transplant bone disease 7 10 % of kidney transplanted patients develope a fracture. The risk is higher in postmenopausal female transplanted patients. Diabetic,
Posttransplant Bone Disease Budapest 2007 Post-transplant bone disease 7 10 % of kidney transplanted patients develope a fracture. The risk is higher in postmenopausal female transplanted patients. Diabetic,
PRIMARY HYPERPARATHYROIDISM
 PRIMARY HYPERPARATHYROIDISM HYPERPARATHYROIDISM Inappropriate excess secretion of Parathyroid Hormone in Primary Hyperparathyroidism Appropriate Hypersecretion in Secondary Hyperparathyroidism PTH and
PRIMARY HYPERPARATHYROIDISM HYPERPARATHYROIDISM Inappropriate excess secretion of Parathyroid Hormone in Primary Hyperparathyroidism Appropriate Hypersecretion in Secondary Hyperparathyroidism PTH and
CKD-MBD CKD mineral bone disorder
 CKD Renal bone disease Dr Mike Stone University Hospital Llandough Affects 5 10 % of population Increasingly common Ageing, diabetes, undetected hypertension Associated with: Cardiovascular disease Premature
CKD Renal bone disease Dr Mike Stone University Hospital Llandough Affects 5 10 % of population Increasingly common Ageing, diabetes, undetected hypertension Associated with: Cardiovascular disease Premature
Therapeutic golas in the treatment of CKD-MBD
 Therapeutic golas in the treatment of CKD-MBD Hemodialysis clinic Clinical University Center Sarajevo Bantao, 04-08.10.2017, Sarajevo Abbvie Satellite symposium 06.10.2017 Chronic Kidney Disease Mineral
Therapeutic golas in the treatment of CKD-MBD Hemodialysis clinic Clinical University Center Sarajevo Bantao, 04-08.10.2017, Sarajevo Abbvie Satellite symposium 06.10.2017 Chronic Kidney Disease Mineral
Improvement of adynamic bone disease after renal transplantation
 Brazilian Journal of Medical and Biological Research (2006) 39: 31-41 Adynamic bone disease after transplantation ISSN 0100-879X 31 Improvement of adynamic bone disease after renal transplantation K.A.
Brazilian Journal of Medical and Biological Research (2006) 39: 31-41 Adynamic bone disease after transplantation ISSN 0100-879X 31 Improvement of adynamic bone disease after renal transplantation K.A.
Metabolic Bone Disease (Past, Present and Future Challenges in the Management)
") Metabolic Bone Disease 871 151 Metabolic Bone Disease (Past, Present and Future Challenges in the Management) SNA RIZVI INTRODUCTION The past 40 years have seen some important historical events leading
Metabolic Bone Disease 871 151 Metabolic Bone Disease (Past, Present and Future Challenges in the Management) SNA RIZVI INTRODUCTION The past 40 years have seen some important historical events leading
Bsml Polymorphism of the Vitamin D Receptor Gene in Hyperparathyroid or Hypoparathyroid Dialysis Patients
 Clinical Chemistry / BSMI POLYMORPHISM OF THE VITAMIN D RECEPTOR GENE Bsml Polymorphism of the Vitamin D Receptor Gene in Hyperparathyroid or Hypoparathyroid Dialysis Patients Jacopo Tagliabue, MD,1 Marco
Clinical Chemistry / BSMI POLYMORPHISM OF THE VITAMIN D RECEPTOR GENE Bsml Polymorphism of the Vitamin D Receptor Gene in Hyperparathyroid or Hypoparathyroid Dialysis Patients Jacopo Tagliabue, MD,1 Marco
Persistent knee pain in a patient with systemic lupus erythematosus
 CASE REPORT Port J Nephrol Hypert 2018; 32(4): 374-378 Advance Access publication 31 October 2018 Persistent knee pain in a patient with systemic lupus erythematosus Miguel Bigotte Vieira 1, *, Joana Monteiro
CASE REPORT Port J Nephrol Hypert 2018; 32(4): 374-378 Advance Access publication 31 October 2018 Persistent knee pain in a patient with systemic lupus erythematosus Miguel Bigotte Vieira 1, *, Joana Monteiro
