Detection of the motor points of the abdominal muscles
|
|
|
- Bartholomew Eaton
- 6 years ago
- Views:
Transcription
1 Eur Eur J Appl Physiol manuscript No. (will (to be inserted by the editor) Detection of the motor points of the abdominal muscles E.J. McCaughey. A.N. McLean. D.B. Allan. H. Gollee. Recieved: date/ Accepted:date Abstract Purpose: Abdominal Functional Electrical Stimulation (AFES) is a technique intended to improve respiratory function in tetraplegia where breathing is affected due to abdominal muscle paralysis. Although it is known that optimal muscle contraction is achieved when electrical stimulation is applied close to the muscle motor point, AFES studies have used a variety of electrode positions. This study aims to investigate the feasibility of using Neuromuscular Electrical Stimulation to detect the motor points of the abdominal muscles, and to evaluate the intrasubject repeatability and intersubject uniformity of their positions, to find the most suitable AFES electrode location. Methods: Low frequency stimulation (0.5 Hz) was applied to the abdominal muscles of 10 able bodied and 5 tetraplegic participants. The electrode positions which achieved the strongest muscle contractions were recorded as the motor point positions, with measurements repeated once. For 5 able bodied participants assessments were repeated after 18 months, in seated and supine positions. Results: Intersubject uniformity ranged from 2.8% to 8.8%. Motor point positions were identified with intrasubject repeatability of <1.7 cm, deemed adequate relative to standard AFES electrode size. Intrasubject repeatability shows motor point positions changed little (<1.7 cm) after 18 months but varied between seated and supine positions with repeatability of up to 3.1 cm. Conclusions: A simple technique to locate the motor points of the abdominal muscles is presented and shown to have an adequate intrasubject repeatability, enabling the optimum AFES electrode location to be identified for each user. Key words: Abdominal; Electrical stimulation; Motor point; Respiratory; Spinal cord injury E.J. McCaughey. Henrik Gollee. Centre for Rehabilitation Engineering, School of Engineering, University of Glasgow, Glasgow, Scotland, UK Tel.: Fax: e.mccaughey.1@research.gla.ac.uk A.N. McLean. D.B. Allan. Queen Elizabeth National Spinal Injuries Unit, Southern General Hospital, Glasgow, Scotland, UK
2 Abbreviations AFES: Abdominal Functional Electrical Stimulation EO: External Oblique FES: Functional Electrical Stimulation NMES: Neuromuscular Electrical Stimulation RA: Rectus Abdominis 1 Introduction Neuromuscular Electrical Stimulation (NMES) is a method of applying short electrical pulse trains to a motor nerve, causing contraction of the associated muscle. The term Functional Electrical Stimulation (FES) is used when NMES aims to restore lost or damaged function (Moe and Post, 1962), caused by neurological damage such as that resulting from stroke or spinal cord injury. An injury to the cervical region of the spinal cord can lead to paralysis affecting all four limbs, termed tetraplegia. In tetraplegia paralysis also affects the major breathing muscles, with the result that many people with this condition have poor respiratory function. Respiratory infections associated with this poor respiratory function are a leading cause of rehospitalisation for this population (Cardenas et al, 2004). For most people with tetraplegia exhalation is compromised due to paralysis of the abdominal muscles, affecting cough and forced exhalation. Transcutaneous FES applied to the abdominal muscles, termed Abdominal Functional Electrical Stimulation (AFES), has been shown to improve respiratory function in this population (Butler et al, 2011; Gollee et al, 2007; Langbein et al, 2001; Lee et al, 2008; McLachlan et al, 2013; Taylor et al, 2002). These studies have used a variety of empirically derived electrode locations, designed to stimulate the Rectus Abdominis (RA) and/or External Oblique (EO) muscles. When using transcutaneous FES the most robust muscle contraction, at the lowest stimulation level, can be achieved when the stimulating electrodes are located at the motor point, defined as the point on the skin above the muscle where an electrical pulse applied transcutaneously evokes a muscle twitch with the least injected current (Gobbo et al, 2014). Gobbo et al (2011, 2014) have shown that placing the electrodes at the motor point maximises force output and minimises discomfort. Botter et al (2011) suggest that motor point charts, such as those often provided with an FES device, may be too general to enable accurate identification of the precise motor point location for an individual to achieve a consistent muscle contraction across a group. This conclusion was reached after using NMES to identify the position of the motor points of muscles in the leg and finding that these motor point positions had generally poor intersubject uniformity. While anatomical charts showing the location of the motor points for the limbs have long been available (Reid, 1920), less information is available about the motor points of the abdominal wall muscles. Bell et al (2007) studied the anatomical structures underlying the sites at which AFES is usually applied. They found that, although the electrode location approximately corresponded to the location of the neuromuscular structures innervating the abdominal muscles, there were significant differences in these structures in different subjects. The location of the motor points of the abdominal muscles, how they vary between subjects and whether they are time and posture dependent has not been
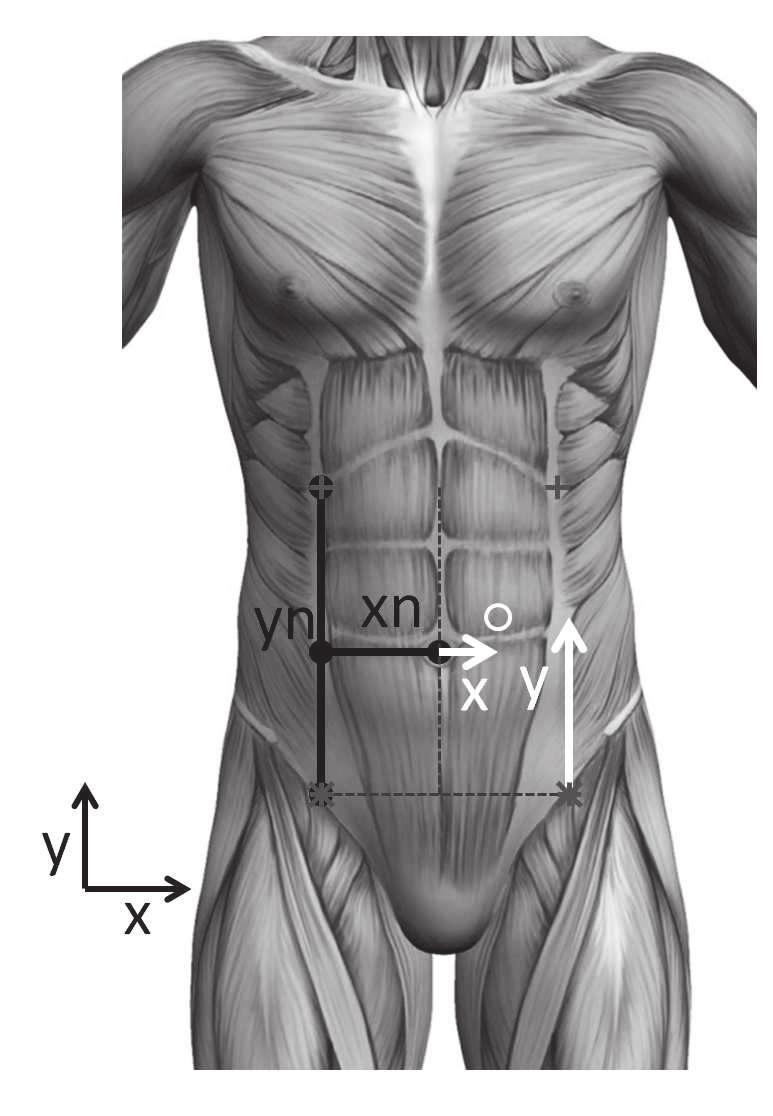
3 investigated in detail. This information would be useful in optimising the electrode placement in AFES, and could help to understand variations in the effectiveness of AFES in different settings. In this study NMES was used to identify the positions of the motor points of the abdominal muscles in able bodied and tetraplegic participants. The aims of this study were (i) to assess the feasibility of using NMES to detect the position of the motor points of the RA and EO muscles and the repeatability of this technique, (ii) to evaluate the intersubject uniformity of these motor point positions, and (iii) to evaluate how the motor point locations depend on posture and whether they vary with time. 2 Methods 2.1 Participants Ten able bodied (5 males, age 29.5±7.9 years (mean± standard deviation) (range 24 to 40 years)) and five tetraplegic participants (demographics shown in Table 1) were recruited. The tetraplegic participants, who were sub-acute inpatients at a university teaching hospital, were able to breathe independently, but had no useful abdominal muscle movement resulting in reduced respiratory function. The study was approved by the relevant local ethics committees and all participants gave written informed consent. 2.2 Motor point detection A virtual line was taken superiorly from the highest point of the iliac crest (top of the hip bone) until reaching the costal margin, with this distance used as the reference measurement in the superior direction (yn). The lateral distance between the umbilicus and this virtual line was taken as the reference measure in the lateral direction (xn). Table 1: Tetraplegic participant demographics. AIS = American Spinal Injuries Association Impairment Scale. AIS score refers to the function and sensation below the injury level: A no motor function or sensation, B no motor function with sensation, C severely compromised motor function with sensation. ID Sex Age Injury AIS Time post (years) level score injury (days) 1 M 77 C3/4 C 31 2 M 24 C5/6 A 52 3 M 32 C5 B 46 4 M 20 C5 C 29 5 M 24 C5/6 C 19
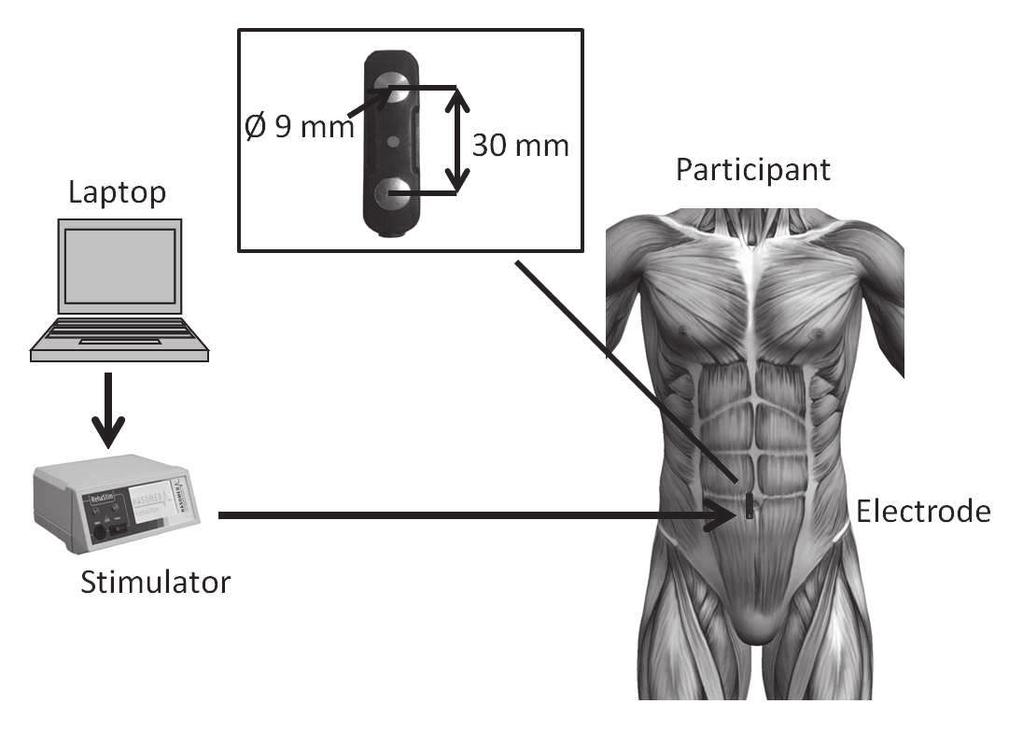
