Neonatal presentation of citrullinemia
|
|
|
- Marybeth Willis
- 6 years ago
- Views:
Transcription

1 SWISS SOCIETY OF NEONATOLOGY Winner of the Case of the Year Award 2014 Neonatal presentation of citrullinemia May 2014
2 2 Anastaze-Stelle K, Hagerman A, Fluss J, Borradori-Tolsa C, Kanavaki A, Sizonenko S, Parvex P, Megevand-Lador C, Bonafe L, Kern I, Geneva Developmental Unit (ASK, BTC, SS, MLC), Geneva Neonatology Unit (HA), Geneva Neurology (FJ), Geneva Radiology (KA), Geneva Nephrology (PP), Lausanne Metabolic Unit (BL), Geneva metabolic Unit (KI), Geneva and Lausanne University Children s Hospitals, Switzerland Swiss Society of Neonatology, Thomas M Berger, Webmaster
3 3 Severe hyperammonemia in a newborn is an uncommon problem, which is typically revealed by symptoms of encephalopathy that may include seizures. Etiologies include sepsis, severe liver failure and inborn errors of metabolism, mainly urea cycle disorders, but also organic acidurias, fatty acid oxidation disorders and several others. INTRODUCTION This male infant was born by normal vaginal delivery to a 27-year-old G2/P1 at 38 4/7 weeks of gestation after an uneventful pregnancy. No risks for infection were recorded. Umbilical arterial cord-ph was 7.26, Apgar scores 9, 10 and 10 at 1, 5 and 10 minutes, respectively. Birth weight was 3300 g (P50), length 51 cm (P25-50) and head circumference 35.5 cm (P50). CASE REPORT The infant was breastfed in the delivery room and showed vigorous sucking. However, after transfer to the maternity ward, the mother expressed concerns as the child consistently refused to feed and regurgitated abun dantly. On day 3 of life, the infant appeared increasingly lethargic before developing a sudden episode of generalized hypertonia with deviation of the eyes to the right during a few seconds. A similar episode, 2 hours later, was accompanied by clonus of the right arm. On neurological examination, the fontanel and pupils appeared normal, but lethargy, axial hypotonia, peripheral hypertonia particularly of the right arm, an enhanced grasping reflex and diminished su-
4 4 cking reflex were observed. Blood gases, glucose and electro lytes values were normal. The encephalopathic infant was transferred to the NICU for further work-up and treatment of suspected convulsions. Phenobarbital was started and the patient was intubated due to a rapidly progressive comatose state. Antibiotic and antiviral coverage were initiated. Laboratory exams included a complete blood count, C-reactive protein and blood chemistry. All came back within their reference range, except for marked hyperammonemia at 688 µmol/l 70 hours after birth and an increased lactate concentration of 4.8 mmol/l. As there was no acidosis and no evidence of an infection or liver failure, a urea cycle disorder was strongly suspected. Ammonia increased to a maximal value of 1164 µmol/l 3 hours later, while ammonia-scavenging therapy was commenced. A loading dose of intravenous sodium benzoate and arginine were started. The patient was sent to the operating room for insertion of a hemodiafiltration catheter. After 24 hours of hemodiafiltration with concurrent administration of glucose, sodium benzoate and arginine, ammonia levels stabilized below 200 µmol/l. At that time, metabolic laboratory results revealed markedly increased plasma citrulline of 2090 µmol/l, glutamine of 1286 µmol/l and decreased ornithine levels of 29 µmol/l, consistent with a deficiency of argininosuccinate synthase (citrulli nemia type 1). An EEG recorded 2 days after
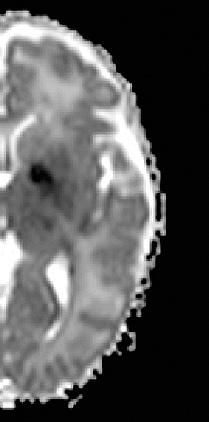
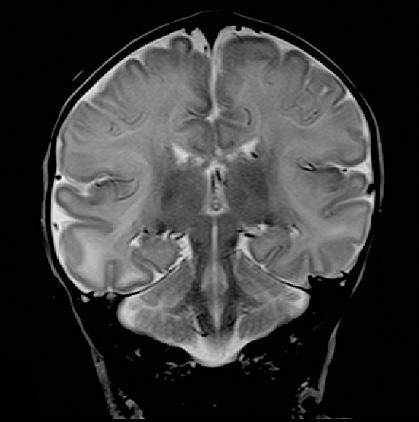
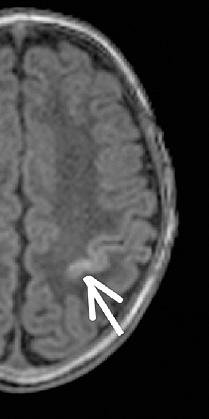
5 5 the first convulsions showed isolated multifocal temporal spikes without further clinical seizures. After three days in a deep coma, the baby recovered slowly and displayed an almost normal neurological exam one week later. In parallel, nasogastric tube feeding was progressively weaned to oral feeding. Treatment consisted of a protein-controlled diet, the ammonium-scavenging drug sodium benzoate and arginine. The amount of protein and essential amino acids in the diet and medication dosages were adjusted according to his clinical condition, weight and ammonia and amino acid profiles. Phenobarbital was tapered off over 25 days. Brain MRI on day 7 showed diffuse white matter abnormalities, multiple ischemic-hemorrhagic lesions and bilateral restriction of the diffusion coefficient in the globus pallidus, the splenium of the corpus callosum, the periinsular and perirolandic cortex (Fig. 1). Follow-up MRI performed two weeks later confirmed the diffuse white matter abnormalities, and showed bilateral symmetric globus pallidus abnormal signal intensity and bilateral cortical laminar necrosis at the level of the central sulcus (Fig. 2). The infant was discharged home at 5 weeks of age in good general health, albeit yet with a slightly abnormal neurological exam displaying enhanced sensitivity to noise and increased patellar reflexes.
6 6 Up to his current age of 9 months, he did not experience any metabolic decompensation, and demonstrated normal weight gain, height and head growth. Neurodevelopmental assessment was performed at 3 months: the infant appeared alert, with good social interactions, but displayed a limited range of spontaneous movements with atypical postures, a tendency to keep his fists clenched, a persistent marked asymmetric tonic neck reflex, axial hypotonia and peripheral hypertonia. On the Baley-II Scales of Infant Development, his scores were within the range of moderately delayed psychomotor development. On follow-up at 9 months, he appeared cheerful, with good eye contact, visual exploration and tracking; however, he did not reach for objects, had not started babbling and could not yet sit unsupported. In addition to his marked psych omotor delay, he displayed early signs of possible dystonic cerebral palsy with intermittent decreases in axial tonus, associated with hypertonia and athetosis of the extremities. DISCUSSION The differential diagnosis of encephalopathy and/or seizures in a newborn is broad; therefore, a few key points should be kept in mind. Is it a term infant? Was delivery uneventful? Did symptoms occur after a symptom-free interval of more than hours? What are the results of the baseline laboratory workup? Clues to the initial differential diagnosis are listed in the table.
7 7 The onset of neurological symptoms after a symptomfree interval of more than hours following a normal delivery with normal Apgar scores renders hypoxic-ischemic encephalopathy unlikely. Neonatal arterial ischemic stroke may also present with delayed focal seizures but in general with normal alertness up to the event and in between seizures. Neonatal cere bral sinus venous thrombosis might be associated with non-specific signs and profound lethargy. Sepsis may obviously also be associated with progressive encephalo pathy: a sepsis work-up is generally warranted and antimicrobial therapy should be started while waiting for laboratory results. The key features of increasingly poor feeding, vomiting and progressive lethargy with or without seizures should quickly direct towards a metabolic origin. Hence, whenever performing blood gas analysis or a sepsis work-up in a newborn aged 2 to 7 days of age with signs of progressive encephalopathy, measurement of serum ammonia concentration should be included (1). Initial investigations in our patient included a full blood count, blood gas analysis, liver and renal function tests, rapidly followed by a plasma amino acid profile, urinary organic acid, cerebral ultrasound and, after clinical stabilization, brain MRI. The infant had highly elevated serum ammonia levels associated with normal serum glucose and anion gap suggestive of a urea cycle defect.
:")
; C)")
8 8 Fig. 1 A B First MRI (4 days after onset of symptoms): A) DWI and B) ADC map: bilateral symmetric globus pallidus restricted diffusion (white arrow); C) T2WI: diffuse white matter signal abnormality.
