A case of bilateral adrenal haemorrhage following traumatic brain injury
|
|
|
- Robyn Walker
- 6 years ago
- Views:
Transcription
1 Journal of Intensive Care This Provisional PDF corresponds to the article as it appeared upon acceptance. Fully formatted PDF and full text (HTML) versions will be made available soon. A case of bilateral adrenal haemorrhage following traumatic brain injury Journal of Intensive Care Sample 5102() 3:4 doi: /s Mervyn Leong (leong.mervyn@gmail.com) Madhav Pendyala (madhav.pendyala@gmail.com) Joga Chaganti (joga.chaganti@svha.org.au) Suhel Al-Soufi (Suhel.Al-Soufi@svha.org.au) Sample ISSN Article type Case report Submission date 30 October 2014 Acceptance date 15 January 2015 Article URL Like all articles in BMC journals, this peer-reviewed article can be downloaded, printed and distributed freely for any purposes (see copyright notice below). Articles in BMC journals are listed in PubMed and archived at PubMed Central. For information about publishing your research in BMC journals or any BioMed Central journal, go to Leong et al.; licensee BioMed Central. This is an Open Access article distributed under the terms of the Creative Commons Attribution License ( which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited. The Creative Commons Public Domain Dedication waiver ( applies to the data made available in this article, unless otherwise stated.
2 A case of bilateral adrenal haemorrhage following traumatic brain injury Mervyn Leong 1* * Corresponding author leong.mervyn@gmail.com Madhav Pendyala 1 madhav.pendyala@gmail.com Joga Chaganti 2 joga.chaganti@svha.org.au Suhel Al-Soufi 1 Suhel.Al-Soufi@svha.org.au 1 Intensive Care Unit, St Vincent s Hospital, Sydney, Australia 2 Department of Radiology, St Vincent s Hospital, Sydney, Australia Abstract We report the case of a 57-year-old man who sustained an isolated severe traumatic brain injury (TBI). During his admission to the intensive care unit (ICU), he developed marked arterial hypotension of unclear cause. Eventually, the presence of renal angle tenderness on clinical examination and a low random-cortisol level lead to the suspicion of primary adrenal insufficiency. A computed tomography scan of his abdomen demonstrated new bilateral adrenal haemorrhages. This diagnosis is not unlikely to be missed, as symptoms and laboratory tests are often nonspecific. Keywords Traumatic brain injury, Adrenal haemorrhage, Adrenal insufficiency Background Bilateral adrenal haemorrhages in the context of traumatic brain injury (TBI) are difficult to diagnose clinically despite appropriate symptoms and laboratory parameters as these are often nonspecific. Serum cortisol levels or the short synacthen test may not be specific for the diagnosis of primary adrenal insufficiency in critical ill patients, and there is a lack of data regarding normal cortisol levels in critical illness [1-4] Diagnosis can be made with computed tomography scan of the abdomen. We report a case of bilateral adrenal haemorrhages in an isolated TBI.
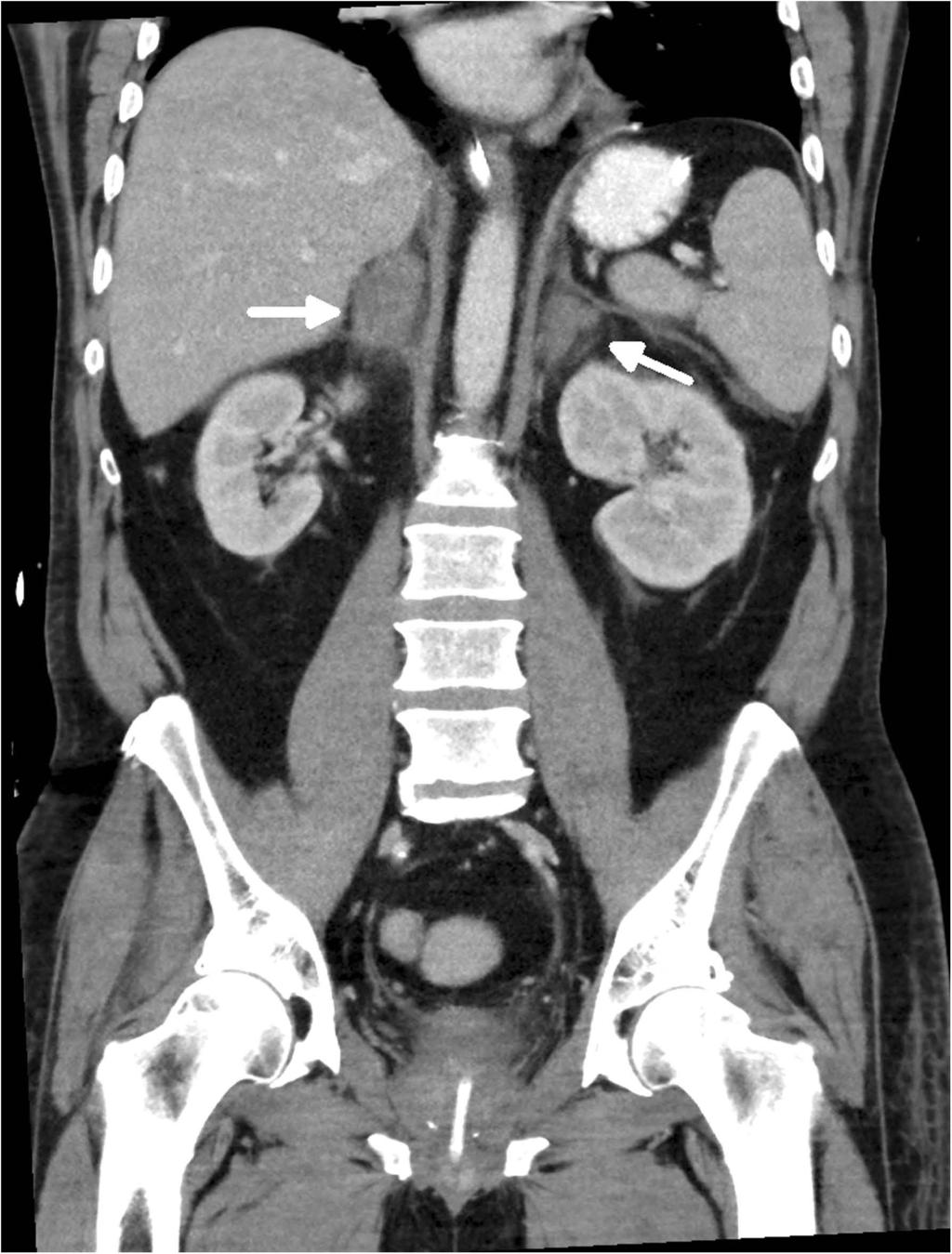
