Jaundice Meningitis Basic Fluid Management
|
|
|
- Rudolph Jordan
- 6 years ago
- Views:
Transcription
1 Jaundice Meningitis Basic Fluid Management
2 To be able to thoroughly evaluate and treat Hyperbilirubinemia To be able to recognize meningitis and treat Understand and calculate daily maintenance fluid volume needs for a well child. Understand and calculate daily maintenance sodium and potassium needs for a well child Estimate and replace fluid and electrolytes in the dehydrated child

3
4 Hyperbilirubinemia was more of a problem prior to Rhogam approval in Since, the use of Rhogam Hemolytic Disease of the Newborn (HDN) has dramatically decreased. We no longer see the high bilirubin levels that necessitate double volume exchange transfusion.
5 Kernicterus Unconjugated bilirubin encephalopathy Three Clinical Phases hypotonia, lethargy, poor suck in the first day or so hypertonia +/- opisthotonus towards the end of the first week when there is often also a high-pitched cry, fever and seizures then a third phase when the baby again becomes hypotonic Survivors tend to have choreoathetoid cerebral palsy and hearing impairment.
6 ASSESS An Infant s Risk It s not just the Bhutani Nomogram and Bilitool
7 Family History Pregnancy History Birth History Feeding History Stooling History Weight Loss Sepsis Risk Time of Onset of Jaundice Newborn Bilirubin Results
8 Family History of Jaundice Cystic Fibrosis G6PD Other Blood Disorders or Hemolytic Processes Ethnicity
9 Blood Type Rh Isoimmune Antibodies Maternal Diabetes Hepatitis
10 Gestational Age Birth Trauma In s and Out s and Other Vitals Weight Loss-Calculated as % decreased from Birth Weight Feeding History-Latch,Frequency,Interest Stool color, frequency, and passage of meconium in the first 24 hours
11 REMEMBER JAUNDICE IN THE FIRST 24 HOURS IS NEVER NORMAL Direct Hyperbilirubinemia needs further investigation Direct Hyperbilirubinemia >2mg/dl or >10% of the total serum bili
12
13 When using this nomogram, remember that "risk" refers to the risk of a subsequent bilirubin level in that infant >95%ile for age.
14 Hour-specific Nomogram for Risk Stratification Infants age Total bilirubin Risk zone 36 hours 12.9 mg/dl High Risk Risk zone is one of several risk factors for developing severe hyperbilirubinemia. Please see AAP Phototherapy Guidelines below. If phototherapy threshold IS exceeded, please also review AAP Guidelines for Exchange Transfusion. If phototherapy threshold IS NOT exceeded, please see recommended follow-up in sidebar to the right. A follow-up bilirubin is recommended in 6-12 hours if known hemolysis by direct Coomb's or ETCO (end-tidal carbon monoxide) and otherwise recommended within 24 hours (high risk) AAP Phototherapy Guidelines (2004) Neurotoxicity risk zone Start phototherapy? Approximate threshold at 36 hours of age Lower Risk (>= 38 weeks and well) No 13.6 mg/dl Medium Risk (>=38 weeks + neurotoxicity risk factors OR 35 to 37 6/7 weeks and well) Yes 11.7 mg/dl Higher Risk (35 to 37 6/7 weeks and neurotoxicity risk factors) Yes 9.6 mg/dl
15 Maximum Rate of increase in bilirubin for an infant with a non-hemolytic process is 5mg/dl/24 hours or 0.2mg/dl/hr This is helpful to calculate because if you are fortunate to have a previous bili level then at a level greater than or close 0.2mg/dl/hr you will reach light level.
16 CBC with diff and peripheral smear Reticulocyte Count Coomb s Electrolytes Albumin LFT s If history warrants, sepsis work-up


17 Adequate Hydration Phototherapy Additional Labs Repeat Bilirubin

18

19
20
21 Fever Irritability Nausea Vomiting Headache Myalgia Back Pain Photophobia
22

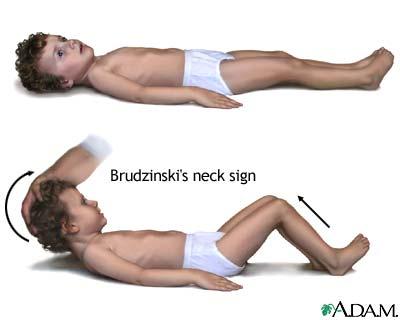
23 Bulging Fontanelle in Infants Irritable Stiff Neck Positive Kernig and Brudniski Sign

24
25
26 CSF finding Viral Bacterial Partially Treated Bacterial Lyme Fungal TB Leukocytes/ mm 3 < 1000 > 1000 [a] > 1000 < 500 < 500 < 300 Polymorphon 20 40% [b] > 85 90% > 80% < 10% < 10 20% < 10 20% [b] uclear cells Protein N or < 100 > > 100 < 100 > > (mg/dl) Glucose N [c] UD to < 40 < 40 N < 40 < 40 (mg/dl) Blood-toglucose ratio N < 0.4 < 0.4 N < 0.4 < 0.4 Positive smear [d] Positive culture PCR or other methods > 85% [e] 80% < 40% < 30% Rare > 95% < 90% > 30% [f] < 30% Enterovirus, herpesvirus 16S RNA, bacterial DNA 16S RNA, bacterial DNA Borrelia burdgorferi antibodies Histoplasma Mycobacteriu and m Cryptococcu tuberculosis s antigen, India ink for Cryptococcu s
27 Bacteria Antibiotic of Choice Other Useful Antibiotics Neisseria meningitidis Penicillin G or ampicillin Cefotaxime or ceftriaxone Haemophilus influenzae Cefotaxime or ceftriaxone Ampicillin or chloramphenicol [a] Streptococcus pneumoniae [b] 1. Penicillin-susceptible (MIC Penicillin G or ampicillin < 0.1 μg/ml) 2. Penicillin-intermediate Cefotaxime or ceftriaxone (MIC = μg/ml) with/without vancomycin 3. Penicillin-resistant (MIC = Cefotaxime or ceftriaxone [c] 1.0 μg/ml) plus vancomycin 4. Cephalosporinnonsusceptible (MIC > 0.5 plus vancomycin Cefotaxime or ceftriaxone [c] μg/ml) Cefotaxime or ceftriaxone Cefepime or meropenem Cefepime or meropenem Add rifampin to antibiotics of choice Meropenem + vancomycin (see text) New fluoroquinolones d Listeria monocytogenes Ampicillin? gentamicin Trimethoprimsulfamethoxazole Streptococcus agalactiae Penicillin G? gentamicin Ampicillin? gentamicin Enterobacteriaceae Cefotaxime or ceftriaxone with/without aminoglycoside Cefepime or meropenem Pseudomonas aeruginosa Ceftazidime + amikacin Cefepime or meropenem
28 Supportive Care with fluids (TREAT Shock!), antiemetic (Zofran) Cefotaxime/Ceftriaxone Vancomycin dosed at 60mg/kg/day/q6 Adjunct therapy with dexamethasone at mg/kg/day/BID-TID. Needs to be administered before or during first dose of antibiotics
29 Streptococcus pneumoniae days Neisseria meningitidis 4-7 days Haemophilus influenzae 7-10 days
30 Seizures Infarctions Septic Shock Subdural Effusions Prolonged Fevers Hearing Loss

31
32



33 Sugar Water Salt
34 Shock or acute deficits Treat shock or dehydration first Maintenance Calculate fluid and electrolytes for normal situations. Adjustments Adjust for or fluid or electrolyte needs. Reassess therapy regularly
35 Isotonic Solution-Normal Saline/Lactated Ringers Bolus 20cc/kg Bolus to perfusion and clinical improvement If no improvement after the third bolus reassess and other fluids or pressors
36 Holliday-Segar Method This method is based on the assumption that for every 100 calories metabolized 100ml of water is required. This method is based on metabolic rate. THIS METHOD DOES NOT WORK FOR INFANTS LESS THAN 14 DAYS OLD
37 Weight = Kilocalories expended = Volume (ml) of H 2 O needed Weight kcal / 24hr cc / 24 hr Infant < 10 kg (4) 100 kcal / kg 100 cc/kg Child kg (2) For each kg (1) 1000 kcal + 50 kcal per kg over cc+ 50cc/kg 1500 kcal + 20 kcal per kg over cc+20cc/kg Max ~2400 cc/day (~100 cc/hr)***
38 Sodium 3 meq / 100 kcal (100 ml fluid) = 30 meq NaCl / L Potassium 2 meq/100 kcal (100 ml fluid) = 20 meq KCl / L
39 50 grams dextrose per 1000 ml water Glucose is the principle nutrition for the brain, heart and red blood cells. 5% Dextrose (metabolizes to glucose) provides adequate short term nutrition in the resting state (20% of caloric RDA).