9 9 C
: A) T1WI: bilateral")

10 10 Fig.2 A B Follow-up MRI (2 weeks after the first MRI): A) T1WI: bilateral globus pallidus hyperintensity (white arrow); B) T1WI: bilateral central sulcus hyper-intensity compatible with cortical laminar necrosis (white arrow); C) T2 WI: pronounced diffuse white matter signal abnormalities
11 11 C
12 12 symptoms < 24h of life term neonatal hyper NH 4 + PH organic acidemia symptoms > 24h of life PH N or h hypoglycemia fatty acid oxidation Fig.3 Algorithm for the evaluation of neonatal hyperammonemia, adapted from Burton B. (3) and Häberle et al. (4) (THAN: transient hyperammonemia of the newborn; CPS1D: carbamyl phosphate synthetase deficiency; OTC: ornithine transcarbamylase deficiency; OAT D: ornithine aminotransferase deficiency; ASL D: arginosuccinate lyase deficiency; ASS D: arginosuccinate synthetase deficiency = citrullinemia type 1)
13 13 preterm THAN: glutamine or N full term organic acidemia N or : CPS1 D citrulline h orotic acid ASL D h ornithine N=OTC h= OAT D h h ASS D= citrullinemia
14 14 Stroke Intracranial hemorrhage Extrinsic intoxication Intracranial infections / sepsis Hypoxic-ischemic insult preterm, complicated delivery, abnormal Apgar score, neonatal alloimmune thrombocytopenia, inherited coagulopathy complicated delivery common, maternal or placental disorders, cardiac disorders, inherited coagulopathy infectious risk may be present (prolonged rupture of membranes, maternal fever pre- or post-partum, Group B streptococcus infection) Intrinsic metabolic intoxication medication given to mother or child complicated delivery, abnormal Apgar score Medical history usually in the first several days of life, rarely present at birth uncomplicated term birth, progressive refusal to feed, vomiting no may be present variable, occurrence after 24 hours Symptomfree interval complete blood count, baseline coagulation profile no specific laboratory exams but performed to find causes and exclude others diagnosis may occur may range from 12h to several days toxicological screening depending on the disease: abnormal ph, glucose, lactate, ammonia, ketones... Table abnormal blood count, elevated CRP, PCT and IL6 Laboratory cord ph, base excess, elevated liver enzymes and decreased renal function, CPK, troponin Differential diagnosis of neonatal encephalopathy +/- seizures: distinguishing features
15 15 The differential diagnosis of metabolic causes of neonatal hyperammonemia is obviously not restricted to urea cycle defects, but also includes organic acidemias (propionic aciduria, methylmalonic aciduria), which cause secondary derangement of the urea cycle function, fatty oxidation defects, pyruvate carboxylase deficiency (PCD) as well as several other enzymatic deficiencies (Fig. 3). Organic acidurias are characterized by low blood ph, abnormal anion gab and elevated urinary ketones. Transient hyperammonemia of the newborn (THAN) should also be considered in premature newborns, keeping in mind that respiratory distress is a prominent early symptom occurring before12 hours of life in THAN, with ammonia levels rising earlier and to higher levels than in UCD (2). THAN is typically characterised by a lack of glutamine elevation. In our patient, normal ph, absence of organic aciduria, normal acylcarnitines, elevated glutamine and highly elevated citrulline and orotic acid pointed towards the diagnosis of citrullinemia, which was later confirmed by molecular diagnosis. This autosomal recessive urea cycle disorder results from a deficiency of the enzyme arginosuccinate synthetase (ASS), which links citrulline and aspartate to form arginosuccinic acid. ASS1 mutations disabling enzymatic activity lead to severe acute hyperammonemic encephalopathic decompensation within the first days of life, whereas
16 16 milder mutations may present after weeks, months or even years with more chronic symptoms (5). In one large published study featuring 70 ASS patients, 34% presented symp toms during the first 30 days of life, 18 % between 1 month and 2 years, 28% between 2 and 12 years, leaving 10% during adolescence and adulthood (6). In the neonatal period, symptoms of hyperammonemia are not very specific: frequently observed findings include poor feeding, vomiting, irritability, tachypnea, somnolence, progressing to lethargy, hypothermia, coma and eventually seizures (7). Rapid reduction of ammonia is the first goal of treatment in the hyperammonemic neonate, as significant hyperammonemia induces irreversible damage to the developing brain within a few hours. This is achieved by immediately ceasing protein intake, reversing catabolism through high glucose intake, addition of nitrogen-scavenging drugs and hemodialysis if ammonia levels exceed µmol/l (8, 9). Detailed recommendations have been published by Haberle et al. (4). In most UCDs, arginine should be added to enhance residual activity of the urea cycle. Addition of N-carbamylglutamate may be considered in undiagnosed UCD patients. The pathophysiology of hyperammonemia induced brain damage is mediated by complex and not completely elucidated alterations in several amino acid path ways, neurotransmission, failure of energy pro-
17 17 duction by the Krebs cycle, impaired creatine metabolism, excessive nitric oxide synthesis, oxidative stress and multiple alterations in signal transduction pathways (7, 10). Glutamine is synthesized in the astrocytes from glutamate and ammonia in an attempt to limit hyperammonemia; this causes astrocytic swelling and thereby cytotoxic edema. Intracellular reversal releases glutamate into the intercellular space. Excessive activation of NMDA receptors by glutamate causes an excitotoxic insult triggering cell death by apoptosis or necrosis (7, 10). In our patient, initial MRI showed diffuse abnormal signal of the white matter, bilateral globus pallidus lesions, sparing of the thalami, and lesions of the periinsular and perirolandic cortex. Preferential alterations of the white matter and basal ganglia with sparing of the thalami is indeed reported as a characteristic pattern of urea cycle disorders on MRI, helping to different iate this entity from hypoxic-ischemic lesions (10, 11). In more severe hyperammonemia involving the cortex, the periinsular region is affected first, with progressive extension into the frontal, parietal, temporal and finally occipital lobes (11). Restricted diffusion correlates also with higher and more prolonged ammonia and glutamate levels and more severe neurological sequelae; in the most severe cases, restricted diffusion may even affect the thalami (11).
18 18 Overall prognosis of infants with neonatal presentation of UCD is poor with high perinatal mortality. Most surviving patients display moderate to severe mental retardation as well as significant developmental disabilities (4, 10, 12). In a large retrospective study, only 35 % of UCD patients with neonatal presentation survived beyond 11 years, as opposed to 87% of those with later presentation (6). Several authors attempted to correlate the degree of hyperammonemia with clinical outcome: not surprisingly, earlier, higher and more prolonged ammonia levels correlated negatively with neurological outcome (4, 7). Normal psychomotor development is very unlikely when the initial ammonia is >300 µmol/l and when the maximum ammonia reach levels over 480 µmol/l (4). After initial decompensation, long-term outcome is also influenced by external factors, such as the occurrence of infections, stress and poor treatment compliance, which may precipitate further episodes of hyperammonemia causing additional injuries. Long-term treatment is based on keeping a nutritional balance to avoid malnutrition or catabolism and protein overload that could lead to metabolic decompensation. Dietary protein intake should be kept at the minimum safe level; protein requirements per kg body weight are highest in the neonatal period and decrease steadily as growth slows down. Suggested safe intakes are found in Braissant et al. (7) but must be adjusted individually by regular monitoring of plasma
19 19 protein, prealbumin and amino acid levels. In patients with severe UCD, it is often helpful to replace around one fourth of the natural protein by essential amino acids (4). Sufficient calories must be provided, according to age and individual requirements; moreover energy and protein intake should be spread over 24 hours, avoiding long intervals at night that may induce a catabolic state. In addition, the nitrogen-scavenger sodium benzoate or its alternative phenylbutyrate (Ammonaps ) must be given to promote nitrogen excretion (4, 7). These drugs have a narrow therapeutic range; over-dosing may deplete essential amino acids and precipitate catabolism. Arginine becomes an essential amino acid and should be substituted. Daily management is challenging for caregivers and children who live with the fear of a new decompensation that may occasionally require inpatient management in a metabolic center far away from home and ultimately aggravate the child s disability and overall prognosis (12, 13). Liver transplantation (LT) should be considered an option in particular when there is poor metabolic control. Even if LT prevents further episodes of metabolic decompensation, final outcome obviously depends on the preexisting neurological deficit. Timing of LT requires a balance between the increased risk of performing LT in very small infants and the risk of further episodes of decompensation due to the delay in performing the procedure; some authors advocate therefore transplanting before the age of 1 year (4, 14).
20 20 In rare cases when diagnosis is made before birth, sodium benzoate infusion to the mother started a few hours before delivery, along with classical dietary and medical treatment started right after delivery, was shown to prevent neonatal hyperammonemia (5). Neonatal screening for UCDs is not widely promoted as there is no effective sensitive and specific maker and in many cases, severe hyperammonemia occurs before screening results would become available (1, 4).
