Celiac Disease. Disclosures 5/6/2015. Goals/Objectives. Jeff Hunt, DO, FACOI. Speaker for Abbvie. Consultant for Janssen Pharmaceuticals
|
|
|
- Eustace Lane
- 6 years ago
- Views:
Transcription


1 Celiac Disease Jeff Hunt, DO, FACOI Gastroenterology United of Tulsa OSU Medical Center Disclosures Speaker for Abbvie Consultant for Janssen Pharmaceuticals Research projects with Abbvie Goals/Objectives History of Celiac Pathology of Celiac Disease Clinical features of CD Who and when to test Treatment 1
2 What is celiac disease? A chronic, genetic, auto-immune mediated, small bowel disorder characterized by mucosal inflammation, villous atrophy, and crypt hyperplasia, which occurs upon exposure to dietary gluten, and demonstrates improvement after withdrawal of gluten Alternative names: Celiac sprue, sprue Gluten intolerance Gluten-sensitive enteropathy Spectrum of celiac disease Classic disease 1)Villous atrophy; symptoms of malabsorption such as steatorrhea 2)Weight loss, or other signs of nutrient or vitamin deficiency 3)Resolution of mucosal lesions and symptoms upon withdrawal of gluten from the diet, within a few weeks to months These patient have antibodies to gliadin and tissue transglutaminase Atypical celiac disease Latent celiac disease Classic Spectrum of celiac disease Atypical celiac disease Minor gastrointestinal complaints Anemia, dental enamel defects, osteoporosis, arthritis, increased transaminases, neurological symptoms, or infertility Shows mucosal damage and possess the celiac specific antibody pattern Latent celiac disease 2
3 Classic Spectrum of celiac disease Atypical celiac disease Latent celiac disease Normal jejunal mucosa and minor or no symptoms at one or more time points while on a normal, gluten-containing diet Two variants 1) CD present in past, recovered completely and remained silent when a normal diet was reintroduced 2) Normal mucosa was diagnosed at an earlier occasion while ingesting a normal diet, but celiac disease developed later History Recognized 1st century AD κοιλιακός, (koiliakós, abdominal) Sprue coined in 18 th century Derived from a Dutch word meaning aphthous disease 20 th century Link between cereals and celiac made by Willem Karel Dicke, a Dutch pediatrician During WWII, when cereals were scarce, children s symptoms improved only to return with cereal consumption Van de Kamer showed the water-insoluble portion, gluten moiety of wheat produced intestinal injury 1. Feldman, Mark, Lawrence Friedman, and Lawrence Brandt, Schleisenger and Fordtran s Gastrointestinal and Liver Disease. Philadelphia, PA: Saunders, Elsevier, Print. History 1954 Paulley: first accurate description of the characteristic intestinal lesions 1986 Howell: observed celiac was associated with HLA- DQ2 haplotypes 1993 Lundin: DQ2 gene products preferentially presents gluten-derived gliadin peptides to intestinal mucosal T cells Feldman, Mark, Lawrence Friedman, and Lawrence Brandt, Schleisenger and Fordtran s Gastrointestinal and Liver Disease. Philadelphia, PA: Saunders, Elsevier, Print. 3
4 Epidemiology Whites of northern European ancestry Silent celiac disease, a positive serology and villus atrophy with few or no symptoms, is approximately seven times more common than symptomatic celiac disease Feldman, Mark, Lawrence Friedman, and Lawrence Brandt, Schleisenger and Fordtran s Gastrointestinal and Liver Disease. Philadelphia, PA: Saunders, Elsevier, Print. Epidemiology One of the largest studies in the US: 13,145 subjects who underwent screening (4,508 first-degree relatives of those with celiac disease, 1,275 second-degree relatives, 3,236 symptomatic patients, and 4,126 not-at-risk individuals) Prevalence is 1:22 in first-degree relatives 1:39 in second-degree relatives 1:56 in symptomatic patients In the not-at-risk group, the prevalence was 1:133 or ~1% of the population, ~4 million Fasano A, Berti I, Gerarduzzi T, et al. Prevalence of celiac disease in at-risk and not-at-risk groups in the United States: a large multicenter study. Arch Intern Med 2003; 163:286 Epidemiology One of the largest screening investigations of celiac disease was performed in 17,201 school children (6 to 15) from Italy and represented 69 percent of the eligible population The prevalence was 1:184 and the ratio of undiagnosed to diagnosed celiac disease was 7:1; most children had minor but significant symptoms [2] Catassi C, Fabiani E, Ratsch IM, et al. The coeliac iceberg in Italy. A multicentre antigliadin antibodies screening for coeliac disease in school-age subjects. Acta Paediatr Suppl 1996; 412:29 4
5 Pathology Studies of epithelial cell kinetics suggest that villus atrophy is a misnomer and there is evidence for an actual increase in enteropoiesis in the crypts Wright,et al, estimated that intestinal mucosa in patients with celiac produces six times as many cells per hour per crypt as does normal small intestine and that the cell cycle time is halved, reflecting premature shedding [4] Feldman, Mark, Lawrence Friedman, and Lawrence Brandt, Schleisenger and Fordtran s Gastrointestinal and Liver Disease. Philadelphia, PA: Saunders, Elsevier, Print. Pathogenesis Triggered by an environmental agent (gliadin) in genetically predisposed persons Complex interplay of varying environmental, genetic, and immune factors How these control expression of celiac and change from latent to overt disease remains unknown Pathogenesis ENVIRONMENTAL FACTORS Several wheat proteins are responsible for the grain s toxicity Prolamins (storage form of wheat protein rich in proline and glutamine) are referred to as gliadins Prolamins from wheat, barley, rye and oats have immunologic cross-reactivity and can trigger celiac Oats have the smallest proportion of prolamin and is usually tolerated in those with celiac disease Grains that do not activate disease: rice, corn, sorghum, and millet 5
6 Potential Causes/Protectors Rotavirus Adenovirus Surgery Pregnancy Infection Emotional stress Smoking? (adult onset) Breastfeeding GENETIC FACTORS Pathogenesis Concordance for CD in first-degree relatives ranges between 8% and 18% and reaches 70% in monozygotic twins [1] Close association with HLA-DQ2 and HLA-DQ8 genes HLA-DQ2 is present in more than 90% of persons with celiac disease compared with approximately 35% of general population However, only a minority of persons who express DQ2 actually develop CD, indicating that genes other than those encoding the DQ2 are involved in the development of CD Still much unknown Some of which are also associated with type 1 diabetes (15q26) [5] Houlston RS, Tomlinson IP, Ford D, et al. Linkage analysis of candidate regions for coeliac disease genes. Hum Mol Genet 1997; 6:1335. Feldman, Mark, Lawrence Friedman, and Lawrence Brandt, Schleisenger and Fordtran s Gastrointestinal and Liver Disease. Philadelphia, PA: Saunders, Elsevier, Print. IMMUNE FACTORS Pathogenesis Both humoral- and cell-mediated immune responses IgA and IgG serum antibodies to purified gliadin, all major fractions of gliadin, detected in the serum of patients with untreated CD IgA antibodies to endomysium, a connective tissue structure surrounding smooth muscle, are virtually pathognomonic for CD and are found only rarely in the absence of disease Now known that the target auto-antigen contained within the endomysium is the enzyme Tissue Transglutaminase-2 (TTG) 6
7 Clinical Features SUBCLINICAL DISEASE Mild and non-specific symptoms such as fatigue, iron deficiency, or otherwise unexplained elevations in serum aminotransferases, or no symptoms at all Establishing the diagnosis of subclinical disease is important 1) Danger of malignancy 2) Presence of nutritional deficiencies 3) Association with autoimmune disorders Clinical Features GASTROINTESTINAL FEATURES Classic signs: flatulence, diarrhea with bulky, foul-smelling, floating stools due to steatorrhea Malabsorption leading to growth failure, weight loss, anemia, neurologic disorders from deficiencies of B vitamins, and osteopenia from low vitamin D and calcium NON-GI FEATURES Neuropsychiatric Clinical Features Headache, peripheral neuropathy, ataxia, depression, dysthymia, anxiety, and epilepsy Peripheral neuropathy have been described in up to 50 percent of patients with celiac disease and may precede the diagnosis [1] Neuropathy may be associated with lymphoma and deficiencies of vitamins B1 (thiamine), B3 (niacin), B6 (pyridoxine), B12 (cobalamine), and E Gluten-free diet has been shown to have a favorable effect on headaches and dysthymia. Does not improve peripheral neuropathies Feldman, Mark, Lawrence Friedman, and Lawrence Brandt, Schleisenger and Fordtran s Gastrointestinal and Liver Disease. Philadelphia, PA: Saunders, Elsevier, Print. 7

8 Non-GI Clinical Features Metabolic bone disease Common and can occur in the absence of gastrointestinal symptoms Higher likelihood of secondary hyperparathyroidism that is probably due to Vitamin D deficiency Axial skeletal bone density can normalize on gluten-free diet, while loss of bone density in the appendicular skeleton may persist Hyposplenism Several case reports of hyposplenism (pathogenesis unknown) Prophylactic vaccinations for encapsulated organisms (Streptococcus, Neisseria, Hemophilus) are recommended Feldman, Mark, Lawrence Friedman, and Lawrence Brandt, Schleisenger and Fordtran s Gastrointestinal and Liver Disease. Philadelphia, PA: Saunders, Elsevier, Print. Howell-Jolly Bodies Non-GI Clinical Features Kidney disease Glomerular IgA deposition is common and may occur in as many as 1/3 of patients. Majority have no clinical manifestations of renal disease Idiopathic pulmonary hemosiderosis Coexistance of CD and idiopathic pulmonary hemosiderosis (Lane-Hamilton syndrome) reported in a few cases Gluten free diet has been associated with remission of pulmonary symptoms in several patients 8