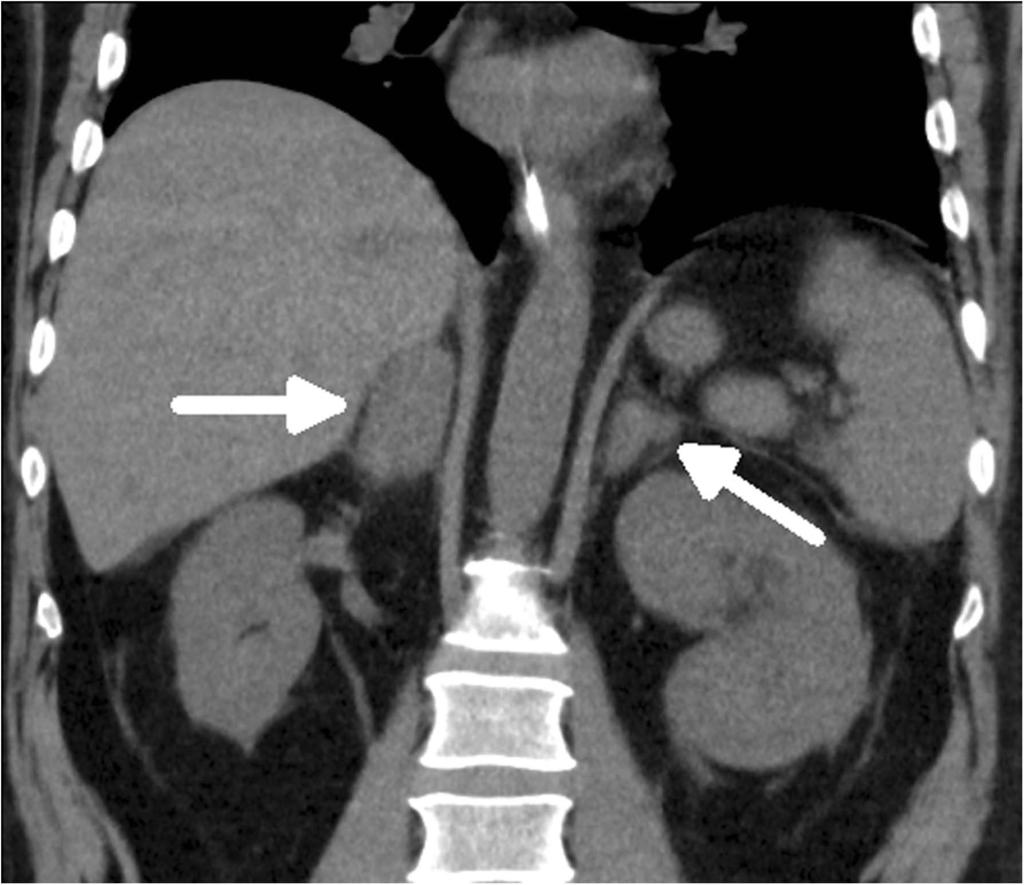
3 Case presentation A 57-year-old man sustained an isolated severe traumatic brain injury as a result of being struck as a pedestrian by a cyclist. On admission to the emergency department, he had a Glasgow Coma Scale of eight, equal pupil size and reaction to light. He was hypertensive with a systemic blood pressure of 250/110 mmhg and in a sinus rhythm with 80 beats per minute. The patient was intubated for airway protection as he was vomiting profusely. A computed tomography scan of the brain showed an acute right frontal subdural hematoma resulting in 1.1 cm of midline shift. In addition, there were bilateral fronto-temporal haemorrhagic contusions, diffuse subarachnoid blood along with right-sided parafalcine and uncal herniation. Whole-body computed tomography did not show any evidence of spinal, thoracic, abdominal or pelvic injury. The patient was taken to theatres for right frontal decompressive craniectomy and evacuation of his subdural hematoma. An intra-parenchymal Codman catheter was inserted to monitor intra-cranial pressure. Following his admission to our intensive care unit, the patient developed intracranial hypertension, which was controlled with deep sedation, continuous paralysis, targeted temperature management and infusion of hypertonic saline. He required in the first 4 days of his intensive care unit (ICU) admission infusion of noradrenaline in a dose of up to 0.25 mcg/kg/min and concomitant infusion of vasopressin at a dose of up to 0.01 U/min to maintain an adequate cerebral perfusion pressure. The random-cortisol level at this stage was judged to be adequate with 452 and 700 nmol/l at two subsequent days. On day 6 of his ICU admission, following the cessation of vasopressors, he developed autonomic dysfunction with severe hypertension, which required temporary treatment with multiple enteral and intravenous anti-hypertensive medications. In the second week of his admission to the ICU, the patient became again progressively hypotensive despite cessation of his anti-hypertensive medication. In the presence of lowgrade fever, sepsis was suspected and antibiotics were empirically started. The patient had ongoing vasopressor requirements without response to intravascular volume replacement or a demonstrable cardiac cause. Cultures of sputum, blood and urine samples yielded no subsequent growth, and the white cell count remained normal. Eventually, primary adrenal insufficiency was suspected when renal angle tenderness was noted on clinical examination and a blood sample tested for random-cortisol showed a low level (116 nmol/l). A computed tomography scan of his abdomen demonstrated newly enlarged adrenal glands with heterogeneous attenuation and surrounding stranding which was highly suggestive of bilateral adrenal haemorrhages (Figure 1). The remainder of abdominal viscera appeared normal. The initial computed tomography scan was performed with contrast enhancement. However, a follow-up scan without contrast confirmed the diagnosis of bilateral adrenal haemorrhages (Figure 2).
