Ring 18 04/2017. Mosaicism (N=30) No mosaicism 53% Ring18/ monosomy 18 27% Ring 18/ der 18 13% Ring 18/ nl 18 3% Ring 18/ nl 18/ mono 18 3%
|
|
|
- Gervais Ray
- 5 years ago
- Views:
Transcription


1 04/2017 Ring 18 Mosaicism (N=30) No mosaicism 53% Ring18/ monosomy 18 27% Ring 18/ der 18 13% Ring 18/ nl 18 3% Ring 18/ nl 18/ mono 18 3% % GH deficiency 93 Hypotonia 92 Hearing Loss 80 Chronic otitis media 74 Microcephaly 70 Reflux 68 Respiratory difficulties 67 Hyperopia 67 Feeding difficulties 61 Constipation 58 Narrow ear canals 50 Strabismus 47 Hypothyroid 41 pulmonary stenosis 38 Ptosis 38 Jaundice 37 % Scoliosis/kyphosis 31 G or NG tube/ dysphagia 30 Seizures 26 Atrial septal defect 25 Nystagmus 20 Cleft palate 19 patent foramen ovale 17 Metatarsus aductus 13 Asthma 13 patent ductus arteriosus 12 Vertical talus 10 Bifid uvula 10 Club feet 9 Astigmatism 8 Pes cavus 7 Overlapping toes 7 Pectus excavatum 4
2 Behavior : Adults (BASC-2) n=5 Common problem: Evading others to avoid social contact 60% No problems identified Hostile threatening behaviors Anti-social and rule-breaking behaviors Social Impairment (SRS-2) (ages ) n=12 Common problems: Picking up social cues 92% Interpreting social cues 83% Social communication 83% Motivated to engage in social behavior 67% Repetitive behaviors / obsessing same routines 58% Social Impairment (SRS-2) (adults) n=5 Common problems: Interpreting social cues 80% Repetitive behaviors /obsessing same routines 60% Natural History (>age 18) n=7 Living Situation: Home with parents 4 With parents in independent area 2 Unknown 1 Highest Educational Level: Attending High School 1 High School Graduate (diploma) 1 Currently attends college 1 Vocational School (certificate/degree) 1 Some College/University (no degree) 1 Marital Status/Children Married (no) 5 Married (unknown) 2 Children (none) 5 Children (unknown) 2 Work (Volunteer, Part-time, Full-time): Yes 3 No 2 Less common problems: Picking up social cues 20% Executive Functioning: Adults (BRIEF-A) n=5 : Keeping track of own problem solving successes or failure 60% Managing current and future oriented tasks 60% Less common problems Acting on an impulse 20% Understanding their effect on others 20% Begin a task independently 20% Keep work and living spaces orderly and organized 20%
3 Ring 18: Current Ages & Age at Death Deceased Current Age Age in Years Age deceased Gender Cause of death Past medical history 4 years 5 months 5 years 1 month 5 years 8 months F F F Lung failure Had been vomiting prior to death. No acute cause of death. Had not been ill for the last 9 months Congenital heart disease; chronic lung disease; congestive heart failure ASD; seizures; cerebellar stroke; coloboma of Iris; spastic quadriparesis; pulmonary hypertension; respiratory insufficiency; obstructive sleep apnea; aspiration pneumonia; GERD; asthma Hydrocephalus; severe hypotonia; poor cough reflex with hypoventilation; used to have heart failure Complex congenital heart disease; history of seizures; cleft palate; G tube and fundoplication; partial agenesis of corpus callosum; chronic lung disease; tendency for hypoglycemia; optic atrophy

4 18q 04/2017
5 Proximal 18q No recognizable facial features Mild global developmental delay Normal birth weight Poor muscle tone Normal growth More severe expressive language delay 2 with larger deletions had hearing loss 18q- Natural History 4 individuals age 18 and over Living Situation: Live with their parents/guardians 2 Martial Status/Children: Never married 2 No children 2 Work (Volunteer, Part-time, Full-time): Yes 1 No 1 Behavior- Adults (BASC-2) n=2 Performing basic tasks safely 100% Overly active, acting without thinking 100% Odd behaviors 100% Antisocial & rule breaking behaviors 100% Inability to adapt to change 100% No Problems Avoiding social contact 0% Interacting with peers 0% Ability to work for a common goal 0% Highest educational level: Did Not Complete High School 1 High School Graduate (certificate) 1 Social Impairment Ages (SRS-2) n=4 Repeating behaviors /obsessing over routines 100% Expressing social communication 100% Interpreting Social Cues 75% Motivation to Engage in Social Behavior 75% Inability to pick up on social cues 50% Social Impairment - Adults (SRS-2) n=2 Interpreting social cues 100% Repeating behaviors /obsessing over the routines 100% Inability to pick up on social cues 100% No problems Motivation to engage in social behavior 0% Executive Functioning in Adults (BRIEF A) n=2 Keeping track of problem solving successes or failures 100% Remembering information in order to complete a task 100% Move from one situation to another 100% Beginning tasks 100% Managing current & future oriented tasks 100% Inhibiting behavior or not act on an impulse 100% Understand the effect of behaviors on others 100% Keeping work & living spaces orderly 100% Modulating emotional response 100%
6 Adults with Proximal 18q Potential conditions in a neonate Structural Palate abnormality Functional Respiratory difficulties Feeding difficulties Central apnea Hypotonia Biochemical Jaundice Initial evaluations Cardiology evaluation 50% have cardiac defects Hearing evaluation 30% with hearing deficits Renal ultrasound 43% with reflux Vision evaluation 64% with optic problems MRI 62% abnormal findings Referrals to Appropriate subspecialist as indicated by initial evaluations Genetics Follow up Parents genotyped for balanced rearrangements Early intervention/developmental services The Chromosome 18 Registry & Research Society The Chromosome 18 Clinical Research Center Closely monitor and manage Failure to thrive/ growth failure Weight gain Linear growth Sinus/ ear infections Genitourinary: Reflux Gastrointestinal Immunology/Rheumatology: Atopic disorders Orthopedics Scoliosis Respiratory issues Neurology: Seizure disorder Tremors hypotonia Development: Milestones Speech delay School performance Behavioral/ mood changes Annual Screenings Vision Hearing
7 Distal18q with TCF4 deletion 18q- Natural History 13 individuals age 18 and over Living Situation: Live with their parents/guardians 8 Group home 3 Martial Status/Children: Never married 11 No children 11 Work (Volunteer, Part-time, Full-time): Yes 1 No 10 Highest educational level: Did Not Complete High School 4 Attending high school 2 High School Graduate (certificate) 5 Behavior- Adults (BASC-2) n=9 Performing basic tasks safely 100% Expressing ideas in a way understood by others 100% Interacting with peers 100% Less Nervous, fearful and worrisome tendencies 11% Acting in a hostile, threatening manner 11% Incapacitating sadness or stress 11% Behaving overly sensitive about minor problems 11% Social Impairment - Adults (SRS-2) n=6 Expressing social communication 100% Interpreting social cues 100% Inability to pick up on social cues 100% Motivation to engage in social behavior 100% Repeating behaviors /obsessing over the routines 83% Social Impairment Ages (SRS-2) n=18 Interpreting social cues 100% Expressing social communication 100% Repeating behaviors /obsessing over routines 89% Inability to pick up on social cues 83% Motivation to engage in social behavior 50% Executive Functioning in Adults (BRIEF A) n=8 Remembering information in order to complete a task 50% Modulating emotional response 50% Least Move from one situation to another 25% Beginning tasks 25% Inhibiting behavior or not act on an impulse 25% Understand the effect of behaviors on others 25% Keeping work & living spaces orderly 25% Keeping track of problem solving successes or failures 25%
8 Distal18q with TCF4 deletion Main features of a TCF4 deletion TCF4 +/ (N=28) TCF4 +/+ (N=9) Average age Age range verbal No Yes Overall IQ 4 mo. (2 11mo) 54 (50 82) corpus callosum abn. 68% 0% hyperventilation 39% 33% Autism 71% 38% TCF4 Projects: Skin cells > ips cells > neurons Gene expression differences Drug testing Biomarker identification TCF4 +/ = people with 18q deletions that include the TCF4 gene. TCF4 +/+ = people with terminal deletions of 18q deletions close to but not including the TCF4 gene. Effects of growth hormone treatment Reanalysis of data from 2005 paper B Mental Age (Months) Change in mental age score of 3 children with TCF4 deletions before and after GH treatment Chronologic Age (Months) Effect of Childhood GH treatment in adults with 18q- Adults with 18q- who are: GH deficient Treated with GH from childhood Remained GH deficient BMI Height Cognitive flexibility Problem solving Frustration control



9 Distal 18q Reference Group Distal 18q Reference Group Medical and Developmental History n=14 Feature % Feature % Motor Developmental delay 100 Congenital heart abn. 54 Delayed myelination 100 Allergic rhinitis 50 Hypotonia 93 Sinusitis 50 Foot anomalies 86 Eczema 44 Atretic/stenotic ear canals 77 Intention tremors 42 Neonatal complications 77 Strabismus 38 Growth hormone deficiency 71 Pneumonia 36 Hearing loss 71 Scoliosis 33 Recurrent ear infections 69 IgA deficiency 33 Hypospadias (2/3 boys) 67 Umbilical hernia 33 Complication during pregnancy 67 Autoimmune disorders 31 Tapered fingers 64 Thyroid abnormality 31 Flat midface 60 Constipation 29 Proximal thumbs 57 Kidney malformations 25 Palate abnormality 57 Hyper flexibility of joints 21 Food/ drug allergies 56 Seizures 20 Gastro-esophageal reflux 56 Developmental Milestones = Average score = the full range of scores = the normal range Behavioral Measures IQ = normal IQ range = average IQ score = mild ID range = severe to profound = Average score = the full range of scores = normal range = at risk range = problem range