Index. B BMC. See Bone mineral content BMD. See Bone mineral density Bone anabolic impact, Bone mass acquisition
 A Acid base balance dietary protein detrimental effects of, 19 Acid base balance bicarbonate effects, 176 in bone human studies, 174 mechanisms, 173 174 in muscle aging, 174 175 alkali supplementation
A Acid base balance dietary protein detrimental effects of, 19 Acid base balance bicarbonate effects, 176 in bone human studies, 174 mechanisms, 173 174 in muscle aging, 174 175 alkali supplementation
hypercalcemia of malignancy hyperparathyroidism PHPT the most common cause of hypercalcemia in the outpatient setting the second most common cause
 hyperparathyroidism A 68-year-old woman with documented osteoporosis has blood tests showing elevated serum calcium and parathyroid hormone (PTH) levels: 11.2 mg/dl (8.8 10.1 mg/dl) and 88 pg/ml (10-60),
hyperparathyroidism A 68-year-old woman with documented osteoporosis has blood tests showing elevated serum calcium and parathyroid hormone (PTH) levels: 11.2 mg/dl (8.8 10.1 mg/dl) and 88 pg/ml (10-60),
Marie-Claude Monier-Faugere, Hanna Mawad, and Hartmut H. Malluche
 Opposite Effects of Calcitriol and Paricalcitol on the Parathyroid Hormone-(1-84)/Large Carboxy-Terminal- Parathyroid Hormone Fragments Ratio in Patients with Stage 5 Chronic Kidney Disease Marie-Claude
Opposite Effects of Calcitriol and Paricalcitol on the Parathyroid Hormone-(1-84)/Large Carboxy-Terminal- Parathyroid Hormone Fragments Ratio in Patients with Stage 5 Chronic Kidney Disease Marie-Claude
The Role of the Laboratory in Metabolic Bone Disease
 The Role of the Laboratory in Metabolic Bone Disease Howard Morris PhD, FAACB, FFSc(RCPA) President, IFCC Professor of Medical Sciences, University of South Australia, Clinical Scientist, SA Pathology
The Role of the Laboratory in Metabolic Bone Disease Howard Morris PhD, FAACB, FFSc(RCPA) President, IFCC Professor of Medical Sciences, University of South Australia, Clinical Scientist, SA Pathology
Basic and clinical aspects of parathyroid hyperplasia in chronic kidney disease
 http://www.kidney-international.org & 2006 International Society of Nephrology Basic and clinical aspects of parathyroid hyperplasia in chronic kidney disease M Fukagawa 1, S Nakanishi 1 and JJ Kazama
http://www.kidney-international.org & 2006 International Society of Nephrology Basic and clinical aspects of parathyroid hyperplasia in chronic kidney disease M Fukagawa 1, S Nakanishi 1 and JJ Kazama
Glycaemic control and serum intact parathyroid hormone levels in diabetic patients on haemodialysis therapy
 Nephrol Dial Transplant (2008) 23: 315 320 doi: 10.1093/ndt/gfm639 Advance Access publication 23 October 2007 Original Article Glycaemic control and serum intact parathyroid hormone levels in diabetic
Nephrol Dial Transplant (2008) 23: 315 320 doi: 10.1093/ndt/gfm639 Advance Access publication 23 October 2007 Original Article Glycaemic control and serum intact parathyroid hormone levels in diabetic
Treatment Options for Chronic Kidney. Goce Spasovski, R. Macedonia
 Treatment Options for Chronic Kidney Disease: Metabolic Introduction Bone Disease to Renagel Goce Spasovski, R. Macedonia Budapest, August 29, 2011 Session Objectives Definition of the problem of CKD-MBD
Treatment Options for Chronic Kidney Disease: Metabolic Introduction Bone Disease to Renagel Goce Spasovski, R. Macedonia Budapest, August 29, 2011 Session Objectives Definition of the problem of CKD-MBD
Bone strength is proportional to bone mass, measured with DXA. Bone turnover markers indicate the status of bone quality.