21 21 1. Bachmann C. Long-term outcome of patients with urea cycle disorders and the question of neonatal screening. Eur J Pediatr 2003;162:S29-S33 REFERENCES 2. Hudak ML, Jones MD, Brusilow SW. Differentiation of transient hyperammonemia of the newborn and urea cycle enzyme defects by clinical presentation. J Pediatr 1985;107: Burton BK. Inborn errors of metabolism in infancy: a guide to diagnosis. Pediatrics 1998;102:e69 4. Haberle J, Boddaert N, Burlina A, et al. Suggested guidelines for the diagnosis and management of urea cycle disorders. Orphanet J Rare Dis 2012;7:32 5. Das AM, Illsinger S, Hartmann H, et al., Prenatal benzoate treatment in urea cycle defects. Arch Dis Child Fetal Neonatal Ed 2009;94:F216-F Summar ML, Dobbelaere D, Brusilow S, Lee B. Diagnosis, symptoms, frequency and mortality of 260 patients with urea cycle disorders from a 21-year, multicentre study of acute hyperammonaemic episodes. Acta Paediatr 2008;97: Braissant O, McLin VA, Cudalbu C. Ammonia toxicity to the brain. J Inher Metab Dis 2013;36: Auron A, Brophy PD. Hyperammonemia in review: pathophysiology, diagnosis, and treatment. Pediatr Nephrol 2012;27: Spinale JM, Laskin BL, Sondheimer N, Swartz SJ, Goldstein SL. High-dose continuous renal replacement therapy for neonatal hyperammonemia. Pediatr Nephrol 2013;28: Gropman AL, Summar M, Leonard JV. Neurological implications of urea cycle disorders. J Inher Metab Dis 2007;30:
22 Bireley WR, Van Hove JL, Gallagher RC, Fenton LZ. Urea cycle disorders: brain MRI and neurological outcome. Pediatr Radiol 2012;42: Bachmann C. Outcome and survival of 88 patients with urea cycle disorders: a retrospective evaluation. Eur J Pediatr 2003;162: Singh RH. Nutritional management of patients with urea cycle disorders. J Inher Metab Dis 2007;30: Campeau PM, Pivalizza PJ, Miller G, et al. Early orthotopic liver transplantation in urea cycle defects: follow up of a developmental outcome study. Mol Genet Metab 2010;100 (Suppl 1):S84-S87
23

24 concept & design by mesch.ch SUPPORTED BY CONTACT Swiss Society of Neonatology
Urea Cycle Disorders Prior Authorization Program Summary
 Urea Cycle Disorders Prior Authorization Program Summary FDA APPROVED INDICATIONS DOSAGE 1,2 Agent(s) Indication(s) Dosing -Adjunctive therapy in the chronic management of patients with urea cycle disorders
Urea Cycle Disorders Prior Authorization Program Summary FDA APPROVED INDICATIONS DOSAGE 1,2 Agent(s) Indication(s) Dosing -Adjunctive therapy in the chronic management of patients with urea cycle disorders
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Urea Cycle Disorders Page 1 of 7 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Urea Cycle Disorders Prime Therapeutics will review Prior Authorization requests
Urea Cycle Disorders Page 1 of 7 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Urea Cycle Disorders Prime Therapeutics will review Prior Authorization requests
Urea Cycle Defects. Dr Mick Henderson. Biochemical Genetics Leeds Teaching Hospitals Trust. MetBioNet IEM Introductory Training
 Urea Cycle Defects Dr Mick Henderson Biochemical Genetics Leeds Teaching Hospitals Trust The Urea Cycle The urea cycle enables toxic ammonia molecules to be converted to the readily excreted and non toxic
Urea Cycle Defects Dr Mick Henderson Biochemical Genetics Leeds Teaching Hospitals Trust The Urea Cycle The urea cycle enables toxic ammonia molecules to be converted to the readily excreted and non toxic
TRANSAMINATION AND UREA CYCLE
 TRANSAMINATION AND UREA CYCLE USMAN SUMO FRIEND TAMBUNAN ARLI ADITYA PARIKESIT SEPTIANA BIOINFORMATICS GROUP DEPARTEMENT OF CHEMISTRY FACULTY OF MATHEMATIC AND SCIENCE UNIVERSITY OF INDONESIA What is transamination?
TRANSAMINATION AND UREA CYCLE USMAN SUMO FRIEND TAMBUNAN ARLI ADITYA PARIKESIT SEPTIANA BIOINFORMATICS GROUP DEPARTEMENT OF CHEMISTRY FACULTY OF MATHEMATIC AND SCIENCE UNIVERSITY OF INDONESIA What is transamination?
UREA CYCLE DISORDERS - The What, Why, How and When
 UREA CYCLE DISORDERS - The What, Why, How and When George A. Diaz, MD, PhD Program for Inherited Metabolic Diseases Department of Genetics and Genomic Sciences Department of Pediatrics Icahn School of
UREA CYCLE DISORDERS - The What, Why, How and When George A. Diaz, MD, PhD Program for Inherited Metabolic Diseases Department of Genetics and Genomic Sciences Department of Pediatrics Icahn School of
Newborn Screen & Development Facts about the genetic diseases new since March 2006 (Excluding Cystic Fibrosis)
") Newborn Screen & Development Facts about the genetic diseases new since March 2006 (Excluding Cystic Fibrosis) 1) Argininosuccinic acidemia (ASA) a) Incidence: ~1 in 70,000 b) Deficiency in an enzyme of
Newborn Screen & Development Facts about the genetic diseases new since March 2006 (Excluding Cystic Fibrosis) 1) Argininosuccinic acidemia (ASA) a) Incidence: ~1 in 70,000 b) Deficiency in an enzyme of
UPDATE ON UREA CYCLE DISORDERS TREATMENT
 UPDATE ON UREA CYCLE DISORDERS TREATMENT George A. Diaz, MD, PhD Program for Inherited Metabolic Diseases Department of Genetics and Genomic Sciences Icahn School of Medicine at Mount Sinai Disclosure
UPDATE ON UREA CYCLE DISORDERS TREATMENT George A. Diaz, MD, PhD Program for Inherited Metabolic Diseases Department of Genetics and Genomic Sciences Icahn School of Medicine at Mount Sinai Disclosure
The spectrum and outcome of the. neonates with inborn errors of. metabolism at a tertiary care hospital
 The spectrum and outcome of the neonates with inborn errors of metabolism at a tertiary care hospital Dr. Sevim Ünal Neonatology Division, Ankara Children s Hematology Oncology Research Hospital, Ankara,
The spectrum and outcome of the neonates with inborn errors of metabolism at a tertiary care hospital Dr. Sevim Ünal Neonatology Division, Ankara Children s Hematology Oncology Research Hospital, Ankara,
LOW CITRULLINE AS A MARKER FOR THE PROXIMAL UREA CYCLE DEFECTS EXPERIENCE OF THE NEW ENGLAND NEWBORN SCREENING PROGRAM
 LOW CITRULLINE AS A MARKER FOR THE PROXIMAL UREA CYCLE DEFECTS EXPERIENCE OF THE NEW ENGLAND NEWBORN SCREENING PROGRAM Inderneel Sahai, MD, FACMG Newborn Screening and Genetic Testing Symposium Oct 2014
LOW CITRULLINE AS A MARKER FOR THE PROXIMAL UREA CYCLE DEFECTS EXPERIENCE OF THE NEW ENGLAND NEWBORN SCREENING PROGRAM Inderneel Sahai, MD, FACMG Newborn Screening and Genetic Testing Symposium Oct 2014
ESPEN Congress Madrid 2018
 ESPEN Congress Madrid 2018 Inborn Errors Of Metabolism Urea Cycle Disorders Diagnosis And Care F. Feillet (FR) Urea cycle disorders, diagnosis and care F Feillet National reference centre for Inborn errors
ESPEN Congress Madrid 2018 Inborn Errors Of Metabolism Urea Cycle Disorders Diagnosis And Care F. Feillet (FR) Urea cycle disorders, diagnosis and care F Feillet National reference centre for Inborn errors
SWISS SOCIETY OF NEONATOLOGY. Neonatal cerebral infarction
 SWISS SOCIETY OF NEONATOLOGY Neonatal cerebral infarction May 2002 2 Mann C, Neonatal and Pediatric Intensive Care Unit, Landeskrankenhaus und Akademisches Lehrkrankenhaus Feldkirch, Austria Swiss Society
SWISS SOCIETY OF NEONATOLOGY Neonatal cerebral infarction May 2002 2 Mann C, Neonatal and Pediatric Intensive Care Unit, Landeskrankenhaus und Akademisches Lehrkrankenhaus Feldkirch, Austria Swiss Society
First report of carglumic acid in a patient with citrullinemia type 1 (argininosuccinate synthetase deficiency)
") Received: 14 June 2017 Accepted: 20 June 2017 DOI: 10.1111/jcpt.12593 CASE REPORT First report of carglumic acid in a patient with citrullinemia type 1 (argininosuccinate synthetase deficiency) E. Kose
Received: 14 June 2017 Accepted: 20 June 2017 DOI: 10.1111/jcpt.12593 CASE REPORT First report of carglumic acid in a patient with citrullinemia type 1 (argininosuccinate synthetase deficiency) E. Kose
Proceedings of a Consensus Conference for the
 Proceedings of a Consensus Conference for the Management of Patients with Urea Cycle Disorders Marshall Summar, MD, and Mendel Tuchman, MD In an effort to develop standards for the treatment of patients
Proceedings of a Consensus Conference for the Management of Patients with Urea Cycle Disorders Marshall Summar, MD, and Mendel Tuchman, MD In an effort to develop standards for the treatment of patients
Urea Cycle Disorders and Hyperammonemia: Diagnosable Treatable Screenable
 Urea Cycle Disorders and Hyperammonemia: Diagnosable Treatable Screenable Marshall L. Summar, M.D. Chief, Division of Genetics and Metabolism Children s National Medical Center Washington, DC, USA Disclosure
Urea Cycle Disorders and Hyperammonemia: Diagnosable Treatable Screenable Marshall L. Summar, M.D. Chief, Division of Genetics and Metabolism Children s National Medical Center Washington, DC, USA Disclosure
Objectives. Birth Depression Management. Birth Depression Terms
 Objectives Birth Depression Management Regional Perinatal Outreach Program 2016 Understand the terms and the clinical characteristics of birth depression. Be familiar with the evidence behind therapeutic
Objectives Birth Depression Management Regional Perinatal Outreach Program 2016 Understand the terms and the clinical characteristics of birth depression. Be familiar with the evidence behind therapeutic
Jana Novotná, Bruno Sopko. Department of the Medical Chemistry and Clinical Biochemistry The 2nd Faculty of Medicine, Charles Univ.