10 Distal 18q (all) Management Guide Potential conditions in a neonate Structural Hernias (inguinal, umbilical) Cryptorchidism, chordee, and hypospadias in >50% of males Palate abnormality Functional Respiratory and feeding difficulties Hypotonia Biochemical Jaundice Initial evaluations after diagnosis Cardiology evaluation 29% have cardiac defects Orthopedic exam 74% with foot defects Otolaryngology including audiology evaluation >50% with hearing loss Thyroid levels 15% with hypothyroidism Renal ultrasound 18% with reflux or malformations Ophthalmology exam 72% with optic problems Genitourinary Neurology / cerebral MRI evaluation Pediatric anesthesiology if surgery is indicated Referrals to Appropriate subspecialist as indicated by initial evaluations Genetics Follow up Parents genotyped for balanced rearrangements Early intervention/developmental services The Chromosome 18 Registry & Research Society The Chromosome 18 Clinical Research Center Closely monitor and manage Failure to thrive/ growth failure Weight gain Linear growth Sinus/ ear infections Genitourinary Reflux Immunology/Rheumatology IgA deficiency Atopic disorders Arthritis Other autoimmune conditions Neurology Seizure disorder Intention tremors Hypotonia Orthopedics Scoliosis or kyphosis Development Milestones School performance Behavioral/ mood changes Annual Screenings Thyroid Vision Hearing
11 Distal 18q (with deletion not including TCF4) 18q- Natural History 104 individuals age 18 and over Living Situation: Live with their parents/guardians 60 With parents in independent area 3 Spouse/partner 5 Independent 5 Supervised independent living program 3 Group Home / Host / Extended Family 8 With roommate 3 Dormitory 1 Unknown 16 Martial Status/Children: Never married 78 Married 4 2 No live births 1 One live birth 3 Three live births 1 No children 77 2 Work (Volunteer, Part-time, Full-time): Yes 48 No 36 0 Highest educational level: Did Not Complete High School 6 Attending High School 6 High School Graduate (certificate) 18 High School Graduate (diploma) 29 High School Graduate (unknown) 3 Attending College/University 9 Some Vocational School (no degree) 1 Some College/University (no degree) 6 Associate Degree 1 Bachelor Degree 2 Master Degree 1 Vocational School Degree/Certificate 5 Unknown 17 Behavior- Adults (BASC-2) n=70 Performing basic tasks safely 46% Avoiding social contact 46% Ability to work for a common goal 39% Expressing ideas in a way understood by others 30% Odd Behaviors 30% Least Nervous, fearful and worrisome tendencies 17% Anti-social and rule-breaking behaviors 11% Distractible unable to concentrate 10% Social Impairment - Adults (SRS-2) n=61 Interpreting social cues 70% Repeating behaviors /obsessing over the routines 67% Expressing social communication 62% Motivation to engage in social behavior 54% Inability to pick up on social cues 51% Social Impairment Ages (SRS-2) n=59 Repeating behaviors /obsessing over routines 81% Interpreting social cues 78% Expressing social communication 73% Inability to pick up on social cues 64% Motivation to engage in social behavior 56% Executive Functioning in Adults (BRIEF A) n=78 Keeping track of problem solving successes or failures 62% Move from one situation to another 56% Remembering information in order to complete a task 54% Managing current & future oriented tasks 54% Least Keeping work & living spaces orderly 29% Inhibiting behavior or not act on an impulse 28%
12 18q : Current Ages & Age at Death Proximal 8% Complex TCF4 +/ Distal 32% 35% 5% Proximal 18q Age in years Age deceased Gender Cause of death Past medical history 11 years 7 months M Seizure complications At 5 months parents report that he has never breathed normally; spastic cerebral palsy; dysphagia-g-tube; Nissen fundoplication; epilepsy; pneumonia several times/aspirating; obstructive apnea; allergic to mold, morphine and codeine; hiatal hernia Complex Rearrangements Age deceased Gender Cause of death Past medical history 15 months F N/A 2 years 6 months M 13 years 3 months M Heart complications after heart surgery N/A 16 yrs 3 months M Kidney and heart failure 23 years M Complications after bowel obstruction surgery. Multiple congenital heart defects; G-tube; hernia repair; intestine malrotations; hydrocephalus; pallor optic nerves; severe sleep apnea Multiple heart surgeries; malrotated bowel; hypothyroidism; reactive airway disease Central hypotonia; 2 yrs 4 months: hypertonia; bilateral hearing loss; severe developmental delay; renal reflux; feeding difficulties; G-tube; aspiration Profound developmental delay; sleep disorder; staring spells; mitral and aortic valve insufficiency; bilateral hypoplastic kidneys; chronic renal insufficiency Neonatal complications; ASD; tricuspid insufficiency ; pulmonary valve stenosis; pneumonia several times; seizures; kidney stone; tracheomalacia; significant pulmonary disease 31 years F N/A No medical records available 45 years F Choking due to a recurrent habit of retaining food in her cheeks No medical records available
13 Distal 18q, TCF4 +/ Age deceased 22 mo F 6 rs 10 mo M Gender Cause of death Past medical history Admitted to the Hospital for central apnea. Developed tachycardia Aspiration ( at the time of death had cold/congestion). Admitted to the Hospital for not breathing. Cause of death : aspiration 8 yr M Sepsis 13 yr M 13 yr 3 mo F Sepsis (developed an infection on his liver which was not able to to be controlled and spread to other organs) Very unexpectedly and suddenly. Fell ill what appeared a cold, got antibiotics, After two days, when mother went to check on her in the morning found her struggling to breath, Emergency help, but she passed away. Post mortem findings: Intussusception. 16 yr 3 mo F N/A Respiratory distress;central apnea; respiratory tract infections very often; silent aspirations; failure to thrive; oropharyngeal dysphagia Reactive airway disease; pneumonia; dehydration; diarrhea; ASD which was closed spontaneously Never walked, talked or sit; poor immune system; developed interstitial lung disease and asthma; apnea; obstructed bowels; aspiration secondary to GERD; ASD; seizures; corneal staphyloma (Right) Immature lung development as a newborn; cortical blindness; pneumonia very often; silent aspirations; central apnea Only few medical records available: often respiratory infections; hypoplastic corpus callosum; Bronchitis always turned into bronchial pneumonia', at about 3 x a year; one lung functions only at 10% due to scarred tissues from pneumonia; asthma 16 yr 5 mo M Sudden death 17 yr 8 mo M 20 yr 11 mo F Was taking a nap and did not wake up. The cause of death was considered "natural causes". Death certificate:" cardiac arrest". Vomiting; poor feeding tolerance; Worsening apneic episodes; Adynamic illeus 22 yr F N/A 31 yr 8 mo M N/A Pneumonia many times; history of asthma; glaucoma in the left eye; transplant surgery in the left eye Had fluid in his lungs at birth, and required O2 for 4 days; abnormal tone and meconium stained amniotic fluid; IUGR; hypospadias and chordee; no medical records available after 3 months of age Recurrent aspiration pneumonia; central apnea; Irregular breathing cycles; history of cyclical vomiting; GE reflux; constipation; malrotation of intestine; pulmonary stenosis Pneumonia in multiple times; asthma; alopecia totalis; fused kidneys; trouble with swallowing and controlling secretions Seizures; pyloric stenosis; salivary gland surgery; orchiectomy; has had 3 pancreatitis/vomiting attacks; nonverbal, on wheelchair Distal 18q, TCF4 +/+ Age deceased Gender Cause of death Past medical history 8 yr 4 m F N/A 9 yr 4 m M Pulmonary hemorrhage per grandmother 10 yr 3 mo F N/A 12 years 9 m M N/A Pneumonia newborn; PDA (patent ductus arteriosus); PFO (patent foramen ovale); failure to thrive; congenital hypothyroidism; cleft palate; bifid thumb; club feet; slightly alrotated right kidney; records only as an infant. Nonverbal; nonambulatory; G-J tube for severe GERD; severe encephalopathy; seizure disorder; severe hypertonicity; spastic quadriparesis idiopathic pulmonary hemosiderosis; frequent pneumonias; respiratory distress; sinus arrythmia; minimal mitral regurgitation; several hospitalizations for pulmonary bleeding Records only at a very young age (2 yrs old): neonate: periodic breathing; episodes of apnea; pyloric stenosis; cleft palate; silent aspirations; jejunostomy tube; oropharyngeal dysmotility History of heart murmur-resolved; pulmonary valve stenosis-resolved? ; 19 yr 9 mo M Sudden death dysarthria; MRI: Chiari I malformation 20 yr 3 mo F Deep vein thrombosis then pulmonary Acquired hypothyroidism; hearing loss; records available up to 13 yrs old. embolism? Actual report n/a Only few records available 20 yr 6 mo F N/A History of gastroenteritis; failure to thrive ( records available only as a toddler) 25 yr 6 mo F N/A Failure to thrive; bilateral aural atresia; cleft palate; significant developmental delay; records available only until 7 years old Meningitis at 9 months old; asthma at 12 yrs old and lasted for about 8 yrs; 31 yr6 mo F Sudden, unstoppable epileptic event mitral insufficiency; history of seizures as a young adult: onset at 5 yrs old; periventricular leukomalacia ( MRI) 49 yr 8 m F N/A Torticollis; probable scoliosis; tremors starting at the age of 4 years old, and getting worse over the years; hearing loss; cerebral atrophy (MRI)


14 18p 04/ p deletions 18p Critical Regions
15 18p (cen) Newborn Physical Findings (N=31) Neonatal complications 74% Feeding Difficulties 42% Respiratory Difficulties 29% Jaundice 29% Hypoglycemia 10% Muscle tone abnormalities 84% Hypotonia 71% Mix abnormal tone 13% Immediate Referral Early Childhood Developmental services (OT, PT, ST) - Developmental delay 100% Genetics evaluation and counseling - Parental chromosome analysis or FISH Ophthalmology evaluation Strabismus 2% Optic nerve abnormalities 13% Congenital cataracts 6% Refractive Errors 52% Astigmatism 29% Hyperopia 32% Myopia 13% Initial Physical evaluation for: Cardiac Abnormalities 29% Holoprosencephaly findings 13% Single central incisor 10% Septo-optic dysplasia 3% Pectus Excavatum 29% Hernia (Inguinal, hiatal, umbilical) 29% Monitor and Refer Seizures 16% Nystagmus 6% Kyphosis/ Scoliosis 19% Reflux 13% Consipation 32% Growth hormone deficiency 35% Panhypotitutarism 6% Thyroid abnormalities 16% Hearing loss 22% Recurrent ear infections 61% Findings reported in more than 25% of this population include: Muscle tone abnormalities 88% Transient neonatal complications 63% Chronic otitis media 56% Refractive errors 53% Findings on the holoprosencephaly spectrum 31% Constipation 31% Strabismus 31% Cardiac anomalies 25% Growth hormone deficiency 25% Other less common findings include seizures, scoliosis, pectus excavatum, ptosis, hearing loss, and thyroid abnormalities.