4 Both measurements, performed on the right hand side of the body as illustrated in Figure 1, were recorded using a measuring tape and assumed to remain fixed throughout each assessment. They were therefore used to normalise motor point positions in the corresponding direction to allow intersubject comparison. Figure 1: Diagram of reference and motor point position measurements. A virtual line was taken superiorly from the highest point of the iliac crest until reaching the costal margin. The superior length of this line (yn) and its lateral distance from the umbilicus (xn) were used as reference measurements for motor point positions. Motor point positions were normalised with respect to these distances. The white arrows illustrate the definition of the superior (y) and lateral (x) position of a motor point (represented by the white circle). The experimental setup is shown in Figure 2. To locate the motor points, a bar electrode (MLADDF30, ADInstruments, New Zealand) with two 9 mm diameter electrode contacts and 30 mm spacing between the contacts was used. Electrolytic gel was applied to the electrode to aid the transfer of current to the skin. To locate the position of the motor points of the EO muscles, the bar electrode was positioned horizontally, inferior of the costal margin. A neuromuscular stimulator (Rehastim v1, Hasomed GmbH, Germany) was used to apply single biphasic stimulation pulses, at a frequency of 0.5 Hz with a pulsewidth of 100 μs. The current was adjusted on a participant by participant basis (20 to 60 ma). The bar electrode was moved laterally until the observed muscle contraction was strongest. This point of maximum contraction, determined visually and from participant feedback, was recorded as the motor point position. To locate the motor points of the RA muscles, the electrode was positioned vertically, approximately 3 cm lateral of the umbilicus, and moved laterally and superiorly until the strongest muscle contraction was observed. This procedure was performed on both sides of the body, with the order in which each motor point was located being randomised. The position of each motor point was measured superiorly from the highest point of the iliac crest (y) and laterally from the umbilicus (x), as illustrated in Figure 1. The same researcher recorded the motor point positions for all participants, using the same measuring tape. This procedure took approximately two to five minutes. Figure 2: Diagram of experimental set up, with the inset showing the dimensions of the bar electrode used to apply stimulation. To detect the position of the motor point of the respective muscles, the electrode was placed on the abdomen and moved until the greatest contraction of that muscle was observed. Able bodied participants were initially asked to attend one assessment session (A1). Each participant was asked to sit in an upright position and the landmark measurements and motor point positions were recorded. The measurements or the motor point positions were repeated after a rest period of approximately 30 minutes, during which time participants were free to walk around. The total duration of the session, summarised in Figure 3a, was approximately one hour.
5 a) Able bodied. b) Tetraplegic. Figure 3: Experimental protocol showing periods of anatomical measurements, motor point detection and rest for the able bodied and tetraplegic participants. For the tetraplegic participants the same motor point detection procedure was used, but this was conducted at the participant s bedside, with participants in a supine position due to the acute stage of their spinal cord injury. For these participants the procedure was repeated after three days as shown in Figure 3b. Both measurements are referred to as assessment T1. Five of the able bodied participants (3 males, age 28.8±7.4 years (mean± standard deviation) (range 25 to 42 years)) were recalled after an 18 month period, and the assessment procedure repeated. Motor points were detected with the participants in both an upright seated (A2) and supine (A3) position. The assessments are summarised in Table 2. Table 2: Summary of assessment procedures. Assessment Participant Posture Repeat Time of assessment A1 Able bodied Seated 30 minutes Baseline A2 Able bodied Seated 30 minutes 18 months after A1. A3 Able bodied Supine 30 minutes 18 months after A1. T1 Tetraplegic Supine 3 days Baseline 2.3 Statistical Considerations Motor point positions are reported as absolute positions in the superior (y) and lateral (x) direction and as percentage values normalised by the corresponding reference distance, as described above. For each assessment session, the mean of the two measurements is taken as the motor point position for each participant, and the mean values (± standard deviation) across all participants are reported for the absolute and normalised results. The standard deviation of the normalised results was used to describe the uniformity across all participants. A Student s independent t-test was used to test for a statistically significant difference (p<0.05) in the group motor point positions recorded at A1 and T1. To assess the repeatability of measurements, the coefficient of repeatability (CoR) was calculated as 2 times the standard deviation of the difference between two measurements, across all participants, giving a 95% confidence range (Bland and Altman, 1986). The repeatability of the motor point detection technique was assessed by calculating the CoR for the two repeat measurements taken at each assessment session, across all participants. The dependency of motor point position on time
6 was evaluated by calculating the CoR between the motor point positions recorded for each participant at A1 compared to those from A2 (18 months later), for those participants who took part in both assessment sessions. Whether motor point positions changed with posture was assessed by calculating the CoR between the motor point positions recorded for each participant at A2 (seated) with those at A3 (supine). 3 Results The normalised locations of the motor points of the RA and EO recorded at A1 (able bodied, black symbols) and T1 (tetraplegic, grey symbols) are shown in Figure 4. Figure 4a depicts the motor points for each participant (taken as the mean of the two repeat measurements). Figure 4b shows the normalised motor point positions for each muscle, grouped by assessment. While the median motor point positions of the EO muscles are in approximately the same normalised position for both assessment groups, the range of the positions when measured superiorly from the iliac crest line was relatively large. For the RA muscles, the positions of the two assessment groups are different in both the lateral and superior directions. Also shown are the normalised locations of the umbilicus in the superior direction, which indicates that these also differ between both assessment groups. The mean (± standard deviation) motor point positions recorded at A1 and T1 are shown in Table 3 as absolute and normalised measurements. It can be seen that the absolute motor point positions recorded at T1 were all statistically significantly different from the motor point positions recorded at A1 when measured from the iliac crest (Y ). However, when these measurements were normalised to allow for more effective comparison between groups, Y n, only the motor points of the RA muscles were in a statistically significantly different position at T1 compared to A1, with these motor points found to be statistically significantly closer to the costal margin. a) Normalised individual motor point positions recorded at A1 (black ) and T1 (white o), with the position of the umbilicus for each participant shown on the midline. Also shown are the landmarks for the reference measurements (top of the iliac crest (grey *), corresponding point on the costal margin (grey +)). b) Normalised group motor point positions (median and inter-quartile ranges) recorded at A1 (black) and T1 (grey). Figure 4: Individual and group motor point position of the external oblique (outer left and right) and rectus abdominis (inner left and right) muscles of ten able bodied (assessment A1, black symbols) and five tetraplegic (assessment T1, grey symbols) participants, with the position of the umbilicus shown on the midline. Motor point positions are normalised to the reference measurements shown in Figure 1.
7 Table 3: Mean position and standard deviation (intersubject uniformity) of the position of the Rectus Abdominis (RA) and External Oblique (EO) motor points for assessment A1 (10 able bodied participants) and T1 (5 tetraplegic participants). Results are expressed as absolute distances measured superiorly from the iliac crest (Y and laterally from the umbilicus X ), and corresponding normalised distance with respect to the reference measurements ( Y n and ± standard deviations s. * indicates mean at T1 is statistically significantly different to mean at A1. X n ), Ass. Muscle Y s y sx X Yn syn X n sxn [cm] [cm] [%] [%] A1 RA Right 6.2± ± ± ±4.0 RA Left 6.2± ± ± ±2.8 EO Right 9.2± ± ± ±7.8 EO Left 9.1± ± ± ±6.3 T1 RA Right 9.9±4.3 * 4.8± ±5.8 * 28.0±2.5 RA Left 9.8±4.5 * 4.8± ±7.1 * 28.1±4.1 * EO Right 12.6±4.3 * 14.7± ± ±5.8 EO Left 13.0±5.0 * 14.8± ± ±3.9 Table 4 shows the mean coefficient of repeatability between the two measurements of motor point position recorded at all assessments (A1, T1, A2 and A3, CoR ) which provides a measure of the repeatability of the measurement technique. The comparison between assessments A1 and A2 (5 common able bodied participants, 18 months apart), CoR(A1,A2), shows the repeatability of the motor point position over time, while the coefficient of repeatability between assessment A2 (seated) and A3 (supine) shows the influence of posture (CoR(A2,A3)) on the motor point position. From CoR it can be concluded that 95% of test-retest measurement differences would be less than 1.7 cm, with a similar CoR even after an 18 month period (CoR(A1,A2)). The CoR is greater if tests are performed with different postures (CoR(A2,A3)), indicating a dependence of motor point position on posture in particular for the RA muscle when measured in the superior direction (y).
