Evidence-based Management of Fever in Infants and Young Children
|
|
|
- Scarlett Robbins
- 6 years ago
- Views:
Transcription
1 Evidence-based Management of Fever in Infants and Young Children Shabnam Jain, MD, MPH Associate Professor of Pediatrics Emory University Medical Director for Clinical Effectiveness
2 Objectives Understand an evidence based approach for managing febrile infants and young children in the outpatient setting Review Children s Healthcare of Atlanta fever guidelines 2
3 Fever in Infants and Young Children Very common childhood illness Vast majority are benign/self limited Some can be serious/life threatening (SBI) Meningitis, bacteremia, UTI, pneumonia Challenge is to distinguish the two when to initiate antibiotics Risk Stratification 3
4 Systematic approach to a febrile child General Appearance: Well appearing patient Past History: previously healthy Age Separate guidelines available for sickle cell, immunocompromised, etc 0 28 days days 2 6 months >6 24 months Source of Fever 0-28 days days 2-6 mth Well appearing? Y Past History? Age? N Source of fever? >6-24 mth 4
5 Definition of fever Rectal temperature of >38 C (100.4 F) Highest documented temperature at home or in ED is the degree of fever Temp threshold for screening may be higher Under 2 months: any fever requires attention >2 months: screening cut off is higher 5
6 1. Febrile neonate (0-28 days) High risk of serious bacterial infections (SBI) reduced immunity localize poorly maternal pathogens (E coli, GBS), listeria, HSV Exhibit few early signs of infection General appearance alone can be deceptive Routine testing and routine treatment Byington et al; Pantell et al, Pediatrics, July
7 Management: 0-28 days Complete sepsis evaluation for any fever (temp>38 C) CBC/diff and blood culture UA and urine culture LP (cell count, gram stain, gluc/prt, culture) Chest X ray if resp symptoms or signs Stool culture if diarrhea HSV screening: based on risk factors 7
8 Management: 0-28 days Routine sepsis work up (blood, urine, CSF) If risk factors for HSV: send HSV tests Anti infectives: Ampicillin mg/kg IV AND Cefotaxime 50 mg/kg IV Acyclovir: 20 mg/kg/dose (if HSV screening done) Admit to hospital 8
9 Key Concepts: 0-28 days Temp threshold: Any fever (>38 C) Routine testing (complete sepsis evaluation) Routine admission for empiric antibiotics 9
10 2. Febrile day old Risk of SBI remains, but less Lower risk of perinatal infections Listeria much less likely HSV much less likely No objective criteria to reliably identify infants at high risk Screening tests to identify infants at low risk * Routine testing, selective treatment (if not at low risk) *1990s: Baker, Baskin, Jeskiewicz 10
11 Boston, Philadelphia, Rochester Criteria Boston Philadelphia Rochester Age days days <60 days Temp >38 >38.2 >38 History/ Exam No immuniz/ abx/ well appearing/no SSTI 99% NPV for SBI Reassuring exam Full term, no abx, well/ no focal infection WBC <20, 000 <15, K (ABC<1,500) UA <10 WBC <10 WBC, GS <10 WBC CSF <10/HPF <8/HPF, GS CXR Neg (if done) Neg Antibiotics IM Ceftriaxone No abx No abx Children s Healthcare of Atlanta Emory Unive 11
12 Low Risk Criteria (29-60 days)* Well appearance Previously Healthy No focal bacterial infection Labs: WBC: 5 15 K ABC < 1,500 UA < 10 WBC/hpf, no nitrite CSF: <10 WBC, neg gram stain Chest X ray: no infiltrate *CHOA fever guideline days 12
13 Management (29-60 days) Partial sepsis evaluation (CBCD/bld cx and UA/UCx) Consider LP If work up negative and reliable follow up may d/c Without antibiotics With Ceftriaxone 50 mg/kg (LP must be done) If low risk criteria not met: Perform LP if not already done Admit for antibiotics (Cefotaxime 50 mg//kg) 13
14 What about a URI/OM/UTI? URI does not rule in a viral etiology* Neither does it rule out an SBI Same management with or w/o URI What about OM? With fever same management No fever forego sepsis eval with caution Mask SBI Difficulty if fever occurs later What about UTI? LP and admit for antibiotics** **Paquette et al, PEC 2011 **Dore-Bergeron et al, Pediatrics, 2009 *Byington et al; Pediatrics
15 What about bronchiolitis? Recognizable viral syndrome lower risk of SBI* <28 days: substantial risk of SBI > 28 days: SBI 1 7% with bronchiolitis VS 10 17% w/o UTI risk remains 0 28 days: full w/u, abx days: Blood & urine screen (may hold LP if RSV+) If starting antibiotics need to do LP *Greenes, PIDJ 1999; Purcell, ADC 2002 Titus, Pediatrics 2003; Levine, Pediatrics
16 Key Concepts: days Temp threshold: Any fever (>38 C) Routine testing, selective treatment Other viral source of infection lower risk of SBI LP not mandatory Antibiotics not always necessary If starting antibiotics perform LP 16
17 Common sources of fever Viral: Non specific viral illness eg URI, AGE, flu Well defined viral illness eg bronchiolitis, varicella, croup, stomatitis Bacterial: Non specific bacterial illness eg Otitis media Well defined bacterial infection eg pneumonia, localized cellulitis, UTI 17
18 3. Febrile 2-6 month old Usually have benign source of fever At risk for occult bacteremia (Pneumococcus, HIB) and UTI Starting to develop immunity (innate and/or vaccinations) Exam more reliable but signs and symptoms not completely developed Selective testing & selective treatment (based on source and height of fever) 18
19 Management (2-6 mth age) Targeted history to determine exposures and symptoms that may suggest a source for the fever Thorough exam to determine findings suggesting an etiology for the fever Many children in this age group do not need testing (depending on source and temp) 19
20 Management (2-6 mth age) CBC diff and blood culture UA, Urine Cx *CHOA Fever clinical practice guideline 20
21 Key Concepts: 2-6 month old fever A source for the fever is important and helpful in limiting work up Temp cut off: >39 UTI is the most common SBI Selective testing, selective treatment 21
22 Should we worry about fever>6 mth age? Early 1990s (H flu invasive organism, high risk of complications) Conservative approach to febrile child Late 1990s (H flu gone, Pneumococcus main etiology of OB) 2000s Pneumococcal vaccine PCV 7 in 2000, PCV 13 in 2010 Given at 2, 4, 6 months + booster Highly immunogenic, 97% effective 22
23 Invasive Pneumo Disease<5 yr age after PVC 7 *Pilishvili et al, JInfectDis,
24 Pneumococcal 13 Vaccine* 8 children s hospitals in 2011 *Tan TQ, Clin Microbiol Rev, 2012 **PIDJ, Mar 2013 Kaplan et al 24
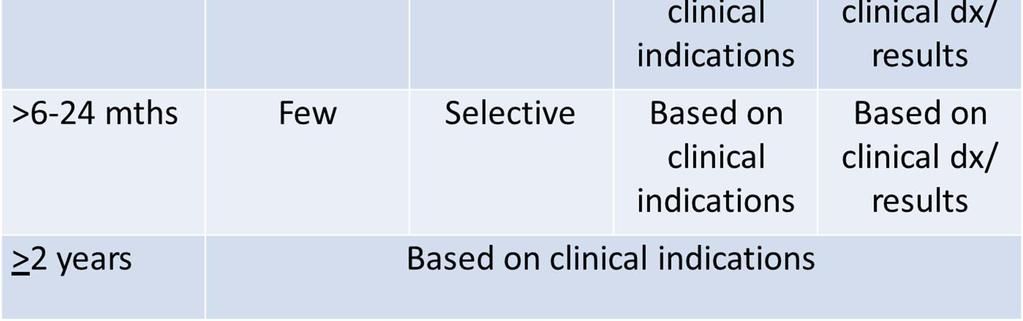
