greater than 10 will be considered ill appearing; a score of 10 or less will be considered well appearing.
|
|
|
- Mavis Charles
- 6 years ago
- Views:
Transcription

1
2
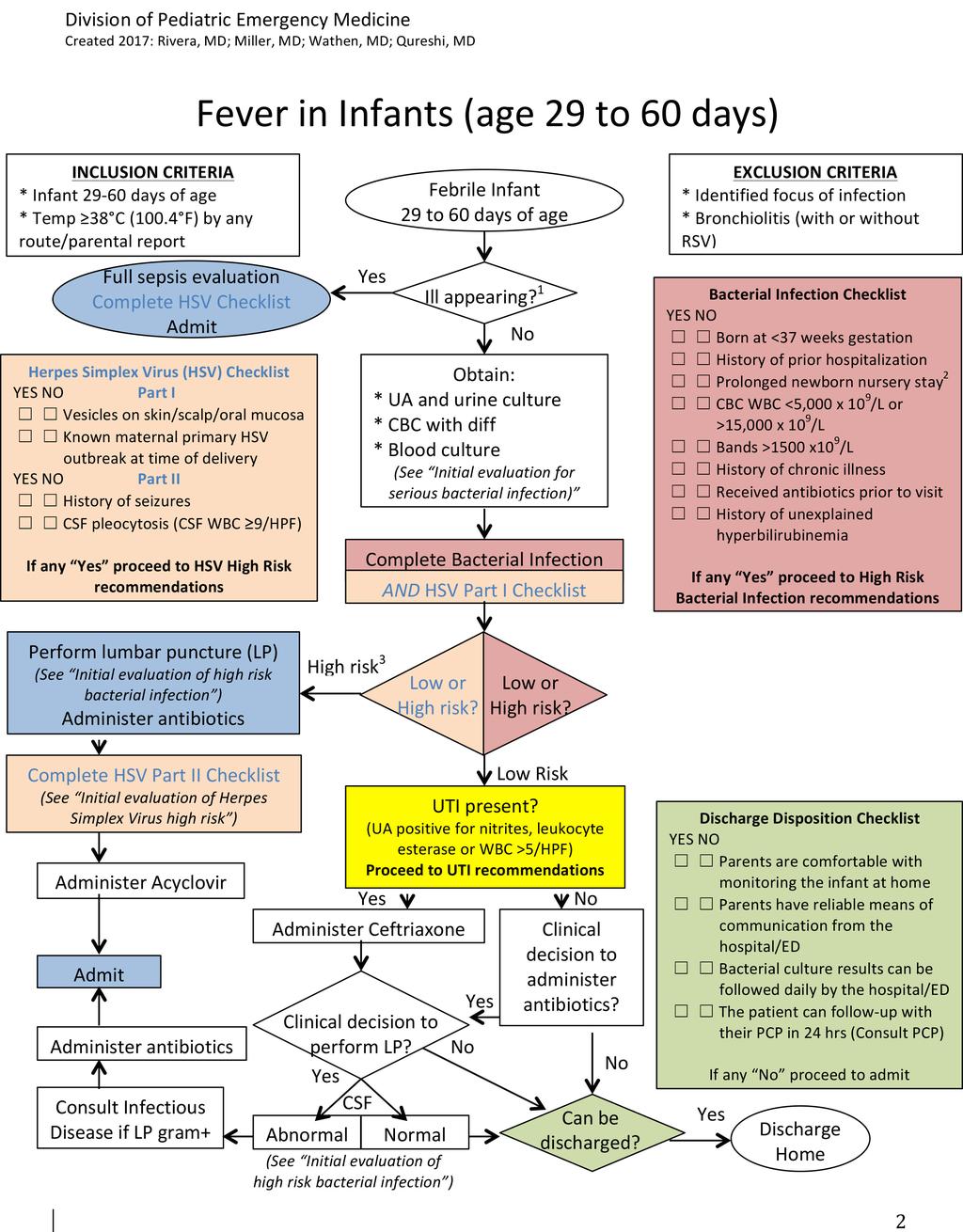
3 1 Use the Yale Observation Scale to assess whether the patient is ill or well appearing. A score greater than 10 will be considered ill appearing; a score of 10 or less will be considered well appearing. 2 Prolonged newborn nursery stay is defined as a hospital stay after birth longer that 48 hours for vaginal delivery or longer than 72 hours for cesarean delivery. 3 The category of High Risk should be awarded to infants with a yes response in either the Bacterial Infection Checklist OR Herpes Simplex Virus Part I Checklist. Fever in Infant Definition Fever is one of the most common reasons for emergency department (ED) evaluation of young infants. Because of an immature immune system, vaccine naivety, and exposure to unique pathogens in the perinatal period, the febrile young infant is at high risk for serious bacterial infection (SBI), such as urinary tract infection (UTI), bacteremia, and bacterial meningitis. Signs of a serious bacterial infection include cyanosis, poor peripheral circulation, petechial rash, and inconsolability. Up to 10% of infants 29 to 60 days of age who present with fever without an evident source of infection may have a bacterial infection. The prevalence of SBI among this age group is 10% for UTI, 2% for bacteremia and 1% for meningitis. Infants who present low risk factors have <5% risk for any bacterial infection and <0.5% for bacterial meningitis. For infants who are at low risk of Herpes Simplex Virus (HSV) infection, the estimated risk of HSV disease is <0.3%. Fever in Infant days Clinical Practice Guideline Application This guideline was developed for the evaluation and management of infants from 29 to 60 days of age who present with fever on exam or by history and without focus of infection. This guideline can also be applied to premature infants who were born at less than 37 weeks gestation, infants with prior history of hospitalization, prolonged newborn nursery course, or co- morbid conditions predisposing to severe or recurrent bacterial illness, including genetic, congenital, neuromuscular or neurodevelopmental abnormalities. This guideline does not apply to infants with a known focus of infection, clinical diagnosis of bronchiolitis with or without respiratory syncytial virus (RSV) infection, or age 28 days or 61 days old. Alternative Clinical Practice Guideline Considerations Febrile Neonate/ Fever in Infants 28 Days of Age Clinical Practice Guideline: Infants who are 28 days who present with fever by exam or history without an associated focus of infection. Bronchiolitis/ Wheezing in children <24 Months of Age Clinical Practice Guideline: Patients with signs and symptoms of viral lower respiratory tract infection, associated with rhinitis, cough, tachypnea, wheezing, rales, use of accessory muscles and/or nasal flaring; consistent with a clinical diagnosis of bronchiolitis. 3
4 Yale Observation Scale An observational scale consisting of 6 observational items originally characterized and clubbed by McCarthy et al. (Pediatrics 1982), and validated in young febrile children to detect a serious illness. An infant with a score greater than 10 is considered ill appearing; while a score of 10 or less is considered well appearing. Observation item Normal (Score=1) Moderate Impairment (Score=3) Severe Impairment (Score=5) 1. Quality of cry Strong with normal tone OR Content and not crying Whimpering OR Sobbing Weak OR Moaning OR High pitched 2. Reaction to parent stimulation Cries briefly then stops OR Content and not crying Cries off and on Continually cry OR Hardly responds 3. State variation If awake- > stays awake OR If asleep and stimulated - > wakes up quickly Eyes close briefly awakes up with prolonged stimulation Awake OR Falls to sleep OR Does not wake up 4. Color Pink Pale extremities OR Acrocyanosis Pale OR Cyanotic OR Mottled OR Ashen 5. Hydration Skin normal, eyes normal AND Mucous membranes moist Skin, eyes- normal AND Mouth slightly dry Skin doughy/tented AND Dry mucous membranes AND/OR Sunken eyes 6. Response (talk, smile) to social overtures Alerts Alerts briefly No alerting The observation item for response to social overtures (#6) was modified to present only the characteristics corresponding to infants less than 2 months of age. Initial evaluation of the febrile infant Serious bacterial UTI and bacteremia Infection recommendations High Risk Bacterial Infection Recommendations (See Bacterial Infection Checklist) Pneumonia Meningitis a. CBC with differential, b. Blood culture c. Urine analysis with microscopy d. Urine culture (catheter/suprapubic specimen) Order chest radiography only if any of the following are met: a. Presence of respiratory symptoms (nasal congestion with cough), OR b. Fever >102.2 F (39 C), OR c. WBC 20,000 x 10 9 /L Only for ill appearing infants (Yale score >10), infants at high risk of bacterial infection (See Bacterial Infection Checklist) and infants with a clinical decision to perform a lumbar puncture prior to antibiotic administration: a. Lumbar puncture (Cerebrospinal fluid (CSF) studies) i. Bacterial culture ii. Gram Stain (GS) iii. Cell count and differential iv. Protein v. Glucose 4
5 Herpes Simplex Virus (HSV) High Risk Recommendations (See Herpes Simplex Virus Checklist) Disseminated HSV infection and HSV encephalitis vi. Enterovirus PCR * If CSF pleocytosis (CSF WBC 9/HPF) is present, proceed to HSV High Risk recommendations. * If traumatic LP (RBC >10,000/HPF), treat as if CSF pleocytosis is present. a. BMP b. Liver function test (if CMP not done) c. HSV 1/2 serum PCR d. HSV PCR of any suspicious HSV lesion on the skin, eye and mouth e. Lumbar puncture (additional CSF studies) i. HSV 1/2 CSF PCR * Optional: HSV surface culture of conjunctiva, mouth and anus in viral culture media. Urinary Tract Infection (UTI) recommendations The management of UTI in febrile infants days is determined by the evaluating physician s clinical criteria. Infants who are at low risk of SBI, and who have been diagnosed with UTI, have <0.3% risk of bacterial meningitis. A lumbar puncture (LP) is not required. If a clinical decision to administer antibiotics is reached, a lumbar puncture can be performed with CSF gram stain, cell count, differential, protein, glucose, and bacterial culture, prior to antibiotic administration. If the CSF results are abnormal, the infant should be managed in accordance to high risk bacterial infection or HSV recommendations, as appropriate. If the clinical decision to NOT perform a lumbar puncture is reached, the infant may receive an initial IV/IM Ceftriaxone dose and be safely discharged home with oral Cefdinir if they meet discharge criteria. The decision to hospitalize and observe vs discharge home with close follow up in 24 hours should be made in conjunction with the parent(s)/caregiver(s), given than the infant may require a second dose of IV/IM Ceftriaxone. The results of bacterial cultures should be followed daily by the hospital or Emergency Department (ED). If a culture is found to be positive for bacterial infection, the infant should be called back to the ED. If an LP was not previously done, it may be done at this time and started on IV antibiotics. CSF culture after antibiotic therapy may yield negative results, but CSF cell count, differential, protein, and glucose will remain suggestive of bacterial meningitis. Infectious disease service may be consulted for further management recommendations, particularly in the presence of gram+ stain. The prevalence of adverse events or delayed SBI diagnosis in infants at low risk with diagnosis of UTI is 0.1%. Additional laboratory studies for consideration Type of infant Study Evaluation IF the infant presents fever and respiratory symptoms * Rapid RSV * Rapid Influenza * Respiratory viral panel * Presence of viral illness. Treatment considerations Clinical setting Medication Dose UTI first dose Ceftriaxone 50 mg/kg IV/IM Outpatient Cefdinir (250mg/5mL) 14mg/kg PO daily for 10 days 5
