Potassium A NNA VINNIKOVA, M. D.
|
|
|
- Kristopher Mathews
- 6 years ago
- Views:
Transcription

1 Potassium A NNA VINNIOVA, M. D. DIVISION OF NEPHROLOGY Graphics by permission from The Fluid, Electrolyte and Acid-Base Companion, S. Faubel and J. Topf,
2 Do you want to hear a Sodium joke?
3 Do you want to hear a Sodium joke? Na
4 Do you want to hear a Sodium joke? Na Do you want to hear a Potassium joke?
5 Do you want to hear a Sodium joke? Na Do you want to hear a Potassium joke?!
6 POTASSIUM Main intracellular cation Cl

7 POTASSIUM Main intracellular cation Cl since first organisms



8 Potassium: basics 60 meq 4000 meq
9 Potassium: physiologic roles 1. Cell volume maintenance 2. Resting potential E m =-61 log r[ + ] c [Na + ] c r[ + ] e [Na + ] e 3. Action potential
10 Q1: Match EG with an electrical event 1 2 A. Depolarization of resting potential in pacemaker cells and slowed conduction B. Hyperpolarization of resting potential in pacemaker cells and increased automaticity
11 Pacemaker action potential
12 Hypokalemia Hyperpolarization
13 Normokalemia: pacemaker cells
14 Hypokalemia: pacemaker cells Hyperpolarization
15 Hypokalemia: pacemaker cells Hyperpolarization
16 Hypokalemia: pacemaker cells Brisk action potential Hyperpolarization


17 Hypokalemia: pacemaker cells Brisk action potential Enhanced excitability/ectopy Hyperpolarization
18 Hypokalemia: cardiac myocytes U-wave Delayed repolarization

19 Hypokalemia: hyperpolarization of resting potential, enhanced excitability/ectopy, delayed repolarization

20 Life-threatening hypokalemia: prolonged QT/torsades/reentrant arrhythmias
21 Hyperkalemia Depolarization
22 Normokalemia
23 Hyperkalemia Depolarization
24 Hyperkalemia Depolarization

25 Hyperkalemia Slowed conduction Depolarization
26 Cardiac cycle effect of hyperkalemia Peaked T wave Decreased automaticity, slowed conduction Brisk repolarization

27 Hyperkalemia and EG changes, the Fisherman

28 Life-threatening hyperkalemia: heart blocks, sine wave, VT/Vfib/asystole

29 Hyperkalemia: depolarization of resting potential, slowed conduction, brisk repolarization
30 Q1: Match EG with an electrical event 1 2 A. Depolarization of resting potential in pacemaker cells and slowed conduction B. Hyperpolarization of resting potential in pacemaker cells and increased automaticity

31 Q1: Match EG with an electrical event 1 2 A. Depolarization of resting potential in pacemaker cells and slowed conduction B. Hyperpolarization of resting potential in pacemaker cells and increased automaticity 1-A, 2-B
32 Potassium balance Internal External

33 Potassium balance _cells How much potassium is outside and inside the cell? Why?

34 Potassium balance _cells _Na,-ATPase
35 Potassium balance _cells _Na,-ATPase What regulates Na, -ATPase?

36 Potassium balance _cells _Na,-ATPase Digoxin is a classic blocker of Na, -ATPase

37 Potassium balance _cells _Na,-ATPase α-adrenergic stimulation inhibits and β2-adrenergic stimulation activates Na, -ATPase
38 Q2 Which pressor is most likely to cause hyperkalemia? A. Epinephrine B. Levophed C. Neosynephrine
39 Q2 Which pressor is most likely to cause hyperkalemia? A. Epinephrine: α1 α2 β1 β2 - least B. Levophed: α1 α2 β1 C. Neosynephrine: α1 - most
40 Potassium balance _cells _Na,-ATPase
41 Potassium balance _cells _Na,-ATPase Why should insulin stimulate Na, -ATPase?
42 Potassium balance _cells _Na,-ATPase Why should insulin stimulate Na, -ATPase? Let s take a standard breakfast:
43 Potassium balance _cells _Na,-ATPase
44 Potassium balance _cells _Na,-ATPase
45 Potassium balance _cells _Na,-ATPase
46 Potassium balance _cells _Na,-ATPase




47 Potassium balance _cells _Na,-ATPase This is more than in our entire blood volume!
48 Q3 A 28 year old patient with DM I presents to ER with N/V. Na 132, 5.8, Cl 100, bicarb 12, BUN 30, cr 1.0, glucose 612 What is the cause of patient s hyperkalemia? A. Metabolic acidosis B. Insulin deficiency C. Hypertonicity D. B and C E. All of the above
49 Q3 A 28 year old patient with DM I presents to ER with N/V. Na 132, 5.8, Cl 100, bicarb 12, BUN 30, cr 1.0, glucose 612 What is the cause of patient s hyperkalemia? A. Metabolic acidosis B. Insulin deficiency C. Hypertonicity D. B and C E. All of the above

50 Potassium balance _cells _changes in ph

51 Potassium balance _cells Rhabdomyolysis Tumor lysis Dead tissue Treatment of megaloblastic anemia


52 Potassium balance _kidney Glomerulus filters potassium
53 Potassium balance _kidney_distal nephron

54 Potassium balance _kidney_ increased distal flow
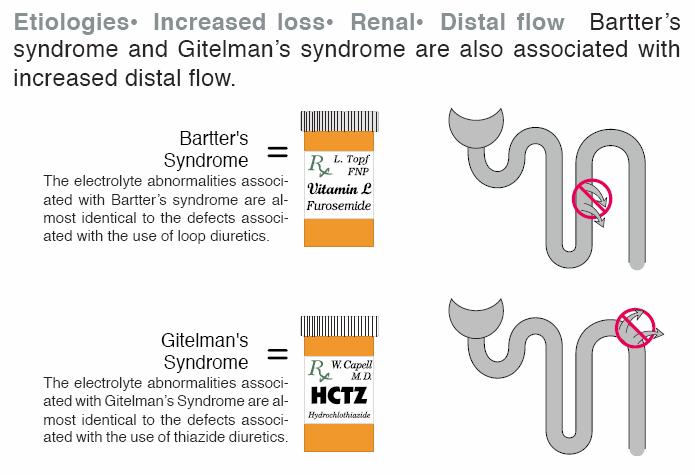
55 Hypokalemia
56 Q4 A 26-year-old Asian male presents to the emergency room with flaccid muscle weakness. He denies diarrhea or vomiting. Na 138 meq/l, 1.8 meq/l, Cl 104 meq/l HCO3 26 meq/l, Glucose 97 mg/dl, BUN12 mg/dl Which of the following would be most appropriate : A. Cl, 200 meq po daily B. Serum thyroid-stimulating hormone level C. Acetazolamide D. None of the above
57 Q4 A 26-year-old Asian male presents to the emergency room with flaccid muscle weakness. He denies diarrhea or vomiting. Na 138 meq/l, 1.8 meq/l, Cl 104 meq/l HCO3 26 meq/l, Glucose 97 mg/dl, BUN12 mg/dl Which of the following would be most appropriate : A. Cl, 200 meq po daily B. Serum thyroid-stimulating hormone level C. Acetazolamide D. None of the above
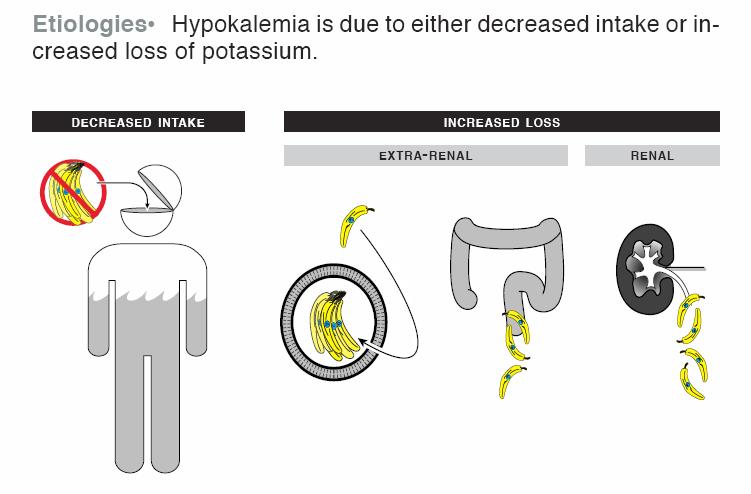
58 Hypokalemia
59 Hypokalemia
60 Case 1 32 year old wf w h/o GI motility disorder s/p multiple surgeries, with short bowel syndrome Has h/o hypokalemia with low-normal BP, carries diagnosis of Bartter s syndrome from outside institution Presented to ED c/o abdominal pain
61 Case 1 Labs: > Patient admitted to floor w tele