 Bone strength is proportional to bone mass, measured with DXA Bone quality depend on bone architecture, rate of bone turnover, quality of bone matrix. Bone turnover markers indicate the status of bone
Bone strength is proportional to bone mass, measured with DXA Bone quality depend on bone architecture, rate of bone turnover, quality of bone matrix. Bone turnover markers indicate the status of bone
Different effects of calcitriol and parathytoidectomy on the PTH-calcium curve in dialysis patients with severe hyperparathyroidism
 Nephrol Dial Transplant (996) : 8-87 Original Article Nephrology Dialysis Transplantation Different effects of calcitriol and parathytoidectomy on the PTH-calcium curve in dialysis patients with severe
Nephrol Dial Transplant (996) : 8-87 Original Article Nephrology Dialysis Transplantation Different effects of calcitriol and parathytoidectomy on the PTH-calcium curve in dialysis patients with severe
Comparison between Whole and Intact Parathyroid Hormone Assays
 tap_926 42..49 Therapeutic Apheresis and Dialysis 15(Supplement 1):42 49 doi: 10.1111/j.1744-9987.2011.00926.x Therapeutic Apheresis and Dialysis 2011 International Society for Apheresis Comparison between
tap_926 42..49 Therapeutic Apheresis and Dialysis 15(Supplement 1):42 49 doi: 10.1111/j.1744-9987.2011.00926.x Therapeutic Apheresis and Dialysis 2011 International Society for Apheresis Comparison between
The Calcium Conundrum: When, What and How to Give Calcium in Pediatric CKD/ESRD
 The Calcium Conundrum: When, What and How to Give Calcium in Pediatric CKD/ESRD Jess Tower MS RD LD 3/18/19 Children s Mercy Hospital jdtower@cmh.edu 816 460 1067 Disclosures Nothing to disclose 1 How
The Calcium Conundrum: When, What and How to Give Calcium in Pediatric CKD/ESRD Jess Tower MS RD LD 3/18/19 Children s Mercy Hospital jdtower@cmh.edu 816 460 1067 Disclosures Nothing to disclose 1 How
Should cinacalcet be used in patients who are not on dialysis?
 Should cinacalcet be used in patients who are not on dialysis? Jorge B Cannata-Andía and José Luis Fernández-Martín Affiliations: Bone and Mineral Research Unit. Hospital Universitario Central de Asturias.
Should cinacalcet be used in patients who are not on dialysis? Jorge B Cannata-Andía and José Luis Fernández-Martín Affiliations: Bone and Mineral Research Unit. Hospital Universitario Central de Asturias.
A clinical assessment of the relationship between bone scintigraphy and serum biochemical markers in hemodialysis patients
 ORIGINAL ARTICLE Annals of Nuclear Medicine Vol. 18, No. 6, 513 518, 2004 A clinical assessment of the relationship between bone scintigraphy and serum biochemical markers in hemodialysis patients Seiji
ORIGINAL ARTICLE Annals of Nuclear Medicine Vol. 18, No. 6, 513 518, 2004 A clinical assessment of the relationship between bone scintigraphy and serum biochemical markers in hemodialysis patients Seiji
CKD Mineral and Bone Disorder Management in Kidney Transplant Recipients
 In Practice CKD Mineral and Bone Disorder Management in Kidney Transplant Recipients Hala M. Alshayeb, MD, 1 Michelle A. Josephson, MD, 1 and Stuart M. Sprague, DO 2 Kidney transplantation, the most effective
In Practice CKD Mineral and Bone Disorder Management in Kidney Transplant Recipients Hala M. Alshayeb, MD, 1 Michelle A. Josephson, MD, 1 and Stuart M. Sprague, DO 2 Kidney transplantation, the most effective
Case Report A Reference Finding Rarely Seen in Primary Hyperparathyroidism: Brown Tumor
 Case Reports in Medicine Volume 2012, Article ID 432676, 4 pages doi:10.1155/2012/432676 Case Report A Reference Finding Rarely Seen in Primary Hyperparathyroidism: Brown Tumor F. Mantar, 1 S. Gunduz,
Case Reports in Medicine Volume 2012, Article ID 432676, 4 pages doi:10.1155/2012/432676 Case Report A Reference Finding Rarely Seen in Primary Hyperparathyroidism: Brown Tumor F. Mantar, 1 S. Gunduz,
Nuove terapie in ambito Nefrologico: Etelcalcetide (AMG-416)
") Nuove terapie in ambito Nefrologico: Etelcalcetide (AMG-416) Antonio Bellasi, MD, PhD U.O.C. Nefrologia & Dialisi ASST-Lariana, Ospedale S. Anna, Como, Italy Improvement of mineral and bone metabolism
Nuove terapie in ambito Nefrologico: Etelcalcetide (AMG-416) Antonio Bellasi, MD, PhD U.O.C. Nefrologia & Dialisi ASST-Lariana, Ospedale S. Anna, Como, Italy Improvement of mineral and bone metabolism
The Skeletal Response to Aging: There s No Bones About It!