40
41 We need Sodium 3 meq per 100 ml = 30 meq NaCl / L We have: Normal Saline (0.9% NaCl) = 154 meq/l ½ NS (0.45% NaCl) = 72 meq/l ¼ NS (0.2% NaCl) = 34 meq/l Potassium 2 meq/l per 100 ml = 20 meq/l Order: D5 ¼ NS with 20 meq KCl/L for maintenance fluid Why then is Everyone writing for 1/2NS or NS on the Pediatric Wards?
42 Many sick patients need more than ¼ NS (0.2% NaCl). They are at risk for hyponatremia with hypotonic fluid. Due to Elevated Anti-Diuretic Hormone (ADH). Infection Drugs Hypovolemia Neurologic disease Pain / anxiety Surgery / anesthesia
43 Older Child 3% (30 ml/kg) 6% (60 ml/kg) 9% (90 ml/kg) Infant Preillness weight illness 5% (50 ml/kg) 10% (100 ml/kg) 15% (150 ml/kg) EXAMINATION weight/preillness weight Dehydration Mild Moderate Severe Skin turgor Normal Tenting None Skin (touch) Normal Dry Clammy x100%= % Buccal mucosa/lips Dry Dry Parched/cracked Eyes Normal Deep set Sunken Tears Present Reduced None Fontanelle Flat Soft Sunken Dehydrated=Necessary Fluid Replacement CNS Consolable Irritable Lethargic/obtunded Pulse rate Normal Slightly increased Increased Pulse quality Normal Weak Feeble/impalpable Capillary refill Normal ~2 sec >3 sec Urine output Normal to Decreased Decreased Anuric Data from Kliegman RM, Behrman RE, Jenson HB, et al: Nelson textbook of pediatrics, 18th ed. Philadelphia, WB Saunders, 2007; and Oski FA: Principles and practice of pediatrics, 4th ed. Philadelphia, JB Lippincott, 2006

44 Johns Hopkins: The Harriet Lane Handbook, 19th ed.
45 Anything over 40cc/kg/day or 20cc/kg/shift needs to be replaced. Replacement fluid is either ½ NS or NS Remember to Reassess your Patient!
46 Method: Give 5 10 ml of oral rehydration solution (ORS) every 5 10 minutes, gradually increasing volume Deficit replacement: Mild dehydration = 50 ml/kg over 4 hours Moderate dehydration = 100 ml/kg over 4 hours Maintenance: Infants should resume formula/breastmilk by mouth (PO) ad lib. Children should continue with regular diet Ongoing losses: Regardless of the degree of dehydration, give additional 10 ml/kg of ORS for each additional diarrheal stool
 ½ Normal to Isotonic")
 Hypertonic Saline")



, CSW")



47 Hypotonic Saline (0.2% NaCl) ½ Normal to Isotonic Saline ( % NaCl) Hypertonic Saline (3% NaCl) Well NPO children with no medical problems. Mild illness not effecting water/electrolyte balance. Critically ill children Sepsis, pneumonia, dehydration Significant CNS injury ( ICP), CSW Hypervolemic states Congestive heart failure, liver failure, nephrotic syndrome Children who need to maintain higher effective serum osmolality Mild CNS injury, DKA, postoperative, gastroenteritis Severe, symptomatic, Hyponatremia 47



48
49 Bhutani VK, Johnson L, Sivieri EM. Predictive ability of a predischarge hour-specific serum bilirubin for subsequent significant hyperbilirubinemia in healthy term and nearterm newborns. Pediatrics.1999;103 (1):6 14 AAP Guidelines on Hyperbilirubinemia Fay, Schellhase, Suresh. Bilirubin Screening for Normal Newborns: A Critique of the Hour- Specific Bilirubin Nomogram.Pediatrics;2009;
50 The Johns Hopkins Hospital. The Harriet Lane Handbook. Elsevier/Mosby.2011.Print Long: Principles and Practices of Pediatric Infectious Disease Revised Reprint. Elsevier.2009.Print A special thanks to Dr. John Brandt, pediatric nephrologists, for contributing to the fluids lecture.
Principles of Infusion Therapy: Fluids
 Principles of Infusion Therapy: Fluids Christie Heinzman, MSN, APRN-CNP Acute Care Pediatric Nurse Practitioner Cincinnati Children s Hospital Medical Center May 22, 2018 Conflict of Interest Disclosure
Principles of Infusion Therapy: Fluids Christie Heinzman, MSN, APRN-CNP Acute Care Pediatric Nurse Practitioner Cincinnati Children s Hospital Medical Center May 22, 2018 Conflict of Interest Disclosure
Dr. Dafalla Ahmed Babiker Jazan University
 Dr. Dafalla Ahmed Babiker Jazan University objectives Overview Definition of dehydration Causes of dehydration Types of dehydration Diagnosis, signs and symptoms Management of dehydration Complications
Dr. Dafalla Ahmed Babiker Jazan University objectives Overview Definition of dehydration Causes of dehydration Types of dehydration Diagnosis, signs and symptoms Management of dehydration Complications
Fluid & Elyte Case Discussion. Hooman N IUMS 2013
 Fluid & Elyte Case Discussion Hooman N IUMS 2013 Objectives Know maintenance water and electrolyte requirements. Assess hydration status. Determine replacement fluids (oral and iv) Know how to approach
Fluid & Elyte Case Discussion Hooman N IUMS 2013 Objectives Know maintenance water and electrolyte requirements. Assess hydration status. Determine replacement fluids (oral and iv) Know how to approach
GUIDELINE FOR THE MANAGEMENT OF MENINGITIS. All children with suspected or confirmed meningitis
 GUIDELINE FOR THE MANAGEMENT OF MENINGITIS Reference: Mennigitis Version No: 1 Applicable to All children with suspected or confirmed meningitis Classification of document: Area for Circulation: Author:
GUIDELINE FOR THE MANAGEMENT OF MENINGITIS Reference: Mennigitis Version No: 1 Applicable to All children with suspected or confirmed meningitis Classification of document: Area for Circulation: Author:
Pediatric Dehydration and Oral Rehydration. May 16/17
 Pediatric Dehydration and Oral Rehydration May 16/17 Volume Depletion (hypovolemia): refers to any condition in which the effective circulating volume is reduced. It can be produced by salt and water loss
Pediatric Dehydration and Oral Rehydration May 16/17 Volume Depletion (hypovolemia): refers to any condition in which the effective circulating volume is reduced. It can be produced by salt and water loss
Safe and Healthy Beginnings. M. Jeffrey Maisels MD William Beaumont Hospital Royal Oak, MI
 Safe and Healthy Beginnings M. Jeffrey Maisels MD William Beaumont Hospital Royal Oak, MI jmaisels@beaumont.edu Risk Factors There are 2 kinds Those that increase the risk of subsequently developing a
Safe and Healthy Beginnings M. Jeffrey Maisels MD William Beaumont Hospital Royal Oak, MI jmaisels@beaumont.edu Risk Factors There are 2 kinds Those that increase the risk of subsequently developing a
Hypo/Hypernatremia. Stuart L. Goldstein MD. Director, Center for Acute Care Nephrology Cincinnati Children s Hospital
 Hypo/Hypernatremia Stuart L. Goldstein MD Director, Center for Acute Care Nephrology Cincinnati Children s Hospital Objectives Understand Fluid cellular shifts Understand maintenance fluid and calculations
Hypo/Hypernatremia Stuart L. Goldstein MD Director, Center for Acute Care Nephrology Cincinnati Children s Hospital Objectives Understand Fluid cellular shifts Understand maintenance fluid and calculations
Fundamentals of Pharmacology for Veterinary Technicians Chapter 19
 Figure 19-1 Figure 19-2A Figure 19-2B Figure 19-3 Figure 19-4A1 Figure 19-4A2 Figure 19-4B Figure 19-4C Figure 19-4D Figure 19-5 Figure 19-6A Figure 19-6B A Figure 19-7A B Figure 19-7B C Figure 19-7C D
Figure 19-1 Figure 19-2A Figure 19-2B Figure 19-3 Figure 19-4A1 Figure 19-4A2 Figure 19-4B Figure 19-4C Figure 19-4D Figure 19-5 Figure 19-6A Figure 19-6B A Figure 19-7A B Figure 19-7B C Figure 19-7C D
