Aberrant hormone receptors in primary aldosteronism. André Lacroix, MD
|
|
|
- Roderick Goodman
- 6 years ago
- Views:
Transcription
 Controversias Clinicas en Enfermedades Suprarenales Buenos Aires, May 13,")
1 Aberrant hormone receptors in primary aldosteronism André Lacroix, MD Professor of Medicine Centre hospitalier de l Université de Montréal (CHUM) Controversias Clinicas en Enfermedades Suprarenales Buenos Aires, May 13, 2011


2 Aberrant hormone receptors Ectopic receptors GIPR β-adren receptors in adrenocortical cells ACTHR HTR4 LHCGR Eutopic Receptors AVPR1A G s AC G s AC camp G s AC ATP G q/i PLC ATP + camp ATP Cholesterol DAG, IP3 PKA P N M TF mrnas Protein Cortisol M Cortisol ACTHindependent Cushing s syndrome in AIMAH and adenomas Modified from Lacroix, Endocrine Reviews 22: 75, 2001

3 Aberrant receptors in all types of adrenal adenomas? Lacroix et al TEM 15: , 2004
4 Definition: primary aldosteronism Syndrome resulting from excess production of aldosterone Renin-independent production from unknown mechanism Causes cardiovascular damage, hypertension, sodium retention, renin suppression, potassium excretion that if prolonged and severe may lead to hypokalemia Funder et al J Clin Endocrinol Metab 93: 3266, 2008
5 Epidemiology of primary aldosteronism % incidence of HBP in USA population > 18 yo (NHANES) Low-renin essential hypertension: 25% Primary aldo: % of HBP ( ) Primary aldo: 7-10% of HBP ( ) Mulatero et al J Clin Endo Metab, 89:1045, 2004 Rossi et al J Am Coll Cardiol 48:2293, 2006 Mosso et al Hypertension 42: 161, 2003 Gordon et al Clin Exp Pharmacol Physiol 21:315:1994
6 Etiologies of Primary Aldosteronism Aldosterone-producing adenomas (APA): % ACTH-responsive (80-85%) Renin-responsive (15-20%) Idiopathic hyperaldosteronism (IHA; bilateral): % Primary adrenal hyperplasia (PAH; unilateral): < 2% Bilateral macronodular adrenal hyperplasia: < 2% Aldo/DOC-producing adrenal carcinoma: < 2% Aldosterone-producing ovarian tumor: < 1% Familial hyperaldosteronism (FH): < 2% Glucocorticoid-remediable aldosteronism (GRA;FH type I) Familial hyperaldosteronism type II (APA or IHA)
7 Primary aldosteronism Angiotensinogen Angiotensinogen Renin Renin A-II-independant aldosterone secretion Angiotensin-I Angiotensin-II ACE Constitutive secretion? Angiotensin-I Activating mutation of AT1R? Aldosterone Angiotensin-II Loss of inhibition (ANP, dopamine)? ACE Aldosterone Aberrant activating receptor? AT1R AT1R AT1R AT1R Bilateral Hyperplasia Unilateral adenoma

8 Science 331: 768, / 22 APA (2.8 cms) familial hyperplasia
 expressing aberrant receptors Lacroix et al, Clin Endocrinol, 75:1-15,")
9 Hypothesis of sequential genetic events leading to unilateral tumors or bilateral macronodular adrenal hyperplasia (AIMAH) expressing aberrant receptors Lacroix et al, Clin Endocrinol, 75:1-15, 2010
10 Aberant hormone receptors in aldosterone producing adenomas Increased expression of ACTH receptor (MC2R) in aldosterone-producing adenoma (APA) Arnaldi, G., Mancini, V., Costantini, C., Giovagnetti, M., Petrelli, M., Masini, A., Bertagna, X. & Mantero, F. ACTH receptor mrna in human adrenocortical tumors: overexpression in aldosteronomas. Endocr Res, 24, , 1998 Schubert, B., Fassnacht, M., Beuschlein, F., Zenkert, S., Allolio, B. & Reincke, M. Angiotensin II type 1 receptor and ACTH receptor expression in human adrenocortical neoplasms. Clin Endocrinol (Oxf), 54, , 2001 Ye, P., Mariniello, B., Mantero, F., Shibata, H. & Rainey, W.E. G-protein-coupled receptors in aldosterone-producing adenomas: a potential cause of hyperaldosteronism. J Endocrinol, 195, 39-48, 2007 Diurnal rythmn of aldosterone in APA suppressible by dexamethasone Increase after ACTH stimulation, stress

11 Regulation of aldosterone by cisapride and 5-HTR4 expression in aldosteronomas Cisapride Pre-op HTR4 by PCR Post-op Pre-op Post-op Cartier et al. European Journal of Endocrinology, 153, , 2005 Lefebvre et al. JCEM 87: , 2002

12 LH receptor overexpression in APA Saner-Amigh, K... Mantero, Rainey et al. J Clin Endocrinol Metab;91: , 2006
13 Aberrant hormone receptors in aldosterone producing adenomas Recent transcriptome studies showing > 15-fold increased expression of GPCR in aldosterone-producing adenomas (APA) Serotonin (HTR4) LHCGR GNRHR Glutamate receptor metabotropic 3 Endothelin receptor type B-like protein ACTH MC2R Ye P, Mariniello B, Mantero F, Shibata H, Rainey, W.E. G-protein-coupled receptors in aldosterone-producing adenomas: a potential cause of hyperaldosteronism. Journal of Endocrinology 195, 39-48, 2007
14 Strategy of in vivo investigation for aberrant receptors in primary aldosteronism Transient modulation of the ligands of potential aberrant adrenocortical hormone receptors Aldosterone response
15 Initial screening for aberrant responses Blood samples for aldosterone, renin, cortisol, ACTH, steroids/peptides q 30 min Perform under pretreatment with dexamethasone 1 mg q 6 h x 48h to suppress endogenous ACTH Modified from Lacroix et al The Endocrinologist 9, 9-15, 1999
16 Further investigation Lacroix et al The Endocrinologist 9, 9-15, 1999
17 Upright posture tests in primary aldosteronism Aldosterone (pmol/l) Upright posture patient A patient B patient C patient D patient E Time (minutes) Renin activity (ng/ml/h) 2 1,6 1,2 0,8 0,4 0 Upright posture patient A patient B patient C patient D patient E Time (minutes)
18 In vivo tests in a patient with aldosteronoma Lampron et al JCEM. 94:750-6, 2009

19 Aberrant receptors in aldosteronoma -B: GIPR+ adenoma -C: GIPR- adenoma -D: Adjacent adrenal GIPR immunohistochemistry Lampron et al JCEM. 94:750-6, 2009


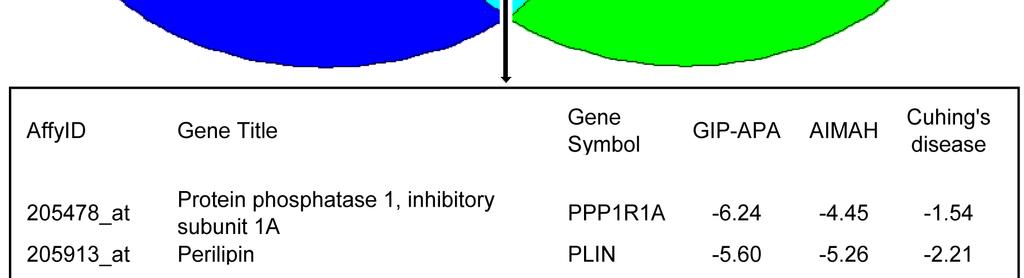
20 Gene expression profiling of adrenals with GIP-dependent steroid production
21 In vivo screening for aberrant receptors in primary aldosteronism 12 patients 5 APA, 7 IHA vs 8 normals Aberrant aldosterone responses in vivo: increased response to metoclopramide in 11/12 renin-independent upright posture : 5/12 vasopressin: 6/12 LHRH: 3/12 TRH: 1, glucagon: 1 Mixed meal: none Zwermann, O., Suttmann, Y., Bidlingmaier, M., Beuschlein, F. & Reincke, M. Screening for Membrane Hormone Receptor Expression in Primary Aldosteronism. Eur J Endocrinol, 160, , 2009
22 In vitro screening for aberrant receptors in primary aldosteronism 14 APA, 1 unilateral hyperplasia vs 6 normals high levels of AGTR1, MC2R, AVPR1A and HTR4 LHCGR in APA and normal tissues GNRH: 4/15 TSHR: 1/15 Good correlation between in vivo and in vitro results in 3 cases studied with both aproaches Zwermann, O., Suttmann, Y., Bidlingmaier, M., Beuschlein, F. & Reincke, M. Screening for Membrane Hormone Receptor Expression in Primary Aldosteronism. Eur J Endocrinol, 160, , 2009