 93 patients presenting with iron deficiency anemia found 12 percent of small bowel biopsy findings compatible with celiac(some had esophagitis and gastritis) Another report showed 6% of 85 patients")
9 Non-GI Clinical Features OB/GYN Delayed menarch Earlier menapause Infertility 9-fold increase in miscarriage rates Lower birth weights Premature births Eliakim and Sherer, Gynecol Obstet Invest, 51:3,2001 Soni and Badawy, J Reprod Med, 55:3, 2010 Ozgor, B, Scand J Gastroenterology, 45:395, 2010 Iron/folate deficiency Lab Anomalies CD may be a surprisingly frequent cause of iron deficiency anemia (with all EGDS bx duodenum!) 93 patients presenting with iron deficiency anemia found 12 percent of small bowel biopsy findings compatible with celiac(some had esophagitis and gastritis) Another report showed 6% of 85 patients with iron deficiency anemia had CD [3] Coagulopathy due to impaired absorption of vitamin K Feldman, Mark, Lawrence Friedman, and Lawrence Brandt, Schleisenger and Fordtran s Gastrointestinal and Liver Disease. Philadelphia, PA: Saunders, Elsevier, Print. Associated Conditions DERMATITIS HERPETIFORMIS Multiple intensely pruritic papules and vesicles that occur in grouped arrangements, usually involving the elbows, dorsal forearms, knees, scalp, back, and buttocks 9

10 Associated Conditions Histologic dx by demonstrating granular IgA deposits along the dermal-epidermal basement membrane Dermatitis herpetiformis responds to gluten withdrawal Dapsone if no response to GF diet DIABETES MELLITIS Associated Conditions CD is closely associated with Type I DM 2.6%-7.8% of adults with type I DM had IgA autoantibodies to endomysium or tissue transglutaminase Most were proven to have CD on small bowel biopsy Multiple genetic loci shared, including HLA-DR3, DQ2, and DQ8 Associated Conditions SELECTIVE IGA DEFICIENCY Association well established/serologic testing errors! IgA deficiency affects between 1 in 400/1 in 800 members of general population Occurs in 2 to 3% of patients with CD DOWN SYNDROME Prevalence of biopsy-proven celiac disease has been reported to be as high as 16% 20-fold increase compared with the general population 10
11 Associated Conditions LIVER Mild chronic elevation in serum AST (ranging 29 to 80) and ALT (ranging ) In patients with cryptogenic transaminasemia celiac serology was positive in 6% and duodenal biopsies suggested celiac disease in 4% Gluten-free diet, normalize 63-90% within a year THYROID Increased incidence of autoimmune thyroid disease Hypothyroid is more frequent Age at Diagnosis Other Autoimmune Conditions % % % Over 20 34% Ventura, et al Associated Conditions INFLAMMATORY BOWEL DISEASE Associated more frequently with UC than Crohn s Risk of IBD in patients with celiac elevated 10-fold while risk of CD in patients with IBD was comparable to controls First-degree relatives of patients with celiac may be at a fivefold increased risk of developing UC compared with the general pop ATROPHIC GLOSSITIS Has been described in association with CD; responds to a glutenfree diet Oral symptoms frequent in patients with CD; helpful tool in diagnosing CD 11
12 Who Should Be Tested? Patients with S/S or labs showing malabsorption, chronic diarrhea with weight loss, steatorrhea, postprandial abdominal pain, bloating Iron deficiency anemia, folate or vitamin B12 deficiency, persistent elevation of liver enzymes, recurrent aphthous ulcerations or stomatitis, dental enamel hypoplasia, and idiopathic peripheral neuropathy Patients with type I DM as well as first-degree relatives of individuals with CD if they have signs, symptoms, or laboratory evidence of CD Diagnosis No single test can confidently establish the diagnosis of CD in every individual All testing should be performed while patients are on a gluten-rich diet for at least two weeks! Three components to diagnosis Serologic studies Endoscopic/histologic evaluation Genetics SEROLOGIC STUDIES Diagnosis IgA anti-tissue transglutaminase (TTG) antibody is the single preferred test for detection of CD with a sensitivity and specificity of 95% Greater titer = greater likelihood of a true positive result Other serologic tests Anti-gliadin Ab (lowest sensitivity and specificity) Anti-endomysial Ab (moderate sensitivity and specificity) Anti-deamidated gliadin peptides (moderate to high sensitivity and specificity) Presence of IgA deficiency is increased in those with CD (2-3%)! When there is a high probability of CD total IgA should be measured, especially if IgA serology is negative Alternative approach is to include both IgA and IgG-based testing 12
 and four from the second and third portion of the duodenum Mucosa may appear atrophic, have")
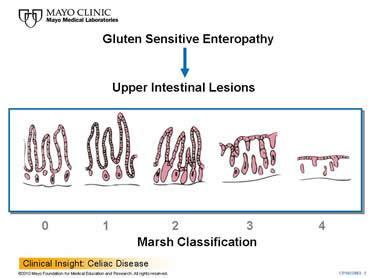
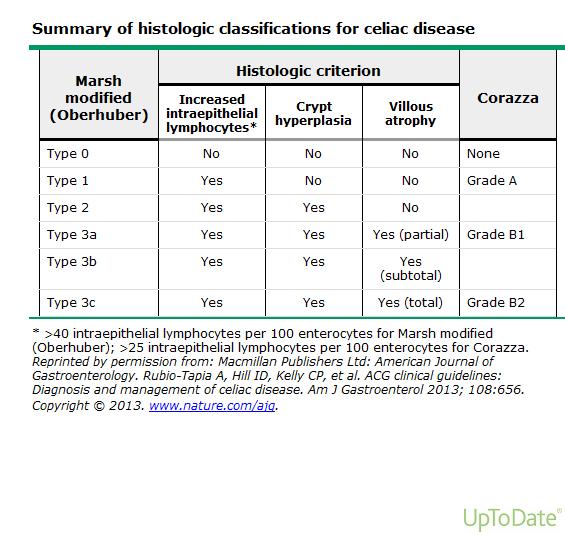
13 Diagnosis Endoscopic/histologic evaluation Patients with a positive serology, and patients with a high probability of CD, regardless of the serology, should undergo upper endoscopy with small bowel biopsies to confirm the diagnosis Two biopsies from the duodenal bulb (either 9- or 12-o clock position) and four from the second and third portion of the duodenum Mucosa may appear atrophic, have fissures, a nodular appearance, or folds may be scalloped, but these are not universally present and can be seen with other disorders Pathology Marsh proposed a sequence of progression of the celiac lesions Normal, preinfiltrative mucosa (stage 0) Increase in intraepithelial lymphocytes, infiltration of the lamina propria with lymphocytes (stage 1) Crypt hyperplasia (stage 2) Villus atrophy (stage 3) Feldman, Mark, Lawrence Friedman, and Lawrence Brandt, Schleisenger and Fordtran s Gastrointestinal and Liver Disease. Philadelphia, PA: Saunders, Elsevier, Print. 13


14 Pathology 14
15 Diagnosis OTHER CAUSES OF VILLOUS ATROPHY; NOT ALL VILLOUS ATROPHY IS CELIAC! Tropical sprue Small-bowel bacterial overgrowth Drug-associated enteropathy Whipple s disease Collagenous sprue Crohn s disease Eosinophilic enteritis Intestinal lymphoma/tuberculosis Infectious enteritis Malnutrition AIDS enteropathy Diagnosis DISORDERS SEEN WITH LYMPHOCYTIC DUODENOSIS Helicobacter pylori Medications (NSAID s) Small bowel bacterial overgrowth Systemic autoimmune disorders GENETIC TESTING Diagnosis HLA-DQ2/DQ8 genotype testing should be used to effectively rule out the disease in selected clinical situations 1. Equivocal small-bowel histology in seronegative patients 2. Evaluation of patients on a GFD in whom no testing for CD was done before GFD 3. Patients with discrepant celiac-specific serology and histology More than 99% of patients with CD have HLA DQ2 and/or DQ8 compared with 40% of general population High negative predictive value (>99%) essentially excludes the possibility of CD if neither HLA DQ2 or DQ8 are present! 15
16 Treatment Six key elements in the management of patients with CD Consultation with a skilled dietitian Education about the disease Lifelong adherence to a GFD Identification and treatment of nutritional deficiencies Access to an advocacy group Continuous long-term follow-up by a multidisciplinary team DIETARY COUNSELING Treatment A GFD is the only effective treatment for CD Recommended for patients with classic CD, atypical CD, and asymptomatic or silent CD Patients with latent CD (positive IgA endomysial antibody, but normal small bowel biopsy) are currently not advised to be on a GFD, but should continue to be monitored and re-biopsied if symptoms develop GLUTEN FREE DIET Principle sources are wheat, barley, and rye Not completely possible to eliminate due to contamination of foods with trace amounts of gluten Gluten free indicates a diet that contains gluten at such a low level as to be considered harmless 16

17 2012, $4.2 BILLION 2017, $6.6 BILLION Treatment In general, the following dietary advice can be given to all patients Avoid wheat, rye, and barley Soybean or tapioca flours, rice, corn, buckwheat, and potatoes are safe Read labels to look for additives that may contain gluten Distilled alcoholic beverages and vinegars, as well as wine, are gluten free. Beer, ale, lagers, and malt vinegars should be avoided Oats should be introduced into the diet with caution and patients should be monitored for adverse reactions. Oat consumption should be limited to g/day (approximately 2 ounces) in patients with mild disease upon presentation or whose disease is in remission after a stringent GFD. The latter patients should be followed carefully for clinical or serologic evidence of disease recurrence after reintroducing oats. Patients with severe disease should avoid oats altogether! Treatment MONITORING RESPONSE TO A GFD Rapidity of response is variable ~70% of patients have noticeable clinical improvement in two weeks Symptoms improve faster than histology Patient labs re-evaluated 4-6 weeks following initiation of a GFD: CBC, CMP, B12, iron studies and serologic testing IgA TTG or IGA DGP should be used to monitor the response to a GFD A pre-treatment antibody level should be determined at the time of diagnosis Exclusion of gluten = gradual decline in serum antibody levels (t1/2 is 6 to 8 weeks). Normal baseline values in 3 to 12 months Normal antibody levels do not indicate recovery from villous atrophy If levels are not falling the patient is usually continuing to ingest gluten either intentionally or inadvertently 17