Crash Cart therapy for Severe Jaundice. Dr Sandeep Kadam Neonatologist Pune
 Crash Cart therapy for Severe Jaundice Dr Sandeep Kadam Neonatologist Pune Objectives Assessment & stabilization Role of Investigations Management principles Steps for a crash-cart approach Assess Risk
Crash Cart therapy for Severe Jaundice Dr Sandeep Kadam Neonatologist Pune Objectives Assessment & stabilization Role of Investigations Management principles Steps for a crash-cart approach Assess Risk
Basic Fluid and Electrolytes
 Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
11/8/12. KERNICTERUS: The reason we have to care about bilirubin. MANAGING JAUNDICE IN THE BREASTFEEDING INFANT AKA: Lack of Breastfeeding Jaundice
 MANAGING JAUNDICE IN THE BREASTFEEDING INFANT AKA: Lack of Breastfeeding Jaundice November 16, 2012 Orange County Lawrence M. Gartner, M.D. University of Chicago and Valley Center, California KERNICTERUS:
MANAGING JAUNDICE IN THE BREASTFEEDING INFANT AKA: Lack of Breastfeeding Jaundice November 16, 2012 Orange County Lawrence M. Gartner, M.D. University of Chicago and Valley Center, California KERNICTERUS:
Paediatric Directorate
 Paediatric Directorate Dehydration Guidelines Primary cause of dehydration diarrhoea +/- vomiting. Approximately 10%Children < 5yrs present with gastroenteritis each year Diagnosis History - sudden change
Paediatric Directorate Dehydration Guidelines Primary cause of dehydration diarrhoea +/- vomiting. Approximately 10%Children < 5yrs present with gastroenteritis each year Diagnosis History - sudden change
Fever in the Newborn Period
 Fever in the Newborn Period 1. Definitions 1 2. Overview 1 3. History and Physical Examination 2 4. Fever in Infants Less than 3 Months Old 2 a. Table 1: Rochester criteria for low risk infants 3 5. Fever
Fever in the Newborn Period 1. Definitions 1 2. Overview 1 3. History and Physical Examination 2 4. Fever in Infants Less than 3 Months Old 2 a. Table 1: Rochester criteria for low risk infants 3 5. Fever
PAEDIATRIC FLUIDS RCH DEHYDRATION
 PAEDIATRIC FLUIDS RCH DEHYDRATION AIMS Understand normal fluids electrolyte requirements/ maintenance Understand how to assess DEHYDRATION in children Understand the difference between DEHYDRATION and
PAEDIATRIC FLUIDS RCH DEHYDRATION AIMS Understand normal fluids electrolyte requirements/ maintenance Understand how to assess DEHYDRATION in children Understand the difference between DEHYDRATION and
Chapter 4 Fluid Management
 Chapter 4 Fluid Management First Nations and Inuit Health Branch (FNIHB) Pediatric Clinical Practice Guidelines for Nurses in Primary Care. The content of this chapter has been reviewed October 2009. Table
Chapter 4 Fluid Management First Nations and Inuit Health Branch (FNIHB) Pediatric Clinical Practice Guidelines for Nurses in Primary Care. The content of this chapter has been reviewed October 2009. Table
Emergency Neurological Life Support Meningitis and Encephalitis
 Emergency Neurological Life Support Meningitis and Encephalitis Version: 2.0 Last Updated: 19-Mar-2016 Checklist & Communication Meningitis and Encephalitis Table of Contents Emergency Neurological Life
Emergency Neurological Life Support Meningitis and Encephalitis Version: 2.0 Last Updated: 19-Mar-2016 Checklist & Communication Meningitis and Encephalitis Table of Contents Emergency Neurological Life
Disorders of water and sodium homeostasis. Prof A. Pomeranz 2017
 Disorders of water and sodium homeostasis Prof A. Pomeranz 2017 Pediatric (Nephrology) Tool Box Disorders of water and sodium homeostasis Pediatric Nephrology Tool Box Hyponatremiaand and Hypernatremia
Disorders of water and sodium homeostasis Prof A. Pomeranz 2017 Pediatric (Nephrology) Tool Box Disorders of water and sodium homeostasis Pediatric Nephrology Tool Box Hyponatremiaand and Hypernatremia
Clinical evaluation Jaundice skin and mucous membranes
 JAUNDICE Framework The definition of Neonatal Jaundice Billirubin Metabolism Special characteristic in neonates Dangerous of the Hyperbillirubinemia The diseases in relation with Neonatal Jaundice Objectives:
JAUNDICE Framework The definition of Neonatal Jaundice Billirubin Metabolism Special characteristic in neonates Dangerous of the Hyperbillirubinemia The diseases in relation with Neonatal Jaundice Objectives:
Severe neonatal hyperbilirubinemia leading to exchange transfusion
 Original Article Medical Journal of the Islamic Republic of Iran (MJIRI) Iran University of Medical Sciences Severe neonatal hyperbilirubinemia leading to exchange transfusion Downloaded from mjiri.iums.ac.ir
Original Article Medical Journal of the Islamic Republic of Iran (MJIRI) Iran University of Medical Sciences Severe neonatal hyperbilirubinemia leading to exchange transfusion Downloaded from mjiri.iums.ac.ir
Acute Bilirubin Encephalopathy in Healthy Term Neonates Requiring Exchange Transfusion
 Iranian Journal of Neonatology 8 Acute Bilirubin Encephalopathy in Healthy Term Neonates Requiring Exchange Transfusion Seyedeh Fatemeh Khatami* 1, Pouya Parvaresh 2 *1-Department of Pediatrics, Division
Iranian Journal of Neonatology 8 Acute Bilirubin Encephalopathy in Healthy Term Neonates Requiring Exchange Transfusion Seyedeh Fatemeh Khatami* 1, Pouya Parvaresh 2 *1-Department of Pediatrics, Division
Aurora Health Care South Region EMS st Quarter CE Packet
 Name: Dept: Date: Aurora Health Care South Region EMS 2010 1 st Quarter CE Packet Meningitis Meningitis is an inflammatory disease of the leptomeninges. Leptomeninges refer to the pia matter and the arachnoid
Name: Dept: Date: Aurora Health Care South Region EMS 2010 1 st Quarter CE Packet Meningitis Meningitis is an inflammatory disease of the leptomeninges. Leptomeninges refer to the pia matter and the arachnoid
Approach to the management of Hyperbilirubinemia in Term Newborn Infant
 Approach to the management of Hyperbilirubinemia in Term Newborn Infant Mohammad Bagher Hosseini MD Neonatologist Assosiated professor of Tabriz University of Medical science May 2011 Case1 You are called
Approach to the management of Hyperbilirubinemia in Term Newborn Infant Mohammad Bagher Hosseini MD Neonatologist Assosiated professor of Tabriz University of Medical science May 2011 Case1 You are called
Fluid supplementation in term neonates with severe hyperbilirubinemia: a randomized controlled trial study
 International Journal of Contemporary Pediatrics Bandyopadhyay A et al. Int J Contemp Pediatr. 2017 May;4(3):853-857 http://www.ijpediatrics.com pissn 2349-3283 eissn 2349-3291 Original Research Article
International Journal of Contemporary Pediatrics Bandyopadhyay A et al. Int J Contemp Pediatr. 2017 May;4(3):853-857 http://www.ijpediatrics.com pissn 2349-3283 eissn 2349-3291 Original Research Article
Fluid and Electrolytes: Parenteral
 Article fluid & electrolytes Fluid and Electrolytes: Parenteral Fluid Therapy Kenneth B. Roberts, MD* Objectives After completing this article, readers should be able to: 1. Relate maintenance fluid and
Article fluid & electrolytes Fluid and Electrolytes: Parenteral Fluid Therapy Kenneth B. Roberts, MD* Objectives After completing this article, readers should be able to: 1. Relate maintenance fluid and