4 Figure 1 Coronal contrast-enhanced scan. Demonstrating enlarged bilateral adrenal glands of heterogeneous attenuation (average U) (white arrow) with surrounding stranding. Figure 2 Coronal noncontrast progress scan 4 days later. Showing diffuse thickening of bilateral adrenal glands (white arrow) with ongoing stranding. Within 1 day of initiation of regular intravenous hydrocortisone 50 mg every 6 h, the hemodynamic status rapidly improved allowing the discontinuation of all vasopressors. Soon anti-hypertensive medication had to be recommenced. Following discharge of this patient to the ward, hydrocortisone was reduced to oral 40 mg mane and 10 mg midi. Fludrocortisone 0.1 mg was added to the treatment to prevent episodes of orthostatic hypotension. The patient was subsequently transferred to a rehabilitation centre where initially he had been progressing well with mobility and cognition. He represented eventually with postural hypotension, which lead to an increase of fludrocortisone to 0.15 mg. Discussion Bilateral adrenal haemorrhages have been described in association with a host of clinical conditions such as septic shock (Waterhouse-Fredrickson syndrome) [5], disseminated intravascular coagulation, heparin-induced thrombocytopenia and thrombosis syndrome, antiphospholipid antibody syndrome, metastatic cancer, amyloidosis and granulomatous disorders. To our knowledge, there have been no reported cases of adrenal haemorrhage in the context of isolated severe traumatic brain injury. We can only speculate on the nature of the association of traumatic brain injury and bilateral adrenal haemorrhage. After severe traumatic brain injuries, adrenal insufficiency can occur as a consequence of primary dysfunction of the hypothalamus or pituitary gland. However, the pathogenesis of adrenal haemorrhage is somewhat unclear. The anatomical blood supply of the adrenal glands is arranged in a way that the arterial blood supply is greater than the limited venous drainage capacity. Various factors can result in vascular engorgement and venous stasis within the adrenal glands. Stress-related ACTH secretion increases adrenal blood flow [6] while the catecholamine surge contributes to adrenal vein spasm. Platelet aggregation followed by venous thrombosis and disruption of the vascular endothelium further contribute to the development of intramedullary ischaemia and bleeding. We suspect that patients with severe traumatic brain injury who have high catecholamine levels and release tissue thromboplastin from damaged brain are at risk for bilateral adrenal haemorrhage to occur. In the reported case, there was no evidence of any blunt trauma apart from isolated traumatic brain injury. The patient did not have a past medical history of malignancy or haematological disorder. Repeated coagulation profiles did not demonstrate any haematological abnormalities such as disseminated intravascular coagulation. The patient was not prescribed heparin or any other anticoagulant in the first weeks of his admission as this was considered to be contraindicated. We believe therefore that the bilateral adrenal haemorrhages were a consequence of the isolated traumatic brain injury.
5 Bilateral adrenal haemorrhages in the context of traumatic brain injury are difficult to recognise clinically, and the diagnosis might be missed despite dramatic symptoms. Abdominal or flank tenderness on examination of a patient with isolated severe TBI and shock should raise the suspicion of adrenal failure. Further suggestive though unspecific features are fever, anorexia, nausea and confusion, and in particular, hypotension or shock as are laboratory clues such as leukocytosis, hyperkalemia and hyponatremia in the presence of an unaccountable fall in haemoglobin [7]. Symptoms of adrenal insufficiency can be similar to that of the systemic inflammatory response syndrome and sepsis which are frequently seen in severe traumatic brain injury [8]. Adrenal insufficiency can be confused with other endocrine disorders related to TBI such as syndrome of inappropriate antidiuretic hormone secretion and cerebral salt wasting [2-4]. We believe that the lower than expected cortisol level in this patient is consistent with adrenal insufficiency caused by bilateral adrenal haemorrhages. However, serum cortisol levels or the short synacthen test may not be specific for the diagnosis of primary adrenal insufficiency in critical ill patients. Fluctuations in serum cortisol levels are frequent and not necessarily indicative of actual damage to the adrenal gland [1-4]. There is also a lack of consensus regarding normal cortisol levels in critical illness. The diagnosis of adrenal haemorrhage can be made by a computed tomography scan of the abdomen demonstrating adrenal gland enlargement with high attenuation without contrast enhancement. Progress CT scans performed weeks after the acute phase may show progressive adrenal gland atrophy with variable degree of calcification. Ultrasonographic imaging of the abdomen may aid the diagnoses in the acute situation given that it is a bedside investigation that is easily accessible. Ultrasonographic examination usually reveals hyperechoic masses with central echogenic areas. Although magnetic resonance imaging may be helpful to exclude the presence of tumours and provide an estimate for the age of haemorrhage, there is very little evidence found in the literature. In some cases, there may be spontaneous recovery even years after the original injury but patients with bilateral adrenal infarctions often require lifelong adrenal replacement therapy [9]. Conclusions This case demonstrates that bilateral adrenal haemorrhage can be a rare consequence of severe TBI. The diagnosis is difficult, as symptoms and laboratory test are often unspecific, but abdominal or flank tenderness on examination of a patient with isolated severe TBI and shock should raise the suspicion of adrenal failure and prompt appropriate imaging. Consent Written and verbal consent was obtained from the patient and his next of kin for publication of this case report and use of accompanying images. A copy of the written consent is available for review by the Editor in Chief of this journal.
6 Competing interests The authors declare that they have no competing interests. Authors contributions MP and ML performed the literature review and compiled the case report and discussion. SA revised the manuscript critically for important intellectual content. JC reviewed and selected the relevant images and interpreted the radiological findings for this case. All authors read and approved the final manuscript. Acknowledgements We would like to acknowledge Dr. Barry Johnston for his contribution towards proofreading of the manuscript. References 1. Olivecrona Z, Dahlqvist P, Koskinen LO. Acute neuro-endocrine profile and prediction of outcome after severe brain injury. Scand J Trauma Resusc Emerg Med. 2013;21: Savaridas T, Andrews PJ, Harris B. Cortisol dynamics following acute severe brain injury. Intensive Care Med. 2004;30: Webster JB, Bell KR. Primary adrenal insufficiency following traumatic brain injury: a case report and review of the literature. Arch Phys Med Rehabil. 1997;78: Hwang JJ, Hwang DY. Treatment of endocrine disorders in the neuroscience intensive care unit. Curr Treat Options Neurol. 2014;16: Migeon CJ, Kenny FM, Hung W, Voorhess ML. Study of adrenal function in children with meningitis. Pediatrics. 1967;40: Streeten D. Adrenal hemorrhage. Endocrinologist. 1996;6: Rao RH, Vagnucci AH, Amico JA. Bilateral massive adrenal hemorrhage: early recognition and treatment. Ann Intern Med. 1989;110: Powner DJ, Boccalandro C. Adrenal insufficiency following traumatic brain injury in adults. Curr Opin Crit Care. 2008;14: Vella A, Nippoldt TB, Morris 3rd JC. Adrenal hemorrhage: a 25-year experience at the Mayo Clinic. Mayo Clin Proc. 2001;76:161 8.
