Pediatric Airway Emergencies
|
|
|
- Nickolas Jessie Small
- 6 years ago
- Views:
Transcription
1 Pediatric Airway Emergencies The University of Texas Medical Branch Department of Otolaryngology, Grand Rounds Presentation November 23, 2005 Steven T. Wright, M.D. Faculty Advisor: Seckin Ulualp, M.D.
2 ASA Task Force on Management of the Difficult Airway - Definitions: difficult airway = the clinical situation in which a conventionally trained anesthesiologist experiences difficulty with mask ventilation, difficulty with tracheal intubation, or both. difficult mask ventilation = (1) inability of unassisted anesthesiologist to maintain SpO2 > 90% using 100% oxygen and positive pressure mask ventilation in a patient whose SpO2 was 90% before anesthetic intervention; or (2) inability of the unassisted anesthesiologist to prevent or reverse signs of inadequate ventilation during positive pressure mask ventilation. difficult laryngoscopy = not being able to see any part of the vocal cords with conventional laryngoscopy difficult intubation = proper insertion with conventional laryngoscopy requires either (1) more than three attempts or (2) more than ten minutes
3 Pediatric PeriOperative Cardiac Arrest (POCA) Registry Collects data from 63 large institutions to correlate perioperative pediatric deaths and anesthesia The majority are medication related cardiac deaths : Respiratory events increased from 20 percent to 27 percent. The most common event leading to cardiac arrest in this category was laryngospasm, followed by airway obstruction, inadequate oxygenation, inadvertent extubation, difficult intubation and bronchospasm.

4 Pediatric Airway Emergencies Infrequently encountered Stridor History and Physical Examination Multiple Etiologies Congenital Inflammatory Iatrogenic Neoplastic Traumatic

 including tracheostomy and")
5 Urgency Must assess the urgency of the situation Full and frank discussion of the risks with the parents (and child if appropriate) including tracheostomy and failure to secure the airway
6 Infant larynx: -More superior in neck -Epiglottis shorter, angled more over glottis -Vocal cords slanted: anterior commissure more inferior - Vocal process 50% of length -Larynx cone-shaped: narrowest at subglottic cricoid ring -Softer, more pliable: may be gently flexed or rotated anteriorly Infant tongue is larger Head is naturally flexed Anatomy


7 History Assess the urgency of the situation Simultaneous History and Physical Choking Aggravating factors Feeding, sleeping, positioning Throat or neck pain Birth history Prenatal
8 Signs of impending respiratory failure Increased respiratory rate Nasal flaring Use of accessory muscles Cyanosis

9 Stertor Physical Examination Stridor Bulky oropharyngeal noise Inspiratory, expiratory, or both Supraglottic Inspiratory Glottic Inspiratory progressing to biphasic Subglottic Inspiratory progressing to biphasic Tracheal Expiratory

10 Flexible Laryngoscopy: Proper Equipment Assess nares/choanae Assess adenoid and lingual tonsil Assess TVC mobility Assess laryngeal structures

11 Plain films: Radiology: Chest and airway AP and lateral Expiratory films
12 Airway Flouroscopy Quick, noninvasive, and dynamic study Supraglottic: 33% Glottic: 17% Subglottic: 80% Tracheal: 73% Bronchial: 80% Far superior to plain films Disadv: radiation exposure 10 rads (0.1Gy) per 1 minute



13 MRI/CT Usually not useful in an acute setting More reliable for evaluating neck masses and congenital anomalies of the lower airway and vascular system
14 Treatment Options Heliox Oral Airways Intubation Endotracheal Laryngeal Mask Tracheostomy EXIT procedure

15 Heliox Graham s Law: flow rate is inversely proportional to the square root of its density Helium 7x less dense than Nitrogen Shown to be effective in upper airway obstruction, viral croup, postextubation stridor
16 Heliox Gosz et al: Immediate positive response in 73% of patients Average duration of treatment 15min to 384 hours (overall mean of 29.1hrs) Laryngotracheobronchitis were more likely to respond than other causes. (other causes were upper airway obstruction, postextubation stridor, congenital heart disease)
17 Endotracheal Intubation Multicenter study 156 out of 1288 total ED intubations Rapid Sequence Intubation (81%) Without medications (16%) Sedation without neuromuscular blockade (6%) Overall successful intubations RSI 99% Non RSI 97% Only 1 out of 156 required surgical intervention
18 Rapid Sequence Intubation Recommended for every emergency intubation involving a child with intact upper airway reflexes by the Pediatric Emergency Medicine Committee of the American College of Emergency Physicians Simultaneous administration of a neuromuscular blockade agent and a sedative
19 Intubation Rule of 4 s: Age+4/4 = ETT size Mucosal injury at 25cm of pressure. Therefore, always check for leak. Spontaneous ventilation: allows for a limited examination of the dynamics of vocal cord motion. Apneic technique: Turn to FiO2 100% prior to extubation. 6L O2/min flow via laryngoscope General rule to work apneic in a proportional amount of time as reoxygenation.

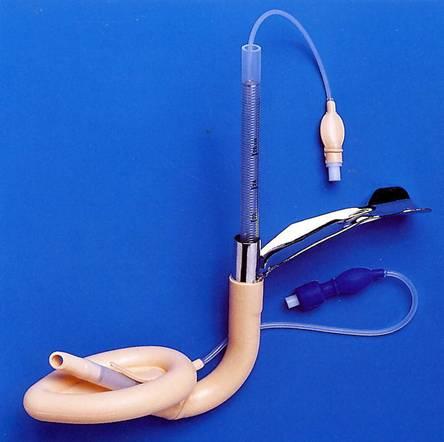

20 Laryngeal Mask Airway


21 Tracheotomy Cricothyroidotomy is difficult b/c of small membrane and flexibility Early complications Pneumothorax, bleeding, decannulation, obstruction, infections Late complications Granuloma, decannulation, SGS, tracheocutaneous fistula

22 EXIT Procedure (ex utero intrapartum treatment) Prenatal diagnosis is crucial Flattened diaphragms, polyhydramnios The head, neck, thorax, and one arm are delivered. Uteroplacental circulation can be maintained for minutes
23 Specific Etiologies of Airway Emergencies Congenital Neck Masses Congenital anomalies Syndromic patients Inflammatory Foreign Bodies
24 Congenital Neck Masses Dermoid cysts Mesoderm/ectoderm Teratoid cysts and teratomas All 3 layers 20% incidence of maternal polyhydramnios
25 Congenital Neck Masses Lymphangiomas Capillary, cavernous, cystic types More airway obstructive when found in the anterior triangle
26 CHAOS (congenital high airway obstruction syndrome) Emergent airway management at the time of delivery is key for survival Prenatally Flattened diaphragms, polyhydramnios, cervical mass TEAM Members Maternal-fetal specialist Neonatalogist Anesthesiologist Otolaryngologist Patient
27 Laryngotracheobronchitis Parainfluenza type 1 Generalized mucosal edema of the larynx, trachea, bronchi (Croup)
28 Laryngotracheobronchitis Treatment Humidification No scientific data to support May worsen the situation Racemic Epinephrine Reduces mucosal edema/bronchial relaxation Steroids Systemic vs. Inhaled Intubation

29 Bacterial Tracheitis Complication of viral laryngotracheobronch itis Fever, white count, respiratory distress following a complicated course of croup Staphylococcus aureus Endoscopy and Intubation


