PEDIATRIC TRAUMA I: ABDOMINAL TRAUMA BURNS. December 19, 2012
|
|
|
- Daniel Moore
- 6 years ago
- Views:
Transcription

1 PEDIATRIC TRAUMA I: ABDOMINAL TRAUMA BURNS Niel F. Miele,, M.D. December 19, 2012
2 EPIDEMIOLOGY Major Trauma responsible for <50% of mortality in children 1-14 years Majority are blunt, not penetrating Motor Vehicle crashes Falls House Fires
3 ABDOMINAL BLUNT TRAUMA Difficult to assess Few signs of external injury Associated head injuries Should be suspected in any child who has multiple systems injuries
4 ABDOMINAL BLUNT TRAUMA APPROACH Primary Survey Airway Maintenance with C-Spine Protection Breathing Circulation with hemorrhage control Pulse and Perfusion BP drop is late sign Disability: Neurologic status Exposure/Environmental control Secondary Survey
5 CASE 4 year old, rear seat passenger in MVC, lap belt only, unconscious, intubated at scene, BP = 66/40 Fluids? Minimal BP: x Age What type and how much? After 2 boluses, consider blood loss What if no access?

6 EZ IntraOsseous
7 DIAGNOSTIC STUDIES CT scan of abdomen standard of care Ultrasound is adjunct IVP and UCG indicated if blood at urethral meatus Foley is contraindicated Diagnostic Peritoneal Lavage is rare House Fires
8
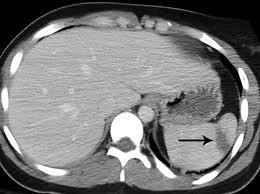
9 CASE 12 year old riding bicycle Flipped over front of bicycle; no LOC Handlebar hit below left rib cage Exam: Alert, awake No neck tenderness Slight LUQ tenderness
10 CASE Can you clear neck clinically?
11 CASE Clearing Clearing neck Awake, alert (not altered) Can answer questions No vertebral tenderness No distracting injuries
12 CASE Can you clear neck clinically? Do you image the abdomen? How? Abdominal series? Focused Abdominal Sonographic Technique? CT of abdomen with IV contrast?
13
14 SPLENIC LACERATION 5 Stages Consider non-operative management if: Grade I or II without a blush Stable hemoglobin over hours No clotting issues
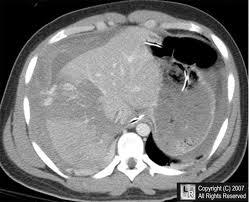
15 CASE Same patient, but pain is over right upper quadrant Do same imaging rules apply?
16
17 HOLLOW VISCUS INJURY Difficult to detect Consider if increasing abdominal pain or distension Vast majority require operative intervention Duodenal hematoma may be managed nonoperatively Most resolve in 1-3 weeks using gastric decompression only
18 BURNS: EPIDEMIOLOGY 2/3 are scald burns 1/5 are contact with hot substances Remainder are flame burns 10-30% may be due to abuse Cigarette burns Scald burns with straight line demarcation

19 FIRST DEGREE BURN Superficial, dry, painful to touch Heals in 1 week


20 SECOND DEGREE BURN Partial thickness Bullae or weeping, painful Heals in 1 to 3 weeks

21 THIRD DEGREE BURN May appear similar to 2 nd degree, but not painful Charred, hard, parchment-like Full-thickness
22 The rule of nines altered for the anthropomorphic differences of infancy and childhood. Klein G L, Herndon D N Pediatrics in Review 2004;25: by American Academy of Pediatrics
23 PATHOGENESIS Burn Shock and Burn Edema Loss of fluid from intravascular space Fluid accumulation in interstital space Inhalation Injury Hypermetabolism? SIRS
24 MANAGEMENT < 10% TBSA outpatient management Occlusive dressing with daily change Protect sking from contamination Eliminate air movement (reduces pain) Decrease water loss Topical antibiotics Silvadene Bacitracin
25 MANAGEMENT OF EXTENSIVE BURN Remove from scene, extinguish burn Remove jewelry Chemical burn Remove clothing and irrigate with water ABC s
26 SMOKE INHALATION IN BURNS Consider thermal injury Intubate if any stridor or hoarseness Consider intubation for soot in nose or below cords Consider carbon monoxide poisoning 100% Oxygen
27 IMMEDIATE MANAGEMENT ABC S Cool sterile saline dressings? Debride blisters Cover with topical antibiotics Separate fingers Pain management Check tetanus status IV/IO access
28 FLUID MANAGEMENT Parkland Formula (for replacement) Wt (kg) x % TBSA x 4 1 st half in 8 hours, 2 nd half in 16 hours Don t forget maintenace fluids Further fluid management may be adjusted to keep urine > 1 ml/kg/hr
29 CRITERIA FOR BURN CENTER >20% TBSA, or >10% TBSA in children < 10 years 3 rd degree burns > 5% TBSA 2 nd or 3 rd degree burns in critical areas Hands, feet, perineum, genitalia, major joints Burns with associated inhalation injuries Electric or lightning burns
30 CRITERIA FOR BURN CENTER Severe burns complicated by trauma (may need trauma center first) Pre-existing disease that could complicate management Circumferential burns of extremities or chest
31 TRANSPORT TO BURN CENTER Cover patient with dry sheet Transport crews should be aware of hypothermia risks Avoid saline soaked dressings Avoid antimicrobial creams Will delay transfer Need to be removed at burn center
Pediatric Burn Management Justin D. Klein, MD Associate Burn Director Lisa C. Vitale, RN Burn Program Coordinator
 Pediatric Burn Management Justin D. Klein, MD Associate Burn Director Lisa C. Vitale, RN Burn Program Coordinator Lecture Overview Burn statistics and etiologies Pre-hospital evaluation Anatomy of a burn
Pediatric Burn Management Justin D. Klein, MD Associate Burn Director Lisa C. Vitale, RN Burn Program Coordinator Lecture Overview Burn statistics and etiologies Pre-hospital evaluation Anatomy of a burn
EmergencyKT: Management of Thermal Injury in Adult Patients
 EmergencyKT: Management of Thermal Injury in Adult Patients Remove patient from source of injury, including burned clothing and jewelry Does patient appear to have minor burns? (See Box A) No Notify Burn
EmergencyKT: Management of Thermal Injury in Adult Patients Remove patient from source of injury, including burned clothing and jewelry Does patient appear to have minor burns? (See Box A) No Notify Burn
Burn Priorities of Care: Triage/Treatment/Transfer. Via Christi Regional Burn Center Sarah Fischer, MSN, RN
 Burn Priorities of Care: Triage/Treatment/Transfer Via Christi Regional Burn Center Sarah Fischer, MSN, RN Disclosure I have nothing to disclose Objectives Identify American Burn Association referral criteria
Burn Priorities of Care: Triage/Treatment/Transfer Via Christi Regional Burn Center Sarah Fischer, MSN, RN Disclosure I have nothing to disclose Objectives Identify American Burn Association referral criteria
IMMEDIATE EMERGENCY BURN CARE » THERMAL BURNS » ELECTRICAL BURNS » CHEMICAL BURNS FIRST AID FOR THE THREE MAJOR CATEGORIES
 IMMEDIATE EMERGENCY BURN CARE 1. Treat according to BLS or ACLS Protocol 2. Use airway and C-Spine precautions. 3. Stop the burning process. FIRST AID FOR THE THREE MAJOR CATEGORIES» THERMAL BURNS + Stop
IMMEDIATE EMERGENCY BURN CARE 1. Treat according to BLS or ACLS Protocol 2. Use airway and C-Spine precautions. 3. Stop the burning process. FIRST AID FOR THE THREE MAJOR CATEGORIES» THERMAL BURNS + Stop
BURNS MODULE. In the paediatric population consider non-accidental injury as a mechanism for burn injuries.