25 4. Febrile >6-24 mth olds High immunization rates Risk of bacteremia in FWLS: 0.25% * Pneumococcus usually self resolves Clinical exam is very helpful Risk of bacterial meningitis: 3/10,000 UTI is most common occult bacterial infection Vast majority of children in this age group do not need blood testing Benign neglect.. Watchful waiting Selective UTI screening *Wilkinson et al, Acad Emer Med,
26 Management of fever >6-24 mth old In well appearing, previously healthy, 6 24 month old with fever: Primary immunization status If UTD routine blood work not needed Source of fever If source present routine blood work not needed *Urine* If immuniz not UTD and no source of fever and temp>39 C : CBCD, bld cx UTI screening (based on risk factors) 26
27 Fever >6-24 months* CBCD, blood cx UTI screening (based on risk factors) *CHOA Fever clinical practice guideline 27
28 UTI Pyelonephritis: most common SBI in childhood UTI (<8 yr of age): 7 8% girls; 2% boys Fever without source 2 24 mth: UTI prevalence 5%* Prevalence depends on: Age: first year of life Gender: F:M relative risk 2.27 Race: less in blacks Circumcision: 3 to 4 fold decrease Presence of other source**: reduces risk of UTI Duration (>2 days), height of temp (>39)** *Hoberman J Pediatr 1993; Haddon Med J Aust 1999 **Gorelick, Shaw et al: 1998,2000,
29 2011/2016 AAP UTI Practice Guideline* Diagnosis and Management of Initial UTI in febrile (>38 C) infants and children 2 24 mth In a child with fever without source: Ill appearing and abx planned: screen for UTI (UA and UC) Not ill appearing : assess probability of UTI Low probability f/u without testing Not low probability screen for UTI Selective urine testing based on probability of UTI *Pediatrics Sep 2011, Dec


30 Probability of UTI* a Probability of UTI exceeds 1% even with no risk factors. *AAP UTI Clinical Practice Guideline, Pediatrics, 2011/
31 Who to Test for UTI*? Threshold to test should be < 3% probability of UTI <1% or <2%, depending on: Contact during illness Comfort with diagnostic uncertainty *AAP UTI Clinical Practice Guideline, Pediatrics, 2011/
32 How to obtain sample? Option 1: catheter / suprapubic Option 2: bag specimen if negative if positive monitor catheter/suprapubic 2 Step Process for ED UTI Screening. Lavelle et al, Pediatrics, July
33 UTI Treatment Route: Oral and parenteral equally efficacious* Most children can be treated orally, except: Toxic Unable to take orals Noncompliance Choice of abx: based on local patterns Cefprozil Duration: 7 14 days *Hoberman Pediatrics
34 Key Concepts: Fever >2 mth age Screening tests based on source of fever and height of temp After 6 months of age, if immunizations UTD blood work usually not needed UTI screening based on probability of UTI (# of risk factors) 34
35 Summary Initial management of fever in infant/young child: Appearance Past Medical history Age Immunization status Source of fever Current epidemiology Combination of clinical and lab criteria Balancing risk of disease and risk of testing/therapy 35

36 Management of febrile infants/young children 36
4/14/2010. Theoretical purpose of fever? Andrea Marmor, MD, MSEd Assistant Clinical Professor, Pediatrics UCSF April 13, 2010
 Andrea Marmor, MD, MSEd Assistant Clinical Professor, Pediatrics UCSF April 13, 2010 Parental touch? Absence of fever more reliable than presence. Axillary and tympanic Vulnerable to environmental and
Andrea Marmor, MD, MSEd Assistant Clinical Professor, Pediatrics UCSF April 13, 2010 Parental touch? Absence of fever more reliable than presence. Axillary and tympanic Vulnerable to environmental and
Faculty Disclosure. Stephen I. Pelton, MD. Dr. Pelton has listed no financial interest/arrangement that would be considered a conflict of interest.
 Faculty Disclosure Stephen I. Pelton, MD Dr. Pelton has listed no financial interest/arrangement that would be considered a conflict of interest. Advances in the management of fever in infants 0 to 3 and
Faculty Disclosure Stephen I. Pelton, MD Dr. Pelton has listed no financial interest/arrangement that would be considered a conflict of interest. Advances in the management of fever in infants 0 to 3 and
Hot Hot Tot:! The Hot Tot. Fever in KIds <90 Days 5/26/10
 Hot Hot Tot:! Fever in KIds
Hot Hot Tot:! Fever in KIds
The Febrile Infant. SJRH ED Rounds Dec By: Robin Clouston
 1 The Febrile Infant SJRH ED Rounds Dec 11 2018 By: Robin Clouston 2 Objectives Discuss the risk of serious bacterial infection (SBI) in the neonate or young infant (
1 The Febrile Infant SJRH ED Rounds Dec 11 2018 By: Robin Clouston 2 Objectives Discuss the risk of serious bacterial infection (SBI) in the neonate or young infant (
EPG Clinical Guidelines
 Guidelines for the Management of Febrile Young Children Neonate age 7 days Temperature > 38 C, documented at home or in the ED Complete blood count with manual differential (CBCD), urinalysis (UA), urine
Guidelines for the Management of Febrile Young Children Neonate age 7 days Temperature > 38 C, documented at home or in the ED Complete blood count with manual differential (CBCD), urinalysis (UA), urine
Disclosures. Background. Definitions. Why Worry about these Infants? Goals. Bacterial infection in the neonate and young infant: a review
 Disclosures Bacterial infection in the neonate and young infant: a review Russell J. McCulloh, MD Med-Peds Infectious Diseases August 8, 2017 I have no financial interests to disclose Funding: Eva and
Disclosures Bacterial infection in the neonate and young infant: a review Russell J. McCulloh, MD Med-Peds Infectious Diseases August 8, 2017 I have no financial interests to disclose Funding: Eva and
Beyond the Reflex Arc: An Evidence-Based Discussion of the Management of Febrile Infants
 Beyond the Reflex Arc: An Evidence-Based Discussion of the Management of Febrile Infants Cole Condra, MD MSc Division of Emergency Medical Services Children s Mercy Hospital October 1, 2011 Disclosure
Beyond the Reflex Arc: An Evidence-Based Discussion of the Management of Febrile Infants Cole Condra, MD MSc Division of Emergency Medical Services Children s Mercy Hospital October 1, 2011 Disclosure
+ Objectives. n Define who is at risk for SBI. n Clarify risk stratification. n Provide treatment guidelines. n Bust some myths
 Objectives n Define wo is at risk for SBI n Clarify risk stratification n Provide treatment guidelines Neonatal Fever Benjamin B. Constance, MD, FAWM n Bust some myts Based on Case wat do you want to know?
Objectives n Define wo is at risk for SBI n Clarify risk stratification n Provide treatment guidelines Neonatal Fever Benjamin B. Constance, MD, FAWM n Bust some myts Based on Case wat do you want to know?