7
8
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Iatrogenic Central Diabetes Insipidus Induced by Vasopressin Withdrawal
 Open Journal of Clinical & Medical Case Reports Volume 1 (2015) Issue 7 Abstract ISSN 2379-1039 Iatrogenic Central Diabetes Insipidus Induced by Vasopressin Withdrawal * Joseph R Shiber, MD ; Donald Johnson,
Open Journal of Clinical & Medical Case Reports Volume 1 (2015) Issue 7 Abstract ISSN 2379-1039 Iatrogenic Central Diabetes Insipidus Induced by Vasopressin Withdrawal * Joseph R Shiber, MD ; Donald Johnson,
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Heparin-Induced Thrombocytopenia causing Adrenal Insufficiency
 Heparin-Induced Thrombocytopenia causing Adrenal Insufficiency NATASHA MALKANI, MD LAHEY CLINIC INTERNAL MEDICINE, PGY-2 TUFTS UNIVERSITY SCHOOL OF MEDICINE Objective Describe mechanism of HIT Describe
Heparin-Induced Thrombocytopenia causing Adrenal Insufficiency NATASHA MALKANI, MD LAHEY CLINIC INTERNAL MEDICINE, PGY-2 TUFTS UNIVERSITY SCHOOL OF MEDICINE Objective Describe mechanism of HIT Describe
Update sulle lesioni emorragiche posttraumatiche
 Update sulle lesioni emorragiche posttraumatiche Corrado Iaccarino Neurochirurgia-Neurotraumatologia AOU Parma Neurochirurgia d'urgenza IRCCS ASMN Reggio Emilia LAW UPDATING This document provides recommendations
Update sulle lesioni emorragiche posttraumatiche Corrado Iaccarino Neurochirurgia-Neurotraumatologia AOU Parma Neurochirurgia d'urgenza IRCCS ASMN Reggio Emilia LAW UPDATING This document provides recommendations
Traumatic Brain Injury
 Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
Moron General Hospital Ciego de Avila Cuba. Department of Neurological Surgery
 Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
Case 1. Case 5/30/2013. Traumatic Brain Injury : Review, Update, and Controversies
 Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Management of Severe Traumatic Brain Injury
 Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic and Non Traumatic Adrenal Emergencies
 Traumatic and Non Traumatic Adrenal Emergencies Michael N. Patlas, MD, FRCPC (1), Christine O. Menias, MD (2), Douglas S. Katz, MD, FACR (3), Ania Z. Kielar, MD, FRCPC (4), Alla M. Rozenblit, MD (5), Jorge
Traumatic and Non Traumatic Adrenal Emergencies Michael N. Patlas, MD, FRCPC (1), Christine O. Menias, MD (2), Douglas S. Katz, MD, FACR (3), Ania Z. Kielar, MD, FRCPC (4), Alla M. Rozenblit, MD (5), Jorge
Clinical Guideline. SPEG MCN Protocols Sub Group SPEG Steering Group
 Clinical Guideline SECONDARY CARE MANAGEMENT OF SUSPECTED ADRENAL CRISIS IN CHILDREN AND YOUNG PEOPLE Date of First Issue 24/01/2015 Approved 28/09/2017 Current Issue Date 16/06/2017 Review Date 01/09/2019
Clinical Guideline SECONDARY CARE MANAGEMENT OF SUSPECTED ADRENAL CRISIS IN CHILDREN AND YOUNG PEOPLE Date of First Issue 24/01/2015 Approved 28/09/2017 Current Issue Date 16/06/2017 Review Date 01/09/2019
LOSS OF CONSCIOUSNESS & ASSESSMENT. Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT
 LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University
 Dr Mubarak Abdelrahman Assistant Professor Jazan University") Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Unrestricted. Dr ppooransari fellowship of perenatalogy
 Unrestricted Dr ppooransari fellowship of perenatalogy Assessment of severity of hemorrhage Significant drops in blood pressure are generally not manifested until substantial bleeding has occurred, and
Unrestricted Dr ppooransari fellowship of perenatalogy Assessment of severity of hemorrhage Significant drops in blood pressure are generally not manifested until substantial bleeding has occurred, and
Critical illness and endocrinology. ICU Fellowship Training Radboudumc
 Critical illness and endocrinology ICU Fellowship Training Radboudumc Critical illness Ultimate form of severe physical stress Generates an orchestrated endocrine response to provide the energy for fight
Critical illness and endocrinology ICU Fellowship Training Radboudumc Critical illness Ultimate form of severe physical stress Generates an orchestrated endocrine response to provide the energy for fight
INTENSIVE CARE MEDICINE CPD EVENING. Dr Alastair Morgan Wednesday 13 th September 2017
 INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
Pituitary Apoplexy. Updated: April 22, 2018 CLINICAL RECOGNITION
 Pituitary Apoplexy Zeina C Hannoush, MD. Assistant Professor of Clinical Medicine. Division of Endocrinology, Diabetes and Metabolism. University of Miami, Miller School of Medicine. Roy E Weiss, MD, PhD,
Pituitary Apoplexy Zeina C Hannoush, MD. Assistant Professor of Clinical Medicine. Division of Endocrinology, Diabetes and Metabolism. University of Miami, Miller School of Medicine. Roy E Weiss, MD, PhD,
Online Supplementary Data. Country Number of centers Number of patients randomized
 A Randomized, Double-Blind, -Controlled, Phase-2B Study to Evaluate the Safety and Efficacy of Recombinant Human Soluble Thrombomodulin, ART-123, in Patients with Sepsis and Suspected Disseminated Intravascular
A Randomized, Double-Blind, -Controlled, Phase-2B Study to Evaluate the Safety and Efficacy of Recombinant Human Soluble Thrombomodulin, ART-123, in Patients with Sepsis and Suspected Disseminated Intravascular
Contents. Contributors. Reviewers. Acknowledgements I CARDIOVASCULAR COMPLICATIONS
 Contributors Reviewers Acknowledgements Preface xii xvi xvii xviii I CARDIOVASCULAR COMPLICATIONS 1 Cardiac Complications of Cancer and Anticancer Treatment 3 Introduction 3 Malignant Pericardial Effusion
Contributors Reviewers Acknowledgements Preface xii xvi xvii xviii I CARDIOVASCULAR COMPLICATIONS 1 Cardiac Complications of Cancer and Anticancer Treatment 3 Introduction 3 Malignant Pericardial Effusion