CNS Infections. Philip Gothard Consultant in Infectious Diseases Hospital for Tropical Diseases, London. Hammersmith Acute Medicine 2011
 CNS Infections Philip Gothard Consultant in Infectious Diseases Hospital for Tropical Diseases, London Hammersmith Acute Medicine 2011 Case 1 HISTORY 27y man Unwell 3 days Fever Headache Photophobia Previously
CNS Infections Philip Gothard Consultant in Infectious Diseases Hospital for Tropical Diseases, London Hammersmith Acute Medicine 2011 Case 1 HISTORY 27y man Unwell 3 days Fever Headache Photophobia Previously
IDPH ESF-8 Plan: Pediatric and Neonatal Surge Annex Sample Pediatric Admission Orders 2015
 Purpose: To provide guidance to practitioners caring for pediatric patients who need inpatient hospital care during a disaster. Disclaimer: This guideline is not meant to be all inclusive, replace an existing
Purpose: To provide guidance to practitioners caring for pediatric patients who need inpatient hospital care during a disaster. Disclaimer: This guideline is not meant to be all inclusive, replace an existing
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on the Approach to Pediatric Anemia and Pallor. These podcasts are designed to give medical students an overview of key
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on the Approach to Pediatric Anemia and Pallor. These podcasts are designed to give medical students an overview of key
Background OVER 30 ISSUES IDENTIFIED! Key opportunities. What we ve done. October 31, 2012
 Background Hyperbilirubinemia: Developed by CMNRP s Jaundice Working Group Strategic planning meeting of CMNRP and its committees Multiple tables identified jaundice as a problem/priority Opportunity to
Background Hyperbilirubinemia: Developed by CMNRP s Jaundice Working Group Strategic planning meeting of CMNRP and its committees Multiple tables identified jaundice as a problem/priority Opportunity to
Bacterial meningitis
 Bacterial meningitis Is an acute purulent infection in the subarachnoid space that is associated with inflammation reaction in the brain and cerebral blood vessels that causes decreased conciuosness, seizure,
Bacterial meningitis Is an acute purulent infection in the subarachnoid space that is associated with inflammation reaction in the brain and cerebral blood vessels that causes decreased conciuosness, seizure,
Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014
 Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014 Prep Question You are camping with a group of boys at a rural campground in the southeastern Unites States when one of the campers is bitten
Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014 Prep Question You are camping with a group of boys at a rural campground in the southeastern Unites States when one of the campers is bitten
Antibiotic Resistance Pattern of Blood and CSF Culture Isolates At NHLS Academic Laboratories (2005)
") Antibiotic Resistance Pattern of Blood and CSF Culture Isolates At NHLS Academic Laboratories (2005) Streptococcus pneumoniae (SP) Blood Culture Isolates Penicillin intermediate Penicillin Cefotaxime 336
Antibiotic Resistance Pattern of Blood and CSF Culture Isolates At NHLS Academic Laboratories (2005) Streptococcus pneumoniae (SP) Blood Culture Isolates Penicillin intermediate Penicillin Cefotaxime 336
Blue Babies, Twitchy Toddlers, and Kool Kids. By Beth Paton, MSN, RN, PNP, CEN, CPEN, FAEN
 Blue Babies, Twitchy Toddlers, and Kool Kids By Beth Paton, MSN, RN, PNP, CEN, CPEN, FAEN I have no disclosures OBJECTIVES By the end of this presentation, the learner will Discuss etiologies of cyanosis
Blue Babies, Twitchy Toddlers, and Kool Kids By Beth Paton, MSN, RN, PNP, CEN, CPEN, FAEN I have no disclosures OBJECTIVES By the end of this presentation, the learner will Discuss etiologies of cyanosis
ADVOCATE CHRIST MEDICAL CENTER DKA (DIABETIC KETOACIDOSIS) TREATMENT GUIDELINES
 TREATMENT GUIDELINES") ADVOCATE CHRIST MEDICAL CENTER DKA (DIABETIC KETOACIDOSIS) TREATMENT GUIDELINES DEFINITION -Glucose >250 mg/dl*, anion gap > 16, + ketones * Glucose < 250 does not exclude DKA especially if anion gap >
ADVOCATE CHRIST MEDICAL CENTER DKA (DIABETIC KETOACIDOSIS) TREATMENT GUIDELINES DEFINITION -Glucose >250 mg/dl*, anion gap > 16, + ketones * Glucose < 250 does not exclude DKA especially if anion gap >
MODULE VI. Diarrhea and Dehydration
 MODULE VI Diarrhea and Dehydration ACUTE DIARRHEA Increased number of bowel movements! Loose and watery stools Fluid and electrolyte loss ACUTE DIARRHEA TYPES Watery Bloody diarrhea (dysentery) DIARRHEA
MODULE VI Diarrhea and Dehydration ACUTE DIARRHEA Increased number of bowel movements! Loose and watery stools Fluid and electrolyte loss ACUTE DIARRHEA TYPES Watery Bloody diarrhea (dysentery) DIARRHEA
Fever Without a Source Age: 0-28 Day Pathway - Emergency Department Evidence Based Outcome Center
 Age: 0-28 Day Pathway - Emergency Department EXCLUSION CRITERIA Toxic appearing No fever Born < 37 weeks gestational age INCLUSION CRITERIA Non-toxic with temperature > 38 C (100.4 F) < 36 C (96.5 F) measured
Age: 0-28 Day Pathway - Emergency Department EXCLUSION CRITERIA Toxic appearing No fever Born < 37 weeks gestational age INCLUSION CRITERIA Non-toxic with temperature > 38 C (100.4 F) < 36 C (96.5 F) measured
PAEDIATRIC ACUTE CARE GUIDELINE. Jaundice Neonatal
 Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Jaundice Neonatal Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should be read
Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Jaundice Neonatal Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should be read
KENT STATE UNIVERSITY HEALTH CARE OF CHILDREN Nursing Pediatrics Case Studies: Child Dehydration
 Courtney Wiener 9/9/10 KENT STATE UNIVERSITY HEALTH CARE OF CHILDREN Nursing 30020 - Pediatrics Case Studies: Child Dehydration Introduction: Dehydration can be life threatening to a child since a majority
Courtney Wiener 9/9/10 KENT STATE UNIVERSITY HEALTH CARE OF CHILDREN Nursing 30020 - Pediatrics Case Studies: Child Dehydration Introduction: Dehydration can be life threatening to a child since a majority
IV Fluids. I.V. Fluid Osmolarity Composition 0.9% NaCL (Normal Saline Solution, NSS) Uses/Clinical Considerations
 Uses/Clinical Considerations") IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
Central Nervous System Infection
 Central Nervous System Infection Lingyun Shao Department of Infectious Diseases Huashan Hospital, Fudan University Definition Meningitis: an inflammation of the arachnoid membrane, the pia mater, and the
Central Nervous System Infection Lingyun Shao Department of Infectious Diseases Huashan Hospital, Fudan University Definition Meningitis: an inflammation of the arachnoid membrane, the pia mater, and the
What to Do when the Lights Don t Work- Neonatal Hyperbilirubinemia
 What to Do when the Lights Don t Work- Neonatal Hyperbilirubinemia Dr G Elske Hildes-Ripstein Dept of Child Health and Pediatrics University of Manitoba, College of Medicine Annual Scientific Assembly;
What to Do when the Lights Don t Work- Neonatal Hyperbilirubinemia Dr G Elske Hildes-Ripstein Dept of Child Health and Pediatrics University of Manitoba, College of Medicine Annual Scientific Assembly;
CNS INFECTIONS 1 Acute meningitis
