Harmony: Ensuring That Your Documentation, OASIS, and Coding Are Compatible
|
|
|
- Whitney Miles
- 6 years ago
- Views:
Transcription

. www.homehealthsection.")
1 Harmony: Ensuring That Your Documentation, OASIS, and Coding Are Compatible Speaker(s): Arlynn Hansell, PT, HCS D, HCS O, COS C Cindy Krafft, PT, MS Session Type: Educational Sessions Session Level: Basic This information is the property of the author(s) and should not be copied or otherwise used without the express written permission of the author(s). Home Health Section of the American Physical Therapy Association Page 1 of 28 total pages
2 Harmony: Ensure your documentation, OASIS and coding are compatible Presented by: Cindy Krafft, MS, PT; CEO Kornetti & Krafft Health Care Solutions Arlynn Hansell, PT, HCS-D, HCS-O, COS-C, Owner, Therapy and More, LLC 1 Disclosure No relevant financial relationship exists for the speakers 2 distributed without permission. 1

3 The Presenters For the past 10 years, Cindy has been a nationally recognized educator in the areas of documentation, regulation, therapy utilization and OASIS. She has served in several national projects as well as an expert resource for OASIS Updates. Her focus is on providing the knowledge and tools to operationalize external requirements. Cindy has been involved at the senior leadership level for the Home Health Section of the American Physical Therapy Association and is the current President of that organization. She has been working with APTA and CMS to clarify regulatory expectations and address proposed payment methodologies to ensure the long term participation of therapy services in home health. She has written 2 books The How-to Guide to Therapy Documentation and An Interdisciplinary Approach to Home Care. 3 The Presenters Arlynn Hansell has been a Physical Therapist in the home health setting since October 1998, holding positions of field therapist, rehab manager, and quality/compliance assurance. As owner of Therapy and More, LLC, she assists agencies in achieving therapy documentation and practice excellence in order to better position themselves against auditors. Consulting services further consist of OASIS auditing and coding practice. She has developed the comprehensive electronic document, e Q&A, containing up-to-date guidance on OASIS Q&As. She remains current with certifications in HCS-D, HCS-O, and COS-C. Arlynn has been a member of the American Physical Therapy Association since 1995, where she currently serves on the Practice Committee of the Home Health Section. She will begin proudly serving her new term as Vice President of the HHS at CSM Arlynn is a member of the BMSC Home Health Advisory Panel, where she serves as Secretary. She is involved in the creation and editing of the HCS-D and HCS-O certification exams. With DecisionHealth, she has developed the online course ICD-10 Coding for Therapists, and is the technical editor of the Home Care Clinical Specialist OASIS C1 Certification Study Guide. 4 distributed without permission. 2
4 Session Objectives Prevent revenue loss and avoid fraud charges. Connect how proper in-depth documentation will enable comprehensive and correct coding and ensure correct OASIS reviews. Integrate OASIS instruction on common difficult M items with audit review commentary. Introduce changes coming in the ICD-10 code set that therapists need to be aware of. 5 Home Health Payment Methodology Being fiscally responsible is NOT the same as being financially driven. 6 distributed without permission. 3
5 Where Does the Money Come From? When the OASIS gets crunched, a CFS score is generated (e.g. C1F2S3), which becomes the HHRG score (e.g ), and translates into the HIPPS (e.g. 1AGMS), which carries a monetary value. Certain M items within the OASIS contribute to the Clinical C score (see next slide) Certain diagnosis codes contribute case mix points as well toward the C score ADL items within the OASIS contribute toward the Functional F score, as well as potentially help toward combining with diagnosis codes to assist with C score points Therapy visits solely contribute toward the Service Utilization S score 7 $$$ OASIS Data Items that Impact Payment (HHRG) M0110 (Episode timing) M1020 (Primary diagnosis) M1022 (Secondary diagnoses) M1024 (Payment diagnoses) M1030 (Therapy at home) M1200 (Vision) M1242 (Pain) M1308 (Number pressure ulcers) M1324 (Most problematic stage) M1334 (Stasis ulcer status) M1342 (Surgical wound status) M1400 (Dyspnea) M1620 (Bowel incontinence) M1630 (Bowel ostomy) M2030 (Injectable medications) M1810 or M1820 (Dressing) M1830 (Bathing) M1840 (Toileting) M1850 (Transferring) M1860 (Ambulation) M2200 (Therapy need) 8 distributed without permission. 4
6 Case Mix Scoring Table Final Rule Dimension 0-13 Therapy Visits 1 st & 2 nd Episodes EARLY Therapy Visits 0-13 Therapy Visits 3 rd + Episodes LATER Therapy Visits All Episodes 20 + Therapy Visits Equation (2 or 4) Clinical C (sum of C points) C Functional (sum of points) F F F Service Utilization (number of therapy visits) S S S S S Effect of Missed visits PPS Amount - Beginning $4, PPS Amount Final $4, PPS Amount Change ($626.73) PPS Begin Casemix Weight PPS End Casemix Weight PPS Casemix Weight Change Beginning Svs Utilization S3 Ending Svs Utilization S1 PPS M2200 Therapy 18 PPS Therapy Utilization 15 PPS PT Vst Bill 9 PPS PT Vst Non Bill 2 PPS OT Vst Bill 6 PPS OT Vst Non Bill 1 Did we lose money?? 10 distributed without permission. 5
7 Chart Threats Recovery Auditors (RACs) employ a staff consisting of nurses, therapists, certified coders and a physician. 2 of the criteria they look for: 1. Improper payments under MCR Parts A and B for services that were not medically necessary 2. Improper payments for services where the documentation does not support the claim. 11 Claim-supported Documentation The claim (chart submitted for payment) should read like it is all the same patient. The Plan of Care (485) must be consistent with OASIS responses in the reporting of diagnoses, mental and functional status, order, goals, etc. In turn, the visit documentation by all disciplines should reflect the 485 and OASIS as well. Troubles begin for agencies when the documentation does not appear cohesive, and visits are performed that do not appear to be necessary for the patient. 12 distributed without permission. 6
8 Results of Analysis Data Concerns that coding, OASIS and therapy utilization data has been influenced by the payment model Cost Questionable accuracy of cost report data and completeness of reporting Correlation Cannot find clear correlation between utilization & patient characteristics/ need End Result Cannot accurately correlate payment to those patients who need greater resources ($) The Home Health Industry is either part of the problem or part of the solution Let s back up: Conditions of Participation Medicare Benefit Policy Manual 2, Chapter 7 holds the guidance for Home Health Services: Section pertains to therapy services: Physical Therapy, Speech-Language Pathology Services, and Occupational Therapy Defines skilled therapy service: The inherent complexity of the service is such that it can be performed safely and/or effectively only by or under the general supervision of a skilled therapist. To be covered, the skilled services must also be reasonable and necessary to the treatment of the patient's illness or injury or to the restoration or maintenance of function affected by the patient's illness or injury. 14 distributed without permission. 7



9 Conditions for Coverage of Therapy Services Skills of a qualified therapist are needed to restore function Patient s condition requires a qualified therapist to design or establish a maintenance program Skills of a qualified therapist are required to perform maintenance therapy Restorative Maintenance Maintenance Medical Necessity Per the Conditions of Participation 2, the services must be consistent with: the nature and severity of the illness or injury, the patient's particular medical needs, the amount, frequency, and duration of the services must be reasonable; and. the services must be considered to be specific, safe, and effective treatment for the patient's condition, meeting the standards noted for the FA (Functional Assessment). 16 distributed without permission. 8
10 Defining Key Therapy Concepts Skill proficiency, facility, or dexterity that is acquired or developed through training or experience; an art, trade, or technique Reasonable governed by or being in accordance with reason or sound thinking; not excessive or extreme Necessary Exclusive to the therapist The amount makes sense The care is indispensible Absolutely essential; needed to achieve a certain result or effect; requisite Making the Connection OASIS Therapy Documentation 18 distributed without permission. 9
11 Does it All Make Sense? SOC ReAssess OASIS Visits Evals 19 Integrating the OASIS into practice One method to correlate documentation to items within the OASIS is by using OASIS item language within the evaluation documentation. 20 distributed without permission. 10
 a.d. used for ambulation and any impact on how clothing is gathered from those locations Safety of the patient in gathering items alone (falls risk, mental impairments, etc.")