6 SBI Inpatient (High Risk Bacterial Infection Recommendations) Suspected meningitis (Unless LP shows gram- organism) HSV coverage Ampicillin AND EITHER Cefotaxime OR Ceftriaxone OR Gentamicin Vancomycin AND Ceftriaxone Acyclovir mg/kg IV/IM every 6 hours mg/kg IV/IM every 6 hours 50 mg/kg IV/IM every 12 hours 5mg/kg IV every 24 hours 15mg/kg IV every 6-8 hours 50 mg/kg IV/IM every 12 hours 20 mg/kg IV every 8 hours (HSV High risk recommendations) Ganciclovir (First line alternative therapy) 6 mg/ kg IV every 12 hours Alternative regimen to IV acyclovir should be considered when there is national shortage or depleted hospital supplies. In this setting, IV acyclovir should be reserved for neonates (infants 0-28 days) with any positives on the HSV checklist and/or proven HSV disease. Indications for disposition Disposition Criteria Discharge home a. Parents are comfortable with monitoring the infant at home b. Parents have reliable means of communication from the hospital/ Emergency Department (ED) c. Bacterial culture results can be followed daily by the hospital/ ED d. The patient can follow- up with their primary care physician (PCP) in 24 hrs (Consult PCP prior to discharge) Hospitalization a. Toxic/ill appearance b. Clinical signs of sepsis, like hypotension or poor capillary refill c. Confirmed SBI: meningitis, bacteremia d. Vomiting or inability to tolerate oral medication e. Lack of adequate outpatient follow- up (no telephone, parents live far from hospital, no PCP) f. Failure to respond to outpatient therapy Inpatient a. Infants should be admitted to the hospital for hours pending observation/ blood, CSF, and urine culture results, and viral testing (if done) discharge b. If respiratory virus or enterovirus testing is positive (if done), it is recommendations safe to discharge infants after 24 hours of negative CSF, blood, and urine cultures if discharge criteria are met c. If viral testing is negative (if done), it is safe to discharge well appearing infants after hours of negative CSF, blood, and urine cultures if discharge criteria are met d. Note that children who undergo HSV testing may need to be observed longer than 26 hours e. If HSV testing or any bacterial cultures grow a pathogen, treat appropriately f. High risk infants who do not meet discharge criteria should remain hospitalized until safe and adequate follow up can be provided in the outpatient setting 6
7 Goal and Metrics Document the use of the Yale Observation Scale to identify well appearing infants. Reduce length of hospitalization for infants who are hospitalized to <30 hours for infants who are low risk. Increase the percent of hospitalized infants who are hospitalized appropriately. Increase the percent of infants who have a UA performed via any method of collection on the first day of encounter. Decrease the percent of infants who get a CXR within 24 hours of presentation without documented respiratory symptoms. Increase use of recommended empiric antibiotic regimens within 24 hours of presentation. Increase use of recommended empiric antibiotic regimen within 90 minutes for infants at high risk for SBI or HSV. REFERENCES AAP SUBCOMMITTEE ON URINARY TRACT INFECTION. Reaffirmation of AAP Clinical Practice Guideline: The Diagnosis and Management of the Initial Urinary Tract Infection in Febrile Infants and Young Children 2 24 Months of Age. Pediatrics. 2016;138(6):e Bang A, Chaturvedi P. Yale Observation Scale for prediction of bacteremia in febrile children. Indian journal of pediatrics. 2009;76(6): Biondi E, Evans R, Mischler M, et al. Epidemiology of bacteremia in febrile infants in the United States. Pediatrics. 2013;132(6): Biondi EA, Mischler M, Jerardi KE, et al. Blood culture time to positivity in febrile infants with bacteremia. JAMA Pediatr. 2014;168(9): Byington CL, Reynolds CC, Korgenski K, et al. Costs and infant outcomes after implementation of a care process model for febrile infants. Pediatrics. 2012; 130(1):e Centers for Disease Control and Prevention (CDC). Trends in perinatal group B streptococcal disease: United States, MMWR Morb Mortal Wkly Rep. 2009;58(5): Dagan R, Sofer S, Phillip M, et al. Ambulatory care of febrile infants younger than 2 months of age classified as being at low risk for having serious bacterial infections. J Pediatr. 1988;112(3): Greenhow TL, Hung YY, Herz AM, et al. The changing epidemiology of serious bacterial infections in young infants. Pediatr Infect Dis J. 2014;33(6): Herr SM, Wald ER, Pitetti RD, et al. Enhanced urinalysis improves identification of febrile infants ages 60 days and younger at low risk for serious bacterial illness. Pediatrics. 2001;108(4): Huebner RE, Mbelle N, Forrest B, Madore DV, Klugman KP. Immunogenicity after one, two or three doses and impact on the antibody response to coadministered antigens of a nonavalent pneumococcal conjugate vaccine in infants of Soweto, South Africa. Pediatr Infect Dis J. 2002;21 (11):
8 Huppler AR, Eickhoff JC, Wald ER. Performance of low- risk criteria in the evaluation of young infants with fever: review of the literature. Pediatrics. 2010;125(2): Jaskiewicz JA, McCarthy CA, Richardson AC, et al. Febrile infants at low risk for serious bacterial infection an appraisal of the Rochester criteria and implications for management. Febrile Infant Collaborative Study Group. Pediatrics. 1994;94(3): Ishimine P. The evolving approach to the young child who has fever and no obvious source. Emerg Med Clin North Am. 2007;25(4): , vii. McCarthy PL, Lembo RM, Baron MA, Fink HD, Cicchetti DV. Predictive value of abnormal physical examination findings in ill- appearing and well- appearing febrile children. Pediatrics. 1985;76(2): McCarthy PL, Sharpe MR, Spiesel SZ, et al. Observation scales to identify serious illness in febrile children. Pediatrics 1982, 70: Westra SJ, et al. ACR Appropriateness Criteria Fever Without Source or Unknown Origin Child. Journal of the American College of Radiology. 2016, 13(8):
Fever in neonates (age 0 to 28 days)
") Fever in neonates (age 0 to 28 days) INCLUSION CRITERIA Infant 28 days of life Temperature 38 C (100.4 F) by any route/parental report EXCLUSION CRITERIA Infants with RSV Febrile Infant 28 days old Ill
Fever in neonates (age 0 to 28 days) INCLUSION CRITERIA Infant 28 days of life Temperature 38 C (100.4 F) by any route/parental report EXCLUSION CRITERIA Infants with RSV Febrile Infant 28 days old Ill
Fever in Young Infants 7 90 days of age
 Fever in Young Infants 7 90 days of age Derek Zhorne, MD Clinical Assistant Professor of Pediatrics Pediatric Hospitalist Disclosures I have no actual or potential conflicts in relation to this presentation.
