Diuretics are drugs that increase the volume of urine excreted. Most diuretic agents are inhibitors of renal ion transporters that decrease the
|
|
|
- Shawn Richard
- 5 years ago
- Views:
Transcription
1 Diuretics
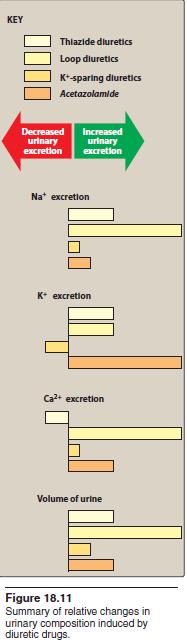
2 Diuretics are drugs that increase the volume of urine excreted. Most diuretic agents are inhibitors of renal ion transporters that decrease the reabsorption of Na+ at different sites in the nephron. As a result, Na+ and other ions, such as Cl, enter the urine in greater than normal amounts along with water, which is carried passively to maintain osmotic equilibrium. Diuretics, thus, increase the volume of urine and often change its ph, as well as the ionic composition of the urine and blood. The diuretic effect of the different classes of diuretics varies considerably, with the increase in Na+ secretion varying from less than 2% for the weak potassium-sparing diuretics to over 20% for the potent loop diuretics. In addition to the ion transport inhibitors, other types of diuretics include osmotic diuretics, aldosterone antagonists, and carbonic anhydrase inhibitors. Diuretics are most commonly used for management of abnormal fluid retention (edema) or treatment of hypertension.
3
4
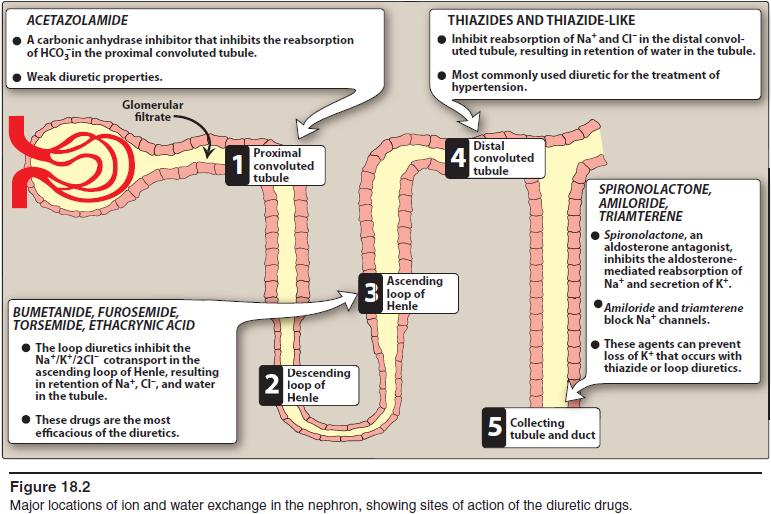
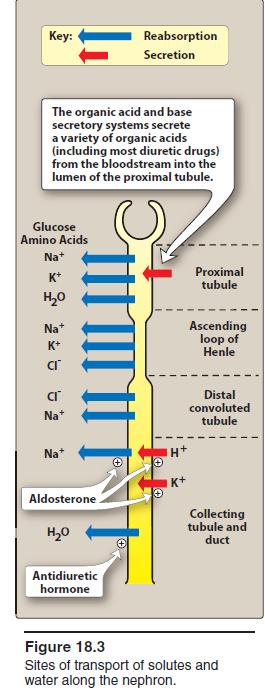
5 Approximately 16% to 20% of the blood plasma entering the kidneys is filtered from the glomerular capillaries into Bowman s capsule. The filtrate although normally free of proteins and blood cells, contains most of the low molecular weight plasma components in concentrations similar to that in the plasma. These include glucose, sodium bicarbonate, amino acids, and other organic solutes, as well as electrolytes, such as Na+, K+, and Cl. The kidney regulates the ionic composition and volume of urine by active reabsorption or secretion of ions and/or passive reabsorption of water at five functional zones along the nephron: 1) the proximal convoluted tubule. 2) the descending loop of Henle. 3) the ascending loop of Henle. 4) the distal convoluted tubule. 5) the collecting tubule and duct.
6
7 A. Proximal convoluted tubule In the proximal convoluted tubule located in the cortex of the kidney, almost all the glucose, bicarbonate, amino acids, and other metabolites are reabsorbed. Approximately two-thirds of the Na+ is also reabsorbed. Chloride enters the lumen of the tubule in exchange for an anion, such as oxalate, as well as paracellularly through the lumen. Water follows passively from the lumen to the blood to maintain osmolar equality. If not for the extensive reabsorption of solutes and water in the proximal tubule, the mammalian organism would rapidly become dehydrated and fail to maintain normal osmolarity. The Na+ that is reabsorbed is pumped into the interstitium by Na+/K+ - adenosine triphosphatase (ATPase) pump, thereby maintaining normal levels of Na+ and K+ in the cell. Carbonic anhydrase in the luminal membrane and cytoplasm of the proximal tubular cells modulates the reabsorption of bicarbonate.
8 The proximal tubule is the site of the organic acid and base secretory systems. The organic acid secretory system, located in the middle-third of the proximal tubule, secretes a variety of organic acids, such as uric acid, some antibiotics, and diuretics, from the bloodstream into the proximal tubular lumen. Most diuretic drugs are delivered to the tubular fluid via this system. The organic acid secretory system is saturable, and diuretic drugs in the bloodstream compete for transfer with endogenous organic acids such as uric acid. The organic base secretory system, located in the upper and middle segments of the proximal tubule, is responsible for the secretion of creatinine and choline.
9 B. Descending loop of Henle: The remaining filtrate, which is isotonic, next enters the descending limb of the loop of Henle and passes into the medulla of the kidney. The osmolarity increases along the descending portion of the loop of Henle because of the countercurrent mechanism that is responsible for water reabsorption. This results in a tubular fluid with a threefold increase in salt concentration. Osmotic diuretics exert part of their action in this region. C. Ascending loop of Henle: The cells of the ascending tubular epithelium are unique in being impermeable to water. Active reabsorption of Na+, K+, and Cl is mediated by a Na+/K+/2Cl cotransporter. Both Mg2+ and Ca2+ enter the interstitial fluid via the paracellular pathway. The ascending loop is, thus, a diluting region of the nephron. Approximately 25% to 30% of the tubular sodium chloride returns to the interstitial fluid, thereby helping to maintain high osmolarity. Because the ascending loop of Henle is a major site for salt reabsorption, drugs affecting this site, such as loop diuretics have the greatest diuretic effect.
10 D. Distal convoluted tubule The cells of the distal convoluted tubule are also impermeable to water. About 10% of the filtered sodium chloride is reabsorbed via a Na+/Cl transporter that is sensitive to thiazide diuretics. Calcium reabsorption is mediated by passage through a channel and then transported by a Na+/Ca2+-exchanger into the interstitial fluid. The mechanism, thus, differs from that in the loop of Henle. Additionally, Ca2+ excretion is regulated by parathyroid hormone in this portion of the tubule. E. Collecting tubule and duct The principal cells of the collecting tubule and duct are responsible for Na+, K+, and water transport, whereas the intercalated cells affect H+ secretion. Sodium enters the principal cells through channels (epithelial sodium channels) that are inhibited by amiloride and triamterene. Once inside the cell, Na+ reabsorption relies on a Na+/K+-ATPase pump to be transported into the blood. Aldosterone receptors in the principal cells influence Na+ reabsorption and K+ secretion. Aldosterone increases the synthesis of Na+ channels and of the Na+/K+- ATPase pump, which when combined increase Na+ reabsorption. Antidiuretic hormone (ADH; vasopressin) receptors promote the reabsorption of water from the collecting tubules and ducts.
11 THIAZIDES AND RELATED AGENTS The thiazides are the most widely used diuretics. They are sulfonamide derivatives. All thiazides affect the distal convoluted tubule, and all have equal maximum diuretic effects, differing only in potency. Thiazides are sometimes called low ceiling diuretics, because increasing the dose above normal therapeutic doses does not promote further diuretic response. A. Thiazides Chlorothiazide [klor-oh-thye-ah-zide] was the first orally active diuretic that was capable of affecting the severe edema often seen in hepatic cirrhosis and heart failure with minimal side effects. Its properties are representative of the thiazide group, although hydrochlorothiazide [hi-dro-klor-oh-thye-ah-zide] and chlorthalidone are now used more commonly. Hydrochlorothiazide is more potent, so the required dose is considerably lower than that of chlorothiazide, but the efficacy is comparable to that of the parent drug. In all other aspects, hydrochlorothiazide resembles chlorothiazide. [Note: Chlorthalidone, indapamide, and metolazone are referred to as thiazide-like diuretics, because they contain the sulfonamide residue in their chemical structures, and their mechanism of action is similar. However, they are not truly thiazides.]
12 Mechanism of action: The thiazide and thiazide-like diuretics act mainly in the cortical region of the ascending loop of Henle and the distal convoluted tubule to decrease the reabsorption of Na+, apparently by inhibition of a Na+/Cl cotransporter on the luminal membrane of the tubules. They have a lesser effect in the proximal tubule. As a result, these drugs increase the concentration of Na+ and Cl in the tubular fluid. [Note: Because the site of action of the thiazide derivatives is on the luminal membrane, these drugs must be excreted into the tubular lumen to be effective. Therefore, with decreased renal function, thiazide diuretics lose efficacy. The efficacy of these agents may be diminished with concomitant use of NSAIDs, such as indomethacin, which inhibit production of renal prostaglandins, thereby reducing renal blood flow.