 Definition CNS INFECTIONS 1 Acute meningitis DR. BADRI PAUDEL Bacterial meningitis is a medical emergency. Meningitis is an acute infection within the subarachnoid space. usually secondary bacteremia or
Definition CNS INFECTIONS 1 Acute meningitis DR. BADRI PAUDEL Bacterial meningitis is a medical emergency. Meningitis is an acute infection within the subarachnoid space. usually secondary bacteremia or
Supplemental Information
 FROM THE AMERICAN ACADEMY OF PEDIATRICS Supplemental Information SUPPLEMENTAL FIGURE 2 Forest plot of all included RCTs using a random-effects model and M-H statistics with the outcome of hyponatremia
FROM THE AMERICAN ACADEMY OF PEDIATRICS Supplemental Information SUPPLEMENTAL FIGURE 2 Forest plot of all included RCTs using a random-effects model and M-H statistics with the outcome of hyponatremia
Brain abscess rupturing into the lateral ventricle causing meningitis: a case report
 Brain abscess rupturing into the lateral ventricle causing meningitis: a case report Endry Martinez, and Judith Berger SBH Health System, 4422 Third Ave, Bronx, NY 10457 Key words: brain abscess, rupture
Brain abscess rupturing into the lateral ventricle causing meningitis: a case report Endry Martinez, and Judith Berger SBH Health System, 4422 Third Ave, Bronx, NY 10457 Key words: brain abscess, rupture
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
ANTIBIOTIC GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED MENINGITIS AND ENCEPHALITIS IN ADULTS
 ANTIBIOTIC GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED MENINGITIS AND ENCEPHALITIS IN ADULTS Version 4.0 Date ratified February 2009 Review date February 2011 Ratified by Authors Consultation Evidence
ANTIBIOTIC GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED MENINGITIS AND ENCEPHALITIS IN ADULTS Version 4.0 Date ratified February 2009 Review date February 2011 Ratified by Authors Consultation Evidence
Practice Guidelines for the Management of Bacterial Meningitis
 IDSA GUIDELINES Practice Guidelines for the Management of Bacterial Meningitis Allan R. Tunkel, 1 Barry J. Hartman, 2 Sheldon L. Kaplan, 3 Bruce A. Kaufman, 4 Karen L. Roos, 5 W. Michael Scheld, 6 and
IDSA GUIDELINES Practice Guidelines for the Management of Bacterial Meningitis Allan R. Tunkel, 1 Barry J. Hartman, 2 Sheldon L. Kaplan, 3 Bruce A. Kaufman, 4 Karen L. Roos, 5 W. Michael Scheld, 6 and
Original Article Effect of Intravenous Fluid Supplementation on Serum Bilirubin Level in Jaundiced Healthy Neonates during Conventional Phototherapy
 Original Article Effect of Intravenous Fluid Supplementation on Serum Bilirubin Level in Jaundiced Healthy Neonates during Conventional Phototherapy Abstract R. Iranpour MD*, R. Nohekhan MD**, I. Haghshenas
Original Article Effect of Intravenous Fluid Supplementation on Serum Bilirubin Level in Jaundiced Healthy Neonates during Conventional Phototherapy Abstract R. Iranpour MD*, R. Nohekhan MD**, I. Haghshenas
With Dr. Sarah Reid and Dr. Sarah Curtis
 5. Headaches 6. Known diabetes 7. Specific high risk groups (ie. Teenagers, children on insulin pumps and those from lower socio-economic status). Episode 63 Pediatric Diabetic Ketoacidosis With Dr. Sarah
5. Headaches 6. Known diabetes 7. Specific high risk groups (ie. Teenagers, children on insulin pumps and those from lower socio-economic status). Episode 63 Pediatric Diabetic Ketoacidosis With Dr. Sarah
EVALUATION OF A SICK CHILD WITH FEVER
 EVALUATION OF A SICK CHILD WITH FEVER Learning objectives At the conclusion of this learning activity, participants should be able to; Discuss the different etiologies of acute illness in a child Identify
EVALUATION OF A SICK CHILD WITH FEVER Learning objectives At the conclusion of this learning activity, participants should be able to; Discuss the different etiologies of acute illness in a child Identify
An Intriguing Case of Meningitis. Tiffany Mylius MLS (ASCP)
") An Intriguing Case of Meningitis { Tiffany Mylius MLS (ASCP) A 4yo male presents with 2wk history of URI symptoms. On the day of admission, the patient woke up with a HA in the morning, took a nap later
An Intriguing Case of Meningitis { Tiffany Mylius MLS (ASCP) A 4yo male presents with 2wk history of URI symptoms. On the day of admission, the patient woke up with a HA in the morning, took a nap later
OB Well Baby Nursery Admission (Term) [ ] For specialty focused order sets for your patient, refer to: General
![OB Well Baby Nursery Admission (Term) [ ] For specialty focused order sets for your patient, refer to: General](/thumbs/85/91909911.jpg "OB Well Baby Nursery Admission (Term) [ ] For specialty focused order sets for your patient, refer to: General") OB Well Baby Nursery Admission (Term) [3040000234] For specialty focused order sets for your patient, refer to: 3040000424 Neonatal Circumcision Order Set 3040000522 Neonatal Herpes Viral Order Set 3040000524
OB Well Baby Nursery Admission (Term) [3040000234] For specialty focused order sets for your patient, refer to: 3040000424 Neonatal Circumcision Order Set 3040000522 Neonatal Herpes Viral Order Set 3040000524
Intravenous Fluids: In the ER and on the floor. MEValletta,, MD August 4, 2005 Resident Core Conference Lecture Series
 Intravenous Fluids: In the ER and on the floor MEValletta,, MD August 4, 2005 Resident Core Conference Lecture Series Objectives Understand appropriate fluid resuscitation Understand appropriate fluid
Intravenous Fluids: In the ER and on the floor MEValletta,, MD August 4, 2005 Resident Core Conference Lecture Series Objectives Understand appropriate fluid resuscitation Understand appropriate fluid
FLUID THERAPY: IT S MORE THAN JUST LACTATED RINGERS
 FLUID THERAPY: IT S MORE THAN JUST LACTATED RINGERS Elisa M. Mazzaferro, MS, DVM, PhD, DACVECC Cornell University Veterinary Specialists, Stamford, CT, USA Total body water constitutes approximately 60%
FLUID THERAPY: IT S MORE THAN JUST LACTATED RINGERS Elisa M. Mazzaferro, MS, DVM, PhD, DACVECC Cornell University Veterinary Specialists, Stamford, CT, USA Total body water constitutes approximately 60%
Breastfeeding, Jaundice and Hyperbilirubinemia in the Newborn. Jeremy Jones, DO Oklahoma State University Center for Health Sciences
 Breastfeeding, Jaundice and Hyperbilirubinemia in the Newborn Jeremy Jones, DO Oklahoma State University Center for Health Sciences Table of Contents Learning Objectives Practice Gap The Newborn Baby and
Breastfeeding, Jaundice and Hyperbilirubinemia in the Newborn Jeremy Jones, DO Oklahoma State University Center for Health Sciences Table of Contents Learning Objectives Practice Gap The Newborn Baby and
4/11/2017 COMMUNITY ACQUIRED PNEUMONIA. Disclaimer. A Review of How to Treat Common Infections in a Pediatric Patient. Objectives for Technicians
 Disclaimer A Review of How to Treat Common Infections in a Pediatric Patient Tara Bergland reports that she has no actual or potential conflict of interest in relation to this presentation. Off label use
Disclaimer A Review of How to Treat Common Infections in a Pediatric Patient Tara Bergland reports that she has no actual or potential conflict of interest in relation to this presentation. Off label use
FEVER. What is fever?
