Trauma, severe injury. dr. Péter Kanizsai Semmelweis University, Dept. of Anaesthesia and Intensive Care Division of Oxyology and Emergency Medicine
|
|
|
- Wilfred Fisher
- 5 years ago
- Views:
Transcription



1 Trauma, severe injury dr. Péter Kanizsai Semmelweis University, Dept. of Anaesthesia and Intensive Care Division of Oxyology and Emergency Medicine

2 What is severe injury? Severe injury : a significant acquired brain injury, paraplegia, quadriplegia, amputation of a limb or burns to more that 50 percent of the body; or any other injury specified by the regulations for the purposes of this definition The following injuries (have been prescribed by regulation) as severe injuries: permanent blindness burns to not more than 50 percent of the body that cause severe disfigurement and comprise of full thickness burns: to the head, neck, arms or lower legs; or that result in severe difficulties in performing mobility, communication and self care tasks a brachial plexus injury that results in the loss of the use of a limb
3 How can we tell it is severe? Revised Trauma Score (RTS) Injury Severity Score (ISS) Coded Value GCS SBP (mm Hg) RR (breaths /min) < 50 < > > Glasgow Coma Scale (GCS) Systolic Blood Pressure (SBP) Respiratory Rate (RR) Coded Value > > RTS = GCS SBP RR
4 TRISS Trauma Score - Injury Severity Score : TRISS TRISS determines the probability of survival (Ps) of a patient from the ISS and RTS using the following formulae: Where 'b' is calculated from:

5 Trauma facts Epidemiology Leading cause of death in the first 4 decades 150,000 deaths annually in the US mortality 17 % in Europe Permanent disability 3 times the mortality rate Trauma related dollar costs exceed $400 billion annually
6

7 Trimodal (classic) death distribution Courtesy of dr. Z. Pető, University of Szeged

8 Bimodal death distribution

9 The Nebraska experience, 1976


10 Organizational aspects Improved resuscitation/critical care A advanced T trauma L life S - support
11 The ATLS Concept ABCDE approach to evaluation and treatment Treat greatest threat to life first Definitive diagnosis not immediately important Time is of essence Do no further harm Good recordkeeping is of paramonunt!
12 ATLS Concept Airway with c-spine protection Breathing / ventilation / oxygenation Circulation: stop the bleeding! Disability / neurological status Expose / Environment / body temperature
13 The trauma team An effective trauma system needs the teamwork of EMS, emergency medicine, trauma surgery, and surgery subspecialists Trauma roles Trauma captain Interventionalists Nurses Recorder

14 Trauma Team
15 Initial Assessment / Management Injury Transfer Primary Survey Resuscitation Re-evaluation Adjuncts Detailed Secondary Survey Optimize patient status Re-evaluation Adjuncts Courtesy of dr. Z. Pető, University of Szeged
16 Initial assessment organizational aspects (time dependent team work) always seek info on the mechanism of injury any death in the same compartment high velocity collision ejection vital signs prioritize primary survey and initial stabilization are simultaneous activities!
17 Quick Assessment What is a quick, simple way to assess a patient in 10 seconds? Identify yourself Ask the patient his or her name Ask the patient what happened Courtesy of dr. Z. Pető, University of Szeged



18 Methods of primary survey Physical examination look, listen and feel BP HR SpO 2 CRT temperature PoC techniques: ABG analysis FAST CXR, C-spine Imaging CT MR


19 Focused Assessment with Sonography in Trauma FAST
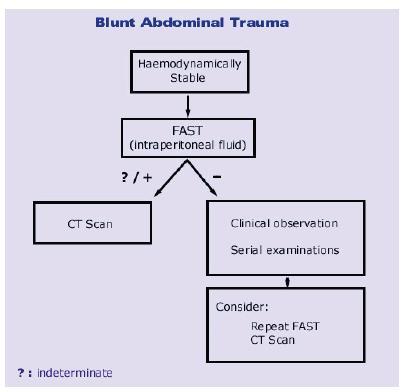
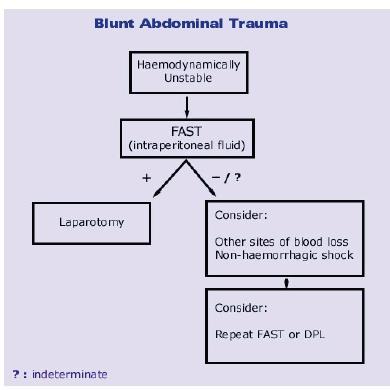
20 FAST

21 Systematic approach A airways with cervical spine protection First you'll need to judge if the airway patent? Have the patient speak to you to establish patency and to evaluate for voice change and stridor Is there evidence of pooling secretions or cyanosis? If airway is intact: look for problems which may cause the patient to lose that airway in the near future. facial injury causing obstruction or bleeding laryngeal fractures expanding hematomas GCS of 9 or less requires intubation
 accessory muscle use (tension pneumothorax) open chest wounds (open pneumothroax).")
 dullness (hemothorax, FAST) subcutaneous emphysema (airway injury) paradoxical movements (flail chest) crepitation & point")
22 Systematic approach B - breathing Inspect: look for cyanosis, JVD (tension pneumothorax or cardiac tamponade) symmetric movement of the chest (flail chest) accessory muscle use (tension pneumothorax) open chest wounds (open pneumothroax). Ausculate: listen for stridor (upper airway injury), lung breath sounds (pneumo or hemothorax) Percuss: feel for: hyper-resonance (pneumothorax) dullness (hemothorax, FAST) subcutaneous emphysema (airway injury) paradoxical movements (flail chest) crepitation & point tendnerness(rib fractures) bruising (pulmonary contusion).
23 Systematic approach C- Circulation Hemorrhage should be assumed in any hypotensive trauma patient Rapid assessment of hemodynamic status Level of consciousness Skin color Pulses in four extremities Blood pressure and pulse pressure
24 Systematic approach Circulation Interventions Cardiac monitor Apply pressure to sites of external hemorrhage Establish IV access 2 large bore IVs Central lines if indicated Cardiac tamponade decompression if indicated (FAST) Volume resuscitation Have blood ready if needed Level One infusers available Foley catheter to monitor resuscitation
25 Systematic approach C - circulation Feel for pulses. as a rule of thumb: if a radial pulse is palpable, it suggests a systolic blood pressure of at least 80 mm Hg. if the femoral or carotid are palpable, these suggest a systolic blood pressure of at least 60 mm Hg. Most patients will have a tachycardic response. exceptions: Neurogenic shock to sympathetic cord disruption Beta blockade, Calcium channel blockade Elderly Children and young adults Conditioned athletes start with a lower basal level.

