Pediatric Mysteries (including FWS / FUO) 13 June 2017 Tony Moody MD Duke Pediatric Infectious Diseases
|
|
|
- Chloe Daniel
- 6 years ago
- Views:
Transcription

1 Pediatric Mysteries (including FWS / FUO) 13 June 2017 Tony Moody MD Duke Pediatric Infectious Diseases
2 Disclosures Advisory board member for GSK (for belimumab pregnancy registry). Co-founder of Grid Therapeutics (formerly Cue Biologics). Chief Medical Officer, DHVI. 2
3 Learning Objectives Describe the differences between FUO and FWS. Recommend appropriate diagnostic tests for these conditions. Prescribe appropriate therapy. 3
4 What I will talk about Fever without source (FWS) Fever of unknown origin (FUO) Recurrent infections
5 Case 1 10 yo with recurrent fevers to 102 F daily for six weeks also has generalized malaise unusual rash on legs good workup by PMD family worried
6 Case 2 8 mo with third episode of pneumonia growth reasonable no FHx of recurrent illnesses CXR with multifocal infiltrates PMD worried
7 Case 3 5 yo with daily fevers increasing in height for four weeks some cervical lymphadenopathy tired look initial lab work normal weight curve has flattened
8 Commonalities in each case symptoms not explained by typical childhood illness patterns persistence beyond the norm ain t right
9 Definitions fever without source (FWS) fever of recent onset no adequate explanation based on history and physical exam
10 Definitions fever without source (FWS) fever without localizing signs
11 Definitions fever of unknown origin (FUO) fever of >7 days duration no diagnosis after initial work-up
12 The Distinction FWS vs. FUO differential diagnoses different needs more immediate evaluation can take a more thoughtful approach
13 FWS fever without source (FWS) fever of recent onset (<1 week)
14 FWS fever without source (FWS) no adequate explanation based on history and physical exam (should be careful H+P)
15 FWS Epidemiology 5-10% (22%) of children with fever lack localizing signs peak incidence in 2 nd year of life estimated a practicing pediatrician sees this once every 4-5 days
16 FWS some are presenting with a new chronic illness some are gravely ill most are not
17 FWS the evaluation is a bit like panning for gold you must always pay attention!
18 FUO FUOs are different you are out of the acute stage you have already done a work-up
19 FUO two approaches to further work-up test for everything at once test in a stepwise fashion
20 FUO Epidemiology most have uncommon presentations of common illnesses case series only 5 of 418 had rare disorder
21 FUO Epidemiology most series state that 10-20% of cases never get a diagnosis (50%) unlike adults, most children get better
22 FUO in cases of FUO, three services are routinely consulted Infectious Diseases Rheumatology Hematology/Oncology
23 Infectious Diseases Hematology/ Oncology Rheumatology
24 FUO Epidemiology most case series report that diagnoses are infectious > rheumatologic > oncologic
25 FWS & FUO direct your work-up with two principles in mind 1. Look for things that are common. 2. Look for things that will kill you.
26 FWS Rational Work-up historically, two worrisome illnesses meningitis bacteremia and a third (UTI) that could be hard to diagnose
27 Bacterial disease in FWS neonates (0-3 months) Streptococcus agalactiae Escherichia coli Listeria monocytogenes
28 Bacterial disease in FWS infant / toddler (3 mos to 3 yrs) Haemophilus influenzae type B Streptococcus pneumoniae Neisseria meningitidus
29 Bacterial disease in FWS children / adolescents (3-19+ yrs) Streptococcus pneumoniae Neisseria meningitidus
30 Historical FWS historically, 3-5% of children with FWS had bacteremia and, 5-10% of those would develop meningitis if not treated
31 Historical FWS historically, 3-5% of children with FWS had bacteremia plus, 10% would develop a localized infection
32 Historical FWS historically, 3-5% of children with FWS had bacteremia and, 30% would have persistence of bacteremia
33 Historical FWS historically, 3-5% of children with FWS had bacteremia overall badness rate of %
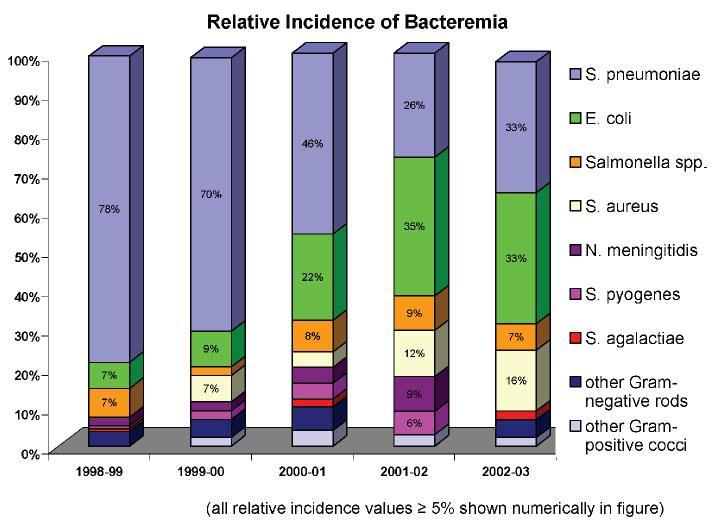
34 Shifting FWS we now have excellent vaccine coverage against Haemophilus influenzae type B Streptococcus pneumoniae
35
36
37
38
39 Current FWS now <1% of children with FWS have bacteremia, and risk of complications lower badness rate <<1%
40
41
42

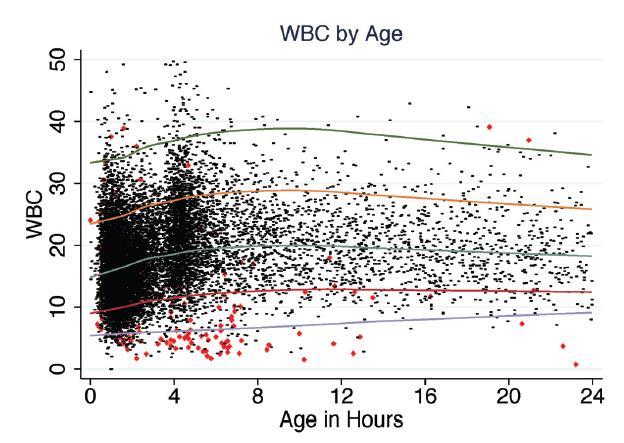
43 WBC ANC I/T Plt
44
45 FWS Work-up after careful H+P for everyone blood culture, CBC/D
46
47
48
49 FWS Work-up after careful H+P for girls <2yo, boys <6mo (to 1yo if uncircumcised) urine culture, U/A
50 FWS Work-up after careful H+P if <3mo, if suspicion, if exposed CSF culture, CSF analysis
51 FWS Work-up after careful H+P consider a CXR
52 FWS Empirical Tx if work-up is unrevealing, consider antibiotic therapy
53 FWS Empirical Tx consider antibiotic therapy if unsure of follow-up unsure of reliability no relationship with family
54 FWS Antibiotics ceftriaxone and daily follow-up orals in select cases
55 FUO Rational Work-up patient should have already had blood culture, CBC/D urine culture, U/A CXR
56 FUO Rational Work-up what now makes the list of things that are common, or things that could kill you?
57 FUO Rational Work-up Rheumatology send ESR, CRP consider ANA unless obvious disease, I don t push beyond this
58 FUO Rational Work-up Hematology/Oncology repeat CBC + manual differential send chemistries, including Ca and uric acid call H/O, discuss BM
59 FUO Rational Work-up Infectious Diseases serial blood cultures (endocarditis) place PPD (tuberculosis) send viral studies (sinus, pharynx, stool, urine) send complement (CH50)
60 FUO Rational Work-up Infectious Diseases, p2 consider imaging bone scan (osteomyelitis) MRI (bones, joints) CT (occult abscesses)
61 FUO Rational Work-up Infectious Diseases, p3 consider cardiology (Kawasaki) consider unusual cultures / tests Brucella, MOTT, Bartonella, Francisella, HACEK, Mycoplasma, etc.
