AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA
|
|
|
- Rosaline Riley
- 6 years ago
- Views:
Transcription
1 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research. All rights reserved.
2 DISCLOSURE* Relevant Financial Relationship(s) None Off Label Usage None *A provider must disclose the above information to learners prior to beginning of the educational activity (ACCME)
3 When Not to Do AVS Patient without confirmed PA Patient who does not want to pursue the surgical option Young patient with marked PA and unilateral adrenal macroadenoma on CT (and normal appearing contralateral adrenal)
 with")
 AVS")
4 APA clinical phenotype in a young patient (<35 yr) with unilateral adrenal macroadenoma (>1-cm) AVS not needed


5 Prevalence by Age -- Autopsy Data The development of adrenocortical nodules is, in part, a function of age 7%! Kloos et al., Endo Rev 16:460, 1995

6 Algorithm that will be part of revised ES PA Guidelines to be published in 2016
7 Lim V, Guo Q, Grant CS, Thompson GB, Richards ML, Farley DR, Young WF Jr. Accuracy of adrenal imaging and adrenal venous sampling in predicting surgical cure of primary aldosteronism. J Clin Endocrinol Metab Aug;99(8):
8 When to Do AVS Patient with confirmed PA and: o Who wants to pursue the surgical option and o Who is >35 yrs old or <35 yrs old and lack of unilateral macroadenoma on CT
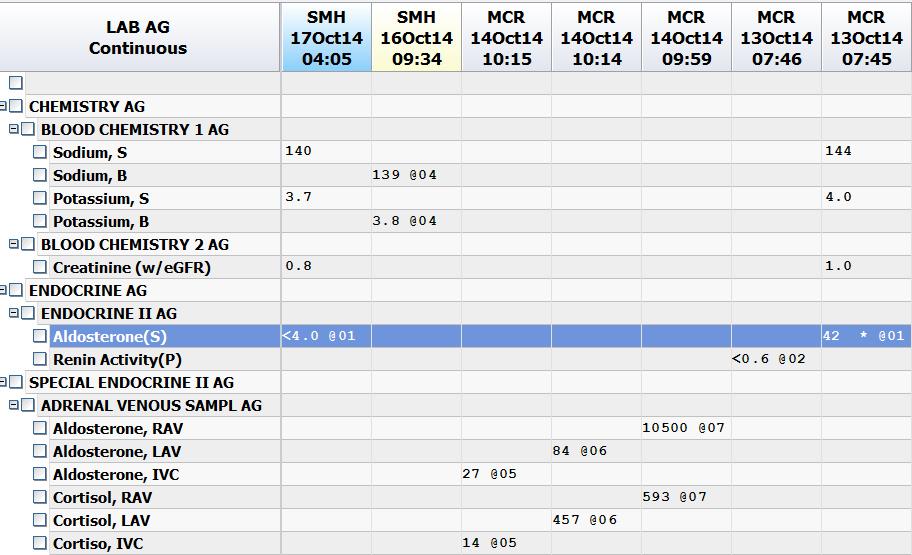
9 68-Year-Old Man Hypertension x 9 yrs: Intermittent spontaneous hypokalemia noted on routine testing over the last 2 yrs Asymptomatic no spells Suboptimal BP control on a CCB, ACE-I, central α-2 agonist, and β-adrenergic blocker Also takes 40 meq KCl/d Physical exam: normal phenotype, BP = 140/83 mm Hg, HR 84 bpm, BMI 29.4 Initial labs: Na + = 144 meq/l, K + = 4.0 meq/l, creatinine = 1.0 mg/dl
 - PRA = <0.")
10 PAC/PRA Ratio - PAC = 42 ng/dl (1165 pmol/l) - PRA = <0.6 ng/ml/hr
11 PA Confirmatory Test 24-hr urine on ambient sodium diet: - Sodium = 269 meq - Aldosterone = 34 mcg (94 nmol)


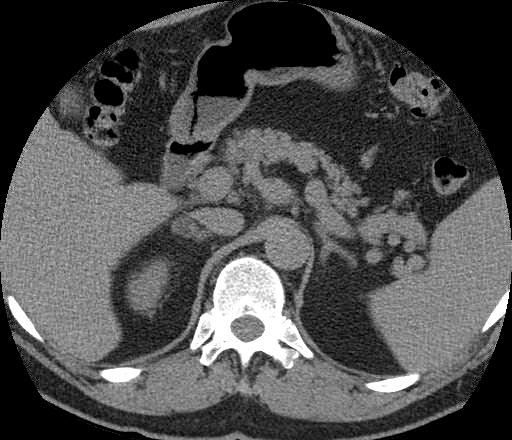
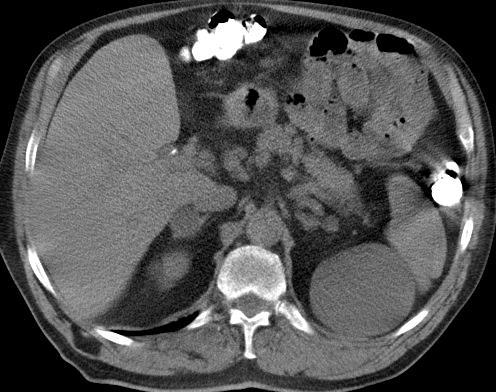
12 Adrenal CT: Radiologist report: normal adrenals


13 Adrenal Venous Sampling
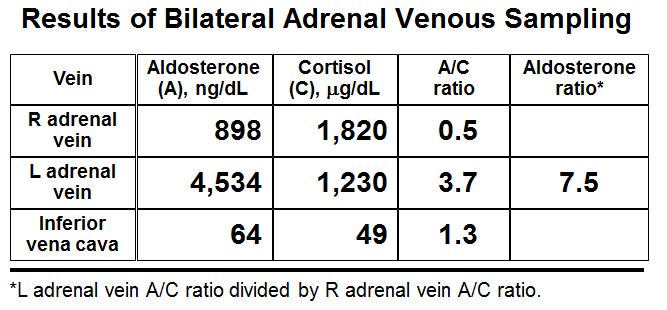
14 Step 1: Was cannulation of both AVs successful? AV [cortisol] should be >5-fold higher than IVC [cortisol] from BOTH AVs If successful, go to step 2. If not successful, stop. Adrenal Vein Sampling* Vein RT Adrenal Vein LT Adrenal Vein Aldosterone (A) ng/dl Cortisol (C) mcg/dl A/C Ratio Aldosterone Ratio IVC 14
15 Adrenal Vein Sampling* Vein RT Adrenal Vein LT Adrenal Vein Aldosterone (A) ng/dl Cortisol (C) mcg/dl A/C Ratio Aldosterone Ratio IVC Step 2: Where is Aldo coming from? To correct for dilution (from inferior phrenic vein) on the LT AV sample, divide each AV [aldo] by it s respective AV [cortisol] for the A/C Ratio
16 Adrenal Vein Sampling* Vein RT Adrenal Vein LT Adrenal Vein Aldosterone (A) ng/dl Cortisol (C) mcg/dl A/C Ratio Aldosterone Ratio 102 : 1 IVC Step 3: Where is Aldo coming from? Unilateral if A/C ratio from the dominant adrenal is >4-fold higher than A/C ratio from lower adrenal Maybe unilateral or bilateral if aldosterone lateralization ratio (ALR) is between 3:1 and 4:1 Bilateral if ALR is <3:1
17 Aldosterone Lateralization Ratio 100 APA (n=102) IHA (n=84) PAH (n=8) The patient I am presenting 10 ALR = 4:1 1 Young WF, Stanson AW, Thompson GB, et al. Surgery. 2004;136:
18 Step 4: Consider contralateral suppression The A/C ratio from the nondominant adrenal should be less than the A/C ratio from the IVC In this case example 0.2 is less than divided by 1.9 = 0.1 Adrenal Vein Sampling* Vein RT Adrenal Vein LT Adrenal Vein Aldosterone (A) ng/dl Cortisol (C) mcg/dl A/C Ratio Aldosterone Ratio 102 : 1 IVC
19 Contralateral A/C ratio 100 APA (n=102) IHA (n=84) PAH (n=8) Contralateral A/C ratio divided by the IVC A/C ratio Young WF, Stanson AW, Thompson GB, et al. Surgery. 2004;136:
20
21 Follow-up 9 Months Postop: - Hypokalemia resolved and BP = 125/65 mm Hg on low-doses of 2 BP meds
22

23
24
25 AVS Summary 203 patients; % success rate Based on CT: o 46 patients (24%) would have been bypassed for surgery o 42 pts (22%) would have had unnecessary surgery CT accuracy = 53% Surgery 136: , 2004.
: 16 mcg (Na + = 418 meq) CT: 6-mm LT nodule KKM019")
26 AVS Case 2: 35-yr-old woman with new onset hypertension Normal serum potassium BP treated with ACE-I PAC = 16 ng/dl PRA = <0.6 ng/ml/hr ARR = > hr urine aldo (high Na + diet): 16 mcg (Na + = 418 meq) CT: 6-mm LT nodule KKM019