 Amino acid metabolism II. Urea cycle Jana Novotná, Bruno Sopko Department of the Medical Chemistry and Clinical Biochemistry The 2nd Faculty of Medicine, Charles Univ. Nitrogen balance Tissue proteins
Amino acid metabolism II. Urea cycle Jana Novotná, Bruno Sopko Department of the Medical Chemistry and Clinical Biochemistry The 2nd Faculty of Medicine, Charles Univ. Nitrogen balance Tissue proteins
Carbamoyl phosphate synthetase 1 deficiency: First report of this rare metabolic disorder in Kingdom of Bahrain with novel mutation
 Alsahlawi et al. 1 CASE REPORT PEER REVIEWED OPEN ACCESS Carbamoyl phosphate synthetase 1 deficiency: First report of this rare metabolic disorder in Kingdom of Bahrain with novel mutation Z. Alsahlawi,
Alsahlawi et al. 1 CASE REPORT PEER REVIEWED OPEN ACCESS Carbamoyl phosphate synthetase 1 deficiency: First report of this rare metabolic disorder in Kingdom of Bahrain with novel mutation Z. Alsahlawi,
Col Rama Krishna Sanjeev Military Hospital Chennai Prof Shanmughasundaram Mehta Hospital, Chennai
 Col Rama Krishna Sanjeev Military Hospital Chennai Prof Shanmughasundaram Mehta Hospital, Chennai 11 day old male neonate admitted on 26/6 to our Hospital with c/olethargy -since day1 abnormal movements
Col Rama Krishna Sanjeev Military Hospital Chennai Prof Shanmughasundaram Mehta Hospital, Chennai 11 day old male neonate admitted on 26/6 to our Hospital with c/olethargy -since day1 abnormal movements
SWISS SOCIETY OF NEONATOLOGY. Spontaneous intestinal perforation or necrotizing enterocolitis?
 SWISS SOCIETY OF NEONATOLOGY Spontaneous intestinal perforation or necrotizing enterocolitis? June 2004 2 Stocker M, Berger TM, Neonatal and Pediatric Intensive Care Unit, Children s Hospital of Lucerne,
SWISS SOCIETY OF NEONATOLOGY Spontaneous intestinal perforation or necrotizing enterocolitis? June 2004 2 Stocker M, Berger TM, Neonatal and Pediatric Intensive Care Unit, Children s Hospital of Lucerne,
UK NATIONAL METABOLIC BIOCHEMISTRY NETWORK GUIDELINES FOR THE INVESTIGATION OF HYPERAMMONAEMIA
 UK NATIONAL METABOLIC BIOCHEMISTRY NETWORK GUIDELINES FOR THE INVESTIGATION OF HYPERAMMONAEMIA Hyperammonaemia results from defective catabolism of amino acids to urea. Recognition and treatment of hyperammonaemia,
UK NATIONAL METABOLIC BIOCHEMISTRY NETWORK GUIDELINES FOR THE INVESTIGATION OF HYPERAMMONAEMIA Hyperammonaemia results from defective catabolism of amino acids to urea. Recognition and treatment of hyperammonaemia,
SWISS SOCIETY OF NEONATOLOGY. Severe apnea and bradycardia in a term infant
 SWISS SOCIETY OF NEONATOLOGY Severe apnea and bradycardia in a term infant October 2014 2 Walker JH, Arlettaz Mieth R, Däster C, Division of Neonatology, University Hospital Zurich, Switzerland Swiss Society
SWISS SOCIETY OF NEONATOLOGY Severe apnea and bradycardia in a term infant October 2014 2 Walker JH, Arlettaz Mieth R, Däster C, Division of Neonatology, University Hospital Zurich, Switzerland Swiss Society
SWISS SOCIETY OF NEONATOLOGY. Bart s syndrome with severe newborn encephalopathy: a delayed diagnosis
 SWISS SOCIETY OF NEONATOLOGY Bart s syndrome with severe newborn encephalopathy: a delayed diagnosis May 2003 2 Buettiker V, Hogan P, Badawi N, Department of Neonatology (BV, NB), Department of Dermatology
SWISS SOCIETY OF NEONATOLOGY Bart s syndrome with severe newborn encephalopathy: a delayed diagnosis May 2003 2 Buettiker V, Hogan P, Badawi N, Department of Neonatology (BV, NB), Department of Dermatology
Extensive cystic periventricular leukomalacia following early-onset group B streptococcal sepsis in a very low birth weight infant
 SWISS SOCIETY OF NEONATOLOGY Extensive cystic periventricular leukomalacia following early-onset group B streptococcal sepsis in a very low birth weight infant July 2012 2 Berger TM, Caduff JC, Neonatal
SWISS SOCIETY OF NEONATOLOGY Extensive cystic periventricular leukomalacia following early-onset group B streptococcal sepsis in a very low birth weight infant July 2012 2 Berger TM, Caduff JC, Neonatal
Urea cycle disorder presenting as bilateral mesial temporal sclerosis an unusual cause of seizures: a case report and review of the literature
 Wang et al. Journal of Medical Case Reports (2018) 12:208 https://doi.org/10.1186/s13256-018-1750-8 CASE REPORT Open Access Urea cycle disorder presenting as bilateral mesial temporal sclerosis an unusual
Wang et al. Journal of Medical Case Reports (2018) 12:208 https://doi.org/10.1186/s13256-018-1750-8 CASE REPORT Open Access Urea cycle disorder presenting as bilateral mesial temporal sclerosis an unusual
Hypoglycaemia of the neonate. Dr. L.G. Lloyd Dept. Paediatrics
 Hypoglycaemia of the neonate Dr. L.G. Lloyd Dept. Paediatrics Why is glucose important? It provides 60-70% of energy needs Utilization obligatory by red blood cells, brain and kidney as major source of
Hypoglycaemia of the neonate Dr. L.G. Lloyd Dept. Paediatrics Why is glucose important? It provides 60-70% of energy needs Utilization obligatory by red blood cells, brain and kidney as major source of
TITLE: NURSING GUIDELINES FOR THE MANAGEMENT OF CHILDREN WITH UREA CYCLE DEFECTS. Eilish O Connell, Clinical Education Facilitator, NCIMD
 NO. OF PAGES: Page 1 of 16 SUPERCEDES: N/A NURSING GUIDELINES FOR THE MANAGEMENT OF CHILDREN WITH UREA CYCLE DEFECTS NAME/ Eilish O Connell, Clinical Education Facilitator, NCIMD SIGNATURE: DATE: NAME/
NO. OF PAGES: Page 1 of 16 SUPERCEDES: N/A NURSING GUIDELINES FOR THE MANAGEMENT OF CHILDREN WITH UREA CYCLE DEFECTS NAME/ Eilish O Connell, Clinical Education Facilitator, NCIMD SIGNATURE: DATE: NAME/
THE ED APPROACH OF THE CHILD WITH SUSPECTED METABOLIC DISEASE
 THE ED APPROACH OF THE CHILD WITH SUSPECTED METABOLIC DISEASE Dr. Nadeem Qureshi M.D, FAAP, FCCM Associate Professor Pediatrics School of Medicine. St Louis University Attending Physician Pediatric Emergency
THE ED APPROACH OF THE CHILD WITH SUSPECTED METABOLIC DISEASE Dr. Nadeem Qureshi M.D, FAAP, FCCM Associate Professor Pediatrics School of Medicine. St Louis University Attending Physician Pediatric Emergency
SWISS SOCIETY OF NEONATOLOGY. Neonatal gastric perforation
 SWISS SOCIETY OF NEONATOLOGY Neonatal gastric perforation September 2002 2 Zankl A, Stähelin J, Roth K, Boudny P and Zeilinger G, Children s Hospital of Aarau (ZA, SJ, RK, ZG) and Institute of Pathology
SWISS SOCIETY OF NEONATOLOGY Neonatal gastric perforation September 2002 2 Zankl A, Stähelin J, Roth K, Boudny P and Zeilinger G, Children s Hospital of Aarau (ZA, SJ, RK, ZG) and Institute of Pathology
Organic acidaemias (OAs) & Urea cycle disorders (UCDs) PRESENTATION & MANAGEMENT
 & Urea cycle disorders (UCDs) PRESENTATION & MANAGEMENT") Great Ormond Street Hospital London 20/04/2018 Organic acidaemias (OAs) & Urea cycle disorders (UCDs) PRESENTATION & MANAGEMENT Spyros P. Batzios, MD, MSc, PhD OAs & UCDs How do they present? neonatal
Great Ormond Street Hospital London 20/04/2018 Organic acidaemias (OAs) & Urea cycle disorders (UCDs) PRESENTATION & MANAGEMENT Spyros P. Batzios, MD, MSc, PhD OAs & UCDs How do they present? neonatal
NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY
 & COOLING THERAPY") Background NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY A perinatal hypoxic-ischaemic insult may present with varying degrees of neonatal encephalopathy, neurological disorder and
Background NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY A perinatal hypoxic-ischaemic insult may present with varying degrees of neonatal encephalopathy, neurological disorder and
SWISS SOCIETY OF NEONATOLOGY. Diagnostic evaluation of a symptomatic cerebrovascular accident in a neonate with focal convulsions
 SWISS SOCIETY OF NEONATOLOGY Diagnostic evaluation of a symptomatic cerebrovascular accident in a neonate with focal convulsions July 2013 2 Anderson S, Rimensberger P, Service de Néonatologie et des Soins
SWISS SOCIETY OF NEONATOLOGY Diagnostic evaluation of a symptomatic cerebrovascular accident in a neonate with focal convulsions July 2013 2 Anderson S, Rimensberger P, Service de Néonatologie et des Soins
ARGININOSUCCINIC ACIDEMIA (or ARGININOSUCCINATE LYASE DEFICIENCY) RECOMMENDATIONS ON EMERGENCY MANAGEMENT OF METABOLIC DISEASES
 RECOMMENDATIONS ON EMERGENCY MANAGEMENT OF METABOLIC DISEASES") ARGININOSUCCINIC ACIDEMIA (or ARGININOSUCCINATE LYASE DEFICIENCY) RECOMMENDATIONS ON EMERGENCY MANAGEMENT OF METABOLIC DISEASES Patient s name: Date of birth: Please read carefully. Meticulous and prompt
ARGININOSUCCINIC ACIDEMIA (or ARGININOSUCCINATE LYASE DEFICIENCY) RECOMMENDATIONS ON EMERGENCY MANAGEMENT OF METABOLIC DISEASES Patient s name: Date of birth: Please read carefully. Meticulous and prompt
Scottish Medicines Consortium
 Scottish Medicines Consortium carglumic acid 200mg dispersible tablets (Carbaglu ) No. 299/06 Orphan Europe 8 September 2006 The Scottish Medicines Consortium (SMC) has completed its assessment of the