16 Deletion of entire short arm of 18p Behavior in 18p-(cen) Adults (BASC-2) n=15 : Poor social skills 40% Avoiding social contact 40% No problems identified: Overly active and acting without thinking Engaging in anti-social and rule-breaking behaviors Incapacitating sadness or stress Easily distractible and unable to concentrate Deletion of part of the short arm of 18p Behavior in 18p-(non-centromere) Adults (BASC-2) n=17 Common problems: Inability to adapt readily to changes 53% Inability to work with others for a common goal 50% Less common problems Nervous, fearful and worrisome tendencies 18% Easily distractible and unable to concentrate 12% Hostile and threatening behavior 6% Anti-social and rule-breaking behaviors 6% Executive Functioning in 18 p-(cen) Adults (BRIEF-A) n=16 : Moving from one situation to another 69% Keeping track problem solving successes/failures 50% No problems identified: Inability to inhibit, resist, or not act on an impulse Executive Functioning in 18 p-(noncentromere) Adults (BRIEF-A) n=16 Common problems: Tracking of problem solving successes/failures 75% Moving from one situation to another 75% Keeping work and living spaces orderly 63% Managing current and future oriented tasks 56% Remembering information to complete a task 56% Beginning a task or independently generate ideas 50% Modulating emotional response 50% Less common problems: The inability to inhibit, resist, or not act on impulse 19% Social Impairment in 18p- (cen) individuals Adults n=17 (SRS-2) Picking up on social cues 54% Repeating behaviors/ obsessing same routines 53% Expressing social communication 53% Less common problems: Interpreting social cues once they are picked up 47% Motivation to engage in social behavior 35% Social Impairment in 18p- (cen) individuals years n=14 (SRS-2) Common problems: Obsessing over the same routines and rituals 86% Interpreting social cues 79% Motivated to engage in social behavior 71% Social communication 71% Picking up on social cues 71% Social Impairment in 18p- (non-centromere) individuals Adults n=15 (SRS-2) Common problems: Repeating behaviors and obsessing over routines 67% Interpreting social cues 67% Picking up on social cues 60% Social communication 60% Motivation to engage in social behavior 60% Social Impairment in 18p- (non-centromere) individuals years n=18 (SRS-2) Common problems: Obsessing over the same routines and rituals 78% Pick up on social cues 72% Interpret social cues 67% Social communication 61% Less Motivation to engage in social behavior 44%
17 18p- Natural History (>18 years) n=27 n=27 Living Situation: 18p-cen 18p-non-cen Live with their parents With parent in independent area 0 2 Supervised independent living program 0 2 Apartment alone 3 3 Group home 1 0 Unknown 8 5 Highest educational level: Did Not Complete High School 1 2 Attending High School 3 2 High School Graduate (certificate) 6 2 High School Graduate (diploma) 6 5 Attending College/University 1 2 Some College/University (no degree) 0 3 Associates Degree 2 4 Vocational School Degree/Certificate 0 2 Unknown 8 5 Martial Status/Children: Married (no) Married (unknown) 8 5 Separated / Divorced 0 1 Children (none) Children (unknown) 8 5 Work (Volunteer, Part-time, Full-time): Yes No 6 8 Unknown 8 5 Deceased 18p : Current Ages & Age at Death Current Age in years Age deceased Gender Cause of death Past medical history 13 years F Brain bleed post cardiac surgery 22 years 4 months F Pneumonia complicated by lupus Goldenhar syndrome; severe GE reflux; complex congenital heart disease Lupus nephritis; hypothyroid; adrenocorticotropic hormone deficiency



18 18p (cen) continued = Average score = the full range of scores = the normal range = normal IQ range = average IQ score = mild ID range = severe to profound = Average score = the full range of scores = normal range = at risk range = problem range
19 Chromosome 18p Dosage Sensitive Genes (66 genes in total on 18p) 1 1,000,000 CETN1 SMCHD1 EMILIN2 TGIF DLGAP1 CETN1 = Male infertility Our data: None evaluated 0/22 adult males are fathers SMCHD1 = FSH Dystrophy 2 Digeneic DUX4 2 nd gene (small array, A allele) Age of onset before age 20 Progressive muscle weakness (asymmetric); shoulders upper arms, lower leg Our data: 0/21 affected (8-30 years old; ave. age 18) 2/83 genetically at risk EMILIN2 -?? Or any of 20 genes Our data: 11 18p- = poor platelet function & 8 Tet18p = normal platelet function TGIF = Holoprosencephaly Our data: 6/65 (single central incisor, iris coloboma, piuitary abn.) LAMA1 LCCR30 ANKRD12 LAMA1 = Tortuous Retinal Vasculature and keratosis pilaris Our data: 1/32 had retinal vascular anomalies 7/79 keratosis pilaris - from chart review (common in typical population) GNAL = Dystonia (Muscle Cramps) Age of onset 31.3 yrs. Range 7-54 years Common effects = neck 82%, speech 92% Our data: neuro exam = 0/17 evaluated met criteria medical records = 2/58 had dystonia 10,000,000 IMPA2 GNAL AFG3L2 PTPN2 AFG3L2 = Spinalcerebellar ataxia 28 Age of onset 24 years Range 3-60 years Likelihood of diagnosis = 93% Slowly progressive gait & limb ataxia - incoordination 100% Dysarthria- motor speech problem with articulation 100% Our data: :0/15 met criteria (8-30 years old; ave. age 16) PTPN2 - Inflammatory bowel disease (IBD) Mice with only 1 copy of PTPN2 have increased susceptibility to inflammatory bowel disease (IBD) Genetic Studies: Our data: Crohn s Disease & Ulcerative Colitis Rheumatoid arthritis Type 1 Diabetes?? 0/67 have IBD 11/67 had an autoimmune condition (juvenile rheumatoid arthritis, Sjogrens syndrome, hypothyroidism, graves, celiac, vitiligo, psoriasis, and alopecia) hg19 Centromere DLGAP1, LCCR30. ANKRD12, IMPA2 = implicated in autism Our data: 8/56 clinically significant GARS scores
04/ p. 18p deletions. 18p Critical Regions
 18p 04/2017 18p deletions 18p Critical Regions 18p (cen) Newborn Physical Findings (N=31) Neonatal complications 74% Feeding Difficulties 42% Respiratory Difficulties 29% Jaundice 29% Hypoglycemia 10%
18p 04/2017 18p deletions 18p Critical Regions 18p (cen) Newborn Physical Findings (N=31) Neonatal complications 74% Feeding Difficulties 42% Respiratory Difficulties 29% Jaundice 29% Hypoglycemia 10%
Proximal 18q- Treatment and Surveillance ICD-10 = Q99.9 or Q93.89
 Proximal 18q- Treatment and Surveillance ICD-10 = Q99.9 or Q93.89 These recommendations are inclusive of the entire population of people with Proximal 18q deletions even though each person has a unique
Proximal 18q- Treatment and Surveillance ICD-10 = Q99.9 or Q93.89 These recommendations are inclusive of the entire population of people with Proximal 18q deletions even though each person has a unique
Tetrasomy 18p Treatment and Surveillance ICD-10 =Q93.2
 Tetrasomy 18p Treatment and Surveillance ICD-10 =Q93.2 These recommendations are inclusive of the entire population of people with Tetrasomy 18p. It should be noted that there is a great deal of variation
Tetrasomy 18p Treatment and Surveillance ICD-10 =Q93.2 These recommendations are inclusive of the entire population of people with Tetrasomy 18p. It should be noted that there is a great deal of variation
18p- Treatment and Surveillance ICD-10 = Q99.9 or Q93.89
 18p- Treatment and Surveillance ICD-10 = Q99.9 or Q93.89 These recommendations are inclusive of the entire population of people with 18p deletions. Even though about half of this group have deletions of
18p- Treatment and Surveillance ICD-10 = Q99.9 or Q93.89 These recommendations are inclusive of the entire population of people with 18p deletions. Even though about half of this group have deletions of
Distal 18q- Treatment and Surveillance ICD-10 = Q99.9 or Q93.89
 Distal 18q- Treatment and Surveillance ICD-10 = Q99.9 or Q93.89 These recommendations are inclusive of the entire population of people with Distal 18q deletions even though each person has a unique deletion.
Distal 18q- Treatment and Surveillance ICD-10 = Q99.9 or Q93.89 These recommendations are inclusive of the entire population of people with Distal 18q deletions even though each person has a unique deletion.
(i) Family 1. The male proband (1.III-1) from European descent was referred at
 Family 1. The male proband (1.III-1) from European descent was referred at") 1 Supplementary Note Clinical descriptions of families (i) Family 1. The male proband (1.III-1) from European descent was referred at age 14 because of scoliosis. He had normal development. Physical evaluation
1 Supplementary Note Clinical descriptions of families (i) Family 1. The male proband (1.III-1) from European descent was referred at age 14 because of scoliosis. He had normal development. Physical evaluation
Legal aspects in accidents and neglect.