Fever in Young Infants 7 90 days of age Derek Zhorne, MD Clinical Assistant Professor of Pediatrics Pediatric Hospitalist Disclosures I have no actual or potential conflicts in relation to this presentation.
Fever Without a Source Age: 0-28 Day Pathway - Emergency Department Evidence Based Outcome Center
 Age: 0-28 Day Pathway - Emergency Department EXCLUSION CRITERIA Toxic appearing No fever Born < 37 weeks gestational age INCLUSION CRITERIA Non-toxic with temperature > 38 C (100.4 F) < 36 C (96.5 F) measured
Age: 0-28 Day Pathway - Emergency Department EXCLUSION CRITERIA Toxic appearing No fever Born < 37 weeks gestational age INCLUSION CRITERIA Non-toxic with temperature > 38 C (100.4 F) < 36 C (96.5 F) measured
Beyond the Reflex Arc: An Evidence-Based Discussion of the Management of Febrile Infants
 Beyond the Reflex Arc: An Evidence-Based Discussion of the Management of Febrile Infants Cole Condra, MD MSc Division of Emergency Medical Services Children s Mercy Hospital October 1, 2011 Disclosure
Beyond the Reflex Arc: An Evidence-Based Discussion of the Management of Febrile Infants Cole Condra, MD MSc Division of Emergency Medical Services Children s Mercy Hospital October 1, 2011 Disclosure
The Febrile Infant. SJRH ED Rounds Dec By: Robin Clouston
 1 The Febrile Infant SJRH ED Rounds Dec 11 2018 By: Robin Clouston 2 Objectives Discuss the risk of serious bacterial infection (SBI) in the neonate or young infant (
1 The Febrile Infant SJRH ED Rounds Dec 11 2018 By: Robin Clouston 2 Objectives Discuss the risk of serious bacterial infection (SBI) in the neonate or young infant (
Fever in the Newborn Period
 Fever in the Newborn Period 1. Definitions 1 2. Overview 1 3. History and Physical Examination 2 4. Fever in Infants Less than 3 Months Old 2 a. Table 1: Rochester criteria for low risk infants 3 5. Fever
Fever in the Newborn Period 1. Definitions 1 2. Overview 1 3. History and Physical Examination 2 4. Fever in Infants Less than 3 Months Old 2 a. Table 1: Rochester criteria for low risk infants 3 5. Fever
Evaluating Fever in Infants. Derek Zhorne, MD Clinical Assistant Professor of Pediatrics Pediatric Hospitalist
 Evaluating Fever in Infants Derek Zhorne, MD Clinical Assistant Professor of Pediatrics Pediatric Hospitalist Disclosures I have no actual or potential conflicts in relation to this presentation. I will
Evaluating Fever in Infants Derek Zhorne, MD Clinical Assistant Professor of Pediatrics Pediatric Hospitalist Disclosures I have no actual or potential conflicts in relation to this presentation. I will
Faculty Disclosure. Stephen I. Pelton, MD. Dr. Pelton has listed no financial interest/arrangement that would be considered a conflict of interest.
 Faculty Disclosure Stephen I. Pelton, MD Dr. Pelton has listed no financial interest/arrangement that would be considered a conflict of interest. Advances in the management of fever in infants 0 to 3 and
Faculty Disclosure Stephen I. Pelton, MD Dr. Pelton has listed no financial interest/arrangement that would be considered a conflict of interest. Advances in the management of fever in infants 0 to 3 and
Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014
 Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014 Prep Question You are camping with a group of boys at a rural campground in the southeastern Unites States when one of the campers is bitten
Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014 Prep Question You are camping with a group of boys at a rural campground in the southeastern Unites States when one of the campers is bitten
EVALUATION OF A SICK CHILD WITH FEVER
 EVALUATION OF A SICK CHILD WITH FEVER Learning objectives At the conclusion of this learning activity, participants should be able to; Discuss the different etiologies of acute illness in a child Identify
EVALUATION OF A SICK CHILD WITH FEVER Learning objectives At the conclusion of this learning activity, participants should be able to; Discuss the different etiologies of acute illness in a child Identify
Fevers and Seizures in Infants and Young Children
 Fevers and Seizures in Infants and Young Children Kellie Holtmeier, PharmD Pediatric Clinical Pharmacist University of New Mexico Hospital Disclosure I have no conflicts of interest 1 Pharmacist Objectives
Fevers and Seizures in Infants and Young Children Kellie Holtmeier, PharmD Pediatric Clinical Pharmacist University of New Mexico Hospital Disclosure I have no conflicts of interest 1 Pharmacist Objectives
1. Introduction Algorithm: Infant with Fever 0-28 Days Algorithm: Infant with Fever Days...3
 These guidelines are designed to assist clinicians and are not intended to supplant good clinical judgement or to establish a protocol for all patients with this condition. MANAGEMENT OF FEVER 38 C (100.4F)
These guidelines are designed to assist clinicians and are not intended to supplant good clinical judgement or to establish a protocol for all patients with this condition. MANAGEMENT OF FEVER 38 C (100.4F)
EPG Clinical Guidelines
 Guidelines for the Management of Febrile Young Children Neonate age 7 days Temperature > 38 C, documented at home or in the ED Complete blood count with manual differential (CBCD), urinalysis (UA), urine
Guidelines for the Management of Febrile Young Children Neonate age 7 days Temperature > 38 C, documented at home or in the ED Complete blood count with manual differential (CBCD), urinalysis (UA), urine
Evidence-based Management of Fever in Infants and Young Children
 Evidence-based Management of Fever in Infants and Young Children Shabnam Jain, MD, MPH Associate Professor of Pediatrics Emory University Medical Director for Clinical Effectiveness Objectives Understand
Evidence-based Management of Fever in Infants and Young Children Shabnam Jain, MD, MPH Associate Professor of Pediatrics Emory University Medical Director for Clinical Effectiveness Objectives Understand
Hot Hot Tot:! The Hot Tot. Fever in KIds <90 Days 5/26/10
 Hot Hot Tot:! Fever in KIds
Hot Hot Tot:! Fever in KIds
Rational Evaluation of the Febrile Infant
 Disclosures Rational Evaluation of the Febrile Infant Samir S. Shah, MD, MSCE Professor, Department of Pediatrics University of Cincinnati College of Medicine Director, Division of Hospital Medicine Attending
Disclosures Rational Evaluation of the Febrile Infant Samir S. Shah, MD, MSCE Professor, Department of Pediatrics University of Cincinnati College of Medicine Director, Division of Hospital Medicine Attending
+ Objectives. n Define who is at risk for SBI. n Clarify risk stratification. n Provide treatment guidelines. n Bust some myths
 Objectives n Define wo is at risk for SBI n Clarify risk stratification n Provide treatment guidelines Neonatal Fever Benjamin B. Constance, MD, FAWM n Bust some myts Based on Case wat do you want to know?