 BURNS MODULE INTRODUCTION Burns are a common cause of trauma. Most burn injuries are a result of flame burns, with scalds also occurring commonly. Electrical and chemical burns are less common. 1 Concurrent
BURNS MODULE INTRODUCTION Burns are a common cause of trauma. Most burn injuries are a result of flame burns, with scalds also occurring commonly. Electrical and chemical burns are less common. 1 Concurrent
Children's National Medical Center The Division of Trauma and Burn Burn Education Module Post-test
 Children's National Medical Center The Division of Trauma and Burn Burn Education Module Post-test Purpose: To provide nurses with on overview of burn injuries in pediatric patients. Learning Objectives:
Children's National Medical Center The Division of Trauma and Burn Burn Education Module Post-test Purpose: To provide nurses with on overview of burn injuries in pediatric patients. Learning Objectives:
At the conclusion of this course the learner will be able to
 Objectives At the conclusion of this course the learner will be able to 1. Discuss basic anatomy and pathophysiology of burns 2. Describe burn injuries in terms of size, depth, coloration and characteristics
Objectives At the conclusion of this course the learner will be able to 1. Discuss basic anatomy and pathophysiology of burns 2. Describe burn injuries in terms of size, depth, coloration and characteristics
Objectives. Initial Burn Care and Fluid Resuscitation 6/5/2015 INITIAL MANAGEMENT
 Initial Burn Care and Fluid Resuscitation Sarah Taylor MSN, RN, ACNS-BC Clinical Nurse Specialist Trauma Burn Center University of Michigan Health System Ann Arbor, MI Objectives Discuss the initial assessment
Initial Burn Care and Fluid Resuscitation Sarah Taylor MSN, RN, ACNS-BC Clinical Nurse Specialist Trauma Burn Center University of Michigan Health System Ann Arbor, MI Objectives Discuss the initial assessment
Burn injury. A : patent airway with smoking inhalation, stridor. D: E4V5M6,pupil 2mm RTLBE
 Burn injury Pinyong Uthaitas Emergency Department Faculty of Medicine, Ramathibodi Hospital A Thai man 52 year old came to the hospital due to flam burn ½ hr ago at his house. He gain conscious but hoarseness
Burn injury Pinyong Uthaitas Emergency Department Faculty of Medicine, Ramathibodi Hospital A Thai man 52 year old came to the hospital due to flam burn ½ hr ago at his house. He gain conscious but hoarseness
Burns. A Comprehensive Review Assessment & Management
 Burns A Comprehensive Review Assessment & Management 1 Objectives Understand types of Burns Understand the pathophysiology of the Burns Understand Rule of Nine Understand Classification of Burns Identify
Burns A Comprehensive Review Assessment & Management 1 Objectives Understand types of Burns Understand the pathophysiology of the Burns Understand Rule of Nine Understand Classification of Burns Identify
Management of Acute Burn Injuries: The First 24 Hours
 Speaker Disclosure I, Debbie Harrell, MSN, RN, NE BC, have no financial relationships to disclose. I will not discuss off label uses of any pharmaceutical products or medical devices. Management of Acute
Speaker Disclosure I, Debbie Harrell, MSN, RN, NE BC, have no financial relationships to disclose. I will not discuss off label uses of any pharmaceutical products or medical devices. Management of Acute
EMERGENCYROOM BURN MANAGEMENT
 EMERGENCYROOM INITIAL ASSESSMENT PRIMARY SURVEY A = Airway and C-spine immobilization B = Breathing and Ventilation C = Circulation D = Disability, Neurologic Deficit E = Expose (remove all clothing and
EMERGENCYROOM INITIAL ASSESSMENT PRIMARY SURVEY A = Airway and C-spine immobilization B = Breathing and Ventilation C = Circulation D = Disability, Neurologic Deficit E = Expose (remove all clothing and
ITLS Pediatric Provider Course Advanced Pre-Test
 ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
Outpatient Burn Care for Primary Care: Who needs a referral?
