Director, Burn Center MetroHealth Medical Center Professor of Surgery Case Western Reserve University
|
|
|
- Anthony Simon
- 6 years ago
- Views:
Transcription
1 Director, Burn Center MetroHealth Medical Center Professor of Surgery Case Western Reserve University
2 BLAST INJURY Which of following statements concerning blast lung injury are FALSE? 1)Blast lung injury should be suspected in victims with dyspnea and chest pain 2)May result in air emboli 3)CXR demonstrates butterfly pattern of infiltrates 4) All suspected victims of blast lung injury require immediate intubation with high PEEP settings 5) IV fluid should be minimized
3 BLAST INJURY Dr. Charles Yowler does not have a significant financial relationship to report.
4 BLAST INJURY Common in war WW I shell shock WW II air bombing campaigns IEDs Terrorist Attacks Industrial explosions
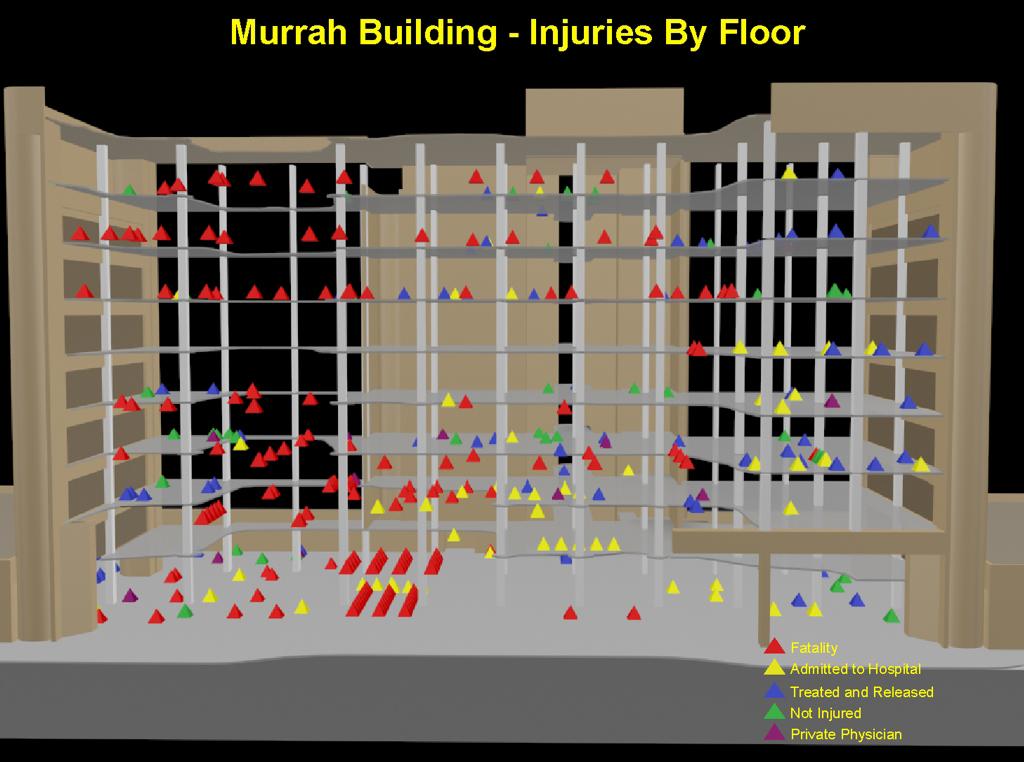
5 TERRORIST ATTACKS Boston Marathon (4/15/20013) 3 deaths, 264 wounded Oklahoma City (4/19/1995) 168 deaths, 680 wounded, damaged 324 buildings in a 16 block area London Subway (7/7/2005) 52 died, 700 injured in 4 separate bombing incidents
6 NDUSTRIAL EXPLOSIONS West Texas Fertilizer Plant (4/17/2013) 15 deaths, 60 injured Texas City (4/16/1947) Largest non-nuclear explosion in history 581 deaths, 133 missing, 5,000 injured with 1,784 hospitalized
7 PATHOPHYSIOLOGY
8 PATHOPHYSIOLOGY Spallation occurs when a pressure wave moves from a medium of higher density into a medium of lesser density Burst of water at the surface following an underwater explosion Implosion occurs when gases within tissues are compressed by the blast overpressure Shearing occurs at the interface of two tissues of differing density and thus different movement by the blast
9 PRIMARY BLAST INJURY (PBI) Tissue injury due to transfer of energy from the blast wave uncommon in survivors since victims close enough to the blast to suffer PBI are usually killed by secondary and tertiary blast injuries may occur in military actions due to armor protection from secondary blast injury
10 SECONDARY BLAST INJURY Shrapnel Most common injury in survivors Penetrating injuries to brain, spine, trunk and extremities Injuries may be more severe than normally seen at civilian trauma centers
11 TERTIARY BLAST INJURY Injury secondary to displacement of the patient s body by the blast wave Blunt injury to brain, spine, trunk and extremities
12 QUATENARY BLAST INJURY Crush Burn Inhalation Injury Radiological Psychological
13
14 BLAST LUNG INJURY Clinical Diagnosis Suspect in patients with hypoxia, dyspnea and chest pain May have hemoptysis, wheezing, hypotension
15 BLAST LUNG INJURY Alveolar injury to the blast wave May result in air emboli, hemothorax/pneumothorax, bronchopleural fistula CXR with butterfly pattern ABG, CT scan

16 BLAST LUNG INJURY

17 BLAST LUNG INJURY
18 BLAST LUNG INJURY Initial evaluation HFM for victims complaining of SOB, dyspnea, altered mental status or with documented hypoxia Do not intubate in field unless there is airway compromise or respiratory failure is imminent Hypotension may be secondary to tension pneumothorax Minimal IV fluids if not hypotensive Victims with no symptoms and normal CXR at 6 hours may be discharged However, delayed lung injury has been noted hours after the blast injury
19 BLAST LUNG INJURY Treatment HFM oxygen for hypoxia Chest tubes as indicated Intubation should only be utilized for airway compromise or impending respiratory failure Positive pressure ventilation increases the risk of death from air emboli ARDSnet guidelines with minimal use of PEEP
20 ABDOMINAL BLAST INJURY Intestinal blast injury Bowel wall hemorrhage, immediate and delayed bowel perforation Mesenteric injuries with ischemic segments and delayed bowel perforations Solid organs Lacerations Testicular rupture
21 ABDOMINAL BLAST INJURY Initial evaluation Physical signs may be minimal in absence of immediate perforation FAST CT scan with contrast poor sensitivity for intestinal injuries Serial abdominal exams and labs Immediate tachycardia is common. Beware, tachycardia that is progressive or does not respond to fluids and pain management.