Pre-hospital Response to Trauma and Brain Injury. Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center
 Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Lumbar puncture. Invasive procedure: diagnostic or therapeutic. The subarachnoid space 4-13 ys: ml Replenished: 4-6 h Routine LP (3-5 ml): <1h
: <1h") Lumbar puncture Lumbar puncture Invasive procedure: diagnostic or therapeutic. The subarachnoid space 4-13 ys: 65-150ml Replenished: 4-6 h Routine LP (3-5 ml):
Lumbar puncture Lumbar puncture Invasive procedure: diagnostic or therapeutic. The subarachnoid space 4-13 ys: 65-150ml Replenished: 4-6 h Routine LP (3-5 ml):
ICU treatment of the trauma patient. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 ICU treatment of the trauma patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Christian Kleber Surgical Intensive Care Unit - The trauma surgery Perspective Langenbecks
ICU treatment of the trauma patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Christian Kleber Surgical Intensive Care Unit - The trauma surgery Perspective Langenbecks
2. Blunt abdominal Trauma
 Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
Classical CNS Disease Patterns
 Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
NOTTINGHAM UNIVERSITY HOSPITAL NHS TRUST: Clinical Chemistry Guidelines
 Adrenocortical Insufficiency Guideline Document Information Policy Reference: Adrenocortical Insufficiency Issue: 1: Version 3 Author Job Title: Peter Prinsloo Consultant in Chemical Pathology STATUS:
Adrenocortical Insufficiency Guideline Document Information Policy Reference: Adrenocortical Insufficiency Issue: 1: Version 3 Author Job Title: Peter Prinsloo Consultant in Chemical Pathology STATUS:
Chapter 5: Sepsis Stephen Lo
 Chapter 5: Sepsis Stephen Lo Introduction Sepsis and its consequence are the bread and butter of intensive care medicine and management of it is time critical. This chapter will discuss the definitions,
Chapter 5: Sepsis Stephen Lo Introduction Sepsis and its consequence are the bread and butter of intensive care medicine and management of it is time critical. This chapter will discuss the definitions,
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdominal radiotherapy, toxic effects of, 636 637 Acute promyelocytic leukemia, associated with acquired bleeding problems, 614 615 Acute renal
Note: Page numbers of article titles are in boldface type. A Abdominal radiotherapy, toxic effects of, 636 637 Acute promyelocytic leukemia, associated with acquired bleeding problems, 614 615 Acute renal
CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE
 CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE 1 ABBREVIATIONS ACCP = American College of Chest Physicians ARF =
CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE 1 ABBREVIATIONS ACCP = American College of Chest Physicians ARF =
Case Report Internal Jugular Vein Thrombosis in Isolated Tuberculous Cervical Lymphadenopathy
 Volume 2016, Article ID 5184196, 4 pages http://dx.doi.org/10.1155/2016/5184196 Case Report Internal Jugular Vein Thrombosis in Isolated Tuberculous Cervical Lymphadenopathy Sanjay Khaladkar, Avadhesh
Volume 2016, Article ID 5184196, 4 pages http://dx.doi.org/10.1155/2016/5184196 Case Report Internal Jugular Vein Thrombosis in Isolated Tuberculous Cervical Lymphadenopathy Sanjay Khaladkar, Avadhesh
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage. Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA
 Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth. Objectives 11/7/2017
 Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
London Strategic Clinical Networks. My AKI. Guidance for patients with, or recovering from, acute kidney injury
 London Strategic Clinical Networks My AKI Guidance for patients with, or recovering from, acute kidney injury Supporting the delivery of equitable, high quality AKI care through collaboration www.londonaki.net
London Strategic Clinical Networks My AKI Guidance for patients with, or recovering from, acute kidney injury Supporting the delivery of equitable, high quality AKI care through collaboration www.londonaki.net
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 3/12/2011 Radiology Quiz of the Week # 11 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 3/12/2011 Radiology Quiz of the Week # 11 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Subdural hemorrhages in acute lymphoblastic leukemia: case report and literature review
 Yin et al. Chinese Neurosurgical Journal (2016) 2:25 DOI 10.1186/s41016-016-0045-4 CHINESE NEUROSURGICAL SOCIETY CASE REPORT CHINESE MEDICAL ASSOCIATION Subdural hemorrhages in acute lymphoblastic leukemia:
Yin et al. Chinese Neurosurgical Journal (2016) 2:25 DOI 10.1186/s41016-016-0045-4 CHINESE NEUROSURGICAL SOCIETY CASE REPORT CHINESE MEDICAL ASSOCIATION Subdural hemorrhages in acute lymphoblastic leukemia:
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
The central nervous system
 Sectc.qxd 29/06/99 09:42 Page 81 Section C The central nervous system CNS haemorrhage Subarachnoid haemorrhage Cerebral infarction Brain atrophy Ring enhancing lesions MRI of the pituitary Multiple sclerosis
Sectc.qxd 29/06/99 09:42 Page 81 Section C The central nervous system CNS haemorrhage Subarachnoid haemorrhage Cerebral infarction Brain atrophy Ring enhancing lesions MRI of the pituitary Multiple sclerosis
Canadian Trauma Trials Collaborative. Occult Pneumothorax in Critical Care (OPTICC): Standardized Data Collection Sheet
: Standardized Data Collection Sheet") Canadian Trauma Trials Collaborative STUDY CENTRE: Institution: City / Province: / Occult Pneumothorax in Critical Care (OPTICC): Standardized Sheet PATIENT DEMOGRAPHICS: First Name: Health record number
Canadian Trauma Trials Collaborative STUDY CENTRE: Institution: City / Province: / Occult Pneumothorax in Critical Care (OPTICC): Standardized Sheet PATIENT DEMOGRAPHICS: First Name: Health record number
