The Straw that Broke the Child s Back SPORTS Symposium E. John Stanley PT,SCS
|
|
|
- Deirdre Gordon
- 6 years ago
- Views:
Transcription
1 The Straw that Broke the Child s Back 2017 SPORTS Symposium E. John Stanley PT,SCS
2 Learning Objectives: 1.Identify 3 characteristics of kids at risk for back injuries. 2.Describe the impact of flexibility, strength, and neuromuscular control in back pain. 3.Outline a basic program to eliminate back pain in children and adolescents.
3 Nothing to Disclose Disclosures:






4 My Child Has Back Pain

5 My Child Has Back Pain Soft Tissue Injuries Bone related injuries Disc injury Other Pathologies




6 Back Pain: Where, When and Why

7 Back Pain: Where, When and Why Is it centrally located or peripheral? Does it cover more than one segment or is it point specific? Does it move/travel/ radiate anywhere?

8 Back Pain: Where, When and Why When does the back hurt? At rest? During activities? After activities? Only during homework?



9 Back Pain: Where, When and Why

10 Back Pain: Where, When and Why



11 X-rays, CTs and MRI s Oh my!






12 Poking and Prodding
13 Treatment options: Duct Tape & Hammers The role of the physical therapy is one of guided education and not one of fixing Educate to empower the patient.

14 Treatment options: Duct Tape & Hammers Typical treatment begins with by addressing any specific muscular spasms and tightness.

15 Treatment options: Duct Tape Progress with mobilization of hypomobile segments and alignment of any malpositioned segments. & Hammers
16 Treatment options: Duct Tape & Hammers Stabilization techniques for both holding as well as control
17 Treatment options: Duct Tape & Hammers Simultaneous strengthening of support musculature and addressing any particular muscular imbalance(s).

18 Treatment options: Duct Tape & Hammers Reintroduction of sport-specific or activity specific demands

19 Enough is Enough Or is it? Increased irritation or inflammation may require episodic bracing to allow for healing

20 Enough is Enough Or is it? Multi-disciplinary approach

21 Enough is Enough Or is it? If location, nature, and/or intensity of pain change significantly then there is increased concern that you are no longer treating the original source of the pain. More diagnostics may be warranted.
22 Case Study #1: Spondylolis 14yo female who was playing soccer and attempted a header when another player collided with her in May. She had pain but was able to finish the game. She is a year-round soccer player but will also participate in volleyball, cross-country and track. Parents and coach decide to rest her 6 weeks after which she is essentially pain free. She attempts to participate in a soccer camp but begins having significant pain. X-rays in late July were negative but bone scan in early August showed stress reaction. She is placed in TLSO at that time full time wearing schedule. She wears brace for 1month and then is referred to therapy. Presents for evaluation early October and has been wearing brace and full activity restrictions since since July.
23 Case Study #1: Spondylolis Exam Findings: Noted at evaluation are continued pain 3-4/10 and which increases as she moves into hip extension. She is able to demonstrate standing active motions without pain (extension is not tested however). Limitations in both lumbar and thoracic segment mobility - hinge point noted at L2-3 segments with lateral flexion. Limitations in lower extremity flexibility noted in bilateral hip flexors, quadriceps, hamstrings Weakness noted in core musculature and proximal hip musculature especially for hip abduction and extension.
24 Case Study #1: Spondylolis Treatment: Consists of 21 visits over 12 weeks. She is pain free with therapy and home exercise program in addition to continued brace wear at reduced schedule by 4 weeks early October She is able to begin jogging out of the brace by early November physician gave her the option to discharge from therapy but patient/family would like to continue. She is self-progressing running distance and speed and performing plyometrics in therapy by early December and is transitioned to consult model of care. At time of discharge she is noted to continue to have hypomobility in the lumbar spine that limits forward flexion hamstring tightness has resolved. She is able to fully return to her prior level of activities. However she does sustain additional injuries including re-injury of L5 facet.

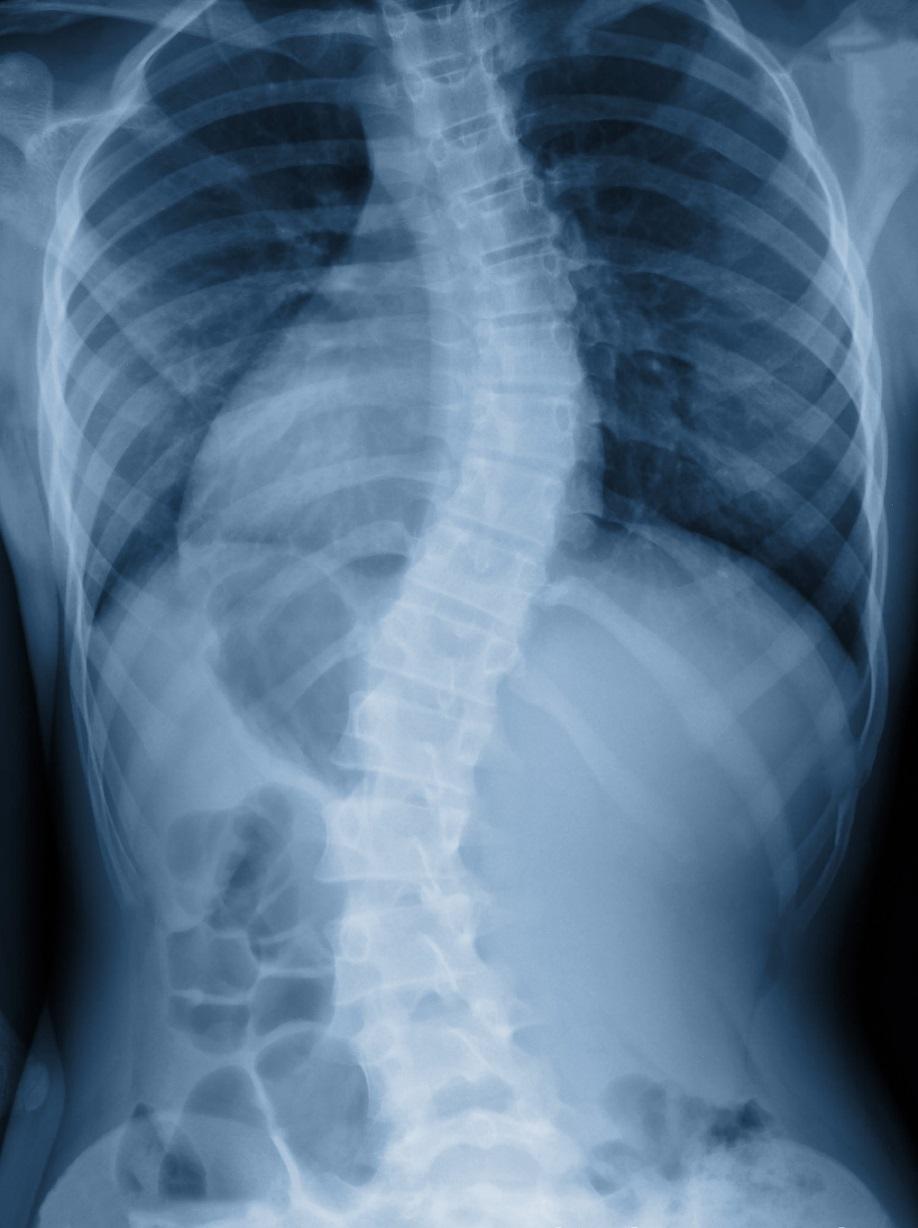
25 Case study #2: Segmental Malalignment 13yo male diagnosed with scoliosis. X-rays show 15deg right convex curve from T6-T10. Presents to therapy with right periscapular pain rated baseline of 3/10 and worst of 6/10.
26 Case study #2: Segmental Malalignment 13yo male diagnosed with scoliosis. X-rays show 15deg right convex curve from T6-T10. Presents to therapy with right periscapular pain rated baseline of 3/10 and worst of 6/10. Patient goal is to return to high level of hiphop dancing specifically to be able to perform head spins without pain.
27 Case study #2: Segmental Malalignment Exam findings: Noted left body rotation of T9 segment. Paraspinal spasms and pain to palpation along the right medial scapular border. Trigger points throughout bilateral upper traps. Poor scapular control with overutilization of upper trapezius to initiate UE motion. Flexion pattern for lumbar stabilization Vertical compression test 2/4