27
28 AVS Case 2: Results of Bilateral Adrenal Venous Sampling Vein R adrenal vein L adrenal vein Inferior vena cava Aldosterone (A), ng/dl Cortisol (C), g/dl A:C ratio *L adrenal vein A:C ratio divided by R adrenal vein A:C ratio. Aldosterone ratio* 15.5 KKM019

29 AVS Case 2: The best next step in this case is: 1. RT adrenalectomy 2. LT adrenalectomy 3. Bilateral adrenalectomy 4. Repeat AVS 5. Option 5 (something else)

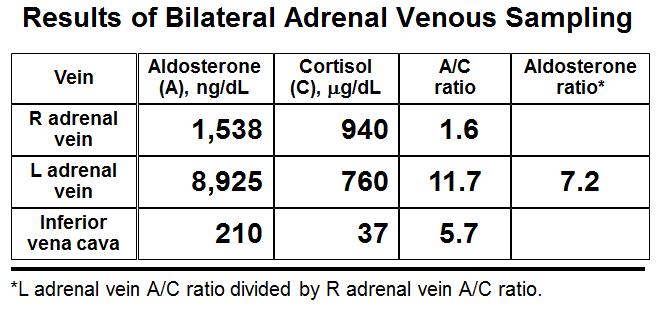
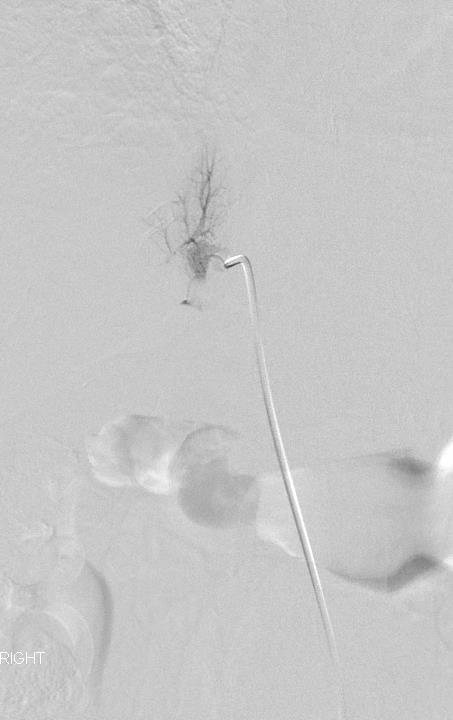
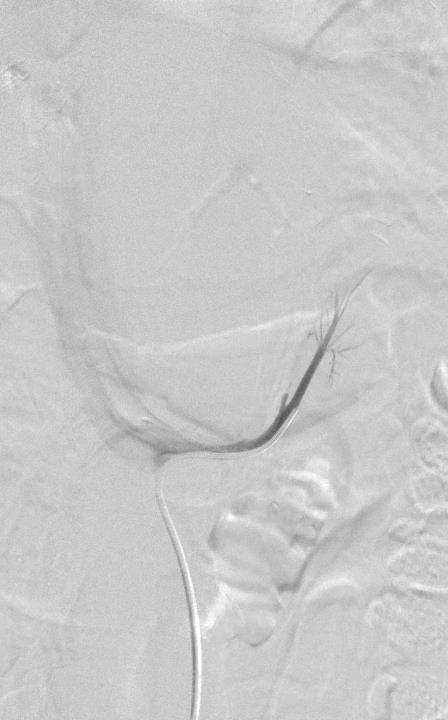
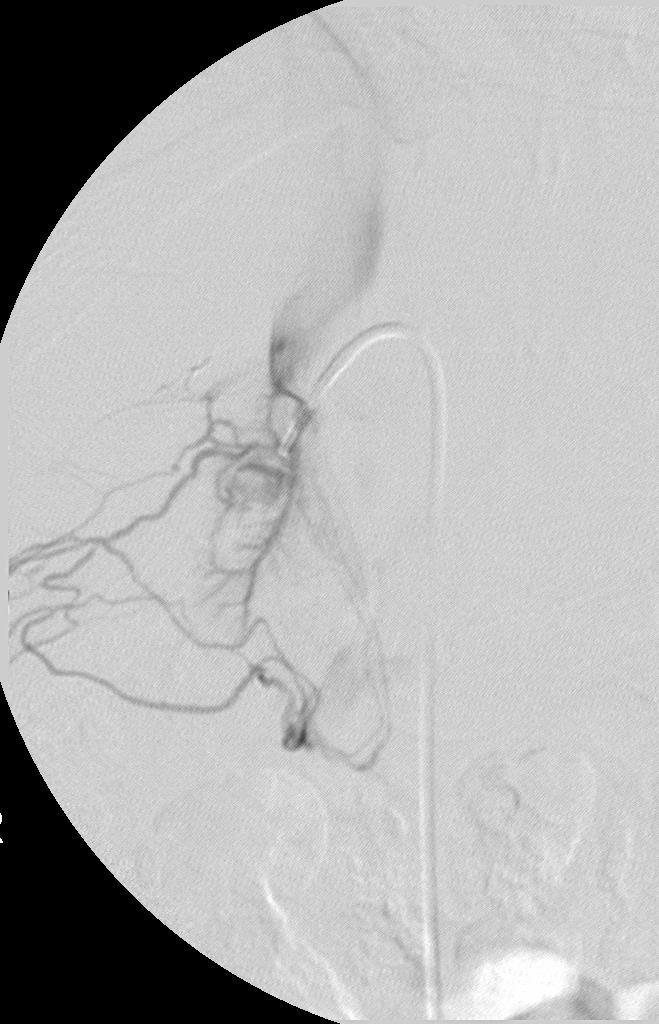
30 AVS Case 3: 57-yr-old woman with BP x 20 yrs & accelerated x 2 yrs; spontaneous hypokalemia x 2 yrs BP treated with CCB, ACE-I, ARB & KCL 80 meq/d PAC = 37 ng/dl PRA = <0.6 ng/ml/hr ARR = > 45 CT: 11-mm RT nodule DHY261
31
, g/dl 24 522 27 A:C ratio 0.36 0.96 1.22 *L adrenal vein A:C ratio divided by R adrenal vein A:C ratio.")
32 AVS Case 3: Results of Bilateral Adrenal Venous Sampling Vein R adrenal vein L adrenal vein Inferior vena cava Aldosterone (A), ng/dl Cortisol (C), g/dl A:C ratio *L adrenal vein A:C ratio divided by R adrenal vein A:C ratio. Aldosterone ratio* 2.7 DHY261

33 AVS Case 3: The best next step in this case is: 1. RT adrenalectomy 2. LT adrenalectomy 3. Bilateral adrenalectomy 4. Repeat AVS 5. Option 5 (something else)

, g/dl 24 522 27 A:C ratio 0.36 0.")
34 AVS Case 3: Results of Bilateral Adrenal Venous Sampling Vein R adrenal vein L adrenal vein Inferior vena cava Aldosterone (A), ng/dl Cortisol (C), g/dl A:C ratio Aldosterone ratio* 2.7 DHY261


35 AVS Case 4: 39-yr-old woman with poorly controlled BP on 3 drugs Spontaneous hypokalemia PAC = 41 ng/dl PRA = <0.6 ng/ml/hr ARR = > 68 CT: 9-mm RT nodule & 8-mm LT nodule GQH042

36
, ng/dl 250 4267 98")

37 AVS Case 4: Results of Bilateral Adrenal Venous Sampling Vein R adrenal vein L adrenal vein Inferior vena cava Aldosterone (A), ng/dl Cortisol (C), g/dl A:C ratio *R adrenal vein A:C ratio divided by L adrenal vein A:C ratio. Aldosterone ratio* 22.1 GQH 042

38 AVS Case 4: The best next step in this case is: 1. RT adrenalectomy 2. LT adrenalectomy 3. Bilateral adrenalectomy 4. Repeat AVS 5. Option 5 (something else)
39