8 Table 4: Mean coefficient of repeatability ( CoR ) of the position of the motor points of the Rectus Abdominis (RA) and External Oblique (EO) muscles recorded 30 minutes apart for: 10 able bodied participants (A1); 5 able bodied participants after 18 months in seated position (A2); 5 able bodied participants after 18 months in supine position (A3) and 3 days apart for 5 tetraplegic participants in supine position (T1). Also shown is the mean CoR of the motor point positions recorded 18 months apart (CoR(A1,A2)) and in a seated and supine position (CoR(A2,A3)). Results are expressed as absolute distances measured superiorly from the iliac crest (y) and laterally from the umbilicus (x). CoR CoR(A1,A2) CoR(A2,A3) Muscle y x y x y x [cm] [cm] [cm] [cm] [cm] [cm] RA Right RA Left EO Right EO Left Discussion In this study the feasibility of using NMES to detect the position of the motor points of the RA and EO muscles was demonstrated in ten able bodied and five tetraplegic participants. The motor points of these muscle groups could be easily detected in all participants. It was shown that these motor points have a range of intersubject uniformities, and that repeatability of their positions within subjects was adequate, both at the same assessment session and when repeated after 18 months. Variations in posture resulted in changes of the position of the motor points of the RA muscle. The results of this study suggest that this technique can be easily adopted to reliably detect the positions of the motor points of the abdominal muscles. Owing to the fact that the abdominal muscles are often not included in standard motor point charts (Reid, 1920), and the adequate repeatability found in this study, we suggest that this technique should be adopted as standard procedure to select the optimum electrode location when using AFES to support respiration in tetraplegia. This method of motor point detection may also be beneficial to select the optimum electrode placement when using NMES to improve muscle strength, endurance and appearance in the able bodied population. When analysing the position of the motor points of muscles in the leg Botter et al (2011) developed criteria which allowed intersubject uniformity, a measure of the spread of motor point positions across participants, to be classed as good <4%, fair 4 6% or poor >6%. It was found that when classifying the intersubject uniformity of the motor point position measurements recorded at assessments A1 and T1 (cf. s xn and s yn in Table3, 3 were good, 6 were fair
9 and 7 were poor. It should be noted that Botter et al (2011) based their uniformity calculations on normalising the muscles by their estimated lengths, while in this study the locations are normalised by anatomical reference measurements. Nevertheless, the range of intersubject uniformity observed here suggests that the use of standard motor point locations may not be suitable for detecting the exact location of the motor points of the abdominal muscles, agreeing with the finding of Botter et al (2011) for the muscles of the leg. Bland and Altman (1986) recommend the CoR as a method of assessing test-retest repeatability with a 95% confidence. In this study the largest CoR between the motor point positions recorded at A1, A2, A3 and T1 were 1.6 cm for the EO and 1.2 cm for the RA muscles. Between the two measurements of motor point position compared here, no restrictions were placed on participant movement, indicating that NMES can be used to detect the position of the motor points with good repeatability, even after time and activity. When the positions of the motor points were detected after 18 months the largest CoR was also 1.6 cm, indicating that the positions of the motor points remain relative constant over time. The electrodes typically used for AFES studies are approximately 5 cm long with a space of approximately 3 cm between the electrodes (Gollee et al, 2007; Langbein et al, 2001), meaning that the CoR would fall within this area. This suggests that use of the motor point detection technique outlined here to locate the position of the motor points once for each individual, at the start of a course of AFES, would be adequate. Placement of the stimulating electrodes at the motor points appeared to lead to a more effective muscle contraction compared to when using empirically derived electrode locations. The effect of this should be twofold. Firstly, this should lead to a greater benefit from using AFES which may, in turn, lead to a greater improvement in the respiratory function of the user and improve their quality of life. Secondly, it should ensure a consistent muscle contraction across AFES studies. The motor points of the tetraplegic participants were detected in a supine position due to the acute stage of their spinal cord injury. For these participants the motor points of the RA muscles, when measured in the superior direction, were statistically significantly closer to the costal margin than for the able bodied participants (cf. Y n for RA in Table 3). This posture dependance of motor point position was further highlighted by the large CoR recorded when the motor points of five able bodied participants were detected in a seated and supine position (cf. CoR(A2,A3), Table 4). This suggests that motor point positions should be re-identified if posture changes occur. Dyskinesia, a movement disorder causing involuntary muscle movements, has been reported to affect the abdominal muscles (Linazasoro et al, 2005). The application of Botulinum toxin A for nerve blocking has been used to treat dyskinesia (Hallett et al, 2013). For effective nerve blocking Botulinum toxin A should be applied at the motor point (Lee et al, 2009). The detection of the motor points of the abdominal muscles using the methods outlined here could aid in the application of Botulinum toxin A for treating dyskinesia of the abdominal wall. Anatomical investigations of innervation of the abdominal muscles (Bell et al, 2007) suggest that the RA and EO muscles have more than one motor point. In this study, the focus was to detect the location where the strongest contraction was observed. For some of the able bodied participants there appeared to be a second motor point of the RA muscle, located slightly inferior to the costal margin. This motor point was not present in all participants, or could not be as easily detected as the other motor points documented. It may be situated deeper than the other motor points, or may
10 have belonged to another muscle group situated proximal to the RA muscle. While Langbein et al (2001) used an electrode position which would have stimulated this second motor point of the RA muscle, the difficulty of detection found here would suggest that the application of AFES at this location would not achieve a strong muscle contraction. The motor points of the EO muscle reported here were the only motor points of this muscle detected. A potential limitation of this study was the accuracy of motor point position measurement. By using a standard measuring tape the resolution was approximately 0.25 cm which may account for some of the CoR and intersubject uniformity values which were observed. One approach to increase measurement accuracy would be to use position markers in combination with an accurate position measurement system to record the motor point positions. However, these devices tend to be large, making them impractical in a clinical setting. Additionally, previous motor point detection studies have used a pen electrode to apply stimulation (Botter et al, 2011; Gobbo et al, 2011). In this study a bar electrode, which spreads stimulation over a larger surface area, was used to minimise user discomfort. The low CoR suggests that the measurement inaccuracies did not have a major influence on accurately locating the position of the motor points. 5 Conclusion In this study NMES was used to reliably detect the position of the motor points of the abdominal muscles. The results of this study show that while position of the motor points of the RA and EO muscles change little over time, they were found to be posture dependent, and variations were observed between participants. This motor point detection technique should enable the optimum AFES electrode location for each user to be identified, which if adopted as a standard technique for all AFES studies, would allow easier comparison of results. Acknowledgements E.J. McCaughey would like to thank the EPSRC for a scholarship to help fund this project. Conflict of interest None. References Bell S, Shaw-Dunn J, Gollee H, Allan DB, Fraser MH, McLean AN (2007) Improving respiration in patients with tetraplegia by functional electrical stimulation: an anatomical perspective. Clin Anat 20(6): Bland JM, Altman DG (1986) Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1(8476): Botter A, Oprandi G, Lanfranco F, Allasia S, Maffiuletti NA, Minetto MA (2011) Atlas of the muscle motor points for the lower limb: implications for electrical stimulation procedures and electrode positioning. Eur J Appl Physiol 111(10):
11 Butler J, JL, Gorman R, Boswell-Ruys C, Saboisky J, Lee B, Gandevia S (2011) Posterolateral surface electrical stimulation of abdominal expiratory muscles to enhance cough in spinal cord injury. Neurorehabil Neural Repair 25(2): Cardenas D, Hoffman J, Kirshblum S, McKinley W (2004) Etiology and incidence of rehospitalization after traumatic spinal cord injury: a multicenter analysis. Arch Phys Med Rehabil 85(11): Gobbo M, Gaffurini P, Bissolotti L, Esposito F, Orizio C (2011) Transcutaneous neuromuscular electrical stimulation: influence of electrode positioning and stimulus amplitude settings on muscle response. Eur J Appl Physiol 111(10): Gobbo M, Maffiuletti NA, Orizio C, Minetto MA (2014) Muscle motor point identification is essential for optimizing neuromuscular electrical stimulation use. J Neuroeng Rehabil 11(1):17 Gollee H, Hunt K, Allan D, Fraser M, McLean A (2007) A control system for automatic electrical stimulation of abdominal muscles to assist respiratory function in tetraplegia. Med Eng Phys 29(7): Hallett M, Albanese A, Dressler D, Segal KR, Simpson DM, Truong D, Jankovic J (2013) Evidence-based review and assessment of botulinum neurotoxin for the treatment of movement disorders. Toxicon 67: Langbein W, Maloney C, Kandare F, Stanic U, Nemchausky B, Jaeger R (2001) Pulmonary function testing in spinal cord injury: effects of abdominal muscle stimulation. J Rehabil Res Dev 38(5): Lee B, Boswell-Ruys C, Butler J, Gandevia S (2008) Surface functional electrical stimulation of the abdominal muscles to enhance cough and assist tracheostomy decannulation after high-level spinal cord injury. J Spinal Cord Med 31(1):78 82 Lee N, You J, Park H, Myoung H, Lee S, Hwang J, Kim H, Kim S, Lee K (2009) The validity and reliability of the motor point detection system: a preliminary investigation of motor points of the triceps surae muscles. Arch Phys Med Rehabil 90(2): Linazasoro G, Blercom NV, Lasa A, Fernández JM, Aranzábal I (2005) Etiological and therapeutical observations in a case of belly dancer s dyskinesia. Mov Disord 20 2 : McLachlan A, McLean A, Allan D, Gollee H (2013) Changes in pulmonary function measures following a passive abdominal functional electrical stimulation training program. J Spinal Cord Med 36(2): Moe J, Post H (1962) Functional electrical stimulation for ambulation in hemiplegia. J Lancet 82: Reid RW (1920) Motor points in relation to the surface of the body. J Anat 54(Pt 4): Sheffler L, Chae J (2007) Neuromuscular electrical stimulation in neurorehabilitation. Muscle Nerve 35(5): Taylor P, Tromans A, Harris K, Swain I (2002) Electrical stimulation of abdominal muscles for control of blood pressure and augmentation of cough in a C3/4 level tetraplegic. Spinal Cord 40(1):34 36