 Outpatient Burn Care for Primary Care: Who needs a referral? J. Kevin Bailey, MD Associate Professor Department of Surgery Division of Trauma, Critical Care and Burn The Ohio State University Wexner Medical
Outpatient Burn Care for Primary Care: Who needs a referral? J. Kevin Bailey, MD Associate Professor Department of Surgery Division of Trauma, Critical Care and Burn The Ohio State University Wexner Medical
INITIAL CARE AND TREATMENT OF BURN INJURIES. November 10,
 INITIAL CARE AND TREATMENT OF BURN INJURIES 2 11/10/2012 November 10, 2012 2 Oregon Burn Center Only burn center in Oregon and SW Washington New unit 16 beds, 20,000 square feet Opened in February 2002
INITIAL CARE AND TREATMENT OF BURN INJURIES 2 11/10/2012 November 10, 2012 2 Oregon Burn Center Only burn center in Oregon and SW Washington New unit 16 beds, 20,000 square feet Opened in February 2002
Abdomen and Genitalia Injuries. Chapter 28
 Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
Burns and electrical injuries. Shelley Westwood, RN, BSN
 Burns and electrical injuries Shelley Westwood, RN, BSN Burns A burn is an injury caused by fire, heat, chemicals, radiation, or electricity. Burns are traumatic in that they can cause extreme pain, permanent
Burns and electrical injuries Shelley Westwood, RN, BSN Burns A burn is an injury caused by fire, heat, chemicals, radiation, or electricity. Burns are traumatic in that they can cause extreme pain, permanent
Chapter 29. Objectives. Objectives 01/09/2013. Burns
 Chapter 29 Burns Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms introduced in
Chapter 29 Burns Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms introduced in
Approved By: Airway and Breathing A. Initially give humidified high flow oxygen at 15 L (100%) using a nonrebreather
 using a nonrebreather") Subject: BURN CARE CLINICAL GUIDELINE Originator: Approval Date: 2015 Approved By: Policy: All burn patients presenting to XXXXXX Hospital will have appropriate assessment, stabilization and evaluation
Subject: BURN CARE CLINICAL GUIDELINE Originator: Approval Date: 2015 Approved By: Policy: All burn patients presenting to XXXXXX Hospital will have appropriate assessment, stabilization and evaluation
The immediate management of burns patients should be similar to management of trauma.
 CATS Clinical Guideline Burns The National Burn Care Review recommends that children with burns should be treated in a Burn Centre. Chelsea and Westminster may take non-ventilated children, Broomfield
CATS Clinical Guideline Burns The National Burn Care Review recommends that children with burns should be treated in a Burn Centre. Chelsea and Westminster may take non-ventilated children, Broomfield
BLS, ILS, ALS OTEP BURNS BURN INTRODUCTION TYPES OF BURNS
 BURNS BLS, ILS, ALS OTEP While we do understand this presentation is an instructional tool for all levels of certification, taking this into consideration everyone taking this class must remember that
BURNS BLS, ILS, ALS OTEP While we do understand this presentation is an instructional tool for all levels of certification, taking this into consideration everyone taking this class must remember that
A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion
 A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion Christopher Butts PhD, DO Surgical Critical Care Fellow Cooper University Hospital H&P 10 year old female presents as a trauma
A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion Christopher Butts PhD, DO Surgical Critical Care Fellow Cooper University Hospital H&P 10 year old female presents as a trauma
Shenandoah Co. Fire & Rescue. Injuries to. and Spine. December EMS Training Bill Streett Training Section Chief
 Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#
Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#
Dóra Ujvárosy MD. Medical University of Debrecen Oxyology and Emergency Department
 Dóra Ujvárosy MD. Medical University of Debrecen Oxyology and Emergency Department Functions Definition A burn is a type of injury to the skin caused by heat, electricity, chemicals, light, radiation or
Dóra Ujvárosy MD. Medical University of Debrecen Oxyology and Emergency Department Functions Definition A burn is a type of injury to the skin caused by heat, electricity, chemicals, light, radiation or
Wisecracks 1. What are the indications for an escharotomy 2. What are the primary considerations in mechanical ventilation of burn patients
 Chapter 63 Thermal Burns Episode Overview Questions 1. List zones of burns 2. List 6 indications for intubation in the burn patient 3. List and describe 2 formulas for fluid resuscitation 4. Describe depth
Chapter 63 Thermal Burns Episode Overview Questions 1. List zones of burns 2. List 6 indications for intubation in the burn patient 3. List and describe 2 formulas for fluid resuscitation 4. Describe depth
Current Trends in Burn Care
 Objectives Current Trends in Burn Care Jordan Murphy, BSN, CFRN Clinical Educator-KY/FL PHI Air Medical Describes normal skin anatomy. Differentiates pathophysiology related to etiology of injury. Identify
Objectives Current Trends in Burn Care Jordan Murphy, BSN, CFRN Clinical Educator-KY/FL PHI Air Medical Describes normal skin anatomy. Differentiates pathophysiology related to etiology of injury. Identify
Muscle spasm Diminished bowel sounds Nausea/vomiting
 3 4 5 6 7 8 9 0 Chapter 8: Abdomen and Genitalia Injuries Abdominal Injuries Abdomen is major body cavity extending from to pelvis. Contains organs that make up digestive, urinary, and genitourinary systems.
3 4 5 6 7 8 9 0 Chapter 8: Abdomen and Genitalia Injuries Abdominal Injuries Abdomen is major body cavity extending from to pelvis. Contains organs that make up digestive, urinary, and genitourinary systems.