Scottish Medicines Consortium carglumic acid 200mg dispersible tablets (Carbaglu ) No. 299/06 Orphan Europe 8 September 2006 The Scottish Medicines Consortium (SMC) has completed its assessment of the
ETIOLOGY AND PATHOGENESIS OF HYPOXIC-ISCHEMIC ENCEPHALOPATHY
 ETIOLOGY AND PATHOGENESIS OF HYPOXIC-ISCHEMIC ENCEPHALOPATHY HYPOXIC-ISCHEMIC ENCEPHALOPATHY Hypoxic-İschemic Encephalopathy Encephalopathy due to hypoxic-ischemic injury [Hypoxic-ischemic encephalopathy
ETIOLOGY AND PATHOGENESIS OF HYPOXIC-ISCHEMIC ENCEPHALOPATHY HYPOXIC-ISCHEMIC ENCEPHALOPATHY Hypoxic-İschemic Encephalopathy Encephalopathy due to hypoxic-ischemic injury [Hypoxic-ischemic encephalopathy
Ornithine Transcarbamylase Deficiency (OTCD) Recommendations on Emergency Management of Metabolic Disease
 Recommendations on Emergency Management of Metabolic Disease") Ornithine Transcarbamylase Deficiency (OTCD) Recommendations on Emergency Management of Metabolic Disease Patient s Name: Date of Birth: MRN in KFSH&RC: Please read carefully. Meticulous and prompt treatment
Ornithine Transcarbamylase Deficiency (OTCD) Recommendations on Emergency Management of Metabolic Disease Patient s Name: Date of Birth: MRN in KFSH&RC: Please read carefully. Meticulous and prompt treatment
Carbamoyl Phosphate Synthetase (code 50470) Notice of Assessment
 Notice of Assessment") Carbamoyl Phosphate Synthetase (code 50470) Notice of Assessment June 2013 DISCLAIMER: This document was originally drafted in French by the Institut national d'excellence en santé et en services sociaux
Carbamoyl Phosphate Synthetase (code 50470) Notice of Assessment June 2013 DISCLAIMER: This document was originally drafted in French by the Institut national d'excellence en santé et en services sociaux
Guideline for the diagnosis and management of isovaleryl-coa-dehydrogenase deficiency (isovaleric acidemia) - a systematic review -
 - a systematic review -") Guideline for the diagnosis and management of isovaleryl-coa-dehydrogenase deficiency (isovaleric acidemia) - a systematic review - Guideline development group International interdisciplinary guideline
Guideline for the diagnosis and management of isovaleryl-coa-dehydrogenase deficiency (isovaleric acidemia) - a systematic review - Guideline development group International interdisciplinary guideline
Work-Up and Initial Management of Common Metabolic Emergencies in the Inpatient Setting
 Work-Up and Initial Management of Common Metabolic Emergencies in the Inpatient Setting Kristin Lindstrom, MD Division of Genetics and Metabolism Phoenix Children s Hospital AzAAP Pediatrics in the Red
Work-Up and Initial Management of Common Metabolic Emergencies in the Inpatient Setting Kristin Lindstrom, MD Division of Genetics and Metabolism Phoenix Children s Hospital AzAAP Pediatrics in the Red
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC
, RN, RNC-NIC") Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
Evidence-Based Update: Using Glucose Gel to Treat Neonatal Hypoglycemia
 Neonatal Nursing Education Brief: Evidence-Based Update: Using Glucose Gel to Treat Neonatal Hypoglycemia http://www.seattlechildrens.org/healthcare-professionals/education/continuing-medicalnursing-education/neonatal-nursing-education-briefs/
Neonatal Nursing Education Brief: Evidence-Based Update: Using Glucose Gel to Treat Neonatal Hypoglycemia http://www.seattlechildrens.org/healthcare-professionals/education/continuing-medicalnursing-education/neonatal-nursing-education-briefs/
Basal Ganglia Involvement in Mitochondrial Acetoacetyl-CoA Thiolase deficiency (T2).
.") Basal Ganglia Involvement in Mitochondrial Acetoacetyl-CoA Thiolase deficiency (T2). Stéphanie Paquay Robert Debré Hospital Reference Center For Metabolic Diseases Paris, France Mitochondrial Acetoacetyl-CoA
Basal Ganglia Involvement in Mitochondrial Acetoacetyl-CoA Thiolase deficiency (T2). Stéphanie Paquay Robert Debré Hospital Reference Center For Metabolic Diseases Paris, France Mitochondrial Acetoacetyl-CoA
Senior Vice President, Medical Affairs and Health Outcomes, 150 South Saunders Road, Lake Forest, IL 60045, Horizon Pharma USA, Inc, USA
 Research Hyperammonemic crises in patients with urea cycle disorders on chronic nitrogen scavenger therapy with either sodium phenylbutyrate or glycerol phenylbutyrate Jeffrey D Kent 1, Robert J Holt,2
Research Hyperammonemic crises in patients with urea cycle disorders on chronic nitrogen scavenger therapy with either sodium phenylbutyrate or glycerol phenylbutyrate Jeffrey D Kent 1, Robert J Holt,2
Amino Acid Metabolism
 Amino Acid Metabolism The continuous degradation and synthesis of cellular proteins occur in all forms of life. Each day humans turn over 1 2% of their total body protein, principally muscle protein. Approximately
Amino Acid Metabolism The continuous degradation and synthesis of cellular proteins occur in all forms of life. Each day humans turn over 1 2% of their total body protein, principally muscle protein. Approximately
Urea is the major end product of nitrogen catabolism in humans One nitrogen free NH3 other nitrogen aspartate. carbon oxygen CO2 liver,
 Urea is the major end product of nitrogen catabolism in humans Urea is the major disposal form of amino groups derived from amino acids, and accounts about 90% percent of the nitrogencontaining components
Urea is the major end product of nitrogen catabolism in humans Urea is the major disposal form of amino groups derived from amino acids, and accounts about 90% percent of the nitrogencontaining components
EU RISK MANAGEMENT PLAN (EU RMP) Nutriflex Omega peri emulsion for infusion , version 1.1
 Nutriflex Omega peri emulsion for infusion , version 1.1") EU RISK MANAGEMENT PLAN (EU RMP) Nutriflex Omega peri emulsion for infusion 13.7.2015, version 1.1 III.1. Elements for a Public Summary III.1.1. Overview of disease epidemiology Patients may need parenteral
EU RISK MANAGEMENT PLAN (EU RMP) Nutriflex Omega peri emulsion for infusion 13.7.2015, version 1.1 III.1. Elements for a Public Summary III.1.1. Overview of disease epidemiology Patients may need parenteral
Urea cycle disorders (UCD) compromise a group of inherited metabolic disorders with an estimated overall prevalence
 compromise a group of inherited metabolic disorders with an estimated overall prevalence") Early Clinical Manifestations and Eating Patterns in Patients with Urea Cycle Disorders Thatjana Gardeitchik, MD 1,2, Maureen Humphrey, APD 1,3, Judy Nation, APD 1,3, and Avihu Boneh, MD, PhD 1,4 Objectives
Early Clinical Manifestations and Eating Patterns in Patients with Urea Cycle Disorders Thatjana Gardeitchik, MD 1,2, Maureen Humphrey, APD 1,3, Judy Nation, APD 1,3, and Avihu Boneh, MD, PhD 1,4 Objectives
Neonatal Therapeutic Hypothermia. A Wasunna Professor of Neonatal Medicine and Pediatrics School of Medicine, University of Nairobi
 Neonatal Therapeutic Hypothermia A Wasunna Professor of Neonatal Medicine and Pediatrics School of Medicine, University of Nairobi Definition of Perinatal Asphyxia *No agreed universal definition ACOG/AAP
Neonatal Therapeutic Hypothermia A Wasunna Professor of Neonatal Medicine and Pediatrics School of Medicine, University of Nairobi Definition of Perinatal Asphyxia *No agreed universal definition ACOG/AAP
SWISS SOCIETY OF NEONATOLOGY. Prolonged arterial hypotension due to propofol used for endotracheal intubation in a newborn infant
 SWISS SOCIETY OF NEONATOLOGY Prolonged arterial hypotension due to propofol used for endotracheal intubation in a newborn infant July 2001 2 Wagner B, Intensive Care Unit, University Children s Hospital
SWISS SOCIETY OF NEONATOLOGY Prolonged arterial hypotension due to propofol used for endotracheal intubation in a newborn infant July 2001 2 Wagner B, Intensive Care Unit, University Children s Hospital
Metabolic Disorders. Chapter Thomson - Wadsworth
 Metabolic Disorders Chapter 28 1 Metabolic Disorders Inborn errors of metabolism group of diseases that affect a wide variety of metabolic processes; defective processing or transport of amino acids, fatty
Metabolic Disorders Chapter 28 1 Metabolic Disorders Inborn errors of metabolism group of diseases that affect a wide variety of metabolic processes; defective processing or transport of amino acids, fatty
Neonatal Seizure. Dr.Nawar Yahya. Presented by: Sarah Khalil Zeina Shamil Zainab Waleed Zainab Qahtan. Supervised by:
 Neonatal Seizure Supervised by: Dr.Nawar Yahya Presented by: Sarah Khalil Zeina Shamil Zainab Waleed Zainab Qahtan Objectives: What is neonatal seizure Etiology Clinical presentation Differential diagnosis
Neonatal Seizure Supervised by: Dr.Nawar Yahya Presented by: Sarah Khalil Zeina Shamil Zainab Waleed Zainab Qahtan Objectives: What is neonatal seizure Etiology Clinical presentation Differential diagnosis
Introduction to Organic Acidemias. Hilary Vernon, MD PhD Assistant Professor of Genetic Medicine Johns Hopkins University 7.25.