 The Skeletal Response to Aging: There s No Bones About It! April 7, 2001 Joseph E. Zerwekh, Ph.D. Interrelationship of Intestinal, Skeletal, and Renal Systems to the Overall Maintenance of Normal Calcium
The Skeletal Response to Aging: There s No Bones About It! April 7, 2001 Joseph E. Zerwekh, Ph.D. Interrelationship of Intestinal, Skeletal, and Renal Systems to the Overall Maintenance of Normal Calcium
Protocol GTC : A Randomized, Open Label, Parallel Design Study of Sevelamer Hydrochloride (Renagel ) in Chronic Kidney Disease Patients.
 in Chronic Kidney Disease Patients.") Protocol GTC-68-208: A Randomized, Open Label, Parallel Design Study of Sevelamer Hydrochloride (Renagel ) in Chronic Kidney Disease Patients. These results are supplied for informational purposes only.
Protocol GTC-68-208: A Randomized, Open Label, Parallel Design Study of Sevelamer Hydrochloride (Renagel ) in Chronic Kidney Disease Patients. These results are supplied for informational purposes only.
Long-term effect of cinacalcet hydrochloride on abdominal aortic calcification in patients on hemodialysis with secondary hyperparathyroidism
 Long-term effect of cinacalcet hydrochloride on abdominal aortic calcification in patients on hemodialysis with secondary hyperparathyroidism Kazunori Nakayama 1, 2, Kazushi Nakao 1, 2, Yuji Takatori 1,
Long-term effect of cinacalcet hydrochloride on abdominal aortic calcification in patients on hemodialysis with secondary hyperparathyroidism Kazunori Nakayama 1, 2, Kazushi Nakao 1, 2, Yuji Takatori 1,
Radiographic Appearance Of Primary Hyperparathyroidism With Atypical Parathyroid Adenoma
 ISPUB.COM The Internet Journal of Internal Medicine Volume 6 Number 2 Radiographic Appearance Of Primary Hyperparathyroidism With Atypical Parathyroid Adenoma P George, N Philip, B Pawar Citation P George,
ISPUB.COM The Internet Journal of Internal Medicine Volume 6 Number 2 Radiographic Appearance Of Primary Hyperparathyroidism With Atypical Parathyroid Adenoma P George, N Philip, B Pawar Citation P George,
Significance of minimodeling in dialysis patients with adynamic bone disease
 Kidney International, Vol. (5), pp. 33 39 DIALYSIS TRANSPLANTATION Significance of minimodeling in dialysis patients with adynamic bone disease YOSHIFUMI UBARA,TETSUO TAGAMI,SYOHEI NAKANISHI, NAOKI SAWA,
Kidney International, Vol. (5), pp. 33 39 DIALYSIS TRANSPLANTATION Significance of minimodeling in dialysis patients with adynamic bone disease YOSHIFUMI UBARA,TETSUO TAGAMI,SYOHEI NAKANISHI, NAOKI SAWA,
Osteoporosis and Chronic Kidney Disease: Diagnosis and Treatment Recommendations
 Osteoporosis and Chronic Kidney Disease: Diagnosis and Treatment Recommendations Nancy E. Lane, MD Director, Center for Musculoskeletal Health Endowed Professor of Medicine and Rheumatology University
Osteoporosis and Chronic Kidney Disease: Diagnosis and Treatment Recommendations Nancy E. Lane, MD Director, Center for Musculoskeletal Health Endowed Professor of Medicine and Rheumatology University
PART FOUR. Metabolism and Nutrition
 PART FOUR Metabolism and Nutrition Advances in Peritoneal Dialysis, Vol. 21, 2005 Maria Mesquita, 1 Eric Wittersheim, 2 Anne Demulder, 2 Max Dratwa, 1 Pierre Bergmann 3 Bone Cytokines and Renal Osteodystrophy
PART FOUR Metabolism and Nutrition Advances in Peritoneal Dialysis, Vol. 21, 2005 Maria Mesquita, 1 Eric Wittersheim, 2 Anne Demulder, 2 Max Dratwa, 1 Pierre Bergmann 3 Bone Cytokines and Renal Osteodystrophy
Management of CKD. Goce Spasovski, R. Macedonia