62 FUO Rational Work-up Infectious Diseases, p4 every child getting an FUO w/u should get HIV testing!!!
63 FUO Rational Work-up Infectious Diseases, p5 never forget STIs send RPR, culture for GC, culture for Chlamydia
64 FUO Rational Work-up Infectious Diseases, p6 culture any site / fluid / tissue you can
65 FUO Further Work-up zebras are just that, uncommon don t send tests for unusual genetic disorders unless the history dictates it
66 FUO Empirical Tx in general, NONE
67 FUO Empirical Tx we know that 1. most children will get better 2. most children have common illnesses 3. it hasn t killed them yet!
68 FUO Empirical Tx giving antibiotics to a child with FUO, especially after it has been going on for a while, is like shooting a gun into a dark room (please just send them to ID clinic)
69 Finally when is it too much? my kid has a cold constantly my kid has had three pneumonias this year my kid has had pneumonia and meningitis and a joint infection
70 Immune Deficiency these are uncommon, but you will see them never forget HIV!!! and consider SCID, CGD, digeorge, etc.
71 Immune Deficiency context is everything daycare? playmates? family history? siblings? underlying disorders? past history?
72 Finally when is it too much? my kid has a cold constantly (probably daycare)
73 Finally when is it too much? my kid has had three pneumonias this year (worrisome, asthma?)
74 Finally when is it too much? my kid has had pneumonia and meningitis and a joint infection (ain t right)
75 Case 1 10 yo with recurrent fevers to 102 F daily for six weeks also has generalized malaise unusual rash on legs good workup by PMD family worried
76 Case 2 8 mo with third episode of pneumonia growth reasonable no FHx of recurrent illnesses CXR with multifocal infiltrates PMD worried
77 Case 3 5 yo with daily fevers increasing in height for four weeks some cervical lymphadenopathy tired look initial lab work normal weight curve has flattened
78 Final Word Please call. Seriously. We love this stuff. Fellow pager (inpatient) / (outpatient) consults / questions ( )
79

80 ID Emergencies in Pediatrics 13 June 2017 Tony Moody MD Duke Pediatric Infectious Diseases
81 Goals discuss infections that can kill or maim without prompt attention outline presentation, labs needed, interventions needed
82 Case 1 You are in the ED on Wednesday, near the end of your shift. You are asked to eyeball an 11 mo with decreased feeding and urination, fever and lethargy, all with sudden onset. On exam you see a rash on with small, non-blanching, red macules with dark centers.


83
84 Case 1 Your next action for this patient should be A. diagnose a viral illness and discharge B. obtain a blood culture C. perform a lumbar puncture D. administer ceftriaxone IM.
85 Case 1½ Children in his daycare room should A. receive routine care B. receive vaccination against pneumococcus C. receive rifampin prophylaxis D. have lumbar punctures performed.
86 Case 2 On Thursday, you see a 6yo with 3 days of fever & sore throat. Her mother reports a red, raised rash. You find HR 120, T 39. Her L leg below the knee is swollen. She is crying and inconsolable.
87 Case 2 Your next action for this patient should be A. LA Bicillin for strep throat B. start oral penicillin C. start IV penicillin and clindamycin D. call for a surgical consult.
88 Case 3 On Friday, you see a 20mo with a 2 day history of fever & fussiness. Her mother notes the child is refusing to walk and is fussy with diaper changes. You see a child with T 38.5 and holding her R leg flexed and externally rotated.
89 Case 3 Your next action for this patient should be A. call for an orthopedic consult B. call radiology for a hip ultrasound C. start meropenem D. diagnose toxic synovitis and discharge on NSAIDs.
90 Case 4 On Sunday, you see a 5yo with 3-4 days of congestion / rhinorrhea. This morning his mother noted the acute onset of R eye swelling. On exam you see tense edema of the eyelid with proptosis, lateral gaze paralysis, conjunctival injection.
91 Case 4 Your next action for this patient should be A. IVIG infusion B. Call ENT / Ophtho C. start 3 rd generation cephalosporin D. thyroid studies.
92 Case 5 On Monday, you see a 2yo whose family are recovering from a flulike illness. He had been recovering until this morning when he developed a distressed look and high fever. On exam he has inspiratory stridor, retractions, and a normal O 2 saturation.
93 Case 5 Your next action for this patient should be A. Immediate intubation B. CXR C. Chest CT D. administer nebulized albuterol.
94 Case 5½ The CXR is shows no foreign body, little parenchymal disease. Now A. Immediate intubation B. start vancomycin C. Chest CT D. administer nebulized albuterol.
95 Case 6 In 1985, you see a 3yo who had mild fever and cough followed by the sudden onset of respiratory distress and irritability. She is hoarse, sitting in mother s lap, leaning forward, drooling, and has retractions.
96 Case 6 Your next action for this patient should be A. Immediate intubation by the intern B. CXR C. immediate intubation by an anesthesiologist D. start an IV for antibiotics.
Fever in the Newborn Period
 Fever in the Newborn Period 1. Definitions 1 2. Overview 1 3. History and Physical Examination 2 4. Fever in Infants Less than 3 Months Old 2 a. Table 1: Rochester criteria for low risk infants 3 5. Fever
Fever in the Newborn Period 1. Definitions 1 2. Overview 1 3. History and Physical Examination 2 4. Fever in Infants Less than 3 Months Old 2 a. Table 1: Rochester criteria for low risk infants 3 5. Fever
Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014
 Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014 Prep Question You are camping with a group of boys at a rural campground in the southeastern Unites States when one of the campers is bitten
Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014 Prep Question You are camping with a group of boys at a rural campground in the southeastern Unites States when one of the campers is bitten
Fevers and Seizures in Infants and Young Children
 Fevers and Seizures in Infants and Young Children Kellie Holtmeier, PharmD Pediatric Clinical Pharmacist University of New Mexico Hospital Disclosure I have no conflicts of interest 1 Pharmacist Objectives
Fevers and Seizures in Infants and Young Children Kellie Holtmeier, PharmD Pediatric Clinical Pharmacist University of New Mexico Hospital Disclosure I have no conflicts of interest 1 Pharmacist Objectives
Welcome to Big Sky Country. Pediatrics Infectious disease update. Todd TwogoodMD
 Welcome to Big Sky Country Pediatrics Infectious disease update Todd TwogoodMD My kid is always sick!! We have to deal with parents Snotty nose kids Average number of colds in children from Oct to March
Welcome to Big Sky Country Pediatrics Infectious disease update Todd TwogoodMD My kid is always sick!! We have to deal with parents Snotty nose kids Average number of colds in children from Oct to March
My kid is always sick!!