30 Acute Supraglottitis Mild URI that progresses over a few hours to severe throat pain, drooling, and fever H. influenza, parainfluenza Treatment Intubation Empiric Abx
31 Congenital Syndromes Close embryological development of the airways and the craniofacial structures Early complications are usually more profound Late complications may be more subtle
32 Congenital Syndromes and Airway Emergencies Syndromes of facial anomalies Pierre Robin Sequence Treacher Collins Goldenhar/Hemifacial microsomia Deformities of skull shape Crouzon s/apert s Pfieffer


33 Pierre Robin Sequence Micrognathia, relative macroglossia with or without cleft palate Intubation via the lateral tongue approach Tracheotomy Glossopexy Subperiosteal release of mandible
34 Hypoplastic cheeks, zygomatic arches, and mandible; Microtia with possible hearing loss; High arched or cleft palate; Macrostomia (abnormally large mouth); Colobomas; Increased anterior facial height; Malocclusion (anterior open bite); Small oral cavity and airway with a normal-sized tongue; Treacher Collins
35 Goldenhar & Hemifacial Microsomia Oculoauricular dysplasia Limited atlanto-occipital extension
36 Klippel-Feil Congential fusion of any 2 of the 7 cervical vertebrae Short, immobile neck
37 Crouzon s/ Apert s Abnormal closure of the cranial sutures Nasal cavity Nasophayrngeal stenosis- leads to OSA Associated anomalies SGS Tracheal sleeves Treatment Nasal decongestants/ stents Selective adenoid/tonsillectomy Tracheostomy Midface advancement

38 Mucopolysaccharidoses Hunter s, Hurler s, Marateaux-Lamy Progressive infiltration of MPS within the airway structures Treatment Tracheostomy Death by age 10-15
39 Down s Syndrome Midface hypoplasia, macroglossia, narrow nasopharynx, and shortened palate. Immature immune system Tendency towards obesity GERD is very prominent Equals a very difficult patient to sedate and still maintain an airway Longer lifespan of these patients leads to an increase in the incidence of CHF and pulmonary hypertension secondary to OSA
40 Down s Syndrome Mitchell et al. 23 Downs Patients 48% OSA 43% Laryngomalacia Systemic comorbidities 61% GERD Cause of Upper airway obstruction is age related <2yrs old: laryngomalacia is most common cause Age dependent progression to OSA >2yrs old: OSA is most common cause Delay in diagnosis is common because symptoms overlap
41 Down s Syndrome Jacobs et al. 55 of 71 patients underwent upper airway surgery (all had DL/B at the same time) 44 T&A with pillar plication, 4 UPPP Overall: 76% had significant or complete relief 24% had moderate or severe residual symptoms Failures: Greater number of obstructive sites Laryngotracheal stenosis (23% of failures) Tongue base More severe UAO Recommendations: Comprehensive preoperative airway evaluation Tailor the surgical procedure for the site of obstruction Close follow up for failures

42 Choanal Atresia Failure of the breakdown of the buccopharyngel membrane McGovern Nipple and nasogastric feeding CHARGE association Colobomas Heart abnormalities Renal anomalies Genital abnormalities Ear abnormalities
43 Foreign Bodies 2-4year olds Acute episode of choking/gagging Triad of acute wheeze, cough and unilateral diminished sounds only in 50% 5-40% of patients manifest no obvious signs

44 Foreign Bodies Severity is determined by complete vs partial obstruction Peanuts are most common Right mainstem Larger diameter More airflow than left Narrow angle of divergence Carina sits on the left side

45 Foreign Bodies
46 Foreign Bodies Plain radiography: 25% of bronchial lesions and >50% of tracheal lesions do not show up Airway Flouroscopy: Above the carina: 32-40% Below the carina: 80-90% DL/B: Gold Standard