18 Treatment SMALL BOWEL BIOPSY Need for follow-up biopsy in patients with clinical improvement has been debated since serologic testing can be used to monitor recovery and compliance with the diet Endoscopy with biopsy should be performed in patients with established CD who fail to respond to a GFD or who relapse with symptoms despite a GFD Treatment NON-RESPONDERS Individuals who have persistent symptoms or serologic and/or histologic abnormalities after two years on a GFD ~5% fail to respond to diet changes Those who fail to respond fall into 5 main categories Poor compliance or inadvertent gluten ingestion Clinical or histologic features that overlap with celiac disease but are caused by other disorders Concurrent disorders No response to GFD (refractory CD) Patients with ulcerative jejunitis or intestinal lymphoma Treatment REFRACTORY CELIAC DISEASE 1 to 2%) Type I RCD, lymphocyte infiltration of the small-intestinal mucosa is similar to that seen in untreated CD (MC type in the US) Type II RCD, CD3-positive intraepithelial T-cells exhibit a lack of expression of normal cell surface differentiation markers such as CD8 These T-cell abnormalities are associated with a significantly less favorable prognosis as compared to Type I RCD 18
19 Treatment TYPE I RCD Exclude inadvertent gluten exposure and evaluation for and treatment of nutritional deficiencies Severe cases use systemic steroid therapy with prednisone or a similar agent If incomplete response to steroids or if recurs when the dose is reduced Azathioprine, budesonide or mesalamine can be used TYPE II RCD Treatment Same as Type I RCD, however, symptoms and signs of disease are more severe and are less likely to respond to further therapy Malnutrition may be severe and require TPN Systemic corticosteroids, budesonide, azathioprine, 6-MP, methotrexate, cyclosporine, anti-tnf antibodies Transformation to enteropathy-associated T-cell lymphoma (EATCL) is a prominent risk and may require treatment by surgery, chemotherapy, or bone marrow transplantation In some patients EATCL may run a prolonged, non-aggressive course but the overall prognosis remains poor ULCERATIVE JEJUNITIS Treatment Can progress into lymphoma. Consider in patients nonresponsive to steroids Multiple chronic, benign-appearing ulcers, most commonly in jejunum Intestinal strictures can lead to small bowel obstruction Evaluate with abdominal CT/MR enterography or upper endoscopy. If negative, follow with capsule endoscopy Responds poorly to a GFD and is associated with poor prognosis (~1/3 of patients die from complications) Prognosis can be improved if the ulcerated or strictured segment can be resected 19
20 Treatment OTHER ASPECTS OF MANAGEMENT Repletion of nutritional deficiencies Vitamins A, D, E, K, B6, B12, copper, zinc, carotene, folate, ferritin, iron, thiamine, magnesium, and selenium Prevention of bone loss Should be evaluated for bone loss using a DEXA scan yearly Vaccinations Vaccinate for encapsulated organisms due to hyposplenism Screening family members Currently, screening 1st-degree relatives (especially siblings) should be considered Who should be screened? Symptoms, signs, or laboratory evidence suggestive of malabsorption, chronic diarrhea with weight loss, steatorrhea, postprandial abdominal pain, and bloating. (Strong recommendation, high level of evidence) Patients with symptoms, signs, or laboratory evidence for which CD is a treatable cause should be considered for testing for CD. (Strong recommendation, moderate level of evidence) Patients with a first-degree family member who has a confirmed diagnosis of CD should be tested if they show possible signs or symptoms or laboratory evidence of CD. (Strong recommendation, high level of evidence) Consider testing asymptomatic relatives of a first-degree family member with a confirmed diagnosis of CD. (Conditional recommendation, high level of evidence) If have elevated serum aminotransferase levels when no other etiology is found. (Strong recommendation, high level of evidence) Patients with Type I DM if any digestive symptoms, or signs, or laboratory evidence suggestive of CD. (Strong recommendation, high level of evidence) 20

21 Complications Ulcerative Jejunitis Malignancy risk Enteropathy associated T-cell lymphoma and GI cancers Refractory Disease to GFD can develop with chronic non-adherence to diet. Patients who have no initial response to a gluten-free diet Patients who experience initial clinical improvement on a gluten-free diet, but, after a period of remission, develop disease refractory to gluten abstinence Ulcerative Jejunitis Typically seen in refractory sprue presents with Benign-appearing ulcers most often in the jejunum and symptoms of malabsorption, nausea, anorexia, fever, abdominal pain, and diarrhea. Evaluate with CT, MRI, and EGD. If nothing is found capsule endoscopy is required. Responds poorly to GFD. Up to 1/3 of patients die from complications, outcome seems to be better if strictures can be surgically removed. T-cell Lymphoma Fever, hepatomegaly, splenomegaly, duodenal mass, or ascites, may help with the diagnosis, but their presence implies more advanced disease. Other presentations: acute perforation, gastrointestinal obstruction, gastrointestinal hemorrhage. Diagnose with CT, MRI, upper endoscopy, and capsule endoscopy. Hard to distinguish lymphoma from occult celiac disease. A full thickness biopsy may be required to make the diagnosis when radioimaging is inconclusive. 5 year survival only 10% 21

22 Refractory Sprue Type 1: A normal population of intraepithelial lymphocytes. Type 2: An aberrant or premalignant population of intraepithelial lymphocytes. Can progress to enteropathy-associated T-cell lymphoma and ulcerative jejunitis. Diagnosis is based upon clonality analysis of T-cell receptors and immunophenotyping. The diagnosis can be established on biopsy; CT, MRI, and 18F-FDG PET scans can help identify suspicious areas. Differentiating is important as it can predict the progression of disease. A study assessed survival rate after 5 years for type 1 and type 2. At 5 years survival rate was 96% for type 1 vs. 58% for type 2. These findings were mostly like do to the development of T-cell lymphoma Refractory Sprue Type 1: treat with budesonide Treatment for severely ill patient s - hydrocortisone 100 mg IV Q6H, for those that can tolerate food use prednisolone mg PO QD. Type 2: prednisolone mg PO QD + Azathroprine or 6- mercaptopurine 2mg/kg/day. For those that can not tolerate Azathroprine or 6-MP use methotrexate 25 mg/week. Other agents: mesalamine, cladribine, and TNF-a inhibitors Research Kansas Farmers and glutenfree wheat research Lactobacillus to pre-treat flour or dough Immune modulation with the use of Necator americanus (hookworm) to desensitize celiac patients 22
23 Future Therapies Alvine Pharmaceuticals, ALV003 Degrades 33-AA long leftover chain Phase 2b study BioLineRx, BL7010 Binds to immunogenic portion of gluten preventing gliadin from entering blood Randomized, placebo controlled study in latter 2015 Celimmune, AMG 714 Monoclonal Ab to IL-15 (cytokine that leads to loss of tolerance) Phase 2 study Future Therapies Alba Therapeutics, Larazotide Acetate Oral peptide that regulates tight junctions in the bowel Prevents leaky gut Phase 2b studies ImmunosanT, Nexvax2 Intradermal, disease modifying immunotherapy Makes tolerant or reprograms their immune system to gluten Recruiting for phase 2 trials Patient Resources / Celiac disease foundation / Gluten Intolerance Group of N. America / Natl. Found. For Celiac Awareness / Canadian Celiac Association / Celiac Sprue Association Blumer, I. and Crowe, Sheila. Celiac Disease for Dummies, Wiley,

24 Thank You! 24
Coeliac Disease: Diagnosis and clinical features
 Coeliac Disease: Diagnosis and clinical features Australasian Gastrointestinal Pathology Society AGM 28 Oct 2016 Dr. Hooi Ee Gastroenterologist, Sir Charles Gairdner Hospital Coeliac disease Greek: koiliakos
Coeliac Disease: Diagnosis and clinical features Australasian Gastrointestinal Pathology Society AGM 28 Oct 2016 Dr. Hooi Ee Gastroenterologist, Sir Charles Gairdner Hospital Coeliac disease Greek: koiliakos
Small bowel diseases. Györgyi Műzes 2015/16-I. Semmelweis University, 2nd Dept. of Medicine
 Small bowel diseases Györgyi Műzes 2015/16-I. Semmelweis University, 2nd Dept. of Medicine Celiac disease (revised definition!) a systemic autoimmune disorder Occurs in genetically susceptible individuals
Small bowel diseases Györgyi Műzes 2015/16-I. Semmelweis University, 2nd Dept. of Medicine Celiac disease (revised definition!) a systemic autoimmune disorder Occurs in genetically susceptible individuals
Kristin Kenrick, FRNZCGP Department of General Practice and Rural Health Dunedin School of Medicine (Supported by Coeliac New Zealand)
") Kristin Kenrick, FRNZCGP Department of General Practice and Rural Health Dunedin School of Medicine (Supported by Coeliac New Zealand) That you will go away thinking about your practice population, and
Kristin Kenrick, FRNZCGP Department of General Practice and Rural Health Dunedin School of Medicine (Supported by Coeliac New Zealand) That you will go away thinking about your practice population, and
Celiac Disease. M. Nedim Ince, MD University of Iowa Hospital
 Celiac Disease M. Nedim Ince, MD University of Iowa Hospital Contents Cases Definition Etiopathogenesis Pathology Diagnosis Management of the disease Management of complications Case I Five year old boy
Celiac Disease M. Nedim Ince, MD University of Iowa Hospital Contents Cases Definition Etiopathogenesis Pathology Diagnosis Management of the disease Management of complications Case I Five year old boy
Definition. Celiac disease is an immune-mediated enteropathy caused by a permanent sensitivity to gluten in genetically susceptible individuals.