13 Actions: a. Increased excretion of Na+ and Cl : Thiazide and thiazide-like diuretics cause diuresis with increased Na+ and Cl excretion, which can result in the excretion of very hyperosmolar (concentrated) urine. This latter effect is unique, as the other diuretic classes are unlikely to produce a hyperosmolar urine. The diuretic action is not affected by the acid base status of the body, and hydrochlorothiazide does not change the acid base status of the blood. b. Loss of K+: Because thiazides increase Na+ in the filtrate arriving at the distal tubule, more K+ is also exchanged for Na+, resulting in a continual loss of K+ from the body with prolonged use of these drugs. Thus, serum K+ should be measured periodically (more frequently at the beginning of therapy) to monitor for the development of hypokalemia. c. Loss of Mg2+: can occur with chronic use of thiazide diuretics, particularly in elderly patients. The mechanism for the magnesuria is not understood.
14 d. Decreased urinary calcium excretion: Thiazide and thiazide like diuretics decrease the Ca2+ content of urine by promoting the reabsorption of Ca2+ in the distal convoluted tubule where parathyroid hormone regulates reabsorption. This effect contrasts with the loop diuretics, which increase the Ca2+ concentration in the urine. e. Reduced peripheral vascular resistance: An initial reduction in blood pressure results from a decrease in blood volume and, therefore, a decrease in cardiac output. With continued therapy, volume recovery occurs. However, there are continued antihypertensive effects, resulting from reduced peripheral vascular resistance caused by relaxation of arteriolar smooth muscle. How these agents induce vasodilation is unknown.
15 Therapeutic uses: a. Hypertension: Clinically, the thiazides are a mainstay of antihypertensive medication, because they are inexpensive, convenient to administer, and well tolerated. They are effective in reducing blood pressure in the majority of patients with mild to moderate essential hypertension. Blood pressure can be maintained with a daily dose of thiazide, which causes lower peripheral resistance without having a major diuretic effect. Some patients can be continued for years on thiazides alone; however, many patients require additional medication for blood pressure control such as adrenergic blockers, angiotensinconverting enzyme inhibitors, or angiotensin receptor blockers. The antihypertensive actions of angiotensin- converting enzyme inhibitors are enhanced when given in combination with the thiazides.
16 b. Heart failure: Loop diuretics (not thiazides) are the diuretics of choice in reducing extracellular volume in heart failure. However, thiazide diuretics may be added if additional diuresis is needed. When given in combination, thiazides should be administered 30 minutes prior to loop diuretics in order to allow the thiazide time to reach the site of action and produce effect. c. Hypercalciuria: The thiazides can be useful in treating idiopathic hypercalciuria, because they inhibit urinary Ca2+ excretion. This is particularly beneficial for patients with calcium oxalate stones in the urinary tract. d. Diabetes insipidus: Thiazides have the unique ability to produce a hyperosmolar urine. Thiazides can substitute for ADH in the treatment of nephrogenic diabetes insipidus. The urine volume of such individuals may drop from 11 L/d to about 3 L/d when treated with the drug.
17 Pharmacokinetics: The drugs are effective orally. Most thiazides take 1 to 3 weeks to produce a stable reduction in blood pressure, and they exhibit a prolonged half-life. All thiazides are secreted by the organic acid secretory system of the kidney.
18 Adverse effects: o These mainly involve problems in fluid and electrolyte balance. a. Potassium depletion: Hypokalemia is the most frequent problem with the thiazide diuretics, and it can predispose patients who are taking digoxin to ventricular arrhythmias. Often, K+ can be supplemented by dietary measures such as increasing the consumption of citrus fruits, bananas, and prunes. In some cases, K+ supplementation may be necessary. Thiazides decrease the intravascular volume, resulting in activation of the renin angiotensin aldosterone system. Increased aldosterone contributes significantly to urinary K+ losses. Under these circumstances, the K+ deficiency can be overcome by spironolactone, which interferes with aldosterone action, or by administering triamterene or amiloride, which act to retain K+. Low-sodium diets blunt the potassium depletion caused by thiazide diuretics.
19 b. Hyponatremia: Hyponatremia may develop due to elevation of ADH as a result of hypovolemia, as well as diminished diluting capacity of the kidney and increased thirst. Limiting water intake and lowering the diuretic dose can prevent hyponatremia. c. Hyperuricemia: Thiazides increase serum uric acid by decreasing the amount of acid excreted by the organic acid secretory system. Being insoluble, uric acid deposits in the joints and may precipitate a gouty attack in predisposed individuals. Therefore, thiazides should be used with caution in patients with gout or high levels of uric acid. d. Volume depletion: This can cause orthostatic hypotension or light-headedness.
20 e. Hypercalcemia: The thiazides inhibit the secretion of Ca2+, sometimes leading to hypercalcemia (elevated levels of Ca2+ in the blood). f. Hyperglycemia: Therapy with thiazides can lead to glucose intolerance, possibly due to impaired release of insulin and tissue uptake of glucose. New-onset diabetes has been reported more often with thiazides than with other antihypertensive agents. Patients with diabetes who are taking thiazides should monitor glucose to assess the need for an adjustment in diabetes therapy.
21 Thiazide-like diuretics These compounds lack the thiazide structure, but, like the thiazides, they have the unsubstituted sulfonamide group and, therefore, share their mechanism of action. The therapeutic uses and adverse effect profiles are similar to those of the thiazides. Chlorthalidone: Chlorthalidone [klor-thal-idone] is a nonthiazide derivative that behaves pharmacologically like hydrochlorothiazide. It has a long duration of action and, therefore, is often used once daily to treat hypertension.
22 Metolazone: Metolazone [me-tol-ah-zone] is more potent than the thiazides and, unlike the thiazides, causes Na+ excretion even in advanced renal failure. Indapamide: Indapamide [in-dap-a-mide] is a lipid-soluble, nonthiazide diuretic that has a long duration of action. At low doses, it shows significant antihypertensive action with minimal diuretic effects. Indapamide is metabolized and excreted by the gastrointestinal tract and the kidneys. Thus, it is less likely to accumulate in patients with renal failure and may be useful in their treatment.
23 LOOP OR HIGH-CEILING DIURETICS Bumetanide [byoo-met-ah-nide], furosemide [fur-ohse-mide], torsemide [TOR-se-mide], and ethacrynic [eth-a-krin-ik] acid have their major diuretic action on the ascending limb of the loop of Henle Of all the diuretics, these drugs have the highest efficacy in mobilizing Na+ and Cl from the body. They produce copious amounts of urine. Furosemide is the most commonly used of these drugs. Bumetanide and torsemide are much more potent than furosemide, and the use of these agents is increasing. Ethacrynic acid is used infrequently due to its adverse effect profile.
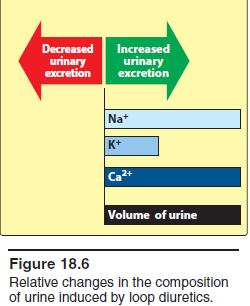
24 A. Bumetanide, furosemide, torsemide, and ethacrynic acid Mechanism of action: Loop diuretics inhibit the cotransport of Na+/K+/2Cl in the luminal membrane in the ascending limb of the loop of Henle. Reabsorption of these ions is decreased. These agents have the greatest diuretic effect of all the diuretic drugs, since the ascending limb accounts for reabsorption of 25% to 30% of filtered NaCl, and downstream sites are unable to compensate for the increased Na+ load. Actions: Loop diuretics act promptly, even in patients with poor renal function or lack of response to other diuretics. Changes in the composition of the urine induced by loop diuretics are shown [Note: Unlike thiazides, loop diuretics increase the Ca2+ content of urine. In patients with normal serum Ca2+ concentrations, hypocalcemia does not result, because Ca2+ is reabsorbed in the distal convoluted tubule.] The loop diuretics may increase renal blood flow, possibly by enhancing prostaglandin synthesis. NSAIDs inhibit renal prostaglandin synthesis and can reduce the diuretic action of loop diuretics.
25
26 Therapeutic uses: The loop diuretics are the drugs of choice for reducing acute pulmonary edema and acute/chronic peripheral edema caused from heart failure or renal impairment. Because of their rapid onset of action, particularly when given intravenously, the drugs are useful in emergency situations such as acute pulmonary edema. Loop diuretics (along with hydration) are also useful in treating hypercalcemia, because they stimulate tubular Ca2+ excretion. They also are useful in the treatment of hyperkalemia. Pharmacokinetics: Loop diuretics are administered orally or parenterally. Their duration of action is relatively brief (2 to 4 hours), allowing patients to predict the window of diuresis. They are secreted into urine.
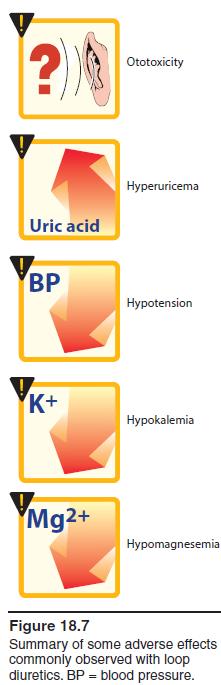
27 Adverse effects: a. Ototoxicity: Reversible or permanent hearing loss may occur with loop diuretics, particularly when used in conjunction with other ototoxic drugs (for example, aminoglycoside antibiotics). Ethacrynic acid is the most likely to cause deafness. Although less common, vestibular function may also be affected, inducing vertigo. b. Hyperuricemia: Furosemide and ethacrynic acid compete with uric acid for the renal secretory systems, thus blocking its secretion and, in turn, causing or exacerbating gouty attacks. c. Acute hypovolemia: Loop diuretics can cause a severe and rapid reduction in blood volume, with the possibility of hypotension, shock, and cardiac arrhythmias. d. Potassium depletion: The heavy load of Na+ presented to the collecting tubule results in increased exchange of tubular Na+ for K+, leading to the possibility of hypokalemia. The loss of K+ from cells in exchange for H+ leads to hypokalemic alkalosis. Use of potassium-sparing diuretics or supplementation with K+ can prevent the development of hypokalemia. e. Hypomagnesemia: Chronic use of loop diuretics combined with low dietary intake of Mg2+ can lead to hypomagnesemia, particularly in the elderly. This can be corrected by oral supplementation.