47 Airway Foreign Bodies
Upper Airway Obstruction
 Upper Airway Obstruction Adriaan Pentz Division of Otorhinolaryngology University of Stellenbosch and Tygerberg Hospital Stridor/Stertor Auditory manifestations of disordered respiratory function ie noisy
Upper Airway Obstruction Adriaan Pentz Division of Otorhinolaryngology University of Stellenbosch and Tygerberg Hospital Stridor/Stertor Auditory manifestations of disordered respiratory function ie noisy
Stridor, Stertor, and Snoring: Pediatric Upper Airway Obstruction. Nathan Page, MD Pediatrics in the Red Rocks June?
 Stridor, Stertor, and Snoring: Pediatric Upper Airway Obstruction Nathan Page, MD Pediatrics in the Red Rocks June? I have no disclosures I do not plan to discuss unapproved or off label use of products
Stridor, Stertor, and Snoring: Pediatric Upper Airway Obstruction Nathan Page, MD Pediatrics in the Red Rocks June? I have no disclosures I do not plan to discuss unapproved or off label use of products
THE DIFFICULT PEDIATRIC AIRWAY. Learning Objectives. The Pediatric Airway 6/7/18. Jason W. Gatling, MD Department of Anesthesiology June 7, 2018
 THE DIFFICULT PEDIATRIC AIRWAY Jason W. Gatling, MD Department of Anesthesiology June 7, 2018 Learning Objectives At the conclusion of this activity, the participants should be able to: 1. Describe what
THE DIFFICULT PEDIATRIC AIRWAY Jason W. Gatling, MD Department of Anesthesiology June 7, 2018 Learning Objectives At the conclusion of this activity, the participants should be able to: 1. Describe what
Anesthetic consideration in Clefts & Craniofacial surgery
 Anesthetic consideration in Clefts & Craniofacial surgery พญ.เด อนเพ ญ ห อร ตนาเร อง ภาคว ชาว ส ญญ ว ทยา คณะแพทย แพทยศาสตร มหาว ทยาล ยขอนแก น Preoperative evaluation Cleft lip & Cleft palate reconstruction
Anesthetic consideration in Clefts & Craniofacial surgery พญ.เด อนเพ ญ ห อร ตนาเร อง ภาคว ชาว ส ญญ ว ทยา คณะแพทย แพทยศาสตร มหาว ทยาล ยขอนแก น Preoperative evaluation Cleft lip & Cleft palate reconstruction
Pediatric Airway Emergencies November 2005
 TITLE: Pediatric Airway Emergencies SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: November 23, 2005 RESIDENT PHYSICIAN: Steven Wright, MD FACULTY ADVISOR: Seckin Ulualp, MD SERIES
TITLE: Pediatric Airway Emergencies SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: November 23, 2005 RESIDENT PHYSICIAN: Steven Wright, MD FACULTY ADVISOR: Seckin Ulualp, MD SERIES
STRIDOR. Respiratory system. Lecture
 STRIDOR Stridor is a continuous inspiratory harsh sound produced by partial obstruction in the region of the larynx or trachea. Total obstruction cyanosis & death. Etiology Acute stridor Infectious croup
STRIDOR Stridor is a continuous inspiratory harsh sound produced by partial obstruction in the region of the larynx or trachea. Total obstruction cyanosis & death. Etiology Acute stridor Infectious croup
Pediatric Airway Disorders Speaker Disclosure Outline
 Pediatric Airway Disorders G. Paul Digoy, M.D. Director of Pediatric Otolaryngology OU Health Sciences Center Paul-Digoy@ouhsc.edu Office: 405 271-5504 Speaker Disclosure Speakers, moderators, or panelists
Pediatric Airway Disorders G. Paul Digoy, M.D. Director of Pediatric Otolaryngology OU Health Sciences Center Paul-Digoy@ouhsc.edu Office: 405 271-5504 Speaker Disclosure Speakers, moderators, or panelists
Evaluation and Management of Pediatric Stridor
 Evaluation and Management of Pediatric Stridor Pamela Nicklaus, MD FACS Associate Professor Fellowship Director Pediatric Otolaryngology Children s Mercy Hospital and Clinics 2013 Children's 2013 Mercy
Evaluation and Management of Pediatric Stridor Pamela Nicklaus, MD FACS Associate Professor Fellowship Director Pediatric Otolaryngology Children s Mercy Hospital and Clinics 2013 Children's 2013 Mercy
Neonatal Airway Disorders, Treatments, and Outcomes. Steven Goudy, MD Pediatric Otolaryngology Emory University Medical Center
 Neonatal Airway Disorders, Treatments, and Outcomes Steven Goudy, MD Pediatric Otolaryngology Emory University Medical Center Disclosure I have nothing to disclose Neonatal and Pediatric Tracheostomy Tracheostomy
Neonatal Airway Disorders, Treatments, and Outcomes Steven Goudy, MD Pediatric Otolaryngology Emory University Medical Center Disclosure I have nothing to disclose Neonatal and Pediatric Tracheostomy Tracheostomy
Multilevel airway obstruction including rare tongue base mass presenting as severe croup in an infant. Tara Brennan, MD 2,3
 Multilevel airway obstruction including rare tongue base mass presenting as severe croup in an infant Tara Brennan, MD 2,3 Jeffrey C. Rastatter, MD, FAAP 1,2 1 Department of Otolaryngology, Northwestern
Multilevel airway obstruction including rare tongue base mass presenting as severe croup in an infant Tara Brennan, MD 2,3 Jeffrey C. Rastatter, MD, FAAP 1,2 1 Department of Otolaryngology, Northwestern
Angkana Lurngnateetape,, MD. Department of Anesthesiology Siriraj Hospital
 AIRWAY MANAGEMENT Angkana Lurngnateetape,, MD. Department of Anesthesiology Siriraj Hospital Perhaps the most important responsibility of the anesthesiologist is management of the patient s airway Miller
AIRWAY MANAGEMENT Angkana Lurngnateetape,, MD. Department of Anesthesiology Siriraj Hospital Perhaps the most important responsibility of the anesthesiologist is management of the patient s airway Miller
Pre anaesthetic evaluation of difficult tracheal intubation
 Pre anaesthetic evaluation of difficult tracheal intubation Dr. AL. Meenakshi Sundaram M.D., D.A., GC Member,ISA National Professor of Anesthesiology Thanjavur Medical College Thanjavur, TamilNadu Phone:
Pre anaesthetic evaluation of difficult tracheal intubation Dr. AL. Meenakshi Sundaram M.D., D.A., GC Member,ISA National Professor of Anesthesiology Thanjavur Medical College Thanjavur, TamilNadu Phone:
Subject Index. Bacterial infection, see Suppurative lung disease, Tuberculosis
 Subject Index Abscess, virtual 107 Adenoidal hypertrophy, features 123 Airway bleeding, technique 49, 50 Airway stenosis, see Stenosis, airway Anaesthesia biopsy 47 complications 27, 28 flexible 23 26
Subject Index Abscess, virtual 107 Adenoidal hypertrophy, features 123 Airway bleeding, technique 49, 50 Airway stenosis, see Stenosis, airway Anaesthesia biopsy 47 complications 27, 28 flexible 23 26
REVERSE LMA INSERTION IN A NEONATE WITH KLIPPEL-FEIL SYNDROME
 REVERSE LMA INSERTION IN A NEONATE WITH KLIPPEL-FEIL SYNDROME - Case report - TARIQ AL ZAHRANI * Klippel-Feil syndrome (KFS) was first described by Maurice Klippel and Andre Feil in 1912 in a patient with
REVERSE LMA INSERTION IN A NEONATE WITH KLIPPEL-FEIL SYNDROME - Case report - TARIQ AL ZAHRANI * Klippel-Feil syndrome (KFS) was first described by Maurice Klippel and Andre Feil in 1912 in a patient with
AIRWAY MANAGEMENT SUZANNE BROWN, CRNA
 AIRWAY MANAGEMENT SUZANNE BROWN, CRNA OBJECTIVE OF LECTURE Non Anesthesia Sedation Providers Review for CRNA s Informal Questions encouraged 2 AIRWAY MANAGEMENT AWARENESS BASICS OF ANATOMY EQUIPMENT 3
AIRWAY MANAGEMENT SUZANNE BROWN, CRNA OBJECTIVE OF LECTURE Non Anesthesia Sedation Providers Review for CRNA s Informal Questions encouraged 2 AIRWAY MANAGEMENT AWARENESS BASICS OF ANATOMY EQUIPMENT 3
4. Neoplastic: benign & malignant. 5. Allergic rhinitis & nasal polyp. 6. hypertrophied tonsils or adenoids. L 5
 L 5 Stertor& Stridor Stertor& stridor are both auditory manifestation of disordered respiratory function. Stertor: Is a low pitched snoring or snuffly sound caused by obstruction of the airway above the