Fever in neonates (age 0 to 28 days)
") Fever in neonates (age 0 to 28 days) INCLUSION CRITERIA Infant 28 days of life Temperature 38 C (100.4 F) by any route/parental report EXCLUSION CRITERIA Infants with RSV Febrile Infant 28 days old Ill
Fever in neonates (age 0 to 28 days) INCLUSION CRITERIA Infant 28 days of life Temperature 38 C (100.4 F) by any route/parental report EXCLUSION CRITERIA Infants with RSV Febrile Infant 28 days old Ill
Fever in the Newborn Period
 Fever in the Newborn Period 1. Definitions 1 2. Overview 1 3. History and Physical Examination 2 4. Fever in Infants Less than 3 Months Old 2 a. Table 1: Rochester criteria for low risk infants 3 5. Fever
Fever in the Newborn Period 1. Definitions 1 2. Overview 1 3. History and Physical Examination 2 4. Fever in Infants Less than 3 Months Old 2 a. Table 1: Rochester criteria for low risk infants 3 5. Fever
Fevers and Seizures in Infants and Young Children
 Fevers and Seizures in Infants and Young Children Kellie Holtmeier, PharmD Pediatric Clinical Pharmacist University of New Mexico Hospital Disclosure I have no conflicts of interest 1 Pharmacist Objectives
Fevers and Seizures in Infants and Young Children Kellie Holtmeier, PharmD Pediatric Clinical Pharmacist University of New Mexico Hospital Disclosure I have no conflicts of interest 1 Pharmacist Objectives
Fever Without a Source Age: 0-28 Day Pathway - Emergency Department Evidence Based Outcome Center
 Age: 0-28 Day Pathway - Emergency Department EXCLUSION CRITERIA Toxic appearing No fever Born < 37 weeks gestational age INCLUSION CRITERIA Non-toxic with temperature > 38 C (100.4 F) < 36 C (96.5 F) measured
Age: 0-28 Day Pathway - Emergency Department EXCLUSION CRITERIA Toxic appearing No fever Born < 37 weeks gestational age INCLUSION CRITERIA Non-toxic with temperature > 38 C (100.4 F) < 36 C (96.5 F) measured
Fever in Babies. Too much testing or not enough testing? Martin E. Weisse, M.D. Pediatric Infectious Diseases
 Fever in Babies Too much testing or not enough testing? Martin E. Weisse, M.D. Pediatric Infectious Diseases Disclosures I have nothing to disclose Learning Objectives At the end of the talk, participants
Fever in Babies Too much testing or not enough testing? Martin E. Weisse, M.D. Pediatric Infectious Diseases Disclosures I have nothing to disclose Learning Objectives At the end of the talk, participants
Judith Klein, MD 2011 FEVER IN THE FIRST 36 MONTHS OF LIFE
 Judith Klein, MD 2011 FEVER IN THE FIRST 36 MONTHS OF LIFE Objectives A short history of the kiddie fever business Vaccinations Rapid viral testing Biomarkers Month-by-month approach to fevers in these
Judith Klein, MD 2011 FEVER IN THE FIRST 36 MONTHS OF LIFE Objectives A short history of the kiddie fever business Vaccinations Rapid viral testing Biomarkers Month-by-month approach to fevers in these
1. Introduction Algorithm: Infant with Fever 0-28 Days Algorithm: Infant with Fever Days...3
 These guidelines are designed to assist clinicians and are not intended to supplant good clinical judgement or to establish a protocol for all patients with this condition. MANAGEMENT OF FEVER 38 C (100.4F)
These guidelines are designed to assist clinicians and are not intended to supplant good clinical judgement or to establish a protocol for all patients with this condition. MANAGEMENT OF FEVER 38 C (100.4F)
Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014
 Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014 Prep Question You are camping with a group of boys at a rural campground in the southeastern Unites States when one of the campers is bitten
Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014 Prep Question You are camping with a group of boys at a rural campground in the southeastern Unites States when one of the campers is bitten
Infant Fever, What s Old What s New Brian R. Moore, M.D., F.A.A.P.
 Infant Fever, What s Old What s New Brian R. Moore, M.D., F.A.A.P. PEM Fellowship Director Assistant Professor, Departments of Emergency Medicine and Pediatrics University of New Mexico Health Science
Infant Fever, What s Old What s New Brian R. Moore, M.D., F.A.A.P. PEM Fellowship Director Assistant Professor, Departments of Emergency Medicine and Pediatrics University of New Mexico Health Science
greater than 10 will be considered ill appearing; a score of 10 or less will be considered well appearing.
 1 Use the Yale Observation Scale to assess whether the patient is ill or well appearing. A score greater than 10 will be considered ill appearing; a score of 10 or less will be considered well appearing.
1 Use the Yale Observation Scale to assess whether the patient is ill or well appearing. A score greater than 10 will be considered ill appearing; a score of 10 or less will be considered well appearing.
Fever in Young Infants 7 90 days of age
 Fever in Young Infants 7 90 days of age Derek Zhorne, MD Clinical Assistant Professor of Pediatrics Pediatric Hospitalist Disclosures I have no actual or potential conflicts in relation to this presentation.
Fever in Young Infants 7 90 days of age Derek Zhorne, MD Clinical Assistant Professor of Pediatrics Pediatric Hospitalist Disclosures I have no actual or potential conflicts in relation to this presentation.
Fever and Infections in Pediatrics
 Fever and Infections in Pediatrics Dr. Todd Twogood 2019 update Big Sky Conference Pediatric Fever and illness The most common reason for children to be taken to the doctor for acute illness Major concern
Fever and Infections in Pediatrics Dr. Todd Twogood 2019 update Big Sky Conference Pediatric Fever and illness The most common reason for children to be taken to the doctor for acute illness Major concern
Rational Evaluation of the Febrile Infant
 Disclosures Rational Evaluation of the Febrile Infant Samir S. Shah, MD, MSCE Professor, Department of Pediatrics University of Cincinnati College of Medicine Director, Division of Hospital Medicine Attending
Disclosures Rational Evaluation of the Febrile Infant Samir S. Shah, MD, MSCE Professor, Department of Pediatrics University of Cincinnati College of Medicine Director, Division of Hospital Medicine Attending
Fever in Infants: Pediatric Dilemmas in Antibiotherapy
 Fever in Infants: Pediatric Dilemmas in Antibiotherapy Jahzel M. Gonzalez Pagan, MD, FAAP Pediatric Emergency Medicine Associate Professor, UPH Medical Advisor, SJCH June 9 th, 2017 S Objectives S Review
Fever in Infants: Pediatric Dilemmas in Antibiotherapy Jahzel M. Gonzalez Pagan, MD, FAAP Pediatric Emergency Medicine Associate Professor, UPH Medical Advisor, SJCH June 9 th, 2017 S Objectives S Review
 Fever Phobia and the ED Doc Ran Goldman, MD (rgoldman@cw.bc.ca) BC Children s Hospital, Professor, University of British Columbia SLIDES ON : www.clinicalpeds.com/whistler Define Fever 38.0 o Doesn t
Fever Phobia and the ED Doc Ran Goldman, MD (rgoldman@cw.bc.ca) BC Children s Hospital, Professor, University of British Columbia SLIDES ON : www.clinicalpeds.com/whistler Define Fever 38.0 o Doesn t
Fever in Children. Dr Shane George Staff Specialist - Emergency Medicine & Children s Critical Care Gold Coast University Hospital
 Fever in Children Dr Shane George Staff Specialist - Emergency Medicine & Children s Critical Care Gold Coast University Hospital Update on Children s services @ GCUH Dedicated Children s Pod in the Emergency
Fever in Children Dr Shane George Staff Specialist - Emergency Medicine & Children s Critical Care Gold Coast University Hospital Update on Children s services @ GCUH Dedicated Children s Pod in the Emergency
Fever. National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital
 Fever National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital Case 1 4-month-old well-appearing girl admitted for croup and respiratory distress.
Fever National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital Case 1 4-month-old well-appearing girl admitted for croup and respiratory distress.