40 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research. All rights reserved.
41 When Not to Do IPSS Patient without confirmed CS IPSS does NOT diagnose CS; IPSS only tells you where ACTH is coming from Patient with typical pituitarydependent CS presentation + definite pituitary adenoma on MRI Patient with obvious ectopic ACTH and tumor is co-localized with cross sectional imaging and octreotide scintigraphy or FDG-PET
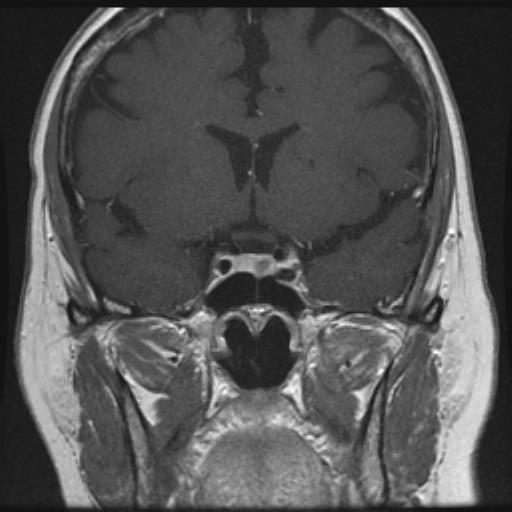
42 41-Year-Old Woman Slowly developing symptoms over 5 yrs: Dx with DM 4 yrs ago Dx with hypertension 2 yrs ago Osteoporosis with 2 nontraumatic stress fractures Gained 100# over past 3 yrs Proximal muscle weakness; hirsutism Irritable I am always freaking out BMI 48.8 kg/m2
43 41-Year-Old Woman Lab: Serum cortisol: 26 mcg/dl 8 AM; 19 mcg/dl 4 PM Midnight salivary cortisol = 296 ng/dl (N <100) 24-hr UFC = 63 and 97 mcg (N <45) 1-mg overnight DST = 12 mcg/dl ACTH = 63 pg/ml (N <60) Head MRI
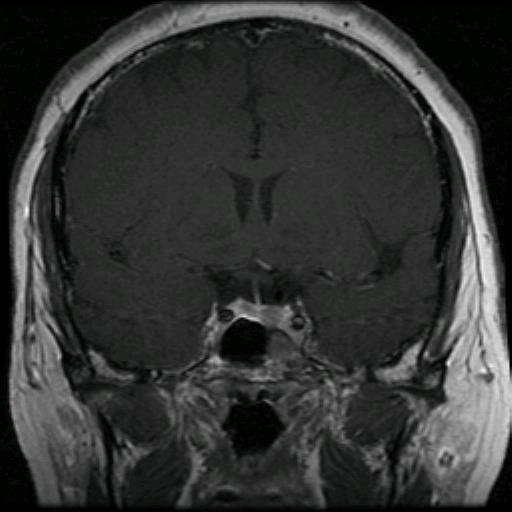
44 41-Year-Old Woman
45 41-Year-Old Woman Do we need IPSS here? No, we need a pituitary surgeon Lost 30# of wt BP meds D/C
46 Confirmed Cushing s Syndrome (CS) Serum ACTH Undetectable Adrenal CT Mid-normal to increased Pituitary MRI Unilateral adrenal mass: Adenoma Carcinoma Bilateral adrenal masses: AIMAH PPNAD Bilateral cortisolsecreting adenomas Definite pituitary tumor IPSS usually not needed if clinical picture fits pituitary CS Normal or if clinical picture fits ectopic CS IPSS
47 Confirmed Cushing s Syndrome (CS) Serum ACTH Mid-normal to increased Pituitary MRI Definite pituitary tumor If clinical picture fits with pituitary-dependent CS (eg, female, slow onset, mild to moderate CS, UFC <600 mcg) then IPSS usually not needed Normal or if clinical picture fits ectopic CS IPSS
48 64-Year-Old Woman Well until 5 months ago: Severe reflux and preop Nissen labs showed serum K+ = 2.2 meq/l Has noticed redness and rounding of the face; scalp hair thinning; easy bruising New onset DM BMI 25.2 kg/m2
49 64-Year-Old Woman Lab: Serum cortisol: 46 mcg/dl 8 AM; 43 mcg/dl 4 PM Midnight salivary cortisol = ND 24-hr UFC = 1084 mcg (N <45) 1-mg overnight DST = ND ACTH = 151 pg/ml (N <60) Head MRI
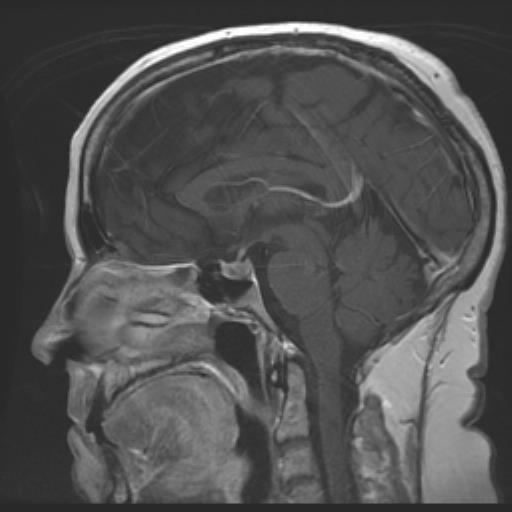
50 64-Year-Old Woman


51 64-Year-Old Woman Do we need IPSS here? No, we need a cross sectional imaging + octreotide scintigraphy or FDG-PET
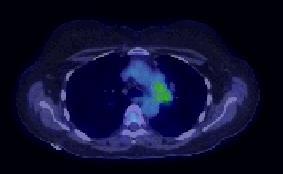

52 FDG-PET



53
54 Confirmed Cushing s Syndrome (CS) Serum ACTH Mid-normal to increased Pituitary MRI Definite pituitary tumor If clinical picture fits with pituitary-dependent CS (eg, female, slow onset, mild to moderate CS, UFC <600 mcg) then IPSS usually not needed Normal or if clinical picture fits ectopic CS IPSS
55 When to Do IPSS Patient with confirmed ACTHdependent CS and: o Has rapid onset and severe CS and negative cross sectional imaging o Has mild or intermediate degree CS, but negative pituitary MRI
56 50-Year-Old Woman Signs & symptoms of CS slowly developed over 10 yrs: 80 pound central weight gain (130# to 210#) Dorsocervical & supraclavicular fat pads Easy bruising Decreased proximal muscle strength New onset hypertension & diabetes Patient says: I am trapped in a fat cocoon.. who am I and where did I go?
57
58 50-Year-Old Woman Serum cortisols = 36 mcg/dl a.m. 36 mcg/dl p.m. 24-hr UFC = 531 mcg ACTH = 151 pg/ml Na + = 139 meq/l; K + = 3.7 meq/l