12 OASIS Instruction Standard method of teaching 21 What if this were taught as well? Clinicians should go beyond checking the box and document functionally what the patient is required to do in order to dress: The location of the clothing (dresser, closet, wardrobe) a.d. used for ambulation and any impact on how clothing is gathered from those locations Safety of the patient in gathering items alone (falls risk, mental impairments, etc.) Impairments impacting dressing abilities (limited ROM, endurance, mental limitations, etc.) 22 distributed without permission. 11
13 But don t stop there! Clinicians should also document what the patient is unable to perform during the activity and why: can t access the closet due to. difficulty with handling pants and walker simultaneously. required frequent vc for sequencing in the dressing activity required assistance with donning LE items due to right knee flexion limited to 15 degrees Remember, the ADL items are all about the patient s ability to SAFELY perform the task. Any of the above items will impact that safety, potentially showing the need for scores other than [0] independent. 23 OASIS and Care Planning With the added information, the documentation not only supports the OASIS score, but forms the platform for needed skilled intervention, helping to drive the plan of care. 24 distributed without permission. 12
14 ICF Model For the assessment of individuals: What is the person's level of functioning? What is the disability? For individual treatment planning: What treatments or interventions can maximize functioning? From gathering further information into why the patient was scored at a particular level, the criteria for functioning and disability are assessed, allowing the treatment plan to start formulating. 25 M1200 Vision Score [1] or [2] indicates some level of visual deficit. Are the therapists going to fix the vision problem? No. But don t assume then that it has no impact on your practice. Consider how the deficit is affecting visual functioning are there field cuts, a kyphotic posture limiting the visual field, decreased cervical ROM limiting the visual field? How is safety affected? Do compensatory strategies need to be taught? Do you regularly document any visual problems as well as any necessary intervention to adjust for the deficit? Arlynn Hansell and should not be distributed or 26 distributed without permission. 13


, not just ADLs.")
15 Assessing Pain 27 Defining Interfering Pain Pain interferes with activity when the pain results in the activity being performed less often than otherwise desired, requires the patient to have additional assistance in performing the activity, or causes the activity to take longer to complete. Include all activities (e.g., sleeping, recreational activities, watching television), not just ADLs. distributed without permission. 14

16 M1610 Urinary Incontinence Therapists need to investigate why this is occurring: Bladder issues RN Environmental issues OT, MSW Clothing management OT Cognitive implications OT/SLP Mobility PT/OT Is something happening in the home that causes it to be a night only/day only issue? 29 Any incontinence and Falls Number one site of falls in the home: the bathroom In a vain effort to avoid incontinence (bladder or bowel), the client hurries up and ultimately falls, as the increase in gait velocity has rendered them unsteady. PTs can address gait velocity to improve their safety for these situations. Ultimately, this may impact both the gait and transfer items within the OASIS. Is it a velocity issue? How easy was the sit to stand maneuver? Is their assistive device kept within reach? Discuss in the visit note the relationship between the incontinence and activity limitations/impairments 30 distributed without permission. 15
? Have they suffered a loss of recreational activities? Toss out the Theraband!")
17 Depression Need to determine contributing factors Are they depressed because they are homebound? Are they tying their need for care to their self-esteem? Are their life roles changing (from CG to dependent)? Have they suffered a loss of recreational activities? Toss out the Theraband! Maybe they gave up baking or gardening because they didn t know how to modify it! Find out if they have stopped performing their normal recreational activities, and why. Are you even addressing depression in your evaluation (knowing they have a diagnosis of it)? This is important because if it is marked in M2250d that interventions will be provided, and it is coded, the criteria must be addressed at some point during the episode. If this is a therapyonly case, then it is the therapist s responsibility. 31 ADL items As therapists, it is here that we have the opportunity to capitalize on incorporating OASIS documentation into our evaluation and visit notes. Using the same language translates to an easy comparison of apples to apples, readily indicating support of the OASIS score. 32 distributed without permission. 16
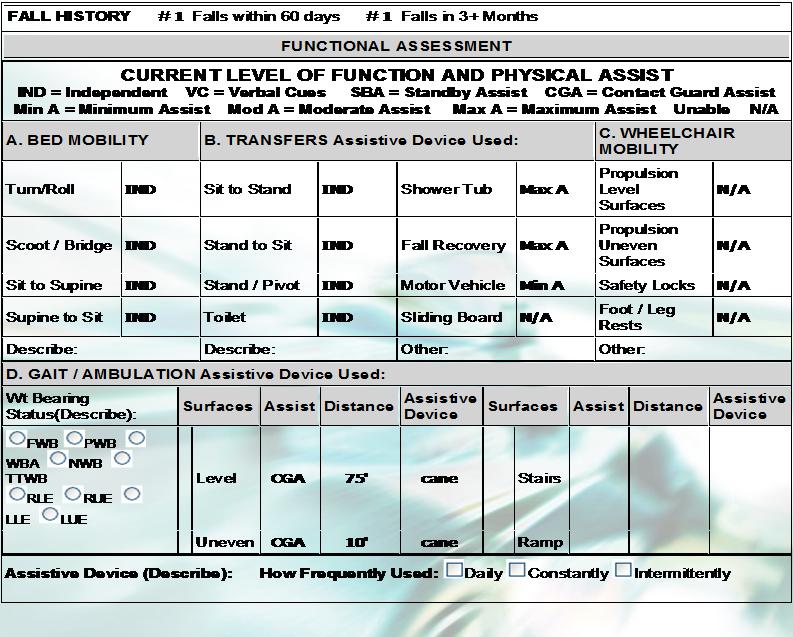
18 Objective Measures Stating the assist level alone is not sufficient, as assistance levels are a subjective opinion, not an objective measure. Qualify it with a description of what the assistance entailed, why it was needed. B. TRANSFERS Assistive Device Used: Note documentation: Sit to Stand SBA Stand to Sit Stand / Pivot Toilet SBA SBA SBA What does this tell you? What else could have been added to the documentation? 33 Quality of Performance For example, how can PT indicate support for the SN that scored the bathing item M1830 as [2] Able to bathe with intermittent assistance? The PT can document: Patient requires verbal cues for walker placement during turns when ambulating, thus mandating assistance for safely accessing the shower. This supports the SOC clinician s choice of [2] for M1830, and helps to drive where treatment is needed. 34 distributed without permission. 17
19 Does that prior statement tell you more than this? Max assistance for what particular activity? What type of assistance? Will the next therapist going in to visit know what specifically needs to be addressed? Assist Level Training / Intervention Rolling L R Assistive Device Supine - max Ax1 Sit Sit - max Ax1 Supine 35 Charting Examples 36 distributed without permission. 18
20 37 38 distributed without permission. 19

 Ambulation/Locomotion: Current ability to walk safely, once in a standing position, or use a wheelchair, once in a seated")
21 39 (M1850) Transferring: Current ability to move safely from bed to chair, or ability to turn and position self in bed if patient is bedfast. 0 - Able to independently transfer 1 - Able to transfer with minimal human assistance or with use of an assistive device 2 - Able to bear weight and pivot during the transfer process but unable to transfer self 3 - Unable to transfer self and is unable to bear weight or pivot when transferred by another person 4 - Bedfast, unable to transfer but is able to turn and position self in bed 5 - Bedfast, unable to transfer and is unable to turn and position self (M1860) Ambulation/Locomotion: Current ability to walk safely, once in a standing position, or use a wheelchair, once in a seated position, on a variety of surfaces. 0 - Able to independently walk on even and uneven surfaces and negotiate stairs with or without railings (i.e., needs no human assistance or assistive device) 1 - With the use of a one-handed device (e.g. cane, single crutch, hemi-walker), able to independently walk on even and uneven surfaces and negotiate stairs with or withoutrailings 2 - Requires use of a two-handed device (e.g., walker or crutches) to walk alone on a level surface and/or requires human supervision or assistance to negotiate stairs or steps or uneven surfaces 3 - Able to walk only with the supervision or assistance of another person at all times 40 distributed without permission. 20
22 Another example.. 41 D. GAIT / AMBULATION Assistive Device Used: Wt Bearing Status(Describe): Surface s Assis t Distanc e Assistiv e Device Surface s Assis t Distanc e Assistiv e Device FWB PWB WBA NWB TTWB Clear RLE RUE Level UA 0 FWW Stair s LLE LUE Clear Uneve n UA 0 FWW Ram p (M1860) Ambulation/Locomotion: Current ability to walk safely, once in a standing position, or use a wheelchair, once in a seated position, on a variety of surfaces. 0 - Able to independently walk on even and uneven surfaces and negotiate stairs with or without railings (i.e., needs no human assistance or assistive device) 1 - With the use of a one-handed device (e.g. cane, single crutch, hemi-walker), able to independently walk on even and uneven surfaces and negotiate stairs with or withoutrailings 2 - Requires use of a two-handed device (e.g., walker or crutches) to walk alone on a level surface and/or requires human supervision or assistance to negotiate stairs or steps or uneven surfaces 3 - Able to walk only with the supervision or assistance of another person at all times 42 distributed without permission. 21

23 B. TRANSFERS Assistive Device Used: Sit to Stand SBA Shower Tub Min A Stand to Sit SBA Fall Recovery Max A Stand / Pivot SBA Motor Vehicle Min A Toilet SBA Sliding Board N/A 43 ICD-10: documentation and the therapist 44 distributed without permission. 22
24 Guidance has not changed for the pending ICD-10 code set in that all of the top six diagnoses must be addressed in the POC through assessment/evaluation or treatment. When a chart is coded, what is listed should be only those diagnoses that 3 : will be monitored, evaluated, or treated by the agency, or those that will impact the treatment of the patient 45 Ensure all diagnoses are confirmed or validated by the physician. If a particular diagnosis is not originally stated in the medical record (referral, H&P, F2F, etc.), documentation must be included in the medical chart of query with confirmation. What shouldn t get coded: long-term conditions that are stable or have no direct impact on the POC (e.g., GERD, anemia). 46 distributed without permission. 23




 47 Documentation in ICD-9-CM Documentation in ICD-10-CM Was the")

25 In addition to greater attention to coding the true underlying condition, documentation of that condition needs to be enhanced in preparation for the greater specificity of ICD- 10. More detail will be required, and what that means for the therapist is deeper investigation of what happened to the patient, more detail about the comorbidities, and more specific documentation will be mandatory. For instance: Fractures need specific location, closed vs. open, displaced vs. nondisplaced Pressure ulcers need exact location (R vs. L) and stage Other ulcers need etiology per MD, clinician will need to stage it (depth of ulcer) 47 Documentation in ICD-9-CM Documentation in ICD-10-CM Was the fracture more involved? Hip fracture what part of the bone was involved Right versus Left open or closed displaced versus nondisplaced fx was the healing routine or delayed malunion versus nonunion Is the present condition actually a sequela from an earlier condition 48 distributed without permission. 24
26 Gait In ICD-9 4, gait has basically three options for coding for Difficulty in Walking, Abnormal Gait and Ataxia. In ICD-10 5, the option has expanded to 6 categories, so descriptive documentation and correct verbiage is important so that the codes assigned are appropriate. 1. R26.0 Ataxic gait 2. R26.1 Paralytic gait 3. R26.2 Difficulty in walking, not elsewhere classified 4. R26.8 Other abnormalities of gait and mobility R26.81 Unsteadiness on feet R26.89 Other abnormalities of gait and mobility 5. R26.9 Unspecified abnormalities of gait and mobility 6. R27.0 Ataxia, unspecified 49 Description of gait codes The six gait categories are expanded on the next slide. Essentially, the coding guidelines state that clinicians should investigate the cause of the gait abnormality. If the gait abnormality is integral to the condition causing the abnormal gait, then code the condition and not the abnormal gait. 50 distributed without permission. 25
 is integral to a patient with hemiplegia due to a CVA, lower back pain, or when using aftercare following joint replacement (Z47.")