ATLS: Initial Assessment and Management. SAUSHEC Medical Student Lecture Series
 ATLS: Initial Assessment and Management SAUSHEC Medical Student Lecture Series Objectives Identify sequence of priorities in assessing the multiply injured patient Apply principles outlined in primary
ATLS: Initial Assessment and Management SAUSHEC Medical Student Lecture Series Objectives Identify sequence of priorities in assessing the multiply injured patient Apply principles outlined in primary
Burn Injuries & Its Management M JARI.MD
 Burn Injuries & Its Management M JARI.MD 1 BURNS Wounds caused by exposure to: 1. excessive heat 2. Chemicals 3. fire/steam 4. radiation 5. electricity 2 BURNS Results in 10-20 thousand deaths annually
Burn Injuries & Its Management M JARI.MD 1 BURNS Wounds caused by exposure to: 1. excessive heat 2. Chemicals 3. fire/steam 4. radiation 5. electricity 2 BURNS Results in 10-20 thousand deaths annually
Chapter 24 Soft Tissue Injuries Presentation Notes
 Names: Chapter 24 Soft Tissue Injuries Presentation Notes Anatomy of the Skin - Function of the Skin control Soft-Tissue Injuries injuries Soft-tissue damage the skin injuries Break in the of the skin
Names: Chapter 24 Soft Tissue Injuries Presentation Notes Anatomy of the Skin - Function of the Skin control Soft-Tissue Injuries injuries Soft-tissue damage the skin injuries Break in the of the skin
of Trauma Assembly 27 th Page 1
 Eastern Association for the Surgery of Trauma 27 th Annual Scientific Assembly Sunrise Session 08 To Scan or Not To Scan Thatt is the Question January 16, 2014 Waldorf Astoria Naples Naples, Floridaa Page
Eastern Association for the Surgery of Trauma 27 th Annual Scientific Assembly Sunrise Session 08 To Scan or Not To Scan Thatt is the Question January 16, 2014 Waldorf Astoria Naples Naples, Floridaa Page
Aviation Rescue Swimmer Course
 Aviation Rescue Swimmer Course Primary Survey LT 5.4 December 2003 1 Objectives List the procedures used in a primary survey. Demonstrate primary survey procedures used in a mock trauma (moulage) scenario
Aviation Rescue Swimmer Course Primary Survey LT 5.4 December 2003 1 Objectives List the procedures used in a primary survey. Demonstrate primary survey procedures used in a mock trauma (moulage) scenario
ITLS Pediatric Provider Course Basic Pre-Test
 ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials
 Preparatory Materials") Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
Cellular and Tissue Effects. Pathophysiology of the Burn Wound. Special Topics: Thermal Burns & Smoke Inhalation
 Special Topics: Thermal Burns & Smoke Inhalation MEDICAL RESPONDER AND RECEIVER SEMINAR; EXPLOSION AND BLAST INJURIES Pathophysiology of the Burn Wound The burn wound is the source of virtually all ill
Special Topics: Thermal Burns & Smoke Inhalation MEDICAL RESPONDER AND RECEIVER SEMINAR; EXPLOSION AND BLAST INJURIES Pathophysiology of the Burn Wound The burn wound is the source of virtually all ill
Review. A. abrasion B. contusion C. hematoma D. avulsion
 Chapter 24 Review Review 1. A young male was struck in the forearm with a baseball and complains of pain to the area. Slight swelling and ecchymosis are present, but no external bleeding. What type of
Chapter 24 Review Review 1. A young male was struck in the forearm with a baseball and complains of pain to the area. Slight swelling and ecchymosis are present, but no external bleeding. What type of
Chapter 28. Objectives. Objectives 01/09/2013. Bleeding and Soft-Tissue Trauma
 Chapter 28 Bleeding and Soft-Tissue Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define
Chapter 28 Bleeding and Soft-Tissue Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of
 Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
Focused History and Physical Examination of the
 Henry: EMT Prehospital Care, Revised 3 rd Edition Lecture Notes Chapter 10: Focused History and Physical Examination of Trauma Patients Chapter 10 Focused History and Physical Examination of the Trauma
Henry: EMT Prehospital Care, Revised 3 rd Edition Lecture Notes Chapter 10: Focused History and Physical Examination of Trauma Patients Chapter 10 Focused History and Physical Examination of the Trauma
Pediatrics Grand Rounds 1 June University of Texas Health Science Center at San Antonio. Management of Burn Wounds. Management of Burn Wounds
 Management of Burn Wounds Management of Burn Wounds History of Burn Care Pathophysiology of Burn Lillian F. Liao, MD, MPH Division of Trauma and Emergency Surgery Department of Surgery UTHSCSA Acute burn
Management of Burn Wounds Management of Burn Wounds History of Burn Care Pathophysiology of Burn Lillian F. Liao, MD, MPH Division of Trauma and Emergency Surgery Department of Surgery UTHSCSA Acute burn
Pediatric Abdomen Trauma
 Pediatric Abdomen Trauma Susan D. John, MD, FACR Pediatric Trauma Trauma is leading cause of death and disability in children and adolescents Causes and effects vary between age groups Blunt trauma predominates
Pediatric Abdomen Trauma Susan D. John, MD, FACR Pediatric Trauma Trauma is leading cause of death and disability in children and adolescents Causes and effects vary between age groups Blunt trauma predominates
Pediatric Trauma Care
 2013 Standard Trauma Care Procedures (Pediatric) Traumatic injuries require prompt care and transportation. Always suspect cervical injury. Note the mechanism of injury and any other condition that may
2013 Standard Trauma Care Procedures (Pediatric) Traumatic injuries require prompt care and transportation. Always suspect cervical injury. Note the mechanism of injury and any other condition that may
PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT
 PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT Board Approved June 2007 Revised December 2009 Revised July 2011 Revised June 2015 435 Hunter Street Fredericksburg, VA 22401
PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT Board Approved June 2007 Revised December 2009 Revised July 2011 Revised June 2015 435 Hunter Street Fredericksburg, VA 22401
Subtle Signs of Child Abuse Child s Protection Office MOH Presented by Dr.Fatoumah Alabdulrazzaq M.D,FRCPC,FAAP,PEM(C)
") Subtle Signs of Child Abuse Child s Protection Office MOH Presented by Dr.Fatoumah Alabdulrazzaq M.D,FRCPC,FAAP,PEM(C) Cutaneous Injuries Bruise : injury to soft tissues in which skin is not broken, characterized
Subtle Signs of Child Abuse Child s Protection Office MOH Presented by Dr.Fatoumah Alabdulrazzaq M.D,FRCPC,FAAP,PEM(C) Cutaneous Injuries Bruise : injury to soft tissues in which skin is not broken, characterized
OUTLINE SHEET 5.4 PRIMARY SURVEY
 ENABLING OBJECTIVES: 4.7 List the procedures used in a primary survey. 4.8 Demonstrate primary survey procedures used in a mock trauma (moulage) scenario without injury to personnel or damage to equipment.