 FEVER What is fever? Fever is defined as a rectal temperature 38 C (100.4 F), and a value >40 C (104 F) is called hyperpyrexia. Body temperature fluctuates in a defined normal range (36.6-37.9 C [97.9-100.2
FEVER What is fever? Fever is defined as a rectal temperature 38 C (100.4 F), and a value >40 C (104 F) is called hyperpyrexia. Body temperature fluctuates in a defined normal range (36.6-37.9 C [97.9-100.2
Neonatal Jaundice Hyperbilirubinemia
 Neonatal Jaundice Hyperbilirubinemia Dr. Abdulrahman Al Nemri, MD Chairman Pediatric Department Associate Professor of Pediatric Consultant Neonatologist 100 $ questions on Neonatal Jaundice (NJ) 1. What
Neonatal Jaundice Hyperbilirubinemia Dr. Abdulrahman Al Nemri, MD Chairman Pediatric Department Associate Professor of Pediatric Consultant Neonatologist 100 $ questions on Neonatal Jaundice (NJ) 1. What
Fluid therapy in children
 Fluid therapy in children TJ Neuhaus and G Reusz Lucerne and Budapest ESPN 2012 Kraków Parenteral maintenance in children Daily requirements - Holliday and Segar, 1957 Fluid Patient weight: 25 kg 1-10
Fluid therapy in children TJ Neuhaus and G Reusz Lucerne and Budapest ESPN 2012 Kraków Parenteral maintenance in children Daily requirements - Holliday and Segar, 1957 Fluid Patient weight: 25 kg 1-10
Pneumococcal Meningitis Meningitis is an inflammation of the lining around the brain and spinal cord. Most severe cases
 Pneumococcal Meningitis Meningitis is an inflammation of the lining around the brain and spinal cord. Most severe cases are caused by bacteria. Pneumococcal bacteria (Streptococcus pneumoniae) are the
Pneumococcal Meningitis Meningitis is an inflammation of the lining around the brain and spinal cord. Most severe cases are caused by bacteria. Pneumococcal bacteria (Streptococcus pneumoniae) are the
CASE-BASED SMALL GROUP DISCUSSION MHD II
 MHD II, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II Session 11 April 11, 2016 STUDENT COPY MHD II, Session 11, Student Copy Page 2 CASE HISTORY 1 Chief complaint: Our baby
MHD II, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II Session 11 April 11, 2016 STUDENT COPY MHD II, Session 11, Student Copy Page 2 CASE HISTORY 1 Chief complaint: Our baby
Outcome of Neonatal Hyperbilirubinemia in a Tertiary Care Hospital in Bangladesh
 Brief Communication Outcome of Neonatal Hyperbilirubinemia in a Tertiary Care Hospital in Bangladesh Choudhury Habibur Rasul, Md Abul Hasan, Farhana Yasmin Submitted: 29 Jun 2009 Accepted: 25 Dec 2009
Brief Communication Outcome of Neonatal Hyperbilirubinemia in a Tertiary Care Hospital in Bangladesh Choudhury Habibur Rasul, Md Abul Hasan, Farhana Yasmin Submitted: 29 Jun 2009 Accepted: 25 Dec 2009
Revised Authors: Malathi Balasundaram MD, Vinod K. Bhutani, MD, FAAP
 Severe Hyperbilirubinemia Prevention (SHP Toolkit) Revised Authors: Malathi Balasundaram MD, Vinod K. Bhutani, MD, FAAP Original Authors: Richard Bell, MD, Lisa Bollman, RN, CPHQ, Courtney Nisbet, RN,
Severe Hyperbilirubinemia Prevention (SHP Toolkit) Revised Authors: Malathi Balasundaram MD, Vinod K. Bhutani, MD, FAAP Original Authors: Richard Bell, MD, Lisa Bollman, RN, CPHQ, Courtney Nisbet, RN,
Pare. Blalock. Shires. shock caused by circulating toxins treatment with phlebotomy. shock caused by hypovolemia treatment with plasma replacement
 Pare shock caused by circulating toxins treatment with phlebotomy Blalock shock caused by hypovolemia treatment with plasma replacement Shires deficit in functional extracellular volume treatment with
Pare shock caused by circulating toxins treatment with phlebotomy Blalock shock caused by hypovolemia treatment with plasma replacement Shires deficit in functional extracellular volume treatment with
BACTERIAL MENINGITIS: A FIVE YEAR ( ) RETROSPECTIVE STUDY AT UNIVERSITY MALAYA MEDICAL CENTer (UMMC), KUALA LUMPUR, MALAYSIA
 RETROSPECTIVE STUDY AT UNIVERSITY MALAYA MEDICAL CENTer (UMMC), KUALA LUMPUR, MALAYSIA") BACTERIAL MENINGITIS: A FIVE YEAR (2001-2005) RETROSPECTIVE STUDY AT UNIVERSITY MALAYA MEDICAL CENTer (UMMC), KUALA LUMPUR, MALAYSIA H Erleena Nur, I Jamaiah, M Rohela and V Nissapatorn Department of Parasitology,
BACTERIAL MENINGITIS: A FIVE YEAR (2001-2005) RETROSPECTIVE STUDY AT UNIVERSITY MALAYA MEDICAL CENTer (UMMC), KUALA LUMPUR, MALAYSIA H Erleena Nur, I Jamaiah, M Rohela and V Nissapatorn Department of Parasitology,
4/11/2017. A Review of How to Treat Common Infections in a Pediatric Patient. Disclaimer. Objectives for Pharmacists
 A Review of How to Treat Common Infections in a Pediatric Patient Tara Bergland, Pharm D. PGY2 Pediatric Pharmacy Resident Tara-bergland@uiowa.edu Disclaimer Tara Bergland reports that she has no actual
A Review of How to Treat Common Infections in a Pediatric Patient Tara Bergland, Pharm D. PGY2 Pediatric Pharmacy Resident Tara-bergland@uiowa.edu Disclaimer Tara Bergland reports that she has no actual
Summary. Meningitis. Meningitis. Conflicts of interests. Meningitis what s new?