27 51 For patients needing gait training, the correct principal diagnosis code usually is the illness, especially if there is a disease code indicating gait problem as part of the illness. For example, abnormalities of gait and mobility category, (R26.-) is integral to a patient with hemiplegia due to a CVA, lower back pain, or when using aftercare following joint replacement (Z47.1) of the lower extremity. If the therapist or physician documents abnormal gait or unsteady gait, attempt to obtain the definitive diagnosis or a more specific description of the abnormal gait problem, such as R26.0 (ataxic gait), R26.1 (paralytic gait), R26.81 (unsteadiness on feet gait), R26.89 (other abnormalities of gait and mobility), or R26.9 (unspecified abnormalities of gait and mobility). If the patient has difficulty walking associated with a chronic condition of the bone or joint, R26.2 (difficulty in walking, not elsewhere classified) is the appropriate code to use. 52 distributed without permission. 26
28 REFERENCES 1. Federal Register. Vol.79 No. 215 Section 42 CFR. Nov.6, CMS Medicare Benefit Policy Manual. Chapter 7. Section Rev. 144, latest issue Instruments/HomeHealthQualityInits/Downloads/HHQIAttachmentD.pdf. Accessed July 6, ICD-9-CM Official Guidelines for Coding and Reporting, ICD-10-CM Official Guidelines for Coding and Reporting, distributed without permission. 27
Girling Reviewer Training: Session 1. Therapy Practice in 2011: What the Reviewers Need to Know. May 10, 2011
 Girling Reviewer Training: Session 1 Therapy Practice in 2011: What the Reviewers Need to Know May 10, 2011 Presented by: Nancy Buseth RN, PT Senior Rehabilitation Consultant Fazzi Associates, Inc. 243
Girling Reviewer Training: Session 1 Therapy Practice in 2011: What the Reviewers Need to Know May 10, 2011 Presented by: Nancy Buseth RN, PT Senior Rehabilitation Consultant Fazzi Associates, Inc. 243
What am I Looking For?: A Reviewer s Guide to Therapy Documentation
 What am I Looking For?: A Reviewer s Guide to Therapy Documentation Presented By: Cindy Krafft MS PT, COS-C Director of Rehabilitation Consulting Services President - Home Health Section APTA November
What am I Looking For?: A Reviewer s Guide to Therapy Documentation Presented By: Cindy Krafft MS PT, COS-C Director of Rehabilitation Consulting Services President - Home Health Section APTA November
Therapy Documentation: Beyond Reasonable and Necessary
 Therapy Documentation: Beyond Reasonable and Necessary August 30, 2012 Presented by: Cindy Krafft PT, MS Director of Rehabilitation Consulting Services Fazzi Associates 243 King Street, Suite 246 Northampton,
Therapy Documentation: Beyond Reasonable and Necessary August 30, 2012 Presented by: Cindy Krafft PT, MS Director of Rehabilitation Consulting Services Fazzi Associates 243 King Street, Suite 246 Northampton,
Therapy Goals and Reassessments: Setting the Expectations
 Therapy Goals and Reassessments: Setting the Expectations Presented by: Cindy Krafft PT, MS Director of Rehabilitation Consulting Services Fazzi Associates, Inc. 243 King Street, Suite 246 Northampton,
Therapy Goals and Reassessments: Setting the Expectations Presented by: Cindy Krafft PT, MS Director of Rehabilitation Consulting Services Fazzi Associates, Inc. 243 King Street, Suite 246 Northampton,
Managing Non-Routine Medical Supplies
 Managing Non-Routine Medical Supplies DecisionHealth Teleconference September 23, 2008 Lynda Laff Laff Associates 117 Club Course Drive Hilton Head Island, South Carolina 29928 (843) 671-4170 llaff@laffassociates.com
Managing Non-Routine Medical Supplies DecisionHealth Teleconference September 23, 2008 Lynda Laff Laff Associates 117 Club Course Drive Hilton Head Island, South Carolina 29928 (843) 671-4170 llaff@laffassociates.com
PT Visit with Supervisory Visit
 Clinician: Mileage: Gender: Agency Name/Branch: M F Time In: Time Out: DOB: HCPCS Select the home health service type that reflects the primary reason for this visit: (G0151) Services Performed by a qualified
Clinician: Mileage: Gender: Agency Name/Branch: M F Time In: Time Out: DOB: HCPCS Select the home health service type that reflects the primary reason for this visit: (G0151) Services Performed by a qualified
Patient Name (Last Name, First Name) & MRN: Mileage: Gender: Agency Name/Branch: DOB: / / BP: (Prior) Position Side Heart Rate: Respirations:
 & MRN: Mileage: Gender: Agency Name/Branch: DOB: / / BP: (Prior) Position Side Heart Rate: Respirations:") Clinician: Mileage: Gender: Agency Name/Branch: M F Time In: Time Out: DOB: HCPCS Select the home health service type that reflects the primary reason for this visit: (G0152) Services Performed by a qualified
Clinician: Mileage: Gender: Agency Name/Branch: M F Time In: Time Out: DOB: HCPCS Select the home health service type that reflects the primary reason for this visit: (G0152) Services Performed by a qualified
Housekeeping. Co-Treatment: A Creative Partnership. Harmony Healthcare International, Inc. Objectives. Copyright 2012 All Rights Reserved 1
 Co-Treatment: A Creative Partnership HARMONY UNIVERSITY The Provider Unit of (HHI) Presented by: Carrie Mullin, OTR/L Corporate Consultant/Denial Manager Cyndi Ouellette, RPT Regional Director of Operations
Co-Treatment: A Creative Partnership HARMONY UNIVERSITY The Provider Unit of (HHI) Presented by: Carrie Mullin, OTR/L Corporate Consultant/Denial Manager Cyndi Ouellette, RPT Regional Director of Operations
Risk Adjustment for Clinicians. Risk Adjustment Resource. Logistic Regression Models 4/2/2012
 Risk Adjustment for Clinicians Teresa Northcutt RN BSN COS C HCS D Missouri Alliance for Home Care Annual Conference 2012 Risk Adjustment Resource Home Health Agency Quality Measures: Logistic Regression
Risk Adjustment for Clinicians Teresa Northcutt RN BSN COS C HCS D Missouri Alliance for Home Care Annual Conference 2012 Risk Adjustment Resource Home Health Agency Quality Measures: Logistic Regression
MAHC 10 FALL RISK ASSESSMENT Clinician Education Program
 MAHC 10 FALL RISK ASSESSMENT Clinician Education Program The MAHC 10 is a multi factorial, validated fall assessment especially designed for use with community dwelling patients. It fully satisfies the
MAHC 10 FALL RISK ASSESSMENT Clinician Education Program The MAHC 10 is a multi factorial, validated fall assessment especially designed for use with community dwelling patients. It fully satisfies the
Top 10 ICD-10 Coding Errors (and how to fix them!) Presented by Jennifer Warfield, BSN, HCS-D, COS-C Education Director, PPS Plus
 Presented by Jennifer Warfield, BSN, HCS-D, COS-C Education Director, PPS Plus") (and how to fix them!) Presented by Jennifer Warfield, BSN, HCS-D, COS-C Education Director, PPS Plus Top 10 ICD-10 Coding Errors (and how to fix them!) Top 10 Primary Diagnoses In ICD-10 ICD-10 Codes
(and how to fix them!) Presented by Jennifer Warfield, BSN, HCS-D, COS-C Education Director, PPS Plus Top 10 ICD-10 Coding Errors (and how to fix them!) Top 10 Primary Diagnoses In ICD-10 ICD-10 Codes
Summary Slide. Summary Slide. Documentation. Summary Slide. Documentation
 Summary Slide Summary Slide Summary Slide Documentation Documentation 1 Documentation Evidence of Patient Care Evidence of patient care Proves care was given Reason for treatment Treatment effectiveness
Summary Slide Summary Slide Summary Slide Documentation Documentation 1 Documentation Evidence of Patient Care Evidence of patient care Proves care was given Reason for treatment Treatment effectiveness
Clinical Information for Wheeled Mobility Page 1 of 6
 Clinical Information for Wheeled Mobility Page 1 of 6 PART A: PATIENT / PROVIDER INFORMATION - Please Print Name: Sponsor Soc. Sec. No: Address: City: St: Zip: Phone: ( ) Age: Sex: Height: Weight: Date
Clinical Information for Wheeled Mobility Page 1 of 6 PART A: PATIENT / PROVIDER INFORMATION - Please Print Name: Sponsor Soc. Sec. No: Address: City: St: Zip: Phone: ( ) Age: Sex: Height: Weight: Date