59 Pituitary MRI shows a full sella, but no tumor

60

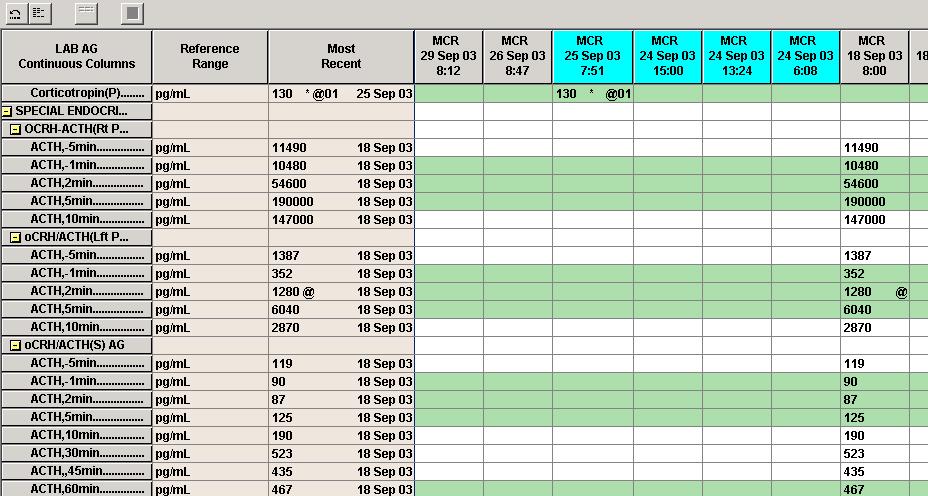
61 PV IPSS Cortisol ACTH with CRH increased Post Pre CRH: from / / to to = 356% 97 = % Time RT IPS LT IPS PV PV ACTH ACTH ACTH cortisol -5 min min min min min min min min If concerned about adequacy of IPSS, check PRL levels
62
63 IPSS Case 2: 50-year-old man with severe ACTH-dependent CS (note: + PRL gradient) Time RT IPS LT IPS PV PV ACTH ACTH ACTH cortisol -5 min min min min min min min min
AVS and IPSS: The Basics and the Pearls
 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2018 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2018 Mayo Foundation for Medical Education and Research.
William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA
 The Year in Adrenal William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA Division of ENDOCRINOLOGY, DIABETES, METABOLISM & NUTRITION 2018 Mayo Foundation for Medical Education
The Year in Adrenal William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA Division of ENDOCRINOLOGY, DIABETES, METABOLISM & NUTRITION 2018 Mayo Foundation for Medical Education
Primary Aldosteronism
 Primary Aldosteronism Odelia Cooper, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism Cedars-Sinai Medical Center HYPERTENSION CENTER Barriers to diagnosing primary
Primary Aldosteronism Odelia Cooper, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism Cedars-Sinai Medical Center HYPERTENSION CENTER Barriers to diagnosing primary
Incidental Adrenal Nodules Differential Diagnosis
 Adrenal Stuff Richard J. Auchus, MD, PhD, FACE Division of Metabolism, Endocrinology & Diabetes Departments of Internal Medicine & Pharmacology University of Michigan/VA Ann Arbor Incidental Adrenal Nodules
Adrenal Stuff Richard J. Auchus, MD, PhD, FACE Division of Metabolism, Endocrinology & Diabetes Departments of Internal Medicine & Pharmacology University of Michigan/VA Ann Arbor Incidental Adrenal Nodules
Differential Diagnosis of Cushing s Syndrome
 Differential Diagnosis of Cushing s Syndrome Cushing s the Diagnostic Challenge Julia Kharlip, MD and Caitlin White, MD Endocrinology, Diabetes and Metabolism Perelman School of Medicine at the University
Differential Diagnosis of Cushing s Syndrome Cushing s the Diagnostic Challenge Julia Kharlip, MD and Caitlin White, MD Endocrinology, Diabetes and Metabolism Perelman School of Medicine at the University
Endocrine Topic Review. Sethanant Sethakarun, MD
 Endocrine Topic Review Sethanant Sethakarun, MD Definition Cushing's syndrome comprises a large group of signs and symptoms that reflect prolonged and in appropriately high exposure of tissue to glucocorticoids
Endocrine Topic Review Sethanant Sethakarun, MD Definition Cushing's syndrome comprises a large group of signs and symptoms that reflect prolonged and in appropriately high exposure of tissue to glucocorticoids
October 13, Surgical Nuances to Managing Cushing s Disease. Cortisol Regulation. Cushing s Syndrome Excess Cortisol. Sandeep Kunwar, M.D.
 Surgical Nuances to Managing Cushing s Disease Cortisol Regulation Sandeep Kunwar, M.D. Surgical Director, California Center for Pituitary Disorders Associate Clinical Professor, University of California,
Surgical Nuances to Managing Cushing s Disease Cortisol Regulation Sandeep Kunwar, M.D. Surgical Director, California Center for Pituitary Disorders Associate Clinical Professor, University of California,
27 F with new onset hypertension and weight gain. Rajesh Jain Endorama 10/01/2015
 27 F with new onset hypertension and weight gain Rajesh Jain Endorama 10/01/2015 HPI 27 F with hypertension x 1 year BP 130-140/90 while on amlodipine 5 mg daily She also reports weight gain, 7 LB, mainly
27 F with new onset hypertension and weight gain Rajesh Jain Endorama 10/01/2015 HPI 27 F with hypertension x 1 year BP 130-140/90 while on amlodipine 5 mg daily She also reports weight gain, 7 LB, mainly
Updates in primary hyperaldosteronism and the rule
 Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. Professor of Medicine and Physiology and Functional Genomics University of Florida College of Medicine and NF/SGVHS The 20-50
Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. Professor of Medicine and Physiology and Functional Genomics University of Florida College of Medicine and NF/SGVHS The 20-50
How to Recognize Adrenal Disease
 How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
Adrenocorticotropic Hormone-Independent Cushing Syndrome with Bilateral Cortisol-Secreting Adenomas
 Case Report Endocrinol Metab 2013;28:133-137 http://dx.doi.org/10.3803/enm.2013.28.2.133 pissn 2093-596X eissn 2093-5978 Adrenocorticotropic Hormone-Independent Cushing Syndrome with Bilateral Cortisol-Secreting
Case Report Endocrinol Metab 2013;28:133-137 http://dx.doi.org/10.3803/enm.2013.28.2.133 pissn 2093-596X eissn 2093-5978 Adrenocorticotropic Hormone-Independent Cushing Syndrome with Bilateral Cortisol-Secreting
MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL?
 MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL? Alice C. Levine, MD Professor of Medicine Division of Endocrinology, Diabetes and Bone Diseases Georgia-AACE 2017 Annual Meeting
MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL? Alice C. Levine, MD Professor of Medicine Division of Endocrinology, Diabetes and Bone Diseases Georgia-AACE 2017 Annual Meeting
Approach to Adrenal Incidentaloma. Alice Y.Y. Cheng, MD, FRCP
 Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Upon completion, participants should be able to:
 Learning Objectives Upon completion, participants should be able to: Describe the causes of secondary hypertension and the prevalence of primary aldosteronism Discuss the diagnostic approach to primary
Learning Objectives Upon completion, participants should be able to: Describe the causes of secondary hypertension and the prevalence of primary aldosteronism Discuss the diagnostic approach to primary
The Work-up and Treatment of Adrenal Nodules
 The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
Updates in primary hyperaldosteronism and the rule
 Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of
Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of
CUSHING SYNDROME Dr. Muhammad Sarfraz
 Indep Rev Jul-Dec 2018;20(7-12) CUSHING SYNDROME Dr. Muhammad Sarfraz IR-655 Abstract: It is defined as clinical condition in which there are increased free circulating glucocorticoides casused by excessive
Indep Rev Jul-Dec 2018;20(7-12) CUSHING SYNDROME Dr. Muhammad Sarfraz IR-655 Abstract: It is defined as clinical condition in which there are increased free circulating glucocorticoides casused by excessive
Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone
 Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Adrenal incidentaloma guideline for Northern Endocrine Network
 Adrenal incidentaloma guideline for Northern Endocrine Network Definition of adrenal incidentaloma Adrenal mass detected on an imaging study done for indications that are not related to an adrenal problem
Adrenal incidentaloma guideline for Northern Endocrine Network Definition of adrenal incidentaloma Adrenal mass detected on an imaging study done for indications that are not related to an adrenal problem
Year 2004 Paper two: Questions supplied by Megan 1
 Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management
 C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management Padma S Menon Professor of Endocrinology, Seth G S Medical College & KEM Hospital, Mumbai A clinical syndrome resulting
C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management Padma S Menon Professor of Endocrinology, Seth G S Medical College & KEM Hospital, Mumbai A clinical syndrome resulting
The Evaluation of the Incidental Adrenal Mass and Not-So-Incidental Adrenal Hormone Excess
 The Evaluation of the Incidental Adrenal Mass and Not-So-Incidental Adrenal Hormone Excess Richard J. Auchus, MD, PhD, FACE Depts. Internal Medicine/MEND & Pharmacology Endocrinology Fellowship Program
The Evaluation of the Incidental Adrenal Mass and Not-So-Incidental Adrenal Hormone Excess Richard J. Auchus, MD, PhD, FACE Depts. Internal Medicine/MEND & Pharmacology Endocrinology Fellowship Program
Subclinical Cushing s Syndrome
 Subclinical Cushing s Syndrome AACE 26th Annual Scientific & Clinical Congress Associate Clinical Professor of Medicine and Clinical Chief University of Miami Miller Scholl of Medicine Miami, Florida aayala2@miami.edu