28 Case study #2: Segmental Malalignment Treatment: Attends 6 weeks of PT 1x/week Initially given HEP for basic supine core activation, general spine and lower extremity stretching. Initial treatments addressed scapular mobility, periscapular spasms and neuromuscular control of core and scapulae moving from supine and prone positions to seated. Updated HEP for advancement of core and scapular strengthening after 2 weeks

29 Case study #2: Segmental Treatment: Cont d Malalignment Week 3 he begins a progressive return to dance. Week 4 no longer having shoulder / thoracic pain but now with neck pain. Noted rotation in T1 segment which is addressed using muscle energy techniques with good resolution. Continues to improve control of core and scapular control as we increase challenges in terms of resistance, weight bearing and change of position (inverted). Able to return fully to all dance moves at week 6 and transitioned to consult model of care.
Evaluating the Athlete Questionnaire
 Evaluating the Athlete Questionnaire Prior to developing the strength and conditioning training plan the coach should first evaluate factors from the athlete s questionnaire that may impact the strength
Evaluating the Athlete Questionnaire Prior to developing the strength and conditioning training plan the coach should first evaluate factors from the athlete s questionnaire that may impact the strength
Case Studies: Low Back Pain in the Athlete. Jim Messerly DO
 Case Studies: Low Back Pain in the Athlete Jim Messerly DO Nothing to disclose Case #1 History 15 y/o male presents for evaluation of his low back pain. His pain has been present for several months. The
Case Studies: Low Back Pain in the Athlete Jim Messerly DO Nothing to disclose Case #1 History 15 y/o male presents for evaluation of his low back pain. His pain has been present for several months. The
ACE s Essentials of Exercise Science for Fitness Professionals TRUNK
 ACE s Essentials of Exercise Science for Fitness Professionals TRUNK Posture and Balance Posture refers to the biomechanical alignment of the individual body parts and the orientation of the body to the
ACE s Essentials of Exercise Science for Fitness Professionals TRUNK Posture and Balance Posture refers to the biomechanical alignment of the individual body parts and the orientation of the body to the
Sterile gauze used at incision site. Check brace for rubbing or irritation. Compression garment at elbow to be used with physician s authorization
 ULNAR COLLATERAL LIGAMENT RECONSTRUCTION GUIDELINE Functional Outcome Measure KJOC (Appendix 1) should be completed at initial evaluation and at all identified times through guideline, Phase 1 Immediate
ULNAR COLLATERAL LIGAMENT RECONSTRUCTION GUIDELINE Functional Outcome Measure KJOC (Appendix 1) should be completed at initial evaluation and at all identified times through guideline, Phase 1 Immediate
9180 KATY FREEWAY, STE. 200 (713)
") OSTEOCHONDRAL AUTOGRAFT TRANSPLANTATION Patella/Trochlea Rehabilitation Guidelines PHASE I - PROTECTION PHASE (WEEKS 0-6) Goals: - Protection of healing tissue from load and shear forces - Decrease pain
OSTEOCHONDRAL AUTOGRAFT TRANSPLANTATION Patella/Trochlea Rehabilitation Guidelines PHASE I - PROTECTION PHASE (WEEKS 0-6) Goals: - Protection of healing tissue from load and shear forces - Decrease pain
The Athlete s Lumbar Spine: Current Concepts
 The Athlete s Lumbar Spine: Current Concepts Content / Objectives Anatomy Common injuries Treatment and prevention Pablo Vazquez Seoane, M.D. 44 th Annual Sports Medicine Symposium January 19 21, 2017
The Athlete s Lumbar Spine: Current Concepts Content / Objectives Anatomy Common injuries Treatment and prevention Pablo Vazquez Seoane, M.D. 44 th Annual Sports Medicine Symposium January 19 21, 2017
Pilates for Pole Athletes
 Pilates for Pole Athletes Maria E. Moore July 2, 2018 Body Arts and Science International Comprehensive Teacher Training Program, 2017 Breathe Pilates & Fitness Harrisonburg, VA Abstract Pole dancing has
Pilates for Pole Athletes Maria E. Moore July 2, 2018 Body Arts and Science International Comprehensive Teacher Training Program, 2017 Breathe Pilates & Fitness Harrisonburg, VA Abstract Pole dancing has
Medial Patellofemoral Ligament Reconstruction Guidelines Brian Grawe Protocol
 Medial Patellofemoral Ligament Reconstruction Guidelines Brian Grawe Protocol Progression is based on healing constraints, functional progression specific to the patient. Phases and time frames are designed
Medial Patellofemoral Ligament Reconstruction Guidelines Brian Grawe Protocol Progression is based on healing constraints, functional progression specific to the patient. Phases and time frames are designed
9180 KATY FREEWAY, STE. 200 (713)
") AUTOLOGOUS CHONDROCYTE IMPLANTATION Femoral Condyle Rehabilitation Guidelines PHASE I - PROTECTION PHASE (WEEKS 0-6) Goals: - Protect healing tissue from load and shear forces - Decrease pain and effusion
AUTOLOGOUS CHONDROCYTE IMPLANTATION Femoral Condyle Rehabilitation Guidelines PHASE I - PROTECTION PHASE (WEEKS 0-6) Goals: - Protect healing tissue from load and shear forces - Decrease pain and effusion
Bone-Patellar tendon-bone Autograft ACL Recon. Date of Surgery: Patient Name:
 Dx: o Right o Left Bone-Patellar tendon-bone Autograft ACL Recon Date of Surgery: Patient Name: PT/OT: Please evaluate and treat. Follow attached protocol. 2-3 x per week x 6 weeks. Signature/Date: GENERAL
Dx: o Right o Left Bone-Patellar tendon-bone Autograft ACL Recon Date of Surgery: Patient Name: PT/OT: Please evaluate and treat. Follow attached protocol. 2-3 x per week x 6 weeks. Signature/Date: GENERAL
ATHLETIC CONDITIONING ON THE ARC BARREL
 ATHLETIC CONDITIONING ON THE ARC BARREL page 1 INTRODUCTION The STOTT PILATES Athletic Conditioning stream serves as a bridge between STOTT PILATES standard repertoire and the CORE Athletic Conditioning
ATHLETIC CONDITIONING ON THE ARC BARREL page 1 INTRODUCTION The STOTT PILATES Athletic Conditioning stream serves as a bridge between STOTT PILATES standard repertoire and the CORE Athletic Conditioning
Hip and Spine of the Athlete
 Hip and Spine of the Athlete Kyle Turner, ATC Assistant Athletic Trainer Kansas City Royals Sean Bardenett, DPT Manual Therapist Kansas City Royals Talk to DCs about spine.. Outline Regional Interdependence
Hip and Spine of the Athlete Kyle Turner, ATC Assistant Athletic Trainer Kansas City Royals Sean Bardenett, DPT Manual Therapist Kansas City Royals Talk to DCs about spine.. Outline Regional Interdependence
IFAST Assessment. Name: Date: Sport: Review Health Risk Assessment on initial consult form. List Client Goals (what brings you here?
 IFAST Assessment Name: Date: Sport: Review Health Risk Assessment on initial consult form List Client Goals (what brings you here?) Cardiovascular Measurements Blood Pressure Resting Heart Rate Body Composition