 Welcome to Big Sky Country My kid is always sick!! Pediatrics Infectious disease update Todd Twogood MD We have to deal with parents Snotty nose kids Average number of colds in children from Oct to March
Welcome to Big Sky Country My kid is always sick!! Pediatrics Infectious disease update Todd Twogood MD We have to deal with parents Snotty nose kids Average number of colds in children from Oct to March
EPG Clinical Guidelines
 Guidelines for the Management of Febrile Young Children Neonate age 7 days Temperature > 38 C, documented at home or in the ED Complete blood count with manual differential (CBCD), urinalysis (UA), urine
Guidelines for the Management of Febrile Young Children Neonate age 7 days Temperature > 38 C, documented at home or in the ED Complete blood count with manual differential (CBCD), urinalysis (UA), urine
4/14/2010. Theoretical purpose of fever? Andrea Marmor, MD, MSEd Assistant Clinical Professor, Pediatrics UCSF April 13, 2010
 Andrea Marmor, MD, MSEd Assistant Clinical Professor, Pediatrics UCSF April 13, 2010 Parental touch? Absence of fever more reliable than presence. Axillary and tympanic Vulnerable to environmental and
Andrea Marmor, MD, MSEd Assistant Clinical Professor, Pediatrics UCSF April 13, 2010 Parental touch? Absence of fever more reliable than presence. Axillary and tympanic Vulnerable to environmental and
GUIDELINE FOR THE MANAGEMENT OF MENINGITIS. All children with suspected or confirmed meningitis
 GUIDELINE FOR THE MANAGEMENT OF MENINGITIS Reference: Mennigitis Version No: 1 Applicable to All children with suspected or confirmed meningitis Classification of document: Area for Circulation: Author:
GUIDELINE FOR THE MANAGEMENT OF MENINGITIS Reference: Mennigitis Version No: 1 Applicable to All children with suspected or confirmed meningitis Classification of document: Area for Circulation: Author:
The McMaster at night Pediatric Curriculum
 The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
Hot Hot Tot:! The Hot Tot. Fever in KIds <90 Days 5/26/10
 Hot Hot Tot:! Fever in KIds
Hot Hot Tot:! Fever in KIds
Pediatric TB Lisa Armitige, MD, PhD September 28, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
Objectives. Case Presentation. Respiratory Emergencies
 Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
An Intriguing Case of Meningitis. Tiffany Mylius MLS (ASCP)
") An Intriguing Case of Meningitis { Tiffany Mylius MLS (ASCP) A 4yo male presents with 2wk history of URI symptoms. On the day of admission, the patient woke up with a HA in the morning, took a nap later
An Intriguing Case of Meningitis { Tiffany Mylius MLS (ASCP) A 4yo male presents with 2wk history of URI symptoms. On the day of admission, the patient woke up with a HA in the morning, took a nap later
Fever Without a Source Age: 0-28 Day Pathway - Emergency Department Evidence Based Outcome Center
 Age: 0-28 Day Pathway - Emergency Department EXCLUSION CRITERIA Toxic appearing No fever Born < 37 weeks gestational age INCLUSION CRITERIA Non-toxic with temperature > 38 C (100.4 F) < 36 C (96.5 F) measured
Age: 0-28 Day Pathway - Emergency Department EXCLUSION CRITERIA Toxic appearing No fever Born < 37 weeks gestational age INCLUSION CRITERIA Non-toxic with temperature > 38 C (100.4 F) < 36 C (96.5 F) measured
TB Intensive Houston, Texas. Childhood Tuberculosis Kim Connelly Smith. November 12, 2009
 TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
Evidence-based Management of Fever in Infants and Young Children
 Evidence-based Management of Fever in Infants and Young Children Shabnam Jain, MD, MPH Associate Professor of Pediatrics Emory University Medical Director for Clinical Effectiveness Objectives Understand
Evidence-based Management of Fever in Infants and Young Children Shabnam Jain, MD, MPH Associate Professor of Pediatrics Emory University Medical Director for Clinical Effectiveness Objectives Understand
Fever in neonates (age 0 to 28 days)
") Fever in neonates (age 0 to 28 days) INCLUSION CRITERIA Infant 28 days of life Temperature 38 C (100.4 F) by any route/parental report EXCLUSION CRITERIA Infants with RSV Febrile Infant 28 days old Ill
Fever in neonates (age 0 to 28 days) INCLUSION CRITERIA Infant 28 days of life Temperature 38 C (100.4 F) by any route/parental report EXCLUSION CRITERIA Infants with RSV Febrile Infant 28 days old Ill
3/25/2012. numerous micro-organismsorganisms
 Congenital & Neonatal TB A Case of Tuberculosis Congenital or Acquired? Felicia Dworkin, MD NYC DOHMH Bureau TB Control World TB Day March 23, 2012 Congenital TB: acquired by the fetus during pregnancy
Congenital & Neonatal TB A Case of Tuberculosis Congenital or Acquired? Felicia Dworkin, MD NYC DOHMH Bureau TB Control World TB Day March 23, 2012 Congenital TB: acquired by the fetus during pregnancy
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
FEVER. What is fever?
 FEVER What is fever? Fever is defined as a rectal temperature 38 C (100.4 F), and a value >40 C (104 F) is called hyperpyrexia. Body temperature fluctuates in a defined normal range (36.6-37.9 C [97.9-100.2
FEVER What is fever? Fever is defined as a rectal temperature 38 C (100.4 F), and a value >40 C (104 F) is called hyperpyrexia. Body temperature fluctuates in a defined normal range (36.6-37.9 C [97.9-100.2
Fever in Babies. Too much testing or not enough testing? Martin E. Weisse, M.D. Pediatric Infectious Diseases
 Fever in Babies Too much testing or not enough testing? Martin E. Weisse, M.D. Pediatric Infectious Diseases Disclosures I have nothing to disclose Learning Objectives At the end of the talk, participants
Fever in Babies Too much testing or not enough testing? Martin E. Weisse, M.D. Pediatric Infectious Diseases Disclosures I have nothing to disclose Learning Objectives At the end of the talk, participants
Fever in Children. Dr Shane George Staff Specialist - Emergency Medicine & Children s Critical Care Gold Coast University Hospital
 Fever in Children Dr Shane George Staff Specialist - Emergency Medicine & Children s Critical Care Gold Coast University Hospital Update on Children s services @ GCUH Dedicated Children s Pod in the Emergency
Fever in Children Dr Shane George Staff Specialist - Emergency Medicine & Children s Critical Care Gold Coast University Hospital Update on Children s services @ GCUH Dedicated Children s Pod in the Emergency
Fever. National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital
 Fever National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital Case 1 4-month-old well-appearing girl admitted for croup and respiratory distress.
Fever National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital Case 1 4-month-old well-appearing girl admitted for croup and respiratory distress.
Community Acquired Pneumonia
 April 2014 References: 1. Bradley JS, Byington CL, Shah SS, Alverson B, Carter ER, Harrison C, Kaplan SL Mace SE, McCracken Jr. GH, Moor MR, St. Peter SD, Stockwell JA, and Swanson JT. The Management of
April 2014 References: 1. Bradley JS, Byington CL, Shah SS, Alverson B, Carter ER, Harrison C, Kaplan SL Mace SE, McCracken Jr. GH, Moor MR, St. Peter SD, Stockwell JA, and Swanson JT. The Management of
Faculty Disclosure. Stephen I. Pelton, MD. Dr. Pelton has listed no financial interest/arrangement that would be considered a conflict of interest.