L 5 Stertor& Stridor Stertor& stridor are both auditory manifestation of disordered respiratory function. Stertor: Is a low pitched snoring or snuffly sound caused by obstruction of the airway above the
Sohit Paul Kanotra M.D. Director, Pediatric Aerodigestive Center
 Sohit Paul Kanotra M.D. Director, Pediatric Aerodigestive Center Children s Hospital of New Orleans Assistant Professor, Otolaryngology-Head & Neck Surgery, Louisiana State University. I do not have any
Sohit Paul Kanotra M.D. Director, Pediatric Aerodigestive Center Children s Hospital of New Orleans Assistant Professor, Otolaryngology-Head & Neck Surgery, Louisiana State University. I do not have any
Respiratory Management in Pediatrics
 Respiratory Management in Pediatrics Children s Hospital Omaha Critical Care Transport Sue Holmer RN, C-NPT Objectives Examine the differences between the pediatric and adults airways. Recognize respiratory
Respiratory Management in Pediatrics Children s Hospital Omaha Critical Care Transport Sue Holmer RN, C-NPT Objectives Examine the differences between the pediatric and adults airways. Recognize respiratory
Pediatric Difficult Airway Management. R2 Nichakan Rewurai R2 Pattiya Suttidate Supervisor: Assist. Prof. Sahatsa Mandee
 Pediatric Difficult Airway Management R2 Nichakan Rewurai R2 Pattiya Suttidate Supervisor: Assist. Prof. Sahatsa Mandee The pediatric difficult airway is associated with a high risk for complications during
Pediatric Difficult Airway Management R2 Nichakan Rewurai R2 Pattiya Suttidate Supervisor: Assist. Prof. Sahatsa Mandee The pediatric difficult airway is associated with a high risk for complications during
Basic Science Review Wound Healing
 Subglottic Stenosis Deborah P. Wilson, M.D. Faculty Advisor: Norman Friedman, M.D. The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation April 14, 1999 Basic Science
Subglottic Stenosis Deborah P. Wilson, M.D. Faculty Advisor: Norman Friedman, M.D. The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation April 14, 1999 Basic Science
Recognizing the Difficult Airway in Pediatric Patients. Nancy L. Glass, MD, MBA,
 Recognizing the Difficult Airway in Pediatric Patients Nancy L. Glass, MD, MBA, FAAP nglass@bcm.edu @DrNancyGlass1 None Disclosures Learning Objectives At the end of this presentation, participants will
Recognizing the Difficult Airway in Pediatric Patients Nancy L. Glass, MD, MBA, FAAP nglass@bcm.edu @DrNancyGlass1 None Disclosures Learning Objectives At the end of this presentation, participants will
Pediatric upper airway and congenital anomalies
 Anesthesiology Clin N Am 20 (2002) 747 766 Pediatric upper airway and congenital anomalies Andrew Infosino, MD Department of Anesthesia and Perioperative Care, University of California at San Francisco,
Anesthesiology Clin N Am 20 (2002) 747 766 Pediatric upper airway and congenital anomalies Andrew Infosino, MD Department of Anesthesia and Perioperative Care, University of California at San Francisco,
Stridor in Children. Agrício Nubiato Crespo and Rodrigo Cesar e Silva
 Stridor in Children Agrício Nubiato Crespo and Rodrigo Cesar e Silva Introduction Stridor can be defined as the audible sign produced by the turbulent air flow through a narrow segment of the respiratory
Stridor in Children Agrício Nubiato Crespo and Rodrigo Cesar e Silva Introduction Stridor can be defined as the audible sign produced by the turbulent air flow through a narrow segment of the respiratory
Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2
 Miss. kamlah 1 Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2 Acute Epiglottitis Is an infection of the epiglottis, the long narrow structure that closes off the glottis
Miss. kamlah 1 Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2 Acute Epiglottitis Is an infection of the epiglottis, the long narrow structure that closes off the glottis
When managing the airway of a pediatric patient,
 Lesson 242: PreAnesthetic Assessment of the Pediatric Patient With a Difficult Airway WRITTEN BY: Omar Saleh,* Amir Baluch, Bharat Dara, and Alan D. Kaye *Medical student, University of Mississippi School
Lesson 242: PreAnesthetic Assessment of the Pediatric Patient With a Difficult Airway WRITTEN BY: Omar Saleh,* Amir Baluch, Bharat Dara, and Alan D. Kaye *Medical student, University of Mississippi School
Objectives. Case Presentation. Respiratory Emergencies
 Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
Anatomy of the Airway
 Anatomy of the Airway Nagelhout, 5 th edition, Chapter 26 Morgan & Mikhail, 5 th edition, Chapter 23 Mary Karlet, CRNA, PhD Airway Anatomy The airway consists of the nose, pharynx, larynx, trachea, and
Anatomy of the Airway Nagelhout, 5 th edition, Chapter 26 Morgan & Mikhail, 5 th edition, Chapter 23 Mary Karlet, CRNA, PhD Airway Anatomy The airway consists of the nose, pharynx, larynx, trachea, and
October Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE
 October 2017 Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE This workbook is designed to introduce to you the difference between paediatric and adult anatomy and physiology. It will also give
October 2017 Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE This workbook is designed to introduce to you the difference between paediatric and adult anatomy and physiology. It will also give
Advanced Airway Management
 CHAPTER 37 Advanced Airway Management Airway Anatomy and Physiology Review Respiratory System: The Airway Respiratory System (Supine) Physiology: Factors of Adequate Breathing Functioning brainstem Open
CHAPTER 37 Advanced Airway Management Airway Anatomy and Physiology Review Respiratory System: The Airway Respiratory System (Supine) Physiology: Factors of Adequate Breathing Functioning brainstem Open
 Evaluation of the Airway A history and physical examination with specific reference to the airway should be performed in all children who require sedation or anesthesia. In particular, a history of a congenital
Evaluation of the Airway A history and physical examination with specific reference to the airway should be performed in all children who require sedation or anesthesia. In particular, a history of a congenital
Respiratory Anesthetic Emergencies in Oral and Maxillofacial Surgery. By: Lillian Han
 Respiratory Anesthetic Emergencies in Oral and Maxillofacial Surgery By: Lillian Han Background: Respiratory anesthetic emergencies are the most common complications during the administration of anesthesia
Respiratory Anesthetic Emergencies in Oral and Maxillofacial Surgery By: Lillian Han Background: Respiratory anesthetic emergencies are the most common complications during the administration of anesthesia
Pediatric Otolaryngology for Anesthetists followed by the delightful Airway Disorders in Infants and Children
 Pediatric Otolaryngology for Anesthetists followed by the delightful Airway Disorders in Infants and Children Andrew M. Shapiro, MD Private Practice, Pediatric Otolaryngology Clinical Associate Professor
Pediatric Otolaryngology for Anesthetists followed by the delightful Airway Disorders in Infants and Children Andrew M. Shapiro, MD Private Practice, Pediatric Otolaryngology Clinical Associate Professor
Advanced Airway Management. University of Colorado Medical School Rural Track
 Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
Diagnosis & Management of the Difficult Airway
 Diagnosis & Management of the Difficult Airway Dr. E. Rawlings Plymouth Anaesthetic Department Complications of Airway Management Medicolegal Serious morbidity Mortality Complications of Airway Management