62 EG 1 Case 1

63 EG 2 Case 1
64 Case 1 Labs 5 days later. Still with nausea, diarrhea, requiring TPN U 222, U Na 83

65 EG 3 Case 1
66 Case 1 Labs in 2011: U 163, U Na 23 Plasma aldosterone 250 Labs in 2009 (had ileostomy at that time): U Cl <15, U Na <10, U 107

67 Hypokalemia Ethiologies_increased loss_renal_non-reabsorbable anions_hypokalemia in vomiting is due to renal loss of
68 Hypokalemia Cl HCO 3 - Na +
69 Case 2 47 yo bf w h/o HTN since age 20 and chronic hypokalemia (on thiazide), as well as DMII and mild obesity. She was seen in renal clinic in 2004, BP 160/100 BMP Plasma aldosterone 12, plasma renin <0.15 (PA/PRA >80) Started on eplerenone, but later lost to renal f/u
70 Case 2 I saw patient in 2010, at that time BP 170/91 on eplerenone 25, chlorthalidone 25, lisinopril 40, atenolol 50 and amlodipine 10. She is also on Cl 40 bid Labs: Plasma aldosterone 34, plasma renin 0.4 (PA/PRA 85)
71 Case 2 Inspra increased to 50 mg and chlorthalidone changed to maxzide (triamterene/hctz) F/u BP 120/80 and labs: In 2012 pt developed worsening glycemic control (A1C 8) Is her metabolic syndrome worsened by aldosterone excess?
72 Case 2 Decision to pursue hyperaldosteronism w/u: Abd CT showed a Rt adrenal adenoma Adrenal Vein Sampling lateralized overproduction of aldosterone to Rt adrenal Pt underwent Rt adrenalectomy
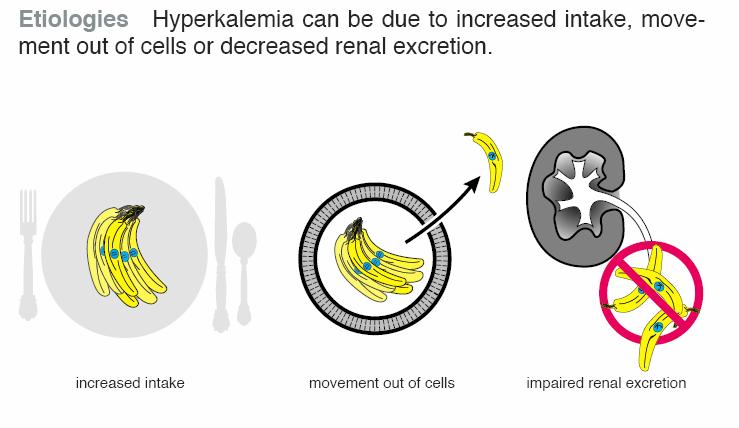
73 Case 2 After adrenalectomy, hypertension controlled on 3 meds: atenolol, lisinopril and chlorthalidone A1C down to 6
74 Hypokalemia Ethiologies_increased loss_renal_hypomagnesemia

75 Hypokalemia Ethiologies_increased loss_renal_hypomagnesemia Mg 2+
76 Hypokalemia
77 Hypokalemia
78 Hypokalemia
79 Hypokalemia

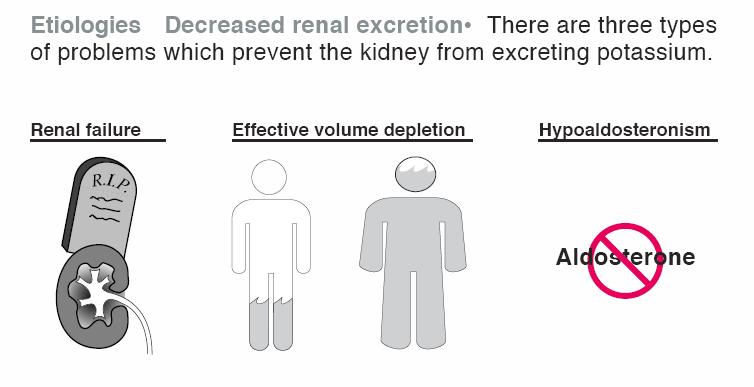
80 Hyperkalemia
81 Hyperkalemia
82 Hyperkalemia

83 Hyperkalemia: high diet
84 Hyperkalemia
85 Hyperkalemia
86 Hyperkalemia Cyclosporine, Tacrolimus Heparin
87 Hyperkalemia
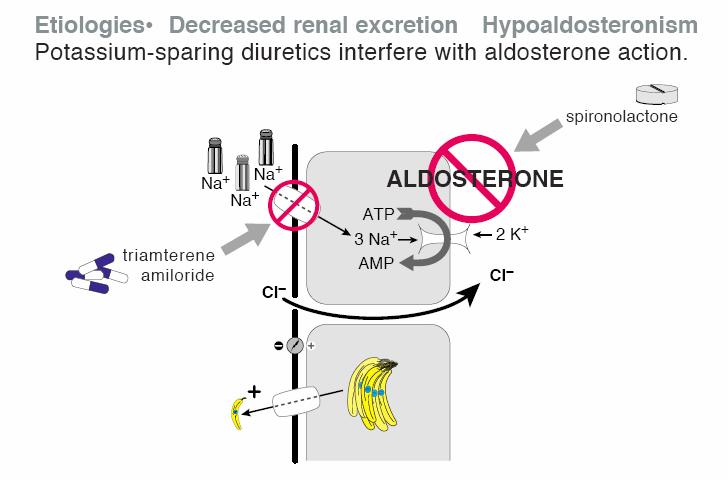
88 Hyperkalemia eplerenone
89 Q5 A 39-year-old male with AIDS is admitted with pneumocystis pneumonia and treated with prednisone and intravenous trimethoprim-sulfamethoxazole. On examination, BP is 125/77, HR 98, RR 22. He appears tachypneic with diffuse rales on chest auscultation. Laboratory Studies Na 138 meq/l, 6.0 meq/l, Cl 99 meq/l HCO3 28 meq/l, BUN 10 mg/dl, Scr 0.9 mg/dl Which of the following would be the most appropriate: A. Discontinue trimethoprim-sulfamethoxazole and start pentamidine B. Discontinue trimethoprim-sulfamethoxazole and start atovaquone C. Fludrocortisone D. Sodium bicarbonate
90 Q5 A 39-year-old male with AIDS is admitted with pneumocystis pneumonia and treated with prednisone and intravenous trimethoprim-sulfamethoxazole. On examination, BP is 125/77, HR 98, RR 22. He appears tachypneic with diffuse rales on chest auscultation. Laboratory Studies Na 138 meq/l, 6.0 meq/l, Cl 99 meq/l HCO3 28 meq/l, BUN 10 mg/dl, Scr 0.9 mg/dl Which of the following would be the most appropriate: A. Discontinue trimethoprim-sulfamethoxazole and start pentamidine B. Discontinue trimethoprim-sulfamethoxazole and start atovaquone C. Fludrocortisone D. Sodium bicarbonate
91 Treatment of hyperkalemia