 Management of CKD complications Introduction Bone disease to Renagel Goce Spasovski, R. Macedonia Istanbul, June 4, 2011 Session Objectives - Mineral and Bone Disorders (MBD) Bone disease a part of CKD
Management of CKD complications Introduction Bone disease to Renagel Goce Spasovski, R. Macedonia Istanbul, June 4, 2011 Session Objectives - Mineral and Bone Disorders (MBD) Bone disease a part of CKD
KDOQI COMMENTARY VOL 55, NO 5, MAY 2010
 VOL 55, NO 5, MAY 2010 KDOQI COMMENTARY KDOQI US Commentary on the 2009 KDIGO Clinical Practice Guideline for the Diagnosis, Evaluation, and Treatment of CKD Mineral and Bone Disorder (CKD-MBD) Katrin
VOL 55, NO 5, MAY 2010 KDOQI COMMENTARY KDOQI US Commentary on the 2009 KDIGO Clinical Practice Guideline for the Diagnosis, Evaluation, and Treatment of CKD Mineral and Bone Disorder (CKD-MBD) Katrin
Race Is a Major Determinant of Secondary Hyperparathyroidism in Uremic Patients
 J Am Soc Nephrol 11: 330 334, 2000 Race Is a Major Determinant of Secondary Hyperparathyroidism in Uremic Patients AJAY GUPTA,* LEE R. KALLENBACH, GERARD ZASUWA,* and GEORGE W. DIVINE *Division of Nephrology
J Am Soc Nephrol 11: 330 334, 2000 Race Is a Major Determinant of Secondary Hyperparathyroidism in Uremic Patients AJAY GUPTA,* LEE R. KALLENBACH, GERARD ZASUWA,* and GEORGE W. DIVINE *Division of Nephrology
Clinical benefits of an adherence monitoring program in the management of secondary hyperparathyroidism with cinacalcet:
 Clinical benefits of an adherence monitoring program in the management of secondary hyperparathyroidism with cinacalcet: Results of a prospective randomized controlled study Forni Valentina¹, Pruijm Menno¹,
Clinical benefits of an adherence monitoring program in the management of secondary hyperparathyroidism with cinacalcet: Results of a prospective randomized controlled study Forni Valentina¹, Pruijm Menno¹,
Renal Association Clinical Practice Guideline in Mineral and Bone Disorders in CKD
 Nephron Clin Pract 2011;118(suppl 1):c145 c152 DOI: 10.1159/000328066 Received: May 24, 2010 Accepted: December 6, 2010 Published online: May 6, 2011 Renal Association Clinical Practice Guideline in Mineral
Nephron Clin Pract 2011;118(suppl 1):c145 c152 DOI: 10.1159/000328066 Received: May 24, 2010 Accepted: December 6, 2010 Published online: May 6, 2011 Renal Association Clinical Practice Guideline in Mineral
Advances in Peritoneal Dialysis, Vol. 22, 2006
 Advances in Peritoneal Dialysis, Vol. 22, 2006 M. Carmen Sánchez González, 1 Fernando López Barea, 2 M. Auxiliadora Bajo, 1 Rafael Selgas, 1 for the Collaborators of the Multicenter Study Group* Serum
Advances in Peritoneal Dialysis, Vol. 22, 2006 M. Carmen Sánchez González, 1 Fernando López Barea, 2 M. Auxiliadora Bajo, 1 Rafael Selgas, 1 for the Collaborators of the Multicenter Study Group* Serum
Risk factors and clinical course of hungry bone syndrome after total parathyroidectomy in dialysis patients with secondary hyperparathyroidism
 Ho et al. BMC Nephrology (2017) 18:12 DOI 10.1186/s12882-016-0421-5 RESEARCH ARTICLE Open Access Risk factors and clinical course of hungry bone syndrome after total parathyroidectomy in dialysis patients
Ho et al. BMC Nephrology (2017) 18:12 DOI 10.1186/s12882-016-0421-5 RESEARCH ARTICLE Open Access Risk factors and clinical course of hungry bone syndrome after total parathyroidectomy in dialysis patients
AACE Southern States Chapter Lecture. Basics
 AACE Southern States Chapter Lecture Unusual Bone Cases Basics Osteoporosis Osteomalacia Renal Osteodystrophy Multiple Myeloma 1 Osteoporosis Definition Modeling, Bone Remodeling Bone Resorption > Bone