26 Systematic approach C - circulation ATLS Classification of hemorrhagic shock Heart Rate Blood Pressure Findings Blood Loss Treatment Class I Normalfast Normal <15% Normal Saline Class II Normalfast Normallow Narrowed Pulse Pressure 15-30% Normal Saline Class III Fast Low Altered Mentation 30-40% NS + Blood Class IV Fast Low Obtunded >40% NS + Blood
27 Systematic approach D - disability Quick assessment of mental status via the AVPU scale: Alert - a fully awake patient. Voice - the patient responds when verbally addressed. Response to voice can be verbal, motor, or with eyes. Pain - the patient makes a response on any of the three component measures only when pain stimulus is delivered. Unresponsive - If the patient does not give any eye, voice or motor response to voice or painful stimuli. Perform a gross motor/sensory examination to determine if CNS is intact. Assess pupils for size, symmetry and reactivity. The Glascow Coma Score (GCS) evaluates mental status via assessment of eye opening, motor response, verbal response. (best possible :15, worst possible:3)

28 Disability Interventions Spinal cord injury High dose steroids if within 8 hours not recommended any more! ICP monitor- Neurosurgical consultation Elevated ICP Head of bed elevated Mannitol Hyperventilation Emergent decompression

29 Consider Early Transfer Use time before transfer for resuscitation! Do not delay transfer for diagnostic tests!

30 What is the secondary survey? The complete history and physical examination
31 Secondary survey 1. Head, eyes, ears, nose, and throat (HEENT) a. Assess for evidence of a basilar skull fracture by identifying the presence of Battle s sign (ecchymosis over the mastoid), raccoon eyes (ecchymosis around the eyes) or hemotympanum (blood behind the eardrum) Look for a cerebrospinal fluid (CSF) leak :rhinorrhea or otorrhea. b. Assess for depressed skull fractures by careful palpation. Do not fiddle with foreign bodies and bone fragments! c. Assess for facial injury and stability by palpating the facial bones. Severe fractures carry the risk of airway occlusion! Malocclusion of the teeth may indicate a mandible fracture. d. Look for lacerations that will require repair. Scalp lacerations can bleed vigorously. e. Determine visual acuity and assess pupillary size and function. f. Examine the nasal septum for a hematoma!
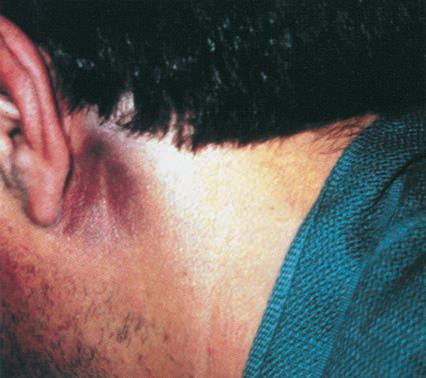
32 Secondary survey 2. Cervical spine/neck a. Palpate the cervical spine and identify areas of tenderness, swelling or step-off deformity. b. Look for penetrating injuries within the neck. c. Evaluate for subcutaneous emphysema, which may be associated with laryngotracheal injury or pneumothorax. 3. Chest a. Palpate the sternum, clavicles, and ribs for tenderness or crepitus. The presence of subcutaneous emphysema suggests an underlying pneumothorax. b. Look for bruising or deformity to suggest an injury to the underlying lung


33
34 Secondary survey 4. Abdomen a. Assess for any distention, tenderness, rebound or guarding. Watch for injuries to the liver and spleen. b. Flank ecchymosis may suggest a retroperitoneal bleed. c. The presence of a seat belt sign is correlated with an eight-fold higher relative risk of intraperitoneal injury d. Reliable assessment of the abdomen may be compromised (altered mental status, intoxication with alcohol or illicit drugs, or the presence of painful distracting injuries. 5. Back a. Log roll the patient with assistance while maintaining spinal alignment. Palpate the entire spine for any spinous process tenderness. b. Assess for hidden wounds in the axilla, under the cervical collar, and in the gluteal region.


35
36 Secondary survey 6. Pelvis a. In order to assess the stability of the pelvis gently employed anterior posterior compression of the anterior superior iliac spines, lateral compression of iliac crests, and cranial caudal distraction of opposite iliac crests. This should be performed one time only! b. Palpate the symphysis pubis for pain, crepitus, or widening. c. Pelvic fractures can be responsible for as much as 2-4 L of occult blood loss. 7. Perineum a. Evaluate the perineum for ecchymosis (pelvic fracture or urethral disruption.) 8. Urethra a. Look for blood at the urethral meatus to assess for possible urethral disruption before placing a urinary catheter.

37 Always inspect the back!




38
39 Secondary survey 9. Extremity examination a. Re-check the vascular status of each extremity, including pulses, color, capillary refill, and temperature. b. Inspect every inch, palpate every bone, and check the range of motion of all joints. Assess for deformity, crepitus, tenderness, swelling, and lacerations. c. Unstable fractures or those associated with neurovascular compromise should be reduced immediately. (hemostasis, preventing further injury, and enhancing patient comfort). 10. Neurologic a. At this time, a complete neurologic examination should be done: - repeat GCS score - reevaluation of the pupils - a cranial nerve examination - a complete sensory and motor examination - testing of the deep tendon reflexes - assessment of the response to plantar stimulation.


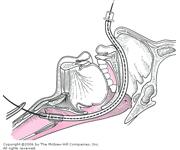
40 Airway management Aim: secure and permanent airway intubation surgical





41
42 Why do patients die despite all our efforts? What causes delayed trauma mortality?
43 Infection Complications Frequent COD in pts who survive longer than 3 days. Immune system is frequently depressed because of physiological response or treatment Accidents take place in dirty environment &id=10&rnd=
44 Acute Respiratory Distress Inflammatory syndrome-disrupts the alveolarcapillary membrane The permeability increases and proteins/fluid shift into the interstitial space A cascading failure begins that eventually leads to alveolar collapse &id=10&rnd=
45 Systemic Inflammatory Response Inflammation is a normal defensive response to insult/injury Creates a lethal microenvironment Vascular system shunts elements to area Leukocytes Plasma proteins platelets &id=10&rnd=
46 Systemic Inflammatory Response Local inflammation is generally self limiting (8-10 days) Systemic Organs remote from insult show signs Temperature abnormalities Tachycardia Ventilation abnormalities &id=10&rnd=