IFAST Assessment Name: Date: Sport: Review Health Risk Assessment on initial consult form List Client Goals (what brings you here?) Cardiovascular Measurements Blood Pressure Resting Heart Rate Body Composition
Sports Rehabilitation & Performance Center Medial Patellofemoral Ligament Reconstruction Guidelines * Follow physician s modifications as prescribed
 The following MPFL guidelines were developed by the Sports Rehabilitation and Performance Center team at Hospital for Special Surgery. Progression is based on healing constraints, functional progression
The following MPFL guidelines were developed by the Sports Rehabilitation and Performance Center team at Hospital for Special Surgery. Progression is based on healing constraints, functional progression
Paradigm Shift. Biomedical Model. Regional Interdependence Model. Evidence to Support R-I Exam
 A Clinical Approach to Assessing and Addressing Movement Pattern Dysfunction Models of Adverse Health Regional Interdependence Evidence to Support R-I Systematic Assessment Case Studies using System Implementation
A Clinical Approach to Assessing and Addressing Movement Pattern Dysfunction Models of Adverse Health Regional Interdependence Evidence to Support R-I Systematic Assessment Case Studies using System Implementation
S p o r t s & O r t h o p a e d i c S p e c i a l i s t s A n t e r i o r I n s t a b i l i t y P r o t o c o l
 S p o r t s & O r t h o p a e d i c S p e c i a l i s t s This protocol provides appropriate guidelines for the rehabilitation of patients with anterior instability. The protocol draws evidence from the
S p o r t s & O r t h o p a e d i c S p e c i a l i s t s This protocol provides appropriate guidelines for the rehabilitation of patients with anterior instability. The protocol draws evidence from the
OSTEOCHONDRAL AUTOGRAFT TRANSPLANTATION
 OSTEOCHONDRAL AUTOGRAFT TRANSPLANTATION FEMORAL CONDYLE REHABILITATION PROGRAM PHASE I - PROTECTION PHASE (WEEKS 0-6) Protection of healing tissue from load and shear forces Decrease pain and effusion
OSTEOCHONDRAL AUTOGRAFT TRANSPLANTATION FEMORAL CONDYLE REHABILITATION PROGRAM PHASE I - PROTECTION PHASE (WEEKS 0-6) Protection of healing tissue from load and shear forces Decrease pain and effusion
Mark Adickes, M.D. Orthopedics and Sports Medicine 7200 Cambridge St. #10A Houston, Texas Phone: Fax:
 Mark Adickes, M.D. Orthopedics and Sports Medicine 7200 Cambridge St. #10A Houston, Texas 77030 Phone: 713-986-6016 Fax: 713-986-5411 MENISCAL REPAIR PROTOCOL Longitudinal Meniscal Repair This rehabilitation
Mark Adickes, M.D. Orthopedics and Sports Medicine 7200 Cambridge St. #10A Houston, Texas 77030 Phone: 713-986-6016 Fax: 713-986-5411 MENISCAL REPAIR PROTOCOL Longitudinal Meniscal Repair This rehabilitation
RN(EC) ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***
 ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***") HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient - Certain conditions are more prevalent in particular age groups (Hip pain in children may refer to the knee from Legg-Calve-Perthes
HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient - Certain conditions are more prevalent in particular age groups (Hip pain in children may refer to the knee from Legg-Calve-Perthes
Secrets and Staples of Training the Athletic Shoulder
 Secrets and Staples of Training the Athletic Shoulder Eric Beard Corrective Exercise Specialist Athletic Performance Enhancement Specialist EricBeard.com AthleticShoulder.com Presentation Overview Rationale
Secrets and Staples of Training the Athletic Shoulder Eric Beard Corrective Exercise Specialist Athletic Performance Enhancement Specialist EricBeard.com AthleticShoulder.com Presentation Overview Rationale
Efficient Examination Printable Templates
 Efficient Examination Printable Templates Seated Tests and Measures Sidelying Tests and Measures -Seated posture -Strength testing (gluteus medius) -Neurological examination (SLUMP test, dermatomes, -Sacroiliac
Efficient Examination Printable Templates Seated Tests and Measures Sidelying Tests and Measures -Seated posture -Strength testing (gluteus medius) -Neurological examination (SLUMP test, dermatomes, -Sacroiliac
APPLICATION OF THE MOVEMENT SYSTEMS MODEL TO THE MANAGEMENT COMMON HIP PATHOLOGIES
 APPLICATION OF THE MOVEMENT SYSTEMS MODEL TO THE MANAGEMENT COMMON HIP PATHOLOGIES Tracy Porter, PT, DPT Des Moines University Department of Physical Therapy Objectives Review current literature related
APPLICATION OF THE MOVEMENT SYSTEMS MODEL TO THE MANAGEMENT COMMON HIP PATHOLOGIES Tracy Porter, PT, DPT Des Moines University Department of Physical Therapy Objectives Review current literature related
Lumbopelvic And Dural Tension Dysfunctions Common In Figure Skaters
 Lumbopelvic And Dural Tension Dysfunctions Common In Figure Skaters Presented by Melinda Couch, PT Several musculoskeletal patterns occuring in the pelvis and lumbar spine can be observed in figure skaters.
Lumbopelvic And Dural Tension Dysfunctions Common In Figure Skaters Presented by Melinda Couch, PT Several musculoskeletal patterns occuring in the pelvis and lumbar spine can be observed in figure skaters.
Femoral Condyle Rehabilitation Guidelines
 Femoral Condyle Rehabilitation Guidelines PHASE I - PROTECTION PHASE (WEEKS 0-6) Brace: Protect healing tissue from load and shear forces Decrease pain and effusion Restore full passive knee extension
Femoral Condyle Rehabilitation Guidelines PHASE I - PROTECTION PHASE (WEEKS 0-6) Brace: Protect healing tissue from load and shear forces Decrease pain and effusion Restore full passive knee extension
Joshua D. Stein, M.D. Trinity Clinic Orthopaedic and Sports Medicine 1327 Troup Hwy Tyler, TX (903) ARTHROSCOPIC DECOMPRESSION PROTOCOL
 ARTHROSCOPIC DECOMPRESSION PROTOCOL") Joshua D. Stein, M.D. Trinity Clinic Orthopaedic and Sports Medicine 1327 Troup Hwy Tyler, TX 75701 (903) 510-8840 ARTHROSCOPIC DECOMPRESSION PROTOCOL This rehabilitation protocol has been developed for
Joshua D. Stein, M.D. Trinity Clinic Orthopaedic and Sports Medicine 1327 Troup Hwy Tyler, TX 75701 (903) 510-8840 ARTHROSCOPIC DECOMPRESSION PROTOCOL This rehabilitation protocol has been developed for
Thoracic Spine Management. Jason Zafereo, PT, OCS, FAAOMPT
 Thoracic Spine Management Jason Zafereo, PT, OCS, FAAOMPT Clinical i l Orthopedic Rehabilitation ti Education Objectives Describe the treatment interventions used for the management of pain from contractile
Thoracic Spine Management Jason Zafereo, PT, OCS, FAAOMPT Clinical i l Orthopedic Rehabilitation ti Education Objectives Describe the treatment interventions used for the management of pain from contractile