 Conflicts of interests what s new? CB has been an investigator on investigator-initiated pneumonia research projects funded by Pfizer CB is co-chair of the Australian Technical Advisory Group of Immunisation,
Conflicts of interests what s new? CB has been an investigator on investigator-initiated pneumonia research projects funded by Pfizer CB is co-chair of the Australian Technical Advisory Group of Immunisation,
Abnormalities in serum sodium. David Metz Paediatric Nephrology
 Abnormalities in serum sodium David Metz Paediatric Nephrology Basics Total body sodium regulated by aldosterone and ANP Mediated by intravascular volume (not sodium) RAAS and intrarenal determines Na
Abnormalities in serum sodium David Metz Paediatric Nephrology Basics Total body sodium regulated by aldosterone and ANP Mediated by intravascular volume (not sodium) RAAS and intrarenal determines Na
Neonatal Jaundice for Infants 35 Weeks Gestational Age v.3
 Neonatal Jaundice for Infants 35 Weeks Gestational Age v.3 Approval & Citation Explanation of Evidence Ratings Summary of Version Changes Inclusion Criteria Previously healthy Age 14 days Born at 35 wks
Neonatal Jaundice for Infants 35 Weeks Gestational Age v.3 Approval & Citation Explanation of Evidence Ratings Summary of Version Changes Inclusion Criteria Previously healthy Age 14 days Born at 35 wks
Febrile Seizures. Preface. Definition, Evaluation, Assessment, and Prognosis. Definition
 Febrile Seizures Guideline significantly revised by Rebecca Latch, MD, in collaboration with the ANGELS team. Last reviewed by Rebecca Latch, MD, July 22, 2016. Guideline replaced Evaluation and Treatment
Febrile Seizures Guideline significantly revised by Rebecca Latch, MD, in collaboration with the ANGELS team. Last reviewed by Rebecca Latch, MD, July 22, 2016. Guideline replaced Evaluation and Treatment
Water (Dysnatremia) & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua
 & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua") Water (Dysnatremia) & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua Assistant Professor Nephrology Unit, Department of Medicine College of Medicine,
Water (Dysnatremia) & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua Assistant Professor Nephrology Unit, Department of Medicine College of Medicine,
1. Introduction Algorithm: Infant with Fever 0-28 Days Algorithm: Infant with Fever Days...3
 These guidelines are designed to assist clinicians and are not intended to supplant good clinical judgement or to establish a protocol for all patients with this condition. MANAGEMENT OF FEVER 38 C (100.4F)
These guidelines are designed to assist clinicians and are not intended to supplant good clinical judgement or to establish a protocol for all patients with this condition. MANAGEMENT OF FEVER 38 C (100.4F)
Evidence- Based Medicine Fluid Therapy
 Evidence- Based Medicine Fluid Therapy Ndidi Musa M.D. Assosciate Professor of Pediatrics Medical College of Wisconsin/ Children s Hospital of Wisconsin Disclosures A. I have no relevant financial relationships
Evidence- Based Medicine Fluid Therapy Ndidi Musa M.D. Assosciate Professor of Pediatrics Medical College of Wisconsin/ Children s Hospital of Wisconsin Disclosures A. I have no relevant financial relationships
Rebecca T Slagle, MN, APRN, NNP-BC. Speak up!!
 Rebecca T Slagle, MN, APRN, NNP-BC Speak up!! Objectives: Understand the incidence and prevalence of sepsis in the newborn period Identify the risk factors for neonatal sepsis List the most frequent causative
Rebecca T Slagle, MN, APRN, NNP-BC Speak up!! Objectives: Understand the incidence and prevalence of sepsis in the newborn period Identify the risk factors for neonatal sepsis List the most frequent causative
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES
 Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Septic Shock. Kathryn Sims, PGY I
 Septic Shock Kathryn Sims, PGY I A 6 y.o. previously healthy boy presents to the ED with 7 days of fever accompanied by chills. Further history reveals the patient has also been experiencing dysuria for
Septic Shock Kathryn Sims, PGY I A 6 y.o. previously healthy boy presents to the ED with 7 days of fever accompanied by chills. Further history reveals the patient has also been experiencing dysuria for
Pediatric Sodium Disorders
 Pediatric Sodium Disorders Guideline developed by Ron Sanders, Jr., MD, MS, in collaboration with the ANGELS team. Last reviewed by Ron Sanders, Jr., MD, MS on May 20, 2016. Definitions, Physiology, Assessment,
Pediatric Sodium Disorders Guideline developed by Ron Sanders, Jr., MD, MS, in collaboration with the ANGELS team. Last reviewed by Ron Sanders, Jr., MD, MS on May 20, 2016. Definitions, Physiology, Assessment,
CNS Infections. GBS Streptococcus agalactiae. Meningitis - Neonate
 CNS Infections GBS Streptococcus agalactiae Bacterial meningitis - Pathophysiology - general Specific organisms - Age Hosts Treatment/Prevention Distinguish from viral disease Common commensal flora childbearing
CNS Infections GBS Streptococcus agalactiae Bacterial meningitis - Pathophysiology - general Specific organisms - Age Hosts Treatment/Prevention Distinguish from viral disease Common commensal flora childbearing
11/9/2012. Group B Streptococcal Infections: Consensus and Controversies. Prevention of Early-Onset GBS Disease in the USA.
 Group B Streptococcal Infections: Consensus and Controversies Carol J. Baker, M.D. Professor of Pediatrics, Molecular Virology and Microbiology Executive Director, Center for Vaccine Awareness and Research
Group B Streptococcal Infections: Consensus and Controversies Carol J. Baker, M.D. Professor of Pediatrics, Molecular Virology and Microbiology Executive Director, Center for Vaccine Awareness and Research
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University
 Dr Mubarak Abdelrahman Assistant Professor Jazan University") Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
I have no financial disclosures
 Athina Sikavitsas DO Children's Emergency Services University of Michigan Discuss DKA Presentation Assessment Treatment I have no financial disclosures 1 6 Y/O male presents with vomiting and abdominal
Athina Sikavitsas DO Children's Emergency Services University of Michigan Discuss DKA Presentation Assessment Treatment I have no financial disclosures 1 6 Y/O male presents with vomiting and abdominal
3 HYDROXY 3 METHYLGLUTARYL CoA (3 HMG CoA) LYASE DEFICIENCY RECOMMENDATIONS ON EMERGENCY MANAGEMENT OF METABOLIC DISEASES
 LYASE DEFICIENCY RECOMMENDATIONS ON EMERGENCY MANAGEMENT OF METABOLIC DISEASES") 3 HYDROXY 3 METHYLGLUTARYL CoA (3 HMG CoA) LYASE DEFICIENCY RECOMMENDATIONS ON EMERGENCY MANAGEMENT OF METABOLIC DISEASES Patient s name: Date of birth: Please read carefully. Meticulous and prompt treatment
3 HYDROXY 3 METHYLGLUTARYL CoA (3 HMG CoA) LYASE DEFICIENCY RECOMMENDATIONS ON EMERGENCY MANAGEMENT OF METABOLIC DISEASES Patient s name: Date of birth: Please read carefully. Meticulous and prompt treatment
KASHVET VETERINARIAN RESOURCES FLUID THERAPY AND SELECTION OF FLUIDS
 KASHVET VETERINARIAN RESOURCES FLUID THERAPY AND SELECTION OF FLUIDS INTRODUCTION Formulating a fluid therapy plan for the critical small animal patient requires careful determination of the current volume
KASHVET VETERINARIAN RESOURCES FLUID THERAPY AND SELECTION OF FLUIDS INTRODUCTION Formulating a fluid therapy plan for the critical small animal patient requires careful determination of the current volume
+ Objectives. n Define who is at risk for SBI. n Clarify risk stratification. n Provide treatment guidelines. n Bust some myths
 Objectives n Define wo is at risk for SBI n Clarify risk stratification n Provide treatment guidelines Neonatal Fever Benjamin B. Constance, MD, FAWM n Bust some myts Based on Case wat do you want to know?
Objectives n Define wo is at risk for SBI n Clarify risk stratification n Provide treatment guidelines Neonatal Fever Benjamin B. Constance, MD, FAWM n Bust some myts Based on Case wat do you want to know?