92 Treatment of hyperkalemia

93 Treatment of hyperkalemia
94 Hyperkalemia Depolarization
95 Hyperkalemia IV Ca raises threshold potential Depolarization
96 Q6 A 57-year-old female with ESRD secondary to diabetic nephropathy maintained on chronic hemodialysis is seen on a non-dialysis day. Na 134 meq/l, 7.3 meq/l, Cl 102 meq/l HCO3 19 meq/l, BUN 22 mg/dl, Cr 6 mg/dl All of the following would lower the serum potassium EXCEPT: A. Insulin and glucose B. Albuterol C. Sodium bicarbonate D. Sodium polystyrene sulfonate E. Hemodialysis
97 Q6 A 57-year-old female with ESRD secondary to diabetic nephropathy maintained on chronic hemodialysis is seen on a non-dialysis day. Na 134 meq/l, 7.3 meq/l, Cl 102 meq/l HCO3 19 meq/l, BUN 22 mg/dl, Cr 6 mg/dl All of the following would lower the serum potassium EXCEPT: A. Insulin and glucose B. Albuterol C. Sodium bicarbonate D. Sodium polystyrene sulfonate E. Hemodialysis
98 Treatment of hyperkalemia

99 Treatment of hyperkalemia

100 Treatment of hyperkalemia
Normal range of serum potassium is meq/l true hyperkalemia manifests clinically as : Clinical presentation : muscle and cardiac dysfunction
 Potassium Disorders hyperkalemia Potassium is mainly an cation? What is the major physiological role of potassium in the body? What is the major regulatory system of serum potassium level? Which part of
Potassium Disorders hyperkalemia Potassium is mainly an cation? What is the major physiological role of potassium in the body? What is the major regulatory system of serum potassium level? Which part of
A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY
 A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY Case 57 y.o. male CC: Weakness HPI: About 20 years ago, he developed bilateral lower extremity weakness. Laboratory
A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY Case 57 y.o. male CC: Weakness HPI: About 20 years ago, he developed bilateral lower extremity weakness. Laboratory
Electrolyte Imbalance and Resuscitation. Dr. Mehmet Okumuş Sütçü Imam University Faculty of Medicine Department of Emergency Medicine
 Electrolyte Imbalance and Resuscitation Dr. Mehmet Okumuş Sütçü Imam University Faculty of Medicine Department of Emergency Medicine Presentation plan Definition of the electrolyte disturbances Conditions
Electrolyte Imbalance and Resuscitation Dr. Mehmet Okumuş Sütçü Imam University Faculty of Medicine Department of Emergency Medicine Presentation plan Definition of the electrolyte disturbances Conditions
Potassium regulation. -Kidney is a major regulator for potassium Homeostasis.
 Potassium regulation. -Kidney is a major regulator for potassium Homeostasis. Normal potassium intake, distribution, and output from the body. Effects of severe hyperkalemia Partial depolarization of cell
Potassium regulation. -Kidney is a major regulator for potassium Homeostasis. Normal potassium intake, distribution, and output from the body. Effects of severe hyperkalemia Partial depolarization of cell
CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018
 CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018 Case 1 Potassium Clearance A 70 kg male is placed on CVVH with a total ultrafiltration rate (effluent rate) of 20 ml/kg/hr. The Blood Flow
CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018 Case 1 Potassium Clearance A 70 kg male is placed on CVVH with a total ultrafiltration rate (effluent rate) of 20 ml/kg/hr. The Blood Flow
CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018
 CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018 Case 1 Potassium Clearance A 70 kg male is placed on CVVH with a total ultrafiltration rate (effluent rate) of 20 ml/kg/hr. The Blood Flow
CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018 Case 1 Potassium Clearance A 70 kg male is placed on CVVH with a total ultrafiltration rate (effluent rate) of 20 ml/kg/hr. The Blood Flow
Clinical Pearls in Renal Medicine
 Clinical Pearls in Renal Medicine Joel A. Gordon MD Professor of Medicine Nephrology Division Staff Physician Kidney Disease and Blood Pressure Clinic Disclosures None of my financial holdings will have
Clinical Pearls in Renal Medicine Joel A. Gordon MD Professor of Medicine Nephrology Division Staff Physician Kidney Disease and Blood Pressure Clinic Disclosures None of my financial holdings will have
Diseases of the Adrenal gland
 Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
DIABETIC KETOACIDOSIS (DKA) K E M I A D E Y E R I, P G Y - 1
 K E M I A D E Y E R I, P G Y - 1") DIABETIC KETOACIDOSIS (DKA) K E M I A D E Y E R I, P G Y - 1 QUESTION # 1 7 year old boy comes to the ER with a 2 week history of abdominal pain and weight loss. Further history reveals polyuria and polydipsia,
DIABETIC KETOACIDOSIS (DKA) K E M I A D E Y E R I, P G Y - 1 QUESTION # 1 7 year old boy comes to the ER with a 2 week history of abdominal pain and weight loss. Further history reveals polyuria and polydipsia,
Pare. Blalock. Shires. shock caused by circulating toxins treatment with phlebotomy. shock caused by hypovolemia treatment with plasma replacement
 Pare shock caused by circulating toxins treatment with phlebotomy Blalock shock caused by hypovolemia treatment with plasma replacement Shires deficit in functional extracellular volume treatment with
Pare shock caused by circulating toxins treatment with phlebotomy Blalock shock caused by hypovolemia treatment with plasma replacement Shires deficit in functional extracellular volume treatment with
A Mnemonic for the Treatment of Hyperkalemia. Nick Wolters, PGY1 Resident Grandview Medical Center
 A Mnemonic for the Treatment of Hyperkalemia Nick Wolters, PGY1 Resident Grandview Medical Center Hyperkalemia 30 YOF, ESRD, missed 2 dialysis sessions over the last week Potassium level came back at 7
A Mnemonic for the Treatment of Hyperkalemia Nick Wolters, PGY1 Resident Grandview Medical Center Hyperkalemia 30 YOF, ESRD, missed 2 dialysis sessions over the last week Potassium level came back at 7
Hyperkalemia. Katarzyna Bigaj PGY -1
 Hyperkalemia Katarzyna Bigaj PGY -1 Definition Hyperkalaemia is defined as a potassium level > 5.5 meq/l Moderate hyperkalaemia is a serum potassium > 6.0 meq/l Severe hyperkalaemia is a serum potassium
Hyperkalemia Katarzyna Bigaj PGY -1 Definition Hyperkalaemia is defined as a potassium level > 5.5 meq/l Moderate hyperkalaemia is a serum potassium > 6.0 meq/l Severe hyperkalaemia is a serum potassium
Anna Vinnikova, M.D. Division of Nephrology Virginia Commonwealth University
 Metabolic Acidosis Anna Vinnikova, M.D. Division of Nephrology Virginia Commonwealth University Graphics by permission from The Fluid, Electrolyte and Acid-Base Companion, S. Faubel and J. Topf, http://www.pbfluids.com
Metabolic Acidosis Anna Vinnikova, M.D. Division of Nephrology Virginia Commonwealth University Graphics by permission from The Fluid, Electrolyte and Acid-Base Companion, S. Faubel and J. Topf, http://www.pbfluids.com
Hyperkalemia Protect, Shift, and Eliminate
 Disclosure Michael C. Thomas reports no relevant financial relationships. Lytes Off in Vegas! The Acute Management of Potassium and Calcium Disorders Program Objectives Design a plan to replace and monitor
Disclosure Michael C. Thomas reports no relevant financial relationships. Lytes Off in Vegas! The Acute Management of Potassium and Calcium Disorders Program Objectives Design a plan to replace and monitor