ADDISON S DISEASE THE FACTS YOU NEED TO KNOW
 ADDISON S DISEASE THE FACTS YOU NEED TO KNOW WHAT IS Addison's disease is a severe or total deficiency of the hormones made in the adrenal cortex, caused by its destruction. There are normally two adrenal
ADDISON S DISEASE THE FACTS YOU NEED TO KNOW WHAT IS Addison's disease is a severe or total deficiency of the hormones made in the adrenal cortex, caused by its destruction. There are normally two adrenal
Neuroprotective Effects for TBI. Craig Williamson, MD
 Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
P-RMS: LT/H/PSUR/0004/001
 Core Safety Profile Active substance: Dalteparine Pharmaceutical form(s)/strength: Solution for injection, 2500 I.U./0.2ml, 2500 I.U./ml, 5000 I.U./0.2ml, 7500 I.U./0.3ml, 7500 I.U./0.75ml, 10000 I.U./0.4ml,
Core Safety Profile Active substance: Dalteparine Pharmaceutical form(s)/strength: Solution for injection, 2500 I.U./0.2ml, 2500 I.U./ml, 5000 I.U./0.2ml, 7500 I.U./0.3ml, 7500 I.U./0.75ml, 10000 I.U./0.4ml,
Traumatic brain Injury- An open eye approach
 Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS. ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS
 FOR THROMBOLYSIS") NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
Medical Review Guidelines Magnetic Resonance Angiography
 Medical Review Guidelines Magnetic Resonance Angiography Medical Guideline Number: MRG2001-05 Effective Date: 2/13/01 Revised Date: 2/14/2006 OHCA Reference OAC 317:30-5-24. Radiology. (f) Magnetic Resonance
Medical Review Guidelines Magnetic Resonance Angiography Medical Guideline Number: MRG2001-05 Effective Date: 2/13/01 Revised Date: 2/14/2006 OHCA Reference OAC 317:30-5-24. Radiology. (f) Magnetic Resonance
Traumatic Brain Injury Pathways for Adult ED Patients Being Admitted to Trauma Service
 tic Brain Injury Pathways for Adult ED Patients Being Admitted to Service Revision Team Tyler W. Barrett, MD, MSCI Elizabeth S. Compton, NP Bradley M. Dennis, MD Oscar D. Guillamondegui, MD, MPH Michael
tic Brain Injury Pathways for Adult ED Patients Being Admitted to Service Revision Team Tyler W. Barrett, MD, MSCI Elizabeth S. Compton, NP Bradley M. Dennis, MD Oscar D. Guillamondegui, MD, MPH Michael
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal compartment syndrome, as complication of fluid resuscitation, 331 338 abdominal perfusion pressure, 332 fluid restriction practice
Index Note: Page numbers of article titles are in boldface type. A Abdominal compartment syndrome, as complication of fluid resuscitation, 331 338 abdominal perfusion pressure, 332 fluid restriction practice
SPECIAL PATHOPHYSIOLOGY SHOCK
 SPECIAL PATHOPHYSIOLOGY SHOCK 1. How do we call blood pressure values below the reference range? 1.Hypovolemia. 2. Hypothermia. 3. Hypooncia. 4. Hypoosmia. 5. Hypotension. 2. What is acute circulatory
SPECIAL PATHOPHYSIOLOGY SHOCK 1. How do we call blood pressure values below the reference range? 1.Hypovolemia. 2. Hypothermia. 3. Hypooncia. 4. Hypoosmia. 5. Hypotension. 2. What is acute circulatory
Medicines Protocol HYPERTONIC SALINE 5%
 Medicines Protocol HYPERTONIC SALINE 5% HYPERTONIC SALINE 5% v1.0 1/4 Protocol Details Version 1.0 Legal category POM Staff grades Registered Paramedic Registered Nurse Specialist Paramedic (Critical Care)
Medicines Protocol HYPERTONIC SALINE 5% HYPERTONIC SALINE 5% v1.0 1/4 Protocol Details Version 1.0 Legal category POM Staff grades Registered Paramedic Registered Nurse Specialist Paramedic (Critical Care)
Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone
 Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Supplementary Online Content
 Supplementary Online Content Cooper DJ, Nichol A, Bailey M, et al. Effect of early sustained prophylactic hypothermia on neurologic outcomes among patients with severe traumatic brain injury: the POLAR
Supplementary Online Content Cooper DJ, Nichol A, Bailey M, et al. Effect of early sustained prophylactic hypothermia on neurologic outcomes among patients with severe traumatic brain injury: the POLAR
Conflict of Interest Disclosure J. Claude Hemphill III, MD,MAS. Difficult Diagnosis and Treatment: New Onset Obtundation
 Difficult Diagnosis and Treatment: New Onset Obtundation J. Claude Hemphill III, MD, MAS Kenneth Rainin Chair in Neurocritical Care Professor of Neurology and Neurological Surgery University of California,
Difficult Diagnosis and Treatment: New Onset Obtundation J. Claude Hemphill III, MD, MAS Kenneth Rainin Chair in Neurocritical Care Professor of Neurology and Neurological Surgery University of California,
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Severe traumatic brain injury. Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre
 Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
Traumatic Brain Injury TBI Presented by Bill Masten
 1 2 Cerebrum two hemispheres and four lobes. Cerebellum (little brain) coordinates the back and forth ballet of motion. It judges the timing of every movement precisely. Brainstem coordinates the bodies
1 2 Cerebrum two hemispheres and four lobes. Cerebellum (little brain) coordinates the back and forth ballet of motion. It judges the timing of every movement precisely. Brainstem coordinates the bodies
Venous Thromboembolism Prophylaxis
 Approved by: Venous Thromboembolism Prophylaxis Vice President and Chief Medical Officer; and Vice President and Chief Operating Officer Corporate Policy & Procedures Manual Number: Date Approved January
Approved by: Venous Thromboembolism Prophylaxis Vice President and Chief Medical Officer; and Vice President and Chief Operating Officer Corporate Policy & Procedures Manual Number: Date Approved January
Sepsis Management: Past, Present, and Future
 Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
CEDR 2018 QCDR Measures for CMS 2018 MIPS Performance Year Reporting
 ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had
ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had
Adrenal incidentaloma guideline for Northern Endocrine Network
 Adrenal incidentaloma guideline for Northern Endocrine Network Definition of adrenal incidentaloma Adrenal mass detected on an imaging study done for indications that are not related to an adrenal problem
Adrenal incidentaloma guideline for Northern Endocrine Network Definition of adrenal incidentaloma Adrenal mass detected on an imaging study done for indications that are not related to an adrenal problem
EAST MULTICENTER STUDY DATA DICTIONARY
 EAST MULTICENTER STUDY DATA DICTIONARY Does the Addition of Daily Aspirin to Standard Deep Venous Thrombosis Prophylaxis Reduce the Rate of Venous Thromboembolic Events? Data Entry Points and appropriate
EAST MULTICENTER STUDY DATA DICTIONARY Does the Addition of Daily Aspirin to Standard Deep Venous Thrombosis Prophylaxis Reduce the Rate of Venous Thromboembolic Events? Data Entry Points and appropriate
Acute cerebral MCA ischemia with secondary severe head injury and acute intracerebral and subdural haematoma. Case report
 214 Balasa et al - Acute cerebral MCA ischemia Acute cerebral MCA ischemia with secondary severe head injury and acute intracerebral and subdural haematoma. Case report D. Balasa 1, A. Tunas 1, I. Rusu
214 Balasa et al - Acute cerebral MCA ischemia Acute cerebral MCA ischemia with secondary severe head injury and acute intracerebral and subdural haematoma. Case report D. Balasa 1, A. Tunas 1, I. Rusu
Transfusion Requirements and Management in Trauma RACHEL JACK
 Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Michael Avant, M.D. The Children s Hospital of GHS
 Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
CT findings in patients with Cabazitaxel induced pelvic pain and haematuria: a case series
 Malalagama et al. Cancer Imaging (2017) 17:17 DOI 10.1186/s40644-017-0119-3 CASE SERIES CT findings in patients with Cabazitaxel induced pelvic pain and haematuria: a case series Geethal N. Malalagama
Malalagama et al. Cancer Imaging (2017) 17:17 DOI 10.1186/s40644-017-0119-3 CASE SERIES CT findings in patients with Cabazitaxel induced pelvic pain and haematuria: a case series Geethal N. Malalagama
Cerebro-vascular stroke
 Cerebro-vascular stroke CT Terminology Hypodense lesion = lesion of lower density than the normal brain tissue Hyperdense lesion = lesion of higher density than normal brain tissue Isodense lesion = lesion
Cerebro-vascular stroke CT Terminology Hypodense lesion = lesion of lower density than the normal brain tissue Hyperdense lesion = lesion of higher density than normal brain tissue Isodense lesion = lesion
Yes No Unknown. Major Infection Information
 Rehospitalization Intervention Check any that occurred during this hospitalization. Pacemaker without ICD ICD Atrial arrhythmia ablation Ventricular arrhythmia ablation Cardioversion CABG (coronary artery
Rehospitalization Intervention Check any that occurred during this hospitalization. Pacemaker without ICD ICD Atrial arrhythmia ablation Ventricular arrhythmia ablation Cardioversion CABG (coronary artery
Written Guidelines for Laboratory Testing in Intensive Care - Still Effective After 3 Years
 Written Guidelines for Laboratory Testing in Intensive Care - Still Effective After 3 Years S. M. MEHARI, J. H. HAVILL Intensive Care Unit, Waikato Hospital, Hamilton, NEW ZEALAND ABSTRACT Objective: The
Written Guidelines for Laboratory Testing in Intensive Care - Still Effective After 3 Years S. M. MEHARI, J. H. HAVILL Intensive Care Unit, Waikato Hospital, Hamilton, NEW ZEALAND ABSTRACT Objective: The
IV Fluids. I.V. Fluid Osmolarity Composition 0.9% NaCL (Normal Saline Solution, NSS) Uses/Clinical Considerations
 Uses/Clinical Considerations") IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
Iron-deficiency anemia as a rare cause of cerebral venous thrombosis and pulmonary embolism. NICASTRO, Nicolas, SCHNIDER, Armin, LEEMANN, Béatrice
 Article Iron-deficiency anemia as a rare cause of cerebral venous thrombosis and pulmonary embolism NICASTRO, Nicolas, SCHNIDER, Armin, LEEMANN, Béatrice Abstract Cerebral venous thrombosis (CVT) is a
Article Iron-deficiency anemia as a rare cause of cerebral venous thrombosis and pulmonary embolism NICASTRO, Nicolas, SCHNIDER, Armin, LEEMANN, Béatrice Abstract Cerebral venous thrombosis (CVT) is a
Objectives. Pathophysiology of Steroids. Question 1. Pathophysiology 3/1/2010. Steroids in Septic Shock: An Update
 Objectives : An Update Michael W. Perry PharmD, BCPS PGY2 Critical Care Resident Palmetto Health Richland Hospital Review the history of steroids in sepsis Summarize the current guidelines for steroids
Objectives : An Update Michael W. Perry PharmD, BCPS PGY2 Critical Care Resident Palmetto Health Richland Hospital Review the history of steroids in sepsis Summarize the current guidelines for steroids
V. CENTRAL NERVOUS SYSTEM TRAUMA
 V. CENTRAL NERVOUS SYSTEM TRAUMA I. Concussion - Is a clinical syndrome of altered consiousness secondary to head injury - Brought by a change in the momentum of the head when a moving head suddenly arrested
V. CENTRAL NERVOUS SYSTEM TRAUMA I. Concussion - Is a clinical syndrome of altered consiousness secondary to head injury - Brought by a change in the momentum of the head when a moving head suddenly arrested
Case Report Spontaneous Intramural Duodenal Hematoma: Pancreatitis, Obstructive Jaundice, and Upper Intestinal Obstruction
 Case Reports in Surgery Volume 2016, Article ID 5321081, 4 pages http://dx.doi.org/10.1155/2016/5321081 Case Report Spontaneous Intramural Duodenal Hematoma: Pancreatitis, Obstructive Jaundice, and Upper