47

48
49 Multi Organ Dysfunction Syndrome 7%-15% of critically ill patients suffer failure of at least two organ systems Failure of three or more organ systems leads to a 90%-95% mortality rate Trauma patients are very susceptible to Prolonged circulatory shock Tissue hypoxemia Infection &id=10&rnd=
50 MODS Either primary or secondary Results from acute immune and inflammatory response Chemistry is complicated The immune system turns on normal cells and destroys them &id=10&rnd=
51 Myoglobinuria Trauma causes increased breakdown of skeletal muscles the muscle releases myoglobin and potassium myoglobin is a large molecule that blocks the renal tubules kidney failure &id=10&rnd=
52 DIC Initially hypercoagulation leading to organ ischemia. Simultaneous micro vascular hemorrhage and clotting Clotting agents are consumed faster than created Most likely results from damage to the endothelium Results in uncontrolled bleeding additional to the blood loss due to the initial insult &id=10&rnd=
53 All the above will lead to HYPOVOLAEMIC SHOCK!
54 What is shock? Generalized State of Hypoperfusion Inadequate oxygen delivery Catecholamines and other responses Anaerobic metabolism Cellular dysfunction Cell death Courtesy of dr. Z. Pető, University of Szeged
55 Signs of shock Alteration in level of consciousness, anxiety Cold, diaphoretic skin Tachycardia Tachypnea, shallow respirations Hypotension Decreased urinary output Courtesy of dr. Z. Pető, University of Szeged
56 Interventions Direct pressure / tourniquet Reduce pelvic volume STOP the bleeding! Operation Angioembolization Splint fractures Courtesy of dr. Z. Pető, University of Szeged

57 The IT clamp
58 Fluid resuscitation Vascular access? Type? Volume? Monitor response Prevent hypothermia!


59 Vascular access? F= ΔP x π x r 4 8η x l
60 Type? Volume? Aim is to restore circulation -team approach -no benefit of colloid over crystalloid -give 2 litres of crystalloid initially (N.S.) -blood sample for serology, clotting screen -to keep Hb>80 g/l cell saver techniques are required -2 units of 0 neg blood can be transfused in emergency -always try to transfuse fully compatible bloodaim to a PLT count > 75 G/l and TT < 1,5 -if 1-1,5 blood volume was repleted give FFP and PLT complex -keep calcium > 1,13 mm/l and fibrinogen > 1 g/l -prevent DIC -New guidelines suggest use of (1 unit of PBC, 1 unit of FFP and 1 unit of platelet)
61 General emergency remarks Time dependency: Golden hour (?) Not scientifically supported But it s a good rule of thumb Definitive care is the answer- not field care
62 General emergency remarks Allocation care is allocated to patient transfer only if unavoidable prioritize according to severity
63 General emergency remarks Integration multidisciplinary approach in trauma care there is no I, only we consultation and referral 24/7
64 Now let s go and operate! Fractures need mended! Save the patients life with quick and extended operations!
65 But what if patient is too old? patient is exsanguinated? patient is hypothermic? patient is haemodynamically unstable? etc..


66 A new paradigm Damage control
67 Definitive care vs. damage control early total care borderline era damage control
68 In a timely fashion Most patients are not ready for intervention Long operations will result in large fluid and heat loss Not all threatening injuries are real threat to life Surgeons need self control


69 Vicious circle in major torso trauma KC Sihler, LM Napolitano : Massive Transfusion New Insights Chest, 2009; 36

70 Damage control Choosing the right candidate - hypothermia: T<34 C acidosis ph < 7,2 lactate > 5 mmol/l coagulopathy SBP < 70 Hgmm Transfusion > 15 units ISS > 36