22 EAR BLAST INJURY Most susceptible organ to blast pressure wave TM perforation Disruption of ossicular chain TM perforation is sensitive and should increase suspicion of other blast organ injuries. However, it is not very specific and the great majority of patients with TM injury will have no other blast injury
23 EAR BLAST INJURY All victims of blast exposure should undergo screening audiograms which may be performed as an outpatient Majority of TM perforations heal without operative intervention Patients with TM perforation require long term follow up for cholesteatoma
24 EXTREMITY INJURY Traumatic amputation from PBI is rare In a series of 3,000 victims of blast injury, the amputation rate was 1.2% Most extremity injuries are penetrating from second blast injury or blunt from tertiary/quaternary injury. Pre-hospital tourniquets may be life saving
25 CRUSH SYNDROME Tissue ischemia from compression prior to extrication and/or compartment syndrome following extrication Hypotension Acute kidney injury Hypocalcemia Hyperkalemia Metabolic acidosis Cardiac arrhythmia
26 CRUSH SYNDROME Pre-hospital IV fluids (1.5 liters/hour) Consider tourniquet Hospital Sodium bicarbonate 1 meq/kg push and consider drip IV fluids to maintain UO > 300 ml/hr Calcium gluconate as needed
27 EYE INJURY Ocular injury in 28% of survivors of terrorist attacks Usually due to secondary blast effect PBI may result in hyphema, retinal detachment
28 EYE INJURY Assume open globe injury in all patients presenting with ocular injuries Fine-cut CT scans of orbits to locate metallic foreign bodies MRI may be useful to locate nonmetallic foreign bodies
29 NEUROLOGIC INJURY Classically described following secondary, tertiary and quaternary blast isnjury TBI due to PBI has been recognized following recent conflicts WW I shell shock felt to be a psychological disorder may have been due to PBI
30 NEUROLOGIC INJURY Iraq and Afghanistan 40% of deaths due to IEDs PATHOPHYSIOLOGY PBI Blast injury to thorax can lead to propagation of high-pressure waves that are transmitted to the brain by the systemic circulation
31 NEUROLOGIC INJURY Body armor although protective against secondary blast injury has ben shown to increase the effects of PBI to the thorax in animal models Body armor with shock absorbing properties are in development
32 NEUROLOGIC INJURY PET scans of veterans with suspected TBI and PTSD revealed abnormalities in brain stems of patients with TBI from blast injury versus PTSD Many of those affected have no injuries that require immediate medical attention High index of suspicion in survivors of events involving blasts
33 BURN INJURY Bomb-related burns typically <20% TBSA Pre-hospital Stop the burning IV fluids (100 kg patient with 80% burn requires 2 liters of fluid in the first hour) Intubate for airway compromise or unconsciousness Minimal relationship between facial burns and airway compromise
34 INHALATION INJURY Inhalation injury typically treated with low TV and high PEEP This may lead to death in patients with PBI who may develop air emboli Chemical inhalation must also be considered in industrial explosions
35 PEDIATRIC CONCERNS Child more susceptible to PBI due to less truncal soft tissue to absorb blast wave and increased compliance of ribs Will maintain BP despite significant hemorrhage More susceptible to tertiary injury due to decreased mass
36 PEDIATRIC CONCERNS Consider tension pneumothorax in any hypotensive, hypoxic child Increased incidence of solid organ injury due to compliance of ribs Increased incidence of high cervical fractures SCIWORA
37 MASS CASUALTY Civilian blast injury involves a mass casualty event Triage at scene avoid overwhelming hospitals with early transfer of minimally injured Hospitals must have areas where minimally injured can be screened for delayed treatment
38 HARTFORD CONSENSUS Conference met in response to mass shooting events in US Traditional approach to criminal/terrorist mass casualty events was to keep all medical first responders from entering the area until law enforcement had cleared the area This led to delays of several hours for any victims to receive medical attention
39 HARTFORD CONSENSUS Law enforcement had no responsibility to treat the wounded or clear the scene they also had no training in this area In contrast, the military had recognized the importance of early buddy care and every soldier was trained in basic first aid including control of exsanguination with direct pressure or tourniquets
40 HARTFORD CONSENSUS THREAT Threat suppression Hemorrhage control Rapid extrication Assessment by medical providers Transport to definitive care
41 SUMMARY Majority of survivors with penetrating and blunt injuries with no PBI Significant PBI usually involves lung and abdomen Minimize airway pressures in patients with suspected blast lung injury Law enforcement organizations need training in control of hemorrhage and medical evacuation
42 SUMMARY Terrorists bombings can overwhelm urban trauma centers hospital response of transfer to trauma center is not feasible in most urban areas Industrial explosions typically occur in rural areas with limited medical facilities Military bases also typically in rural areas and military hospital is small
43 BLAST INJURY Which of following statements concerning blast lung injury are FALSE? 1)Blast lung injury should be suspected in victims with dyspnea and chest pain 2)May result in air emboli 3)CXR demonstrates butterfly pattern of infiltrates 4) All suspected victims of blast lung injury require immediate intubation with high PEEP settings 5) IV fluid should be minimized
Civilian Hospital Response to Mass Casualty Events The Israeli Experience
 Civilian Hospital Response to Mass Casualty Events The Israeli Experience William Schecter, MD Professor of Clinical Surgery University of California, San Francisco Chief of Surgery San Francisco General
Civilian Hospital Response to Mass Casualty Events The Israeli Experience William Schecter, MD Professor of Clinical Surgery University of California, San Francisco Chief of Surgery San Francisco General
Management of Blast Injuries
 Management of Blast Injuries Fawzi al-ayoubi, MD, FACS, PhD-Cand Chief, Division of Trauma & Acute Care Surgery, MH Acting Chair, Department of General Surgery and Trauma Surgery, MH Medical Chair, Service
Management of Blast Injuries Fawzi al-ayoubi, MD, FACS, PhD-Cand Chief, Division of Trauma & Acute Care Surgery, MH Acting Chair, Department of General Surgery and Trauma Surgery, MH Medical Chair, Service
Student Guide Module 4: Pediatric Trauma
 Student Guide Module 4: Pediatric Trauma Problem based learning exercise objectives Understand how to manage traumatic injuries in mass casualty events. Discuss the features and the approach to pediatric
Student Guide Module 4: Pediatric Trauma Problem based learning exercise objectives Understand how to manage traumatic injuries in mass casualty events. Discuss the features and the approach to pediatric
Explosive Injuries. Jeff Rabrich, DO, EMT-P EMS Medical Director St. Luke s - Roosevelt Hospital New York, NY. Saturday, September 24, 11
 Explosive Injuries Jeff Rabrich, DO, EMT-P EMS Medical Director St. Luke s - Roosevelt Hospital New York, NY Objectives Review recent bombing events in US Discuss Triage strategies and scene management
Explosive Injuries Jeff Rabrich, DO, EMT-P EMS Medical Director St. Luke s - Roosevelt Hospital New York, NY Objectives Review recent bombing events in US Discuss Triage strategies and scene management
CHEST INJURY PULMONARY CONTUSION
 CHEST INJURY PULMONARY CONTUSION Introduction Pulmonary contusion refers to blunt traumatic lung parenchymal injury which results in oedema and haemorrhaging into alveolar spaces. It may also result in
CHEST INJURY PULMONARY CONTUSION Introduction Pulmonary contusion refers to blunt traumatic lung parenchymal injury which results in oedema and haemorrhaging into alveolar spaces. It may also result in
MODULE IV. Pediatric Trauma
 MODULE IV Pediatric Trauma PRE-HOSPITAL HIGH RISK CRITERIA Blunt injury Significant injury; physiologic compromise Penetrating injuries Thorax, abdomen, head and neck High risk burns: > 10% second degree
MODULE IV Pediatric Trauma PRE-HOSPITAL HIGH RISK CRITERIA Blunt injury Significant injury; physiologic compromise Penetrating injuries Thorax, abdomen, head and neck High risk burns: > 10% second degree
EMS System for Metropolitan Oklahoma City and Tulsa 2018 Medical Control Board Treatment Protocols
 EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
Medical NREMT-PTE. NREMT Paramedic Trauma Exam.
 Medical NREMT-PTE NREMT Paramedic Trauma Exam https://killexams.com/pass4sure/exam-detail/nremt-pte Question: 41 Which of the following most accurately describes the finding of jugular venous distension
Medical NREMT-PTE NREMT Paramedic Trauma Exam https://killexams.com/pass4sure/exam-detail/nremt-pte Question: 41 Which of the following most accurately describes the finding of jugular venous distension
Training Surgeons for Disasters
 SURGICAL RESPONSE TO DISASTERS Training Surgeons for Disasters M. Margaret Knudson MD, FACS Chief of Surgery, San Francisco General Hospital and Trauma Center A MASS CASUALTY EVENT IS NOT JUST ANOTHER
SURGICAL RESPONSE TO DISASTERS Training Surgeons for Disasters M. Margaret Knudson MD, FACS Chief of Surgery, San Francisco General Hospital and Trauma Center A MASS CASUALTY EVENT IS NOT JUST ANOTHER
Paramedic Trauma
 Western Technical College 10531920 Paramedic Trauma Course Outcome Summary Course Information Description Career Cluster Instructional Level Total Credits 3.00 Total Hours 72.00 This course teaches the
Western Technical College 10531920 Paramedic Trauma Course Outcome Summary Course Information Description Career Cluster Instructional Level Total Credits 3.00 Total Hours 72.00 This course teaches the
EMS System for Metropolitan Oklahoma City and Tulsa 2019 Medical Control Board Treatment Protocols
 EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #2 Blunt Trauma
 McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #2 Blunt Trauma Blunt trauma is the most common cause of traumatic death and disability. The definition
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #2 Blunt Trauma Blunt trauma is the most common cause of traumatic death and disability. The definition
PARA107 Summary. Page 1-3: Page 4-6: Page 7-10: Page 11-13: Page 14-17: Page 18-21: Page 22-25: Page 26-28: Page 29-33: Page 34-36: Page 37-38:
 PARA107 Summary Page 1-3: Page 4-6: Page 7-10: Page 11-13: Page 14-17: Page 18-21: Page 22-25: Page 26-28: Page 29-33: Page 34-36: Page 37-38: Injury, Mechanisms of Injury, Time Critical Guidelines Musculoskeletal
PARA107 Summary Page 1-3: Page 4-6: Page 7-10: Page 11-13: Page 14-17: Page 18-21: Page 22-25: Page 26-28: Page 29-33: Page 34-36: Page 37-38: Injury, Mechanisms of Injury, Time Critical Guidelines Musculoskeletal
3. D Objective: Chapter 4, Objective 4 Page: 79 Rationale: A carbon dioxide level below 35 mmhg indicates hyperventilation.
 1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
Kinetic Energy Energy in Motion KE = Mass (weight) X Velocity (speed)² 2 Double Weight = Energy Double Speed = Energy IS THE GREATEST DETERMINANT
 X Velocity (speed)² 2 Double Weight = Energy Double Speed = Energy IS THE GREATEST DETERMINANT") 1 Chapter 17 Blunt Trauma 2 Introduction to Blunt Trauma Most common cause of trauma death and disability exchange between an object and the human body, without intrusion through the skin 3 Blunt trauma
1 Chapter 17 Blunt Trauma 2 Introduction to Blunt Trauma Most common cause of trauma death and disability exchange between an object and the human body, without intrusion through the skin 3 Blunt trauma
Civilian versus Military Trauma Management
 Western University From the SelectedWorks of Vivian C. McAlister November, 2010 Civilian versus Military Trauma Management Vivian C. McAlister Available at: https://works.bepress.com/vivianmcalister/151/
Western University From the SelectedWorks of Vivian C. McAlister November, 2010 Civilian versus Military Trauma Management Vivian C. McAlister Available at: https://works.bepress.com/vivianmcalister/151/
Pediatric Trauma Care
 2013 Standard Trauma Care Procedures (Pediatric) Traumatic injuries require prompt care and transportation. Always suspect cervical injury. Note the mechanism of injury and any other condition that may
2013 Standard Trauma Care Procedures (Pediatric) Traumatic injuries require prompt care and transportation. Always suspect cervical injury. Note the mechanism of injury and any other condition that may
Orthopaedic Blast Injuries
 Orthopaedic Blast Injuries OTA Disaster Preparedness Committee Christopher Born, MD (Chair) Mark McAndrew, MD Christiaan Mamczak, DO Eric Pagenkopf, MD Mark Richardson, MD David Teague, MD Philip Wolinsky,
Orthopaedic Blast Injuries OTA Disaster Preparedness Committee Christopher Born, MD (Chair) Mark McAndrew, MD Christiaan Mamczak, DO Eric Pagenkopf, MD Mark Richardson, MD David Teague, MD Philip Wolinsky,
PARAMEDIC COURSE OBJECTIVES
 ELEMENT TITLE PARAMEDIC COURSE OBJECTIVES 100000 INTRODUCTION TO PARAMEDICINE 101000 Introduction to Paramedicine 101000T Discuss the characteristics of the profession of paramedicine. 102000 EMS Systems
ELEMENT TITLE PARAMEDIC COURSE OBJECTIVES 100000 INTRODUCTION TO PARAMEDICINE 101000 Introduction to Paramedicine 101000T Discuss the characteristics of the profession of paramedicine. 102000 EMS Systems
Pediatric Trauma Karim Rafaat, MD
 Pediatric Trauma Karim Rafaat, MD Goals Time is short I m going to presume you know your basic ATLS (that s that whole ABCD thing, by the way) Discuss each general trauma susceptible region Focus on: Epidemiology
Pediatric Trauma Karim Rafaat, MD Goals Time is short I m going to presume you know your basic ATLS (that s that whole ABCD thing, by the way) Discuss each general trauma susceptible region Focus on: Epidemiology
European Resuscitation Council
 European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
ITLS Pediatric Provider Course Advanced Pre-Test
 ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D.
 1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D. Sacral-coccygeal 2. A 36-year-old male sustains blunt force thoracic
1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D. Sacral-coccygeal 2. A 36-year-old male sustains blunt force thoracic
CLINICAL MANUAL. Trauma System Activation Trauma Code Criteria
 CLINICAL MANUAL Policy Number: CM T-28 Approved by: Nursing Congress, Management Forum Issue Date: 09/1999 Applies to: Downtown Value(s): Respect, Integrity, Innovation Page(s): 1 of 4 Trauma System Activation
CLINICAL MANUAL Policy Number: CM T-28 Approved by: Nursing Congress, Management Forum Issue Date: 09/1999 Applies to: Downtown Value(s): Respect, Integrity, Innovation Page(s): 1 of 4 Trauma System Activation
Basic Assessment and Treatment of Trauma
 Basic Assessment and Treatment of Trauma Final Exam Version 1 1. In which of the following scenarios would the potential for serious injury or death be the GREATEST? A. 77-kg (170-lb) man who falls 1.2
Basic Assessment and Treatment of Trauma Final Exam Version 1 1. In which of the following scenarios would the potential for serious injury or death be the GREATEST? A. 77-kg (170-lb) man who falls 1.2
In ESH we usually see blunt chest trauma but penetrating injuries also treated here (usually as single injuries, like stab wound)
") Chest Trauma Dr Csaba Dioszeghy MD PhD FRCEM FFICM FERC East Surrey Hospital Emergency Department Scope Thoracic injuries are common and can be life threatening In ESH we usually see blunt chest trauma
Chest Trauma Dr Csaba Dioszeghy MD PhD FRCEM FFICM FERC East Surrey Hospital Emergency Department Scope Thoracic injuries are common and can be life threatening In ESH we usually see blunt chest trauma
Pre-hospital Trauma Life Support. Rattiya Banjungam Emergency Physician, Khon Kaen Hospital
 Pre-hospital Trauma Life Support Rattiya Banjungam Emergency Physician, Khon Kaen Hospital Golden principles of Prehospital Trauma Care Golden Hour There is a golden hour if you are critically injured,
Pre-hospital Trauma Life Support Rattiya Banjungam Emergency Physician, Khon Kaen Hospital Golden principles of Prehospital Trauma Care Golden Hour There is a golden hour if you are critically injured,
ITLS Advanced Pre-Test Annotated Key 8 th Edition
 1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
Outline. Madrid Bombing - Injuries 10/2/2015. Clinical Manifestation of Blast Injuries
 Clinical Manifestation of Blast Injuries ADVANCED EXPLOSIONS & BLAST INJURIES Outline Types of injuries seen Injury characterization Specific Injuries - Primary - Secondary - Tertiary - Quaternary - Quinary
Clinical Manifestation of Blast Injuries ADVANCED EXPLOSIONS & BLAST INJURIES Outline Types of injuries seen Injury characterization Specific Injuries - Primary - Secondary - Tertiary - Quaternary - Quinary
SESSION PLAN FAA LEVEL 3 AWARD IN FIRST AID AT WORK (RQF) AWARD IN FIRST AID AT WORK AT SCQF LEVEL 6 REQUALIFICATION COURSE.
 AWARD IN FIRST AID AT WORK AT SCQF LEVEL 6 REQUALIFICATION COURSE.") FAA LEVEL 3 AWARD IN FIRST AID AT WORK (RQF) AWARD IN FIRST AID AT WORK AT SCQF LEVEL 6 REQUALIFICATION COURSE Unit 1 : Emergency First Aid in the Workplace : 6 hour duration Full qualification requires
FAA LEVEL 3 AWARD IN FIRST AID AT WORK (RQF) AWARD IN FIRST AID AT WORK AT SCQF LEVEL 6 REQUALIFICATION COURSE Unit 1 : Emergency First Aid in the Workplace : 6 hour duration Full qualification requires
Chapter 29 - Chest_and_Abdominal_Trauma
 Introduction to Emergency Medical Care 1 OBJECTIVES 29.1 Define key terms introduced in this chapter. Slides 11, 15, 18, 27 29.2 Describe mechanisms of injury commonly associated with chest injuries. Slides
Introduction to Emergency Medical Care 1 OBJECTIVES 29.1 Define key terms introduced in this chapter. Slides 11, 15, 18, 27 29.2 Describe mechanisms of injury commonly associated with chest injuries. Slides
CHEST INJURIES. Jacek Piątkowski M.D., Ph. D.
 CHEST INJURIES Jacek Piątkowski M.D., Ph. D. CHEST INJURIES 3-4% of all injuries 8% of patients hospitalized due to injuries 65% of patients who died at the accident place CLASSIFICATION OF THE CHEST INJURIES
CHEST INJURIES Jacek Piątkowski M.D., Ph. D. CHEST INJURIES 3-4% of all injuries 8% of patients hospitalized due to injuries 65% of patients who died at the accident place CLASSIFICATION OF THE CHEST INJURIES
Prehospital Resuscitation for the 21 st Century Simulation Case. VF/Asystole
 Prehospital Resuscitation for the 21 st Century Simulation Case VF/Asystole Case History 1 (hypovolemic cardiac arrest secondary to massive upper GI bleed) 56 year-old male patient who fainted in the presence
Prehospital Resuscitation for the 21 st Century Simulation Case VF/Asystole Case History 1 (hypovolemic cardiac arrest secondary to massive upper GI bleed) 56 year-old male patient who fainted in the presence
PEDIATRIC TRAUMA: Implications for Respiratory Care
 PEDIATRIC TRAUMA: Implications for Respiratory Care 17 th Annual Rainbow Respiratory Conference - September 4, 2015 Mike Dingeldein, MD Pediatric Surgeon Pediatric Trauma Medical Director Disclosures none
PEDIATRIC TRAUMA: Implications for Respiratory Care 17 th Annual Rainbow Respiratory Conference - September 4, 2015 Mike Dingeldein, MD Pediatric Surgeon Pediatric Trauma Medical Director Disclosures none
Radiological Injuries
 Radiological Injuries Chapter 30 Radiological Injuries The reader is strongly advised to supplement material in this chapter with the following two references: 1. Medical Management of Radiological Casualties
Radiological Injuries Chapter 30 Radiological Injuries The reader is strongly advised to supplement material in this chapter with the following two references: 1. Medical Management of Radiological Casualties
6. Knowledge and Skill Comparison (Paramedic)
") 6. Knowledge and Skill Comparison (Paramedic) The order of content is not meant to imply the order of delivery. a. Paramedic: New Course Considerations When planning and conducting a new Paramedic course,
6. Knowledge and Skill Comparison (Paramedic) The order of content is not meant to imply the order of delivery. a. Paramedic: New Course Considerations When planning and conducting a new Paramedic course,
Trauma Overview. Chapter 22
 Trauma Overview Chapter 22 Kinematics of Trauma Injuries are the leading cause of death among children and young adults. Kinematics introduces the basic physical concepts that dictate how injuries occur
Trauma Overview Chapter 22 Kinematics of Trauma Injuries are the leading cause of death among children and young adults. Kinematics introduces the basic physical concepts that dictate how injuries occur
Pediatric Aspects of Advanced Trauma Life Support: Transition from EMS to the Trauma Room PEDIATRIC TRAUMA DIRECTOR, HASBRO CHILDREN S HOSPITAL
 Pediatric Aspects of Advanced Trauma Life Support: Transition from EMS to the Trauma Room HALE WILLS, MD PEDIATRIC TRAUMA DIRECTOR, HASBRO CHILDREN S HOSPITAL Objectives 1. Identify the critical components
Pediatric Aspects of Advanced Trauma Life Support: Transition from EMS to the Trauma Room HALE WILLS, MD PEDIATRIC TRAUMA DIRECTOR, HASBRO CHILDREN S HOSPITAL Objectives 1. Identify the critical components
ITLS Pediatric Provider Course Basic Pre-Test
 ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
Restore adequate respiratory and circulatory conditions. Reduce pain
 Pre-hospital management of the trauma patient is best performed by an integrated team focused on minimizing the time from injury to definitive care at an appropriate trauma center. Dispatchers, first responders,
Pre-hospital management of the trauma patient is best performed by an integrated team focused on minimizing the time from injury to definitive care at an appropriate trauma center. Dispatchers, first responders,
You Are the Emergency Medical Responder
 Lesson 32: Injuries to the Chest, Abdomen and Genitalia You Are the Emergency Medical Responder Your police unit responds to a call in a part of town plagued by violence. When you arrive, you find the
Lesson 32: Injuries to the Chest, Abdomen and Genitalia You Are the Emergency Medical Responder Your police unit responds to a call in a part of town plagued by violence. When you arrive, you find the
McCann Technical School 70 Hodges Cross Road North Adams, MA Medical Assisting Program
 MA 104 MEDICAL SOCIAL SCIENCE 4 Credits Fall Semester Part IV FIRST RESPONDER Syllabus McCann Technical School 70 Hodges Cross Road North Adams, MA 01247 Medical Assisting Program INSTRUCTORS: Laurie Tuper,
MA 104 MEDICAL SOCIAL SCIENCE 4 Credits Fall Semester Part IV FIRST RESPONDER Syllabus McCann Technical School 70 Hodges Cross Road North Adams, MA 01247 Medical Assisting Program INSTRUCTORS: Laurie Tuper,
 55-year-old male with 2nd and 3rd degree burns to face, chest, and arms on 25% of the body Respirations: 34 Pulse: 120 Mental Status: moans to painful stimulus Mucous membranes charred Stridor 10 cm scalp
55-year-old male with 2nd and 3rd degree burns to face, chest, and arms on 25% of the body Respirations: 34 Pulse: 120 Mental Status: moans to painful stimulus Mucous membranes charred Stridor 10 cm scalp
Abdomen and Genitalia Injuries. Chapter 28
 Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Competency Log Professional Responder Courses
 Competency Log Professional Responder Courses Check off each competency once successfully demonstrated. This log may be used as a support tool when teaching a Professional Responder course. Refer to the
Competency Log Professional Responder Courses Check off each competency once successfully demonstrated. This log may be used as a support tool when teaching a Professional Responder course. Refer to the
No conflicts of interest
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Skin is the largest, most important organ % of total body weight Functions: - -Sensation - Regulation AKA: System
 1 Chapter 20 Soft-Tissue Injury 2 Introduction to Soft-Tissue Injury Skin is the largest, most important organ % of total body weight Functions: - -Sensation - Regulation AKA: System 3 Epidemiology Most
1 Chapter 20 Soft-Tissue Injury 2 Introduction to Soft-Tissue Injury Skin is the largest, most important organ % of total body weight Functions: - -Sensation - Regulation AKA: System 3 Epidemiology Most
EMERGENCY MEDICAL SERVICES ONLINE COURSE CATALOG. TargetSolutions. Technology with a Purpose
 EMERGENCY MEDICAL SERVICES ONLINE COURSE CATALOG 1 Technology with a Purpose TargetSolutions delivers employee training that helps organizations achieve compliance, mitigate We risk, believe reduce a well-trained
EMERGENCY MEDICAL SERVICES ONLINE COURSE CATALOG 1 Technology with a Purpose TargetSolutions delivers employee training that helps organizations achieve compliance, mitigate We risk, believe reduce a well-trained
Radiological Injuries
 Chapter 28 The reader is strongly advised to supplement material in this chapter with the following two references: 1. Armed Forces Radiobiology Research Institute. Medical Management of Radiological Casualties.
Chapter 28 The reader is strongly advised to supplement material in this chapter with the following two references: 1. Armed Forces Radiobiology Research Institute. Medical Management of Radiological Casualties.
Emergency Room Resuscitation of the Unstable Trauma Patient
 Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
The Management of Chest Trauma. Tom Scaletta, MD FAAEM Immediate Past President, AAEM
 The Management of Chest Trauma Tom Scaletta, MD FAAEM Immediate Past President, AAEM Trichotomizing Rib Fractures Upper 1-3 vascular injuries Middle 4-9 Lower 10-12 12 liver/spleen injuries Management
The Management of Chest Trauma Tom Scaletta, MD FAAEM Immediate Past President, AAEM Trichotomizing Rib Fractures Upper 1-3 vascular injuries Middle 4-9 Lower 10-12 12 liver/spleen injuries Management
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials
 Preparatory Materials") Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
Z19.2 Cross Reference to Patient Care Maps & Clinical Care Procedures
 2017-04-07 Old version G1 Code of Ethics G2 Scope and Function G3 Scene Assessment G4 Triage G5 Primary Survey G6 Shock G7 Load and Go G8 Secondary Survey G9 Unconscious Patient G10A Obstructed Airway
2017-04-07 Old version G1 Code of Ethics G2 Scope and Function G3 Scene Assessment G4 Triage G5 Primary Survey G6 Shock G7 Load and Go G8 Secondary Survey G9 Unconscious Patient G10A Obstructed Airway
CARDIAC ARREST IN SPECIAL CIRCUMSTANCES 2
 CARDIAC ARREST IN SPECIAL CIRCUMSTANCES 2 M1 Objectives To understand how resuscitation techniques should be modified in the special circumstances of: Hypothermia Immersion and submersion Poisoning Pregnancy
CARDIAC ARREST IN SPECIAL CIRCUMSTANCES 2 M1 Objectives To understand how resuscitation techniques should be modified in the special circumstances of: Hypothermia Immersion and submersion Poisoning Pregnancy