Your first patient of the day
 Your first patient of the day 1 month old male with 2 days of fussiness Decreased stool output for 3 days Poor latch during breastfeeding noted at 3AM on day of arrival to the ED Started spitting up later
Your first patient of the day 1 month old male with 2 days of fussiness Decreased stool output for 3 days Poor latch during breastfeeding noted at 3AM on day of arrival to the ED Started spitting up later
Antibiotic Protocols for Paediatrics Steve Biko Academic Hospital
 Antibiotic Protocols for Paediatrics Steve Biko Academic Hospital Respiratory tract infections in children Uncomplicated URTI A child with a cold should not receive an antibiotic Paracetamol (15 mg/kg/dose
Antibiotic Protocols for Paediatrics Steve Biko Academic Hospital Respiratory tract infections in children Uncomplicated URTI A child with a cold should not receive an antibiotic Paracetamol (15 mg/kg/dose
Scott Williams, MD Pediatric Nephrology OLOL Children s Hospital September 29, Controversies in Urinary Tract Infections
 Scott Williams, MD Pediatric Nephrology OLOL Children s Hospital September 29, 2013 Controversies in Urinary Tract Infections Disclaimer I have no affiliations with any pharmaceutical or equipment company
Scott Williams, MD Pediatric Nephrology OLOL Children s Hospital September 29, 2013 Controversies in Urinary Tract Infections Disclaimer I have no affiliations with any pharmaceutical or equipment company
Advanced Pediatric Emergency Medicine Assembly
 (+)Kathy Shaw, MD, FACEP Associate Chair and PSO, Department of Pediatrics, Perelman School of Medicine, University of Pennsylvania; Nicolas Crognale Endowed Chair and Chief, Division of Enmergency Medicine,
(+)Kathy Shaw, MD, FACEP Associate Chair and PSO, Department of Pediatrics, Perelman School of Medicine, University of Pennsylvania; Nicolas Crognale Endowed Chair and Chief, Division of Enmergency Medicine,
CRACKCast E167 Pediatric Fever. Key Concepts. CrackCast Show Notes Pediatric Fever April 2018
 CRACKCast E167 Pediatric Fever Key Concepts Fever is the #1 kids are brought to the ED! Vaccination (for Haemophilus influenzae type b and Streptococcus pneumoniae) has dropped the rates of serious bacterial
CRACKCast E167 Pediatric Fever Key Concepts Fever is the #1 kids are brought to the ED! Vaccination (for Haemophilus influenzae type b and Streptococcus pneumoniae) has dropped the rates of serious bacterial
Pediatric Urinary Tract Infections
 Pediatric Urinary Tract Infections Sarmistha B. Hauger M.D. Pediatric Infectious Diseases Specially For Children Dell Children s Medical Center of Central Texas CME Conference 5/08 Pediatric UTI Epidemiology
Pediatric Urinary Tract Infections Sarmistha B. Hauger M.D. Pediatric Infectious Diseases Specially For Children Dell Children s Medical Center of Central Texas CME Conference 5/08 Pediatric UTI Epidemiology
Evaluating Fever in Infants. Derek Zhorne, MD Clinical Assistant Professor of Pediatrics Pediatric Hospitalist
 Evaluating Fever in Infants Derek Zhorne, MD Clinical Assistant Professor of Pediatrics Pediatric Hospitalist Disclosures I have no actual or potential conflicts in relation to this presentation. I will
Evaluating Fever in Infants Derek Zhorne, MD Clinical Assistant Professor of Pediatrics Pediatric Hospitalist Disclosures I have no actual or potential conflicts in relation to this presentation. I will
CHAPTER 167 Pediatric Fever
 CHAPTER 167 Pediatric Fever Nathan W. Mick Fever is the most common chief complaint of pediatric patients presenting to the emergency department (ED), accounting for up to 20% of ED visits. Most cases
CHAPTER 167 Pediatric Fever Nathan W. Mick Fever is the most common chief complaint of pediatric patients presenting to the emergency department (ED), accounting for up to 20% of ED visits. Most cases
UTI Update: Have We Been Led Astray? Disclosure. Objectives
 UTI Update: Have We Been Led Astray? KAAP Sept 28, 2012 Robert Wittler, MD 1 Disclosure Neither I nor any member of my immediate family has a financial relationship or interest with any entity related
UTI Update: Have We Been Led Astray? KAAP Sept 28, 2012 Robert Wittler, MD 1 Disclosure Neither I nor any member of my immediate family has a financial relationship or interest with any entity related
The McMaster at night Pediatric Curriculum
 The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
Dr. Bob Wilson Golden BC
 Fever in Infants Under 3 Mon. Dr. Bob Wilson Golden BC What is the risk of serious bacterial infection in a febrile 2 A. 5% B. 10% C. 25% D. 50% E. 100% month old infant? What is the most common congenital
Fever in Infants Under 3 Mon. Dr. Bob Wilson Golden BC What is the risk of serious bacterial infection in a febrile 2 A. 5% B. 10% C. 25% D. 50% E. 100% month old infant? What is the most common congenital
Urinary tract infection. Mohamed Ahmed Fouad Lecturer of pediatrics Jazan faculty of medicine
 Urinary tract infection Mohamed Ahmed Fouad Lecturer of pediatrics Jazan faculty of medicine Objectives To differentiate between types of urinary tract infections To recognize the epidemiology of UTI in
Urinary tract infection Mohamed Ahmed Fouad Lecturer of pediatrics Jazan faculty of medicine Objectives To differentiate between types of urinary tract infections To recognize the epidemiology of UTI in
Management of Complex Febrile Seizures
 Management of Complex Febrile Seizures An 13 month old girl presents to the ED after having a shaking episode at home. Mom describes shaking of both arms and legs, lasting 20 minutes. The child has no
Management of Complex Febrile Seizures An 13 month old girl presents to the ED after having a shaking episode at home. Mom describes shaking of both arms and legs, lasting 20 minutes. The child has no
10/11/2017 TOPICS FOR TODAY THE FEBRILE CHILD IS THERE TRUTH IN GOOGLE? EVIDENCE BASED PEDIATRIC EMERGENCY MEDICINE: ARE YOU PRACTICING IT?
 EVIDENCE BASED PEDIATRIC EMERGENCY MEDICINE: ARE YOU PRACTICING IT? Richard M. Cantor, MD FAAP/FACEP Professor of Emergency Medicine and Pediatrics Director of Pediatric Emergency Services Director, Pediatric
EVIDENCE BASED PEDIATRIC EMERGENCY MEDICINE: ARE YOU PRACTICING IT? Richard M. Cantor, MD FAAP/FACEP Professor of Emergency Medicine and Pediatrics Director of Pediatric Emergency Services Director, Pediatric
11/9/2012. Group B Streptococcal Infections: Consensus and Controversies. Prevention of Early-Onset GBS Disease in the USA.
 Group B Streptococcal Infections: Consensus and Controversies Carol J. Baker, M.D. Professor of Pediatrics, Molecular Virology and Microbiology Executive Director, Center for Vaccine Awareness and Research
Group B Streptococcal Infections: Consensus and Controversies Carol J. Baker, M.D. Professor of Pediatrics, Molecular Virology and Microbiology Executive Director, Center for Vaccine Awareness and Research
Fever in the Pediatric Patient (part one)
") Fever in the Pediatric Patient (part one) Heather Wolfe, MD, FAAP Medical Director, Lutheran Children s Hospital Medical Education Participant Objectives: 1. Discuss pediatric fever and the concept of
Fever in the Pediatric Patient (part one) Heather Wolfe, MD, FAAP Medical Director, Lutheran Children s Hospital Medical Education Participant Objectives: 1. Discuss pediatric fever and the concept of
UTI are the most common genitourinary disease of childhood. The prevalence of UTI at all ages is girls and 1% of boys.