ENABLING OBJECTIVES: 4.7 List the procedures used in a primary survey. 4.8 Demonstrate primary survey procedures used in a mock trauma (moulage) scenario without injury to personnel or damage to equipment.
Printed copies of this document may not be up to date, obtain the most recent version from Author Position
 Children s Acute Transport Service Clinical Guidelines Burns Management Document Control Information Author E Borrows E Randle Author Position PICU/BURNS Consultant CATS Consultant Document Owner E. Polke
Children s Acute Transport Service Clinical Guidelines Burns Management Document Control Information Author E Borrows E Randle Author Position PICU/BURNS Consultant CATS Consultant Document Owner E. Polke
Case Report: Burns Reid Sadoway PGY1 Emergency Medicine, Dalhousie
 Case Report: Burns Reid Sadoway PGY1 Emergency Medicine, Dalhousie History 3 yo boy, presents to pediatric ED with mother Child can be heard crying inside waiting/patient room, has both hands bandaged
Case Report: Burns Reid Sadoway PGY1 Emergency Medicine, Dalhousie History 3 yo boy, presents to pediatric ED with mother Child can be heard crying inside waiting/patient room, has both hands bandaged
NOTE If it is necessary to perform abdominal thrusts, expose the abdominal area prior to pressing on the abdomen.
 ENABLING OBJECTIVES: 4.7 List the procedures used in a primary survey. 4.8 Demonstrate primary survey procedures used in a mock trauma (moulage) scenario without injury to personnel or damage to equipment.
ENABLING OBJECTIVES: 4.7 List the procedures used in a primary survey. 4.8 Demonstrate primary survey procedures used in a mock trauma (moulage) scenario without injury to personnel or damage to equipment.
Burn wounds - Determining the size and type degree
 1 Burn wounds - Determining the size and type degree Determining surface area of burn (Open hand only for small burns) 1 2 Burn depth Most burns are a combination of superficial and deeper burns and the
1 Burn wounds - Determining the size and type degree Determining surface area of burn (Open hand only for small burns) 1 2 Burn depth Most burns are a combination of superficial and deeper burns and the
Lecture Notes. Chapter 9: Smoke Inhalation Injury and Burns
 Lecture Notes Chapter 9: Smoke Inhalation Injury and Burns Objectives List the factors that influence mortality rate Describe the nature of smoke inhalation and the fire environment Recognize the pulmonary
Lecture Notes Chapter 9: Smoke Inhalation Injury and Burns Objectives List the factors that influence mortality rate Describe the nature of smoke inhalation and the fire environment Recognize the pulmonary
Thermal Burns PFN: SOMEML07. Terminal Learning Objective. References. Hours: 3.0 Instructor: Action: Communicate knowledge of thermal burns
 Thermal Burns PFN: SOMEML07 Hours: 3.0 Instructor: Slide 1 Terminal Learning Objective Action: Communicate knowledge of thermal burns Condition: Given a lecture in a classroom environment Standard: Received
Thermal Burns PFN: SOMEML07 Hours: 3.0 Instructor: Slide 1 Terminal Learning Objective Action: Communicate knowledge of thermal burns Condition: Given a lecture in a classroom environment Standard: Received
Pediatric Trauma. Sept 2nd, Patrick Murphy Neil Merritt
 Pediatric Trauma Sept 2nd, 2015 Patrick Murphy Neil Merritt Objectives Objectives Medical Expert 1. Describe the types of pediatric injuries sustained with a given mode of trauma, and identify the most
Pediatric Trauma Sept 2nd, 2015 Patrick Murphy Neil Merritt Objectives Objectives Medical Expert 1. Describe the types of pediatric injuries sustained with a given mode of trauma, and identify the most
Patient Assessment. Chapter 8
 Patient Assessment Chapter 8 Patient Assessment Scene size-up Initial assessment Focused history and physical exam Vital signs History Detailed physical exam Ongoing assessment Patient Assessment Process
Patient Assessment Chapter 8 Patient Assessment Scene size-up Initial assessment Focused history and physical exam Vital signs History Detailed physical exam Ongoing assessment Patient Assessment Process
 55-year-old male with 2nd and 3rd degree burns to face, chest, and arms on 25% of the body Respirations: 34 Pulse: 120 Mental Status: moans to painful stimulus Mucous membranes charred Stridor 10 cm scalp
55-year-old male with 2nd and 3rd degree burns to face, chest, and arms on 25% of the body Respirations: 34 Pulse: 120 Mental Status: moans to painful stimulus Mucous membranes charred Stridor 10 cm scalp
UBC Department of Urologic Sciences Lecture Series. Urological Trauma
 UBC Department of Urologic Sciences Lecture Series Urological Trauma Disclaimer: This is a lot of information to cover and we are unlikely to cover it all today These slides are to be utilized for your
UBC Department of Urologic Sciences Lecture Series Urological Trauma Disclaimer: This is a lot of information to cover and we are unlikely to cover it all today These slides are to be utilized for your
Responsibility This guideline applies to teams of health professions caring for burn patients.
 Page 1 of 9 Guideline: Initial Assessment & Management of Burn Injuries Purpose This document provides a guideline for the initial assessment and management of burn patients. It is not intended as a full
Page 1 of 9 Guideline: Initial Assessment & Management of Burn Injuries Purpose This document provides a guideline for the initial assessment and management of burn patients. It is not intended as a full
You Are the Emergency Medical Responder
 Lesson 32: Injuries to the Chest, Abdomen and Genitalia You Are the Emergency Medical Responder Your police unit responds to a call in a part of town plagued by violence. When you arrive, you find the
Lesson 32: Injuries to the Chest, Abdomen and Genitalia You Are the Emergency Medical Responder Your police unit responds to a call in a part of town plagued by violence. When you arrive, you find the
Restore adequate respiratory and circulatory conditions. Reduce pain
 Pre-hospital management of the trauma patient is best performed by an integrated team focused on minimizing the time from injury to definitive care at an appropriate trauma center. Dispatchers, first responders,
Pre-hospital management of the trauma patient is best performed by an integrated team focused on minimizing the time from injury to definitive care at an appropriate trauma center. Dispatchers, first responders,
3. D Objective: Chapter 4, Objective 4 Page: 79 Rationale: A carbon dioxide level below 35 mmhg indicates hyperventilation.