 Introduction to Organic Acidemias Hilary Vernon, MD PhD Assistant Professor of Genetic Medicine Johns Hopkins University 7.25.2014 A Brief Historical Overview Garrod, Archibald E. 1902. The Incidence of
Introduction to Organic Acidemias Hilary Vernon, MD PhD Assistant Professor of Genetic Medicine Johns Hopkins University 7.25.2014 A Brief Historical Overview Garrod, Archibald E. 1902. The Incidence of
Hyperammonemia: Diagnostic Experience At The Metabolism Laboratory
 ISPUB.COM The Internet Journal of Laboratory Medicine Volume 1 Number 2 Hyperammonemia: Diagnostic Experience At The Metabolism Laboratory A Rao, P Varma, Sumitra, S Dhanya Citation A Rao, P Varma, Sumitra,
ISPUB.COM The Internet Journal of Laboratory Medicine Volume 1 Number 2 Hyperammonemia: Diagnostic Experience At The Metabolism Laboratory A Rao, P Varma, Sumitra, S Dhanya Citation A Rao, P Varma, Sumitra,
Neonatal Hypoglycaemia
 Neonatal Hypoglycaemia Dr Shubha Srinivasan Paediatric Endocrinologist The Children s Hospital at Westmead Hypoglycaemia and the Brain CSF glucose is 2/3 that of plasma Intracerebral glucose 1/3 that of
Neonatal Hypoglycaemia Dr Shubha Srinivasan Paediatric Endocrinologist The Children s Hospital at Westmead Hypoglycaemia and the Brain CSF glucose is 2/3 that of plasma Intracerebral glucose 1/3 that of
NEONATAL SEIZURES-PGPYREXIA REVIEW
 NEONATAL SEIZURES-PGPYREXIA REVIEW This is a very important Postgraduate topics will few Q asked in undergraduation also. Lets see them in detail. References: 1.Volpe s Neurology of newborn 2.Nelson s
NEONATAL SEIZURES-PGPYREXIA REVIEW This is a very important Postgraduate topics will few Q asked in undergraduation also. Lets see them in detail. References: 1.Volpe s Neurology of newborn 2.Nelson s
No social problems noted No past med hx Mother had spontaneous rupture of fetal membranes SB born on Needed to be resuscitated at birth
 No social problems noted No past med hx Mother had spontaneous rupture of fetal membranes SB born on 9-16-2011 Needed to be resuscitated at birth (included assisted vent) Had generalized edema and possible
No social problems noted No past med hx Mother had spontaneous rupture of fetal membranes SB born on 9-16-2011 Needed to be resuscitated at birth (included assisted vent) Had generalized edema and possible
SWISS SOCIETY OF NEONATOLOGY. Potentially fatal complications of peripherally inserted central venous catheters (PICCs)
") SWISS SOCIETY OF NEONATOLOGY Potentially fatal complications of peripherally inserted central venous catheters (PICCs) October 2001 2 Berger TM, Neonatal and Pediatric Intensive Care Unit, Children s Hospital
SWISS SOCIETY OF NEONATOLOGY Potentially fatal complications of peripherally inserted central venous catheters (PICCs) October 2001 2 Berger TM, Neonatal and Pediatric Intensive Care Unit, Children s Hospital
Drug-induced Hyperammonemia (HA)
") Drug-induced hyperammonemia: are there specific therapies? NACCT Boston 2016 Florian Eyer Department of Clinical Toxicology & Poison Control Centre Munich TUM School of Medicine Technical University of
Drug-induced hyperammonemia: are there specific therapies? NACCT Boston 2016 Florian Eyer Department of Clinical Toxicology & Poison Control Centre Munich TUM School of Medicine Technical University of
Difficulties at Birth: Long Term Developmental Outcomes
 Difficulties at Birth: Long Term Developmental Outcomes Alan D. Bedrick MD Division of Neonatology and Developmental Biology Department of Pediatrics University of Arizona Tucson, Arizona DISCLOSURE I
Difficulties at Birth: Long Term Developmental Outcomes Alan D. Bedrick MD Division of Neonatology and Developmental Biology Department of Pediatrics University of Arizona Tucson, Arizona DISCLOSURE I
Volume 3 (2017) Issue 10 ISSN Keywords. Introduction. Case Report. Open Journal of Clinical & Medical Case Reports
 Issue 10 ISSN Keywords. Introduction. Case Report. Open Journal of Clinical & Medical Case Reports") Open Journal of Clinical & Medical Case Reports Volume 3 (2017) Issue 10 ISSN 2379-1039 Recurrent hyperammonemia in an 80-year-old woman with congenital urea cycle abnormality Junji Yamaguchi, MD*; Koichi
Open Journal of Clinical & Medical Case Reports Volume 3 (2017) Issue 10 ISSN 2379-1039 Recurrent hyperammonemia in an 80-year-old woman with congenital urea cycle abnormality Junji Yamaguchi, MD*; Koichi
Metabolic Changes in ASD. Norma J. Arciniegas, MD Simón E. Carlo, MD Instituto Filius
 Metabolic Changes in ASD Norma J. Arciniegas, MD Simón E. Carlo, MD Instituto Filius 12 patients 3 Autism: Ages 3/3/3.7 3 PDD: Ages 3/3/6 3 Asperger: Ages 6/7/15.1 3 Speech delay and Sensory Problems (SHL):
Metabolic Changes in ASD Norma J. Arciniegas, MD Simón E. Carlo, MD Instituto Filius 12 patients 3 Autism: Ages 3/3/3.7 3 PDD: Ages 3/3/6 3 Asperger: Ages 6/7/15.1 3 Speech delay and Sensory Problems (SHL):
3 HYDROXY 3 METHYLGLUTARYL CoA (3 HMG CoA) LYASE DEFICIENCY RECOMMENDATIONS ON EMERGENCY MANAGEMENT OF METABOLIC DISEASES
 LYASE DEFICIENCY RECOMMENDATIONS ON EMERGENCY MANAGEMENT OF METABOLIC DISEASES") 3 HYDROXY 3 METHYLGLUTARYL CoA (3 HMG CoA) LYASE DEFICIENCY RECOMMENDATIONS ON EMERGENCY MANAGEMENT OF METABOLIC DISEASES Patient s name: Date of birth: Please read carefully. Meticulous and prompt treatment
3 HYDROXY 3 METHYLGLUTARYL CoA (3 HMG CoA) LYASE DEFICIENCY RECOMMENDATIONS ON EMERGENCY MANAGEMENT OF METABOLIC DISEASES Patient s name: Date of birth: Please read carefully. Meticulous and prompt treatment
Hypoxic ischemic brain injury in neonates - early MR imaging findings
 Hypoxic ischemic brain injury in neonates - early MR imaging findings Poster No.: C-1208 Congress: ECR 2015 Type: Authors: Keywords: DOI: Educational Exhibit E.-M. Heursen, R. Reina Cubero, T. Guijo Hernandez,
Hypoxic ischemic brain injury in neonates - early MR imaging findings Poster No.: C-1208 Congress: ECR 2015 Type: Authors: Keywords: DOI: Educational Exhibit E.-M. Heursen, R. Reina Cubero, T. Guijo Hernandez,
New developments in Urea Cycle Disorders and its impact on patients
 New developments in Urea Cycle Disorders and its impact on patients Johannes Häberle University Children s Hospital Zurich, Division of Metabolism 16 June 2015 SFEIM 2015, Lille, France The urea cycle
New developments in Urea Cycle Disorders and its impact on patients Johannes Häberle University Children s Hospital Zurich, Division of Metabolism 16 June 2015 SFEIM 2015, Lille, France The urea cycle
Inborn Errors of Metabolism (IEM)
") Clinical Presentation Inborn Errors of Metabolism (IEM) Click on the following: - Clinical Pearl - link to movie clip - link to picture Investigations Blood Work Urine No Acidosis NH 4 + Metabolic Acidosis
Clinical Presentation Inborn Errors of Metabolism (IEM) Click on the following: - Clinical Pearl - link to movie clip - link to picture Investigations Blood Work Urine No Acidosis NH 4 + Metabolic Acidosis
Birth Asphyxia - Summary of the previous meeting and protocol overview
 Birth Asphyxia - Summary of the previous meeting and protocol overview Dr Ornella Lincetto, WHO Geneve Milano, 11June 2007 Vilka är Personality egenskaper med den astrologiska Tvillingarna? Objective of
Birth Asphyxia - Summary of the previous meeting and protocol overview Dr Ornella Lincetto, WHO Geneve Milano, 11June 2007 Vilka är Personality egenskaper med den astrologiska Tvillingarna? Objective of
TOXIC AND NUTRITIONAL DISORDER MODULE
 TOXIC AND NUTRITIONAL DISORDER MODULE Objectives: For each of the following entities the student should be able to: 1. Describe the etiology/pathogenesis and/or pathophysiology, gross and microscopic morphology
TOXIC AND NUTRITIONAL DISORDER MODULE Objectives: For each of the following entities the student should be able to: 1. Describe the etiology/pathogenesis and/or pathophysiology, gross and microscopic morphology
Inborn Errors of Metabolism in the Emergency Department. Will Davies June 2014