23 32 yo, 28 wk pregnant BP: 180/120, low K + High PAC/RA ratio 2 cm left APA Days Renin-independent increase of aldosterone after GnRH (114%) and HCG (77%) Aldosterone levels increase after longacting GnRH analog despite suppression of LH

24 Albiger, Eur J Endo 164: 405, 2011
25 In vivo screening for aberrant receptors in primary aldosteronism 21 patients (8F, 13M). 11 APA, 10 IHA Protocol under dexamethasone: 18 suppression Aberrant aldosterone responses in 83%: renin-independent upright posture : 9 vasopressin: 10 increased 5HT4 agonist response: 14 GnRH: 7; LH: 1 GIP:1; TRH: 1; isoproterenol:1 Aberrant mild cortisol co-response in 10 Grunenwald, Mazzuco, Mermejo, Bourdeau, Lacroix Endo Society 2010
26 Frequency of aberrant aldosterone response % of patients total IH APA Aberrant responses Grunenwald, Mermejo, Mazzuco, Bourdeau, Lacroix Endo Society 2010
27 Aberrant responses to various tests aldosterone response > 50% no response of aldosterone Grunenwald, Mermejo, Mazzuco, Bourdeau, Lacroix Endo Society HT4 agonist upright posture vasopressin LHRH TRH mixt meal Grunenwald, Mermejo, Mazzuco, Bourdeau, Lacroix Endo Society 2010
28 Aberrant responses to various tests % of aldosterone increase ACTH 5-HT4 agonist upright posture vasopressin LHRH TRH mixed meal Grunenwald, Mermejo, Mazzuco, Bourdeau, Lacroix Endo Society 2010
29 Aberrant cortisol co-response to various tests no response of cortisol cortisol response >50% HT4 agonist upright posture vasopressin LHRH TRH mixt meal 8/10 patients with cosecretion of cortisol (ACTH suppressed) and aldosterone had at least one aberrant response of cortisol Grunenwald et al, Endo Society 2010

30 Expression levels of mrna for various GPCR by quantitative PCR in resected aldosteronomas AVPR1A, AVPR1B, AVPR Relative receptor expression Control AVPR1A Control AVPR1B Control AVPR2 HT4R, HT7R HT4R Control HT7R Control AGTR1, AGTR2 AGTR1 Control AGTR2 Control GNRHR, LHCGR, GIPR GNRHR Control LHCGR Control GIPR MC2R, FSHR, GCGR Control MC2R Control FSHR Control GCGR Relative receptor expression Relative receptor expression Relative receptor expression Control ADRB1, ADRB2, ADRB Control ADRB1 Control ADRB2 Control ADRB3 Relative receptor expression Relative receptor expression Good correlations between in vivo stimulation and receptor levels Elevated mrna levels do not always predict clinical response Mermejo LM, Grunenwald S, MazzucoTL, Bourdeau I, Lacroix A Endo Society 2011

31 Clinical Case: AIMAH secreting aldosterone and cortisol 65 y.o. woman from Haiti, retired nurse High blood pressure x 8 yrs: 152/89 to 173/105 Recurrent hypokalemia on ARB, CCB requiring potassium supplements of 40 meq daily Diabetes x 4 years well controlled on metformin BMI of 24.3 No Cushing s signs or hirsutism No pertinent family history
32 Initial investigation Normal fasting blood glucose, creatinine Na + : 139 mmol/l, K + : 3.1 mmol/l Standing plasma aldosterone concentration: 962 pmol/l (N: ) Standing plasma renin activity: 0.2 ng/ml/h (N: < 5.3) Plasma aldosterone/renin ratio: > 1000 (N: < 555) 24-h urinary aldosterone on high salt: 106 nmol/d (N: <36) Urinary free cortisol: nmol/d (N:55-330) Dexa 1 mg : morning cortisol : 128 nmol/l (N < 50) Plasma ACTH: <0.5 pmol/l (N: 2-11) Urinary catecholamines/metanephrins: normal range
33 Consultant: your suggestions? Differential diagnosis: Primary aldosteronism Bilateral macronodular adrenal hyperplasia Sub-clinical cortisol secretion Further investigations: 1: CRH test: ACTH < 0.5 pmol/l 2: ACTH test: cortisol: 246 to 1375 nmol/l 17-OH-P: 4.4 to 52.9 nmol/l 3: Aberrant receptor protocol
34 Aldosterone and cortisol-secreting AIMAH Plasma Aldosterone (% of basal) Vasopressin DDAVP Tegaserod Posture Plasma Aldosterone (% of basal) Meal ACTH LHRH TRH Time (minutes) Renin activity: 0.2 ng/ml/h during all tests Time (minutes)
35 Aldosterone and cortisol-secreting AIMAH Vasopressin Tegaserod Meal ACTH LHRH TRH 500 DDAVP Posture 1000 Plasma cortisol (% of basal) Plasma cortisol (% of basal) Time (minutes) ACTH:< 0.5 pmol/l during various tests Time (minutes)
36 Further evaluation and therapy Possible coronary disease prevented isoproterenol infusion Pre-treatment with propranolol or ARB x 3 days did not modify aldosterone or cortisol response to upright posture Moderate hypertension, diabetes, osteopenia and sub-clinical cortisol production in addition to primary aldosteronism Diagnosis of mixed aldosterone and cortisol secreting AIMAH with regulation at least by by vasopressin (renin-and ACTH-independent) Surgical therapy Right adrenalectomy Response of aldosterone and cortisol to upright posture reduced by 50% Spironolactone 100 mg daily, CCB, stop potassium; Bisphosphonates, calcium, vit D, aspirin: BP below 135/80
37 Clinical Case: Primary aldosteronism and AIMAH 51 yo woman HBP x 15 years Hypokalemia Primary aldo x 1989 Bilateral nodular UFC: nmol/d Dex 1 mg: p F: 91 nmol/l 1990: Right adrenalectomy Rx: Aldactone, Midamor, Cardizem, Captopril Left adrenal size increase Plasma Cortisol (nmol/l) DEXA 1mg/hr AVP 10 iu im 2 Years Post-op op D2 9D3 Time (hours)
38 Aberrant Adrenal Hormone Receptors Therapeutic Potential in IHA? Aberrant receptor GIP β-adrenergic LH/hCG V 1 -vasopressin Serotonin R4 Angiotensin II TSH Therapy Somatostatin/GIPR blocker β-blockers GnRH analogs AVPR1A antagonist HTR4 antagonist AGTR1 antagonist L-thyroxine
39 CONCLUSIONS 1) Primary aldosteronism is renin-independent but not autonomous in the majority of cases 2) Aberrant adrenal hormone receptors appear to be frequently implicated in the regulation of aldosterone secretion in unilateral aldosteronomas and bilateral idiopathic hyperaldosteronism 3) The aberrant regulation of aldosterone secretion can be modulated by ectopic receptors or by increased activity of eutopic receptors 4) Single or multiple adrenal receptors can be aberrantly functional
40 Remaining questions Consequences of aberrant receptors on Aldo/Renin Ratios (ARR) depending on: posture? fasting? menstrual cycle? Consequences of aberrant hormone receptors (AVPR1A) on saline infusion tests in diagnosis of primary aldosteronism Consequences of ACTH receptor level on response to ACTH and interpretation of lateralisation during adrenal vein sampling? Link between aberrant receptors and K + channel mutations?