Subclinical Cushing s Syndrome AACE 26th Annual Scientific & Clinical Congress Associate Clinical Professor of Medicine and Clinical Chief University of Miami Miller Scholl of Medicine Miami, Florida aayala2@miami.edu
A short & obese - girl
 A short & obese - girl Presented by :Dr.Amit P Ghawade (DNB Resident-1st Year ) Guide :Dr.S.Ramkumar MD(pediatrics) ICH & HC, Chennai, DM(endocrinology) AIIMS, Delhi Department of Pediatric Endocrinology
A short & obese - girl Presented by :Dr.Amit P Ghawade (DNB Resident-1st Year ) Guide :Dr.S.Ramkumar MD(pediatrics) ICH & HC, Chennai, DM(endocrinology) AIIMS, Delhi Department of Pediatric Endocrinology
ADRENAL VEIN SAMPLING: AN INTEGRAL PART OF MANAGING COMPLICATED ADRENAL HYPERTENSION- SAFE? WORTH IT?
 ADRENAL VEIN SAMPLING: AN INTEGRAL PART OF MANAGING COMPLICATED ADRENAL HYPERTENSION- SAFE? WORTH IT? Chaitanya Ahuja, M.D. Assistant Professor, Vascular and Interventional Radiology Director of Interventional
ADRENAL VEIN SAMPLING: AN INTEGRAL PART OF MANAGING COMPLICATED ADRENAL HYPERTENSION- SAFE? WORTH IT? Chaitanya Ahuja, M.D. Assistant Professor, Vascular and Interventional Radiology Director of Interventional
Diseases of the Adrenal gland
 Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
Primary Aldosteronism: screening, diagnosis and therapy
 Primary Aldosteronism: screening, diagnosis and therapy Jacques W.M. Lenders, internist DEPT. OF INTERNAL MEDICINE, RADBOUD UNIVERSITY NIJMEGEN MEDICAL CENTER, NIJMEGEN,THE NETHERLANDS DEPT. OF INTERNAL
Primary Aldosteronism: screening, diagnosis and therapy Jacques W.M. Lenders, internist DEPT. OF INTERNAL MEDICINE, RADBOUD UNIVERSITY NIJMEGEN MEDICAL CENTER, NIJMEGEN,THE NETHERLANDS DEPT. OF INTERNAL
Primary Aldosteronism & Implications for Primary Hypertension
 & Implications for Primary Hypertension Richard J. Auchus, MD, PhD, FACE Professor and Fellowship Program Director Depts of Internal Medicine/MEND & Pharmacology University of Michigan Disclosures Contracted
& Implications for Primary Hypertension Richard J. Auchus, MD, PhD, FACE Professor and Fellowship Program Director Depts of Internal Medicine/MEND & Pharmacology University of Michigan Disclosures Contracted
ADRENAL INCIDENTALOMA. Jamii St. Julien
 ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
Adrenal Mass. Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016
 Adrenal Mass Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016 Case Presentation 65F found to have a 4cm left adrenal mass in 2012 now presents with 6.7cm left adrenal mass PMHx:
Adrenal Mass Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016 Case Presentation 65F found to have a 4cm left adrenal mass in 2012 now presents with 6.7cm left adrenal mass PMHx:
Cushing s Syndrome. Diagnosis. GuidelineCentral.com. Key Points. Diagnosis
 Cushing s Syndrome Consultant: Endocrine Society of Cushing s Syndrome Clinical Practice Guideline Writing Committee Key Points GuidelineCentral.com Key Points The most common cause of Cushing s syndrome
Cushing s Syndrome Consultant: Endocrine Society of Cushing s Syndrome Clinical Practice Guideline Writing Committee Key Points GuidelineCentral.com Key Points The most common cause of Cushing s syndrome
PITUITARY: JUST THE BASICS PART 2 THE PATIENT
 PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
TREATMENT OF CUSHING S DISEASE
 TREATMENT OF CUSHING S DISEASE Surgery, Radiation, Medication Peter J Snyder, MD Professor of Medicine Disclosures Novartis Research grant Pfizer Consultant Ipsen Research grant Cortendo Research grant
TREATMENT OF CUSHING S DISEASE Surgery, Radiation, Medication Peter J Snyder, MD Professor of Medicine Disclosures Novartis Research grant Pfizer Consultant Ipsen Research grant Cortendo Research grant
Adrenal Vein Sampling: A Critical Tool for Subtyping Primary Aldosteronism
 Adrenal Vein Sampling: A Critical Tool for Subtyping Primary Aldosteronism Disclosures No conflicts of interest relevant to this presentation Jason W. Pinchot, M.D. Assistant Professor, Vascular and Interventional
Adrenal Vein Sampling: A Critical Tool for Subtyping Primary Aldosteronism Disclosures No conflicts of interest relevant to this presentation Jason W. Pinchot, M.D. Assistant Professor, Vascular and Interventional
Cortisol levels. Naturally produced by the adrenal Cortisol
 1 + 2 Cortisol levels asleep awake Naturally produced by the adrenal Cortisol Man made tablets, injections, creams & inhalers Cortisone Hydrocortisone Prednisone Prednisolone Betamethasone Methylprednisolone
1 + 2 Cortisol levels asleep awake Naturally produced by the adrenal Cortisol Man made tablets, injections, creams & inhalers Cortisone Hydrocortisone Prednisone Prednisolone Betamethasone Methylprednisolone
Adrenal gland Incidentaloma
 Adrenal gland Incidentaloma Topic review 17 sep 2008 Anatomy 1 Anatomical consideration Blood supply Artery: small branches from Inf. phrenic, renal artery and aorta Vein: Rt : medial aspect to IVC Lt
Adrenal gland Incidentaloma Topic review 17 sep 2008 Anatomy 1 Anatomical consideration Blood supply Artery: small branches from Inf. phrenic, renal artery and aorta Vein: Rt : medial aspect to IVC Lt
MedKorat Endocrine Day 2018 Approach to common adrenal disorder
 MedKorat Endocrine Day 2018 Approach to common adrenal disorder Rungnapa Laortanakul, MD Nov.2018 Outline Adrenal insufficiency Cushing s syndrome Pheochromocytoma Primary Aldosteronism Adrenal incidentaloma
MedKorat Endocrine Day 2018 Approach to common adrenal disorder Rungnapa Laortanakul, MD Nov.2018 Outline Adrenal insufficiency Cushing s syndrome Pheochromocytoma Primary Aldosteronism Adrenal incidentaloma
Endocrine MR. Jan 30, 2015 Michael LaFata, MD
 Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
Conferencia III: Dilemas en el tratamiento de Feocromocitomas y Paragangliomas. Dilemmas in Management of Pheochromocytoma and Paraganglioma
 Conferencia III: Dilemas en el tratamiento de Feocromocitomas y Paragangliomas Dilemmas in Management of Pheochromocytoma and Paraganglioma William F. Young, Jr., MD, MSc Mayo Clinic Rochester, MN, USA
Conferencia III: Dilemas en el tratamiento de Feocromocitomas y Paragangliomas Dilemmas in Management of Pheochromocytoma and Paraganglioma William F. Young, Jr., MD, MSc Mayo Clinic Rochester, MN, USA
Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypercortisolism
 Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypercortisolism Howard Sachs, MD Patients Course, 2017 Associate Professor of Clinical Medicine UMass Medical School Adrenal
Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypercortisolism Howard Sachs, MD Patients Course, 2017 Associate Professor of Clinical Medicine UMass Medical School Adrenal
Diagnostic Accuracy of Adrenal Venous Sampling in Comparison with Other Parameters in Primary Aldosteronism
 Endocrine Journal 2008, 55 (5), 839 846 Diagnostic Accuracy of Adrenal Venous Sampling in Comparison with Other Parameters in Primary Aldosteronism ISAO MINAMI, TAKANOBU YOSHIMOTO, YUKI HIRONO, HAJIME
Endocrine Journal 2008, 55 (5), 839 846 Diagnostic Accuracy of Adrenal Venous Sampling in Comparison with Other Parameters in Primary Aldosteronism ISAO MINAMI, TAKANOBU YOSHIMOTO, YUKI HIRONO, HAJIME
Adrenal Incidentalomas. G Stephen DeCherney, MD, MPH Clinical Professor of Medicine Division of Endocrinology UNC School of Medicine
 Adrenal Incidentalomas G Stephen DeCherney, MD, MPH Clinical Professor of Medicine Division of Endocrinology UNC School of Medicine Disclosures No financial, investment, or consulting relationship with
Adrenal Incidentalomas G Stephen DeCherney, MD, MPH Clinical Professor of Medicine Division of Endocrinology UNC School of Medicine Disclosures No financial, investment, or consulting relationship with
Primary aldosteronism (PA), the most common endocrine
, the most common endocrine") Mineralocorticoids Impact of Accessory Hepatic Veins on Adrenal Vein Sampling for Identification of Surgically Curable Primary Aldosteronism Diego Miotto, Renzo De Toni, Gisella Pitter, Teresa Maria Seccia,
Mineralocorticoids Impact of Accessory Hepatic Veins on Adrenal Vein Sampling for Identification of Surgically Curable Primary Aldosteronism Diego Miotto, Renzo De Toni, Gisella Pitter, Teresa Maria Seccia,
SECONDARY HYPERTENSION
 SECONDARY HYPERTENSION Grand round for Medical student 25 October 2013 By Rungnapa Laortanakul, MD. OUTLINE Overview of HT Secondary HT Resistance HT Primary aldosteronism Pheochromocytoma Cushing s syndrome