 Faculty Disclosure Stephen I. Pelton, MD Dr. Pelton has listed no financial interest/arrangement that would be considered a conflict of interest. Advances in the management of fever in infants 0 to 3 and
Faculty Disclosure Stephen I. Pelton, MD Dr. Pelton has listed no financial interest/arrangement that would be considered a conflict of interest. Advances in the management of fever in infants 0 to 3 and
EVALUATION OF A SICK CHILD WITH FEVER
 EVALUATION OF A SICK CHILD WITH FEVER Learning objectives At the conclusion of this learning activity, participants should be able to; Discuss the different etiologies of acute illness in a child Identify
EVALUATION OF A SICK CHILD WITH FEVER Learning objectives At the conclusion of this learning activity, participants should be able to; Discuss the different etiologies of acute illness in a child Identify
A Practical Approach to Leukopenia/Neutropenia in Children. Vandy Black, M.D., M.Sc., FAAP OLOL Children s Hospital August 24, 2014
 A Practical Approach to Leukopenia/Neutropenia in Children Vandy Black, M.D., M.Sc., FAAP OLOL Children s Hospital August 24, 2014 Disclosures EPIC trial MAST Therapeutics SUSTAIN trial Selexys Pharmaceuticals
A Practical Approach to Leukopenia/Neutropenia in Children Vandy Black, M.D., M.Sc., FAAP OLOL Children s Hospital August 24, 2014 Disclosures EPIC trial MAST Therapeutics SUSTAIN trial Selexys Pharmaceuticals
The Febrile Infant. SJRH ED Rounds Dec By: Robin Clouston
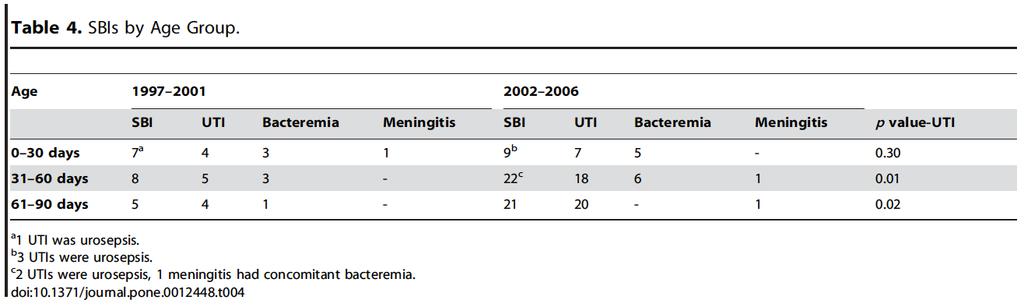
 1 The Febrile Infant SJRH ED Rounds Dec 11 2018 By: Robin Clouston 2 Objectives Discuss the risk of serious bacterial infection (SBI) in the neonate or young infant (
1 The Febrile Infant SJRH ED Rounds Dec 11 2018 By: Robin Clouston 2 Objectives Discuss the risk of serious bacterial infection (SBI) in the neonate or young infant (
Upper Airway Emergencies
 Upper Airway Emergencies Selena Hariharan, M.D. Assistant Professor of Pediatrics Division of Pediatric Emergency Medicine Cincinnati Children s Hospital Medical Center CASE # 1 A 9 year old boy, previously
Upper Airway Emergencies Selena Hariharan, M.D. Assistant Professor of Pediatrics Division of Pediatric Emergency Medicine Cincinnati Children s Hospital Medical Center CASE # 1 A 9 year old boy, previously
PNEUMONIA IN CHILDREN. IAP UG Teaching slides
 PNEUMONIA IN CHILDREN 1 INTRODUCTION 156 million new episodes / yr. worldwide 151 million episodes developing world 95% in developing countries 19% of all deaths in children
PNEUMONIA IN CHILDREN 1 INTRODUCTION 156 million new episodes / yr. worldwide 151 million episodes developing world 95% in developing countries 19% of all deaths in children
Fever and Infections in Pediatrics
 Fever and Infections in Pediatrics Dr. Todd Twogood 2019 update Big Sky Conference Pediatric Fever and illness The most common reason for children to be taken to the doctor for acute illness Major concern
Fever and Infections in Pediatrics Dr. Todd Twogood 2019 update Big Sky Conference Pediatric Fever and illness The most common reason for children to be taken to the doctor for acute illness Major concern
Assessment of limping child (beware the child who does not weight bear at all):
:") Department of Paediatrics Clinical Guideline Acutely Limping Child and Septic Arthritis Assessment of limping child (beware the child who does not weight bear at all): History Careful history of any significant
Department of Paediatrics Clinical Guideline Acutely Limping Child and Septic Arthritis Assessment of limping child (beware the child who does not weight bear at all): History Careful history of any significant
Osteomyelitis Samir S. Shah, MD, MSCE
 Osteomyelitis Samir S. Shah, MD, MSCE Professor, Department of Pediatrics University of Cincinnati College of Medicine Director, Division of Hospital Medicine Attending Physician in Infectious Diseases
Osteomyelitis Samir S. Shah, MD, MSCE Professor, Department of Pediatrics University of Cincinnati College of Medicine Director, Division of Hospital Medicine Attending Physician in Infectious Diseases
CNS Infections. Philip Gothard Consultant in Infectious Diseases Hospital for Tropical Diseases, London. Hammersmith Acute Medicine 2011
 CNS Infections Philip Gothard Consultant in Infectious Diseases Hospital for Tropical Diseases, London Hammersmith Acute Medicine 2011 Case 1 HISTORY 27y man Unwell 3 days Fever Headache Photophobia Previously
CNS Infections Philip Gothard Consultant in Infectious Diseases Hospital for Tropical Diseases, London Hammersmith Acute Medicine 2011 Case 1 HISTORY 27y man Unwell 3 days Fever Headache Photophobia Previously
SEPTIC ARTHRITIS. Dr Ahmed Husam Al Ahmed Rheumatologist SYRIA. University of Science and technology Hospital Sanaa Yemen 18/Dec/2014
 SEPTIC ARTHRITIS Dr Ahmed Husam Al Ahmed Rheumatologist SYRIA University of Science and technology Hospital Sanaa Yemen 18/Dec/2014 Objectives be able to define Septic Arthritis know what factors predispose
SEPTIC ARTHRITIS Dr Ahmed Husam Al Ahmed Rheumatologist SYRIA University of Science and technology Hospital Sanaa Yemen 18/Dec/2014 Objectives be able to define Septic Arthritis know what factors predispose
1. Introduction Algorithm: Infant with Fever 0-28 Days Algorithm: Infant with Fever Days...3
 These guidelines are designed to assist clinicians and are not intended to supplant good clinical judgement or to establish a protocol for all patients with this condition. MANAGEMENT OF FEVER 38 C (100.4F)
These guidelines are designed to assist clinicians and are not intended to supplant good clinical judgement or to establish a protocol for all patients with this condition. MANAGEMENT OF FEVER 38 C (100.4F)
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Student Guide Module 5: Management of Prevalent Infections in Children Following a Disaster
 Student Guide Module 5: Management of Prevalent Infections in Children Following a Disaster Objectives for this session Section I - Integrated Management of Childhood Illness (IMCI) Understand the IMCI
Student Guide Module 5: Management of Prevalent Infections in Children Following a Disaster Objectives for this session Section I - Integrated Management of Childhood Illness (IMCI) Understand the IMCI
Background. Background. Headache Examination. Headache History. Primary vs. Secondary Headaches. Headaches In Children: Why Worry?