41 Aknowledgments Co-investigators Isabelle Bourdeau Pavel Hamet Johanne Tremblay Lab Endocrine Pathophysiology Livia Mermejo Antoine Lampron M H Soares Costa Tania Mazzuco Solange Grunenwald Sylvie Oble CHUM Endocrinology Ariane Godbout J-M Boutin Pierre D Amour Hortensia Mircescu Shirley Ferguson Sylvie Blaquière Chantal Dejou Philippe Arjane Walter Schurch Other centers Pierre Larochelle Hervé Lefebvre Funding Grant MA Canadian Institutes of Health Research
Role of aberrant hormone receptors André Lacroix, MD
 New Mechanisms of Adrenal Tumorigenesis Role of aberrant hormone receptors André Lacroix, MD Professor of Medicine Centre hospitalier de l Université de Montréal (CHUM) Controversias Clinicas en Enfermedades
New Mechanisms of Adrenal Tumorigenesis Role of aberrant hormone receptors André Lacroix, MD Professor of Medicine Centre hospitalier de l Université de Montréal (CHUM) Controversias Clinicas en Enfermedades
Year 2004 Paper two: Questions supplied by Megan 1
 Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
AVS and IPSS: The Basics and the Pearls
 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2018 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2018 Mayo Foundation for Medical Education and Research.
Primary Aldosteronism
 Primary Aldosteronism Odelia Cooper, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism Cedars-Sinai Medical Center HYPERTENSION CENTER Barriers to diagnosing primary
Primary Aldosteronism Odelia Cooper, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism Cedars-Sinai Medical Center HYPERTENSION CENTER Barriers to diagnosing primary
Clarification of hypertension Diagnosis of primary hyperaldosteronism
 Nr. 1/2010 Clarification of hypertension Diagnosis of primary hyperaldosteronism Marc Beineke The significance of the /renin ratio (ARR) in the diagnosis of normoalaemic and hypokalaemic primary hyperaldosteronism,
Nr. 1/2010 Clarification of hypertension Diagnosis of primary hyperaldosteronism Marc Beineke The significance of the /renin ratio (ARR) in the diagnosis of normoalaemic and hypokalaemic primary hyperaldosteronism,
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA
 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.
Updates in primary hyperaldosteronism and the rule
 Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. Professor of Medicine and Physiology and Functional Genomics University of Florida College of Medicine and NF/SGVHS The 20-50
Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. Professor of Medicine and Physiology and Functional Genomics University of Florida College of Medicine and NF/SGVHS The 20-50
A Rare Case of ACTH-independent Macronodular Adrenal Hyperplasia Associated with Aldosterone-producing Adenoma
 CASE REPORT A Rare Case of ACTHindependent Macronodular Adrenal Hyperplasia Associated with Aldosteroneproducing Adenoma Eri Hayakawa 1, Takanobu Yoshimoto 1, Kiichiro Hiraishi 1, Masako Kato 1, Hajime
CASE REPORT A Rare Case of ACTHindependent Macronodular Adrenal Hyperplasia Associated with Aldosteroneproducing Adenoma Eri Hayakawa 1, Takanobu Yoshimoto 1, Kiichiro Hiraishi 1, Masako Kato 1, Hajime
Primary Aldosteronism: screening, diagnosis and therapy
 Primary Aldosteronism: screening, diagnosis and therapy Jacques W.M. Lenders, internist DEPT. OF INTERNAL MEDICINE, RADBOUD UNIVERSITY NIJMEGEN MEDICAL CENTER, NIJMEGEN,THE NETHERLANDS DEPT. OF INTERNAL
Primary Aldosteronism: screening, diagnosis and therapy Jacques W.M. Lenders, internist DEPT. OF INTERNAL MEDICINE, RADBOUD UNIVERSITY NIJMEGEN MEDICAL CENTER, NIJMEGEN,THE NETHERLANDS DEPT. OF INTERNAL
Primary aldosteronism clinical practice guidelines: a re-appraisal The Management of Primary Aldosteronism
 Primary aldosteronism clinical practice guidelines: a re-appraisal The Management of Primary Aldosteronism Prof. FRANCO MANTERO Division of Endocrinology University of Padua Italy Case Detection, Diagnosis
Primary aldosteronism clinical practice guidelines: a re-appraisal The Management of Primary Aldosteronism Prof. FRANCO MANTERO Division of Endocrinology University of Padua Italy Case Detection, Diagnosis
CASE REPORT. Abstract. Introduction. Misaki Miyata 1,2, Masanori Yoshida 1,2, Junji Shinoda 1, Hironobu Sasano 3 and Yutaka Oiso 4
 CASE REPORT A Marked Difference in the Vasopressin Responsiveness Between the Adrenal Glands in a Patient with Adrenocorticotropin-independent Macronodular Adrenal Hyperplasia Misaki Miyata 1,2, Masanori
CASE REPORT A Marked Difference in the Vasopressin Responsiveness Between the Adrenal Glands in a Patient with Adrenocorticotropin-independent Macronodular Adrenal Hyperplasia Misaki Miyata 1,2, Masanori
Endocrine. Endocrine as it relates to the kidney. Sarah Elfering, MD University of Minnesota
 Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Updates in primary hyperaldosteronism and the rule
 Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of
Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of
Approach to Adrenal Incidentaloma. Alice Y.Y. Cheng, MD, FRCP
 Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone
 Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Spectrum of Hypertension & Hypokalemia
 Spectrum of Hypertension & Hypokalemia Farheen K. Dojki, PGY-6 Hypertension Fellow, ASH Hypertension Center Dr. Dojki does not have any relevant financial relationships with any commercial interests. OBJECTIVES:
Spectrum of Hypertension & Hypokalemia Farheen K. Dojki, PGY-6 Hypertension Fellow, ASH Hypertension Center Dr. Dojki does not have any relevant financial relationships with any commercial interests. OBJECTIVES:
Endocrine hypertensionmolecules. Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015
 Endocrine hypertensionmolecules and genes Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015 Plan Mineralocorticoid hypertension Myths surrounding Primary Aldosteronism (PA) New developments
Endocrine hypertensionmolecules and genes Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015 Plan Mineralocorticoid hypertension Myths surrounding Primary Aldosteronism (PA) New developments
The Work-up and Treatment of Adrenal Nodules
 The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
How to Recognize Adrenal Disease
 How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
Upon completion, participants should be able to:
 Learning Objectives Upon completion, participants should be able to: Describe the causes of secondary hypertension and the prevalence of primary aldosteronism Discuss the diagnostic approach to primary
Learning Objectives Upon completion, participants should be able to: Describe the causes of secondary hypertension and the prevalence of primary aldosteronism Discuss the diagnostic approach to primary
CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES
 HORMONES OF ADRENAL CORTEX R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES CONVERSION OF CHOLESTROL TO PREGNENOLONE MINERALOCORTICOCOIDES
HORMONES OF ADRENAL CORTEX R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES CONVERSION OF CHOLESTROL TO PREGNENOLONE MINERALOCORTICOCOIDES
Adrenal incidentaloma guideline for Northern Endocrine Network
 Adrenal incidentaloma guideline for Northern Endocrine Network Definition of adrenal incidentaloma Adrenal mass detected on an imaging study done for indications that are not related to an adrenal problem