 Definition 1 Definition Celiac disease is an immune-mediated enteropathy caused by a permanent sensitivity to gluten in genetically susceptible individuals. It occurs in symptomatic subjects with gastrointestinal
Definition 1 Definition Celiac disease is an immune-mediated enteropathy caused by a permanent sensitivity to gluten in genetically susceptible individuals. It occurs in symptomatic subjects with gastrointestinal
Tips for Managing Celiac Disease. Robert Berger MD FRCPC Gastroenterology New Brunswick Internal Medicine Update April 22, 2016
 Tips for Managing Celiac Disease Robert Berger MD FRCPC Gastroenterology New Brunswick Internal Medicine Update April 22, 2016 Disclosures None relevant to this presentation Objectives Briefly review the
Tips for Managing Celiac Disease Robert Berger MD FRCPC Gastroenterology New Brunswick Internal Medicine Update April 22, 2016 Disclosures None relevant to this presentation Objectives Briefly review the
ACG Clinical Guideline: Diagnosis and Management of Celiac Disease
 ACG Clinical Guideline: Diagnosis and Management of Celiac Disease Alberto Rubio-Tapia, MD 1, Ivor D. Hill, MD 2, Ciarán P. Kelly, MD 3, Audrey H. Calderwood, MD 4 and Joseph A. Murray, MD 1 1 Division
ACG Clinical Guideline: Diagnosis and Management of Celiac Disease Alberto Rubio-Tapia, MD 1, Ivor D. Hill, MD 2, Ciarán P. Kelly, MD 3, Audrey H. Calderwood, MD 4 and Joseph A. Murray, MD 1 1 Division
Coeliac Disease Bible Class Questions and Answers
 Coeliac Disease Bible Class Questions and Answers Jan Hendrik Niess What is the definition of coeliac disease? Coeliac disease is an immune reaction to gluten (wheat, barely, rye) in an genetic predisposed
Coeliac Disease Bible Class Questions and Answers Jan Hendrik Niess What is the definition of coeliac disease? Coeliac disease is an immune reaction to gluten (wheat, barely, rye) in an genetic predisposed
Refractory celiac disease (RCD) KASSEM BARADA LEBANESE SOCIETY OF GASTROENTEROLOGY NOVEMBER, 2014
 KASSEM BARADA LEBANESE SOCIETY OF GASTROENTEROLOGY NOVEMBER, 2014") Refractory celiac disease (RCD) KASSEM BARADA LEBANESE SOCIETY OF GASTROENTEROLOGY NOVEMBER, 2014 Case scenario (1) A 49 year woman presents with intermittent watery diarrhea and bloating of two years
Refractory celiac disease (RCD) KASSEM BARADA LEBANESE SOCIETY OF GASTROENTEROLOGY NOVEMBER, 2014 Case scenario (1) A 49 year woman presents with intermittent watery diarrhea and bloating of two years
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE SCOPE. Coeliac disease: recognition, assessment and management of coeliac disease
 Appendix B: NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE 1 Guideline title SCOPE Coeliac disease: recognition, assessment and management of coeliac disease 1.1 Short title Coeliac disease 2 The remit
Appendix B: NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE 1 Guideline title SCOPE Coeliac disease: recognition, assessment and management of coeliac disease 1.1 Short title Coeliac disease 2 The remit
Dr Kristin Kenrick. Senior Lecturer Dunedin School of Medicine
 Dr Kristin Kenrick Senior Lecturer Dunedin School of Medicine Kristin Kenrick, FRNZCGP Department of General Practice and Rural Health Dunedin School of Medicine (Supported by Coeliac New Zealand) Because
Dr Kristin Kenrick Senior Lecturer Dunedin School of Medicine Kristin Kenrick, FRNZCGP Department of General Practice and Rural Health Dunedin School of Medicine (Supported by Coeliac New Zealand) Because
Malabsorption is characterized by defective absorption of: Fats fat- and water-soluble vitamins Proteins Carbohydrates Electrolytes Minerals water
 Malabsorption Malabsorption is characterized by defective absorption of: Fats fat- and water-soluble vitamins Proteins Carbohydrates Electrolytes Minerals water presents most commonly as chronic diarrhea
Malabsorption Malabsorption is characterized by defective absorption of: Fats fat- and water-soluble vitamins Proteins Carbohydrates Electrolytes Minerals water presents most commonly as chronic diarrhea
Laboratory Methods for Diagnosing Celiac Disease. Vijay Kumar, PhD, FACB IMMCO Diagnostics, Inc. Buffalo, NY
 Laboratory Methods for Diagnosing Celiac Disease Vijay Kumar, PhD, FACB IMMCO Diagnostics, Inc. Buffalo, NY Prevalence of Celiac Disease Group With Symptoms Adults Children Associated Symptoms Chronic
Laboratory Methods for Diagnosing Celiac Disease Vijay Kumar, PhD, FACB IMMCO Diagnostics, Inc. Buffalo, NY Prevalence of Celiac Disease Group With Symptoms Adults Children Associated Symptoms Chronic
Celiac Disease (CD) Diagnosis and Whom to Screen
 Diagnosis and Whom to Screen") Celiac Disease (CD) Diagnosis and Whom to Screen Maureen Leonard MD Fellow, MassGeneral Hospital for Children Twitter-Follow me @CeliacDoc Follow the MGH Celiac Center @CeliacResearch Conflicts of Interest
Celiac Disease (CD) Diagnosis and Whom to Screen Maureen Leonard MD Fellow, MassGeneral Hospital for Children Twitter-Follow me @CeliacDoc Follow the MGH Celiac Center @CeliacResearch Conflicts of Interest
Coeliac Disease in 2016: A shared care between GPs and gastroenterologists. Dr Roslyn Vongsuvanh
 Coeliac Disease in 2016: A shared care between GPs and gastroenterologists Dr Roslyn Vongsuvanh Ms JM 23 year old female Born in Australia. Parents from Lebanon. Engineering student Presents with lethargy
Coeliac Disease in 2016: A shared care between GPs and gastroenterologists Dr Roslyn Vongsuvanh Ms JM 23 year old female Born in Australia. Parents from Lebanon. Engineering student Presents with lethargy
Summary for the Diagnosis of Gluten-Sensitive Entropathy Celiac Disease
 Summary for the Diagnosis of Gluten-Sensitive Entropathy Celiac Disease Celiac disease is an immune medical condition that is caused by ingestion of gluten in genetically susceptible individuals. The damage
Summary for the Diagnosis of Gluten-Sensitive Entropathy Celiac Disease Celiac disease is an immune medical condition that is caused by ingestion of gluten in genetically susceptible individuals. The damage
Celiac Disease. Marian Rewers, MD, PhD. Professor & Clinical Director Barbara Davis Center for Diabetes University of Colorado School of Medicine
 Celiac Disease Marian Rewers, MD, PhD Professor & Clinical Director Barbara Davis Center for Diabetes University of Colorado School of Medicine No relevant financial relationships with any commercial interests
Celiac Disease Marian Rewers, MD, PhD Professor & Clinical Director Barbara Davis Center for Diabetes University of Colorado School of Medicine No relevant financial relationships with any commercial interests
Level 2. Non Responsive Celiac Disease KEY POINTS:
 Level 2 Non Responsive Celiac Disease KEY POINTS: Celiac Disease (CD) is an autoimmune condition triggered by ingestion of gluten leading to intestinal damage and a variety of clinical manifestations.
Level 2 Non Responsive Celiac Disease KEY POINTS: Celiac Disease (CD) is an autoimmune condition triggered by ingestion of gluten leading to intestinal damage and a variety of clinical manifestations.
NICE guideline Published: 2 September 2015 nice.org.uk/guidance/ng20
 Coeliac disease: recognition, assessment and management NICE guideline Published: 2 September 2015 nice.org.uk/guidance/ng20 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Coeliac disease: recognition, assessment and management NICE guideline Published: 2 September 2015 nice.org.uk/guidance/ng20 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Done By : shady soghayr
 Done By : shady soghayr Malabsorption Malabsorption is characterized by defective absorption of: Fats fat- and water-soluble vitamins Proteins Carbohydrates Electrolytes Minerals Water presents most commonly
Done By : shady soghayr Malabsorption Malabsorption is characterized by defective absorption of: Fats fat- and water-soluble vitamins Proteins Carbohydrates Electrolytes Minerals Water presents most commonly
NIH Public Access Author Manuscript Am J Gastroenterol. Author manuscript; available in PMC 2014 May 01.