 UTI are the most common genitourinary disease of childhood. The prevalence of UTI at all ages is girls and 1% of boys. 1-3% of Below 1 yr. male: female ratio is 4:1 especially among uncircumcised males,
UTI are the most common genitourinary disease of childhood. The prevalence of UTI at all ages is girls and 1% of boys. 1-3% of Below 1 yr. male: female ratio is 4:1 especially among uncircumcised males,
IDPH ESF-8 Plan: Pediatric and Neonatal Surge Annex Sample Pediatric Admission Orders 2015
 Purpose: To provide guidance to practitioners caring for pediatric patients who need inpatient hospital care during a disaster. Disclaimer: This guideline is not meant to be all inclusive, replace an existing
Purpose: To provide guidance to practitioners caring for pediatric patients who need inpatient hospital care during a disaster. Disclaimer: This guideline is not meant to be all inclusive, replace an existing
Approaching Neutropenia in Children. SW Florida Osteopathic Medical Society: 39 th Annual Seminars in Family Practice
 Approaching Neutropenia in Children SW Florida Osteopathic Medical Society: 39 th Annual Seminars in Family Practice Approaching Neutropenia in Children Emad Salman M.D Golisano Children s Hospital of
Approaching Neutropenia in Children SW Florida Osteopathic Medical Society: 39 th Annual Seminars in Family Practice Approaching Neutropenia in Children Emad Salman M.D Golisano Children s Hospital of
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
Pediatric Potpourri WAPA Spring Conference. Russell Migita, MD Seattle Children s Hospital University of Washington School of Medicine
 Pediatric Potpourri WAPA Spring Conference Russell Migita, MD Seattle Children s Hospital University of Washington School of Medicine April 22, 2017 Most Common Pediatric Complaints Respiratory Distress
Pediatric Potpourri WAPA Spring Conference Russell Migita, MD Seattle Children s Hospital University of Washington School of Medicine April 22, 2017 Most Common Pediatric Complaints Respiratory Distress
FEBRILE SEIZURES. IAP UG Teaching slides
 FEBRILE SEIZURES 1 DEFINITION Febrile seizures are seizures that occur between the age of 6 and 60 months with a temperature of 38 C or higher, that are not the result of central nervous system infection
FEBRILE SEIZURES 1 DEFINITION Febrile seizures are seizures that occur between the age of 6 and 60 months with a temperature of 38 C or higher, that are not the result of central nervous system infection
CNS Infections. GBS Streptococcus agalactiae. Meningitis - Neonate
 CNS Infections GBS Streptococcus agalactiae Bacterial meningitis - Pathophysiology - general Specific organisms - Age Hosts Treatment/Prevention Distinguish from viral disease Common commensal flora childbearing
CNS Infections GBS Streptococcus agalactiae Bacterial meningitis - Pathophysiology - general Specific organisms - Age Hosts Treatment/Prevention Distinguish from viral disease Common commensal flora childbearing
Hot Stuff: The Febrile Child
 Hot Stuff: The Febrile Child Dr. Shannon MacPhee, Department of Emergency Medicine, Division Head Pediatric Emergency Medicine. IWK Health Centre. Dalhousie University November 2017 Know when to suspect
Hot Stuff: The Febrile Child Dr. Shannon MacPhee, Department of Emergency Medicine, Division Head Pediatric Emergency Medicine. IWK Health Centre. Dalhousie University November 2017 Know when to suspect
Should blood cultures be obtained in all infants 3 to 36 months presenting with significant fever? abstract CLINICAL QUESTION REVIEW
 CLINICAL QUESTION REVIEW CQR is a recurring section in Hospital Pediatrics where authors start with a relevant clinical question, find and synthesize the recent literature and provide their best answer
CLINICAL QUESTION REVIEW CQR is a recurring section in Hospital Pediatrics where authors start with a relevant clinical question, find and synthesize the recent literature and provide their best answer
TOPICS. Wheezing/Asthma THE BEST PEDIATRIC LITERATURE THAT STILL AFFECT YOUR PRACTICE
 THE BEST PEDIATRIC LITERATURE THAT STILL AFFECT YOUR PRACTICE Ghazala Q. Sharieff MD, MBA Wheezing/asthma Croup Immunizations and fever Appendicitis Complex febrile seizures Procedures Head Injury Zofran
THE BEST PEDIATRIC LITERATURE THAT STILL AFFECT YOUR PRACTICE Ghazala Q. Sharieff MD, MBA Wheezing/asthma Croup Immunizations and fever Appendicitis Complex febrile seizures Procedures Head Injury Zofran
Advanced Pediatric Emergency Medicine Assembly
 (+)Joan Shook, MD, FACEP Professor of Pediatrics, Baylor College of Medicine; Chief Safety Officer and Chief Clinical Information Officer, Texas Children's Hospital Advanced Pediatric Emergency Medicine
(+)Joan Shook, MD, FACEP Professor of Pediatrics, Baylor College of Medicine; Chief Safety Officer and Chief Clinical Information Officer, Texas Children's Hospital Advanced Pediatric Emergency Medicine
Dilemmas in the Management of Meningitis & Encephalitis HEADACHE AND FEVER. What is the best initial approach for fever, headache, meningisums?
 Dilemmas in the Management of Meningitis & Encephalitis Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine HEADACHE AND FEVER What is the best initial approach for fever,
Dilemmas in the Management of Meningitis & Encephalitis Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine HEADACHE AND FEVER What is the best initial approach for fever,
Community Acquired Pneumonia
 April 2014 References: 1. Bradley JS, Byington CL, Shah SS, Alverson B, Carter ER, Harrison C, Kaplan SL Mace SE, McCracken Jr. GH, Moor MR, St. Peter SD, Stockwell JA, and Swanson JT. The Management of
April 2014 References: 1. Bradley JS, Byington CL, Shah SS, Alverson B, Carter ER, Harrison C, Kaplan SL Mace SE, McCracken Jr. GH, Moor MR, St. Peter SD, Stockwell JA, and Swanson JT. The Management of
DENISE K. SUR, MD, and ELISE L. BUKONT, DO, University of California, Los Angeles, Los Angeles, California. a complete physical examination,
 Evaluating Fever of Unidentifiable Source in Young Children DENISE K. SUR, MD, and ELISE L. BUKONT, DO, University of California, Los Angeles, Los Angeles, California Most children will have been evaluated
Evaluating Fever of Unidentifiable Source in Young Children DENISE K. SUR, MD, and ELISE L. BUKONT, DO, University of California, Los Angeles, Los Angeles, California Most children will have been evaluated
EVALUATION OF A SICK CHILD WITH FEVER
 EVALUATION OF A SICK CHILD WITH FEVER Learning objectives At the conclusion of this learning activity, participants should be able to; Discuss the different etiologies of acute illness in a child Identify
EVALUATION OF A SICK CHILD WITH FEVER Learning objectives At the conclusion of this learning activity, participants should be able to; Discuss the different etiologies of acute illness in a child Identify
NIH Public Access Author Manuscript Pediatrics. Author manuscript; available in PMC 2007 November 14.