Adrenal incidentaloma guideline for Northern Endocrine Network Definition of adrenal incidentaloma Adrenal mass detected on an imaging study done for indications that are not related to an adrenal problem
Hormones. Introduction to Endocrine Disorders. Hormone actions. Modulation of hormone levels. Modulation of hormone levels
 Introduction to Endocrine Disorders Hormones Self-regulating system (homeostasis) Affect: Growth Metabolism Reproduction Fluid and electrolyte balance Hormone actions Endocrine gland Hormone synthesis
Introduction to Endocrine Disorders Hormones Self-regulating system (homeostasis) Affect: Growth Metabolism Reproduction Fluid and electrolyte balance Hormone actions Endocrine gland Hormone synthesis
ULTIMATE BEAUTY OF BIOCHEMISTRY. Dr. Veena Bhaskar S Gowda Dept of Biochemistry 30 th Nov 2017
 ULTIMATE BEAUTY OF BIOCHEMISTRY Dr. Veena Bhaskar S Gowda Dept of Biochemistry 30 th Nov 2017 SUSPECTED CASE OF CUSHING S SYNDROME Clinical features Moon face Obesity Hypertension Hunch back Abdominal
ULTIMATE BEAUTY OF BIOCHEMISTRY Dr. Veena Bhaskar S Gowda Dept of Biochemistry 30 th Nov 2017 SUSPECTED CASE OF CUSHING S SYNDROME Clinical features Moon face Obesity Hypertension Hunch back Abdominal
Disorders of the Adrenal Cortex
 Disorders of the Adrenal Cortex Cushing s Syndrome and Primary Aldosteronism 凌雁 Yan Ling Department of Endocrinology and Metabolism Zhongshan Hospital Fudan University Cushing s Syndrome Definition of
Disorders of the Adrenal Cortex Cushing s Syndrome and Primary Aldosteronism 凌雁 Yan Ling Department of Endocrinology and Metabolism Zhongshan Hospital Fudan University Cushing s Syndrome Definition of
Hofland et al. Orphanet Journal of Rare Diseases 2013, 8:142
 Hofland et al. Orphanet Journal of Rare Diseases 2013, 8:142 RESEARCH Open Access ACTH-independent macronodular adrenocortical hyperplasia reveals prevalent aberrant in vivo and in vitro responses to hormonal
Hofland et al. Orphanet Journal of Rare Diseases 2013, 8:142 RESEARCH Open Access ACTH-independent macronodular adrenocortical hyperplasia reveals prevalent aberrant in vivo and in vitro responses to hormonal
About 20% of the Canadian population
 Mineralocorticoid Hypertension: Common and Treatable Hypertension is the most common chronic disease treated by the primary-care physician. It is now evident that mineralocorticoid hypertension, which
Mineralocorticoid Hypertension: Common and Treatable Hypertension is the most common chronic disease treated by the primary-care physician. It is now evident that mineralocorticoid hypertension, which
C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management
 C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management Padma S Menon Professor of Endocrinology, Seth G S Medical College & KEM Hospital, Mumbai A clinical syndrome resulting
C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management Padma S Menon Professor of Endocrinology, Seth G S Medical College & KEM Hospital, Mumbai A clinical syndrome resulting
27 F with new onset hypertension and weight gain. Rajesh Jain Endorama 10/01/2015
 27 F with new onset hypertension and weight gain Rajesh Jain Endorama 10/01/2015 HPI 27 F with hypertension x 1 year BP 130-140/90 while on amlodipine 5 mg daily She also reports weight gain, 7 LB, mainly
27 F with new onset hypertension and weight gain Rajesh Jain Endorama 10/01/2015 HPI 27 F with hypertension x 1 year BP 130-140/90 while on amlodipine 5 mg daily She also reports weight gain, 7 LB, mainly
A case of Adrenocoricotrophic hormone -independent bilateral adrenocortical macronodular hyperplasia concomitant with primary aldosteronism
 Tokumoto et al. BMC Surgery (2017) 17:97 DOI 10.1186/s12893-017-0293-z CASE REPORT Open Access A case of Adrenocoricotrophic hormone -independent bilateral adrenocortical macronodular hyperplasia concomitant
Tokumoto et al. BMC Surgery (2017) 17:97 DOI 10.1186/s12893-017-0293-z CASE REPORT Open Access A case of Adrenocoricotrophic hormone -independent bilateral adrenocortical macronodular hyperplasia concomitant
Primary Aldosteronism & Implications for Primary Hypertension
 & Implications for Primary Hypertension Richard J. Auchus, MD, PhD, FACE Professor and Fellowship Program Director Depts of Internal Medicine/MEND & Pharmacology University of Michigan Disclosures Contracted
& Implications for Primary Hypertension Richard J. Auchus, MD, PhD, FACE Professor and Fellowship Program Director Depts of Internal Medicine/MEND & Pharmacology University of Michigan Disclosures Contracted
Incidental Adrenal Nodules Differential Diagnosis
 Adrenal Stuff Richard J. Auchus, MD, PhD, FACE Division of Metabolism, Endocrinology & Diabetes Departments of Internal Medicine & Pharmacology University of Michigan/VA Ann Arbor Incidental Adrenal Nodules
Adrenal Stuff Richard J. Auchus, MD, PhD, FACE Division of Metabolism, Endocrinology & Diabetes Departments of Internal Medicine & Pharmacology University of Michigan/VA Ann Arbor Incidental Adrenal Nodules
Aberrant expression of multiple hormone receptors in ACTH-independent macronodular adrenal hyperplasia causing Cushing s syndrome
 European Journal of Endocrinology (21) 163 293 299 ISSN 84-4643 CLINICAL STUDY Aberrant expression of multiple hormone receptors in ACTH-independent macronodular adrenal hyperplasia causing Cushing s syndrome
European Journal of Endocrinology (21) 163 293 299 ISSN 84-4643 CLINICAL STUDY Aberrant expression of multiple hormone receptors in ACTH-independent macronodular adrenal hyperplasia causing Cushing s syndrome
Texte titre présentation titre texte titre présentation titre text
 Hyperplasie macronodulaire des surrénales : stratégies de recherche de nouveaux gènes de prédisposition Texte titre présentation titre texte titre présentation titre text Auteur Pr Guillaume - Assié titre
Hyperplasie macronodulaire des surrénales : stratégies de recherche de nouveaux gènes de prédisposition Texte titre présentation titre texte titre présentation titre text Auteur Pr Guillaume - Assié titre
Adrenal incidentaloma
 Adrenal incidentaloma Prevalence 5% post-mortem series 4% CT series 6-20% CT series in patients with Hx extra-adrenal malignancy Commoner with increasing age Associated with adrenal hyperfunction in 15%
Adrenal incidentaloma Prevalence 5% post-mortem series 4% CT series 6-20% CT series in patients with Hx extra-adrenal malignancy Commoner with increasing age Associated with adrenal hyperfunction in 15%
Vasopressin-Responsive ACTH-Independent Macronodular Adrenal Hyperplasia Causing Cushing s Syndrome
 TZU CHI MED J September 2007 Vol 19 No 3 available at http://health.elsevier.com/tcmj Tzu Chi Medical Journal Case Report Vasopressin-Responsive ACTH-Independent Macronodular Adrenal Hyperplasia Causing
TZU CHI MED J September 2007 Vol 19 No 3 available at http://health.elsevier.com/tcmj Tzu Chi Medical Journal Case Report Vasopressin-Responsive ACTH-Independent Macronodular Adrenal Hyperplasia Causing
The Management of Primary Aldosteronism: Case Detection, Diagnosis, and Treatment: An Endocrine Society Clinical Practice Guideline
 SPECIAL FEATURE Clinical Practice Guideline The Management of Primary Aldosteronism: Case Detection, Diagnosis, and Treatment: An Endocrine Society Clinical Practice Guideline John W. Funder, Robert M.
SPECIAL FEATURE Clinical Practice Guideline The Management of Primary Aldosteronism: Case Detection, Diagnosis, and Treatment: An Endocrine Society Clinical Practice Guideline John W. Funder, Robert M.