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours
 Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Pediatric Trauma. Sept 2nd, Patrick Murphy Neil Merritt
 Pediatric Trauma Sept 2nd, 2015 Patrick Murphy Neil Merritt Objectives Objectives Medical Expert 1. Describe the types of pediatric injuries sustained with a given mode of trauma, and identify the most
Pediatric Trauma Sept 2nd, 2015 Patrick Murphy Neil Merritt Objectives Objectives Medical Expert 1. Describe the types of pediatric injuries sustained with a given mode of trauma, and identify the most
Review. A. abrasion B. contusion C. hematoma D. avulsion
 Chapter 24 Review Review 1. A young male was struck in the forearm with a baseball and complains of pain to the area. Slight swelling and ecchymosis are present, but no external bleeding. What type of
Chapter 24 Review Review 1. A young male was struck in the forearm with a baseball and complains of pain to the area. Slight swelling and ecchymosis are present, but no external bleeding. What type of
Pediatric Trauma. July 27 th, Suzana Buac, PGY4. Dr. Neil Merritt
 Pediatric Trauma July 27 th, 2016. Suzana Buac, PGY4 Dr. Neil Merritt Case 5yoM fall from roof Fall from roof of home while father was shingling 5yoM fall from roof Fall from roof of home while father
Pediatric Trauma July 27 th, 2016. Suzana Buac, PGY4 Dr. Neil Merritt Case 5yoM fall from roof Fall from roof of home while father was shingling 5yoM fall from roof Fall from roof of home while father
Trauma Registry Documentation December 16, 2014
 Trauma Registry Documentation December 16, 2014 The State of Florida now requires ALL Acute Care hospitals to submit data to the statetrauma Registry. Although Baptist Health hospitals are NOT Trauma Centers
Trauma Registry Documentation December 16, 2014 The State of Florida now requires ALL Acute Care hospitals to submit data to the statetrauma Registry. Although Baptist Health hospitals are NOT Trauma Centers
Explosions and Blast Injuries
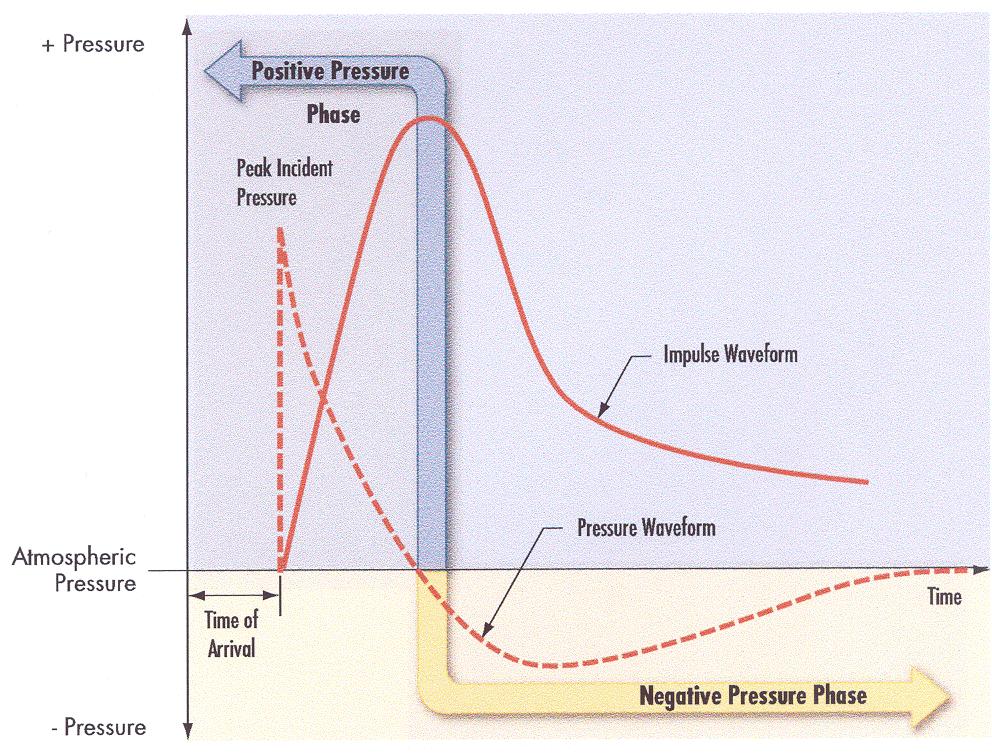
 Explosions and Blast Injuries Definition The almost instantaneous conversion of a solid or liquid into a gas at 10-15,000 times the original volume producing Blast wave Fragmentation Incendiary effects
Explosions and Blast Injuries Definition The almost instantaneous conversion of a solid or liquid into a gas at 10-15,000 times the original volume producing Blast wave Fragmentation Incendiary effects
PEDIATRIC TRAUMA I: ABDOMINAL TRAUMA BURNS. December 19, 2012
 PEDIATRIC TRAUMA I: ABDOMINAL TRAUMA BURNS Niel F. Miele,, M.D. December 19, 2012 EPIDEMIOLOGY Major Trauma responsible for
PEDIATRIC TRAUMA I: ABDOMINAL TRAUMA BURNS Niel F. Miele,, M.D. December 19, 2012 EPIDEMIOLOGY Major Trauma responsible for
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of
 Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
MANAGEMENT OF THORACIC TRAUMA. Luis H. Tello MV, MS DVM, COS Portland Hospital Classic Banfield Pet Hospital - USA
 MANAGEMENT OF THORACIC TRAUMA Luis H. Tello MV, MS DVM, COS Portland Hospital Classic Banfield Pet Hospital - USA luis.tello@banfield.com Chest Trauma: Big threat!!!! CAUSES OF THORACIC TRAUMA Blunt Trauma
MANAGEMENT OF THORACIC TRAUMA Luis H. Tello MV, MS DVM, COS Portland Hospital Classic Banfield Pet Hospital - USA luis.tello@banfield.com Chest Trauma: Big threat!!!! CAUSES OF THORACIC TRAUMA Blunt Trauma
Penetrating Trauma in Pediatric Patients. Heidi P. Cordi, MD, MPH, MS, EMTP, FACEP, FAADM EMS WEEK 2017
 Penetrating Trauma in Pediatric Patients Heidi P. Cordi, MD, MPH, MS, EMTP, FACEP, FAADM EMS WEEK 2017 Introduction Trauma is the leading cause of death between ages of 1-18 years Penetrating injury accounts
Penetrating Trauma in Pediatric Patients Heidi P. Cordi, MD, MPH, MS, EMTP, FACEP, FAADM EMS WEEK 2017 Introduction Trauma is the leading cause of death between ages of 1-18 years Penetrating injury accounts
Competencies and Objectives
 Competencies and Objectives Chapter 1 EMS Systems Preparatory Emergency Medical Services (EMS) Systems Research Public Health Chapter 2 Workforce Safety and Wellness Medicine Infectious Diseases Preparatory
Competencies and Objectives Chapter 1 EMS Systems Preparatory Emergency Medical Services (EMS) Systems Research Public Health Chapter 2 Workforce Safety and Wellness Medicine Infectious Diseases Preparatory
Initial Management of Crush Injuries. Cindy Goodrich RN, MS, CCRN Airlift Northwest
 Initial Management of Crush Injuries Cindy Goodrich RN, MS, CCRN Airlift Northwest Case Presentation Called to isolated logging road MVC: logging truck vs tree Arrival to Scene Logging Truck vs Tree
Initial Management of Crush Injuries Cindy Goodrich RN, MS, CCRN Airlift Northwest Case Presentation Called to isolated logging road MVC: logging truck vs tree Arrival to Scene Logging Truck vs Tree
APPROACH TO TRAUMA. Dr E.Memary Anesthesiologist Assistant Professor of SBMU
 APPROACH TO TRAUMA Dr E.Memary Anesthesiologist Assistant Professor of SBMU Objectives Describe the initial approach to the injured patient, including the primary and secondary surveys. Identify the types
APPROACH TO TRAUMA Dr E.Memary Anesthesiologist Assistant Professor of SBMU Objectives Describe the initial approach to the injured patient, including the primary and secondary surveys. Identify the types
2. Blunt abdominal Trauma
 Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
Chapter 29 - Chest Injuries
 1 2 3 4 5 6 7 8 9 National EMS Education Standard Competencies (1 of 5) Trauma Applies fundamental knowledge to provide basic emergency care and transportation based on assessment findings for an acutely
1 2 3 4 5 6 7 8 9 National EMS Education Standard Competencies (1 of 5) Trauma Applies fundamental knowledge to provide basic emergency care and transportation based on assessment findings for an acutely
ADMINISTRATIVE REQUIREMENT MANUAL EFFECTIVE DATE
 PURPOSE: I. To establish the minimum requirements for a first responder training course in first aid, which all first responders must take, in order to meet the requirements of M.G.L. c. 111, 201 and 105
PURPOSE: I. To establish the minimum requirements for a first responder training course in first aid, which all first responders must take, in order to meet the requirements of M.G.L. c. 111, 201 and 105
SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services OBJECTIVES DEFINITION 11/8/2017. Identify SCIWORA.
 SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services Identify SCIWORA. OBJECTIVES Identify the population at risk. To identify anatomic and physiologic reasons for SCIWORA. To
SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services Identify SCIWORA. OBJECTIVES Identify the population at risk. To identify anatomic and physiologic reasons for SCIWORA. To
Clinical Pathway: Management Of The Life-Threatening Overdose
 Clinical Pathway: Management Of The Life-Threatening Overdose Intravenous access Oxygen Pulse oximetry n-invasive blood pressure monitoring Accu-Check ECG monitoring and ECG Chest x-ray Respiratory depression?
Clinical Pathway: Management Of The Life-Threatening Overdose Intravenous access Oxygen Pulse oximetry n-invasive blood pressure monitoring Accu-Check ECG monitoring and ECG Chest x-ray Respiratory depression?
BIG BANG THEORY PHYSICS AND PHYSIOLOGY OF BLAST
 BIG BANG THEORY PHYSICS AND PHYSIOLOGY OF BLAST JUSTIN LEMIEUX, MD STANFORD EMERGENCY MEDICINE DISCLOSURES This presentation includes proprietary (patent-pending) technology that my team is currently developing
BIG BANG THEORY PHYSICS AND PHYSIOLOGY OF BLAST JUSTIN LEMIEUX, MD STANFORD EMERGENCY MEDICINE DISCLOSURES This presentation includes proprietary (patent-pending) technology that my team is currently developing
Aurora Health Care EMS Continuing Education Spring 2011 Packet THORACIC TRAUMA THE PREHOSPITAL APPROACH TO CHEST INJURY MANAGEMENT
 Aurora Health Care EMS Continuing Education Spring 2011 Packet THORACIC TRAUMA Chest injuries are significant contributors to death from major trauma and can be difficult to assess adequately in the pre-hospital
Aurora Health Care EMS Continuing Education Spring 2011 Packet THORACIC TRAUMA Chest injuries are significant contributors to death from major trauma and can be difficult to assess adequately in the pre-hospital
BASE HOSPITAL PROTOCOL INDEX
 BASE HOSPITAL PROTOCOL INDEX 1. EPIC-Kids Algorithm 2. EPIC-Adult-Algorithm 3. External Hemorrhage Control Protocol 4. Spinal Motion Restriction 1-15; 01-16 Airway/Breathing O 2 sat
BASE HOSPITAL PROTOCOL INDEX 1. EPIC-Kids Algorithm 2. EPIC-Adult-Algorithm 3. External Hemorrhage Control Protocol 4. Spinal Motion Restriction 1-15; 01-16 Airway/Breathing O 2 sat
Emergency Care Progress Log
 Emergency Care Progress Log For further details on the National Occupational Competencies for EMRs, please visit www.paramedic.ca. Check off each skill once successfully demonstrated the Instructor. All
Emergency Care Progress Log For further details on the National Occupational Competencies for EMRs, please visit www.paramedic.ca. Check off each skill once successfully demonstrated the Instructor. All
Skin Anatomy and Physiology
 Skin Anatomy and Physiology Body s largest organ Three layers: Epidermis Dermis Subcutaneous tissue 1 2 Skin Anatomy and Physiology Complex system, variety of functions Sensation Control of water loss
Skin Anatomy and Physiology Body s largest organ Three layers: Epidermis Dermis Subcutaneous tissue 1 2 Skin Anatomy and Physiology Complex system, variety of functions Sensation Control of water loss
DR. SAAD AL-MUHAYAWI, M.D., FRCSC. ORL Head & Neck Surgery
 TRAUMA IN ORL DR. SAAD AL-MUHAYAWI, M.D., FRCSC Associate Professor & Consultant ORL Head & Neck Surgery TYPES OF TRAUMA EAR & TEMPORAL BONE TRAUMA NOSE & FACIAL BONES TRAUMA LARYNGEAL TRAUMA NECK TRAUMA
TRAUMA IN ORL DR. SAAD AL-MUHAYAWI, M.D., FRCSC Associate Professor & Consultant ORL Head & Neck Surgery TYPES OF TRAUMA EAR & TEMPORAL BONE TRAUMA NOSE & FACIAL BONES TRAUMA LARYNGEAL TRAUMA NECK TRAUMA
Clues of a Ruptured Globe
 Definition any eye that has sustained a full thickness traumatic disruption of the cornea or sclera Overwhelmingly, rupture accidents occur in young men, small children and the elderly Corneal laceration
Definition any eye that has sustained a full thickness traumatic disruption of the cornea or sclera Overwhelmingly, rupture accidents occur in young men, small children and the elderly Corneal laceration
Face and Throat Injuries. Chapter 26
 Face and Throat Injuries Chapter 26 Anatomy of the Head Landmarks of the Neck Injuries to the Face Injuries around the face can lead to upper airway obstructions. Bleeding from the face can be profuse.
Face and Throat Injuries Chapter 26 Anatomy of the Head Landmarks of the Neck Injuries to the Face Injuries around the face can lead to upper airway obstructions. Bleeding from the face can be profuse.
! Please rate by checking ( ): 5 = Highest, best or most.! 1 = Lowest, least, or worst
: 5 = Highest, best or most.! 1 = Lowest, least, or worst") Day 1 Evaluation Please rate by checking ( ): 5 = Highest, best or most. Please rate the extent to which your personal objectives were met 20 6 1 Please rate the appropriateness of the physical facilities
Day 1 Evaluation Please rate by checking ( ): 5 = Highest, best or most. Please rate the extent to which your personal objectives were met 20 6 1 Please rate the appropriateness of the physical facilities
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal injuries, abdominal wall muscle injury, 212 213 diaphragmatic spasm, 212 liver injury, 213 214 pancreatic injury, 216 rectus
Index Note: Page numbers of article titles are in boldface type. A Abdominal injuries, abdominal wall muscle injury, 212 213 diaphragmatic spasm, 212 liver injury, 213 214 pancreatic injury, 216 rectus
Explosive Blast Traumatic Brain Injury Geoffrey Ling, M.D., Ph.D.