28
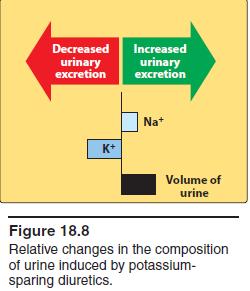
29 POTASSIUM-SPARING DIURETICS Potassium-sparing diuretics act in the collecting tubule to inhibit Na+ reabsorption and K+ excretion. The major use of potassium sparing agents is in the treatment of hypertension (most often in combination with a thiazide) and in heart failure (aldosterone antagonists). It is extremely important that potassium levels are closely monitored in patients treated with potassiumsparing diuretics. These drugs should be avoided in patients with renal dysfunction because of the increased risk of hyperkalemia. Within this class, there are drugs with two distinct mechanisms of action: aldosterone antagonists and sodium channel blockers.
30
31 A. Aldosterone antagonists: spironolactone and eplerenone Mechanism of action: Spironolactone [spear-oh-no-laktone] is a synthetic steroid that antagonizes aldosterone at intracellular cytoplasmic receptor sites rendering the spironolactone receptor complex inactive. It prevents translocation of the receptor complex into the nucleus of the target cell, ultimately resulting in a failure to produce mediator proteins that normally stimulate the Na+/K+-exchange sites of the collecting tubule. Thus, a lack of mediator proteins prevents Na+ reabsorption and, therefore, K+ and H+ secretion. Eplerenone [eh- PLEH-reh-none] is another aldosterone receptor antagonist, which has actions comparable to those of spironolactone, although it may have less endocrine effects than spironolactone.
32 Actions: In most edematous states, blood levels of aldosterone are high, causing retention of Na+. Spironolactone antagonizes the activity of aldosterone, resulting in retention of K+ and excretion of Na+. Similar to thiazides and loop diuretics, the effect of these agents may be diminished by administration of NSAIDs. Therapeutic uses: a. Diuretic: Although the aldosterone antagonists have a low efficacy in mobilizing Na+ from the body in comparison with the other diuretics, they have the useful property of causing the retention of K+. These agents are often given in conjunction with thiazide or loop diuretics to prevent K+ excretion that would otherwise occur with these drugs. Since these drugs work by a mechanism in the later parts of the kidney, these agents can potentiate the effects of more proximally acting agents Spironolactone is the diuretic of choice in patients with hepatic cirrhosis, as edema in these patients is caused by secondary hyperaldosteronism.
33 b. Secondary hyperaldosteronism: Spironolactone is particularly effective in clinical situations associated with secondary hyperaldosteronism, such as hepatic cirrhosis and nephrotic syndrome. c. Heart failure: Aldosterone antagonists prevent remodeling that occurs as compensation for the progressive failure of the heart. Use of these agents has been shown to decrease mortality associated with heart failure, particularly in those with reduced ejection fraction. d. Resistant hypertension: Resistant hypertension, defined by the use of three or more medications without reaching the blood pressure goal, often responds well to aldosterone antagonists. This effect can be seen in those with or without elevated aldosterone levels. e. Ascites: Accumulation of fluid in the abdominal cavity (ascites) is a common complication of hepatic cirrhosis. Spironolactone is effective in this condition. f. Polycystic ovary syndrome: Spironolactone is often used off-label for the treatment of polycystic ovary syndrome. It blocks androgen receptors and inhibits steroid synthesis at high doses, thereby helping to offset increased androgen levels seen in this disorder.
34 Pharmacokinetics: Both spironolactone and eplerenone are absorbed after oral administration and are significantly bound to plasma proteins. Spironolactone is extensively metabolized and converted to several active metabolites. The metabolites, along with the parent drug, are thought to be responsible for the therapeutic effects. 5. Adverse effects: Spironolactone can cause gastric upset. Because it chemically resembles some of the sex steroids, spironolactone may induce gynecomastia in male patients and menstrual irregularities in female patients. Hyperkalemia, nausea, lethargy, and mental confusion can occur. At low doses, spironolactone can be used chronically with few side effects. Potassium-sparing diuretics should be used with caution with other medications that can induce hyperkalemia, such as angiotensinconverting enzyme inhibitors and potassium supplements.
35 Triamterene and amiloride Triamterene [trye-am-ter-een] and amiloride [a-mil-oh-ride] block Na+ transport channels, resulting in a decrease in Na+/K+ exchange. Although they have a K+-sparing diuretic action similar to that of the aldosterone antagonists, their ability to block the Na+/K+-exchange site in the collecting tubule does not depend on the presence of aldosterone. Like the aldosterone antagonists, these agents are not very efficacious diuretics. Both triamterene and amiloride are commonly used in combination with other diuretics, usually for their potassium sparing properties. Much like the aldosterone antagonists, they prevent the loss of K+ that occurs with thiazide and loop diuretics. The side effects of triamterene include increased uric acid, renal stones, and K+ retention.
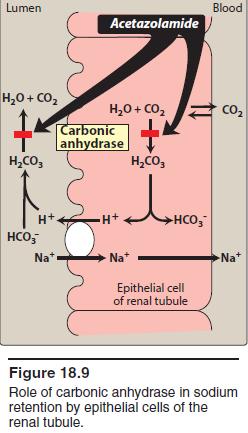
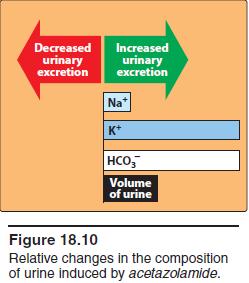
36 CARBONIC ANHYDRASE INHIBITOR Acetazolamide [ah-set-a-zole-a-mide] and other carbonic anhydrase inhibitors are more often used for their other pharmacologic actions than for their diuretic effect, because they are much less efficacious than the thiazide or loop diuretics. A. Acetazolamide Mechanism of action: Acetazolamide inhibits carbonic anhydrase located intracellularly (cytoplasm) and on the apical membrane of the proximal tubular epithelium. [Note: Carbonic anhydrase catalyzes the reaction of CO2 and H2O, leading to H2CO3, which spontaneously ionizes to H+ andhco3 (bicarbonate).] The decreased ability to exchange Na+ for H+ in the presence of acetazolamide results in a mild diuresis. Additionally, HCO3 is retained in the lumen, with marked elevation in urinary ph. The loss of HCO3 causes a hyperchloremic metabolic acidosis and decreased diuretic efficacy following several days of therapy. Changes in the composition. Phosphate excretion is increased by an unknown mechanism.
37
38
39 Therapeutic uses: a. Glaucoma: Acetazolamide decreases the production of aqueous humor and reduces intraocular pressure in patients with chronic open-angle glaucoma, probably by blocking carbonic anhydrase in the ciliary body of the eye. Topical carbonic anhydrase inhibitors, such as dorzolamide and brinzolamide, have the advantage of not causing systemic effects. b. Mountain sickness: Acetazolamide can be used in the prophylaxis of acute mountain sickness. Acetazolamide prevents weakness, breathlessness, dizziness, nausea, and cerebral as well as pulmonary edema characteristic of the syndrome.
40 Pharmacokinetics: Acetazolamide can be administered orally or intravenously. It is approximately 90% protein bound and eliminated renally by both active tubular secretion and passive reabsorption. Adverse effects: Metabolic acidosis (mild), potassium depletion, renal stone formation, drowsiness, and paresthesia may occur. The drug should be avoided in patients with hepatic cirrhosis, because it could lead to a decreased excretion of NH4.+
41 Osmotic Diuretics A number of simple, hydrophilic chemical substances that are filtered through the glomerulus, such as mannitol [MAN-i-tol] and urea [yu- REE-ah], result in some degree of diuresis. Filtered substances that undergo little or no reabsorption will cause an increase in urinary output. The presence of these substances results in a higher osmolarity of the tubular fluid and prevents further water reabsorption, resulting in osmotic diuresis. Only a small amount of additional salt may also be excreted. Because osmotic diuretics are used to increase water excretion rather than Na+ excretion, they are not useful for treating conditions in which Na+ retention occurs. They are used to maintain urine flow following acute toxic ingestion of substances capable of producing acute renal failure.