S p o r t s & O r t h o p a e d i c S p e c i a l i s t s D R. R Y A N F A D E R
 S p o r t s & O r t h o p a e d i c S p e c i a l i s t s D R. R Y A N F A D E R H I P A R T H R O S C O P Y W I T H L A B R A L R E P A I R P R O T O C O L This protocol provides appropriate guidelines
S p o r t s & O r t h o p a e d i c S p e c i a l i s t s D R. R Y A N F A D E R H I P A R T H R O S C O P Y W I T H L A B R A L R E P A I R P R O T O C O L This protocol provides appropriate guidelines
APPENDIX: The Houston Astros Stretching Program
 Vol. 35, No. 4, 2007 Glenohumeral Internal Rotation Deficits 1 APPENDIX: The Houston Astros Stretching Program Our Flexibility program consists of 5 positions. Four of the 5 have 2 variations of each position.
Vol. 35, No. 4, 2007 Glenohumeral Internal Rotation Deficits 1 APPENDIX: The Houston Astros Stretching Program Our Flexibility program consists of 5 positions. Four of the 5 have 2 variations of each position.
Anterior Cruciate Ligament Hamstring Rehabilitation Protocol
 Anterior Cruciate Ligament Hamstring Rehabilitation Protocol Focus on exercise quality avoid overstressing the donor area while it heals. Typically, isolated hamstring strengthening begins after the 6
Anterior Cruciate Ligament Hamstring Rehabilitation Protocol Focus on exercise quality avoid overstressing the donor area while it heals. Typically, isolated hamstring strengthening begins after the 6
Hip Arthroscopy Femoroacetabular Impingement (FAI) Ryan W. Hess, MD Tracey Pederson, PCC Office: (763) Fax: (763)
 Ryan W. Hess, MD Tracey Pederson, PCC Office: (763) Fax: (763)") Hip Arthroscopy Femoroacetabular Impingement (FAI) Ryan W. Hess, MD Tracey Pederson, PCC Office: (763) 302-2223 Fax: (763) 302-2401 GENERAL GUIDELINES: Despite the minimally invasive nature of hip arthroscopy,
Hip Arthroscopy Femoroacetabular Impingement (FAI) Ryan W. Hess, MD Tracey Pederson, PCC Office: (763) 302-2223 Fax: (763) 302-2401 GENERAL GUIDELINES: Despite the minimally invasive nature of hip arthroscopy,
ANTERIOR CRUCTIATE LIGAMENT RECONSTRUCTION COLLATERAL LIGAMENT RECONSTRUCION/REPAIR AND MENISCUS REPAIR REHABILITATION PROTOCOL
 ANTERIOR CRUCTIATE LIGAMENT RECONSTRUCTION COLLATERAL LIGAMENT RECONSTRUCION/REPAIR AND MENISCUS REPAIR REHABILITATION PROTOCOL GENERAL GUIDELINES - The local anesthetic (similar to novacaine) in your
ANTERIOR CRUCTIATE LIGAMENT RECONSTRUCTION COLLATERAL LIGAMENT RECONSTRUCION/REPAIR AND MENISCUS REPAIR REHABILITATION PROTOCOL GENERAL GUIDELINES - The local anesthetic (similar to novacaine) in your
History Prior to Presenting to Us
 2013 Part 3 Cox Certification in Maui Case Report Chronic Severe S Scoliosis (Lumbar dextroscoliosis and Thoracic levoscoliosis) treated successfully using Chiropractic for over 30 years and Cox Technic
2013 Part 3 Cox Certification in Maui Case Report Chronic Severe S Scoliosis (Lumbar dextroscoliosis and Thoracic levoscoliosis) treated successfully using Chiropractic for over 30 years and Cox Technic
Stiff Ribs can cause pain in the LEGS!
 Stiff Ribs can cause pain in the LEGS! Presenter: Kym Finch 2018 Massage and Myotherapy Australia Conference Gold Coast Outcomes Challenge Teach Develop Challenge your thought process Teach new skills
Stiff Ribs can cause pain in the LEGS! Presenter: Kym Finch 2018 Massage and Myotherapy Australia Conference Gold Coast Outcomes Challenge Teach Develop Challenge your thought process Teach new skills
Anterior Labrum Repair Protocol
 Anterior Labrum Repair Protocol Stage I (0-4 weeks): Key Goals: Protect the newly repaired shoulder. Allow for decreased inflammation and healing. Maintain elbow, wrist and hand function. Maintain scapular
Anterior Labrum Repair Protocol Stage I (0-4 weeks): Key Goals: Protect the newly repaired shoulder. Allow for decreased inflammation and healing. Maintain elbow, wrist and hand function. Maintain scapular
Adolescent Idiopathic Scoliosis
 Adolescent Idiopathic Scoliosis Adolescent idiopathic scoliosis is characterized by a lateral bending and twisting of the spine. It is the most common spinal deformity affecting adolescents 10 to 16 years
Adolescent Idiopathic Scoliosis Adolescent idiopathic scoliosis is characterized by a lateral bending and twisting of the spine. It is the most common spinal deformity affecting adolescents 10 to 16 years
Labral Repair with a Microfracture
 Labral Repair with a Microfracture This protocol should be used as a guideline for progression and should be tailored to the needs of the individual patient. Strict protective weight bearing status for
Labral Repair with a Microfracture This protocol should be used as a guideline for progression and should be tailored to the needs of the individual patient. Strict protective weight bearing status for
Arthroscopic Bankart Repair Rehabilitation Protocol Dr. Mark Adickes
 Arthroscopic Bankart Repair Rehabilitation Protocol Dr. Mark Adickes Introduction: This rehabilitation protocol has been developed for the patient following an arthroscopic Bankart (anteroinferior labral
Arthroscopic Bankart Repair Rehabilitation Protocol Dr. Mark Adickes Introduction: This rehabilitation protocol has been developed for the patient following an arthroscopic Bankart (anteroinferior labral
BANKART REPAIR PROTOCOL
 BANKART REPAIR PROTOCOL Clarkstown Division This rehabilitation protocol has been developed for the patient following Bankart surgical procedure for anterior shoulder instability. The protocol is divided
BANKART REPAIR PROTOCOL Clarkstown Division This rehabilitation protocol has been developed for the patient following Bankart surgical procedure for anterior shoulder instability. The protocol is divided
ARTHROSCOPIC DECOMPRESSION PROTOCOL Dr. Steven Flores
 ARTHROSCOPIC DECOMPRESSION PROTOCOL Dr. Steven Flores This rehabilitation protocol has been developed for the patient following an arthroscopic decompression surgical procedure. The arthroscopic decompression
ARTHROSCOPIC DECOMPRESSION PROTOCOL Dr. Steven Flores This rehabilitation protocol has been developed for the patient following an arthroscopic decompression surgical procedure. The arthroscopic decompression
SLAP LESION REPAIR PROTOCOL
 SLAP LESION REPAIR PROTOCOL Clarkstown Division This rehabilitation protocol has been developed for the patient following a SLAP (Superior Labrum Anterior Posterior) repair. It is extremely important to
SLAP LESION REPAIR PROTOCOL Clarkstown Division This rehabilitation protocol has been developed for the patient following a SLAP (Superior Labrum Anterior Posterior) repair. It is extremely important to
Rehabilitation Guidelines for Anterior Cruciate Ligament (ACL) Reconstruction
 Reconstruction") Rehabilitation Guidelines for Anterior Cruciate Ligament (ACL) Reconstruction The knee is the body's largest joint, and the place where the femur, tibia, and patella meet to form a hinge-like joint. These