 1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
Advanced Paediatric Nursing. Burn Trauma. 26 April Wong Tze Wing NC (Burns), Burns Centre, Surgery, PWH
, Burns Centre, Surgery, PWH") Advanced Paediatric Nursing Burn Trauma 26 April 2016 Wong Tze Wing NC (Burns), Burns Centre, Surgery, PWH Objective: Understand burn trauma in children Understand Important nursing interventions in burn
Advanced Paediatric Nursing Burn Trauma 26 April 2016 Wong Tze Wing NC (Burns), Burns Centre, Surgery, PWH Objective: Understand burn trauma in children Understand Important nursing interventions in burn
EMS System for Metropolitan Oklahoma City and Tulsa 2019 Medical Control Board Treatment Protocols
 EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
1/3/2008. Karen Burke Priscilla LeMone Elaine Mohn-Brown. Medical-Surgical Nursing Care, 2e Karen Burke, Priscilla LeMone, and Elaine Mohn-Brown
 Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 46 Caring for Clients with Burns Types of Burns Thermal Dry heat flame Moist heat steam or hot liquid
Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 46 Caring for Clients with Burns Types of Burns Thermal Dry heat flame Moist heat steam or hot liquid
WOUNDS. Emergency Procedures in PT
 WOUNDS Emergency Procedures in PT Types of Wounds Abrasions uppermost layer scraped away, minor capillary bleeding occurs, nerve endings exposed Lacerations skin tear with edges jagged and uneven Incisions
WOUNDS Emergency Procedures in PT Types of Wounds Abrasions uppermost layer scraped away, minor capillary bleeding occurs, nerve endings exposed Lacerations skin tear with edges jagged and uneven Incisions
Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing
 1 2 3 4 5 6 Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing D-Disability Chief complaint and/or Mechanism
1 2 3 4 5 6 Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing D-Disability Chief complaint and/or Mechanism
PEDIATRIC TRAUMA EMERGENCIES
 PEDIATRIC TRAUMA EMERGENCIES Last Revised: January 2015 1 PEDIATRIC COMA SCALE Indicator Eye Opening Spontaneous 4 To verbal stimuli 3 To pain only 2 No response 1 Verbal Response Oriented, appropriate
PEDIATRIC TRAUMA EMERGENCIES Last Revised: January 2015 1 PEDIATRIC COMA SCALE Indicator Eye Opening Spontaneous 4 To verbal stimuli 3 To pain only 2 No response 1 Verbal Response Oriented, appropriate
Chapter 21: Burns Introduction to Burn Injuries (1 of 2) Introduction to Burn Injuries (2 of 2) Reduction in Burn Injuries Pathophysiology of Burns
 Introduction to Burn Injuries (2 of 2) Reduction in Burn Injuries Pathophysiology of Burns") 1 2 3 4 5 6 7 8 Chapter 21: Burns Introduction to Burn Injuries (1 of 2) 1.25-2 million Americans treated for burns annually 50,000 require 3-5% considered life threatening leading cause of death for children
1 2 3 4 5 6 7 8 Chapter 21: Burns Introduction to Burn Injuries (1 of 2) 1.25-2 million Americans treated for burns annually 50,000 require 3-5% considered life threatening leading cause of death for children
Child as a victim of injury. Maciej Dudkiewicz M.D. Ph.D. Dpt of Anaesthesia and Intensive Care Medical University of Lodz
 Child as a victim of injury Maciej Dudkiewicz M.D. Ph.D. Dpt of Anaesthesia and Intensive Care Medical University of Lodz Epidemiology Trauma is most common cause of mortality and morbidity in the US pediatric
Child as a victim of injury Maciej Dudkiewicz M.D. Ph.D. Dpt of Anaesthesia and Intensive Care Medical University of Lodz Epidemiology Trauma is most common cause of mortality and morbidity in the US pediatric
Burns Management in the Emergency Department
 Management in the Emergency Department (Referral Proforma) Time/Date of injury (24hr) Patient demographic data sticker Airway Please remember to protect C-spine until clinically cleared as stable Administer
Management in the Emergency Department (Referral Proforma) Time/Date of injury (24hr) Patient demographic data sticker Airway Please remember to protect C-spine until clinically cleared as stable Administer
Pan Scan Instead of Clinical Exam? David A. Spain, MD
 Pan Scan Instead of Clinical Exam? David A. Spain, MD Granted, some patients don t t need CT scan Platinum Package Stanford Special CT Scan Head Neck Chest Abdomen Pelvis Takes about 20 minutes to do
Pan Scan Instead of Clinical Exam? David A. Spain, MD Granted, some patients don t t need CT scan Platinum Package Stanford Special CT Scan Head Neck Chest Abdomen Pelvis Takes about 20 minutes to do
Printed copies of this document may not be up to date, obtain the most recent version from Author Position
 Children s Acute Transport Service Clinical Guidelines Burns Management Document Control Information Author E Borrows E Randle, L Chigaru Author Position PICU/BURNS Consultant CATS Consultants Document
Children s Acute Transport Service Clinical Guidelines Burns Management Document Control Information Author E Borrows E Randle, L Chigaru Author Position PICU/BURNS Consultant CATS Consultants Document
INSTRUCTOR GUIDE FOR TACTICAL FIELD CARE 3B BURNS AND FRACTURES
 INSTRUCTOR GUIDE FOR TACTICAL FIELD CARE 3B BURNS AND FRACTURES 180801 1 Tactical Combat Casualty Care for Medical Personnel 1. August 2017 (Based on TCCC-MP Guidelines 180801 In this presentation, we
INSTRUCTOR GUIDE FOR TACTICAL FIELD CARE 3B BURNS AND FRACTURES 180801 1 Tactical Combat Casualty Care for Medical Personnel 1. August 2017 (Based on TCCC-MP Guidelines 180801 In this presentation, we
Speaker Disclosure Emergent Burn Care I, Debbie Harrell, MSN, RN, NE BC, have no financial relationships to disclose.