42 Osmotic diuretics are a mainstay of treatment for patients with increased intracranial pressure or acute renal failure due to shock, drug toxicities, and trauma. Maintaining urine flow preserves long-term kidney function and may save the patient from dialysis. [Note: Mannitol is not absorbed when given orally and should be given intravenously.] Adverse effects include extracellular water expansion and dehydration, as well as hypo- or hypernatremia. The expansion of extracellular water results because the presence of mannitol in the extracellular fluid extracts water from the cells and causes hyponatremia until diuresis occurs
43
Diuretic Agents Part-1. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Diuretic Agents Part-1 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Kidneys eliminates waste products and regulates the volume, electrolyte and ph of
Diuretic Agents Part-1 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Kidneys eliminates waste products and regulates the volume, electrolyte and ph of
PRINCIPLES OF DIURETIC ACTIONS:
 DIURETIC: A drug that increases excretion of solutes Increased urine volume is secondary All clinically useful diuretics act by blocking Na + reabsorption Has the highest EC to IC ratio = always more sodium
DIURETIC: A drug that increases excretion of solutes Increased urine volume is secondary All clinically useful diuretics act by blocking Na + reabsorption Has the highest EC to IC ratio = always more sodium
Pharmacology I [PHL 313] Diuretics. Dr. Mohammad Nazam Ansari
![Pharmacology I [PHL 313] Diuretics. Dr. Mohammad Nazam Ansari](/thumbs/90/104323364.jpg "Pharmacology I [PHL 313] Diuretics. Dr. Mohammad Nazam Ansari") Pharmacology I [PHL 313] Diuretics Dr. Mohammad Nazam Ansari Renal Pharmacology Kidneys: Each adult kidney weighs 125-170g in males and 115-155g in females, represent 0.5% of total body weight, but receive
Pharmacology I [PHL 313] Diuretics Dr. Mohammad Nazam Ansari Renal Pharmacology Kidneys: Each adult kidney weighs 125-170g in males and 115-155g in females, represent 0.5% of total body weight, but receive
Therapeutics of Diuretics
 (Last Updated: 08/22/2018) Created by: Socco, Samantha Therapeutics of Diuretics Thambi, M. (2017). The Clinical Use of Diuretics. Lecture presented at PHAR 503 Lecture in UIC College of Pharmacy, Chicago.
(Last Updated: 08/22/2018) Created by: Socco, Samantha Therapeutics of Diuretics Thambi, M. (2017). The Clinical Use of Diuretics. Lecture presented at PHAR 503 Lecture in UIC College of Pharmacy, Chicago.
DIURETICS. Assoc. Prof. Bilgen Başgut
 DIURETICS Assoc. Prof. Bilgen Başgut Classification of Diuretics The best way to classify diuretics is to look for their Site of action in the nephron A. Diuretics that inhibit transport in the Proximal
DIURETICS Assoc. Prof. Bilgen Başgut Classification of Diuretics The best way to classify diuretics is to look for their Site of action in the nephron A. Diuretics that inhibit transport in the Proximal
Diuretics (Saluretics)
") Diuretics (Saluretics) Diuretics increase urine excretion mainly by reabsorption of salts and water from kidney tubules These agents are ion transport inhibitors that decrease the reabsorption of Na+ at
Diuretics (Saluretics) Diuretics increase urine excretion mainly by reabsorption of salts and water from kidney tubules These agents are ion transport inhibitors that decrease the reabsorption of Na+ at
Renal Pharmacology. Diuretics: Carbonic Anhydrase Inhibitors Thiazides Loop Diuretics Potassium-sparing Diuretics BIMM118
 Diuretics: Carbonic Anhydrase Inhibitors Thiazides Loop Diuretics Potassium-sparing Diuretics Renal Pharmacology Kidneys: Represent 0.5% of total body weight, but receive ~25% of the total arterial blood
Diuretics: Carbonic Anhydrase Inhibitors Thiazides Loop Diuretics Potassium-sparing Diuretics Renal Pharmacology Kidneys: Represent 0.5% of total body weight, but receive ~25% of the total arterial blood
Diuretic Agents Part-2. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Diuretic Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Potassium-sparing diuretics The Ion transport pathways across the luminal and basolateral
Diuretic Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Potassium-sparing diuretics The Ion transport pathways across the luminal and basolateral
Chapter 21. Diuretic Agents. Mosby items and derived items 2008, 2002 by Mosby, Inc., an affiliate of Elsevier Inc.
 Chapter 21 Diuretic Agents Renal Structure and Function Kidneys at level of umbilicus Each weighs 160 to 175 g and is 10 to 12 cm long Most blood flow per gram of weight in body 22% of cardiac output (CO)
Chapter 21 Diuretic Agents Renal Structure and Function Kidneys at level of umbilicus Each weighs 160 to 175 g and is 10 to 12 cm long Most blood flow per gram of weight in body 22% of cardiac output (CO)
DIURETICS-4 Dr. Shariq Syed
 DIURETICS-4 Dr. Shariq Syed AIKTC - Knowledge Resources & Relay Center 1 Pop Quiz!! Loop diuretics act on which transporter PKCC NKCC2 AIKTCC I Don t know AIKTC - Knowledge Resources & Relay Center 2 Pop
DIURETICS-4 Dr. Shariq Syed AIKTC - Knowledge Resources & Relay Center 1 Pop Quiz!! Loop diuretics act on which transporter PKCC NKCC2 AIKTCC I Don t know AIKTC - Knowledge Resources & Relay Center 2 Pop
Low Efficacy Diuretics. Potassium sparing diuretics. Carbonic anhydrase inhibitors. Osmotic diuretics. Miscellaneous
 University of Al Qadisiyah College of Pharmacy Dr. Bassim I Mohammad, MBChB, MSc, Ph.D Low Efficacy Diuretics 1. Potassium sparing diuretics 2. Carbonic anhydrase inhibitors 3. Osmotic diuretics 4. Miscellaneous
University of Al Qadisiyah College of Pharmacy Dr. Bassim I Mohammad, MBChB, MSc, Ph.D Low Efficacy Diuretics 1. Potassium sparing diuretics 2. Carbonic anhydrase inhibitors 3. Osmotic diuretics 4. Miscellaneous
Diuretics having the quality of exciting excessive excretion of urine. OED. Inhibitors of Sodium Reabsorption Saluretics not Aquaretics
 Diuretics having the quality of exciting excessive excretion of urine. OED Inhibitors of Sodium Reabsorption Saluretics not Aquaretics 1 Sodium Absorption Na Entry into the Cell down an electrochemical
Diuretics having the quality of exciting excessive excretion of urine. OED Inhibitors of Sodium Reabsorption Saluretics not Aquaretics 1 Sodium Absorption Na Entry into the Cell down an electrochemical
Chapter 15 Diuretic Agents
 Chapter 15 Diuretic Agents Diuretics Diuretics are agents that increase the rate of urine formation and salt excretion. Diuresis = increased water formation, but the term is also used to indicate increased
Chapter 15 Diuretic Agents Diuretics Diuretics are agents that increase the rate of urine formation and salt excretion. Diuresis = increased water formation, but the term is also used to indicate increased
Diuretic Use in Neonates
 Neonatal Nursing Education Brief: Diuretic Use in the Neonate http://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/ Diuretics
Neonatal Nursing Education Brief: Diuretic Use in the Neonate http://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/ Diuretics
Chapter 15. Diuretic Agents
 Chapter 15. Diuretic Agents Katzung PHARMACOLOGY, 9e > Section III. Cardiovascular-Renal Drugs > Chapter 15. Diuretic Agents > Diuretic Agents: Introduction Abnormalities in fluid volume and electrolyte
Chapter 15. Diuretic Agents Katzung PHARMACOLOGY, 9e > Section III. Cardiovascular-Renal Drugs > Chapter 15. Diuretic Agents > Diuretic Agents: Introduction Abnormalities in fluid volume and electrolyte
Osmotic Diuretics and Carbonic anhydrase inhibitors
 Lecture : Osmotic Diuretics and Carbonic anhydrase inhibitors Contents : Explanation Summary Questions 1 DIURETICS Definition: Are drugs that increase renal excretion of sodium and water resulting in increase
Lecture : Osmotic Diuretics and Carbonic anhydrase inhibitors Contents : Explanation Summary Questions 1 DIURETICS Definition: Are drugs that increase renal excretion of sodium and water resulting in increase
LESSON ASSIGNMENT. Diuretic and Antidiuretic Agents. After you finish this lesson you should be able to:
 LESSON ASSIGNMENT SUBCOURSE MD0806 LESSON 8 Therapeutics III. Diuretic and Antidiuretic Agents. LESSON ASSIGNMENT Paragraphs 8-1--8-7. LESSON OBJECTIVES After you finish this lesson you should be able
LESSON ASSIGNMENT SUBCOURSE MD0806 LESSON 8 Therapeutics III. Diuretic and Antidiuretic Agents. LESSON ASSIGNMENT Paragraphs 8-1--8-7. LESSON OBJECTIVES After you finish this lesson you should be able
Chapter 19 The Urinary System Fluid and Electrolyte Balance
 Chapter 19 The Urinary System Fluid and Electrolyte Balance Chapter Outline The Concept of Balance Water Balance Sodium Balance Potassium Balance Calcium Balance Interactions between Fluid and Electrolyte
Chapter 19 The Urinary System Fluid and Electrolyte Balance Chapter Outline The Concept of Balance Water Balance Sodium Balance Potassium Balance Calcium Balance Interactions between Fluid and Electrolyte
Potassium regulation. -Kidney is a major regulator for potassium Homeostasis.
 Potassium regulation. -Kidney is a major regulator for potassium Homeostasis. Normal potassium intake, distribution, and output from the body. Effects of severe hyperkalemia Partial depolarization of cell
Potassium regulation. -Kidney is a major regulator for potassium Homeostasis. Normal potassium intake, distribution, and output from the body. Effects of severe hyperkalemia Partial depolarization of cell
014 Chapter 14 Created: 9:25:14 PM CST
 014 Chapter 14 Created: 9:25:14 PM CST Student: 1. Functions of the kidneys include A. the regulation of body salt and water balance. B. hydrogen ion homeostasis. C. the regulation of blood glucose concentration.
014 Chapter 14 Created: 9:25:14 PM CST Student: 1. Functions of the kidneys include A. the regulation of body salt and water balance. B. hydrogen ion homeostasis. C. the regulation of blood glucose concentration.