12
13
14
15
16
17 1 Costal Margin Costal Margin Normalised distance from IC to CM Left * 0.1 Umbilicus A1 (able bodied) 0 Iliac crest T1 (tetraplegic) Normalised distance from UM to IC * * * Right *
Effect of electrode position of low intensity neuromuscular electrical stimulation on the evoked force in the quadriceps femoris muscle
 DOI 10.1186/s13104-017-2630-9 BMC Research Notes RESEARCH NOTE Open Access Effect of electrode position of low intensity neuromuscular electrical stimulation on the evoked force in the quadriceps femoris
DOI 10.1186/s13104-017-2630-9 BMC Research Notes RESEARCH NOTE Open Access Effect of electrode position of low intensity neuromuscular electrical stimulation on the evoked force in the quadriceps femoris
Optimal electrode placement for non-invasive electrical stimulation of human abdominal muscles
 Page 1 of 22 Articles in PresS. J Appl Physiol (December 21, 2006). doi:10.1152/japplphysiol.00865.2006 Optimal electrode placement for non-invasive electrical stimulation of human abdominal muscles Julianne
Page 1 of 22 Articles in PresS. J Appl Physiol (December 21, 2006). doi:10.1152/japplphysiol.00865.2006 Optimal electrode placement for non-invasive electrical stimulation of human abdominal muscles Julianne
Electrical Stimulation of Abdominal Muscles to Produce Cough in Spinal Cord Injury: Effect of Stimulus Intensity
 552527NNRXXX10.1177/1545968314552527Neurorehabilitation and Neural RepairMcBain et al research-article2014 Clinical Research Article Electrical Stimulation of Abdominal Muscles to Produce Cough in Spinal
552527NNRXXX10.1177/1545968314552527Neurorehabilitation and Neural RepairMcBain et al research-article2014 Clinical Research Article Electrical Stimulation of Abdominal Muscles to Produce Cough in Spinal
Detection of Breathing Phases*
 SERBIAN JOURNAL OF ELECTRICAL ENGINEERING Vol. 6, No. 3, December 2009, 389-398 UDK: 615.849:621.37]:616.24-008.4 Detection of Breathing Phases* Ivan Božić 1,a, Djordje Klisić 1, Andrej Savić 1 Abstract:
SERBIAN JOURNAL OF ELECTRICAL ENGINEERING Vol. 6, No. 3, December 2009, 389-398 UDK: 615.849:621.37]:616.24-008.4 Detection of Breathing Phases* Ivan Božić 1,a, Djordje Klisić 1, Andrej Savić 1 Abstract:
Abdominal stimulation for respiratory support in tetraplegia: a tutorial review
 JOURNAL OF AUTOMATIC CONTROL, UNIVERSITY OF BELGRADE, VOL. 8(2):85-92, 28 c Abdominal for respiratory support in tetraplegia: a tutorial review H. Gollee, K. J. Hunt, M. H. Fraser, and A. N. McLean Abstract
JOURNAL OF AUTOMATIC CONTROL, UNIVERSITY OF BELGRADE, VOL. 8(2):85-92, 28 c Abdominal for respiratory support in tetraplegia: a tutorial review H. Gollee, K. J. Hunt, M. H. Fraser, and A. N. McLean Abstract
Erigo User Script 1. Erigo Background Information. 2. Intended use and indications
 Erigo User Script 1. Erigo Background Information The Erigo was developed in collaboration with the Spinal Cord Injury Center at the Balgrist University Hospital in Zurich, Switzerland and the Orthopaedic
Erigo User Script 1. Erigo Background Information The Erigo was developed in collaboration with the Spinal Cord Injury Center at the Balgrist University Hospital in Zurich, Switzerland and the Orthopaedic
Optimal electrode placement for noninvasive electrical stimulation of human abdominal muscles
 J Appl Physiol 102: 1612 1617, 2007. First published December 26, 2006; doi:10.1152/japplphysiol.00865.2006. Optimal electrode placement for noninvasive electrical stimulation of human abdominal muscles
J Appl Physiol 102: 1612 1617, 2007. First published December 26, 2006; doi:10.1152/japplphysiol.00865.2006. Optimal electrode placement for noninvasive electrical stimulation of human abdominal muscles
Haemodynamic and Respiratory Responses to Abdominal Muscle FES A Pilot Study
 Haemodynamic and Respiratory Responses to Abdominal Muscle FES A Pilot Study H Rischbieth 1 *, J Clark 1, S Donohoe 1, J Strayer 1,2, M Jelbart 1, K Stiller 3, T McDonald 3, R Marshall 1,2. FES Clinic,
Haemodynamic and Respiratory Responses to Abdominal Muscle FES A Pilot Study H Rischbieth 1 *, J Clark 1, S Donohoe 1, J Strayer 1,2, M Jelbart 1, K Stiller 3, T McDonald 3, R Marshall 1,2. FES Clinic,
Muscle motor point identification is essential for optimizing neuromuscular electrical stimulation use
 Gobbo et al. Journal of NeuroEngineering and Rehabilitation 2014, 11:17 JOURNAL OF NEUROENGINEERING JNERAND REHABILITATION COMMENTARY Open Access Muscle motor point identification is essential for optimizing
Gobbo et al. Journal of NeuroEngineering and Rehabilitation 2014, 11:17 JOURNAL OF NEUROENGINEERING JNERAND REHABILITATION COMMENTARY Open Access Muscle motor point identification is essential for optimizing
FES Standing: The Effect of Arm Support on Stability and Fatigue During Sit-to-Stand Manoeuvres in SCI Individuals
 FES Standing: The Effect of Arm Support on Stability and Fatigue During Sit-to-Stand Manoeuvres in SCI Individuals Musfirah Abd Aziz and Nur Azah Hamzaid Abstract Functional Electrical Stimulation (FES)
FES Standing: The Effect of Arm Support on Stability and Fatigue During Sit-to-Stand Manoeuvres in SCI Individuals Musfirah Abd Aziz and Nur Azah Hamzaid Abstract Functional Electrical Stimulation (FES)
Lack of muscle control (Stroke, bladder control, neurological disorders) Mechanical movement therapist assisted
 Mechanical movement therapist assisted") By Lisa Rosenberg Electrical Current Stimulates muscles and nerves Produces movement Helps Individuals with Disabilities Lack of muscle control (Stroke, bladder control, neurological disorders) Passive
By Lisa Rosenberg Electrical Current Stimulates muscles and nerves Produces movement Helps Individuals with Disabilities Lack of muscle control (Stroke, bladder control, neurological disorders) Passive
DELSYS. Purpose. Hardware Concepts. Software Concepts. Technical Note 101: EMG Sensor Placement
 Technical Note 101: EMG Sensor Placement Purpose This technical note addresses proper placement technique for Delsys Surface EMG Sensors. The technique is demonstrated through an experiment in which EMG
Technical Note 101: EMG Sensor Placement Purpose This technical note addresses proper placement technique for Delsys Surface EMG Sensors. The technique is demonstrated through an experiment in which EMG
Functional electrical stimulation. FES applications
 Functional electrical stimulation FES applications For all therapeutic areas The functional electrical stimulation (FES) is highly important for the therapy and rehabilitation of paralytic illnesses. If
Functional electrical stimulation FES applications For all therapeutic areas The functional electrical stimulation (FES) is highly important for the therapy and rehabilitation of paralytic illnesses. If
Biceps Activity EMG Pattern Recognition Using Neural Networks
 Biceps Activity EMG Pattern Recognition Using eural etworks K. Sundaraj University Malaysia Perlis (UniMAP) School of Mechatronic Engineering 0600 Jejawi - Perlis MALAYSIA kenneth@unimap.edu.my Abstract:
Biceps Activity EMG Pattern Recognition Using eural etworks K. Sundaraj University Malaysia Perlis (UniMAP) School of Mechatronic Engineering 0600 Jejawi - Perlis MALAYSIA kenneth@unimap.edu.my Abstract:
Medical Coverage Policy Functional Neuromuscular Electrical Stimulation EFFECTIVE DATE: 10/16/212 POLICY LAST UPDATED: 09/11/2014
 Medical Coverage Policy Functional Neuromuscular Electrical Stimulation EFFECTIVE DATE: 10/16/212 POLICY LAST UPDATED: 09/11/2014 OVERVIEW Neuromuscular Electrical Stimulation, (NMES), involves the use
Medical Coverage Policy Functional Neuromuscular Electrical Stimulation EFFECTIVE DATE: 10/16/212 POLICY LAST UPDATED: 09/11/2014 OVERVIEW Neuromuscular Electrical Stimulation, (NMES), involves the use
Hemifacial spasm. Parkinson's Disease Center and Movement Disorders Clinic
 Parkinson's Disease Center and Movement Disorders Clinic 7200 Cambridge Street, 9th Floor, Suite 9A Houston, Texas 77030 713-798-2273 phone www.jankovic.org Hemifacial spasm Diagnosis Hemifacial spasm
Parkinson's Disease Center and Movement Disorders Clinic 7200 Cambridge Street, 9th Floor, Suite 9A Houston, Texas 77030 713-798-2273 phone www.jankovic.org Hemifacial spasm Diagnosis Hemifacial spasm
A Measurement of Lower Limb Angles Using Wireless Inertial Sensors during FES Assisted Foot Drop Correction with and without Voluntary Effort
 A Measurement of Lower Limb Angles Using Wireless Inertial Sensors during FES Assisted Foot Drop Correction with and without Voluntary Effort Takashi Watanabe, Shun Endo, Katsunori Murakami, Yoshimi Kumagai,
A Measurement of Lower Limb Angles Using Wireless Inertial Sensors during FES Assisted Foot Drop Correction with and without Voluntary Effort Takashi Watanabe, Shun Endo, Katsunori Murakami, Yoshimi Kumagai,
A New Health Strategy to Prevent Pressure Ulcer Formation in Paraplegics using Computer and Sensory Substitution via the Tongue
 A New Health Strategy to Prevent Pressure Ulcer Formation in Paraplegics using Computer and Sensory Substitution via the Tongue Alexandre MOREAU-GAUDRY a,c,1, Anne PRINCE b, Jacques DEMONGEOT a,c and Yohan
A New Health Strategy to Prevent Pressure Ulcer Formation in Paraplegics using Computer and Sensory Substitution via the Tongue Alexandre MOREAU-GAUDRY a,c,1, Anne PRINCE b, Jacques DEMONGEOT a,c and Yohan
Proximally vs distally placed electrodes in a knee extension task. Eur J Transl Myol 26 (2):
:") Comparison of proximally versus distally placed spatially distributed sequential stimulation electrodes in a dynamic knee extension task Marco Laubacher (1,2), Efe A. Aksöz (1,2), Stuart Binder-Macleod
Comparison of proximally versus distally placed spatially distributed sequential stimulation electrodes in a dynamic knee extension task Marco Laubacher (1,2), Efe A. Aksöz (1,2), Stuart Binder-Macleod
GRASPING IN HIGH LESIONED TETRAPLEGIC SUBJECTS USING THE EMG CONTROLLED NEUROPROSTHESIS
 Journal of NeuroRehabilitation vol. 10, pp. 251-255, 1998 GRASPING IN HIGH LESIONED TETRAPLEGIC SUBJECTS USING THE EMG CONTROLLED NEUROPROSTHESIS Thierry Keller*, Armin Curt*, Milos R. Popovic**, Volker
Journal of NeuroRehabilitation vol. 10, pp. 251-255, 1998 GRASPING IN HIGH LESIONED TETRAPLEGIC SUBJECTS USING THE EMG CONTROLLED NEUROPROSTHESIS Thierry Keller*, Armin Curt*, Milos R. Popovic**, Volker
Optoelectronic plethysmography demonstrates abrogation of regional chest wall motion dysfunction in patients with pectus excavatum after Nuss repair
 Journal of Pediatric Surgery (2012) 47, 160 164 www.elsevier.com/locate/jpedsurg Optoelectronic plethysmography demonstrates abrogation of regional chest wall motion dysfunction in patients with pectus
Journal of Pediatric Surgery (2012) 47, 160 164 www.elsevier.com/locate/jpedsurg Optoelectronic plethysmography demonstrates abrogation of regional chest wall motion dysfunction in patients with pectus
APPLICATION OF MUSCLE/NERVE STIMULATION IN HEALTH AND DISEASE
 APPLICATION OF MUSCLE/NERVE STIMULATION IN HEALTH AND DISEASE Advances in Muscle Research Volume 4 Series Editor G.J.M. Stienen, Vrije Universiteit, Amsterdam, The Netherlands Application of Muscle/Nerve
APPLICATION OF MUSCLE/NERVE STIMULATION IN HEALTH AND DISEASE Advances in Muscle Research Volume 4 Series Editor G.J.M. Stienen, Vrije Universiteit, Amsterdam, The Netherlands Application of Muscle/Nerve
904 IEEE TRANSACTIONS ON NEURAL SYSTEMS AND REHABILITATION ENGINEERING, VOL. 26, NO. 4, APRIL 2018
 904 IEEE TRANSACTIONS ON NEURAL SYSTEMS AND REHABILITATION ENGINEERING, VOL. 26, NO. 4, APRIL 2018 Influence of Elbow Flexion and Stimulation Site on Neuromuscular Electrical Stimulation of the Biceps
904 IEEE TRANSACTIONS ON NEURAL SYSTEMS AND REHABILITATION ENGINEERING, VOL. 26, NO. 4, APRIL 2018 Influence of Elbow Flexion and Stimulation Site on Neuromuscular Electrical Stimulation of the Biceps
Spinal Cord (2014), 1 5. & 2014 International Spinal Cord Society All rights reserved /14
, 1 5. & 2014 International Spinal Cord Society All rights reserved /14") (214), 1 5 & 214 International Society All rights reserved 1362-4393/14 www.nature.com/sc ORIGINAL ARTICLE Electrical stimulation-evoked contractions blunt orthostatic hypotension in sub-acute spinal cord-injured
(214), 1 5 & 214 International Society All rights reserved 1362-4393/14 www.nature.com/sc ORIGINAL ARTICLE Electrical stimulation-evoked contractions blunt orthostatic hypotension in sub-acute spinal cord-injured
Neuromuscular electrical stimulation of completely paralyzed abdominal muscles in spinal cord-injured patients: a pilot study
 (2008) 46, 445 450 & 2008 International Society All rights reserved 1362-4393/08 $30.00 www.nature.com/sc ORIGINAL ARTICLE Neuromuscular electrical stimulation of completely paralyzed abdominal muscles
(2008) 46, 445 450 & 2008 International Society All rights reserved 1362-4393/08 $30.00 www.nature.com/sc ORIGINAL ARTICLE Neuromuscular electrical stimulation of completely paralyzed abdominal muscles
Muscle Weakness Or Paralysis With Compromise Of Peripheral Nerve
 Muscle Weakness Or Paralysis With Compromise Of Peripheral Nerve Muscle weakness or complete paralysis may be secondary to an interruption in the communication between the brain and nerve cells in the
Muscle Weakness Or Paralysis With Compromise Of Peripheral Nerve Muscle weakness or complete paralysis may be secondary to an interruption in the communication between the brain and nerve cells in the
Thoracolumbar Anatomy Eric Shamus Catherine Patla Objectives
 1 2 Thoracolumbar Anatomy Eric Shamus Catherine Patla Objectives List the muscular and ligamentous attachments of the thoracic and lumbar spine Describe how the muscles affect the spine and upper extremity
1 2 Thoracolumbar Anatomy Eric Shamus Catherine Patla Objectives List the muscular and ligamentous attachments of the thoracic and lumbar spine Describe how the muscles affect the spine and upper extremity
Spinal Cord Injury and Physical Activity: Transforming Rehabilitation Mary P. Galea PhD
 Spinal Cord Injury and Physical Activity: Professor of Clinical Physiotherapy The University of Melbourne 1 2 Rehabilitation after spinal cord injury Based on: Expectations regarding functional outcomes
Spinal Cord Injury and Physical Activity: Professor of Clinical Physiotherapy The University of Melbourne 1 2 Rehabilitation after spinal cord injury Based on: Expectations regarding functional outcomes
Does your spasticity...
 QUESTIONS Does your spasticity... help or limit your walking? make it difficult to breathe or take a deep breath? help or hinder your ability to get in and out of bed? cause pain? Affect your posture in
QUESTIONS Does your spasticity... help or limit your walking? make it difficult to breathe or take a deep breath? help or hinder your ability to get in and out of bed? cause pain? Affect your posture in
Effect of Horizontal Support on Abdominal Muscle Activation and Load During a Vertical Chest Press Exercise on a Dual Adjustable Pulley Apparatus
 Effect of Horizontal Support on Abdominal Muscle Activation and Load During a Vertical Chest Press Exercise on a Dual Adjustable Pulley Apparatus D.S. Peckinpaugh C.T. Guzell Department of Kinesiology
Effect of Horizontal Support on Abdominal Muscle Activation and Load During a Vertical Chest Press Exercise on a Dual Adjustable Pulley Apparatus D.S. Peckinpaugh C.T. Guzell Department of Kinesiology
LIVING ANATOMY: IMPLICATIONS OF RESPIRATION CONVOCATION MARCH 16, 2019 PAMELA L. WILSON, D.O.
 LIVING ANATOMY: IMPLICATIONS OF RESPIRATION CONVOCATION MARCH 16, 2019 PAMELA L. WILSON, D.O. I believe you are taught anatomy in our school more thoroughly than any other school to date, because we want
LIVING ANATOMY: IMPLICATIONS OF RESPIRATION CONVOCATION MARCH 16, 2019 PAMELA L. WILSON, D.O. I believe you are taught anatomy in our school more thoroughly than any other school to date, because we want
Chapter 20: Muscular Fitness and Assessment
 Chapter 20: Muscular Fitness and Assessment American College of Sports Medicine. (2010). ACSM's resource manual for guidelines for exercise testing and prescription (6th ed.). New York: Lippincott, Williams
Chapter 20: Muscular Fitness and Assessment American College of Sports Medicine. (2010). ACSM's resource manual for guidelines for exercise testing and prescription (6th ed.). New York: Lippincott, Williams
Hand of Hope. For hand rehabilitation. Member of Vincent Medical Holdings Limited
 Hand of Hope For hand rehabilitation Member of Vincent Medical Holdings Limited Over 17 Million people worldwide suffer a stroke each year A stroke is the largest cause of a disability with half of all
Hand of Hope For hand rehabilitation Member of Vincent Medical Holdings Limited Over 17 Million people worldwide suffer a stroke each year A stroke is the largest cause of a disability with half of all
Transcutaneous Electrical Nerve Stimulation (TENS)
") Transcutaneous Electrical Nerve Stimulation (TENS) Authors: SCIRE Community Team Reviewed by: Amrit Dhaliwal, PT Last updated: July 27, 2017 Transcutaneous electrical nerve stimulation (TENS) is a non-drug
Transcutaneous Electrical Nerve Stimulation (TENS) Authors: SCIRE Community Team Reviewed by: Amrit Dhaliwal, PT Last updated: July 27, 2017 Transcutaneous electrical nerve stimulation (TENS) is a non-drug
MUSCLE BEHAVIOR IN ARTIFICIALLY ACTIVATED MUSCLE - MEASUREMENTS ON NEUROLOGICALLY INTACT AND PARAPLEGIC SUBJECTS METHODS
 MUSCLE BEHAVIOR IN ARTIFICIALLY ACTIVATED MUSCLE - MEASUREMENTS ON NEUROLOGICALLY INTACT AND PARAPLEGIC SUBJECTS Margit Gföhler, Johann Wassermann 2, Prisca Eser 3, Tanja Kakebeeke 3, Helga E. Lechner
MUSCLE BEHAVIOR IN ARTIFICIALLY ACTIVATED MUSCLE - MEASUREMENTS ON NEUROLOGICALLY INTACT AND PARAPLEGIC SUBJECTS Margit Gföhler, Johann Wassermann 2, Prisca Eser 3, Tanja Kakebeeke 3, Helga E. Lechner
Functional Electrical Stimulation-Assisted Walking: Enhancement of Voluntary Walking Function Among Persons with Severe Hemiplegia Post Stroke
 Functional Electrical Stimulation-Assisted Walking: Enhancement of Voluntary Walking Function Among Persons with Severe Hemiplegia Post Stroke Naaz Kapadia Date: May 10, 2010 Research Coordinator-Physiotherapist
Functional Electrical Stimulation-Assisted Walking: Enhancement of Voluntary Walking Function Among Persons with Severe Hemiplegia Post Stroke Naaz Kapadia Date: May 10, 2010 Research Coordinator-Physiotherapist
Muscles of the Core. PSK 4U Mr. S. Kelly North Grenville DHS
 Muscles of the Core PSK 4U Mr. S. Kelly North Grenville DHS Intercostal Muscles Run between the ribs Provide shape and movement for chest wall External intercostals: aid in both quiet (passive) and forced
Muscles of the Core PSK 4U Mr. S. Kelly North Grenville DHS Intercostal Muscles Run between the ribs Provide shape and movement for chest wall External intercostals: aid in both quiet (passive) and forced
III. Based upon our criteria and review of the peer-reviewed literature, NMES has not been proven to be effective and is
 MEDICAL POLICY SUBJECT: NEUROMUSCULAR ELECTRICAL PAGE: 1 OF: 5 If a product excludes coverage for a service, it is not covered, and medical policy criteria do not apply. If a commercial product, including
MEDICAL POLICY SUBJECT: NEUROMUSCULAR ELECTRICAL PAGE: 1 OF: 5 If a product excludes coverage for a service, it is not covered, and medical policy criteria do not apply. If a commercial product, including
International Journal of Pharma and Bio Sciences EFFECT OF ABDOMINAL COMPRESSION BINDER ON PULMONARY FUNCTION IN ADULT PARAPLEGICS ABSTRACT
 Research Article Allied sciences International Journal of Pharma and Bio Sciences ISSN 0975-6299 EFFECT OF ABDOMINAL COMPRESSION BINDER ON PULMONARY FUNCTION IN ADULT PARAPLEGICS ARIJIT KUMAR DAS 1, TUSHAR
Research Article Allied sciences International Journal of Pharma and Bio Sciences ISSN 0975-6299 EFFECT OF ABDOMINAL COMPRESSION BINDER ON PULMONARY FUNCTION IN ADULT PARAPLEGICS ARIJIT KUMAR DAS 1, TUSHAR
Electrical stimulation to reduce the overload in upper limbs on SPT
 Electrical stimulation to reduce the overload in upper limbs during sitting pivot transfer in paraplegic: a preliminary study Ana Claudia G. Lopes (1,2), Claudia Ochoa-Diaz (3), Roberto S. Baptista (3),
Electrical stimulation to reduce the overload in upper limbs during sitting pivot transfer in paraplegic: a preliminary study Ana Claudia G. Lopes (1,2), Claudia Ochoa-Diaz (3), Roberto S. Baptista (3),
Protocol. Functional Neuromuscular Electrical Stimulation
 Protocol Functional Neuromuscular Electrical Stimulation (80301) Medical Benefit Effective Date: 04/01/10 Next Review Date: 01/13 Preauthorization* Yes Review Dates: 03/07, 05/08, 05/09, 01/10, 01/11,
Protocol Functional Neuromuscular Electrical Stimulation (80301) Medical Benefit Effective Date: 04/01/10 Next Review Date: 01/13 Preauthorization* Yes Review Dates: 03/07, 05/08, 05/09, 01/10, 01/11,
3 Movements of the Trunk. Flexion Rotation Extension
 3 Movements of the Trunk Flexion Rotation Extension 1 TRUNK FLEXION 2 TRUNK FLEXION: Rectus Abdominalis O: Crest of Pubis & ligaments covering front of symphysis pubis. I: By «3 portions into cartilages
3 Movements of the Trunk Flexion Rotation Extension 1 TRUNK FLEXION 2 TRUNK FLEXION: Rectus Abdominalis O: Crest of Pubis & ligaments covering front of symphysis pubis. I: By «3 portions into cartilages
Energy for Muscle Contractions: Direct phosphorylation. Creatine phosphate loses a phosphate to ADP to create ATP
 Energy for Muscle Contractions: Direct phosphorylation Aerobic respiration Anaerobic respiration (lactic acid fermentation) Creatine phosphate loses a phosphate to ADP to create ATP Requires oxygen to
Energy for Muscle Contractions: Direct phosphorylation Aerobic respiration Anaerobic respiration (lactic acid fermentation) Creatine phosphate loses a phosphate to ADP to create ATP Requires oxygen to
NEUROCARE 1000/4P NEUROMUSCULAR ELECTRIC STIMULATOR FOR DIABETIC NEUROPATHY TREATMENT
 NEUROCARE 1000/4P NEUROMUSCULAR ELECTRIC STIMULATOR FOR DIABETIC NEUROPATHY TREATMENT Diabetic neuropathies are common in almost 50 percent of all sufferers. Although current studies still don t pinpoint
NEUROCARE 1000/4P NEUROMUSCULAR ELECTRIC STIMULATOR FOR DIABETIC NEUROPATHY TREATMENT Diabetic neuropathies are common in almost 50 percent of all sufferers. Although current studies still don t pinpoint
Redefining Neurorehab. Improve Function. Maximize Independence. Enhance Quality of Life.