ENDOCRINE FORMS OF HYPERTENSION. Michael Stowasser
 ENDOCRINE FORMS OF HYPERTENSION Michael Stowasser Hypertension Unit, University Department of Medicine, Princess Alexandra Hospital, Brisbane 4102, Australia. ENDOCRINE FORMS OF HYPERTENSION Mineralocorticoid
ENDOCRINE FORMS OF HYPERTENSION Michael Stowasser Hypertension Unit, University Department of Medicine, Princess Alexandra Hospital, Brisbane 4102, Australia. ENDOCRINE FORMS OF HYPERTENSION Mineralocorticoid
Subclinical Cushing s Syndrome
 Subclinical Cushing s Syndrome AACE 26th Annual Scientific & Clinical Congress Associate Clinical Professor of Medicine and Clinical Chief University of Miami Miller Scholl of Medicine Miami, Florida aayala2@miami.edu
Subclinical Cushing s Syndrome AACE 26th Annual Scientific & Clinical Congress Associate Clinical Professor of Medicine and Clinical Chief University of Miami Miller Scholl of Medicine Miami, Florida aayala2@miami.edu
as ACTH-independent macronodular adrenal hyperplasia (AIMAH)
") Endocrinol Metab 26(1):1-11, March 2011 REVIEW ARTICLE ACTH-Independent Macronodular Adrenal Hyperplasia Livia M. Mermejo, Tânia L. Mazzuco, Solange Grunenwald, Maria Candida B. V. Fragoso, Isabelle Bourdeau,
Endocrinol Metab 26(1):1-11, March 2011 REVIEW ARTICLE ACTH-Independent Macronodular Adrenal Hyperplasia Livia M. Mermejo, Tânia L. Mazzuco, Solange Grunenwald, Maria Candida B. V. Fragoso, Isabelle Bourdeau,
ADRENAL INCIDENTALOMA. Jamii St. Julien
 ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
Assistant Professor of Endocrinology
 Pathophysiology Of Adrenal Disorder Dr.Rezvan Salehidoost Assistant Professor of Endocrinology Pathophysiology Of Adrenal Disorder The adrenal glands lie at the superior pole of each kidney and are composed
Pathophysiology Of Adrenal Disorder Dr.Rezvan Salehidoost Assistant Professor of Endocrinology Pathophysiology Of Adrenal Disorder The adrenal glands lie at the superior pole of each kidney and are composed
Secondary Hypertension: A Real World Approach
 Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
The endocrine system is made up of a complex group of glands that secrete hormones.
 1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
Dimitrios Linos, M.D., Ph.D. Professor of Surgery National & Kapodistrian University of Athens
 Dimitrios Linos, M.D., Ph.D. Professor of Surgery National & Kapodistrian University of Athens What is an adrenal incidentaloma? An adrenal incidentaloma is defined as an adrenal tumor initially diagnosed
Dimitrios Linos, M.D., Ph.D. Professor of Surgery National & Kapodistrian University of Athens What is an adrenal incidentaloma? An adrenal incidentaloma is defined as an adrenal tumor initially diagnosed
ADRENAL VEIN SAMPLING: AN INTEGRAL PART OF MANAGING COMPLICATED ADRENAL HYPERTENSION- SAFE? WORTH IT?
 ADRENAL VEIN SAMPLING: AN INTEGRAL PART OF MANAGING COMPLICATED ADRENAL HYPERTENSION- SAFE? WORTH IT? Chaitanya Ahuja, M.D. Assistant Professor, Vascular and Interventional Radiology Director of Interventional
ADRENAL VEIN SAMPLING: AN INTEGRAL PART OF MANAGING COMPLICATED ADRENAL HYPERTENSION- SAFE? WORTH IT? Chaitanya Ahuja, M.D. Assistant Professor, Vascular and Interventional Radiology Director of Interventional
TREATMENT OF CUSHING S DISEASE
 TREATMENT OF CUSHING S DISEASE Surgery, Radiation, Medication Peter J Snyder, MD Professor of Medicine Disclosures Novartis Research grant Pfizer Consultant Ipsen Research grant Cortendo Research grant
TREATMENT OF CUSHING S DISEASE Surgery, Radiation, Medication Peter J Snyder, MD Professor of Medicine Disclosures Novartis Research grant Pfizer Consultant Ipsen Research grant Cortendo Research grant
Aldosterone synthase inhibitors. John McMurray BHF Cardiovascular Research Centre University of Glasgow
 Aldosterone synthase inhibitors John McMurray BHF Cardiovascular Research Centre University of Glasgow Inhibition of aldosterone synthesis is hypothesized to be of benefit to patients with cardiovascular
Aldosterone synthase inhibitors John McMurray BHF Cardiovascular Research Centre University of Glasgow Inhibition of aldosterone synthesis is hypothesized to be of benefit to patients with cardiovascular
Adrenal Mass. Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016
 Adrenal Mass Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016 Case Presentation 65F found to have a 4cm left adrenal mass in 2012 now presents with 6.7cm left adrenal mass PMHx:
Adrenal Mass Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016 Case Presentation 65F found to have a 4cm left adrenal mass in 2012 now presents with 6.7cm left adrenal mass PMHx:
Neuroendocrine Disorders in Women
 Neuroendocrine Disorders in Women Ursula B. Kaiser, M.D. Chief, Division of Endocrinology, Diabetes and Hypertension Brigham and Women s Hospital Professor of Medicine, Harvard Medical School Case Presentation
Neuroendocrine Disorders in Women Ursula B. Kaiser, M.D. Chief, Division of Endocrinology, Diabetes and Hypertension Brigham and Women s Hospital Professor of Medicine, Harvard Medical School Case Presentation
The diversity of abnormal hormone receptors in adrenal Cushing s syndrome allows novel pharmacological therapies
 Brazilian Journal of Medical and Biological Research (2000) 33: 1201-1209 Abnormal hormone receptors in adrenal Cushing s syndrome ISSN 0100-879X 1201 The diversity of abnormal hormone receptors in adrenal
Brazilian Journal of Medical and Biological Research (2000) 33: 1201-1209 Abnormal hormone receptors in adrenal Cushing s syndrome ISSN 0100-879X 1201 The diversity of abnormal hormone receptors in adrenal
John Sutton, DO, FACOI, FACE, CCD. Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989
 John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 Gonadal Physiology and Disease 3 No Disclosures Gonadal Axis Hypothalamic-pituitary-gonadal Feedback mechanisms
John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 Gonadal Physiology and Disease 3 No Disclosures Gonadal Axis Hypothalamic-pituitary-gonadal Feedback mechanisms
Endocrine MR. Jan 30, 2015 Michael LaFata, MD
 Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
Endocrine Emergencies: Recognition and Management
 Endocrine Emergencies: Recognition and Management John Wass Department of Endocrinology, Oxford University, UK An Update on Acute Medical Emergencies for Psychiatrists Royal College of Psychiatrists' address
Endocrine Emergencies: Recognition and Management John Wass Department of Endocrinology, Oxford University, UK An Update on Acute Medical Emergencies for Psychiatrists Royal College of Psychiatrists' address
Adrenal Vein Sampling: A Critical Tool for Subtyping Primary Aldosteronism
 Adrenal Vein Sampling: A Critical Tool for Subtyping Primary Aldosteronism Disclosures No conflicts of interest relevant to this presentation Jason W. Pinchot, M.D. Assistant Professor, Vascular and Interventional
Adrenal Vein Sampling: A Critical Tool for Subtyping Primary Aldosteronism Disclosures No conflicts of interest relevant to this presentation Jason W. Pinchot, M.D. Assistant Professor, Vascular and Interventional
Resistant hypertension is defined as blood. Primary Hyperaldosteronism Decoded: A Case of Curable Resistant Hypertension.