Na + Transport 1 and 2 Linda Costanzo, Ph.D.
 Na + Transport 1 and 2 Linda Costanzo, Ph.D. OBJECTIVES: After studying this lecture, the student should understand: 1. The terminology applied to single nephron function, including the meaning of TF/P
Na + Transport 1 and 2 Linda Costanzo, Ph.D. OBJECTIVES: After studying this lecture, the student should understand: 1. The terminology applied to single nephron function, including the meaning of TF/P
The principal functions of the kidneys
 Renal physiology The principal functions of the kidneys Formation and excretion of urine Excretion of waste products, drugs, and toxins Regulation of body water and mineral content of the body Maintenance
Renal physiology The principal functions of the kidneys Formation and excretion of urine Excretion of waste products, drugs, and toxins Regulation of body water and mineral content of the body Maintenance
DIURETICS-2. Dr. Shariq Syed. Shariq AIKC/TYB/2014
 DIURETICS-2 Dr. Syed Structure of Kidney Blood filtered by functional unit: Nephron Except for cells, proteins, other large molecules, rest gets filtered Structure of Kidney 3 major regions of nephron
DIURETICS-2 Dr. Syed Structure of Kidney Blood filtered by functional unit: Nephron Except for cells, proteins, other large molecules, rest gets filtered Structure of Kidney 3 major regions of nephron
NORMAL POTASSIUM DISTRIBUTION AND BALANCE
 NORMAL POTASSIUM DISTRIBUTION AND BALANCE 98% of body potassium is contained within cells, principally muscle cells, and is readily exchangeable. Only 2% is in ECF. Daily intake exceeds the amount in ECF.
NORMAL POTASSIUM DISTRIBUTION AND BALANCE 98% of body potassium is contained within cells, principally muscle cells, and is readily exchangeable. Only 2% is in ECF. Daily intake exceeds the amount in ECF.
Physio 12 -Summer 02 - Renal Physiology - Page 1
 Physiology 12 Kidney and Fluid regulation Guyton Ch 20, 21,22,23 Roles of the Kidney Regulation of body fluid osmolarity and electrolytes Regulation of acid-base balance (ph) Excretion of natural wastes
Physiology 12 Kidney and Fluid regulation Guyton Ch 20, 21,22,23 Roles of the Kidney Regulation of body fluid osmolarity and electrolytes Regulation of acid-base balance (ph) Excretion of natural wastes
Lecture Topics 利尿药. Diuretics. Diuretic Classes. Definition of diuretic:
 利尿药 Diuretics 四川大学药理教研室朱玲副教授 (zhuling529@163.com) Lecture Topics You need to know these things: high efficacy furosemide moderate hydrochlorothiazide low spironolactonum triameterenum Mechanism of action
利尿药 Diuretics 四川大学药理教研室朱玲副教授 (zhuling529@163.com) Lecture Topics You need to know these things: high efficacy furosemide moderate hydrochlorothiazide low spironolactonum triameterenum Mechanism of action
 Page 1 of 23 Print Close Window Note: Large images and tables on this page may necessitate printing in landscape mode. Copyright The McGraw-Hill Companies. All rights reserved. Basic and Clinical Pharmacology
Page 1 of 23 Print Close Window Note: Large images and tables on this page may necessitate printing in landscape mode. Copyright The McGraw-Hill Companies. All rights reserved. Basic and Clinical Pharmacology
DIURETICS CARBONIC ANHYDRASE INHIBITORS THIAZIDE THIAZIDE-LIKE OSMOTIC DIURETICS LOOP DIURETICS POTASSIUM SPARING DIURETICS
 DIURETICS A diuretic is any substance that promotes diuresis, that is, the increased production of urine. This includes forced diuresis. There are several categories of diuretics. All diuretics increase
DIURETICS A diuretic is any substance that promotes diuresis, that is, the increased production of urine. This includes forced diuresis. There are several categories of diuretics. All diuretics increase
Functions of Proximal Convoluted Tubules
 1. Proximal tubule Solute reabsorption in the proximal tubule is isosmotic (water follows solute osmotically and tubular fluid osmolality remains similar to that of plasma) 60-70% of water and solute reabsorption
1. Proximal tubule Solute reabsorption in the proximal tubule is isosmotic (water follows solute osmotically and tubular fluid osmolality remains similar to that of plasma) 60-70% of water and solute reabsorption
Composition: Each Tablet contains. Pharmacokinetic properties:
 Composition: Each Tablet contains Torsemide 5/10/20/40/100mg Pharmacokinetic properties: Torsemide is well absorbed from the gastrointestinal tract. Peak serum concentrations are achieved within 1 hour
Composition: Each Tablet contains Torsemide 5/10/20/40/100mg Pharmacokinetic properties: Torsemide is well absorbed from the gastrointestinal tract. Peak serum concentrations are achieved within 1 hour
Renal System Dr. Naim Kittana Department of Biomedical Sciences Faculty of Medicine & Health Sciences An-Najah National University
 Renal System Dr. Naim Kittana Department of Biomedical Sciences Faculty of Medicine & Health Sciences An-Najah National University Declaration The content and the figures of this seminar were directly
Renal System Dr. Naim Kittana Department of Biomedical Sciences Faculty of Medicine & Health Sciences An-Najah National University Declaration The content and the figures of this seminar were directly
One Minute Movies: Molecular Action at the Nephron Joy Killough / Westwood High School / Austin,TX
 One Minute Movies: Molecular Action at the Nephron Joy Killough / Westwood High School / Austin,TX To prepare your nephron model: ( A nephron is a tubule and the glomerulus. There are about a million of
One Minute Movies: Molecular Action at the Nephron Joy Killough / Westwood High School / Austin,TX To prepare your nephron model: ( A nephron is a tubule and the glomerulus. There are about a million of
DIURETICS-3 Dr. Shariq Syed
 DIURETICS-3 Dr. Shariq Syed AIKTC - Knowledge Resources & Relay Center 1 Pop Quiz!! Diuretics primarily prevent the reabsorption of K Na Cl I Don t know, Too busy with periodic exams! AIKTC - Knowledge
DIURETICS-3 Dr. Shariq Syed AIKTC - Knowledge Resources & Relay Center 1 Pop Quiz!! Diuretics primarily prevent the reabsorption of K Na Cl I Don t know, Too busy with periodic exams! AIKTC - Knowledge
BCH 450 Biochemistry of Specialized Tissues
 BCH 450 Biochemistry of Specialized Tissues VII. Renal Structure, Function & Regulation Kidney Function 1. Regulate Extracellular fluid (ECF) (plasma and interstitial fluid) through formation of urine.
BCH 450 Biochemistry of Specialized Tissues VII. Renal Structure, Function & Regulation Kidney Function 1. Regulate Extracellular fluid (ECF) (plasma and interstitial fluid) through formation of urine.
Osmoregulation and Renal Function
 1 Bio 236 Lab: Osmoregulation and Renal Function Fig. 1: Kidney Anatomy Fig. 2: Renal Nephron The kidneys are paired structures that lie within the posterior abdominal cavity close to the spine. Each kidney
1 Bio 236 Lab: Osmoregulation and Renal Function Fig. 1: Kidney Anatomy Fig. 2: Renal Nephron The kidneys are paired structures that lie within the posterior abdominal cavity close to the spine. Each kidney
Therapeutic Uses of Diuretics
 DIURETICS Diuretics are drugs that promote the output of urine excreted by the Kidneys. The primary action of most diuretics is the direct inhibition of a + transport at one or more of the four major anatomical
DIURETICS Diuretics are drugs that promote the output of urine excreted by the Kidneys. The primary action of most diuretics is the direct inhibition of a + transport at one or more of the four major anatomical
Renal Quiz - June 22, 21001
 Renal Quiz - June 22, 21001 1. The molecular weight of calcium is 40 and chloride is 36. How many milligrams of CaCl 2 is required to give 2 meq of calcium? a) 40 b) 72 c) 112 d) 224 2. The extracellular
Renal Quiz - June 22, 21001 1. The molecular weight of calcium is 40 and chloride is 36. How many milligrams of CaCl 2 is required to give 2 meq of calcium? a) 40 b) 72 c) 112 d) 224 2. The extracellular
Vertebrates possess kidneys: internal organs which are vital to ion and water balance and excretion.
 The Kidney Vertebrates possess kidneys: internal organs which are vital to ion and water balance and excretion. The kidney has 6 roles in the maintenance of homeostasis. 6 Main Functions 1. Ion Balance
The Kidney Vertebrates possess kidneys: internal organs which are vital to ion and water balance and excretion. The kidney has 6 roles in the maintenance of homeostasis. 6 Main Functions 1. Ion Balance
Osmotic Regulation and the Urinary System. Chapter 50
 Osmotic Regulation and the Urinary System Chapter 50 Challenge Questions Indicate the areas of the nephron that the following hormones target, and describe when and how the hormones elicit their actions.
Osmotic Regulation and the Urinary System Chapter 50 Challenge Questions Indicate the areas of the nephron that the following hormones target, and describe when and how the hormones elicit their actions.
1. a)label the parts indicated above and give one function for structures Y and Z
label the parts indicated above and give one function for structures Y and Z") Excretory System 1 1. Excretory System a)label the parts indicated above and give one function for structures Y and Z W- renal cortex - X- renal medulla Y- renal pelvis collecting center of urine and then
Excretory System 1 1. Excretory System a)label the parts indicated above and give one function for structures Y and Z W- renal cortex - X- renal medulla Y- renal pelvis collecting center of urine and then
BIOLOGY - CLUTCH CH.44 - OSMOREGULATION AND EXCRETION.