71 Practice of damage control

72 Practice of damage control
73 Priorities in the multiple injured victim Save life - Resuscitation, ATLS (advanced trauma life support) e.g. chest drain, amputation, laparotomy Save limb - Revascularization - Fasciotomy Save fracture - Debridement - Reposition, stabilization, alignement
74 Take home messages Trauma is best managed by a team approach Importance of ATLS A thorough primary and secondary survey is key to identify life threatening injuries Once a life threatening injury is discovered, intervention should not be delayed Disposition is determined by the patient s condition as well as available resources.
ATLS: Initial Assessment and Management. SAUSHEC Medical Student Lecture Series
 ATLS: Initial Assessment and Management SAUSHEC Medical Student Lecture Series Objectives Identify sequence of priorities in assessing the multiply injured patient Apply principles outlined in primary
ATLS: Initial Assessment and Management SAUSHEC Medical Student Lecture Series Objectives Identify sequence of priorities in assessing the multiply injured patient Apply principles outlined in primary
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of
 Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
3. D Objective: Chapter 4, Objective 4 Page: 79 Rationale: A carbon dioxide level below 35 mmhg indicates hyperventilation.
 1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
INTERNATIONAL TRAUMA LIFE SUPPORT
 INTERNATIONAL TRAUMA LIFE SUPPORT NC ITLS Rev. 2/18 STUDENT GUIDE TO INTERNATIONAL TRAUMA LIFE SUPPORT What to wear ITLS is a practical course that stresses hands-on teaching. You should wear comfortable
INTERNATIONAL TRAUMA LIFE SUPPORT NC ITLS Rev. 2/18 STUDENT GUIDE TO INTERNATIONAL TRAUMA LIFE SUPPORT What to wear ITLS is a practical course that stresses hands-on teaching. You should wear comfortable
APPROACH TO TRAUMA. Dr E.Memary Anesthesiologist Assistant Professor of SBMU
 APPROACH TO TRAUMA Dr E.Memary Anesthesiologist Assistant Professor of SBMU Objectives Describe the initial approach to the injured patient, including the primary and secondary surveys. Identify the types
APPROACH TO TRAUMA Dr E.Memary Anesthesiologist Assistant Professor of SBMU Objectives Describe the initial approach to the injured patient, including the primary and secondary surveys. Identify the types
Patient Assessment. Chapter 8
 Patient Assessment Chapter 8 Patient Assessment Scene size-up Initial assessment Focused history and physical exam Vital signs History Detailed physical exam Ongoing assessment Patient Assessment Process
Patient Assessment Chapter 8 Patient Assessment Scene size-up Initial assessment Focused history and physical exam Vital signs History Detailed physical exam Ongoing assessment Patient Assessment Process
European Resuscitation Council
 European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
Emergency Room Resuscitation of the Unstable Trauma Patient
 Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D.
 1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D. Sacral-coccygeal 2. A 36-year-old male sustains blunt force thoracic
1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D. Sacral-coccygeal 2. A 36-year-old male sustains blunt force thoracic
Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing
 1 2 3 4 5 6 Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing D-Disability Chief complaint and/or Mechanism
1 2 3 4 5 6 Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing D-Disability Chief complaint and/or Mechanism
PRE-HOSPITAL EMERGENCY CARE COURSE.
 PRE-HOSPITAL EMERGENCY CARE COURSE www.basics.org.uk Chest Assessment & Management BASICS Education March 2016 Objectives To understand the importance of oxygenation and ventilation To be able to describe
PRE-HOSPITAL EMERGENCY CARE COURSE www.basics.org.uk Chest Assessment & Management BASICS Education March 2016 Objectives To understand the importance of oxygenation and ventilation To be able to describe
Patient Assessment From Brady s First Responder (8th Edition) 83 Questions
 83 Questions") Patient Assessment From Brady s First Responder (8th Edition) 83 Questions 1. Which question is important if your patient may be a candidate for surgery? p. 183 *A.) When did you last eat? B.) What is
Patient Assessment From Brady s First Responder (8th Edition) 83 Questions 1. Which question is important if your patient may be a candidate for surgery? p. 183 *A.) When did you last eat? B.) What is
Focused History and Physical Examination of the
 Henry: EMT Prehospital Care, Revised 3 rd Edition Lecture Notes Chapter 10: Focused History and Physical Examination of Trauma Patients Chapter 10 Focused History and Physical Examination of the Trauma
Henry: EMT Prehospital Care, Revised 3 rd Edition Lecture Notes Chapter 10: Focused History and Physical Examination of Trauma Patients Chapter 10 Focused History and Physical Examination of the Trauma
TNP Teaching Station E Focus: Intubated Patient, Interpersonal Violence
 TNP Teaching Station E Focus: Intubated Patient, Interpersonal Violence Objective Upon completion of this teaching station the learner will be able to: 1. demonstrate appropriate assessment for a hemodynamically
TNP Teaching Station E Focus: Intubated Patient, Interpersonal Violence Objective Upon completion of this teaching station the learner will be able to: 1. demonstrate appropriate assessment for a hemodynamically
The Primary Survey. C. Clay Cothren, MD FACS. Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado
 The Primary Survey C. Clay Cothren, MD FACS Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado Outlining the ABCs Why do we need such an approach? The
The Primary Survey C. Clay Cothren, MD FACS Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado Outlining the ABCs Why do we need such an approach? The
History Data Panel. Case 030 Preg Trauma. Presenting Complaint Altered mental status s/p MVC. Person Giving Information EMS
 History Data Panel Presenting Complaint Altered mental status s/p MVC Person Giving Information EMS History of Present Illness 28 year old woman, 35 weeks pregnant per report of her husband the passenger.
History Data Panel Presenting Complaint Altered mental status s/p MVC Person Giving Information EMS History of Present Illness 28 year old woman, 35 weeks pregnant per report of her husband the passenger.
 55-year-old male with 2nd and 3rd degree burns to face, chest, and arms on 25% of the body Respirations: 34 Pulse: 120 Mental Status: moans to painful stimulus Mucous membranes charred Stridor 10 cm scalp
55-year-old male with 2nd and 3rd degree burns to face, chest, and arms on 25% of the body Respirations: 34 Pulse: 120 Mental Status: moans to painful stimulus Mucous membranes charred Stridor 10 cm scalp
Patient Care Report Guidelines
 A rrival on scene / Scene assessment C omplaint H istory A. Position of patient B. Impression of patient C. Does the patient acknowledge your presence D. Any significant characteristics of the scene A.
A rrival on scene / Scene assessment C omplaint H istory A. Position of patient B. Impression of patient C. Does the patient acknowledge your presence D. Any significant characteristics of the scene A.
1. Which of the following organs is contained in the retroperitoneal region of the abdomen? A. Stomach B. Liver C. Kidney D.
 1. Which of the following organs is contained in the retroperitoneal region of the abdomen? A. Stomach B. Liver C. Kidney D. Uterus 2. What is Sellick's maneuver? A. A method allowing the rescuer to hold
1. Which of the following organs is contained in the retroperitoneal region of the abdomen? A. Stomach B. Liver C. Kidney D. Uterus 2. What is Sellick's maneuver? A. A method allowing the rescuer to hold