Rehabilitation Guidelines for Anterior Cruciate Ligament (ACL) Reconstruction The knee is the body's largest joint, and the place where the femur, tibia, and patella meet to form a hinge-like joint. These
Rotator Cuff Repair Protocol
 Protocol This rehabilitation protocol has been developed for the patient following a rotator cuff surgical procedure. This protocol will vary in length and aggressiveness depending on factors such as:
Protocol This rehabilitation protocol has been developed for the patient following a rotator cuff surgical procedure. This protocol will vary in length and aggressiveness depending on factors such as:
Alejandro Verdugo m.d.
 Alejandro Verdugo m.d. Proximal Hamstring Rupture: Physical Therapy Protocol The intent of this protocol is to provide guidelines for your patient s therapy progression. It is not intended to serve as
Alejandro Verdugo m.d. Proximal Hamstring Rupture: Physical Therapy Protocol The intent of this protocol is to provide guidelines for your patient s therapy progression. It is not intended to serve as
Arthroscopic Rotator Cuff Repair Protocol:
 Arthroscopic Rotator Cuff Repair Protocol: The intent of this protocol is to provide the therapist and patient with guidelines for the post-operative rehabilitation course after arthroscopic SLAP repair.
Arthroscopic Rotator Cuff Repair Protocol: The intent of this protocol is to provide the therapist and patient with guidelines for the post-operative rehabilitation course after arthroscopic SLAP repair.
Cervical Spine Exercise and Manual Therapy for the Autonomous Practitioner
 Cervical Spine Exercise and Manual Therapy for the Autonomous Practitioner Eric Chaconas PT, PhD, DPT, FAAOMPT Assistant Professor and Assistant Program Director Doctor of Physical Therapy Program Eric
Cervical Spine Exercise and Manual Therapy for the Autonomous Practitioner Eric Chaconas PT, PhD, DPT, FAAOMPT Assistant Professor and Assistant Program Director Doctor of Physical Therapy Program Eric
Microfracture. This protocol should be used as a guideline for progression and should be tailored to the needs of the individual patient.
 This protocol should be used as a guideline for progression and should be tailored to the needs of the individual patient. Strict protective weight bearing status for two months (8-9 weeks). Allow to place
This protocol should be used as a guideline for progression and should be tailored to the needs of the individual patient. Strict protective weight bearing status for two months (8-9 weeks). Allow to place
Thoracolumbar Spine Conditions: Treatment and Return to Play
 Thoracolumbar Spine Conditions: Treatment and Return to Play C H R I S T O P H E R B U R K S, MD B I E N V I L L E O R T H O P A E D I C S P E C I A L I S T S O C E A N S P R I N G S, MS Thoracolumbar
Thoracolumbar Spine Conditions: Treatment and Return to Play C H R I S T O P H E R B U R K S, MD B I E N V I L L E O R T H O P A E D I C S P E C I A L I S T S O C E A N S P R I N G S, MS Thoracolumbar
The SOSORT Educational Committee
 The SOSORT Educational Committee Presents: Adult Scoliosis (AS) Rehabilitation: Select Case Histories Illustrating Treatment Options for Adults with Scoliosis and Related Complexities ELENA SALVÀ INSTITUT
The SOSORT Educational Committee Presents: Adult Scoliosis (AS) Rehabilitation: Select Case Histories Illustrating Treatment Options for Adults with Scoliosis and Related Complexities ELENA SALVÀ INSTITUT
ACL and Knee Injury Prevention. Presented by: Zach Kirkpatrick, PT, MPT, SCS
 ACL and Knee Injury Prevention Presented by: Zach Kirkpatrick, PT, MPT, SCS ACL Anatomy ACL Mechanism of Injury Contact ACL Tear Noncontact ACL Tear ACL MOI and Pathology Common in young individual who
ACL and Knee Injury Prevention Presented by: Zach Kirkpatrick, PT, MPT, SCS ACL Anatomy ACL Mechanism of Injury Contact ACL Tear Noncontact ACL Tear ACL MOI and Pathology Common in young individual who
Outline. Training Interventions for Youth Baseball Athletes. 3 Rehabilitation Focus Points. What Training to Perform?
 Outline Training Interventions for Youth Baseball Athletes Tim L. Uhl PhD ATC PT FNATA Division of Athletic Training Department of Rehabilitation Sciences College of Health Sciences University of Kentucky
Outline Training Interventions for Youth Baseball Athletes Tim L. Uhl PhD ATC PT FNATA Division of Athletic Training Department of Rehabilitation Sciences College of Health Sciences University of Kentucky
S p o r t s & O r t h o p a e d i c S p e c i a l i s t s D R. R Y A N F A D E R
 S p o r t s & O r t h o p a e d i c S p e c i a l i s t s D R. R Y A N F A D E R H I P A R T H R O S C O P Y W I T H This protocol provides appropriate guidelines for the rehabilitation of patients following
S p o r t s & O r t h o p a e d i c S p e c i a l i s t s D R. R Y A N F A D E R H I P A R T H R O S C O P Y W I T H This protocol provides appropriate guidelines for the rehabilitation of patients following
Rehab protocol. Phase I: Immediate Post-Surgical Phase: Typically 0-4 weeks; 2 PT visits. Goals:
 Reverse Total shoulder arthroplasty Rehab protocol Phase I: Immediate Post-Surgical Phase: Typically 0-4 weeks; 2 PT visits Allow healing of soft tissue Maintain integrity of replaced joint Gradually increase
Reverse Total shoulder arthroplasty Rehab protocol Phase I: Immediate Post-Surgical Phase: Typically 0-4 weeks; 2 PT visits Allow healing of soft tissue Maintain integrity of replaced joint Gradually increase
Cervical Spine in Baseball
 Cervical Spine in Baseball Robert G Watkins, IV, MD Co-Director, Marina Spine Center Marina del Rey, CA Vice Chief of Staff Cedars-Marina del Rey Hospital Disclosures n Pioneer / RTI Consulting, Royalties
Cervical Spine in Baseball Robert G Watkins, IV, MD Co-Director, Marina Spine Center Marina del Rey, CA Vice Chief of Staff Cedars-Marina del Rey Hospital Disclosures n Pioneer / RTI Consulting, Royalties
Hip Arthroscopy Rehabilitation Protocol
 Hip Arthroscopy Rehabilitation Protocol 1. Concepts: a. Range of motion and weight bearing restrictions must be adhered to during the initial rehab process (4 total weeks of ROM and weight bearing restrictions)
Hip Arthroscopy Rehabilitation Protocol 1. Concepts: a. Range of motion and weight bearing restrictions must be adhered to during the initial rehab process (4 total weeks of ROM and weight bearing restrictions)
Medial Collateral Ligament Repair Protocol-Dr. McClung
 Medial Collateral Ligament Repair Protocol-Dr. McClung Brace: Normally patients will be wearing post-op knee brace locked in 30 degrees for ambulation and sleeping but drop-locked for sitting and knee
Medial Collateral Ligament Repair Protocol-Dr. McClung Brace: Normally patients will be wearing post-op knee brace locked in 30 degrees for ambulation and sleeping but drop-locked for sitting and knee