Diagnosis & Management of the Difficult Airway Dr. E. Rawlings Plymouth Anaesthetic Department Complications of Airway Management Medicolegal Serious morbidity Mortality Complications of Airway Management
Unilateral Supraglottoplasty for Severe Laryngomalacia in Children. Nasser A Fageeh, MD, FRCSC, FACS*
 Bahrain Medical Bulletin, Vol. 37, No. 1, March 2015 Unilateral Supraglottoplasty for Severe Laryngomalacia in Children Nasser A Fageeh, MD, FRCSC, FACS* Objective: To study the efficacy of Unilateral
Bahrain Medical Bulletin, Vol. 37, No. 1, March 2015 Unilateral Supraglottoplasty for Severe Laryngomalacia in Children Nasser A Fageeh, MD, FRCSC, FACS* Objective: To study the efficacy of Unilateral
IAEM Clinical Guideline 9 Laryngomalacia. Version 1 September, Author: Dr Farah Mustafa
 IAEM Clinical Guideline 9 Laryngomalacia Version 1 September, 2016 Author: Dr Farah Mustafa Guideline lead: Dr Áine Mitchell, in collaboration with IAEM Clinical Guideline committee and Our Lady s Children
IAEM Clinical Guideline 9 Laryngomalacia Version 1 September, 2016 Author: Dr Farah Mustafa Guideline lead: Dr Áine Mitchell, in collaboration with IAEM Clinical Guideline committee and Our Lady s Children
Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018
 Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Andrea Losier OTTAWA ON 332 PEDS ER CASES Pediatric ED Cases
Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Andrea Losier OTTAWA ON 332 PEDS ER CASES Pediatric ED Cases
Section 4.1 Paediatric Tracheostomy Introduction
 Bite- sized training from the GTC Section 4.1 Paediatric Tracheostomy Introduction This is one of a series of bite- sized chunks of educational material developed by the Global Tracheostomy Collaborative.
Bite- sized training from the GTC Section 4.1 Paediatric Tracheostomy Introduction This is one of a series of bite- sized chunks of educational material developed by the Global Tracheostomy Collaborative.
Airway Workshop Lecture. University of Ottawa
 Airway Workshop Lecture Department of Anesthesiology University of Ottawa Overview Ventilation Airway assessment Difficult airways Airway management equipment aids Intubation/Improving Intubation Success
Airway Workshop Lecture Department of Anesthesiology University of Ottawa Overview Ventilation Airway assessment Difficult airways Airway management equipment aids Intubation/Improving Intubation Success
Airway/Breathing. Chapter 5
 Airway/Breathing Chapter 5 Airway/Breathing Introduction Skillful, rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur
Airway/Breathing Chapter 5 Airway/Breathing Introduction Skillful, rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur
Dr.Bharghavi.M 2 nd year post graduate Dept of Anaesthesia
 DIFFICULT AIRWAY CANNOT VENTILATE, CANNOT INTUBATE. Dr.Bharghavi.M 2 nd year post graduate Dept of Anaesthesia Difficult airway According to AMERICAN SOCIETY OF ANAESTHESIOLOGISTS Difficult Airway is defined
DIFFICULT AIRWAY CANNOT VENTILATE, CANNOT INTUBATE. Dr.Bharghavi.M 2 nd year post graduate Dept of Anaesthesia Difficult airway According to AMERICAN SOCIETY OF ANAESTHESIOLOGISTS Difficult Airway is defined
Hyoid Bone. Lower Airway. Aspiration. Larynx. Cartilages of the Larynx. Larynx Tracheobronchial Tree (TB Tree) Trachea Bronchi Bronchioles
 Trachea Bronchi Bronchioles") Lower Airway Larynx Tracheobronchial Tree (TB Tree) Trachea Bronchi Bronchioles Respiratory Terminal Hyoid Bone Not part of the larynx. The Hyoid bone is an anchor for the anterior muscles of the neck
Lower Airway Larynx Tracheobronchial Tree (TB Tree) Trachea Bronchi Bronchioles Respiratory Terminal Hyoid Bone Not part of the larynx. The Hyoid bone is an anchor for the anterior muscles of the neck
Tracheostomy and Ventilator Education Program Module 2: Respiratory Anatomy
 Tracheostomy and Ventilator Education Program Module 2: Respiratory Anatomy Disclaimer This material is intended for use by trained family members and caregivers of children with tracheostomies who are
Tracheostomy and Ventilator Education Program Module 2: Respiratory Anatomy Disclaimer This material is intended for use by trained family members and caregivers of children with tracheostomies who are
Pediatric Airway- You Swallowed What?
 Pediatric Airway- You Swallowed What? Staci Kothbauer, CRNA, MS, APNP University of Wisconsin Hospital American Family Children s Hospital Madison, WI 1 Objectives * Understand basic pediatric airway anatomy
Pediatric Airway- You Swallowed What? Staci Kothbauer, CRNA, MS, APNP University of Wisconsin Hospital American Family Children s Hospital Madison, WI 1 Objectives * Understand basic pediatric airway anatomy
Airway Anatomy. Soft palate. Hard palate. Nasopharynx. Tongue. Oropharynx. Hypopharynx. Thyroid cartilage
 Airway Anatomy Hard palate Soft palate Tongue Nasopharynx Oropharynx Hypopharynx Thyroid cartilage Airway Anatomy Hyoid bone Thyroid cartilage Cricoid cartilage Trachea Cricothyroid membrane Airway Anatomy
Airway Anatomy Hard palate Soft palate Tongue Nasopharynx Oropharynx Hypopharynx Thyroid cartilage Airway Anatomy Hyoid bone Thyroid cartilage Cricoid cartilage Trachea Cricothyroid membrane Airway Anatomy
Airway/Breathing. Chapter 5
 Airway/Breathing Chapter 5 Airway/Breathing Introduction Rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur rapidly
Airway/Breathing Chapter 5 Airway/Breathing Introduction Rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur rapidly
Transporting Children With Serious Respiratory Illness: A Presentation For Non-Specialty Teams
 Transporting Children With Serious Respiratory Illness: A Presentation For Non-Specialty Teams Laurie Gehrke, R.N., BSN, CPEN, CEN, CMTE Pediatric Transport Team Blank Children s Hospital Des Moines, Iowa
Transporting Children With Serious Respiratory Illness: A Presentation For Non-Specialty Teams Laurie Gehrke, R.N., BSN, CPEN, CEN, CMTE Pediatric Transport Team Blank Children s Hospital Des Moines, Iowa
Paediatric Otolaryngology
 Paediatric Otolaryngology Antony A Narula MA FRCS FRCS Ed Consultant St Mary s & Ealing Hospitals Hon. Professor, Middlesex University 17 th July 2004 Otology Acute Otitis Media Otitis Media with Effusion
Paediatric Otolaryngology Antony A Narula MA FRCS FRCS Ed Consultant St Mary s & Ealing Hospitals Hon. Professor, Middlesex University 17 th July 2004 Otology Acute Otitis Media Otitis Media with Effusion
PANELISTS. Controversial Issues In Common Interventions In ORL 4/10/2014
 Controversial Issues In Common Interventions In ORL Mohamed Hesham,MD Alexandria Faculty of Medicine PANELISTS Prof. Ahmed Eldaly Prof. Hamdy EL-Hakim Prof. Hossam Thabet Prof. Maged El-Shenawy Prof. Prince
Controversial Issues In Common Interventions In ORL Mohamed Hesham,MD Alexandria Faculty of Medicine PANELISTS Prof. Ahmed Eldaly Prof. Hamdy EL-Hakim Prof. Hossam Thabet Prof. Maged El-Shenawy Prof. Prince
Simulation 01: Two Year-Old Child in Respiratory Distress (Croup)
") Simulation 01: Two Year-Old Child in Respiratory Distress (Croup) Flow Chart Opening Scenario 2 year-old child in respiratory distress - assess Section 1 Type: IG audible stridor with insp + exp wheezing;
Simulation 01: Two Year-Old Child in Respiratory Distress (Croup) Flow Chart Opening Scenario 2 year-old child in respiratory distress - assess Section 1 Type: IG audible stridor with insp + exp wheezing;
ORIGINAL ARTICLE. Synchronous Airway Lesions and Outcomes in Infants With Severe Laryngomalacia Requiring Supraglottoplasty
