Northwest Community EMS System - Continuing Education March 2015 Trauma QI Case Reviews - CE Credit Questions
|
|
|
- Eleanore Robbins
- 6 years ago
- Views:
Transcription
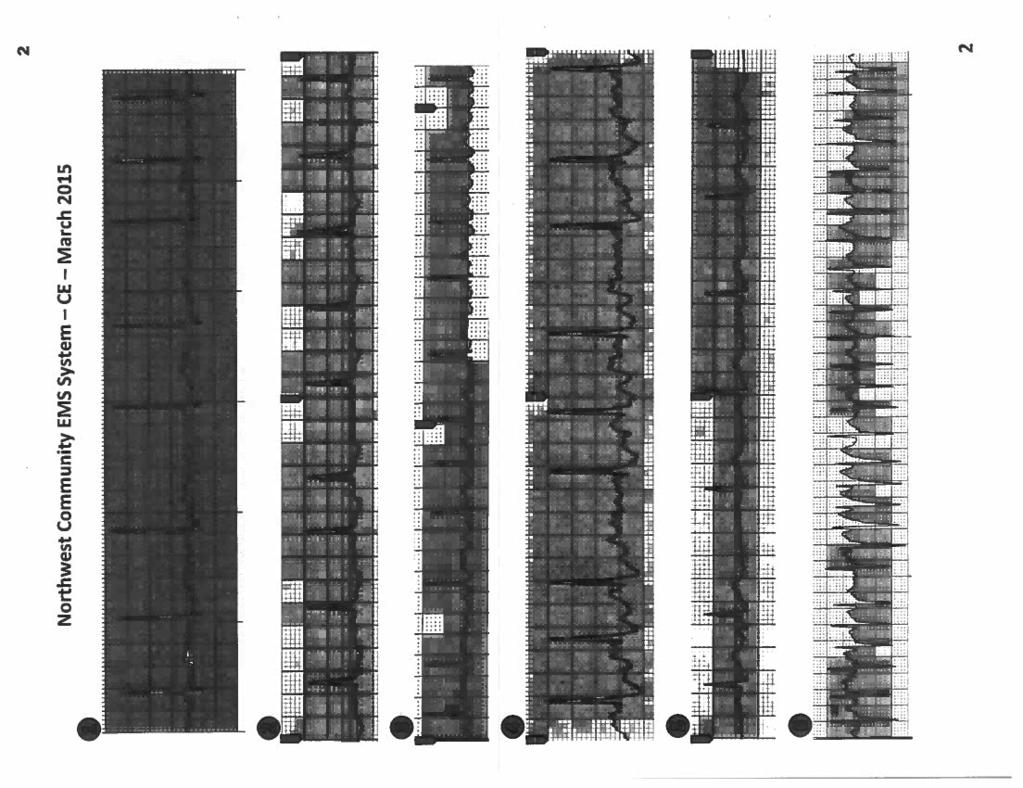
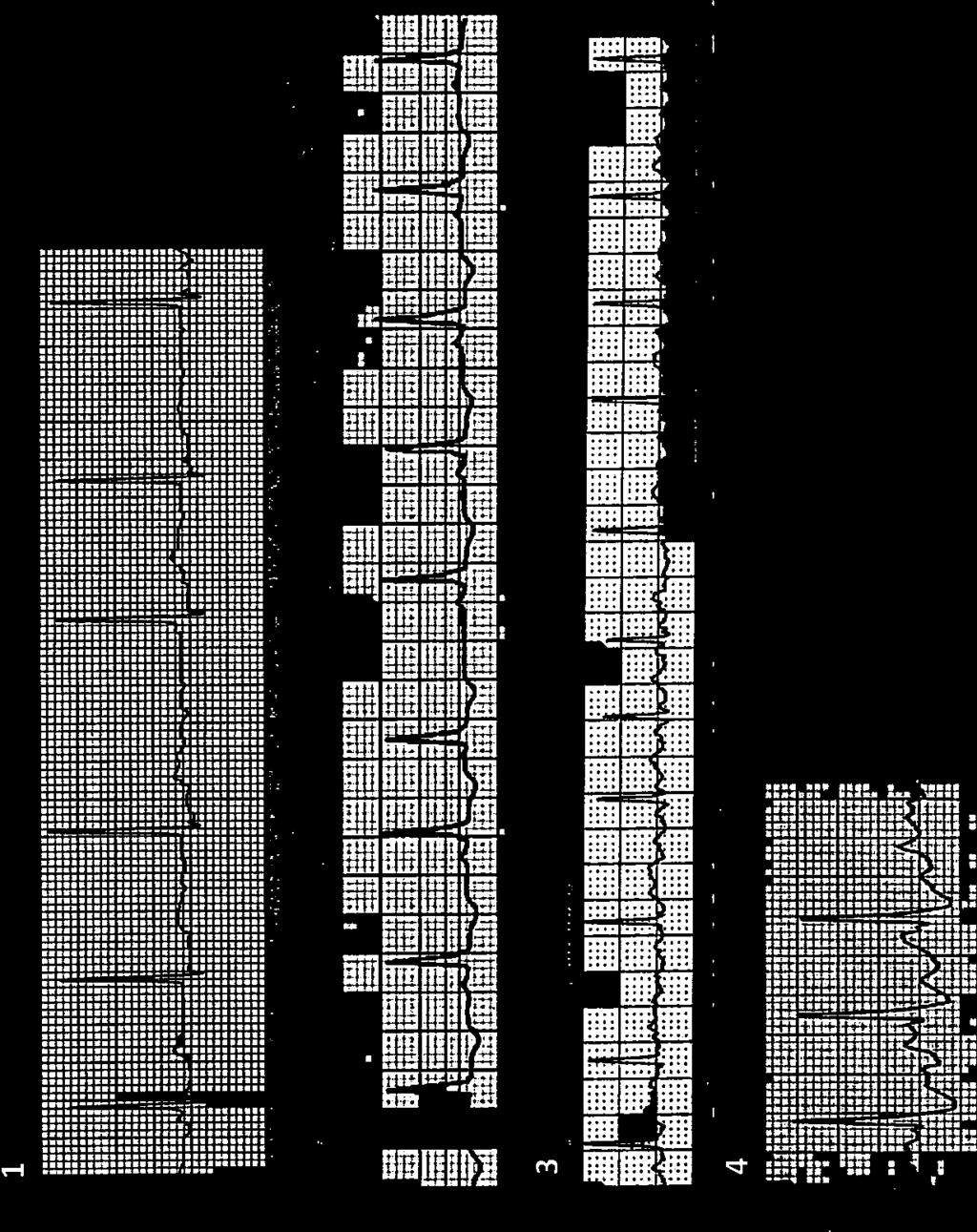
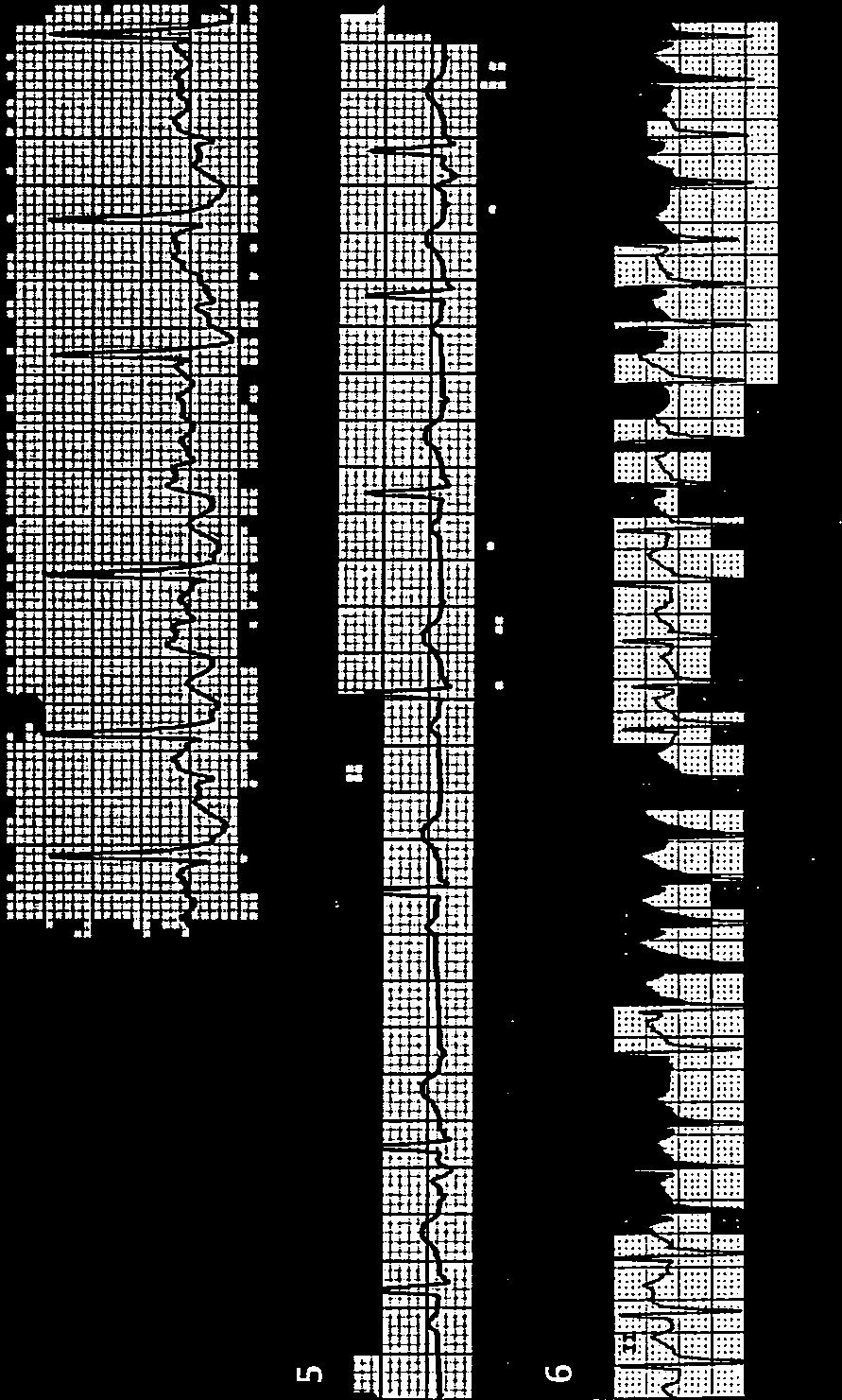
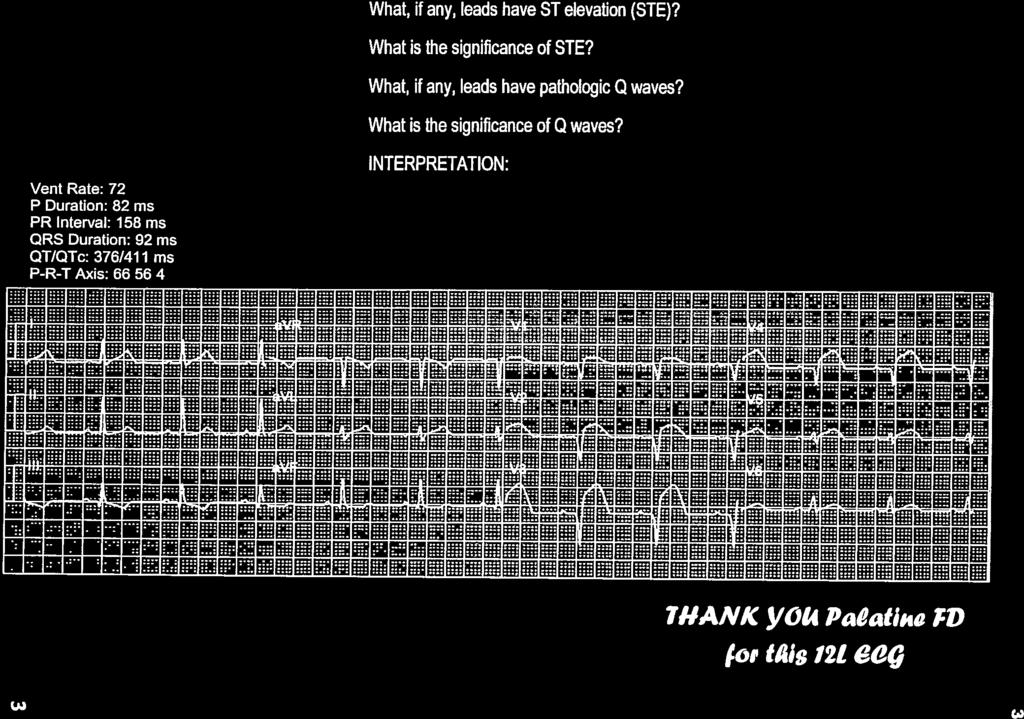
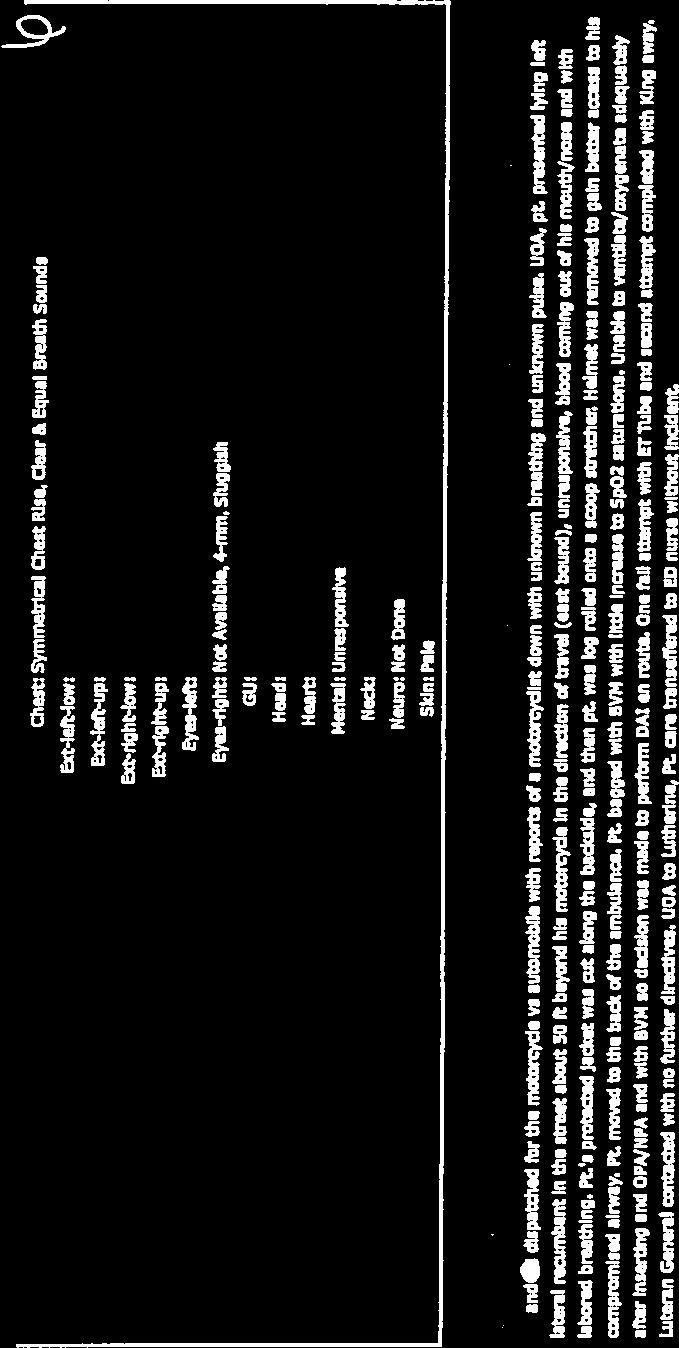
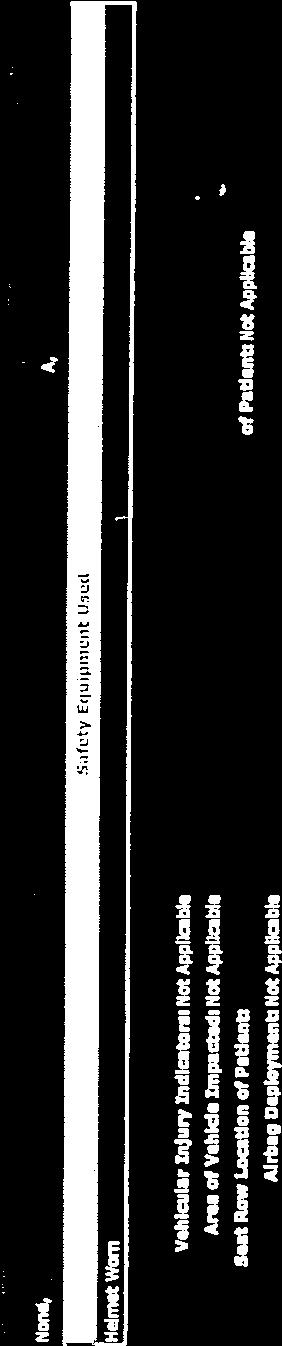
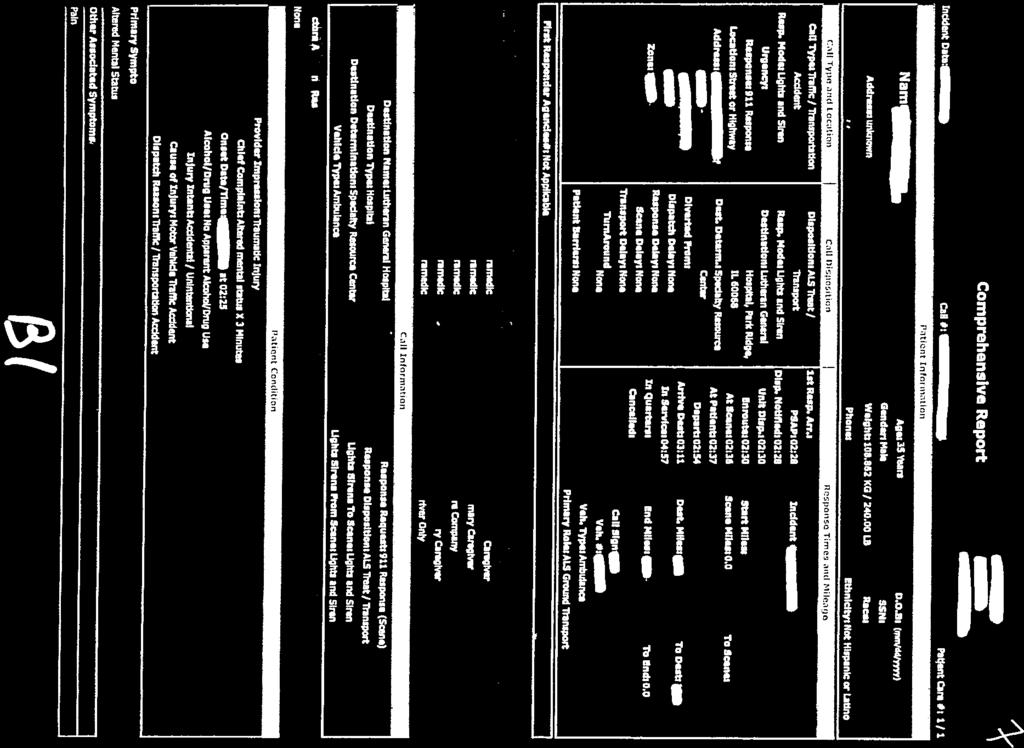
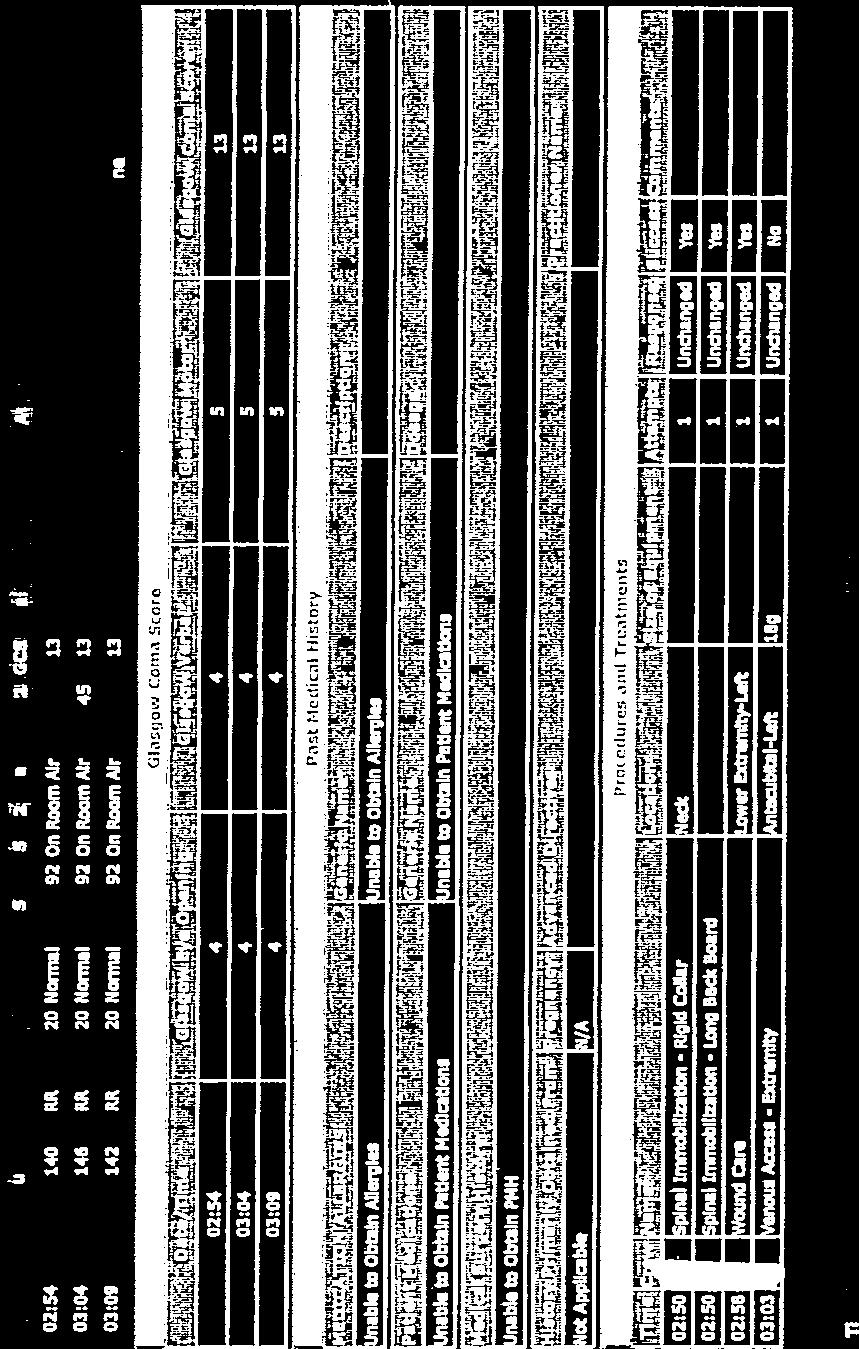
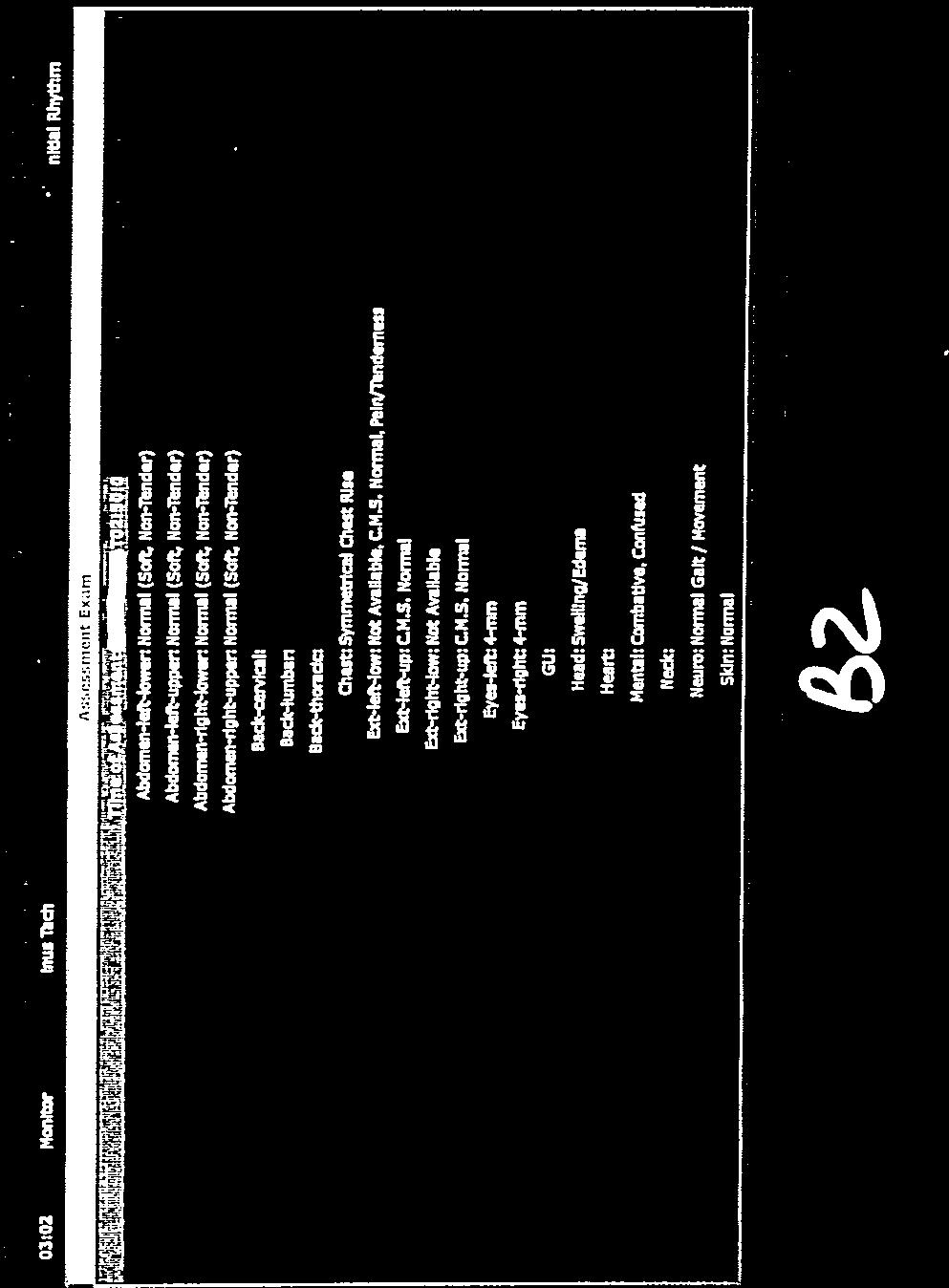
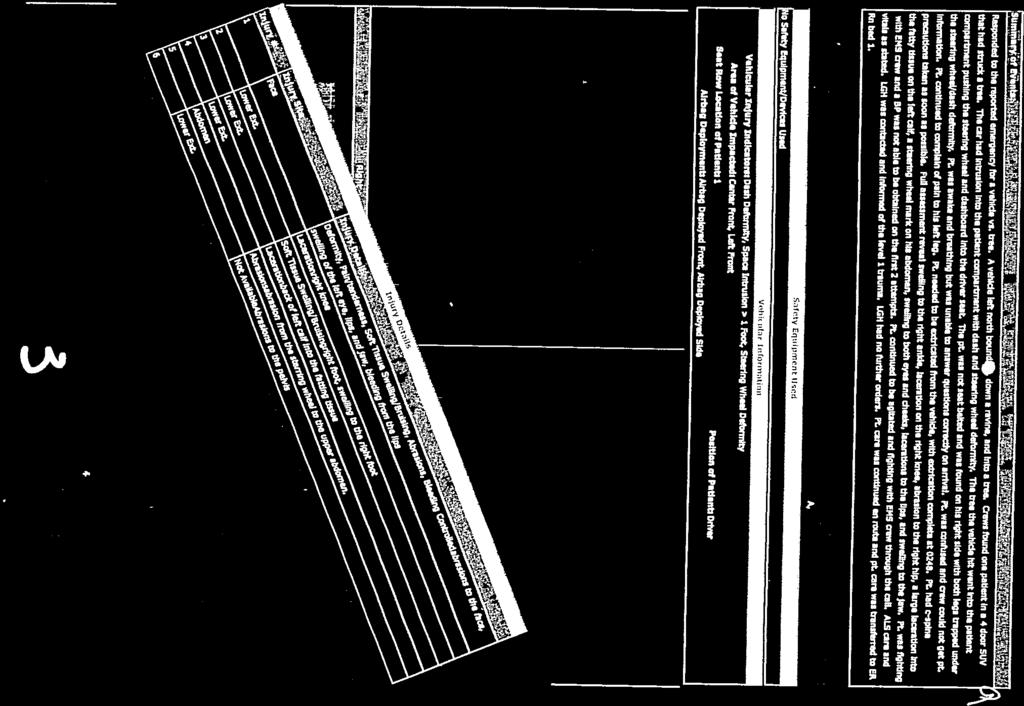
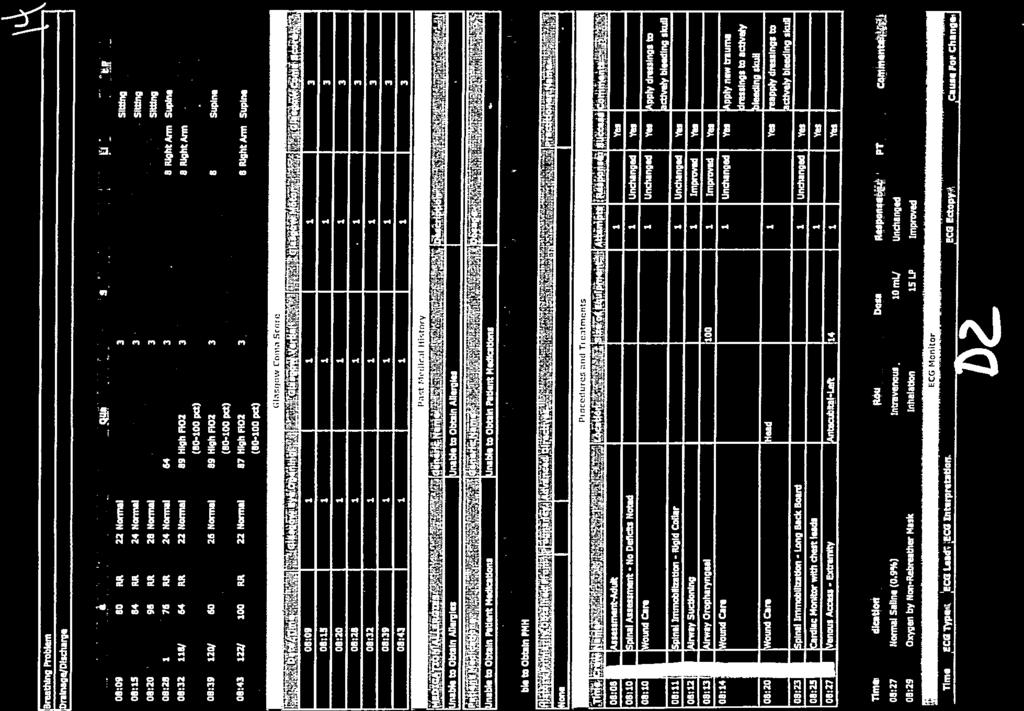
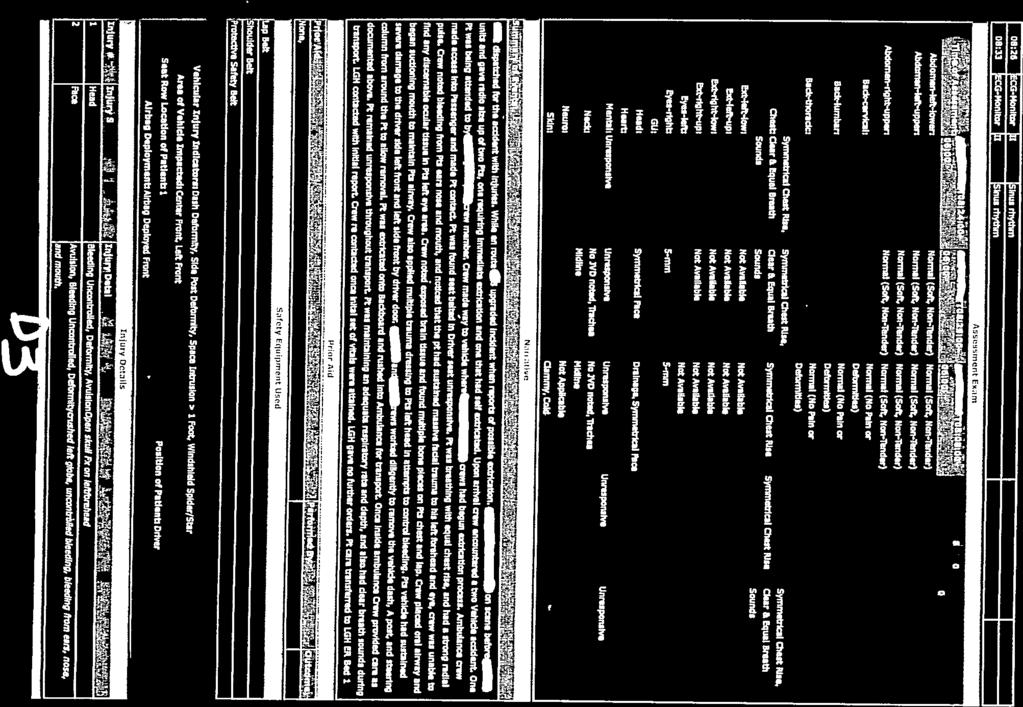
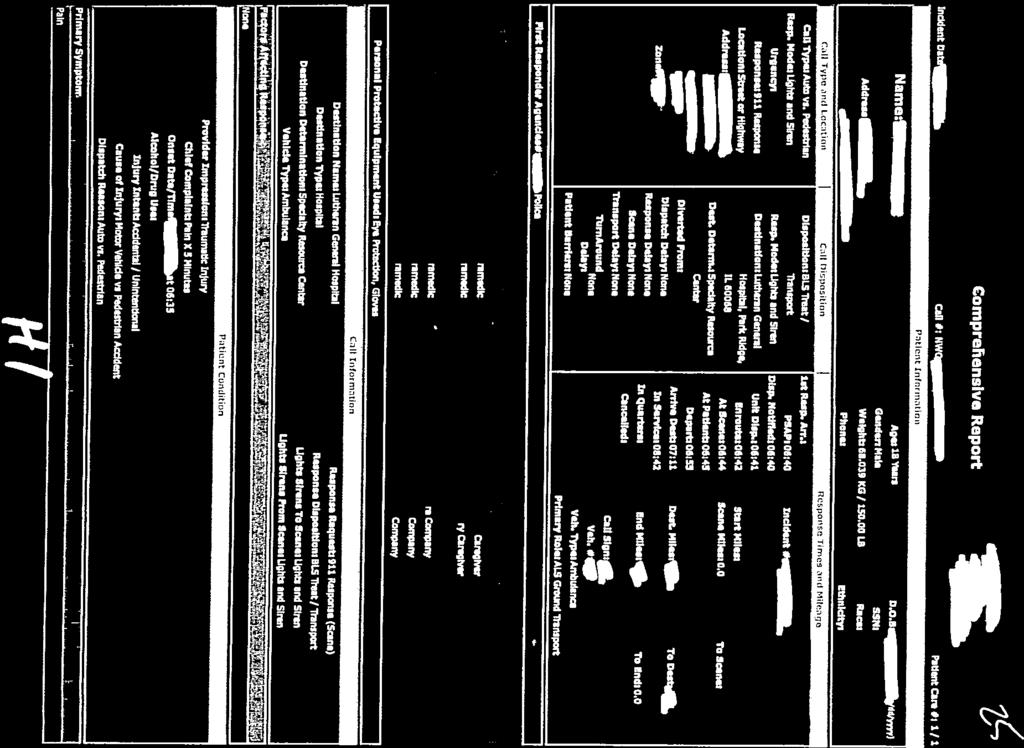
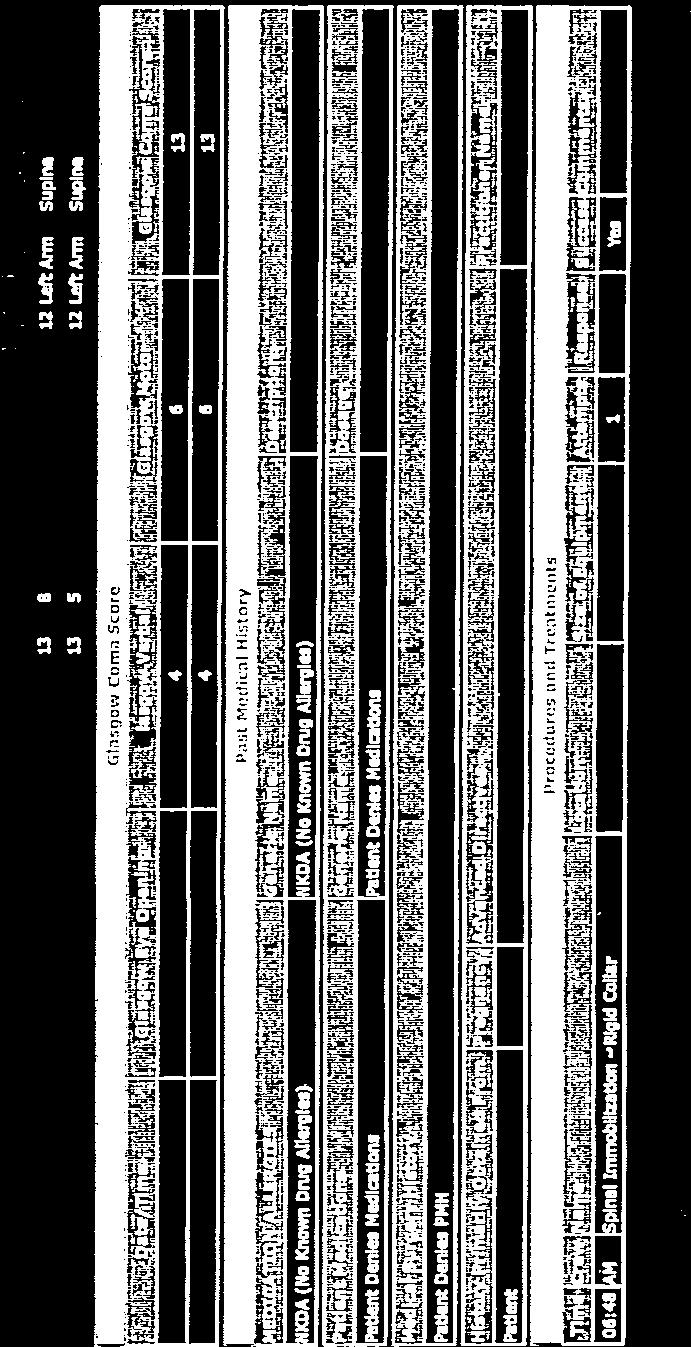
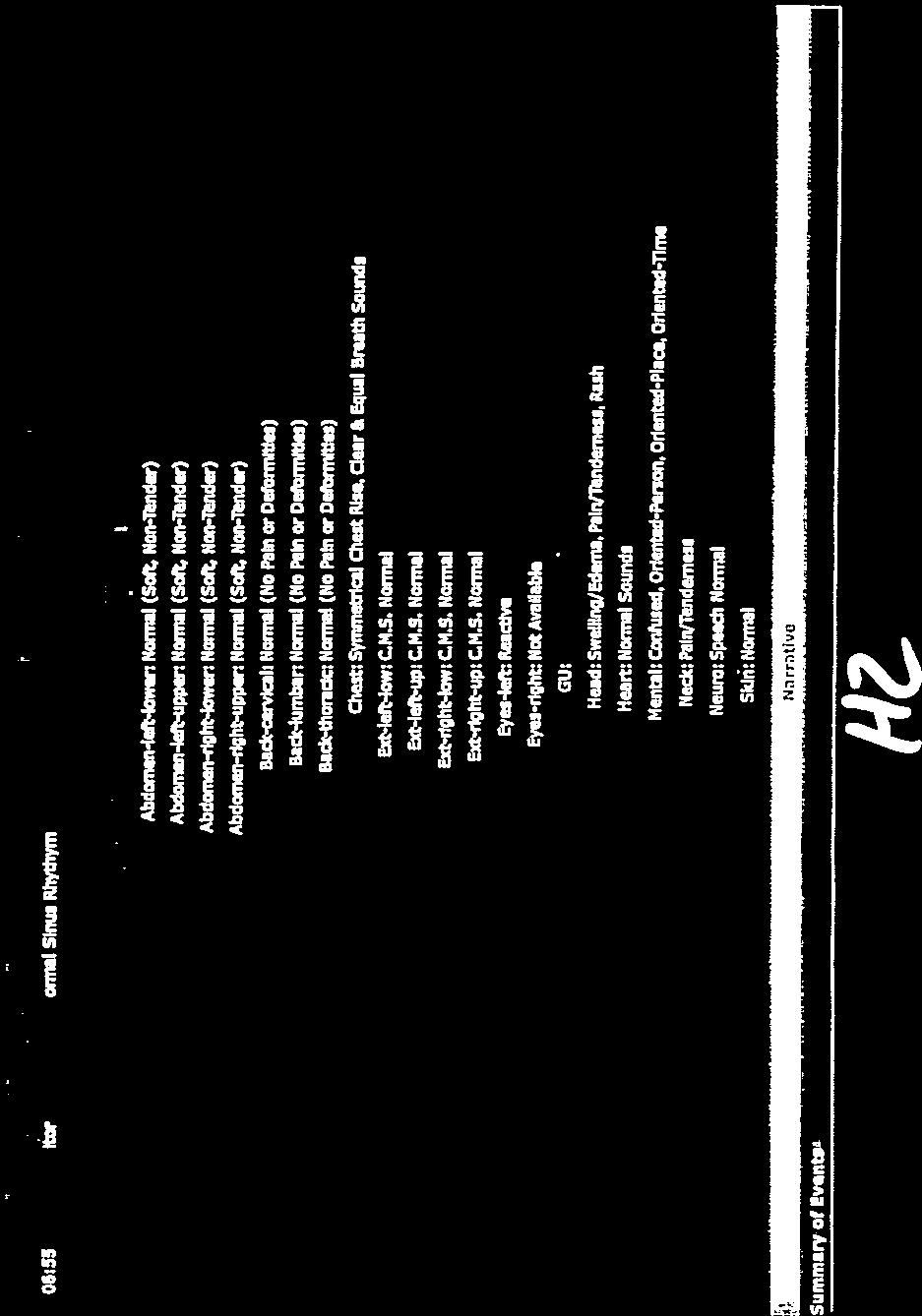