 Inborn Errors of Metabolism in the Emergency Department Will Davies June 2014 Inborn Errors of Metabolism in the Emergency Department Overview Although individually rare, altogether they are 1:1000-2500
Inborn Errors of Metabolism in the Emergency Department Will Davies June 2014 Inborn Errors of Metabolism in the Emergency Department Overview Although individually rare, altogether they are 1:1000-2500
Isovaleric Acidemia: Quick reference guide
 Isovaleric Acidemia: Quick reference guide Introduction Isovaleric acidemia (IVA) is an inborn error of the leucine pathway caused by defects of the isovaleryl-oadehydrogenase (IV). The clinical presentation
Isovaleric Acidemia: Quick reference guide Introduction Isovaleric acidemia (IVA) is an inborn error of the leucine pathway caused by defects of the isovaleryl-oadehydrogenase (IV). The clinical presentation
Case Report Extensive Cortical Diffusion Restriction in a 50-Year-Old Female with Hyperammonemic Encephalopathy and Status Epilepticus
 Case Reports in Neurological Medicine, Article ID 257094, 4 pages http://dx.doi.org/10.1155/2014/257094 Case Report Extensive Cortical Diffusion Restriction in a 50-Year-Old Female with Hyperammonemic
Case Reports in Neurological Medicine, Article ID 257094, 4 pages http://dx.doi.org/10.1155/2014/257094 Case Report Extensive Cortical Diffusion Restriction in a 50-Year-Old Female with Hyperammonemic
SWISS SOCIETY OF NEONATOLOGY. Vein of Galen aneurysm: Aneurysmal characteristics and clinical features as predictive factors
 SWISS SOCIETY OF NEONATOLOGY Vein of Galen aneurysm: Aneurysmal characteristics and clinical features as predictive factors April 2010 2 Pronzini F, Fontijn J, Fauchère JC, Bucher HU, Clinic of Neonatology,
SWISS SOCIETY OF NEONATOLOGY Vein of Galen aneurysm: Aneurysmal characteristics and clinical features as predictive factors April 2010 2 Pronzini F, Fontijn J, Fauchère JC, Bucher HU, Clinic of Neonatology,
Birth Asphyxia. Perinatal Depression. Birth Asphyxia. Risk Factors maternal. Risk Factors fetal. Risk Factors Intrapartum 2/12/2011
 Birth Asphyxia Perinatal Depression Sara Brown, ARNP Children s Hospital and Regional Medical Center May occur in utero, during labor/delivery or during the neonatal period Condition of impaired blood
Birth Asphyxia Perinatal Depression Sara Brown, ARNP Children s Hospital and Regional Medical Center May occur in utero, during labor/delivery or during the neonatal period Condition of impaired blood
SWISS SOCIETY OF NEONATOLOGY. Symptomatic congenital CMV infection after recurrent maternal infection
 SWISS SOCIETY OF NEONATOLOGY Symptomatic congenital CMV infection after recurrent maternal infection May 2017 Mack I, Burckhardt MA, Heininger U, Prüfer F, Wellmann S, Department of Pediatric Infectious
SWISS SOCIETY OF NEONATOLOGY Symptomatic congenital CMV infection after recurrent maternal infection May 2017 Mack I, Burckhardt MA, Heininger U, Prüfer F, Wellmann S, Department of Pediatric Infectious
Neonatal Hypoglycemia
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Neonatal Hypoglycemia. These podcasts are designed to give medical students an overview of key topics in pediatrics.
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Neonatal Hypoglycemia. These podcasts are designed to give medical students an overview of key topics in pediatrics.
Should infants with perinatal thrombosis be screened for thrombophilia and treated by anticoagulants?
 Should infants with perinatal thrombosis be screened for thrombophilia and treated by anticoagulants? Shoshana Revel-Vilk, MD MSc Pediatric Hematology Center, Pediatric Hematology/Oncology Department,
Should infants with perinatal thrombosis be screened for thrombophilia and treated by anticoagulants? Shoshana Revel-Vilk, MD MSc Pediatric Hematology Center, Pediatric Hematology/Oncology Department,
Hypoxic-Ischemic Encephalopathy. TW de Witt University of Pretoria Department of Paediatrics Neonatology
 Hypoxic-Ischemic Encephalopathy TW de Witt University of Pretoria Department of Paediatrics Neonatology Background HIE remains a serious condition that causes significant mortality and longterm morbidity.
Hypoxic-Ischemic Encephalopathy TW de Witt University of Pretoria Department of Paediatrics Neonatology Background HIE remains a serious condition that causes significant mortality and longterm morbidity.
NEONATAL SEIZURE. IAP UG Teaching slides
 NEONATAL SEIZURE 1 INTRODUCTION One of the important neonatal neurological emergencies requiring immediate medical care. Contribute to significant morbidity and mortality Incidence is around 0.5 to 0.8%
NEONATAL SEIZURE 1 INTRODUCTION One of the important neonatal neurological emergencies requiring immediate medical care. Contribute to significant morbidity and mortality Incidence is around 0.5 to 0.8%
Neonatal Hypotonia. Encephalopathy acute No encephalopathy. Neurology Chapter of IAP
 The floppy infant assumes a frog legged position. On ventral suspension, the baby can not maintain limb posture against gravity and assumes the position of a rag doll. Encephalopathy acute No encephalopathy
The floppy infant assumes a frog legged position. On ventral suspension, the baby can not maintain limb posture against gravity and assumes the position of a rag doll. Encephalopathy acute No encephalopathy
Module : Clinical correlates of disorders of metabolism Block 3, Week 2
 Module : Clinical correlates of disorders of metabolism Block 3, Week 2 Department of Paediatrics and Child Health University of Pretoria Tutor : Prof DF Wittenberg : dwittenb@medic.up.ac.za Aim of this
Module : Clinical correlates of disorders of metabolism Block 3, Week 2 Department of Paediatrics and Child Health University of Pretoria Tutor : Prof DF Wittenberg : dwittenb@medic.up.ac.za Aim of this
ISOVALERIC ACIDAEMIA -ACUTE DECOMPENSATION (standard version)
") Contact Details Name: Hospital Telephone: This protocol has 5 pages ISOVALERIC ACIDAEMIA -ACUTE DECOMPENSATION (standard version) Please read carefully. Meticulous treatment is very important as there
Contact Details Name: Hospital Telephone: This protocol has 5 pages ISOVALERIC ACIDAEMIA -ACUTE DECOMPENSATION (standard version) Please read carefully. Meticulous treatment is very important as there
Study of role of MRI brain in evaluation of hypoxic ischemic encephalopathy
 Original article: Study of role of MRI brain in evaluation of hypoxic ischemic encephalopathy *Dr Harshad Bhagat, ** Dr Ravindra Kawade, ***Dr Y.P.Sachdev *Junior Resident, Department Of Radiodiagnosis,
Original article: Study of role of MRI brain in evaluation of hypoxic ischemic encephalopathy *Dr Harshad Bhagat, ** Dr Ravindra Kawade, ***Dr Y.P.Sachdev *Junior Resident, Department Of Radiodiagnosis,
The breakdown of fats to provide energy occurs in segregated membrane-bound compartments
 CPT1a deficiency The breakdown of fats to provide energy occurs in segregated membrane-bound compartments of the cell known as mitochondria. Carnitine palmitoyltransferase Ia (CPT1a) is a protein that
CPT1a deficiency The breakdown of fats to provide energy occurs in segregated membrane-bound compartments of the cell known as mitochondria. Carnitine palmitoyltransferase Ia (CPT1a) is a protein that
CLINICAL SIGNS SUGGESTIVE OF A NEUROMETABOLIC DISEASE. Bwee Tien Poll-The Amsterdam UMC The Netherlands
 CLINICAL SIGNS SUGGESTIVE OF A NEUROMETABOLIC DISEASE Bwee Tien Poll-The Amsterdam UMC The Netherlands FRAMEWORK OF PRINCIPALS 1. Problem-oriented clinical approach 2. Biomarkers in plasma, urine, CSF
CLINICAL SIGNS SUGGESTIVE OF A NEUROMETABOLIC DISEASE Bwee Tien Poll-The Amsterdam UMC The Netherlands FRAMEWORK OF PRINCIPALS 1. Problem-oriented clinical approach 2. Biomarkers in plasma, urine, CSF
Complete Recovery of Perfusion Abnormalities in a Cardiac Arrest Patient Treated with Hypothermia: Results of Cerebral Perfusion MR Imaging
 pissn 2384-1095 eissn 2384-1109 imri 2018;22:56-60 https://doi.org/10.13104/imri.2018.22.1.56 Complete Recovery of Perfusion Abnormalities in a Cardiac Arrest Patient Treated with Hypothermia: Results