 Background Headaches In Children: Why Worry? Marcy Yonker MD FAHS Associate Professor of Pediatrics University of Arizona Director, Pediatric Headache Program Phoenix Children s Hospital Headaches are
Background Headaches In Children: Why Worry? Marcy Yonker MD FAHS Associate Professor of Pediatrics University of Arizona Director, Pediatric Headache Program Phoenix Children s Hospital Headaches are
LABORATORY PROCEDURES IMAGING/RADIOLOGY PROCEDURES THERAPY GVH EMERGENCY DEPARTMENT PROCECURES
 PROCEDURE CHARGES / HOSPITAL may vary depending on circumstances. Prices subject to change. LABORATORY PROCEDURES Basic Metabolic Panel $112.00 80048 Comprehensive Metabolic Panel $140.00 80053 UA Micro
PROCEDURE CHARGES / HOSPITAL may vary depending on circumstances. Prices subject to change. LABORATORY PROCEDURES Basic Metabolic Panel $112.00 80048 Comprehensive Metabolic Panel $140.00 80053 UA Micro
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
General Medical Concerns
 General Medical Concerns General Medical Concerns Fred Reifsteck MD Head Team Physician University of Georgia Missed Time: school, work, practice, games Decreased Performance Physical/ Mental stress: New
General Medical Concerns General Medical Concerns Fred Reifsteck MD Head Team Physician University of Georgia Missed Time: school, work, practice, games Decreased Performance Physical/ Mental stress: New
11/9/2012. Group B Streptococcal Infections: Consensus and Controversies. Prevention of Early-Onset GBS Disease in the USA.
 Group B Streptococcal Infections: Consensus and Controversies Carol J. Baker, M.D. Professor of Pediatrics, Molecular Virology and Microbiology Executive Director, Center for Vaccine Awareness and Research
Group B Streptococcal Infections: Consensus and Controversies Carol J. Baker, M.D. Professor of Pediatrics, Molecular Virology and Microbiology Executive Director, Center for Vaccine Awareness and Research
TB Nurse Case Management San Antonio, Texas March 7 9, Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012
 TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
I have no disclosures
 Disclosures Streptococcal Pharyngitis: Update and Current Guidelines Richard A. Jacobs, MD, PhD Emeritus Professor of Medicine Division of Infectious Diseases I have no disclosures CID 2012:55;e 86-102
Disclosures Streptococcal Pharyngitis: Update and Current Guidelines Richard A. Jacobs, MD, PhD Emeritus Professor of Medicine Division of Infectious Diseases I have no disclosures CID 2012:55;e 86-102
USAID Health Care Improvement Project. pneumonia) respiratory infections through improved case management (amb/hosp)
 respiratory infections through improved case management (amb/hosp)") Improvement objective: : decrease morbidity and mortality due to acute upper (rhinitis, sinusitis, pharyngitis) and lower (bronchitis, pneumonia) respiratory infections through improved case management
Improvement objective: : decrease morbidity and mortality due to acute upper (rhinitis, sinusitis, pharyngitis) and lower (bronchitis, pneumonia) respiratory infections through improved case management
 Fever Phobia and the ED Doc Ran Goldman, MD (rgoldman@cw.bc.ca) BC Children s Hospital, Professor, University of British Columbia SLIDES ON : www.clinicalpeds.com/whistler Define Fever 38.0 o Doesn t
Fever Phobia and the ED Doc Ran Goldman, MD (rgoldman@cw.bc.ca) BC Children s Hospital, Professor, University of British Columbia SLIDES ON : www.clinicalpeds.com/whistler Define Fever 38.0 o Doesn t
The McMaster at night Pediatric Curriculum
 The McMaster at night Pediatric Curriculum Robinson, J, et al. and the Canadian Pediatric Society. Urinary tract infection in infants and children: Diagnosis and management. Pediatr Child Health 2014;
The McMaster at night Pediatric Curriculum Robinson, J, et al. and the Canadian Pediatric Society. Urinary tract infection in infants and children: Diagnosis and management. Pediatr Child Health 2014;
Beyond the Reflex Arc: An Evidence-Based Discussion of the Management of Febrile Infants
 Beyond the Reflex Arc: An Evidence-Based Discussion of the Management of Febrile Infants Cole Condra, MD MSc Division of Emergency Medical Services Children s Mercy Hospital October 1, 2011 Disclosure
Beyond the Reflex Arc: An Evidence-Based Discussion of the Management of Febrile Infants Cole Condra, MD MSc Division of Emergency Medical Services Children s Mercy Hospital October 1, 2011 Disclosure
Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2
 Miss. kamlah 1 Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2 Acute Epiglottitis Is an infection of the epiglottis, the long narrow structure that closes off the glottis
Miss. kamlah 1 Epiglottitis. Bronchitis. Bronchiolitis. Pneumonia. Croup syndrome. Miss. kamlah 2 Acute Epiglottitis Is an infection of the epiglottis, the long narrow structure that closes off the glottis
Viral Meningitis. 2. Use the information on the Possible Diseases sheet to complete the other four columns in the chart.
 Disease Detectives Part 1: What is wrong with Mike? Yesterday, Mike Wright developed a severe headache, a high fever, and a stiff neck. Then, he became nauseated and began vomiting. He just wanted medicine
Disease Detectives Part 1: What is wrong with Mike? Yesterday, Mike Wright developed a severe headache, a high fever, and a stiff neck. Then, he became nauseated and began vomiting. He just wanted medicine
Andrea Marmor, MD Associate Clinical Professor, Pediatrics UCSF San Francisco General Hospital
 Andrea Marmor, MD Associate Clinical Professor, Pediatrics UCSF San Francisco General Hospital Carambola is a 16 mo old girl brought to the ED for crying nonstop She has been not herself for about a week,
Andrea Marmor, MD Associate Clinical Professor, Pediatrics UCSF San Francisco General Hospital Carambola is a 16 mo old girl brought to the ED for crying nonstop She has been not herself for about a week,
Osteomyelitis and Septic Joints; Practical Considerations. Coleen K. Cunningham
 Osteomyelitis and Septic Joints; Practical Considerations Coleen K. Cunningham Goals/objectives To improve understanding of the diagnosis, treatment, and follow-up of pediatric bone and joint infections
Osteomyelitis and Septic Joints; Practical Considerations Coleen K. Cunningham Goals/objectives To improve understanding of the diagnosis, treatment, and follow-up of pediatric bone and joint infections
Paediatric Wheeze and pneumonia. RCH Asthma RCH bronchiolitis RCH pneumonia Dr S Rajapaksa