AACE Southern States Chapter Lecture Unusual Bone Cases Basics Osteoporosis Osteomalacia Renal Osteodystrophy Multiple Myeloma 1 Osteoporosis Definition Modeling, Bone Remodeling Bone Resorption > Bone
GUIDELINE 1. EVALUATION OF CALCIUM AND PHOSPHORUS METABOLISM
 GUIDELINE 1. EVALUATION OF CALCIUM AND PHOSPHORUS METABOLISM 1.1 Serum levels of calcium, phosphorus, alkaline phosphatase, total CO 2, and PTH measured by a first-generation immunometric parathyroid hormone
GUIDELINE 1. EVALUATION OF CALCIUM AND PHOSPHORUS METABOLISM 1.1 Serum levels of calcium, phosphorus, alkaline phosphatase, total CO 2, and PTH measured by a first-generation immunometric parathyroid hormone
Pediatric CKD-MBD: pathophysiology and management
 Pediatric CKD-MBD: pathophysiology and management Justine Bacchetta, MD, PhD Reference Center for Rare Renal Diseases Reference Center for Rare Diseases of Calcium and Phosphate Bron, France Overview of
Pediatric CKD-MBD: pathophysiology and management Justine Bacchetta, MD, PhD Reference Center for Rare Renal Diseases Reference Center for Rare Diseases of Calcium and Phosphate Bron, France Overview of
K/DOQI-recommended intact PTH levels do not prevent low-turnover bone disease in hemodialysis patients
 http://www.kidney-international.org & 2008 International Society of Nephrology original article see commentary on page 674 K/DOQI-recommended intact PTH levels do not prevent low-turnover bone disease
http://www.kidney-international.org & 2008 International Society of Nephrology original article see commentary on page 674 K/DOQI-recommended intact PTH levels do not prevent low-turnover bone disease
Yueming Sun Æ Huihua Cai Æ Jianfeng Bai Æ Hanlin Zhao Æ Yi Miao
 World J Surg (2009) 33:1674 1679 DOI 10.1007/s00268-009-0086-3 Endoscopic Total Parathyroidectomy and Partial Parathyroid Tissue Autotransplantation for Patients with Secondary Hyperparathyroidism: A New
World J Surg (2009) 33:1674 1679 DOI 10.1007/s00268-009-0086-3 Endoscopic Total Parathyroidectomy and Partial Parathyroid Tissue Autotransplantation for Patients with Secondary Hyperparathyroidism: A New
Effects of Anti RANK ligand Denosumab on Beta Thalassemia induced osteoporosis
 Effects of Anti RANK ligand Denosumab on Beta Thalassemia induced osteoporosis Mohamed Yassin 1 Ashraf T. Soliman2, Mohamed O. Abdelrahman3, Vincenzo De Sanctis 4 Departments of, 1 Hematology 2Pediatric
Effects of Anti RANK ligand Denosumab on Beta Thalassemia induced osteoporosis Mohamed Yassin 1 Ashraf T. Soliman2, Mohamed O. Abdelrahman3, Vincenzo De Sanctis 4 Departments of, 1 Hematology 2Pediatric
II. RELATION TO BONE DISEASE INTRODUCTION. M.M. POPOVTZER, W.E. HUFFER, W.P. GElS, W.S. HAMMOND, T.E. STARZL
 II. RELATION TO BONE DISEASE M.M. POPOVTZER, W.E. HUFFER, W.P. GElS, W.S. HAMMOND, T.E. STARZL INTRODUCTION It has been generally assumed that azotemic osteodystrophy resolves after kidney transplantation
II. RELATION TO BONE DISEASE M.M. POPOVTZER, W.E. HUFFER, W.P. GElS, W.S. HAMMOND, T.E. STARZL INTRODUCTION It has been generally assumed that azotemic osteodystrophy resolves after kidney transplantation
PREVALENCE AND PATTERNS OF HYPERPARATHYROIDISM AND MINERAL BONE DISEASE IN PATIENTS WITH CHRONIC KIDNEY DISEASE AT KENYATTA NATIONAL HOSPITAL
 PREVALENCE AND PATTERNS OF HYPERPARATHYROIDISM AND MINERAL BONE DISEASE IN PATIENTS WITH CHRONIC KIDNEY DISEASE AT KENYATTA NATIONAL HOSPITAL DR. ANNE MUGERA The Problem Chronic Kidney disease is a worldwide