Basic Fluid and Electrolytes
 Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
Endocrine. Endocrine as it relates to the kidney. Sarah Elfering, MD University of Minnesota
 Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
WATER, SODIUM AND POTASSIUM
 WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
PP-US-DSE Relypsa, Inc. All rights reserved. Relypsa and the Relypsa logo are trademarks of Relypsa, Inc.
 1 2 There are 4 main objectives that I d like to cover with you today: First, to review the definition, prevalence, and risk of hyperkalemia in certain populations Second, to review why RAASi are recommended
1 2 There are 4 main objectives that I d like to cover with you today: First, to review the definition, prevalence, and risk of hyperkalemia in certain populations Second, to review why RAASi are recommended
Instrumental determination of electrolytes in urine. Amal Alamri
 Instrumental determination of electrolytes in urine Amal Alamri What is the Electrolytes? Electrolytes are positively and negatively chargedions, Found in Within body's cells extracellular fluids, including
Instrumental determination of electrolytes in urine Amal Alamri What is the Electrolytes? Electrolytes are positively and negatively chargedions, Found in Within body's cells extracellular fluids, including
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance
 Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Conflict of interest
 Hyperkalemia in Heart and Kidney patients: Rescue is here Wajeh Qunibi, MD, FACP Professor of Medicine University of Texas Health Science Center San Antonio, TX CARDIORENAL CONNECTION April 28, 2017 Conflict
Hyperkalemia in Heart and Kidney patients: Rescue is here Wajeh Qunibi, MD, FACP Professor of Medicine University of Texas Health Science Center San Antonio, TX CARDIORENAL CONNECTION April 28, 2017 Conflict
How to approach resistant hypertension. Teh-Li Huo, M.D., Ph.D.
 How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
Chapter 27: WATER, ELECTROLYTES, AND ACID-BASE BALANCE
 Chapter 27: WATER, ELECTROLYTES, AND ACID-BASE BALANCE I. RELATED TOPICS Integumentary system Cerebrospinal fluid Aqueous humor Digestive juices Feces Capillary dynamics Lymph circulation Edema Osmosis
Chapter 27: WATER, ELECTROLYTES, AND ACID-BASE BALANCE I. RELATED TOPICS Integumentary system Cerebrospinal fluid Aqueous humor Digestive juices Feces Capillary dynamics Lymph circulation Edema Osmosis
K+ Ann Crawford, RN, PhD, CNS, CEN
 Hyperkalemia: Management of a Critical Electrolyte Disturbance K+ Ann Crawford, RN, PhD, CNS, CEN Balancing Fluid Intracellular fluid (ICF) Extracellular fluid (ECF) Intravascular interstitial Hormonal
Hyperkalemia: Management of a Critical Electrolyte Disturbance K+ Ann Crawford, RN, PhD, CNS, CEN Balancing Fluid Intracellular fluid (ICF) Extracellular fluid (ECF) Intravascular interstitial Hormonal
FLUIDS/ELECTROLYTES. Sahir Kalim, MD MMSc. Department of Medicine, Division of Nephrology, Massachusetts General Hospital Harvard Medical School
 FLUIDS/ELECTROLYTES Sahir Kalim, MD MMSc Department of Medicine, Division of Nephrology, Massachusetts General Hospital Harvard Medical School Dr. Kalim has no potential conflicts of interest to disclose.
FLUIDS/ELECTROLYTES Sahir Kalim, MD MMSc Department of Medicine, Division of Nephrology, Massachusetts General Hospital Harvard Medical School Dr. Kalim has no potential conflicts of interest to disclose.
Virtual Mentor American Medical Association Journal of Ethics April 2007, Volume 9, Number 4:
 Virtual Mentor American Medical Association Journal of Ethics April 2007, Volume 9, Number 4: 295-299. Clinical pearl Hyperkalemia: newer considerations by Amar D. Bansal and David S. Goldfarb, MD Maintenance
Virtual Mentor American Medical Association Journal of Ethics April 2007, Volume 9, Number 4: 295-299. Clinical pearl Hyperkalemia: newer considerations by Amar D. Bansal and David S. Goldfarb, MD Maintenance
Potassium secretion. E k = -61 log ([k] inside / [k] outside).
![Potassium secretion. E k = -61 log ([k] inside / [k] outside).](/thumbs/80/80478709.jpg "Potassium secretion. E k = -61 log ([k] inside / [k] outside).") 1 Potassium secretion In this sheet, we will continue talking about ultrafiltration in kidney but with different substance which is K+. Here are some informations that you should know about potassium;
1 Potassium secretion In this sheet, we will continue talking about ultrafiltration in kidney but with different substance which is K+. Here are some informations that you should know about potassium;
THE HYPERKALEMIC SYNDROMES
 THE HYPERKALEMIC SYNDROMES K + BALANCE Cells (3400 meq) ECF (60 meq) External K Pump insulin catechols Na intake Leak K ph; osmolality membrane integrity distal Na + renal { delivery output aldosterone
THE HYPERKALEMIC SYNDROMES K + BALANCE Cells (3400 meq) ECF (60 meq) External K Pump insulin catechols Na intake Leak K ph; osmolality membrane integrity distal Na + renal { delivery output aldosterone
Therapeutic Challenges in CKD & ESRD: Managing Acid-base & electrolytes. No financial disclosure
 Therapeutic Challenges in CKD & ESRD: Managing Acid-base & electrolytes Qi Qian, MD, FASN Mayo Clinic, College of Medicine No financial disclosure 2016 MFMER 3563115-1 ü - ü - 1. Acidosis 2. Hyperkalemia
Therapeutic Challenges in CKD & ESRD: Managing Acid-base & electrolytes Qi Qian, MD, FASN Mayo Clinic, College of Medicine No financial disclosure 2016 MFMER 3563115-1 ü - ü - 1. Acidosis 2. Hyperkalemia
NORMAL POTASSIUM DISTRIBUTION AND BALANCE
 NORMAL POTASSIUM DISTRIBUTION AND BALANCE 98% of body potassium is contained within cells, principally muscle cells, and is readily exchangeable. Only 2% is in ECF. Daily intake exceeds the amount in ECF.
NORMAL POTASSIUM DISTRIBUTION AND BALANCE 98% of body potassium is contained within cells, principally muscle cells, and is readily exchangeable. Only 2% is in ECF. Daily intake exceeds the amount in ECF.
Chapter 21. Diuretic Agents. Mosby items and derived items 2008, 2002 by Mosby, Inc., an affiliate of Elsevier Inc.
 Chapter 21 Diuretic Agents Renal Structure and Function Kidneys at level of umbilicus Each weighs 160 to 175 g and is 10 to 12 cm long Most blood flow per gram of weight in body 22% of cardiac output (CO)
Chapter 21 Diuretic Agents Renal Structure and Function Kidneys at level of umbilicus Each weighs 160 to 175 g and is 10 to 12 cm long Most blood flow per gram of weight in body 22% of cardiac output (CO)
Water, Electrolytes, and Acid-Base Balance
 Chapter 27 Water, Electrolytes, and Acid-Base Balance 1 Body Fluids Intracellular fluid compartment All fluids inside cells of body About 40% of total body weight Extracellular fluid compartment All fluids
Chapter 27 Water, Electrolytes, and Acid-Base Balance 1 Body Fluids Intracellular fluid compartment All fluids inside cells of body About 40% of total body weight Extracellular fluid compartment All fluids
PMH: DM HTN Colon cancer s/p left hemicolectomy, chemo Now with mets to liver and peritoneum. Restarted on chemo 2/4/13 oxaliplatin, cepecitabine
 3.5.2013 75 y.o M with PMH of HTN, DM II with nephropathy, CKD stage III(b/l cr 1.5), colon cancer s/p hemicolectomy (8/2011) now with recurrence and mets to liver and peritoneum undergoing chemo at woodhull,
3.5.2013 75 y.o M with PMH of HTN, DM II with nephropathy, CKD stage III(b/l cr 1.5), colon cancer s/p hemicolectomy (8/2011) now with recurrence and mets to liver and peritoneum undergoing chemo at woodhull,
CALCINEURIN INHIBITORS AND HYPERKALEMIA. Sheena Surindran, MD 3/22/2011
 CALCINEURIN INHIBITORS AND HYPERKALEMIA Sheena Surindran, MD 3/22/2011 DISTAL TUBULE K SECRETION EFFECTS OF CYCLOSPORINE ON RAS AND POTASSIUM EXCRETION 10 pts on CsA and prednisone / 10 on AZT and prednisone
CALCINEURIN INHIBITORS AND HYPERKALEMIA Sheena Surindran, MD 3/22/2011 DISTAL TUBULE K SECRETION EFFECTS OF CYCLOSPORINE ON RAS AND POTASSIUM EXCRETION 10 pts on CsA and prednisone / 10 on AZT and prednisone
Definition : Stages : ( RIFLE vs. AKIN ) Causes and classification : Pre-renal Renal Post- renal Clinical manifestations and Complication Management
 Causes and classification : Pre-renal Renal Post- renal Clinical manifestations and Complication Management") AKI Definition : Stages : ( RIFLE vs. AKIN ) Causes and classification : Pre-renal Renal Post- renal Clinical manifestations and Complication Management and indications for RRT Etiology prerenal causes
AKI Definition : Stages : ( RIFLE vs. AKIN ) Causes and classification : Pre-renal Renal Post- renal Clinical manifestations and Complication Management and indications for RRT Etiology prerenal causes
Low Efficacy Diuretics. Potassium sparing diuretics. Carbonic anhydrase inhibitors. Osmotic diuretics. Miscellaneous
 University of Al Qadisiyah College of Pharmacy Dr. Bassim I Mohammad, MBChB, MSc, Ph.D Low Efficacy Diuretics 1. Potassium sparing diuretics 2. Carbonic anhydrase inhibitors 3. Osmotic diuretics 4. Miscellaneous
University of Al Qadisiyah College of Pharmacy Dr. Bassim I Mohammad, MBChB, MSc, Ph.D Low Efficacy Diuretics 1. Potassium sparing diuretics 2. Carbonic anhydrase inhibitors 3. Osmotic diuretics 4. Miscellaneous
Hypokalemia. Etiology of hypokalemia
 Hypokalemia The total body K+ storage: 50~55 meq/kg ( approximately 3000~4000 meq) 98% of the body K+ is located in the cells The net effect is that [K+c] is about 140 meq/l and [K+e] is only 4~5 meq/l
Hypokalemia The total body K+ storage: 50~55 meq/kg ( approximately 3000~4000 meq) 98% of the body K+ is located in the cells The net effect is that [K+c] is about 140 meq/l and [K+e] is only 4~5 meq/l
CCRN Review - Renal. CCRN Review - Renal 10/16/2014. CCRN Review Renal. Sodium Critical Value < 120 meq/l > 160 meq/l
 CCRN Review Renal Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Sodium 136-145 Critical Value < 120 meq/l > 160 meq/l Sodium Etiology
CCRN Review Renal Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Sodium 136-145 Critical Value < 120 meq/l > 160 meq/l Sodium Etiology
Electrolytes and other equally exciting topics
 Electrolytes and other equally exciting topics Rebecca A. Snyder Summer School 2010 Why do we care? Why do we care? Why do we care? Torsades is bad. Because medical records cares even more. Because apparently
Electrolytes and other equally exciting topics Rebecca A. Snyder Summer School 2010 Why do we care? Why do we care? Why do we care? Torsades is bad. Because medical records cares even more. Because apparently
Hypertension Pharmacotherapy: A Practical Approach
 Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Renal Physiology Part II. Bio 219 Napa Valley College Dr. Adam Ross
 Renal Physiology Part II Bio 219 Napa Valley College Dr. Adam Ross Fluid and Electrolyte balance As we know from our previous studies: Water and ions need to be balanced in order to maintain proper homeostatic
Renal Physiology Part II Bio 219 Napa Valley College Dr. Adam Ross Fluid and Electrolyte balance As we know from our previous studies: Water and ions need to be balanced in order to maintain proper homeostatic
Fluid and electrolyte balance, imbalance
 Fluid and electrolyte balance, imbalance Body fluid The fluids are distributed throughout the body in various compartments. Body fluid is composed primarily of water Water is the solvent in which all solutes
Fluid and electrolyte balance, imbalance Body fluid The fluids are distributed throughout the body in various compartments. Body fluid is composed primarily of water Water is the solvent in which all solutes
HYPERKALEMIA. Best Practices in Managing. in Chronic Kidney Disease
 + Best Practices in Managing HYPERKALEMIA in Chronic Kidney Disease Hyperkalemia in Chronic Kidney Disease (CKD) Treatment with RAAS Inhibitors (RAASi) in CKD Diagnosis and Evaluation of Hyperkalemia Treatment
+ Best Practices in Managing HYPERKALEMIA in Chronic Kidney Disease Hyperkalemia in Chronic Kidney Disease (CKD) Treatment with RAAS Inhibitors (RAASi) in CKD Diagnosis and Evaluation of Hyperkalemia Treatment
Potassium as a Treatable Biomarker in Cardiovascular Disease: New Keys to Hyperkalemia
 Potassium as a Treatable Biomarker in Cardiovascular Disease: New Keys to Hyperkalemia Nicholas Wettersten, MD Associate Professor Heart Failure, Mechanical Circulatory Support and Transplant March 1 st,
Potassium as a Treatable Biomarker in Cardiovascular Disease: New Keys to Hyperkalemia Nicholas Wettersten, MD Associate Professor Heart Failure, Mechanical Circulatory Support and Transplant March 1 st,
Saint-Antoine Hospital, Paris. Medical Intensive Unit Care. Hafid Ait-Oufella, MD.PhD. Dyscalcemia. Dyskalemia
 Dyskalemia Dyscalcemia Hafid Ait-Oufella, MD.PhD. Medical Intensive Unit Care Saint-Antoine Hospital, Paris Potassium K + Molecular weight: 39 1gr K + =2.5mmol Potassium disorders in ICU : Our experience
Dyskalemia Dyscalcemia Hafid Ait-Oufella, MD.PhD. Medical Intensive Unit Care Saint-Antoine Hospital, Paris Potassium K + Molecular weight: 39 1gr K + =2.5mmol Potassium disorders in ICU : Our experience
PRINCIPLES OF DIURETIC ACTIONS:
 DIURETIC: A drug that increases excretion of solutes Increased urine volume is secondary All clinically useful diuretics act by blocking Na + reabsorption Has the highest EC to IC ratio = always more sodium
DIURETIC: A drug that increases excretion of solutes Increased urine volume is secondary All clinically useful diuretics act by blocking Na + reabsorption Has the highest EC to IC ratio = always more sodium
Calcium (Ca 2+ ) mg/dl
 mg/dl") Quick Guide to Laboratory Values Use this handy cheat-sheet to help you monitor laboratory values related to fluid and electrolyte status. Remember, normal values may vary according to techniques used
Quick Guide to Laboratory Values Use this handy cheat-sheet to help you monitor laboratory values related to fluid and electrolyte status. Remember, normal values may vary according to techniques used
Na concentration in the extracellular compartment is 140
 هللامسب Na regulation: Na concentration in the extracellular compartment is 140 meq\l. Na is important because: -It determines the volume of extracellular fluid : the more Na intake will expand extracellular
هللامسب Na regulation: Na concentration in the extracellular compartment is 140 meq\l. Na is important because: -It determines the volume of extracellular fluid : the more Na intake will expand extracellular
Acid-base balance is one of the most important of the body s homeostatic mechanisms Acid-base balance refers to regulation of hydrogen ion (H + )
") Acid-base balance is one of the most important of the body s homeostatic mechanisms Acid-base balance refers to regulation of hydrogen ion (H + ) concentration in body fluids Precise regulation of ph at