 Speaker Disclosure Emergent Burn Care I, Debbie Harrell, MSN, RN, NE BC, have no financial relationships to disclose. Debbie Harrell RN, MSN, Shriners Hospitals for Children Cincinnati Cincinnati, Ohio
Speaker Disclosure Emergent Burn Care I, Debbie Harrell, MSN, RN, NE BC, have no financial relationships to disclose. Debbie Harrell RN, MSN, Shriners Hospitals for Children Cincinnati Cincinnati, Ohio
McCann Technical School 70 Hodges Cross Road North Adams, MA Medical Assisting Program
 MA 104 MEDICAL SOCIAL SCIENCE 4 Credits Fall Semester Part IV FIRST RESPONDER Syllabus McCann Technical School 70 Hodges Cross Road North Adams, MA 01247 Medical Assisting Program INSTRUCTORS: Laurie Tuper,
MA 104 MEDICAL SOCIAL SCIENCE 4 Credits Fall Semester Part IV FIRST RESPONDER Syllabus McCann Technical School 70 Hodges Cross Road North Adams, MA 01247 Medical Assisting Program INSTRUCTORS: Laurie Tuper,
Imaging in the Trauma Patient
 Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
PEDIATRIC TRAUMA: Implications for Respiratory Care
 PEDIATRIC TRAUMA: Implications for Respiratory Care 17 th Annual Rainbow Respiratory Conference - September 4, 2015 Mike Dingeldein, MD Pediatric Surgeon Pediatric Trauma Medical Director Disclosures none
PEDIATRIC TRAUMA: Implications for Respiratory Care 17 th Annual Rainbow Respiratory Conference - September 4, 2015 Mike Dingeldein, MD Pediatric Surgeon Pediatric Trauma Medical Director Disclosures none
Purpose To outline the pre-hospital and inter-hospital assessment and management of patients with major burns.
 Major Burns HELI.CLI.08 Purpose To outline the pre-hospital and inter-hospital assessment and management of patients with major burns. Procedure Management of Severe Burns For Review Aug 2015 1. Introduction
Major Burns HELI.CLI.08 Purpose To outline the pre-hospital and inter-hospital assessment and management of patients with major burns. Procedure Management of Severe Burns For Review Aug 2015 1. Introduction
Little Kids in Big Crashes The Bio-mechanics of Kids in Car Crashes. Lisa Schwing, RN Trauma Program Manager Dayton Children s
 Little Kids in Big Crashes The Bio-mechanics of Kids in Car Crashes Lisa Schwing, RN Trauma Program Manager Dayton Children s Very Little Research There has been very little research on the forces a crash
Little Kids in Big Crashes The Bio-mechanics of Kids in Car Crashes Lisa Schwing, RN Trauma Program Manager Dayton Children s Very Little Research There has been very little research on the forces a crash
Introduction to Advanced Trauma Life Support ATLS
 Introduction to Advanced Trauma Life Support ATLS Objectives Concepts of primary & secondary survey Priorities & Life threatening conditions Clinical & Surgical skills Basic knowledge Rapid assessment
Introduction to Advanced Trauma Life Support ATLS Objectives Concepts of primary & secondary survey Priorities & Life threatening conditions Clinical & Surgical skills Basic knowledge Rapid assessment
Pediatric Trauma Cases
 Pediatric Trauma Cases QPEM 2018 Barbara Blackie, MD, MEd, FRCPC DISCLOSURE I do not have any relevant financial relationship with commercial interest to disclose. Learning Objectives -Manage interactive
Pediatric Trauma Cases QPEM 2018 Barbara Blackie, MD, MEd, FRCPC DISCLOSURE I do not have any relevant financial relationship with commercial interest to disclose. Learning Objectives -Manage interactive
Emergency Room Resuscitation of the Unstable Trauma Patient
 Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D.
 1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D. Sacral-coccygeal 2. A 36-year-old male sustains blunt force thoracic
1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D. Sacral-coccygeal 2. A 36-year-old male sustains blunt force thoracic
Thermal Injuries. Manika Bhandari, Malika Bhola, Rucha Desai, Dhruvika Joshi, Abir Shamim Life Science 4M03
 Thermal Injuries Manika Bhandari, Malika Bhola, Rucha Desai, Dhruvika Joshi, Abir Shamim Life Science 4M03 INTRODUCTION Anatomy of the skin The skin has three anatomical layers Epidermis Dermis Subcutaneous
Thermal Injuries Manika Bhandari, Malika Bhola, Rucha Desai, Dhruvika Joshi, Abir Shamim Life Science 4M03 INTRODUCTION Anatomy of the skin The skin has three anatomical layers Epidermis Dermis Subcutaneous
First Aid Fact Sheet 2005 Standards
 First Aid Fact Sheet 2005 Standards Five Leading Causes of Unintentional death: 1. Motor vehicle accidents 2. Falls 3. Poisonings 4. Drownings 5. Choking Good Samaritan Laws laws that give legal protection
First Aid Fact Sheet 2005 Standards Five Leading Causes of Unintentional death: 1. Motor vehicle accidents 2. Falls 3. Poisonings 4. Drownings 5. Choking Good Samaritan Laws laws that give legal protection
Trauma Registry Documentation December 16, 2014
 Trauma Registry Documentation December 16, 2014 The State of Florida now requires ALL Acute Care hospitals to submit data to the statetrauma Registry. Although Baptist Health hospitals are NOT Trauma Centers
Trauma Registry Documentation December 16, 2014 The State of Florida now requires ALL Acute Care hospitals to submit data to the statetrauma Registry. Although Baptist Health hospitals are NOT Trauma Centers
Skin Anatomy and Physiology
 Skin Anatomy and Physiology Body s largest organ Three layers: Epidermis Dermis Subcutaneous tissue 1 2 Skin Anatomy and Physiology Complex system, variety of functions Sensation Control of water loss
Skin Anatomy and Physiology Body s largest organ Three layers: Epidermis Dermis Subcutaneous tissue 1 2 Skin Anatomy and Physiology Complex system, variety of functions Sensation Control of water loss
Paediatric Trauma. A/Prof Drew Richardson. The Canberra Hospital May MB BS (Hons) FACEM Grad CertHE MD
 FACEM Grad CertHE MD") Paediatric Trauma A/Prof Drew Richardson MB BS (Hons) FACEM Grad CertHE MD The Canberra Hospital May 2013 Objectives Identify unique anatomic and physiologic characteristics of injured children Describe
Paediatric Trauma A/Prof Drew Richardson MB BS (Hons) FACEM Grad CertHE MD The Canberra Hospital May 2013 Objectives Identify unique anatomic and physiologic characteristics of injured children Describe
MANAGEMENT OF SOLID ORGAN INJURIES
 MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
Selective Spine Assessment & Spinal Motion Restriction
 Selective Spine Assessment & Spinal Motion Restriction Supersedes: 02-09-15 Effective: 10-20-15 Spinal cord injury may be the result of direct blunt and/or penetrating trauma, compression forces (axial
Selective Spine Assessment & Spinal Motion Restriction Supersedes: 02-09-15 Effective: 10-20-15 Spinal cord injury may be the result of direct blunt and/or penetrating trauma, compression forces (axial
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University
 Dr Mubarak Abdelrahman Assistant Professor Jazan University") Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
5/2/2018. Notice. Putting Humpty Dumpty Back Together Again
 Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
EMS System for Metropolitan Oklahoma City and Tulsa 2018 Medical Control Board Treatment Protocols
 EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
PARA107 Summary. Page 1-3: Page 4-6: Page 7-10: Page 11-13: Page 14-17: Page 18-21: Page 22-25: Page 26-28: Page 29-33: Page 34-36: Page 37-38:
 PARA107 Summary Page 1-3: Page 4-6: Page 7-10: Page 11-13: Page 14-17: Page 18-21: Page 22-25: Page 26-28: Page 29-33: Page 34-36: Page 37-38: Injury, Mechanisms of Injury, Time Critical Guidelines Musculoskeletal
PARA107 Summary Page 1-3: Page 4-6: Page 7-10: Page 11-13: Page 14-17: Page 18-21: Page 22-25: Page 26-28: Page 29-33: Page 34-36: Page 37-38: Injury, Mechanisms of Injury, Time Critical Guidelines Musculoskeletal
Trauma Overview. Chapter 22
 Trauma Overview Chapter 22 Kinematics of Trauma Injuries are the leading cause of death among children and young adults. Kinematics introduces the basic physical concepts that dictate how injuries occur
Trauma Overview Chapter 22 Kinematics of Trauma Injuries are the leading cause of death among children and young adults. Kinematics introduces the basic physical concepts that dictate how injuries occur
Basic Assessment and Treatment of Trauma
 Basic Assessment and Treatment of Trauma Final Exam Version 1 1. In which of the following scenarios would the potential for serious injury or death be the GREATEST? A. 77-kg (170-lb) man who falls 1.2
Basic Assessment and Treatment of Trauma Final Exam Version 1 1. In which of the following scenarios would the potential for serious injury or death be the GREATEST? A. 77-kg (170-lb) man who falls 1.2
Pediatric Aspects of Advanced Trauma Life Support: Transition from EMS to the Trauma Room PEDIATRIC TRAUMA DIRECTOR, HASBRO CHILDREN S HOSPITAL
 Pediatric Aspects of Advanced Trauma Life Support: Transition from EMS to the Trauma Room HALE WILLS, MD PEDIATRIC TRAUMA DIRECTOR, HASBRO CHILDREN S HOSPITAL Objectives 1. Identify the critical components
Pediatric Aspects of Advanced Trauma Life Support: Transition from EMS to the Trauma Room HALE WILLS, MD PEDIATRIC TRAUMA DIRECTOR, HASBRO CHILDREN S HOSPITAL Objectives 1. Identify the critical components
TITLE OF CASE: Burn Injuries and Management
 TITLE OF CASE: Burn Injuries and Management AUTHOR OF CASE: Magdalena Malinowska SUMMARY: Patient is a 23 year old female who was brought in by EMS to the Emergency Room post a motor vehicle accident in
TITLE OF CASE: Burn Injuries and Management AUTHOR OF CASE: Magdalena Malinowska SUMMARY: Patient is a 23 year old female who was brought in by EMS to the Emergency Room post a motor vehicle accident in
TRAUMATIC EMERGENCIES
 TRAUMATIC EMERGENCIES I. General. A. Follow General Principles/Routine Care protocol unless otherwise indicated. B. Limit scene time for trauma patients, with goal of 15 minutes. C. See Appendix B for
TRAUMATIC EMERGENCIES I. General. A. Follow General Principles/Routine Care protocol unless otherwise indicated. B. Limit scene time for trauma patients, with goal of 15 minutes. C. See Appendix B for
ITLS Advanced Pre-Test Annotated Key 8 th Edition
 1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
Assessment of the Trauma Patient
 CHAPTER 10 Assessment of the Trauma Patient Overall Assessment Scheme Scene Size-Up Initial Assessment Trauma Physical Exam Vital Signs & SAMPLE History Medical SAMPLE History Physical Exam & Vital Signs
CHAPTER 10 Assessment of the Trauma Patient Overall Assessment Scheme Scene Size-Up Initial Assessment Trauma Physical Exam Vital Signs & SAMPLE History Medical SAMPLE History Physical Exam & Vital Signs
Review. 1. Peritonitis would MOST likely result following injury to the: A. liver. B. spleen. C. kidney. D. stomach.
 Chapter 28 Review Review 1. Peritonitis would MOST likely result following injury to the: A. liver. B. spleen. C. kidney. D. stomach. Review Answer: D Rationale: In general, solid organs bleed when injured
Chapter 28 Review Review 1. Peritonitis would MOST likely result following injury to the: A. liver. B. spleen. C. kidney. D. stomach. Review Answer: D Rationale: In general, solid organs bleed when injured