Objectives n Define wo is at risk for SBI n Clarify risk stratification n Provide treatment guidelines Neonatal Fever Benjamin B. Constance, MD, FAWM n Bust some myts Based on Case wat do you want to know?
ENCEPHALITIS. Diana Montoya Melo
 ENCEPHALITIS Diana Montoya Melo 4 yo female patient, brought to the ED after having a GTC seizure 30 mins ago, which lasted up to a min. Mom reports that he has a ho 3 days of fever and runny nose, associated
ENCEPHALITIS Diana Montoya Melo 4 yo female patient, brought to the ED after having a GTC seizure 30 mins ago, which lasted up to a min. Mom reports that he has a ho 3 days of fever and runny nose, associated
Disclosures. Background. Definitions. Why Worry about these Infants? Goals. Bacterial infection in the neonate and young infant: a review
 Disclosures Bacterial infection in the neonate and young infant: a review Russell J. McCulloh, MD Med-Peds Infectious Diseases August 8, 2017 I have no financial interests to disclose Funding: Eva and
Disclosures Bacterial infection in the neonate and young infant: a review Russell J. McCulloh, MD Med-Peds Infectious Diseases August 8, 2017 I have no financial interests to disclose Funding: Eva and
4/14/2010. Theoretical purpose of fever? Andrea Marmor, MD, MSEd Assistant Clinical Professor, Pediatrics UCSF April 13, 2010
 Andrea Marmor, MD, MSEd Assistant Clinical Professor, Pediatrics UCSF April 13, 2010 Parental touch? Absence of fever more reliable than presence. Axillary and tympanic Vulnerable to environmental and
Andrea Marmor, MD, MSEd Assistant Clinical Professor, Pediatrics UCSF April 13, 2010 Parental touch? Absence of fever more reliable than presence. Axillary and tympanic Vulnerable to environmental and
Fever in Infants: Pediatric Dilemmas in Antibiotherapy
 Fever in Infants: Pediatric Dilemmas in Antibiotherapy Jahzel M. Gonzalez Pagan, MD, FAAP Pediatric Emergency Medicine Associate Professor, UPH Medical Advisor, SJCH June 9 th, 2017 S Objectives S Review
Fever in Infants: Pediatric Dilemmas in Antibiotherapy Jahzel M. Gonzalez Pagan, MD, FAAP Pediatric Emergency Medicine Associate Professor, UPH Medical Advisor, SJCH June 9 th, 2017 S Objectives S Review
 Fever Phobia and the ED Doc Ran Goldman, MD (rgoldman@cw.bc.ca) BC Children s Hospital, Professor, University of British Columbia SLIDES ON : www.clinicalpeds.com/whistler Define Fever 38.0 o Doesn t
Fever Phobia and the ED Doc Ran Goldman, MD (rgoldman@cw.bc.ca) BC Children s Hospital, Professor, University of British Columbia SLIDES ON : www.clinicalpeds.com/whistler Define Fever 38.0 o Doesn t
Fever in Babies. Too much testing or not enough testing? Martin E. Weisse, M.D. Pediatric Infectious Diseases
 Fever in Babies Too much testing or not enough testing? Martin E. Weisse, M.D. Pediatric Infectious Diseases Disclosures I have nothing to disclose Learning Objectives At the end of the talk, participants
Fever in Babies Too much testing or not enough testing? Martin E. Weisse, M.D. Pediatric Infectious Diseases Disclosures I have nothing to disclose Learning Objectives At the end of the talk, participants
PEDIATRIC INFECTIOUS DISEASES UPDATE. Neonatal HSV. Recognition, Diagnosis, and Management Coleen Cunningham MD
 Neonatal HSV Recognition, Diagnosis, and Management Coleen Cunningham MD Important questions Who is at risk? When do you test? What tests do you perform? When do you treat? What is appropriate therapy?
Neonatal HSV Recognition, Diagnosis, and Management Coleen Cunningham MD Important questions Who is at risk? When do you test? What tests do you perform? When do you treat? What is appropriate therapy?
FEVER. What is fever?
 FEVER What is fever? Fever is defined as a rectal temperature 38 C (100.4 F), and a value >40 C (104 F) is called hyperpyrexia. Body temperature fluctuates in a defined normal range (36.6-37.9 C [97.9-100.2
FEVER What is fever? Fever is defined as a rectal temperature 38 C (100.4 F), and a value >40 C (104 F) is called hyperpyrexia. Body temperature fluctuates in a defined normal range (36.6-37.9 C [97.9-100.2
Judith Klein, MD 2011 FEVER IN THE FIRST 36 MONTHS OF LIFE
 Judith Klein, MD 2011 FEVER IN THE FIRST 36 MONTHS OF LIFE Objectives A short history of the kiddie fever business Vaccinations Rapid viral testing Biomarkers Month-by-month approach to fevers in these
Judith Klein, MD 2011 FEVER IN THE FIRST 36 MONTHS OF LIFE Objectives A short history of the kiddie fever business Vaccinations Rapid viral testing Biomarkers Month-by-month approach to fevers in these
Estimating RSV Disease Burden in the United States
 Estimating RSV Disease Burden in the United States Brian Rha, MD, MSPH Medical Epidemiologist, Division of Viral Diseases Centers for Disease Control and Prevention Severe Acute Respiratory Infection Surveillance
Estimating RSV Disease Burden in the United States Brian Rha, MD, MSPH Medical Epidemiologist, Division of Viral Diseases Centers for Disease Control and Prevention Severe Acute Respiratory Infection Surveillance
Fever. National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital
 Fever National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital Case 1 4-month-old well-appearing girl admitted for croup and respiratory distress.
Fever National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital Case 1 4-month-old well-appearing girl admitted for croup and respiratory distress.