 Redefining Neurorehab Improve Function. Maximize Independence. Enhance Quality of Life. What is MyndMove? MyndMove is the first therapy to deliver significant lasting voluntary upper extremity function
Redefining Neurorehab Improve Function. Maximize Independence. Enhance Quality of Life. What is MyndMove? MyndMove is the first therapy to deliver significant lasting voluntary upper extremity function
COURAGE KENNY RESEARCH INITIATIVES IN SPINAL CORD INJURY REHABILITATION
 COURAGE KENNY RESEARCH INITIATIVES IN SPINAL CORD INJURY REHABILITATION Maggie Weightman PT, PhD Courage Kenny Research Center/Courage Kenny Rehabilitation Institute 15June 2018 DISCLOSURE NONE Current
COURAGE KENNY RESEARCH INITIATIVES IN SPINAL CORD INJURY REHABILITATION Maggie Weightman PT, PhD Courage Kenny Research Center/Courage Kenny Rehabilitation Institute 15June 2018 DISCLOSURE NONE Current
You make us tic. Leading an active life... syntic. contic + biotic + The first choice in the device-assisted conservative therapy of incontinence
 Leading an active life... p r e m i u m l i n e You make us tic syntic biotic + contic + The first choice in the device-assisted conservative therapy of incontinence Multifunctional and nevertheless customized...
Leading an active life... p r e m i u m l i n e You make us tic syntic biotic + contic + The first choice in the device-assisted conservative therapy of incontinence Multifunctional and nevertheless customized...
Intramachine and intermachine reproducibility of concentric performance: A study of the Con-Trex MJ and the Cybex Norm dynamometers
 Isokinetics and Exercise Science 12 (4) 91 97 91 IOS Press Intramachine and intermachine reproducibility of concentric performance: A study of the Con-Trex MJ and the Cybex Norm dynamometers C. Bardis
Isokinetics and Exercise Science 12 (4) 91 97 91 IOS Press Intramachine and intermachine reproducibility of concentric performance: A study of the Con-Trex MJ and the Cybex Norm dynamometers C. Bardis
Last Updated: July 20, 2016 Articles up-to-date as of: July 2015
 Reviewer ID: Christie Chan, John Zhu, Jeremy Mak, Kyle Diab Type of Outcome Measure: 10 Meter Walk Test (10MWT) Total articles: 21 Author ID Year Amatachaya Datta 2009 Ditunno et al. 2007 Duffell 2015
Reviewer ID: Christie Chan, John Zhu, Jeremy Mak, Kyle Diab Type of Outcome Measure: 10 Meter Walk Test (10MWT) Total articles: 21 Author ID Year Amatachaya Datta 2009 Ditunno et al. 2007 Duffell 2015
EFFECTS OF PULSE DURATION ON MUSCLE FATIGUE DURING ELECTRICAL STIMULATION INDUCING MODERATE-LEVEL CONTRACTION
 EFFECTS OF PULSE DURATION ON MUSCLE FATIGUE DURING ELECTRICAL STIMULATION INDUCING MODERATE-LEVEL CONTRACTION WOOHYOUNG JEON, MS, and LISA GRIFFIN, PhD Department of Kinesiology and Health Education, University
EFFECTS OF PULSE DURATION ON MUSCLE FATIGUE DURING ELECTRICAL STIMULATION INDUCING MODERATE-LEVEL CONTRACTION WOOHYOUNG JEON, MS, and LISA GRIFFIN, PhD Department of Kinesiology and Health Education, University
Gross Anatomy ABDOMEN/SESSION 1 Dr. Firas M. Ghazi
 Anterior Abdominal Wall Structure, muscles and surface anatomy Curricular Objectives By the end of this session students are expected to: Practical 1. Identify the hip and distinguish the three bones forming
Anterior Abdominal Wall Structure, muscles and surface anatomy Curricular Objectives By the end of this session students are expected to: Practical 1. Identify the hip and distinguish the three bones forming
Chapter 3: Thorax. Thorax
 Chapter 3: Thorax Thorax Thoracic Cage I. Thoracic Cage Osteology A. Thoracic Vertebrae Basic structure: vertebral body, pedicles, laminae, spinous processes and transverse processes Natural kyphotic shape,
Chapter 3: Thorax Thorax Thoracic Cage I. Thoracic Cage Osteology A. Thoracic Vertebrae Basic structure: vertebral body, pedicles, laminae, spinous processes and transverse processes Natural kyphotic shape,
Biomedical Instrumentation
 University of Zagreb Faculty of Electrical Engineering and Computing Biomedical Instrumentation Electrical stimulation prof.dr.sc. Ratko Magjarević December 2015 Electrical stimulation The effect of electric
University of Zagreb Faculty of Electrical Engineering and Computing Biomedical Instrumentation Electrical stimulation prof.dr.sc. Ratko Magjarević December 2015 Electrical stimulation The effect of electric
Benefit of triple-strap abdominal binder on voluntary cough in patients with spinal cord injury
 (2011), 1 5 & 2011 International Society All rights reserved 1362-4393/11 $32.00 www.nature.com/sc ORIGINAL ARTICLE Benefit of triple-strap abdominal binder on voluntary cough in patients with spinal cord
(2011), 1 5 & 2011 International Society All rights reserved 1362-4393/11 $32.00 www.nature.com/sc ORIGINAL ARTICLE Benefit of triple-strap abdominal binder on voluntary cough in patients with spinal cord
Neurostyle. Medical Innovation for Better Life
 Neurostyle Medical Innovation for Better Life Neurostyle Pte Ltd is a company dedicated to design, develop, manufacture and distribute neurological and neuromuscular medical devices. Strategically located
Neurostyle Medical Innovation for Better Life Neurostyle Pte Ltd is a company dedicated to design, develop, manufacture and distribute neurological and neuromuscular medical devices. Strategically located
EE 791 Lecture 10. FES April 1, EE 791 Lecture 10 1
 EE 791 Lecture 10 FES April 1, 2013 EE 791 Lecture 10 1 Normal Functional Control EE 791 Lecture 10 2 Current uses of FES Cardiovascular Exercise Breathing assist Grasping and Reaching Transfer and Standing
EE 791 Lecture 10 FES April 1, 2013 EE 791 Lecture 10 1 Normal Functional Control EE 791 Lecture 10 2 Current uses of FES Cardiovascular Exercise Breathing assist Grasping and Reaching Transfer and Standing
ASYNCHRONOUS NEUROMUSCULAR ELECTRICAL STIMULATION
 ASYNCHRONOUS NEUROMUSCULAR ELECTRICAL STIMULATION By RYAN JAMES DOWNEY A DISSERTATION PRESENTED TO THE GRADUATE SCHOOL OF THE UNIVERSITY OF FLORIDA IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE
ASYNCHRONOUS NEUROMUSCULAR ELECTRICAL STIMULATION By RYAN JAMES DOWNEY A DISSERTATION PRESENTED TO THE GRADUATE SCHOOL OF THE UNIVERSITY OF FLORIDA IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE
Department of Physical Therapy, Graduate School, Catholic University of Pusan, Busan, Korea 2
 Original Article Journal of Exercise Rehabilitation 2014;10(4):230-235 Reliability of ultrasound in combination with surface electromyogram for evaluating the activity of abdominal muscles in individuals
Original Article Journal of Exercise Rehabilitation 2014;10(4):230-235 Reliability of ultrasound in combination with surface electromyogram for evaluating the activity of abdominal muscles in individuals
Mechanical contribution of expiratory muscles to pressure generation during spinal cord stimulation
 Mechanical contribution of expiratory muscles to pressure generation during spinal cord stimulation A. F. DIMARCO, J. R. ROMANIUK, K. E. KOWALSKI, AND G. SUPINSKI Pulmonary Division, Department of Medicine,
Mechanical contribution of expiratory muscles to pressure generation during spinal cord stimulation A. F. DIMARCO, J. R. ROMANIUK, K. E. KOWALSKI, AND G. SUPINSKI Pulmonary Division, Department of Medicine,
Introduction to TMS Transcranial Magnetic Stimulation
 Introduction to TMS Transcranial Magnetic Stimulation Lisa Koski, PhD, Clin Psy TMS Neurorehabilitation Lab Royal Victoria Hospital 2009-12-14 BIC Seminar, MNI Overview History, basic principles, instrumentation
Introduction to TMS Transcranial Magnetic Stimulation Lisa Koski, PhD, Clin Psy TMS Neurorehabilitation Lab Royal Victoria Hospital 2009-12-14 BIC Seminar, MNI Overview History, basic principles, instrumentation
NVM5 NERVE MONITORING SYSTEM AN INTRODUCTION TO
 AN INTRODUCTION TO NVM5 NERVE MONITORING SYSTEM This booklet is designed to inform you about the use of NVM5 nerve monitoring in the course of your surgery. It is not meant to replace any personal conversations
AN INTRODUCTION TO NVM5 NERVE MONITORING SYSTEM This booklet is designed to inform you about the use of NVM5 nerve monitoring in the course of your surgery. It is not meant to replace any personal conversations
Meredith Jane Kuipers
 Functional Electrical Stimulation as a Neuroprosthesis for Sitting Balance: Measuring Respiratory Function and Seated Postural Control in Able-bodied Individuals and Individuals with Spinal Cord Injury
Functional Electrical Stimulation as a Neuroprosthesis for Sitting Balance: Measuring Respiratory Function and Seated Postural Control in Able-bodied Individuals and Individuals with Spinal Cord Injury
MultiStim SWITCH and MultiStim SENSOR Setting the trend in nerve stimulation
 MultiStim SWITCH and MultiStim SENSOR Setting the trend in nerve stimulation Plexus and Epidural Anaesthesia The essential advantage regarding safety MultiStim SENSOR and MultiStim SWITCH With MultiStim
MultiStim SWITCH and MultiStim SENSOR Setting the trend in nerve stimulation Plexus and Epidural Anaesthesia The essential advantage regarding safety MultiStim SENSOR and MultiStim SWITCH With MultiStim
Introduction. The Inner Core Muscles. Why Train The Inner Core? How Do You Train The Inner Core?