Pediatric Advanced Life Support
 Pediatric Advanced Life Support Pediatric Chain of Survival Berg M D et al. Circulation 2010;122:S862-S875 Prevention Early cardiopulmonary resuscitation (CPR) Prompt access to the emergency response system
Pediatric Advanced Life Support Pediatric Chain of Survival Berg M D et al. Circulation 2010;122:S862-S875 Prevention Early cardiopulmonary resuscitation (CPR) Prompt access to the emergency response system
The Primary Survey. Clay Cothren Burlew, MD FACS
 The Primary Survey Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Attending Surgeon, Denver Health Medical Center Associate Professor of Surgery, University of Colorado Outlining the
The Primary Survey Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Attending Surgeon, Denver Health Medical Center Associate Professor of Surgery, University of Colorado Outlining the
Introduction to Advanced Trauma Life Support ATLS
 Introduction to Advanced Trauma Life Support ATLS Objectives Concepts of primary & secondary survey Priorities & Life threatening conditions Clinical & Surgical skills Basic knowledge Rapid assessment
Introduction to Advanced Trauma Life Support ATLS Objectives Concepts of primary & secondary survey Priorities & Life threatening conditions Clinical & Surgical skills Basic knowledge Rapid assessment
ITLS Advanced Pre-Test Annotated Key 8 th Edition
 1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
68W COMBAT MEDIC POCKET GUIDE
 GTA 08-05-058 68W COMBAT MEDIC POCKET GUIDE PART I: TRAUMA TREATMENT This publication contains technical information that is for official Government use only. Distribution is limited to U.S. Government
GTA 08-05-058 68W COMBAT MEDIC POCKET GUIDE PART I: TRAUMA TREATMENT This publication contains technical information that is for official Government use only. Distribution is limited to U.S. Government
Emergency Medical Training Services Emergency Medical Technician Basic Program Outlines Outline Topic: ASSESSMENT Revised: 11/2013
 Emergency Medical Training Services Emergency Medical Technician Basic Program Outlines Outline Topic: ASSESSMENT Revised: 11/2013 DEFINITIONS General Impression - EMT develops a plan of action from the
Emergency Medical Training Services Emergency Medical Technician Basic Program Outlines Outline Topic: ASSESSMENT Revised: 11/2013 DEFINITIONS General Impression - EMT develops a plan of action from the
Pre-hospital Trauma Life Support. Rattiya Banjungam Emergency Physician, Khon Kaen Hospital
 Pre-hospital Trauma Life Support Rattiya Banjungam Emergency Physician, Khon Kaen Hospital Golden principles of Prehospital Trauma Care Golden Hour There is a golden hour if you are critically injured,
Pre-hospital Trauma Life Support Rattiya Banjungam Emergency Physician, Khon Kaen Hospital Golden principles of Prehospital Trauma Care Golden Hour There is a golden hour if you are critically injured,
Restore adequate respiratory and circulatory conditions. Reduce pain
 Pre-hospital management of the trauma patient is best performed by an integrated team focused on minimizing the time from injury to definitive care at an appropriate trauma center. Dispatchers, first responders,
Pre-hospital management of the trauma patient is best performed by an integrated team focused on minimizing the time from injury to definitive care at an appropriate trauma center. Dispatchers, first responders,
ITLS Pediatric Provider Course Basic Pre-Test
 ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
Pediatric Trauma Practice. Guideline for Management of the Child in Shock. Background
 Pediatric Trauma Practice Guideline for Management of the Child in Shock Background Guideline for Management Trauma is the leading cause of death in children and adolescents in the United States. Although
Pediatric Trauma Practice Guideline for Management of the Child in Shock Background Guideline for Management Trauma is the leading cause of death in children and adolescents in the United States. Although
The ABC s of Chest Trauma
 The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials
 Preparatory Materials") Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
the bleeding won t stop? Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital
 Royal Alexandra Hospital") What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
oriented evaluation of your patient and establishing priorities of care based on existing and
 1 Chapter 12: Patient Assessment in the Field 2 Patient assessment means conducting a - oriented evaluation of your patient and establishing priorities of care based on existing and potential threats to
1 Chapter 12: Patient Assessment in the Field 2 Patient assessment means conducting a - oriented evaluation of your patient and establishing priorities of care based on existing and potential threats to
Overview. Overview. Chapter 30. Injuries to the Head and Spine 9/11/2012. Review of the Nervous and Skeletal Systems. Devices for Immobilization
 Chapter 30 Injuries to the Head and Spine Slide 1 Overview Review of the Nervous and Skeletal Systems The Nervous System The Skeletal System Devices for Immobilization Cervical Spine Short Backboards Long
Chapter 30 Injuries to the Head and Spine Slide 1 Overview Review of the Nervous and Skeletal Systems The Nervous System The Skeletal System Devices for Immobilization Cervical Spine Short Backboards Long
Aurora Health Care EMS Continuing Education Spring 2011 Packet THORACIC TRAUMA THE PREHOSPITAL APPROACH TO CHEST INJURY MANAGEMENT
 Aurora Health Care EMS Continuing Education Spring 2011 Packet THORACIC TRAUMA Chest injuries are significant contributors to death from major trauma and can be difficult to assess adequately in the pre-hospital
Aurora Health Care EMS Continuing Education Spring 2011 Packet THORACIC TRAUMA Chest injuries are significant contributors to death from major trauma and can be difficult to assess adequately in the pre-hospital
VAO BASIC SUPPORT CLINICAL APPROACH TO THE PATIENT HANDOUT
 CLINICAL APPROACH TO THE PATIENT HANDOUT 1 I am the most important part of patient care. How can you expect to treat a patient appropriately if you don t follow through on basic primary care? Remember:
CLINICAL APPROACH TO THE PATIENT HANDOUT 1 I am the most important part of patient care. How can you expect to treat a patient appropriately if you don t follow through on basic primary care? Remember:
Introduction to Emergency Medical Care 1
 Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
Anesthesia for multiple trauma: from the scene to the OR
 Anesthesia for multiple trauma: from the scene to the OR Gary Hartstein,, M.D. Service d'anesthésie-réanimationsie-réanimation Service des Urgences CHU Liège B.35 4000 Liège Course outline philosophy of
Anesthesia for multiple trauma: from the scene to the OR Gary Hartstein,, M.D. Service d'anesthésie-réanimationsie-réanimation Service des Urgences CHU Liège B.35 4000 Liège Course outline philosophy of
Basic Assessment and Treatment of Trauma
 Basic Assessment and Treatment of Trauma Final Exam Version 1 1. In which of the following scenarios would the potential for serious injury or death be the GREATEST? A. 77-kg (170-lb) man who falls 1.2
Basic Assessment and Treatment of Trauma Final Exam Version 1 1. In which of the following scenarios would the potential for serious injury or death be the GREATEST? A. 77-kg (170-lb) man who falls 1.2
Shenandoah Co. Fire & Rescue. Injuries to. and Spine. December EMS Training Bill Streett Training Section Chief
 Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#
Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#
TRAUMA PATIENT ASSESSMENT