Community Acquired Pneumonia
 April 2014 References: 1. Bradley JS, Byington CL, Shah SS, Alverson B, Carter ER, Harrison C, Kaplan SL Mace SE, McCracken Jr. GH, Moor MR, St. Peter SD, Stockwell JA, and Swanson JT. The Management of
April 2014 References: 1. Bradley JS, Byington CL, Shah SS, Alverson B, Carter ER, Harrison C, Kaplan SL Mace SE, McCracken Jr. GH, Moor MR, St. Peter SD, Stockwell JA, and Swanson JT. The Management of
Feverish illness: assessment and initial management in children younger than 5 years of age
 Feverish illness: assessment and initial management in children younger than 5 years of age NICE guideline Draft for consultation, November, 2006 If you wish to comment on this version of the guideline,
Feverish illness: assessment and initial management in children younger than 5 years of age NICE guideline Draft for consultation, November, 2006 If you wish to comment on this version of the guideline,
The McMaster at night Pediatric Curriculum
 The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
GUIDELINE FOR THE MANAGEMENT OF MENINGITIS. All children with suspected or confirmed meningitis
 GUIDELINE FOR THE MANAGEMENT OF MENINGITIS Reference: Mennigitis Version No: 1 Applicable to All children with suspected or confirmed meningitis Classification of document: Area for Circulation: Author:
GUIDELINE FOR THE MANAGEMENT OF MENINGITIS Reference: Mennigitis Version No: 1 Applicable to All children with suspected or confirmed meningitis Classification of document: Area for Circulation: Author:
Fever in children aged less than 5 years
 Fever in children aged less than 5 years A fever is defined as a temperature greater than 38 degrees celsius Height and duration of fever do not identify serious illness. However fever in children younger
Fever in children aged less than 5 years A fever is defined as a temperature greater than 38 degrees celsius Height and duration of fever do not identify serious illness. However fever in children younger
Antibiotic Protocols for Paediatrics Steve Biko Academic Hospital
 Antibiotic Protocols for Paediatrics Steve Biko Academic Hospital Respiratory tract infections in children Uncomplicated URTI A child with a cold should not receive an antibiotic Paracetamol (15 mg/kg/dose
Antibiotic Protocols for Paediatrics Steve Biko Academic Hospital Respiratory tract infections in children Uncomplicated URTI A child with a cold should not receive an antibiotic Paracetamol (15 mg/kg/dose
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
Dr. Bob Wilson Golden BC
 Fever in Infants Under 3 Mon. Dr. Bob Wilson Golden BC What is the risk of serious bacterial infection in a febrile 2 A. 5% B. 10% C. 25% D. 50% E. 100% month old infant? What is the most common congenital
Fever in Infants Under 3 Mon. Dr. Bob Wilson Golden BC What is the risk of serious bacterial infection in a febrile 2 A. 5% B. 10% C. 25% D. 50% E. 100% month old infant? What is the most common congenital
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A AAP. See American Academy of Pediatrics (AAP) Acyclovir dosing in infants, 185 187 American Academy of Pediatrics (AAP) COFN of, 199 204 Amphotericin
Note: Page numbers of article titles are in boldface type. A AAP. See American Academy of Pediatrics (AAP) Acyclovir dosing in infants, 185 187 American Academy of Pediatrics (AAP) COFN of, 199 204 Amphotericin
PNEUMONIA IN CHILDREN. IAP UG Teaching slides
 PNEUMONIA IN CHILDREN 1 INTRODUCTION 156 million new episodes / yr. worldwide 151 million episodes developing world 95% in developing countries 19% of all deaths in children
PNEUMONIA IN CHILDREN 1 INTRODUCTION 156 million new episodes / yr. worldwide 151 million episodes developing world 95% in developing countries 19% of all deaths in children
The Child with HIV and a Fever 1
 The Child with HIV and a Fever 1 Author: Andrew Riordan Amanda Williams Date of preparation: August 2003 Date reviewed: February 2012 Next review date: February 2014 Contents 1. Introduction 2. HIV disease
The Child with HIV and a Fever 1 Author: Andrew Riordan Amanda Williams Date of preparation: August 2003 Date reviewed: February 2012 Next review date: February 2014 Contents 1. Introduction 2. HIV disease
Your first patient of the day
 Your first patient of the day 1 month old male with 2 days of fussiness Decreased stool output for 3 days Poor latch during breastfeeding noted at 3AM on day of arrival to the ED Started spitting up later
Your first patient of the day 1 month old male with 2 days of fussiness Decreased stool output for 3 days Poor latch during breastfeeding noted at 3AM on day of arrival to the ED Started spitting up later
NICE guideline Published: 13 July 2016 nice.org.uk/guidance/ng51
 Sepsis: recognition, diagnosis and early management NICE guideline Published: 13 July 2016 nice.org.uk/guidance/ng51 NICE 2016. All rights reserved. Last updated July 2016 Your responsibility The recommendations
Sepsis: recognition, diagnosis and early management NICE guideline Published: 13 July 2016 nice.org.uk/guidance/ng51 NICE 2016. All rights reserved. Last updated July 2016 Your responsibility The recommendations
BRONCHIOLITIS PEDIATRIC
 DEFINITION Bronchiolitis is typically defined as the first episode of wheezing in infants < 24 months of age. It is a viral illness of the lower respiratory tract that causes tachypnea, bronchospasm, and
DEFINITION Bronchiolitis is typically defined as the first episode of wheezing in infants < 24 months of age. It is a viral illness of the lower respiratory tract that causes tachypnea, bronchospasm, and
MICROBIOLOGICAL TESTING IN PICU
 MICROBIOLOGICAL TESTING IN PICU This is a guideline for the taking of microbiological samples in PICU to diagnose or exclude infection. The diagnosis of infection requires: Ruling out non-infectious causes
MICROBIOLOGICAL TESTING IN PICU This is a guideline for the taking of microbiological samples in PICU to diagnose or exclude infection. The diagnosis of infection requires: Ruling out non-infectious causes
Guidelines/Guidance/CAP/ Hospitalized Child. PHM Boot Camp 2014 Jay Tureen, MD June 19, 2014
 Guidelines/Guidance/CAP/ Hospitalized Child PHM Boot Camp 2014 Jay Tureen, MD June 19, 2014 CAP in Children: Epi Greatest cause of death in children worldwide Estimated > 2 M deaths in children In developed
Guidelines/Guidance/CAP/ Hospitalized Child PHM Boot Camp 2014 Jay Tureen, MD June 19, 2014 CAP in Children: Epi Greatest cause of death in children worldwide Estimated > 2 M deaths in children In developed
11/9/2012. Group B Streptococcal Infections: Consensus and Controversies. Prevention of Early-Onset GBS Disease in the USA.
 Group B Streptococcal Infections: Consensus and Controversies Carol J. Baker, M.D. Professor of Pediatrics, Molecular Virology and Microbiology Executive Director, Center for Vaccine Awareness and Research
Group B Streptococcal Infections: Consensus and Controversies Carol J. Baker, M.D. Professor of Pediatrics, Molecular Virology and Microbiology Executive Director, Center for Vaccine Awareness and Research
IDPH ESF-8 Plan: Pediatric and Neonatal Surge Annex Sample Pediatric Admission Orders 2015
 Purpose: To provide guidance to practitioners caring for pediatric patients who need inpatient hospital care during a disaster. Disclaimer: This guideline is not meant to be all inclusive, replace an existing
Purpose: To provide guidance to practitioners caring for pediatric patients who need inpatient hospital care during a disaster. Disclaimer: This guideline is not meant to be all inclusive, replace an existing
All About RSV (Respiratory Syncytial Virus)
") All About RSV (Respiratory Syncytial Virus) A Guide for Parents What is RSV? RSV stands for respiratory syncytial virus, the most frequent cause of serious respiratory tract infections in infants and children
All About RSV (Respiratory Syncytial Virus) A Guide for Parents What is RSV? RSV stands for respiratory syncytial virus, the most frequent cause of serious respiratory tract infections in infants and children
Urinary tract infection. Mohamed Ahmed Fouad Lecturer of pediatrics Jazan faculty of medicine
 Urinary tract infection Mohamed Ahmed Fouad Lecturer of pediatrics Jazan faculty of medicine Objectives To differentiate between types of urinary tract infections To recognize the epidemiology of UTI in
Urinary tract infection Mohamed Ahmed Fouad Lecturer of pediatrics Jazan faculty of medicine Objectives To differentiate between types of urinary tract infections To recognize the epidemiology of UTI in
Reviewing the recent literature to answer clinical questions: Should I change my practice?