 Introduction Pilates focuses on the deep postural muscles, including the pelvic floor, the transversus abdominis (TA) and the multifidus. These deep postural muscles are also referred to as the core. Improving
Introduction Pilates focuses on the deep postural muscles, including the pelvic floor, the transversus abdominis (TA) and the multifidus. These deep postural muscles are also referred to as the core. Improving
PHYSICAL EDUCATION. 4º E.S.O. 2nd TERM. The skeletal and muscular systems.
 PHYSICAL EDUCATION 4º E.S.O. 2nd TERM. The skeletal and muscular systems. PARTS OF THE BODY Head Torso / Trunk Dorsal: Back Ventral: Thorax y Abdomen Extremities Superior: Arm Forearm Hand Joint: Shoulder
PHYSICAL EDUCATION 4º E.S.O. 2nd TERM. The skeletal and muscular systems. PARTS OF THE BODY Head Torso / Trunk Dorsal: Back Ventral: Thorax y Abdomen Extremities Superior: Arm Forearm Hand Joint: Shoulder
Comparing NMES Stimulation Intensity at Various Lengths of the Tibialis Anterior
 City University of New York (CUNY) CUNY Academic Works Dissertations, Theses, and Capstone Projects Graduate Center 6-3-2014 Comparing NMES Stimulation Intensity at Various Lengths of the Tibialis Anterior
City University of New York (CUNY) CUNY Academic Works Dissertations, Theses, and Capstone Projects Graduate Center 6-3-2014 Comparing NMES Stimulation Intensity at Various Lengths of the Tibialis Anterior
Motor and sensory nerve conduction studies
 3 rd Congress of the European Academy of Neurology Amsterdam, The Netherlands, June 24 27, 2017 Hands-on Course 2 Assessment of peripheral nerves function and structure in suspected peripheral neuropathies
3 rd Congress of the European Academy of Neurology Amsterdam, The Netherlands, June 24 27, 2017 Hands-on Course 2 Assessment of peripheral nerves function and structure in suspected peripheral neuropathies
CERVICAL SPINE TIPS A
 CERVICAL SPINE TIPS A Musculoskeletal Approach to managing Neck Pain An ALGORITHM, as a management guide Rick Bernau & Ian Wallbridge June 2010 THE PROCESS An interactive approach to the management of
CERVICAL SPINE TIPS A Musculoskeletal Approach to managing Neck Pain An ALGORITHM, as a management guide Rick Bernau & Ian Wallbridge June 2010 THE PROCESS An interactive approach to the management of
Pulmonary Functions and Effect of Incentive Spirometry During Acute and Post Acute Period in Tetraplegia
 IJPMR 13, April 2002; 28-34 Pulmonary Functions and Effect of Incentive Spirometry During Acute and Post Acute Period in Tetraplegia Dr M Joshi, M.D., Research Associate Dr N Mathur, M.S., DNB, Associate
IJPMR 13, April 2002; 28-34 Pulmonary Functions and Effect of Incentive Spirometry During Acute and Post Acute Period in Tetraplegia Dr M Joshi, M.D., Research Associate Dr N Mathur, M.S., DNB, Associate
2 Gait Laboratory, Queen Mary's Hospital, London, UK. 3 One Small Step Gait Laboratory, Guy's Hospital London, UK
 Upper and Lower Limb Electrical Stimulation in Paediatrics Held at Queen Mary's Hospital, Roehampton, London Thursday, 13th June 2002 The aim of the workshop was to promote discussion and the exchange
Upper and Lower Limb Electrical Stimulation in Paediatrics Held at Queen Mary's Hospital, Roehampton, London Thursday, 13th June 2002 The aim of the workshop was to promote discussion and the exchange
TMG - BMC LTD. Mirje 6 Tel: ( ) Ljubljana Fax: ( ) TENSIOMYOGRAPHY (TMG) MEASUREMENT RESULTS
 Ljubljana Fax: ( ) TENSIOMYOGRAPHY (TMG) MEASUREMENT RESULTS") TMG - BMC LTD. Mirje 6 Tel: (00 386 1) 4210 037 1000 Ljubljana Fax: (00 386 1) 2425 382 Slovenia Email: info@tmg.si Europe (EU) Web: www.tmg.si TENSIOMYOGRAPHY (TMG) MEASUREMENT RESULTS Subject: Adrian
TMG - BMC LTD. Mirje 6 Tel: (00 386 1) 4210 037 1000 Ljubljana Fax: (00 386 1) 2425 382 Slovenia Email: info@tmg.si Europe (EU) Web: www.tmg.si TENSIOMYOGRAPHY (TMG) MEASUREMENT RESULTS Subject: Adrian
Resting-State Functional Connectivity in Stroke Patients After Upper Limb Robot-Assisted Therapy: A Pilot Study
 Resting-State Functional Connectivity in Stroke Patients After Upper Limb Robot-Assisted Therapy: A Pilot Study N. Kinany 1,3,4(&), C. Pierella 1, E. Pirondini 3,4, M. Coscia 2, J. Miehlbradt 1, C. Magnin
Resting-State Functional Connectivity in Stroke Patients After Upper Limb Robot-Assisted Therapy: A Pilot Study N. Kinany 1,3,4(&), C. Pierella 1, E. Pirondini 3,4, M. Coscia 2, J. Miehlbradt 1, C. Magnin
Test-Retest Reliability of the StepWatch Activity Monitor Outputs in Healthy Adults
 Journal of Physical Activity and Health, 2010, 7, 671-676 2010 Human Kinetics, Inc. Test-Retest Reliability of the StepWatch Activity Monitor Outputs in Healthy Adults Suzie Mudge, Denise Taylor, Oliver
Journal of Physical Activity and Health, 2010, 7, 671-676 2010 Human Kinetics, Inc. Test-Retest Reliability of the StepWatch Activity Monitor Outputs in Healthy Adults Suzie Mudge, Denise Taylor, Oliver
GLOSSARY. Active assisted movement: movement where the actions are assisted by an outside force.