 Al-Al Bayt University Princess Salma Faculty of Nursing Adult Health nursing Course Title :Child Health Nursing Course Number :1001341 Credit Hours :3 Pre requisite :1001222 Placement : Instructor:,, Course
Al-Al Bayt University Princess Salma Faculty of Nursing Adult Health nursing Course Title :Child Health Nursing Course Number :1001341 Credit Hours :3 Pre requisite :1001222 Placement : Instructor:,, Course
Salt Lake Orthopaedic Clinic Initial Visit Form
 Salt Lake Orthopaedic Clinic Initial Visit Form Name: Today s Date: Date of Birth: Age: Height: Weight: Handedness (R/L): Referring Physician: Primary Care Physician: Chief Complaint Why are you seeing
Salt Lake Orthopaedic Clinic Initial Visit Form Name: Today s Date: Date of Birth: Age: Height: Weight: Handedness (R/L): Referring Physician: Primary Care Physician: Chief Complaint Why are you seeing
Anna & John J. Sie Center for Down Syndrome Affiliates
 Anna & John J. Sie Center for Down Syndrome Affiliates Types of Medical Research Bench or basic research: done in a controlled laboratory setting using nonhuman subjects Clinical research: answer questions
Anna & John J. Sie Center for Down Syndrome Affiliates Types of Medical Research Bench or basic research: done in a controlled laboratory setting using nonhuman subjects Clinical research: answer questions
PAGE 1 NEURO-OPHTHALMIC QUESTIONNAIRE NAME: AGE: DATE OF EXAM: CHART #: (Office Use Only)
") PAGE 1 NEURO-OPHTHALMIC QUESTIONNAIRE NAME: AGE: DATE OF EXAM: CHART #: (Office Use Only) 1. What is the main problem that you are having? (If additional space is required, please use the back of this
PAGE 1 NEURO-OPHTHALMIC QUESTIONNAIRE NAME: AGE: DATE OF EXAM: CHART #: (Office Use Only) 1. What is the main problem that you are having? (If additional space is required, please use the back of this
NYEIS Version 4.3 (ICD) ICD - 10 Codes Available in NYEIS at time of version launch (9/23/2015)
 ICD - 10 Codes Available in NYEIS at time of version launch (9/23/2015)") D82.1 Di George's syndrome E63.9 Nutritional deficiency, unspecified E70.21 Tyrosinemia E70.29 Other disorders of tyrosine metabolism E70.30 Albinism, unspecified E70.5 Disorders of tryptophan metabolism
D82.1 Di George's syndrome E63.9 Nutritional deficiency, unspecified E70.21 Tyrosinemia E70.29 Other disorders of tyrosine metabolism E70.30 Albinism, unspecified E70.5 Disorders of tryptophan metabolism
Ring 18. Our Mission: To help individuals. they face so they might lead healthy, happy, and productive lives. Normal Chromosomes
 The Chromosome 18 Registry & Research Society Ring 18 There are five major conditions involving large changes of chromosome 18. Each of these conditions has a wide variety of characteristics. Additionally,
The Chromosome 18 Registry & Research Society Ring 18 There are five major conditions involving large changes of chromosome 18. Each of these conditions has a wide variety of characteristics. Additionally,
New Patient Questionnaire Pediatric Orthopaedic Surgery
 Page 1 of 5 New Patient Questionnaire Pediatric Orthopaedic Surgery First Name: Last Name: Middle: DOB: Height: Weight: Primary Care Physician/Pediatrician Name: Address: Phone Number: Chief Compliant
Page 1 of 5 New Patient Questionnaire Pediatric Orthopaedic Surgery First Name: Last Name: Middle: DOB: Height: Weight: Primary Care Physician/Pediatrician Name: Address: Phone Number: Chief Compliant
PEDIATRICS. Module Topic/Content Student Learning Outcomes Resources Clinical Assessment Activities Course/Clinical Outcomes
 PEDIATRICS N332 Outline 1 Welcome back: Instructor Role and Student Role Discuss course requirements. Explain personal learning style and study patterns. Explain critical thinking and clinical judgment
PEDIATRICS N332 Outline 1 Welcome back: Instructor Role and Student Role Discuss course requirements. Explain personal learning style and study patterns. Explain critical thinking and clinical judgment
PEDIATRIC MEDICAL HISTORY QUESTIONNAIRE
 Division of Otolaryngology Main Phone: 847 504-3300 Main Fax: 847 504-3305 Mihir Bhayani, MD Judy L. Chen, MD Mark E. Gerber, MD, FACS, FAAP Joseph Raviv, MD Ilana Seligman, MD, FACS, FAAP Michael J. Shinners,
Division of Otolaryngology Main Phone: 847 504-3300 Main Fax: 847 504-3305 Mihir Bhayani, MD Judy L. Chen, MD Mark E. Gerber, MD, FACS, FAAP Joseph Raviv, MD Ilana Seligman, MD, FACS, FAAP Michael J. Shinners,
Laser Vein Center Thomas Wright MD Page 1 of 4
 Demographics Laser Vein Center Thomas Wright MD Page 1 of 4 Patient Name: Address: City, St, Zip Primary Phone: Alternate: DOB: Social Security #: Insurance Information Primary Insurance ID# Group# Subscriber
Demographics Laser Vein Center Thomas Wright MD Page 1 of 4 Patient Name: Address: City, St, Zip Primary Phone: Alternate: DOB: Social Security #: Insurance Information Primary Insurance ID# Group# Subscriber
RHEUMATOLOGY PATIENT HISTORY FORM
 !! RAMOS RHEUMATOLOGY, PC RHEUMATOLOGY PATIENT HISTORY FORM Date: / / NAME: Birthdate: / / Last First M. I. Age: Sex: F M Marital status: Never married Married Divorced Separated Widowed Partnered/significant
!! RAMOS RHEUMATOLOGY, PC RHEUMATOLOGY PATIENT HISTORY FORM Date: / / NAME: Birthdate: / / Last First M. I. Age: Sex: F M Marital status: Never married Married Divorced Separated Widowed Partnered/significant
PLEASE LET US KNOW YOUR REASON FOR TODAY S VISIT : CURRENT MEDICATIONS (WITH DOSAGE) PLEASE INCLUDE VITAMINS AND HERBAL MEDICATIONS:
 PLEASE INCLUDE VITAMINS AND HERBAL MEDICATIONS:") 1 NAME: DATE OF BIRTH PLEASE LET US KNOW YOUR REASON FOR TODAY S VISIT : CURRENT MEDICATIONS (WITH DOSAGE) PLEASE INCLUDE VITAMINS AND HERBAL MEDICATIONS: PAST MEDICAL HISTORY (YOUR MEDICAL HISTORY) :
1 NAME: DATE OF BIRTH PLEASE LET US KNOW YOUR REASON FOR TODAY S VISIT : CURRENT MEDICATIONS (WITH DOSAGE) PLEASE INCLUDE VITAMINS AND HERBAL MEDICATIONS: PAST MEDICAL HISTORY (YOUR MEDICAL HISTORY) :
New Patient Information
 Geoffrey G Glidden MD PA New Patient Information Name Address City/State/Zip Cell Phone Home Phone DL# SSN# Age of Birth Sex: Male / Female Your employer Occupation Work Phone E-Mail Referring Physician
Geoffrey G Glidden MD PA New Patient Information Name Address City/State/Zip Cell Phone Home Phone DL# SSN# Age of Birth Sex: Male / Female Your employer Occupation Work Phone E-Mail Referring Physician
Single Married Divorced Widowed Male Female
 Annual Physical Form General Information Name Birth Date Phone Email Address Street Address City State Zip Marital Status Gender Single Married Divorced Widowed Male Female Employment Information Position
Annual Physical Form General Information Name Birth Date Phone Email Address Street Address City State Zip Marital Status Gender Single Married Divorced Widowed Male Female Employment Information Position
NEW PATIENT QUESTIONNAIRE For Dr Benoy Benny. Section 1: Today s Date: Date of Birth: Age:
 Baylor Physical Medicine and Rehabilitation NEW PATIENT QUESTIONNAIRE For Dr Benoy Benny Dear Patient: Please complete this questionnaire before you come for your appointment. Be sure to call us as soon
Baylor Physical Medicine and Rehabilitation NEW PATIENT QUESTIONNAIRE For Dr Benoy Benny Dear Patient: Please complete this questionnaire before you come for your appointment. Be sure to call us as soon
Premium Specialty: Pediatrics
 Premium Specialty: Pediatrics Credentialed Specialties include: Adolescent Medicine, Pediatric Adolescent, and Pediatrics This document is designed to be used in conjunction with the UnitedHealth Premium
Premium Specialty: Pediatrics Credentialed Specialties include: Adolescent Medicine, Pediatric Adolescent, and Pediatrics This document is designed to be used in conjunction with the UnitedHealth Premium
The 14 th International Fragile X Conference, Garden Grove, CA, Friday, July 18 th, 2014
 Presenters: Sharon Kidd, MPH, PhD; Ave Lachiewicz, MD; Deborah Barbouth, MD; Robin Blitz, MD; Carol Delahunty, MD; Dianne McBrien, MD; Elizabeth Berry-Kravis, MD, PhD The 14 th International Fragile X
Presenters: Sharon Kidd, MPH, PhD; Ave Lachiewicz, MD; Deborah Barbouth, MD; Robin Blitz, MD; Carol Delahunty, MD; Dianne McBrien, MD; Elizabeth Berry-Kravis, MD, PhD The 14 th International Fragile X
Patient Name: Date of Birth:
 Patient Name: Date of Birth: Marital Status: Single Married Divorced Widowed Height: Referring Doctor: Weight: Primary Care Dr.: Preferred Pharmacy:(name/address) ALLERGIES: Do you have any drug allergies?
Patient Name: Date of Birth: Marital Status: Single Married Divorced Widowed Height: Referring Doctor: Weight: Primary Care Dr.: Preferred Pharmacy:(name/address) ALLERGIES: Do you have any drug allergies?