 SECTION: Adult Trauma Emergencies PROTOCOL TITLE: Injury General Trauma Management REVISED: 06/2015 OVERVIEW Each year, one out of three Americans sustains a traumatic injury. Trauma is a major cause of
SECTION: Adult Trauma Emergencies PROTOCOL TITLE: Injury General Trauma Management REVISED: 06/2015 OVERVIEW Each year, one out of three Americans sustains a traumatic injury. Trauma is a major cause of
Major Trauma Scenarios. Ballarat Health Services Emergency Medicine Training Hub
 Major Trauma Scenarios Ballarat Health Services Emergency Medicine Training Hub Trauma Scenario 1 You receive a phone call from the ambulance service. They have a 27 yr old male involved in a MCA, he is
Major Trauma Scenarios Ballarat Health Services Emergency Medicine Training Hub Trauma Scenario 1 You receive a phone call from the ambulance service. They have a 27 yr old male involved in a MCA, he is
Assessment and Scoring Tools
 Assessment and Scoring Tools 2013 APGAR Scale 0 points 1 point 2 points Heart Rate Absent 100 Respiratory Rate Absent Slow, irregular Good, drying Irritability Flaccid Some flexion Active motion
Assessment and Scoring Tools 2013 APGAR Scale 0 points 1 point 2 points Heart Rate Absent 100 Respiratory Rate Absent Slow, irregular Good, drying Irritability Flaccid Some flexion Active motion
Trauma is a Disease Lets Get it Right A Good Trauma Examination Gives Your Patient Increased Odds for a Good Outcome
 A Good Trauma Examination Gives Your Patient Increased Odds for a Good Outcome druffol@lumc.edu 708.216.4541 Lets Get it Right Trauma is a Disease Importance of Trauma Care and the trauma provider role
A Good Trauma Examination Gives Your Patient Increased Odds for a Good Outcome druffol@lumc.edu 708.216.4541 Lets Get it Right Trauma is a Disease Importance of Trauma Care and the trauma provider role
You Are the Emergency Medical Responder
 Lesson 32: Injuries to the Chest, Abdomen and Genitalia You Are the Emergency Medical Responder Your police unit responds to a call in a part of town plagued by violence. When you arrive, you find the
Lesson 32: Injuries to the Chest, Abdomen and Genitalia You Are the Emergency Medical Responder Your police unit responds to a call in a part of town plagued by violence. When you arrive, you find the
North Oaks Trauma Symposium Friday, November 3, 2017
 + Evaluation and Management of Facial Trauma D Antoni Dennis, MD North Oaks ENT an Allergy November 3, 2017 + Financial Disclosure I do not have any conflicts of interest or financial interest to disclose
+ Evaluation and Management of Facial Trauma D Antoni Dennis, MD North Oaks ENT an Allergy November 3, 2017 + Financial Disclosure I do not have any conflicts of interest or financial interest to disclose
Polytrauma. Same stuff-different day! 9/14/2012. Managing the difficult airway in Multi-Systems Trauma. Jerry J Ryman CRT
 Managing the difficult airway in Multi-Systems Trauma Jerry J Ryman CRT Polytrauma More than 1 organ system involved Pulmonary Circulatory Neurological Integumentary Musculo-skeletal Genito-urinary Endocrine
Managing the difficult airway in Multi-Systems Trauma Jerry J Ryman CRT Polytrauma More than 1 organ system involved Pulmonary Circulatory Neurological Integumentary Musculo-skeletal Genito-urinary Endocrine
APPROACH TO TRAUMA CARE
 APPROACH TO TRAUMA CARE Timothy Murray, RN, CFRN Jan 2017 OBJECTIVES Demonstrate Concepts of Primary and Secondary Patient Assessment Establish Management Priorities in Trauma Situations Initiating Interventions
APPROACH TO TRAUMA CARE Timothy Murray, RN, CFRN Jan 2017 OBJECTIVES Demonstrate Concepts of Primary and Secondary Patient Assessment Establish Management Priorities in Trauma Situations Initiating Interventions
ITLS Pediatric Provider Course Advanced Pre-Test
 ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
Chapter 34. Objectives. Objectives 01/09/2013. Chest Trauma
 Chapter 34 Chest Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms introduced
Chapter 34 Chest Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms introduced
D. Pre-Hospital Trauma Triage and Bypass Algorithm
 D. Pre-Hospital Trauma Triage and Bypass Algorithm Hospital bypass is defined as transporting the patient to the nearest hospital that has the appropriate level of care for the patient s suspected severity
D. Pre-Hospital Trauma Triage and Bypass Algorithm Hospital bypass is defined as transporting the patient to the nearest hospital that has the appropriate level of care for the patient s suspected severity
MASSACHUSETTS DEPARTMENT OF PUBLIC HEALTH OFFICE OF EMERGENCY MEDICAL SERVICES Basic EMT Practical Examination Cardiac Arrest Management
 Basic EMT Practical Examination 6.0 - Cardiac Arrest Management Station 1 RESUSCITATION & DEFIBRILLATION No Point WHILE FUNCTIONING AS FIRST RESCUER: Point 1. Verbalizes or takes body substance isolation
Basic EMT Practical Examination 6.0 - Cardiac Arrest Management Station 1 RESUSCITATION & DEFIBRILLATION No Point WHILE FUNCTIONING AS FIRST RESCUER: Point 1. Verbalizes or takes body substance isolation
PEDIATRIC TRAUMA: Implications for Respiratory Care
 PEDIATRIC TRAUMA: Implications for Respiratory Care 17 th Annual Rainbow Respiratory Conference - September 4, 2015 Mike Dingeldein, MD Pediatric Surgeon Pediatric Trauma Medical Director Disclosures none
PEDIATRIC TRAUMA: Implications for Respiratory Care 17 th Annual Rainbow Respiratory Conference - September 4, 2015 Mike Dingeldein, MD Pediatric Surgeon Pediatric Trauma Medical Director Disclosures none
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: Shock Revised: 11/2013
 Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: Shock Revised: 11/2013 (12 questions on trauma exam from this outline) DEFINITIONS Aerobic metabolism
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: Shock Revised: 11/2013 (12 questions on trauma exam from this outline) DEFINITIONS Aerobic metabolism
Damage Control in Abdominal and Pelvic Injuries
 Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Student Guide Module 4: Pediatric Trauma
 Student Guide Module 4: Pediatric Trauma Problem based learning exercise objectives Understand how to manage traumatic injuries in mass casualty events. Discuss the features and the approach to pediatric
Student Guide Module 4: Pediatric Trauma Problem based learning exercise objectives Understand how to manage traumatic injuries in mass casualty events. Discuss the features and the approach to pediatric
Assessment of the Trauma Patient
 CHAPTER 10 Assessment of the Trauma Patient Overall Assessment Scheme Scene Size-Up Initial Assessment Trauma Physical Exam Vital Signs & SAMPLE History Medical SAMPLE History Physical Exam & Vital Signs
CHAPTER 10 Assessment of the Trauma Patient Overall Assessment Scheme Scene Size-Up Initial Assessment Trauma Physical Exam Vital Signs & SAMPLE History Medical SAMPLE History Physical Exam & Vital Signs
EMS System for Metropolitan Oklahoma City and Tulsa 2019 Medical Control Board Treatment Protocols
 EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
Chapter 13. Objectives. Objectives 01/09/2013. Patient Assessment
 Chapter 13 Patient Assessment Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms
Chapter 13 Patient Assessment Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms
The Management of Trauma. Trauma. Ways of Trauma Management. Why it s important 08/06/2012. RTC s account for most injuries. Injury is a disease
 The Management of Trauma RTC s account for most injuries Followed by assaults, drownings, falls, burns Injury is a disease Trauma 400 350 300 Trimodal Distribution of Death Laceration : Brain Brainstem