CMS CLARIFICATION JIMMO VS. SEBELIUS
 CMS CLARIFICATION JIMMO VS. SEBELIUS Liz Almeida-Sanborn, MS, PT, President Maria Maggi, PT, Vice President of Compliance Jodi Wenzel, MPT, Vice President of Operations OBJECTIVES Participants will: Understand
CMS CLARIFICATION JIMMO VS. SEBELIUS Liz Almeida-Sanborn, MS, PT, President Maria Maggi, PT, Vice President of Compliance Jodi Wenzel, MPT, Vice President of Operations OBJECTIVES Participants will: Understand
Financial & Management Aspects of OASIS C2
 Financial & Management Aspects of OASIS C2 Presented By: Melinda A. Gaboury, COS C Healthcare Provider Solutions, Inc. 615 399 7499 info@healthcareprovidersolutions.com WHAT DOES OASIS C2 IMPACT? HHRG/HIPPS
Financial & Management Aspects of OASIS C2 Presented By: Melinda A. Gaboury, COS C Healthcare Provider Solutions, Inc. 615 399 7499 info@healthcareprovidersolutions.com WHAT DOES OASIS C2 IMPACT? HHRG/HIPPS
Total Hip Replacement Rehabilitation: Progression and Restrictions
 Total Hip Replacement Rehabilitation: Progression and Restrictions The success of total hip replacement (THR) is a result of predictable pain relief, improvements in quality of life, and restoration of
Total Hip Replacement Rehabilitation: Progression and Restrictions The success of total hip replacement (THR) is a result of predictable pain relief, improvements in quality of life, and restoration of
Gregory H. Tchejeyan, M.D. Orthopaedic Surgery of the Hip and Knee
 TOTAL KNEE REPLACEMENT (TKR) POST-OPERATIVE REHABILITATION PROTOCOL PRE-OPERATIVE PHYSICAL THERAPY The patient is seen for a pre-operative physical therapy session which includes: o Review of the TKR protocol.
TOTAL KNEE REPLACEMENT (TKR) POST-OPERATIVE REHABILITATION PROTOCOL PRE-OPERATIVE PHYSICAL THERAPY The patient is seen for a pre-operative physical therapy session which includes: o Review of the TKR protocol.
Physical Therapy Diagnosis and Documentation Tips
 1 This tool is designed to assist the Physical Therapist in consultation with the physician, in the selection of an appropriate according to Medicare coverage guidelines. The documentation tips will add
1 This tool is designed to assist the Physical Therapist in consultation with the physician, in the selection of an appropriate according to Medicare coverage guidelines. The documentation tips will add
2 Master the ICD 10 Payment System to Prevent Revenue Losses
 Master the ICD 10 Payment System to Prevent Revenue Losses Tricia A. Twombly BSN RN HCS D HCS O COS C CHCE AHIMA Approved ICD 10 CM Trainer Senior Director, DecisionHealth Chief Executive Officer, BMSC
Master the ICD 10 Payment System to Prevent Revenue Losses Tricia A. Twombly BSN RN HCS D HCS O COS C CHCE AHIMA Approved ICD 10 CM Trainer Senior Director, DecisionHealth Chief Executive Officer, BMSC
PREVENTING FALLS AT HOME
 PREVENTING FALLS AT HOME INFORMATION FOR OLDER ADULTS, FAMILIES, AND CAREGIVERS READ THIS PAMPHLET TO LEARN: The Dangers of Falls. When You Are at Risk for a Fall. How You Can Help Prevent Falls at Home.
PREVENTING FALLS AT HOME INFORMATION FOR OLDER ADULTS, FAMILIES, AND CAREGIVERS READ THIS PAMPHLET TO LEARN: The Dangers of Falls. When You Are at Risk for a Fall. How You Can Help Prevent Falls at Home.
Total Hip Replacement Protocol
 Total Hip Replacement Protocol Applicability: Physician Practice Date Effective: 12/2016 Department: Rehabilitation Services Supersedes: Total Hip Replacement Standard of Care Date Last Reviewed / or Date
Total Hip Replacement Protocol Applicability: Physician Practice Date Effective: 12/2016 Department: Rehabilitation Services Supersedes: Total Hip Replacement Standard of Care Date Last Reviewed / or Date
Fall Prevention: A Primer for CNAs. 1.0 Inservice Hour
 Fall Prevention: A Primer for CNAs 1.0 Inservice Hour NOTE: This course is not accredited for RNs, LPNs, LVNs, or APNs. This course is approved for 1 contact hour (1 inservice hour) for Certified Nursing
Fall Prevention: A Primer for CNAs 1.0 Inservice Hour NOTE: This course is not accredited for RNs, LPNs, LVNs, or APNs. This course is approved for 1 contact hour (1 inservice hour) for Certified Nursing
COURSE OUTLINE. Course Number Course Title Credits PTA 210 PTA Techniques & Modalities 4. Pre-requisite PTA 106, PTA 112 Co-requisite PTA 211
 COURSE OUTLINE Course Number Course Title Credits PTA 210 PTA Techniques & Modalities 4 Hours: lecture/lab/other 3/2/0 Catalog description: Pre-requisite PTA 106, PTA 112 Co-requisite PTA 211 Implementation
COURSE OUTLINE Course Number Course Title Credits PTA 210 PTA Techniques & Modalities 4 Hours: lecture/lab/other 3/2/0 Catalog description: Pre-requisite PTA 106, PTA 112 Co-requisite PTA 211 Implementation
TABLE 3: CY 2019 CASE-MIX ADJUSTMENT VARIABLES AND SCORES
 TABLE 3: CY 2019 CASE-MIX ADJUSTMENT VARIABLES SCORES Episode number within sequence of adjacent episodes 1 or 2 1 or 2 3+ 3+ Therapy 0-13 14+ 0-13 14+ EQUATION: 1 2 3 4 CLINICAL DIMENSION 1 Primary or
TABLE 3: CY 2019 CASE-MIX ADJUSTMENT VARIABLES SCORES Episode number within sequence of adjacent episodes 1 or 2 1 or 2 3+ 3+ Therapy 0-13 14+ 0-13 14+ EQUATION: 1 2 3 4 CLINICAL DIMENSION 1 Primary or
9/5/2016. Documenting Compliantly and Efficiently: Best Practices and Techniques. Course Objectives. Legal Disclaimer
 Documenting Compliantly and Efficiently: Best Practices and Techniques Veda Collmer, Esq., OTR/L Course Objectives Participants will be able to identify basic information required for documenting in the
Documenting Compliantly and Efficiently: Best Practices and Techniques Veda Collmer, Esq., OTR/L Course Objectives Participants will be able to identify basic information required for documenting in the
Physical Therapy. Physical Therapy Payment Policy Page 1
 Physical Therapy I. Policy University Health Alliance (UHA) will reimburse for physical therapy when it is determined to be medically necessary and when it meets the medical criteria guidelines (subject
Physical Therapy I. Policy University Health Alliance (UHA) will reimburse for physical therapy when it is determined to be medically necessary and when it meets the medical criteria guidelines (subject
January 2013 CMS Quarterly Q&As
 Category 2 January 2013 CMS Quarterly Q&As Question 1. We have been receiving an increased number of TRICARE pediatric/newborn patient referrals who require OASIS documentation. Our pediatric/maternity
Category 2 January 2013 CMS Quarterly Q&As Question 1. We have been receiving an increased number of TRICARE pediatric/newborn patient referrals who require OASIS documentation. Our pediatric/maternity
Occupational Therapy. Occupational Therapy Payment Policy Page 1
 Occupational Therapy I. Policy Occupational therapy is a form of rehabilitation therapy involving the treatment of neuromusculoskeletal function through the use of specific tasks or goal-directed activities
Occupational Therapy I. Policy Occupational therapy is a form of rehabilitation therapy involving the treatment of neuromusculoskeletal function through the use of specific tasks or goal-directed activities
Therapy Utilization: Getting it Right
 Therapy Utilization: Getting it Right Presented By: Cindy Krafft MS PT Director of Rehabilitation Consulting Services December 15, 2011 243 King Street, Suite 246 Northampton, MA 01060 Phone: 413-584-5300
Therapy Utilization: Getting it Right Presented By: Cindy Krafft MS PT Director of Rehabilitation Consulting Services December 15, 2011 243 King Street, Suite 246 Northampton, MA 01060 Phone: 413-584-5300
Improving your value as an Athletic Trainer
 Improving your value as an Athletic Trainer Presented by Amy DeRosa Vice President and Partner, IncreMedical and Medadept Pennsylvania Athletic Trainers Society, Inc. Annual Meeting General Session June
Improving your value as an Athletic Trainer Presented by Amy DeRosa Vice President and Partner, IncreMedical and Medadept Pennsylvania Athletic Trainers Society, Inc. Annual Meeting General Session June