PREVALENCE AND PATTERNS OF HYPERPARATHYROIDISM AND MINERAL BONE DISEASE IN PATIENTS WITH CHRONIC KIDNEY DISEASE AT KENYATTA NATIONAL HOSPITAL DR. ANNE MUGERA The Problem Chronic Kidney disease is a worldwide
PARSABIV (etelcalcetide)
") PARSABIV (etelcalcetide) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and
PARSABIV (etelcalcetide) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and
Clinician s Guide to Prevention and Treatment of Osteoporosis
 Clinician s Guide to Prevention and Treatment of Osteoporosis Published: 15 August 2014 committee of the National Osteoporosis Foundation (NOF) Tipawan khiemsontia,md outline Basic pathophysiology screening
Clinician s Guide to Prevention and Treatment of Osteoporosis Published: 15 August 2014 committee of the National Osteoporosis Foundation (NOF) Tipawan khiemsontia,md outline Basic pathophysiology screening
Diagnosis and Treatment of Osteoporosis. Department of Endocrinology and Metabolism Ajou University School of Medicine.
 Diagnosis and Treatment of Osteoporosis Department of Endocrinology and Metabolism Ajou University School of Medicine Yoon-Sok CHUNG WCIM, COEX, Seoul, 27Oct2014 Case 1 71-year old woman Back pain Emergency
Diagnosis and Treatment of Osteoporosis Department of Endocrinology and Metabolism Ajou University School of Medicine Yoon-Sok CHUNG WCIM, COEX, Seoul, 27Oct2014 Case 1 71-year old woman Back pain Emergency
Month/Year of Review: September 2012 Date of Last Review: September 2010
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Profile of mineral bone disease in Pre-dialytic stage 3-5 Chronic Kidney Disease Patients: A Cross-Sectional Study
 Profile of mineral bone disease in Pre-dialytic stage 3-5 Chronic Kidney Disease Patients: A Cross-Sectional Study Balaraman Velayudham 1, Praveen Balaguru 2, Nagendran Vijayakumar 3, Shankar.P 4 1,3,4-Dept.
Profile of mineral bone disease in Pre-dialytic stage 3-5 Chronic Kidney Disease Patients: A Cross-Sectional Study Balaraman Velayudham 1, Praveen Balaguru 2, Nagendran Vijayakumar 3, Shankar.P 4 1,3,4-Dept.
Total Parathyroidectomy with Forearm Autotransplantation as the Treatment of Choice for Secondary Hyperparathyroidism
 The Journal of International Medical Research 2011; 39: 978 987 Total Parathyroidectomy with Forearm Autotransplantation as the Treatment of Choice for Secondary Hyperparathyroidism J NARANDA 1,2, R EKART
The Journal of International Medical Research 2011; 39: 978 987 Total Parathyroidectomy with Forearm Autotransplantation as the Treatment of Choice for Secondary Hyperparathyroidism J NARANDA 1,2, R EKART
Parsabiv the control of calcimimetic delivery you ve always wanted, the sustained lowering of shpt lab values your patients deserve 1
 Parsabiv the control of calcimimetic delivery you ve always wanted, the sustained lowering of shpt lab values your patients deserve 1 Not an actual Parsabiv vial. The displayed vial is for illustrative
Parsabiv the control of calcimimetic delivery you ve always wanted, the sustained lowering of shpt lab values your patients deserve 1 Not an actual Parsabiv vial. The displayed vial is for illustrative
Case Report Combined Effect of a Locking Plate and Teriparatide for Incomplete Atypical Femoral Fracture: Two Case Reports of Curved Femurs
 Case Reports in Orthopedics Volume 2015, Article ID 213614, 5 pages http://dx.doi.org/10.1155/2015/213614 Case Report Combined Effect of a Locking Plate and Teriparatide for Incomplete Atypical Femoral
Case Reports in Orthopedics Volume 2015, Article ID 213614, 5 pages http://dx.doi.org/10.1155/2015/213614 Case Report Combined Effect of a Locking Plate and Teriparatide for Incomplete Atypical Femoral