SECONDARY HYPERTENSION Grand round for Medical student 25 October 2013 By Rungnapa Laortanakul, MD. OUTLINE Overview of HT Secondary HT Resistance HT Primary aldosteronism Pheochromocytoma Cushing s syndrome
Primary aldosteronism clinical practice guidelines: a re-appraisal The Management of Primary Aldosteronism
 Primary aldosteronism clinical practice guidelines: a re-appraisal The Management of Primary Aldosteronism Prof. FRANCO MANTERO Division of Endocrinology University of Padua Italy Case Detection, Diagnosis
Primary aldosteronism clinical practice guidelines: a re-appraisal The Management of Primary Aldosteronism Prof. FRANCO MANTERO Division of Endocrinology University of Padua Italy Case Detection, Diagnosis
Clarification of hypertension Diagnosis of primary hyperaldosteronism
 Nr. 1/2010 Clarification of hypertension Diagnosis of primary hyperaldosteronism Marc Beineke The significance of the /renin ratio (ARR) in the diagnosis of normoalaemic and hypokalaemic primary hyperaldosteronism,
Nr. 1/2010 Clarification of hypertension Diagnosis of primary hyperaldosteronism Marc Beineke The significance of the /renin ratio (ARR) in the diagnosis of normoalaemic and hypokalaemic primary hyperaldosteronism,
CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES
 HORMONES OF ADRENAL CORTEX R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES CONVERSION OF CHOLESTROL TO PREGNENOLONE MINERALOCORTICOCOIDES
HORMONES OF ADRENAL CORTEX R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES CONVERSION OF CHOLESTROL TO PREGNENOLONE MINERALOCORTICOCOIDES
14 Girl with Cushing s Disease: An Update. Kristen Dillard, MD Endorama October 17, 2013
 14 Girl with Cushing s Disease: An Update Kristen Dillard, MD Endorama October 17, 2013 Initial Presentation Pt initially presented to pediatrician for school physical in fall 2012. Pt was found to be
14 Girl with Cushing s Disease: An Update Kristen Dillard, MD Endorama October 17, 2013 Initial Presentation Pt initially presented to pediatrician for school physical in fall 2012. Pt was found to be
Adrenal venous sampling as used in a patient with primary pigmented nodular adrenocortical disease
 Original Article on Translational Imaging in Cancer Patient Care Adrenal venous sampling as used in a patient with primary pigmented nodular adrenocortical disease Xiaoxin Peng 1, Yintao Yu 1, Yi Ding
Original Article on Translational Imaging in Cancer Patient Care Adrenal venous sampling as used in a patient with primary pigmented nodular adrenocortical disease Xiaoxin Peng 1, Yintao Yu 1, Yi Ding
Spectrum of Hypertension & Hypokalemia
 Spectrum of Hypertension & Hypokalemia Farheen K. Dojki, PGY-6 Hypertension Fellow, ASH Hypertension Center Dr. Dojki does not have any relevant financial relationships with any commercial interests. OBJECTIVES:
Spectrum of Hypertension & Hypokalemia Farheen K. Dojki, PGY-6 Hypertension Fellow, ASH Hypertension Center Dr. Dojki does not have any relevant financial relationships with any commercial interests. OBJECTIVES:
Stelios Mantis, MD DuPage Medical Group Pediatric Endocrinology
 Stelios Mantis, MD DuPage Medical Group Pediatric Endocrinology 4 11 13 Initial Presentation Pt initially presented to pediatrician for school physical in fall 2012. Pt was found to be overweight (BMI:
Stelios Mantis, MD DuPage Medical Group Pediatric Endocrinology 4 11 13 Initial Presentation Pt initially presented to pediatrician for school physical in fall 2012. Pt was found to be overweight (BMI:
Current Management of Adrenal Cortical Carcinoma
 Current Management of Adrenal Cortical Carcinoma American Association of Clinical Endocrinologists Texas Chapter of the AACE Annual Meeting And Texas Endocrine Surgery Symposium August 4, 2017 Jeffrey
Current Management of Adrenal Cortical Carcinoma American Association of Clinical Endocrinologists Texas Chapter of the AACE Annual Meeting And Texas Endocrine Surgery Symposium August 4, 2017 Jeffrey
A Rare Case of ACTH-independent Macronodular Adrenal Hyperplasia Associated with Aldosterone-producing Adenoma
 CASE REPORT A Rare Case of ACTHindependent Macronodular Adrenal Hyperplasia Associated with Aldosteroneproducing Adenoma Eri Hayakawa 1, Takanobu Yoshimoto 1, Kiichiro Hiraishi 1, Masako Kato 1, Hajime
CASE REPORT A Rare Case of ACTHindependent Macronodular Adrenal Hyperplasia Associated with Aldosteroneproducing Adenoma Eri Hayakawa 1, Takanobu Yoshimoto 1, Kiichiro Hiraishi 1, Masako Kato 1, Hajime
How to approach resistant hypertension. Teh-Li Huo, M.D., Ph.D.
 How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
Dimitrios Linos, M.D., Ph.D. Professor of Surgery National & Kapodistrian University of Athens
 Dimitrios Linos, M.D., Ph.D. Professor of Surgery National & Kapodistrian University of Athens What is an adrenal incidentaloma? An adrenal incidentaloma is defined as an adrenal tumor initially diagnosed
Dimitrios Linos, M.D., Ph.D. Professor of Surgery National & Kapodistrian University of Athens What is an adrenal incidentaloma? An adrenal incidentaloma is defined as an adrenal tumor initially diagnosed
A 64 year old man referred for evaluation of suspected hyperaldosteronism
 A 64 year old man referred for evaluation of suspected hyperaldosteronism Dr. Dickens does not have any relevant financial relationships with any commercial interests. ENDORAMA: 64 year old man referred
A 64 year old man referred for evaluation of suspected hyperaldosteronism Dr. Dickens does not have any relevant financial relationships with any commercial interests. ENDORAMA: 64 year old man referred
2
 1 2 General % Obesity 90 Hypertension 85 Skin Plethora 70 Hirsutism/hair loss 75 Striae 50 Acne 35 Bruising/thinning 35 Musculoskeletal Osteopenia/porosis 80 Weakness 65 Neuropsych % Lability,euphoria,insomnia,
1 2 General % Obesity 90 Hypertension 85 Skin Plethora 70 Hirsutism/hair loss 75 Striae 50 Acne 35 Bruising/thinning 35 Musculoskeletal Osteopenia/porosis 80 Weakness 65 Neuropsych % Lability,euphoria,insomnia,
Pituitary Adenomas: Evaluation and Management. Fawn M. Wolf, MD 10/27/17
 Pituitary Adenomas: Evaluation and Management Fawn M. Wolf, MD 10/27/17 Over 18,000 pituitaries examined at autopsy: -10.6% contained adenomas (1.5-27%) -Frequency similar for men and women and across
Pituitary Adenomas: Evaluation and Management Fawn M. Wolf, MD 10/27/17 Over 18,000 pituitaries examined at autopsy: -10.6% contained adenomas (1.5-27%) -Frequency similar for men and women and across
A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY
 A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY Case 57 y.o. male CC: Weakness HPI: About 20 years ago, he developed bilateral lower extremity weakness. Laboratory
A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY Case 57 y.o. male CC: Weakness HPI: About 20 years ago, he developed bilateral lower extremity weakness. Laboratory
Disorders of the Adrenal Cortex
 Disorders of the Adrenal Cortex Cushing s Syndrome and Primary Aldosteronism 凌雁 Yan Ling Department of Endocrinology and Metabolism Zhongshan Hospital Fudan University Cushing s Syndrome Definition of
Disorders of the Adrenal Cortex Cushing s Syndrome and Primary Aldosteronism 凌雁 Yan Ling Department of Endocrinology and Metabolism Zhongshan Hospital Fudan University Cushing s Syndrome Definition of
ACTH-dependent Cushing s Syndrome Update AACE MI Chapter Annual Meeting September 22, Lynnette K. Nieman DEOB, NIDDK, NIH, DHHS
 ACTH-dependent Cushing s Syndrome Update AACE MI Chapter Annual Meeting September 22, 2018 Lynnette K. Nieman DEOB, NIDDK, NIH, DHHS Objectives At the conclusion of this presentation, participants should
ACTH-dependent Cushing s Syndrome Update AACE MI Chapter Annual Meeting September 22, 2018 Lynnette K. Nieman DEOB, NIDDK, NIH, DHHS Objectives At the conclusion of this presentation, participants should
The endocrine system is made up of a complex group of glands that secrete hormones.
 1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
EndocrinologyUpdate. Endoscopic Transnasal Surgical Technique for Pituitary Tumors
 EndocrinologyUpdate Endocrinology News from Mayo Clinic Vol. 4, No. 1, 2009 Endoscopic Transnasal Surgical Technique for Pituitary Tumors INSIDE THIS ISSUE 3 Primary Aldosteronism: The Role of Adrenal
EndocrinologyUpdate Endocrinology News from Mayo Clinic Vol. 4, No. 1, 2009 Endoscopic Transnasal Surgical Technique for Pituitary Tumors INSIDE THIS ISSUE 3 Primary Aldosteronism: The Role of Adrenal