Preferred language: PATIENT INFORMATION. Date of birth (dd/mm/yyyy): Age: Sex: Male Female. City: State: Country: Zip code:
: Age: Sex: Male Female. City: State: Country: Zip code:") ADULT INTAKE QUESTIONNAIRE Please fill out this form as completely as possible. This information will help us to better assess whether you are a good candidate for the program. Today s date (dd/mm/yyyy):
ADULT INTAKE QUESTIONNAIRE Please fill out this form as completely as possible. This information will help us to better assess whether you are a good candidate for the program. Today s date (dd/mm/yyyy):
ANY FAMILY HISTORY OF ANEURYSM OR DVT?
 NAME: D/O/B: DATE: MR# WHAT PROBLEM(S) BRINGS YOU HERE TODAY? WHO SENT YOU TO US? DOCTOR/OTHER WHICH DOCTOR? WHAT SURGERY HAVE YOU HAD AND WHEN? (LIST) 1. 2. 3. 4. 5. 6. 7. HOW MUCH ALCOHOL DO YOU DRINK
NAME: D/O/B: DATE: MR# WHAT PROBLEM(S) BRINGS YOU HERE TODAY? WHO SENT YOU TO US? DOCTOR/OTHER WHICH DOCTOR? WHAT SURGERY HAVE YOU HAD AND WHEN? (LIST) 1. 2. 3. 4. 5. 6. 7. HOW MUCH ALCOHOL DO YOU DRINK
J. Van Lier Ribbink, M.D., F.A.C.S. Center for Endocrine and Pancreas Surgery at Honor Health
 J. Van Lier Ribbink, M.D., F.A.C.S. Center for Endocrine and Pancreas Surgery at Honor Health Patient Clinical Information Questionnaire 1.0 Date of Questionnaire Completion; / / 2.0 Patient Data 2.1 Name:
J. Van Lier Ribbink, M.D., F.A.C.S. Center for Endocrine and Pancreas Surgery at Honor Health Patient Clinical Information Questionnaire 1.0 Date of Questionnaire Completion; / / 2.0 Patient Data 2.1 Name:
New Patient Paperwork
 New Patient Paperwork Date: Phone: Patient: Last Name First Name Initial Street Address: City/State/Zip Code: Sex: M F Age: Birthdate: Single Married Widowed Separated Divorced Email: Newsletter? Y N Insured
New Patient Paperwork Date: Phone: Patient: Last Name First Name Initial Street Address: City/State/Zip Code: Sex: M F Age: Birthdate: Single Married Widowed Separated Divorced Email: Newsletter? Y N Insured
Laser Vein Center Thomas Wright MD RVT Page 1 of 4
 Demographics Laser Vein Center Thomas Wright MD RVT Page 1 of 4 Patient Name: Address: City, St, Zip Primary Phone: Alternate: DOB: Social Security #: Marital Status: Married Single Other Emergency Contact:
Demographics Laser Vein Center Thomas Wright MD RVT Page 1 of 4 Patient Name: Address: City, St, Zip Primary Phone: Alternate: DOB: Social Security #: Marital Status: Married Single Other Emergency Contact:
How much do you know about illnesses or health problems for your parents, grandparents, brothers, sisters, and/or children? 1 A lot Some None at all
 Family Health History Please answer each question as honestly as possible. There are no right or wrong answers to nay of the questions. It is important that you answer as many questions as you can. We
Family Health History Please answer each question as honestly as possible. There are no right or wrong answers to nay of the questions. It is important that you answer as many questions as you can. We
MEDICAL HISTORY. Previous Nephrologist. Medication taken Insulin Oral Both. Who manages your diabetes? Blindness Yes No Hearing Problems Yes No
 MEDICAL HISTORY Please mark YES or NO and fill in appropriate blanks as needed Chronic Yes No If yes, year diagnosed Previous Nephrologist Transplant Yes No If yes, date Donor type Living Deceased Related
MEDICAL HISTORY Please mark YES or NO and fill in appropriate blanks as needed Chronic Yes No If yes, year diagnosed Previous Nephrologist Transplant Yes No If yes, date Donor type Living Deceased Related
City State Zip. Cell Phone. Other Phone. Gender Male Female Status Single Married Divorced Widowed. Height Weight EXERCISE Yes No Times per Week
 Patient Name (First Middle Last) Date of Birth Social Security # Address City State Zip Home Phone Work Phone Cell Phone Other Phone Email Place of Birth Occupation Retired Yes No Gender Male Female Status
Patient Name (First Middle Last) Date of Birth Social Security # Address City State Zip Home Phone Work Phone Cell Phone Other Phone Email Place of Birth Occupation Retired Yes No Gender Male Female Status
Accompanied by Relationship MEDICAL BACKGROUND INFORMATION. Please name the professionals that you have seen for this condition:
 Name: Age: Date: Accompanied by Relationship E-mail: @ MEDICAL BACKGROUND INFORMATION Please name the professionals that you have seen for this condition: Name Specialty Town Phone Who is your primary
Name: Age: Date: Accompanied by Relationship E-mail: @ MEDICAL BACKGROUND INFORMATION Please name the professionals that you have seen for this condition: Name Specialty Town Phone Who is your primary
New Patient History. Name: DOB: Sex: Date: If yes, give the name of the physician who did your evaluation or ordered your tests:
 New Patient History Name: DOB: Sex: Date: Chief Complaint: 1. Give a brief description of the problem you are seeking treatment for today: 2. Have you been evaluated for this problem or had any tests for
New Patient History Name: DOB: Sex: Date: Chief Complaint: 1. Give a brief description of the problem you are seeking treatment for today: 2. Have you been evaluated for this problem or had any tests for
Welcome to About Women by Women
 Welcome to About Women by Women Today s Date New Patient Questionnaire Name: Birth Date: / / Home Phone: Address: Cell Phone: Work Phone: Occupation: Employer: Marital Status: Married Living w/ Partner
Welcome to About Women by Women Today s Date New Patient Questionnaire Name: Birth Date: / / Home Phone: Address: Cell Phone: Work Phone: Occupation: Employer: Marital Status: Married Living w/ Partner
The following sections describe medical concerns related to specific organs or body. systems. Cardiac
 Aniella was born in 2005 and was prenatally diagnosed with full trisomy 18. She lives in the United States. Participation in the TRIS project began in 2011. Mother was 36 and father was 32 years old at
Aniella was born in 2005 and was prenatally diagnosed with full trisomy 18. She lives in the United States. Participation in the TRIS project began in 2011. Mother was 36 and father was 32 years old at
Amarillo Surgical Group Doctor: Date:
 Office Visit Information (General Surgery) Amarillo Surgical Group Doctor: Date: Patient s Information Name: Last First Middle Social Security #: Date of Birth: Age Gender: [ Male / Female ] Marital Status:
Office Visit Information (General Surgery) Amarillo Surgical Group Doctor: Date: Patient s Information Name: Last First Middle Social Security #: Date of Birth: Age Gender: [ Male / Female ] Marital Status:
TEXAS VASCULAR ASSOCIATES, P.A. PATIENT CLINICAL INTAKE FORM
 TEXAS VASCULAR ASSOCIATES, P.A. PATIENT CLINICAL INTAKE FORM PATIENT NAME: DATE OF BIRTH: TVA Physician being seen: Date of Visit: PAST MEDICAL HISTORY HEART PROBLEMS NEUROLOGICAL Congestive Heart Failure
TEXAS VASCULAR ASSOCIATES, P.A. PATIENT CLINICAL INTAKE FORM PATIENT NAME: DATE OF BIRTH: TVA Physician being seen: Date of Visit: PAST MEDICAL HISTORY HEART PROBLEMS NEUROLOGICAL Congestive Heart Failure
NEUROLOGICAL SURGERY, P.C.
 NEUROLOGICAL SURGERY, P.C. PATIENT INFORMATION Name Date of Birth Age Address City Sate NY Zip Home ( ) - Cell ( ) - Work ( ) - Ext: Email Address _ Sex M F Soc. Sec. #: / / Single Married Widowed Separated
NEUROLOGICAL SURGERY, P.C. PATIENT INFORMATION Name Date of Birth Age Address City Sate NY Zip Home ( ) - Cell ( ) - Work ( ) - Ext: Email Address _ Sex M F Soc. Sec. #: / / Single Married Widowed Separated
Please be sure to check with your insurance company to make sure that Dr. Kohli is covered under your plan.
 Dear You are scheduled for an appointment with Dr. Manoj Kohli at Christie Clinic in the Department of Rheumatology on at. Please check in on the first floor. The office is located on the 2 nd floor of
Dear You are scheduled for an appointment with Dr. Manoj Kohli at Christie Clinic in the Department of Rheumatology on at. Please check in on the first floor. The office is located on the 2 nd floor of
PLEASE COMPLETE ALL SECTIONS OF THIS FORM
 PLEASE COMPLETE ALL SECTIONS OF THIS FORM Patient Name: Date of Birth: Referring Doctor? (Name, telephone number and address) Chief Complaint: Why have you come here? How did it start? What are the symptoms?
PLEASE COMPLETE ALL SECTIONS OF THIS FORM Patient Name: Date of Birth: Referring Doctor? (Name, telephone number and address) Chief Complaint: Why have you come here? How did it start? What are the symptoms?