Proximal Hamstring Rupture: Physical Therapy Protocol
 Proximal Hamstring Rupture: Physical Therapy Protocol The intent of this protocol is to provide guidelines for your patient s therapy progression. It is not intended to serve as a recipe for treatment.
Proximal Hamstring Rupture: Physical Therapy Protocol The intent of this protocol is to provide guidelines for your patient s therapy progression. It is not intended to serve as a recipe for treatment.
Shoulder Arthroscopy with Rotator Cuff Repair Rehabilitation Protocol
 General Notes: As tolerated should be understood to include with safety for the surgical procedure; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing too
General Notes: As tolerated should be understood to include with safety for the surgical procedure; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing too
ACL Rehabilitation Guidelines
 ACL Rehabilitation Guidelines General Information: These guidelines have been developed to service the spectrum of ACL injured people (non-athlete elite athlete). For this reason, example exercises are
ACL Rehabilitation Guidelines General Information: These guidelines have been developed to service the spectrum of ACL injured people (non-athlete elite athlete). For this reason, example exercises are
l. Initiate early proprioceptive activity and progress by means of distraction techniques: i. eyes open to eyes closed ii. stable to unstable m.
 Meniscus Repair 1. Defined a. Sutures or bioabsorbable fixation devices (arrows, darts, screws, etc.) bring together and fixate the edges of a tear in the meniscus in order to maintain the shock absorption
Meniscus Repair 1. Defined a. Sutures or bioabsorbable fixation devices (arrows, darts, screws, etc.) bring together and fixate the edges of a tear in the meniscus in order to maintain the shock absorption
Hip Arthroscopy Rehabilitation Gluteus Medius Repair with or without Labral Debridement. Normalize gait pattern with brace (if indicated) and crutches
 and crutches") General Guidelines: Hip Arthroscopy Rehabilitation Gluteus Medius Repair with or without Labral Debridement Normalize gait pattern with brace (if indicated) and crutches Weight-bearing: 20 lbs foot flat
General Guidelines: Hip Arthroscopy Rehabilitation Gluteus Medius Repair with or without Labral Debridement Normalize gait pattern with brace (if indicated) and crutches Weight-bearing: 20 lbs foot flat
Meniscus Repair Rehabilitation Protocol
 Meniscus Repair Rehabilitation Protocol GENERAL GUIDELINES - Use the cryotherapy cuff continuously for the first 72 hours, then as needed thereafter - Ensure that the cuff never contacts the skin directly
Meniscus Repair Rehabilitation Protocol GENERAL GUIDELINES - Use the cryotherapy cuff continuously for the first 72 hours, then as needed thereafter - Ensure that the cuff never contacts the skin directly
Functional Movement Screen (Cook, 2001)
") Functional Movement Screen (Cook, 2001) TEST 1 DEEP SQUAT Purpose - The Deep Squat is used to assess bilateral, symmetrical, mobility of the hips, knees, and ankles. The dowel held overhead assesses bilateral,
Functional Movement Screen (Cook, 2001) TEST 1 DEEP SQUAT Purpose - The Deep Squat is used to assess bilateral, symmetrical, mobility of the hips, knees, and ankles. The dowel held overhead assesses bilateral,
LEG LENGTH INEQUALITY: Sports Medicine Perspective
 LEG LENGTH INEQUALITY: Sports Medicine Perspective Debra A. Zillmer, M.D. M&M Orthopaedics, Ltd 18 Year Old Experienced Cross Country Runner: Sept Sr Year Pain in left lower leg with running Pain now prevents
LEG LENGTH INEQUALITY: Sports Medicine Perspective Debra A. Zillmer, M.D. M&M Orthopaedics, Ltd 18 Year Old Experienced Cross Country Runner: Sept Sr Year Pain in left lower leg with running Pain now prevents
THE OLDER TENNIS AND GOLF ATHLETE: INJURY MANAGEMENT AND PREVENTION
 THE OLDER TENNIS AND GOLF ATHLETE: INJURY MANAGEMENT AND PREVENTION William Micheo, MD Professor and Chairman Physical Medicine, Rehabilitation, and Sports Medicine Department University of Puerto Rico
THE OLDER TENNIS AND GOLF ATHLETE: INJURY MANAGEMENT AND PREVENTION William Micheo, MD Professor and Chairman Physical Medicine, Rehabilitation, and Sports Medicine Department University of Puerto Rico
10/5/2017. Cervical Manual Evaluation and Mobilizations. Upper Cervical Stability Testing Alar Ligament
 Cervical Manual Evaluation and Mobilizations Upper Cervical Stability Testing Alar Ligament Upper Cervical Stability Testing Transverse Ligament 1 Upper Cervical Stability Testing Transverse Plane Positive
Cervical Manual Evaluation and Mobilizations Upper Cervical Stability Testing Alar Ligament Upper Cervical Stability Testing Transverse Ligament 1 Upper Cervical Stability Testing Transverse Plane Positive
Overhead Athlete Rehabilitation Guidelines
 Overhead Athlete Rehabilitation Guidelines This document is designed to be used as a guideline in the rehabilitation of the athlete playing overhead sports, mainly baseball and softball, but also including
Overhead Athlete Rehabilitation Guidelines This document is designed to be used as a guideline in the rehabilitation of the athlete playing overhead sports, mainly baseball and softball, but also including
Superior Labrum Repair Protocol - SLAP
 Superior Labrum Repair Protocol - SLAP Stage I (0-4 weeks): Key Goals: Protect the newly repaired shoulder. Allow for decreased inflammation and healing. Maintain elbow, wrist and hand function. Maintain
Superior Labrum Repair Protocol - SLAP Stage I (0-4 weeks): Key Goals: Protect the newly repaired shoulder. Allow for decreased inflammation and healing. Maintain elbow, wrist and hand function. Maintain
DPT 772 Spine Notebook Matt Kubalski, SPT
 DPT 772 Spine Notebook Matt Kubalski, SPT Table of Contents: IMPAIRMENTS/CLASSIFICATIONS PAGES Neck Pain with Mobility Deficit: Cervicalgia, Pain in thoracic spine - JOSPT 3-6 Neck Pain with Headache:
DPT 772 Spine Notebook Matt Kubalski, SPT Table of Contents: IMPAIRMENTS/CLASSIFICATIONS PAGES Neck Pain with Mobility Deficit: Cervicalgia, Pain in thoracic spine - JOSPT 3-6 Neck Pain with Headache:
WHY BASIC HIP FLEXOR STRETCHES DON'T ALWAYS WORK
 WHY BASIC HIP FLEXOR STRETCHES DON'T ALWAYS WORK Do you do a daily stretching routine only to find that your muscles tighten back up throughout the day? Do you continue to stretch your hamstrings but still
WHY BASIC HIP FLEXOR STRETCHES DON'T ALWAYS WORK Do you do a daily stretching routine only to find that your muscles tighten back up throughout the day? Do you continue to stretch your hamstrings but still
SLAP LESION REPAIR PROTOCOL Dr. Steven Flores