 NIH Public Access Author Manuscript Published in final edited form as: Am J Gastroenterol. 2013 May ; 108(5): 656 677. doi:10.1038/ajg.2013.79. AMERICAN COLLEGE OF GASTROENTEROLOGY CLINICAL GUIDELINE:
NIH Public Access Author Manuscript Published in final edited form as: Am J Gastroenterol. 2013 May ; 108(5): 656 677. doi:10.1038/ajg.2013.79. AMERICAN COLLEGE OF GASTROENTEROLOGY CLINICAL GUIDELINE:
Sheila E. Crowe, MD, FRCPC, FACP, FACG, AGAF Department of Medicine University of California, San Diego
 Severe and Emergency Presentations of Celiac Disease Sheila E. Crowe, MD, FRCPC, FACP, FACG, AGAF Department of Medicine University of California, San Diego Case Presentation (1) 63 year old male transferred
Severe and Emergency Presentations of Celiac Disease Sheila E. Crowe, MD, FRCPC, FACP, FACG, AGAF Department of Medicine University of California, San Diego Case Presentation (1) 63 year old male transferred
 SUMMARY Coeliac disease is a common food intolerance in Western populations, in which it has a prevalence of about 1%. In early infancy, when the transition is made to a gluten-containing diet (particularly
SUMMARY Coeliac disease is a common food intolerance in Western populations, in which it has a prevalence of about 1%. In early infancy, when the transition is made to a gluten-containing diet (particularly
Mashhad University of Medical Sciences. Azita Ganji MD, MPH
 Mashhad University of Medical Sciences Azita Ganji MD, MPH 30.2.95 CD Food sensitivity (NCGS, ) Food intolerance IBS Gluten translocate through the epithelial mucosa via increased tight junction (TJ)
Mashhad University of Medical Sciences Azita Ganji MD, MPH 30.2.95 CD Food sensitivity (NCGS, ) Food intolerance IBS Gluten translocate through the epithelial mucosa via increased tight junction (TJ)
The Changing Face of Celiac Disease. John Snyder, MD
 The Changing Face of Celiac Disease John Snyder, MD Special Thanks Blair and Steve Raber, founders of the Children s National Celiac Disease Program Rhonda and Peter Resnick, for providing a generous gift
The Changing Face of Celiac Disease John Snyder, MD Special Thanks Blair and Steve Raber, founders of the Children s National Celiac Disease Program Rhonda and Peter Resnick, for providing a generous gift
Supplemental Table 1: Moderate and severe definitions of Celiac Disease Symptom Diary
 Supplemental Table 1: Moderate and severe definitions of Celiac Disease Symptom Diary symptoms CDSD Symptom Diarrhea Constipation Abdominal Pain Bloating Nausea Tiredness Moderate Once or twice between
Supplemental Table 1: Moderate and severe definitions of Celiac Disease Symptom Diary symptoms CDSD Symptom Diarrhea Constipation Abdominal Pain Bloating Nausea Tiredness Moderate Once or twice between
Tuesday 10 th April 2018 Dr Rukhsana Hussain. Disclaimers apply:
 Tuesday 10 th April 2018 Dr Rukhsana Hussain What is Non-Coeliac Gluten Sensitivity (NCGS)? Symptoms Pathophysiology Diagnosis Treatment Summary NCGS is a condition in which consumption of gluten leads
Tuesday 10 th April 2018 Dr Rukhsana Hussain What is Non-Coeliac Gluten Sensitivity (NCGS)? Symptoms Pathophysiology Diagnosis Treatment Summary NCGS is a condition in which consumption of gluten leads
FM CFS leaky gut April pag 1
 FM CFS leaky gut April 21 2018 pag 1 FIBROMYALGIA / CHRONIC FATIGUE SYNDROME AND LEAKY GUT. SUMMARY OF CLINICAL TRIAL DESIGN. Double-blind randomized placebo-controlled challenge with gluten and milk protein
FM CFS leaky gut April 21 2018 pag 1 FIBROMYALGIA / CHRONIC FATIGUE SYNDROME AND LEAKY GUT. SUMMARY OF CLINICAL TRIAL DESIGN. Double-blind randomized placebo-controlled challenge with gluten and milk protein
GPMP and TCA Coeliac disease
 MP and TCA Coeliac disease ITEM: prepares MP (721) REVIEWS MP (732) prepared TCA (723) REVIEW TCA (732) PATIENT DETAILS: DETAILS: DATE PREPARED: Does a current management plan or Team care arrangement
MP and TCA Coeliac disease ITEM: prepares MP (721) REVIEWS MP (732) prepared TCA (723) REVIEW TCA (732) PATIENT DETAILS: DETAILS: DATE PREPARED: Does a current management plan or Team care arrangement
Histologic Follow-up of People With Celiac Disease on a Gluten-Free Diet Slow and Incomplete Recovery
 Anatomic Pathology / HISTOLOGIC FOLLOW-UP OF PEOPLE WITH CELIAC DISEASE ON A GLUTEN-FREE DIET Histologic Follow-up of People With Celiac Disease on a Gluten-Free Diet Slow and Incomplete Recovery Peter
Anatomic Pathology / HISTOLOGIC FOLLOW-UP OF PEOPLE WITH CELIAC DISEASE ON A GLUTEN-FREE DIET Histologic Follow-up of People With Celiac Disease on a Gluten-Free Diet Slow and Incomplete Recovery Peter
Coeliac Disease: Symptoms, Diagnosis, Treatment and Management
 Coeliac Disease: Symptoms, Diagnosis, Treatment and Management Dr Matthew Kurien Senior Clinical Lecturer and Honorary Consultant Gastroenterologist, University of Sheffield Benign Diseases Talk Outline
Coeliac Disease: Symptoms, Diagnosis, Treatment and Management Dr Matthew Kurien Senior Clinical Lecturer and Honorary Consultant Gastroenterologist, University of Sheffield Benign Diseases Talk Outline
The Changing Face of Celiac Disease. John Snyder, MD
 The Changing Face of Celiac Disease John Snyder, MD OVERVIEW Brief Background on the Basics Changing Face 1. Autoimmune Nature and Impact 2. Diagnosis Does everyone need a biopsy? Should genetic testing
The Changing Face of Celiac Disease John Snyder, MD OVERVIEW Brief Background on the Basics Changing Face 1. Autoimmune Nature and Impact 2. Diagnosis Does everyone need a biopsy? Should genetic testing
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
OHTAC Recommendation
 OHTAC Recommendation Clinical Utility of Serologic Testing for Celiac Disease in Asymptomatic Patients Presented to the Ontario Health Technology Advisory Committee in May and June 2011 July 2011 Background
OHTAC Recommendation Clinical Utility of Serologic Testing for Celiac Disease in Asymptomatic Patients Presented to the Ontario Health Technology Advisory Committee in May and June 2011 July 2011 Background
CELIAC DISEASE. A Family Physician Perspective. Dr. Kanwal Brar BSc MD CCFP June 6, 2015
 CELIAC DISEASE A Family Physician Perspective Dr. Kanwal Brar BSc MD CCFP June 6, 2015 Conflict of interest: No conflicts of interest or medical disclosures pertaining to this talk Objectives: Through
CELIAC DISEASE A Family Physician Perspective Dr. Kanwal Brar BSc MD CCFP June 6, 2015 Conflict of interest: No conflicts of interest or medical disclosures pertaining to this talk Objectives: Through
Preface and outline of the thesis
 Preface Celiac disease (CD) is characterized by a chronic immune reaction in the small intestine to the gluten proteins that are present in a (Western) daily diet, derived from wheat, barley and rye. It
Preface Celiac disease (CD) is characterized by a chronic immune reaction in the small intestine to the gluten proteins that are present in a (Western) daily diet, derived from wheat, barley and rye. It
A Practical Approach to Small Bowel Biopsies: All that flattens is not sprue
 A Practical Approach to Small Bowel Biopsies: All that flattens is not sprue UCSF Liver and Gastrointestinal Pathology Update Sept. 4, 2009 How to Go Wrong When Evaluating Small Bowel Biopsies, Based on
A Practical Approach to Small Bowel Biopsies: All that flattens is not sprue UCSF Liver and Gastrointestinal Pathology Update Sept. 4, 2009 How to Go Wrong When Evaluating Small Bowel Biopsies, Based on
Treatment of celiac disease: expected outcomes and how to address the refractory patient Joseph A Murray The Mayo Clinic Rochester, MN 55906
 Treatment of celiac disease: expected outcomes and how to address the refractory patient Joseph A Murray The Mayo Clinic Rochester, MN 55906 OBJECTIVES 1. To outline the expected results of treatment with
Treatment of celiac disease: expected outcomes and how to address the refractory patient Joseph A Murray The Mayo Clinic Rochester, MN 55906 OBJECTIVES 1. To outline the expected results of treatment with
WALSALL COELIAC DISEASE FLOWCHART
 WALSALL COELIAC DISEASE FLOWCHART CLINICAL SUSPICION OF COELIAC DISEASE ( Which can present at any age ) [see Box A or Box B] DO NOT START GLUTEN FREE DIET BEFORE ANY INVESTIGATIONS Test for IgA Tissue
WALSALL COELIAC DISEASE FLOWCHART CLINICAL SUSPICION OF COELIAC DISEASE ( Which can present at any age ) [see Box A or Box B] DO NOT START GLUTEN FREE DIET BEFORE ANY INVESTIGATIONS Test for IgA Tissue
Lower Gastrointestinal Tract KNH 406
 Lower Gastrointestinal Tract KNH 406 Lower GI Tract A&P Small Intestine Anatomy Duodenum, jejunum, ileum Maximum surface area for digestion and absorption Specialized enterocytes from stem cells of crypts
Lower Gastrointestinal Tract KNH 406 Lower GI Tract A&P Small Intestine Anatomy Duodenum, jejunum, ileum Maximum surface area for digestion and absorption Specialized enterocytes from stem cells of crypts
GLUTEN RELATED DISORDERS
 Celiac disease Overcoming clinical challenges Disclosures Scientific Advisory Board Cellimune, Immunsant, Innovate Pharmaceuticals Peter HR Green MD Phyllis and Ivan Seidenberg Professor of Medicine Director,
Celiac disease Overcoming clinical challenges Disclosures Scientific Advisory Board Cellimune, Immunsant, Innovate Pharmaceuticals Peter HR Green MD Phyllis and Ivan Seidenberg Professor of Medicine Director,
PATHOLOGY OF NON NEOPLASTIC LESIONS OF THE UPPER GASTROINTESTINAL TRACT.
 PATHOLOGY OF NON NEOPLASTIC LESIONS OF THE UPPER GASTROINTESTINAL TRACT. OESOPHAGEAL LESIONS OESOPHAGITIS AND OTHER NON NEOPLASTIC DISORDERS Corrosive Gastroesophageal reflux (GERD), Pills, Acid intake,
PATHOLOGY OF NON NEOPLASTIC LESIONS OF THE UPPER GASTROINTESTINAL TRACT. OESOPHAGEAL LESIONS OESOPHAGITIS AND OTHER NON NEOPLASTIC DISORDERS Corrosive Gastroesophageal reflux (GERD), Pills, Acid intake,
New and Emerging Therapies for Gluten-Related Conditions
 New and Emerging Therapies for Gluten-Related Conditions Jocelyn Silvester, MD PhD FRCPC June 11, 2017 Disclosures Funding CIHR, NIH, Canadian Celiac Association Collaboration Biomedal SG Glutenostics
New and Emerging Therapies for Gluten-Related Conditions Jocelyn Silvester, MD PhD FRCPC June 11, 2017 Disclosures Funding CIHR, NIH, Canadian Celiac Association Collaboration Biomedal SG Glutenostics
Non responsive coeliac disease: next steps for investigation. Dr Peter Mooney Clinical Research Fellow Royal Hallamshire Hospital, Sheffield, UK
 Non responsive coeliac disease: next steps for investigation Dr Peter Mooney Clinical Research Fellow Royal Hallamshire Hospital, Sheffield, UK Outline Cases Non Responsive Coeliac Disease Causes Investigation
Non responsive coeliac disease: next steps for investigation Dr Peter Mooney Clinical Research Fellow Royal Hallamshire Hospital, Sheffield, UK Outline Cases Non Responsive Coeliac Disease Causes Investigation
Jackson Madison Vicksburg
 Celiac Sprue Table of contents GI ASSOCIATES ED U CATIO N AL SERIES Celiac Sprue What is it? 1 What causes sprue? How common is it? What are the risk factors? Lupus Erythematosus Type 1 diabetes (juvenile
Celiac Sprue Table of contents GI ASSOCIATES ED U CATIO N AL SERIES Celiac Sprue What is it? 1 What causes sprue? How common is it? What are the risk factors? Lupus Erythematosus Type 1 diabetes (juvenile
The management of adults with coeliac disease in primary care
 The management of adults with coeliac disease in primary care The purpose of this document is to assist healthcare professionals who are responsible for the diagnosis and management of patients with coeliac
The management of adults with coeliac disease in primary care The purpose of this document is to assist healthcare professionals who are responsible for the diagnosis and management of patients with coeliac
Novita In Tema Di Alternative Alla Dieta Aglutinata
 Novita In Tema Di Alternative Alla Dieta Aglutinata Alessio Fasano, M.D. W. Allan Walker Chair in Pediatric Gastroenterology and Nutrition Professor of Pediatrics Harvard Medical School Mucosal Biology
Novita In Tema Di Alternative Alla Dieta Aglutinata Alessio Fasano, M.D. W. Allan Walker Chair in Pediatric Gastroenterology and Nutrition Professor of Pediatrics Harvard Medical School Mucosal Biology
(Leven and Tomer, 3002). González et al, 3002). Reffubat et al, 7002). (ISPAD) 3000
. González et al, 3002). Reffubat et al, 7002). (ISPAD) 3000") The association between type 1 diabetes mellitus and autoimmune thyroid diseases has long been documented. Both are organ specific T- cell mediated disease, and have a similar pathogenesis, which involves
The association between type 1 diabetes mellitus and autoimmune thyroid diseases has long been documented. Both are organ specific T- cell mediated disease, and have a similar pathogenesis, which involves
Female Collegiate Volleyball Player with Celiac Disease: A Case Report
 Female Collegiate Volleyball Player with Celiac Disease: A Case Report Lindsey E. Eberman, Michelle A. Cleary, Ron E. Zuri, and Gary Salvador Florida International University, USA Abstract: Estimates of
Female Collegiate Volleyball Player with Celiac Disease: A Case Report Lindsey E. Eberman, Michelle A. Cleary, Ron E. Zuri, and Gary Salvador Florida International University, USA Abstract: Estimates of
Clinical Utility of Serologic Testing for Celiac Disease in Asymptomatic Patients
 Ontario Health Technology Assessment Series 2011; Vol. 11, No. 3 Clinical Utility of Serologic Testing for Celiac Disease in Asymptomatic Patients An Evidence-Based Analysis July 2011 Medical Advisory
Ontario Health Technology Assessment Series 2011; Vol. 11, No. 3 Clinical Utility of Serologic Testing for Celiac Disease in Asymptomatic Patients An Evidence-Based Analysis July 2011 Medical Advisory
PEDIATRIC INFLAMMATORY BOWEL DISEASE
 PEDIATRIC INFLAMMATORY BOWEL DISEASE Alexis Rodriguez, MD Pediatric Gastroenterology Advocate Children s Hospital Disclosers Abbott Nutrition - Speaker Inflammatory Bowel Disease Chronic inflammatory disease
PEDIATRIC INFLAMMATORY BOWEL DISEASE Alexis Rodriguez, MD Pediatric Gastroenterology Advocate Children s Hospital Disclosers Abbott Nutrition - Speaker Inflammatory Bowel Disease Chronic inflammatory disease
Prescribing Guidelines on Gluten-Free products. Information for GPs
 Prescribing Guidelines on Gluten-Free products Information for GPs This guideline should be used in conjunction with NICE clinical guideline 86 Coeliac disease: recognition and assessment of coeliac disease.
Prescribing Guidelines on Gluten-Free products Information for GPs This guideline should be used in conjunction with NICE clinical guideline 86 Coeliac disease: recognition and assessment of coeliac disease.
Treatment of Inflammatory Bowel Disease. Michael Weiss MD, FACG
 Treatment of Inflammatory Bowel Disease Michael Weiss MD, FACG What is IBD? IBD is an immune-mediated chronic intestinal disorder, characterized by chronic or relapsing inflammation within the GI tract.
Treatment of Inflammatory Bowel Disease Michael Weiss MD, FACG What is IBD? IBD is an immune-mediated chronic intestinal disorder, characterized by chronic or relapsing inflammation within the GI tract.
Video Capsule Endoscopy in the Evaluation of Celiac Patients with Persistent or Recurrent Symptoms. Who and When?
 International Journal of Celiac Disease, 2016, Vol. 4, No. 2, xx Available online at http://pubs.sciepub.com/ijcd/4/2/5 Science and Education Publishing DOI:10.12691/ijcd-4-2-5 Video Capsule Endoscopy
International Journal of Celiac Disease, 2016, Vol. 4, No. 2, xx Available online at http://pubs.sciepub.com/ijcd/4/2/5 Science and Education Publishing DOI:10.12691/ijcd-4-2-5 Video Capsule Endoscopy
Southern Derbyshire Shared Care Pathology Guidelines. Coeliac Disease
 Southern Derbyshire Shared Care Pathology Guidelines Coeliac Disease Purpose of Guideline When and how to investigate patients for Coeliac Disease What the results mean When and how to refer patients Monitoring
Southern Derbyshire Shared Care Pathology Guidelines Coeliac Disease Purpose of Guideline When and how to investigate patients for Coeliac Disease What the results mean When and how to refer patients Monitoring
Follow-up of Celiac Disease
 Follow-up of Celiac Disease Benjamin Lebwohl MD, MS Director of Clinical Research Celiac Disease Center Columbia University celiacdiseasecenter.org BL114@columbia.edu @BenjaminLebwohl Disclosures None
Follow-up of Celiac Disease Benjamin Lebwohl MD, MS Director of Clinical Research Celiac Disease Center Columbia University celiacdiseasecenter.org BL114@columbia.edu @BenjaminLebwohl Disclosures None
Guidelines NICE, not NICE and the Daily Mail. Dr Andy Poullis Consultant Gastroenterologist
 Guidelines NICE, not NICE and the Daily Mail 2018 Dr Andy Poullis Consultant Gastroenterologist Coeliac IBS Gall bladder polyps PEI PPI Who to test for Coeliac persistent unexplained abdominal or gastrointestinal
Guidelines NICE, not NICE and the Daily Mail 2018 Dr Andy Poullis Consultant Gastroenterologist Coeliac IBS Gall bladder polyps PEI PPI Who to test for Coeliac persistent unexplained abdominal or gastrointestinal
Coeliac disease in children
 Art & science paediatric nursing Coeliac disease in children Paul SP et al (2015) Coeliac disease in children. Nursing Standard. 29, 49, 36-41. Date of submission: March 2 2015; date of acceptance: March
Art & science paediatric nursing Coeliac disease in children Paul SP et al (2015) Coeliac disease in children. Nursing Standard. 29, 49, 36-41. Date of submission: March 2 2015; date of acceptance: March
ORIGINAL ARTICLE Histopathological features of coeliac disease in a sample of Sudanese patients
 Malaysian J Pathol 2016; 38(3) : 267 272 ORIGINAL ARTICLE Histopathological features of coeliac disease in a sample of Sudanese patients MA Noha MOKHTAR, SO MEKKI, HMY MUDAWI*, SH SULAIMAN**, MA TAHIR,
Malaysian J Pathol 2016; 38(3) : 267 272 ORIGINAL ARTICLE Histopathological features of coeliac disease in a sample of Sudanese patients MA Noha MOKHTAR, SO MEKKI, HMY MUDAWI*, SH SULAIMAN**, MA TAHIR,