Adrenal Disorders. Disclosure: I do not have any conflicts of interest
 Adrenal Disorders Robert G. Dluhy, M.D. Disclosure: I do not have any conflicts of interest Robert G. Dluhy, MD Case 1 28 y.o. male with no significant past medical history presents with 6-8 months of
Adrenal Disorders Robert G. Dluhy, M.D. Disclosure: I do not have any conflicts of interest Robert G. Dluhy, MD Case 1 28 y.o. male with no significant past medical history presents with 6-8 months of
False-positive inferior petrosal sinus sampling in the diagnosis of Cushing s disease
 J Neurosurg 83:1087 1091, 1995 False-positive inferior petrosal sinus sampling in the diagnosis of Cushing s disease Report of two cases YOSHIHIRO YAMAMOTO, M.D., D.M.SC., DUDLEY H. DAVIS, M.D., TODD B.
J Neurosurg 83:1087 1091, 1995 False-positive inferior petrosal sinus sampling in the diagnosis of Cushing s disease Report of two cases YOSHIHIRO YAMAMOTO, M.D., D.M.SC., DUDLEY H. DAVIS, M.D., TODD B.
Resistant hypertension is defined as blood. Primary Hyperaldosteronism Decoded: A Case of Curable Resistant Hypertension.
 Case Review Primary Hyperaldosteronism Decoded: A Case of Curable Resistant Hypertension Timothy R. Larsen, DO, Wadie David, Susan Steigerwalt, MD, Shukri David, MD Department of Internal Medicine, Section
Case Review Primary Hyperaldosteronism Decoded: A Case of Curable Resistant Hypertension Timothy R. Larsen, DO, Wadie David, Susan Steigerwalt, MD, Shukri David, MD Department of Internal Medicine, Section
Index. F Fatigue, 59 Food-dependent Cushing s syndrome, 286
 A Abdominal red striae, 57, 58 Aberrant hormone receptors, AIMAH familial forms, 215 investigative protocols, 217 218 molecular mechanisms, 216, 217 paracrine mechanisms, 216 steroidogenesis, 212 213 in
A Abdominal red striae, 57, 58 Aberrant hormone receptors, AIMAH familial forms, 215 investigative protocols, 217 218 molecular mechanisms, 216, 217 paracrine mechanisms, 216 steroidogenesis, 212 213 in
in Primary Care (Part 2) Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University
 Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University") Common Endocrine Problems Seen in Primary Care (Part 2) Lecture #34 Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University None Conflict of Interest Topics to be Covered
Common Endocrine Problems Seen in Primary Care (Part 2) Lecture #34 Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University None Conflict of Interest Topics to be Covered
ACTH stimulation test and computed tomography are useful for differentiating the subtype of primary aldosteronism
 2017, 64 (1), 65-73 Original ACTH stimulation test and computed tomography are useful for differentiating the subtype of primary aldosteronism Ayako Moriya 1), Masaaki Yamamoto 1), Shunsuke Kobayashi 1),
2017, 64 (1), 65-73 Original ACTH stimulation test and computed tomography are useful for differentiating the subtype of primary aldosteronism Ayako Moriya 1), Masaaki Yamamoto 1), Shunsuke Kobayashi 1),
The Management of adrenal incidentaloma
 The Management of adrenal incidentaloma Dimitrios Linos, MD Director of Surgery, Hygeia Hospital, Athens, Greece Consultant in Surgery, Massachusetts General Hospital, Boston, USA 8 th Postgraduate Course
The Management of adrenal incidentaloma Dimitrios Linos, MD Director of Surgery, Hygeia Hospital, Athens, Greece Consultant in Surgery, Massachusetts General Hospital, Boston, USA 8 th Postgraduate Course
PREOPERATIVE DIAGNOSIS AND LOCALIZATION OF ALDOSTERONE-PRODUCING ADENOMA BY ADRENAL VENOUS SAMPLING AFTER ADMINISTRATION OF METOCLOPRAMIDE
 K.D. Wu, T.S. Liao, Y.M. Chen, et al PREOPERATIVE DIAGNOSIS AND LOCALIZATION OF ALDOSTERONE-PRODUCING ADENOMA BY ADRENAL VENOUS SAMPLING AFTER ADMINISTRATION OF METOCLOPRAMIDE Kwan-Dun Wu, Tsou-Song Liao,
K.D. Wu, T.S. Liao, Y.M. Chen, et al PREOPERATIVE DIAGNOSIS AND LOCALIZATION OF ALDOSTERONE-PRODUCING ADENOMA BY ADRENAL VENOUS SAMPLING AFTER ADMINISTRATION OF METOCLOPRAMIDE Kwan-Dun Wu, Tsou-Song Liao,
3- & 12-Year-Old Sisters with Li-Fraumeni Syndrome KRISTEN DILLARD, M.D. ENDORAMA FEBRUARY 28, 2013
 3- & 12-Year-Old Sisters with Li-Fraumeni Syndrome KRISTEN DILLARD, M.D. ENDORAMA FEBRUARY 28, 2013 Presentation Sisters referred by Peds Oncology to Endo clinic for adrenocortical carcinoma screening
3- & 12-Year-Old Sisters with Li-Fraumeni Syndrome KRISTEN DILLARD, M.D. ENDORAMA FEBRUARY 28, 2013 Presentation Sisters referred by Peds Oncology to Endo clinic for adrenocortical carcinoma screening
Challenging Pituitary Cases. Laurence Katznelson, MD Professor of Medicine and Neurosurgery Stanford University School of Medicine
 Challenging Pituitary Cases Laurence Katznelson, MD Professor of Medicine and Neurosurgery Stanford University School of Medicine 1 34 yo male has incidental finding of large macroadenoma, with prolactin
Challenging Pituitary Cases Laurence Katznelson, MD Professor of Medicine and Neurosurgery Stanford University School of Medicine 1 34 yo male has incidental finding of large macroadenoma, with prolactin
Cushing s syndrome and adrenal insufficiency
 Cushing s syndrome and adrenal insufficiency Clinician expectations 1 ALIREZA ESTEGHAMATI,MD PROFESSOR OF ENDOCRINOLOGY TUMS APRIL 2016 Main Challenges Rare but important Mild forms (unrecognized) Cyclic
Cushing s syndrome and adrenal insufficiency Clinician expectations 1 ALIREZA ESTEGHAMATI,MD PROFESSOR OF ENDOCRINOLOGY TUMS APRIL 2016 Main Challenges Rare but important Mild forms (unrecognized) Cyclic
Endocrine hypertensionmolecules. Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015
 Endocrine hypertensionmolecules and genes Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015 Plan Mineralocorticoid hypertension Myths surrounding Primary Aldosteronism (PA) New developments
Endocrine hypertensionmolecules and genes Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015 Plan Mineralocorticoid hypertension Myths surrounding Primary Aldosteronism (PA) New developments
Indications for Surgical Removal of Adrenal Glands
 The adrenal glands are orange-colored endocrine glands which are located on the top of both kidneys. The adrenal glands are triangular shaped and measure about one-half inch in height and 3 inches in length.
The adrenal glands are orange-colored endocrine glands which are located on the top of both kidneys. The adrenal glands are triangular shaped and measure about one-half inch in height and 3 inches in length.
Measurement of Renin Activity using Tandem Mass Spectrometry Ravinder J Singh, PhD, DABCC Mayo Clinic, Rochester, MN
 Measurement of Renin Activity using Tandem Mass Spectrometry Ravinder J Singh, PhD, DABCC Mayo Clinic, Rochester, MN Renin Angiotension System Weber, et al. NEJM 2001; 345:1690. Renin Angiotension System
Measurement of Renin Activity using Tandem Mass Spectrometry Ravinder J Singh, PhD, DABCC Mayo Clinic, Rochester, MN Renin Angiotension System Weber, et al. NEJM 2001; 345:1690. Renin Angiotension System
Therapeutic Objectives. Cushing s Disease Surgical Results. Cushing s Disease Surgical Results: Macroadenomas 10/24/2015
 Therapeutic Objectives Update on the Management of Lewis S. Blevins, Jr., M.D. Correct the syndrome by lowering daily cortisol secretion to normal Eradicate any tumor that might threaten the health of
Therapeutic Objectives Update on the Management of Lewis S. Blevins, Jr., M.D. Correct the syndrome by lowering daily cortisol secretion to normal Eradicate any tumor that might threaten the health of
Potassium A NNA VINNIKOVA, M. D.
 Potassium A NNA VINNIOVA, M. D. DIVISION OF NEPHROLOGY Graphics by permission from The Fluid, Electrolyte and Acid-Base Companion, S. Faubel and J. Topf, http://www.pbfluids.com Do you want to hear a Sodium
Potassium A NNA VINNIOVA, M. D. DIVISION OF NEPHROLOGY Graphics by permission from The Fluid, Electrolyte and Acid-Base Companion, S. Faubel and J. Topf, http://www.pbfluids.com Do you want to hear a Sodium
JACK L. SNITZER, DO INTERNAL MEDICINE BOARD REVIEW COURSE 2018 PITUITARY
 JACK L. SNITZER, DO INTERNAL MEDICINE BOARD REVIEW COURSE 2018 PITUITARY JACK L. SNITZER, D.O. Peninsula Regional Endocrinology 1415 S. Division Street Salisbury, MD 21804 Phone:410-572-8848 Fax:410-572-6890
JACK L. SNITZER, DO INTERNAL MEDICINE BOARD REVIEW COURSE 2018 PITUITARY JACK L. SNITZER, D.O. Peninsula Regional Endocrinology 1415 S. Division Street Salisbury, MD 21804 Phone:410-572-8848 Fax:410-572-6890