 Case Review Primary Hyperaldosteronism Decoded: A Case of Curable Resistant Hypertension Timothy R. Larsen, DO, Wadie David, Susan Steigerwalt, MD, Shukri David, MD Department of Internal Medicine, Section
Case Review Primary Hyperaldosteronism Decoded: A Case of Curable Resistant Hypertension Timothy R. Larsen, DO, Wadie David, Susan Steigerwalt, MD, Shukri David, MD Department of Internal Medicine, Section
Endocrine Hypertension
 Endocrine Hypertension 1 No Disclosures Endocrine Hypertension Objectives: 1. Understand Endocrine disorders causing hypertension 2. Understand clinical presentation of Pheochromocytoma and Hyperaldosteronism
Endocrine Hypertension 1 No Disclosures Endocrine Hypertension Objectives: 1. Understand Endocrine disorders causing hypertension 2. Understand clinical presentation of Pheochromocytoma and Hyperaldosteronism
Diseases of the Adrenal gland
 Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
G-protein-coupled receptors in aldosterone-producing adenomas: a potential cause of hyperaldosteronism
 39 G-protein-coupled receptors in aldosterone-producing adenomas: a potential cause of hyperaldosteronism Ping Ye, Barbara Mariniello 1, Franco Mantero 1, Hirotaka Shibata 2 and William E Rainey Department
39 G-protein-coupled receptors in aldosterone-producing adenomas: a potential cause of hyperaldosteronism Ping Ye, Barbara Mariniello 1, Franco Mantero 1, Hirotaka Shibata 2 and William E Rainey Department
CUSHING SYNDROME Dr. Muhammad Sarfraz
 Indep Rev Jul-Dec 2018;20(7-12) CUSHING SYNDROME Dr. Muhammad Sarfraz IR-655 Abstract: It is defined as clinical condition in which there are increased free circulating glucocorticoides casused by excessive
Indep Rev Jul-Dec 2018;20(7-12) CUSHING SYNDROME Dr. Muhammad Sarfraz IR-655 Abstract: It is defined as clinical condition in which there are increased free circulating glucocorticoides casused by excessive
LONG-TERM EFFECTS OF SURGICAL MENAGEMENT OF PRIMARY ALDOSTERONISM ON THE CARDIOVASCULAR SISTEM
 LONG-TERM EFFECTS OF SURGICAL MENAGEMENT OF PRIMARY ALDOSTERONISM ON THE CARDIOVASCULAR SISTEM Riccardo Marsili, Pietro Iacconi, Massimo Chiarugi, Giampaolo Bernini*, Alessandra Bacca*, Paolo Miccoli Department
LONG-TERM EFFECTS OF SURGICAL MENAGEMENT OF PRIMARY ALDOSTERONISM ON THE CARDIOVASCULAR SISTEM Riccardo Marsili, Pietro Iacconi, Massimo Chiarugi, Giampaolo Bernini*, Alessandra Bacca*, Paolo Miccoli Department
Inquadramento Clinico dell IncIdentaloma SurrenalIco
 Ferrara, 7 dicembre 2012 Inquadramento Clinico dell IncIdentaloma SurrenalIco Marta Bondanelli Sezione di Endocrinologia Dip. di Scienze Mediche Università degli Studi di Ferrara ADRENAL INCIDENTALOMA
Ferrara, 7 dicembre 2012 Inquadramento Clinico dell IncIdentaloma SurrenalIco Marta Bondanelli Sezione di Endocrinologia Dip. di Scienze Mediche Università degli Studi di Ferrara ADRENAL INCIDENTALOMA
A 64 year old man referred for evaluation of suspected hyperaldosteronism
 A 64 year old man referred for evaluation of suspected hyperaldosteronism Dr. Dickens does not have any relevant financial relationships with any commercial interests. ENDORAMA: 64 year old man referred
A 64 year old man referred for evaluation of suspected hyperaldosteronism Dr. Dickens does not have any relevant financial relationships with any commercial interests. ENDORAMA: 64 year old man referred
European Journal of Endocrinology (2010) ISSN
 ISSN") European Journal of Endocrinology (2010) 163 129 138 ISSN 0804-4643 CLINICAL STUDY Aberrant cortisol regulations in bilateral macronodular adrenal hyperplasia: a frequent finding in a prospective study
European Journal of Endocrinology (2010) 163 129 138 ISSN 0804-4643 CLINICAL STUDY Aberrant cortisol regulations in bilateral macronodular adrenal hyperplasia: a frequent finding in a prospective study
14 Girl with Cushing s Disease: An Update. Kristen Dillard, MD Endorama October 17, 2013
 14 Girl with Cushing s Disease: An Update Kristen Dillard, MD Endorama October 17, 2013 Initial Presentation Pt initially presented to pediatrician for school physical in fall 2012. Pt was found to be
14 Girl with Cushing s Disease: An Update Kristen Dillard, MD Endorama October 17, 2013 Initial Presentation Pt initially presented to pediatrician for school physical in fall 2012. Pt was found to be
MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL?
 MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL? Alice C. Levine, MD Professor of Medicine Division of Endocrinology, Diabetes and Bone Diseases Georgia-AACE 2017 Annual Meeting
MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL? Alice C. Levine, MD Professor of Medicine Division of Endocrinology, Diabetes and Bone Diseases Georgia-AACE 2017 Annual Meeting
Prognosis of primary aldosteronism in Japan: results from a nationwide epidemiological study
 Endocrine Journal 2013 Or i g i n a l Advance Publication doi: 10.1507/endocrj. EJ13-0353 Prognosis of primary aldosteronism in Japan: results from a nationwide epidemiological study Yoshihiro Miyake 1),
Endocrine Journal 2013 Or i g i n a l Advance Publication doi: 10.1507/endocrj. EJ13-0353 Prognosis of primary aldosteronism in Japan: results from a nationwide epidemiological study Yoshihiro Miyake 1),
CPY 605 ADVANCED ENDOCRINOLOGY
 CPY 605 ADVANCED ENDOCRINOLOGY THE ADRENAL CORTEX PRESENTED BY WAINDIM NYIAMBAM YVONNE HS09A187 INTRODUCTION Two adrenal glands lie on top of each kidney. Each gland between 6 and 8g in weight is composed
CPY 605 ADVANCED ENDOCRINOLOGY THE ADRENAL CORTEX PRESENTED BY WAINDIM NYIAMBAM YVONNE HS09A187 INTRODUCTION Two adrenal glands lie on top of each kidney. Each gland between 6 and 8g in weight is composed
How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016
 How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016 World beaters..! Michel Joffres et al. BMJ Open 2013;3:e003423 Hypertension often poorly controlled
How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016 World beaters..! Michel Joffres et al. BMJ Open 2013;3:e003423 Hypertension often poorly controlled
Adrenocorticotropic Hormone-Independent Cushing Syndrome with Bilateral Cortisol-Secreting Adenomas
 Case Report Endocrinol Metab 2013;28:133-137 http://dx.doi.org/10.3803/enm.2013.28.2.133 pissn 2093-596X eissn 2093-5978 Adrenocorticotropic Hormone-Independent Cushing Syndrome with Bilateral Cortisol-Secreting
Case Report Endocrinol Metab 2013;28:133-137 http://dx.doi.org/10.3803/enm.2013.28.2.133 pissn 2093-596X eissn 2093-5978 Adrenocorticotropic Hormone-Independent Cushing Syndrome with Bilateral Cortisol-Secreting
BRIEF REPORT. Clinical Studies
 Brief Report LEUPROLIDE ACETATE THERAPY IN LUTEINIZING HORMONE DEPENDENT CUSHING S SYNDROME ANDRÉ LACROIX, M.D., PAVEL HAMET, M.D., PH.D., AND JEAN-MARIE BOUTIN, M.D., PH.D. CORTICOTROPIN-INDEPENDENT Cushing
Brief Report LEUPROLIDE ACETATE THERAPY IN LUTEINIZING HORMONE DEPENDENT CUSHING S SYNDROME ANDRÉ LACROIX, M.D., PAVEL HAMET, M.D., PH.D., AND JEAN-MARIE BOUTIN, M.D., PH.D. CORTICOTROPIN-INDEPENDENT Cushing
William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA
 The Year in Adrenal William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA Division of ENDOCRINOLOGY, DIABETES, METABOLISM & NUTRITION 2018 Mayo Foundation for Medical Education
The Year in Adrenal William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA Division of ENDOCRINOLOGY, DIABETES, METABOLISM & NUTRITION 2018 Mayo Foundation for Medical Education
Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypercortisolism
 Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypercortisolism Howard Sachs, MD Patients Course, 2017 Associate Professor of Clinical Medicine UMass Medical School Adrenal
Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypercortisolism Howard Sachs, MD Patients Course, 2017 Associate Professor of Clinical Medicine UMass Medical School Adrenal
Laura Stewart, MD, FRCPC Clinical Associate Professor Division of Pediatric Endocrinology University of British Columbia
 Precocious Puberty Laura Stewart, MD, FRCPC Clinical Associate Professor Division of Pediatric Endocrinology University of British Columbia Faculty Disclosure Faculty: Laura Stewart No relationships with
Precocious Puberty Laura Stewart, MD, FRCPC Clinical Associate Professor Division of Pediatric Endocrinology University of British Columbia Faculty Disclosure Faculty: Laura Stewart No relationships with
Audit of Adrenal Function Tests. Kate Davies Senior Lecturer in Children s Nursing London South Bank University London, UK
 Audit of Adrenal Function Tests Kate Davies Senior Lecturer in Children s Nursing London South Bank University London, UK Introduction Audit Overview of adrenal function tests Education Audit why? Explore
Audit of Adrenal Function Tests Kate Davies Senior Lecturer in Children s Nursing London South Bank University London, UK Introduction Audit Overview of adrenal function tests Education Audit why? Explore
BRIEF REPORT. Clinical Studies A (a selective b 3. In Vivo Studies
 BRIEF REPORT Brief Report PROPRANOLOL THERAPY FOR ECTOPIC b-adrenergic RECEPTORS IN ADRENAL CUSHING S SYNDROME ANDRÉ LACROIX, M.D., JOHANNE TREMBLAY, PH.D., GUY ROUSSEAU, PH.D., MICHEL BOUVIER, PH.D.,
BRIEF REPORT Brief Report PROPRANOLOL THERAPY FOR ECTOPIC b-adrenergic RECEPTORS IN ADRENAL CUSHING S SYNDROME ANDRÉ LACROIX, M.D., JOHANNE TREMBLAY, PH.D., GUY ROUSSEAU, PH.D., MICHEL BOUVIER, PH.D.,
Aldosterone-Producing Adrenocortical Carcinoma with Co-Secretion of Cortisol and Estradiol: A Case Report* Karen Lazaro and Perie Adorable-Wagan
 Case RePort Journal of the ASEAN Federation of Endocrine Societies with Co-Secretion of Cortisol and Estradiol: A Case Report* Karen Lazaro and Perie Adorable-Wagan Section of Endocrinology, Diabetes and
Case RePort Journal of the ASEAN Federation of Endocrine Societies with Co-Secretion of Cortisol and Estradiol: A Case Report* Karen Lazaro and Perie Adorable-Wagan Section of Endocrinology, Diabetes and
Index. F Fatigue, 59 Food-dependent Cushing s syndrome, 286
 A Abdominal red striae, 57, 58 Aberrant hormone receptors, AIMAH familial forms, 215 investigative protocols, 217 218 molecular mechanisms, 216, 217 paracrine mechanisms, 216 steroidogenesis, 212 213 in
A Abdominal red striae, 57, 58 Aberrant hormone receptors, AIMAH familial forms, 215 investigative protocols, 217 218 molecular mechanisms, 216, 217 paracrine mechanisms, 216 steroidogenesis, 212 213 in
Hypertension and Diabetes. Edward Shahady MD Medical Director Diabetes Master Clinician Program Florida Academy of Family Physicians
 Hypertension and Diabetes Edward Shahady MD Medical Director Diabetes Master Clinician Program Florida Academy of Family Physicians Objectives Describe the prevalence of hypertension and hypertension control
Hypertension and Diabetes Edward Shahady MD Medical Director Diabetes Master Clinician Program Florida Academy of Family Physicians Objectives Describe the prevalence of hypertension and hypertension control
Abnormal Responsiveness to Dexamethasone- Suppressed CRH Test in Patients With Bilateral Adrenal Incidentalomas
 ORIGINAL ARTICLE Abnormal Responsiveness to Dexamethasone- Suppressed CRH Test in Patients With Bilateral Adrenal Incidentalomas D. A. Vassiliadi, M. Tzanela, V. Tsatlidis, E. Margelou, M. Tampourlou,
ORIGINAL ARTICLE Abnormal Responsiveness to Dexamethasone- Suppressed CRH Test in Patients With Bilateral Adrenal Incidentalomas D. A. Vassiliadi, M. Tzanela, V. Tsatlidis, E. Margelou, M. Tampourlou,
Diagnostic Role of Captopril Challenge Test in Korean Subjects with High Aldosterone-to-Renin Ratios
 Original Article Endocrinol Metab 2016;31:277-283 http://dx.doi.org/10.3803/enm.2016.31.2.277 pissn 2093-596X eissn 2093-5978 Diagnostic Role of Captopril Challenge Test in Korean Subjects with High Aldosterone-to-Renin
Original Article Endocrinol Metab 2016;31:277-283 http://dx.doi.org/10.3803/enm.2016.31.2.277 pissn 2093-596X eissn 2093-5978 Diagnostic Role of Captopril Challenge Test in Korean Subjects with High Aldosterone-to-Renin
Adrenal gland Incidentaloma
 Adrenal gland Incidentaloma Topic review 17 sep 2008 Anatomy 1 Anatomical consideration Blood supply Artery: small branches from Inf. phrenic, renal artery and aorta Vein: Rt : medial aspect to IVC Lt
Adrenal gland Incidentaloma Topic review 17 sep 2008 Anatomy 1 Anatomical consideration Blood supply Artery: small branches from Inf. phrenic, renal artery and aorta Vein: Rt : medial aspect to IVC Lt
A Rare Case of Subclinical Primary Aldosteronism and Subclinical Cushing s Syndrome without Cardiovascular Complications
 Tokai J Exp Clin Med., Vol. 41, No. 1, pp. 35-41, 216 A Rare Case of Subclinical Primary Aldosteronism and Subclinical Cushing s Syndrome without Cardiovascular Complications Natsumi KITAJIMA *1, Toshiro
Tokai J Exp Clin Med., Vol. 41, No. 1, pp. 35-41, 216 A Rare Case of Subclinical Primary Aldosteronism and Subclinical Cushing s Syndrome without Cardiovascular Complications Natsumi KITAJIMA *1, Toshiro
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences. Endocrinology. (Review) Year 5 Internal Medicine
 Year 5 Internal Medicine") Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
Adrenocortical Scan. Quality Control. Adult Dose Range
 chapter 1 Adrenocortical Scan RADIOPHARMACY Radionuclide 131 I t 1/2 : 8.1 days Energies: 364 kev Type: β, γ, fission product Radiopharmaceutical 131 I-6-β-Iodomethyl-19-norcholesterol (NP-59). Available
chapter 1 Adrenocortical Scan RADIOPHARMACY Radionuclide 131 I t 1/2 : 8.1 days Energies: 364 kev Type: β, γ, fission product Radiopharmaceutical 131 I-6-β-Iodomethyl-19-norcholesterol (NP-59). Available
Endocrine System Hormones. AP Biology
 Endocrine System Hormones 2007-2008 Regulation Why are hormones needed? u chemical messages from one body part to another u communication needed to coordinate whole body u daily homeostasis & regulation
Endocrine System Hormones 2007-2008 Regulation Why are hormones needed? u chemical messages from one body part to another u communication needed to coordinate whole body u daily homeostasis & regulation
Checking the Right Box at the Right Age: the Art of Pediatric Endocrine Testing
 Checking the Right Box at the Right Age: the Art of Pediatric Endocrine Testing Jean-Pierre Chanoine, MD Endocrinology and Diabetes Unit British Columbia s Children s Hospital Objectives 1. Interpret the
Checking the Right Box at the Right Age: the Art of Pediatric Endocrine Testing Jean-Pierre Chanoine, MD Endocrinology and Diabetes Unit British Columbia s Children s Hospital Objectives 1. Interpret the
pharmacology sheet #9 Adrenal Steroids Mineral corticoids & Glucocorticoids
 Adrenal Steroids Mineral corticoids & Glucocorticoids Extra notes : Slide 2: - All Steroids are synthesized in the adrenal gland and secreted from it, It consists of an outer cortex and an inner medulla.