 ORIGINAL ARTICLE Synchronous Airway Lesions and Outcomes in Infants With Severe Laryngomalacia Requiring Supraglottoplasty James W. Schroeder Jr, MD; Naveen D. Bhandarkar, MD; Lauren D. Holinger, MD Objective:
ORIGINAL ARTICLE Synchronous Airway Lesions and Outcomes in Infants With Severe Laryngomalacia Requiring Supraglottoplasty James W. Schroeder Jr, MD; Naveen D. Bhandarkar, MD; Lauren D. Holinger, MD Objective:
Wheeze. Dr Jo Harrison
 Wheeze Dr Jo Harrison 9.9.14 Wheeze - Physiology a continuous musical sound that lasts longer than 250 msec. can be high-pitched or low-pitched, consist of single or multiple notes, and occur during inspiration
Wheeze Dr Jo Harrison 9.9.14 Wheeze - Physiology a continuous musical sound that lasts longer than 250 msec. can be high-pitched or low-pitched, consist of single or multiple notes, and occur during inspiration
1.0 Abstract. Title. Keywords. Sevoflurane. Anaesthesia. Difficult to intubate (DTI) Rationale and Background
 Rationale and Background") 1.0 Abstract Title A prospective, open-label, multicenter, post marketing, observational study to investigate the effectiveness of Sevoflurane anaesthesia in difficult-to-intubate Egyptian patients. Keywords
1.0 Abstract Title A prospective, open-label, multicenter, post marketing, observational study to investigate the effectiveness of Sevoflurane anaesthesia in difficult-to-intubate Egyptian patients. Keywords
TRACHEOSTOMY. Tracheostomy means creation an artificial opening in the trachea with tracheostomy tube insertion
 TRACHEOSTOMY Definition Tracheostomy means creation an artificial opening in the trachea with tracheostomy tube insertion Indications for tracheostomy 1-upper airway obstruction with stridor, air hunger,
TRACHEOSTOMY Definition Tracheostomy means creation an artificial opening in the trachea with tracheostomy tube insertion Indications for tracheostomy 1-upper airway obstruction with stridor, air hunger,
THE DIFFICULT PAEDIATRIC AIRWAY
 THE DIFFICULT PAEDIATRIC AIRWAY INTRODUCTION A difficult airway in anaesthesia is defined as the clinical situation in which a conventionally trained anaesthetist experiences difficulties with facemask
THE DIFFICULT PAEDIATRIC AIRWAY INTRODUCTION A difficult airway in anaesthesia is defined as the clinical situation in which a conventionally trained anaesthetist experiences difficulties with facemask
Management of Pediatric Tracheostomy
 Management of Pediatric Tracheostomy Deepak Mehta Associate Professor Of Otolaryngology Director Pediatric Aerodigestive Center Definitions Tracheotomy: The making of an incision in the trachea The name
Management of Pediatric Tracheostomy Deepak Mehta Associate Professor Of Otolaryngology Director Pediatric Aerodigestive Center Definitions Tracheotomy: The making of an incision in the trachea The name
Acute Laryngitis in Childhood
 Acute Laryngitis in Childhood Hany Simon Junior Viral croup Definition The term croup syndrome characterizes a group of diseases with variable anatomic involvement and etiology, and is clinically manifested
Acute Laryngitis in Childhood Hany Simon Junior Viral croup Definition The term croup syndrome characterizes a group of diseases with variable anatomic involvement and etiology, and is clinically manifested
DIFFICULT ASTHMA. Dr. Prathyusha Dr. S.Balasubramanian KKCTH
 DIFFICULT ASTHMA Dr. Prathyusha Dr. S.Balasubramanian KKCTH CASE SUMMARY 11 yr old girl, Neyveli Treated as moderate persistent asthma x 5 years On Seroflo [ LABA + steroid ] 250 2 puffs BD and intermittent
DIFFICULT ASTHMA Dr. Prathyusha Dr. S.Balasubramanian KKCTH CASE SUMMARY 11 yr old girl, Neyveli Treated as moderate persistent asthma x 5 years On Seroflo [ LABA + steroid ] 250 2 puffs BD and intermittent
Anatomy and Physiology. The airways can be divided in to parts namely: The upper airway. The lower airway.
 Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced
Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced
Case Presentation Topic: Difficult to Ventilate Difficult to Intubate
 Case Presentation Topic: Difficult to Ventilate Difficult to Intubate Dr. K. Shruthi Jeevan 1 st Year Post Graduate Department of Anaesthesiology CASE SCENARIO : 1 A 65 years old female patient, resident
Case Presentation Topic: Difficult to Ventilate Difficult to Intubate Dr. K. Shruthi Jeevan 1 st Year Post Graduate Department of Anaesthesiology CASE SCENARIO : 1 A 65 years old female patient, resident
Other methods for maintaining the airway (not definitive airway as still unprotected):
:") Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
The Pediatric Patient. Morgen Bernius, MD NCEMS Conference February 24, 2007
 The Pediatric Patient Morgen Bernius, MD NCEMS Conference February 24, 2007 Rule #1: Everyone Loves the Pediatric Patient Pediatrics in EMS Approximately 10% of all EMS treatment is for children younger
The Pediatric Patient Morgen Bernius, MD NCEMS Conference February 24, 2007 Rule #1: Everyone Loves the Pediatric Patient Pediatrics in EMS Approximately 10% of all EMS treatment is for children younger
SWISS SOCIETY OF NEONATOLOGY. Peripartal management of a prenatally diagnosed large oral cyst
 SWISS SOCIETY OF NEONATOLOGY Peripartal management of a prenatally diagnosed large oral cyst May 2007 2 Fontana M, Berger TM, Winiker H, Jöhr M, Nagel H, Neonatal and Pediatric Intensive Care Unit (FM,
SWISS SOCIETY OF NEONATOLOGY Peripartal management of a prenatally diagnosed large oral cyst May 2007 2 Fontana M, Berger TM, Winiker H, Jöhr M, Nagel H, Neonatal and Pediatric Intensive Care Unit (FM,
Common Pediatric Respiratory Illness and Emergencies
 Common Pediatric Respiratory Illness and Emergencies Rob Cloutier, MD Assistant Professor Emergency Medicine & Pediatrics Oregon Health & Science University Overview Review key differences between pediatric
Common Pediatric Respiratory Illness and Emergencies Rob Cloutier, MD Assistant Professor Emergency Medicine & Pediatrics Oregon Health & Science University Overview Review key differences between pediatric
Hoarseness. Common referral Hoarseness reflects any abnormality of normal phonation
 Hoarseness Kevin Katzenmeyer, MD Faculty Advisor: Byron J Bailey, MD The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation October 24, 2001 Hoarseness Common referral
Hoarseness Kevin Katzenmeyer, MD Faculty Advisor: Byron J Bailey, MD The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation October 24, 2001 Hoarseness Common referral
Airway Management. Teeradej Kuptanon, MD
 Airway Management Teeradej Kuptanon, MD Outline Anatomy Detect difficult airway Rapid sequence intubation Difficult ventilation Difficult intubation Surgical airway access ICU setting Intubation Difficult
Airway Management Teeradej Kuptanon, MD Outline Anatomy Detect difficult airway Rapid sequence intubation Difficult ventilation Difficult intubation Surgical airway access ICU setting Intubation Difficult
Intubation techniques
 Operative Techniques in Otolaryngology (2005) 16, 166-170 FEATURE ARTICLES Intubation techniques Geoffrey Lane, MB, BChir, FRCA From the Department of Anesthesiology, The University of Colorado Health
Operative Techniques in Otolaryngology (2005) 16, 166-170 FEATURE ARTICLES Intubation techniques Geoffrey Lane, MB, BChir, FRCA From the Department of Anesthesiology, The University of Colorado Health
Unit 14: The Respiratory System
 Unit 14: The Respiratory System See what you already know! 1. Fill in the diagram on your own 2. Collaborate with your partner The Respiratory System The major function of the respiratory system is gas