 Reviewing the recent literature to answer clinical questions: Should I change my practice? JILL MILLER, MD PEM ATTENDING CHKD ASSISTANT PROFESSOR PEDIATRICS, EVMS Objectives Review the literature to answer
Reviewing the recent literature to answer clinical questions: Should I change my practice? JILL MILLER, MD PEM ATTENDING CHKD ASSISTANT PROFESSOR PEDIATRICS, EVMS Objectives Review the literature to answer
CNS Infections. Philip Gothard Consultant in Infectious Diseases Hospital for Tropical Diseases, London. Hammersmith Acute Medicine 2011
 CNS Infections Philip Gothard Consultant in Infectious Diseases Hospital for Tropical Diseases, London Hammersmith Acute Medicine 2011 Case 1 HISTORY 27y man Unwell 3 days Fever Headache Photophobia Previously
CNS Infections Philip Gothard Consultant in Infectious Diseases Hospital for Tropical Diseases, London Hammersmith Acute Medicine 2011 Case 1 HISTORY 27y man Unwell 3 days Fever Headache Photophobia Previously
Blue Babies, Twitchy Toddlers, and Kool Kids. By Beth Paton, MSN, RN, PNP, CEN, CPEN, FAEN
 Blue Babies, Twitchy Toddlers, and Kool Kids By Beth Paton, MSN, RN, PNP, CEN, CPEN, FAEN I have no disclosures OBJECTIVES By the end of this presentation, the learner will Discuss etiologies of cyanosis
Blue Babies, Twitchy Toddlers, and Kool Kids By Beth Paton, MSN, RN, PNP, CEN, CPEN, FAEN I have no disclosures OBJECTIVES By the end of this presentation, the learner will Discuss etiologies of cyanosis
Objectives. Pneumonia. Pneumonia. Epidemiology. Prevalence 1/7/2012. Community-Acquired Pneumonia in infants and children
 Objectives Community-Acquired in infants and children Review of Clinical Practice Guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America - 2011 Sabah Charania,
Objectives Community-Acquired in infants and children Review of Clinical Practice Guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America - 2011 Sabah Charania,
Emergency Neurological Life Support Meningitis and Encephalitis
 Emergency Neurological Life Support Meningitis and Encephalitis Version: 2.0 Last Updated: 19-Mar-2016 Checklist & Communication Meningitis and Encephalitis Table of Contents Emergency Neurological Life
Emergency Neurological Life Support Meningitis and Encephalitis Version: 2.0 Last Updated: 19-Mar-2016 Checklist & Communication Meningitis and Encephalitis Table of Contents Emergency Neurological Life
CASE-BASED SMALL GROUP DISCUSSION MHD II
 MHD II, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II Session 11 April 11, 2016 STUDENT COPY MHD II, Session 11, Student Copy Page 2 CASE HISTORY 1 Chief complaint: Our baby
MHD II, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II Session 11 April 11, 2016 STUDENT COPY MHD II, Session 11, Student Copy Page 2 CASE HISTORY 1 Chief complaint: Our baby
DENISE K. SUR, MD, and ELISE L. BUKONT, DO, University of California, Los Angeles, Los Angeles, California. a complete physical examination,
 Evaluating Fever of Unidentifiable Source in Young Children DENISE K. SUR, MD, and ELISE L. BUKONT, DO, University of California, Los Angeles, Los Angeles, California Most children will have been evaluated
Evaluating Fever of Unidentifiable Source in Young Children DENISE K. SUR, MD, and ELISE L. BUKONT, DO, University of California, Los Angeles, Los Angeles, California Most children will have been evaluated
Appropriate Antibiotic Prescribing. Frank Romanelli, Pharm.D., MPH, AAHIVP Professor & Associate Dean Paul F. Parker Endowed Professor of Pharmacy
 Appropriate Antibiotic Prescribing Frank Romanelli, Pharm.D., MPH, AAHIVP Professor & Associate Dean Paul F. Parker Endowed Professor of Pharmacy Objectives Discuss CDCs Core Elements of abx stewardship.
Appropriate Antibiotic Prescribing Frank Romanelli, Pharm.D., MPH, AAHIVP Professor & Associate Dean Paul F. Parker Endowed Professor of Pharmacy Objectives Discuss CDCs Core Elements of abx stewardship.
Pediatric Respiratory Infections
 Pediatric Respiratory Infections Brenda Kelly PharmD BCPS Residency Program Director Virginia Mason Memorial, Yakima, Washington brendakelly@yvmh.org Disclosure The presenter has no actual or potential
Pediatric Respiratory Infections Brenda Kelly PharmD BCPS Residency Program Director Virginia Mason Memorial, Yakima, Washington brendakelly@yvmh.org Disclosure The presenter has no actual or potential
USAID Health Care Improvement Project. pneumonia) respiratory infections through improved case management (amb/hosp)
 respiratory infections through improved case management (amb/hosp)") Improvement objective: : decrease morbidity and mortality due to acute upper (rhinitis, sinusitis, pharyngitis) and lower (bronchitis, pneumonia) respiratory infections through improved case management
Improvement objective: : decrease morbidity and mortality due to acute upper (rhinitis, sinusitis, pharyngitis) and lower (bronchitis, pneumonia) respiratory infections through improved case management
Dilemmas in the Management of Meningitis & Encephalitis HEADACHE AND FEVER. What is the best initial approach for fever, headache, meningisums?
 Dilemmas in the Management of Meningitis & Encephalitis Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine HEADACHE AND FEVER What is the best initial approach for fever,
Dilemmas in the Management of Meningitis & Encephalitis Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine HEADACHE AND FEVER What is the best initial approach for fever,
ANTIBIOTIC GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED MENINGITIS AND ENCEPHALITIS IN ADULTS
 ANTIBIOTIC GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED MENINGITIS AND ENCEPHALITIS IN ADULTS Version 4.0 Date ratified February 2009 Review date February 2011 Ratified by Authors Consultation Evidence
ANTIBIOTIC GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED MENINGITIS AND ENCEPHALITIS IN ADULTS Version 4.0 Date ratified February 2009 Review date February 2011 Ratified by Authors Consultation Evidence
Consulted With Post/Committee/Group Date Melanie Chambers Lead Nurse Children and young people March 2016 Andrea Stanley
 Feverish illness in children: Assessment and initial management in children younger than 5 years CLINICAL GUIDELINES Register no: 10043 Status: Public Developed in response to: Update and improve practice
Feverish illness in children: Assessment and initial management in children younger than 5 years CLINICAL GUIDELINES Register no: 10043 Status: Public Developed in response to: Update and improve practice
PEDIATRIC INFLUENZA CLINICAL PRACTICE GUIDELINES
 PEDIATRIC INFLUENZA CLINICAL PRACTICE GUIDELINES DEFINITIONS AND BACKGROUND Uncomplicated influenza illness is characterized by the abrupt onset of constitutional and respiratory signs and symptoms. Signs
PEDIATRIC INFLUENZA CLINICAL PRACTICE GUIDELINES DEFINITIONS AND BACKGROUND Uncomplicated influenza illness is characterized by the abrupt onset of constitutional and respiratory signs and symptoms. Signs
Group B Streptococcus
 Group B Streptococcus (Invasive Disease) Infants Younger than 90 Days Old DISEASE REPORTABLE WITHIN 24 HOURS OF DIAGNOSIS Per N.J.A.C. 8:57, healthcare providers and administrators shall report by mail
Group B Streptococcus (Invasive Disease) Infants Younger than 90 Days Old DISEASE REPORTABLE WITHIN 24 HOURS OF DIAGNOSIS Per N.J.A.C. 8:57, healthcare providers and administrators shall report by mail
Turkish Thoracic Society
 Türk Toraks Derneği Turkish Thoracic Society Pocket Books Series Diagnosis and Treatment of Community Acquired Pneumonia in Children Short Version (Handbook) in English www.toraks.org.tr This report was
Türk Toraks Derneği Turkish Thoracic Society Pocket Books Series Diagnosis and Treatment of Community Acquired Pneumonia in Children Short Version (Handbook) in English www.toraks.org.tr This report was
CHAPTER 167 Pediatric Fever
 CHAPTER 167 Pediatric Fever Nathan W. Mick Fever is the most common chief complaint of pediatric patients presenting to the emergency department (ED), accounting for up to 20% of ED visits. Most cases
CHAPTER 167 Pediatric Fever Nathan W. Mick Fever is the most common chief complaint of pediatric patients presenting to the emergency department (ED), accounting for up to 20% of ED visits. Most cases
Kidz Medical Services Infant Exposed to Genital Herpes Simplex Virus
 Kidz Medical Services Infant Exposed to Genital Herpes Simplex Virus Guideline: HSV Guideline: I. Herpes Simplex Virus (HSV): A. HSV is an enveloped, double-stranded DNA virus that enters the body via
Kidz Medical Services Infant Exposed to Genital Herpes Simplex Virus Guideline: HSV Guideline: I. Herpes Simplex Virus (HSV): A. HSV is an enveloped, double-stranded DNA virus that enters the body via
Rebecca T Slagle, MN, APRN, NNP-BC. Speak up!!
 Rebecca T Slagle, MN, APRN, NNP-BC Speak up!! Objectives: Understand the incidence and prevalence of sepsis in the newborn period Identify the risk factors for neonatal sepsis List the most frequent causative
Rebecca T Slagle, MN, APRN, NNP-BC Speak up!! Objectives: Understand the incidence and prevalence of sepsis in the newborn period Identify the risk factors for neonatal sepsis List the most frequent causative
RESEARCH ARTICLE ABSTRACT
 RESEARCH ARTICLE Evaluating the Impact of Implementing a Clinical Practice Guideline for Febrile Infants With Positive Respiratory Syncytial Virus or Enterovirus Testing Adrienne DePorre, MD, a David D.