Case Reports in Surgery Volume 2016, Article ID 5321081, 4 pages http://dx.doi.org/10.1155/2016/5321081 Case Report Spontaneous Intramural Duodenal Hematoma: Pancreatitis, Obstructive Jaundice, and Upper
Supplemental Digital Content: Definitions Based on the International Classification of Diseases, Ninth Revision, Clinical Modification
 Supplemental Digital Content: Definitions Based on the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) Diagnose and Procedures Codes 1. ICD-9-CM definition of
Supplemental Digital Content: Definitions Based on the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) Diagnose and Procedures Codes 1. ICD-9-CM definition of
Bilateral adrenal haemorrhage secondary to intra-abdominal sepsis: a case report
 Bilateral adrenal haemorrhage secondary to intra-abdominal sepsis: a case report Authors Egan, Aoife M;Larkin, John O;Ryan, Ronan S;Waldron, Ronan Citation Cases Journal. 2009 Jun 09;2(1):6894 Download
Bilateral adrenal haemorrhage secondary to intra-abdominal sepsis: a case report Authors Egan, Aoife M;Larkin, John O;Ryan, Ronan S;Waldron, Ronan Citation Cases Journal. 2009 Jun 09;2(1):6894 Download
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Brain Injuries. Presented By Dr. Said Said Elshama
 Brain Injuries Presented By Dr. Said Said Elshama Types of head injuries 1- Scalp injuries 2- Skull injuries 3- Intra Cranial injuries ( Brain ) Anatomical structure of meninges Intra- Cranial Injuries
Brain Injuries Presented By Dr. Said Said Elshama Types of head injuries 1- Scalp injuries 2- Skull injuries 3- Intra Cranial injuries ( Brain ) Anatomical structure of meninges Intra- Cranial Injuries
Introduction to Emergency Medical Care 1
 Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
No Financial Interest
 Pituitary Apoplexy Michael Vaphiades, D.O. Professor Department of Ophthalmology, Neurology, Neurosurgery University of Alabama at Birmingham, Birmingham, AL No Financial Interest N E U R O L O G I C
Pituitary Apoplexy Michael Vaphiades, D.O. Professor Department of Ophthalmology, Neurology, Neurosurgery University of Alabama at Birmingham, Birmingham, AL No Financial Interest N E U R O L O G I C
OCCULT PRESENTATIONS OF MESENTERIC INFARCT IN A KIDNEY TRANSPLANT RECIPIENT
 OCCULT PRESENTATIONS OF MESENTERIC INFARCT IN A KIDNEY TRANSPLANT RECIPIENT Yu-Tso Liao 1, Yen-Chun Hsu 2, Yu-Chang Yeh 2, Wing-Sum Chan 3 Abstract Mesenteric infarct is a critical disease; it would be
OCCULT PRESENTATIONS OF MESENTERIC INFARCT IN A KIDNEY TRANSPLANT RECIPIENT Yu-Tso Liao 1, Yen-Chun Hsu 2, Yu-Chang Yeh 2, Wing-Sum Chan 3 Abstract Mesenteric infarct is a critical disease; it would be
SHOCK AETIOLOGY OF SHOCK (1) Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function
 Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function") SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
A Guide to the Radiologic Evaluation of Extra-Axial Hemorrhage
 July 2013 A Guide to the Radiologic Evaluation of Extra-Axial Hemorrhage John Dickson, Harvard Medical School Year III Agenda 1. Define extra-axial hemorrhage and introduce its subtypes 2. Review coup
July 2013 A Guide to the Radiologic Evaluation of Extra-Axial Hemorrhage John Dickson, Harvard Medical School Year III Agenda 1. Define extra-axial hemorrhage and introduce its subtypes 2. Review coup
10. Severe traumatic brain injury also see flow chart Appendix 5
 10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
8th Annual NKY TBI Conference 3/28/2014
 Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
HEAD AND NECK IMAGING. James Chen (MS IV)
") HEAD AND NECK IMAGING James Chen (MS IV) Anatomy Course Johns Hopkins School of Medicine Sept. 27, 2011 OBJECTIVES Introduce cross sectional imaging of head and neck Computed tomography (CT) Review head
HEAD AND NECK IMAGING James Chen (MS IV) Anatomy Course Johns Hopkins School of Medicine Sept. 27, 2011 OBJECTIVES Introduce cross sectional imaging of head and neck Computed tomography (CT) Review head
Traumatic brain injuries are caused by external mechanical forces such as: - Falls - Transport-related accidents - Assault
 PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 6/23/2012 Radiology Quiz of the Week # 78 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 6/23/2012 Radiology Quiz of the Week # 78 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE
 2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism A pulmonary embolism (PE) is
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism A pulmonary embolism (PE) is
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
Cluster headache associated with acute maxillary sinusitis.
 Cluster headache associated with acute maxillary sinusitis. Edvardsson, Bengt Published in: SpringerPlus DOI: 10.1186/2193-1801-2-509 2013 Link to publication Citation for published version (APA): Edvardsson,
Cluster headache associated with acute maxillary sinusitis. Edvardsson, Bengt Published in: SpringerPlus DOI: 10.1186/2193-1801-2-509 2013 Link to publication Citation for published version (APA): Edvardsson,
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK. Alexandria Rydz
 EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
JUSTIFICATION PROTOCOLS FOR CT SCANNING ALBURY WODONGA HEALTH WODONGA CAMPUS
 JUSTIFICATION PROTOCOLS FOR CT SCANNING ALBURY WODONGA HEALTH WODONGA CAMPUS JUSTIFICATION PROTOCOLS FOR CT SCANNING INTRODUCTION: In accordance with the Victorian Radiation Act 2005 Wodonga Medical Imaging,
JUSTIFICATION PROTOCOLS FOR CT SCANNING ALBURY WODONGA HEALTH WODONGA CAMPUS JUSTIFICATION PROTOCOLS FOR CT SCANNING INTRODUCTION: In accordance with the Victorian Radiation Act 2005 Wodonga Medical Imaging,
The ABC s of Chest Trauma
 The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries