IMRT IN HEAD NECK CANCER
|
|
|
- Annabel Green
- 5 years ago
- Views:
Transcription
1 IMRT IN HEAD NECK CANCER


2 THE SEARCH FOR CONFORMALITY

3 CONVENTIONAL RT Simple field arrangements Uniformly radiate both the target and the surrounding normal tissues. Includes the use of rectangular blocks to shield normal structures.
.")
4 CONFORMAL RT Multiple fields, including oblique and noncoplanar fields Varying weightage and wedges. Shaped blocks :Blocks may be Cerrobend blocks, or motor-driven Multi Leaf Collimators (MLC). CT-based 3D planning

5
6 INTENSITY MODULATED RADIOTHERAPY IMRT is a higher form of 3DCRT. Two forms: Forward planned IMRT :basically a form of complex 3DCRT using field-in-field technique. Inverse planned IMRT : requires Inverse Treatment Planning (ITP) software.
7 Forward Planning Inverse Planning Beam parameters (beam orientation, shape, modifier, beam weights, etc.) 3D dose distribution 3D dose distribution. Beams Fluence Profile If not satisfactory, then modify the beam parameters If objective criteria is not satisfied, Then, changes the beam parameters and/ or objective criteria
8 INVERSE PLANNING The user specifies the dose and dose-volume constraints for the PTV and OARs, using a system of priorities and weights. Normally the beam arrangement is predefined also. The system performs iterative calculations with a quadratic function, to achieve the best possible dose distribution based on the given dose constraints. After this, the accurate dose distribution is recalculated after considering the machine (jaw & MLC) parameters.
9 DOSE CONSTRAINTS 1.Based on physical parameters. Dose based Dose volume based 2.Biological model Tumor control probability. Normal tissue complication probability. EUD. Effective volume.

10 OPTIMISATION The process by which the optimum beam weight or intensity distribution is determined that can best satisfy the objective function/ cost function/ score as specified by planner. Conformality Target coverage OAR sparing Homogeneity
11 OPTIMISATION ALGORITHMS Essential for speeding up the optimisation process. The algorithms are almost entirely iterative ones. This means that they start with an initial guess for the beam profiles and modify the profiles step by step, until the optimum is found.

12 Beamlets The desired dose constraints are used to generate a fluence matrix. Fluence across the individual beams are modulated to create beamlets of different fluence.






13 DELIVERY TECHNIQUES Step-and shoot: done by superposing a number of different beam shapes with the same gantry orientationthese are called segments. Created by differing MLC arrangements, where the target is differentially blocked. Dynamic/ sliding window: the MLCs sweep across the field with different speeds and durations to create the same effect. Segments

14 STEP & SHOOT VS SLIDING WINDOW IMRT
15 COMPLEX 3DCRT/ FORWARD PLANNED IMRT (WESTBANK EXPERIENCE)

16 95% DOSE COLOUR WASH 7 Beam arrangement

17 DVH L parotid 42% >30Gy R parotid 55%>30 Gy
18 3DCRT VS IMRT

19
20 IMRT vs Rapid Arc vs Tomotherapy
 Improved critical structure sparing (EUD of surrounding normal tissue reduced by 17.4% for BOT and 27.")
21 Dosimetric study (N=10) All patients had oropharyngeal carcinoma (5 BOT, 5 tonsil) 2 sets of plans: IMRT vs Tomotherapy Improved dose homogeneity within the target volume with HT (SD within the PTV reduced by 71%) Improved critical structure sparing (EUD of surrounding normal tissue reduced by 17.4% for BOT and 27.1% for tonsil) 80% reduction in NTCP of parotid glands

22 Dosimetric study (N=29) Patients of carcinoma oropharynx, hypopharynx and larynx Conventional (Sliding Window) IMRT vs Rapid Arc(single arc) vs Rapid Arc (double arc) Both variants of rapid arc were significantly better in sparing normal tissue. Average doses to ipsilateral parotid were 40 Gy vs 36.2 Gy vs 34.4 Gy & to contralateral parotid were 32.6 Gy vs 30.9 Gy vs 28.2 Gy Rapid arc (double arc) also significantly improved target coverage & homogeneity with respect to conventional IMRT.

23 PRACTICALITIES OF IMRT
24 PROCESS OF IMRT PLANNING Immobilization Planning CT Image transfer Contouring of volumes Margins Treatment planning Selection of optimum plan (dose distribution & DVH analysis) Plan quality assurance Plan implementation Position verification (2D/3D) Treatment execution









25 WORKFLOW CT simulator TPS LA Unified Database QA LA console

26 ITP SOFTWARE INTERFACE: SETTING PRIORITIES & CONSTRAINTS DVH Fluence Map
27 WHAT HAPPENS IN IMRT QA? The patient s plan is opened on the CT dataset of the phantom. Gantry angles are set to zero. The plan is recalculated. The new plan is executed with the phantom in place. Point doses (measured & calculated) are compared to ensure accurate dose calculation by the TPS has been done.
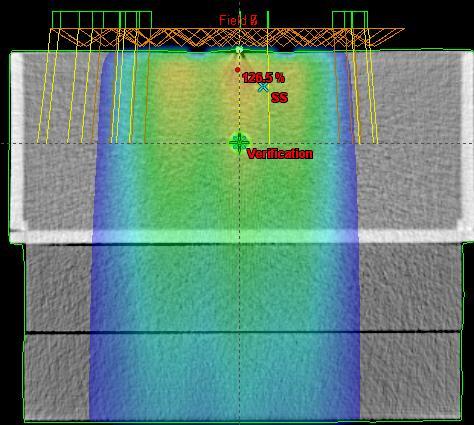
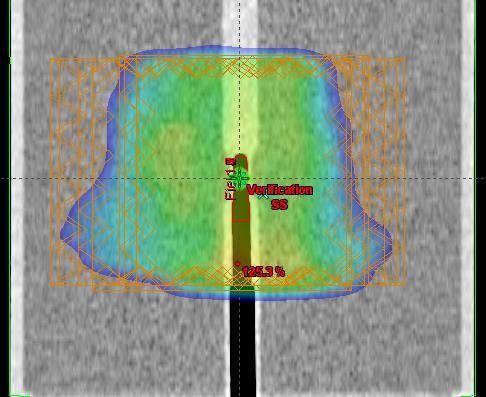
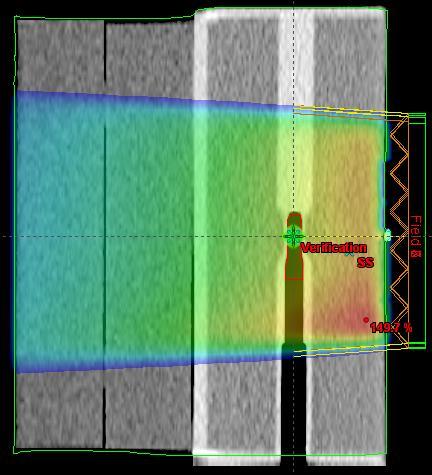
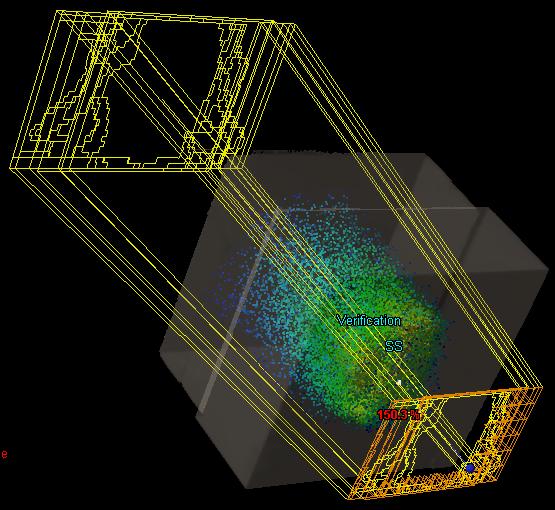
28 QUALITY ASSURANCE: WATER PHANTOM


29 QUALITY ASSURANCE: IMATRIXX (ION CHAMBER ARRAY)
30 IMRT DOSE & FRACTIONATION
31 EUD Standard dose constraints assume that the whole organ is being uniformly irradiated at 1.8-2Gy/#. In IMRT, aside from use of higher dose/# (in SIB), most OARs are only partially irradiated. There is also a steep dose gradient within a given OAR. Equivalent Uniform Dose (EUD) is that dose, which had the organ been wholly and uniformly irradiated,would have produced the same biological effect. Complex voxel-based calculation.
32 SIB-IMRT/SMART VS SEQUENTIAL IMRT Dosimtric advantage: Superior PTV conformality & superior parotid gland sparing. Dogan et al (2003) Logistical advantage : lesser number of treatment days required. Radiobiogical advantage: Due to higher dose/# (to the target) and lesser duration of treatment, the NTD (Normalised Total Dose=EQD2) is actually higher than the Nominal Dose.
33 Nancy Lee, et al SIB-IMRT VS CONCOMITANT BOOST RT (CBRT) (MSKCC, 2006) Study period Sep Jun 2004 N=293 All were patients of Ca oropharynx (112 were stage III/IV). 41 received SIB-IMRT with concurrent chemotherapy 71 received conventional 2DRT with late concomitant boost (CBRT) along with concurrent chemotherapy RT dose was 70 Gy. Parotid dose constraint for IMRT was mean dose <=26 Gy. Significant advantage in terms of PEG-dependancy & severe xerostomia at 2 years, in favour of IMRT.
34 COMMON SIB DOSE SCHEDULES (1) 70 Gy/35# to PTV (GTV) 63 Gy/35# to PTV (CTV1:high risk microscopic ds) 54 Gy/35# to PTV (CTV2: low risk microscopic ds) (2) 66 Gy/30# to PTV (GTV) 60 Gy/30# to PTV (CTV1:high risk microscopic ds) 54 Gy/30# to PTV (CTV2: low risk microscopic ds)
35 CLINICAL IMPACT OF IMRT

36 What happens to the parotid glands in Conventional RT?
37 PAROTID DOSE & XEROSTOMIA Eisbruch et al (1999): A mean parotid dose of < 26 Gy should be planning goal. Eisbruch et al (2007): Substantial parotid flow recovery (upto 86% of pretreatment levels) at 2 years if mean doses are between 25-30Gy. Eisbruch et al (2010): Severe xerostomia (<25% of baseline) avoided if mean parotid dose kept to <20Gy (if one parotid is to be spared) or <25 Gy (if both are to be spared)
38 DOES PAROTID-SPARING IMRT HAVE A NEGATIVE IMPACT ON LOCAL CONTROL? Cannon & Lee (2008): (N=3) All patient had recurrence near a spared parotid gland. Eisbruch et al (2005): (N=158, all stage III/IV) 19/23 failures occurred in-field, within the high-dose volume. Suggest that clinical rather than dosimetric factors predicted outcome & suggested treatment intensification in these advanced cases.
39 SUBMANDIBULAR GLAND DOSE & XEROSTOMIA Xerostomia does not correlate with parotid doses alone. If submandibular gland doses are kept to =<39Gy, then also there is good recovery of salivary flow rates at 2 years.
40 CONSTRICTOR DOSE & DYSPHAGIA Levendag et al (2007): Significant correlation between doses to superior and middle constrictors and incidence of severe dysphagia. Steep dose response curve, with 19% increase in probability with every 10Gy dose. Bhide et al (2009): No statistically significant correlation between radiation dose to the pharyngeal constrictors and observer-assessed/ patient-reported severe dysphagia at 1 year
41 IMRT : IMPACT ON QOL Evidence-based review by Nutting et al (2010): Significant heterogeneity in data. Conflicting results.
42 IS CONC CHEMO NECESSARY WITH SIB-IMRT? IF REQUIRED, IS IT TOLERATED?


43 CHEMO: BED
44 RTOG (2010) N=69 (14 institutions) All patients of Ca oropharynx, stage T1-T2,N0-N1,M0 No chemo was permitted RT dose was 66Gy/30# to PTV(gross disease) and 54-60Gy/30# to PTV (subclinical) Median FU=2.8 years 2-yr LRF was only 9%. Very low rate of severe (>grade 2) late toxicities: skin (12%), mucosa(24%). Xerostomia (grade 2) was seen in 55% patients at 6 months but reduced to 16% at 2 years Moderately hypofractionated IMRT without chemotherapy in early oropharyngeal carcinomas, is safe & well-tolerated.

45
46 SIB-IMRT with conc chemotherapy is welltolerated and effective for all common headneck sites. Trials included mostly locally advanced cases. Locoregional failure rates are around 5-20%. Overall survival rates are around 60-85%. 2-yr severe xerostomia rates are around 0-30%.
47 IMRT IN HNC: THE EVIDENCE SO FAR
48 2 Meta-analyses
49 30 studies, including 3 RCTs so far comparing IMRT with conventional RT/3DCRT Of the 3 RCTs, 2 are small studies on Nasopharyngeal cancer, from China. The 3 rd is the PARSPORT study from UK on oro-hypopharyngeal and laryngeal cancers.
50 Pow et al (n=51) : Stage II NPX: 2DRT vs IMRT: IMRT significantly increased xerostomia-related but not overall HRQoL. Kam et al (n=60): Stage I & II NPX: 2DRT vs IMRT: IMRT significantly reduced the clinicianassessed (but not the patient reported!!) grade 2-4 xerostomia at both 6 weeks and 12 months.
51 PARSPORT
52
53 OTHER STUDIES IN ORAL/OROHYPOPHARYNGEAL/LARYNGEAL CANCERS 15 non-randomised studies: IMRT (n=959) vs 2DRT/3DCRT (n=1455) All report reduced acute & late xerostomia, leading to better xerostomia- HR QoL 2 studies have reported statistically significant improvements in tumor control.
 were within the high-dose volume & only 25%")
54 Siemens trial (3DCRT vs IMRT) N=60 The aim was to analyse location of site of locoregional failure and their dose-volume correlation It was found that the majority of failures (75%) were within the high-dose volume & only 25% were marginal.

55 IMRT led to significant improvements in acute grade 3 toxicities of skin, mucous membrane & pharynx IMRT also led to significant delayed progress to grade 2 toxicity in the above sites Mean dose to the target also significantly improved with IMRT compared to conv RT

56 ONGOING/ UNPUBLISHED RCTS OF IMRT IN HNC
57 IMRT: VARIATIONS
58 IMRT is not a magic- box & there is no single right answer. Hence, as before, the treatment methods and results remain very much dependant on the physician s approach. Almost every area of IMRT planning sees significant variation in approach between any 2 clinicians.
59 Dose levels: 2/3 Dose prescription technique: to 2-3 different PTVs OR different levels to GTV, CTV,PTV Boost technique: SIB/sequential Dose to electively irradiated nodes : 50 & 60Gy/ uniformly 50 Gy/ uniformly 60 Gy Spinal cord constraint parameter: max/ 1%/2%/ 1cc/2cc (ICRU 83 recommends reporting all OARs on D 2% ) Spinal cord dose constraint : 45/47/48/50 Gy Parotid constraint parameter: whole parotid/ (parotid-ptv)
60 PATTERN OF CARE SURVEY IN HEAD & NECK CANCER JYOTIRUP GOSWAMI & SUMAN MALLIK (AROICON 2011) Aims & objectives: As new paradigms and techniques emerge and older ones are eclipsed in the treatment of head and neck cancer, it is important to gauge attitudes and approaches in the Radiation Oncology community. This study was an attempt to objectively analyse a few subjective but highly crucial issues relating to practice in head and neck cancers. Materials & methods: Keeping constraints of time and convenience in mind, a brief questionnaire comprising 20 key questions was framed and circulated by to radiation oncologists of Consultant rank across India, in both government and corporate sectors, between June 2011-August The questions related to diagnosis, radiotherapy planning, chemotherapy protocol, supportive care,follow up and management of post-radiotherapy recurrences. Responses were collated and analysed
61 % of patients undergoing Triple scopy for staging: (a) 0-20 (b) (c) (d)>60 % of patients undergoing PET-CT for staging: (a) 0-20 (b) (c) (d)>60 Indication for Induction chemotherapy for oropharyngeal/hypopharyngeal/laryngeal cancers: (a) stage II onwards (b) stage III onwards (c) only stage IV (d) not considered Induction chemotherapy regime & no of cycles: (a) TPFx3 (b) PFx3 (c)tipx3 (d) Others Spinal cord tolerance parameter: (a) Max dose (b) 1% volume (c) 1cc volume (d) 2cc volume Spinal cord tolerance dose (Gy):-- Parotid dose constraints for IMRT: (a) Average dose to whole parotid <26 Gy (b)dose received by 50% of Whole parotid <30 Gy (c) Average dose to (Whole parotid-ptv) <26 Gy (d) Dose received by 50% of (Whole parotid- PTV) <30 Gy (e) Average dose to whole parotid<20 Gy % of patients on IMRT: (a) 0-30% (b) 30-50% (c) >50% IMRT fractionation: (a) Conventional (b) SIB SIB-IMRT dose levels: PET-CT based RT planning: (a) Yes (b) No Routine counselling for PEG tube insertion before RT: (a) Yes (b) No Routine Triple scopy for follow-up: (a) Yes No (b) Routine Imaging for follow-up: (a) Yes (b) No Imaging modality for follow-up: (a) CT (b) MR (c) PET-CT Preferred management of locoregional recurrence post-radiotherapy: (a) Surgery alone (b) Surgery + systemic therapy (c) Reirradiation Preferred chemotherapy regime for locoregional recurrence: (a) Platinum (b) Taxane-Platinum doublet (c) Others---- Preferred biologically targeted agent for locoregional recurrence: (a) Cetuximab (b) Nimotuzumab (c) Others--- Reirradiation safegap: (a) >6 months (b) >2 years (c) Other---- Reirradiation dose: (a) Gy (b) Gy (c) > 60 Gy
62 Results: Out of 80 s sent, only 25 (31.25%) responded. Most clinicians (68%) were still using maximum dose as spinal cord tolerance dose parameter and the preferred threshold, in 52% was 44-46Gy. Majority of clinicians (68%) were using intensity modulated radiotherapy (IMRT) in fewer than 30% of cases. Most (68%) were using simultaneous integrated boost as preferred IMRT schedule. Conclusions: While the study is a work in progress, it underlines the importance of good communication and evidence-based approaches.
63 THANK YOU
Efficient SIB-IMRT planning of head & neck patients with Pinnacle 3 -DMPO
 Investigations and research Efficient SIB-IMRT planning of head & neck patients with Pinnacle 3 -DMPO M. Kunze-Busch P. van Kollenburg Department of Radiation Oncology, Radboud University Nijmegen Medical
Investigations and research Efficient SIB-IMRT planning of head & neck patients with Pinnacle 3 -DMPO M. Kunze-Busch P. van Kollenburg Department of Radiation Oncology, Radboud University Nijmegen Medical
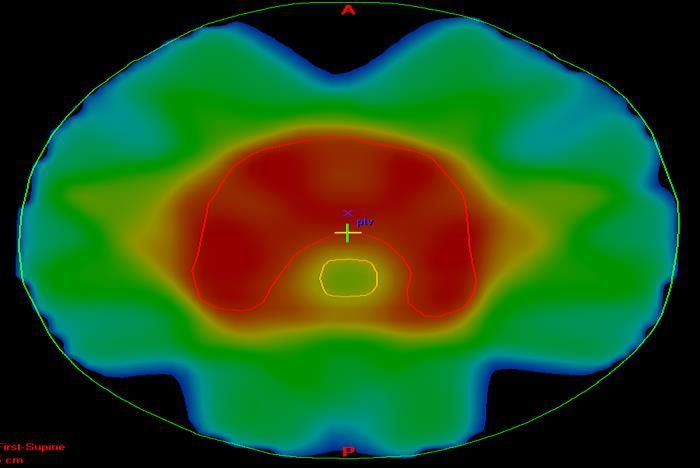
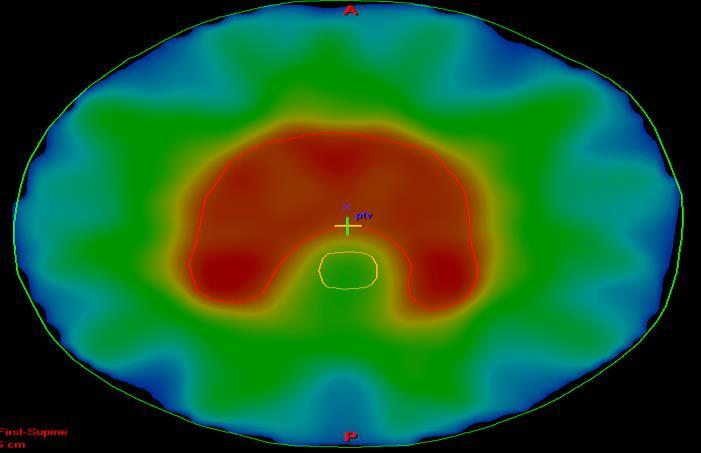
Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer
 Techniques in Head and Neck Cancer") 1 Charles Poole April Case Study April 30, 2012 Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer Abstract: Introduction: This study
1 Charles Poole April Case Study April 30, 2012 Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer Abstract: Introduction: This study
IMRT - the physician s eye-view. Cinzia Iotti Department of Radiation Oncology S.Maria Nuova Hospital Reggio Emilia
 IMRT - the physician s eye-view Cinzia Iotti Department of Radiation Oncology S.Maria Nuova Hospital Reggio Emilia The goals of cancer therapy Local control Survival Functional status Quality of life Causes
IMRT - the physician s eye-view Cinzia Iotti Department of Radiation Oncology S.Maria Nuova Hospital Reggio Emilia The goals of cancer therapy Local control Survival Functional status Quality of life Causes
A VMAT PLANNING SOLUTION FOR NECK CANCER PATIENTS USING THE PINNACLE 3 PLANNING SYSTEM *
 Romanian Reports in Physics, Vol. 66, No. 2, P. 401 410, 2014 A VMAT PLANNING SOLUTION FOR NECK CANCER PATIENTS USING THE PINNACLE 3 PLANNING SYSTEM * M. D. SUDITU 1,2, D. ADAM 1,2, R. POPA 1,2, V. CIOCALTEI
Romanian Reports in Physics, Vol. 66, No. 2, P. 401 410, 2014 A VMAT PLANNING SOLUTION FOR NECK CANCER PATIENTS USING THE PINNACLE 3 PLANNING SYSTEM * M. D. SUDITU 1,2, D. ADAM 1,2, R. POPA 1,2, V. CIOCALTEI
Potential benefits of intensity-modulated proton therapy in head and neck cancer van de Water, Tara Arpana
 University of Groningen Potential benefits of intensity-modulated proton therapy in head and neck cancer van de Water, Tara Arpana IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's
University of Groningen Potential benefits of intensity-modulated proton therapy in head and neck cancer van de Water, Tara Arpana IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's
Treatment Planning Evaluation of Volumetric Modulated Arc Therapy (VMAT) for Craniospinal Irradiation (CSI)
 for Craniospinal Irradiation (CSI)") Treatment Planning Evaluation of Volumetric Modulated Arc Therapy (VMAT) for Craniospinal Irradiation (CSI) Tagreed AL-ALAWI Medical Physicist King Abdullah Medical City- Jeddah Aim 1. Simplify and standardize
Treatment Planning Evaluation of Volumetric Modulated Arc Therapy (VMAT) for Craniospinal Irradiation (CSI) Tagreed AL-ALAWI Medical Physicist King Abdullah Medical City- Jeddah Aim 1. Simplify and standardize
Quality assurance and credentialing requirements for sites using inverse planned IMRT Techniques
 TROG 08.03 RAVES Quality assurance and credentialing requirements for sites using inverse planned IMRT Techniques Introduction Commissioning and quality assurance of planning systems and treatment delivery
TROG 08.03 RAVES Quality assurance and credentialing requirements for sites using inverse planned IMRT Techniques Introduction Commissioning and quality assurance of planning systems and treatment delivery
Potential benefits of intensity-modulated proton therapy in head and neck cancer van de Water, Tara Arpana
 University of Groningen Potential benefits of intensity-modulated proton therapy in head and neck cancer van de Water, Tara Arpana IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's
University of Groningen Potential benefits of intensity-modulated proton therapy in head and neck cancer van de Water, Tara Arpana IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's
Utilizzo delle tecniche VMAT nei trattamenti del testa collo Marta Scorsetti M.D.
 Utilizzo delle tecniche VMAT nei trattamenti del testa collo Marta Scorsetti M.D. Radiotherapy and Radiosurgery Dpt. Istituto Clinico Humanitas, Milan, Italy. Higher doses to the tumor Better sparing of
Utilizzo delle tecniche VMAT nei trattamenti del testa collo Marta Scorsetti M.D. Radiotherapy and Radiosurgery Dpt. Istituto Clinico Humanitas, Milan, Italy. Higher doses to the tumor Better sparing of
Chapter 2. Level II lymph nodes and radiation-induced xerostomia
 Chapter 2 Level II lymph nodes and radiation-induced xerostomia This chapter has been published as: E. Astreinidou, H. Dehnad, C.H. Terhaard, and C.P Raaijmakers. 2004. Level II lymph nodes and radiation-induced
Chapter 2 Level II lymph nodes and radiation-induced xerostomia This chapter has been published as: E. Astreinidou, H. Dehnad, C.H. Terhaard, and C.P Raaijmakers. 2004. Level II lymph nodes and radiation-induced
TOMOTERAPIA in Italia: Esperienze a confronto
 TOMOTERAPIA in Italia: Esperienze a confronto BARD 20 novembre 2010 L esperienza di Reggio Emilia Testa collo Alessandro Muraglia Reasons for the use of tomotherapy: - Complex tumor geometry and proximity
TOMOTERAPIA in Italia: Esperienze a confronto BARD 20 novembre 2010 L esperienza di Reggio Emilia Testa collo Alessandro Muraglia Reasons for the use of tomotherapy: - Complex tumor geometry and proximity
A Comparison of IMRT and VMAT Technique for the Treatment of Rectal Cancer
 A Comparison of IMRT and VMAT Technique for the Treatment of Rectal Cancer Tony Kin Ming Lam Radiation Planner Dr Patricia Lindsay, Radiation Physicist Dr John Kim, Radiation Oncologist Dr Kim Ann Ung,
A Comparison of IMRT and VMAT Technique for the Treatment of Rectal Cancer Tony Kin Ming Lam Radiation Planner Dr Patricia Lindsay, Radiation Physicist Dr John Kim, Radiation Oncologist Dr Kim Ann Ung,
Clinical experience with TomoDirect System Tangential Mode
 Breast Cancer Clinical experience with TomoDirect System Tangential Mode European Institute of Oncology Milan, Italy Disclosure & Disclaimer An honorarium is provided by Accuray for this presentation The
Breast Cancer Clinical experience with TomoDirect System Tangential Mode European Institute of Oncology Milan, Italy Disclosure & Disclaimer An honorarium is provided by Accuray for this presentation The
The objective of this lecture is to integrate our knowledge of the differences between 2D and 3D planning and apply the same to various clinical
 The objective of this lecture is to integrate our knowledge of the differences between 2D and 3D planning and apply the same to various clinical sites. The final aim will be to be able to make out these
The objective of this lecture is to integrate our knowledge of the differences between 2D and 3D planning and apply the same to various clinical sites. The final aim will be to be able to make out these
Dosimetric Comparison of Intensity-Modulated Radiotherapy versus 3D Conformal Radiotherapy in Patients with Head and Neck Cancer
 Dosimetric Comparison of Intensity-Modulated Radiotherapy versus 3D Conformal Radiotherapy in Patients with Head and Neck Cancer 1- Doaa M. AL Zayat. Ph.D of medical physics, Ayadi-Al Mostakbl Oncology
Dosimetric Comparison of Intensity-Modulated Radiotherapy versus 3D Conformal Radiotherapy in Patients with Head and Neck Cancer 1- Doaa M. AL Zayat. Ph.D of medical physics, Ayadi-Al Mostakbl Oncology
Treatment Planning for Lung. Kristi Hendrickson, PhD, DABR University of Washington Dept. of Radiation Oncology
 Treatment Planning for Lung Kristi Hendrickson, PhD, DABR University of Washington Dept. of Radiation Oncology Outline of Presentation Dosimetric planning strategies for SBRT lung Delivery techniques Examples
Treatment Planning for Lung Kristi Hendrickson, PhD, DABR University of Washington Dept. of Radiation Oncology Outline of Presentation Dosimetric planning strategies for SBRT lung Delivery techniques Examples
Potential benefits of intensity-modulated proton therapy in head and neck cancer van de Water, Tara Arpana
 University of Groningen Potential benefits of intensity-modulated proton therapy in head and neck cancer van de Water, Tara Arpana IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's
University of Groningen Potential benefits of intensity-modulated proton therapy in head and neck cancer van de Water, Tara Arpana IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's
Original Article. Teyyiba Kanwal, Muhammad Khalid, Syed Ijaz Hussain Shah, Khawar Nadeem
 Original Article Treatment Planning Evaluation of Sliding Window and Multiple Static Segments Technique in Intensity Modulated Radiotherapy for Different Beam Directions Teyyiba Kanwal, Muhammad Khalid,
Original Article Treatment Planning Evaluation of Sliding Window and Multiple Static Segments Technique in Intensity Modulated Radiotherapy for Different Beam Directions Teyyiba Kanwal, Muhammad Khalid,
Reena Phurailatpam. Intensity Modulated Radiation Therapy of Medulloblastoma using Helical TomoTherapy: Initial Experience from planning to delivery
 Intensity Modulated Radiation Therapy of Medulloblastoma using Helical TomoTherapy: Initial Experience from planning to delivery Reena Phurailatpam Tejpal Gupta, Rakesh Jalali, Zubin Master, Bhooshan Zade,
Intensity Modulated Radiation Therapy of Medulloblastoma using Helical TomoTherapy: Initial Experience from planning to delivery Reena Phurailatpam Tejpal Gupta, Rakesh Jalali, Zubin Master, Bhooshan Zade,
Head and Neck Treatment Planning: A Comparative Review of Static Field IMRT RapidArc TomoTherapy HD. Barbara Agrimson, BS RT(T)(R), CMD
(R), CMD") Head and Neck Treatment Planning: A Comparative Review of Static Field IMRT RapidArc TomoTherapy HD Barbara Agrimson, BS RT(T)(R), CMD Disclaimer This presentation will mention equipment by trade name.
Head and Neck Treatment Planning: A Comparative Review of Static Field IMRT RapidArc TomoTherapy HD Barbara Agrimson, BS RT(T)(R), CMD Disclaimer This presentation will mention equipment by trade name.
Silvia Pella, PhD, DABR Brian Doozan, MS South Florida Radiation Oncology Florida Atlantic University Advanced Radiation Physics Boca Raton, Florida
 American Association of Medical Dosimetrists 2015 Silvia Pella, PhD, DABR Brian Doozan, MS South Florida Radiation Oncology Florida Atlantic University Advanced Radiation Physics Boca Raton, Florida Most
American Association of Medical Dosimetrists 2015 Silvia Pella, PhD, DABR Brian Doozan, MS South Florida Radiation Oncology Florida Atlantic University Advanced Radiation Physics Boca Raton, Florida Most
IMRT - Intensity Modulated Radiotherapy
 IMRT - Intensity Modulated Radiotherapy Advanced product in the RT technology Aims to deliver radiation more precisely to the tumor, while relatively limiting dose to the surrounding normal tissues 7 position
IMRT - Intensity Modulated Radiotherapy Advanced product in the RT technology Aims to deliver radiation more precisely to the tumor, while relatively limiting dose to the surrounding normal tissues 7 position
CURRICULUM OUTLINE FOR TRANSITIONING FROM 2-D RT TO 3-D CRT AND IMRT
 CURRICULUM OUTLINE FOR TRANSITIONING FROM 2-D RT TO 3-D CRT AND IMRT Purpose The purpose of this curriculum outline is to provide a framework for multidisciplinary training for radiation oncologists, medical
CURRICULUM OUTLINE FOR TRANSITIONING FROM 2-D RT TO 3-D CRT AND IMRT Purpose The purpose of this curriculum outline is to provide a framework for multidisciplinary training for radiation oncologists, medical
Defining Target Volumes and Organs at Risk: a common language
 Defining Target Volumes and Organs at Risk: a common language Eduardo Rosenblatt Section Head Applied Radiation Biology and Radiotherapy (ARBR) Section Division of Human Health IAEA Objective: To introduce
Defining Target Volumes and Organs at Risk: a common language Eduardo Rosenblatt Section Head Applied Radiation Biology and Radiotherapy (ARBR) Section Division of Human Health IAEA Objective: To introduce
International Multispecialty Journal of Health (IMJH) ISSN: [ ] [Vol-3, Issue-9, September- 2017]
![International Multispecialty Journal of Health (IMJH) ISSN: [ ] [Vol-3, Issue-9, September- 2017]](/thumbs/84/90586123.jpg "International Multispecialty Journal of Health (IMJH) ISSN: [ ] [Vol-3, Issue-9, September- 2017]") Dosimetric evaluation of carcinoma nasopharynx using Volumetric Modulated Arc Therapy (VMAT): An institutional experience from Western India Dr. Upendra Nandwana 1, Dr. Shuchita Pathak 2, Dr. TP Soni 3,
Dosimetric evaluation of carcinoma nasopharynx using Volumetric Modulated Arc Therapy (VMAT): An institutional experience from Western India Dr. Upendra Nandwana 1, Dr. Shuchita Pathak 2, Dr. TP Soni 3,
Simultaneous Integrated Boost or Sequential Boost in the Setting of Standard Dose or Dose De-escalation for HPV- Associated Oropharyngeal Cancer
 Simultaneous Integrated Boost or Sequential Boost in the Setting of Standard Dose or Dose De-escalation for HPV- Associated Oropharyngeal Cancer Dawn Gintz, CMD, RTT Dosimetry Coordinator of Research and
Simultaneous Integrated Boost or Sequential Boost in the Setting of Standard Dose or Dose De-escalation for HPV- Associated Oropharyngeal Cancer Dawn Gintz, CMD, RTT Dosimetry Coordinator of Research and
Helical tomotherapy for head and neck squamous cell carcinoma: Dosimetric comparison with linear accelerator-based step-and-shoot IMRT
 Original Article Free full text available from www.cancerjournal.net Helical tomotherapy for head and neck squamous cell carcinoma: Dosimetric comparison with linear accelerator-based step-and-shoot IMRT
Original Article Free full text available from www.cancerjournal.net Helical tomotherapy for head and neck squamous cell carcinoma: Dosimetric comparison with linear accelerator-based step-and-shoot IMRT
THE TRANSITION FROM 2D TO 3D AND TO IMRT - RATIONALE AND CRITICAL ELEMENTS
 THE TRANSITION FROM 2D TO 3D AND TO IMRT - RATIONALE AND CRITICAL ELEMENTS ICTP SCHOOL ON MEDICAL PHYSICS FOR RADIATION THERAPY DOSIMETRY AND TREATMENT PLANNING FOR BASIC AND ADVANCED APPLICATIONS March
THE TRANSITION FROM 2D TO 3D AND TO IMRT - RATIONALE AND CRITICAL ELEMENTS ICTP SCHOOL ON MEDICAL PHYSICS FOR RADIATION THERAPY DOSIMETRY AND TREATMENT PLANNING FOR BASIC AND ADVANCED APPLICATIONS March
Intensity Modulated Radiation Therapy (IMRT)
") Intensity Modulated Radiation Therapy (IMRT) Policy Number: Original Effective Date: MM.05.006 03/09/2004 Line(s) of Business: Current Effective Date: HMO; PPO 06/24/2011 Section: Radiology Place(s) of
Intensity Modulated Radiation Therapy (IMRT) Policy Number: Original Effective Date: MM.05.006 03/09/2004 Line(s) of Business: Current Effective Date: HMO; PPO 06/24/2011 Section: Radiology Place(s) of
IMRT Planning Basics AAMD Student Webinar
 IMRT Planning Basics AAMD Student Webinar March 12, 2014 Karen Chin Snyder, MS Senior Associate Physicist Department of Radiation Oncology Disclosures The presenter has received speaker honoraria from
IMRT Planning Basics AAMD Student Webinar March 12, 2014 Karen Chin Snyder, MS Senior Associate Physicist Department of Radiation Oncology Disclosures The presenter has received speaker honoraria from
Optimization of RapidArc for Head-and-Neck Radiotherapy. Jessica Emily Salazar. Department of Medical Physics Duke University.
 Optimization of RapidArc for Head-and-Neck Radiotherapy by Jessica Emily Salazar Department of Medical Physics Duke University Date: Approved: Shiva Das, Supervisor Ryan McMahon Robert Reiman Thesis submitted
Optimization of RapidArc for Head-and-Neck Radiotherapy by Jessica Emily Salazar Department of Medical Physics Duke University Date: Approved: Shiva Das, Supervisor Ryan McMahon Robert Reiman Thesis submitted
Practice teaching course on head and neck cancer management
 28-29 October 2016 - Saint-Priest en Jarez, France Practice teaching course on head and neck cancer management IMPROVING THE PATIENT S LIFE LIFE THROUGH MEDICAL MEDICAL EDUCATION EDUCATION www.excemed.org
28-29 October 2016 - Saint-Priest en Jarez, France Practice teaching course on head and neck cancer management IMPROVING THE PATIENT S LIFE LIFE THROUGH MEDICAL MEDICAL EDUCATION EDUCATION www.excemed.org
Implementation of advanced RT Techniques
 Implementation of advanced RT Techniques Tibor Major, PhD National Institute of Oncology Budapest, Hungary 2. Kongres radiološke tehnologije, Vukovar, 23-25. September 2016. Current RT equipments at NIO,
Implementation of advanced RT Techniques Tibor Major, PhD National Institute of Oncology Budapest, Hungary 2. Kongres radiološke tehnologije, Vukovar, 23-25. September 2016. Current RT equipments at NIO,
Chapters from Clinical Oncology
 Chapters from Clinical Oncology Lecture notes University of Szeged Faculty of Medicine Department of Oncotherapy 2012. 1 RADIOTHERAPY Technical aspects Dr. Elemér Szil Introduction There are three possibilities
Chapters from Clinical Oncology Lecture notes University of Szeged Faculty of Medicine Department of Oncotherapy 2012. 1 RADIOTHERAPY Technical aspects Dr. Elemér Szil Introduction There are three possibilities
Multi-Case Knowledge-Based IMRT Treatment Planning in Head and Neck Cancer. Shelby Mariah Grzetic. Graduate Program in Medical Physics Duke University
 Multi-Case Knowledge-Based IMRT Treatment Planning in Head and Neck Cancer by Shelby Mariah Grzetic Graduate Program in Medical Physics Duke University Date: Approved: Joseph Y. Lo, Co-Supervisor Shiva
Multi-Case Knowledge-Based IMRT Treatment Planning in Head and Neck Cancer by Shelby Mariah Grzetic Graduate Program in Medical Physics Duke University Date: Approved: Joseph Y. Lo, Co-Supervisor Shiva
The Physics of Oesophageal Cancer Radiotherapy
 The Physics of Oesophageal Cancer Radiotherapy Dr. Philip Wai Radiotherapy Physics Royal Marsden Hospital 1 Contents Brief clinical introduction Imaging and Target definition Dose prescription & patient
The Physics of Oesophageal Cancer Radiotherapy Dr. Philip Wai Radiotherapy Physics Royal Marsden Hospital 1 Contents Brief clinical introduction Imaging and Target definition Dose prescription & patient
Corporate Medical Policy
 Corporate Medical Policy Intensity Modulated Radiation Therapy (IMRT) of Head and Neck File Name: Origination: Last CAP Review: Next CAP Review: Last Review: intensity_modulated_radiation_therapy_imrt_of_head_and_neck
Corporate Medical Policy Intensity Modulated Radiation Therapy (IMRT) of Head and Neck File Name: Origination: Last CAP Review: Next CAP Review: Last Review: intensity_modulated_radiation_therapy_imrt_of_head_and_neck
Radiation Damage Comparison between Intensity Modulated Radiotherapy (IMRT) and Field-in-field (FIF) Technique In Breast Cancer Treatments
 and Field-in-field (FIF) Technique In Breast Cancer Treatments") Radiation Damage Comparison between Intensity Modulated Radiotherapy () and Field-in-field (FIF) Technique In Breast Cancer Treatments Huisi Ai 1 and Hualin Zhang 2 1. Department of Radiation Oncology,
Radiation Damage Comparison between Intensity Modulated Radiotherapy () and Field-in-field (FIF) Technique In Breast Cancer Treatments Huisi Ai 1 and Hualin Zhang 2 1. Department of Radiation Oncology,
IMRT QUESTIONNAIRE. Address: Physicist: Research Associate: Dosimetrist: Responsible Radiation Oncologist(s)
") IMRT QUESTIONNAIRE Institution: Date: / / Address: Physicist: e-mail: Telephone: Fax: Research Associate: email: Telephone: Fax: Dosimetrist: email: Telephone: Fax: Responsible Radiation Oncologist(s)
IMRT QUESTIONNAIRE Institution: Date: / / Address: Physicist: e-mail: Telephone: Fax: Research Associate: email: Telephone: Fax: Dosimetrist: email: Telephone: Fax: Responsible Radiation Oncologist(s)
Alexandria University Faculty of Medicine. Alexandria Journal of Medicine.
 Alexandria Journal of Medicine (2013) 49, 379 384 Alexandria University Faculty of Medicine Alexandria Journal of Medicine www.sciencedirect.com ORIGINAL ARTICLE Three dimensional conformal postoperative
Alexandria Journal of Medicine (2013) 49, 379 384 Alexandria University Faculty of Medicine Alexandria Journal of Medicine www.sciencedirect.com ORIGINAL ARTICLE Three dimensional conformal postoperative
Master s science Thesis. Evaluation of gantry angle optimization for IMRT treatment planning systems using the Pareto front approach.
 Master s science Thesis Evaluation of gantry angle optimization for IMRT treatment planning systems using the Pareto front approach Maria Thor Supervisors: Anna Karlsson 1, Claus Behrens 1, Per Engström
Master s science Thesis Evaluation of gantry angle optimization for IMRT treatment planning systems using the Pareto front approach Maria Thor Supervisors: Anna Karlsson 1, Claus Behrens 1, Per Engström
Automated Plan Quality Check with Scripting. Rajesh Gutti, Ph.D. Clinical Medical Physicist
 Automated Plan Quality Check with Scripting Rajesh Gutti, Ph.D. Clinical Medical Physicist Veera.Gutti@BSWHealth.org Outline Introduction - BSW Automation in Treatment planning Eclipse Scripting API Script
Automated Plan Quality Check with Scripting Rajesh Gutti, Ph.D. Clinical Medical Physicist Veera.Gutti@BSWHealth.org Outline Introduction - BSW Automation in Treatment planning Eclipse Scripting API Script
Protons for Head and Neck Cancer. William M Mendenhall, M.D.
 Protons for Head and Neck Cancer William M Mendenhall, M.D. Protons for Head and Neck Cancer Potential Advantages: Reduce late complications via more conformal dose distributions Likely to be the major
Protons for Head and Neck Cancer William M Mendenhall, M.D. Protons for Head and Neck Cancer Potential Advantages: Reduce late complications via more conformal dose distributions Likely to be the major
Radiation Therapy for breast with Tomotherapy: When?
 Radiation Therapy for breast with Tomotherapy: When? Roberto Orecchia Chair of Radiation Therapy at the University of Milan, IEO & CNAO Quarto incontro italo-francese sul carcinoma mammario: Problematiche
Radiation Therapy for breast with Tomotherapy: When? Roberto Orecchia Chair of Radiation Therapy at the University of Milan, IEO & CNAO Quarto incontro italo-francese sul carcinoma mammario: Problematiche
Knowledge-Based IMRT Treatment Planning for Prostate Cancer: Experience with 101. Cases from Duke Clinic. Deon Martina Dick
 Knowledge-Based IMRT Treatment Planning for Prostate Cancer: Experience with 101 Cases from Duke Clinic by Deon Martina Dick Department of Medical Physics Duke University Date: Approved: Joseph Lo, Chair
Knowledge-Based IMRT Treatment Planning for Prostate Cancer: Experience with 101 Cases from Duke Clinic by Deon Martina Dick Department of Medical Physics Duke University Date: Approved: Joseph Lo, Chair
Lung Spine Phantom. Guidelines for Planning and Irradiating the IROC Spine Phantom. MARCH 2014
 Lung Spine Phantom Guidelines for Planning and Irradiating the IROC Spine Phantom. MARCH 2014 The study groups are requesting that each institution keep the phantom for no more than 2 week. During this
Lung Spine Phantom Guidelines for Planning and Irradiating the IROC Spine Phantom. MARCH 2014 The study groups are requesting that each institution keep the phantom for no more than 2 week. During this
Advances in external beam radiotherapy
 International Conference on Modern Radiotherapy: Advances and Challenges in Radiation Protection of Patients Advances in external beam radiotherapy New techniques, new benefits and new risks Michael Brada
International Conference on Modern Radiotherapy: Advances and Challenges in Radiation Protection of Patients Advances in external beam radiotherapy New techniques, new benefits and new risks Michael Brada
MANAGEMENT OF CA HYPOPHARYNX
 MANAGEMENT OF CA HYPOPHARYNX GENERAL TREATMENT RECOMMENDATIONS BASED ON HYPOPHARYNX TUMOR STAGE For patients presenting with early-stage definitive radiotherapy alone or voice-preserving surgery are viable
MANAGEMENT OF CA HYPOPHARYNX GENERAL TREATMENT RECOMMENDATIONS BASED ON HYPOPHARYNX TUMOR STAGE For patients presenting with early-stage definitive radiotherapy alone or voice-preserving surgery are viable
4/25/2018. Proton Therapy for Head and Neck Cancer: The Future is Now. Disclosures. Overview. Physical limitations of photons
 Proton Therapy for Head and Neck Cancer: The Future is Now Michael Chuong, MD Radiation Oncologist Disclosures None Overview Physical limitations of photons Dosimetric/clinical proton data for HNC Proton
Proton Therapy for Head and Neck Cancer: The Future is Now Michael Chuong, MD Radiation Oncologist Disclosures None Overview Physical limitations of photons Dosimetric/clinical proton data for HNC Proton
IMAT: intensity-modulated arc therapy
 : intensity-modulated arc therapy M. Iori S. Maria Nuova Hospital, Medical Physics Department Reggio Emilia, Italy 1 Topics of the talk Rotational IMRT techniques: modalities & dedicated inverse-planning
: intensity-modulated arc therapy M. Iori S. Maria Nuova Hospital, Medical Physics Department Reggio Emilia, Italy 1 Topics of the talk Rotational IMRT techniques: modalities & dedicated inverse-planning
3D-CRT Breast Cancer Planning
 3D-CRT Breast Cancer Planning Tips and Tricks Bednář, V. 3D-CRT Obsolete or not? There are more advanced techniques than 3D-CRT, but 3D-CRT has some advantages: Availability and price Forward planning
3D-CRT Breast Cancer Planning Tips and Tricks Bednář, V. 3D-CRT Obsolete or not? There are more advanced techniques than 3D-CRT, but 3D-CRT has some advantages: Availability and price Forward planning
State of the art for radiotherapy of SCCHN
 State of the art for radiotherapy of SCCHN Less side effects Cured More organ & function preservation Head & neck cancer = 42 000 new cases / year in Europe Not cured Local failure Distant failure More
State of the art for radiotherapy of SCCHN Less side effects Cured More organ & function preservation Head & neck cancer = 42 000 new cases / year in Europe Not cured Local failure Distant failure More
Vincent Grégoire, Radiation Oncologist, Brussels, Belgium Cai Grau, Radiation Oncologist, Aarhus, Denmark. Tunis March 2017
 Guidelines for the delineation of the primary tumour Clinical Target Volumes (CTV) in laryngeal, hypopharyngeal, oropharyngeal and oral cavity SCC (version 5.1) Vincent Grégoire, Radiation Oncologist,
Guidelines for the delineation of the primary tumour Clinical Target Volumes (CTV) in laryngeal, hypopharyngeal, oropharyngeal and oral cavity SCC (version 5.1) Vincent Grégoire, Radiation Oncologist,
Helical Tomotherapy Experience. TomoTherapy Whole Brain Head & Neck Prostate Lung Summary. HI-ART TomoTherapy System. HI-ART TomoTherapy System
 The Challenges Associated with Differential Dose Delivery using IMRT Chester Ramsey, Ph.D. Director of Medical Physics Thompson Cancer Center Knoxville, Tennessee, U.S.A Collaborators Chester Ramsey, Ph.D.
The Challenges Associated with Differential Dose Delivery using IMRT Chester Ramsey, Ph.D. Director of Medical Physics Thompson Cancer Center Knoxville, Tennessee, U.S.A Collaborators Chester Ramsey, Ph.D.
Address for Correspondence: Department of Medical Physics, Khwaja Yunus Ali University, Enayetpur, Sirajgonj ,
 ORIGINAL ARTICLE Dosimetric Comparison of Different 3DCRT Techniques in Left Breast Cancer Radiotherapy Planning Abdus Sattar Mollah 1 and Meher Niger Sharmin 2 1 Department of Medical Physics, KhwajaYunus
ORIGINAL ARTICLE Dosimetric Comparison of Different 3DCRT Techniques in Left Breast Cancer Radiotherapy Planning Abdus Sattar Mollah 1 and Meher Niger Sharmin 2 1 Department of Medical Physics, KhwajaYunus
A Dosimetric Comparison of Whole-Lung Treatment Techniques. in the Pediatric Population
 A Dosimetric Comparison of Whole-Lung Treatment Techniques in the Pediatric Population Corresponding Author: Christina L. Bosarge, B.S., R.T. (R) (T) Indiana University School of Medicine Department of
A Dosimetric Comparison of Whole-Lung Treatment Techniques in the Pediatric Population Corresponding Author: Christina L. Bosarge, B.S., R.T. (R) (T) Indiana University School of Medicine Department of
Page 1. Helical (Spiral) Tomotherapy. UW Helical Tomotherapy Unit. Helical (Spiral) Tomotherapy. MVCT of an Anesthetized Dog with a Sinus Tumor
 Tomotherapy. UW Helical Tomotherapy Unit. Helical (Spiral) Tomotherapy. MVCT of an Anesthetized Dog with a Sinus Tumor") Helical (Spiral) Tomotherapy Novel Clinical Applications of IMRT Linac Ring Gantry CT Detector X-Ray Fan Beam Binary Multileaf Collimator Binary MLC Leaves James S Welsh, MS, MD Department of Human Oncology
Helical (Spiral) Tomotherapy Novel Clinical Applications of IMRT Linac Ring Gantry CT Detector X-Ray Fan Beam Binary Multileaf Collimator Binary MLC Leaves James S Welsh, MS, MD Department of Human Oncology
IROC Liver Phantom. Guidelines for Planning and Irradiating the IROC Liver Phantom. Revised July 2015
 IROC Liver Phantom Guidelines for Planning and Irradiating the IROC Liver Phantom. Revised July 2015 The study groups are requests that each institution keep the phantom for no more than 2 weeks. During
IROC Liver Phantom Guidelines for Planning and Irradiating the IROC Liver Phantom. Revised July 2015 The study groups are requests that each institution keep the phantom for no more than 2 weeks. During
A TREATMENT PLANNING STUDY COMPARING VMAT WITH 3D CONFORMAL RADIOTHERAPY FOR PROSTATE CANCER USING PINNACLE PLANNING SYSTEM *
 Romanian Reports in Physics, Vol. 66, No. 2, P. 394 400, 2014 A TREATMENT PLANNING STUDY COMPARING VMAT WITH 3D CONFORMAL RADIOTHERAPY FOR PROSTATE CANCER USING PINNACLE PLANNING SYSTEM * D. ADAM 1,2,
Romanian Reports in Physics, Vol. 66, No. 2, P. 394 400, 2014 A TREATMENT PLANNING STUDY COMPARING VMAT WITH 3D CONFORMAL RADIOTHERAPY FOR PROSTATE CANCER USING PINNACLE PLANNING SYSTEM * D. ADAM 1,2,
The role of Radiation Oncologist: Hi-tech treatments for liver metastases
 The role of Radiation Oncologist: Hi-tech treatments for liver metastases Icro Meattini, MD Radiotherapy-Oncology Unit AOU Careggi Hospital Florence University, Italy Liver Metastases - Background The
The role of Radiation Oncologist: Hi-tech treatments for liver metastases Icro Meattini, MD Radiotherapy-Oncology Unit AOU Careggi Hospital Florence University, Italy Liver Metastases - Background The
Intensity Modulated RadioTherapy
 Intensity Modulated RadioTherapy A clinical application of a small accelerator University Medical Center Groningen A.A. van t Veld PhD I. Hoveijn PhD part 1 part2 CERN/KVI accelerator school, Zeegse, June
Intensity Modulated RadioTherapy A clinical application of a small accelerator University Medical Center Groningen A.A. van t Veld PhD I. Hoveijn PhD part 1 part2 CERN/KVI accelerator school, Zeegse, June
Outline. Contour quality control. Dosimetric impact of contouring errors and variability in Intensity Modulated Radiation Therapy (IMRT)
") Dosimetric impact of contouring errors and variability in Intensity Modulated Radiation Therapy (IMRT) James Kavanaugh, MS DABR Department of Radiation Oncology Division of Medical Physics Outline Importance
Dosimetric impact of contouring errors and variability in Intensity Modulated Radiation Therapy (IMRT) James Kavanaugh, MS DABR Department of Radiation Oncology Division of Medical Physics Outline Importance
Evaluation of Monaco treatment planning system for hypofractionated stereotactic volumetric arc radiotherapy of multiple brain metastases
 Evaluation of Monaco treatment planning system for hypofractionated stereotactic volumetric arc radiotherapy of multiple brain metastases CASE STUDY Institution: Odette Cancer Centre Location: Sunnybrook
Evaluation of Monaco treatment planning system for hypofractionated stereotactic volumetric arc radiotherapy of multiple brain metastases CASE STUDY Institution: Odette Cancer Centre Location: Sunnybrook
RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS. Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1.
 RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1. 550 000 NEW PATIENTS/YEAR WITH HEAD AND NECK CANCER ALL
RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1. 550 000 NEW PATIENTS/YEAR WITH HEAD AND NECK CANCER ALL
SBRT fundamentals. Outline 8/2/2012. Stereotactic Body Radiation Therapy Quality Assurance Educational Session
 Stereotactic Body Radiation Therapy Quality Assurance Educational Session J Perks PhD, UC Davis Medical Center, Sacramento CA SBRT fundamentals Extra-cranial treatments Single or small number (2-5) of
Stereotactic Body Radiation Therapy Quality Assurance Educational Session J Perks PhD, UC Davis Medical Center, Sacramento CA SBRT fundamentals Extra-cranial treatments Single or small number (2-5) of
IROC Head and Neck Phantom. Guidelines for Planning and Irradiating the IROC IMRT Phantom. Revised MARCH 2014
 IROC Head and Neck Phantom Guidelines for Planning and Irradiating the IROC IMRT Phantom. Revised MARCH 2014 The study groups are requesting that each institution keep the phantom for a period of time
IROC Head and Neck Phantom Guidelines for Planning and Irradiating the IROC IMRT Phantom. Revised MARCH 2014 The study groups are requesting that each institution keep the phantom for a period of time
Intensity modulated radiotherapy (IMRT) for treatment of post-operative high grade glioma in the right parietal region of brain
 for treatment of post-operative high grade glioma in the right parietal region of brain") 1 Carol Boyd March Case Study March 11, 2013 Intensity modulated radiotherapy (IMRT) for treatment of post-operative high grade glioma in the right parietal region of brain History of Present Illness:
1 Carol Boyd March Case Study March 11, 2013 Intensity modulated radiotherapy (IMRT) for treatment of post-operative high grade glioma in the right parietal region of brain History of Present Illness:
Kenny Guida, DMP, DABR March 21 st, 2015
 Kenny Guida, DMP, DABR March 21 st, 2015 Breast Cancer Treatment planning and delivery Hypofractionation Trials Hybrid Planning History Techniques RTOG 1005 Trial Hybrid-VMAT Research project 3D Tangents
Kenny Guida, DMP, DABR March 21 st, 2015 Breast Cancer Treatment planning and delivery Hypofractionation Trials Hybrid Planning History Techniques RTOG 1005 Trial Hybrid-VMAT Research project 3D Tangents
Feasibility of the partial-single arc technique in RapidArc planning for prostate cancer treatment
 Chinese Journal of Cancer Original Article Feasibility of the partial-single arc technique in RapidArc planning for prostate cancer treatment Suresh Rana 1 and ChihYao Cheng 2 Abstract The volumetric modulated
Chinese Journal of Cancer Original Article Feasibility of the partial-single arc technique in RapidArc planning for prostate cancer treatment Suresh Rana 1 and ChihYao Cheng 2 Abstract The volumetric modulated
A treatment planning study comparing Elekta VMAT and fixed field IMRT using the varian treatment planning system eclipse
 Peters et al. Radiation Oncology 2014, 9:153 RESEARCH Open Access A treatment planning study comparing Elekta VMAT and fixed field IMRT using the varian treatment planning system eclipse Samuel Peters
Peters et al. Radiation Oncology 2014, 9:153 RESEARCH Open Access A treatment planning study comparing Elekta VMAT and fixed field IMRT using the varian treatment planning system eclipse Samuel Peters
Guidelines for the use of inversely planned treatment techniques in Clinical Trials: IMRT, VMAT, TomoTherapy
 Guidelines for the use of inversely planned treatment techniques in Clinical Trials: IMRT, VMAT, TomoTherapy VERSION 2.1 April 2015 Table of Contents Abbreviations & Glossary... 3 Executive Summary...
Guidelines for the use of inversely planned treatment techniques in Clinical Trials: IMRT, VMAT, TomoTherapy VERSION 2.1 April 2015 Table of Contents Abbreviations & Glossary... 3 Executive Summary...
Accuracy Requirements and Uncertainty Considerations in Radiation Therapy
 Departments of Oncology and Medical Biophysics Accuracy Requirements and Uncertainty Considerations in Radiation Therapy Introduction and Overview 6 August 2013 Jacob (Jake) Van Dyk Conformality 18 16
Departments of Oncology and Medical Biophysics Accuracy Requirements and Uncertainty Considerations in Radiation Therapy Introduction and Overview 6 August 2013 Jacob (Jake) Van Dyk Conformality 18 16
Protocol of Radiotherapy for Head and Neck Cancer
 106 年 12 月修訂 Protocol of Radiotherapy for Head and Neck Cancer Indication of radiotherapy Indication of definitive radiotherapy with or without chemotherapy (1) Resectable, but medically unfit, or high
106 年 12 月修訂 Protocol of Radiotherapy for Head and Neck Cancer Indication of radiotherapy Indication of definitive radiotherapy with or without chemotherapy (1) Resectable, but medically unfit, or high
ICRU Report 91 Was ist neu, was ändert sich?
 DEGRO Stereotaxie Meeting 21.10.2017 ICRU Report 91 Was ist neu, was ändert sich? Lotte Wilke, Stephanie Tanadini-Lang, Matthias Guckenberger Klinik für Radio-Onkologie, Universitätsspital Zürich History
DEGRO Stereotaxie Meeting 21.10.2017 ICRU Report 91 Was ist neu, was ändert sich? Lotte Wilke, Stephanie Tanadini-Lang, Matthias Guckenberger Klinik für Radio-Onkologie, Universitätsspital Zürich History
Leila E. A. Nichol Royal Surrey County Hospital
 2 nd UK and Ireland Dosimetry Check User Meeting Symposium Clatterbridge Cancer Centre, 24 th October 2012 Leila E. A. Nichol Royal Surrey County Hospital Leila.Nichol@nhs.net *My experience with Dosimetry
2 nd UK and Ireland Dosimetry Check User Meeting Symposium Clatterbridge Cancer Centre, 24 th October 2012 Leila E. A. Nichol Royal Surrey County Hospital Leila.Nichol@nhs.net *My experience with Dosimetry
RapidArc vs Conventional IMRT for Head and Neck Cancer Irradiation: Is Faster Necessary Better?
 DOI:10.22034/APJCP.2018.19.1.207 RESEARCH ARTICLE Editorial Process: Submission:10/05/2017 Acceptance:12/13/2017 RapidArc vs Conventional IMRT for Head and Neck Cancer Irradiation: Is Faster Necessary
DOI:10.22034/APJCP.2018.19.1.207 RESEARCH ARTICLE Editorial Process: Submission:10/05/2017 Acceptance:12/13/2017 RapidArc vs Conventional IMRT for Head and Neck Cancer Irradiation: Is Faster Necessary
Completion of Treatment Planning. Eugene Lief, Ph.D. Christ Hospital Jersey City, New Jersey USA
 Completion of Treatment Planning Eugene Lief, Ph.D. Christ Hospital Jersey City, New Jersey USA Outline Entering Prescription Plan Printout Print and Transfer DRR Segment BEV Export to R&V Physician approval
Completion of Treatment Planning Eugene Lief, Ph.D. Christ Hospital Jersey City, New Jersey USA Outline Entering Prescription Plan Printout Print and Transfer DRR Segment BEV Export to R&V Physician approval
REVISITING ICRU VOLUME DEFINITIONS. Eduardo Rosenblatt Vienna, Austria
 REVISITING ICRU VOLUME DEFINITIONS Eduardo Rosenblatt Vienna, Austria Objective: To introduce target volumes and organ at risk concepts as defined by ICRU. 3D-CRT is the standard There was a need for a
REVISITING ICRU VOLUME DEFINITIONS Eduardo Rosenblatt Vienna, Austria Objective: To introduce target volumes and organ at risk concepts as defined by ICRU. 3D-CRT is the standard There was a need for a
The Evolution of SBRT and Hypofractionation in Thoracic Radiation Oncology
 The Evolution of SBRT and Hypofractionation in Thoracic Radiation Oncology (specifically, lung cancer) 2/10/18 Jeffrey Kittel, MD Radiation Oncology, Aurora St. Luke s Medical Center Outline The history
The Evolution of SBRT and Hypofractionation in Thoracic Radiation Oncology (specifically, lung cancer) 2/10/18 Jeffrey Kittel, MD Radiation Oncology, Aurora St. Luke s Medical Center Outline The history
RPC Liver Phantom Highly Conformal Stereotactic Body Radiation Therapy
 RPC Liver Phantom Highly Conformal Stereotactic Body Radiation Therapy Guidelines for Planning and Irradiating the RPC Liver Phantom. Revised Dec 2005 Credentialing for this protocol requires four steps:
RPC Liver Phantom Highly Conformal Stereotactic Body Radiation Therapy Guidelines for Planning and Irradiating the RPC Liver Phantom. Revised Dec 2005 Credentialing for this protocol requires four steps:
A guide to using multi-criteria optimization (MCO) for IMRT planning in RayStation
 for IMRT planning in RayStation") A guide to using multi-criteria optimization (MCO) for IMRT planning in RayStation By David Craft Massachusetts General Hospital, Department of Radiation Oncology Revised: August 30, 2011 Single Page Summary
A guide to using multi-criteria optimization (MCO) for IMRT planning in RayStation By David Craft Massachusetts General Hospital, Department of Radiation Oncology Revised: August 30, 2011 Single Page Summary
Additional Questions for Review 2D & 3D
 Additional Questions for Review 2D & 3D 1. For a 4-field box technique, which of the following will deliver the lowest dose to the femoral heads? a. 100 SSD, equal dmax dose to all fields b. 100 SSD, equal
Additional Questions for Review 2D & 3D 1. For a 4-field box technique, which of the following will deliver the lowest dose to the femoral heads? a. 100 SSD, equal dmax dose to all fields b. 100 SSD, equal
IROC Head and Neck Phantom. Guidelines for Planning and Irradiating the IROC IMRT Phantom. Revised April 2014
 IROC Head and Neck Phantom Guidelines for Planning and Irradiating the IROC IMRT Phantom. Revised April 2014 The IROC Houston is requesting that each institution keep the phantom for two weeks. During
IROC Head and Neck Phantom Guidelines for Planning and Irradiating the IROC IMRT Phantom. Revised April 2014 The IROC Houston is requesting that each institution keep the phantom for two weeks. During
Clinical Impact of Couch Top and Rails on IMRT and Arc Therapy
 Texas Medical Center Library DigitalCommons@TMC UT GSBS Dissertations and Theses (Open Access) Graduate School of Biomedical Sciences 8-2011 Clinical Impact of Couch Top and Rails on IMRT and Arc Therapy
Texas Medical Center Library DigitalCommons@TMC UT GSBS Dissertations and Theses (Open Access) Graduate School of Biomedical Sciences 8-2011 Clinical Impact of Couch Top and Rails on IMRT and Arc Therapy
A review of RTTQA audit. Karen Venables
 A review of RTTQA audit Karen Venables CHART 8 hours on the machine Chart cord CHART QA: Phantoms(1 st use of anatomical phantoms) Designed for treatments in Bronchus and Head and Neck (2D only) Outlines
A review of RTTQA audit Karen Venables CHART 8 hours on the machine Chart cord CHART QA: Phantoms(1 st use of anatomical phantoms) Designed for treatments in Bronchus and Head and Neck (2D only) Outlines
Changing Paradigms in Radiotherapy
 Changing Paradigms in Radiotherapy Marco van Vulpen, MD, PhD Mouldroomdag-2015 Towards the elimination of invasion 1 NIH opinion on the future of oncology Twenty-five years from now,i hope that we won
Changing Paradigms in Radiotherapy Marco van Vulpen, MD, PhD Mouldroomdag-2015 Towards the elimination of invasion 1 NIH opinion on the future of oncology Twenty-five years from now,i hope that we won
A STUDY OF PLANNING DOSE CONSTRAINTS FOR TREATMENT OF NASOPHARYNGEAL CARCINOMA USING A COMMERCIAL INVERSE TREATMENT PLANNING SYSTEM
 doi:10.1016/j.ijrobp.2004.02.040 Int. J. Radiation Oncology Biol. Phys., Vol. 59, No. 3, pp. 886 896, 2004 Copyright 2004 Elsevier Inc. Printed in the USA. All rights reserved 0360-3016/04/$ see front
doi:10.1016/j.ijrobp.2004.02.040 Int. J. Radiation Oncology Biol. Phys., Vol. 59, No. 3, pp. 886 896, 2004 Copyright 2004 Elsevier Inc. Printed in the USA. All rights reserved 0360-3016/04/$ see front
Partial Breast Irradiation using adaptive MRgRT
 Partial Breast Irradiation using adaptive MRgRT Shyama Tetar, radiation-oncologist VUmc Amsterdam 15-12-2017 5 th Vumc SBRT symposium 2017 Current practice Breast conserving treatment (BCT) Breast conserving
Partial Breast Irradiation using adaptive MRgRT Shyama Tetar, radiation-oncologist VUmc Amsterdam 15-12-2017 5 th Vumc SBRT symposium 2017 Current practice Breast conserving treatment (BCT) Breast conserving
BLADDER RADIOTHERAPY PLANNING DOCUMENT
 A 2X2 FACTORIAL RANDOMISED PHASE III STUDY COMPARING STANDARD VERSUS REDUCED VOLUME RADIOTHERAPY WITH AND WITHOUT SYNCHRONOUS CHEMOTHERAPY IN MUSCLE INVASIVE BLADDER CANCER (ISRCTN 68324339) BLADDER RADIOTHERAPY
A 2X2 FACTORIAL RANDOMISED PHASE III STUDY COMPARING STANDARD VERSUS REDUCED VOLUME RADIOTHERAPY WITH AND WITHOUT SYNCHRONOUS CHEMOTHERAPY IN MUSCLE INVASIVE BLADDER CANCER (ISRCTN 68324339) BLADDER RADIOTHERAPY
Can we deliver the dose distribution we plan in HDR-Brachytherapy of Prostate Cancer?
 Can we deliver the dose distribution we plan in HDR-Brachytherapy of Prostate Cancer? Dimos Baltas Dept. of Medical Physics & Engineering, Strahlenklinik, Klinikum Offenbach GmbH 63069 Offenbach, Germany
Can we deliver the dose distribution we plan in HDR-Brachytherapy of Prostate Cancer? Dimos Baltas Dept. of Medical Physics & Engineering, Strahlenklinik, Klinikum Offenbach GmbH 63069 Offenbach, Germany
Linac or Non-Linac Demystifying And Decoding The Physics Of SBRT/SABR
 Linac or Non-Linac Demystifying And Decoding The Physics Of SBRT/SABR PhD, FAAPM, FACR, FASTRO Department of Radiation Oncology Indiana University School of Medicine Indianapolis, IN, USA Indra J. Das,
Linac or Non-Linac Demystifying And Decoding The Physics Of SBRT/SABR PhD, FAAPM, FACR, FASTRO Department of Radiation Oncology Indiana University School of Medicine Indianapolis, IN, USA Indra J. Das,
Int J Clin Exp Med 2015;8(9): /ISSN: /IJCEM Gang Zhou, Yanze Sun, Jianjun Qian, Ye Tian, Xueguan Lu
: /ISSN: /IJCEM Gang Zhou, Yanze Sun, Jianjun Qian, Ye Tian, Xueguan Lu") Int J Clin Exp Med 2015;8(9):15975-15982 www.ijcem.com /ISSN:1940-5901/IJCEM0009616 Original Article The dosimetric comparison of the radiotherapeutic plans between composite and synchronous approaches
Int J Clin Exp Med 2015;8(9):15975-15982 www.ijcem.com /ISSN:1940-5901/IJCEM0009616 Original Article The dosimetric comparison of the radiotherapeutic plans between composite and synchronous approaches
IROC Lung Phantom 3D CRT / IMRT. Guidelines for Planning and Irradiating the IROC Lung Phantom. Revised Dec 2015
 IROC Lung Phantom 3D CRT / IMRT Guidelines for Planning and Irradiating the IROC Lung Phantom. Revised Dec 2015 The IROC requests that each institution keep the phantom for no more than 2 weeks. During
IROC Lung Phantom 3D CRT / IMRT Guidelines for Planning and Irradiating the IROC Lung Phantom. Revised Dec 2015 The IROC requests that each institution keep the phantom for no more than 2 weeks. During
Dosimetric Effects of Using Generalized Equivalent Uniform Dose (geud) in Plan Optimization
 in Plan Optimization") Dosimetric Effects of Using Generalized Equivalent Uniform Dose (geud) in Plan Optimization Ontida Apinorasethkul, MS, CMD AAMD Indianapolis June 14, 2017 Disclaimer This presentation is not sponsored
Dosimetric Effects of Using Generalized Equivalent Uniform Dose (geud) in Plan Optimization Ontida Apinorasethkul, MS, CMD AAMD Indianapolis June 14, 2017 Disclaimer This presentation is not sponsored
PEDIATRIC ORBITAL TUMORS RADIOTHERAPY PLANNING
 PEDIATRIC ORBITAL TUMORS RADIOTHERAPY PLANNING ANATOMY ANATOMY CONT ANATOMY CONT. ANATOMY CONT. EYE OF A CHILD Normal tissue tolerance doses (in conventional #) TD 5/5 TD 50/5 Endpoint Gy Gy Optic nerve
PEDIATRIC ORBITAL TUMORS RADIOTHERAPY PLANNING ANATOMY ANATOMY CONT ANATOMY CONT. ANATOMY CONT. EYE OF A CHILD Normal tissue tolerance doses (in conventional #) TD 5/5 TD 50/5 Endpoint Gy Gy Optic nerve
A feedback constraint optimization method for intensity-modulated radiation therapy of nasopharyngeal carcinoma
 ONCOLOGY LETTERS 10: 2043-2050, 2015 A feedback constraint optimization method for intensity-modulated radiation therapy of nasopharyngeal carcinoma YONGWU LI, XIAONAN SUN, QI WANG, QINXUAN ZHOU, BENXING
ONCOLOGY LETTERS 10: 2043-2050, 2015 A feedback constraint optimization method for intensity-modulated radiation therapy of nasopharyngeal carcinoma YONGWU LI, XIAONAN SUN, QI WANG, QINXUAN ZHOU, BENXING
Protocol of Radiotherapy for Small Cell Lung Cancer
 107 年 12 月修訂 Protocol of Radiotherapy for Small Cell Lung Cancer Indication of radiotherapy Limited stage: AJCC (8th edition) stage I-III (T any, N any, M0) that can be safely treated with definitive RT
107 年 12 月修訂 Protocol of Radiotherapy for Small Cell Lung Cancer Indication of radiotherapy Limited stage: AJCC (8th edition) stage I-III (T any, N any, M0) that can be safely treated with definitive RT
NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) BONE (Version , 03/28/18)
 BONE (Version , 03/28/18)") BONE (Version 2.2018, 03/28/18) NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) Radiation Therapy Specialized techniques such as intensity-modulated RT (IMRT); particle beam RT with protons, carbon ions,
BONE (Version 2.2018, 03/28/18) NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) Radiation Therapy Specialized techniques such as intensity-modulated RT (IMRT); particle beam RT with protons, carbon ions,
Direct machine parameter optimization for intensity modulated radiation therapy (IMRT) of oropharyngeal cancer a planning study
 of oropharyngeal cancer a planning study") JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 10, NUMBER 4, FALL 2009 Direct machine parameter optimization for intensity modulated radiation therapy (IMRT) of oropharyngeal cancer a planning study
JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 10, NUMBER 4, FALL 2009 Direct machine parameter optimization for intensity modulated radiation therapy (IMRT) of oropharyngeal cancer a planning study
Specification of Tumor Dose. Prescription dose. Purpose
 Specification of Tumor Dose George Starkschall, Ph.D. Department of Radiation Physics U.T. M.D. Anderson Cancer Center Prescription dose What do we mean by a dose prescription of 63 Gy? Isocenter dose
Specification of Tumor Dose George Starkschall, Ph.D. Department of Radiation Physics U.T. M.D. Anderson Cancer Center Prescription dose What do we mean by a dose prescription of 63 Gy? Isocenter dose