Acid-base balance is one of the most important of the body s homeostatic mechanisms Acid-base balance refers to regulation of hydrogen ion (H + ) concentration in body fluids Precise regulation of ph at
Acid-Base Balance 11/18/2011. Regulation of Potassium Balance. Regulation of Potassium Balance. Regulatory Site: Cortical Collecting Ducts.
 Influence of Other Hormones on Sodium Balance Acid-Base Balance Estrogens: Enhance NaCl reabsorption by renal tubules May cause water retention during menstrual cycles Are responsible for edema during
Influence of Other Hormones on Sodium Balance Acid-Base Balance Estrogens: Enhance NaCl reabsorption by renal tubules May cause water retention during menstrual cycles Are responsible for edema during
Nephrology / Urology. Hyperkalemia Causes and Definition Lecturio Online Medical Library. Definition. Epidemiology of Hyperkalemia.
 Nephrology / Urology Hyperkalemia Causes and Definition Lecturio Online Medical Library See online here Hyperkalemia is defined by the serum potassium level when it is higher than 5.5mEq/L. It is usually
Nephrology / Urology Hyperkalemia Causes and Definition Lecturio Online Medical Library See online here Hyperkalemia is defined by the serum potassium level when it is higher than 5.5mEq/L. It is usually
Major intra and extracellular ions Lec: 1
 Major intra and extracellular ions Lec: 1 The body fluids are solutions of inorganic and organic solutes. The concentration balance of the various components is maintained in order for the cell and tissue
Major intra and extracellular ions Lec: 1 The body fluids are solutions of inorganic and organic solutes. The concentration balance of the various components is maintained in order for the cell and tissue
BIOL 2402 Fluid/Electrolyte Regulation
 Dr. Chris Doumen Collin County Community College BIOL 2402 Fluid/Electrolyte Regulation 1 Body Water Content On average, we are 50-60 % water For a 70 kg male = 40 liters water This water is divided into
Dr. Chris Doumen Collin County Community College BIOL 2402 Fluid/Electrolyte Regulation 1 Body Water Content On average, we are 50-60 % water For a 70 kg male = 40 liters water This water is divided into
There are many buffers in the kidney, but the main one is the phosphate buffer.
 9 Yanal Obada Zalat Renal Control of AcidBase Balance The kidneys play three major roles in the maintenance of normal acidbase balance: 1excretion of H+ (fixed _non volatile H+) 2Reabsorption of filtrated
9 Yanal Obada Zalat Renal Control of AcidBase Balance The kidneys play three major roles in the maintenance of normal acidbase balance: 1excretion of H+ (fixed _non volatile H+) 2Reabsorption of filtrated
Diuretics (Saluretics)
") Diuretics (Saluretics) Diuretics increase urine excretion mainly by reabsorption of salts and water from kidney tubules These agents are ion transport inhibitors that decrease the reabsorption of Na+ at
Diuretics (Saluretics) Diuretics increase urine excretion mainly by reabsorption of salts and water from kidney tubules These agents are ion transport inhibitors that decrease the reabsorption of Na+ at
Management of Acute Kidney Injury in the Neonate. Carolyn Abitbol, M.D. University of Miami Miller School of Medicine / Holtz Children s Hospital
 Management of Acute Kidney Injury in the Neonate Carolyn Abitbol, M.D. University of Miami Miller School of Medicine / Holtz Children s Hospital Objectives Summarize the dilemmas in diagnosing & recognizing
Management of Acute Kidney Injury in the Neonate Carolyn Abitbol, M.D. University of Miami Miller School of Medicine / Holtz Children s Hospital Objectives Summarize the dilemmas in diagnosing & recognizing
Therapeutics of Diuretics
 (Last Updated: 08/22/2018) Created by: Socco, Samantha Therapeutics of Diuretics Thambi, M. (2017). The Clinical Use of Diuretics. Lecture presented at PHAR 503 Lecture in UIC College of Pharmacy, Chicago.
(Last Updated: 08/22/2018) Created by: Socco, Samantha Therapeutics of Diuretics Thambi, M. (2017). The Clinical Use of Diuretics. Lecture presented at PHAR 503 Lecture in UIC College of Pharmacy, Chicago.
Chapter 19 The Urinary System Fluid and Electrolyte Balance
 Chapter 19 The Urinary System Fluid and Electrolyte Balance Chapter Outline The Concept of Balance Water Balance Sodium Balance Potassium Balance Calcium Balance Interactions between Fluid and Electrolyte
Chapter 19 The Urinary System Fluid and Electrolyte Balance Chapter Outline The Concept of Balance Water Balance Sodium Balance Potassium Balance Calcium Balance Interactions between Fluid and Electrolyte
Acid-Base Balance Dr. Gary Mumaugh
 Acid-Base Balance Dr. Gary Mumaugh Introduction Acid-base balance is one of the most important of the body s homeostatic mechanisms Acid-base balance refers to regulation of hydrogen ion (H + ) concentration
Acid-Base Balance Dr. Gary Mumaugh Introduction Acid-base balance is one of the most important of the body s homeostatic mechanisms Acid-base balance refers to regulation of hydrogen ion (H + ) concentration
Complications of Acute and Chronic Kidney Disease: A Focus on Hyperkalemia. Mitchell H. Rosner, MD James Tumlin, MD Peter A. McCullough, MD, MPH
 Complications of Acute and Chronic Kidney Disease: A Focus on Hyperkalemia Mitchell H. Rosner, MD James Tumlin, MD Peter A. McCullough, MD, MPH Case #1 A 29 year-old male with ESRD secondary to focal segmental
Complications of Acute and Chronic Kidney Disease: A Focus on Hyperkalemia Mitchell H. Rosner, MD James Tumlin, MD Peter A. McCullough, MD, MPH Case #1 A 29 year-old male with ESRD secondary to focal segmental
Drug-Induced Diabetes May Not Be Harmful But Should Be Prevented. Jeffrey A. Cutler, MD, MPH
 Drug-Induced Diabetes May Not Be Harmful But Should Be Prevented Jeffrey A. Cutler, MD, MPH Overview Focus on thiazide-like diuretics (not BB) Diuretic-induced versus diureticassociated diabetes Role of
Drug-Induced Diabetes May Not Be Harmful But Should Be Prevented Jeffrey A. Cutler, MD, MPH Overview Focus on thiazide-like diuretics (not BB) Diuretic-induced versus diureticassociated diabetes Role of
Potassium, Aldosterone, and Hypertension: How Physiology Determines Treatment. Jamie Johnston, MD University of Pittsburgh School of Medicine
 Potassium, Aldosterone, and Hypertension: How Physiology Determines Treatment Jamie Johnston, MD University of Pittsburgh School of Medicine No Disclosures Acknowledgements: Evan Ray, MD, PhD Objectives
Potassium, Aldosterone, and Hypertension: How Physiology Determines Treatment Jamie Johnston, MD University of Pittsburgh School of Medicine No Disclosures Acknowledgements: Evan Ray, MD, PhD Objectives
Fundamentals of Pharmacology for Veterinary Technicians Chapter 8
 Figure 8-1 Figure 8-2 Figure 8-3 Figure 8-4 Figure 8-5 Figure 8-7 Figure 8-8 Figure 8-9 TABLE 8-1 Blood Flow Through the Heart The right atrium receives blood from all tissues, except the lungs, through
Figure 8-1 Figure 8-2 Figure 8-3 Figure 8-4 Figure 8-5 Figure 8-7 Figure 8-8 Figure 8-9 TABLE 8-1 Blood Flow Through the Heart The right atrium receives blood from all tissues, except the lungs, through
Hyponatremia and Hypokalemia
 Hyponatremia and Hypokalemia Critical Care in the ED March 21 st, 2019 Hannah Ferenchick, MD 1 No financial disclosures 2 1 Outline: 1. Hyponatremia Diagnosis Initial treatment 2. Hyperkalemia Diagnosis