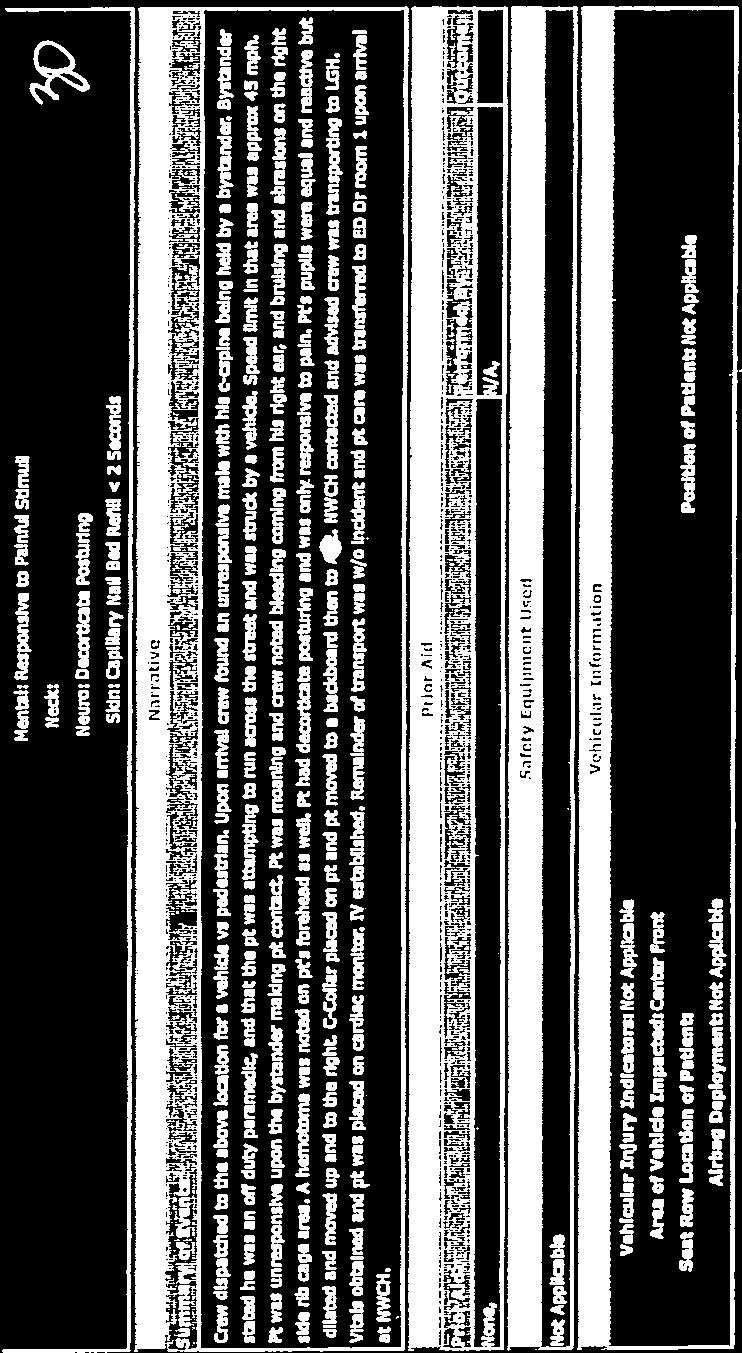
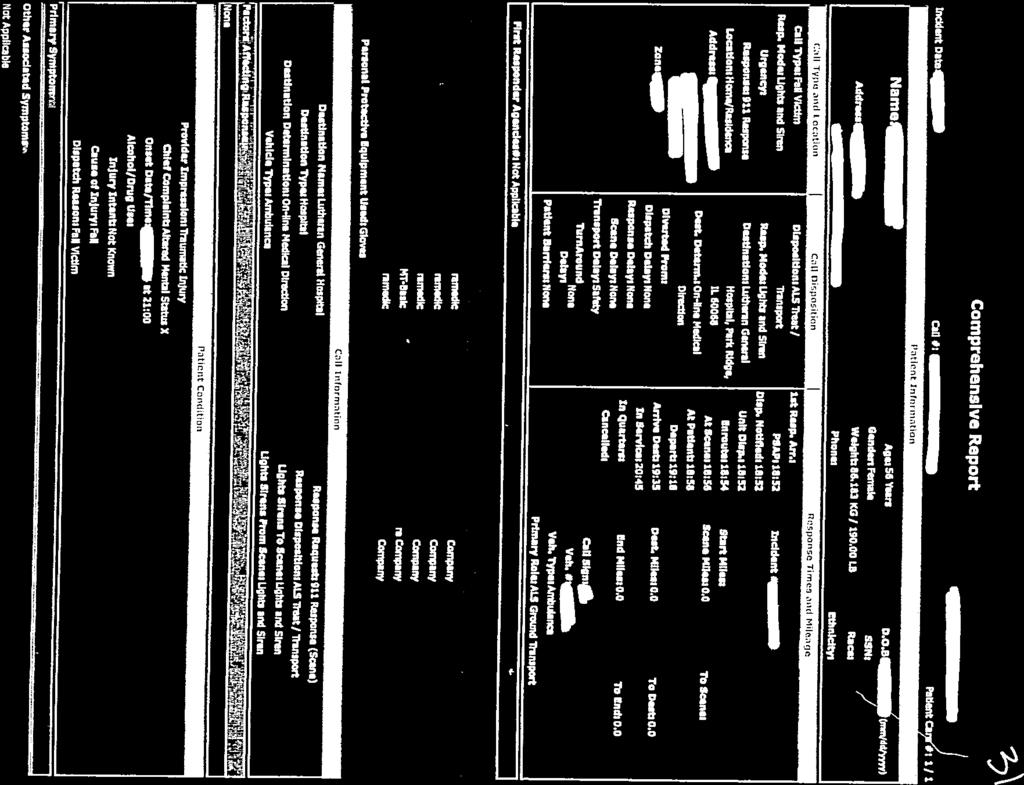
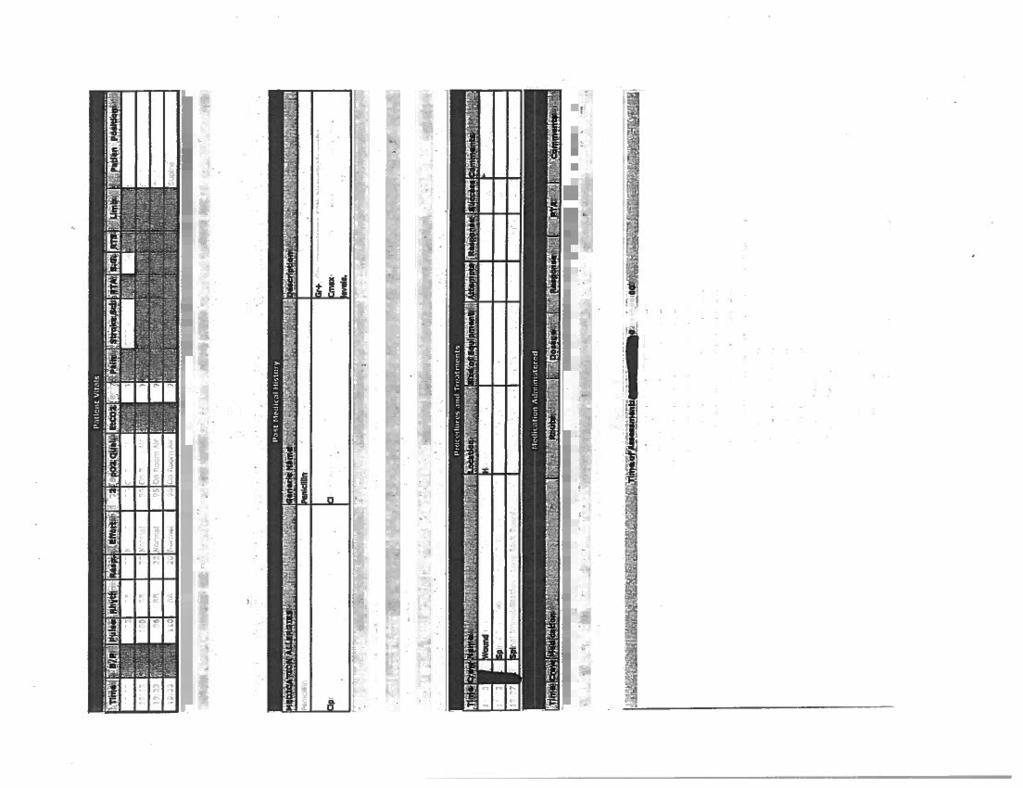
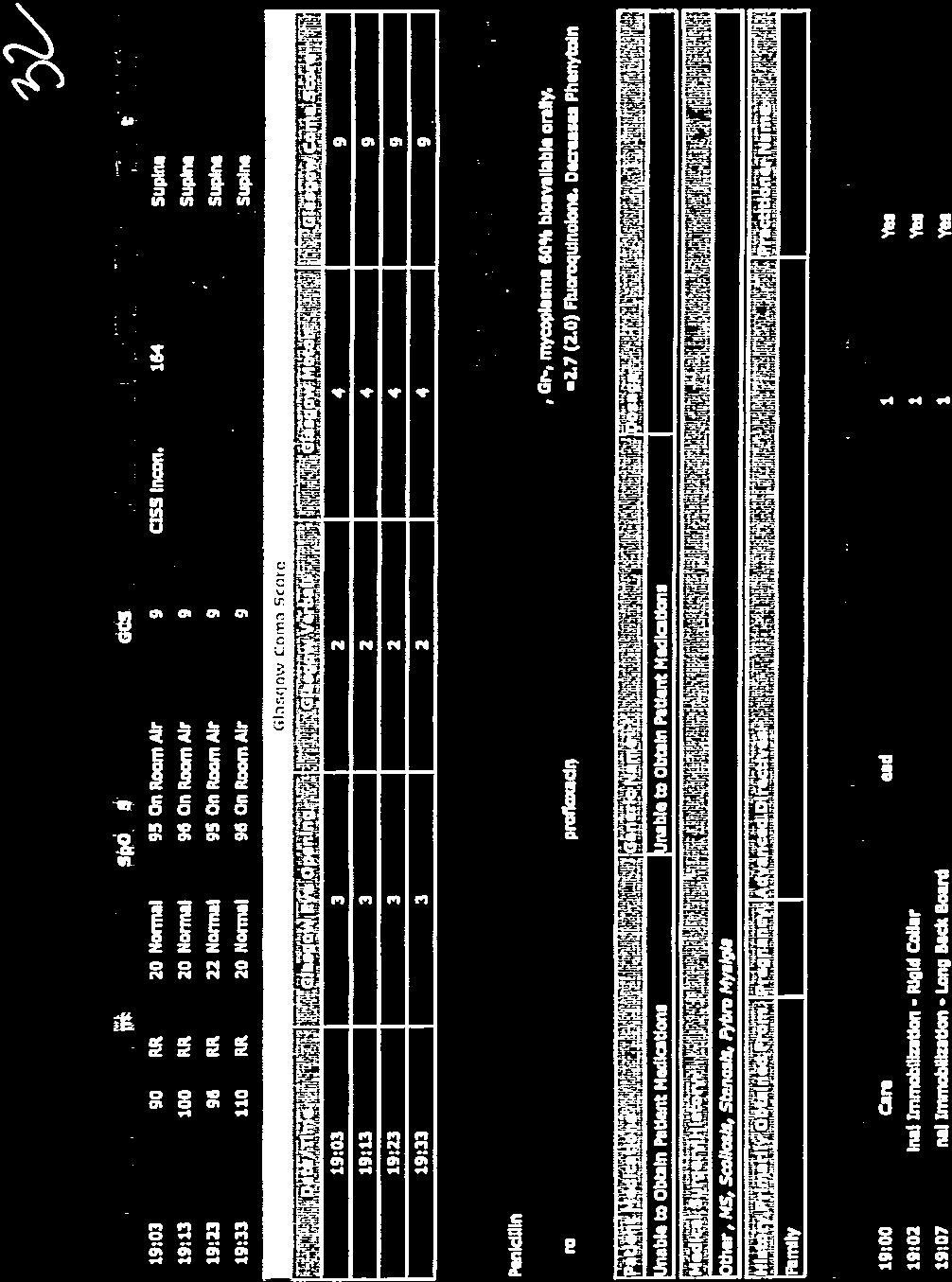
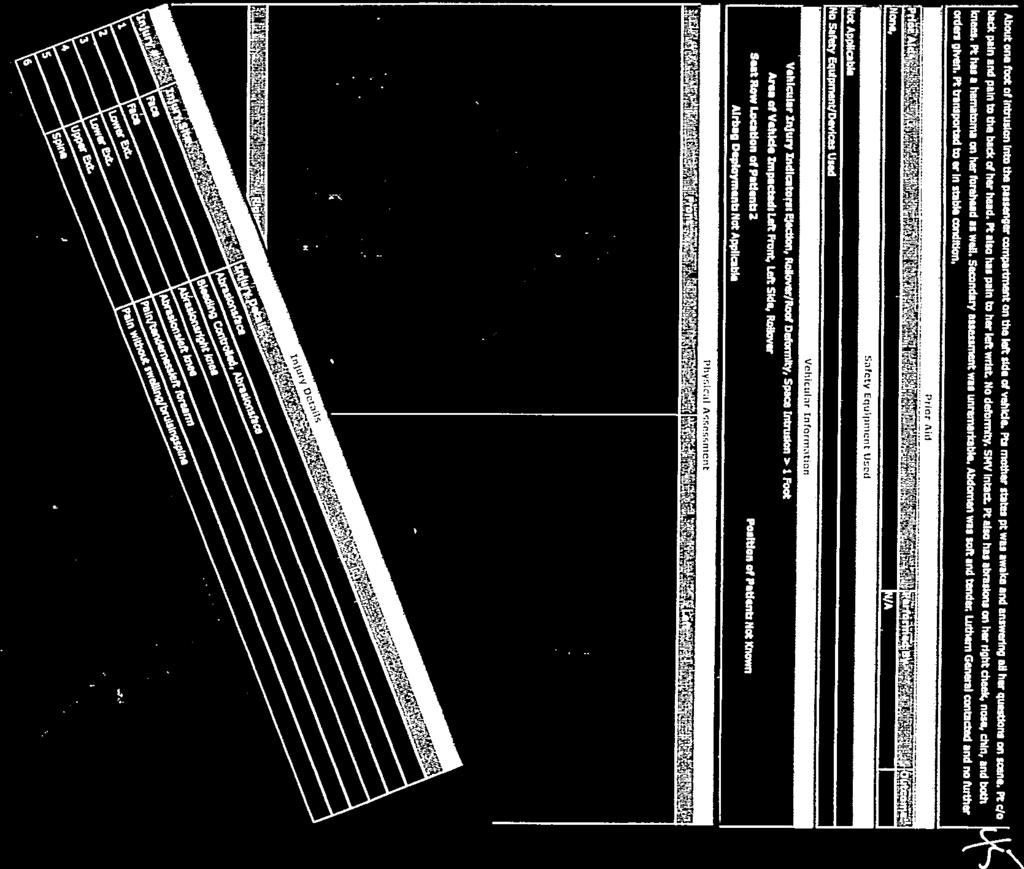
1 Name Employer Date Submitted Northwest Community EMS System - Continuing Education March 2015 Trauma QI Case Reviews - CE Credit Questions To receive credit for this CE module (Materials needed CE handout, SOP s): 1) Interpret the ECG strips on handout page 2 ECG Interpretation ) Interpret the 12L ECG on handout page 3 What, if any, leads have ST elevation (STE)? What is the significance of STE? What, if any, leads have pathological Q waves? What is the significance of Q waves? Interpretation 3) Review PPT slides (avail on NWCEMSS website) and answer the