RESEARCH ARTICLE Evaluating the Impact of Implementing a Clinical Practice Guideline for Febrile Infants With Positive Respiratory Syncytial Virus or Enterovirus Testing Adrienne DePorre, MD, a David D.
Vinita Rane Supervisor: Maryza Graham
 Old bug, new tricks Vinita Rane Supervisor: Maryza Graham 6 week old female Initial presentation (outside Monash): Unwell since 3/52 old Cough, associated with cyanotic episodes Coryza Lethargy Vomiting
Old bug, new tricks Vinita Rane Supervisor: Maryza Graham 6 week old female Initial presentation (outside Monash): Unwell since 3/52 old Cough, associated with cyanotic episodes Coryza Lethargy Vomiting
Charles Krasner, M.D. University of NV, Reno School of Medicine Sierra NV Veterans Affairs Medical Center
 Charles Krasner, M.D. University of NV, Reno School of Medicine Sierra NV Veterans Affairs Medical Center Kathy Peters is a 63 y.o. patient that presents to your urgent care office today with a history
Charles Krasner, M.D. University of NV, Reno School of Medicine Sierra NV Veterans Affairs Medical Center Kathy Peters is a 63 y.o. patient that presents to your urgent care office today with a history
enter the room. Persons immune from previous varicella infection may enter the room without a mask. Those immune by adenoviruses, influenza viruses.
 All clients admitted to the hospital automatically are considered to be on standard precautions. The diseases listed below require standard precautions plus additional precautions that are noted in the
All clients admitted to the hospital automatically are considered to be on standard precautions. The diseases listed below require standard precautions plus additional precautions that are noted in the
Infection Screening for Newborn Babies
 Infection Screening for Newborn Babies Patient Information Leaflet If you require a translation or an alternative format of this leaflet please speak to the nurse in charge or call the Patient Advice Liaison
Infection Screening for Newborn Babies Patient Information Leaflet If you require a translation or an alternative format of this leaflet please speak to the nurse in charge or call the Patient Advice Liaison
Fever in the Pediatric Patient (part one)
") Fever in the Pediatric Patient (part one) Heather Wolfe, MD, FAAP Medical Director, Lutheran Children s Hospital Medical Education Participant Objectives: 1. Discuss pediatric fever and the concept of
Fever in the Pediatric Patient (part one) Heather Wolfe, MD, FAAP Medical Director, Lutheran Children s Hospital Medical Education Participant Objectives: 1. Discuss pediatric fever and the concept of
Critical Review Form Clinical Prediction or Decision Rule
 Critical Review Form Clinical Prediction or Decision Rule Development and Validation of a Multivariable Predictive Model to Distinguish Bacterial from Aseptic Meningitis in Children, Pediatrics 2002; 110:
Critical Review Form Clinical Prediction or Decision Rule Development and Validation of a Multivariable Predictive Model to Distinguish Bacterial from Aseptic Meningitis in Children, Pediatrics 2002; 110:
Diagnosing and managing sepsis in children
 Diagnosing and managing sepsis in children Hague R. Diagnosing and managing sepsis in children. Practitioner Jan 2018;262(1811):21-25 Dr Rosie Hague MD MRCP FRCPCH Consultant in Infectious Diseases and
Diagnosing and managing sepsis in children Hague R. Diagnosing and managing sepsis in children. Practitioner Jan 2018;262(1811):21-25 Dr Rosie Hague MD MRCP FRCPCH Consultant in Infectious Diseases and
abstract ARTICLE BACKGROUND: There is considerable variation in the approach to infants presenting to the
 Management and Outcomes of Previously Healthy, Full-Term, Febrile Infants Ages 7 to 90 Days Tara L. Greenhow, MD, a Yun-Yi Hung, PhD, b Robert H. Pantell, MD c BACKGROUND: There is considerable variation
Management and Outcomes of Previously Healthy, Full-Term, Febrile Infants Ages 7 to 90 Days Tara L. Greenhow, MD, a Yun-Yi Hung, PhD, b Robert H. Pantell, MD c BACKGROUND: There is considerable variation
Shabir A. Madhi Possibilities for reducing neonatal and young infant mortality through Maternal immunization
 Shabir A. Madhi Possibilities for reducing neonatal and young infant mortality through Maternal immunization National Institute for Communicable Diseases & University of Witwatersrand, South Africa Respiratory
Shabir A. Madhi Possibilities for reducing neonatal and young infant mortality through Maternal immunization National Institute for Communicable Diseases & University of Witwatersrand, South Africa Respiratory
Microbiology Laboratory Directors, Infection Preventionists, Primary Care Providers, Emergency Department Directors, Infectious Disease Physicians
 MEMORANDUM DATE: October 1, 2009 TO: FROM: SUBJECT: Microbiology Laboratory Directors, Infection Preventionists, Primary Care Providers, Emergency Department Directors, Infectious Disease Physicians Michael
MEMORANDUM DATE: October 1, 2009 TO: FROM: SUBJECT: Microbiology Laboratory Directors, Infection Preventionists, Primary Care Providers, Emergency Department Directors, Infectious Disease Physicians Michael
Facing the ongoing challenge of the febrile young infant
 DePorre et al. Critical Care (2017) 21:68 DOI 10.1186/s13054-017-1646-9 REVIEW Facing the ongoing challenge of the febrile young infant Adrienne G. DePorre 1,2*, Paul L. Aronson 3 and Russell J. McCulloh
DePorre et al. Critical Care (2017) 21:68 DOI 10.1186/s13054-017-1646-9 REVIEW Facing the ongoing challenge of the febrile young infant Adrienne G. DePorre 1,2*, Paul L. Aronson 3 and Russell J. McCulloh
Cerebrospinal Fluid Glucose and Protein in Disposition and Treatment Decisions
 298 BRIEF REPORTS Givens et al. CSF GLUCOSE AND PROTEIN Cerebrospinal Fluid Glucose and Protein in Disposition and Treatment Decisions Routine laboratory analysis performed when bacterial meningitis is
298 BRIEF REPORTS Givens et al. CSF GLUCOSE AND PROTEIN Cerebrospinal Fluid Glucose and Protein in Disposition and Treatment Decisions Routine laboratory analysis performed when bacterial meningitis is
Recommendations for Hospital Quality Measures in 2011:
 Pediatric Measures: Recommendations for Hospital Quality Measures in 2011: Based on the input of a group of healthcare stakeholders, the following new hospital measures are recommended: 1) Home Management
Pediatric Measures: Recommendations for Hospital Quality Measures in 2011: Based on the input of a group of healthcare stakeholders, the following new hospital measures are recommended: 1) Home Management
Neonatal Herpes Infection: Case Report and Discussion
 BRIEF REPORT Neonatal Herpes Infection: Case Report and Discussion Jordan C. White, MD, and Susanna R. Magee, MD, MPH Neonatal herpes simplex virus (HSV) infections are often life-threatening. Although
BRIEF REPORT Neonatal Herpes Infection: Case Report and Discussion Jordan C. White, MD, and Susanna R. Magee, MD, MPH Neonatal herpes simplex virus (HSV) infections are often life-threatening. Although
Sample Selection- Vignettes
 Sample Selection- Vignettes Rangaraj Selvarangan, BVSc, PhD, D(ABMM) Professor, UMKC School of Medicine Director, Microbiology, Virology and Molecular Infectious Diseases Laboratory Director, Laboratory
Sample Selection- Vignettes Rangaraj Selvarangan, BVSc, PhD, D(ABMM) Professor, UMKC School of Medicine Director, Microbiology, Virology and Molecular Infectious Diseases Laboratory Director, Laboratory
Review of Neonatal Respiratory Problems
 Review of Neonatal Respiratory Problems Respiratory Distress Occurs in about 7% of infants Clinical presentation includes: Apnea Cyanosis Grunting Inspiratory stridor Nasal flaring Poor feeding Tachypnea