 !! www.clutchprep.com Osmoregulation regulation of solute balance and water loss to maintain homeostasis of water content Excretion process of eliminating waste from the body, like nitrogenous waste Kidney
!! www.clutchprep.com Osmoregulation regulation of solute balance and water loss to maintain homeostasis of water content Excretion process of eliminating waste from the body, like nitrogenous waste Kidney
Normal Renal Function
 Normal Renal Function Functions of the Kidney: balances solute and water transport excretes metabolic waste products conserves nutrient regulates acid-base balance secretes hormones that help regulate
Normal Renal Function Functions of the Kidney: balances solute and water transport excretes metabolic waste products conserves nutrient regulates acid-base balance secretes hormones that help regulate
Acid Base Balance. Chapter 26 Balance. ph Imbalances. Acid Base Balance. CO 2 and ph. Carbonic Acid. Part 2. Acid/Base Balance
 Acid Base Balance Chapter 26 Balance Part 2. Acid/Base Balance Precisely balances production and loss of hydrogen ions (ph) The body generates acids during normal metabolism, tends to reduce ph Kidneys:
Acid Base Balance Chapter 26 Balance Part 2. Acid/Base Balance Precisely balances production and loss of hydrogen ions (ph) The body generates acids during normal metabolism, tends to reduce ph Kidneys:
BIPN100 F15 Human Physiology (Kristan) Problem Set #8 Solutions p. 1
 Problem Set #8 Solutions p. 1") BIPN100 F15 Human Physiology (Kristan) Problem Set #8 Solutions p. 1 1. a. Proximal tubule. b. Proximal tubule. c. Glomerular endothelial fenestrae, filtration slits between podocytes of Bowman's capsule.
BIPN100 F15 Human Physiology (Kristan) Problem Set #8 Solutions p. 1 1. a. Proximal tubule. b. Proximal tubule. c. Glomerular endothelial fenestrae, filtration slits between podocytes of Bowman's capsule.
Answers and Explanations
 Answers and Explanations 1. The answer is D [V B 4 b]. Distal K + secretion is decreased by factors that decrease the driving force for passive diffusion of K + across the luminal membrane. Because spironolactone
Answers and Explanations 1. The answer is D [V B 4 b]. Distal K + secretion is decreased by factors that decrease the driving force for passive diffusion of K + across the luminal membrane. Because spironolactone
Furosemide: Properties, Alternatives, and the Medication Approval Process. Heather Brown EMS 209-Advanced Pharmacology Don Knox
 Furosemide: Properties, Alternatives, and the Medication Approval Process Heather Brown EMS 209-Advanced Pharmacology Don Knox Pre-hospital treatment of critical patients is a key factor in determining
Furosemide: Properties, Alternatives, and the Medication Approval Process Heather Brown EMS 209-Advanced Pharmacology Don Knox Pre-hospital treatment of critical patients is a key factor in determining
Questions? Homework due in lab 6. PreLab #6 HW 15 & 16 (follow directions, 6 points!)
") Questions? Homework due in lab 6 PreLab #6 HW 15 & 16 (follow directions, 6 points!) Part 3 Variations in Urine Formation Composition varies Fluid volume Solute concentration Variations in Urine Formation
Questions? Homework due in lab 6 PreLab #6 HW 15 & 16 (follow directions, 6 points!) Part 3 Variations in Urine Formation Composition varies Fluid volume Solute concentration Variations in Urine Formation
LESSON ASSIGNMENT. After completing this lesson, you will be able to: 4-1. Identify the general characteristics of diuretics.
 LESSON ASSIGNMENT LESSON 4 Diuretics. LESSON ASSIGNMENT Paragraphs 4-1 through 4-6. LESSON OBJECTIVES After completing this lesson, you will be able to: 4-1. Identify the general characteristics of diuretics.
LESSON ASSIGNMENT LESSON 4 Diuretics. LESSON ASSIGNMENT Paragraphs 4-1 through 4-6. LESSON OBJECTIVES After completing this lesson, you will be able to: 4-1. Identify the general characteristics of diuretics.
Excretory System 1. a)label the parts indicated above and give one function for structures Y and Z
label the parts indicated above and give one function for structures Y and Z") Excretory System 1 1. Excretory System a)label the parts indicated above and give one function for structures Y and Z W- X- Y- Z- b) Which of the following is not a function of the organ shown? A. to produce
Excretory System 1 1. Excretory System a)label the parts indicated above and give one function for structures Y and Z W- X- Y- Z- b) Which of the following is not a function of the organ shown? A. to produce
Chapter 27: WATER, ELECTROLYTES, AND ACID-BASE BALANCE
 Chapter 27: WATER, ELECTROLYTES, AND ACID-BASE BALANCE I. RELATED TOPICS Integumentary system Cerebrospinal fluid Aqueous humor Digestive juices Feces Capillary dynamics Lymph circulation Edema Osmosis
Chapter 27: WATER, ELECTROLYTES, AND ACID-BASE BALANCE I. RELATED TOPICS Integumentary system Cerebrospinal fluid Aqueous humor Digestive juices Feces Capillary dynamics Lymph circulation Edema Osmosis
I. Metabolic Wastes Metabolic Waste:
 I. Metabolic Wastes Metabolic Waste: a) Carbon Dioxide: by-product of cellular respiration. b) Water: by-product of cellular respiration & dehydration synthesis reactions. c) Inorganic Salts: by-product
I. Metabolic Wastes Metabolic Waste: a) Carbon Dioxide: by-product of cellular respiration. b) Water: by-product of cellular respiration & dehydration synthesis reactions. c) Inorganic Salts: by-product
** TMP mean page 340 in 12 th edition. Questions 1 and 2 Use the following clinical laboratory test results for questions 1 and 2:
 QUESTION Questions 1 and 2 Use the following clinical laboratory test results for questions 1 and 2: Urine flow rate = 1 ml/min Urine inulin concentration = 100 mg/ml Plasma inulin concentration = 2 mg/ml
QUESTION Questions 1 and 2 Use the following clinical laboratory test results for questions 1 and 2: Urine flow rate = 1 ml/min Urine inulin concentration = 100 mg/ml Plasma inulin concentration = 2 mg/ml
Other Factors Affecting GFR. Chapter 25. After Filtration. Reabsorption and Secretion. 5 Functions of the PCT
 Other Factors Affecting GFR Chapter 25 Part 2. Renal Physiology Nitric oxide vasodilator produced by the vascular endothelium Adenosine vasoconstrictor of renal vasculature Endothelin a powerful vasoconstrictor
Other Factors Affecting GFR Chapter 25 Part 2. Renal Physiology Nitric oxide vasodilator produced by the vascular endothelium Adenosine vasoconstrictor of renal vasculature Endothelin a powerful vasoconstrictor
Potassium secretion. E k = -61 log ([k] inside / [k] outside).
![Potassium secretion. E k = -61 log ([k] inside / [k] outside).](/thumbs/80/80478709.jpg "Potassium secretion. E k = -61 log ([k] inside / [k] outside).") 1 Potassium secretion In this sheet, we will continue talking about ultrafiltration in kidney but with different substance which is K+. Here are some informations that you should know about potassium;
1 Potassium secretion In this sheet, we will continue talking about ultrafiltration in kidney but with different substance which is K+. Here are some informations that you should know about potassium;
Renal Physiology - Lectures
 Renal Physiology - Lectures Physiology of Body Fluids PROBLEM SET, RESEARCH ARTICLE Structure & Function of the Kidneys Renal Clearance & Glomerular Filtration PROBLEM SET Regulation of Renal Blood Flow
Renal Physiology - Lectures Physiology of Body Fluids PROBLEM SET, RESEARCH ARTICLE Structure & Function of the Kidneys Renal Clearance & Glomerular Filtration PROBLEM SET Regulation of Renal Blood Flow
Antihypertensive drugs SUMMARY Made by: Lama Shatat
 Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Salt and Water Balance and Nitrogen Excretion
 Announcements Exam is in class on WEDNESDAY. Bring a #2 pencil and your UFID. You must come to your registered class section (except those with DRC accommodations). Office hours Mon 1-3 pm. Teaching evals:
Announcements Exam is in class on WEDNESDAY. Bring a #2 pencil and your UFID. You must come to your registered class section (except those with DRC accommodations). Office hours Mon 1-3 pm. Teaching evals:
Renal Physiology II Tubular functions
 Renal Physiology II Tubular functions LO. 42, 43 Dr. Kékesi Gabriella Basic points of renal physiology 1. Glomerular filtration (GF) a) Ultrafiltration 2. Tubular functions active and passive a) Reabsorption
Renal Physiology II Tubular functions LO. 42, 43 Dr. Kékesi Gabriella Basic points of renal physiology 1. Glomerular filtration (GF) a) Ultrafiltration 2. Tubular functions active and passive a) Reabsorption
Kidney Physiology. Mechanisms of Urine Formation TUBULAR SECRETION Eunise A. Foster Shalonda Reed
 Kidney Physiology Mechanisms of Urine Formation TUBULAR SECRETION Eunise A. Foster Shalonda Reed The purpose of tubular secrection To dispose of certain substances that are bound to plasma proteins. To
Kidney Physiology Mechanisms of Urine Formation TUBULAR SECRETION Eunise A. Foster Shalonda Reed The purpose of tubular secrection To dispose of certain substances that are bound to plasma proteins. To
Acid-Base Balance 11/18/2011. Regulation of Potassium Balance. Regulation of Potassium Balance. Regulatory Site: Cortical Collecting Ducts.