Medical History Form
 Medical History Form NAME DOB / / TODAY S DATE MEDICAL HISTORY What medical Conditions do you have? Select all that apply, or write in if not listed: Diabetes High Blood Pressure Thyroid Disorder Heart
Medical History Form NAME DOB / / TODAY S DATE MEDICAL HISTORY What medical Conditions do you have? Select all that apply, or write in if not listed: Diabetes High Blood Pressure Thyroid Disorder Heart
Patient Name: Date of Birth: Preferred Pharmacy: (name/location/phone #)
") Patient Name: Date of Birth: Referring Doctor: Primary Care Dr: Preferred Pharmacy: (name/location/phone #) CURRENT MEDICATIONS: Please list all Medication Dose Frequency 1 2 3 4 5 6 7 8 9 10 11 12 13
Patient Name: Date of Birth: Referring Doctor: Primary Care Dr: Preferred Pharmacy: (name/location/phone #) CURRENT MEDICATIONS: Please list all Medication Dose Frequency 1 2 3 4 5 6 7 8 9 10 11 12 13
WELCOME TO OUR OFFICE
 WELCOME TO OUR OFFICE Name: Today s Date: First Middle Last Gender: Male Female Date of birth: Age: Home Address: City: State: Zip: Home Phone:( ) Cell Phone:( ) Occupation: SSN: Employer: Time of employment
WELCOME TO OUR OFFICE Name: Today s Date: First Middle Last Gender: Male Female Date of birth: Age: Home Address: City: State: Zip: Home Phone:( ) Cell Phone:( ) Occupation: SSN: Employer: Time of employment
Dr. Hall New Patient Paperwork Please fill out these forms completely
 Dr. Hall New Patient Paperwork Please fill out these forms completely Date of Appointment Complete the enclosed packet and bring it to the appointment along with all X Rays, MRI disc and reports. Please
Dr. Hall New Patient Paperwork Please fill out these forms completely Date of Appointment Complete the enclosed packet and bring it to the appointment along with all X Rays, MRI disc and reports. Please
Patient Medical Information. Last. Sex: M / F Age: Date of Birth: Home Address: City: State: Zip Code: Business Address: City: State: Zip Code:
 Patient Medical Information Name: First Middle Last Sex: M / F Age: Date of Birth: Social Security # Driver s License # Home Address: City: State: Zip Code: Home Phone: Occupation: Cell: Employer: Business
Patient Medical Information Name: First Middle Last Sex: M / F Age: Date of Birth: Social Security # Driver s License # Home Address: City: State: Zip Code: Home Phone: Occupation: Cell: Employer: Business
List of Chapters. 5. Care of the sick child Evidence-based pediatrics (page 77 to 80)
") Illustrated Textbook of Paediatrics, 4th Edition Tom Lissauer, and Graham Clayden, 2012 List of Chapters 1. The child in society 2. History and examination 3. Normal child development, hearing and vision
Illustrated Textbook of Paediatrics, 4th Edition Tom Lissauer, and Graham Clayden, 2012 List of Chapters 1. The child in society 2. History and examination 3. Normal child development, hearing and vision
Capital Health Medical Center - Hopewell NEUROSURGICAL-ONCOLOGY Patient History
 Capital Health Medical Center - Hopewell NEUROSURGICAL-ONCOLOGY Patient History Please take a few minutes and complete the following questions before you see the doctors so that we may learn a bit more
Capital Health Medical Center - Hopewell NEUROSURGICAL-ONCOLOGY Patient History Please take a few minutes and complete the following questions before you see the doctors so that we may learn a bit more
Aicardi Syndrome At a Glance
 Aicardi Syndrome At a Glance Aicardi syndrome is a rare genetic condition found almost exclusively in girls. The complexity of this condition varies widely, with some girls having less obvious differences
Aicardi Syndrome At a Glance Aicardi syndrome is a rare genetic condition found almost exclusively in girls. The complexity of this condition varies widely, with some girls having less obvious differences
34th St. and Civic Center Blvd, Philadelphia, PA 19104, phone
 34th St. and Civic Center Blvd, Philadelphia, PA 19104, phone 215-590-3630 www.chop.edu/gastroenterology Please complete this form prior to your child s visit. Please fax to (215) 590-7224 or e-mail it
34th St. and Civic Center Blvd, Philadelphia, PA 19104, phone 215-590-3630 www.chop.edu/gastroenterology Please complete this form prior to your child s visit. Please fax to (215) 590-7224 or e-mail it
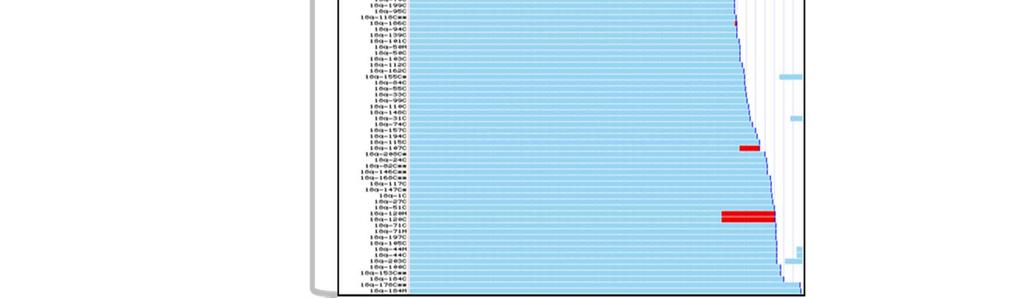
Lab #10: Karyotyping Lab
 Lab #10: Karyotyping Lab INTRODUCTION A karyotype is a visual display of the number and appearance of all chromosomes from a single somatic cell. A normal human karyotype would reveal 46 chromosomes (22
Lab #10: Karyotyping Lab INTRODUCTION A karyotype is a visual display of the number and appearance of all chromosomes from a single somatic cell. A normal human karyotype would reveal 46 chromosomes (22
Past Medical History. Chief Complaint: Patient Name: Appointment Date: Page 1
 Appointment Date: Page 1 Chief Complaint: (Please write reason, symptoms, condition or diagnosis that prompts your appointment) Past Medical History PERSONAL SKIN HISTORY YES NO Yes - Details Melanoma
Appointment Date: Page 1 Chief Complaint: (Please write reason, symptoms, condition or diagnosis that prompts your appointment) Past Medical History PERSONAL SKIN HISTORY YES NO Yes - Details Melanoma
MEDICAL HISTORY FORM FOR FOLLOW-UP
 MEDICAL HISTORY FORM FOR FOLLOW-UP ID NUMBER: 0a) Form Date... / / 0b) Staff Code... Instructions: Whenever numerical responses are required, enter the number so that the last digit appears in the rightmost
MEDICAL HISTORY FORM FOR FOLLOW-UP ID NUMBER: 0a) Form Date... / / 0b) Staff Code... Instructions: Whenever numerical responses are required, enter the number so that the last digit appears in the rightmost
DATE OF BIRTH: MELANOMA INTAKE
 MELANOMA INTAKE GENERAL INFORMATION How was your first diagnosed? (Check the diagnosis that describes your condition.) Melanoma Merkel Cell Carcinoma Squamous Cell Carcinoma Basal Cell Carcinoma Other
MELANOMA INTAKE GENERAL INFORMATION How was your first diagnosed? (Check the diagnosis that describes your condition.) Melanoma Merkel Cell Carcinoma Squamous Cell Carcinoma Basal Cell Carcinoma Other
City State Zip Code. Ethnic Background: Caucasian African-American Asian Hispanic Native American. Previous. Hobbies/Leisure activities:,,,
 History # UPIN # (Please leave blank) Name: First M.I. Last Address: Street (Apt #) City State Zip Code Phone number: ( ) ( ) Home Business Birth Date: / / Day-Month-Year Gender: M F Marital status: (Maiden
History # UPIN # (Please leave blank) Name: First M.I. Last Address: Street (Apt #) City State Zip Code Phone number: ( ) ( ) Home Business Birth Date: / / Day-Month-Year Gender: M F Marital status: (Maiden
Welcome to the Rubin Institute for Advanced Orthopedics!
 Welcome to the Rubin Institute for Advanced Orthopedics! Dear New Patient, Welcome to the Rubin Institute for Advanced Orthopedics! Our goal is to provide you with caring, compassionate and professional
Welcome to the Rubin Institute for Advanced Orthopedics! Dear New Patient, Welcome to the Rubin Institute for Advanced Orthopedics! Our goal is to provide you with caring, compassionate and professional
UnityPoint Clinic - Cardiology
 UnityPoint Clinic - Cardiology Date Completed: Appointment Date: Name: Age: Birthdate: / / FIRST MIDDLE INITIAL LAST Referred by: Family Dr.: Reason for visit: Describe briefly, include date of onset:
UnityPoint Clinic - Cardiology Date Completed: Appointment Date: Name: Age: Birthdate: / / FIRST MIDDLE INITIAL LAST Referred by: Family Dr.: Reason for visit: Describe briefly, include date of onset:
Patient History Form
 Patient History Form Advanced Directive Care Plan? Yes No Name: Birth date: / / Address: Age: Sex: F M STREET DAY YEAR Telephone: Home ( ) CITY STATE DAY YEAR MARITAL STATUS: Divorced Separated Alive/Age
Patient History Form Advanced Directive Care Plan? Yes No Name: Birth date: / / Address: Age: Sex: F M STREET DAY YEAR Telephone: Home ( ) CITY STATE DAY YEAR MARITAL STATUS: Divorced Separated Alive/Age
DIVISION OF CARDIOLOGY
 Name: Date of Birth: / / Home Phone #: Cell Phone #: Work Phone #: Fax #: Address: City: State: Zip: Primary Care Physician: Office Address: Work #: Fax #: Referring Physician (if different): Office Address:
Name: Date of Birth: / / Home Phone #: Cell Phone #: Work Phone #: Fax #: Address: City: State: Zip: Primary Care Physician: Office Address: Work #: Fax #: Referring Physician (if different): Office Address:
PATIENT HISTORY FORM
 Please bring completed history form to your scheduled appointment, if not completed this could delay your office visit. Thank you PATIENT HISTORY FORM Appointment Date Appointment Time Name Referring Physician
Please bring completed history form to your scheduled appointment, if not completed this could delay your office visit. Thank you PATIENT HISTORY FORM Appointment Date Appointment Time Name Referring Physician
Denise L. Newman, Ph.D.
 Denise L. Newman, Ph.D. Clinical and Developmental Psychologist ADULT HISTORY NAME: TODAY S DATE: BIRTH DATE: AGE: GENDER: (circle) Male Female Other MARITAL STATUS: ETHNICITY: HOME ADDRESS: EMAIL ADDRESS:
Denise L. Newman, Ph.D. Clinical and Developmental Psychologist ADULT HISTORY NAME: TODAY S DATE: BIRTH DATE: AGE: GENDER: (circle) Male Female Other MARITAL STATUS: ETHNICITY: HOME ADDRESS: EMAIL ADDRESS:
Room # Critical Care & Pulmonary Consultants, P.C.