following questions. a. How can EtCO2 be useful when assessing & treating trauma pts? b. Should trauma pts be kept warm or cool? i. Why? ii. List 3 ways to accomplish the above temperature control. c. How does hypoxia impact pts with TBI (traumatic brain injury)? d. How does hypotension impact pts with TBI? e. How does combined hypoxia & hypotension affect TBI pts?
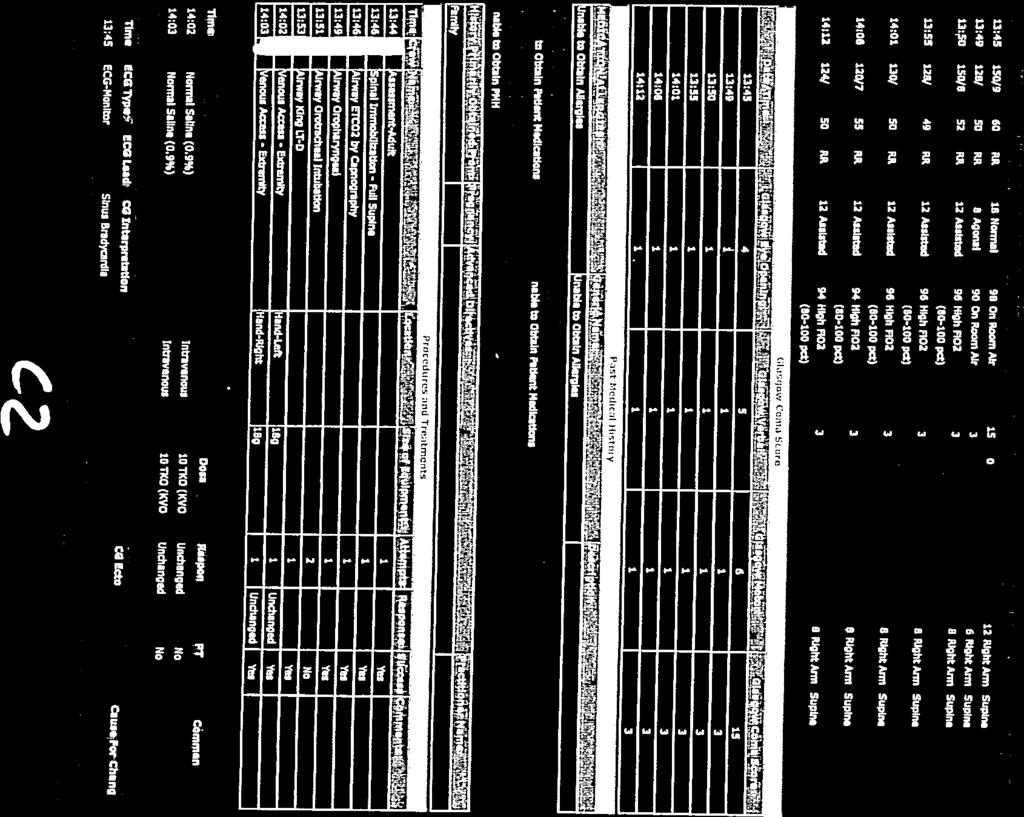
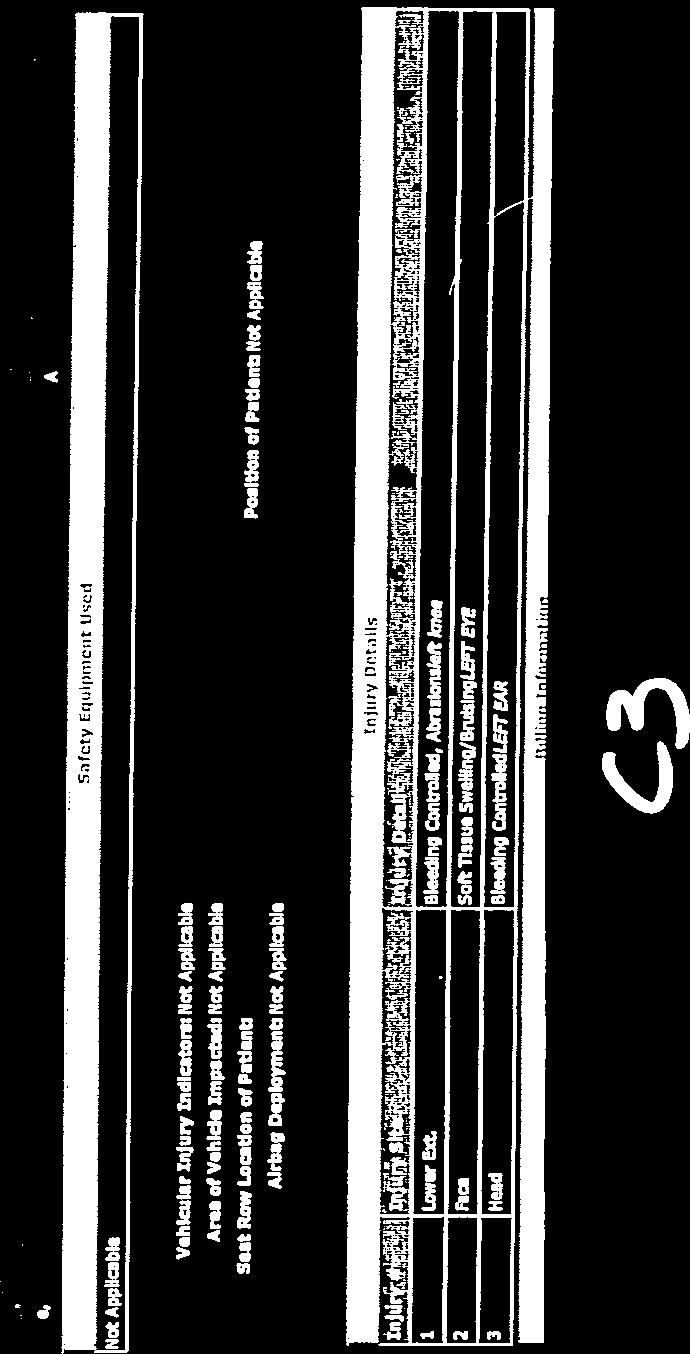
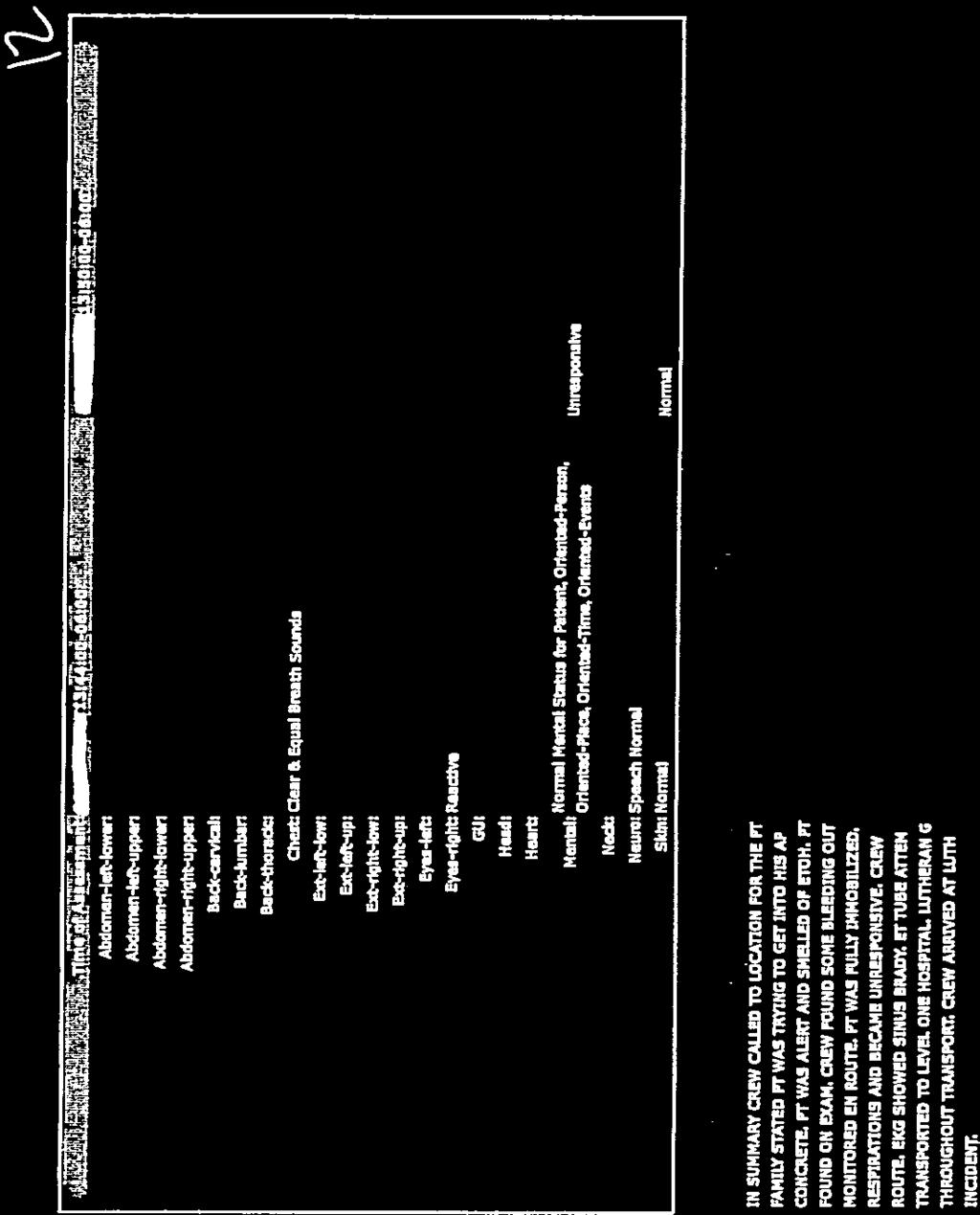
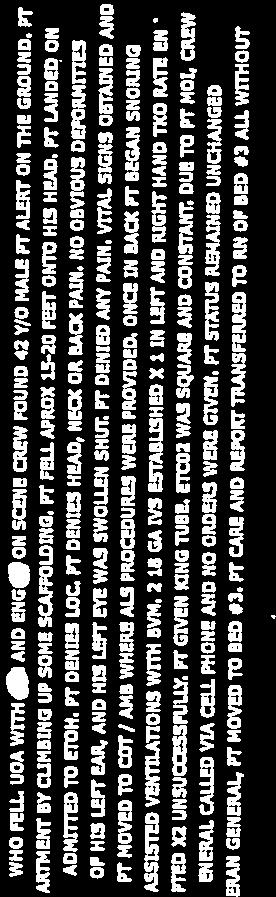
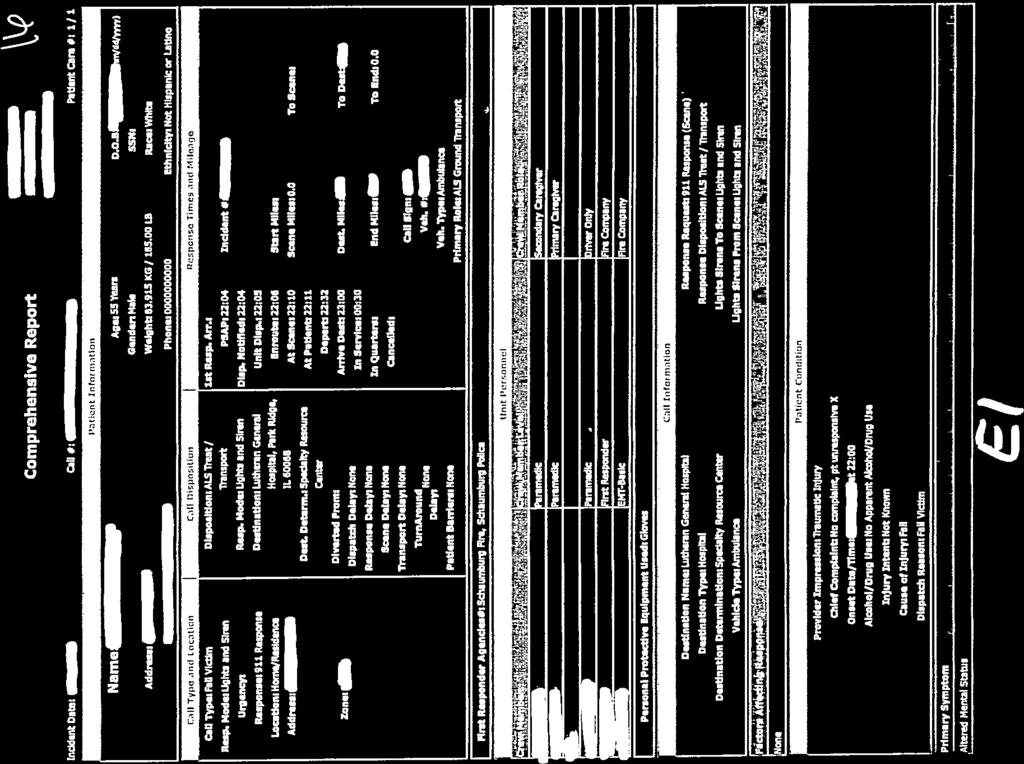
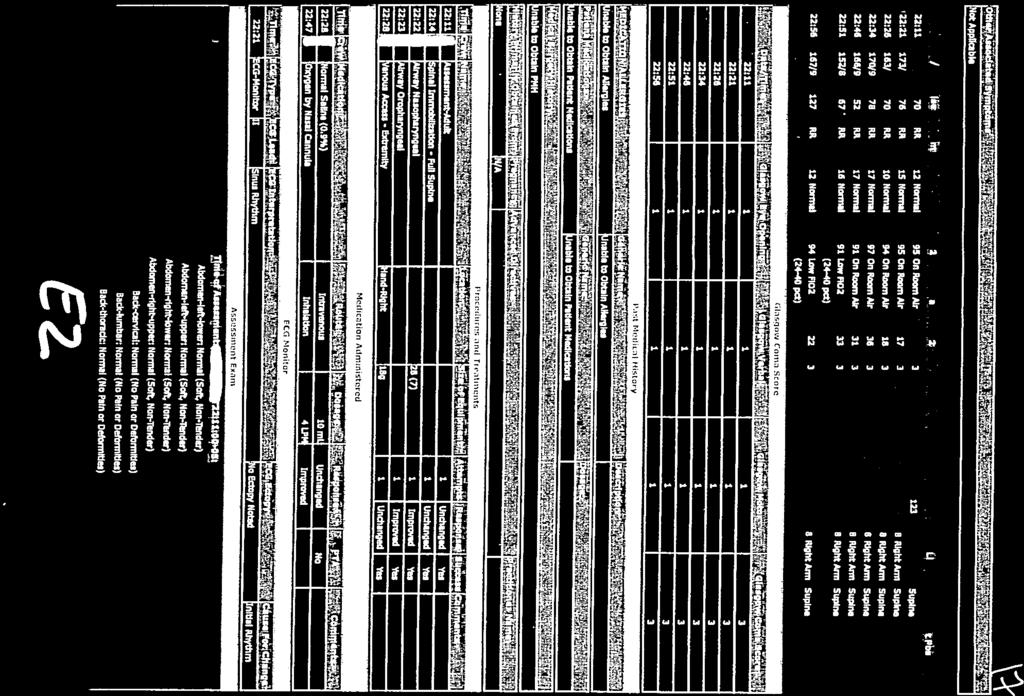
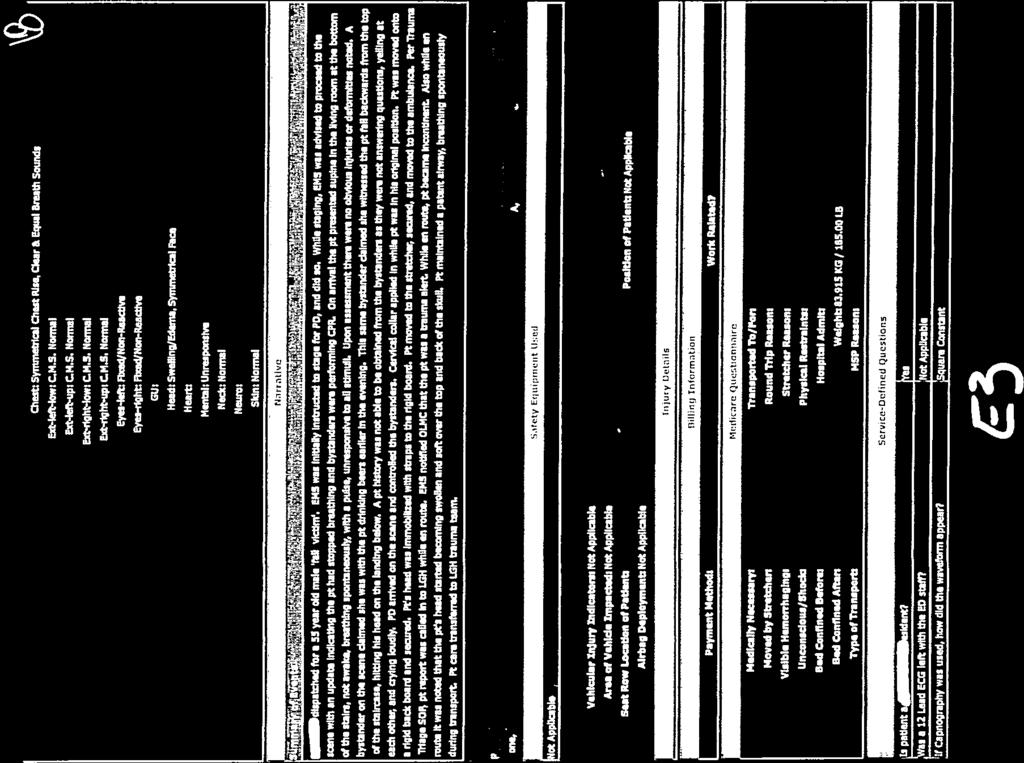
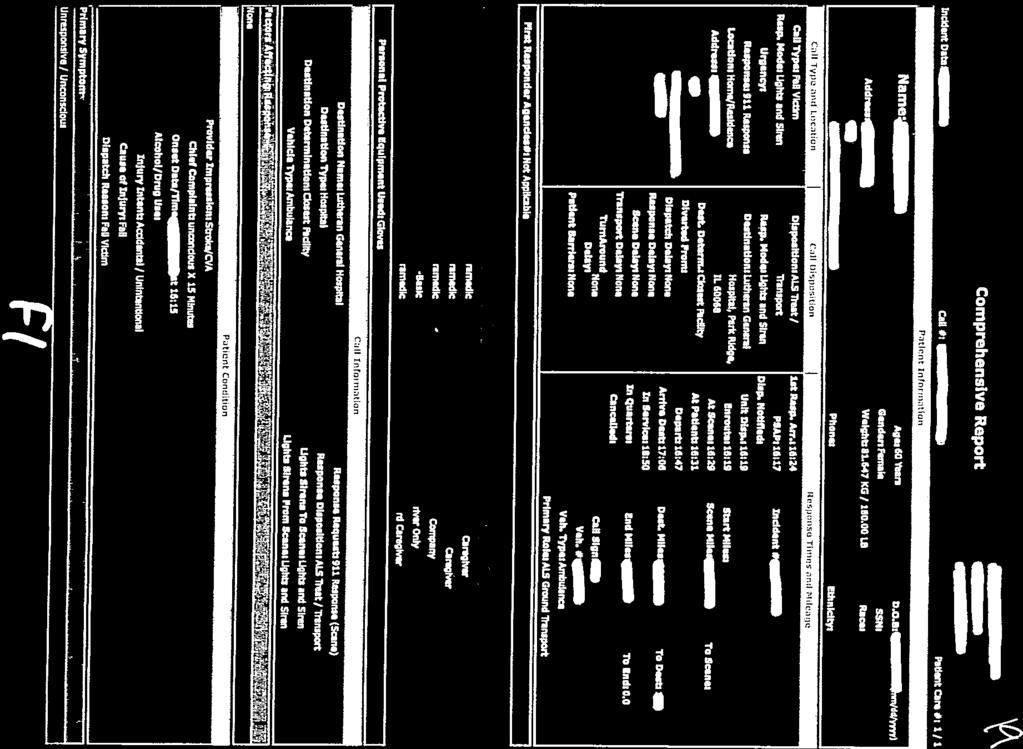
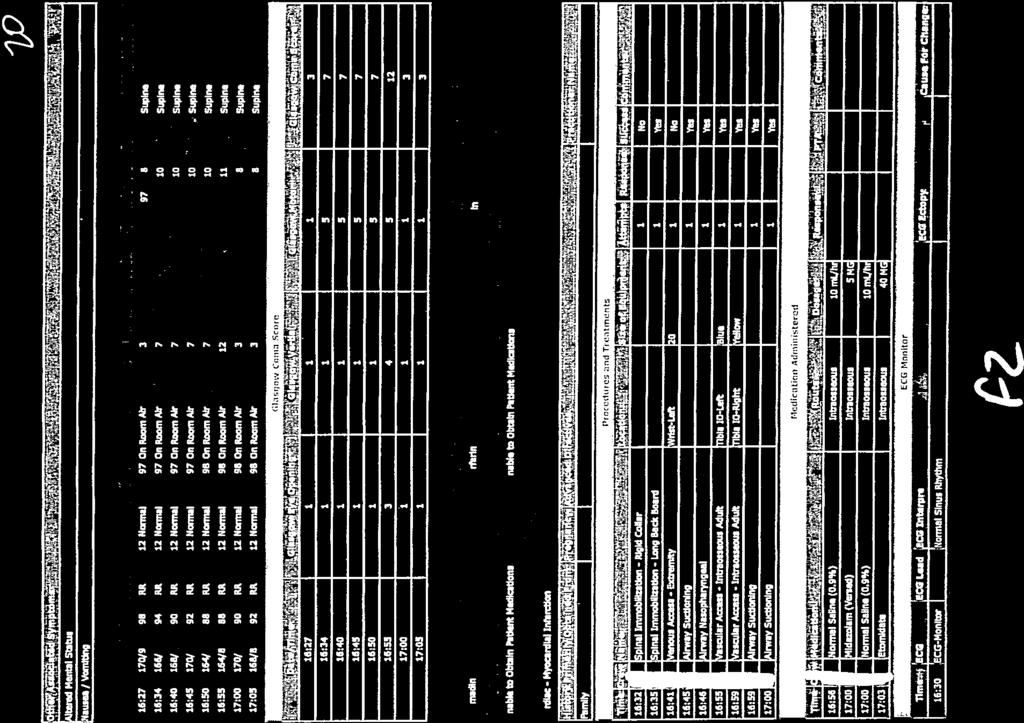
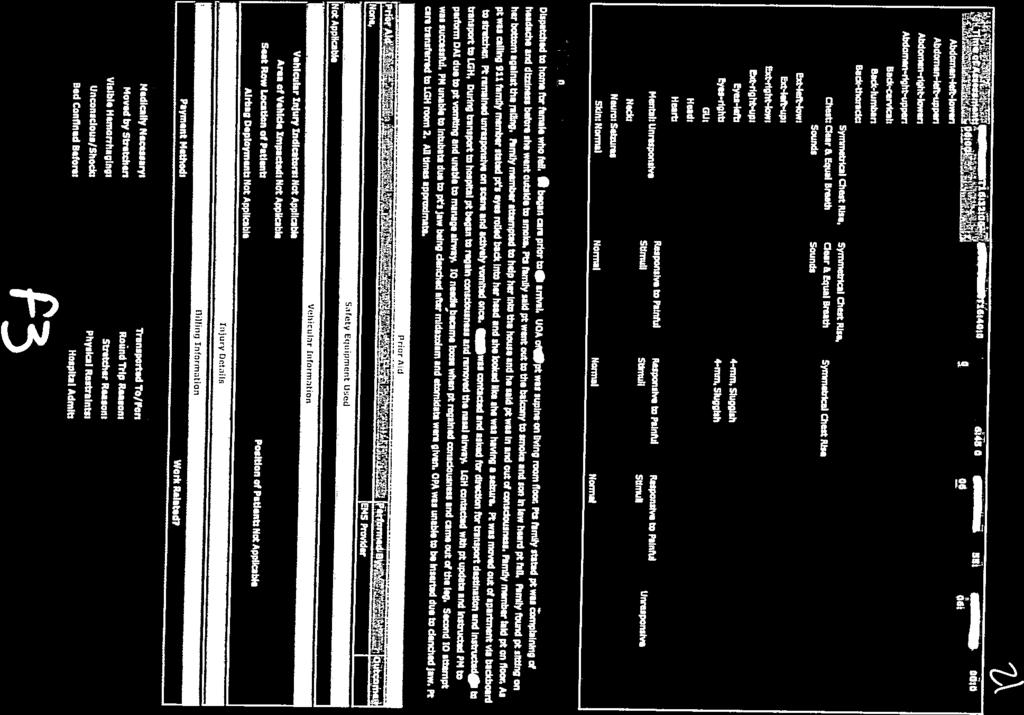