 SLAP LESION REPAIR PROTOCOL Dr. Steven Flores This rehabilitation protocol has been developed for the patient following a SLAP (Superior Labrum Anterior Posterior) repair. It is extremely important to
SLAP LESION REPAIR PROTOCOL Dr. Steven Flores This rehabilitation protocol has been developed for the patient following a SLAP (Superior Labrum Anterior Posterior) repair. It is extremely important to
Latissimus dorsi tendon transfer protocol
 Department of Rehabilitation Services Physical Therapy The intent of this protocol is to provide the physical therapist with a guideline/treatment protocol for the postoperative rehabilitation management
Department of Rehabilitation Services Physical Therapy The intent of this protocol is to provide the physical therapist with a guideline/treatment protocol for the postoperative rehabilitation management
Rotator Cuff Repair Protocol
 Rotator Cuff Repair Protocol Overview a. Begin passive shoulder ROM after surgery (beginning week 1) b. Active assist ROM beginning week 7 after surgery (weeks 7-8) c. Active ROM beginning week 9 after
Rotator Cuff Repair Protocol Overview a. Begin passive shoulder ROM after surgery (beginning week 1) b. Active assist ROM beginning week 7 after surgery (weeks 7-8) c. Active ROM beginning week 9 after
Christopher K. Jones, MD Colorado Springs Orthopaedic Group
 Christopher K. Jones, MD Colorado Springs Orthopaedic Group 719-632-7669 Total Shoulder Replacement You have undergone a shoulder replacement procedure. The performance of the procedure is complete, but
Christopher K. Jones, MD Colorado Springs Orthopaedic Group 719-632-7669 Total Shoulder Replacement You have undergone a shoulder replacement procedure. The performance of the procedure is complete, but
Physical Therapy for the Lower Extremity: What You and Your Patient Should Expect from Rehab
 1 Physical Therapy for the Lower Extremity: What You and Your Patient Should Expect from Rehab Thomas Clennell, PT, DPT, SCS Physical Therapist UCSF Benioff Children s Hospital Oakland Sports Medicine
1 Physical Therapy for the Lower Extremity: What You and Your Patient Should Expect from Rehab Thomas Clennell, PT, DPT, SCS Physical Therapist UCSF Benioff Children s Hospital Oakland Sports Medicine
1-Apley scratch test.
 1-Apley scratch test. The patient attempts to touch the opposite scapula to test range of motion of the shoulder. 1-Testing abduction and external rotation( +ve sign touch the opposite scapula, -ve sign
1-Apley scratch test. The patient attempts to touch the opposite scapula to test range of motion of the shoulder. 1-Testing abduction and external rotation( +ve sign touch the opposite scapula, -ve sign
ULNAR COLLATERAL LIGAMENT (UCL) RECONSTRUCTION REHABILITATION PROTOCOL
 RECONSTRUCTION REHABILITATION PROTOCOL") General Notes As tolerated should be understood to include with safety for the surgical procedure; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing too
General Notes As tolerated should be understood to include with safety for the surgical procedure; a sudden increase in pain, swelling, or other undesirable factors are indicators that you are doing too
Become INJURY PROOF. Featuring Movement Based Healthcare and 5 Site Integrity. Get assessed and find answers
 Become INJURY PROOF Featuring Movement Based Healthcare and 5 Site Integrity Get assessed and find answers Postu Fits Toronto is the first facility of its kind in the world to use movement to assess and
Become INJURY PROOF Featuring Movement Based Healthcare and 5 Site Integrity Get assessed and find answers Postu Fits Toronto is the first facility of its kind in the world to use movement to assess and
Rehab and Return to Swimming for Breaststroker's Knee
 Page 1 of 9 Back Rehab and Return to Swimming for Breaststroker's Knee by June Quick, PT, ATC, CPI DIAGNOSIS Breaststrokers knee or sore knees from swimming usually involves inflammation around the kneecap.
Page 1 of 9 Back Rehab and Return to Swimming for Breaststroker's Knee by June Quick, PT, ATC, CPI DIAGNOSIS Breaststrokers knee or sore knees from swimming usually involves inflammation around the kneecap.
Sports Rehabilitation & Performance Center Rehabilitation Guidelines for Non-operative Treatment of Patellofemoral Instability *
 Sports Rehabilitation & Performance Center Rehabilitation Guidelines for Non-operative Treatment of The following guidelines were developed by the Sports Rehabilitation and Performance Center team at Hospital
Sports Rehabilitation & Performance Center Rehabilitation Guidelines for Non-operative Treatment of The following guidelines were developed by the Sports Rehabilitation and Performance Center team at Hospital
LOW BACK PAIN IN THE FEMALE ATHLETE: THROUGH
 LOW BACK PAIN IN THE FEMALE ATHLETE: THROUGH C THE AGES Rachel Brakke, MD Assistant Professor University of Colorado School of Medicine- Dept of Physical Medicine and Rehabilitation CU Sports Medicine
LOW BACK PAIN IN THE FEMALE ATHLETE: THROUGH C THE AGES Rachel Brakke, MD Assistant Professor University of Colorado School of Medicine- Dept of Physical Medicine and Rehabilitation CU Sports Medicine
The Four Phases of Healing During Rehabilitation Following Rotator Cuff Surgery. Phase 1: Immediate postoperative period (weeks 0-6) Goals
 Goals") The Four Phases of Healing During Rehabilitation Following Rotator Cuff Surgery Phase 1: Immediate postoperative period (weeks 0-6) Maintain/protect integrity of repair Gradually increase PROM Diminish
The Four Phases of Healing During Rehabilitation Following Rotator Cuff Surgery Phase 1: Immediate postoperative period (weeks 0-6) Maintain/protect integrity of repair Gradually increase PROM Diminish
Spinal Alignment and corrective exercise: The importance of posture in the frailer older adult.
 Later Life Training 2013 Conference Spinal Alignment and corrective exercise: The importance of posture in the frailer older adult. PRESENTED BY SHEILA DONE We are all aware why posture and muscle balance
Later Life Training 2013 Conference Spinal Alignment and corrective exercise: The importance of posture in the frailer older adult. PRESENTED BY SHEILA DONE We are all aware why posture and muscle balance
TOTAL SHOULDER ARTHROPLASTY, HEMIARTHROPLASTY OR REVERSE ARTHROPLASTY
 TOTAL SHOULDER ARTHROPLASTY, HEMIARTHROPLASTY OR REVERSE ARTHROPLASTY Philosophy The following is an outline of the standard post-operative rehabilitation program following total shoulder arthroplasty.
TOTAL SHOULDER ARTHROPLASTY, HEMIARTHROPLASTY OR REVERSE ARTHROPLASTY Philosophy The following is an outline of the standard post-operative rehabilitation program following total shoulder arthroplasty.
ACLR Protocol Hamstring Autograft. Name Date. Procedure. Frequency times/week Duration weeks
 Anthony Levenda M.D. Sports Medicine, Shoulder & Knee Reconstruction Direct Line (219) 395-2109 ACLR Protocol Hamstring Autograft Name Date Procedure Procedure Date Frequency 1 2 3 4 5 times/week Duration