Unit 14: The Respiratory System See what you already know! 1. Fill in the diagram on your own 2. Collaborate with your partner The Respiratory System The major function of the respiratory system is gas
McHenry Western Lake County EMS System Optional CE for Paramedics, EMT-B and PHRN s Croup vs. Epiglottitis. Optional #2 2017
 McHenry Western Lake County EMS System Optional CE for Paramedics, EMT-B and PHRN s Croup vs. Epiglottitis Optional #2 2017 The tones go out at 3 am for a child with difficulty breathing. As it is a kid
McHenry Western Lake County EMS System Optional CE for Paramedics, EMT-B and PHRN s Croup vs. Epiglottitis Optional #2 2017 The tones go out at 3 am for a child with difficulty breathing. As it is a kid
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Chronic Stridor in Children These podcasts are designed to give medical students an overview of key topics in pediatrics.
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Chronic Stridor in Children These podcasts are designed to give medical students an overview of key topics in pediatrics.
Unconscious exchange of air between lungs and the external environment Breathing
 Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
If you suspect airway problems, get a second opinion before you anaesthetise, not after!
 Assessing the airway It is more important to be aware of the various methods of dealing with difficult laryngoscopy than to expect to be able to accurately identify the rare difficult patients without
Assessing the airway It is more important to be aware of the various methods of dealing with difficult laryngoscopy than to expect to be able to accurately identify the rare difficult patients without
Preface... Contributors... 1 Embryology... 3
 Contents Preface... Contributors... vii xvii I. Pediatrics 1 Embryology... 3 Pearls... 3 Branchial Arch Derivatives... 3 Branchial Arch Anomalies: Cysts, Sinus, Fistulae... 4 Otologic Development... 4
Contents Preface... Contributors... vii xvii I. Pediatrics 1 Embryology... 3 Pearls... 3 Branchial Arch Derivatives... 3 Branchial Arch Anomalies: Cysts, Sinus, Fistulae... 4 Otologic Development... 4
Overview. The Respiratory System. Chapter 18. Respiratory Emergencies 9/11/2012
 Chapter 18 Respiratory Emergencies Slide 1 Overview Respiratory System Review Anatomy Physiology Breathing Assessment Adequate Breathing Breathing Difficulty Focused History and Physical Examination Emergency
Chapter 18 Respiratory Emergencies Slide 1 Overview Respiratory System Review Anatomy Physiology Breathing Assessment Adequate Breathing Breathing Difficulty Focused History and Physical Examination Emergency
Aetiology. Poor tube management. Small cricoid (acquired on congenital) Reflux Poor general status. Size of tube (leak) Duration of intubation
 Reflux Poor general status. Size of tube (leak) Duration of intubation") Aetiology Poor tube management Size of tube (leak) Duration of intubation Small cricoid (acquired on congenital) Reflux Poor general status Prevention Laryngeal Rest Medical Tubes Cricoid split Developing
Aetiology Poor tube management Size of tube (leak) Duration of intubation Small cricoid (acquired on congenital) Reflux Poor general status Prevention Laryngeal Rest Medical Tubes Cricoid split Developing
Airway Management in a Patient with Klippel-Feil Syndrome Using Extracorporeal Membrane Oxygenator
 Airway Management in a Patient with Klippel-Feil Syndrome Using Extracorporeal Membrane Oxygenator Beckerman Z*, Cohen O, Adler Z, Segal D, Mishali D and Bolotin G Department of Cardiac Surgery, Rambam
Airway Management in a Patient with Klippel-Feil Syndrome Using Extracorporeal Membrane Oxygenator Beckerman Z*, Cohen O, Adler Z, Segal D, Mishali D and Bolotin G Department of Cardiac Surgery, Rambam
Department of Pediatric Otolarygnology. ENT Specialty Programs
 Department of Pediatric Otolarygnology ENT Specialty Programs Staffed by fellowship-trained otolaryngologists, assisted by pediatric nurse practitioners, ENT (Otolaryngology) at Nationwide Children s Hospital
Department of Pediatric Otolarygnology ENT Specialty Programs Staffed by fellowship-trained otolaryngologists, assisted by pediatric nurse practitioners, ENT (Otolaryngology) at Nationwide Children s Hospital
Respiratory System. Clinical notes. Published on Second Faculty of Medicine, Charles University ( https://www.lf2.cuni.cz)
") Published on Second Faculty of Medicine, Charles University ( https://www.lf2.cuni.cz) Respiratory System The test of the respiratory system follows the general rules for written tests (see Continuous
Published on Second Faculty of Medicine, Charles University ( https://www.lf2.cuni.cz) Respiratory System The test of the respiratory system follows the general rules for written tests (see Continuous
-Discussed in the Ebers Papyrus and the Rig Veda BC
 Tracheotomy History -Discussed in the Ebers Papyrus and the Rig Veda -1500 BC History -Treatment obstructive diseases (Antyllus, 2 nd century AD) -Discussed in the writings of Braassarolo (1546) -Considered
Tracheotomy History -Discussed in the Ebers Papyrus and the Rig Veda -1500 BC History -Treatment obstructive diseases (Antyllus, 2 nd century AD) -Discussed in the writings of Braassarolo (1546) -Considered
Discussing feline tracheal disease
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk Discussing feline tracheal disease Author : ANDREW SPARKES Categories : Vets Date : March 24, 2008 ANDREW SPARKES aims to
Vet Times The website for the veterinary profession https://www.vettimes.co.uk Discussing feline tracheal disease Author : ANDREW SPARKES Categories : Vets Date : March 24, 2008 ANDREW SPARKES aims to
Pediatrics Grand Rounds 25 October University of Texas Health Science Center at San Antonio, Texas
 PEDIATRIC ENT & YOU A PATIENT CARE PARTNERSHIP Disclosure Timothy McEvoy, MD has no relevant relationships with commercial interests to disclose. Timothy McEvoy, MD UTHSCSA Department of Otolaryngology-
PEDIATRIC ENT & YOU A PATIENT CARE PARTNERSHIP Disclosure Timothy McEvoy, MD has no relevant relationships with commercial interests to disclose. Timothy McEvoy, MD UTHSCSA Department of Otolaryngology-
Disclosures. Learning Objectives. Coeditor/author. Associate Science Editor, American Heart Association
 Tracheotomy Challenges for airway specialists Elizabeth H. Sinz, MD Professor of Anesthesiology & Neurosurgery Associate Dean for Clinical Simulation Disclosures Coeditor/author Associate Science Editor,
Tracheotomy Challenges for airway specialists Elizabeth H. Sinz, MD Professor of Anesthesiology & Neurosurgery Associate Dean for Clinical Simulation Disclosures Coeditor/author Associate Science Editor,
The Ear, Nose and Throat in MPS
 The Ear, Nose and Throat in MPS Annerose Keilmann Voice Care Center Bad Rappenau, Germany Preciptorship program on MPS Wiesbaden, November 2 nd 2015 Alterations of the outer and middle ear in MPS I narrowing
The Ear, Nose and Throat in MPS Annerose Keilmann Voice Care Center Bad Rappenau, Germany Preciptorship program on MPS Wiesbaden, November 2 nd 2015 Alterations of the outer and middle ear in MPS I narrowing
Perioperative Care in OSA Surgery
 Perioperative Care in OSA Surgery Overview Estimate of Major Peri-Op Complications Risk Factors for Airway Complications Peri-Operative Planning Avoidance of Complications Andrew N. Goldberg, MD, MSCE
Perioperative Care in OSA Surgery Overview Estimate of Major Peri-Op Complications Risk Factors for Airway Complications Peri-Operative Planning Avoidance of Complications Andrew N. Goldberg, MD, MSCE