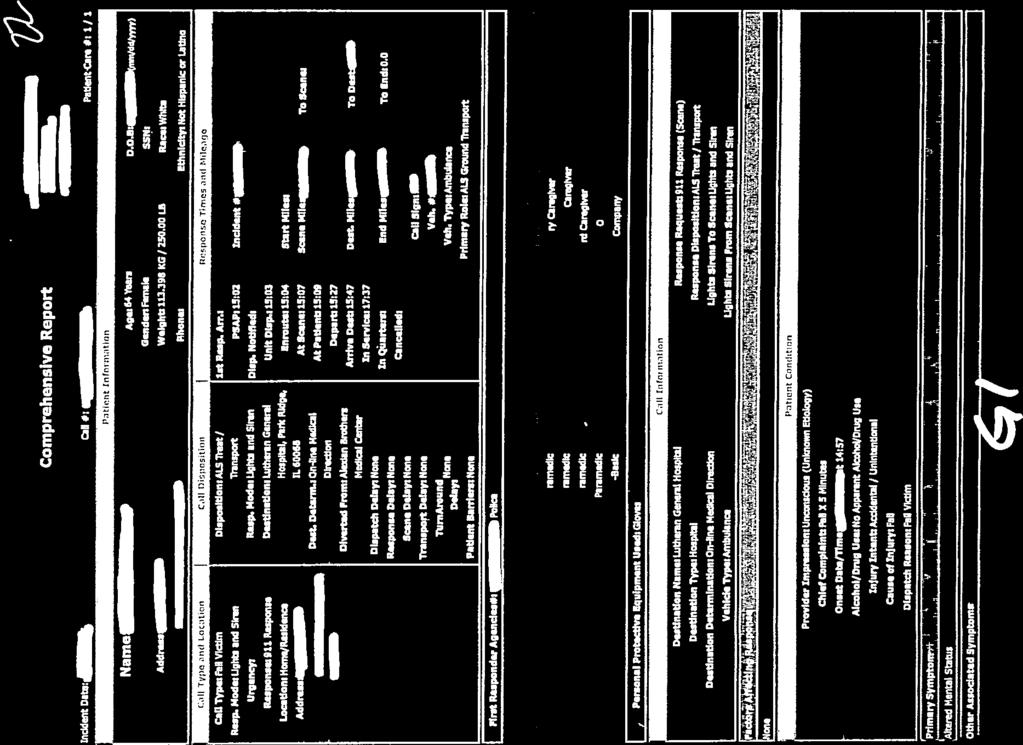
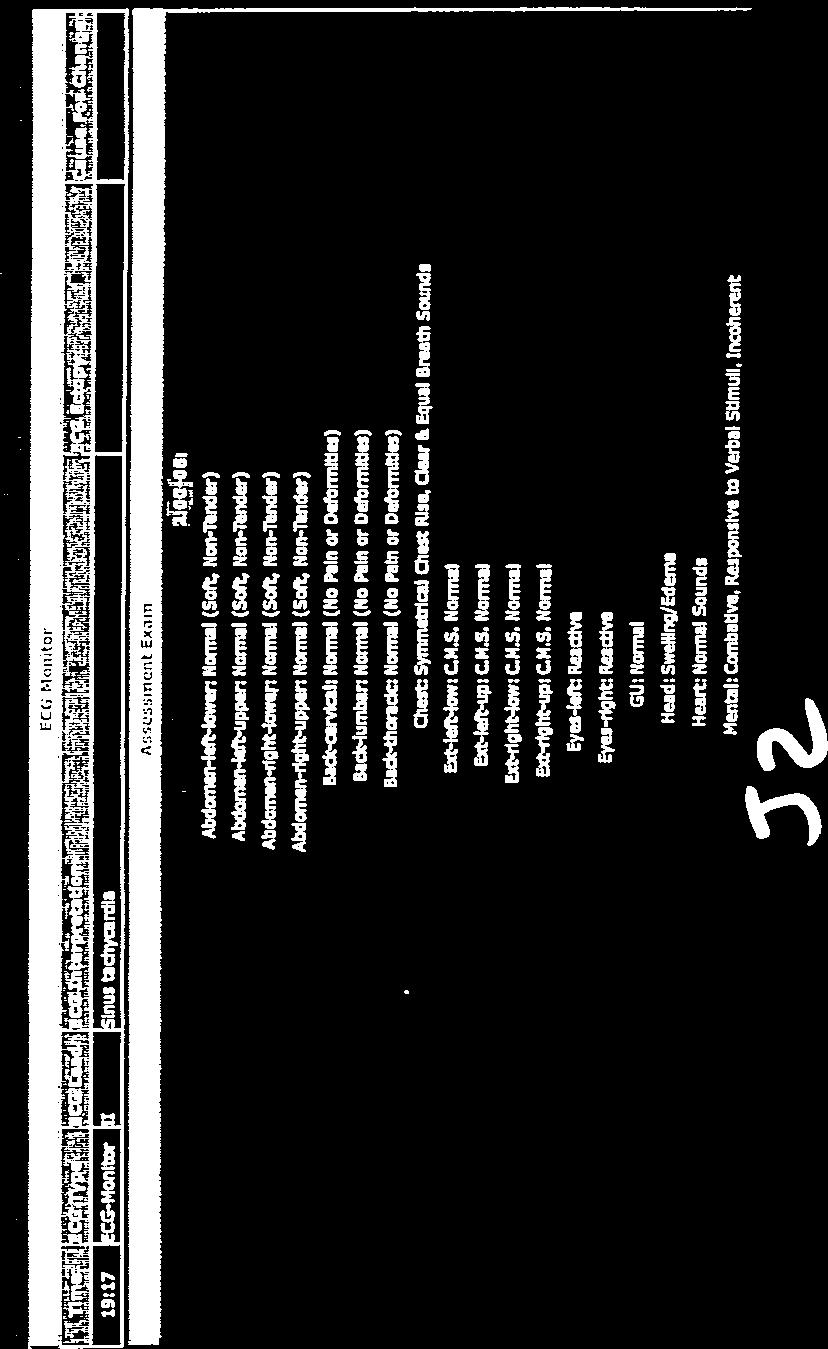
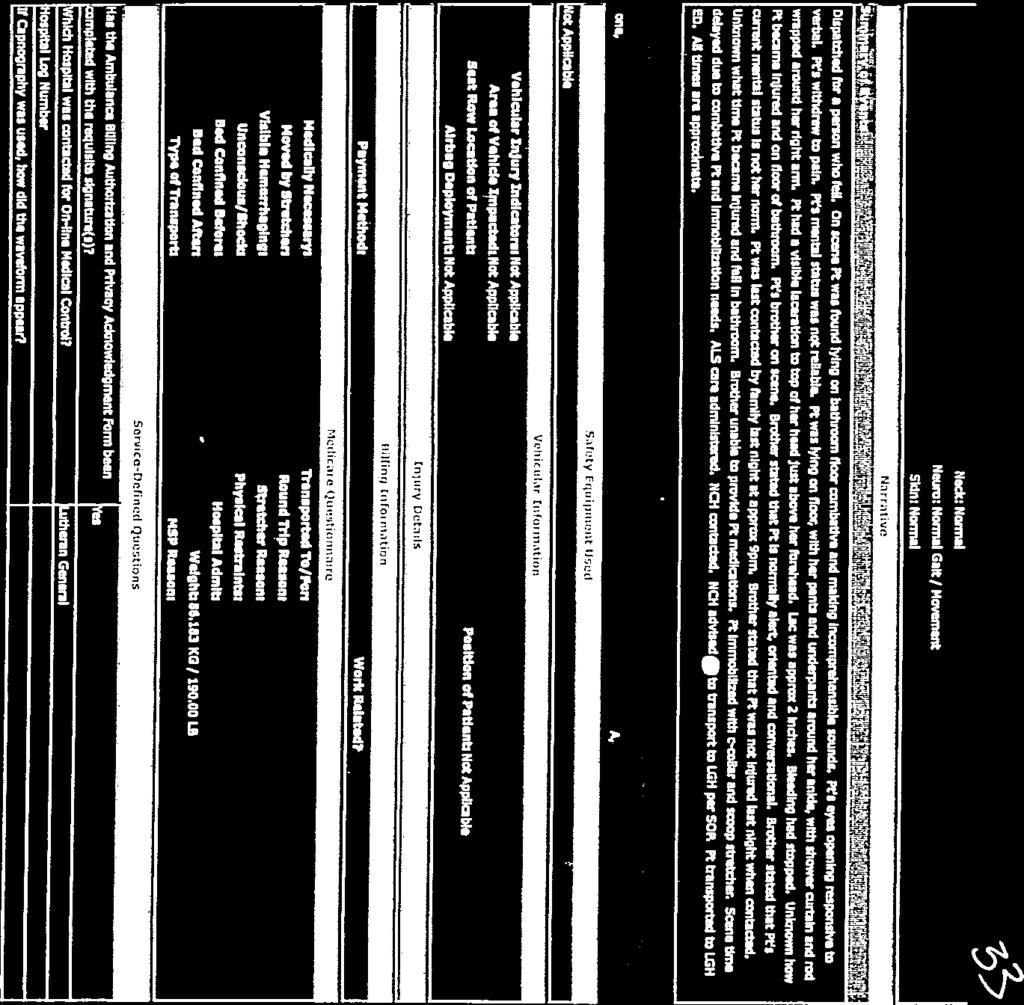
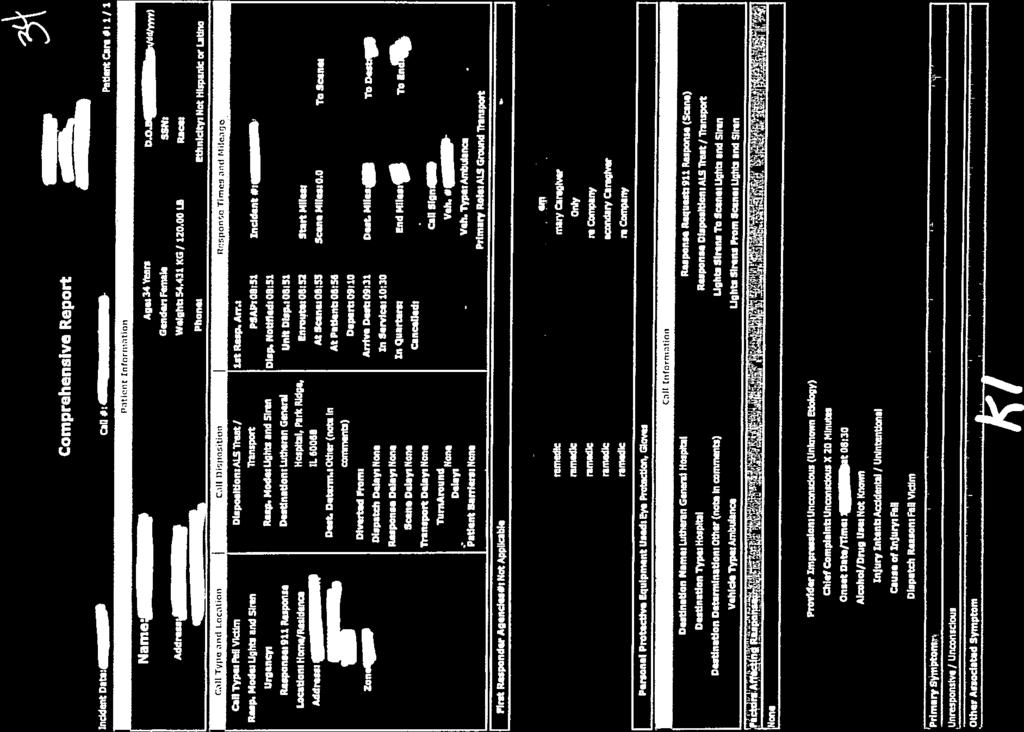
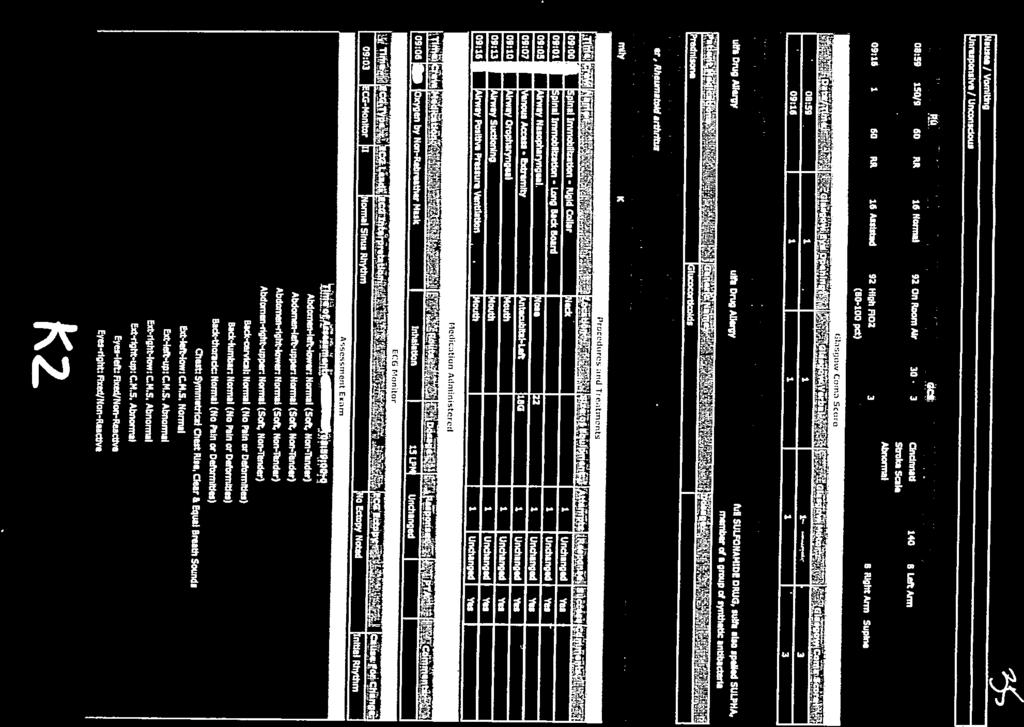
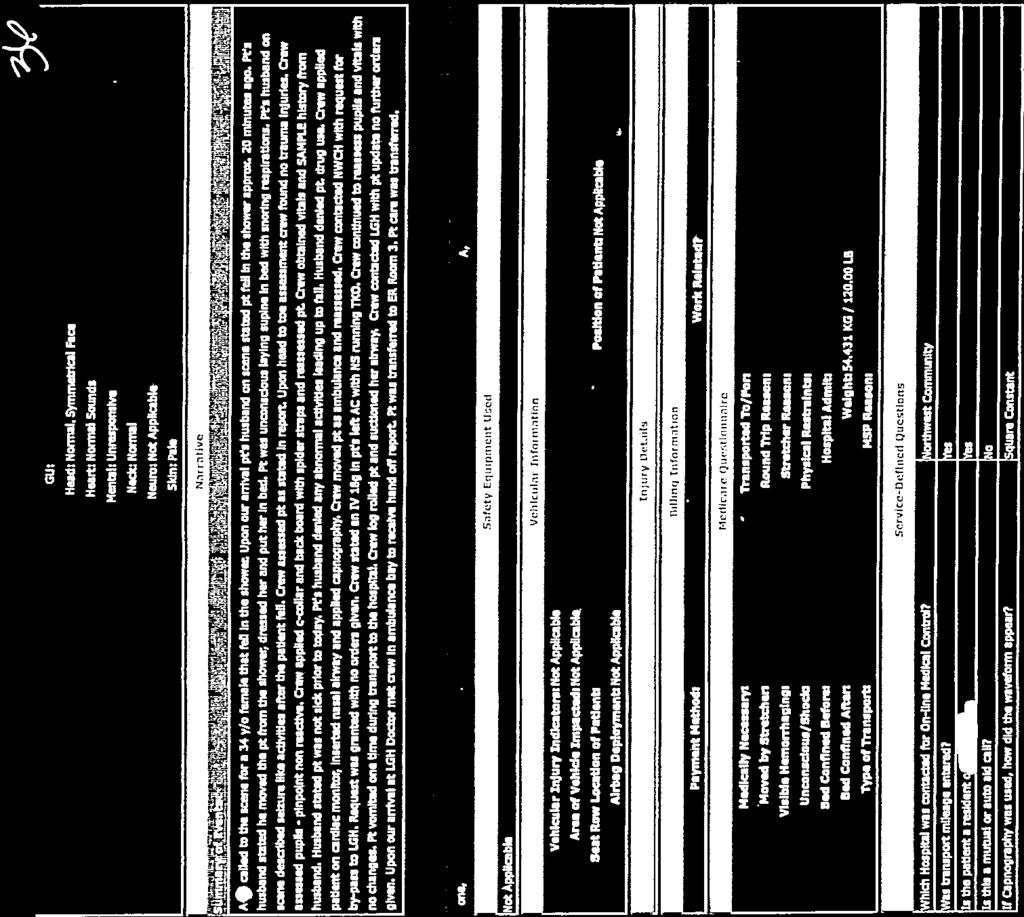
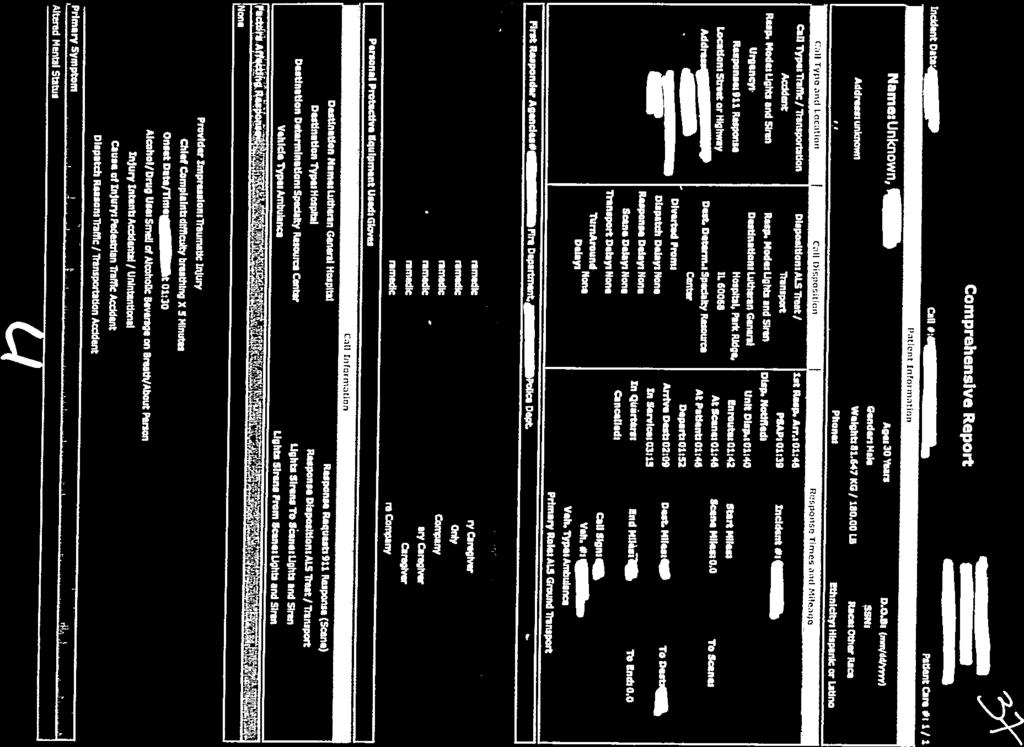
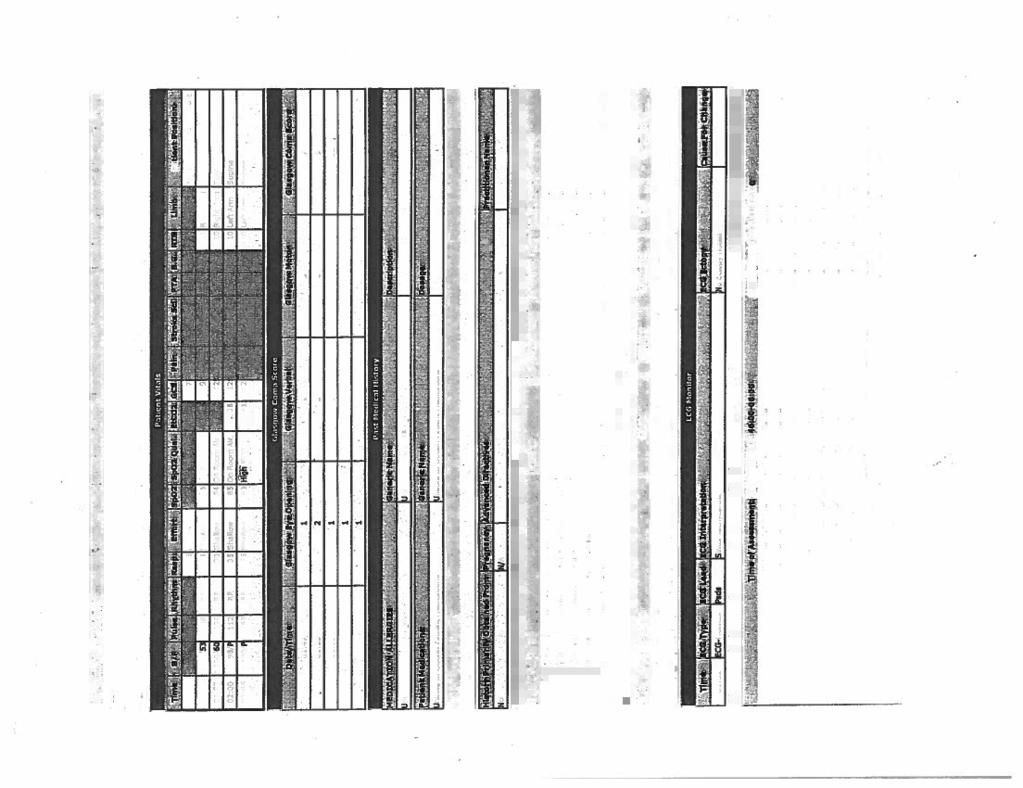
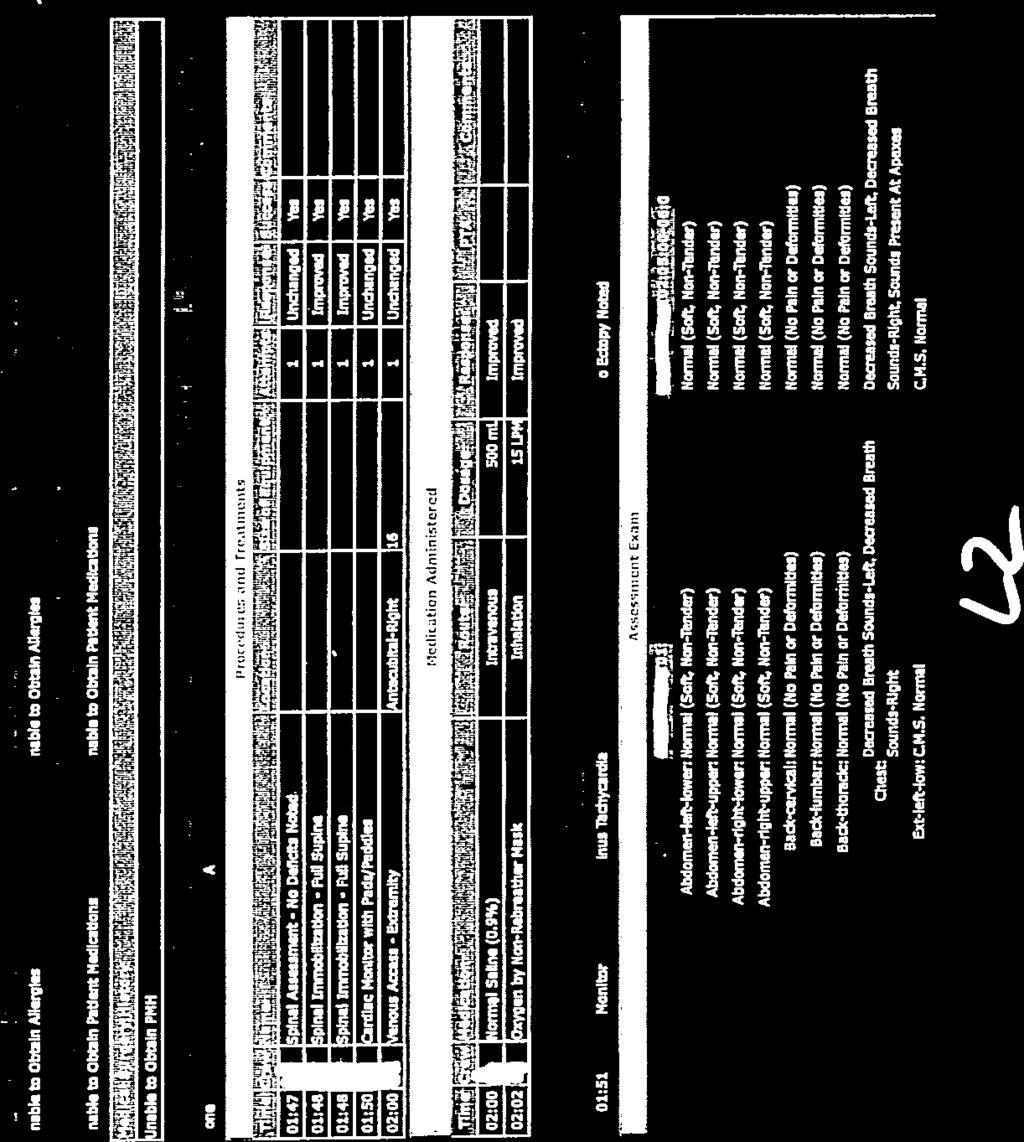
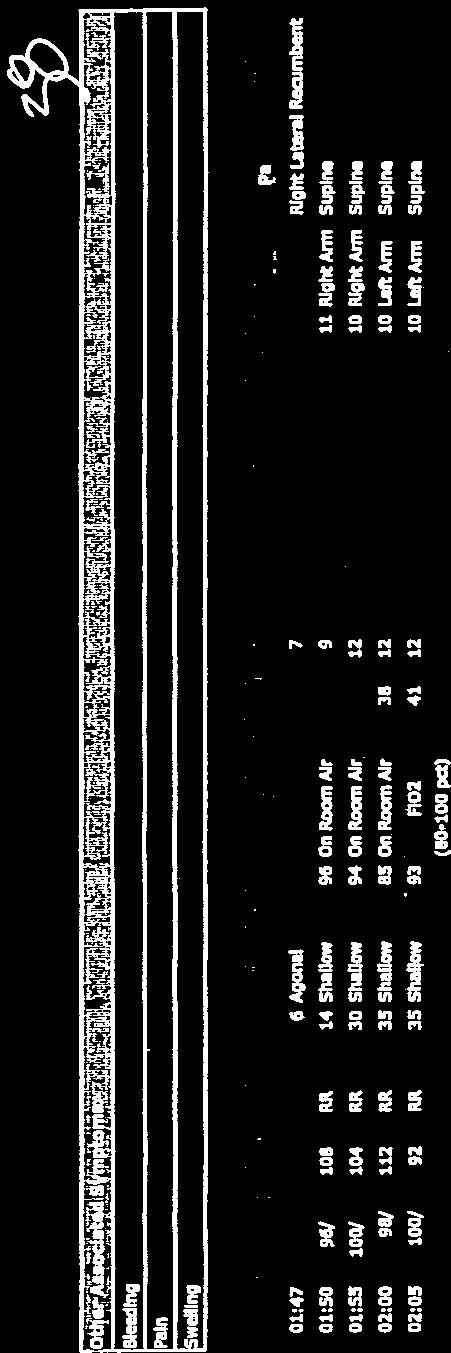
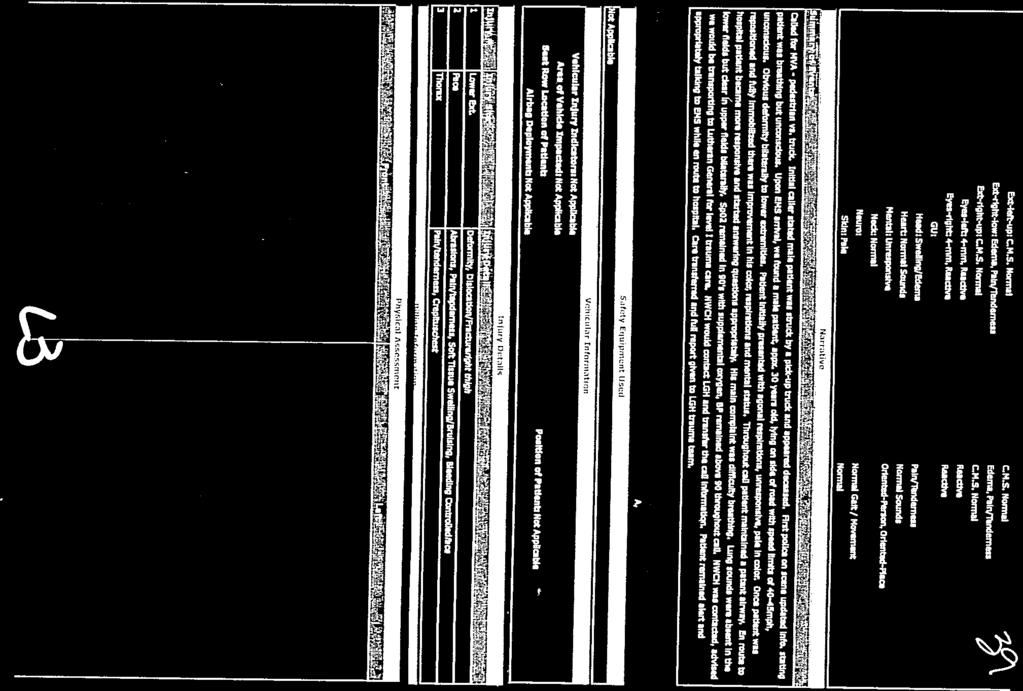
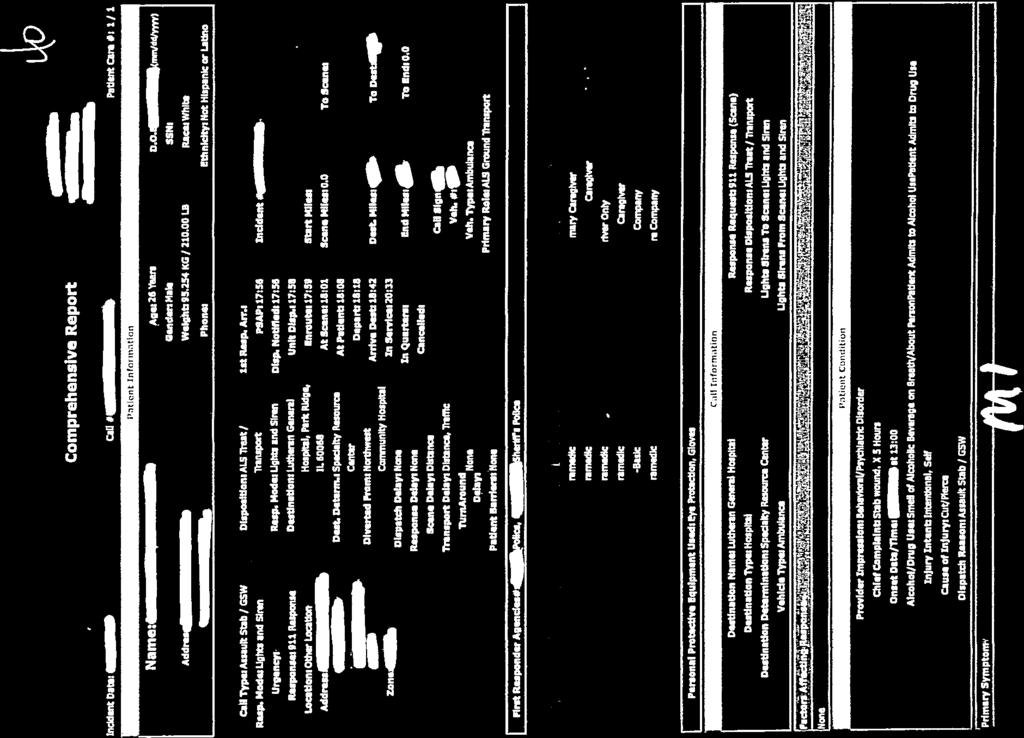
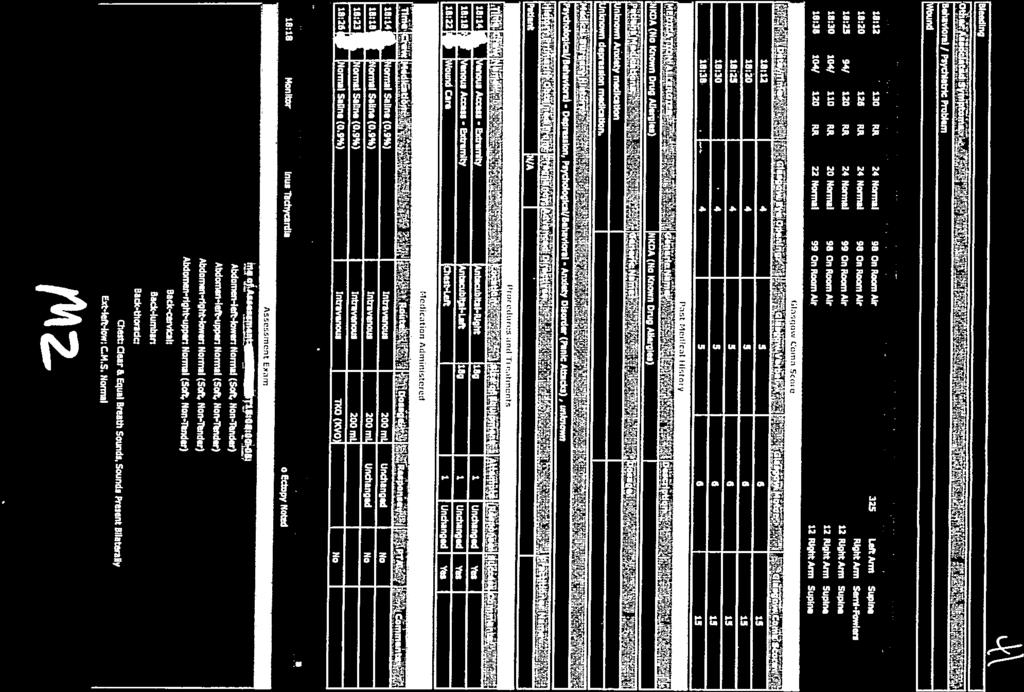
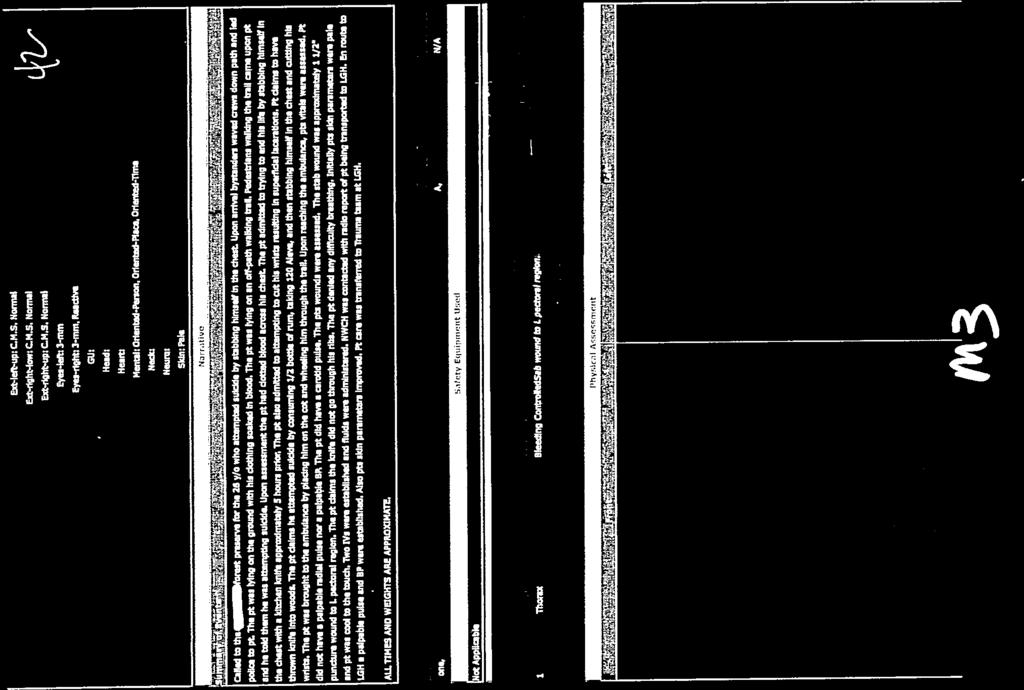
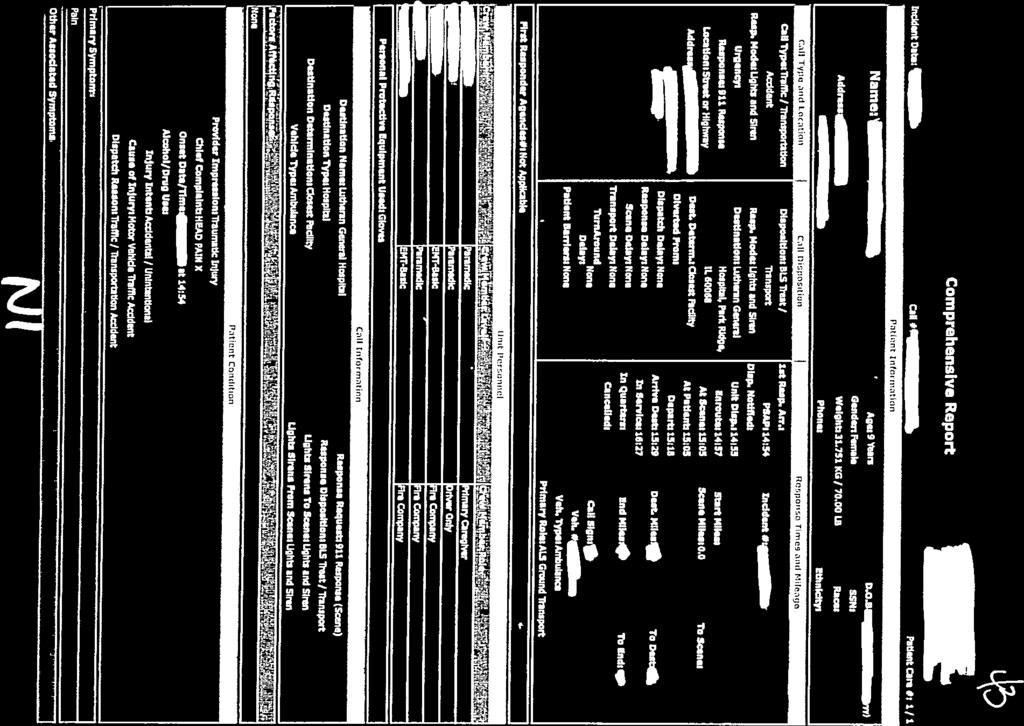
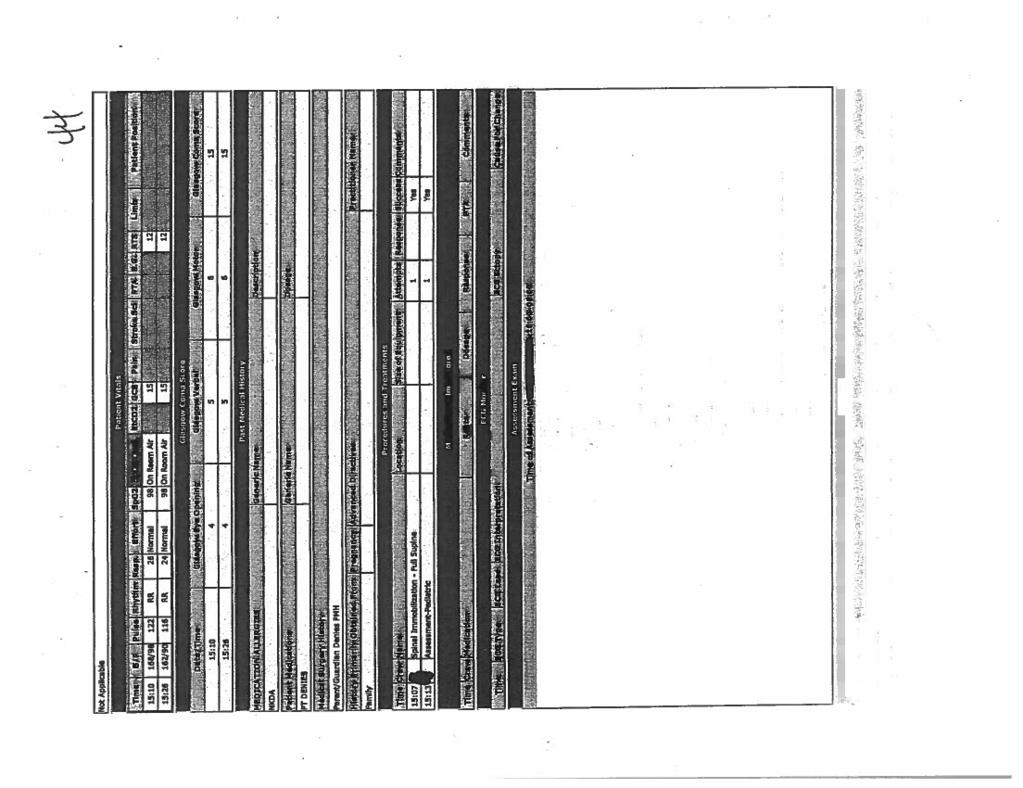
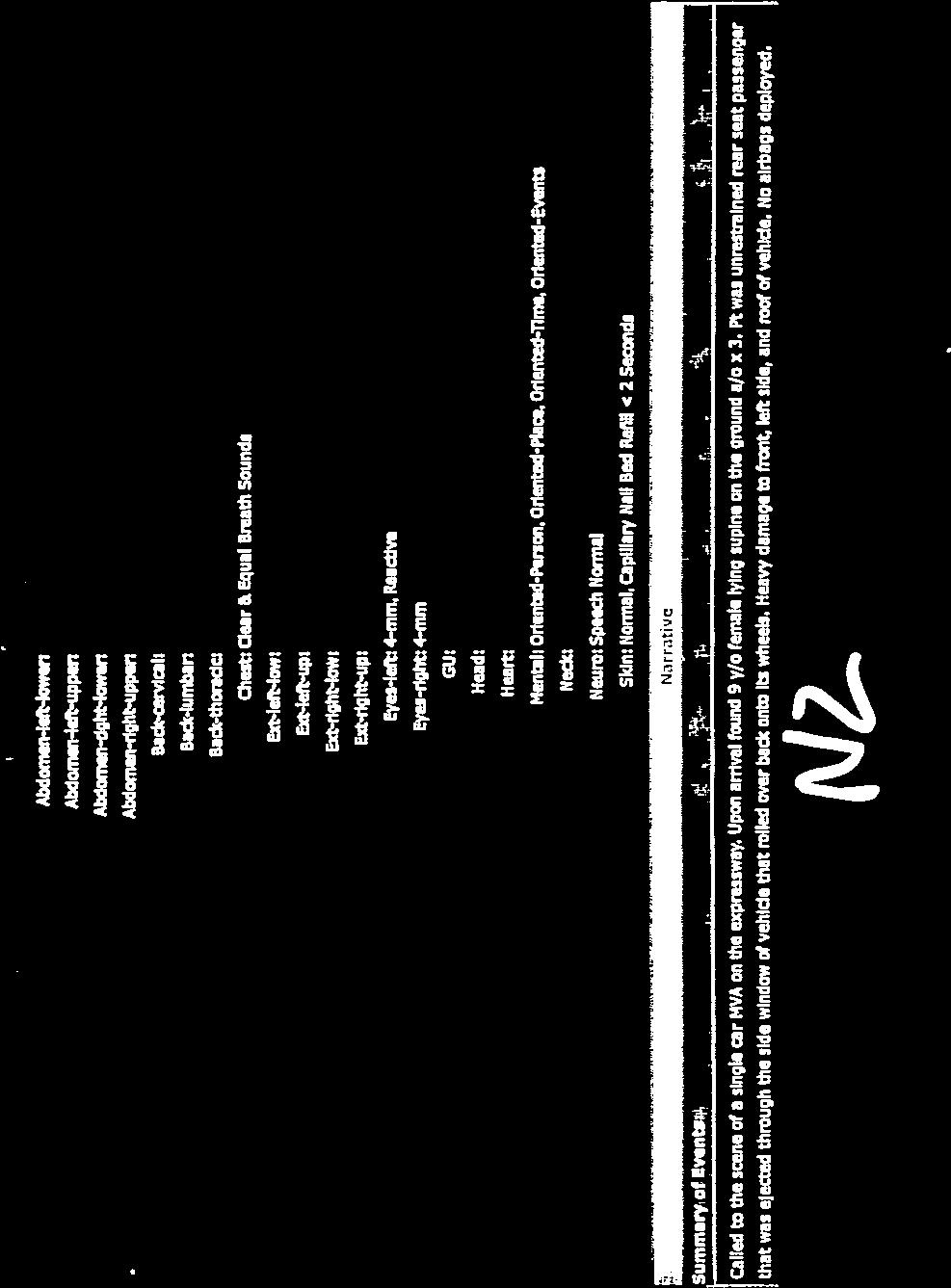
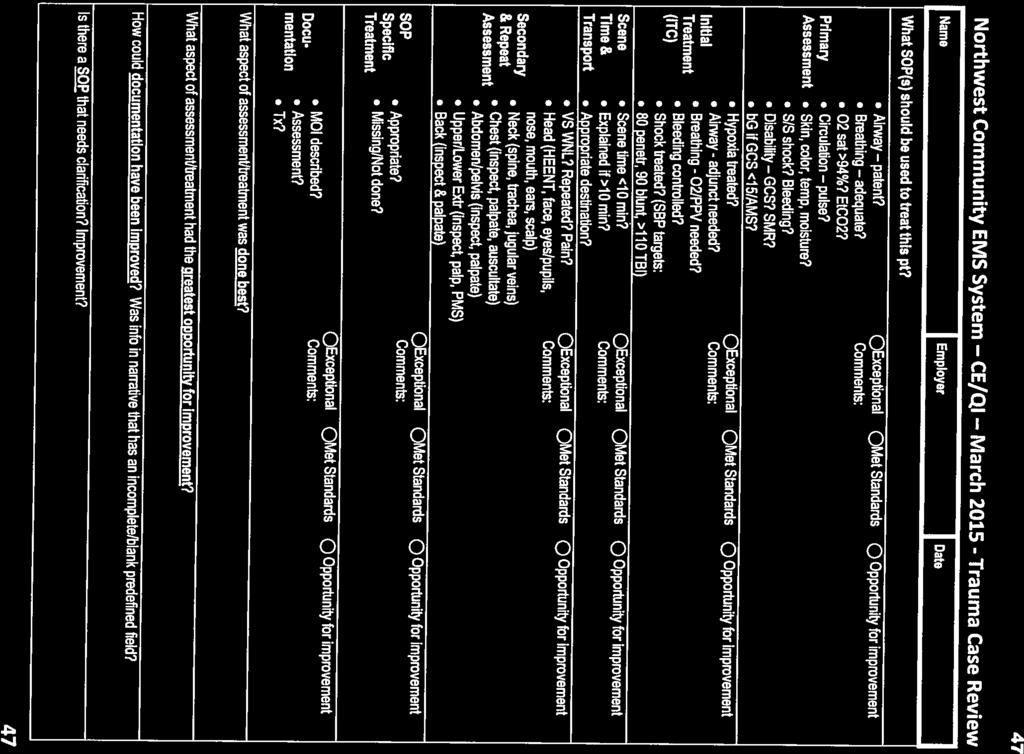
2 f. List 5 pts where hyperoxia is contraindicated. i. ii. iii. iv. v. g. How should oxygen be delivered to pts with an O2 sat less than 92%? h. At what rate should you assist vent in pt with or without an adv airway? 4) Use the following information (also handout pg 47), to HELP analyze and evaluate the calls (epcr s on pages 4-45). Complete the grid on the next page (also handout pg 48), identifying 3 things done well and 3 areas with opportunity for improvement for each call. Primary Assessment (ITC) Initial Treatment Scene Time & Transport Secondary & Repeat Assessment Airway patent? Breathing adequate? O2 sat >94%? EtCO2? Circulation pulse? Airway - adjunct needed? Breathing - O2/PPV needed? Bleeding controlled? Scene time <10 min? Explained if >10 min? VS WNL? Repeated? Pain? Head (HEENT, face, eyes/pupils, nose, mouth, ears, scalp) Neck (spine, trachea, jugular veins) Chest (inspect, palpate, auscultate) Abdomen/pelvis (inspect, palpate) Skin, color, temp, moisture? S/S shock? Bleeding? Disability GCS? SMR? bg if GCS <15/AMS? Hypoxia treated? Shock treated? (SBP targets: 80 penetr, 90 blunt, >110 TBI) Appropriate destination? Upper/Lower Extr (inspect, palp, PMS) Back (inspect & palpate) SOP Specific Tx Appropriate? Missing/Not done? Documentation MOI described? Assessment? Tx? What aspect of assessment/treatment was done best? What aspect of assessment/treatment had the greatest opportunity for improvement? How could documentation have been improved? Was info in narrative that has an incomplete/blank predefined field? Is there a SOP that needs clarification? Improvement?
3 # Done Well Opportunity for Improvement A B C D E F G H I J K L M N



4 Northwest Community EMS System Continuing Education March 2015 Trauma QI Case Reviews Materials Needed Continuing Education March 2015 Trauma QI Case Reviews Diana Neubecker RN BSN EMT-PM EMS System In-Field Coordinator 1 Pen/pencil SOP s NWC EMSS SOP s 2 Objectives Objectives Upon completion the participant will: Correctly interpret the ECG rhythm when given a 6- second rhythm strip. Recognize signs of acute myocardial ischemia and injury, old and new infarction when given a 12L ECG. Analyze and evaluate EMS assessment, treatment and documentation for trauma patients with head, chest, abdominal/pelvic, spine and MSK/extremity injuries when given an epcr. Analyze and evaluate EMS assessment, treatment and DOCUMENTATION for trauma patients with head, chest, abdominal/pelvic, spine and MSK/extremity injuries when given an epcr. Actually PBPI asked for it 3 4 DIANA:ce-tr




5 Northwest Community EMS System Continuing Education March 2015 Trauma QI Case Reviews ECG Interpretation ECG Interpretation ❶ ❹ ❷ ❺ ❸ ❻ L Interpretation Educational Methodology Vent Rate: 72 P Duration: 82 ms PR Interval: 158 ms QRS Duration: 92 ms QT/QTc: 376/411 ms P-R-T Axis: What, if any, leads have ST elevation (STE)? What is the significance of STE? What, if any, leads have pathologic Q waves? What is the significance of Q waves? INTERPRETATION: V1-V5 = STE STE = acute injury V1-V4 = Q waves Q waves = infarction Acute Anteroseptal MI THANK YOU Palatine FD for this 12L ECG 7 Tie together Education & Quality Improvement 8 DIANA:ce-tr





")
 Hypoxia")
 Need higher SBP")
6 Northwest Community EMS System Continuing Education March 2015 Trauma QI Case Reviews Education Quality Improvement None of us is as smart as all of us. Blanchard 9? Changes Needed? Education Policies Procedures SOP s Patient Care epcr s 10 Trauma QI Case Reviews Trauma Tips 1. Avoid under-triage (some over-triage OK) 2. EtCO2 helps detect shock ( EtCO2 w/ shock) 3. Keep pts warm (cold impairs coagulation) Cover, increase amb temp, use warm IVF 4. Traumatic brain injured (TBI) Hypoxia quadruples mortality ( 4 x) Hypotension triples mortality ( 3 x) Need higher SBP for adequate cerebral perfusion Both Hypoxia & Hypotension - mortality 14 x DIANA:ce-tr

 1. Uncomplicated Acute MI 2.")

")

7 Northwest Community EMS System Continuing Education March 2015 Trauma QI Case Reviews Trauma Tips Oxygenation & Ventilation IMC SOP pg 3 Hyperoxia contraindicated: Give O2 only if hypoxia, titrate without causing hyperoxia (94%) 1. Uncomplicated Acute MI 2. Post-cardiac arrest 3. Acute exacerbations COPD 4. Stroke 5. Newborn resuscitation ITC SOP pg 37 SpO % = O2 1-6 L/NC SpO2 < 92% or per protocol = O L (NRB/BVM) Assist ventilation rates - adults Before advanced airway = breaths/minute (asthma: 6-8 BPM) After advanced airway = 8-10 breaths/minute Do NOT hyperventilate Everyone Participates Trauma QI Case Reviews 10 minutes to review your assigned case DIANA:ce-tr




8 Northwest Community EMS System Continuing Education March 2015 Trauma QI Case Reviews Trauma QI Case Reviews For each of the following list 1-2 things. 1. Assessment/treatment done best? What are we doing well? 2. Assessment/treatment had the most opportunity for improvement? ~5 minutes to review & discuss case 3. How could documentation been improved? 4. SOP that needs clarification / modification? What did you learn? DIANA:ce-tr
9

10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37

38
39
40

41
42

43

44
45
46
47
48
49
50
51

52
53
54
55
56
Cardiac Arrest & Therapeutic Hypothermia. Continuing Education May 2012
 Continuing Education May 2012 Cardiac Arrest & Therapeutic Hypothermia Questions/comments on this CE are welcome and should be directed to: Diana Neubecker RN BSN PM NWC EMSS In-Field Coordinator dneubecker@nch.org
Continuing Education May 2012 Cardiac Arrest & Therapeutic Hypothermia Questions/comments on this CE are welcome and should be directed to: Diana Neubecker RN BSN PM NWC EMSS In-Field Coordinator dneubecker@nch.org
Northwest Community EMS System September 2017: Head and Chest Trauma Credit Questions
 NWC EMSS Sept 2017 CE: Head & Chest Trauma. Credit Questions - page 1 Northwest Community EMS System September 2017: Head and Chest Trauma Credit Questions Name: EMS Agency EMSC/Educator reviewer: Date
NWC EMSS Sept 2017 CE: Head & Chest Trauma. Credit Questions - page 1 Northwest Community EMS System September 2017: Head and Chest Trauma Credit Questions Name: EMS Agency EMSC/Educator reviewer: Date
Northwest Community EMS System Continuing Education Class Credit Questions Respiratory Assessment January 2012
 Name (PRINT): Date submitted: Affiliation: Rating: [ ] Complete [ ] Incomplete Reminder: You must schedule to take the class post-test with your assigned hospital EMS Coordinator/educator or their designee
Name (PRINT): Date submitted: Affiliation: Rating: [ ] Complete [ ] Incomplete Reminder: You must schedule to take the class post-test with your assigned hospital EMS Coordinator/educator or their designee
Northwest Community EMS System Continuing Education Class Credit Questions for April 2014 Summer Emergencies
 Northwest Community EMS System Continuing Education Class Credit Questions for April 2014 Summer Emergencies Name (PRINT): Date submitted: Affiliation: Rating: [ ] Complete [ ] Incomplete The answers are
Northwest Community EMS System Continuing Education Class Credit Questions for April 2014 Summer Emergencies Name (PRINT): Date submitted: Affiliation: Rating: [ ] Complete [ ] Incomplete The answers are
Northwest Community EMS System May 2018 CE: Summer Emergencies Credit Questions
 Northwest Community EMS System May 2018 CE: Summer Emergencies Credit Questions Name: EMS Agency/hospital: EMSC/Educator reviewer: Date submitted: Credit awarded (date): Returned for revisions: Revisions
Northwest Community EMS System May 2018 CE: Summer Emergencies Credit Questions Name: EMS Agency/hospital: EMSC/Educator reviewer: Date submitted: Credit awarded (date): Returned for revisions: Revisions
Northwest Community EMS System Feb 2018 CE: Multiple Patient Incidents/ChemPack Intro Credit Questions
 Northwest Community EMS System Feb 2018 CE: Multiple Patient Incidents/ChemPack Intro Credit Questions Name: EMS Agency/hospital: EMSC/Educator reviewer: Date submitted: Credit awarded (date): Returned
Northwest Community EMS System Feb 2018 CE: Multiple Patient Incidents/ChemPack Intro Credit Questions Name: EMS Agency/hospital: EMSC/Educator reviewer: Date submitted: Credit awarded (date): Returned
Northwest Community Healthcare Paramedic Education Program AV Conduction Defects/AV Blocks Connie J. Mattera, M.S., R.N., EMT-P
 Northwest Community Healthcare Paramedic Education Program AV Conduction Defects/ Connie J. Mattera, M.S., R.N., EMT-P Reading assignments: Bledsoe Vol. 3: pp. 88-93; 120-121 (atropine, norepinephrine,
Northwest Community Healthcare Paramedic Education Program AV Conduction Defects/ Connie J. Mattera, M.S., R.N., EMT-P Reading assignments: Bledsoe Vol. 3: pp. 88-93; 120-121 (atropine, norepinephrine,
3. D Objective: Chapter 4, Objective 4 Page: 79 Rationale: A carbon dioxide level below 35 mmhg indicates hyperventilation.
 1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
Northwest Community EMS System November 2018 CE: Cardiac Treatment Credit Questions
 Northwest Community EMS System November 2018 CE: Cardiac Treatment Credit Questions Name: EMS Agency/hospital: EMSC/Educator reviewer: Date submitted: Credit awarded (date): Returned for revisions: Revisions
Northwest Community EMS System November 2018 CE: Cardiac Treatment Credit Questions Name: EMS Agency/hospital: EMSC/Educator reviewer: Date submitted: Credit awarded (date): Returned for revisions: Revisions
Resuscitation Checklist
 Resuscitation Checklist Actions if multiple responders are on scene Is resuscitation appropriate? Conditions incompatible with life Advanced decision in place Based on the information available, the senior
Resuscitation Checklist Actions if multiple responders are on scene Is resuscitation appropriate? Conditions incompatible with life Advanced decision in place Based on the information available, the senior
June 2009 CE. Site code # E-1209
 1 June 2009 CE Site code # 107200E-1209 Region X SOP Review ACS, Asystole/PEA, Bradycardia, VF/Pulseless VT, Conscious Sedation, Region X Field Triage Criteria Prepared by: Sharon Hopkins, RN, BSN, EMT-P
1 June 2009 CE Site code # 107200E-1209 Region X SOP Review ACS, Asystole/PEA, Bradycardia, VF/Pulseless VT, Conscious Sedation, Region X Field Triage Criteria Prepared by: Sharon Hopkins, RN, BSN, EMT-P
Northwest Community EMS System August 2018 CE: Sepsis and Septic Shock Credit Questions
 Northwest Community EMS System August 2018 CE: Sepsis and Septic Shock Credit Questions Name: EMS Agency/hospital: EMSC/Educator reviewer: Date submitted: Credit awarded (date): Returned for revisions:
Northwest Community EMS System August 2018 CE: Sepsis and Septic Shock Credit Questions Name: EMS Agency/hospital: EMSC/Educator reviewer: Date submitted: Credit awarded (date): Returned for revisions:
Which patients can be
 SOP roll-out 2014 One cannot practice the art of medicine if they do not know all the science of medicine first. Paul Matera, M.D., EMTP A clinician becomes competent through the following processes Experience
SOP roll-out 2014 One cannot practice the art of medicine if they do not know all the science of medicine first. Paul Matera, M.D., EMTP A clinician becomes competent through the following processes Experience
Northwest Community EMS System Continuing Education Class Credit Questions for October 2014 Spine Motion Restriction (Didactic)
") Northwest Community EMS System Continuing Education Class Credit Questions for October 2014 Spine Motion Restriction (Didactic) Name (PRINT): Date submitted: Affiliation: Rating: [ ] Complete [ ] Incomplete
Northwest Community EMS System Continuing Education Class Credit Questions for October 2014 Spine Motion Restriction (Didactic) Name (PRINT): Date submitted: Affiliation: Rating: [ ] Complete [ ] Incomplete
SOPs: ACS, Bradycardia with a Pulse; Narrow QRS Complex Tachycardia; Wide Complex Tachycardia with a Pulse.
 Northwest Community EMS System Continuing Education Program April 2018 ACS, ECG/12 Lead Interpretation, Dysrhythmia Management PARTICIPANT handout Jennifer Dyer, RN, BS, EMT-P References: SOPs: ACS, Bradycardia
Northwest Community EMS System Continuing Education Program April 2018 ACS, ECG/12 Lead Interpretation, Dysrhythmia Management PARTICIPANT handout Jennifer Dyer, RN, BS, EMT-P References: SOPs: ACS, Bradycardia
EMT. Chapter 14 Review
 EMT Chapter 14 Review Review 1. All of the following are common signs and symptoms of cardiac ischemia, EXCEPT: A. headache. B. chest pressure. C. shortness of breath. D. anxiety or restlessness. Review
EMT Chapter 14 Review Review 1. All of the following are common signs and symptoms of cardiac ischemia, EXCEPT: A. headache. B. chest pressure. C. shortness of breath. D. anxiety or restlessness. Review
ITLS Advanced Pre-Test Annotated Key 8 th Edition
 1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
Post Resuscitation (ROSC) Care
 Care") Standard Operating Procedure 2.10 Post Resuscitation (ROSC) Care Position Responsible: Medical Director Approved: Clinical Governance Committee Related Documents: This document is the intellectual property
Standard Operating Procedure 2.10 Post Resuscitation (ROSC) Care Position Responsible: Medical Director Approved: Clinical Governance Committee Related Documents: This document is the intellectual property
Routine Patient Care Guidelines - Adult
 Routine Patient Care Guidelines - Adult All levels of provider will complete an initial & focused assessment on every patient, and as standing order, use necessary and appropriate skills and procedures
Routine Patient Care Guidelines - Adult All levels of provider will complete an initial & focused assessment on every patient, and as standing order, use necessary and appropriate skills and procedures
ACLS Prep. Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep.
 November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
Advanced Cardiac Life Support (ACLS) Science Update 2015
 Science Update 2015") 1 2 3 4 5 6 7 8 9 Advanced Cardiac Life Support (ACLS) Science Update 2015 What s New in ACLS for 2015? Adult CPR CPR remains (Compressions, Airway, Breathing Chest compressions has priority over all other
1 2 3 4 5 6 7 8 9 Advanced Cardiac Life Support (ACLS) Science Update 2015 What s New in ACLS for 2015? Adult CPR CPR remains (Compressions, Airway, Breathing Chest compressions has priority over all other
Therapeutic hypothermia
 INDUCED HYPOTHERMIA Dr. Attilla Kiss M.D. Acting Medical Director Emergency Services EMS Medical Director St. John Medical Center OBJECTIVES Define and explain Induced Hypothermia Discuss both pre-hospital
INDUCED HYPOTHERMIA Dr. Attilla Kiss M.D. Acting Medical Director Emergency Services EMS Medical Director St. John Medical Center OBJECTIVES Define and explain Induced Hypothermia Discuss both pre-hospital
MASSACHUSETTS DEPARTMENT OF PUBLIC HEALTH OFFICE OF EMERGENCY MEDICAL SERVICES Basic EMT Practical Examination Cardiac Arrest Management
 Basic EMT Practical Examination 6.0 - Cardiac Arrest Management Station 1 RESUSCITATION & DEFIBRILLATION No Point WHILE FUNCTIONING AS FIRST RESCUER: Point 1. Verbalizes or takes body substance isolation
Basic EMT Practical Examination 6.0 - Cardiac Arrest Management Station 1 RESUSCITATION & DEFIBRILLATION No Point WHILE FUNCTIONING AS FIRST RESCUER: Point 1. Verbalizes or takes body substance isolation
Northwest Community EMS System Continuing Education Class Credit Questions for August 2014 Medical Shock
 Northwest Community EMS System Continuing Education Class Credit Questions for August 2014 Medical Shock Name (PRINT): Date submitted: Affiliation: Rating: [ ] Complete [ ] Incomplete Indicate whether
Northwest Community EMS System Continuing Education Class Credit Questions for August 2014 Medical Shock Name (PRINT): Date submitted: Affiliation: Rating: [ ] Complete [ ] Incomplete Indicate whether
MICHIGAN. Table of Contents. State Protocols. Adult Treatment Protocols
 MICHIGAN State Protocols Protocol Number Protocol Name Adult Treatment Protocols Table of Contents 3.1 Altered Mental Status 3.2 Stroke/Suspected Stroke 3.3 Respiratory Distress 3.4 Seizures 3.5 Sepsis
MICHIGAN State Protocols Protocol Number Protocol Name Adult Treatment Protocols Table of Contents 3.1 Altered Mental Status 3.2 Stroke/Suspected Stroke 3.3 Respiratory Distress 3.4 Seizures 3.5 Sepsis
Appendix E Choose the sign or symptom that best indicates severe respiratory distress.
 Appendix E-2 1. In Kansas EMT-B may monitor pulse oximetry: a. after they complete the EMT-B course b. when the service purchases the state approved pulse oximeters c. when the service director receives
Appendix E-2 1. In Kansas EMT-B may monitor pulse oximetry: a. after they complete the EMT-B course b. when the service purchases the state approved pulse oximeters c. when the service director receives
Emergency Room Resuscitation of the Unstable Trauma Patient
 Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
Wake County EMS System Peer Review/Clinical Data/System Performance
 P a g e 1 Wake County EMS System Peer Review/Clinical Data/System Performance Explanations and Definitions for Reports Wake County EMS engages in regular external review. The System makes quarterly reports
P a g e 1 Wake County EMS System Peer Review/Clinical Data/System Performance Explanations and Definitions for Reports Wake County EMS engages in regular external review. The System makes quarterly reports
A silent chest is. Pediatrics II Asthma, seizures and cardiac arrest. Children are different. Cough variant asthma. Symptoms of severe distress
 Asthma ~21% of all asthma cases are school aged Pediatrics II Asthma, seizures and cardiac arrest Identify 3 symptoms of an asthma exacerbation Bronchospasm Edema of the bronchi Increased mucus production
Asthma ~21% of all asthma cases are school aged Pediatrics II Asthma, seizures and cardiac arrest Identify 3 symptoms of an asthma exacerbation Bronchospasm Edema of the bronchi Increased mucus production
IFT1 Interfacility Transfer of STEMI Patients. IFT2 Interfacility Transfer of Intubated Patients. IFT3 Interfacility Transfer of Stroke Patients
 IFT1 Interfacility Transfer of STEMI Patients IFT2 Interfacility Transfer of Intubated Patients IFT3 Interfacility Transfer of Stroke Patients Interfacility Transfer Guidelines IFT 1 TRANSFER INTERFACILITY
IFT1 Interfacility Transfer of STEMI Patients IFT2 Interfacility Transfer of Intubated Patients IFT3 Interfacility Transfer of Stroke Patients Interfacility Transfer Guidelines IFT 1 TRANSFER INTERFACILITY
Competency Log Professional Responder Courses
 Competency Log Professional Responder Courses Check off each competency once successfully demonstrated. This log may be used as a support tool when teaching a Professional Responder course. Refer to the
Competency Log Professional Responder Courses Check off each competency once successfully demonstrated. This log may be used as a support tool when teaching a Professional Responder course. Refer to the
Pre-hospital Trauma Life Support. Rattiya Banjungam Emergency Physician, Khon Kaen Hospital
 Pre-hospital Trauma Life Support Rattiya Banjungam Emergency Physician, Khon Kaen Hospital Golden principles of Prehospital Trauma Care Golden Hour There is a golden hour if you are critically injured,
Pre-hospital Trauma Life Support Rattiya Banjungam Emergency Physician, Khon Kaen Hospital Golden principles of Prehospital Trauma Care Golden Hour There is a golden hour if you are critically injured,
McCann Technical School 70 Hodges Cross Road North Adams, MA Medical Assisting Program
 MA 104 MEDICAL SOCIAL SCIENCE 4 Credits Fall Semester Part IV FIRST RESPONDER Syllabus McCann Technical School 70 Hodges Cross Road North Adams, MA 01247 Medical Assisting Program INSTRUCTORS: Laurie Tuper,
MA 104 MEDICAL SOCIAL SCIENCE 4 Credits Fall Semester Part IV FIRST RESPONDER Syllabus McCann Technical School 70 Hodges Cross Road North Adams, MA 01247 Medical Assisting Program INSTRUCTORS: Laurie Tuper,
Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing
 1 2 3 4 5 6 Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing D-Disability Chief complaint and/or Mechanism
1 2 3 4 5 6 Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing D-Disability Chief complaint and/or Mechanism
PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT
 PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT Board Approved June 2007 Revised December 2009 Revised July 2011 Revised June 2015 435 Hunter Street Fredericksburg, VA 22401
PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT Board Approved June 2007 Revised December 2009 Revised July 2011 Revised June 2015 435 Hunter Street Fredericksburg, VA 22401
COUNTY OF SACRAMENTO EMERGENCY MEDICAL SERVICES AGENCY
 COUNTY OF SACRAMENTO EMERGENCY MEDICAL SERVICES AGENCY Document # 8024.31 PROGRAM DOCUMENT: Initial Date: 10/26/94 Cardiac Dysrhythmias Last Approval Date: 11/01/16 Effective Date: 11/01/18 Next Review
COUNTY OF SACRAMENTO EMERGENCY MEDICAL SERVICES AGENCY Document # 8024.31 PROGRAM DOCUMENT: Initial Date: 10/26/94 Cardiac Dysrhythmias Last Approval Date: 11/01/16 Effective Date: 11/01/18 Next Review
Emergency Care Progress Log
 Emergency Care Progress Log For further details on the National Occupational Competencies for EMRs, please visit www.paramedic.ca. Check off each skill once successfully demonstrated the Instructor. All
Emergency Care Progress Log For further details on the National Occupational Competencies for EMRs, please visit www.paramedic.ca. Check off each skill once successfully demonstrated the Instructor. All
Hypotension / Shock. Adult Medical Section Protocols. Protocol 30
 Hypotension / Shock History Blood loss - vaginal or gastrointestinal bleeding, AAA, ectopic Fluid loss - vomiting, diarrhea, fever nfection Cardiac ischemia (M, CHF) Medications Allergic reaction regnancy
Hypotension / Shock History Blood loss - vaginal or gastrointestinal bleeding, AAA, ectopic Fluid loss - vomiting, diarrhea, fever nfection Cardiac ischemia (M, CHF) Medications Allergic reaction regnancy
In-hospital Care of the Post-Cardiac Arrest Patient. David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine
 In-hospital Care of the Post-Cardiac Arrest Patient David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine Disclosures I have no financial interest, arrangement,
In-hospital Care of the Post-Cardiac Arrest Patient David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine Disclosures I have no financial interest, arrangement,
Toxins and Environmental: HEAT- and COLD-RELATED EMERGENCIES. Accidental Hypothermia/Cold Exposure
 Toxins and Environmental: HEAT- and COLD-RELATED EMERGENCIES Accidental Hypothermia/Cold Exposure Goal: To aid EMS Providers in: the recognition and treatment of systemic effects of accidental hypothermia
Toxins and Environmental: HEAT- and COLD-RELATED EMERGENCIES Accidental Hypothermia/Cold Exposure Goal: To aid EMS Providers in: the recognition and treatment of systemic effects of accidental hypothermia
Head Trauma Protocol
 Injuries to the head may cause underlying brain tissue damage. Increased intracranial pressure from bleeding or swelling tissue is a common threat after head trauma. Common signs and symptoms of increased
Injuries to the head may cause underlying brain tissue damage. Increased intracranial pressure from bleeding or swelling tissue is a common threat after head trauma. Common signs and symptoms of increased
DRAFT. Refresher Course EMT Paramedic to Paramedic Outline.pdf
 Paramedic Refresher + Transition Course Monday Thursday Lecture (32 hours) (18.1 hours of the 32 are considered Transitional) Friday ACLS Refresher (8 hours) Saturday PALS Refresher (8 hours) TOTAL = 48
Paramedic Refresher + Transition Course Monday Thursday Lecture (32 hours) (18.1 hours of the 32 are considered Transitional) Friday ACLS Refresher (8 hours) Saturday PALS Refresher (8 hours) TOTAL = 48
Basic Assessment and Treatment of Trauma