The Management of Trauma RTC s account for most injuries Followed by assaults, drownings, falls, burns Injury is a disease Trauma 400 350 300 Trimodal Distribution of Death Laceration : Brain Brainstem
A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion
 A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion Christopher Butts PhD, DO Surgical Critical Care Fellow Cooper University Hospital H&P 10 year old female presents as a trauma
A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion Christopher Butts PhD, DO Surgical Critical Care Fellow Cooper University Hospital H&P 10 year old female presents as a trauma
Chapter 26 Head and Spine Trauma The Nervous System The nervous system controls virtually all of our body activities including reflex, voluntary and
 1 2 3 4 5 Chapter 26 Head and Spine Trauma The Nervous System The nervous system controls virtually all of our body activities including reflex, voluntary and involuntary activities Voluntary activities
1 2 3 4 5 Chapter 26 Head and Spine Trauma The Nervous System The nervous system controls virtually all of our body activities including reflex, voluntary and involuntary activities Voluntary activities
EMS System for Metropolitan Oklahoma City and Tulsa 2018 Medical Control Board Treatment Protocols
 EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
In ESH we usually see blunt chest trauma but penetrating injuries also treated here (usually as single injuries, like stab wound)
") Chest Trauma Dr Csaba Dioszeghy MD PhD FRCEM FFICM FERC East Surrey Hospital Emergency Department Scope Thoracic injuries are common and can be life threatening In ESH we usually see blunt chest trauma
Chest Trauma Dr Csaba Dioszeghy MD PhD FRCEM FFICM FERC East Surrey Hospital Emergency Department Scope Thoracic injuries are common and can be life threatening In ESH we usually see blunt chest trauma
Abdomen and Genitalia Injuries. Chapter 28
 Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
TEACHING BASIC LIFE SUPPORT (& ALS)
") TEACHING BASIC LIFE SUPPORT (& ALS) Anton Koželj, R.N., B. Sc., lecturer Faculty of Health Sciences, University of Maribor Žitna ulica 15, 2000 Maribor, Slovenia Fact s To know-how to perform basic life
TEACHING BASIC LIFE SUPPORT (& ALS) Anton Koželj, R.N., B. Sc., lecturer Faculty of Health Sciences, University of Maribor Žitna ulica 15, 2000 Maribor, Slovenia Fact s To know-how to perform basic life
Aviation Rescue Swimmer Course
 Aviation Rescue Swimmer Course Primary Survey LT 5.4 December 2003 1 Objectives List the procedures used in a primary survey. Demonstrate primary survey procedures used in a mock trauma (moulage) scenario
Aviation Rescue Swimmer Course Primary Survey LT 5.4 December 2003 1 Objectives List the procedures used in a primary survey. Demonstrate primary survey procedures used in a mock trauma (moulage) scenario
PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT
 PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT Board Approved June 2007 Revised December 2009 Revised July 2011 Revised June 2015 435 Hunter Street Fredericksburg, VA 22401
PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT Board Approved June 2007 Revised December 2009 Revised July 2011 Revised June 2015 435 Hunter Street Fredericksburg, VA 22401
Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH
 Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH Intended learning outcomes Describe the components of a comprehensive clinician
Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH Intended learning outcomes Describe the components of a comprehensive clinician
Emergency First Response (EFR) Skills Assessment Sheets V4 June 2017
 Skills Assessment Sheets V4 June 2017") Emergency First Response () Skills Assessment Sheets V4 June 2017 Airway management & ventilation Airway management & ventilation Trauma jaw thrust 1 Hand positions 2 Perform jaw thrust / mouth open 3
Emergency First Response () Skills Assessment Sheets V4 June 2017 Airway management & ventilation Airway management & ventilation Trauma jaw thrust 1 Hand positions 2 Perform jaw thrust / mouth open 3
OUTLINE SHEET 5.4 PRIMARY SURVEY
 ENABLING OBJECTIVES: 4.7 List the procedures used in a primary survey. 4.8 Demonstrate primary survey procedures used in a mock trauma (moulage) scenario without injury to personnel or damage to equipment.
ENABLING OBJECTIVES: 4.7 List the procedures used in a primary survey. 4.8 Demonstrate primary survey procedures used in a mock trauma (moulage) scenario without injury to personnel or damage to equipment.
Initial Pelvic Fracture Management. Patrick M Reilly MD FACS February 27, 2010
 Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
Face and Throat Injuries. Chapter 26
 Face and Throat Injuries Chapter 26 Anatomy of the Head Landmarks of the Neck Injuries to the Face Injuries around the face can lead to upper airway obstructions. Bleeding from the face can be profuse.
Face and Throat Injuries Chapter 26 Anatomy of the Head Landmarks of the Neck Injuries to the Face Injuries around the face can lead to upper airway obstructions. Bleeding from the face can be profuse.
Hemorrhage Control. Chapter 6
 Chapter 6 The hemorrhage that take[s] place when a main artery is divided is usually so rapid and so copious that the wounded man dies before help can reach him. Colonel H. M. Gray, 1919 Stop the Bleeding!
Chapter 6 The hemorrhage that take[s] place when a main artery is divided is usually so rapid and so copious that the wounded man dies before help can reach him. Colonel H. M. Gray, 1919 Stop the Bleeding!
NOTE If it is necessary to perform abdominal thrusts, expose the abdominal area prior to pressing on the abdomen.
 ENABLING OBJECTIVES: 4.7 List the procedures used in a primary survey. 4.8 Demonstrate primary survey procedures used in a mock trauma (moulage) scenario without injury to personnel or damage to equipment.
ENABLING OBJECTIVES: 4.7 List the procedures used in a primary survey. 4.8 Demonstrate primary survey procedures used in a mock trauma (moulage) scenario without injury to personnel or damage to equipment.
It s as easy as ABC. Dr Andrew Smith
 It s as easy as ABC Dr Andrew Smith ABCDE A simple method to apply to your assessment of patients. It is a good failsafe in all situations i.e. At an end of an OSCE when you re put under pressure! Correct
It s as easy as ABC Dr Andrew Smith ABCDE A simple method to apply to your assessment of patients. It is a good failsafe in all situations i.e. At an end of an OSCE when you re put under pressure! Correct
ACUTE CLINICAL MANAGEMENT OF TRAUMA Tina Gaarder, MD, PhD
 ACUTE CLINICAL MANAGEMENT OF TRAUMA Tina Gaarder, MD, PhD Trauma represents a leading cause of disability and preventable death and is mainly affecting people between 15 and 40 years of age, accounting
ACUTE CLINICAL MANAGEMENT OF TRAUMA Tina Gaarder, MD, PhD Trauma represents a leading cause of disability and preventable death and is mainly affecting people between 15 and 40 years of age, accounting
Injuries to the Head and Spine
 Injuries to the Head and Spine Anatomy Review Skull Protects the brain Made up of several bones with seam like sutures Regions of the scalp-frontal, occipital, parietal, temporal Bones of face Orbits Mandible
Injuries to the Head and Spine Anatomy Review Skull Protects the brain Made up of several bones with seam like sutures Regions of the scalp-frontal, occipital, parietal, temporal Bones of face Orbits Mandible
EMT. Chapter 8 Review
 EMT Chapter 8 Review 1. During the scene size-up, you should routinely determine all of the following, EXCEPT: A. the mechanism of injury or nature of illness. B. the ratio of pediatric patients to adult