COPYRIGHTED MATERIAL. Adrenal Imaging. 1.1 Introduction. Khaled M. Elsayes 1, Isaac R. Francis 1, Melvyn Korobkin 1 and Gerard M.
 1 Adrenal Imaging Khaled M. Elsayes 1, Isaac R. Francis 1, Melvyn Korobkin 1 and Gerard M. Doherty 2 1 Department of Radiology, University of Michigan 2 Department of Radiology and Surgery, University
1 Adrenal Imaging Khaled M. Elsayes 1, Isaac R. Francis 1, Melvyn Korobkin 1 and Gerard M. Doherty 2 1 Department of Radiology, University of Michigan 2 Department of Radiology and Surgery, University
Original Research Article
 Medrech ISSN No. 2394-3971 Original Research Article TYPE 2 DIABETES WITH RECURRENT OSTEOPOROTIC FRACTURES, OR CUSHING S SYNDROME? Blertina Dyrmishi¹*; Taulant Olldashi²; Prof Asc Thanas Fureraj 3 ; Prof
Medrech ISSN No. 2394-3971 Original Research Article TYPE 2 DIABETES WITH RECURRENT OSTEOPOROTIC FRACTURES, OR CUSHING S SYNDROME? Blertina Dyrmishi¹*; Taulant Olldashi²; Prof Asc Thanas Fureraj 3 ; Prof
Changes in the clinical manifestations of primary aldosteronism
 ORIGINAL ARTICLE Korean J Intern Med 2014;29:217-225 Changes in the clinical manifestations of primary aldosteronism Sun Hwa Kim, Jae Hee Ahn, Ho Cheol Hong, Hae Yoon Choi, Yoon Jung Kim, Nam Hoon Kim,
ORIGINAL ARTICLE Korean J Intern Med 2014;29:217-225 Changes in the clinical manifestations of primary aldosteronism Sun Hwa Kim, Jae Hee Ahn, Ho Cheol Hong, Hae Yoon Choi, Yoon Jung Kim, Nam Hoon Kim,
Endocrine Hypertension
 Endocrine Hypertension 1 No Disclosures Endocrine Hypertension Objectives: 1. Understand Endocrine disorders causing hypertension 2. Understand clinical presentation of Pheochromocytoma and Hyperaldosteronism
Endocrine Hypertension 1 No Disclosures Endocrine Hypertension Objectives: 1. Understand Endocrine disorders causing hypertension 2. Understand clinical presentation of Pheochromocytoma and Hyperaldosteronism
THE HIGHS AND LOWS OF ADRENAL GLAND PATHOLOGY
 THE HIGHS AND LOWS OF ADRENAL GLAND PATHOLOGY Symptoms of Adrenal Gland Disorders 2 Depends on whether it is making too much or too little hormone And on what you Google! Symptoms include obesity, skin
THE HIGHS AND LOWS OF ADRENAL GLAND PATHOLOGY Symptoms of Adrenal Gland Disorders 2 Depends on whether it is making too much or too little hormone And on what you Google! Symptoms include obesity, skin
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences. Endocrinology. (Review) Year 5 Internal Medicine
 Year 5 Internal Medicine") Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
Adrenal incidentaloma
 Adrenal incidentaloma Prevalence 5% post-mortem series 4% CT series 6-20% CT series in patients with Hx extra-adrenal malignancy Commoner with increasing age Associated with adrenal hyperfunction in 15%
Adrenal incidentaloma Prevalence 5% post-mortem series 4% CT series 6-20% CT series in patients with Hx extra-adrenal malignancy Commoner with increasing age Associated with adrenal hyperfunction in 15%
Endocrine. Endocrine as it relates to the kidney. Sarah Elfering, MD University of Minnesota
 Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Inquadramento Clinico dell IncIdentaloma SurrenalIco
 Ferrara, 7 dicembre 2012 Inquadramento Clinico dell IncIdentaloma SurrenalIco Marta Bondanelli Sezione di Endocrinologia Dip. di Scienze Mediche Università degli Studi di Ferrara ADRENAL INCIDENTALOMA
Ferrara, 7 dicembre 2012 Inquadramento Clinico dell IncIdentaloma SurrenalIco Marta Bondanelli Sezione di Endocrinologia Dip. di Scienze Mediche Università degli Studi di Ferrara ADRENAL INCIDENTALOMA
Endogenous Cushing s syndrome: The Philippine general hospital experience
 ORIGINAL ARTICLE Endogenous Cushing s syndrome: The Philippine general hospital experience Tom Edward N. Lo, Joyce M. Cabradilla, Sue Ann Lim, Cecilia A. Jimeno Section of Endocrinology and Metabolism,
ORIGINAL ARTICLE Endogenous Cushing s syndrome: The Philippine general hospital experience Tom Edward N. Lo, Joyce M. Cabradilla, Sue Ann Lim, Cecilia A. Jimeno Section of Endocrinology and Metabolism,
Adrenal Ganglioneuroma Presenting With Adrenal Insufficiency After Unilateral Adrenalectomy
 ISPUB.COM The Internet Journal of Urology Volume 9 Number 1 Adrenal Ganglioneuroma Presenting With Adrenal Insufficiency After Unilateral Adrenalectomy S Bontha, N Sanalkumar, M Istarabadi, G Lepsien,
ISPUB.COM The Internet Journal of Urology Volume 9 Number 1 Adrenal Ganglioneuroma Presenting With Adrenal Insufficiency After Unilateral Adrenalectomy S Bontha, N Sanalkumar, M Istarabadi, G Lepsien,
Functional Pituitary Adenomas. Fawn M. Wolf, MD 2/2/2018
 Functional Pituitary Adenomas Fawn M. Wolf, MD 2/2/2018 Outline Prolactinoma Acromegaly Cushing s disease Thyrotroph adenomas Gonadotroph adenomas Hyperprolactinemia Clinically apparent prolactinomas:
Functional Pituitary Adenomas Fawn M. Wolf, MD 2/2/2018 Outline Prolactinoma Acromegaly Cushing s disease Thyrotroph adenomas Gonadotroph adenomas Hyperprolactinemia Clinically apparent prolactinomas:
Diagnostic Role of Captopril Challenge Test in Korean Subjects with High Aldosterone-to-Renin Ratios
 Original Article Endocrinol Metab 2016;31:277-283 http://dx.doi.org/10.3803/enm.2016.31.2.277 pissn 2093-596X eissn 2093-5978 Diagnostic Role of Captopril Challenge Test in Korean Subjects with High Aldosterone-to-Renin
Original Article Endocrinol Metab 2016;31:277-283 http://dx.doi.org/10.3803/enm.2016.31.2.277 pissn 2093-596X eissn 2093-5978 Diagnostic Role of Captopril Challenge Test in Korean Subjects with High Aldosterone-to-Renin
RECURRENT ADRENAL DISEASE. Megan Applewhite Endorama 2/19/2015 SR , SC
 RECURRENT ADRENAL DISEASE Megan Applewhite Endorama 2/19/2015 SR 2412318, SC 3421561 Category: Adrenal Attendings: Angelos & Grogan PATIENT #1 36yo woman with a hx of Cushing s Syndrome and right adrenalectomy
RECURRENT ADRENAL DISEASE Megan Applewhite Endorama 2/19/2015 SR 2412318, SC 3421561 Category: Adrenal Attendings: Angelos & Grogan PATIENT #1 36yo woman with a hx of Cushing s Syndrome and right adrenalectomy
Adrenal Vein Sampling
 Authoriser: Peter Beresford Page 1 of 10 Adrenal Vein Sampling Indications This test is only appropriate if (1) biochemistry points to hyperaldosteronism and (2) if the patient is for active consideration
Authoriser: Peter Beresford Page 1 of 10 Adrenal Vein Sampling Indications This test is only appropriate if (1) biochemistry points to hyperaldosteronism and (2) if the patient is for active consideration
CUSHING S SYNDROME. Chapter 8. Case: A 43-year-old man with delusions
 Chapter 8 CUSHING S SYNDROME Case: A 43-year-old man with delusions A previously healthy 43-year-old man is brought to the emergency department for evaluation of confusion. The patient has complained to
Chapter 8 CUSHING S SYNDROME Case: A 43-year-old man with delusions A previously healthy 43-year-old man is brought to the emergency department for evaluation of confusion. The patient has complained to
Roles of Clinical Criteria, Computed Tomography Scan, and Adrenal Vein Sampling in Differential Diagnosis of Primary Aldosteronism Subtypes
 ORIGINAL Endocrine ARTICLE Care Roles of Clinical Criteria, Computed Tomography Scan, and Adrenal Vein Sampling in Differential Diagnosis of Primary Aldosteronism Subtypes Paolo Mulatero, Chiara Bertello,
ORIGINAL Endocrine ARTICLE Care Roles of Clinical Criteria, Computed Tomography Scan, and Adrenal Vein Sampling in Differential Diagnosis of Primary Aldosteronism Subtypes Paolo Mulatero, Chiara Bertello,
ADRENAL LESIONS 10/09/2012. Adrenal + lesion. Introduction. Common causes. Anatomy. Financial disclosure. Dr. Boraiah Sreeharsha. Nothing to declare
 ADRENAL LESIONS Financial disclosure Nothing to declare Dr. Boraiah Sreeharsha MBBS;FRCR;FRCPSC Introduction Adrenal + lesion Adrenal lesions are common 9% of the population Increase in the detection rate
ADRENAL LESIONS Financial disclosure Nothing to declare Dr. Boraiah Sreeharsha MBBS;FRCR;FRCPSC Introduction Adrenal + lesion Adrenal lesions are common 9% of the population Increase in the detection rate
Aberrant hormone receptors in primary aldosteronism. André Lacroix, MD
 Aberrant hormone receptors in primary aldosteronism André Lacroix, MD Professor of Medicine Centre hospitalier de l Université de Montréal (CHUM) Controversias Clinicas en Enfermedades Suprarenales Buenos
Aberrant hormone receptors in primary aldosteronism André Lacroix, MD Professor of Medicine Centre hospitalier de l Université de Montréal (CHUM) Controversias Clinicas en Enfermedades Suprarenales Buenos