 Basic Assessment and Treatment of Trauma Final Exam Version 1 1. In which of the following scenarios would the potential for serious injury or death be the GREATEST? A. 77-kg (170-lb) man who falls 1.2
Basic Assessment and Treatment of Trauma Final Exam Version 1 1. In which of the following scenarios would the potential for serious injury or death be the GREATEST? A. 77-kg (170-lb) man who falls 1.2
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
SAN LUIS OBISPO COUNTY EMERGENCY MEDICAL SERVICES AGENCY PREHOSPITAL POLICY
 SAN LUIS OBISPO COUNTY EMERGENCY MEDICAL SERVICES AGENCY PREHOSPITAL POLICY Policy Reference No: 153 [01/08/2013] Formerly Policy No: 201.3 Effective Date: 11/01/2012 Review Date: 03/01/2014 TRAUMA PATIENT
SAN LUIS OBISPO COUNTY EMERGENCY MEDICAL SERVICES AGENCY PREHOSPITAL POLICY Policy Reference No: 153 [01/08/2013] Formerly Policy No: 201.3 Effective Date: 11/01/2012 Review Date: 03/01/2014 TRAUMA PATIENT
ITLS Pediatric Provider Course Basic Pre-Test
 ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Advanced Pre-Test
 ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
Mesa County EMS Protocol Test 2016
 Mesa County EMS Protocol Test 2016 1. Which of the following is incorrect? a. Each EMS and Fire agency should have protocols in place for evaluation of personnel involved in fire suppression operations
Mesa County EMS Protocol Test 2016 1. Which of the following is incorrect? a. Each EMS and Fire agency should have protocols in place for evaluation of personnel involved in fire suppression operations
Manual Defibrillation. CPR AGE: 18 years LOA: Altered HR: N/A RR: N/A SBP: N/A Other: N/A
 ROC AMIODARONE, LIDOCAINE OR PLACEBO FOR OUT OF HOSPITAL CARDIAC ARREST DUE TO VENTRICULAR FIBRILLATION OR TACHYCARDIA (ALPS) STUDY: MEDICAL CARDIAC ARREST MEDICAL DIRECTIVE An Advanced Care Paramedic
ROC AMIODARONE, LIDOCAINE OR PLACEBO FOR OUT OF HOSPITAL CARDIAC ARREST DUE TO VENTRICULAR FIBRILLATION OR TACHYCARDIA (ALPS) STUDY: MEDICAL CARDIAC ARREST MEDICAL DIRECTIVE An Advanced Care Paramedic
Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies)
") SLO County Emergency Medical Services Agency Bulletin 2012-09 PLEASE POST Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies) July
SLO County Emergency Medical Services Agency Bulletin 2012-09 PLEASE POST Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies) July
EMS System for Metropolitan Oklahoma City and Tulsa 2019 Medical Control Board Treatment Protocols
 EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
PEDIATRIC TREATMENT GUIDELINES - CARDIAC VENTRICULAR FIBRILLATION - PULSELESS VENTRICULAR TACHYCARDIA (SJ-PO1) effective 05/01/02
 effective 05/01/02") PEDIATRIC TREATMENT GUIDELINES - CARDIAC VENTRICULAR FIBRILLATION - PULSELESS VENTRICULAR TACHYCARDIA (SJ-PO1) effective 05/01/02 Revision #5 04/19/02 Identify Dysrhythmia DEFIBRILLATE: 2 J/kg, 4 J/kg,
PEDIATRIC TREATMENT GUIDELINES - CARDIAC VENTRICULAR FIBRILLATION - PULSELESS VENTRICULAR TACHYCARDIA (SJ-PO1) effective 05/01/02 Revision #5 04/19/02 Identify Dysrhythmia DEFIBRILLATE: 2 J/kg, 4 J/kg,
SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC
 SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC The following is a summary of the key issues and changes in the AHA 2010 Guidelines for Cardiopulmonary Resuscitation (CPR) and Emergency Cardiac
SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC The following is a summary of the key issues and changes in the AHA 2010 Guidelines for Cardiopulmonary Resuscitation (CPR) and Emergency Cardiac
Patient Assessment From Brady s First Responder (8th Edition) 83 Questions
 83 Questions") Patient Assessment From Brady s First Responder (8th Edition) 83 Questions 1. Which question is important if your patient may be a candidate for surgery? p. 183 *A.) When did you last eat? B.) What is
Patient Assessment From Brady s First Responder (8th Edition) 83 Questions 1. Which question is important if your patient may be a candidate for surgery? p. 183 *A.) When did you last eat? B.) What is
Consider Treatable Underlying Causes Early
 Page 1 of 8 Cardiac Arrest Timeout Checklist Assign roles for Pit Crew CPR o Compressors x 2 o Airway o Lead responsible for coordinating team, making decisions o Medications Continuous compressions at
Page 1 of 8 Cardiac Arrest Timeout Checklist Assign roles for Pit Crew CPR o Compressors x 2 o Airway o Lead responsible for coordinating team, making decisions o Medications Continuous compressions at
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
April 2011 CE. Site code # E The Patient With Heart Failure; CPAP as an Intervention
 April 2011 CE Site code # 107200E-1211 The Patient With Heart Failure; CPAP as an Intervention Prepared by: Lt. Bill Hoover, Medical Officer Wauconda Fire District Reviewed/revised by Sharon Hopkins, RN,
April 2011 CE Site code # 107200E-1211 The Patient With Heart Failure; CPAP as an Intervention Prepared by: Lt. Bill Hoover, Medical Officer Wauconda Fire District Reviewed/revised by Sharon Hopkins, RN,
Regionalization of Post-Cardiac Arrest Care
 Regionalization of Post-Cardiac Arrest Care David A. Pearson, MD, FACEP, FAAEM Department of Emergency Medicine Disclosures I have no financial interest, arrangement, or affiliations and no commercial
Regionalization of Post-Cardiac Arrest Care David A. Pearson, MD, FACEP, FAAEM Department of Emergency Medicine Disclosures I have no financial interest, arrangement, or affiliations and no commercial
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
INTERNATIONAL TRAUMA LIFE SUPPORT
 INTERNATIONAL TRAUMA LIFE SUPPORT NC ITLS Rev. 2/18 STUDENT GUIDE TO INTERNATIONAL TRAUMA LIFE SUPPORT What to wear ITLS is a practical course that stresses hands-on teaching. You should wear comfortable
INTERNATIONAL TRAUMA LIFE SUPPORT NC ITLS Rev. 2/18 STUDENT GUIDE TO INTERNATIONAL TRAUMA LIFE SUPPORT What to wear ITLS is a practical course that stresses hands-on teaching. You should wear comfortable
EMS System for Metropolitan Oklahoma City and Tulsa 2018 Medical Control Board Treatment Protocols
 EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
INDUCED HYPOTHERMIA. F. Ben Housel, M.D.
 INDUCED HYPOTHERMIA F. Ben Housel, M.D. Historical Use of Induced Hypothermia 1950 s - Moderate hypothermia (30-32º C) in open heart surgery to protect brain against global ischemia 1960-1980 s - Use of
INDUCED HYPOTHERMIA F. Ben Housel, M.D. Historical Use of Induced Hypothermia 1950 s - Moderate hypothermia (30-32º C) in open heart surgery to protect brain against global ischemia 1960-1980 s - Use of
Face and Throat Injuries. Chapter 26
 Face and Throat Injuries Chapter 26 Anatomy of the Head Landmarks of the Neck Injuries to the Face Injuries around the face can lead to upper airway obstructions. Bleeding from the face can be profuse.
Face and Throat Injuries Chapter 26 Anatomy of the Head Landmarks of the Neck Injuries to the Face Injuries around the face can lead to upper airway obstructions. Bleeding from the face can be profuse.
August 2012 CE. Site code # E Reading the Scene
 August 2012 CE Site code # 107200E-1212 Reading the Scene Prepared by Sharon Hopkins, RN, BSN, EMT-P To view on the Advocate Condell website visit: www.advocatehealth.com/condell/body.cfm?id=422 Date of
August 2012 CE Site code # 107200E-1212 Reading the Scene Prepared by Sharon Hopkins, RN, BSN, EMT-P To view on the Advocate Condell website visit: www.advocatehealth.com/condell/body.cfm?id=422 Date of
Restore adequate respiratory and circulatory conditions. Reduce pain
 Pre-hospital management of the trauma patient is best performed by an integrated team focused on minimizing the time from injury to definitive care at an appropriate trauma center. Dispatchers, first responders,
Pre-hospital management of the trauma patient is best performed by an integrated team focused on minimizing the time from injury to definitive care at an appropriate trauma center. Dispatchers, first responders,
VAO BASIC SUPPORT CLINICAL APPROACH TO THE PATIENT HANDOUT
 CLINICAL APPROACH TO THE PATIENT HANDOUT 1 I am the most important part of patient care. How can you expect to treat a patient appropriately if you don t follow through on basic primary care? Remember:
CLINICAL APPROACH TO THE PATIENT HANDOUT 1 I am the most important part of patient care. How can you expect to treat a patient appropriately if you don t follow through on basic primary care? Remember:
Outline. Common causes of loss of consciousness. How to assess loss of consciousness. Emergency management of a patient with loss of consciousness.
 Outline Common causes of loss of consciousness. How to assess loss of consciousness. Emergency management of a patient with loss of consciousness. Common causes of loss of consciousness Alterations in
Outline Common causes of loss of consciousness. How to assess loss of consciousness. Emergency management of a patient with loss of consciousness. Common causes of loss of consciousness Alterations in
DYSRHYTHMIAS. D. Assess whether or not it is the arrhythmia that is making the patient unstable or symptomatic
 DYSRHYTHMIAS GENERAL CONSIDERATIONS A. The 2015 American Heart Association Guidelines were referred to for this protocol development. Evidence-based science was implemented in those areas where the AHA
DYSRHYTHMIAS GENERAL CONSIDERATIONS A. The 2015 American Heart Association Guidelines were referred to for this protocol development. Evidence-based science was implemented in those areas where the AHA
No conflicts of interest
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
ATLS: Initial Assessment and Management. SAUSHEC Medical Student Lecture Series
 ATLS: Initial Assessment and Management SAUSHEC Medical Student Lecture Series Objectives Identify sequence of priorities in assessing the multiply injured patient Apply principles outlined in primary
ATLS: Initial Assessment and Management SAUSHEC Medical Student Lecture Series Objectives Identify sequence of priorities in assessing the multiply injured patient Apply principles outlined in primary
European Resuscitation Council
 European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D.
 1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D. Sacral-coccygeal 2. A 36-year-old male sustains blunt force thoracic
1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D. Sacral-coccygeal 2. A 36-year-old male sustains blunt force thoracic
Capnography 101. James A Temple BA, NRP, CCP
 Capnography 101 James A Temple BA, NRP, CCP Expected Outcomes 1. Gain a working knowledge of the physiology and science behind End-Tidal CO2. 2.Relate End-Tidal CO2 to ventilation, perfusion, and metabolism.
Capnography 101 James A Temple BA, NRP, CCP Expected Outcomes 1. Gain a working knowledge of the physiology and science behind End-Tidal CO2. 2.Relate End-Tidal CO2 to ventilation, perfusion, and metabolism.
McHenry Western Lake County EMS System CE for Paramedics, EMT-B and PHRN s Sepsis Patients. November/December 2017
 McHenry Western Lake County EMS System CE for Paramedics, EMT-B and PHRN s Sepsis Patients November/December 2017 This month we are going to take a look at the patient with Sepsis. Webster s defines septic
McHenry Western Lake County EMS System CE for Paramedics, EMT-B and PHRN s Sepsis Patients November/December 2017 This month we are going to take a look at the patient with Sepsis. Webster s defines septic
Chapter 13. Objectives. Objectives 01/09/2013. Patient Assessment
 Chapter 13 Patient Assessment Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms
Chapter 13 Patient Assessment Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms
McHenry Western Lake County EMS System Optional CE for EMT-B, Paramedics and PHRN s Bradycardia and Treatments Optional #7 2018
 McHenry Western Lake County EMS System Optional CE for EMT-B, Paramedics and PHRN s Bradycardia and Treatments Optional #7 2018 This month we will be looking at a specific ECG Rhythm and its treatments
McHenry Western Lake County EMS System Optional CE for EMT-B, Paramedics and PHRN s Bradycardia and Treatments Optional #7 2018 This month we will be looking at a specific ECG Rhythm and its treatments
BLS Practical Skills Examination
 New York State Department of Health BLS Practical Skills Examination ertified First Responder and Emergency Medical Technician 2017 REQUIRED TESTING S EMT - The following skills are identified as being
New York State Department of Health BLS Practical Skills Examination ertified First Responder and Emergency Medical Technician 2017 REQUIRED TESTING S EMT - The following skills are identified as being
B. high blood pressure. D. hearing impairment. 2. Of the following, the LEAST likely reason for an EMS unit to be called
 CHAPTER 36 Geriatrics HANDOUT 36-2: Evaluating Content Mastery Student s Name EVALUATION CHAPTER 36 QUIZ Write the letter of the best answer in the space provided. 1. Among patients over age 65, almost
CHAPTER 36 Geriatrics HANDOUT 36-2: Evaluating Content Mastery Student s Name EVALUATION CHAPTER 36 QUIZ Write the letter of the best answer in the space provided. 1. Among patients over age 65, almost
Old protocol is top bullet and italicized. Revised protocol is subsequent bullets and color coded:
 Old protocol is top bullet and italicized Revised protocol is subsequent bullets and color coded: RED is a State Change Blue is unique to Suffolk County VI. If patient has not taken aspirin and has no
Old protocol is top bullet and italicized Revised protocol is subsequent bullets and color coded: RED is a State Change Blue is unique to Suffolk County VI. If patient has not taken aspirin and has no
CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS
 CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS PRACTICAL STATIONS CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS 1. CARDIAC ARREST MANAGEMENT 2. AIRWAY & RESPIRATORY MANAGEMENT 3. SPINAL IMMOBILIZATION
CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS PRACTICAL STATIONS CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS 1. CARDIAC ARREST MANAGEMENT 2. AIRWAY & RESPIRATORY MANAGEMENT 3. SPINAL IMMOBILIZATION
CrackCast Episode 8 Brain Resuscitation
 CrackCast Episode 8 Brain Resuscitation Episode Overview: 1) Describe 6 therapeutic interventions for the post-arrest brain 2) List 5 techniques for initiating therapeutic hypothermia 3) List 4 mechanisms
CrackCast Episode 8 Brain Resuscitation Episode Overview: 1) Describe 6 therapeutic interventions for the post-arrest brain 2) List 5 techniques for initiating therapeutic hypothermia 3) List 4 mechanisms
ETCO2 MONITORING NON-INTUBATED PATIENTS
 Although the standard of care in ETC02 is well established for intubated patients, there has been little emphasis on the use of capnography in nonintubated patients till now. In addition to confirming
Although the standard of care in ETC02 is well established for intubated patients, there has been little emphasis on the use of capnography in nonintubated patients till now. In addition to confirming
Operation Stroke. How to Reduce the Risk of Stroke Complications
 Operation Stroke How to Reduce the Risk of Stroke Complications Objectives Focus on Acute Stroke as an active disease Discuss the most common stroke complications Describe how first 72 hours sets the stage
Operation Stroke How to Reduce the Risk of Stroke Complications Objectives Focus on Acute Stroke as an active disease Discuss the most common stroke complications Describe how first 72 hours sets the stage
Yolo County Health & Human Services Agency
 Yolo County Health & Human Services Agency Kristin Weivoda EMS Administrator John S. Rose, MD, FACEP Medical Director DATE: December 28, 2017 TO: Yolo County Providers and Agencies FROM: Yolo County EMS
Yolo County Health & Human Services Agency Kristin Weivoda EMS Administrator John S. Rose, MD, FACEP Medical Director DATE: December 28, 2017 TO: Yolo County Providers and Agencies FROM: Yolo County EMS
Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms. Introduction to the Algorithms
 Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Introduction to the Algorithms Cardiac Arrest Algorithms Prehospital Medication Profiles Perspective regarding the EMT- Intermediate
Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Introduction to the Algorithms Cardiac Arrest Algorithms Prehospital Medication Profiles Perspective regarding the EMT- Intermediate
Lesson 4-3: Cardiac Emergencies. CARDIAC EMERGENCIES Angina, AMI, CHF and AED
 Lesson 4-3: Cardiac Emergencies CARDIAC EMERGENCIES Angina, AMI, CHF and AED THREE FAMILIAR CARDIAC CONDITIONS Angina Pectoris Acute Myocardial Infarction Congestive Heart Failure ANGINA PECTORIS Chest
Lesson 4-3: Cardiac Emergencies CARDIAC EMERGENCIES Angina, AMI, CHF and AED THREE FAMILIAR CARDIAC CONDITIONS Angina Pectoris Acute Myocardial Infarction Congestive Heart Failure ANGINA PECTORIS Chest
Chapter 11. Objectives. Objectives 01/09/2013. Baseline Vital Signs, Monitoring Devices, and History Taking
 Chapter 11 Baseline Vital Signs, Monitoring Devices, and History Taking Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights
Chapter 11 Baseline Vital Signs, Monitoring Devices, and History Taking Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights
QI. Read the following questions and choose the most correct answer (20 Marks):
:") Question One: QI. Read the following questions and choose the most correct answer (20 Marks): 1- Some people are very allergic to some drugs like penicillin. This condition is called: a) Septic shock.
Question One: QI. Read the following questions and choose the most correct answer (20 Marks): 1- Some people are very allergic to some drugs like penicillin. This condition is called: a) Septic shock.
Medical First Responder Program Protocols
 Medical Scene Safety Protocol Verify Scene Safety with Police or Dispatch UNKWN Scene Safe? Enter Continue to Appropriate Protocol Possible to Make Safe Make Safe Then Continue Exit Area and Stage Outside
Medical Scene Safety Protocol Verify Scene Safety with Police or Dispatch UNKWN Scene Safe? Enter Continue to Appropriate Protocol Possible to Make Safe Make Safe Then Continue Exit Area and Stage Outside
table of contents pediatric treatment guidelines
 table of contents pediatric treatment guidelines P1 PEDIATRIC PATIENT CARE...70 P2 APPARENT LIFE-THREATENING EVENT (ALTE)...71 P3 CARDIAC ARREST INITIAL CARE AND CPR...72 73 P4 NEONATAL CARE AND RESUSCITATION...74
table of contents pediatric treatment guidelines P1 PEDIATRIC PATIENT CARE...70 P2 APPARENT LIFE-THREATENING EVENT (ALTE)...71 P3 CARDIAC ARREST INITIAL CARE AND CPR...72 73 P4 NEONATAL CARE AND RESUSCITATION...74
SIERRA-SACRAMENTO VALLEY EMS AGENCY PROGRAM POLICY
 SIERRA-SACRAMENTO VALLEY EMS AGENCY PROGRAM POLICY PURPOSE: To identify those patients who are at greatest risk for severe injury and determine the most appropriate facility to transport persons with different
SIERRA-SACRAMENTO VALLEY EMS AGENCY PROGRAM POLICY PURPOSE: To identify those patients who are at greatest risk for severe injury and determine the most appropriate facility to transport persons with different
INFORMAL COPY WHEN PRINTED
 Doc Control Ref: TEM-003 Version 2.0 (Admin use only) Version no: (Admin use only) Effective Date: (Admin use only) 1. Principle Post-return of spontaneous circulation (ROSC) management is an important
Doc Control Ref: TEM-003 Version 2.0 (Admin use only) Version no: (Admin use only) Effective Date: (Admin use only) 1. Principle Post-return of spontaneous circulation (ROSC) management is an important
Pediatric Cardiac Arrest General
 Date: November 15, 2012 Page 1 of 5 Pediatric Cardiac Arrest General This protocol should be followed for all pediatric cardiac arrests. If an arrest is of a known traumatic origin refer to the Dead on
Date: November 15, 2012 Page 1 of 5 Pediatric Cardiac Arrest General This protocol should be followed for all pediatric cardiac arrests. If an arrest is of a known traumatic origin refer to the Dead on
They aren t the same thing. Daniel Dunham
 They aren t the same thing Daniel Dunham Capnometry Displays the value (as a number) of the partial pressure of CO2 Capnography Waveform capnography shows (as a wave) the change in CO2 over time Both are
They aren t the same thing Daniel Dunham Capnometry Displays the value (as a number) of the partial pressure of CO2 Capnography Waveform capnography shows (as a wave) the change in CO2 over time Both are
PARAMEDIC RECERT PROPOSAL (NCCP standards)
") PARAMEDIC RECERT PROPOSAL (NCCP standards) Module I TOPIC Airway, Respiration, Ventilation and Neurotological Management Ventilation ETCO2 Automated Transport Ventilators Oxygenation CPAP Capnography Neurological
PARAMEDIC RECERT PROPOSAL (NCCP standards) Module I TOPIC Airway, Respiration, Ventilation and Neurotological Management Ventilation ETCO2 Automated Transport Ventilators Oxygenation CPAP Capnography Neurological
Future of Cardiac Arrest Management for Paramedics
 Future of Cardiac Arrest Management for Paramedics EMS TODAY 2013 Mark Whitbread Consultant Paramedic London Ambulance Service London Ambulance Service NHS Trust 620 sq miles 8.2 million population 2011/12
Future of Cardiac Arrest Management for Paramedics EMS TODAY 2013 Mark Whitbread Consultant Paramedic London Ambulance Service London Ambulance Service NHS Trust 620 sq miles 8.2 million population 2011/12
History Data Panel. Case 030 Preg Trauma. Presenting Complaint Altered mental status s/p MVC. Person Giving Information EMS
 History Data Panel Presenting Complaint Altered mental status s/p MVC Person Giving Information EMS History of Present Illness 28 year old woman, 35 weeks pregnant per report of her husband the passenger.
History Data Panel Presenting Complaint Altered mental status s/p MVC Person Giving Information EMS History of Present Illness 28 year old woman, 35 weeks pregnant per report of her husband the passenger.
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours
 Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
LOSS OF CONSCIOUSNESS & ASSESSMENT. Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT
 LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
Capnography: The Most Vital Sign
 Capnography: The Most Vital Sign Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com CO
Capnography: The Most Vital Sign Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com CO