 NIH Public Access Author Manuscript Published in final edited form as: Pediatrics. 2006 July ; 118(1): 34 40. Prospective Evaluation of the Risk of Serious Bacterial Infection in Children Who Present to
NIH Public Access Author Manuscript Published in final edited form as: Pediatrics. 2006 July ; 118(1): 34 40. Prospective Evaluation of the Risk of Serious Bacterial Infection in Children Who Present to
Medline Abstracts for References 15,30-37
 Page 1 of 5 Official reprint from UpToDate www.uptodate.com 2013 UpToDate Medline Abstracts for References 15,30-37 of 'Fever without a source in children 3 to 36 months of age' 15 Check for full text
Page 1 of 5 Official reprint from UpToDate www.uptodate.com 2013 UpToDate Medline Abstracts for References 15,30-37 of 'Fever without a source in children 3 to 36 months of age' 15 Check for full text
Nicolette Janzen, MD Texas Children's Hospital
 Which UTIs Need a VCUG? Applying AAP Guidelines Nicolette Janzen, MD Texas Children's Hospital Goals 1 2 3 4 5 Review the guidelines Present clinical scenarios Discuss VCUG and nuclear cystogram Discuss
Which UTIs Need a VCUG? Applying AAP Guidelines Nicolette Janzen, MD Texas Children's Hospital Goals 1 2 3 4 5 Review the guidelines Present clinical scenarios Discuss VCUG and nuclear cystogram Discuss
UTI and VUR practical points and management
 UTI and VUR practical points and management Søren Rittig, Prof., DMSc Child and Adolescent Medicine, Aarhus University Hospital Aarhus, Denmark Outline Definition and diagnosis of UTI Treatment of UTI
UTI and VUR practical points and management Søren Rittig, Prof., DMSc Child and Adolescent Medicine, Aarhus University Hospital Aarhus, Denmark Outline Definition and diagnosis of UTI Treatment of UTI
Sample Selection- Vignettes
 Sample Selection- Vignettes Rangaraj Selvarangan, BVSc, PhD, D(ABMM) Professor, UMKC School of Medicine Director, Microbiology, Virology and Molecular Infectious Diseases Laboratory Director, Laboratory
Sample Selection- Vignettes Rangaraj Selvarangan, BVSc, PhD, D(ABMM) Professor, UMKC School of Medicine Director, Microbiology, Virology and Molecular Infectious Diseases Laboratory Director, Laboratory
Study of culture and sensitivity pattern of urinary tract infection in febrile preschool children in a tertiary care hospital
 International Journal of Contemporary Pediatrics Ashoka C et al. Int J Contemp Pediatr. 2016 Aug;3(3):1032-1036 http://www.ijpediatrics.com pissn 2349-3283 eissn 2349-3291 Research Article DOI: http://dx.doi.org/10.18203/2349-3291.ijcp20162386
International Journal of Contemporary Pediatrics Ashoka C et al. Int J Contemp Pediatr. 2016 Aug;3(3):1032-1036 http://www.ijpediatrics.com pissn 2349-3283 eissn 2349-3291 Research Article DOI: http://dx.doi.org/10.18203/2349-3291.ijcp20162386
Pneumococcal Vaccine Effectiveness. Steven Black, MD Center for Global Health Cincinnati Children s s Hospital Cincinnati, Ohio USA
 Pneumococcal Vaccine Effectiveness Steven Black, MD Center for Global Health Cincinnati Children s s Hospital Cincinnati, Ohio USA Overview Possible effectiveness outcomes for pneumococcal vaccines Pre-licensure
Pneumococcal Vaccine Effectiveness Steven Black, MD Center for Global Health Cincinnati Children s s Hospital Cincinnati, Ohio USA Overview Possible effectiveness outcomes for pneumococcal vaccines Pre-licensure
Central Nervous System Infection
 Central Nervous System Infection Lingyun Shao Department of Infectious Diseases Huashan Hospital, Fudan University Definition Meningitis: an inflammation of the arachnoid membrane, the pia mater, and the
Central Nervous System Infection Lingyun Shao Department of Infectious Diseases Huashan Hospital, Fudan University Definition Meningitis: an inflammation of the arachnoid membrane, the pia mater, and the
J of Evolution of Med and Dent Sci/ eissn , pissn / Vol. 4/ Issue 66/ Aug 17, 2015 Page 11432
 BLOOD CULTURE AND BACTEREMIA PREDICTORS IN INFANTS LESS THAN ONE YEAR OF AGE WITH FEVER WITHOUT SOURCE (FWS) Y. G. Sathish Kumar 1, A. Udayamaliny 2, S. Ankitha 3 HOW TO CITE THIS ARTICLE: Y. G. Sathish
BLOOD CULTURE AND BACTEREMIA PREDICTORS IN INFANTS LESS THAN ONE YEAR OF AGE WITH FEVER WITHOUT SOURCE (FWS) Y. G. Sathish Kumar 1, A. Udayamaliny 2, S. Ankitha 3 HOW TO CITE THIS ARTICLE: Y. G. Sathish
REACTIVE THROMBOCYTOSIS IN FEBRILE CHILDREN WITH SERIOUS BACTERIAL INFECTION Amita Jane D Souza 1, Anil Shetty 2, Divya Krishnan K 3
 REACTIVE THROMBOCYTOSIS IN FEBRILE CHILDREN WITH SERIOUS BACTERIAL INFECTION Amita Jane D Souza 1, Anil Shetty 2, Divya Krishnan K 3 HOW TO CITE THIS ARTICLE: Amita Jane D Souza, Anil Shetty, Divya Krishnan
REACTIVE THROMBOCYTOSIS IN FEBRILE CHILDREN WITH SERIOUS BACTERIAL INFECTION Amita Jane D Souza 1, Anil Shetty 2, Divya Krishnan K 3 HOW TO CITE THIS ARTICLE: Amita Jane D Souza, Anil Shetty, Divya Krishnan
A Practical Approach to Leukopenia/Neutropenia in Children. Vandy Black, M.D., M.Sc., FAAP OLOL Children s Hospital August 24, 2014
 A Practical Approach to Leukopenia/Neutropenia in Children Vandy Black, M.D., M.Sc., FAAP OLOL Children s Hospital August 24, 2014 Disclosures EPIC trial MAST Therapeutics SUSTAIN trial Selexys Pharmaceuticals
A Practical Approach to Leukopenia/Neutropenia in Children Vandy Black, M.D., M.Sc., FAAP OLOL Children s Hospital August 24, 2014 Disclosures EPIC trial MAST Therapeutics SUSTAIN trial Selexys Pharmaceuticals
Osteomyelitis Samir S. Shah, MD, MSCE
 Osteomyelitis Samir S. Shah, MD, MSCE Professor, Department of Pediatrics University of Cincinnati College of Medicine Director, Division of Hospital Medicine Attending Physician in Infectious Diseases
Osteomyelitis Samir S. Shah, MD, MSCE Professor, Department of Pediatrics University of Cincinnati College of Medicine Director, Division of Hospital Medicine Attending Physician in Infectious Diseases
Reviewing the recent literature to answer clinical questions: Should I change my practice?