 Influence of Other Hormones on Sodium Balance Acid-Base Balance Estrogens: Enhance NaCl reabsorption by renal tubules May cause water retention during menstrual cycles Are responsible for edema during
Influence of Other Hormones on Sodium Balance Acid-Base Balance Estrogens: Enhance NaCl reabsorption by renal tubules May cause water retention during menstrual cycles Are responsible for edema during
12/7/10. Excretory System. The basic function of the excretory system is to regulate the volume and composition of body fluids by:
 Excretory System The basic function of the excretory system is to regulate the volume and composition of body fluids by: o o removing wastes returning needed substances to the body for reuse Body systems
Excretory System The basic function of the excretory system is to regulate the volume and composition of body fluids by: o o removing wastes returning needed substances to the body for reuse Body systems
Human Anatomy and Physiology - Problem Drill 23: The Urinary System, Fluid, Electrolyte and Acid-Base Balance
 Human Anatomy and Physiology - Problem Drill 23: The Urinary System, Fluid, Electrolyte and Acid-Base Balance Question No. 1 of 10 Which of the following statements about the functions of the urinary system
Human Anatomy and Physiology - Problem Drill 23: The Urinary System, Fluid, Electrolyte and Acid-Base Balance Question No. 1 of 10 Which of the following statements about the functions of the urinary system
Osmoregulation and the Excretory System
 Honors Biology Study Guide Chapter 25.4 25.10 Name Osmoregulation and the Excretory System FUNCTIONS OF THE EXCRETORY SYSTEM OSMOREGULATION Freshwater: Marine: Land Animals: Sources of Nitrogenous Wastes?
Honors Biology Study Guide Chapter 25.4 25.10 Name Osmoregulation and the Excretory System FUNCTIONS OF THE EXCRETORY SYSTEM OSMOREGULATION Freshwater: Marine: Land Animals: Sources of Nitrogenous Wastes?
RENAL PHYSIOLOGY. Physiology Unit 4
 RENAL PHYSIOLOGY Physiology Unit 4 Renal Functions Primary Function is to regulate the chemistry of plasma through urine formation Additional Functions Regulate concentration of waste products Regulate
RENAL PHYSIOLOGY Physiology Unit 4 Renal Functions Primary Function is to regulate the chemistry of plasma through urine formation Additional Functions Regulate concentration of waste products Regulate
Renal Physiology Part II. Bio 219 Napa Valley College Dr. Adam Ross
 Renal Physiology Part II Bio 219 Napa Valley College Dr. Adam Ross Fluid and Electrolyte balance As we know from our previous studies: Water and ions need to be balanced in order to maintain proper homeostatic
Renal Physiology Part II Bio 219 Napa Valley College Dr. Adam Ross Fluid and Electrolyte balance As we know from our previous studies: Water and ions need to be balanced in order to maintain proper homeostatic
WATER, SODIUM AND POTASSIUM
 WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
BIPN100 F15 Human Physiology (Kristan) Lecture 18: Endocrine control of renal function. p. 1
 Lecture 18: Endocrine control of renal function. p. 1") BIPN100 F15 Human Physiology (Kristan) Lecture 18: Endocrine control of renal function. p. 1 Terms you should understand by the end of this section: diuresis, antidiuresis, osmoreceptors, atrial stretch
BIPN100 F15 Human Physiology (Kristan) Lecture 18: Endocrine control of renal function. p. 1 Terms you should understand by the end of this section: diuresis, antidiuresis, osmoreceptors, atrial stretch
The Excretory System. Biology 20
 The Excretory System Biology 20 Introduction Follow along on page 376 What dangers exist if your body is unable to regulate the fluid balance of your tissues? What challenged would the body have to respond
The Excretory System Biology 20 Introduction Follow along on page 376 What dangers exist if your body is unable to regulate the fluid balance of your tissues? What challenged would the body have to respond
QUIZ/TEST REVIEW NOTES SECTION 2 RENAL PHYSIOLOGY FILTRATION [THE KIDNEYS/URINARY SYSTEM] CHAPTER 19
![QUIZ/TEST REVIEW NOTES SECTION 2 RENAL PHYSIOLOGY FILTRATION [THE KIDNEYS/URINARY SYSTEM] CHAPTER 19](/thumbs/80/80449526.jpg "QUIZ/TEST REVIEW NOTES SECTION 2 RENAL PHYSIOLOGY FILTRATION [THE KIDNEYS/URINARY SYSTEM] CHAPTER 19") 1 QUIZ/TEST REVIEW NOTES SECTION 2 RENAL PHYSIOLOGY FILTRATION [THE KIDNEYS/URINARY SYSTEM] CHAPTER 19 Learning Objectives: Differentiate the following processes: filtration, reabsorption, secretion, excretion
1 QUIZ/TEST REVIEW NOTES SECTION 2 RENAL PHYSIOLOGY FILTRATION [THE KIDNEYS/URINARY SYSTEM] CHAPTER 19 Learning Objectives: Differentiate the following processes: filtration, reabsorption, secretion, excretion
Kidney and urine formation
 Kidney and urine formation Renal structure & function Urine formation Urinary y concentration and dilution Regulation of urine formation 1 Kidney and urine formation 1.Renal structure & function 1)General
Kidney and urine formation Renal structure & function Urine formation Urinary y concentration and dilution Regulation of urine formation 1 Kidney and urine formation 1.Renal structure & function 1)General
2) This is a Point and Click question. You must click on the required structure.
 This is a Point and Click question. You must click on the required structure.") Class: A&P2-1 Description: Test: Excretory Test Points: 144 Test Number: 28379 Printed: 31-March-10 12:03 1) This is a Point and Click question. You must click on the required structure. Click on the Bowman's
Class: A&P2-1 Description: Test: Excretory Test Points: 144 Test Number: 28379 Printed: 31-March-10 12:03 1) This is a Point and Click question. You must click on the required structure. Click on the Bowman's
EXCRETION QUESTIONS. Use the following information to answer the next two questions.
 EXCRETION QUESTIONS Use the following information to answer the next two questions. 1. Filtration occurs at the area labeled A. V B. X C. Y D. Z 2. The antidiuretic hormone (vasopressin) acts on the area
EXCRETION QUESTIONS Use the following information to answer the next two questions. 1. Filtration occurs at the area labeled A. V B. X C. Y D. Z 2. The antidiuretic hormone (vasopressin) acts on the area
CHAPTER 27 LECTURE OUTLINE
 CHAPTER 27 LECTURE OUTLINE I. INTRODUCTION A. Body fluid refers to body water and its dissolved substances. B. Regulatory mechanisms insure homeostasis of body fluids since their malfunction may seriously
CHAPTER 27 LECTURE OUTLINE I. INTRODUCTION A. Body fluid refers to body water and its dissolved substances. B. Regulatory mechanisms insure homeostasis of body fluids since their malfunction may seriously
April 08, biology 2201 ch 11.3 excretion.notebook. Biology The Excretory System. Apr 13 9:14 PM EXCRETORY SYSTEM.
 Biology 2201 11.3 The Excretory System EXCRETORY SYSTEM 1 Excretory System How does the excretory system maintain homeostasis? It regulates heat, water, salt, acid base concentrations and metabolite concentrations
Biology 2201 11.3 The Excretory System EXCRETORY SYSTEM 1 Excretory System How does the excretory system maintain homeostasis? It regulates heat, water, salt, acid base concentrations and metabolite concentrations
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance
 Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Principles of Anatomy and Physiology
 Principles of Anatomy and Physiology 14 th Edition CHAPTER 27 Fluid, Electrolyte, and Acid Base Fluid Compartments and Fluid In adults, body fluids make up between 55% and 65% of total body mass. Body
Principles of Anatomy and Physiology 14 th Edition CHAPTER 27 Fluid, Electrolyte, and Acid Base Fluid Compartments and Fluid In adults, body fluids make up between 55% and 65% of total body mass. Body
RENAL SYSTEM 2 TRANSPORT PROPERTIES OF NEPHRON SEGMENTS Emma Jakoi, Ph.D.