A A ~l~js AM f'ricj\n ACADBl\IY OF 0RTllOPAEDIC SURGEONS ~ J AMERICAN A SOCIATION OF ORTHOPAEDIC SURGEONS. Therapy billing for beginners
 Therapy billing for beginners http://www.aaos.org/news/aaosnow/nov10/managing1.asp 1 of 4 3/25/2014 2:56 PM A A ~l~js AM f'ricj\n ACADBl\IY OF 0RTllOPAEDIC SURGEONS ~ J AMERICAN A SOCIATION OF ORTHOPAEDIC
Therapy billing for beginners http://www.aaos.org/news/aaosnow/nov10/managing1.asp 1 of 4 3/25/2014 2:56 PM A A ~l~js AM f'ricj\n ACADBl\IY OF 0RTllOPAEDIC SURGEONS ~ J AMERICAN A SOCIATION OF ORTHOPAEDIC
Stroke. Objectives: After you take this class, you will be able to:
 Stroke Objectives: After you take this class, you will be able to: 1. Describe the signs of a stroke and how a stroke happens. 2. Discuss stroke risk factors. 3. Detail the care and rehabilitation of a
Stroke Objectives: After you take this class, you will be able to: 1. Describe the signs of a stroke and how a stroke happens. 2. Discuss stroke risk factors. 3. Detail the care and rehabilitation of a
Functional Activity and Mobility
 Functional Activity and Mobility Documentation for Hospitalized Adult The Johns Hopkins University and The Johns Hopkins Health System Corporation Goals for Documentation of Activity and Mobility To develop
Functional Activity and Mobility Documentation for Hospitalized Adult The Johns Hopkins University and The Johns Hopkins Health System Corporation Goals for Documentation of Activity and Mobility To develop
PRACTICAL SOLUTIONS TO REHAB DEMENTIA CARE PART 1 PROMOTING EACH PERSON S BEST ABILITY TO FUNCTION
 The Dementia Problem PRACTICAL SOLUTIONS TO REHAB DEMENTIA CARE PART 1 PROMOTING EACH PERSON S BEST ABILITY TO FUNCTION Efficient, practical & compassionate service is more important than ever before Aging
The Dementia Problem PRACTICAL SOLUTIONS TO REHAB DEMENTIA CARE PART 1 PROMOTING EACH PERSON S BEST ABILITY TO FUNCTION Efficient, practical & compassionate service is more important than ever before Aging
Physical Medicine & Rehabilitation: Maximum Combined Frequency per Day Policy
 Policy Number Physical Medicine & Rehabilitation: Maximum Combined Frequency per Day Policy 2017R0101E Annual Approval Date 7/13/2016 Approved By Payment Policy Oversight Committee IMPORTANT NOTE ABOUT
Policy Number Physical Medicine & Rehabilitation: Maximum Combined Frequency per Day Policy 2017R0101E Annual Approval Date 7/13/2016 Approved By Payment Policy Oversight Committee IMPORTANT NOTE ABOUT
ICD-9-CM Home Health Coding Impact on Reimbursement
 ICD-9-CM Home Health Coding Impact on Reimbursement Presented by HealthCare ConsultLink Linda Parker, RN, BSN, COS-C, HCS-D Objectives Identify principles for determining primary/secondary diagnoses Identify
ICD-9-CM Home Health Coding Impact on Reimbursement Presented by HealthCare ConsultLink Linda Parker, RN, BSN, COS-C, HCS-D Objectives Identify principles for determining primary/secondary diagnoses Identify
Rehab to Home. Stroke Recovery EDUCATION BOOKLET FOR: Care & Safety Tips. Frequently Asked Questions. Working Toward Independence. Adaptive Equipment
 Stroke Recovery Rehab to Home Care & Safety Tips Frequently Asked Questions Working Toward Independence Adaptive Equipment Summary of Progress Different Types of Therapy Personal Goals EDUCATION BOOKLET
Stroke Recovery Rehab to Home Care & Safety Tips Frequently Asked Questions Working Toward Independence Adaptive Equipment Summary of Progress Different Types of Therapy Personal Goals EDUCATION BOOKLET
Provider No Onset Date SOC Date. Clinical Interview
 Plan of Treatment Provider No Onset SOC Clinical Interview The Interview was completed with: Patient Spouse Caregiver Other: Patient Age: Years Mental Status: Alert Oriented x Impaired: Living Situation
Plan of Treatment Provider No Onset SOC Clinical Interview The Interview was completed with: Patient Spouse Caregiver Other: Patient Age: Years Mental Status: Alert Oriented x Impaired: Living Situation
Post Operative Total Hip Replacement Protocol Brian J. White, MD
 Post Operative Total Hip Replacement Protocol Brian J. White, MD www.western-ortho.com The intent of this protocol is to provide guidelines for progression of rehabilitation. It is not intended to serve
Post Operative Total Hip Replacement Protocol Brian J. White, MD www.western-ortho.com The intent of this protocol is to provide guidelines for progression of rehabilitation. It is not intended to serve
Posterior/Direct Total Hip Arthroplasty Rehabilitation Guideline
 Posterior/Direct Total Hip Arthroplasty Rehabilitation Guideline This rehabilitation program is designed to return the individual to their activities as quickly and safely as possible. It is designed for
Posterior/Direct Total Hip Arthroplasty Rehabilitation Guideline This rehabilitation program is designed to return the individual to their activities as quickly and safely as possible. It is designed for
Navigating the Challenges of Hospice Coding. Coding has never been so important for the hospice industry.
 Navigating the Challenges of Hospice Coding Coding has never been so important for the hospice industry. Presentation team: Dawn B. Cheek RN, BSN Clinical Consulting Manager, McBee Associates, Inc. Elizabeth
Navigating the Challenges of Hospice Coding Coding has never been so important for the hospice industry. Presentation team: Dawn B. Cheek RN, BSN Clinical Consulting Manager, McBee Associates, Inc. Elizabeth
Chapter 23. Assisting With Exercise and Activity
 Chapter 23 Assisting With Exercise and Activity Exercise and Activity Illness, surgery, injury, pain, and aging can limit activity. Inactivity, whether mild or severe: Affects every body system Affects
Chapter 23 Assisting With Exercise and Activity Exercise and Activity Illness, surgery, injury, pain, and aging can limit activity. Inactivity, whether mild or severe: Affects every body system Affects
Physical Therapy MM /15/2003
 Physical Therapy Policy Number: Original Effective Date: MM.09.005 07/15/2003 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 06/23/2017 Line(s) of Business Excluded: Federal Employee
Physical Therapy Policy Number: Original Effective Date: MM.09.005 07/15/2003 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 06/23/2017 Line(s) of Business Excluded: Federal Employee
SAULT COLLEGE OF APPLIED ARTS AND TECHNOLOGY SAULT STE. MARIE, ONTARIO COURSE OUTLINE
 SAULT COLLEGE OF APPLIED ARTS AND TECHNOLOGY SAULT STE. MARIE, ONTARIO COURSE OUTLINE COURSE TITLE: Occupational Therapy Principles & CODE NO. : SEMESTER: 2 PROGRAM: AUTHOR: Occupational Therapist Assistant/Physiotherapist
SAULT COLLEGE OF APPLIED ARTS AND TECHNOLOGY SAULT STE. MARIE, ONTARIO COURSE OUTLINE COURSE TITLE: Occupational Therapy Principles & CODE NO. : SEMESTER: 2 PROGRAM: AUTHOR: Occupational Therapist Assistant/Physiotherapist
Falls Prevention Strategy
 Falls Prevention Strategy Accessible Formats & Communication Supports Special accessibility accommodations and materials in alternate formats can be arranged by contacting Brain Injury Community Re-entry
Falls Prevention Strategy Accessible Formats & Communication Supports Special accessibility accommodations and materials in alternate formats can be arranged by contacting Brain Injury Community Re-entry
Knee Replacement PROGRAM. Nightingale. Home Healthcare
 Knee Replacement PROGRAM TM Nightingale Home Healthcare With the help of Nightingale s experienced and professional rehabilitation team, you will be guided through a more complete and successful recovery
Knee Replacement PROGRAM TM Nightingale Home Healthcare With the help of Nightingale s experienced and professional rehabilitation team, you will be guided through a more complete and successful recovery
REX REX Clinical Assessment Guide
 REX Clinical Assessment Guide All product names and brand names in this document are trademarks or registered trademarks of their respective holders. Copyright Rex Bionics Ltd 2016. All rights reserved.