Anthony Levenda M.D. Sports Medicine, Shoulder & Knee Reconstruction Direct Line (219) 395-2109 ACLR Protocol Hamstring Autograft Name Date Procedure Procedure Date Frequency 1 2 3 4 5 times/week Duration
Avon Office 2 Simsbury Rd. Avon, CT Office: (860) Fax: (860) REHABILITATION AFTER REVERSE SHOULDER ARTHROPLASTY
 Fax: (860) REHABILITATION AFTER REVERSE SHOULDER ARTHROPLASTY") Katherine J. Coyner, MD UCONN Musculoskeletal Institute Medical Arts & Research Building 263 Farmington Ave. Farmington, CT 06030 Office: (860) 679-6600 Fax: (860) 679-6649 www.drcoyner.com Avon Office
Katherine J. Coyner, MD UCONN Musculoskeletal Institute Medical Arts & Research Building 263 Farmington Ave. Farmington, CT 06030 Office: (860) 679-6600 Fax: (860) 679-6649 www.drcoyner.com Avon Office
3/10/17 Spinal a Injury 1
 Spinal Injury 1 'Paralysed' Watmough vows he'll have the backbone for Game Two after treatment for neck injury Watmough will have cortisone injected into his spine this morning to speed up the recovery
Spinal Injury 1 'Paralysed' Watmough vows he'll have the backbone for Game Two after treatment for neck injury Watmough will have cortisone injected into his spine this morning to speed up the recovery
POST-OPERATIVE REHABILITATION PROTOCOL FOLLOWING ULNAR COLLATERAL LIGAMENT RECONSTRUCTION USING AUTOGENOUS GRACILIS GRAFT
 Therapist POST-OPERATIVE REHABILITATION PROTOCOL FOLLOWING ULNAR COLLATERAL LIGAMENT RECONSTRUCTION USING AUTOGENOUS GRACILIS GRAFT I. IMMEDIATE POST-OPERATIVE PHASE (0-3 weeks) Protect healing tissue
Therapist POST-OPERATIVE REHABILITATION PROTOCOL FOLLOWING ULNAR COLLATERAL LIGAMENT RECONSTRUCTION USING AUTOGENOUS GRACILIS GRAFT I. IMMEDIATE POST-OPERATIVE PHASE (0-3 weeks) Protect healing tissue
Planning the Objective Exam. Objective Examination of the Cervical Spine. Clearing Tests. Observation. Functional Demonstration.
 Objective Examination of the Cervical Spine Taking the complaint and identifying the damaged structure Planning the Objective Exam With a clear picture from the subjective exam, the objective exam should
Objective Examination of the Cervical Spine Taking the complaint and identifying the damaged structure Planning the Objective Exam With a clear picture from the subjective exam, the objective exam should
Internal Rotation (turning toes/knee toward other leg) 30 degree limit. limit
 30 degree limit. limit") Hip Arthroscopy Patient Education Use of Brace and Crutches: - Wear the brace all times of weight bearing for the first 3 weeks after surgery. This is done to protect your hip and motion into hip extension
Hip Arthroscopy Patient Education Use of Brace and Crutches: - Wear the brace all times of weight bearing for the first 3 weeks after surgery. This is done to protect your hip and motion into hip extension
S p o r t s & O r t h o p a e d i c S p e c i a l i s t s C o n s e r v a t i v e M a s s i v e R o t a t o r C u f f T e a r P r o t o c o l
 S p o r t s & O r t h o p a e d i c S p e c i a l i s t s C o n s e r v a t i v e M a s s i v e R o t a t o r C u f f T e a r P r o t o c o l This protocol provides appropriate guidelines for the rehabilitation
S p o r t s & O r t h o p a e d i c S p e c i a l i s t s C o n s e r v a t i v e M a s s i v e R o t a t o r C u f f T e a r P r o t o c o l This protocol provides appropriate guidelines for the rehabilitation
Strategies for Pediatric Sports Rehabilitation. Marc Sherry PT, LAT, CSCS, PES
 Strategies for Pediatric Sports Rehabilitation Marc Sherry PT, LAT, CSCS, PES 11-14-08 4 Pediatric Rehab Goals 1. Create athlete centered / parent supported treatment and education 2. Understand differential
Strategies for Pediatric Sports Rehabilitation Marc Sherry PT, LAT, CSCS, PES 11-14-08 4 Pediatric Rehab Goals 1. Create athlete centered / parent supported treatment and education 2. Understand differential
Phase I : Immediate Postoperative Phase- Protected Motion. (0-2 Weeks)
") Phase I : Immediate Postoperative Phase- Protected Motion (0-2 Weeks) Appointments Progression Criteria 2 weeks after surgery Rehabilitation appointments begin within 7-10 days of surgery, continue 1-2
Phase I : Immediate Postoperative Phase- Protected Motion (0-2 Weeks) Appointments Progression Criteria 2 weeks after surgery Rehabilitation appointments begin within 7-10 days of surgery, continue 1-2
Dynamic Neural Mobilization as an Adjunct Intervention for a Patient with Cervical Radiculopathy: A Case Report.
 Dynamic Neural Mobilization as an Adjunct Intervention for a Patient with Cervical Radiculopathy: A. Kara Delie, SPT Kristine Erickson, PT, MS, NCS 1 Abstract: Title: Dynamic Neural Mobilization as an
Dynamic Neural Mobilization as an Adjunct Intervention for a Patient with Cervical Radiculopathy: A. Kara Delie, SPT Kristine Erickson, PT, MS, NCS 1 Abstract: Title: Dynamic Neural Mobilization as an
Summary Chart 1 2 months
 NEWBORN Physiological flexion provides stability for posture & random movements Neck righting Labyrinthine righting beginning in prone & supine Primary standing reaction Movements limited by available
NEWBORN Physiological flexion provides stability for posture & random movements Neck righting Labyrinthine righting beginning in prone & supine Primary standing reaction Movements limited by available
Clinical pearls for the shoulder/arm exam and the treatment. What is seeing youare you seeing it
 Clinical pearls for the shoulder/arm exam and the treatment What is seeing youare you seeing it W. Ben Kibler, MD Medical director Case 1 18 y/o R hand dominant high school pitcher, with 6 week hx gradual
Clinical pearls for the shoulder/arm exam and the treatment What is seeing youare you seeing it W. Ben Kibler, MD Medical director Case 1 18 y/o R hand dominant high school pitcher, with 6 week hx gradual
Improving the Functional Strategy of the Volleyball Athlete Ron Hruska, MPA, PT
 Improving the Functional Strategy of the Volleyball Athlete Ron Hruska, MPA, PT PREPARATION PHASE Individual examination, mechanical testing and tri-planar assessment. Frontal Plane Tests: Adduction Lift
Improving the Functional Strategy of the Volleyball Athlete Ron Hruska, MPA, PT PREPARATION PHASE Individual examination, mechanical testing and tri-planar assessment. Frontal Plane Tests: Adduction Lift
Hip Arthroscopy with CAM resection/labral Repair Protocol
 Hip Arthroscopy with CAM resection/labral Repair Protocol As tolerated should be understood to perform with safety for the reconstruction/repair. Pain, limp, swelling, or other undesirable factors are
Hip Arthroscopy with CAM resection/labral Repair Protocol As tolerated should be understood to perform with safety for the reconstruction/repair. Pain, limp, swelling, or other undesirable factors are