 Room # Critical Care & Pulmonary Consultants, P.C. Health History You have been scheduled for an appointment with Critical Care and Pulmonary Consultants, P.C. This health history will help us facilitate
Room # Critical Care & Pulmonary Consultants, P.C. Health History You have been scheduled for an appointment with Critical Care and Pulmonary Consultants, P.C. This health history will help us facilitate
SECTION OF NEUROSURGERY PATIENT INFORMATION SHEET
 SECTION OF NEUROSURGERY PATIENT INFORMATION SHEET EC#: (for office use only) Patient s Name: Today s Date: Age: Date of Birth: Height: Weight: Physician you are seeing today: Marital Status: Married Work
SECTION OF NEUROSURGERY PATIENT INFORMATION SHEET EC#: (for office use only) Patient s Name: Today s Date: Age: Date of Birth: Height: Weight: Physician you are seeing today: Marital Status: Married Work
Optic Nerve Hypoplasia Part 2: Clinical Problems
 Optic Nerve Hypoplasia Part 2: Clinical Problems Hypopituitarism Deficiencies in: Growth hormone Thyroid hormone ACTH (cortisol) Anti-diuretic hormone (diabetes insipidus) Sex hormones Hypothalamic Dysfunction:
Optic Nerve Hypoplasia Part 2: Clinical Problems Hypopituitarism Deficiencies in: Growth hormone Thyroid hormone ACTH (cortisol) Anti-diuretic hormone (diabetes insipidus) Sex hormones Hypothalamic Dysfunction:
The Rehabilitation Institute Cancer Rehabilitation
 DO NOT DRILL The Rehabilitation Institute Cancer Rehabilitation STAR Patient Intake Form Your Name: Date: Your date of birth: Age: Who referred you (if a healthcare provider, please provide address)? Doctors
DO NOT DRILL The Rehabilitation Institute Cancer Rehabilitation STAR Patient Intake Form Your Name: Date: Your date of birth: Age: Who referred you (if a healthcare provider, please provide address)? Doctors
Southwest Service Life Insurance Company
 Southwest Service Life Insurance Company UNDERWRITING GUIDE 2/2012 95587v1Proof.indd 1 95587v1Proof.indd 2 95587v1Proof.indd 3 Acne A A A ADD A A A Addison s Disease D A D AIDS, ARC, HIV Infection D D
Southwest Service Life Insurance Company UNDERWRITING GUIDE 2/2012 95587v1Proof.indd 1 95587v1Proof.indd 2 95587v1Proof.indd 3 Acne A A A ADD A A A Addison s Disease D A D AIDS, ARC, HIV Infection D D
Evergreen Speech & Hearing Clinic, Inc. Transforming Lives Through Improved Communication Since 1979
 Patient Information Form Patient Information Patient Name: Date of Birth: / / Age: Last First MI mo day year Gender: Email Address: Address: City: State: Zip Code: Cell Phone: Home Phone: Work Phone: Referred
Patient Information Form Patient Information Patient Name: Date of Birth: / / Age: Last First MI mo day year Gender: Email Address: Address: City: State: Zip Code: Cell Phone: Home Phone: Work Phone: Referred
UnitedHealth Premium Physician Designation Program Episode Treatment Groups (ETG ) Description and Specialty
 Description and Specialty") UnitedHealth Premium Physician Designation Program Episode Treatment Groups (ETG ) Description and Specialty 666700 Acne Family Medicine, Internal Medicine, Pediatrics 438300 Acute Bronchitis Allergy,
UnitedHealth Premium Physician Designation Program Episode Treatment Groups (ETG ) Description and Specialty 666700 Acne Family Medicine, Internal Medicine, Pediatrics 438300 Acute Bronchitis Allergy,
Pediatric Sleep Questionnaire
 Pediatric Sleep Questionnaire Date Child's Name: Age Gender DOB Referring Physician: Primary Care Physician: Please answer fill out the following questionnaire regarding your child's sleep: What are your
Pediatric Sleep Questionnaire Date Child's Name: Age Gender DOB Referring Physician: Primary Care Physician: Please answer fill out the following questionnaire regarding your child's sleep: What are your
Athens Rheumatology Clinic, LLC Sana Makhdumi, MD
 Athens Rheumatology Clinic, LLC Sana Makhdumi, MD Phone: 706-850-8322 Fax: 706-850-8322 PATIENT HISTORY FORM Date of first appointment: / / Time of appointment: Birthdate: Name LAST FIRST MIDDLE INITIAL
Athens Rheumatology Clinic, LLC Sana Makhdumi, MD Phone: 706-850-8322 Fax: 706-850-8322 PATIENT HISTORY FORM Date of first appointment: / / Time of appointment: Birthdate: Name LAST FIRST MIDDLE INITIAL
PATIENT REGISTRATION
 P Account# PATIENT REGISTRATION Please answer all questions completely. PAYMENT IS EXPECTED WHEN SERVICES ARE RENDERED Date New Update Name Date of Birth Male Last First Middle Female Home Address City/State/Zip
P Account# PATIENT REGISTRATION Please answer all questions completely. PAYMENT IS EXPECTED WHEN SERVICES ARE RENDERED Date New Update Name Date of Birth Male Last First Middle Female Home Address City/State/Zip
Neonatal Hypotonia Guideline Prepared by Dan Birnbaum MD August 27, 2012
 Neonatal Hypotonia Guideline Prepared by Dan Birnbaum MD August 27, 2012 Hypotonia: reduced tension or resistance to range of motion Localization can be central (brain), peripheral (spinal cord, nerve,
Neonatal Hypotonia Guideline Prepared by Dan Birnbaum MD August 27, 2012 Hypotonia: reduced tension or resistance to range of motion Localization can be central (brain), peripheral (spinal cord, nerve,
NEW PATIENT FORM. Please print in ink and fill in all blanks Please fill out front and back. Patient s Full Name
 NEW PATIENT FORM Please print in ink and fill in all blanks Please fill out front and back Patient s Full Name Date of Birth Age Sex Social Security Number Referring Doctor or Family Physician Phone #
NEW PATIENT FORM Please print in ink and fill in all blanks Please fill out front and back Patient s Full Name Date of Birth Age Sex Social Security Number Referring Doctor or Family Physician Phone #
Mercy MS Center New Patient Information
 Mercy MS Center New Patient Information Last Name: First Name: DOB: MULTIPLE SCLEROSIS HISTORY Reason for clinic visit: I have been diagnosed with MS or NMO (Date diagnosed ) I have not been diagnosed
Mercy MS Center New Patient Information Last Name: First Name: DOB: MULTIPLE SCLEROSIS HISTORY Reason for clinic visit: I have been diagnosed with MS or NMO (Date diagnosed ) I have not been diagnosed
Sound View Acupuncture and Chinese Herbs 5410 California Ave SW, #202, Seattle, WA
 Sound View Acupuncture and Chinese Herbs 5410 California Ave SW, #202, Seattle, WA 98136 206.200.3595 Today s date Name Legal name (if different) Phone (primary) (secondary) Address City State Zip Email
Sound View Acupuncture and Chinese Herbs 5410 California Ave SW, #202, Seattle, WA 98136 206.200.3595 Today s date Name Legal name (if different) Phone (primary) (secondary) Address City State Zip Email
Evolution of Genetic Testing. Joan Pellegrino MD Associate Professor of Pediatrics SUNY Upstate Medical University
 Evolution of Genetic Testing Joan Pellegrino MD Associate Professor of Pediatrics SUNY Upstate Medical University Genetic Testing Chromosomal analysis Flourescent in situ hybridization (FISH) Chromosome
Evolution of Genetic Testing Joan Pellegrino MD Associate Professor of Pediatrics SUNY Upstate Medical University Genetic Testing Chromosomal analysis Flourescent in situ hybridization (FISH) Chromosome
Case 1 A 65 year old college professor came to the neurology clinic referred by her family physician because of frequent falling. She had a history of
 Peripheral Nervous System Case 1 A 65 year old college professor came to the neurology clinic referred by her family physician because of frequent falling. She had a history of non-insulin dependent diabetes
Peripheral Nervous System Case 1 A 65 year old college professor came to the neurology clinic referred by her family physician because of frequent falling. She had a history of non-insulin dependent diabetes
New Patient Packet. Patient Name: DOB: Age: Address: City: State: Zip: Address: City: State: Zip: Name: Address: Phone: Fax:
 New Patient Packet Patient Name: DOB: Age: Sex: Male / Female Height: Weight: PHYSICIAN CARE Primary Care Physician: Address: City: State: Zip: Phone: Fax: Referring Physician (if different from PCP):
New Patient Packet Patient Name: DOB: Age: Sex: Male / Female Height: Weight: PHYSICIAN CARE Primary Care Physician: Address: City: State: Zip: Phone: Fax: Referring Physician (if different from PCP):
Patient Name: Date: Address: Primary Care Physician: Online Website On TV In print On the radio
 927 W. Myrtle St. Boise, ID 83702 (208) 947-0100 NEW PATIENT INTAKE Patient Name: Date: Email Address: Primary Care Physician: How did you hear about AVT? (Please mark all that apply) Online Website On
927 W. Myrtle St. Boise, ID 83702 (208) 947-0100 NEW PATIENT INTAKE Patient Name: Date: Email Address: Primary Care Physician: How did you hear about AVT? (Please mark all that apply) Online Website On
LECOM Health Ophthalmology
 Patient Name: Date of Birth: New Patient Questionnaire Your answers will be used by your healthcare provider get an accurate history of your medical conditions and ocular concerns. If you are uncomfortable
Patient Name: Date of Birth: New Patient Questionnaire Your answers will be used by your healthcare provider get an accurate history of your medical conditions and ocular concerns. If you are uncomfortable