REX Clinical Assessment Guide All product names and brand names in this document are trademarks or registered trademarks of their respective holders. Copyright Rex Bionics Ltd 2016. All rights reserved.
A PHYSIATRIC APPROACH TO PATIENTS WITH FACIOSCAPULOHUMERAL MUSCULAR DYSTROPHY
 A PHYSIATRIC APPROACH TO PATIENTS WITH FACIOSCAPULOHUMERAL MUSCULAR DYSTROPHY SUSAN KEESHIN M.D. MEDICAL DIRECTOR DAY REHAB THE SHIRLEY RYAN ABILITY LAB (FORMERLY KNOWN AS RIC) WHAT IS A PHYSIATRIST AND
A PHYSIATRIC APPROACH TO PATIENTS WITH FACIOSCAPULOHUMERAL MUSCULAR DYSTROPHY SUSAN KEESHIN M.D. MEDICAL DIRECTOR DAY REHAB THE SHIRLEY RYAN ABILITY LAB (FORMERLY KNOWN AS RIC) WHAT IS A PHYSIATRIST AND
How Biodex programs give UHS Pruitt the clinical advantage BIODEX
 CASESTUDY How Biodex programs give UHS Pruitt the clinical advantage UHS Pruitt Corporation BIODEX Biodex Medical Systems, Inc. 20 Ramsey Road, Shirley, New York, 11967-4704, Tel: 800-224-6339 (Int l 631-924-9000),
CASESTUDY How Biodex programs give UHS Pruitt the clinical advantage UHS Pruitt Corporation BIODEX Biodex Medical Systems, Inc. 20 Ramsey Road, Shirley, New York, 11967-4704, Tel: 800-224-6339 (Int l 631-924-9000),
Hip Replacement PROGRAM. Nightingale. Home Healthcare
 Hip Replacement PROGRAM TM Nightingale Home Healthcare Why Do I Need A Hip Replacement? Hip replacements are performed for one reason; something has happened to the hip joint that has made it 1) too painful
Hip Replacement PROGRAM TM Nightingale Home Healthcare Why Do I Need A Hip Replacement? Hip replacements are performed for one reason; something has happened to the hip joint that has made it 1) too painful
PHYSICAL MEDICINE AND REHABILITATION CSHCN SERVICES PROGRAM PROVIDER MANUAL
 PHYSICAL MEDICINE AND REHABILITATION CSHCN SERVICES PROGRAM PROVIDER MANUAL NOVEMBER 2017 CSHCN PROVIDER PROCEDURES MANUAL NOVEMBER 2017 PHYSICAL MEDICINE AND REHABILITATION Table of Contents 30.1 Enrollment......................................................................
PHYSICAL MEDICINE AND REHABILITATION CSHCN SERVICES PROGRAM PROVIDER MANUAL NOVEMBER 2017 CSHCN PROVIDER PROCEDURES MANUAL NOVEMBER 2017 PHYSICAL MEDICINE AND REHABILITATION Table of Contents 30.1 Enrollment......................................................................
FSBPT Supervised Clinical Practice Performance Evaluation Tool
 1. Practices in a manner that is safe for the patient 1.1. Responds appropriately in emergency situations 1.2. Recognizes and responds to unexpected changes in patient's physiological condition 1.3. Utilizes
1. Practices in a manner that is safe for the patient 1.1. Responds appropriately in emergency situations 1.2. Recognizes and responds to unexpected changes in patient's physiological condition 1.3. Utilizes
PREVENTING FALLS AT HOME
 PREVENTING FALLS AT HOME INFORMATION FOR OLDER ADULTS, FAMILIES, AND CAREGIVERS READ THIS PAMPHLET TO LEARN: The Dangers of Falls. When You Are at Risk for a Fall. How You Can Help Prevent Falls at Home.
PREVENTING FALLS AT HOME INFORMATION FOR OLDER ADULTS, FAMILIES, AND CAREGIVERS READ THIS PAMPHLET TO LEARN: The Dangers of Falls. When You Are at Risk for a Fall. How You Can Help Prevent Falls at Home.
Medicare Documentation Guidelines For Physical Therapy 2011
 Medicare Documentation Guidelines For Physical Therapy 2011 As we move right along with our review of documentation strategies, this week we will for Medicare Part B and for carriers who follow Medicare
Medicare Documentation Guidelines For Physical Therapy 2011 As we move right along with our review of documentation strategies, this week we will for Medicare Part B and for carriers who follow Medicare
Presented By: Jennifer Birt, OT Reg(MB) Specialized Seating & Mobility Clinical Specialist
 Specialized Seating & Mobility Clinical Specialist") Presented By: Jennifer Birt, OT Reg(MB) Specialized Seating & Mobility Clinical Specialist 2013 1. Define and understand the concept of practical pressure management and categorizing individuals at different
Presented By: Jennifer Birt, OT Reg(MB) Specialized Seating & Mobility Clinical Specialist 2013 1. Define and understand the concept of practical pressure management and categorizing individuals at different
Key Components of Fall Prevention Rein Tideiksaar, PhD FallPrevent, LLC
 Key Components of Fall Prevention Rein Tideiksaar, PhD FallPrevent, LLC This program was supported by a grant from Steps Key Components of Fall Prevention Rein Tideiksaar, PhD FallPrevent, LLC Actions
Key Components of Fall Prevention Rein Tideiksaar, PhD FallPrevent, LLC This program was supported by a grant from Steps Key Components of Fall Prevention Rein Tideiksaar, PhD FallPrevent, LLC Actions
Evaluating Functional Status in Hospitalized Geriatric Patients. UCLA-Santa Monica Geriatric Medicine Didactic Lecture Series
 Evaluating Functional Status in Hospitalized Geriatric Patients UCLA-Santa Monica Geriatric Medicine Didactic Lecture Series Case 88 y.o. woman was admitted for a fall onto her hip. She is having trouble
Evaluating Functional Status in Hospitalized Geriatric Patients UCLA-Santa Monica Geriatric Medicine Didactic Lecture Series Case 88 y.o. woman was admitted for a fall onto her hip. She is having trouble
Physical and Occupational Therapy after Spine Surgery. Preparation for your surgery
 Physical and Occupational Therapy after Spine Surgery Preparation for your surgery Agenda Pre-Operative Exercises What to Expect Post-Operative Plan Spinal Precautions Post-Discharge Plan S A I N T LU
Physical and Occupational Therapy after Spine Surgery Preparation for your surgery Agenda Pre-Operative Exercises What to Expect Post-Operative Plan Spinal Precautions Post-Discharge Plan S A I N T LU
KANSAS MEDICAL ASSISTANCE PROGRAM. Fee-for-Service Provider Manual. Rehabilitative Therapy Services
 Fee-for-Service Provider Manual Rehabilitative Therapy Services Updated 12.2015 PART II (PHYSICAL THERAPY, OCCUPATIONAL THERAPY, SPEECH/LANGUAGE PATHOLOGY) Introduction Section BILLING INSTRUCTIONS Page
Fee-for-Service Provider Manual Rehabilitative Therapy Services Updated 12.2015 PART II (PHYSICAL THERAPY, OCCUPATIONAL THERAPY, SPEECH/LANGUAGE PATHOLOGY) Introduction Section BILLING INSTRUCTIONS Page
Home Health Prospective Payment System. Overview
 Overview Version 6117 January 2017 PBL-046 Java is a registered trademark of Oracle and/or its affiliates. Table of Contents Overview of the... 5 Background and versioning... 5 Changes for this version...
Overview Version 6117 January 2017 PBL-046 Java is a registered trademark of Oracle and/or its affiliates. Table of Contents Overview of the... 5 Background and versioning... 5 Changes for this version...
CLINICAL MAPPING TOOL. Therapy Clinical Care Pathway
 CLINICAL MAPPING TOOL Therapy Clinical Care Pathway 2 Table of Contents Clinical Mapping Tool Procedure Safe Transition Planning Tool 4 5 Benchmarking 8 Clinical Outcome Tracking Form 9 Pathways to Success
CLINICAL MAPPING TOOL Therapy Clinical Care Pathway 2 Table of Contents Clinical Mapping Tool Procedure Safe Transition Planning Tool 4 5 Benchmarking 8 Clinical Outcome Tracking Form 9 Pathways to Success
Rehabilitation following your hip fracture
 Page 1 of 8 Rehabilitation following your hip fracture Introduction The information in this leaflet is a general guide to help you to have the best recovery following your hip fracture. If you have any
Page 1 of 8 Rehabilitation following your hip fracture Introduction The information in this leaflet is a general guide to help you to have the best recovery following your hip fracture. If you have any
GETTING READY FOR TOTAL HIP REPLACEMENT
 GETTING READY FOR TOTAL HIP REPLACEMENT Pre-Op Exercises for a Better Recovery Your Recovery Begins Now Even if your hip replacement surgery is weeks or months away, start getting ready now. People who
GETTING READY FOR TOTAL HIP REPLACEMENT Pre-Op Exercises for a Better Recovery Your Recovery Begins Now Even if your hip replacement surgery is weeks or months away, start getting ready now. People who
Rehabilitation and Restorative Care
 170 25 Rehabilitation and Restorative Care 1. Define important words in this chapter 2. Discuss rehabilitation and restorative care 3. Describe the importance of promoting independence 4. Explain the complications
170 25 Rehabilitation and Restorative Care 1. Define important words in this chapter 2. Discuss rehabilitation and restorative care 3. Describe the importance of promoting independence 4. Explain the complications
Kentucky Medically Frail Provider Attestation v5. Part I. Member Information. Page 1
 Page 1 Kentucky Medically Frail Provider Attestation v5 This Attestation is to be completed by an enrolled Medicaid Provider whose scope of expertise qualifies them to assess the Member for medical frailty.