Hyponatremia and Hypokalemia Critical Care in the ED March 21 st, 2019 Hannah Ferenchick, MD 1 No financial disclosures 2 1 Outline: 1. Hyponatremia Diagnosis Initial treatment 2. Hyperkalemia Diagnosis
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES
 Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Hyperaldosteronism: Conn's Syndrome
 RENAL AND ACID-BASE PHYSIOLOGY 177 Case 31 Hyperaldosteronism: Conn's Syndrome Seymour Simon is a 54-year-old college physics professor who maintains a healthy lifestyle. He exercises regularly, doesn't
RENAL AND ACID-BASE PHYSIOLOGY 177 Case 31 Hyperaldosteronism: Conn's Syndrome Seymour Simon is a 54-year-old college physics professor who maintains a healthy lifestyle. He exercises regularly, doesn't
Hyperkalemia a silent killer? PD Dr. med. Andreas Kistler Kantonsspital Frauenfeld
 Hyperkalemia a silent killer? PD Dr. med. Andreas Kistler Kantonsspital Frauenfeld andreas.kistler@stgag.ch www.nephrologie-thurgau.ch Mr. Hyper K. Lemia charged with serial murder Bild entfernt (copyright)
Hyperkalemia a silent killer? PD Dr. med. Andreas Kistler Kantonsspital Frauenfeld andreas.kistler@stgag.ch www.nephrologie-thurgau.ch Mr. Hyper K. Lemia charged with serial murder Bild entfernt (copyright)
Secondary Hypertension: A Real World Approach
 Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
Acid/Base Disorders 2015
 Objectives - 2 1. Identify acid/base disorders 2. Discuss etiologies for 1 0 acid/base disorders (will not include mixed disorders) 3. Interpret acid/base disorders by interpreting arterial blood gas &
Objectives - 2 1. Identify acid/base disorders 2. Discuss etiologies for 1 0 acid/base disorders (will not include mixed disorders) 3. Interpret acid/base disorders by interpreting arterial blood gas &
Heart failure. Failure? blood supply insufficient for body needs. CHF = congestive heart failure. increased blood volume, interstitial fluid
 Failure? blood supply insufficient for body needs CHF = congestive heart failure increased blood volume, interstitial fluid Underlying causes/risk factors Ischemic heart disease (CAD) 70% hypertension
Failure? blood supply insufficient for body needs CHF = congestive heart failure increased blood volume, interstitial fluid Underlying causes/risk factors Ischemic heart disease (CAD) 70% hypertension
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Stages of Chronic Kidney Disease (CKD)
") Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
ELECTROLYTES RENAL SHO TEACHING
 ELECTROLYTES RENAL SHO TEACHING Metabolic Alkalosis 2 factors are responsible for generation and maintenance of metabolic alkalosis this includes a process that raises serum bicarbonate and a process that
ELECTROLYTES RENAL SHO TEACHING Metabolic Alkalosis 2 factors are responsible for generation and maintenance of metabolic alkalosis this includes a process that raises serum bicarbonate and a process that
Homeostatic Regulation
 Homeostatic Regulation A hormone is :a Water-soluble hormones: Composed of amino acids and bind a receptor protein on the of the target cell. This starts a signal cascade inside the cell and the signal
Homeostatic Regulation A hormone is :a Water-soluble hormones: Composed of amino acids and bind a receptor protein on the of the target cell. This starts a signal cascade inside the cell and the signal
Hello, and thank you for joining us for this presentation on novel approaches to understanding risks and treatment of hyperkalemia.
 Hello, and thank you for joining us for this presentation on novel approaches to understanding risks and treatment of hyperkalemia. PP-US-DSE-00032. 2015 Relypsa, Inc. All rights reserved. Relypsa and
Hello, and thank you for joining us for this presentation on novel approaches to understanding risks and treatment of hyperkalemia. PP-US-DSE-00032. 2015 Relypsa, Inc. All rights reserved. Relypsa and
CSI (Clinical Scenario Investigation): Hyperkalemia
: Hyperkalemia") CSI (Clinical Scenario Investigation): Hyperkalemia Alison Thomas, RN(EC), MN, CNeph(C) Ann Jones, RN(EC), MSN, CNeph(C) Joyce Hunter, RN, Vascular Access Co-ordinator Simcoe Muskoka Regional Kidney Care
CSI (Clinical Scenario Investigation): Hyperkalemia Alison Thomas, RN(EC), MN, CNeph(C) Ann Jones, RN(EC), MSN, CNeph(C) Joyce Hunter, RN, Vascular Access Co-ordinator Simcoe Muskoka Regional Kidney Care
ACID-BASE BALANCE URINE BLOOD AIR
 ACIDBASE BALANCE URINE BLOOD AIR H 2 PO 4 NH 4 HCO 3 KIDNEY H H HCO 3 CELLS Hb H LUNG H 2 CO 3 HHb CO 2 H 2 O ph = 7.4 [HCO 3 ] = 24 meq/l PCO 2 = 40 mm Hg CO 2 PRIMARY RENAL MECHANISMS INVOLVED IN ACIDBASE
ACIDBASE BALANCE URINE BLOOD AIR H 2 PO 4 NH 4 HCO 3 KIDNEY H H HCO 3 CELLS Hb H LUNG H 2 CO 3 HHb CO 2 H 2 O ph = 7.4 [HCO 3 ] = 24 meq/l PCO 2 = 40 mm Hg CO 2 PRIMARY RENAL MECHANISMS INVOLVED IN ACIDBASE
Pharmacology I [PHL 313] Diuretics. Dr. Mohammad Nazam Ansari
![Pharmacology I [PHL 313] Diuretics. Dr. Mohammad Nazam Ansari](/thumbs/90/104323364.jpg "Pharmacology I [PHL 313] Diuretics. Dr. Mohammad Nazam Ansari") Pharmacology I [PHL 313] Diuretics Dr. Mohammad Nazam Ansari Renal Pharmacology Kidneys: Each adult kidney weighs 125-170g in males and 115-155g in females, represent 0.5% of total body weight, but receive
Pharmacology I [PHL 313] Diuretics Dr. Mohammad Nazam Ansari Renal Pharmacology Kidneys: Each adult kidney weighs 125-170g in males and 115-155g in females, represent 0.5% of total body weight, but receive
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: Patho Instructor Notes Revised: 11/2013
 Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: Patho Instructor Notes Revised: 11/2013 Cells form 4 basic tissue groups: 1. Epithelial 2. Connective
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: Patho Instructor Notes Revised: 11/2013 Cells form 4 basic tissue groups: 1. Epithelial 2. Connective
InformRx. Managing Chronic Hyperkalemia. By Pam Scandrett, R.Ph. Risks of High Potassium Levels CLINICAL & REGULATORY NEWS BY PHARMERICA
 Managing Chronic Hyperkalemia By Pam Scandrett, R.Ph. CLINICAL & REGULATORY NEWS BY PHARMERICA JAN/FEB 2019 Potassium (K+) is found inside skeletal muscle, liver, and red blood cells. Normal levels of
Managing Chronic Hyperkalemia By Pam Scandrett, R.Ph. CLINICAL & REGULATORY NEWS BY PHARMERICA JAN/FEB 2019 Potassium (K+) is found inside skeletal muscle, liver, and red blood cells. Normal levels of
Ch. 3: Cells & Their Environment
 Ch. 3: Cells & Their Environment OBJECTIVES: 1. To distinguish different cellular (fluid) compartments 2. Understand movement of substances across cell membranes (passive vs active) 3. To recognize different
Ch. 3: Cells & Their Environment OBJECTIVES: 1. To distinguish different cellular (fluid) compartments 2. Understand movement of substances across cell membranes (passive vs active) 3. To recognize different
Does Adding Examples to the American Society of Anesthesiologists Physical Status Classification Improve Consistency in Assignment to Patients?
 Does Adding Examples to the American Society of Anesthesiologists Physical Status Classification Improve Consistency in Assignment to Patients? Submitted Abstract to the 2015 ASA Annual Meeting 10 Hypothetical
Does Adding Examples to the American Society of Anesthesiologists Physical Status Classification Improve Consistency in Assignment to Patients? Submitted Abstract to the 2015 ASA Annual Meeting 10 Hypothetical