 Paediatric Wheeze and pneumonia RCH Asthma RCH bronchiolitis RCH pneumonia Dr S Rajapaksa Case Charlotte is a 2 ½ year old who presents to ED with shortness of breath and wheeze. She had been picked up
Paediatric Wheeze and pneumonia RCH Asthma RCH bronchiolitis RCH pneumonia Dr S Rajapaksa Case Charlotte is a 2 ½ year old who presents to ED with shortness of breath and wheeze. She had been picked up
ANTIBIOTIC GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED MENINGITIS AND ENCEPHALITIS IN ADULTS
 ANTIBIOTIC GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED MENINGITIS AND ENCEPHALITIS IN ADULTS Version 4.0 Date ratified February 2009 Review date February 2011 Ratified by Authors Consultation Evidence
ANTIBIOTIC GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED MENINGITIS AND ENCEPHALITIS IN ADULTS Version 4.0 Date ratified February 2009 Review date February 2011 Ratified by Authors Consultation Evidence
Choosing an appropriate antimicrobial agent. 3) the spectrum of potential pathogens
 the spectrum of potential pathogens") Choosing an appropriate antimicrobial agent Consider: 1) the host 2) the site of infection 3) the spectrum of potential pathogens 4) the likelihood that these pathogens are resistant to antimicrobial agents
Choosing an appropriate antimicrobial agent Consider: 1) the host 2) the site of infection 3) the spectrum of potential pathogens 4) the likelihood that these pathogens are resistant to antimicrobial agents
TOPICS. Wheezing/Asthma THE BEST PEDIATRIC LITERATURE THAT STILL AFFECT YOUR PRACTICE
 THE BEST PEDIATRIC LITERATURE THAT STILL AFFECT YOUR PRACTICE Ghazala Q. Sharieff MD, MBA Wheezing/asthma Croup Immunizations and fever Appendicitis Complex febrile seizures Procedures Head Injury Zofran
THE BEST PEDIATRIC LITERATURE THAT STILL AFFECT YOUR PRACTICE Ghazala Q. Sharieff MD, MBA Wheezing/asthma Croup Immunizations and fever Appendicitis Complex febrile seizures Procedures Head Injury Zofran
Diagnosing and managing sepsis in children
 Diagnosing and managing sepsis in children Hague R. Diagnosing and managing sepsis in children. Practitioner Jan 2018;262(1811):21-25 Dr Rosie Hague MD MRCP FRCPCH Consultant in Infectious Diseases and
Diagnosing and managing sepsis in children Hague R. Diagnosing and managing sepsis in children. Practitioner Jan 2018;262(1811):21-25 Dr Rosie Hague MD MRCP FRCPCH Consultant in Infectious Diseases and
Fever in Infants: Pediatric Dilemmas in Antibiotherapy
 Fever in Infants: Pediatric Dilemmas in Antibiotherapy Jahzel M. Gonzalez Pagan, MD, FAAP Pediatric Emergency Medicine Associate Professor, UPH Medical Advisor, SJCH June 9 th, 2017 S Objectives S Review
Fever in Infants: Pediatric Dilemmas in Antibiotherapy Jahzel M. Gonzalez Pagan, MD, FAAP Pediatric Emergency Medicine Associate Professor, UPH Medical Advisor, SJCH June 9 th, 2017 S Objectives S Review
2/27/19 TALES FROM THE COMMUNITY PEM DEPT: SCARY CASES! Solomon Behar, MD, FAAP, FACEP March 2, 2019
 TALES FROM THE COMMUNITY PEM DEPT: SCARY CASES! Solomon Behar, MD, FAAP, FACEP March 2, 2019 1 OBJECTIVES v Understand the ddx and management of abdominal masses in kids v Understand strategies for dealing
TALES FROM THE COMMUNITY PEM DEPT: SCARY CASES! Solomon Behar, MD, FAAP, FACEP March 2, 2019 1 OBJECTIVES v Understand the ddx and management of abdominal masses in kids v Understand strategies for dealing
Infectious Disease. Chloe Duke
 Infectious Disease Chloe Duke Learning Objectives Essential - Causes, recognition and Treatment of: Meningitis Sepsis Purpura Important Cervical Adenopathy Tonsillitis and Pharyngitis Otitis Media Pneumonia
Infectious Disease Chloe Duke Learning Objectives Essential - Causes, recognition and Treatment of: Meningitis Sepsis Purpura Important Cervical Adenopathy Tonsillitis and Pharyngitis Otitis Media Pneumonia
Evelyn A. Kluka, MD FAAP November 30, 2011
 Evelyn A. Kluka, MD FAAP November 30, 2011 > 80% of children will suffer from at least one episode of AOM by 3 years of age 40% will have > 6 recurrences by age 7 years Most common diagnosis for which
Evelyn A. Kluka, MD FAAP November 30, 2011 > 80% of children will suffer from at least one episode of AOM by 3 years of age 40% will have > 6 recurrences by age 7 years Most common diagnosis for which
University Health Services at CMU STI Awareness Month specials for students:
 University Health Services at CMU STI Awareness Month specials for students: -Free condoms during April (10 per student) -Free walk-in rapid HIV testing April 22-27 (no appointment needed) -STI Screening
University Health Services at CMU STI Awareness Month specials for students: -Free condoms during April (10 per student) -Free walk-in rapid HIV testing April 22-27 (no appointment needed) -STI Screening
Lisa K. Fitzpatrick, MD, MPH Associate Professor of Medicine Howard University School of Medicine
 Lisa K. Fitzpatrick, MD, MPH Associate Professor of Medicine Howard University School of Medicine HIV Testing Missed Opportunities Acute Retroviral Syndrome Opportunistic Infections Treatment Reminders
Lisa K. Fitzpatrick, MD, MPH Associate Professor of Medicine Howard University School of Medicine HIV Testing Missed Opportunities Acute Retroviral Syndrome Opportunistic Infections Treatment Reminders
Disclosures. Background. Definitions. Why Worry about these Infants? Goals. Bacterial infection in the neonate and young infant: a review
 Disclosures Bacterial infection in the neonate and young infant: a review Russell J. McCulloh, MD Med-Peds Infectious Diseases August 8, 2017 I have no financial interests to disclose Funding: Eva and
Disclosures Bacterial infection in the neonate and young infant: a review Russell J. McCulloh, MD Med-Peds Infectious Diseases August 8, 2017 I have no financial interests to disclose Funding: Eva and
URIs and Pneumonia. Elena Bissell, MD 10/16/2013
 URIs and Pneumonia Elena Bissell, MD 10/16/2013 Objectives Recognize and treat community acquired PNA in children/adults Discern between inpatient and outpatient treatment of PNA Recognize special populations/cases
URIs and Pneumonia Elena Bissell, MD 10/16/2013 Objectives Recognize and treat community acquired PNA in children/adults Discern between inpatient and outpatient treatment of PNA Recognize special populations/cases
ID Emergencies. BGSMC Internal Medicine Edwin Yu
 ID Emergencies BGSMC Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
ID Emergencies BGSMC Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
Dilemmas in the Management of Meningitis & Encephalitis HEADACHE AND FEVER. What is the best initial approach for fever, headache, meningisums?