Review of Neonatal Respiratory Problems Respiratory Distress Occurs in about 7% of infants Clinical presentation includes: Apnea Cyanosis Grunting Inspiratory stridor Nasal flaring Poor feeding Tachypnea
THE COLLEGES OF MEDICINE OF SOUTH AFRICA Incorporated Association not for gain Reg No/Nr 1955/000003/08
 THE COLLEGES OF MEDICINE OF SOUTH AFRICA Incorporated Association not for gain Reg No/Nr 1955/000003/08 DCH(SA) Examination for the Diploma in Child Health of the College of Paediatricians of South Africa
THE COLLEGES OF MEDICINE OF SOUTH AFRICA Incorporated Association not for gain Reg No/Nr 1955/000003/08 DCH(SA) Examination for the Diploma in Child Health of the College of Paediatricians of South Africa
Should blood cultures be obtained in all infants 3 to 36 months presenting with significant fever? abstract CLINICAL QUESTION REVIEW
 CLINICAL QUESTION REVIEW CQR is a recurring section in Hospital Pediatrics where authors start with a relevant clinical question, find and synthesize the recent literature and provide their best answer
CLINICAL QUESTION REVIEW CQR is a recurring section in Hospital Pediatrics where authors start with a relevant clinical question, find and synthesize the recent literature and provide their best answer
Online Video Library Pediatric Emergency Room Puzzlers
 Outreach Education Online Video Library 2009-2010... Pediatric Emergency Room Puzzlers.... Program Handouts This information is provided as a courtesy by Children's Health Care System and its related organizations
Outreach Education Online Video Library 2009-2010... Pediatric Emergency Room Puzzlers.... Program Handouts This information is provided as a courtesy by Children's Health Care System and its related organizations
An Intriguing Case of Meningitis. Tiffany Mylius MLS (ASCP)
") An Intriguing Case of Meningitis { Tiffany Mylius MLS (ASCP) A 4yo male presents with 2wk history of URI symptoms. On the day of admission, the patient woke up with a HA in the morning, took a nap later
An Intriguing Case of Meningitis { Tiffany Mylius MLS (ASCP) A 4yo male presents with 2wk history of URI symptoms. On the day of admission, the patient woke up with a HA in the morning, took a nap later
Community Acquired Pneumonia. Abdullah Alharbi, MD, FCCP
 Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
PYELONEPHRITIS. Wendy Glaberson 11/8/13
 PYELONEPHRITIS Wendy Glaberson 11/8/13 A 19mo infant girl was seen in the ED 3 days ago and diagnosed with a UTI. She was afebrile at the time and discharged on broad spectrum antibiotics. The child returns
PYELONEPHRITIS Wendy Glaberson 11/8/13 A 19mo infant girl was seen in the ED 3 days ago and diagnosed with a UTI. She was afebrile at the time and discharged on broad spectrum antibiotics. The child returns
NEONATAL SEPSIS. Dalima Ari Wahono Astrawinata Departemen Patologi Klinik, FKUI-RSCM
 NEONATAL SEPSIS Dalima Ari Wahono Astrawinata Departemen Patologi Klinik, FKUI- Background Neonatal sepsis : Early-onset Late-onset Early-onset : mostly premature neonates Within 24 hours 85% 24-48 hours
NEONATAL SEPSIS Dalima Ari Wahono Astrawinata Departemen Patologi Klinik, FKUI- Background Neonatal sepsis : Early-onset Late-onset Early-onset : mostly premature neonates Within 24 hours 85% 24-48 hours
Continuing malaria education modules. Module 1 Severe malaria triage, diagnosis, and treatment
 The MalariaCare Toolkit Tools for maintaining high-quality malaria case management services Continuing malaria education modules Module 1 Severe malaria triage, diagnosis, and treatment Download all the
The MalariaCare Toolkit Tools for maintaining high-quality malaria case management services Continuing malaria education modules Module 1 Severe malaria triage, diagnosis, and treatment Download all the
Physician Orders. LEB NICU Sepsis Plan [X or R] = will be ordered unless marked out.
![Physician Orders. LEB NICU Sepsis Plan [X or R] = will be ordered unless marked out.](/thumbs/77/75931338.jpg "Physician Orders. LEB NICU Sepsis Plan [X or R] = will be ordered unless marked out.") Height: cm Weight: kg Allergies: [ ] No known allergies [ ] Latex allergy [ ]Other: [ ] Initiate Powerplan Phase, Phase: LEB NICU Sepsis Phase Admission/Transfer/Discharge [ ] Patient Status Initial Inpatient
Height: cm Weight: kg Allergies: [ ] No known allergies [ ] Latex allergy [ ]Other: [ ] Initiate Powerplan Phase, Phase: LEB NICU Sepsis Phase Admission/Transfer/Discharge [ ] Patient Status Initial Inpatient
RSV Surveillance in the U.S.
 RSV Surveillance in the U.S. Susan I. Gerber, MD Respiratory Virus Program Division of Viral Diseases National Center for Immunization and Respiratory Diseases Centers for Disease Control and Prevention
RSV Surveillance in the U.S. Susan I. Gerber, MD Respiratory Virus Program Division of Viral Diseases National Center for Immunization and Respiratory Diseases Centers for Disease Control and Prevention
Fever and Infections in Pediatrics
 Fever and Infections in Pediatrics Dr. Todd Twogood 2019 update Big Sky Conference Pediatric Fever and illness The most common reason for children to be taken to the doctor for acute illness Major concern
Fever and Infections in Pediatrics Dr. Todd Twogood 2019 update Big Sky Conference Pediatric Fever and illness The most common reason for children to be taken to the doctor for acute illness Major concern
Neonatal Sepsis. Neonatal sepsis ehandbook
 Neonatal Sepsis Neonatal sepsis ehandbook Sepsis Any baby who is unwell must be considered at risk of sepsis 1 in 8 per 1000 lives births The consequences of untreated sepsis are devastating - 10-30% risk
Neonatal Sepsis Neonatal sepsis ehandbook Sepsis Any baby who is unwell must be considered at risk of sepsis 1 in 8 per 1000 lives births The consequences of untreated sepsis are devastating - 10-30% risk
9/15/2017. Joyce Turner RN Director of Clinical Program Development
 Joyce Turner RN Director of Clinical Program Development A toxic response to an infection that spirals out of control attacking the body s own organs and tissues. The infection can be bacterial, viral
Joyce Turner RN Director of Clinical Program Development A toxic response to an infection that spirals out of control attacking the body s own organs and tissues. The infection can be bacterial, viral
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE 1 Guideline title SCOPE Bronchiolitis: diagnosis and management of bronchiolitis in children. 1.1 Short title Bronchiolitis in children 2 The remit The
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE 1 Guideline title SCOPE Bronchiolitis: diagnosis and management of bronchiolitis in children. 1.1 Short title Bronchiolitis in children 2 The remit The
J of Evolution of Med and Dent Sci/ eissn , pissn / Vol. 4/ Issue 66/ Aug 17, 2015 Page 11432
 BLOOD CULTURE AND BACTEREMIA PREDICTORS IN INFANTS LESS THAN ONE YEAR OF AGE WITH FEVER WITHOUT SOURCE (FWS) Y. G. Sathish Kumar 1, A. Udayamaliny 2, S. Ankitha 3 HOW TO CITE THIS ARTICLE: Y. G. Sathish
BLOOD CULTURE AND BACTEREMIA PREDICTORS IN INFANTS LESS THAN ONE YEAR OF AGE WITH FEVER WITHOUT SOURCE (FWS) Y. G. Sathish Kumar 1, A. Udayamaliny 2, S. Ankitha 3 HOW TO CITE THIS ARTICLE: Y. G. Sathish
CRACKCast E167 Pediatric Fever. Key Concepts. CrackCast Show Notes Pediatric Fever April 2018
 CRACKCast E167 Pediatric Fever Key Concepts Fever is the #1 kids are brought to the ED! Vaccination (for Haemophilus influenzae type b and Streptococcus pneumoniae) has dropped the rates of serious bacterial
CRACKCast E167 Pediatric Fever Key Concepts Fever is the #1 kids are brought to the ED! Vaccination (for Haemophilus influenzae type b and Streptococcus pneumoniae) has dropped the rates of serious bacterial