 Reviewing the recent literature to answer clinical questions: Should I change my practice? JILL MILLER, MD PEM ATTENDING CHKD ASSISTANT PROFESSOR PEDIATRICS, EVMS Objectives Review the literature to answer
Reviewing the recent literature to answer clinical questions: Should I change my practice? JILL MILLER, MD PEM ATTENDING CHKD ASSISTANT PROFESSOR PEDIATRICS, EVMS Objectives Review the literature to answer
5/5/2010. Phil Bernard, MD. 2 week old presents to your office with fever to F HR 150 RR 40
 2 week old presents to your office with fever to 101.5 F HR 150 RR 40 BP not obtained obtained Sats 95% Phil Bernard, MD Baraff LJ, Bass JW, Fleisher GR, Klein JO, McCracken GH, Powell KR, et al. Practice
2 week old presents to your office with fever to 101.5 F HR 150 RR 40 BP not obtained obtained Sats 95% Phil Bernard, MD Baraff LJ, Bass JW, Fleisher GR, Klein JO, McCracken GH, Powell KR, et al. Practice
4/11/2017 COMMUNITY ACQUIRED PNEUMONIA. Disclaimer. A Review of How to Treat Common Infections in a Pediatric Patient. Objectives for Technicians
 Disclaimer A Review of How to Treat Common Infections in a Pediatric Patient Tara Bergland reports that she has no actual or potential conflict of interest in relation to this presentation. Off label use
Disclaimer A Review of How to Treat Common Infections in a Pediatric Patient Tara Bergland reports that she has no actual or potential conflict of interest in relation to this presentation. Off label use
Fever in the Pediatric Office Practice
 Fever in the Pediatric Office Practice Jane Murahovschi J Pediatr (Rio J) 2003; 79 Suppl 1:S55-S64 Lester A. Deniega, M.D. Abstract Objective: 1. To determine how to select a child who requires in depth
Fever in the Pediatric Office Practice Jane Murahovschi J Pediatr (Rio J) 2003; 79 Suppl 1:S55-S64 Lester A. Deniega, M.D. Abstract Objective: 1. To determine how to select a child who requires in depth
GUIDELINE FOR THE MANAGEMENT OF MENINGITIS. All children with suspected or confirmed meningitis
 GUIDELINE FOR THE MANAGEMENT OF MENINGITIS Reference: Mennigitis Version No: 1 Applicable to All children with suspected or confirmed meningitis Classification of document: Area for Circulation: Author:
GUIDELINE FOR THE MANAGEMENT OF MENINGITIS Reference: Mennigitis Version No: 1 Applicable to All children with suspected or confirmed meningitis Classification of document: Area for Circulation: Author:
Haemophilus influenzae
 Haemophilus influenzae type b Severe bacterial infection, particularly among infants During late 19th century believed to cause influenza Immunology and microbiology clarified in 1930s Haemophilus influenzae
Haemophilus influenzae type b Severe bacterial infection, particularly among infants During late 19th century believed to cause influenza Immunology and microbiology clarified in 1930s Haemophilus influenzae
Pediatric Mysteries (including FWS / FUO) 13 June 2017 Tony Moody MD Duke Pediatric Infectious Diseases
 13 June 2017 Tony Moody MD Duke Pediatric Infectious Diseases") Pediatric Mysteries (including FWS / FUO) 13 June 2017 Tony Moody MD Duke Pediatric Infectious Diseases Disclosures Advisory board member for GSK (for belimumab pregnancy registry). Co-founder of Grid
Pediatric Mysteries (including FWS / FUO) 13 June 2017 Tony Moody MD Duke Pediatric Infectious Diseases Disclosures Advisory board member for GSK (for belimumab pregnancy registry). Co-founder of Grid
FEVER. What is fever?
 FEVER What is fever? Fever is defined as a rectal temperature 38 C (100.4 F), and a value >40 C (104 F) is called hyperpyrexia. Body temperature fluctuates in a defined normal range (36.6-37.9 C [97.9-100.2
FEVER What is fever? Fever is defined as a rectal temperature 38 C (100.4 F), and a value >40 C (104 F) is called hyperpyrexia. Body temperature fluctuates in a defined normal range (36.6-37.9 C [97.9-100.2
Pediatric and Adolescent Infectious Disease Concerns
 Pediatric and Adolescent Infectious Disease Concerns Sean P. Elliott, MD Professor of Pediatrics Associate Chair of Education, Department of Pediatrics University of Arizona College of Medicine Tucson,
Pediatric and Adolescent Infectious Disease Concerns Sean P. Elliott, MD Professor of Pediatrics Associate Chair of Education, Department of Pediatrics University of Arizona College of Medicine Tucson,
Epidemiology of Infectious Complications of H1N1 Influenza Virus Infection
 Epidemiology of Infectious Complications of H1N1 Influenza Virus Infection Lyn Finelli, DrPH, MS Lead, Influenza Surveillance and Outbreak Response Epidemiology and Prevention Branch Influenza Division
Epidemiology of Infectious Complications of H1N1 Influenza Virus Infection Lyn Finelli, DrPH, MS Lead, Influenza Surveillance and Outbreak Response Epidemiology and Prevention Branch Influenza Division
Pneumococcal Disease and Pneumococcal Vaccines
 Pneumococcal Disease and Epidemiology and Prevention of - Preventable Diseases Note to presenters: Images of vaccine-preventable diseases are available from the Immunization Action Coalition website at
Pneumococcal Disease and Epidemiology and Prevention of - Preventable Diseases Note to presenters: Images of vaccine-preventable diseases are available from the Immunization Action Coalition website at
REVIEW ARTICLE. Occult Serious Bacterial Infection in Infants Younger Than 60 to 90 Days With Bronchiolitis
 REVIEW ARTICLE Occult Serious Bacterial Infection in Infants Younger Than 60 to 90 Days With A Systematic Review Shawn Ralston, MD; Vanessa Hill, MD; Ami Waters, MD Objective: To summarize the risk of
REVIEW ARTICLE Occult Serious Bacterial Infection in Infants Younger Than 60 to 90 Days With A Systematic Review Shawn Ralston, MD; Vanessa Hill, MD; Ami Waters, MD Objective: To summarize the risk of
Bronchitis/Pneumonia Core Content Keith Conover, M.D., FACEP /15/02 Clinical Spectrum Chest pain, shoulder pain, neck pain, abdominal pain,
 Bronchitis/Pneumonia Core Content Keith Conover, M.D., FACEP 1.0 10/15/02 Clinical Spectrum Chest pain, shoulder pain, neck pain, abdominal pain, headache Links with smoking, pollen count, FH of asthma
Bronchitis/Pneumonia Core Content Keith Conover, M.D., FACEP 1.0 10/15/02 Clinical Spectrum Chest pain, shoulder pain, neck pain, abdominal pain, headache Links with smoking, pollen count, FH of asthma
Reactive Thrombocytosis in Febrile Young Infants with Serious Bacterial Infection
 R E S E A R C H P A P E R Reactive Thrombocytosis in Febrile Young Infants with Serious Bacterial Infection S FOUZAS, L MANTAGOU, E SKYLOGIANNI AND A VARVARIGOU From the Department of Pediatrics, University
R E S E A R C H P A P E R Reactive Thrombocytosis in Febrile Young Infants with Serious Bacterial Infection S FOUZAS, L MANTAGOU, E SKYLOGIANNI AND A VARVARIGOU From the Department of Pediatrics, University
4/11/2017. A Review of How to Treat Common Infections in a Pediatric Patient. Disclaimer. Objectives for Pharmacists
 A Review of How to Treat Common Infections in a Pediatric Patient Tara Bergland, Pharm D. PGY2 Pediatric Pharmacy Resident Tara-bergland@uiowa.edu Disclaimer Tara Bergland reports that she has no actual
A Review of How to Treat Common Infections in a Pediatric Patient Tara Bergland, Pharm D. PGY2 Pediatric Pharmacy Resident Tara-bergland@uiowa.edu Disclaimer Tara Bergland reports that she has no actual
Pediatric urinary tract infection. Dr. Nariman Fahmi Pediatrics/2013
 Pediatric urinary tract infection Dr. Nariman Fahmi Pediatrics/2013 objectives EPIDEMIOLOGY CAUSATIVE PATHOGENS PATHOGENESIS CATEGORIES OF URINARY TRACT INFECTIONS AND CLINICAL MANIFESTATIONS IN pediatrics
Pediatric urinary tract infection Dr. Nariman Fahmi Pediatrics/2013 objectives EPIDEMIOLOGY CAUSATIVE PATHOGENS PATHOGENESIS CATEGORIES OF URINARY TRACT INFECTIONS AND CLINICAL MANIFESTATIONS IN pediatrics
Maternal Immunization Efficacy and Safety Saad B. Omer
 Maternal Immunization Efficacy and Safety Saad B. Omer William H. Foege Professor of Global Health Professor of Epidemiology & Pediatrics Emory University, Schools of Public Health & Medicine Pregnancy
Maternal Immunization Efficacy and Safety Saad B. Omer William H. Foege Professor of Global Health Professor of Epidemiology & Pediatrics Emory University, Schools of Public Health & Medicine Pregnancy
Updates in: Pediatric Emergency Medicine
 Updates in: Pediatric Emergency Medicine EDWARD P. JUNKINS, JR, MD, MPH, FAAP ASSOCIATE DEAN, ACADEMIC AFFAIRS PROFESSOR, DEPARTMENT OF PEDIATRICS WESTERN UNIVERSITY OF HEALTH SCIENCES Conflicts of Interest
Updates in: Pediatric Emergency Medicine EDWARD P. JUNKINS, JR, MD, MPH, FAAP ASSOCIATE DEAN, ACADEMIC AFFAIRS PROFESSOR, DEPARTMENT OF PEDIATRICS WESTERN UNIVERSITY OF HEALTH SCIENCES Conflicts of Interest
BRIEF CASE ACUTE PNEUMONIA RESPIRATORY TRACT INFECTIONS MAJOR VIRAL RESPIRATORY PATHOGENS WHAT SPECIMENS SHOULD BE SENT TO R/O VIRAL INFECTION?