Swiss Summary of the Risk Management Plan (RMP) for Parsabiv (Etelcalcetide)
 for Parsabiv (Etelcalcetide)") Swiss Summary of the Risk Management Plan (RMP) for Parsabiv (Etelcalcetide) RMP Summary: Version 1, November 2017 EU RMP: Version 1.0, November 2016 Page 1 of 6 The Risk Management Plan (RMP) is a comprehensive
Swiss Summary of the Risk Management Plan (RMP) for Parsabiv (Etelcalcetide) RMP Summary: Version 1, November 2017 EU RMP: Version 1.0, November 2016 Page 1 of 6 The Risk Management Plan (RMP) is a comprehensive
An overview on adynamic bone disease clinical and therapeutical approaches
 2014/2015 Mariana Barata Santos Barreira de Jesus An overview on adynamic bone disease clinical and therapeutical approaches março, 2015 Mariana Barata Santos Barreira de Jesus An overview on adynamic
2014/2015 Mariana Barata Santos Barreira de Jesus An overview on adynamic bone disease clinical and therapeutical approaches março, 2015 Mariana Barata Santos Barreira de Jesus An overview on adynamic
RENAL OSTEODYSTROPHY continues to
 Variant of Adynamic Bone Disease in Hemodialysis Patients: Fact or Fiction? Lillian A. Rocha, MD, Andrea Higa, MD, Fellype C. Barreto, MD, Luciene M. dos Reis, PhD, Vanda Jorgetti, MD, PhD, Sérgio A. Draibe,
Variant of Adynamic Bone Disease in Hemodialysis Patients: Fact or Fiction? Lillian A. Rocha, MD, Andrea Higa, MD, Fellype C. Barreto, MD, Luciene M. dos Reis, PhD, Vanda Jorgetti, MD, PhD, Sérgio A. Draibe,
Product: Cinacalcet HCl Observational Research Clinical Study Report: Date: 23 July 2012 Page Page 2 2 of of 1203
 Date: 23 July 2012 Page Page 2 2 of of 1203 SYNOPSIS Name of Sponsor: mgen Development Europe Product or Therapeutic rea: Cinacalcet HCl Indication: The reduction of hypercalcaemia in patients with primary
Date: 23 July 2012 Page Page 2 2 of of 1203 SYNOPSIS Name of Sponsor: mgen Development Europe Product or Therapeutic rea: Cinacalcet HCl Indication: The reduction of hypercalcaemia in patients with primary
NDT Advance Access published February 3, 2007
 NDT Advance Access published February 3, 2007 Nephrol Dial Transplant (2007) 1 of 6 doi:10.1093/ndt/gfl840 Original Article Implementation of K/DOQI Clinical Practice Guidelines for Bone Metabolism and
NDT Advance Access published February 3, 2007 Nephrol Dial Transplant (2007) 1 of 6 doi:10.1093/ndt/gfl840 Original Article Implementation of K/DOQI Clinical Practice Guidelines for Bone Metabolism and
2.0 Synopsis. Paricalcitol Capsules M Clinical Study Report R&D/15/0380. (For National Authority Use Only)
") 2.0 Synopsis AbbVie Inc. Name of Study Drug: ABT-358/Zemplar (paricalcitol) Capsules Name of Active Ingredient: paricalcitol Individual Study Table Referring to Part of Dossier: Volume: Page: (For National
2.0 Synopsis AbbVie Inc. Name of Study Drug: ABT-358/Zemplar (paricalcitol) Capsules Name of Active Ingredient: paricalcitol Individual Study Table Referring to Part of Dossier: Volume: Page: (For National
Pathophysiology of parathyroid hyperplasia in chronic kidney disease: preclinical and clinical basis for parathyroid intervention
 NDT Plus (2008) 1 [Suppl 3]: iii2 iii8 doi: 10.1093/ndtplus/sfn079 Pathophysiology of parathyroid hyperplasia in chronic kidney disease: preclinical and clinical basis for parathyroid intervention Shunsuke
NDT Plus (2008) 1 [Suppl 3]: iii2 iii8 doi: 10.1093/ndtplus/sfn079 Pathophysiology of parathyroid hyperplasia in chronic kidney disease: preclinical and clinical basis for parathyroid intervention Shunsuke