 Dilemmas in the Management of Meningitis & Encephalitis Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine HEADACHE AND FEVER What is the best initial approach for fever,
Dilemmas in the Management of Meningitis & Encephalitis Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine HEADACHE AND FEVER What is the best initial approach for fever,
Pediatric Case Studies. Case 1
 Pediatric Case Studies James Naprawa, MD Assistant Clinical Professor Pediatric Emergency Medicine Children s Hospital, Columbus Case 1 Almost 4 year old AA girl PMH UTI x 2 with abdominal pain and fever
Pediatric Case Studies James Naprawa, MD Assistant Clinical Professor Pediatric Emergency Medicine Children s Hospital, Columbus Case 1 Almost 4 year old AA girl PMH UTI x 2 with abdominal pain and fever
ID Emergencies. BUMC-P Internal Medicine Edwin Yu
 ID Emergencies BUMC-P Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
ID Emergencies BUMC-P Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
Reading Test 1 Part A
 Reading Test 1 Part A Page 1 w Copy w Rights w. Reserved o e t ::: m www.oetmaterial.com a t e r i a l. c o m. a u Reading: Part A TIME LIMIT: 15 MINUTES Instructions: Complete the following summary using
Reading Test 1 Part A Page 1 w Copy w Rights w. Reserved o e t ::: m www.oetmaterial.com a t e r i a l. c o m. a u Reading: Part A TIME LIMIT: 15 MINUTES Instructions: Complete the following summary using
Dr. Bob Wilson Golden BC
 Fever in Infants Under 3 Mon. Dr. Bob Wilson Golden BC What is the risk of serious bacterial infection in a febrile 2 A. 5% B. 10% C. 25% D. 50% E. 100% month old infant? What is the most common congenital
Fever in Infants Under 3 Mon. Dr. Bob Wilson Golden BC What is the risk of serious bacterial infection in a febrile 2 A. 5% B. 10% C. 25% D. 50% E. 100% month old infant? What is the most common congenital
Scott Williams, MD Pediatric Nephrology OLOL Children s Hospital September 29, Controversies in Urinary Tract Infections
 Scott Williams, MD Pediatric Nephrology OLOL Children s Hospital September 29, 2013 Controversies in Urinary Tract Infections Disclaimer I have no affiliations with any pharmaceutical or equipment company
Scott Williams, MD Pediatric Nephrology OLOL Children s Hospital September 29, 2013 Controversies in Urinary Tract Infections Disclaimer I have no affiliations with any pharmaceutical or equipment company
Pediatric TB Radiology: It s Not Black and White Part 2
 Experiencing technical difficulties? Please call Adobe Connect for technical assistance at 1-800-422-3623 Pediatric TB Radiology: It s Not Black and White Part 2 June 18, 2018 A National Webinar June 18,
Experiencing technical difficulties? Please call Adobe Connect for technical assistance at 1-800-422-3623 Pediatric TB Radiology: It s Not Black and White Part 2 June 18, 2018 A National Webinar June 18,
+ Objectives. n Define who is at risk for SBI. n Clarify risk stratification. n Provide treatment guidelines. n Bust some myths
 Objectives n Define wo is at risk for SBI n Clarify risk stratification n Provide treatment guidelines Neonatal Fever Benjamin B. Constance, MD, FAWM n Bust some myts Based on Case wat do you want to know?
Objectives n Define wo is at risk for SBI n Clarify risk stratification n Provide treatment guidelines Neonatal Fever Benjamin B. Constance, MD, FAWM n Bust some myts Based on Case wat do you want to know?
4/11/2017 COMMUNITY ACQUIRED PNEUMONIA. Disclaimer. A Review of How to Treat Common Infections in a Pediatric Patient. Objectives for Technicians
 Disclaimer A Review of How to Treat Common Infections in a Pediatric Patient Tara Bergland reports that she has no actual or potential conflict of interest in relation to this presentation. Off label use
Disclaimer A Review of How to Treat Common Infections in a Pediatric Patient Tara Bergland reports that she has no actual or potential conflict of interest in relation to this presentation. Off label use
Paediatric ENT problems
 Paediatric ENT problems Ears Otitis media Otitis media with effusion FBs Otitis externa Ruptured TM Nose FBs Allergic rhinitis Septal perforation expistaxis Throat FB Croup Stidor Tonsillitis Paediatric
Paediatric ENT problems Ears Otitis media Otitis media with effusion FBs Otitis externa Ruptured TM Nose FBs Allergic rhinitis Septal perforation expistaxis Throat FB Croup Stidor Tonsillitis Paediatric
Fever in children aged less than 5 years
 Fever in children aged less than 5 years A fever is defined as a temperature greater than 38 degrees celsius Height and duration of fever do not identify serious illness. However fever in children younger
Fever in children aged less than 5 years A fever is defined as a temperature greater than 38 degrees celsius Height and duration of fever do not identify serious illness. However fever in children younger
Judith Klein, MD 2011 FEVER IN THE FIRST 36 MONTHS OF LIFE
 Judith Klein, MD 2011 FEVER IN THE FIRST 36 MONTHS OF LIFE Objectives A short history of the kiddie fever business Vaccinations Rapid viral testing Biomarkers Month-by-month approach to fevers in these
Judith Klein, MD 2011 FEVER IN THE FIRST 36 MONTHS OF LIFE Objectives A short history of the kiddie fever business Vaccinations Rapid viral testing Biomarkers Month-by-month approach to fevers in these
Hot Stuff: The Febrile Child
 Hot Stuff: The Febrile Child Dr. Shannon MacPhee, Department of Emergency Medicine, Division Head Pediatric Emergency Medicine. IWK Health Centre. Dalhousie University November 2017 Know when to suspect
Hot Stuff: The Febrile Child Dr. Shannon MacPhee, Department of Emergency Medicine, Division Head Pediatric Emergency Medicine. IWK Health Centre. Dalhousie University November 2017 Know when to suspect
Vaccine Information Statement: PEDIATRIC VACCINES (Multiple)
") Vaccine Information Statement: PEDIATRIC VACCINES (Multiple) 1. Your Baby s First Vaccines: What You Need to Know Babies get six vaccines between birth and 6 months of age. These vaccines protect your
Vaccine Information Statement: PEDIATRIC VACCINES (Multiple) 1. Your Baby s First Vaccines: What You Need to Know Babies get six vaccines between birth and 6 months of age. These vaccines protect your
Objectives. Pneumonia. Pneumonia. Epidemiology. Prevalence 1/7/2012. Community-Acquired Pneumonia in infants and children
 Objectives Community-Acquired in infants and children Review of Clinical Practice Guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America - 2011 Sabah Charania,
Objectives Community-Acquired in infants and children Review of Clinical Practice Guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America - 2011 Sabah Charania,
Pneumonia. Definition of pneumonia Infection of the lung parenchyma Usually bacterial
 Pneumonia Definition of pneumonia Infection of the lung parenchyma Usually bacterial Epidemiology of pneumonia Commonest infectious cause of death in the UK and USA Incidence - 5-11 per 1000 per year Worse
Pneumonia Definition of pneumonia Infection of the lung parenchyma Usually bacterial Epidemiology of pneumonia Commonest infectious cause of death in the UK and USA Incidence - 5-11 per 1000 per year Worse
Central Nervous System Infection
 Central Nervous System Infection Lingyun Shao Department of Infectious Diseases Huashan Hospital, Fudan University Definition Meningitis: an inflammation of the arachnoid membrane, the pia mater, and the
Central Nervous System Infection Lingyun Shao Department of Infectious Diseases Huashan Hospital, Fudan University Definition Meningitis: an inflammation of the arachnoid membrane, the pia mater, and the
Welcome to the UCLA Center for East- West Medicine Primary Care