 RESPIRATORY TRACT INFECTIONS BRIEF CASE LABORATORY MEDICINE COURSE 2004 CLINICAL MICROBIOLOGY SERVICE WHAT IS THE DIFFERENTIAL? WHAT TESTS TO ORDER? INTERPRETATION & EVALUATION Dr. Preeti Pancholi 5-6237
RESPIRATORY TRACT INFECTIONS BRIEF CASE LABORATORY MEDICINE COURSE 2004 CLINICAL MICROBIOLOGY SERVICE WHAT IS THE DIFFERENTIAL? WHAT TESTS TO ORDER? INTERPRETATION & EVALUATION Dr. Preeti Pancholi 5-6237
5/23/14. Febrile seizures: Who need further workup? Afebrile seizures: Who needs imaging? Status epilepticus: Most effective treatments
 Febrile seizures: Who need further workup? Afebrile seizures: Who needs imaging? Status epilepticus: Most effective treatments Andi Marmor, MD, MSEd Associate Professor, Pediatrics University of California,
Febrile seizures: Who need further workup? Afebrile seizures: Who needs imaging? Status epilepticus: Most effective treatments Andi Marmor, MD, MSEd Associate Professor, Pediatrics University of California,
Pediatric Respiratory Infections
 Pediatric Respiratory Infections Brenda Kelly PharmD BCPS Residency Program Director Virginia Mason Memorial, Yakima, Washington brendakelly@yvmh.org Disclosure The presenter has no actual or potential
Pediatric Respiratory Infections Brenda Kelly PharmD BCPS Residency Program Director Virginia Mason Memorial, Yakima, Washington brendakelly@yvmh.org Disclosure The presenter has no actual or potential
Does This Child Have a Urinary Tract Infection?
 EVIDENCE-BASED EMERGENCY MEDICINE/RATIONAL CLINICAL EXAMINATION ABSTRACT Does This Child Have a Urinary Tract Infection? EBEM Commentator Contact Rupinder Singh Sahsi, BSc, MD Christopher R. Carpenter,
EVIDENCE-BASED EMERGENCY MEDICINE/RATIONAL CLINICAL EXAMINATION ABSTRACT Does This Child Have a Urinary Tract Infection? EBEM Commentator Contact Rupinder Singh Sahsi, BSc, MD Christopher R. Carpenter,
Urinary Tract Infections in Infants & Toddlers: An Evidence-based Approach. No disclosures. Importance of Topic 5/14/11. Biases
 Urinary Tract Infections in Infants & Toddlers: An Evidence-based Approach Thomas B. Newman, MD, MPH Professor of Epidemiology & Biostatistics and Pediatrics University of California, San Francisco May
Urinary Tract Infections in Infants & Toddlers: An Evidence-based Approach Thomas B. Newman, MD, MPH Professor of Epidemiology & Biostatistics and Pediatrics University of California, San Francisco May
Rebecca T Slagle, MN, APRN, NNP-BC. Speak up!!
 Rebecca T Slagle, MN, APRN, NNP-BC Speak up!! Objectives: Understand the incidence and prevalence of sepsis in the newborn period Identify the risk factors for neonatal sepsis List the most frequent causative
Rebecca T Slagle, MN, APRN, NNP-BC Speak up!! Objectives: Understand the incidence and prevalence of sepsis in the newborn period Identify the risk factors for neonatal sepsis List the most frequent causative
Neutropenic Fever. CID 2011; 52 (4):e56-e93
:e56-e93") Neutropenic Fever www.idsociety.org CID 2011; 52 (4):e56-e93 Definitions Fever: Single oral temperature of 101 F (38.3 C) Temperature 100.4 F (38.0 C) over 1 hour Neutropenia: ANC < 500 cells/mm 3 Expected
Neutropenic Fever www.idsociety.org CID 2011; 52 (4):e56-e93 Definitions Fever: Single oral temperature of 101 F (38.3 C) Temperature 100.4 F (38.0 C) over 1 hour Neutropenia: ANC < 500 cells/mm 3 Expected
Online Video Library Pediatric Emergency Room Puzzlers
 Outreach Education Online Video Library 2009-2010... Pediatric Emergency Room Puzzlers.... Program Handouts This information is provided as a courtesy by Children's Health Care System and its related organizations
Outreach Education Online Video Library 2009-2010... Pediatric Emergency Room Puzzlers.... Program Handouts This information is provided as a courtesy by Children's Health Care System and its related organizations
PEDIATRIC INFECTIOUS DISEASES UPDATE. Neonatal HSV. Recognition, Diagnosis, and Management Coleen Cunningham MD
 Neonatal HSV Recognition, Diagnosis, and Management Coleen Cunningham MD Important questions Who is at risk? When do you test? What tests do you perform? When do you treat? What is appropriate therapy?
Neonatal HSV Recognition, Diagnosis, and Management Coleen Cunningham MD Important questions Who is at risk? When do you test? What tests do you perform? When do you treat? What is appropriate therapy?
INFECTIONS IN KIDS TO TREAT OR NOT TO TREAT?
 INFECTIONS IN KIDS TO TREAT OR NOT TO TREAT? I HAVE NOTHING TO DISCLOSE. Andi Marmor, MD, MSED Professor of Pediatrics University of California, San Francisco Zuckerberg San Francisco General Hospital
INFECTIONS IN KIDS TO TREAT OR NOT TO TREAT? I HAVE NOTHING TO DISCLOSE. Andi Marmor, MD, MSED Professor of Pediatrics University of California, San Francisco Zuckerberg San Francisco General Hospital
Family Centered Pediatric Emergency Department Sickle Cell Assessment of Needs and Strengths (FC-Peds-ED-SCANS) Overall Algorithm
 Overall Algorithm") Family Centered Pediatric Emergency Department Sickle Cell Assessment of Needs and Strengths (FC-Peds-ED-SCANS) Overall Algorithm Decision 1: Triage Decision 2: Analgesic Management Decision 3: Diagnostic
Family Centered Pediatric Emergency Department Sickle Cell Assessment of Needs and Strengths (FC-Peds-ED-SCANS) Overall Algorithm Decision 1: Triage Decision 2: Analgesic Management Decision 3: Diagnostic
Fever accounts for 10% to 20% of all pediatric emergency department
 CME REVIEW ARTICLE Update for the 21st Century Christopher Woll, MD,* Mark I. Neuman, MD, MPH, and Paul L. Aronson, MD* Abstract: Infants aged 90 days or younger with fever are frequently evaluated in
CME REVIEW ARTICLE Update for the 21st Century Christopher Woll, MD,* Mark I. Neuman, MD, MPH, and Paul L. Aronson, MD* Abstract: Infants aged 90 days or younger with fever are frequently evaluated in
Controversies in Diagnosis and Therapy of Neonatal Sepsis
 Controversies in Diagnosis and Therapy of Neonatal Sepsis Sarah S. Long, M.D. Professor of Pediatrics Drexel University College of Medicine Chief, Section of Infectious Diseases St. Christopher s Hospital
Controversies in Diagnosis and Therapy of Neonatal Sepsis Sarah S. Long, M.D. Professor of Pediatrics Drexel University College of Medicine Chief, Section of Infectious Diseases St. Christopher s Hospital