New Agents for Treating Hyperkalemia - Can They Help Us Improve Outcomes in HF?
 New Agents for Treating Hyperkalemia - Can They Help Us Improve Outcomes in HF? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg
New Agents for Treating Hyperkalemia - Can They Help Us Improve Outcomes in HF? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg
Acid Base Disorders: Key Core Concepts. Thomas DuBose M.D., MACP, FASN ASN Board Review Course Online Resource Material 2014
 Acid Base Disorders: Key Core Concepts Thomas DuBose M.D., MACP, FASN ASN Board Review Course Online Resource Material 2014 Speaker Disclosure I, Thomas DuBose, M.D., have no financial relationships or
Acid Base Disorders: Key Core Concepts Thomas DuBose M.D., MACP, FASN ASN Board Review Course Online Resource Material 2014 Speaker Disclosure I, Thomas DuBose, M.D., have no financial relationships or
3/17/2017. Acid-Base Disturbances. Goal. Eric Magaña, M.D. Presbyterian Medical Center Department of Pulmonary and Critical Care Medicine
 Acid-Base Disturbances Eric Magaña, M.D. Presbyterian Medical Center Department of Pulmonary and Critical Care Medicine Goal Provide an approach to determine complex acid-base disorders Discuss the approach
Acid-Base Disturbances Eric Magaña, M.D. Presbyterian Medical Center Department of Pulmonary and Critical Care Medicine Goal Provide an approach to determine complex acid-base disorders Discuss the approach
Non-Anion Gap Metabolic Acidosis. App.GoSoapbox.com then Join Now. Joel M. Topf, M.D.
 Non-Anion Gap Metabolic Acidosis App.GoSoapbox.com 665-971-584 then Join Now Joel M. Topf, M.D. http://pbfluids.com @kidney_boy App.GoSoapbox.com 665-971-584 32 y.o. female with fatigue, weakness and muscle
Non-Anion Gap Metabolic Acidosis App.GoSoapbox.com 665-971-584 then Join Now Joel M. Topf, M.D. http://pbfluids.com @kidney_boy App.GoSoapbox.com 665-971-584 32 y.o. female with fatigue, weakness and muscle
DIURETICS-4 Dr. Shariq Syed
 DIURETICS-4 Dr. Shariq Syed AIKTC - Knowledge Resources & Relay Center 1 Pop Quiz!! Loop diuretics act on which transporter PKCC NKCC2 AIKTCC I Don t know AIKTC - Knowledge Resources & Relay Center 2 Pop
DIURETICS-4 Dr. Shariq Syed AIKTC - Knowledge Resources & Relay Center 1 Pop Quiz!! Loop diuretics act on which transporter PKCC NKCC2 AIKTCC I Don t know AIKTC - Knowledge Resources & Relay Center 2 Pop
ALLHAT. Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic
 1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
HYPERTENSION IN CKD. LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL
 HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
9/14/2017. Acid-Base Disturbances. Goal. Provide an approach to determine complex acid-base disorders
 Acid-Base Disturbances NCNP October 10, 2017 Eric Magaña, M.D. Presbyterian Medical Center Department of Pulmonary and Critical Care Medicine Goal Provide an approach to determine complex acid-base disorders
Acid-Base Disturbances NCNP October 10, 2017 Eric Magaña, M.D. Presbyterian Medical Center Department of Pulmonary and Critical Care Medicine Goal Provide an approach to determine complex acid-base disorders
Nephron Structure inside Kidney:
 In-Depth on Kidney Nephron Structure inside Kidney: - Each nephron has two capillary regions in close proximity to the nephron tubule, the first capillary bed for fluid exchange is called the glomerulus,
In-Depth on Kidney Nephron Structure inside Kidney: - Each nephron has two capillary regions in close proximity to the nephron tubule, the first capillary bed for fluid exchange is called the glomerulus,
Clinical Toxicology Toxicity of Digitalis Glycosides 5 th Year (Lab 3)
") Clinical Toxicology Toxicity of Digitalis Glycosides 5 th Year (Lab 3) Lecturer: Rua Abbas Al-Hamdy Department of Pharmacology & Toxicology University of Al-Mustansiriyah 2017-2018 Introduction: Digitalis
Clinical Toxicology Toxicity of Digitalis Glycosides 5 th Year (Lab 3) Lecturer: Rua Abbas Al-Hamdy Department of Pharmacology & Toxicology University of Al-Mustansiriyah 2017-2018 Introduction: Digitalis
Crisis Management During Liver Transplant Surgery Liver and Intensive Care Group of Europe Newcastle upon Tyne 2005
 Crisis Management During Liver Transplant Surgery Liver and Intensive Care Group of Europe Newcastle upon Tyne 2005 M. Susan Mandell M.D. Ph. D. Department of Anesthesiology University of Colorado Health
Crisis Management During Liver Transplant Surgery Liver and Intensive Care Group of Europe Newcastle upon Tyne 2005 M. Susan Mandell M.D. Ph. D. Department of Anesthesiology University of Colorado Health
1. a)label the parts indicated above and give one function for structures Y and Z
label the parts indicated above and give one function for structures Y and Z") Excretory System 1 1. Excretory System a)label the parts indicated above and give one function for structures Y and Z W- renal cortex - X- renal medulla Y- renal pelvis collecting center of urine and then
Excretory System 1 1. Excretory System a)label the parts indicated above and give one function for structures Y and Z W- renal cortex - X- renal medulla Y- renal pelvis collecting center of urine and then
Cardiorenal and Renocardiac Syndrome
 And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
Hypertension Cases. Katharine Dahl, MD January 10, 2017
 Hypertension Cases Katharine Dahl, MD January 10, 2017 Dr. Dahl arrives late for her AHD hypertension lecture and you are asked to present the epidemiology of hypertension until she arrives. Which of the
Hypertension Cases Katharine Dahl, MD January 10, 2017 Dr. Dahl arrives late for her AHD hypertension lecture and you are asked to present the epidemiology of hypertension until she arrives. Which of the
Metabolic Alkalosis: Vomiting
 RENAL ANL) ACID-BASE PHYSIOLOGY 213 Case 37 Metabolic Alkalosis: Vomiting Maria Cuervo is a 20-year-old philosophy major at a state university. When the "24-hour" stomach flu went around campus during
RENAL ANL) ACID-BASE PHYSIOLOGY 213 Case 37 Metabolic Alkalosis: Vomiting Maria Cuervo is a 20-year-old philosophy major at a state university. When the "24-hour" stomach flu went around campus during
The most current assessment of this problem can be found in the Apex note dated
 Him andpcos Smartphrase:.REFENDOPCOS NOTE: patients with suspected PCOS are welcomed to endocrine clinic. There is also a PCOS clinic is available in the Ob/Gyn Department. I am referring @name@, a @age@
Him andpcos Smartphrase:.REFENDOPCOS NOTE: patients with suspected PCOS are welcomed to endocrine clinic. There is also a PCOS clinic is available in the Ob/Gyn Department. I am referring @name@, a @age@
RISK FACTORS AND TREATMENT STRATEGIES FOR URINARY STONES Review of NASA s Evidence Reports on Human Health Risks
 Mayo Clinic O Brien Urology Research Center RISK FACTORS AND TREATMENT STRATEGIES FOR URINARY STONES 2017 Review of NASA s Evidence Reports on Human Health Risks John C Lieske, MD July 27, 2017 What types
Mayo Clinic O Brien Urology Research Center RISK FACTORS AND TREATMENT STRATEGIES FOR URINARY STONES 2017 Review of NASA s Evidence Reports on Human Health Risks John C Lieske, MD July 27, 2017 What types
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA
 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.