RESPIRATORY FAILURE. Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics
 RESPIRATORY FAILURE Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics What talk is he giving? DO2= CO * CaO2 CO = HR * SV CaO2 = (Hgb* SaO2 * 1.34) + (PaO2 * 0.003) Sound familiar??
RESPIRATORY FAILURE Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics What talk is he giving? DO2= CO * CaO2 CO = HR * SV CaO2 = (Hgb* SaO2 * 1.34) + (PaO2 * 0.003) Sound familiar??
Pediatric Airway and Respiratory Emergencies. Objectives 30/01/2009
 Objectives Pediatric Airway and Respiratory Emergencies Patrick Mahar, MD Review the anatomical differences between adult and pediatric airways Recognize different causes of respiratory comprise in pediatric
Objectives Pediatric Airway and Respiratory Emergencies Patrick Mahar, MD Review the anatomical differences between adult and pediatric airways Recognize different causes of respiratory comprise in pediatric
Difficult Airway. Victor M. Gomez, M.D. Pulmonary Critical Care Medicine Medical City Dallas Hospital
 Difficult Airway Victor M. Gomez, M.D. Pulmonary Critical Care Medicine Medical City Dallas Hospital Difficult Airway Definition Predicting a difficult airway Preparing for a difficult airway Extubation
Difficult Airway Victor M. Gomez, M.D. Pulmonary Critical Care Medicine Medical City Dallas Hospital Difficult Airway Definition Predicting a difficult airway Preparing for a difficult airway Extubation
Pediatric Patients. BCFPD Paramedic Education Program. EMS Education Paramedic Level
 Pediatric Patients BCFPD Program Basic Considerations Much of the initial patient assessment can be done during visual examination of the scene. Involve the caregiver or parent as much as possible. Allow
Pediatric Patients BCFPD Program Basic Considerations Much of the initial patient assessment can be done during visual examination of the scene. Involve the caregiver or parent as much as possible. Allow
Pediatric Shock. Hypovolemia. Sepsis. Most common cause of pediatric shock Small blood volumes (80cc/kg)
") Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Review of Neonatal Respiratory Problems
 Review of Neonatal Respiratory Problems Respiratory Distress Occurs in about 7% of infants Clinical presentation includes: Apnea Cyanosis Grunting Inspiratory stridor Nasal flaring Poor feeding Tachypnea
Review of Neonatal Respiratory Problems Respiratory Distress Occurs in about 7% of infants Clinical presentation includes: Apnea Cyanosis Grunting Inspiratory stridor Nasal flaring Poor feeding Tachypnea
Infectious Upper Airway Obstruction
 Infectious Upper Airway Obstruction Prof. Muhi K. Al-Janabi MRCPCH; DCH; FICMS Consultant Pediatric Pulmonologist Objectives Viral croup Objectives 1. Know and understand the aetiology and natural history
Infectious Upper Airway Obstruction Prof. Muhi K. Al-Janabi MRCPCH; DCH; FICMS Consultant Pediatric Pulmonologist Objectives Viral croup Objectives 1. Know and understand the aetiology and natural history
Neonatal Stridor. Neonatology Roy Rajan, MD. Assistant Professor, Pediatric Otolaryngology Emory University
 Neonatal Stridor Neonatology 2015 Roy Rajan, MD Assistant Professor, Pediatric Otolaryngology Emory University Disclosures None 2 Goals/Objectives Describe embryology related to laryngeal development Define
Neonatal Stridor Neonatology 2015 Roy Rajan, MD Assistant Professor, Pediatric Otolaryngology Emory University Disclosures None 2 Goals/Objectives Describe embryology related to laryngeal development Define
Chapter 2: Airway Management and Ventilation
 Chapter 2: Airway Management and Ventilation Objectives: Upon completion of this topic, the physician will be able to explain and demonstrate the principles of airway management. Specifically, the physician
Chapter 2: Airway Management and Ventilation Objectives: Upon completion of this topic, the physician will be able to explain and demonstrate the principles of airway management. Specifically, the physician
Pediatric Obstructive Sleep apnea An update What else is there to know?
 Pediatric Obstructive Sleep apnea An update What else is there to know? Garani S. Nadaraja, MD, FAAP Medical Director BCH-Oakland Clinical Assistant Professor Division of Pediatric Otolaryngology UCSF
Pediatric Obstructive Sleep apnea An update What else is there to know? Garani S. Nadaraja, MD, FAAP Medical Director BCH-Oakland Clinical Assistant Professor Division of Pediatric Otolaryngology UCSF
Airway Endoscopy The Basics Neonatal Progressive Acute Quiz
 Endoscopy of the Airway Dave Albert Airway Endoscopy The Basics Neonatal Progressive Acute Quiz The laws of Poiseuille and Bernoulli French physician,physicist mathemetician and Dutch Swiss mathemetician
Endoscopy of the Airway Dave Albert Airway Endoscopy The Basics Neonatal Progressive Acute Quiz The laws of Poiseuille and Bernoulli French physician,physicist mathemetician and Dutch Swiss mathemetician
Participant Objectives. Airway Anatomy. Airway Anatomy. Airway Anatomy: Pediatric Considerations. Airway Anatomy: Pediatric Considerations
 Common Pediatric Respiratory Emergencies NAPNAP Chicago Session 314 Wednesday, March 21, 2018 Participant Objectives Discuss upper airway illness in the pediatric population Discuss lower airway illness
Common Pediatric Respiratory Emergencies NAPNAP Chicago Session 314 Wednesday, March 21, 2018 Participant Objectives Discuss upper airway illness in the pediatric population Discuss lower airway illness
HelmiLubis, RidwanMuchtarDaulay, WismanDalimunthe, Rini Savitri Daulay
 Congenital Malformation of the Lung and Airways HelmiLubis, RidwanMuchtarDaulay, WismanDalimunthe, Rini Savitri Daulay DivisiRespirologiDepartemenIlmuKesehatanAnak FakultasKedokteran Universitas Sumatera
Congenital Malformation of the Lung and Airways HelmiLubis, RidwanMuchtarDaulay, WismanDalimunthe, Rini Savitri Daulay DivisiRespirologiDepartemenIlmuKesehatanAnak FakultasKedokteran Universitas Sumatera
Simulation 1: Two Year-Old Child in Respiratory Distress
 Simulation 1: Two Year-Old Child in Respiratory Distress Opening Scenario (Links to Section 1) You are the respiratory therapist in a 300 bed community hospital working the evening shift. At 8:30 PM you
Simulation 1: Two Year-Old Child in Respiratory Distress Opening Scenario (Links to Section 1) You are the respiratory therapist in a 300 bed community hospital working the evening shift. At 8:30 PM you
Management of Upper Airway Obstruction in Pierre Robin Sequence
 Management of Upper Airway Obstruction in Pierre Robin Sequence South Wales Cleft Team Pierre Robin Sequence Triad of cleft palate, micrognathia and airway obstruction was described by St Hilaire in 1822,
Management of Upper Airway Obstruction in Pierre Robin Sequence South Wales Cleft Team Pierre Robin Sequence Triad of cleft palate, micrognathia and airway obstruction was described by St Hilaire in 1822,
Objectives. Module A2: Upper Airway Anatomy & Physiology. Function of the Lungs/Heart. The lung is for gas exchange. Failure of the Lungs/Heart
 Module A2: Upper Airway Anatomy & Physiology Objectives Classify epithelial tissue based on cell type and tissue layers. Identify location of tissue epithelium in the respiratory system. Describe the major
Module A2: Upper Airway Anatomy & Physiology Objectives Classify epithelial tissue based on cell type and tissue layers. Identify location of tissue epithelium in the respiratory system. Describe the major