Page 1 Kentucky Medically Frail Provider Attestation v5 This Attestation is to be completed by an enrolled Medicaid Provider whose scope of expertise qualifies them to assess the Member for medical frailty.
Rehabilitation. Walkers, Crutches, Canes
 Walkers, Crutches, Canes These devices provide support through your arms to limit the amount of weight on your operated hip. Initially, after a total hip replacement you will use a walker to get around.
Walkers, Crutches, Canes These devices provide support through your arms to limit the amount of weight on your operated hip. Initially, after a total hip replacement you will use a walker to get around.
General Fall Prevention
 Slide 1 General Fall Prevention Determining Risk, Implementing Interventions and Managing Falls Senior Vice President of Patient Care Services Hello, I am Anne Panik, Senior Vice President of Patient Care
Slide 1 General Fall Prevention Determining Risk, Implementing Interventions and Managing Falls Senior Vice President of Patient Care Services Hello, I am Anne Panik, Senior Vice President of Patient Care
Occupational Therapy: INTERVENTION AND INDEPENDENCE
 Occupational Therapy: INTERVENTION AND INDEPENDENCE What is Occupational Therapy? A therapy to help people find ways to do things that matter to them Dressing, bathing, toileting Housekeeping Leisure Community
Occupational Therapy: INTERVENTION AND INDEPENDENCE What is Occupational Therapy? A therapy to help people find ways to do things that matter to them Dressing, bathing, toileting Housekeeping Leisure Community
The Complex Rehab Technology Company. Focused on Providing Specialized Products and Related Services to People with Disabilities
 The Complex Rehab Technology Company Focused on Providing Specialized Products and Related Services to People with Disabilities The Complex Rehab Technology Company What is Complex Rehab Technology and
The Complex Rehab Technology Company Focused on Providing Specialized Products and Related Services to People with Disabilities The Complex Rehab Technology Company What is Complex Rehab Technology and
PTA 3 FOUNDATIONS OF PHYSICAL THERAPY II SYLLABUS AND COURSE INFORMATION PACKET. Summer 2017
 PTA 3 FOUNDATIONS OF PHYSICAL THERAPY II SYLLABUS AND COURSE INFORMATION PACKET Summer 2017 3 credits 2 hour lecture/ 8 hours lab Prof. Christina McVey Telephone: 368-5727 Office: S129 Email: Christina.mcvey@kbcc.cuny.edu
PTA 3 FOUNDATIONS OF PHYSICAL THERAPY II SYLLABUS AND COURSE INFORMATION PACKET Summer 2017 3 credits 2 hour lecture/ 8 hours lab Prof. Christina McVey Telephone: 368-5727 Office: S129 Email: Christina.mcvey@kbcc.cuny.edu
PTA 235 PTA Clinical Education II Self Performance Evaluation Instrument
 Mercer County Community College Physical Therapist Assistant Program PTA 235 PTA Clinical Education II Self Performance Evaluation Instrument Learner Dates of Clinical Experience Name of Clinical Site:
Mercer County Community College Physical Therapist Assistant Program PTA 235 PTA Clinical Education II Self Performance Evaluation Instrument Learner Dates of Clinical Experience Name of Clinical Site:
A completed application includes the following:! After a successful application review by our staff If you are selected for placement
 Dear Prospective Client, N e w L i f e K 9 s Thank you for your interest in being matched with one of our incredible service dogs This packet includes the Assistance Dog Application, Medical History Form
Dear Prospective Client, N e w L i f e K 9 s Thank you for your interest in being matched with one of our incredible service dogs This packet includes the Assistance Dog Application, Medical History Form
Physical Therapy Plan of Treatment
 Caring for Your Quality of Life Physical Therapy Plan of Treatment SOC Date Clinical Interview Relevant Background Information The Interview was completed With: Patient Spouse Caregiver Other: _ Patient
Caring for Your Quality of Life Physical Therapy Plan of Treatment SOC Date Clinical Interview Relevant Background Information The Interview was completed With: Patient Spouse Caregiver Other: _ Patient
YOUR TOTAL KNEE REPLACEMENT
 YOUR TOTAL KNEE REPLACEMENT General Guide to getting you back to function. Topics to Cover Walking, step climbing, functional mobility and using assistive devices Transfers in and out of chairs, car, bed
YOUR TOTAL KNEE REPLACEMENT General Guide to getting you back to function. Topics to Cover Walking, step climbing, functional mobility and using assistive devices Transfers in and out of chairs, car, bed
Heidi Sanders, OTR/L. Amy Shuckra, MPT
 Adaptive Equipment Heidi Sanders, OTR/L University of New Mexico Health Sciences Center, Los Pasos Program Amy Shuckra, MPT Shriners Hospitals for Children Salt Lake City, Utah What is Adaptive Equipment?
Adaptive Equipment Heidi Sanders, OTR/L University of New Mexico Health Sciences Center, Los Pasos Program Amy Shuckra, MPT Shriners Hospitals for Children Salt Lake City, Utah What is Adaptive Equipment?
NEW YORK STATE MEDICAID PROGRAM REHABILITATION SERVICES POLICY GUIDELINES
 NEW YORK STATE MEDICAID PROGRAM REHABILITATION SERVICES POLICY GUIDELINES Version 2010-1 June 10, 2010 Page 1 of 8 Table of Contents SECTION I REQUIREMENTS FOR PARTICIPATION IN MEDICAID. 3 PROVIDER/QUALIFYING
NEW YORK STATE MEDICAID PROGRAM REHABILITATION SERVICES POLICY GUIDELINES Version 2010-1 June 10, 2010 Page 1 of 8 Table of Contents SECTION I REQUIREMENTS FOR PARTICIPATION IN MEDICAID. 3 PROVIDER/QUALIFYING
We Have a Great Story to Tell
 We Have a Great Story to Tell Inpatient Outpatient Day Neuro Baylor Scott & White Institute for Rehabilitation Frisco is dedicated to helping patients find their way back from all types of injuries, illnesses,
We Have a Great Story to Tell Inpatient Outpatient Day Neuro Baylor Scott & White Institute for Rehabilitation Frisco is dedicated to helping patients find their way back from all types of injuries, illnesses,
The Inception of the Outlier Provision REISINGER,(JOHN((1(
 1 Following is an Outline of what we will be covering: The Inception of this Provision The Premise behind the Outlier Provision The Unique Terminology of this Provision The Common Perception/Opinion Throughout
1 Following is an Outline of what we will be covering: The Inception of this Provision The Premise behind the Outlier Provision The Unique Terminology of this Provision The Common Perception/Opinion Throughout
Professional Development Workshops
 Training Professional Development Workshops Pressure Injury Prevention & Management Breakfast in Bed Are You Sitting Comfortably Move It, Move It! Meet your presenter... Julia Salmon is a highly experienced
Training Professional Development Workshops Pressure Injury Prevention & Management Breakfast in Bed Are You Sitting Comfortably Move It, Move It! Meet your presenter... Julia Salmon is a highly experienced
SAULT COLLEGE OF APPLIED ARTS AND TECHNOLOGY SAULT STE. MARIE, ONTARIO COURSE OUTLINE
 SAULT COLLEGE OF APPLIED ARTS AND TECHNOLOGY SAULT STE. MARIE, ONTARIO COURSE OUTLINE COURSE TITLE: Occupational Therapy Principles & Clinical Skills I CODE NO. : OPA 115 SEMESTER: 2 PROGRAM: AUTHOR: Occupational
SAULT COLLEGE OF APPLIED ARTS AND TECHNOLOGY SAULT STE. MARIE, ONTARIO COURSE OUTLINE COURSE TITLE: Occupational Therapy Principles & Clinical Skills I CODE NO. : OPA 115 SEMESTER: 2 PROGRAM: AUTHOR: Occupational
AFTER TOTAL HIP REPLACEMENT
 AFTER TOTAL HIP REPLACEMENT Living in Comfort with Your New Hip Getting Back in Step By having a total hip replacement, you re taking the first step toward returning to an active lifestyle. The next step
AFTER TOTAL HIP REPLACEMENT Living in Comfort with Your New Hip Getting Back in Step By having a total hip replacement, you re taking the first step toward returning to an active lifestyle. The next step
NCHA Financial Feature
 NCHA Financial Feature November 2, 2018 CMS Finalizes Calendar Year 2019 Payments and 2020 Policy Changes for Home Health Agencies and Home Infusion Therapy Suppliers The Centers for Medicare and Medicaid
NCHA Financial Feature November 2, 2018 CMS Finalizes Calendar Year 2019 Payments and 2020 Policy Changes for Home Health Agencies and Home Infusion Therapy Suppliers The Centers for Medicare and Medicaid
Medical Necessity Guidelines: Applied Behavioral Analysis (ABA) including Early Intervention for RITogether