 GLOSSARY The technical words used in this guide are listed here in alphabetic order. The first time one of these words is used in the guide, it is written in italics. Sometimes there is reference to a
GLOSSARY The technical words used in this guide are listed here in alphabetic order. The first time one of these words is used in the guide, it is written in italics. Sometimes there is reference to a
Abdomen: Introduction. Prof. Oluwadiya KS
 Abdomen: Introduction Prof. Oluwadiya KS www.oluwadiya.com Abdominopelvic Cavity Abdominal Cavity Pelvic Cavity Extends from the inferior margin of the thorax to the superior margin of the pelvis and the
Abdomen: Introduction Prof. Oluwadiya KS www.oluwadiya.com Abdominopelvic Cavity Abdominal Cavity Pelvic Cavity Extends from the inferior margin of the thorax to the superior margin of the pelvis and the
The Frequency Analysis Method The FAM - a novel tool in physiotherapy for assessing physiological responses in human body
 The Frequency Analysis Method The FAM - a novel tool in physiotherapy for assessing physiological responses in human body *Lehtelä, ML MSc, PT; **Pienimäki, T MD, PhD; ***Alasaarela, E Dr Tech, Prof; ****Vesikukka,
The Frequency Analysis Method The FAM - a novel tool in physiotherapy for assessing physiological responses in human body *Lehtelä, ML MSc, PT; **Pienimäki, T MD, PhD; ***Alasaarela, E Dr Tech, Prof; ****Vesikukka,
What to expect following spinal cord injury. Information for patients Therapy Services
 What to expect following spinal cord injury Information for patients Therapy Services Introduction This leaflet aims to explain what spinal cord injury is and what to expect over the next few months. What
What to expect following spinal cord injury Information for patients Therapy Services Introduction This leaflet aims to explain what spinal cord injury is and what to expect over the next few months. What
PILATES CONDITIONING FOR PATHOLOGY OF THE INTERVETEBRAL DISK
 PILATES CONDITIONING FOR PATHOLOGY OF THE INTERVETEBRAL DISK Ashlee Tinken August 12, 2017 Comprehensive Apparatus Program Pilates Denver June 2015 ABSTRACT The pathology of the intervertebral disk is
PILATES CONDITIONING FOR PATHOLOGY OF THE INTERVETEBRAL DISK Ashlee Tinken August 12, 2017 Comprehensive Apparatus Program Pilates Denver June 2015 ABSTRACT The pathology of the intervertebral disk is
PART ONE. Belly Dance Fitness Technique
 PART ONE Belly Dance Fitness Technique OVERVIEW Understanding belly dance movement The gentle, symmetrical, rhythmic undulations that we practice in Belly dance can help to revitalize almost every part
PART ONE Belly Dance Fitness Technique OVERVIEW Understanding belly dance movement The gentle, symmetrical, rhythmic undulations that we practice in Belly dance can help to revitalize almost every part
Gregory M Yoshida, MD. Lateral curvature of the spine in the coronal plane > 10 degrees on an upright film
 Gregory M Yoshida, MD Lateral curvature of the spine in the coronal plane > 10 degrees on an upright film Measurement Angle made by the endplates of the two most tilted vertebra from horizontal Cobb angle
Gregory M Yoshida, MD Lateral curvature of the spine in the coronal plane > 10 degrees on an upright film Measurement Angle made by the endplates of the two most tilted vertebra from horizontal Cobb angle
Introduction to The Human Body
 1 Introduction to The Human Body FOCUS: The human organism is often examined at seven structural levels: chemical, organelle, cell, tissue, organ, organ system, and the organism. Anatomy examines the structure
1 Introduction to The Human Body FOCUS: The human organism is often examined at seven structural levels: chemical, organelle, cell, tissue, organ, organ system, and the organism. Anatomy examines the structure
Functional Electrical Stimulation (FES): Neurorehabilitation of the Upper Limb and Trunk
: Neurorehabilitation of the Upper Limb and Trunk") Functional Electrical Stimulation (FES): Neurorehabilitation of the Presented by the Occupational Therapy Department - Health Sciences Centre Winnipeg Dr. Kristin Musselman Sunday, June 3, 2018 Winnipeg,
Functional Electrical Stimulation (FES): Neurorehabilitation of the Presented by the Occupational Therapy Department - Health Sciences Centre Winnipeg Dr. Kristin Musselman Sunday, June 3, 2018 Winnipeg,
THE STRATEGIES FOR CONNECTION IN CHILDREN WITH CP
 2015 한국보바스소아학술대회 THE STRATEGIES FOR CONNECTION IN CHILDREN WITH CP KYOUNG SOOK PARK INSTRUCTOR THE BOBATH CONCEPT The NDT/Bobath Concept offers a forward looking interdisciplinary problem solving approach
2015 한국보바스소아학술대회 THE STRATEGIES FOR CONNECTION IN CHILDREN WITH CP KYOUNG SOOK PARK INSTRUCTOR THE BOBATH CONCEPT The NDT/Bobath Concept offers a forward looking interdisciplinary problem solving approach
Exploration of Hand Grasp Patterns Elicitable Through Non-Invasive Proximal Nerve Stimulation
 www.nature.com/scientificreports Received: 24 July 2017 Accepted: 16 November 2017 Published: xx xx xxxx OPEN Exploration of Hand Grasp Patterns Elicitable Through Non-Invasive Proximal Nerve Stimulation
www.nature.com/scientificreports Received: 24 July 2017 Accepted: 16 November 2017 Published: xx xx xxxx OPEN Exploration of Hand Grasp Patterns Elicitable Through Non-Invasive Proximal Nerve Stimulation
THE HUMAN BODY. study of the structure of living organisms. Physiologythe study of how the body works. Ex: studying the structure of the heart.
 HUMAN BODY SYSTEMS Anatomythe study of the structure of living organisms. Ex: studying the structure of the heart. Physiologythe study of how the body works. Ex: how the heart works to pump blood, etc.
HUMAN BODY SYSTEMS Anatomythe study of the structure of living organisms. Ex: studying the structure of the heart. Physiologythe study of how the body works. Ex: how the heart works to pump blood, etc.
THE ROLE OF THE MID-TORSO IN SPEED DEVELOPMENT
 THE ROLE OF THE MID-TORSO IN SPEED DEVELOPMENT The mid-torso is made up of 4 major muscle groups: 1. Rectus Abdominus Origin Base of sternum and bottom ribs Insertion Pubis bone (as part of the pelvis)
THE ROLE OF THE MID-TORSO IN SPEED DEVELOPMENT The mid-torso is made up of 4 major muscle groups: 1. Rectus Abdominus Origin Base of sternum and bottom ribs Insertion Pubis bone (as part of the pelvis)
Compound Action Potential, CAP
 Stimulus Strength UNIVERSITY OF JORDAN FACULTY OF MEDICINE DEPARTMENT OF PHYSIOLOGY & BIOCHEMISTRY INTRODUCTION TO NEUROPHYSIOLOGY Spring, 2013 Textbook of Medical Physiology by: Guyton & Hall, 12 th edition
Stimulus Strength UNIVERSITY OF JORDAN FACULTY OF MEDICINE DEPARTMENT OF PHYSIOLOGY & BIOCHEMISTRY INTRODUCTION TO NEUROPHYSIOLOGY Spring, 2013 Textbook of Medical Physiology by: Guyton & Hall, 12 th edition
Anatomy & Physiology. Introduction
 Anatomy & Physiology Introduction Anatomy: The study of the structure of an organism and the relationship to its parts Anatomy is derived from the Greek word meaning cutting up which is still how we learn
Anatomy & Physiology Introduction Anatomy: The study of the structure of an organism and the relationship to its parts Anatomy is derived from the Greek word meaning cutting up which is still how we learn
بسم الله الرحمن الرحيم
 بسم الله الرحمن الرحيم * Last lecture we talked about : thoracic wall sternum ribs (according to their features they are divided into typical and atypical) vertebral column ( which is made of 33 vertebrae
بسم الله الرحمن الرحيم * Last lecture we talked about : thoracic wall sternum ribs (according to their features they are divided into typical and atypical) vertebral column ( which is made of 33 vertebrae
Optimisation of Hand Posture Stimulation Using an Electrode Array and Iterative Learning Control
 JOURNAL OF AUTOMATIC CONTROL, UNIVERSITY OF BELGRADE, VOL. 21:1-5, 2013 Optimisation of Hand Posture Stimulation Using an Electrode Array and Iterative Learning Control Timothy A. Exell, Christopher T.
JOURNAL OF AUTOMATIC CONTROL, UNIVERSITY OF BELGRADE, VOL. 21:1-5, 2013 Optimisation of Hand Posture Stimulation Using an Electrode Array and Iterative Learning Control Timothy A. Exell, Christopher T.
MINERVA MEDICA COPYRIGHT
 EUR J PHYS REHABIL MED 2008;44:431-5 Robot-assisted therapy for neuromuscular training of sub-acute stroke patients. A feasibility study Aim. Several studies have described the contribution of robotics
EUR J PHYS REHABIL MED 2008;44:431-5 Robot-assisted therapy for neuromuscular training of sub-acute stroke patients. A feasibility study Aim. Several studies have described the contribution of robotics
Respiration & Trunk control The Great Connection. Brief Review of Normal Development of the Rib Cage
 Respiration & Trunk control The Great Connection. are part of a complex combination of interactive systems. Muscles of respiration are part of the musculature of dynamic postural control. First 3 Years
Respiration & Trunk control The Great Connection. are part of a complex combination of interactive systems. Muscles of respiration are part of the musculature of dynamic postural control. First 3 Years
Paraplegia: Exercise and Health Considerations. By: Juli and Trina
 Paraplegia: Exercise and Health Considerations By: Juli and Trina What is paraplegia? Paraplegia is impairment of motor and/or sensory function to the lower extremities, and sometimes the lower trunk Complete
Paraplegia: Exercise and Health Considerations By: Juli and Trina What is paraplegia? Paraplegia is impairment of motor and/or sensory function to the lower extremities, and sometimes the lower trunk Complete
Pilates for Chronic Low Back Pain
 Pilates for Chronic Low Back Pain Julianne Bettencourt March 23, 2015 Course Year: 2014 Integrated Fitness, Visalia, CA Abstract Low back pain is an injury that affects thousands of people every day and
Pilates for Chronic Low Back Pain Julianne Bettencourt March 23, 2015 Course Year: 2014 Integrated Fitness, Visalia, CA Abstract Low back pain is an injury that affects thousands of people every day and
Onpulse TM technology and the geko TM device: The development of a novel system for the prevention of venous thromboembolism
 Onpulse TM technology and the geko TM device: The development of a novel system for the prevention of venous thromboembolism Tucker AT, Bain DS Jawad H, Bain DS, Dawson H, Adams K, Elnahhas T, Johnston
Onpulse TM technology and the geko TM device: The development of a novel system for the prevention of venous thromboembolism Tucker AT, Bain DS Jawad H, Bain DS, Dawson H, Adams K, Elnahhas T, Johnston
CORE STABILITY & LOW BACK PAIN. Tim Ellis, Physiotherapist BA(Hons) BSc(Hons) MHlthSc(Hons) APA
 BSc(Hons) MHlthSc(Hons) APA") CORE STABILITY & LOW BACK PAIN Tim Ellis, Physiotherapist BA(Hons) BSc(Hons) MHlthSc(Hons) APA 1 Core Stability & Low Back Pain In this 8 page ebook, our Principal Physiotherapist, Tim Ellis, explains
CORE STABILITY & LOW BACK PAIN Tim Ellis, Physiotherapist BA(Hons) BSc(Hons) MHlthSc(Hons) APA 1 Core Stability & Low Back Pain In this 8 page ebook, our Principal Physiotherapist, Tim Ellis, explains
Motor and Gait Improvement in Patients With Incomplete Spinal Cord Injury Induced by High-Frequency Repetitive Transcranial Magnetic Stimulation
 Motor and Gait Improvement in Patients With Incomplete Spinal Cord Injury Induced by High-Frequency Repetitive Transcranial Magnetic Stimulation J. Benito, MD, 1 H. Kumru, PhD, 1 N. Murillo, PhD, 1 U.
Motor and Gait Improvement in Patients With Incomplete Spinal Cord Injury Induced by High-Frequency Repetitive Transcranial Magnetic Stimulation J. Benito, MD, 1 H. Kumru, PhD, 1 N. Murillo, PhD, 1 U.
Pallidal Deep Brain Stimulation
 Pallidal Deep Brain Stimulation Treatment for Dystonia Dystonia Dystonia is a neurological disorder characterized by involuntary muscle contractions resulting in abnormal postures. These movements may
Pallidal Deep Brain Stimulation Treatment for Dystonia Dystonia Dystonia is a neurological disorder characterized by involuntary muscle contractions resulting in abnormal postures. These movements may
GLOSSARY OF TERMS ASSOCIATED WITH TENS
 GLOSSARY OF TERMS ASSOCIATED WITH TENS ATP Adenosine Triphosphate that helps to promote protein synthesis. Accommodation Becoming accustomed to stimulation resulting in nerve and muscle fatigue. Acute
GLOSSARY OF TERMS ASSOCIATED WITH TENS ATP Adenosine Triphosphate that helps to promote protein synthesis. Accommodation Becoming accustomed to stimulation resulting in nerve and muscle fatigue. Acute