Early Teen Interview
 I. STUDY NUMBER II. EVENT II. TODAY S DATE / / III. RA INITIALS IV. SITE 1 KENMORE 2 HOME 9 OTHER Early Teen Interview Okay, great. So, let s start the interview. I d like to begin by stressing that there
I. STUDY NUMBER II. EVENT II. TODAY S DATE / / III. RA INITIALS IV. SITE 1 KENMORE 2 HOME 9 OTHER Early Teen Interview Okay, great. So, let s start the interview. I d like to begin by stressing that there
Northwest Georgia Surgical Specialists, PC PAST MEDICAL HISTORY
 orthwest Georgia Surgical Specialists, PC Medical History Form ame Date of visit Last First MI Day ear Date of Birth Age Gender Marital Status Height Weight Day ear Referring Doctor Reason for Visit PAST
orthwest Georgia Surgical Specialists, PC Medical History Form ame Date of visit Last First MI Day ear Date of Birth Age Gender Marital Status Height Weight Day ear Referring Doctor Reason for Visit PAST
SURGICAL BREAST PRACTICE NEW PATIENT QUESTIONNAIRE
 Patient Name MRN DATE: SURGICAL BREAST PRACTICE NEW PATIENT QUESTIONNAIRE Date of birth Age REASON FOR VISIT Abnormal Mammogram R L please specify Lump/Thickening R L upper lower inner outer Pain R L upper
Patient Name MRN DATE: SURGICAL BREAST PRACTICE NEW PATIENT QUESTIONNAIRE Date of birth Age REASON FOR VISIT Abnormal Mammogram R L please specify Lump/Thickening R L upper lower inner outer Pain R L upper
Cardiovascular Genetics Clinic Vascular Questionnaire
 Name: Address: Home Phone: Cell Phone: Email Address: Date of Birth: Primary Care Physician: Why have you been referred for a Cardiovascular Genetics Appointment? Have you had a genetics evaluation? If
Name: Address: Home Phone: Cell Phone: Email Address: Date of Birth: Primary Care Physician: Why have you been referred for a Cardiovascular Genetics Appointment? Have you had a genetics evaluation? If
Emory Clinic Department of Neurological Surgery Second Opinion Questionnaire
 Emory Clinic Department of Neurological Surgery Second Opinion Questionnaire First Name: M.I. Last Name: Date of Birth: Phone: Marital Status: Married Divorced Separated Widowed Single Work Status: Employed
Emory Clinic Department of Neurological Surgery Second Opinion Questionnaire First Name: M.I. Last Name: Date of Birth: Phone: Marital Status: Married Divorced Separated Widowed Single Work Status: Employed
New Patient Form. Patient Demographics. Emergency Information. Employment Information. Page 1 of 7. Family Health Chiropractic Care
 Page 1 of 7 Patient Demographics First Name* Last Name* Date Of Birth* Home Phone* Mobile Phone Phone Gender* Email Preferred Communication Street Address 1* Street Addresss 2 Zip* City* State* Emergency
Page 1 of 7 Patient Demographics First Name* Last Name* Date Of Birth* Home Phone* Mobile Phone Phone Gender* Email Preferred Communication Street Address 1* Street Addresss 2 Zip* City* State* Emergency
Evergreen Speech & Hearing Clinic, Inc. Transforming Lives Through Improved Communication Since 1979
 Patient Information Form Patient Information Patient Name: Date of Birth: / / Age: Last First MI mo day year Gender: Email Address: Address: City: State: Zip Code: Cell Phone: Home Phone: Work Phone: Referred
Patient Information Form Patient Information Patient Name: Date of Birth: / / Age: Last First MI mo day year Gender: Email Address: Address: City: State: Zip Code: Cell Phone: Home Phone: Work Phone: Referred
Osher Center for Integrative Medicine Pediatric Intake Form Name: Date: Date of Birth: Age: Current Pediatrician:
 Pediatric Intake Form Name: Date: Date of Birth: Age: Current Pediatrician: How did you hear about us? What are your goals for this visit? Where would you like to see improvement in your child s health?
Pediatric Intake Form Name: Date: Date of Birth: Age: Current Pediatrician: How did you hear about us? What are your goals for this visit? Where would you like to see improvement in your child s health?
The Advanced Spine Center Jason E. Lowenstein, MD Jamie L. DiGraziano, PA C
 The Advanced Spine Center Jason E. Lowenstein, MD Jamie L. DiGraziano, PA C PEDIATRIC SPINE HISTORY Name of Patient: For Office Use Only: HR: BP: / Date: Date of Birth: Age: Height: ft in Weight: lbs Form
The Advanced Spine Center Jason E. Lowenstein, MD Jamie L. DiGraziano, PA C PEDIATRIC SPINE HISTORY Name of Patient: For Office Use Only: HR: BP: / Date: Date of Birth: Age: Height: ft in Weight: lbs Form
Patient Intake Form for Allegany Ear, Nose, & Throat
 Patient Intake Form for Allegany Ear, se, & Throat Patient Name: What brings you to the office today? Who is your primary care doctor? Please list your current medications: Are you allergic to any medications?
Patient Intake Form for Allegany Ear, se, & Throat Patient Name: What brings you to the office today? Who is your primary care doctor? Please list your current medications: Are you allergic to any medications?
John Wayne Cancer Institute Dr. Foshag Dr. Faries Dr. Bilchik Dr. Leuchter
 John Wayne Cancer Institute Dr. Foshag Essner Dr. Fischer Dr. Faries Dr. Foshag Dr. Bilchik Dr. O'Day Dr. Leuchter Medical Questionnaire Reset Form Date: Name: Gender: Male Female Age: Last First Middle
John Wayne Cancer Institute Dr. Foshag Essner Dr. Fischer Dr. Faries Dr. Foshag Dr. Bilchik Dr. O'Day Dr. Leuchter Medical Questionnaire Reset Form Date: Name: Gender: Male Female Age: Last First Middle
Nutrition Consultation Intake Form Please write or print clearly
 Artemis in the City, LLC Danielle Heard, MS, MS, HHC Clinical & Functional Nutritionist ph: 866-330-5421 fx: 212-535-3234 www.artemisinthecity.com Nutrition Consultation Intake Form Please write or print
Artemis in the City, LLC Danielle Heard, MS, MS, HHC Clinical & Functional Nutritionist ph: 866-330-5421 fx: 212-535-3234 www.artemisinthecity.com Nutrition Consultation Intake Form Please write or print
Feeding Disorders and Growth in Williams Syndrome
 Feeding Disorders and Growth in Williams Syndrome Sharon M. Greis M.A., CCC/SLP BRS-S and Paige Kaplan M.B.B.Ch. Williams Syndrome Clinic The Children s Hospital of Philadelphia Pediatric Feeding & Swallowing
Feeding Disorders and Growth in Williams Syndrome Sharon M. Greis M.A., CCC/SLP BRS-S and Paige Kaplan M.B.B.Ch. Williams Syndrome Clinic The Children s Hospital of Philadelphia Pediatric Feeding & Swallowing
NEW PATIENT VISIT QUESTIONNAIRE
 HeartHealth A Program of the Dalio Institute of Cardiovascular Imaging NEW PATIENT VISIT QUESTIONNAIRE Name: Date of Birth: / / Address: City: State: Zip: Home Phone #: Work Phone #: Cell #: Email: Preferred
HeartHealth A Program of the Dalio Institute of Cardiovascular Imaging NEW PATIENT VISIT QUESTIONNAIRE Name: Date of Birth: / / Address: City: State: Zip: Home Phone #: Work Phone #: Cell #: Email: Preferred
Patient Name Date of Birth MALE / FEMALE Date. Left handed or Right handed. Marital Status: Single Married Divorced Widowed Children?
 PH NEW PATIENT HISTORY Patient Name Date of Birth MALE / FEMALE Date Occupation: Left handed or Right handed Marital Status: Single Married Divorced Widowed Children? Y or N # Previous Treating Physician:
PH NEW PATIENT HISTORY Patient Name Date of Birth MALE / FEMALE Date Occupation: Left handed or Right handed Marital Status: Single Married Divorced Widowed Children? Y or N # Previous Treating Physician:
Approach to the Child with Developmental Delay
 Approach to the Child with Developmental Delay Arwa Nasir Department of Pediatrics University of Nebraska Medical Center DISCLOSURE DECLARATION Approach to the Child with Developmental Delay Arwa Nasir
Approach to the Child with Developmental Delay Arwa Nasir Department of Pediatrics University of Nebraska Medical Center DISCLOSURE DECLARATION Approach to the Child with Developmental Delay Arwa Nasir
Patient to complete this information
 Patient to complete this information Patient s Name Birth date Today s date Referring Physician Primary Care Physician Age Occupation Retired, how long? Prior operations Medications Type Date Name Dose
Patient to complete this information Patient s Name Birth date Today s date Referring Physician Primary Care Physician Age Occupation Retired, how long? Prior operations Medications Type Date Name Dose
1960 FP CENTER FOR SLEEP DISORDERS
 1960 FP CENTER FOR SLEEP DISORDERS Sleep Questionnaire Name: Date: Date of Birth: / / Age: Gender: Height: Weight: lbs. Referring Physician: Occupation: Please give a brief description of your sleep problem
1960 FP CENTER FOR SLEEP DISORDERS Sleep Questionnaire Name: Date: Date of Birth: / / Age: Gender: Height: Weight: lbs. Referring Physician: Occupation: Please give a brief description of your sleep problem
The information you provide us will greatly help us provide the highest quality and most comprehensive care for you.
 Rheumatology (circle location of appointment) 111 Hundertmark Rd. Suite 115N 560 S. Maple St. Suite 400 place patient label here Chaska, MN 55318 Waconia, MN 55387 952-361-2450 952-361-2450 The information
Rheumatology (circle location of appointment) 111 Hundertmark Rd. Suite 115N 560 S. Maple St. Suite 400 place patient label here Chaska, MN 55318 Waconia, MN 55387 952-361-2450 952-361-2450 The information