 including Early Intervention for RITogether") Medical Necessity Guidelines: Applied Behavioral Analysis (ABA) including Effective: August 1, 2017 Clinical Documentation and Prior Authorization Required Applies to: Coverage Guideline, No prior Authorization
Medical Necessity Guidelines: Applied Behavioral Analysis (ABA) including Effective: August 1, 2017 Clinical Documentation and Prior Authorization Required Applies to: Coverage Guideline, No prior Authorization
CPT Coding Peoplefirst. Rehabilitation Clinical Services Team. Current Procedural Terminology. Making Sense of Coding
 CPT Coding 2009 Current Procedural Terminology Making Sense of Coding Peoplefirst Rehabilitation Clinical Services Medicare A versus Medicare B Billing Medicare A PPS - Prospective Payment System Reimbursement
CPT Coding 2009 Current Procedural Terminology Making Sense of Coding Peoplefirst Rehabilitation Clinical Services Medicare A versus Medicare B Billing Medicare A PPS - Prospective Payment System Reimbursement
Table of Contents Treatment Guides Basic Activities of Daily Living Basic and Instrumental Activities of Daily Living 11 Bathing and Showering 13 Dres
 Treatment Guides Basic Activities of Daily Living Basic and Instrumental Activities of Daily Living 11 Bathing and Showering 13 Dressing 15 Feeding 18 Functional Communication 20 Functional Mobility 22
Treatment Guides Basic Activities of Daily Living Basic and Instrumental Activities of Daily Living 11 Bathing and Showering 13 Dressing 15 Feeding 18 Functional Communication 20 Functional Mobility 22
PTA 240 PTA Clinical Education III Student Self Performance Evaluation Instrument
 Mercer County Community College Physical Therapist Assistant Program PTA 240 PTA Clinical Education III Student Self Performance Evaluation Instrument Student/learner Dates of Clinical Experience Name
Mercer County Community College Physical Therapist Assistant Program PTA 240 PTA Clinical Education III Student Self Performance Evaluation Instrument Student/learner Dates of Clinical Experience Name
Moving The Patient. From Our Perspective. From the Patient s Perspective. Techniques, Tips, and Tools
 Moving The Patient From Our Perspective From the Patient s Perspective Techniques, Tips, and Tools From The Perspective of the Health Care Provider Does our training, clinical experience, and knowledge
Moving The Patient From Our Perspective From the Patient s Perspective Techniques, Tips, and Tools From The Perspective of the Health Care Provider Does our training, clinical experience, and knowledge
Cervical Surgeries. DO NOT twist or bend your neck, or lift with your arms, without getting clearance from your doctor.
 Precautions: Cervical Surgeries DO NOT twist or bend your neck, or lift with your arms, without getting clearance from your doctor. If you must bend down to pick up an object, use a grabber instead. Tighten
Precautions: Cervical Surgeries DO NOT twist or bend your neck, or lift with your arms, without getting clearance from your doctor. If you must bend down to pick up an object, use a grabber instead. Tighten
June 21, Harry Feliciano, MD, MPH Senior Medical Director Part A Policy Palmetto GBA PO Box (JM) AG-275 Columbia, SC 29202
 AG-275 Columbia, SC 29202") June 21, 2018 Harry Feliciano, MD, MPH Senior Medical Director Part A Policy Palmetto GBA PO Box 100238 (JM) AG-275 Columbia, SC 29202 Submitted electronically: A.Policy@PalmettoGBA.com RE: Proposed LCD
June 21, 2018 Harry Feliciano, MD, MPH Senior Medical Director Part A Policy Palmetto GBA PO Box 100238 (JM) AG-275 Columbia, SC 29202 Submitted electronically: A.Policy@PalmettoGBA.com RE: Proposed LCD
Medicare Myths-Busters: Dispelling Common Compliance Misconceptions. Learner Objectives. Learner Objectives
 Medicare Myths-Busters: Dispelling Common Compliance Misconceptions Rick Gawenda, PT President Gawenda Seminars & Consulting, Inc. September 30, 2017 Learner Objectives Identify the supervision requirements
Medicare Myths-Busters: Dispelling Common Compliance Misconceptions Rick Gawenda, PT President Gawenda Seminars & Consulting, Inc. September 30, 2017 Learner Objectives Identify the supervision requirements
Assessing Muscle Function and Balance Problems at Home, in the Clinic, and in Research 25 th IOA Colloquium on Aging September 17, 2013
 Assessing Muscle Function and Balance Problems at Home, in the Clinic, and in Research 25 th IOA Colloquium on Aging September 17, 2013 Bjoern Buehring, M.D. University of Wisconsin School of Medicine
Assessing Muscle Function and Balance Problems at Home, in the Clinic, and in Research 25 th IOA Colloquium on Aging September 17, 2013 Bjoern Buehring, M.D. University of Wisconsin School of Medicine
Service Provider Department Phone Number
 Service Provider Department Phone Number A Activities of Daily Living Occupational Therapy Rehabilitation Services 734-593-5620 Adaptive Equipment - home Occupational Therapy Rehabilitation Services 734-593-5620
Service Provider Department Phone Number A Activities of Daily Living Occupational Therapy Rehabilitation Services 734-593-5620 Adaptive Equipment - home Occupational Therapy Rehabilitation Services 734-593-5620
Hip Surgery and Mobility
 Orthopedic Nursing, Part 1 Hip Surgery and Mobility Nursing Best Practice Guidelines Clinical Indications for Hip Surgery Selected fractures of the hip Unremitting pain and irreversible damaged joint from
Orthopedic Nursing, Part 1 Hip Surgery and Mobility Nursing Best Practice Guidelines Clinical Indications for Hip Surgery Selected fractures of the hip Unremitting pain and irreversible damaged joint from
Active Living with Arthritis Podcast #9 Being a Caregiver: Caring for Someone and Managing Your Arthritis
 Active Living with Arthritis Podcast #9 Being a Caregiver: Caring for Someone and Managing Your Arthritis Karen: Welcome to another Active Living with Arthritis podcast, presented by ENACT center at Boston
Active Living with Arthritis Podcast #9 Being a Caregiver: Caring for Someone and Managing Your Arthritis Karen: Welcome to another Active Living with Arthritis podcast, presented by ENACT center at Boston
ICD 10 CM Coding and Documentation
 ICD 10 CM Coding and Documentation Adult Day Health Care Council Karen L. Fabrizio, RHIA, CHTS CP, CPRA April 10, 2014 Presented by: Karen Fabrizio, RHIA CHTS CP CPRA is an AHIMA Approved ICD 10 CM/PCS
ICD 10 CM Coding and Documentation Adult Day Health Care Council Karen L. Fabrizio, RHIA, CHTS CP, CPRA April 10, 2014 Presented by: Karen Fabrizio, RHIA CHTS CP CPRA is an AHIMA Approved ICD 10 CM/PCS
Health and Safety Risk Assessment Guidance
 Ref:CF:026:00 Health and Safety Risk Assessment Guidance Re: Sample People Handling Risk Assessment and Guidance Issue date: June 2018 Review date: June 2021 Author(s) Legislation: Note: National Health
Ref:CF:026:00 Health and Safety Risk Assessment Guidance Re: Sample People Handling Risk Assessment and Guidance Issue date: June 2018 Review date: June 2021 Author(s) Legislation: Note: National Health
National Stroke Association s Guide to Choosing Stroke. Rehabilitation Services
 National Stroke Association s Guide to Choosing Stroke Rehabilitation Services Rehabilitation, often referred to as rehab, is an important part of stroke recovery. Through rehab, you: Re-learn basic skills
National Stroke Association s Guide to Choosing Stroke Rehabilitation Services Rehabilitation, often referred to as rehab, is an important part of stroke recovery. Through rehab, you: Re-learn basic skills
Local Coverage Determination for Hospice Alzheimer's Disease &Related Disorders (L31539)
") Page 1 of 6 Centers for Medicare & Medicaid Services Print Message: If you are experiencing issues printing this page, then please click Return to Previous Page and select the 'Need a PDF?' button. You
Page 1 of 6 Centers for Medicare & Medicaid Services Print Message: If you are experiencing issues printing this page, then please click Return to Previous Page and select the 'Need a PDF?' button. You
Intramedullary Nailing for Femur Fracture Management
 514-412-4400, ext. 23310 thechildren.com/trauma Intramedullary Nailing for Femur Fracture Management A Guide for Parents The femur is the longest bone in the body. It begins at the hip joint and ends at
514-412-4400, ext. 23310 thechildren.com/trauma Intramedullary Nailing for Femur Fracture Management A Guide for Parents The femur is the longest bone in the body. It begins at the hip joint and ends at