 Explosive Blast Traumatic Brain Injury Geoffrey Ling, M.D., Ph.D. Colonel, Medical Corps, US Army Program Manager, DARPA Professor and Vice-Chair, Neurology, USUHS Director, Neuro Critical Care, WRAMC
Explosive Blast Traumatic Brain Injury Geoffrey Ling, M.D., Ph.D. Colonel, Medical Corps, US Army Program Manager, DARPA Professor and Vice-Chair, Neurology, USUHS Director, Neuro Critical Care, WRAMC
Burnt and Blasted: How to Manage Common Injuries from a Galaxy Far, Far Away. Concepts From the Conflicts: New Advances in Trauma Care
 Burnt and Blasted: How to Manage Common Injuries from a Galaxy Far, Far Away WE - 204/ 0.5 Hour(s) Faculty: Jacob Avila, MD This session will cover how to manage injuries on earth or in a galaxy far, far
Burnt and Blasted: How to Manage Common Injuries from a Galaxy Far, Far Away WE - 204/ 0.5 Hour(s) Faculty: Jacob Avila, MD This session will cover how to manage injuries on earth or in a galaxy far, far
PEDIATRIC TREATMENT GUIDELINES - CARDIAC VENTRICULAR FIBRILLATION - PULSELESS VENTRICULAR TACHYCARDIA (SJ-PO1) effective 05/01/02
 effective 05/01/02") PEDIATRIC TREATMENT GUIDELINES - CARDIAC VENTRICULAR FIBRILLATION - PULSELESS VENTRICULAR TACHYCARDIA (SJ-PO1) effective 05/01/02 Revision #5 04/19/02 Identify Dysrhythmia DEFIBRILLATE: 2 J/kg, 4 J/kg,
PEDIATRIC TREATMENT GUIDELINES - CARDIAC VENTRICULAR FIBRILLATION - PULSELESS VENTRICULAR TACHYCARDIA (SJ-PO1) effective 05/01/02 Revision #5 04/19/02 Identify Dysrhythmia DEFIBRILLATE: 2 J/kg, 4 J/kg,
Cases from the Streets. Kelly Buchanan MD, ATC/L EMS Fellow December, 2011
 Cases from the Streets Kelly Buchanan MD, ATC/L EMS Fellow December, 2011 The Scene Car vs Light Pole, 35 mph, front right side damage 10 with no PCI + airbag deployment, starring on windshield Given the
Cases from the Streets Kelly Buchanan MD, ATC/L EMS Fellow December, 2011 The Scene Car vs Light Pole, 35 mph, front right side damage 10 with no PCI + airbag deployment, starring on windshield Given the
Pneumothorax. Defined as air in the pleural space which can occur through a number of mechanisms
 Pneumothorax Defined as air in the pleural space which can occur through a number of mechanisms Traumatic pneumothorax Penetrating chest trauma Common secondary to bullet or knife penetration Chest tube
Pneumothorax Defined as air in the pleural space which can occur through a number of mechanisms Traumatic pneumothorax Penetrating chest trauma Common secondary to bullet or knife penetration Chest tube
Request Card Task ANSWERS
 Request Card Task ANSWERS Medical Student Workbook Author: Dr Sam Leach, SpR Case 1 What differential diagnoses are most likely? Which investigation is most appropriate? Case 1 The most likely diagnosis
Request Card Task ANSWERS Medical Student Workbook Author: Dr Sam Leach, SpR Case 1 What differential diagnoses are most likely? Which investigation is most appropriate? Case 1 The most likely diagnosis
Hypotension / Shock. Adult Medical Section Protocols. Protocol 30
 Hypotension / Shock History Blood loss - vaginal or gastrointestinal bleeding, AAA, ectopic Fluid loss - vomiting, diarrhea, fever nfection Cardiac ischemia (M, CHF) Medications Allergic reaction regnancy
Hypotension / Shock History Blood loss - vaginal or gastrointestinal bleeding, AAA, ectopic Fluid loss - vomiting, diarrhea, fever nfection Cardiac ischemia (M, CHF) Medications Allergic reaction regnancy
Damage Control in Abdominal and Pelvic Injuries
 Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
ATLS: Initial Assessment and Management. SAUSHEC Medical Student Lecture Series
 ATLS: Initial Assessment and Management SAUSHEC Medical Student Lecture Series Objectives Identify sequence of priorities in assessing the multiply injured patient Apply principles outlined in primary
ATLS: Initial Assessment and Management SAUSHEC Medical Student Lecture Series Objectives Identify sequence of priorities in assessing the multiply injured patient Apply principles outlined in primary
NOTICE OF INTENT TO CONDUCT INITIAL EMS TRAINING COURSE
 Request Date: NOTICE OF INTENT TO CONDUCT INITIAL EMS TRAINING COURSE Note: This form MUST be submitted to the Office of EMS & Trauma System (ems@snhdmail.org) at least THIRTY (30) DAYS prior to course
Request Date: NOTICE OF INTENT TO CONDUCT INITIAL EMS TRAINING COURSE Note: This form MUST be submitted to the Office of EMS & Trauma System (ems@snhdmail.org) at least THIRTY (30) DAYS prior to course
2017 Northern Mine Rescue Contest Written Exam (First Aid Competition)
") 2017 Northern Mine Rescue Contest Written Exam (First Aid Competition) 2017 2010 June 5, 2017 Findley Lake, New York 2017 Northern Mine Rescue Contest Written Exam First Aid Competition Directions: Fill
2017 Northern Mine Rescue Contest Written Exam (First Aid Competition) 2017 2010 June 5, 2017 Findley Lake, New York 2017 Northern Mine Rescue Contest Written Exam First Aid Competition Directions: Fill
Disaster Triage START/JUMPSTART
 Disaster Triage START/JUMPSTART Finger Lakes Regional Training Center AGENDA Attendance Ground Rules Presentation Scenarios Additional Resources Evaluation/Certificate Objectives: Define a Mass Casualty
Disaster Triage START/JUMPSTART Finger Lakes Regional Training Center AGENDA Attendance Ground Rules Presentation Scenarios Additional Resources Evaluation/Certificate Objectives: Define a Mass Casualty
Trauma/Burn Clinical Guidelines
 D Trauma/Burn Clinical Guidelines I S A A Quick Guide for the Management of Trauma/Burn Disasters for Emergency Department Personnel S Rev. August 2013 T E www.ynhhs.org/cepdr R Emergency Information for
D Trauma/Burn Clinical Guidelines I S A A Quick Guide for the Management of Trauma/Burn Disasters for Emergency Department Personnel S Rev. August 2013 T E www.ynhhs.org/cepdr R Emergency Information for
The ABC s of Chest Trauma
 The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
PEMSS PROTOCOLS INVASIVE PROCEDURES
 PEMSS PROTOCOLS INVASIVE PROCEDURES Panhandle Emergency Medical Services System SURGICAL AND NEEDLE CRICOTHYROTOMY Inability to intubate is the primary indication for creating an artificial airway. Care
PEMSS PROTOCOLS INVASIVE PROCEDURES Panhandle Emergency Medical Services System SURGICAL AND NEEDLE CRICOTHYROTOMY Inability to intubate is the primary indication for creating an artificial airway. Care
Radiological Investigations of Abdominal Trauma
 76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,