 Instructions: Welcome to the UCLA Center for East- West Medicine Primary Care We ask a lot of questions because we really want to get to know you! Please take your time with the paper work and return it
Instructions: Welcome to the UCLA Center for East- West Medicine Primary Care We ask a lot of questions because we really want to get to know you! Please take your time with the paper work and return it
Management of Common Respiratory Disorders in Children. Whitney Pressler, MD Pediatric Brown Bag Series Webinar June 14, 2016
 Management of Common Respiratory Disorders in Children Whitney Pressler, MD Pediatric Brown Bag Series Webinar June 14, 2016 Disclosures I have no financial relationships to disclose I will not be discussing
Management of Common Respiratory Disorders in Children Whitney Pressler, MD Pediatric Brown Bag Series Webinar June 14, 2016 Disclosures I have no financial relationships to disclose I will not be discussing
4/11/2017. A Review of How to Treat Common Infections in a Pediatric Patient. Disclaimer. Objectives for Pharmacists
 A Review of How to Treat Common Infections in a Pediatric Patient Tara Bergland, Pharm D. PGY2 Pediatric Pharmacy Resident Tara-bergland@uiowa.edu Disclaimer Tara Bergland reports that she has no actual
A Review of How to Treat Common Infections in a Pediatric Patient Tara Bergland, Pharm D. PGY2 Pediatric Pharmacy Resident Tara-bergland@uiowa.edu Disclaimer Tara Bergland reports that she has no actual
Management of Common Respiratory Disorders in Children. Disclosures. Roadmap 6/10/2016
 Management of Common Respiratory Disorders in Children Whitney Pressler, MD Pediatric Brown Bag Series Webinar June 14, 2016 Disclosures I have no financial relationships to disclose I will not be discussing
Management of Common Respiratory Disorders in Children Whitney Pressler, MD Pediatric Brown Bag Series Webinar June 14, 2016 Disclosures I have no financial relationships to disclose I will not be discussing
5/26/10. Upper Airway Emergencies Identify life threatening upper airway infections Recognize and treat anaphylaxis and airway burns in children
 Andi Marmor, MD Assistant Clinical Professor, Pediatrics University of California, San Francisco Upper Airway Emergencies Identify life threatening upper airway infections Recognize and treat anaphylaxis
Andi Marmor, MD Assistant Clinical Professor, Pediatrics University of California, San Francisco Upper Airway Emergencies Identify life threatening upper airway infections Recognize and treat anaphylaxis
Hand, foot and mouth disease
 Hand, foot and mouth disease Symptoms Hand-foot-and-mouth disease on the hand Hand-foot-and-mouth disease on the foot Hand-foot-and-mouth disease may cause all of the following signs and symptoms or just
Hand, foot and mouth disease Symptoms Hand-foot-and-mouth disease on the hand Hand-foot-and-mouth disease on the foot Hand-foot-and-mouth disease may cause all of the following signs and symptoms or just
Pneumococcal Meningitis Meningitis is an inflammation of the lining around the brain and spinal cord. Most severe cases
 Pneumococcal Meningitis Meningitis is an inflammation of the lining around the brain and spinal cord. Most severe cases are caused by bacteria. Pneumococcal bacteria (Streptococcus pneumoniae) are the
Pneumococcal Meningitis Meningitis is an inflammation of the lining around the brain and spinal cord. Most severe cases are caused by bacteria. Pneumococcal bacteria (Streptococcus pneumoniae) are the
Bone and Joint Infections Oh, My
 Bone and Joint Infections Oh, My Dale Jarka, MD,CM, FRCSC The Children s Mercy Hospitals & Clinics The Children's Mercy Hospital 2016 1 Disclosures A: I have no relevant financial relationships with the
Bone and Joint Infections Oh, My Dale Jarka, MD,CM, FRCSC The Children s Mercy Hospitals & Clinics The Children's Mercy Hospital 2016 1 Disclosures A: I have no relevant financial relationships with the
UPPER RESPIRATORY TRACT INFECTIONS. IAP UG Teaching slides
 UPPER RESPIRATORY TRACT INFECTIONS 1 INTRODUCTION Most common problem in children below 5 years. In this age group they get about 6 8 episodes per year. It includes infections of nasal cavity, throat,
UPPER RESPIRATORY TRACT INFECTIONS 1 INTRODUCTION Most common problem in children below 5 years. In this age group they get about 6 8 episodes per year. It includes infections of nasal cavity, throat,
Leukocytosis. dr. Erdélyi, Dániel 2 nd Department of Paediatrics Semmelweis University
 Leukocytosis dr. Erdélyi, Dániel 2 nd Department of Paediatrics Semmelweis University My first day at work in 1997 3y with fever, cough Is this bronchitis, pneumonia, pharyngitis, sinusitis, else? Is this
Leukocytosis dr. Erdélyi, Dániel 2 nd Department of Paediatrics Semmelweis University My first day at work in 1997 3y with fever, cough Is this bronchitis, pneumonia, pharyngitis, sinusitis, else? Is this
10/25/2018. Autoimmunity and how to treat it. Disclosure. Why do we get autoimmunity? James Verbsky MD/PhD Pediatric Rheumatology/Immunology
 Autoimmunity and how to treat it James Verbsky MD/PhD Pediatric Rheumatology/Immunology Disclosure None I will mention drug names and some brand names but I have no financial interest or any other ties
Autoimmunity and how to treat it James Verbsky MD/PhD Pediatric Rheumatology/Immunology Disclosure None I will mention drug names and some brand names but I have no financial interest or any other ties
AZITHROMYCIN H PYLORI TREATMENT
 AZITHROMYCIN H PYLORI TREATMENT Azithromycin H Pylori Treatment How long does it take to feel the effects of azithromycin Azithromycin effect on human cells Can you drink beer when taking azithromycin
AZITHROMYCIN H PYLORI TREATMENT Azithromycin H Pylori Treatment How long does it take to feel the effects of azithromycin Azithromycin effect on human cells Can you drink beer when taking azithromycin
CASE-BASED SMALL GROUP DISCUSSION MHD II
 MHD II, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II Session 11 April 11, 2016 STUDENT COPY MHD II, Session 11, Student Copy Page 2 CASE HISTORY 1 Chief complaint: Our baby
MHD II, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II Session 11 April 11, 2016 STUDENT COPY MHD II, Session 11, Student Copy Page 2 CASE HISTORY 1 Chief complaint: Our baby
McHenry Western Lake County EMS System Optional CE for Paramedics, EMT-B and PHRN s Croup vs. Epiglottitis. Optional #2 2017
 McHenry Western Lake County EMS System Optional CE for Paramedics, EMT-B and PHRN s Croup vs. Epiglottitis Optional #2 2017 The tones go out at 3 am for a child with difficulty breathing. As it is a kid
McHenry Western Lake County EMS System Optional CE for Paramedics, EMT-B and PHRN s Croup vs. Epiglottitis Optional #2 2017 The tones go out at 3 am for a child with difficulty breathing. As it is a kid
Emergency Neurological Life Support Meningitis and Encephalitis
 Emergency Neurological Life Support Meningitis and Encephalitis Version: 2.0 Last Updated: 19-Mar-2016 Checklist & Communication Meningitis and Encephalitis Table of Contents Emergency Neurological Life
Emergency Neurological Life Support Meningitis and Encephalitis Version: 2.0 Last Updated: 19-Mar-2016 Checklist & Communication Meningitis and Encephalitis Table of Contents Emergency Neurological Life
Microbiology Laboratory Directors, Infection Preventionists, Primary Care Providers, Emergency Department Directors, Infectious Disease Physicians
 MEMORANDUM DATE: October 1, 2009 TO: FROM: SUBJECT: Microbiology Laboratory Directors, Infection Preventionists, Primary Care Providers, Emergency Department Directors, Infectious Disease Physicians Michael
MEMORANDUM DATE: October 1, 2009 TO: FROM: SUBJECT: Microbiology Laboratory Directors, Infection Preventionists, Primary Care Providers, Emergency Department Directors, Infectious Disease Physicians Michael