EMT Chapter 8 Review 1. During the scene size-up, you should routinely determine all of the following, EXCEPT: A. the mechanism of injury or nature of illness. B. the ratio of pediatric patients to adult
Algorithms for managing the common trauma patient
 ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
Trauma Registry Documentation December 16, 2014
 Trauma Registry Documentation December 16, 2014 The State of Florida now requires ALL Acute Care hospitals to submit data to the statetrauma Registry. Although Baptist Health hospitals are NOT Trauma Centers
Trauma Registry Documentation December 16, 2014 The State of Florida now requires ALL Acute Care hospitals to submit data to the statetrauma Registry. Although Baptist Health hospitals are NOT Trauma Centers
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours
 Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #3 Penetrating Neck Trauma
 McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #3 Penetrating Neck Trauma Penetrating neck injury (PNI) comprises 5 to 10 percent of traumatic injuries
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #3 Penetrating Neck Trauma Penetrating neck injury (PNI) comprises 5 to 10 percent of traumatic injuries
Fractures of the Thoracic and Lumbar Spine
 A spinal fracture is a serious injury. Nader M. Hebela, MD Fellow of the American Academy of Orthopaedic Surgeons http://orthodoc.aaos.org/hebela Cleveland Clinic Abu Dhabi Cleveland Clinic Abu Dhabi Neurological
A spinal fracture is a serious injury. Nader M. Hebela, MD Fellow of the American Academy of Orthopaedic Surgeons http://orthodoc.aaos.org/hebela Cleveland Clinic Abu Dhabi Cleveland Clinic Abu Dhabi Neurological
Injuries to the Head and Spine From Bradys Emergency Care 10 th Edition
 Injuries to the Head and Spine From Bradys Emergency Care 10 th Edition 1. When performing the four-rescuer log roll, which responder pulls the board into position? A.) Head B.) Waist C.) Knee D.) Shoulder
Injuries to the Head and Spine From Bradys Emergency Care 10 th Edition 1. When performing the four-rescuer log roll, which responder pulls the board into position? A.) Head B.) Waist C.) Knee D.) Shoulder
-Cardiogenic: shock state resulting from impairment or failure of myocardium
 Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Oral and Maxillofacial Surgeons and the seriously injured patient. Barts and The London NHS Trust
 Oral and Maxillofacial Surgeons and the seriously injured patient Barts and The London NHS Trust How do you assess this? Primary Survey A B C D E Airway & Cervical Spine Breathing & Ventilation Circulation
Oral and Maxillofacial Surgeons and the seriously injured patient Barts and The London NHS Trust How do you assess this? Primary Survey A B C D E Airway & Cervical Spine Breathing & Ventilation Circulation
SHOCK AETIOLOGY OF SHOCK (1) Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function
 Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function") SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
Shock and Trauma Resuscitation
 Shock and Trauma Resuscitation Bonjo Batoon, MS, CRNA Bbatoon@som.umaryland.edu Disclaimer Resuscitation is continuously evolving There is no one right way Knowing is half the battle G.I. Joe Having to
Shock and Trauma Resuscitation Bonjo Batoon, MS, CRNA Bbatoon@som.umaryland.edu Disclaimer Resuscitation is continuously evolving There is no one right way Knowing is half the battle G.I. Joe Having to
Injuries to the head and spine
 Injuries to the head and spine Aaron J. Katz, AEMT-P, CIC www.es26medic.net 2013 Nervous System Two sub-systems Central Nervous System ( CNS ) Brain and spinal cord Peripheral Nervous System 12 cranial
Injuries to the head and spine Aaron J. Katz, AEMT-P, CIC www.es26medic.net 2013 Nervous System Two sub-systems Central Nervous System ( CNS ) Brain and spinal cord Peripheral Nervous System 12 cranial
5/2/2018. Notice. Putting Humpty Dumpty Back Together Again
 Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
Evaluation & Management of Penetrating Wounds to the NECK
 Evaluation & Management of Penetrating Wounds to the NECK Goal Effectively identify patients with a high probability of injury requiring surgical intervention Define the role of diagnostic tests in assessing
Evaluation & Management of Penetrating Wounds to the NECK Goal Effectively identify patients with a high probability of injury requiring surgical intervention Define the role of diagnostic tests in assessing
ADC ED/TRAUMA POLICY AND PROCEDURE Policy 270
 Section: ADC Trauma ADC ED/TRAUMA POLICY AND PROCEDURE Policy 270 Subject: Pediatric Trauma Resuscitation Protocol Trauma Coordinator UTMB respects the diverse culture needs, preferences, and expectations
Section: ADC Trauma ADC ED/TRAUMA POLICY AND PROCEDURE Policy 270 Subject: Pediatric Trauma Resuscitation Protocol Trauma Coordinator UTMB respects the diverse culture needs, preferences, and expectations
Emergency Care Progress Log
 Emergency Care Progress Log For further details on the National Occupational Competencies for EMRs, please visit www.paramedic.ca. Check off each skill once successfully demonstrated the Instructor. All
Emergency Care Progress Log For further details on the National Occupational Competencies for EMRs, please visit www.paramedic.ca. Check off each skill once successfully demonstrated the Instructor. All
Caring for Muscle and Bone Injuries From Brady s First Responder (8 th Edition) 54 Questions
 54 Questions") Caring for Muscle and Bone Injuries From Brady s First Responder (8 th Edition) 54 Questions 1. What is caused by overexerting or tearing of a muscle? p. 375 A.) Dislocation B.) Sprain C.) Fracture *D.)
Caring for Muscle and Bone Injuries From Brady s First Responder (8 th Edition) 54 Questions 1. What is caused by overexerting or tearing of a muscle? p. 375 A.) Dislocation B.) Sprain C.) Fracture *D.)
Lesson Plans and Objectives: Review material for article Prep work for article Picture recovery Review for placement on-line.
 Lesson Plans and Objectives: Review material for article Prep work for article Picture recovery Review for placement on-line. After reading the article, the staff will be able to: Define facial trauma
Lesson Plans and Objectives: Review material for article Prep work for article Picture recovery Review for placement on-line. After reading the article, the staff will be able to: Define facial trauma
Emergency Medical Training Services Emergency Medical Technician Basic Program Outlines Outline Topic: Shock Revised: 11/2013
 Emergency Medical Training Services Emergency Medical Technician Basic Program Outlines Outline Topic: Shock Revised: 11/2013 DEFINITIONS Aerobic metabolism is energy using oxygen into cells. Anaerobic
Emergency Medical Training Services Emergency Medical Technician Basic Program Outlines Outline Topic: Shock Revised: 11/2013 DEFINITIONS Aerobic metabolism is energy using oxygen into cells. Anaerobic
Damage Control Resuscitation. VGH Trauma Rounds 2018 Harvey Hawes
 Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
Chapter 32. Objectives. Objectives 01/09/2013. Spinal Column and Spinal Cord Trauma
 Chapter 32 Spinal Column and Spinal Cord Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1.
Chapter 32 Spinal Column and Spinal Cord Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1.
EMT. Chapter 10 Review
 EMT Chapter 10 Review 1. The term shock is MOST accurately defined as: A. a decreased supply of oxygen to the brain. B. cardiovascular collapse leading to inadequate perfusion. C. decreased circulation
EMT Chapter 10 Review 1. The term shock is MOST accurately defined as: A. a decreased supply of oxygen to the brain. B. cardiovascular collapse leading to inadequate perfusion. C. decreased circulation