Adrenal Steroids Mineral corticoids & Glucocorticoids Extra notes : Slide 2: - All Steroids are synthesized in the adrenal gland and secreted from it, It consists of an outer cortex and an inner medulla.
Take Home Messages in Endocrinology
 Conflict of Interest/Disclosures Take Home Messages in Endocrinology None Carolyn Becker, MD 2 Diabetes Thyroid Pituitary Adrenal Hypoglycemia Overview Diagnostic Criteria for T2DM Diabetes should be diagnosed
Conflict of Interest/Disclosures Take Home Messages in Endocrinology None Carolyn Becker, MD 2 Diabetes Thyroid Pituitary Adrenal Hypoglycemia Overview Diagnostic Criteria for T2DM Diabetes should be diagnosed
Adrenal cortex I (biosynthesis of adrenal steroids; renin-angiotensin and glucocorticoid physiology)
") Adrenal cortex I (biosynthesis of adrenal steroids; renin-angiotensin and glucocorticoid physiology) Dr. Szathmári Miklós Semmelweis University First Department of Medicine 24. February 2014. The adrenal
Adrenal cortex I (biosynthesis of adrenal steroids; renin-angiotensin and glucocorticoid physiology) Dr. Szathmári Miklós Semmelweis University First Department of Medicine 24. February 2014. The adrenal
AN INDIVIDUALIZED APPROACH TO THE EVALUATION AND MANAGEMENT OF PRIMARY ALDOSTERONISM
 Review Article AN INDIVIDUALIZED APPROACH TO THE EVALUATION AND MANAGEMENT OF PRIMARY ALDOSTERONISM Anand Vaidya, MD, MMSc 1 ; Carl D. Malchoff, MD, PhD 2 ; Richard J. Auchus, MD, PhD 3 ; on behalf of
Review Article AN INDIVIDUALIZED APPROACH TO THE EVALUATION AND MANAGEMENT OF PRIMARY ALDOSTERONISM Anand Vaidya, MD, MMSc 1 ; Carl D. Malchoff, MD, PhD 2 ; Richard J. Auchus, MD, PhD 3 ; on behalf of
ComprehensivePLUS Hormone Profile with hgh
 OLEBound400: 801 SW 16th St Suite 126 Renton WA 98057 425.271.8689 425.271.8674 (Fax) ComprehensivePLUS Hormone Profile with hgh Doctor ID Patient Name 6206 Doe, Jane Age Sex Date of Birth 44 F Date Collected
OLEBound400: 801 SW 16th St Suite 126 Renton WA 98057 425.271.8689 425.271.8674 (Fax) ComprehensivePLUS Hormone Profile with hgh Doctor ID Patient Name 6206 Doe, Jane Age Sex Date of Birth 44 F Date Collected
Clinical Study Clinical Characteristics of Endogenous Cushing s Syndrome at a Medical Center in Southern Taiwan
 International Endocrinology Volume 2013, Article ID 685375, 7 pages http://dx.doi.org/10.1155/2013/685375 Clinical Study Clinical Characteristics of Endogenous Cushing s Syndrome at a Medical Center in
International Endocrinology Volume 2013, Article ID 685375, 7 pages http://dx.doi.org/10.1155/2013/685375 Clinical Study Clinical Characteristics of Endogenous Cushing s Syndrome at a Medical Center in
Diagnostic Accuracy of Adrenal Venous Sampling in Comparison with Other Parameters in Primary Aldosteronism
 Endocrine Journal 2008, 55 (5), 839 846 Diagnostic Accuracy of Adrenal Venous Sampling in Comparison with Other Parameters in Primary Aldosteronism ISAO MINAMI, TAKANOBU YOSHIMOTO, YUKI HIRONO, HAJIME
Endocrine Journal 2008, 55 (5), 839 846 Diagnostic Accuracy of Adrenal Venous Sampling in Comparison with Other Parameters in Primary Aldosteronism ISAO MINAMI, TAKANOBU YOSHIMOTO, YUKI HIRONO, HAJIME
Adrenal Incidentaloma Management
 Adrenal Incidentaloma Management Full Title of Guideline: Author Management of Incidentally-discovered Adrenal Lesions ( Incidentalomas ) Mr David Chadwick Consultant Endocrine Surgeon david.chadwick2@nuh.nhs.uk
Adrenal Incidentaloma Management Full Title of Guideline: Author Management of Incidentally-discovered Adrenal Lesions ( Incidentalomas ) Mr David Chadwick Consultant Endocrine Surgeon david.chadwick2@nuh.nhs.uk
Potassium, Aldosterone, and Hypertension: How Physiology Determines Treatment. Jamie Johnston, MD University of Pittsburgh School of Medicine
 Potassium, Aldosterone, and Hypertension: How Physiology Determines Treatment Jamie Johnston, MD University of Pittsburgh School of Medicine No Disclosures Acknowledgements: Evan Ray, MD, PhD Objectives
Potassium, Aldosterone, and Hypertension: How Physiology Determines Treatment Jamie Johnston, MD University of Pittsburgh School of Medicine No Disclosures Acknowledgements: Evan Ray, MD, PhD Objectives
Therapeutic Objectives. Cushing s Disease Surgical Results. Cushing s Disease Surgical Results: Macroadenomas 10/24/2015
 Therapeutic Objectives Update on the Management of Lewis S. Blevins, Jr., M.D. Correct the syndrome by lowering daily cortisol secretion to normal Eradicate any tumor that might threaten the health of
Therapeutic Objectives Update on the Management of Lewis S. Blevins, Jr., M.D. Correct the syndrome by lowering daily cortisol secretion to normal Eradicate any tumor that might threaten the health of
Endocrine System Hormones (Ch. 45)
") Endocrine System Hormones (Ch. 45) Regulation Why are hormones needed? chemical messages from one body part to another communication needed to coordinate whole body daily homeostasis & regulation of large
Endocrine System Hormones (Ch. 45) Regulation Why are hormones needed? chemical messages from one body part to another communication needed to coordinate whole body daily homeostasis & regulation of large
Clinical Guideline. SPEG MCN Protocols Sub Group SPEG Steering Group
 Clinical Guideline SECONDARY CARE MANAGEMENT OF SUSPECTED ADRENAL CRISIS IN CHILDREN AND YOUNG PEOPLE Date of First Issue 24/01/2015 Approved 28/09/2017 Current Issue Date 16/06/2017 Review Date 01/09/2019
Clinical Guideline SECONDARY CARE MANAGEMENT OF SUSPECTED ADRENAL CRISIS IN CHILDREN AND YOUNG PEOPLE Date of First Issue 24/01/2015 Approved 28/09/2017 Current Issue Date 16/06/2017 Review Date 01/09/2019
A Case of Primary Aldosteronism Due to Unilateral Adrenal Hyperplasia
 379 Case Report Hypertens Res Vol.28 (2005) No.4 p.379-384 A Case of Primary Aldosteronism Due to Unilateral Adrenal Hyperplasia Yasuyuki KATAYAMA, Nobuki TAKATA* 1, Taiji TAMURA* 2, Akemi YAMAMOTO, Fumihiko
379 Case Report Hypertens Res Vol.28 (2005) No.4 p.379-384 A Case of Primary Aldosteronism Due to Unilateral Adrenal Hyperplasia Yasuyuki KATAYAMA, Nobuki TAKATA* 1, Taiji TAMURA* 2, Akemi YAMAMOTO, Fumihiko