Bowel cancer risk in the under 50s. Greg Rubin Professor of General Practice and Primary Care
 Bowel cancer risk in the under 50s Greg Rubin Professor of General Practice and Primary Care Prevalence of GI problems in the consulting population Thompson et al, Gut 2000 Number of patients % of patients
Bowel cancer risk in the under 50s Greg Rubin Professor of General Practice and Primary Care Prevalence of GI problems in the consulting population Thompson et al, Gut 2000 Number of patients % of patients
Food Choices and Alternative Techniques in Management of IBS: Fad Versus Evidence
 Food Choices and Alternative Techniques in Management of IBS: Fad Versus Evidence Maria Vazquez Roque, MD, MSc Assistant Professor Gastroenterology and Hepatology 2010 MFMER slide-1 Objectives Gluten-free
Food Choices and Alternative Techniques in Management of IBS: Fad Versus Evidence Maria Vazquez Roque, MD, MSc Assistant Professor Gastroenterology and Hepatology 2010 MFMER slide-1 Objectives Gluten-free
IBD 101. Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition
 IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
Supplemental Information
 SPECIAL ARTICLE Supplemental Information 1. VOTING ON BEST PRACTICE STATEMENTS AND GRADING THE STATEMENTS FOR QUALITY OF EVIDENCE The group voted on statements and questions developed from each of the
SPECIAL ARTICLE Supplemental Information 1. VOTING ON BEST PRACTICE STATEMENTS AND GRADING THE STATEMENTS FOR QUALITY OF EVIDENCE The group voted on statements and questions developed from each of the
EDUCATION PRACTICE. Celiac Disease and Persistent Symptoms. Clinical Scenario. The Problem
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2011;9:13 17 EDUCATION PRACTICE Celiac Disease and Persistent Symptoms ALBERTO RUBIO TAPIA, SUSAN H. BARTON, and JOSEPH A. MURRAY Division of Gastroenterology and
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2011;9:13 17 EDUCATION PRACTICE Celiac Disease and Persistent Symptoms ALBERTO RUBIO TAPIA, SUSAN H. BARTON, and JOSEPH A. MURRAY Division of Gastroenterology and
IBD 101. Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition
 IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
2. What is the etiology of celiac disease? Is anything in Mrs. Gaines s history typical of patients with celiac disease? Explain
 Pauline Huang NFSC 470 Case Study I. Understanding the Disease and Pathophysiology 1. The small bowel biopsy results state, flat mucosa with villus atrophy and hyperplastic crypts inflammatory infiltrate
Pauline Huang NFSC 470 Case Study I. Understanding the Disease and Pathophysiology 1. The small bowel biopsy results state, flat mucosa with villus atrophy and hyperplastic crypts inflammatory infiltrate
COSA NON È CELIACHIA ( uno sguardo obliquo )
") COSA NON È CELIACHIA ( uno sguardo obliquo ) Gino Roberto Corazza I Clinica Medica Fondazione IRCCS Policlinico San Matteo Università di Pavia HOLY PAPERS OF COELIAC DISEASE Gut 2012 Gut 2014 JPGN 2012
COSA NON È CELIACHIA ( uno sguardo obliquo ) Gino Roberto Corazza I Clinica Medica Fondazione IRCCS Policlinico San Matteo Università di Pavia HOLY PAPERS OF COELIAC DISEASE Gut 2012 Gut 2014 JPGN 2012
Digestive System 2. Lecture 12. Pathology and Clinical Science 1 (BIOC211) Department of Bioscience. endeavour.edu.au
 Department of Bioscience. endeavour.edu.au") Digestive System 2 Lecture 12 Pathology and Clinical Science 1 (BIOC211) Department of Bioscience Text Reference: Grossman, S.C. & Porth, C.M. (2014). Porth s Pathophysiology: concepts of altered health
Digestive System 2 Lecture 12 Pathology and Clinical Science 1 (BIOC211) Department of Bioscience Text Reference: Grossman, S.C. & Porth, C.M. (2014). Porth s Pathophysiology: concepts of altered health
Massachusetts ACP Meeting Update in Gastroenterology and Hepatology
 Massachusetts ACP Meeting Update in Gastroenterology and Hepatology November 19 th, 2016 Norton J. Greenberger, MD Senior Attending Physician Brigham and Women s Hospital 1 Agenda Stomach and Small Bowel
Massachusetts ACP Meeting Update in Gastroenterology and Hepatology November 19 th, 2016 Norton J. Greenberger, MD Senior Attending Physician Brigham and Women s Hospital 1 Agenda Stomach and Small Bowel
British Society of Gastroenterology. The Management of Adults with Coeliac Disease
 British Society of Gastroenterology The Management of Adults with Coeliac Disease Ciclitira P J, Dewar D H, McLaughlin S D, Sanders DS Index 1.0 Preface 1.1 Purpose of Guidelines 1.2 Formulation of Guidelines
British Society of Gastroenterology The Management of Adults with Coeliac Disease Ciclitira P J, Dewar D H, McLaughlin S D, Sanders DS Index 1.0 Preface 1.1 Purpose of Guidelines 1.2 Formulation of Guidelines
Case Report Seronegative Intestinal Villous Atrophy: A Diagnostic Challenge
 Case Reports in Gastrointestinal Medicine Volume 2016, Article ID 6392028, 4 pages http://dx.doi.org/10.1155/2016/6392028 Case Report Seronegative Intestinal Villous Atrophy: A Diagnostic Challenge Cláudio
Case Reports in Gastrointestinal Medicine Volume 2016, Article ID 6392028, 4 pages http://dx.doi.org/10.1155/2016/6392028 Case Report Seronegative Intestinal Villous Atrophy: A Diagnostic Challenge Cláudio
This report is a comprehensive review of the current
 GASTROENTEROLOGY 2001;120:1526 1540 AGA Technical Review on Celiac Sprue The literature review and the recommendations therein were prepared for the American Gastroenterological Association (AGA) Clinical
GASTROENTEROLOGY 2001;120:1526 1540 AGA Technical Review on Celiac Sprue The literature review and the recommendations therein were prepared for the American Gastroenterological Association (AGA) Clinical
What is your diagnosis? a. Lymphocytic colitis. b. Collagenous colitis. c. Common variable immunodeficiency (CVID) associated colitis
 associated colitis") Case History A 24 year old male presented with fatigue, fever, watery diarrhea, and a cough with sputum production for the past three weeks. His past medical history was significant for recurrent bouts
Case History A 24 year old male presented with fatigue, fever, watery diarrhea, and a cough with sputum production for the past three weeks. His past medical history was significant for recurrent bouts
You Can Read This. Tricks to help keep your graphics clean and easy to understand
 You Can Read This. Tricks to help keep your graphics clean and easy to understand Present. It s inevitable. You re going to have to present something at least once in college. Here s some things to consider:
You Can Read This. Tricks to help keep your graphics clean and easy to understand Present. It s inevitable. You re going to have to present something at least once in college. Here s some things to consider:
Medical Nutrition Therapy: A Case Study Approach 3rd Ed. Case Study 12- Celiac Disease
 Medical Nutrition Therapy: A Case Study Approach 3rd Ed. Case Study 12- Celiac Disease I. Understanding the Disease and Pathophysiology 1. The small bowel biopsy results state, flat mucosa with villus
Medical Nutrition Therapy: A Case Study Approach 3rd Ed. Case Study 12- Celiac Disease I. Understanding the Disease and Pathophysiology 1. The small bowel biopsy results state, flat mucosa with villus
Inflammatory Bowel Diseases (IBD) Clinical aspects Nitsan Maharshak M.D., IBD Center, Department of Gastroenterology and Liver Diseases Tel Aviv Soura
 Clinical aspects Nitsan Maharshak M.D., IBD Center, Department of Gastroenterology and Liver Diseases Tel Aviv Soura") Inflammatory Bowel Diseases (IBD) Clinical aspects Nitsan Maharshak M.D., IBD Center, Department of Gastroenterology and Liver Diseases Tel Aviv Sourasky Medical Center Tel Aviv, Israel IBD- clinical features
Inflammatory Bowel Diseases (IBD) Clinical aspects Nitsan Maharshak M.D., IBD Center, Department of Gastroenterology and Liver Diseases Tel Aviv Sourasky Medical Center Tel Aviv, Israel IBD- clinical features
GI update. Common conditions and concerns my patients frequently asked about
 GI update Common conditions and concerns my patients frequently asked about Specific conditions I ll try to cover today 1. Colon polyps, colorectal cancer and colonoscopy 2. Crohn s disease 3. Peptic ulcer
GI update Common conditions and concerns my patients frequently asked about Specific conditions I ll try to cover today 1. Colon polyps, colorectal cancer and colonoscopy 2. Crohn s disease 3. Peptic ulcer
Copyright ESPGHAN and NASPGHAN. All rights reserved.