 RENAL SYSTEM 2 TRANSPORT PROPERTIES OF NEPHRON SEGMENTS Emma Jakoi, Ph.D. Learning Objectives 1. Identify the region of the renal tubule in which reabsorption and secretion occur. 2. Describe the cellular
RENAL SYSTEM 2 TRANSPORT PROPERTIES OF NEPHRON SEGMENTS Emma Jakoi, Ph.D. Learning Objectives 1. Identify the region of the renal tubule in which reabsorption and secretion occur. 2. Describe the cellular
Nephron Structure inside Kidney:
 In-Depth on Kidney Nephron Structure inside Kidney: - Each nephron has two capillary regions in close proximity to the nephron tubule, the first capillary bed for fluid exchange is called the glomerulus,
In-Depth on Kidney Nephron Structure inside Kidney: - Each nephron has two capillary regions in close proximity to the nephron tubule, the first capillary bed for fluid exchange is called the glomerulus,
Na concentration in the extracellular compartment is 140
 هللامسب Na regulation: Na concentration in the extracellular compartment is 140 meq\l. Na is important because: -It determines the volume of extracellular fluid : the more Na intake will expand extracellular
هللامسب Na regulation: Na concentration in the extracellular compartment is 140 meq\l. Na is important because: -It determines the volume of extracellular fluid : the more Na intake will expand extracellular
RENAL PHYSIOLOGY, HOMEOSTASIS OF FLUID COMPARTMENTS (4) Dr. Attila Nagy 2018
 Dr. Attila Nagy 2018") RENAL PHYSIOLOGY, HOMEOSTASIS OF FLUID COMPARTMENTS (4) Dr. Attila Nagy 2018 Intercalated cells Intercalated cells secrete either H + (Typ A) or HCO 3- (Typ B). In intercalated cells Typ A can be observed
RENAL PHYSIOLOGY, HOMEOSTASIS OF FLUID COMPARTMENTS (4) Dr. Attila Nagy 2018 Intercalated cells Intercalated cells secrete either H + (Typ A) or HCO 3- (Typ B). In intercalated cells Typ A can be observed
organs of the urinary system
 organs of the urinary system Kidneys (2) bean-shaped, fist-sized organ where urine is formed. Lie on either sides of the vertebral column, in a depression beneath peritoneum and protected by lower ribs
organs of the urinary system Kidneys (2) bean-shaped, fist-sized organ where urine is formed. Lie on either sides of the vertebral column, in a depression beneath peritoneum and protected by lower ribs
BIOH122 Human Biological Science 2
 BIOH122 Human Biological Science 2 Session 18 Urinary System 3 Tubular Reabsorption and Secretion Bioscience Department Endeavour College of Natural Health endeavour.edu.au Session Plan o Principles of
BIOH122 Human Biological Science 2 Session 18 Urinary System 3 Tubular Reabsorption and Secretion Bioscience Department Endeavour College of Natural Health endeavour.edu.au Session Plan o Principles of
The Urinary S. (Chp. 10) & Excretion. What are the functions of the urinary system? Maintenance of water-salt and acidbase
 & Excretion. What are the functions of the urinary system? Maintenance of water-salt and acidbase") 10.1 Urinary system The Urinary S. (Chp. 10) & Excretion 10.1 Urinary system What are the functions of the urinary system? 1. Excretion of metabolic wastes (urea, uric acid & creatinine) 1. Maintenance
10.1 Urinary system The Urinary S. (Chp. 10) & Excretion 10.1 Urinary system What are the functions of the urinary system? 1. Excretion of metabolic wastes (urea, uric acid & creatinine) 1. Maintenance
Renal-Related Questions
 Renal-Related Questions 1) List the major segments of the nephron and for each segment describe in a single sentence what happens to sodium there. (10 points). 2) a) Describe the handling by the nephron
Renal-Related Questions 1) List the major segments of the nephron and for each segment describe in a single sentence what happens to sodium there. (10 points). 2) a) Describe the handling by the nephron
BIOL 2402 Fluid/Electrolyte Regulation
 Dr. Chris Doumen Collin County Community College BIOL 2402 Fluid/Electrolyte Regulation 1 Body Water Content On average, we are 50-60 % water For a 70 kg male = 40 liters water This water is divided into
Dr. Chris Doumen Collin County Community College BIOL 2402 Fluid/Electrolyte Regulation 1 Body Water Content On average, we are 50-60 % water For a 70 kg male = 40 liters water This water is divided into
1. remove: waste products: urea, creatinine, and uric acid foreign chemicals: drugs, water soluble vitamins, and food additives, etc.
 Making Water! OR is it really Just Water Just Ask the Nephron!! Author: Patricia L. Ostlund ostlundp@faytechcc.edu (910) 678-9892 Fayetteville Technical Community College Fayetteville, NC 28303 Its just
Making Water! OR is it really Just Water Just Ask the Nephron!! Author: Patricia L. Ostlund ostlundp@faytechcc.edu (910) 678-9892 Fayetteville Technical Community College Fayetteville, NC 28303 Its just
Excretion Chapter 29. The Mammalian Excretory System consists of. The Kidney. The Nephron: the basic unit of the kidney.
 Excretion Chapter 29 The Mammalian Excretory System consists of The Kidney 1. Vertebrate kidneys perform A. Ion balance B. Osmotic balance C. Blood pressure D. ph balance E. Excretion F. Hormone production
Excretion Chapter 29 The Mammalian Excretory System consists of The Kidney 1. Vertebrate kidneys perform A. Ion balance B. Osmotic balance C. Blood pressure D. ph balance E. Excretion F. Hormone production
Spironolactone has not been demonstrated to elevate serum uric acid, to precipitate gout or to alter carbohydrate metabolism.
 SPIRONE Composition Each tablet contains Spironolactone 100 mg. Tablets Action Spironolactone is a specific pharmacologic antagonist of aldosterone, acting primarily through competitive binding of receptors
SPIRONE Composition Each tablet contains Spironolactone 100 mg. Tablets Action Spironolactone is a specific pharmacologic antagonist of aldosterone, acting primarily through competitive binding of receptors
Urine Formation. Urinary Physiology Urinary Section pages Urine Formation. Glomerular Filtration 4/24/2016
 Urine Formation Urinary Physiology Urinary Section pages 9-17 Filtrate Blood plasma minus most proteins Urine
Urine Formation Urinary Physiology Urinary Section pages 9-17 Filtrate Blood plasma minus most proteins Urine
Regulating the Internal Environment. AP Biology
 Regulating the Internal Environment 2006-2007 Conformers vs. Regulators Two evolutionary paths for organisms regulate internal environment maintain relatively constant internal conditions conform to external
Regulating the Internal Environment 2006-2007 Conformers vs. Regulators Two evolutionary paths for organisms regulate internal environment maintain relatively constant internal conditions conform to external
11/05/1431. Urine Formation by the Kidneys Tubular Processing of the Glomerular Filtrate
 Urine Formation by the Kidneys Tubular Processing of the Glomerular Filtrate Chapter 27 pages 327 347 1 OBJECTIVES At the end of this lecture you should be able to describe: Absorptive Characteristics
Urine Formation by the Kidneys Tubular Processing of the Glomerular Filtrate Chapter 27 pages 327 347 1 OBJECTIVES At the end of this lecture you should be able to describe: Absorptive Characteristics
November 30, 2016 & URINE FORMATION
 & URINE FORMATION REVIEW! Urinary/Renal System 200 litres of blood are filtered daily by the kidneys Usable material: reabsorbed back into blood Waste: drained into the bladder away from the heart to the
& URINE FORMATION REVIEW! Urinary/Renal System 200 litres of blood are filtered daily by the kidneys Usable material: reabsorbed back into blood Waste: drained into the bladder away from the heart to the
Water Reabsorption and the Effect of Diuretics on Urine Formation Patricia J. Clark, Ph.D. Department of Biology, IUPUI
 Water Reabsorption and the Effect of Diuretics on Urine Formation Patricia J. Clark, Ph.D. Department of Biology, IUPUI This activity may be done in conjunction with a more traditional urinalysis lab.
Water Reabsorption and the Effect of Diuretics on Urine Formation Patricia J. Clark, Ph.D. Department of Biology, IUPUI This activity may be done in conjunction with a more traditional urinalysis lab.
Outline Urinary System. Urinary System and Excretion. Urine. Urinary System. I. Function II. Organs of the urinary system
 Outline Urinary System Urinary System and Excretion Bio105 Chapter 16 Renal will be on the Final only. I. Function II. Organs of the urinary system A. Kidneys 1. Function 2. Structure III. Disorders of
Outline Urinary System Urinary System and Excretion Bio105 Chapter 16 Renal will be on the Final only. I. Function II. Organs of the urinary system A. Kidneys 1. Function 2. Structure III. Disorders of
Urinary System and Excretion. Bio105 Lecture 20 Chapter 16
 Urinary System and Excretion Bio105 Lecture 20 Chapter 16 1 Outline Urinary System I. Function II. Organs of the urinary system A. Kidneys 1. Function 2. Structure III. Disorders of the urinary system
Urinary System and Excretion Bio105 Lecture 20 Chapter 16 1 Outline Urinary System I. Function II. Organs of the urinary system A. Kidneys 1. Function 2. Structure III. Disorders of the urinary system
Outline Urinary System
 Urinary System and Excretion Bio105 Lecture Packet 20 Chapter 16 Outline Urinary System I. Function II. Organs of the urinary system A. Kidneys 1. Function 2. Structure B. Urine formation 1. Hormonal regulation
Urinary System and Excretion Bio105 Lecture Packet 20 Chapter 16 Outline Urinary System I. Function II. Organs of the urinary system A. Kidneys 1. Function 2. Structure B. Urine formation 1. Hormonal regulation
Renal System and Excretion
 Renal System and Excretion Biology 105 Lecture 19 Chapter 16 Outline Renal System I. Functions II. Organs of the renal system III. Kidneys 1. Structure 2. Function IV. Nephron 1. Structure 2. Function
Renal System and Excretion Biology 105 Lecture 19 Chapter 16 Outline Renal System I. Functions II. Organs of the renal system III. Kidneys 1. Structure 2. Function IV. Nephron 1. Structure 2. Function
Diagram of the inner portions of the kidney
 Excretory and Endocrine functions of the kidney The kidneys are the main excretory organs which eliminate in the urine, most metabolites primarily those containing nitrogen such as ammonia, urea and creatinine.
Excretory and Endocrine functions of the kidney The kidneys are the main excretory organs which eliminate in the urine, most metabolites primarily those containing nitrogen such as ammonia, urea and creatinine.
Medication Review. Renal Drugs. Pharmacy Technician Training Systems Passassured, LLC
 Medication Review Renal Drugs Pharmacy Technician Training Systems Passassured, LLC Medication Review, Renal Drugs PassAssured's Pharmacy Technician Training Program Medication Review Renal Drugs Click
Medication Review Renal Drugs Pharmacy Technician Training Systems Passassured, LLC Medication Review, Renal Drugs PassAssured's Pharmacy Technician Training Program Medication Review Renal Drugs Click