pissn 2384-1095 eissn 2384-1109 imri 2018;22:56-60 https://doi.org/10.13104/imri.2018.22.1.56 Complete Recovery of Perfusion Abnormalities in a Cardiac Arrest Patient Treated with Hypothermia: Results
UNDERSTANDING UREA CYCLE DISORDERS
 UNDERSTANDING UREA CYCLE DISORDERS What is a urea cycle disorder? A urea cycle disorder is a genetic disease that affects how protein is broken down in the body. It is therefore classified as a metabolic
UNDERSTANDING UREA CYCLE DISORDERS What is a urea cycle disorder? A urea cycle disorder is a genetic disease that affects how protein is broken down in the body. It is therefore classified as a metabolic
INBORN ERRORS OF METABOLISM (IEM) IAP UG Teaching slides
 IAP UG Teaching slides") INBORN ERRORS OF METABOLISM (IEM) 1 OBJECTIVES What are IEMs? Categories When to suspect? History and clinical pointers Metabolic presentation Differential diagnosis Emergency and long term management
INBORN ERRORS OF METABOLISM (IEM) 1 OBJECTIVES What are IEMs? Categories When to suspect? History and clinical pointers Metabolic presentation Differential diagnosis Emergency and long term management
Rapid Regression of White Matter Changes in Hypoglycemic Encephalopathy
 www.ksmrm.org JKSMRM 18(4) : 357-361, 2014 pissn 1226-9751 / eissn 2288-3800 Case Report Rapid Regression of White Matter Changes in Hypoglycemic Encephalopathy Sang-wook Son, Kye-ho Lee, Dong-soo Yoo
www.ksmrm.org JKSMRM 18(4) : 357-361, 2014 pissn 1226-9751 / eissn 2288-3800 Case Report Rapid Regression of White Matter Changes in Hypoglycemic Encephalopathy Sang-wook Son, Kye-ho Lee, Dong-soo Yoo
Early Diffusion MR Imaging Findings and Short-Term Outcome in Comatose Patients with Hypoglycemia
 ORIGINAL RESEARCH K. Johkura Y. Nakae Y. Kudo T.N. Yoshida Y. Kuroiwa Early Diffusion MR Imaging Findings and Short-Term Outcome in Comatose Patients with Hypoglycemia BACKGROUND AND PURPOSE: The relationship
ORIGINAL RESEARCH K. Johkura Y. Nakae Y. Kudo T.N. Yoshida Y. Kuroiwa Early Diffusion MR Imaging Findings and Short-Term Outcome in Comatose Patients with Hypoglycemia BACKGROUND AND PURPOSE: The relationship
Guslihan Dasa Tjipta Division of Perinatology Department of Child Health Medical School University of Sumatera Utara
 Guslihan Dasa Tjipta Division of Perinatology Department of Child Health Medical School University of Sumatera Utara 1 Definition Perinatal asphyxia is a fetus/newborn, due to: is an insult to the Lack
Guslihan Dasa Tjipta Division of Perinatology Department of Child Health Medical School University of Sumatera Utara 1 Definition Perinatal asphyxia is a fetus/newborn, due to: is an insult to the Lack
Correlation of Neurodevelopmental Outcome and brain MRI/EEG findings in term HIE infants
 Correlation of Neurodevelopmental Outcome and brain MRI/EEG findings in term HIE infants Ajou University School of Medicine Department of Pediatrics Moon Sung Park M.D. Hee Cheol Jo, M.D., Jang Hoon Lee,
Correlation of Neurodevelopmental Outcome and brain MRI/EEG findings in term HIE infants Ajou University School of Medicine Department of Pediatrics Moon Sung Park M.D. Hee Cheol Jo, M.D., Jang Hoon Lee,
Inborn errors of metabolism
 ESPEN Congress Nice 2010 From child to adult nutrition Inborn errors of metabolism Pascal Crenn Inborn errors of metabolism: from child to adult Pascal Crenn Hôpital Raymond Poincaré 92380 Garches. France
ESPEN Congress Nice 2010 From child to adult nutrition Inborn errors of metabolism Pascal Crenn Inborn errors of metabolism: from child to adult Pascal Crenn Hôpital Raymond Poincaré 92380 Garches. France
State of Florida Hypothermia Protocol. Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology
 State of Florida Hypothermia Protocol Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. Entry Criteria 1. Gestational Age greater than or equal to 35 weeks gestation
State of Florida Hypothermia Protocol Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. Entry Criteria 1. Gestational Age greater than or equal to 35 weeks gestation
Medical Foods for Inborn Errors of Metabolism
 Medical Foods for Inborn Errors of Metabolism Policy Number: Original Effective Date: MM.02.014 02/18/2000 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST 08/23/2013 Section: Medicine Place(s)
Medical Foods for Inborn Errors of Metabolism Policy Number: Original Effective Date: MM.02.014 02/18/2000 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST 08/23/2013 Section: Medicine Place(s)
Study of renal functions in neonatal asphyxia
 Original article: Study of renal functions in neonatal asphyxia *Dr. D.Y.Shrikhande, **Dr. Vivek Singh, **Dr. Amit Garg *Professor and Head, **Senior Resident Department of Pediatrics, Pravara Institute
Original article: Study of renal functions in neonatal asphyxia *Dr. D.Y.Shrikhande, **Dr. Vivek Singh, **Dr. Amit Garg *Professor and Head, **Senior Resident Department of Pediatrics, Pravara Institute
Too Cool? Hypoxic Ischemic Encephalopathy and Therapeutic Hypothermia. Lauren Sacco DNP, ARNP, NNP-BC
 Too Cool? Hypoxic Ischemic Encephalopathy and Therapeutic Hypothermia Lauren Sacco DNP, ARNP, NNP-BC Pathophysiology of HIE Occurs in two energy failure phases: First phase happens during the initial insult
Too Cool? Hypoxic Ischemic Encephalopathy and Therapeutic Hypothermia Lauren Sacco DNP, ARNP, NNP-BC Pathophysiology of HIE Occurs in two energy failure phases: First phase happens during the initial insult
Neonatal Hypoglycaemia Guidelines
 N.B. Staff should be discouraged from printing this document. This is to avoid the risk of out of date printed versions of the document. The Intranet should be referred to for the current version of the
N.B. Staff should be discouraged from printing this document. This is to avoid the risk of out of date printed versions of the document. The Intranet should be referred to for the current version of the
Subcutaneous fat necrosis of the newborn
 SWISS SOCIETY OF NEONATOLOGY Winner of the Case of the Year Award 2003 Subcutaneous fat necrosis of the newborn February 2003 2 Schulzke S, Fahnenstich H, Büchner S, Department of Neonatology (SS, FH),
SWISS SOCIETY OF NEONATOLOGY Winner of the Case of the Year Award 2003 Subcutaneous fat necrosis of the newborn February 2003 2 Schulzke S, Fahnenstich H, Büchner S, Department of Neonatology (SS, FH),
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University
 Dr Mubarak Abdelrahman Assistant Professor Jazan University") Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
SWISS SOCIETY OF NEONATOLOGY. Hypertrophic pyloric stenosis in a preterm infant
 SWISS SOCIETY OF NEONATOLOGY Hypertrophic pyloric stenosis in a preterm infant February 2014 2 Georgi R, Berger M, Schnyder I, Berger S, McDougall J, Division of Neonatology (GR, BM, McDJ), Department
SWISS SOCIETY OF NEONATOLOGY Hypertrophic pyloric stenosis in a preterm infant February 2014 2 Georgi R, Berger M, Schnyder I, Berger S, McDougall J, Division of Neonatology (GR, BM, McDJ), Department
Metabolic diseases of the liver
 Metabolic diseases of the liver Central role in metabolism Causes and mechanisms of dysfunction Clinical patterns of metabolic disease Clinical approach to problem-solving Specific disorders Liver s central
Metabolic diseases of the liver Central role in metabolism Causes and mechanisms of dysfunction Clinical patterns of metabolic disease Clinical approach to problem-solving Specific disorders Liver s central
ANATOMY OF A METABOLIC CRISIS: FAOD-style. Mark S. Korson, MD Tufts Medical Center Boston, MA
 ANATOMY OF A METABOLIC CRISIS: FAOD-style Mark S. Korson, MD Tufts Medical Center Boston, MA NORMAL PHYSIOLOGY Anabolic Eating well Calories eaten > body s needs BRAIN uses GLUCOSE MUSCLE uses GLUCOSE
ANATOMY OF A METABOLIC CRISIS: FAOD-style Mark S. Korson, MD Tufts Medical Center Boston, MA NORMAL PHYSIOLOGY Anabolic Eating well Calories eaten > body s needs BRAIN uses GLUCOSE MUSCLE uses GLUCOSE