 JPGN Journal of Pediatric Gastroenterology and Nutrition Publish Ahead of Print DOI: 10.1097/MPG.0b013e31821a23d0 ESPGHAN guidelines for the diagnosis of coeliac disease in children and adolescents. An
JPGN Journal of Pediatric Gastroenterology and Nutrition Publish Ahead of Print DOI: 10.1097/MPG.0b013e31821a23d0 ESPGHAN guidelines for the diagnosis of coeliac disease in children and adolescents. An
Diagnosis and management of adult coeliac disease: guidelines from the British Society of Gastroenterology
 For numbered affiliations see end of article. Correspondence to David S Sanders, Gastroenterology and Liver Unit, Royal Hallamshire Hospital & University of Sheffield, Sheffield S10 2JF, UK; david.sanders@sth.nhs.uk
For numbered affiliations see end of article. Correspondence to David S Sanders, Gastroenterology and Liver Unit, Royal Hallamshire Hospital & University of Sheffield, Sheffield S10 2JF, UK; david.sanders@sth.nhs.uk
Digestion: Small and Large Intestines Pathology
 Digestion: Small and Large Intestines Pathology Dr. Ritamarie Loscalzo Medical Disclaimer: The information in this presentation is not intended to replace a one onone relationship with a qualified health
Digestion: Small and Large Intestines Pathology Dr. Ritamarie Loscalzo Medical Disclaimer: The information in this presentation is not intended to replace a one onone relationship with a qualified health
Manifestations of gastrointestinal diseases in the oral cavity. Nabil El-Lababidi
 Manifestations of gastrointestinal diseases in the oral cavity Nabil El-Lababidi Types of mouth affections in conjunction with GIT diseases I. Glossitis: Crohn s disease Coeliac disease Kwashiorkhor Malabsorption
Manifestations of gastrointestinal diseases in the oral cavity Nabil El-Lababidi Types of mouth affections in conjunction with GIT diseases I. Glossitis: Crohn s disease Coeliac disease Kwashiorkhor Malabsorption
Allergic disorders of the gastrointestinal tract
 Allergic disorders of the gastrointestinal tract Christopher Justinich, MD Introduction The patient with presumed food hypersensitivity continues to present a challenge for the clinician. In certain instances,
Allergic disorders of the gastrointestinal tract Christopher Justinich, MD Introduction The patient with presumed food hypersensitivity continues to present a challenge for the clinician. In certain instances,
Autoimmune diseases in Turner syndrome
 International Congress Series 1298 (2006) 42 48 www.ics-elsevier.com Autoimmune diseases in Turner syndrome L. Mazzanti a,, R.W. Naeraa b a Department of Pediatrics, University of Bologna, S. Orsola-Malpighi
International Congress Series 1298 (2006) 42 48 www.ics-elsevier.com Autoimmune diseases in Turner syndrome L. Mazzanti a,, R.W. Naeraa b a Department of Pediatrics, University of Bologna, S. Orsola-Malpighi
Non coeliac gluten sensitivity: Clinical relevance and recommendations for future research
 Non coeliac gluten sensitivity: Clinical relevance and recommendations for future research Valencia 2014 Professor David S Sanders Royal Hallamshire Hospital & University of Sheffield, UK Why is the prevalence
Non coeliac gluten sensitivity: Clinical relevance and recommendations for future research Valencia 2014 Professor David S Sanders Royal Hallamshire Hospital & University of Sheffield, UK Why is the prevalence
Dermatitis Herpetiformis (DH) in Association with H. pylori Infection: Description of a Case Report
 in Association with H. pylori Infection: Description of a Case Report") British Journal of Medicine & Medical Research 1(3): 163-169, 2011 SCIENCEDOMAIN international www.sciencedomain.org Dermatitis Herpetiformis (DH) in Association with H. pylori Infection: Description of
British Journal of Medicine & Medical Research 1(3): 163-169, 2011 SCIENCEDOMAIN international www.sciencedomain.org Dermatitis Herpetiformis (DH) in Association with H. pylori Infection: Description of
Serologic Markers CONVENTIONAL ANTIBODIES ANTIBODIES UNCONVENTIONAL. AIH Type I
 Autoimmune Hepatitis By Thomas Frazier Objective What we need to know about AIH Diagnosis Treatment Difficulties in both Liver transplantation concerns AASLD Guidelines: Hepatology. 2010 Jun;51(6):2193-213.
Autoimmune Hepatitis By Thomas Frazier Objective What we need to know about AIH Diagnosis Treatment Difficulties in both Liver transplantation concerns AASLD Guidelines: Hepatology. 2010 Jun;51(6):2193-213.
Prevalence of dental findings of children with celiac disease in Libya: a comparative study
 CASE STUDIES Prevalence of dental findings of children with celiac disease in Libya: a comparative study Khadiga Herwis, Heballah Elturki, Ahmed Ali Department of Pediatric Dentistry, Faculty of Dentistry,
CASE STUDIES Prevalence of dental findings of children with celiac disease in Libya: a comparative study Khadiga Herwis, Heballah Elturki, Ahmed Ali Department of Pediatric Dentistry, Faculty of Dentistry,
Coeliac disease. Questions and Controversies. Professor Andrew Day Paediatric Gastroenterology University of Otago, Christchurch
 Coeliac disease Questions and Controversies Professor Andrew Day Paediatric Gastroenterology University of Otago, Christchurch What is Coeliac disease? Is Coeliac disease the same as it ever was? How to
Coeliac disease Questions and Controversies Professor Andrew Day Paediatric Gastroenterology University of Otago, Christchurch What is Coeliac disease? Is Coeliac disease the same as it ever was? How to
Jason Chan. School of Epidemiology, Public Health and Preventive Medicine. Faculty of Medicine. University of Ottawa
 The Burden of Biopsy-Proven Pediatric Celiac Disease in Ontario, Canada: Derivation of Health Administrative Data Algorithms and Determination of Health Services Utilization Jason Chan Thesis submitted
The Burden of Biopsy-Proven Pediatric Celiac Disease in Ontario, Canada: Derivation of Health Administrative Data Algorithms and Determination of Health Services Utilization Jason Chan Thesis submitted
PERSONALIZED MANAGEMENT OF CELIAC DISEASE: RISK STRATIFICATION AND NOVEL STRATEGIES FOR COMPLICATED PATIENTS
 UNIVERSITA DEGLI STUDI DI MILANO FACULTY OF MEDICINE AND SURGERY RESEARCH DOCTORATE IN GASTROENTEROLOGY CICLE XXVII PERSONALIZED MANAGEMENT OF CELIAC DISEASE: RISK STRATIFICATION AND NOVEL STRATEGIES FOR
UNIVERSITA DEGLI STUDI DI MILANO FACULTY OF MEDICINE AND SURGERY RESEARCH DOCTORATE IN GASTROENTEROLOGY CICLE XXVII PERSONALIZED MANAGEMENT OF CELIAC DISEASE: RISK STRATIFICATION AND NOVEL STRATEGIES FOR
COMMON PROBLEMS IN PAEDIATRIC GASTROENTEROLOGY AKSHAY BATRA CONSULTANT PAEDIATRIC GASTROENTEROLOGIST
 COMMON PROBLEMS IN PAEDIATRIC GASTROENTEROLOGY AKSHAY BATRA CONSULTANT PAEDIATRIC GASTROENTEROLOGIST Paediatric Gastroenterology : Referral Base Common problems Feeding difficulties in infancy Recurrent
COMMON PROBLEMS IN PAEDIATRIC GASTROENTEROLOGY AKSHAY BATRA CONSULTANT PAEDIATRIC GASTROENTEROLOGIST Paediatric Gastroenterology : Referral Base Common problems Feeding difficulties in infancy Recurrent
Diet and Gastrointestinal Problems
 Chapter 20 Diet and Gastrointestinal Problems Objectives Explain uses of diet therapy in gastrointestinal disturbances Identify foods allowed and disallowed in therapeutic diets discussed Adapt normal
Chapter 20 Diet and Gastrointestinal Problems Objectives Explain uses of diet therapy in gastrointestinal disturbances Identify foods allowed and disallowed in therapeutic diets discussed Adapt normal
The ImmuneCare Guide to. Gluten Sensitivity
 The ImmuneCare Guide to Gluten Sensitivity Gluten Sensitivity Introduction Gluten sensitivity, also called non-coeliac gluten sensitivity (NCGS), is a condition related to gluten ingestion that can cause
The ImmuneCare Guide to Gluten Sensitivity Gluten Sensitivity Introduction Gluten sensitivity, also called non-coeliac gluten sensitivity (NCGS), is a condition related to gluten ingestion that can cause
The Aging Digestive System
 The Aging Digestive System shows significant senescence in old age: less saliva food less flavorful, harder swallowing ~half of those over 65 yrs wear dentures gastric mucosa secretes less acid reduces
The Aging Digestive System shows significant senescence in old age: less saliva food less flavorful, harder swallowing ~half of those over 65 yrs wear dentures gastric mucosa secretes less acid reduces
Medical Necessity Guidelines: Upper GI Endoscopy: Certain Elective Procedures
 Medical Necessity Guidelines: Upper GI Endoscopy: Certain Elective Procedures Effective: October 11, 2017 Clinical documentation and prior authorization required Coverage guideline, no prior authorization
Medical Necessity Guidelines: Upper GI Endoscopy: Certain Elective Procedures Effective: October 11, 2017 Clinical documentation and prior authorization required Coverage guideline, no prior authorization
Coeliac Disease in Children and Adolescents with Type 1 Diabetes Mellitus
 Clin Pediatr Endocrinol 1998; 7(2), 125-129 Copyright 1998 by The Japanese Society for Pediatric Endocrinology Coeliac Disease in Children and Adolescents with Type 1 Diabetes Mellitus Francesco Chiarelli,
Clin Pediatr Endocrinol 1998; 7(2), 125-129 Copyright 1998 by The Japanese Society for Pediatric Endocrinology Coeliac Disease in Children and Adolescents with Type 1 Diabetes Mellitus Francesco Chiarelli,
Increased rates of pregnancy complications in women with celiac disease
 ORIGINAL ARTICLE Annals of Gastroenterology (2015) 28, 236-240 Increased rates of pregnancy complications in women with celiac disease Stephanie M. Moleski a, Christina C. Lindenmeyer b, J. Jon Veloski
ORIGINAL ARTICLE Annals of Gastroenterology (2015) 28, 236-240 Increased rates of pregnancy complications in women with celiac disease Stephanie M. Moleski a, Christina C. Lindenmeyer b, J. Jon Veloski
Biomarkers of GI tract diseases. By Dr. Gouse Mohiddin Shaik
 By Dr. Gouse Mohiddin Shaik Introduction The gastrointestinal (GI) tract is a complex system performing multiple biological functions which are anatomically distributed Site for food processing and absorption
By Dr. Gouse Mohiddin Shaik Introduction The gastrointestinal (GI) tract is a complex system performing multiple biological functions which are anatomically distributed Site for food processing and absorption
Diagnosis and management of adult coeliac disease: guidelines from the British Society of Gastroenterology
 Diagnosis and management of adult coeliac disease: guidelines from the British Society of Gastroenterology The Harvard community has made this article openly available. Please share how this access benefits
Diagnosis and management of adult coeliac disease: guidelines from the British Society of Gastroenterology The Harvard community has made this article openly available. Please share how this access benefits
Duodenal Perforation as an Unusual Celiac Disease Presentation in Two Patients
 Elmer Press Case Report Duodenal Perforation as an Unusual Celiac Disease Presentation in Two Patients Imad Absah a, e, Rayna M. Grothe a, D. Dean Potter b, Tsung-Teh Wu c, Joseph A. Murray d Abstract
Elmer Press Case Report Duodenal Perforation as an Unusual Celiac Disease Presentation in Two Patients Imad Absah a, e, Rayna M. Grothe a, D. Dean Potter b, Tsung-Teh Wu c, Joseph A. Murray d Abstract