Clinical Assessment Tool
 Clinical Assessment Tool Child with Suspected Gastroenteritis 0-5 Years Diarrhoea is defined as the passage of three or more loose/watery stools per day, the most common cause of diarrhoea in children
Clinical Assessment Tool Child with Suspected Gastroenteritis 0-5 Years Diarrhoea is defined as the passage of three or more loose/watery stools per day, the most common cause of diarrhoea in children
5/1/2015 SEPSIS SURVIVING SEPSIS CAMPAIGN HOW TO APPROACH THE POSSIBLE SEPTIC CHILD 2015 INFECTION CAN BE CONFIRMED BY:
 SURVIVING SEPSIS CAMPAIGN HOW TO APPROACH THE POSSIBLE SEPTIC CHILD 2015 Omer Nasiroglu MD Baptist Children s Hospital Pediatric Emergency Department SEPSIS IS A SYSTEMIC INFLAMMATORY RESPONSE SYNDROME
SURVIVING SEPSIS CAMPAIGN HOW TO APPROACH THE POSSIBLE SEPTIC CHILD 2015 Omer Nasiroglu MD Baptist Children s Hospital Pediatric Emergency Department SEPSIS IS A SYSTEMIC INFLAMMATORY RESPONSE SYNDROME
Care of the Critically Unwell Patient. fluids
 Care of the Critically Unwell Patient fluids Are we made of water? YES! Humans are like cucumbers Water content at least half of body weight in healty adults (60%) blood volume 7% bw males 6% bw females
Care of the Critically Unwell Patient fluids Are we made of water? YES! Humans are like cucumbers Water content at least half of body weight in healty adults (60%) blood volume 7% bw males 6% bw females
Fluid & Electrolyte Balances in Term & Preterm Infants. Carolyn Abitbol, M.D. University of Miami/ Holtz Children s Hospital
 Fluid & Electrolyte Balances in Term & Preterm Infants Carolyn Abitbol, M.D. University of Miami/ Holtz Children s Hospital Objectives Review maintenance fluid & electrolyte requirements in neonates Discuss
Fluid & Electrolyte Balances in Term & Preterm Infants Carolyn Abitbol, M.D. University of Miami/ Holtz Children s Hospital Objectives Review maintenance fluid & electrolyte requirements in neonates Discuss
MODULE 8B: Management of Group B Dengue with Warning Signs or Dengue with Co-existing Conditions
 MODULE 8B: Management of Group B Dengue with Warning Signs or Dengue with Co-existing Conditions Dengue Clinical Management Acknowledgements This curriculum was developed with technical assistance from
MODULE 8B: Management of Group B Dengue with Warning Signs or Dengue with Co-existing Conditions Dengue Clinical Management Acknowledgements This curriculum was developed with technical assistance from
ACUTE GASTROENTERITIS IN CHILDREN
 ACUTE GASTROENTERITIS IN CHILDREN Prof. Alok Kumar Professor of Pediatrics & Infectious Diseases Faculty of Medical Sciences The University of the West Indies (Cave Hill) 11/6/2017 1 DEFINITION Gastroenteritis
ACUTE GASTROENTERITIS IN CHILDREN Prof. Alok Kumar Professor of Pediatrics & Infectious Diseases Faculty of Medical Sciences The University of the West Indies (Cave Hill) 11/6/2017 1 DEFINITION Gastroenteritis
Dilemmas in the Management of Meningitis & Encephalitis HEADACHE AND FEVER. What is the best initial approach for fever, headache, meningisums?
 Dilemmas in the Management of Meningitis & Encephalitis Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine HEADACHE AND FEVER What is the best initial approach for fever,
Dilemmas in the Management of Meningitis & Encephalitis Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine HEADACHE AND FEVER What is the best initial approach for fever,
Professor of microbiology and immunology Royal College of Pediatricians of Thailand
 Professor of microbiology and immunology Royal College of Pediatricians of Thailand Researching field New vaccines, new antibiotics, nosocomial infection, pediatric AIDS,immunologic deficiency diseases,
Professor of microbiology and immunology Royal College of Pediatricians of Thailand Researching field New vaccines, new antibiotics, nosocomial infection, pediatric AIDS,immunologic deficiency diseases,
Neonatal Sepsis. Neonatal sepsis ehandbook
 Neonatal Sepsis Neonatal sepsis ehandbook Sepsis Any baby who is unwell must be considered at risk of sepsis 1 in 8 per 1000 lives births The consequences of untreated sepsis are devastating - 10-30% risk
Neonatal Sepsis Neonatal sepsis ehandbook Sepsis Any baby who is unwell must be considered at risk of sepsis 1 in 8 per 1000 lives births The consequences of untreated sepsis are devastating - 10-30% risk
Pediatric Intensive Care Unit (PICU) Pediatric Diabetic Ketoacidosis (DKA) Admission Order Set
 Pediatric Diabetic Ketoacidosis (DKA) Admission Order Set") Discontinue all previous orders Weight: kg DKA admit order set is for initial management Ongoing management required based on frequent reassessment of TFI, fluid balance and lab results. Admit to PICU
Discontinue all previous orders Weight: kg DKA admit order set is for initial management Ongoing management required based on frequent reassessment of TFI, fluid balance and lab results. Admit to PICU
Determination of effect of low dose vs moderate dose clofibrate on decreasing serum bilirubin in healthy term neonates
 Original Article Iran J Ped June 2007, Vol 17 (No 2), Pp:108-112 Determination of effect of low dose vs moderate dose clofibrate on decreasing serum bilirubin in healthy term neonates Mohammad Ashkan Moslehi
Original Article Iran J Ped June 2007, Vol 17 (No 2), Pp:108-112 Determination of effect of low dose vs moderate dose clofibrate on decreasing serum bilirubin in healthy term neonates Mohammad Ashkan Moslehi
ID Emergencies. BGSMC Internal Medicine Edwin Yu
 ID Emergencies BGSMC Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
ID Emergencies BGSMC Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
Table 1. Agents to be avoided in G6PD Deficiency Patients MANAGEMENT OF NNJ
 NEONATAL JAUNDICE What is jaundice? Jaundice is apparent clinically when the level of bilirubin in the serum rises above 85µmol/l (5mg/dl). Physiological jaundice is a reflection of the bilirubin load
NEONATAL JAUNDICE What is jaundice? Jaundice is apparent clinically when the level of bilirubin in the serum rises above 85µmol/l (5mg/dl). Physiological jaundice is a reflection of the bilirubin load
GUIDELINE FOR THE MANAGEMENT OF MENINGOCOCCAL DISEASE
 GUIDELINE FOR THE MANAGEMENT OF MENINGOCOCCAL DISEASE Reference: MCD Version No: 1 Applicable to Children with suspected or confirmed meningococcal disease Classification of document: Area for Circulation:
GUIDELINE FOR THE MANAGEMENT OF MENINGOCOCCAL DISEASE Reference: MCD Version No: 1 Applicable to Children with suspected or confirmed meningococcal disease Classification of document: Area for Circulation:
CLINICAL GUIDELINES ID TAG
 CLINICAL GUIDELINES ID TAG Title: Author: Speciality / Division: Directorate: Guideline for the perioperative fluid management in children Kieran O Connor Anaesthetics ATICS Date Uploaded: 26/04/2016 Review
CLINICAL GUIDELINES ID TAG Title: Author: Speciality / Division: Directorate: Guideline for the perioperative fluid management in children Kieran O Connor Anaesthetics ATICS Date Uploaded: 26/04/2016 Review
An Approach to Jaundice Block 10. Dr AJ Terblanche Department of Paediatrics and Child Health
 An Approach to Jaundice Block 10 Dr AJ Terblanche Department of Paediatrics and Child Health JAUNDICE (ICTERUS) Yellow discoloration skin, sclerae, mucous membranes Observed 60% term, 80% preterm infants
An Approach to Jaundice Block 10 Dr AJ Terblanche Department of Paediatrics and Child Health JAUNDICE (ICTERUS) Yellow discoloration skin, sclerae, mucous membranes Observed 60% term, 80% preterm infants
11/21/2017 JUST THE FACTS!
 JUST THE FACTS! Katharine C Long, MD Establish differential diagnosis for the critically ill infant Create management approach for the critically ill infant Identify laboratory tests and interventions
JUST THE FACTS! Katharine C Long, MD Establish differential diagnosis for the critically ill infant Create management approach for the critically ill infant Identify laboratory tests and interventions